Embed Size (px)
Citation preview

Thromboxane Receptors Antagonists
and/or Synthase Inhibitors
Giovanni Davı, Francesca Santilli, and Natale Vazzana
Contents
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 262
2 TP Receptors and Their Antagonism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
2.1 Molecular and Cellular Biology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
2.2 TP Receptor Signaling in Platelets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 265
2.3 TP Receptor Signaling in Vascular Endothelial
and Smooth Muscle Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
3 Drugs Affecting TXA2 Action: Other than COX Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
3.1 Inhibitors of Thromboxane Synthase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
3.2 Dual TXS Inhibition/TP Antagonism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268
4 Dual COXIB/TP Antagonists: A Possible New Twist in NSAID Pharmacology and
Cardiovascular Risk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 270
4.1 TP Antagonists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 271
5 Pathophysiological Rationale for the Superiority of TP-Receptor Antagonists Over
Aspirin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272
5.1 Advantages as an Antithrombotic Agent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272
5.2 Relevance of TP Receptors Inhibition in Atherosclerotic Disease . . . . . . . . . . . . . . . . . . 274
5.3 Ischemic Stroke: The Reasons of a Choice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 275
6 Great Expectations Disappointed: Did Terutroban
Fail to Perform, or PERFORM Did Fail? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 276
6.1 Preliminary Data Revisited . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 276
6.2 The PERFORM Design Revisited . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 278
7 Future Perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 279
8 Conclusions and Implications for Clinical Usefulness
of TP Antagonists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 282
G. Davı (*) • F. Santilli • N. Vazzana
Internal Medicine, University of Chieti, Chieti, Italy
e-mail: [email protected]
P. Gresele et al. (eds.), Antiplatelet Agents, Handbook of Experimental
Pharmacology 210, DOI 10.1007/978-3-642-29423-5_11,# Springer-Verlag Berlin Heidelberg 2012
261
Abstract Atherothrombosis is the major cause of mortality and morbidity in
Western countries. Several clinical conditions are characterized by increased inci-
dence of cardiovascular events and enhanced thromboxane (TX)-dependent platelet
activation. Enhanced TX generation may be explained by mechanisms relatively
insensitive to aspirin. More potent drugs possibly overcoming aspirin efficacy may
be desirable. Thromboxane synthase inhibitors (TXSI) and thromboxane receptor
antagonists (TXRA) have the potential to prove more effective than aspirin due to
their different mechanism of action along the pathway of TXA2. TXSI prevent the
conversion of PGH2 to TXA2, reducing TXA2 synthesis mainly in platelets, whereas
TXRA block the downstream consequences of TXA2 receptors (TP) activation.
TXA2 is a potent inducer of platelet activation through its interaction with TP on
platelets. TP are activated not only by TXA2, but also by prostaglandin (PG) D2,
PGE2, PGF2a, PGH2, PG endoperoxides (i.e., 20-HETE), and isoprostanes, all
representing aspirin-insensitive mechanisms of TP activation. Moreover, TP are
also expressed on several cell types such as macrophages or monocytes, and
vascular endothelial cells, and exert antiatherosclerotic, antivasoconstrictive, and
antithrombotic effects, depending on the cellular target.
Thus, targeting TP receptor, a common downstream pathway for both platelet
and extraplatelet TXA2 aswell as for endoperoxides and isoprostanes, may be a useful
antiatherosclerotic and a more powerful antithrombotic intervention in clinical
settings, such as diabetes mellitus, characterized by persistently enhanced
thromboxane (TX)-dependent platelet activation through isoprostane formation and
low-grade inflammation, leading to extraplatelet sources of TXA2. Among TXRA,
terutroban is an orally active drug in clinical development for use in secondary
prevention of thrombotic events in cardiovascular disease. Despite great expectations
on this drug supported by a large body of preclinical and clinical evidence and
pathophysiological rationale, the PERFORM trial failed to demonstrate the superior-
ity of terutroban over aspirin in secondary prevention of cerebrovascular and cardio-
vascular events among ~20,000 patients with stroke. However, the clinical setting and
the design of the study in which the drug has been challenged may explain, at least in
part, this unexpected finding.
Drugs with dual action, such as dual TXS inhibitors/TP antagonist and dual
COXIB/TP antagonists are currently in clinical development. The theoretical
rationale for their benefit and the ongoing clinical studies are herein discussed.
Keywords Antiplatelet therapy • Atherothrombosis • Ischemic stroke • Platelet
activation • Thromboxane biosynthesis • TP antagonists
1 Introduction
Atherosclerosis and its clinical manifestations (i.e., ischemic heart disease, cere-
brovascular or peripheral artery disease) are major causes of mortality and morbid-
ity in Western countries.
262 G. Davı et al.
Conventional antiplatelet agents such as aspirin or clopidogrel are currently used
in the prevention of cardiovascular events. However, more effective drugs with less
bleeding or gastrointestinal complications are desirable.
Thromboxane (TX) A2 is involved in a diverse range of physiological and
pathophysiological processes, including thrombosis, asthma, myocardial infarction
(MI), inflammation, acquired immunity, and atherogenesis. Thus, the stimulation of
TX/endoperoxide receptors (TP) elicits diverse biological effects under both nor-
mal and pathological conditions. Stimulation of TP results in activation of different
signaling cascades that regulate the cytoskeleton, cell adhesion, motility, nuclear
transcription factors, proliferation, cell survival, and apoptosis (Nakahata 2008).
TXA2 is the major product of the arachidonic acid (AA) metabolism in platelets
that, in response to various stimuli, is produced via the consequent actions of
cyclooxygenase (COX) and TX synthase (TXS). Through its interaction with TP
receptors on platelets, TXA2 is a potent inducer of platelet activation (Davı and
Patrono 2007).
Furthermore, the activation of endothelial TP promotes the expression of adhe-
sion molecules and favors adhesion and infiltration of monocytes/macrophages. TP
receptors exhibit a wide distribution within the cardiovascular system; in fact, these
receptors are membrane-bound G protein-coupled receptors (GPCR) found not only
on platelets but also on circulating inflammatory cells, such as macrophages or
monocytes, and in vascular endothelial cells, and smooth muscle cells (Meja et al.
1997; Miggin and Kinsella 1998).
Thus, antagonists of TP may have some advantages over aspirin as they not only
block the effect of TXA2 on platelets, but also inhibit other ligands such as
prostaglandin (PG) endoperoxides and isoprostanes. Because of the wide distribu-
tion of TP receptors in platelets, in the vascular wall or in atherosclerotic plaques,
TP antagonists inhibit also the effects of TXA2 over TP receptors on vascular cells
or in the plaque. Therefore, antagonists of TP receptors may not only have
antiplatelet effects but also impact endothelial dysfunction and the inflammatory
component of atherosclerosis (Chamorro 2009).
2 TP Receptors and Their Antagonism
2.1 Molecular and Cellular Biology
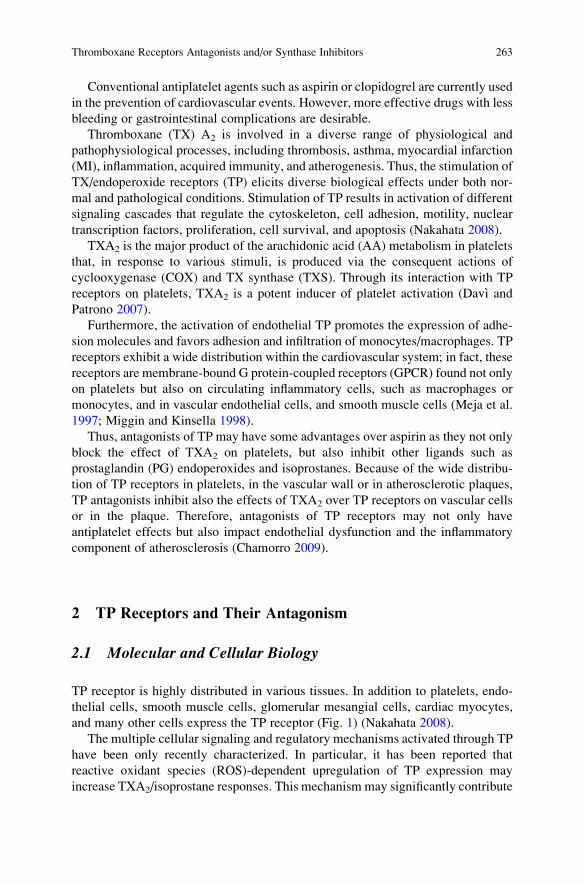
TP receptor is highly distributed in various tissues. In addition to platelets, endo-
thelial cells, smooth muscle cells, glomerular mesangial cells, cardiac myocytes,
and many other cells express the TP receptor (Fig. 1) (Nakahata 2008).
The multiple cellular signaling and regulatory mechanisms activated through TP
have been only recently characterized. In particular, it has been reported that
reactive oxidant species (ROS)-dependent upregulation of TP expression may
increase TXA2/isoprostane responses. This mechanism may significantly contribute
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 263
to platelet activation and atherothrombosis in several clinical setting associated
with enhanced oxidative stress, such as hypercholesterolemia, obesity, and type
2 diabetes mellitus (T2DM). In addition, posttranscriptional modifications of the
receptor, such as phosphorylation or glycation, also determine TP internalization or
ligand desensitization. Whether a TP antagonist may affect this receptorial cross-
talk and these regulatory pathways is still unanswered.
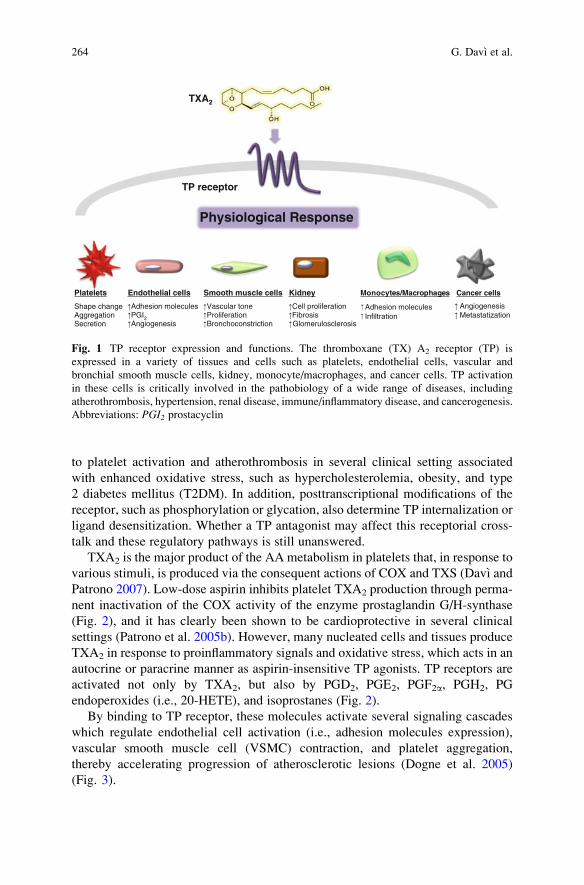
TXA2 is the major product of the AA metabolism in platelets that, in response to
various stimuli, is produced via the consequent actions of COX and TXS (Davı and
Patrono 2007). Low-dose aspirin inhibits platelet TXA2 production through perma-
nent inactivation of the COX activity of the enzyme prostaglandin G/H-synthase
(Fig. 2), and it has clearly been shown to be cardioprotective in several clinical
settings (Patrono et al. 2005b). However, many nucleated cells and tissues produce
TXA2 in response to proinflammatory signals and oxidative stress, which acts in an
autocrine or paracrine manner as aspirin-insensitive TP agonists. TP receptors are
activated not only by TXA2, but also by PGD2, PGE2, PGF2a, PGH2, PG
endoperoxides (i.e., 20-HETE), and isoprostanes (Fig. 2).
By binding to TP receptor, these molecules activate several signaling cascades
which regulate endothelial cell activation (i.e., adhesion molecules expression),
vascular smooth muscle cell (VSMC) contraction, and platelet aggregation,
thereby accelerating progression of atherosclerotic lesions (Dogne et al. 2005)
(Fig. 3).
Platelets
Shape changeAggregationSecretion
Endothelial cells
Adhesion moleculesPGI2Angiogenesis
Smooth muscle cells
Vascular toneProliferationBronchoconstriction
Physiological Response
TP receptor
Kidney
Cell proliferationFibrosisGlomerulosclerosis
Cancer cells
AngiogenesisMetastatization
TXA2
Monocytes/Macrophages
Adhesion moleculesInfiltration
Fig. 1 TP receptor expression and functions. The thromboxane (TX) A2 receptor (TP) is
expressed in a variety of tissues and cells such as platelets, endothelial cells, vascular and
bronchial smooth muscle cells, kidney, monocyte/macrophages, and cancer cells. TP activation
in these cells is critically involved in the pathobiology of a wide range of diseases, including
atherothrombosis, hypertension, renal disease, immune/inflammatory disease, and cancerogenesis.
Abbreviations: PGI2 prostacyclin
264 G. Davı et al.
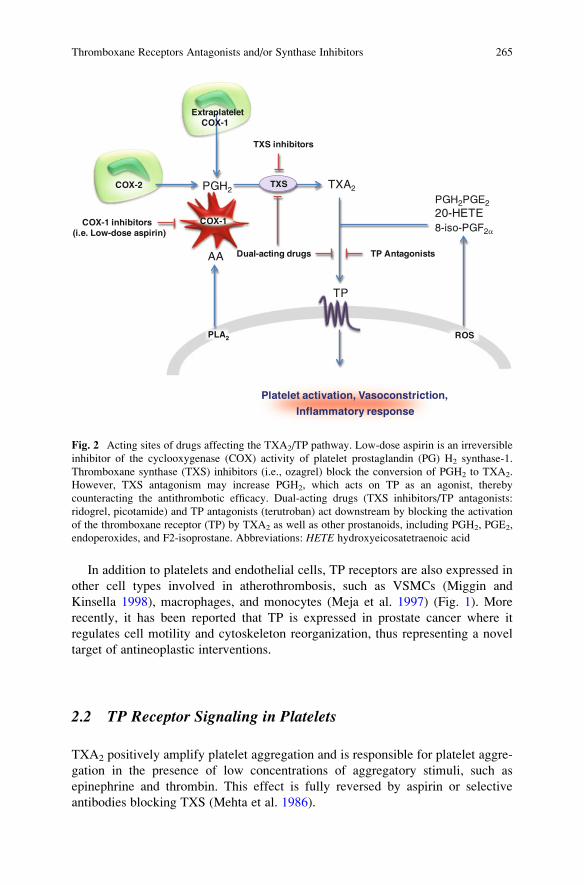
In addition to platelets and endothelial cells, TP receptors are also expressed in
other cell types involved in atherothrombosis, such as VSMCs (Miggin and
Kinsella 1998), macrophages, and monocytes (Meja et al. 1997) (Fig. 1). More
recently, it has been reported that TP is expressed in prostate cancer where it
regulates cell motility and cytoskeleton reorganization, thus representing a novel
target of antineoplastic interventions.
2.2 TP Receptor Signaling in Platelets
TXA2 positively amplify platelet aggregation and is responsible for platelet aggre-
gation in the presence of low concentrations of aggregatory stimuli, such as
epinephrine and thrombin. This effect is fully reversed by aspirin or selective
antibodies blocking TXS (Mehta et al. 1986).
PLA2
AA
PGH2 TXA2
TP
COX-1
TXS
COX-1 inhibitors(i.e. Low-dose aspirin)
TXS inhibitors
TP Antagonists
ROS
PGH2PGE220-HETE 8-iso-PGF2a
Dual-acting drugs
Platelet activation, Vasoconstriction,
Inflammatory response
ExtraplateletCOX-1
COX-2
Fig. 2 Acting sites of drugs affecting the TXA2/TP pathway. Low-dose aspirin is an irreversible
inhibitor of the cyclooxygenase (COX) activity of platelet prostaglandin (PG) H2 synthase-1.
Thromboxane synthase (TXS) inhibitors (i.e., ozagrel) block the conversion of PGH2 to TXA2.
However, TXS antagonism may increase PGH2, which acts on TP as an agonist, thereby
counteracting the antithrombotic efficacy. Dual-acting drugs (TXS inhibitors/TP antagonists:
ridogrel, picotamide) and TP antagonists (terutroban) act downstream by blocking the activation
of the thromboxane receptor (TP) by TXA2 as well as other prostanoids, including PGH2, PGE2,
endoperoxides, and F2-isoprostane. Abbreviations: HETE hydroxyeicosatetraenoic acid
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 265
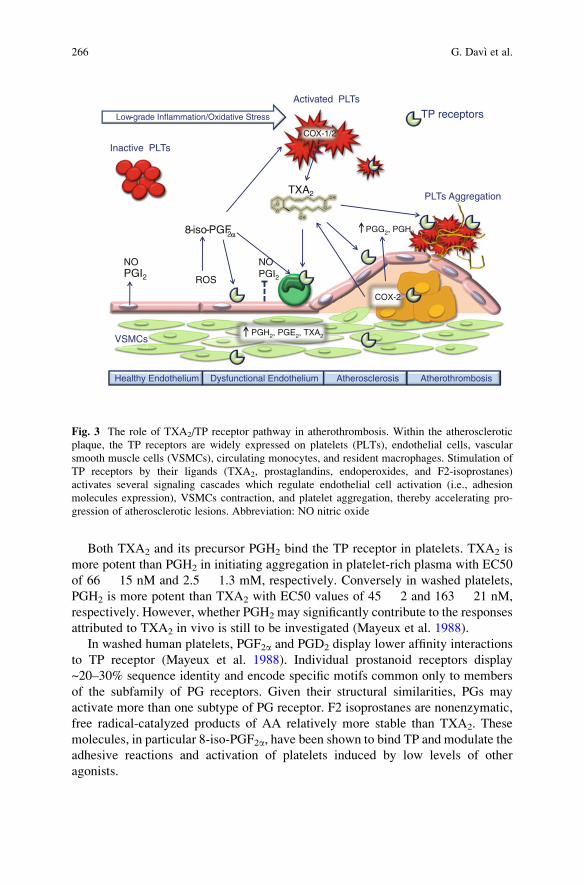
Both TXA2 and its precursor PGH2 bind the TP receptor in platelets. TXA2 is
more potent than PGH2 in initiating aggregation in platelet-rich plasma with EC50
of 66 � 15 nM and 2.5 � 1.3 mM, respectively. Conversely in washed platelets,
PGH2 is more potent than TXA2 with EC50 values of 45 � 2 and 163 � 21 nM,
respectively. However, whether PGH2 may significantly contribute to the responses
attributed to TXA2 in vivo is still to be investigated (Mayeux et al. 1988).
In washed human platelets, PGF2a and PGD2 display lower affinity interactions
to TP receptor (Mayeux et al. 1988). Individual prostanoid receptors display
~20–30% sequence identity and encode specific motifs common only to members
of the subfamily of PG receptors. Given their structural similarities, PGs may
activate more than one subtype of PG receptor. F2 isoprostanes are nonenzymatic,
free radical-catalyzed products of AA relatively more stable than TXA2. These
molecules, in particular 8-iso-PGF2a, have been shown to bind TP and modulate the
adhesive reactions and activation of platelets induced by low levels of other
agonists.
Inactive PLTs
Activated PLTs
PGH2, PGE2, TXA2
ROS
TP receptors
Atherothrombosis
NO NOPGI2
Dysfunctional Endothelium
PLTs Aggregation
Healthy Endothelium
Low-grade Inflammation/Oxidative Stress
COX-2
COX-1/2
8-iso-PGF2
TXA2
2, PGH2PGG2, PGH2
PGI2
Atherosclerosis
VSMCs
Fig. 3 The role of TXA2/TP receptor pathway in atherothrombosis. Within the atherosclerotic
plaque, the TP receptors are widely expressed on platelets (PLTs), endothelial cells, vascular
smooth muscle cells (VSMCs), circulating monocytes, and resident macrophages. Stimulation of
TP receptors by their ligands (TXA2, prostaglandins, endoperoxides, and F2-isoprostanes)
activates several signaling cascades which regulate endothelial cell activation (i.e., adhesion
molecules expression), VSMCs contraction, and platelet aggregation, thereby accelerating pro-
gression of atherosclerotic lesions. Abbreviation: NO nitric oxide
266 G. Davı et al.
2.3 TP Receptor Signaling in Vascular Endothelialand Smooth Muscle Cells
Increased vascular tone due to generation of prostanoids is a main feature of
endothelial dysfunction. In fact, endothelium dysfunction is characterized by an
increased production of prostanoids (i.e., TXA2), which facilitate the penetration of
macrophages in the vessel wall (Feletou et al. 2009). On endothelial cells, TXA2
activates the expression of adhesion proteins, such as ICAM-1, VCAM-1, and
endothelial leukocyte adhesion molecule-1 (ELAM-1) (Ishizuka et al. 1996). TP-
receptor dependent expression of ICAM-1, VCAM-1, and ELAM-1 is mediated by
protein kinase C (Ishizuka et al. 1998). TP activation also stimulates the expression
of leukocytes adhesion molecules (LAM) on endothelial cells (Ashton et al. 2003).
TP activation also promotes prostacyclin (PGI2) production from endothelial cells
through a negative feedback counterregulatory response (Cheng et al. 2002). In
fact, PGI2 attenuates platelet aggregation and VSMC contraction.
In several cardiovascular diseases, endothelial dysfunction is the result of the
release of endothelium-derived contracting factors (EDCF) that counteract the
vasodilator effect of nitric oxide (NO) produced by the endothelial NO synthase.
These endogenous TP agonists produced by the vascular endothelium cause
endothelium-dependent contraction and contribute to endothelial dysfunction, a
key factor in atherogenesis. Endothelium-dependent contractions involve activation
of COXs, production of ROS along with that of EDCFs, which diffuse toward the
vascular smooth muscle cells and activate their TP.
Besides the activity of endothelial COX-1, the activation of TP-receptors on
VSMCs is also relevant (Swinnen et al. 2009). TP-receptor activation stimulates
VSMC proliferation and hypertrophy (Uehara et al. 1988), by potentiating the mito-
genic effects of platelet derived growth factor (PDGF) and by increasing the synthesis
and release of endogenous basic fibroblast growth factor (bFGF) (Ali et al. 1993).
3 Drugs Affecting TXA2 Action: Other than COX Inhibitors
The dramatic success story of aspirin as antiplatelet drug had a paradoxically
negative effect on the development of drugs that work by closely related but distinct
mechanisms to that of aspirin (Fig. 2). TXS inhibitors and TP antagonists were
perceived as too close to aspirin to compete effectively with this inexpensive and
effective drug.
3.1 Inhibitors of Thromboxane Synthase
The inhibitors of TXS prevent the conversion of PGH2 to TXA2. These drugs
reduce TXA2 synthesis mainly in platelets and may improve TXA2-mediated
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 267
pathophysiological conditions, such as thrombosis formation and thrombosis-related
disorders (Dogne et al. 2004). TXS inhibitors also enhance vascular generation of
PGI2, which prevents platelet aggregation induced by all known agonists (FitzGerald
et al. 1985). In fact, TXS inhibition leads to accumulation of PG endoperoxides in
platelets that may be donated to endothelial prostacyclin synthase at sites of platelet–-
vascular interactions (endoperoxide “steal”) (FitzGerald et al. 1985). Consistent with
this hypothesis, increased PGI2 generation in vivo has been reported after administra-
tion of several TXS inhibitors (FitzGerald et al. 1985). As PGI2 may inhibit platelet
activation by both TX-dependent and TX-independent mechanisms, it has been
proposed that TXS inhibitors may be more effective than aspirin to prevent
atherothrombosis.
Several TXS inhibitors—including dazoxiben, dazmagrel, pirmagrel, ozagrel,
isbogrel, and furegrelate—have been tested in clinical settings associated with
enhanced TX generation.
The greatest experience in human thrombotic disease has been gained with
dazoxiben. However, the benefits of this molecule in patients with coronary heart
disease were limited or absent (FitzGerald et al. 1985; Kiff et al. 1983; Thaulow
et al. 1984).
Ozagrel has been used clinically since 1992 in Japan for the treatment of asthma.
Treatment with ozagrel significantly reduced TX generation in patients with coro-
nary or cerebrovascular disease (Uyama et al. 1985; Yui et al. 1984). However, this
effect resulted into limited clinical benefit (Shikano et al. 1987).
It has been proposed that incomplete suppression of TX generation in vivo may
partly account for the lack of clinical efficacy of these drugs. In addition, TXS
inhibition increases PGI2 generation as well as the formation of other prostanoids,
including PGH2 and endoperoxides, which act as TP agonists, thereby
counteracting the reduction of TXA2-mediated events (Nakahata 2008).
3.2 Dual TXS Inhibition/TP Antagonism
Combined TXS inhibitors and TP antagonist may theoretically overcome the
limitations observed for TXS inhibitors. In fact, these drugs do not affect (or
enhance) PGI2 generation, while preventing TP activation by residual TX as well
as by other agonists (Patscheke 1990).
Accordingly, the combined administration of a dual TXS inhibitor/TP antagonist
gives stronger inhibition of platelet aggregation and prolongs bleeding time more
than either drug alone or acetylsalicylic acid (Patrono 1990).
Ridogrel is a drug developed more than 20 years ago as a more potent
antiplatelet agent than aspirin. Ridogrel is a TXA2 inhibitor with additional TP
antagonist properties that further enhance its antiaggregatory effects by diverting
endoperoxide intermediates into the PGI2 production pathway (Meadows and Bhatt
2007).
268 G. Davı et al.
Ridogrel has been studied primarily as an adjunctive agent to thrombolytic
therapy in acute MI. In 1993, animal studies showed that ridogrel limits MI size
after mechanical coronary occlusion and reperfusion at doses enhancing coronary
thrombolysis by streptokinase (Meadows and Bhatt 2007; Vandeplassche et al.
1993).
Thus, the Ridogrel Versus Aspirin Patency Trial (RAPT) was performed to
compare the efficacy and safety of ridogrel with that of aspirin as conjunctive
therapy for thrombolysis in patients with acute MI. However, despite positive
results from initial pilot studies, the largest clinical study, the RAPT, failed to
demonstrate any advantage with this agent over aspirin. In fact, in the study of 907
patients with acute MI, there was no difference in the primary end point of infarct
vessel patency rate between those randomized to ridogrel (72.2%) or aspirin
(75.5%). Despite ridogrel was not superior to aspirin in enhancing the fibrinolytic
efficacy of streptokinase, it was more effective in preventing new ischemic events
(The Ridogrel Versus Aspirin Patency Trial 1994).
In ulcerative colitis, local production of PGE2, PGI2, and TXA2 has been
demonstrated. The inflammatory infiltrate in ulcerative colitis consists of polymor-
phonuclear leukocytes, mononuclear leukocytes, and macrophages, all of which
release considerable amounts of TXA2. Although PGE2 may have protective effects
on intestinal mucosa, TXA2 appears to promote the development of chronic inflam-
matory lesions in the bowel. Thus, an imbalance between the synthesis of
cytoprotective prostaglandins, such as PGE2, and of the pro-inflammatory TXA2
may play a role in the development of chronic inflammation and mucosal damage in
patients with ulcerative colitis.
Treatment with selective inhibitors of TXA2 synthesis, including ridogrel,
reduced the release of TXA2, tissue damage, and the development of chronic
inflammatory lesions in the colon. A pilot clinical trial in patients with chronic
ulcerative colitis demonstrated that high-dose ridogrel (300 mg twice daily) signifi-
cantly reduced colonic mucosal TXA2 release, to 31% of basal levels, without
significantly reducing the levels of protective PGE2. However, two multicentre,
randomized, double-blind studies failed to find significant differences in the pri-
mary efficacy outcome measure among two different doses of ridogrel and placebo.
Thus, there was no clear indication in either trial of an effective dose of ridogrel in
the treatment of ulcerative colitis (Tytgat et al. 2002).
Various mechanisms are likely responsible for the results observed with
ridogrel in clinical trials, including potentially ineffective TP inhibition with the
concentrations of ridogrel used in human studies. As such, there currently are no
clinical indications for preferential use of ridogrel over aspirin.
Another drug with dual action (TXS inhibition/TP antagonism) is picotamide. In
a double blind, randomized trial (ADEP), 2,304 patients with intermittent claudi-
cation were allocated to receive picotamide or placebo. However, the trial showed
only a nonsignificant benefit of picotamide versus placebo in patients with periph-
eral artery disease (PAD) (Basili et al. 2010; Neri Serneri et al. 2004).
More recently, picotamide has been studied in diabetics with PAD randomized
to receive picotamide or aspirin for 2 years (DAVID study). Overall mortality, the
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 269
predefined primary end point, was significantly lower among patients who received
picotamide (3.0%) than in those who received aspirin (5.5%) with a relative risk
ratio for picotamide versus aspirin of 0.55 (95% CI 0.31–0.98%). Conversely, the
combined end point of mortality and morbidity has a slightly lower incidence in the
picotamide group, but this difference does not reach statistical significance (Neri
Serneri et al. 2004). The results of this study should be cautiously interpreted in the
light of its limited statistical power and sample size. In fact, as confirmed by a
recent meta-analysis comparing the efficacy of different antiplatelet treatments in
patients with PAD, picotamide, like aspirin, is not associated with a statistically
significant reduction in cardiovascular adverse events (Violi and Hiatt 2007).
Conversely, a significant reduction in cardiovascular risk is observed with
thienopyridines, suggesting that the presence of PAD may render platelet activation
more critically dependent on ADP than on TXA2 release.
4 Dual COXIB/TP Antagonists: A Possible New Twist in NSAID
Pharmacology and Cardiovascular Risk
In the early 1990s, a new class of nonsteroidal anti-inflammatory drug (NSAID)
became available (COX-2 inhibitors, or COXIBs). The gastrointestinal safety,
dependent upon lack of COX-1 inhibition, coupled with the emerging evidence of
cardiovascular hazard associated with COXIBs, leading to withdrawal of rofecoxib
and valdecoxib, suggested that a potentially safer pharmacological approach
should be combining the anti-inflammatory activity of COXIBs together with a
cardioprotective component which might involve antagonism of TP receptors. This
could be achieved by making a simple combination of existing drugs targeted
against COX-2 or the TP receptor.
The possibility to combine powerful anti-inflammatory activity with TP antago-
nism within a single chemical entity provides the basis for a novel class of safer
NSAIDs and to plan highly innovative studies of structure–activity relationships,
chemical syntheses, and pharmacological investigations.
It has recently been demonstrated (Selg et al. 2007) that a traditional NSAID
(diclofenac) and a selective COXIB (lumiracoxib) possess an additional activity:
weak competitive antagonism at the TP receptor (Rovati et al. 2010). However, in
light of the importance of maintaining a fine balance between TP receptor antago-
nism activity and COX-2 inhibition, the co-administration of two different
molecules is not the best approach because it may result in significantly different
pharmacokinetic profiles. Combining both activities into a single chemical entity
represents a far better strategy (Selg et al. 2007): in fact, developing a compound
with a more “balanced” pharmacological profile relative to these two activities may
help evaluating if blocking the activity of TP might counterbalance the deleterious
cardiovascular effects driven by the PGI2 inhibition observed for COX-2 inhibitors.
270 G. Davı et al.
4.1 TP Antagonists
Several TP antagonists have been developed since the early 1980s. Development of
the earliest TP antagonists has been stopped because of their toxicity (or moderate
activity) in clinical situations, whereas others have not been investigated for
cardiovascular indication, and only the more recent TP antagonists reached clinical
evaluation for their antithrombotic properties (Dogne et al. 2004).
Thus, many TP antagonists have been developed for the treatment of TP-mediated
diseases, such as ifetroban, sulotroban, daltroban, linotroban, ramatoroban, and
seratrodast. Among them, seratorodast is an orally active TP antagonist used clinically
for the treatment of asthma in Japan since 1997 (Nakahata 2008).
However, evidence has been accumulated for a competitive TP antagonist,
terutroban (S-18886), as a potential candidate for atherothrombosis treatment, for
blocking atherosclerosis progression, and for transforming lesions towards a more
stable phenotype.
Terutroban is an orally active TP antagonist in clinical development for use in
secondary prevention of thrombotic events in cardiovascular disease. Terutroban has
been developed as a highly specific, high-affinity TP antagonist. Binding studies show
that the drug displaces the binding of [3H]-SQ29548 on human platelet membranes
with aKi value of 0.65 nmol/L, and theKdvalue for binding of [3H]-S18886 to human
platelet membranes averaged 0.96 nmol/L (Zuccollo et al. 2005). Unlike aspirin and
clopidogrel that bind their respective receptor in an irreversible manner, terutroban
has a reversible and dose-dependent antithrombotic effect within 96 h (Gaussem
et al. 2005).
Escalating doses of terutroban (30 and 100 mg/kg/day) compared with that of
aspirin (5 mg/kg/day) and clopidogrel (3 mg/kg/day) show a significant dose-
dependent effect on platelet aggregation. When used at higher doses, terutroban
is able to reduce collagen-dependent platelet aggregation, at least as well as
clopidogrel. Terutroban reduces platelet deposition on low shear (212 s�1) and
high shear (1,690 s�1) rate conditions (platelet thrombus formation in the Badimon
perfusion chamber) at least as well as clopidogrel, whereas aspirin does not have
any significant effect on platelet deposition. Thus, TP antagonists might be useful in
clinical settings characterized by severe arterial injury and high shear rate, such as
acute coronary syndromes and during and immediately after percutaneous
transluminal coronary angioplasty (Chamorro 2009).
Pharmacokinetics and pharmacodynamics of terutroban have been studied in
patients with PAD (Gaussem et al. 2005). Peak plasma levels are reached between
30 min and 2 h and the half life is 5.8–10 h. Maximal inhibition of U46619-induced
platelet aggregation is achieved within 1 h, and this effect is maintained for at least
12 h. Over the range of studied doses, there is a predictable relation between plasma
drug concentration and degree of platelet inhibition. Plasma concentrations above
10 ng/mL strongly inhibit U46619-induced platelet aggregation. These plasma
concentrations are reached only by dosages higher than 10 mg/day (Gaussem
et al. 2005).
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 271
The antithrombotic effects of increasing doses (1–30 mg/day) of terutroban have
also been demonstrated in PAD (TAIPAD study) using a design based on the
ex vivo evaluation of platelet aggregation. This effect was predictable, dose-
dependent with maximal inhibition at 1 h, and lasted for approximately 48 h at
the oral dose of 30 mg (Fiessinger et al. 2010).
Terutroban does not bind other prostanoid receptors, such as IP or DP receptors,
and thus preserves antivasoconstrictive effects of their natural ligands, PGI2 and
PGD2 (Chamorro 2009).
5 Pathophysiological Rationale for the Superiority of
TP-Receptor Antagonists Over Aspirin
5.1 Advantages as an Antithrombotic Agent
An increased incidence of cardiovascular events and enhanced TX-dependent
platelet activation characterize several clinical conditions, and aspirin is thought
to be the best choice in these settings. However, enhanced TX generation may be
explained by several mechanisms relatively insensitive to aspirin.
Monocytes and macrophages are the largest source of TXA2 and are capable of
newly synthesizing TXA2 via their COX-2 pathway, which has a higher threshold
of inhibition by aspirin than platelet COX-1. Thus, extraplatelet, nucleate sources of
TXA2 biosynthesis, possibly triggered by inflammatory stimuli, are less affected
than platelet TXA2 production by the once-daily regimen of administration and by
the low dose administered, and may be an additional reason for the less than
expected response to aspirin.
Moreover, in clinical settings characterized by enhanced platelet generation,
younger reticulated platelets are increased, platelet COX-2 expression is up-
regulated, and a consistent TX production may be driven by this enzymatic pathway
relatively insensitive to aspirin (Guthikonda et al. 2007; Santilli et al. 2009).
Moreover, TP antagonists block all TP agonists; these include not only TXA2
but also endoperoxide (i.e., 20-HETE) and several isoprostanes, nonenzymatic
products of fatty acid oxidation formed under conditions of increased oxidative
stress (Davı and Falco 2005) and which are not inhibited by aspirin (Fig. 2). Aspirin
has no effect on isoprostanes and can actually increase endoperoxide (i.e., HETE)
production by COX (Meade et al. 1993). Recently, it has been reported that the
signaling mechanism of flow-induced constriction of human and rat cerebral
arteries involves enhanced production of ROS, COX activity, and is mediated by
20-HETE via TP receptors (Toth et al. 2011).
Oxidative stress is responsible for enhanced peroxidation of AA to form biolog-
ically active F2-isoprostanes, such as 8-iso-PGF2a, that is widely recognized as a
reliable marker of lipid peroxidation both in vitro and in vivo (Davı and Falco 2005;
Patrono et al. 2005a).
272 G. Davı et al.
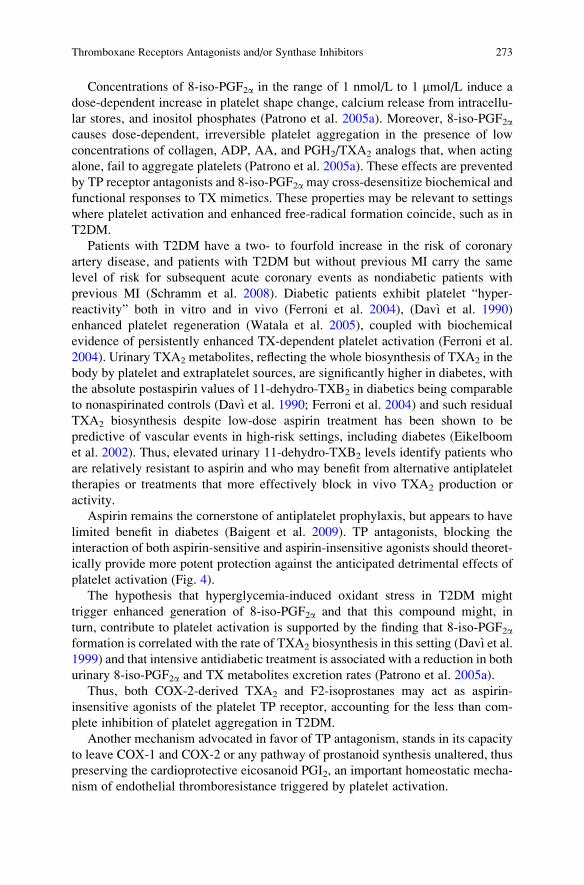
Concentrations of 8-iso-PGF2a in the range of 1 nmol/L to 1 mmol/L induce a
dose-dependent increase in platelet shape change, calcium release from intracellu-
lar stores, and inositol phosphates (Patrono et al. 2005a). Moreover, 8-iso-PGF2acauses dose-dependent, irreversible platelet aggregation in the presence of low
concentrations of collagen, ADP, AA, and PGH2/TXA2 analogs that, when acting
alone, fail to aggregate platelets (Patrono et al. 2005a). These effects are prevented
by TP receptor antagonists and 8-iso-PGF2a may cross-desensitize biochemical and
functional responses to TX mimetics. These properties may be relevant to settings
where platelet activation and enhanced free-radical formation coincide, such as in
T2DM.
Patients with T2DM have a two- to fourfold increase in the risk of coronary
artery disease, and patients with T2DM but without previous MI carry the same
level of risk for subsequent acute coronary events as nondiabetic patients with
previous MI (Schramm et al. 2008). Diabetic patients exhibit platelet “hyper-
reactivity” both in vitro and in vivo (Ferroni et al. 2004), (Davı et al. 1990)
enhanced platelet regeneration (Watala et al. 2005), coupled with biochemical
evidence of persistently enhanced TX-dependent platelet activation (Ferroni et al.
2004). Urinary TXA2 metabolites, reflecting the whole biosynthesis of TXA2 in the
body by platelet and extraplatelet sources, are significantly higher in diabetes, with
the absolute postaspirin values of 11-dehydro-TXB2 in diabetics being comparable
to nonaspirinated controls (Davı et al. 1990; Ferroni et al. 2004) and such residual
TXA2 biosynthesis despite low-dose aspirin treatment has been shown to be
predictive of vascular events in high-risk settings, including diabetes (Eikelboom
et al. 2002). Thus, elevated urinary 11-dehydro-TXB2 levels identify patients who
are relatively resistant to aspirin and who may benefit from alternative antiplatelet
therapies or treatments that more effectively block in vivo TXA2 production or
activity.
Aspirin remains the cornerstone of antiplatelet prophylaxis, but appears to have
limited benefit in diabetes (Baigent et al. 2009). TP antagonists, blocking the
interaction of both aspirin-sensitive and aspirin-insensitive agonists should theoret-
ically provide more potent protection against the anticipated detrimental effects of
platelet activation (Fig. 4).
The hypothesis that hyperglycemia-induced oxidant stress in T2DM might
trigger enhanced generation of 8-iso-PGF2a and that this compound might, in
turn, contribute to platelet activation is supported by the finding that 8-iso-PGF2aformation is correlated with the rate of TXA2 biosynthesis in this setting (Davı et al.
1999) and that intensive antidiabetic treatment is associated with a reduction in both
urinary 8-iso-PGF2a and TX metabolites excretion rates (Patrono et al. 2005a).
Thus, both COX-2-derived TXA2 and F2-isoprostanes may act as aspirin-
insensitive agonists of the platelet TP receptor, accounting for the less than com-
plete inhibition of platelet aggregation in T2DM.
Another mechanism advocated in favor of TP antagonism, stands in its capacity
to leave COX-1 and COX-2 or any pathway of prostanoid synthesis unaltered, thus
preserving the cardioprotective eicosanoid PGI2, an important homeostatic mecha-
nism of endothelial thromboresistance triggered by platelet activation.
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 273
In contrast, depression of COX-2-derived PGI2 by traditional NSAIDS or
COXIBs as well as by anti-inflammatory doses of aspirin removes a constraint on
platelet COX-1-derived TXA2 and other agonists that elevate blood pressure,
promotes atherogenesis, and augments the thrombotic response to plaque rupture.
5.2 Relevance of TP Receptors Inhibition in AtheroscleroticDisease
Treatment with a TP antagonist, but not treatment with aspirin, inhibits atherogen-
esis in apo-E deficient mice (Cayatte et al. 2000), strongly suggesting that TP
antagonists could be superior to aspirin in preventing atheroma. In New Zealand
TXA2
Platelet
COX-1Platelet
COX-1
Extraplateletsources
Platelet activation
COX-2
COX-2 Low-dose aspirin
ROS
8-iso-PGF2α
TP antagonist
ROS
Inflammatorysignals
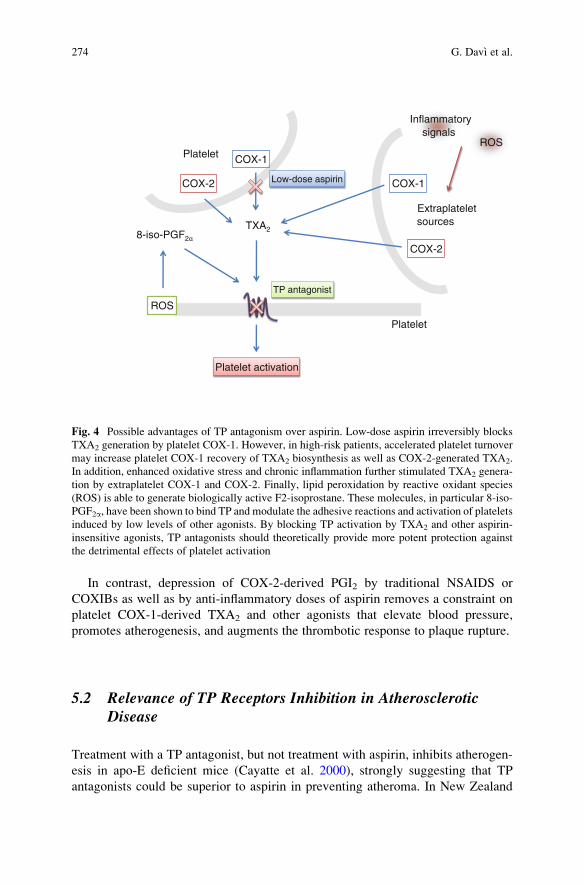
Fig. 4 Possible advantages of TP antagonism over aspirin. Low-dose aspirin irreversibly blocks
TXA2 generation by platelet COX-1. However, in high-risk patients, accelerated platelet turnover
may increase platelet COX-1 recovery of TXA2 biosynthesis as well as COX-2-generated TXA2.
In addition, enhanced oxidative stress and chronic inflammation further stimulated TXA2 genera-
tion by extraplatelet COX-1 and COX-2. Finally, lipid peroxidation by reactive oxidant species
(ROS) is able to generate biologically active F2-isoprostane. These molecules, in particular 8-iso-
PGF2a, have been shown to bind TP and modulate the adhesive reactions and activation of platelets
induced by low levels of other agonists. By blocking TP activation by TXA2 and other aspirin-
insensitive agonists, TP antagonists should theoretically provide more potent protection against
the detrimental effects of platelet activation
274 G. Davı et al.
white rabbits, terutroban induces regression of atherosclerotic lesions of the aorta
detected by magnetic resonance imaging. The concomitant reduction in indexes of
inflammation into the lesions, such as macrophages, apoptotic cells, matrix
metalloproteinase-1, endothelin-1, suggests that selective inhibition of TP receptor
may shift toward a more stable plaque phenotype (Chamorro 2009). Moreover,
injury-induced vascular proliferation is enhanced in mice genetically deficient in
the PGI2 receptor and is reduced in mice lacking the TP receptor or treated with
terutroban. Lack of both prostanoid receptors abolishes postinjury restenosis
(Cheng et al. 2002).
Endogenous TP agonists are produced by the vascular endothelium, especially
under pathological conditions, causing endothelium-dependent contraction and
contributing to endothelial dysfunction. Therefore, TP antagonists may counter-
act endothelial dysfunction in diseases such as hypertension and diabetes (Feletou
et al. 2010). In apoE�/� mice with streptozotocin-induced diabetes, terutroban
reduces aortic atherosclerotic area, with improvement of endothelium-dependent
relaxations to acetylcholine (Santilli et al. 2011). Thus, TP antagonism may
attenuate inflammation and atherogenesis in experimental diabetes.
Administration of terutroban to coronary artery disease or to high-cardiovas-
cular-risk patients on top of aspirin treatment improved endothelial function
assessed by measuring flow-mediated dilatation (FMD) in the brachial artery
(Belhassen et al. 2003; Lesault et al. 2011). The beneficial effect of terutroban
on FMD was detectable after the first intake and persisted up to the end of the
2-week treatment period (Lesault et al. 2011). Thus, TP antagonists can inhibit
prostanoid-mediated vasoconstriction associated with aging and/or cardiovascu-
lar risk factors related to increased oxidative stress and consequent up-regulation
of COX-1 and/or induction of COX-2 (Giannarelli et al. 2010).
5.3 Ischemic Stroke: The Reasons of a Choice
The at least theoretical advantages on platelet inhibition and the actions far beyond
its antithrombotic effect, including the antiproliferative and antiatherogenic
properties, raised the hypothesis that TP-receptor antagonism could play a role in
the clinical prevention of ischemic stroke. Preclinical findings supported this
concept, indicating a greater beneficial effect of TP receptor inhibition over aspirin
in a rat model of ischemic stroke (Gelosa et al. 2010). In a double-blind, parallel
group study in patients with previous ischemic stroke and/or carotid stenosis,
terutroban showed an antithrombotic activity superior to aspirin and similar to
clopidogrel plus aspirin (Bal Dit Sollier et al. 2009). These encouraging data
were the basis for undertaking the Prevention of cerebrovascular and cardiovascu-lar Events of ischemic origin with teRutroban in patients with a history oF ischemicstrOke or tRansient ischaeMic attack (PERFORM) study (Bousser et al. 2009).
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 275
This trial was designed to demonstrate the superiority of terutroban over
aspirin in secondary prevention of cerebrovascular and cardiovascular events
among ~20,000 patients with stroke. The trial (ISRCTN66157730) was recently
halted on the basis of an interim analysis failing to support the superiority hypothe-
sis, after 19,120 patients were randomly assigned, with a mean follow-up of 28·3
months (Bousser et al. 2011).
6 Great Expectations Disappointed: Did Terutroban
Fail to Perform, or PERFORM Did Fail?
The PERFORM was stopped prematurely for futility after 19,120 patients were
randomly assigned, with a mean follow-up of 28 months (Bousser et al. 2011). The
investigators recorded no difference between terutroban and aspirin in the compos-
ite vascular primary end point, or any of the secondary or tertiary end points.
However, the rate of minor bleeding was slightly increased with terutroban.
This apparent discrepancy versus the above-mentioned “great expectations”
around terutroban, supported by a large body of preclinical and clinical evidence
and pathophysiological rationale, draws attention and raises concerns about the
interpretation of the encouraging preclinical data, as well as about the design of the
clinical trial testing the superiority hypothesis of this drug versus aspirin.
6.1 Preliminary Data Revisited
The negative results of the PERFORM trial failed to come up to the expectations
based on the rationale and the preliminary data supporting the superiority of
terutroban over aspirin.
Both the anticipated superior antithrombotic effect and the peculiar antiatherogenic
and antivasoconstrictive properties of TP antagonism need to be reconsidered in
light of the clinical evidence.
Most of the data supporting a more potent antiplatelet effect of terutroban over
aspirin relied upon ex vivo measurements of platelet function, such as optical
aggregation to classical agonists and models of thrombus formation (Bal Dit Sollier
et al. 2009; Fiessinger et al. 2010).
The apparent gap between these premises and the findings of PERFORM
draws attention to the limitations of ex vivo measurements of platelet function in
the characterization of platelet activation and inhibition in vivo: less than
ideal intrasubject and intersubject variability, poor reproducibility on repeated
measurements, variability of the TX-independent component of the different aggre-
gation signals (Santilli et al. 2009).
276 G. Davı et al.
Moreover, measurements of platelet function ex vivo provide an index of
capacity that by no means reflects the extent of platelet activation and inhibition
in vivo. Mechanism-based biochemical measurements would provide a more faith-
ful estimation of the antiplatelet effect of aspirin.
As earlier mentioned, another war horse supporting the expected superiority of
terutroban over aspirin stands in the preservation of the ability of the vasculature to
synthesize the cardioprotective eicosanoid PGI2, an important homeostatic mecha-
nism of endothelial thromboresistance. However, the low-doses of aspirin (100 mg
daily) employed vs. terutroban in the PERFORM trial have been previously shown
to only marginally reduce systemic PGI2 biosynthesis in heart failure and ischemic
heart disease patients, counterbalanced by a profound reduction in TX biosynthesis
(Santilli et al. 2010), consistent with the relative COX-1 selectivity achieved by a
once-daily regimen of low-dose aspirin (Patrono et al. 2008) and the primary role of
COX-2 in PGI2 biosynthesis.
The antivasoconstrictive effect of terutroban, increasing blood flow through
enhanced endothelium-dependent vasodilation, had the theoretical potential to
affect the incidence of ischemic stroke in the PERFORM population, where tradi-
tional cardiovascular risk factors associated with endothelial dysfunction are highly
prevalent. However, it has to be acknowledged that, despite several reports (Santos-
Garcia et al. 2009) suggest an association, no data until now show conclusive
evidence of a direct relation between endothelium-dependent contractions and the
risk of ischemic stroke.
Similarly, the antiproliferative properties of terutroban, shown in a murine
model of vascular injury-induced proliferation of the carotid artery, did not
translate into a clinical benefit. This result might have been anticipated by the
failure to prevent postcoronary angioplasty restenosis by previously developed
TX-prostaglandin receptor antagonists, the CARPORT and the M-HEART (Savage
et al. 1995; Serruys et al. 1991). However, none of these two studies were free of
limitations, the first being an uncontrolled experience relying on a single measure-
ment of an angiographic end point, the second including no measure of the degree
of synthesis inhibition achieved by aspirin or of TP blockade by either antagonist.
Moreover, the M-HEART based the superiority of terutroban over aspirin on the
ability of terutroban to preserve the antiproliferative effect of PGI2 biosynthesis
during angiography, which was short lived and suppressed by the concurrent aspirin
treatment in all patients undergoing PCI (Pratico et al. 2000).
The antiatherogenic properties of TP antagonists were considered as a relevant
plus, stimulating the preferential recruitment of patients with an atherothrombotic
cerebral ischemic event. However, even in this subgroup, no benefit was recorded
for terutroban compared with aspirin in the PERFORM, possibly because their
atheromatous lesions were already well advanced. This assumption is supported by
a study performed in a murine model of atherogenesis, showing that TP antagonism
inhibits initiation and early development of atherosclerotic lesions in mice, but
failed to induce regression of established atherosclerotic disease (Egan et al. 2005).
Thus, the clinical use of TP antagonists would be expected to be useful in the earlier
stages of disease, rather than in reversing accumulated plaque burden in patients
with diffuse, established atherosclerosis.
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 277
6.2 The PERFORM Design Revisited
A few lessons might be drawn by the comparison of PERFORM findings with
similar trials of other antiplatelets vs. aspirin. PERFORM is the second largest
secondary prevention trial of an antiplatelet drug undertaken so far in patients with
cerebral ischemic events. The largest study, PROFESS (Sacco et al. 2008), com-
pared aspirin plus extended-release dipyridamole and clopidogrel in 20,232 patients
followed up for a mean of 30 months. This trial showed similar rates of recurrent
stroke with aspirin plus extended-release dipyridamole and with clopidogrel. Fail-
ure to achieve the superiority goal in both trials raises concerns about the clinical
setting in which selective TP receptor blockade might confer an advantage over
low-dose aspirin. Ischemic stroke might be a difficult setting as compared to MI,
but no trial so far is available to confirm or reject this speculative hypothesis.
Furthermore, the comparative analysis versus previously performed trials in the
same setting unravels the likelihood that the event rate observed in the PERFORM
might be someway lower than expected, thus affecting the statistical power of the
study. Although recent trials (ESPRIT and CSPS 2) have shown similar rates of
strokes with aspirin to those seen in PERFORM (Halkes et al. 2006; Shinohara et al.
2010), the stroke rate with aspirin in PERFORM should have been much higher
because of the enrolment of several patients during the period of highest risk for
recurrence (less than 3 months since the qualifying event) and because 52% of the
qualifying strokes were due to the stroke subtype with the poorer prognosis,
atherothrombosis (compared with about 30% in ESPRIT and CSPS 2). Even in
the PROFESS trial, which, similar to the PERFORM, enrolled patients who had
experienced an ischemic stroke for less than 90 days, the event rates were remark-
ably close to PERFORM, but the proportion of atherothrombotic infarcts was
significantly higher (67% vs. 28%) in PERFORM.
The choice of the lag time after the qualifying event, similar to the PROFESS
trial, might also have affected the effectiveness of the drug: in fact, patients could
be enrolled after the index event in PERFORM much sooner than in other recent
antiplatelet trials. While aspirin has proven benefits when given early after a stroke
(Chen et al. 2000), the efficacy of this strategy for other antiplatelets has not been
definitively proven.
The choice of the dose (30 mg once daily) has been an additional issue advocated
to explain the drug failure to exert superior effects on vascular events than aspirin.
However, the slight excess in minor bleeding with this dose suggests that, even if
higher doses may be more appropriate on the efficacy side, this benefit could be
offset by more hemorrhagic episodes, which seem proportional to the number of
TX-prostaglandin receptors bound by the drug.
The duration of follow-up appears as another critical and still unanswered issue:
given that only 15% of patients were followed up to or beyond 3 years, a difference
in treatment effect might have emerged later, since additional potential longer term
effects of terutroban cannot be excluded.
278 G. Davı et al.
As previously shown for aspirin (Baigent et al. 2009), improving background
risk-factor control could have blunted the ability of terutroban to outperform
aspirin. Nowadays, many patients with a history of occlusive vascular events
would have their risks of recurrence reduced substantially by statins, other modern
drugs, and vascular procedures. If so, and if the other interventions approximately
halve the recurrence risk, then the absolute benefit of adding an antiplatelet
to these other methods might be only about half as great as that of giving an
antiplatelet alone.
Finally, the observation that patients with a history of ischemic stroke before the
qualifying event had a lower event rate with terutroban than with aspirin is worth of
further attention. Although this finding could be attributable to chance, it is plausi-
ble that most of these patients would have been receiving aspirin before their
PERFORM qualifying event, thus the switch to a different antiplatelet drug appears
as a more effective strategy than continuation of aspirin despite having experienced
an event while on aspirin. Lower than expected response to aspirin which translates
into clinical failure might be an expected and relevant phenomenon in particular
subgroups of patients, such as those with diabetes mellitus (representing 27% and
28% of each arm, respectively). Trials that randomly assign patients with a break-
through event while on aspirin to a newer antiplatelet drug or to a different dosing
regimen, rather than to the original aspirin dose, could provide insights into this
issue. Perhaps terutroban could be tested for this specific issue or in clinical settings
where a benefit is anticipated, such as diabetes mellitus. In the PERFORM, only
about one out of five of the patient population had diabetes, thus potentially
affecting the statistical power of the study to test the superiority hypothesis in
diabetes.
7 Future Perspectives
As earlier mentioned, failure of the PERFORM does not preclude the possibility
that TP receptor antagonist may be an effective tool in the prevention of vascular
events in other clinical settings, such as diabetes, where the pathophysiological
premises for a beneficial role look more sound. This might be worth of ad hoc trials,
although the PERFORM findings are likely to discourage any other drug company
from pursuing this drug target.
Moving from the cardiovascular setting, an increasing body of evidence
provides the rationale for a role of TXS and TP receptor signaling in carcinogenesis,
which may arise as a “rescue” setting for the clinical development of these drugs.
TXS signaling has been implicated in the development and progression of
cancer, by acting on a range of tumor cell survival pathways, such as tumor cell
proliferation, induction of apoptosis, invasion and metastasis, and tumor cell
angiogenesis (Cathcart et al. 2010).
Increased expression of TXS and TP-b isoform has been found in the tissues of
patients with bladder cancer. TP-b receptor overexpression in patients with bladder
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 279
cancer is associated with a poorer prognosis (Moussa et al. 2008). Studies in cell
lines and mice have indicated a potential significant role of the TX signaling
pathway in the pathogenesis of human bladder cancer. Stimulation of TP receptors
is associated with a mitogenic response and in phosphorylation of several kinases.
TP receptor antagonists augment in vitro and in vivo responses to cisplatin, by
reducing cell proliferation in vitro, increasing the time of tumor onset, and reducing
the rate of tumor growth in vivo (Moussa et al. 2008). These studies raise the
possibility that the TP-b receptor could serve as a novel therapeutic target in
bladder cancer and its presence and/or overexpression could be used as a predictor
of prognosis and dictate therapy. Recently, increased tissue levels of the TP-breceptor in patients with bladder cancer have been found to be mirrored by
increased urinary levels of TXB2, the major metabolite of TXA2, suggesting that
patients with bladder cancer may be followed for progression or remission of their
disease by quantitation of these substances in their urine (Moussa et al. 2011).
TXS is also overexpressed in nonsmall cell lung cancer (NSCLC), particularly in
the adenocarcinoma subtype. Selective TXS inhibition prevents proliferation and
induces apoptosis (Cathcart et al. 2011).
Clearly, further studies are needed to delineate the role of TXS and TP-breceptors in cancer and to address the challenge of their pharmacological inhibition
through a clinical development program.
8 Conclusions and Implications for Clinical Usefulness
of TP Antagonists
Several clinical conditions are characterized by increased incidence of cardiovas-
cular events and enhanced TX-dependent platelet activation.
Aspirin is thought to be the best choice in these settings. However, the optimum
regimen to suppress TX formation remains undefined. In fact, enhanced TX gener-
ation may be explained by mechanisms relatively insensitive to aspirin.
Extraplatelet, nucleate sources of TXA2 biosynthesis, possibly triggered by
inflammatory stimuli, and F2-isoprostane formation, reflecting ongoing in vivo
oxidative stress, can activate platelets via the platelet TP receptor thus escaping
inhibition of aspirin (Davı et al. 1990).
Thus, the relevance of the TP receptor in the pathogenesis of vascular diseases,
particularly in diabetes, may be due to the fact that not only TXA2, but other
eicosanoids including HETEs and isoprostanes are produced to such an extent as
to activate the TP receptor. Aspirin has no effect on isoprostanes which are formed
nonenzymatically from AA, and aspirin can actually increase HETE production by
COX (Meade et al. 1993).
In clinical settings characterized by enhanced platelet generation, younger
reticulated platelets are increased, and platelet COX-2 expression is up-regulated
and a consistent TX production may be driven by this enzymatic pathway, rela-
tively insensitive to aspirin (Guthikonda et al. 2007; Santilli et al. 2009).
280 G. Davı et al.

An antithrombotic intervention blocking TP may be required, as a common
downstream pathway for both platelet and extraplatelet TXA2 as well as for
isoprostanes. Aspirin does not inhibit isoprostane formation. Moreover, intraplatelet
or extraplatelet TX generation may be only partly inhibited by aspirin under certain
pathological conditions, at least at the usual low doses given for cardiovascular
protection.
Moreover, a TP antagonist has actions far beyond its antithrombotic effect
exerted on platelets and can be attributed to direct effects on endothelial and smooth
muscle cells within the blood vessel wall. These include effects on vascular
adhesion molecules, NO synthase expression and function, oxidant production,
and accumulation of extracellular matrix and advanced glycation end-products.
Thus, TP antagonists may represent an ideal tool to improve our knowledge on
the pathophysiology of cardiovascular diseases and to improve our pharmacologi-
cal “weapons” to counteract them in clinical settings, such as diabetes mellitus,
characterized by persistent enhanced TXA2-dependent platelet activation.
Knowledge Gaps
• The prevention of vascular events by TP receptor antagonists in clinical
settings, such as diabetes, where the pathophysiological premises for a
beneficial role look more sound needs to be defined.
• The hypothesis that TP-b receptor could serve as a novel therapeutic target
in bladder cancer and its presence and/or overexpression could be used as a
predictor of prognosis and dictate therapy needs to be tested.
• More in general, further studies are needed to delineate the role of TXS
and TP-b receptors in cancer and to address the challenge of their phar-
macological inhibition through a clinical development program.
Key Messages
• Thromboxane synthase (TXS) inhibitors and thromboxane receptor (TP)
antagonists have the potential to prove more effective than aspirin due to
their different mechanism of action along the pathway of TXA2. TXS
inhibitors prevent the conversion of PGH2 to TXA2, reducing TXA2
synthesis mainly in platelets, whereas TP antagonists block the down-
stream consequences of TP activation.
• Targeting TP receptor, a common downstream pathway for both platelet and
extraplatelet TXA2 as well as for endoperoxides and isoprostanes, may be a
useful antiatherosclerotic and a more powerful antithrombotic intervention
in clinical settings, such as diabetes mellitus, characterized by persistently
enhanced TX-dependent platelet activation through isoprostane formation
and low-grade inflammation, leading to extraplatelet sources of TXA2.(continued)
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 281

• Despite great expectations on this drug supported by a large body of
preclinical and clinical evidence and pathophysiological rationale, the
PERFORM trial failed to demonstrate the superiority of terutroban over
aspirin in secondary prevention of cerebrovascular and cardiovascular
events among ~20,000 patients with stroke. However, the clinical setting
and the design of the study in which the drug has been challenged, as well
as a sometimes uncritical translation of preclinical data into a rationale for
a clinical trial, may explain, at least in part, this unexpected finding.
• Drugs with dual action, such as dual TXS inhibitors/TP antagonist and
dual COXIB/TP antagonists are currently in clinical development. Besides
the theoretical rationale for their benefit, ongoing clinical studies are
challenging their potential.
References
Ali S, Davis MG, Becker MW, Dorn GW 2nd (1993) Thromboxane A2 stimulates vascular smooth
muscle hypertrophy by up-regulating the synthesis and release of endogenous basic fibroblast
growth factor. J Biol Chem 268:17397–17403
Ashton AW, Ware GM, Kaul DK, Ware JA (2003) Inhibition of tumor necrosis factor alpha-
mediated NFkappaB activation and leukocyte adhesion, with enhanced endothelial apoptosis,
by G protein-linked receptor (TP) ligands. J Biol Chem 278:11858–11866
Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, Buring J, Hennekens C,
Kearney P, Meade T, Patrono C, Roncaglioni MC, Zanchetti A (2009) Aspirin in the primary
and secondary prevention of vascular disease: collaborative meta-analysis of individual partic-
ipant data from randomised trials. Lancet 373:1849–1860
Bal Dit Sollier C, Crassard I, Simoneau G, Bergmann JF, Bousser MG, Drouet L (2009) Effect of
the thromboxane prostaglandin receptor antagonist terutroban on arterial thrombogenesis after
repeated administration in patients treated for the prevention of ischemic stroke. Cerebrovasc
Dis 28:505–513
Basili S, Raparelli V, Vestri A, Di Tanna GL, Violi F (2010) Comparison of efficacy of antiplatelet
treatments for patients with claudication. A meta-analysis. Thromb Haemost 103:766–773
Belhassen L, Pelle G, Dubois-Rande JL, Adnot S (2003) Improved endothelial function by the
thromboxane A2 receptor antagonist S 18886 in patients with coronary artery disease treated
with aspirin. J Am Coll Cardiol 41:1198–1204
Bousser MG, Amarenco P, Chamorro A, Fisher M, Ford I, Fox K, Hennerici MG, Mattle HP,
Rothwell PM (2009) Rationale and design of a randomized, double-blind, parallel-group study
of terutroban 30 mg/day versus aspirin 100 mg/day in stroke patients: the prevention of
cerebrovascular and cardiovascular events of ischemic origin with terutroban in patients with
a history of ischemic stroke or transient ischemic attack (PERFORM) study. Cerebrovasc Dis
27:509–518
Bousser MG, Amarenco P, Chamorro A, Fisher M, Ford I, Fox KM, Hennerici MG, Mattle HP,
Rothwell PM, de Cordoue A, Fratacci MD (2011) Terutroban versus aspirin in patients with
cerebral ischaemic events (PERFORM): a randomised, double-blind, parallel-group trial.
Lancet 377:2013–2022
Cathcart MC, Reynolds JV, O’Byrne KJ, Pidgeon GP (2010) The role of prostacyclin synthase and
thromboxane synthase signaling in the development and progression of cancer. Biochim
Biophys Acta 1805:153–166
282 G. Davı et al.
Cathcart MC, Gately K, Cummins R, Kay E, O’Byrne KJ, Pidgeon GP (2011) Examination of
thromboxane synthase as a prognostic factor and therapeutic target in non-small cell lung
cancer. Mol Cancer 10:25
Cayatte AJ, Du Y, Oliver-Krasinski J, Lavielle G, Verbeuren TJ, Cohen RA (2000) The throm-
boxane receptor antagonist S18886 but not aspirin inhibits atherogenesis in apo E-deficient
mice: evidence that eicosanoids other than thromboxane contribute to atherosclerosis.
Arterioscler Thromb Vasc Biol 20:1724–1728
Chamorro A (2009) TP receptor antagonism: a new concept in atherothrombosis and stroke
prevention. Cerebrovasc Dis 27(Suppl 3):20–27
Chen ZM, Sandercock P, Pan HC, Counsell C, Collins R, Liu LS, Xie JX, Warlow C, Peto R
(2000) Indications for early aspirin use in acute ischemic stroke: a combined analysis of 40 000
randomized patients from the chinese acute stroke trial and the international stroke trial. On
behalf of the CAST and IST collaborative groups. Stroke 31:1240–1249
Cheng Y, Austin SC, Rocca B, Koller BH, Coffman TM, Grosser T, Lawson JA, FitzGerald GA
(2002) Role of prostacyclin in the cardiovascular response to thromboxane A2. Science
296:539–541
Davı G, Falco A (2005) Oxidant stress, inflammation and atherogenesis. Lupus 14:760–764
Davı G, Patrono C (2007) Platelet activation and atherothrombosis. N Engl J Med 357:2482–2494
Davı G, Catalano I, Averna M, Notarbartolo A, Strano A, Ciabattoni G, Patrono C (1990)
Thromboxane biosynthesis and platelet function in type II diabetes mellitus. N Engl J Med
322:1769–1774
Davı G, Ciabattoni G, Consoli A, Mezzetti A, Falco A, Santarone S, Pennese E, Vitacolonna E,
Bucciarelli T, Costantini F, Capani F, Patrono C (1999) In vivo formation of 8-iso-prostaglan-
din f2alpha and platelet activation in diabetes mellitus: effects of improved metabolic control
and vitamin E supplementation. Circulation 99:224–229
Dogne JM, de Leval X, Hanson J, Frederich M, Lambermont B, Ghuysen A, Casini A, Masereel B,
Ruan KH, Pirotte B, Kolh P (2004) New developments on thromboxane and prostacyclin
modulators part I: thromboxane modulators. Curr Med Chem 11:1223–1241
Dogne JM, Hanson J, Pratico D (2005) Thromboxane, prostacyclin and isoprostanes: therapeutic
targets in atherogenesis. Trends Pharmacol Sci 26:639–644
Egan KM, Wang M, Fries S, Lucitt MB, Zukas AM, Pure E, Lawson JA, FitzGerald GA
(2005) Cyclooxygenases, thromboxane, and atherosclerosis: plaque destabilization by
cyclooxygenase-2 inhibition combined with thromboxane receptor antagonism. Circulation
111:334–342
Eikelboom JW, Hirsh J, Weitz JI, Johnston M, Yi Q, Yusuf S (2002) Aspirin-resistant thrombox-
ane biosynthesis and the risk of myocardial infarction, stroke, or cardiovascular death in
patients at high risk for cardiovascular events. Circulation 105:1650–1655
Feletou M, Verbeuren TJ, Vanhoutte PM (2009) Endothelium-dependent contractions in SHR: a
tale of prostanoid TP and IP receptors. Br J Pharmacol 156:563–574
Feletou M, Cohen RA, Vanhoutte PM, Verbeuren TJ (2010) TP receptors and oxidative stress hand
in hand from endothelial dysfunction to atherosclerosis. Adv Pharmacol 60:85–106
Ferroni P, Basili S, Falco A, Davı G (2004) Platelet activation in type 2 diabetes mellitus. J
Thromb Haemost 2:1282–1291
Fiessinger JN, Bounameaux H, Cairols MA, Clement DL, Coccheri S, Fletcher JP, Hoffmann U,
Turpie AG (2010) Thromboxane Antagonism with terutroban in Peripheral Arterial Disease:
the TAIPAD study. J Thromb Haemost 8:2369–2376
FitzGerald GA, Reilly IA, Pedersen AK (1985) The biochemical pharmacology of thromboxane
synthase inhibition in man. Circulation 72:1194–1201
Gaussem P, Reny JL, Thalamas C, Chatelain N, Kroumova M, Jude B, Boneu B, Fiessinger JN
(2005) The specific thromboxane receptor antagonist S18886: pharmacokinetic and pharma-
codynamic studies. J Thromb Haemost 3:1437–1445
Gelosa P, Ballerio R, Banfi C, Nobili E, Gianella A, Pignieri A, Brioschi M, Guerrini U,
Castiglioni L, Blanc-Guillemaud V, Lerond L, Tremoli E, Sironi L (2010) Terutroban, a
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 283
thromboxane/prostaglandin endoperoxide receptor antagonist, increases survival in stroke-
prone rats by preventing systemic inflammation and endothelial dysfunction: comparison
with aspirin and rosuvastatin. J Pharmacol Exp Ther 334:199–205
Giannarelli C, Zafar MU, Badimon JJ (2010) Prostanoid and TP-receptors in atherothrombosis: is
there a role for their antagonism? Thromb Haemost 104:949–954
Guthikonda S, Lev EI, Patel R, DeLao T, Bergeron AL, Dong JF, Kleiman NS (2007) Reticulated
platelets and uninhibited COX-1 and COX-2 decrease the antiplatelet effects of aspirin. J
Thromb Haemost 5:490–496
Halkes PH, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A (2006) Aspirin plus dipyridamole
versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised con-
trolled trial. Lancet 367:1665–1673
Ishizuka T, Suzuki K, Kawakami M, Hidaka T, Matsuki Y, Nakamura H (1996) Thromboxane A2
receptor blockade suppresses intercellular adhesion molecule-1 expression by stimulated
vascular endothelial cells. Eur J Pharmacol 312:367–377
Ishizuka T, Kawakami M, Hidaka T, Matsuki Y, Takamizawa M, Suzuki K, Kurita A, Nakamura
H (1998) Stimulation with thromboxane A2 (TXA2) receptor agonist enhances ICAM-1,
VCAM-1 or ELAM-1 expression by human vascular endothelial cells. Clin Exp Immunol
112:464–470
Kiff PS, Bergman G, Atkinson L, Jewitt DE, Westwick J, Kakkar VV (1983) Haemodynamic and
metabolic effects of dazoxiben at rest and during atrial pacing. Br J Clin Pharmacol
15:73S–77S
Lesault PF, Boyer L, Pelle G, Covali-Noroc A, Rideau D, Akakpo S, Teiger E, Dubois-Rande JL,
Adnot S (2011) Daily administration of the TP receptor antagonist terutroban improved
endothelial function in high-cardiovascular-risk patients with atherosclerosis. Br J Clin
Pharmacol 71:844–851
Mayeux PR, Morton HE, Gillard J, Lord A, Morinelli TA, Boehm A, Mais DE, Halushka PV
(1988) The affinities of prostaglandin H2 and thromboxane A2 for their receptor are similar in
washed human platelets. Biochem Biophys Res Commun 157:733–739
Meade EA, Smith WL, DeWitt DL (1993) Differential inhibition of prostaglandin endoperoxide
synthase (cyclooxygenase) isozymes by aspirin and other non-steroidal anti-inflammatory
drugs. J Biol Chem 268:6610–6614
Meadows TA, Bhatt DL (2007) Clinical aspects of platelet inhibitors and thrombus formation. Circ
Res 100:1261–1275
Mehta P, Mehta J, Lawson D, Krop I, Letts LG (1986) Leukotrienes potentiate the effects of
epinephrine and thrombin on human platelet aggregation. Thromb Res 41:731–738
Meja KK, Barnes PJ, Giembycz MA (1997) Characterization of the prostanoid receptor(s) on
human blood monocytes at which prostaglandin E2 inhibits lipopolysaccharide-induced
tumour necrosis factor-alpha generation. Br J Pharmacol 122:149–157
Miggin SM, Kinsella BT (1998) Expression and tissue distribution of the mRNAs encoding the
human thromboxane A2 receptor (TP) alpha and beta isoforms. Biochim Biophys Acta
1425:543–559
Moussa O, Ashton AW, Fraig M, Garrett-Mayer E, Ghoneim MA, Halushka PV, Watson DK
(2008) Novel role of thromboxane receptors beta isoform in bladder cancer pathogenesis.
Cancer Res 68:4097–4104
Moussa O, Ciupek A, Watson DK, Halushka PV (2011) Urinary thromboxane B(2) and throm-
boxane receptors in bladder cancer: opportunity for detection and monitoring. Prostaglandins
Other Lipid Mediat 96(1–4):41–44
Nakahata N (2008) Thromboxane A2: physiology/pathophysiology, cellular signal transduction
and pharmacology. Pharmacol Ther 118:18–35
Neri Serneri GG, Coccheri S, Marubini E, Violi F (2004) Picotamide, a combined inhibitor of
thromboxane A2 synthase and receptor, reduces 2-year mortality in diabetics with peripheral
arterial disease: the DAVID study. Eur Heart J 25:1845–1852
Patrono C (1990) Biosynthesis and pharmacological modulation of thromboxane in humans.
Circulation 81:I12–I15, discussion I22–I23
284 G. Davı et al.

Patrono C, Falco A, Davı G (2005a) Isoprostane formation and inhibition in atherothrombosis.
Curr Opin Pharmacol 5:198–203
Patrono C, Garcia Rodriguez LA, Landolfi R, Baigent C (2005b) Low-dose aspirin for the
prevention of atherothrombosis. N Engl J Med 353:2373–2383
Patrono C, Baigent C, Hirsh J, Roth G (2008) Antiplatelet drugs: American College of Chest
Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 133:199S–233S
Patscheke H (1990) Thromboxane A2/prostaglandin H2 receptor antagonists. A new therapeutic
principle. Stroke 21:IV139–IV142
Pratico D, Cheng Y, FitzGerald GA (2000) TP or not TP: primary mediators in a close runoff?
Arterioscler Thromb Vasc Biol 20:1695–1698
Rovati GE, Sala A, Capra V, Dahlen SE, Folco G (2010) Dual COXIB/TP antagonists: a possible
new twist in NSAID pharmacology and cardiovascular risk. Trends Pharmacol Sci 31:102–107
Sacco RL, Diener HC, Yusuf S, Cotton D, Ounpuu S, Lawton WA, Palesch Y, Martin RH, Albers
GW, Bath P, Bornstein N, Chan BP, Chen ST, Cunha L, Dahlof B, De Keyser J, Donnan GA,
Estol C, Gorelick P, Gu V, Hermansson K, Hilbrich L, Kaste M, Lu C, Machnig T, Pais P,
Roberts R, Skvortsova V, Teal P, Toni D, Vandermaelen C, Voigt T, Weber M, Yoon BW
(2008) Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. N
Engl J Med 359:1238–1251
Santilli F, Rocca B, De Cristofaro R, Lattanzio S, Pietrangelo L, Habib A, Pettinella C, Recchiuti
A, Ferrante E, Ciabattoni G, Davı G, Patrono C (2009) Platelet cyclooxygenase inhibition by
low-dose aspirin is not reflected consistently by platelet function assays: implications for
aspirin “resistance”. J Am Coll Cardiol 53:667–677
Santilli F, Davı G, Basili S, Lattanzio S, Cavoni A, Guizzardi G, De Feudis L, Traisci G, Pettinella
C, Paloscia L, Minuz P, Meneguzzi A, Ciabattoni G, Patrono C (2010) Thromboxane and
prostacyclin biosynthesis in heart failure of ischemic origin: effects of disease severity and
aspirin treatment. J Thromb Haemost 8:914–922
Santilli F, Mucci L, Davı G (2011) TP receptor activation and inhibition in atherothrombosis: the
paradigm of diabetes mellitus. Intern Emerg Med 6:203–212
Santos-Garcia D, Blanco M, Serena J, Arias S, Millan M, Rodriguez-Yanez M, Leira R, Davalos
A, Castillo J (2009) Brachial arterial flow mediated dilation in acute ischemic stroke. Eur J
Neurol 16:684–690
Savage MP, Goldberg S, Bove AA, Deutsch E, Vetrovec G, Macdonald RG, Bass T, Margolis JR,
Whitworth HB, Taussig A (1995) Effect of thromboxane A2 blockade on clinical outcome and
restenosis after successful coronary angioplasty. Multi-Hospital Eastern Atlantic Restenosis
Trial (M-HEART II). Circulation 92:3194–3200
Schramm TK, Gislason GH, Kober L, Rasmussen S, Rasmussen JN, Abildstrom SZ, Hansen ML,
Folke F, Buch P, Madsen M, Vaag A, Torp-Pedersen C (2008) Diabetes patients requiring
glucose-lowering therapy and nondiabetics with a prior myocardial infarction carry the same
cardiovascular risk: a population study of 3.3 million people. Circulation 117:1945–1954
Selg E, Buccellati C, Andersson M, Rovati GE, Ezinga M, Sala A, Larsson AK, Ambrosio M,
Lastbom L, Capra V, Dahlen B, Ryrfeldt A, Folco GC, Dahlen SE (2007) Antagonism of
thromboxane receptors by diclofenac and lumiracoxib. Br J Pharmacol 152:1185–1195
Serruys PW, Rutsch W, Heyndrickx GR, Danchin N, Mast EG, Wijns W, Rensing BJ, Vos J,
Stibbe J (1991) Prevention of restenosis after percutaneous transluminal coronary angioplasty
with thromboxane A2-receptor blockade. A randomized, double-blind, placebo-controlled
trial. Coronary Artery Restenosis Prevention on Repeated Thromboxane-Antagonism Study
(CARPORT). Circulation 84:1568–1580
Shikano M, Ito T, Ogawa K, Satake T (1987) Effects of a selective thromboxane synthetase
inhibitor (OKY-046) in patients with coronary artery disease during exercise. Jpn Heart J
28:663–674
Shinohara Y, Katayama Y, Uchiyama S, Yamaguchi T, Handa S, Matsuoka K, Ohashi Y, Tanahashi
N, Yamamoto H, Genka C, Kitagawa Y, Kusuoka H, Nishimaru K, Tsushima M, Koretsune Y,
Sawada T, Hamada C (2010) Cilostazol for prevention of secondary stroke (CSPS 2): an aspirin-
controlled, double-blind, randomised non-inferiority trial. Lancet Neurol 9:959–968
Thromboxane Receptors Antagonists and/or Synthase Inhibitors 285
SwinnenM, Vanhoutte D, Van Almen GC, Hamdani N, SchellingsMW, D’Hooge J, Van der Velden
J,WeaverMS,SageEH,Bornstein P,Verheyen FK,VandenDriessche T,ChuahMK,Westermann
D, PaulusWJ, Van deWerf F, Schroen B, Carmeliet P, Pinto YM, Heymans S (2009) Absence of
thrombospondin-2 causes age-related dilated cardiomyopathy. Circulation 120:1585–1597
Thaulow E, Dale J, Myhre E (1984) Effects of a selective thromboxane synthetase inhibitor,
dazoxiben, and of acetylsalicylic acid on myocardial ischemia in patients with coronary artery
disease. Am J Cardiol 53:1255–1258
The Ridogrel Versus Aspirin Patency Trial (1994) Randomized trial of ridogrel, a combined
thromboxane A2 synthase inhibitor and thromboxane A2/prostaglandin endoperoxide receptor
antagonist, versus aspirin as adjunct to thrombolysis in patients with acute myocardial infarc-
tion. Circulation 89:588–595
Toth P, Rozsa B, Springo Z, Doczi T, Koller A (2011) Isolated human and rat cerebral arteries
constrict to increases in flow: role of 20-HETE and TP receptors. J Cereb Blood Flow Metab
31:2096–2105
Tytgat GN, Van Nueten L, Van De Velde I, Joslyn A, Hanauer SB (2002) Efficacy and safety of
oral ridogrel in the treatment of ulcerative colitis: two multicentre, randomized, double-blind
studies. Aliment Pharmacol Ther 16:87–99
Uehara Y, Ishimitsu T, Kimura K, Ishii M, Ikeda T, Sugimoto T (1988) Regulatory effects of
eicosanoids on thymidine uptake by vascular smooth muscle cells of rats. Prostaglandins
36:847–857
Uyama O, Nagatsuka K, Nakabayashi S, Isaka Y, Yoneda S, Kimura K, Abe H (1985) The effect
of a thromboxane synthetase inhibitor, OKY-046, on urinary excretion of immunoreactive
thromboxane B2 and 6-keto-prostaglandin F1 alpha in patients with ischemic cerebrovascular
disease. Stroke 16:241–244
Vandeplassche G, Hermans C, Somers Y, Van de Werf F, de Clerck F (1993) Combined
thromboxane A2 synthase inhibition and prostaglandin endoperoxide receptor antagonism
limits myocardial infarct size after mechanical coronary occlusion and reperfusion at doses
enhancing coronary thrombolysis by streptokinase. J Am Coll Cardiol 21:1269–1279
Violi F, Hiatt W (2007) A critical review of antiplatelet treatment in peripheral arterial disease.
Intern Emerg Med 2:84–87
Watala C, Boncler M, Gresner P (2005) Blood platelet abnormalities and pharmacological
modulation of platelet reactivity in patients with diabetes mellitus. Pharmacol Rep 57
(Suppl):42–58
Yui Y, Hattori R, Takatsu Y, Nakajima H, Wakabayashi A, Kawai C, Kayama N, Hiraku S,
Inagawa T, Tsubojima M et al (1984) Intravenous infusion of a selective inhibitor of throm-
boxane A2 synthetase in man: influence on thromboxane B2 and 6-keto-prostaglandin F1 alpha
levels and platelet aggregation. Circulation 70:599–605
Zuccollo A, Shi C, Mastroianni R, Maitland-Toolan KA, Weisbrod RM, Zang M, Xu S, Jiang B,
Oliver-Krasinski JM, Cayatte AJ, Corda S, Lavielle G, Verbeuren TJ, Cohen RA (2005) The
thromboxane A2 receptor antagonist S18886 prevents enhanced atherogenesis caused by
diabetes mellitus. Circulation 112:3001–3008
286 G. Davı et al.




![ofCardiac f3-Adrenergic Receptorsby(-) [3H]Alprenolol Binding · g-adrenergic antagonists suchas propranolol is several orders of magnitude lower than the affinity of the physiologic,-receptors](https://img.pdfslide.net/doc/110x75/5f1ba8b995455a76d85168e7/ofcardiac-f3-adrenergic-receptorsby-3halprenolol-binding-g-adrenergic-antagonists.jpg)