Embed Size (px)
Citation preview
Ta
S
F
raotorecwiwpsRweb
DH
0d
Seminars in Diagnostic Pathology 22, 198-212
hymic carcinoma: update of current diagnostic criteriand histologic types
aul Suster, MD
rom the Department of Pathology, The Ohio State University and James Cancer Center, Columbus, Ohio.
Thymic carcinomas are rare tumors thought to derive from thymic epithelium. Because of the complexembryological origin of the thymus, whose development includes contributions from the third and, toa lesser extent, the fourth pharyngeal pouches, thymic carcinomas are endowed with great morphologicheterogeneity. A large number of histologic types have been described that resemble tumors arising inother organs. Unfortunately, no definitive pathognomonic histological features or immunohistochem-ical markers are associated with these tumors, making them a real challenge for diagnosis. Because oftheir close similarity with tumors arising at other organs, the diagnosis of thymic carcinoma must beregarded, for the most part, as a diagnosis of exclusion. This review will focus on current criteria fordiagnosis of these tumors, with a review of the various histopathologic appearances that they can adopt.© 2005 Elsevier Inc. All rights reserved.
KEYWORDSThymic carcinoma;Histologicclassification;Diagnostic criteria;Prognosis
acetorrefl
C
TnRasct
Thymic carcinomas have attracted much attention in theecent literature because of their morphologic heterogeneitynd difficulties for precise diagnosis. Because of their lackf organotypical features of thymic differentiation, theseumors were for many years considered as a manifestationf metastatic disease from an occult primary. The firstecognition of such tumors as a primary neoplasm of thymicpithelium was in the study in 1977 by Shimosato andoworkers of squamous cell carcinoma of the thymus.1 Thisas followed by a study by Snover and coworkers2 in 1982
n which several additional histologic variants of this tumorere delineated. Since then, numerous articles have ap-eared in the literature addressing this topic. The largesttudy on these tumors was published in 1991 by Suster andosai.3 In this study of 60 cases, various histologic subtypesere identified, the majority of which could be assigned to
ither a high- or low-grade histologic category, with clinicalehavior paralleling their morphology. Despite the many
Address reprint requests and correspondence: Saul Suster, MD,epartment of Pathology, The Ohio State University Hospital, E411 Doanall, 410 West 10th Avenue, Columbus, OH 43210.
fE-mail address: [email protected].
740-2570/$ -see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1053/j.semdp.2006.02.006
dvances in our understanding of these tumors, thymicarcinoma remains an elusive diagnosis. With very fewxceptions, it continues to be a diagnosis of exclusion, sincehe possibility of a late metastasis or of spread from anccult primary to the mediastinum must always be firstuled out before making this diagnosis. Herein we willeview the current status on these tumors along with anvaluation of the role of special stains and other techniquesor diagnosis and of the most recently described morpho-ogic variants.
linical features and diagnostic criteria
hymic carcinomas are, in general terms, highly aggressiveeoplasms. In the largest study published by Suster andosai,3 two distinct clinical groups were identified: onessociated with a favorable clinical behavior with longurvival, and one associated with a rapidly fatal clinicalourse. These two clinical groups directly correlated withhe histologic grade of the lesions, with the group exhibiting
avorable prognosis being associated with low-grade histol-
owleifrtctw
mtnpmsOatccgdcsshs
todnmsdosllasedcbsaecbrid
eshtco
H
Tlctomnctdbaletlmnrtsw
199Suster Thymic Carcinoma
gy, and the cases with a poor prognosis being associatedith high-grade histology. At the time that paper was pub-
ished, criteria for the morphologic classification of thymicpithelial neoplasms were not yet very well developed and,n retrospect, many of the tumors included in the low-grade,avorable prognostic clinical category most likely would beeclassified today as atypical thymomas (WHO type B3hymoma). The majority of cases that would qualify underurrent criteria for a diagnosis of thymic carcinoma areherefore more likely to correspond to high-grade tumorsith highly aggressive behavior.4–6
Thymic carcinoma can occur in all age groups but isost frequent in adults between 30 and 60 years of age.3 In
he study by Suster and Rosai, a slight male predilection wasoted (1.5:1 male-to-female).3 The majority of patientsresent with symptoms directly attributable to the anteriorediastinal location of the mass, including chest pain,
hortness of breath, and the superior vena cava syndrome.ther symptoms include weight loss, fatigue, fever, and
norexia, and less commonly hypertrophic pulmonary os-eoarthropathy. In a small percentage of patients, the lesionsan be asymptomatic and incidentally discovered on routinehest X-rays.3 Cases associated with a history of myastheniaravis before the development of the tumor have beenescribed3,7,8; in two cases, development of a thymic car-inoma from a preexisting thymoma in patients with long-tanding myasthenia gravis could be histologically demon-trated.7 The tumors often present in advanced stages;owever, examples of well-circumscribed and even encap-ulated lesions can be observed.
Thymic carcinoma is histologically defined as a primaryhymic epithelial neoplasm showing overt cytologic featuresf malignancy with absence of the organotypical features ofifferentiation of the thymus.4 – 6,9,10 Because of the highlyonspecific histology of thymic carcinoma, the criteria foraking this diagnosis should be, in the majority of in-
tances, based on a combination of clinical and morphologicata. The diagnosis of thymic carcinoma, with the exceptionf select cases, cannot be established in a vaccum basedolely on histopathologic examination. The role of histo-ogic examination is mainly to confirm a diagnosis of ma-ignancy (ie, establish the presence of overt cytologicaltypia) and to specify the morphologic type of the lesion (ie,quamous, basaloid, lymphoepithelioma-like, sarcomatoid,tc). It cannot be over-emphasized that there is nothingistinctive or pathognomonic about the histology of thymicarcinoma that can help establish a definitive diagnosisased solely on histologic examination of a biopsy or re-ected specimen. Thorough clinical and radiological studiesre needed to demonstrate the absence of an occult tumorlsewhere or to elicit a history of a remote primary. In manyases, the answer to this question may only be determinedy means of a postmortem examination.3 Exceptions to thisule include cases in which obvious transitions with preex-sting thymic epithelium9 or with well-differentiated areas
isplaying the conventional organotypical features of a pre- nxisting thymoma are demonstrated,7 or when dealing withome variants of thymic carcinoma whose features are soighly distinctive that origin from an alternate source otherhan the thymus would be highly unlikely, such as basaloidarcinoma of the thymus with cystic changes or carcinomaf the thymus with rhabdomyomatous cells.
istopathologic types
hymic carcinoma can show a wide spectrum of morpho-ogic features. A large number of histologic types of thymicarcinoma have been described, the majority of which seemo have their counterpart in similar tumors arising in otherrgans (Table 1). The morphologic spectrum of these tu-ors ranges from that of low-grade, well-differentiated
eoplasms, to high-grade poorly differentiated malignan-ies. A common feature of all thymic carcinomas is the facthat they lack any of the organotypical features of thymicifferentiation (ie, lobulation separated by broad fibrousands originating from the capsule, perivascular spaces,reas of “medullary” differentiation, and a dual cell popu-ation composed of immature T-lymphocytes and thymicpithelial cells). When present, the lymphoid component inhese tumors is made up of either mature T-cells or B-ymphocytes/plasma cells. The most common type of thy-ic carcinoma in Western patients is poorly differentiated,
onkeratinizing squamous cell carcinoma. Primary neu-oendocrine carcinomas of the thymus are a special categoryhat, although belonging in the same family of tumors, shareeveral common features that merit special attention. Theseill be discussed in a separate article in this issue (see
Table 1 Histologic types of thymic carcinoma
Squamous cell carcinoma- Well-differentiated, keratinizing- Moderately differentiated- Poorly-differentiated, non-keratinizing (lymphoepithelioma-
like)Neuroendocrine carcinomaMucoepidermoid carcinomaClear cell carcinomaBasaloid carcinomaCarcinosarcomaSpindle cell (sarcomatoid) carcinomaPapillary carcinomaAdenocarcinoma
- Mucinous- Non-mucinous
Adenosquamous carcinomaDesmoplastic carcinomaAnaplastic carcinomaRhabdoid carcinomaOther rare types
- Hepatoid carcinoma- Rhabdomyomatous carcinoma
euroendocrine carcinoma of the thymus).
S
tppcdtdelafilsmcaat
nopacpabtnaiSfRt
iatmmcrfomTcerpttmc
ccgwlsMwppompmftccF
t
Fo
200 Seminars in Diagnostic Pathology, Vol 22, No 3
quamous cell carcinoma of the thymus
Shimosato and coworkers1 were the first to recognizeumors with features of squamous differentiation as exam-les of primary carcinoma of the thymus. Additional exam-les were subsequently identified.3,11–14 Primary squamousell carcinoma of the thymus can manifest in three formsepending on their degrees of differentiation: well-differen-iated (keratinizing) squamous cell carcinoma, moderatelyifferentiated squamous cell carcinoma, and poorly differ-ntiated (nonkeratinizing) squamous cell carcinoma. Theatter often shows a distinctive syncytial growth patternccompanied by a heavy lymphoplasmacellular stromal in-ltrate, reason why it was dubbed “lymphoepithelioma-
ike” carcinoma of the thymus to acknowledge the closeimilarity with its counterpart in the nasopharynx.2 Squa-ous cell carcinoma is the most common type of thymic
arcinoma.6,8 Most cases occur in middle aged adults withslightly increased female ratio. The tumor presents as an
nterior mediastinal mass, usually invading adjacent struc-ures, with frequent lymph node metastases.
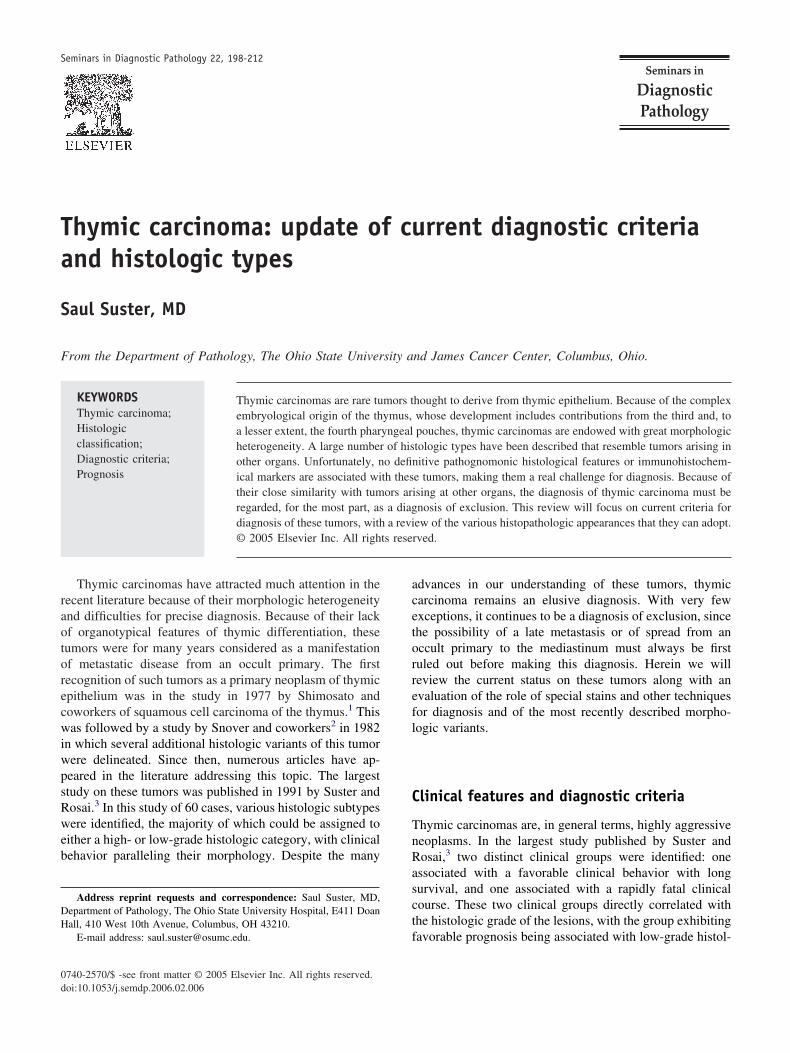
Well-differentiated, keratinizing squamous cell carci-oma shows identical features to its common counterpart inther organs. It is composed of nests or cords of large,olygonal tumor cells showing a pavement-like, epidermoidrrangement. The tumor cells display overt evidence ofytologic atypia manifested by large, vesicular nuclei withrominent eosinophilic nucleoli and mitoses. The cells usu-lly have thick cell membranes and often show intercellularridges. Foci of keratinization and squamous pearl forma-ion are usually easily identified (Figure 1). Focal areas ofecrosis may be present. The tumors are widely invasivend often display a desmoplastic stroma, with accompany-ng neutrophilic, eosinophilic, or lymphocytic infiltration.ome cases can show transitions with areas bearing theeatures of organotypical or atypical thymoma1,7 (Figure 2).are cases have been described in association with mul-
ilocular thymic cysts.15,16 The main differential diagnoses
igure 1 Well-differentiated squamous cell carcinoma of the
whymus with focus of keratin pearl formation.nclude a metastasis of squamous cell carcinoma to medi-stinal lymph nodes and atypical thymoma (WHO type B3hymoma). Distinction of these tumors from atypical thy-oma can be sometimes difficult. In fact, it is likely thatany of the cases reported as well-differentiated squamous
ell carcinoma of the thymus in the literature actually cor-espond to atypical thymomas.1,3,6 The main distinguishingeatures between these two entities include the extensive, aspposed to focal nature of the keratinizing areas in squa-ous cell carcinoma, and the demonstration of immature-lymphocytes intimately admixed with the epithelial tumorells in atypical thymoma. The possibility that well-differ-ntiated squamous cell carcinoma of the thymus arises as aesult of tumor progression from atypical thymoma is sup-orted by the frequent areas of transition observed betweenhese two neoplasms and the overlap in histologic featureshat both can display.7 This could also explain the much
ore favorable prognosis of well-differentiated thymic car-inoma, which closely parallels that of atypical thymoma.1,6
Moderately differentiated squamous cell carcinoma isharacterized by more pronounced cytologic atypia and lesslear-cut evidence of squamous differentiation. The cellsenerally display a higher nuclear-to-cytoplasmic ratio,ith more frequent mitoses and loss of clear-cut intercellu-
ar bridges. Keratinization is usually very focal and incon-picuous and keratin pearls are generally absent (Figure 3).
any of the tumor cells display single cell keratinization,ith deeply eosinophilic cytoplasm surrounding smalliknotic or degenerating nuclei. Areas of necrosis are morerominent than in the well-differentiated tumors and may beften confluent. Lymphovascular invasion is also com-only seen. Some tumors can show prominent peripheral
alisading of tumor cells around small tumor islands. Theost important differential diagnosis is with a metastasis
rom a squamous cell carcinoma of the lung. This distinc-ion is of clinical importance since primary squamous cellarcinoma of the thymus follows a better prognosis than aomparable primary squamous cell carcinoma of the lung
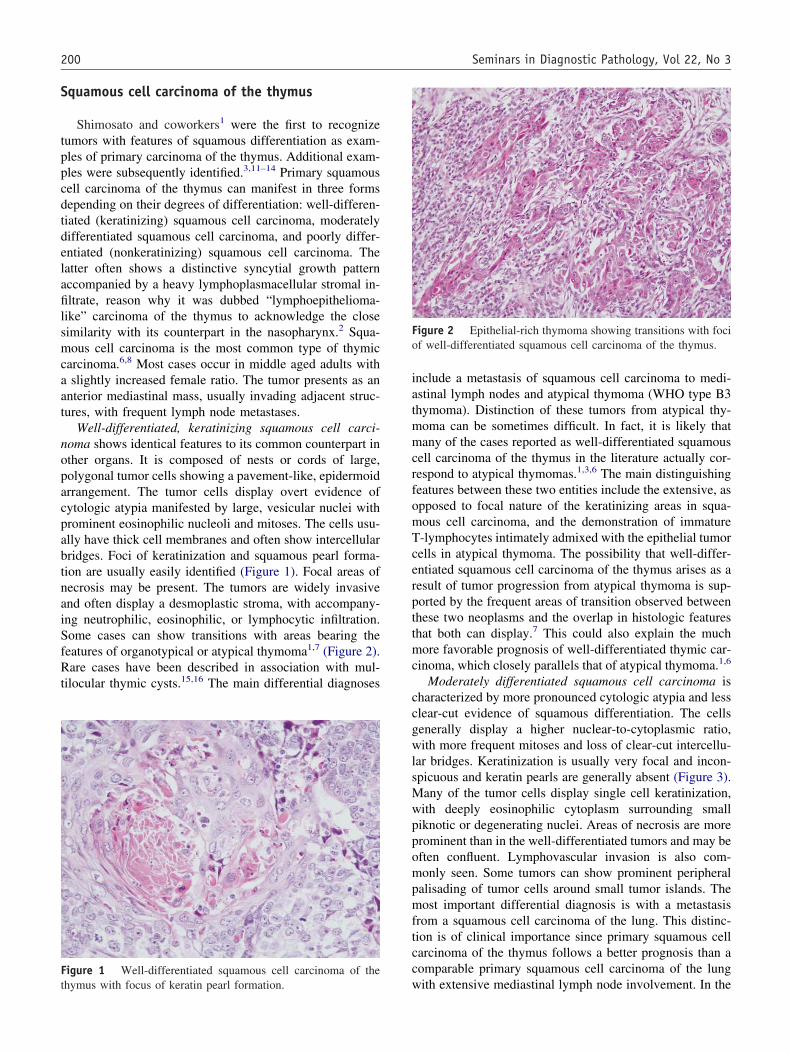
igure 2 Epithelial-rich thymoma showing transitions with focif well-differentiated squamous cell carcinoma of the thymus.
ith extensive mediastinal lymph node involvement. In the
staasnim
ctunblsc(tchcnlt
occhstdioai
wsomAsbipTptntcat
Fst
Fcs
Fc
201Suster Thymic Carcinoma
tudy by Shimosato and coworkers,1 in all cases in whichhe primary thymic tumors could be successfully excisednd treated with postoperative radiation, the patients werelive and well from 1 to 12 years after diagnosis. Endo-copic examination and detailed radiographic studies areecessary to demonstrate absence of bronchial compromisen such tumors and to rule out the possibility of massiveediastinal extension from a bronchogenic primary lesion.Poorly differentiated (nonkeratinizing) squamous cell
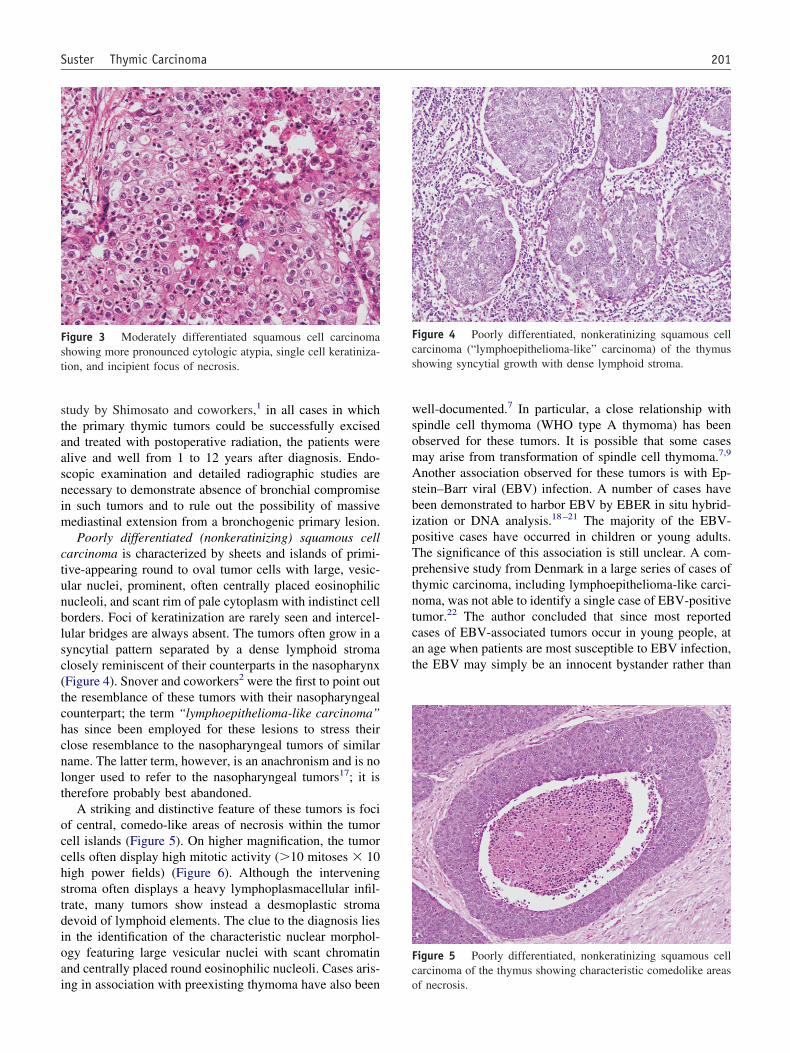
arcinoma is characterized by sheets and islands of primi-ive-appearing round to oval tumor cells with large, vesic-lar nuclei, prominent, often centrally placed eosinophilicucleoli, and scant rim of pale cytoplasm with indistinct cellorders. Foci of keratinization are rarely seen and intercel-ular bridges are always absent. The tumors often grow in ayncytial pattern separated by a dense lymphoid stromalosely reminiscent of their counterparts in the nasopharynxFigure 4). Snover and coworkers2 were the first to point outhe resemblance of these tumors with their nasopharyngealounterpart; the term “lymphoepithelioma-like carcinoma”as since been employed for these lesions to stress theirlose resemblance to the nasopharyngeal tumors of similarame. The latter term, however, is an anachronism and is noonger used to refer to the nasopharyngeal tumors17; it isherefore probably best abandoned.
A striking and distinctive feature of these tumors is focif central, comedo-like areas of necrosis within the tumorell islands (Figure 5). On higher magnification, the tumorells often display high mitotic activity (�10 mitoses � 10igh power fields) (Figure 6). Although the interveningtroma often displays a heavy lymphoplasmacellular infil-rate, many tumors show instead a desmoplastic stromaevoid of lymphoid elements. The clue to the diagnosis liesn the identification of the characteristic nuclear morphol-gy featuring large vesicular nuclei with scant chromatinnd centrally placed round eosinophilic nucleoli. Cases aris-
igure 3 Moderately differentiated squamous cell carcinomahowing more pronounced cytologic atypia, single cell keratiniza-ion, and incipient focus of necrosis.
ng in association with preexisting thymoma have also been o
ell-documented.7 In particular, a close relationship withpindle cell thymoma (WHO type A thymoma) has beenbserved for these tumors. It is possible that some casesay arise from transformation of spindle cell thymoma.7,9
nother association observed for these tumors is with Ep-tein–Barr viral (EBV) infection. A number of cases haveeen demonstrated to harbor EBV by EBER in situ hybrid-zation or DNA analysis.18 –21 The majority of the EBV-ositive cases have occurred in children or young adults.he significance of this association is still unclear. A com-rehensive study from Denmark in a large series of cases ofhymic carcinoma, including lymphoepithelioma-like carci-oma, was not able to identify a single case of EBV-positiveumor.22 The author concluded that since most reportedases of EBV-associated tumors occur in young people, atn age when patients are most susceptible to EBV infection,he EBV may simply be an innocent bystander rather than
igure 4 Poorly differentiated, nonkeratinizing squamous cellarcinoma (“lymphoepithelioma-like” carcinoma) of the thymushowing syncytial growth with dense lymphoid stroma.
igure 5 Poorly differentiated, nonkeratinizing squamous cellarcinoma of the thymus showing characteristic comedolike areas
f necrosis.
huldtcv
M
cstforpmmsompcaasccclic
tmefmcwmmsssscanambvkpicuotdrccictsfT
Fridmi
Ft
202 Seminars in Diagnostic Pathology, Vol 22, No 3
aving any pathogenetic implications. There is also an un-sual case reported in the literature of lymphoepithelioma-ike carcinoma of the thymus with focal neuroblastomatousifferentiation demonstrated by ultrastructural examina-ion.23 Poorly differentiated nonkeratinizing squamous cellarcinoma is a highly aggressive tumor with a mean sur-ival time of approximately 18 months.3
ucoepidermoid carcinoma
Mucoepidermoid carcinoma is a rare form of thymicarcinoma characterized by the intimate admixture ofquamous and mucinous components within the sameumor. The tumors are histologically indistinguishablerom their counterparts in the salivary glands and otherrgans. Although these tumors were initially believed toepresent low-grade carcinomas of the thymus,3,24,25
oorly differentiated and widely invasive cases with auch more aggressive behavior have now been docu-ented.26,27 Approximately 20 cases have been reported
o far in the literature.3,14,24 –27 The tumors can presentver a broad age range, but occur with most frequency iniddle aged adults, without any sex predilection. The
atients can present clinically with symptoms related toompression of adjacent structures due to an expandingnterior mediastinal mass; approximately 50% of casesre asymptomatic. Secondary cystic changes can be ob-erved in association with these tumors in up to 40% ofases,26,27 and will manifest radiographically as multi-ystic masses on chest CT scans. The lesions are grosslyharacterized by relatively well-circumscribed, lobu-ated, rubbery to firm masses showing focal infiltrationnto adjacent structures. The tumors associated with a
igure 6 Higher magnification of poorly differentiated, nonke-atinizing squamous cell carcinoma of the thymus showing prim-tive nuclear morphology, with large, round to oval nuclei withispersed chromatin, small eosinophilic nucleoli, and frequentitoses. Note absence of lymphoplasmacellular stromal infiltrates
n this particular example.
ystic component display on cut surface multiple mul- m
ilocular cystic structures of varying sizes filled withucinous material. Histologically the tumors can display
ither a well-differentiated, low-grade morphology oreatures of high-grade, poorly differentiated mucoepider-oid carcinoma. The well-differentiated neoplasms are
haracterized by sheets and lobules of squamous cellsith minimal atypia displaying intercellular bridges, ad-ixed with singly scattered or small focal collections ofucocytes or goblet cells and small cystically dilated
paces filled with mucin (Figure 7). PAS or mucicarminetains will highlight the cytoplasmic mucin in individualcattered mucocytes, and will also strongly stain theecretions within the cystic spaces. The squamous tumorells usually do not display marked cytologic atypia andre characterized by large, polygonal cells with rounduclei and small nucleoli; mitoses are generally scarcend no areas of necrosis are observed. So-called “inter-ediate” cells, characterized by a squamoid appearance
ut without intercellular bridges are commonly present inarious proportions. Areas of keratinization are rare anderatin pearl formation is almost never seen. Clear cyto-lasmic changes can be observed focally in some tumorsn the squamous component. Cases associated with cystichanges similar to those observed in acquired multiloc-lar thymic cysts can show transitions between the liningf the cysts and the tumor (Figure 8), suggesting that theumor might have arisen from the cyst lining. The poorlyifferentiated variants are characterized by sheets ofound or polygonal tumor cells with occasional smallystic spaces filled with mucinous material. Intermediateells and mucocytes are very scarce and difficult todentify. The cells show enlarged nuclei with increase inhromatin pattern, prominent nucleoli and frequent mi-oses. Foci of necrosis can be identified. The most helpfultain for diagnosis is a mucicarmine, which will highlightoci of intracytoplasmic mucin in scattered tumor cells.ransitions with foci of well-differentiated mucoepider-
igure 7 Well-differentiated mucoepidermoid carcinoma of thehymus showing islands of polygonal squamous cells containing
ultiple cystlike spaces filled with mucin.
ms
tTemtpthictep
C
ecbacctrapactawpwodTb
wpctstpmcip
Ftl
Fta
Fcs
203Suster Thymic Carcinoma
oid carcinoma can also be occasionally seen in well-ampled specimens (Figure 9).26
The clinical behavior of these tumors will depend onhe staging and degree of differentiation of the lesion.umors presenting in high stages and with poorly differ-ntiated histology behave in a much more aggressiveanner than well-circumscribed and well-differentiated
umors. There have been seven tumor-related deaths re-orted so far for these lesions25–27; they all occurred inumors with advanced stage or with poorly differentiatedistology. The differential diagnosis for these lesionsnvolves mainly a late metastasis from a mucoepidermoidarcinoma in the head and neck region or another site. Ahorough clinical history and physical and radiologicalxamination is necessary before making a diagnosis ofrimary thymic mucoepidermoid carcinoma.
igure 8 Well-differentiated mucoepidermoid carcinoma of thehymus (left) showing transitions with the flat cuboidal epitheliumining the cystic cavity.
igure 9 Poorly differentiated mucoepidermoid carcinoma ofhe thymus showing islands of poorly differentiated tumor cells
fdmixed with residual well-differentiated squamoid areas.
lear cell carcinoma of the thymus
Clear cell thymic carcinoma is a rare variant of thymicpithelial neoplasm characterized by cells with abundant opti-ally clear cytoplasm (Figure 10). Fewer than 15 cases haveeen reported so far in the literature.2,3,12–14,28 –30 These tumorsre generally regarded as a high-grade variant of thymic car-inoma with aggressive behavior including massive local re-urrence with infiltration of adjacent organs and distant metas-ases. The largest study by Hasserjian and coworkers30
eported 8 cases of this rare tumor. The tumors affected middleged adults (mean: 52 years) with no sex predilection. Sixatients presented with symptoms of chest pain and dyspneand two were asymptomatic. Tumor size ranged from 4 to 12m, and 2 tumors were grossly cystic. The majority of theumors were widely invasive. In their study, the tumors showed
broad range of cytologic features from uniform clear cellsith minimal atypia, to large, pleomorphic tumor cells withrominent nucleoli. In some cases, transitions of the clear cellsith areas of conventional squamous cell carcinoma could bebserved. In the majority of cases, cytoplasmic glycogen wasemonstrated whereas mucin stains were uniformly negative.here was a striking disparity observed between the ratherland cellular features and the aggressive clinical behavior.
Most of the cases of clear cell tumors of the thymus thate have encountered actually have corresponded to exam-les of well or moderately differentiated squamous cellarcinomas with prominent clear cell change.9 In our cases,ransitions with areas displaying unequivocal features ofquamous differentiation were frequently encountered. Theumors were also often associated with a lobular growthattern and prominent desmoplastic stromal response. Theain differential diagnosis is with metastatic renal cell
arcinoma or a metastasis from other clear cell tumors ofnternal organs. Clinical and radiological correlation is im-ortant for establishing the correct diagnosis. Another pit-
igure 10 Clear cell carcinoma of the thymus. Notice abundantells with optically clear cytoplasm. Other areas of this tumorhowed areas of keratinization.
all for diagnosis is distinction from an as yet underrecog-

ncocsdtmTwcmmctmanttmfshbc
B
liicfcl
bIsTAm1ocmneocassfiwtwtmoicBthr
C
pf
Fmo
Ft
204 Seminars in Diagnostic Pathology, Vol 22, No 3
ized variant of thymoma characterized by prominent clearell changes. These tumors retain the organotypical featuresf thymic differentiation (ie, lobular growth pattern, dualell population with immature T-lymphocytes, perivascularpaces), except that the epithelial tumor cells display abun-ant optically clear cytoplasm. The prognosis for the latterumors is essentially the same as for conventional thymo-as; ie, it will depend on the status of capsular integrity.umors showing extensive invasion at the time of diagnosisill behave in an aggressive fashion similar to thymic
arcinoma, and well-circumscribed and encapsulated tu-ors will behave in an indolent fashion.30 It is possible thatany of these cases may have been misdiagnosed for the
lear cell variant of thymic carcinoma in the past. It isherefore imperative that strict criteria be adhered to inaking the diagnosis of clear cell carcinoma of the thymus,
nd that cytologic and/or architectural features of malig-ancy (ie, nucleolar prominence, mitotic activity, infiltra-ion, lymphovascular invasion) and absence of the organo-ypical features of the thymus be demonstrated beforeaking this diagnosis. A rare tumor showing combined
eatures of thymoma and thymic carcinoma with clear cell,quamous cell and undifferentiated carcinoma componentsas also been described, underscoring the close relationshipetween thymoma and the different variants of thymic car-inoma.31
asaloid carcinoma
Basaloid carcinoma of the thymus is another rare histo-ogical variant characterized by anastomosing cords andslands of small, round, or oval tumor cells showing prom-nent peripheral palisading of nuclei reminiscent of basalell carcinomas of the skin (Figure 11). These tumors arerequently associated with cystic changes. The cystichanges may result from neoplastic transformation of theining in an acquired multilocular thymic cyst or they may
igure 11 Basaloid carcinoma of the thymus showing anasto-osing cords of tumor cells with prominent peripheral palisading
af nuclei.
e secondary to cystic degeneration within the tumor itself.n the latter circumstance, the cells lining the cyst walls willhow similar cytological features as in the tumor cells.here have been ten cases reported in the literature.2,3,32–36
ll tumors were described as large, well circumscribedasses with either focal or extensive cystic changes (Figure
2). The tumor cells in basaloid carcinoma can show a rangef features from bland-appearing oval to spindle shapedells closely reminiscent of the cells in spindle cell thy-oma, to primitive-appearing cells with hyperchromatic
uclei and prominent nucleoli reminiscent of poorly differ-ntiated nonkeratinizing squamous cell carcinoma. Theverriding characteristic is the basaloid arrangement of nu-lei at the periphery of the tumor cell islands. Mitotic figuresre numerous and apoptotic cells can frequently be seencattered throughout. Areas of necrosis are rare. Foci ofquamous differentiation can also be occasionally identi-ed. We have observed cases displaying areas of transitionith conventional spindle cell thymoma. A rare feature is
he presence of focal collections of thymic myoid cellsithin the tumor.9 By immunohistochemical analysis, the
umor cells are reactive for keratin and EMA, and cytoplas-ic tonofilaments and desmosomes have been demonstrated
n ultrastructural examination.33 The differential diagnosisncludes a mediastinal metastasis from a basaloid squamousell carcinoma of the lung or upper aerodigestive tract.asaloid carcinoma is regarded as a low-grade variant of
hymic carcinoma3,33; however, cases with aggressive be-avior, including metastases to lung and liver have beeneported in 30% of cases.2,35,36
arcinosarcoma
Carcinosarcoma is a rare type of biphasic thymic neo-lasm characterized by areas displaying easily identifiableeatures of epithelial differentiation (ie, carcinoma) and
igure 12 Basaloid carcinoma of the thymus showing transi-ions between the tumor and the lining of cystic cavity (top).
reas composed of truly sarcomatous elements. The epithe-
lptstdd“ibchjetsvwe
ndmmmptposbcrttiasdrmtswats
S
ostcfs
ispstcvsSplsltossapwpwhdskmmnbdssthp
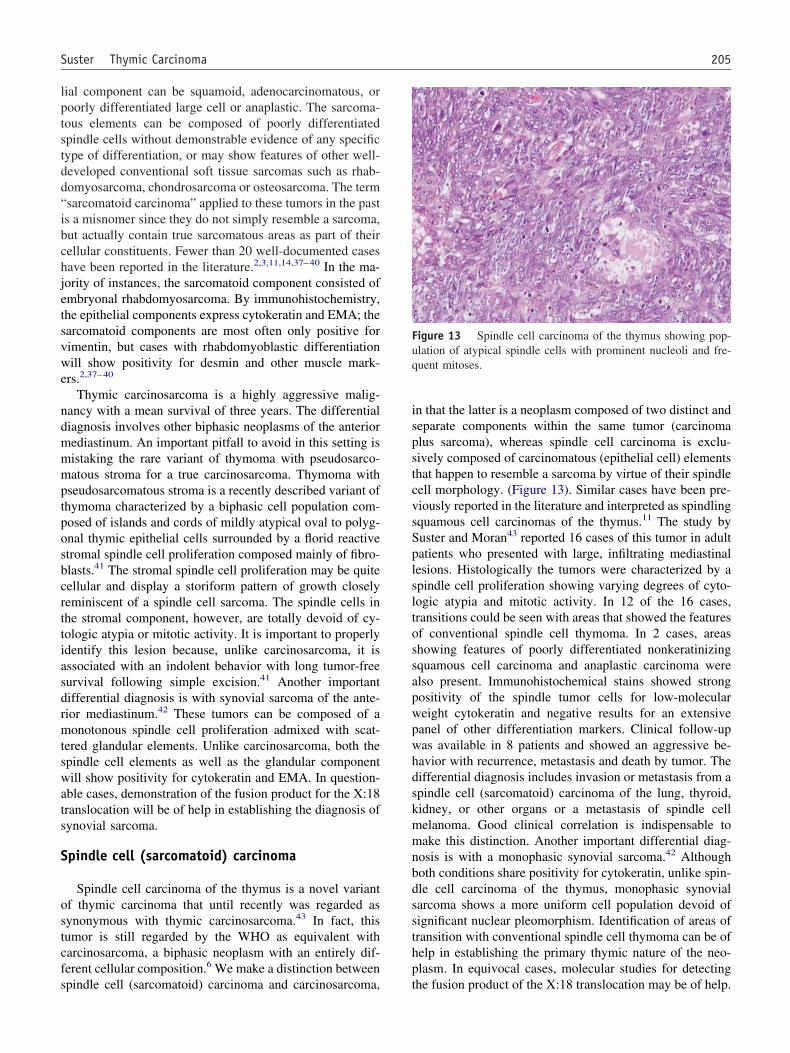
Fuq
205Suster Thymic Carcinoma
ial component can be squamoid, adenocarcinomatous, oroorly differentiated large cell or anaplastic. The sarcoma-ous elements can be composed of poorly differentiatedpindle cells without demonstrable evidence of any specificype of differentiation, or may show features of other well-eveloped conventional soft tissue sarcomas such as rhab-omyosarcoma, chondrosarcoma or osteosarcoma. The termsarcomatoid carcinoma” applied to these tumors in the pasts a misnomer since they do not simply resemble a sarcoma,ut actually contain true sarcomatous areas as part of theirellular constituents. Fewer than 20 well-documented casesave been reported in the literature.2,3,11,14,37– 40 In the ma-ority of instances, the sarcomatoid component consisted ofmbryonal rhabdomyosarcoma. By immunohistochemistry,he epithelial components express cytokeratin and EMA; thearcomatoid components are most often only positive forimentin, but cases with rhabdomyoblastic differentiationill show positivity for desmin and other muscle mark-
rs.2,37– 40
Thymic carcinosarcoma is a highly aggressive malig-ancy with a mean survival of three years. The differentialiagnosis involves other biphasic neoplasms of the anteriorediastinum. An important pitfall to avoid in this setting isistaking the rare variant of thymoma with pseudosarco-atous stroma for a true carcinosarcoma. Thymoma with
seudosarcomatous stroma is a recently described variant ofhymoma characterized by a biphasic cell population com-osed of islands and cords of mildly atypical oval to polyg-nal thymic epithelial cells surrounded by a florid reactivetromal spindle cell proliferation composed mainly of fibro-lasts.41 The stromal spindle cell proliferation may be quiteellular and display a storiform pattern of growth closelyeminiscent of a spindle cell sarcoma. The spindle cells inhe stromal component, however, are totally devoid of cy-ologic atypia or mitotic activity. It is important to properlydentify this lesion because, unlike carcinosarcoma, it isssociated with an indolent behavior with long tumor-freeurvival following simple excision.41 Another importantifferential diagnosis is with synovial sarcoma of the ante-ior mediastinum.42 These tumors can be composed of aonotonous spindle cell proliferation admixed with scat-
ered glandular elements. Unlike carcinosarcoma, both thepindle cell elements as well as the glandular componentill show positivity for cytokeratin and EMA. In question-
ble cases, demonstration of the fusion product for the X:18ranslocation will be of help in establishing the diagnosis ofynovial sarcoma.
pindle cell (sarcomatoid) carcinoma
Spindle cell carcinoma of the thymus is a novel variantf thymic carcinoma that until recently was regarded asynonymous with thymic carcinosarcoma.43 In fact, thisumor is still regarded by the WHO as equivalent witharcinosarcoma, a biphasic neoplasm with an entirely dif-erent cellular composition.6 We make a distinction between
pindle cell (sarcomatoid) carcinoma and carcinosarcoma, tn that the latter is a neoplasm composed of two distinct andeparate components within the same tumor (carcinomalus sarcoma), whereas spindle cell carcinoma is exclu-ively composed of carcinomatous (epithelial cell) elementshat happen to resemble a sarcoma by virtue of their spindleell morphology. (Figure 13). Similar cases have been pre-iously reported in the literature and interpreted as spindlingquamous cell carcinomas of the thymus.11 The study byuster and Moran43 reported 16 cases of this tumor in adultatients who presented with large, infiltrating mediastinalesions. Histologically the tumors were characterized by apindle cell proliferation showing varying degrees of cyto-ogic atypia and mitotic activity. In 12 of the 16 cases,ransitions could be seen with areas that showed the featuresf conventional spindle cell thymoma. In 2 cases, areashowing features of poorly differentiated nonkeratinizingquamous cell carcinoma and anaplastic carcinoma werelso present. Immunohistochemical stains showed strongositivity of the spindle tumor cells for low-moleculareight cytokeratin and negative results for an extensiveanel of other differentiation markers. Clinical follow-upas available in 8 patients and showed an aggressive be-avior with recurrence, metastasis and death by tumor. Theifferential diagnosis includes invasion or metastasis from apindle cell (sarcomatoid) carcinoma of the lung, thyroid,idney, or other organs or a metastasis of spindle cellelanoma. Good clinical correlation is indispensable toake this distinction. Another important differential diag-
osis is with a monophasic synovial sarcoma.42 Althoughoth conditions share positivity for cytokeratin, unlike spin-le cell carcinoma of the thymus, monophasic synovialarcoma shows a more uniform cell population devoid ofignificant nuclear pleomorphism. Identification of areas ofransition with conventional spindle cell thymoma can be ofelp in establishing the primary thymic nature of the neo-lasm. In equivocal cases, molecular studies for detecting
igure 13 Spindle cell carcinoma of the thymus showing pop-lation of atypical spindle cells with prominent nucleoli and fre-uent mitoses.
he fusion product of the X:18 translocation may be of help.
P
rcdeaatciacwocpmspcttictaacscstiicpmotcpmwto
baeascpf
setppeldtdltspclluts
An
ofcna5ntTts
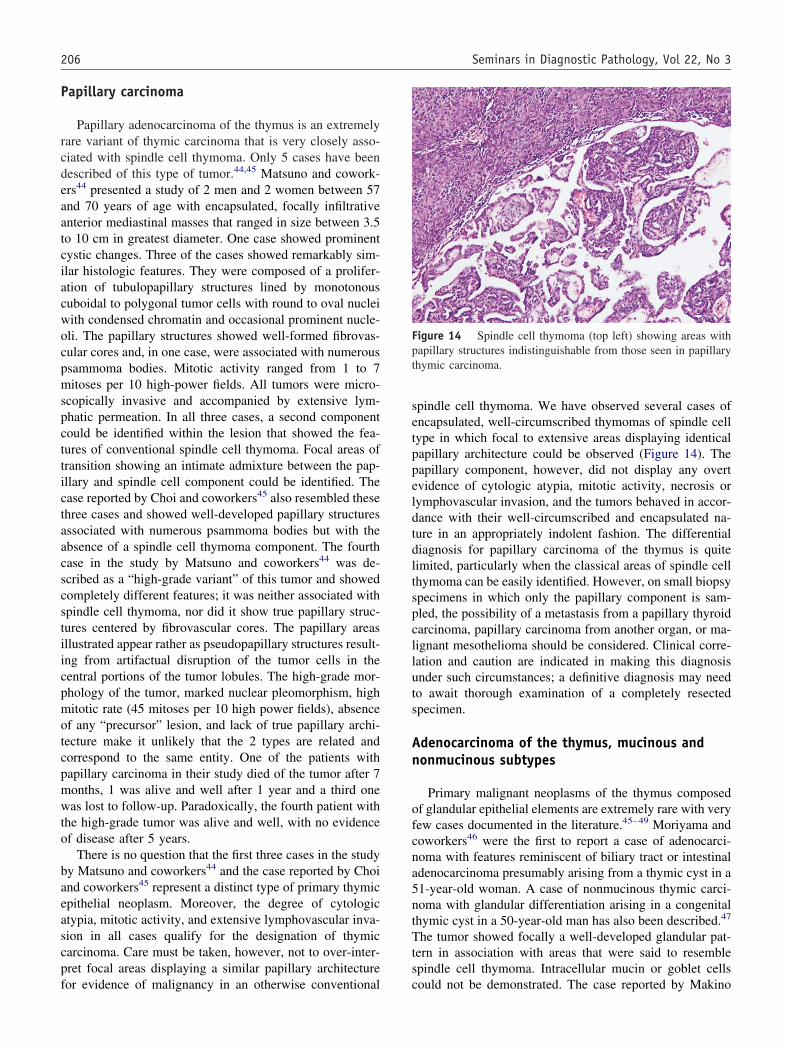
Fpt
206 Seminars in Diagnostic Pathology, Vol 22, No 3
apillary carcinoma
Papillary adenocarcinoma of the thymus is an extremelyare variant of thymic carcinoma that is very closely asso-iated with spindle cell thymoma. Only 5 cases have beenescribed of this type of tumor.44,45 Matsuno and cowork-rs44 presented a study of 2 men and 2 women between 57nd 70 years of age with encapsulated, focally infiltrativenterior mediastinal masses that ranged in size between 3.5o 10 cm in greatest diameter. One case showed prominentystic changes. Three of the cases showed remarkably sim-lar histologic features. They were composed of a prolifer-tion of tubulopapillary structures lined by monotonousuboidal to polygonal tumor cells with round to oval nucleiith condensed chromatin and occasional prominent nucle-li. The papillary structures showed well-formed fibrovas-ular cores and, in one case, were associated with numeroussammoma bodies. Mitotic activity ranged from 1 to 7itoses per 10 high-power fields. All tumors were micro-
copically invasive and accompanied by extensive lym-hatic permeation. In all three cases, a second componentould be identified within the lesion that showed the fea-ures of conventional spindle cell thymoma. Focal areas ofransition showing an intimate admixture between the pap-llary and spindle cell component could be identified. Thease reported by Choi and coworkers45 also resembled thesehree cases and showed well-developed papillary structuresssociated with numerous psammoma bodies but with thebsence of a spindle cell thymoma component. The fourthase in the study by Matsuno and coworkers44 was de-cribed as a “high-grade variant” of this tumor and showedompletely different features; it was neither associated withpindle cell thymoma, nor did it show true papillary struc-ures centered by fibrovascular cores. The papillary areasllustrated appear rather as pseudopapillary structures result-ng from artifactual disruption of the tumor cells in theentral portions of the tumor lobules. The high-grade mor-hology of the tumor, marked nuclear pleomorphism, highitotic rate (45 mitoses per 10 high power fields), absence
f any “precursor” lesion, and lack of true papillary archi-ecture make it unlikely that the 2 types are related andorrespond to the same entity. One of the patients withapillary carcinoma in their study died of the tumor after 7onths, 1 was alive and well after 1 year and a third oneas lost to follow-up. Paradoxically, the fourth patient with
he high-grade tumor was alive and well, with no evidencef disease after 5 years.
There is no question that the first three cases in the studyy Matsuno and coworkers44 and the case reported by Choind coworkers45 represent a distinct type of primary thymicpithelial neoplasm. Moreover, the degree of cytologictypia, mitotic activity, and extensive lymphovascular inva-ion in all cases qualify for the designation of thymicarcinoma. Care must be taken, however, not to over-inter-ret focal areas displaying a similar papillary architecture
or evidence of malignancy in an otherwise conventional cpindle cell thymoma. We have observed several cases ofncapsulated, well-circumscribed thymomas of spindle cellype in which focal to extensive areas displaying identicalapillary architecture could be observed (Figure 14). Theapillary component, however, did not display any overtvidence of cytologic atypia, mitotic activity, necrosis orymphovascular invasion, and the tumors behaved in accor-ance with their well-circumscribed and encapsulated na-ure in an appropriately indolent fashion. The differentialiagnosis for papillary carcinoma of the thymus is quiteimited, particularly when the classical areas of spindle cellhymoma can be easily identified. However, on small biopsypecimens in which only the papillary component is sam-led, the possibility of a metastasis from a papillary thyroidarcinoma, papillary carcinoma from another organ, or ma-ignant mesothelioma should be considered. Clinical corre-ation and caution are indicated in making this diagnosisnder such circumstances; a definitive diagnosis may needo await thorough examination of a completely resectedpecimen.
denocarcinoma of the thymus, mucinous andonmucinous subtypes
Primary malignant neoplasms of the thymus composedf glandular epithelial elements are extremely rare with veryew cases documented in the literature.45– 49 Moriyama andoworkers46 were the first to report a case of adenocarci-oma with features reminiscent of biliary tract or intestinaldenocarcinoma presumably arising from a thymic cyst in a1-year-old woman. A case of nonmucinous thymic carci-oma with glandular differentiation arising in a congenitalhymic cyst in a 50-year-old man has also been described.47
he tumor showed focally a well-developed glandular pat-ern in association with areas that were said to resemblepindle cell thymoma. Intracellular mucin or goblet cells
igure 14 Spindle cell thymoma (top left) showing areas withapillary structures indistinguishable from those seen in papillaryhymic carcinoma.
ould not be demonstrated. The case reported by Makino
ampbfitTopcchmr5uatm(mt
angnbatpnmbehcna
A
mcatadhm
D
o
pdcsoneitebrlsmcbtTs
A
dcinttacothi
Frm
207Suster Thymic Carcinoma
nd coworkers48 in a 39-year-old man presented as a solidass and was unassociated with a cyst; the illustrations
rovided also depict an adenocarcinoma with intestinal oriliary tract-type of features. Choi and coworkers45 were therst to report an example of thymic carcinoma that showed
he features of a mucinous (so-called “colloid”) carcinoma.he tumor occurred in a 15-year-old boy and was composedf islands and small clusters of tumor cells floating in largeools of extracellular mucin. Transitions between the car-inomatous elements and the lining of a residual thymic cystould be observed. The tumor followed an aggressive be-avior with multiple bone metastases and death after 26onths. A similar case of mucinous adenocarcinoma was
eported more recently by Takahashi and coworkers49 in a9-year-old man. The tumor presented as a 10-cm solid,nencapsulated anterior mediastinal mass unassociated withcyst. Following an open chest biopsy, the patient was
reated with radiation therapy with poor success and died 2onths after surgery. It thus appears that the mucinous
“colloid”) variety of primary adenocarcinoma of the thy-us may be associated with a more aggressive behavior
han the nonmucinous types.The differential diagnosis includes a metastasis of an
denocarcinoma from internal organs. This possibilityeeds to always be ruled out by careful clinical and radio-raphic studies before labeling a tumor as a primary ade-ocarcinoma of the thymus. Another condition that needs toe excluded in the differential diagnosis is a carcinomarising from an enteric or foregut cyst.51 For the mucinousumors that resemble so-called “colloid” carcinoma, an im-ortant differential diagnosis is with the rare variant ofeuroendocrine carcinoma of the thymus with prominentucinous stroma.52 The latter condition can closely resem-
le mucinous carcinoma with islands and small clusters ofpithelial cells floating in large pools of mucin. Immuno-istochemical demonstration of positivity for neuroendo-rine markers or ultrastructural demonstration of dense-coreeurosecretory granules will help establish the correct di-gnosis.52
denosquamous carcinoma
Adenosquamous carcinoma is defined as a primary thy-ic epithelial neoplasm in which well-developed glandular
arcinomatous and clearly malignant squamous epithelialreas are admixed within the same lesion.12,13,50 Someumors can also show a small cell carcinoma componentdmixed with the adenosquamous elements.13 The tumorso not differ significantly in clinical presentation and be-avior from otherwise comparable squamous cell carcino-as of the thymus.
esmoplastic carcinoma
We have observed several examples of an unusual form
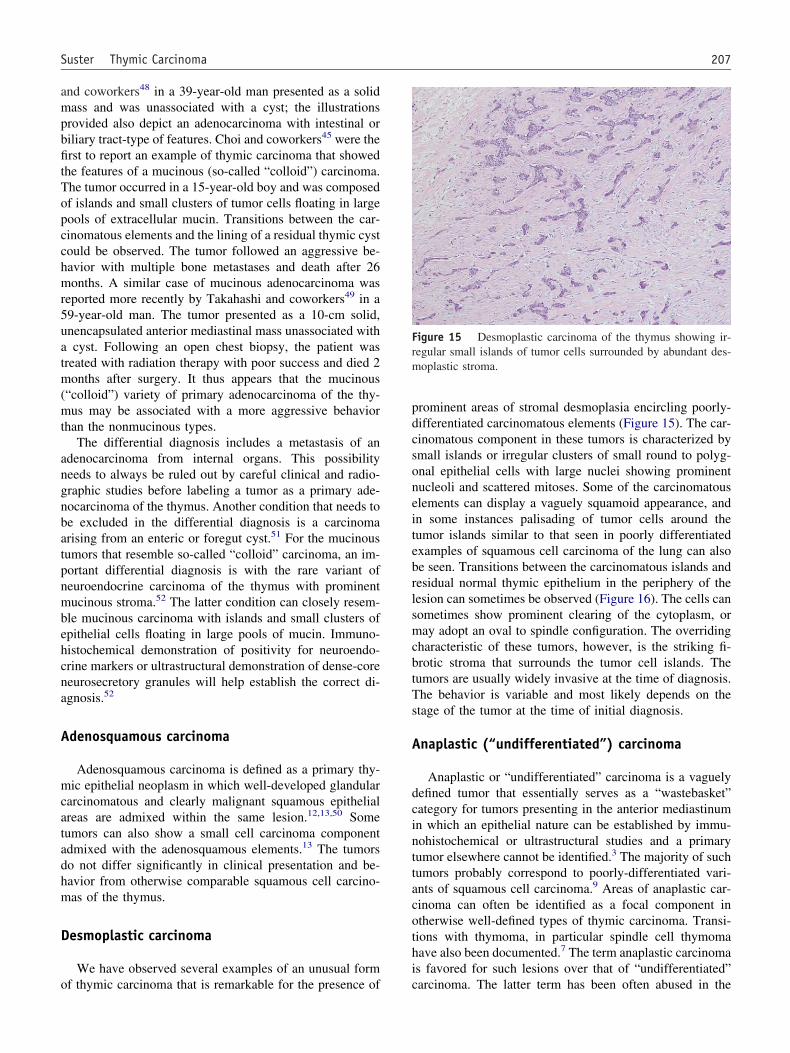
f thymic carcinoma that is remarkable for the presence of crominent areas of stromal desmoplasia encircling poorly-ifferentiated carcinomatous elements (Figure 15). The car-inomatous component in these tumors is characterized bymall islands or irregular clusters of small round to polyg-nal epithelial cells with large nuclei showing prominentucleoli and scattered mitoses. Some of the carcinomatouslements can display a vaguely squamoid appearance, andn some instances palisading of tumor cells around theumor islands similar to that seen in poorly differentiatedxamples of squamous cell carcinoma of the lung can alsoe seen. Transitions between the carcinomatous islands andesidual normal thymic epithelium in the periphery of theesion can sometimes be observed (Figure 16). The cells canometimes show prominent clearing of the cytoplasm, oray adopt an oval to spindle configuration. The overriding
haracteristic of these tumors, however, is the striking fi-rotic stroma that surrounds the tumor cell islands. Theumors are usually widely invasive at the time of diagnosis.he behavior is variable and most likely depends on thetage of the tumor at the time of initial diagnosis.
naplastic (“undifferentiated”) carcinoma
Anaplastic or “undifferentiated” carcinoma is a vaguelyefined tumor that essentially serves as a “wastebasket”ategory for tumors presenting in the anterior mediastinumn which an epithelial nature can be established by immu-ohistochemical or ultrastructural studies and a primaryumor elsewhere cannot be identified.3 The majority of suchumors probably correspond to poorly-differentiated vari-nts of squamous cell carcinoma.9 Areas of anaplastic car-inoma can often be identified as a focal component intherwise well-defined types of thymic carcinoma. Transi-ions with thymoma, in particular spindle cell thymomaave also been documented.7 The term anaplastic carcinomas favored for such lesions over that of “undifferentiated”
igure 15 Desmoplastic carcinoma of the thymus showing ir-egular small islands of tumor cells surrounded by abundant des-oplastic stroma.
arcinoma. The latter term has been often abused in the
llnteftpmtlgmamt
aTuasorl
R
fheydape
csctsdinTeotcHaltm
Flc
Fn
Ft
208 Seminars in Diagnostic Pathology, Vol 22, No 3
iterature and applied indiscriminately to a variety of unre-ated neoplasms, including small cell neuroendocrine carci-omas. It is also contradictory to speak of an “undifferen-iated” carcinoma as the term carcinoma already implies anpithelial line of differentiation, whereas the term “undif-erentiated” designates a tumor without differentiation. Theumors are histologically characterized by marked cellularleomorphism with bizarre nuclear features and atypicalitoses (Figure 17). The differential diagnosis for these
umors includes pleomorphic sarcomas, metastases of ma-ignant melanoma or anaplastic carcinoma from other or-ans, choriocarcinoma and pleomorphic large cell lympho-as of the mediastinum.53,54 Careful clinical correlation
nd application of selected immunohistochemical stainsay be of help in separating anaplastic carcinoma of the
hymus from these conditions.Anaplastic carcinomas of the thymus are associated with
highly aggressive behavior with poor prognosis.3,14,55
here is a recent report, however, of an unusual variant ofndifferentiated large cell carcinoma of the thymus associ-ted with a Castleman disease-like stromal reaction thathowed an indolent behavior despite the high-grade histol-gy.56 It was postulated that the Castleman-like stromalesponse may be related to the indolent behavior of theseesions.
habdoid carcinoma
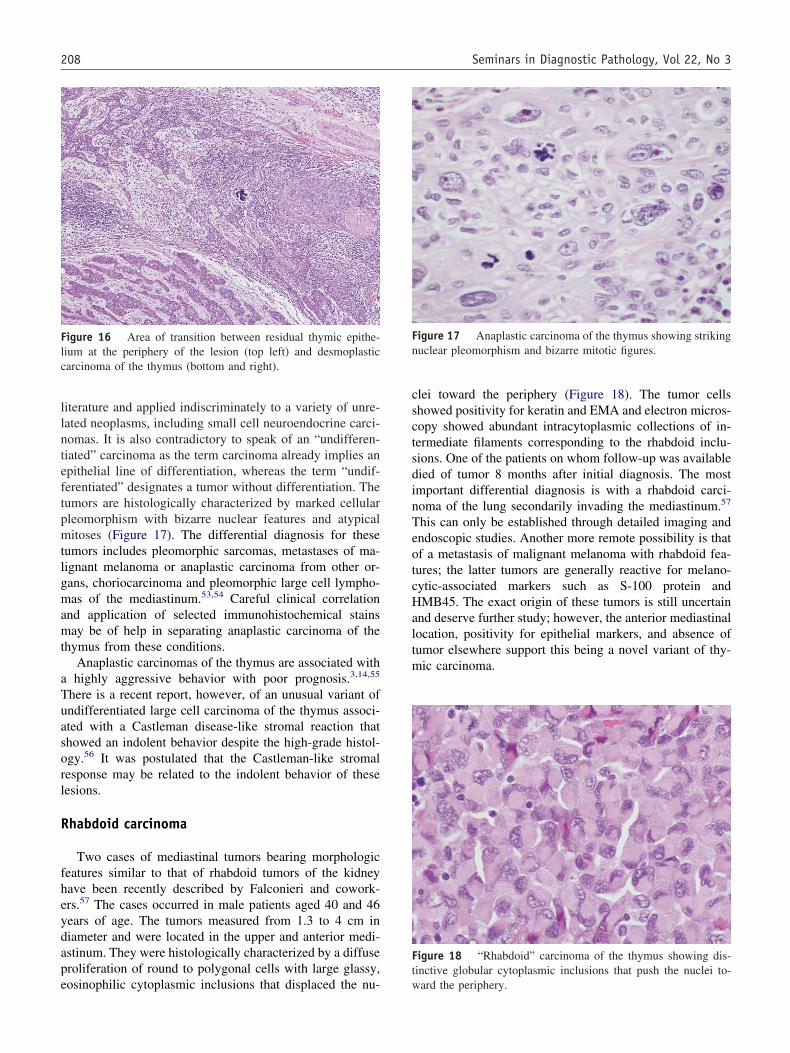
Two cases of mediastinal tumors bearing morphologiceatures similar to that of rhabdoid tumors of the kidneyave been recently described by Falconieri and cowork-rs.57 The cases occurred in male patients aged 40 and 46ears of age. The tumors measured from 1.3 to 4 cm iniameter and were located in the upper and anterior medi-stinum. They were histologically characterized by a diffuseroliferation of round to polygonal cells with large glassy,
igure 16 Area of transition between residual thymic epithe-ium at the periphery of the lesion (top left) and desmoplasticarcinoma of the thymus (bottom and right).
osinophilic cytoplasmic inclusions that displaced the nu- w
lei toward the periphery (Figure 18). The tumor cellshowed positivity for keratin and EMA and electron micros-opy showed abundant intracytoplasmic collections of in-ermediate filaments corresponding to the rhabdoid inclu-ions. One of the patients on whom follow-up was availableied of tumor 8 months after initial diagnosis. The mostmportant differential diagnosis is with a rhabdoid carci-oma of the lung secondarily invading the mediastinum.57
his can only be established through detailed imaging andndoscopic studies. Another more remote possibility is thatf a metastasis of malignant melanoma with rhabdoid fea-ures; the latter tumors are generally reactive for melano-ytic-associated markers such as S-100 protein andMB45. The exact origin of these tumors is still uncertain
nd deserve further study; however, the anterior mediastinalocation, positivity for epithelial markers, and absence ofumor elsewhere support this being a novel variant of thy-ic carcinoma.
igure 17 Anaplastic carcinoma of the thymus showing strikinguclear pleomorphism and bizarre mitotic figures.
igure 18 “Rhabdoid” carcinoma of the thymus showing dis-inctive globular cytoplasmic inclusions that push the nuclei to-
ard the periphery.
O
cr“eedlrtPtrwaccwlpsmps
R
Tsicdlo
ctahchtawstRfa3cti
efwwcrCtdn4vmcMtpcscnvoqwtnt
aHttcithrb(ecinfi
inmsHicds
209Suster Thymic Carcinoma
ther rare types of thymic carcinoma
Other highly unusual morphologic variants of thymicarcinoma have been also described, mostly as single caseeports. A case of thymic carcinoma showing strikinghepatoid” features was reported by Franke and cowork-rs.58 The tumor occurred in a 70-year-old woman as anncapsulated anterior mediastinal mass 18 cm in greatestiameter. Histologically it was composed of sheets of po-ygonal tumor cells or as trabeculae and single cells thatesembled hepatocytes. The tumor cells were immunoreac-ive for cytokeratin and the hepatocyte-specific antigen hep-ar-1, and were negative for a large battery of differentia-
ion markers tested, including AFP, HCG, and PLAP. Localecurrence was noted at 6 months after surgery; the patientas free of disease following radiation and chemotherapy
fter 26 months. An unusual case of thymic carcinomaharacterized by a prominent component of benign rhabdoidells has been described by Moreira de Queiroga and co-orkers.59 The tumor occurred in a 70-year-old woman as a
arge posterior mediastinal mass. Histologically it containedoorly-differentiated adenosquamous carcinoma; inter-persed among the carcinomatous elements were also nu-erous large cells containing brightly eosinophilic cyto-
lasm and small, round eccentrically placed nuclei thattained strongly positive for desmin and myogenin.
ole of special stains and other techniques
he potential use of immunohistochemical stains and ofome of the more novel molecular techniques has beenntensively studied in recent years in the hope that they mayontribute to facilitate the diagnosis and provide predictiveata for clinical outcome in these tumors. Unfortunately,ittle actual progress has been made in this regard and muchf the available data has been contradictory or inconclusive.
A large number of markers have been analyzed in thymicarcinomas. The common minimum denominator for theseumors is the universal expression of cytoplasmic cytoker-tin intermediate filaments in the tumor cells. Some studiesave also shown increased expression of EMA in thymicarcinoma as opposed to thymoma. An interesting findingas been the demonstration of lymphoid markers in theumor cells of thymic carcinoma, including CD5, CD70,nd CD74.60–62 Initial studies seemed very promising and itas proposed that detection of CD5 in the tumor cells could
erve as positive proof to support the diagnosis of primaryhymic carcinoma.60,63,64 In the study by Kornstein andosai,65 the authors found that there were significant dif-
erences in the staining results between two commerciallyvailable CD5 antibodies; clone CD5/54/B4 identified only0% of thymic carcinomas but did not stain other types ofarcinoma, whereas clone 4C7 identified 62% of cases ofhymic carcinoma but also labeled other neoplasms, includ-
ng thymomas, and carcinomas of the stomach, thyroid, Tndometrium and salivary glands. The diagnostic sensitivityor clone CD5/54/B4 was 29% with 100% specificity;hereas the sensitivity of clone 4C7 was found to be 62%ith 96% specificity and a predictive value of 48%. It was
oncluded that clone 4C7 was not sufficiently specific foroutine use, and that strong positive staining with clone5/54/B4 could be used to support a diagnosis of primary
hymic carcinoma. More recent studies have also plainlyemonstrated lack of specificity of CD5 for thymic carci-oma. The study by Tateyama and coworkers66 using theC7 clone showed broad expression of this marker in a wideariety of tumors, including atypical thymomas, malignantesothelioma, lung adenocarcinoma, bladder urothelial car-
inoma, and adenocarcinoma of stomach, colon, and breast.oreover, it should be pointed out that not all variants of
hymic carcinoma are associated with CD5 staining. CD5ositivity is most frequently observed in squamous cellarcinoma of the thymus and has been reported only occa-ionally in poorly differentiated (lymphoepitheliomalike)arcinoma, clear cell carcinoma and papillary carci-oma.60,63,64 Small cell neuroendocrine carcinomas are uni-ersally unreactive for this antigen. Because the diagnosisf thymic carcinoma is a diagnosis of exclusion that re-uires demonstration of absence of a primary tumor else-here, extreme caution should be used in over interpreting
he results of CD5 staining. Additional studies are stilleeded to reliably map the spectrum of immunoreactivity ofhis antibody in nonthymic carcinomas.
CD70, a protein that mediates the interaction between Bnd T-lymphocytes has also been studied in thymic tumors.ishima and coworkers61 in a study of 27 thymic epithelial
umors found that 7/8 thymic carcinomas and 1/5 atypicalhymoma were positive for CD70, whereas the rest of theases, including 13 thymomas, 1 thymic carcinoid and 24ntrathoracic malignancies of nonthymic origin were nega-ive for this marker. The number of cases in this study,owever, was quite limited, and the results of this study stillequire additional validation. Similar observations haveeen made for CD74, a major histocompatibility complexMHC) class II-associated protein.62 This marker was pref-rentially expressed in thymic carcinoma but also markedonventional and atypical thymomas. The study did notnclude an assessment of the expression of this marker inonthymic tumors, thus severely limiting the utility of thisnding for differential diagnosis.
Another aspect of thymic carcinomas that has been stud-ed by immunohistochemistry is the focal expression ofeuroendocrine markers in the tumor cells.67,68 Focal im-unoreactivity for chromogranin, synaptophysin, neuron
pecific enolase (NSE), and a variety of peptides includingCG and ACTH could be detected in scattered tumor cells
n cases of thymic carcinoma of various types and in a fewases of atypical thymoma. This finding was supported byemonstration of dense-core neurosecretory granules incattered cells by electron microscopy in both studies.67,68
his finding has been interpreted as a manifestation of

atm
scKtotvpictoAmdnicPwofntnap
ibob1chcqscti
iamacsiich
teoqtwptcaMdcabdstldim
R
1
1
1
1
1
210 Seminars in Diagnostic Pathology, Vol 22, No 3
berrant differentiation in these neoplasms. Awareness ofhis phenomenon is only of importance to avoid making aisdiagnosis of neuroendocrine carcinoma in such tumors.A series of markers have been studied in an attempt to
eparate thymic carcinoma from thymoma, including p53,-kit (CD117), and Ki-67.69 –72 Overexpression of p53 andi-67 was observed more often in thymic carcinoma than
hymoma.69,72 There appears to be, however, some degreef overlap in the expression of these markers between theseumors that mirrors the complexities encountered on con-entional microscopy, therefore limiting their utility. Ex-ression of c-kit (CD117) has shown considerable prom-se,70,71 since strong staining has been noted in squamousell carcinoma of the thymus and this marker has been, forhe most part, negative in the majority of the cases studiedf thymoma and squamous cell carcinomas at other sites.dditional studies are needed to validate these results. Otherarkers that have been applied with variable success to the
ifferential diagnosis of these tumors include TTF1, calreti-in and other mesothelioma markers.73,74 TTF1 was foundn one study to stain 3/10 cases of large cell undifferentiatedarcinomas of the lung but none of the thymic carcinomas.73
rimary squamous cell carcinomas of the lung, however,ere also negative for this marker. In another study, aboutne third of thymic carcinomas were found to be positiveor calretinin, mesothelin, HBME-1 and CK5/6, and wereegative for TTF1.74 This information is of importance forhe interpretation of small mediastinoscopic biopsies so asot to over interpret the finding of positive mesothelioma-ssociated markers in a mediastinal neoplasm as positiveroof of malignant mesothelioma.
The role of cytogenetics has also been recently addressedn thymic carcinoma. Trisomy 8 and der(16)t(1;16) haveeen reported in a single case of squamous cell carcinomaf the thymus.75 A study using comparative genomic hy-ridization has shown loss of chromosome 16q,6,3p and7p, and gains of 1q,17q and chromosome 18 in thymicarcinoma.76 A single case of carcinosarcoma of the thymusas been studied by cytogenetics, which identified complexhromosomal abnormalities including der(16)t(1;16)(q12;12.1).40 Interestingly, this chromosomal translocation isimilar to that previously encountered in a thymic squamousell carcinoma.75 The cytogenetics of the other histologicypes of thymic carcinoma has not yet been properly stud-ed.
Several cases have been reported in the literature ofntrathoracic malignancies involving the lung and/or medi-stinum that share in common a distinctive t(15;19) chro-osomal translocation.77– 81 These cases have been listed asdistinctive variant of thymic carcinoma in the new WHO
lassification of thymic epithelial neoplasms.6 The tumorshow a predilection for children or young adults, and occurn supra-diaphragmatic midline organs. They are locallynvasive and present with pleural effusion and superior venaava syndrome. The tumors appear to be morphologically
eterogeneous but most often manifest as poorly differen-iated carcinomas similar to nonkeratinizing poorly differ-ntiated (lymphoepitheliomalike) squamous cell carcinomaf the thymus. Foci of squamous differentiation are fre-uently present. All reported cases have shown an ex-remely aggressive behavior with an average survival of 18eeks. Given the uncertainty as to the exact origin andathogenesis of these tumors, I believe it is still prematureo regard them as a separate or distinctive form of thymicarcinoma. Not all cases appear to arise in the mediastinum,nd origin from the thymus has not been demonstrated.oreover, since cytogenetic studies have not yet been un-
ertaken for the lymphoepitheliomalike variant of thymicarcinoma which shares many of the histologic features andggressive clinical behavior with these tumors, the possi-ility that the two may be the same condition cannot beiscounted. Further delineation of this tumor and additionaltudies are necessary to clarify some of these points. For theime being, demonstration of the characteristic 15;19 trans-ocation, or the fusion protein BDR4 by FISH in poorlyifferentiated carcinomas arising in the chest cavity is ofmportance to identify this highly aggressive subset of tu-ors, particularly in children and young adults.18
eferences
1. Shimosato Y, Kameya T, Nagai K, et al: Squamous cell carcinoma ofthe thymus. Am J Surg Pathol 1:109-121, 1977
2. Snover DC, Levine GD, Rosai J: Thymic carcinoma. Five distinctivehistological variants. Am J Surg Pathol 6:451-470, 1982
3. Suster S, Rosai J: Thymic carcinoma. A clinicopathological study of60 cases. Cancer 67:1025-1032, 1991
4. Suster S, Moran CA: Thymoma, atypical thymoma, and thymic car-cinoma. A novel conceptual approach to the classification of neo-plasms of thymic epithelium. Am J Clin Pathol 111:826-833, 1999
5. Suster S, Moran CA: Primary thymic epithelial neoplasms: spectrumof differentiation and histologic features. Semin Diagn Pathol 16:2-17,1999
6. Travis WD, Brambilla E, Muller-Hermelink HK, et al: Pathology andgenetics of tumors of the lung, pleura, thymus and heart, in WorldHealth Organization Classification of Tumours. Lyon, IARC Press,2004
7. Suster S, Moran CA: Primary thymic epithelial neoplasms with com-bined features of thymoma and thymic carcinoma. A clinicopathologicstudy of 22 cases. Am J Surg Pathol 20:1469-1480, 1996
8. Shimosato Y, Mukai K: Atlas of Tumor Pathology: Tumors of theMediastinum, Armed Forces Institute of Pathology (ed 3). WashingtonDC, 1977
9. Suster S, Moran CA: Thymic carcinoma: spectrum of differentiationand histologic types. Pathology 30:111-122, 1998
0. Suster S, Moran CA: The mediastinum, in Weidner N, Cote RJ, SusterS, et al (eds): Modern Surgical Pathology. Philadelphia, PA, WBSaunders Co, 2003, pp 439-504
1. Wick MR, Weiland LH, Scheithauer BW, et al: Primary thymiccarcinomas. Am J Surg Pathol 6:451-470, 1982
2. Truong LD, Mody DR, Cagle PT, et al: Thymic carcinoma: a clini-copathologic study of 13 cases. Am J Surg Pathol 14:151-166, 1990
3. Kuo T-T, Chang J-P, Lin F-J, et al: Thymic carcinomas: histopatho-logical varieties and immunohistochemical study. Am J Surg Pathol14:24-34, 1990
4. Chalabreysse L, Etienne-Mastroianni B, Adeleine P, et al: Thymiccarcinoma: a clinicopathological and immunohistochemical study of
19 cases. Histopathology 44:367-374, 2004
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
211Suster Thymic Carcinoma
5. Leong AS, Brown JH: Malignant transformation in a thymic cyst.Am J Surg Pathol 8:471-475, 1984
6. Fukayama M, Nihei Z, Takizawa T, et al: A case of squamous cellcarcinoma of the thymus, probably originating from thymic cyst. LungCancer 24:415-420, 1984
7. Shanmugaratnam K, Sobin LH, Barnes L, et al: World Health Orga-nization Histological Classification of Tumors. Histological Typing ofTumors of the Upper Respiratory Tract and Ear (ed 2). Berlin,Springer-Verlag, 1991, pp 32–33
8. Dimery IW, Lee JS, Blick M, et al: Association of the Epstein-Barrvirus with lymphoepithelioma of the thymus. Cancer 61:2475-2480,1988
9. Wu TC, Kuo T-T: Study of Epstein-Barr virus early RNA-1 (EBER1)expression by in-situ hybridization in thymic epithelial tumors ofChinese patients in Taiwan. Hum Pathol 24:235-238, 1993
0. Chan PC, Pan CC, Yang AH, et al: Detection of Epstein-Barr virusgenome within thymic epithelial tumors in Taiwanese patients bynested PCR, PCR in-situ hybridization, and RNA in-situ hybridization.J Pathol 197:684-688, 2002
1. Hsueh C, Kuo T-T, Tsang NM, et al: Thymic lymphoepithelioma-likecarcinoma in children: detection of EBV encoded latent membraneprotein-1 gene without 30-bp deletion. Mod Pathol 15:312A, 2002(suppl)
2. Engel PJH: Absence of latent Epstein-Barr virus in thymic epithelialtumors as demonstrated by Epstein-Barr-encoded RNA (EBER) in situhybridization. APMIS 108:393-397, 2000
3. Alguacil-Garcia A, Halliday WC: Thymic carcinoma with focal neu-roblastomatous differentiation. Am J Surg Pathol 11:474-479, 1987
4. Brightman I, Morgan JA, Kunze WP, et al: Primary mucoepidermoidcarcinoma of the thymus: a rare cause of mediastinal tumor. ThoracCardiovasc Surg 40:90-91, 1991
5. Tanaka M, Shimokawa R, Matsubara O, et al: Mucoepidermoid car-cinoma of the thymic region. Acta Pathol Jpn 32:703-712, 1982
6. Moran CA, Suster S: Mucoepidermoid carcinomas of the thymus.Clinicopathologic study of 6 cases. Am J Surg Pathol 19:826-834,1995
7. Nonaka D, Klimstra D, Rosai J: Thymic mucoepidermoid carcinomas.A clinicopathologic study of 10 cases and review of the literature.Am J Surg Pathol 28:1526-1531, 2004
8. Stephens M, Khalin J, Gibbs AR: Primary clear cell carcinoma of thethymus gland. Histopathology 11:763-765, 1987
9. Wolfe JTI, Wick MR, Banks PM, et al: Clear cell carcinoma of thethymus. Mayo Clin Proc 58:365-370, 1983
0. Hasserjian RP, Klimstra DS, Rosai J: Carcinoma of the thymus withclear cell features. Report of eight cases and review of the literature.Am J Surg Pathol 19:835-841, 1995
1. Kuo TT, Chan JKC: Thymic carcinoma arising in thymoma is asso-ciated with alterations in immunohistochemical profile. Am J SurgPathol 22:1474-1481, 1998
2. Hoffman W, Moller P, Manke H-G, et al: Thymoma. A clinicopath-ologic study of 98 patients with special reference to three unusualcases. Pathol Res Pract 179:337-353, 1985
3. Iezzoni JC, Nass LB: Thymic basaloid carcinoma. A case report andreview of the literature. Mod Pathol 9:21-25, 1996
4. Kawashima O, Kamiyoishihara M, Skata S, et al: Basaloid carcinomaof the thymus. Ann Thorac Surg 68:1863-1865, 1999
5. Natsuo T, Hayashida R, Kobayashi K, et al: Thymic basaloid carci-noma with hepatic metastases. Ann Thorac Surg 74:579-582, 2002
6. Tanimura S, Tomoyasu H, Kohno T, et al: Basaloid carcinoma orig-inating from the wall of thymic cyst presenting as pericardial andthoracic effusion; report of a case. Kyobu Geka 55:571-575, 2002
7. Suarez-Vilela D, Salas-Valien JS, Gonzalez-Moran MA, et al: Thymiccarcinosarcoma associated with a spindle cell thymoma: an immuno-histochemical study. Histopathology 21:263-268, 1992
8. Nishimura M, Kodama T, Nishiyama H, et al: A case of sarcomatoidcarcinoma of the thymus. Pathol Int 47:260-263, 1997
9. Okudela K, Nakamura N, Sano J, et al: Thymic carcinosarcoma
consisting of squamous cell carcinomatous and embryonal rhab-domyosarcomatous components. Report of a case and review of theliterature. Pathol Res Pract 197:205-210, 2001
0. Eimoto T, Kitaoka M, Ogawa H, et al: Thymic sarcomatoid carcinomawith skeletal muscle differentiation: report of two cases, one withcytogenetic analysis. Histopathology 40:46-57, 2002
1. Suster S, Moran CA, Chan JKC: Thymoma with pseudosarcomatousstroma. Report of an unusual variant of thymic epithelial neoplasm thatmay simulate carcinosarcoma. Am J Surg Pathol 21:1216-1223, 1997
2. Suster S, Moran CA: Primary synovial sarcomas of the mediastinum.A clincopathological, immunohistochemical and ultrastructural studyof 15 cases. Am J Surg Pathol 29:569-578, 2005
3. Suster S, Moran CA: Spindle cell carcinoma of the thymus. Clinico-pathologic and immunohistochemical study of 15 cases of a novelform of thymic carcinoma. Am J Surg Pathol 23:691-700, 1999
4. Matsuno Y, Morozumi N, Hirohashi S, et al: Papillary carcinoma ofthe thymus. Report of four cases of a new microscopic type of thymiccarcinoma. Am J Surg Pathol 22:873-880, 1998
5. Choi WWL, Lui YH, Lau WH, et al: Adenocarcinoma of the thymus.Report of two cases, including a previously undescribed mucinoussubtype. Am J Surg Pathol 27:124-130, 2003
6. Moriyama S, Shimizu N, Kurita A: A case of adenocarcinoma of thethymus. Nippon Kyobu Geka Gakkai Zasshi 37:717-722, 1989
7. Babu MK, Nirmala V: Thymic carcinoma with glandular differentia-tion arising in a congenital thymic cyst. J Surg Oncol 57:277-279,1994
8. Makino Y, Asada M, Suzuki T, et al: A case of adenocarcinoma of thethymus. Jpn J Thoracic Cardiovasc Surg 46:1168-1171, 1998
9. Takahashi F, Tsuta K, Matsuno Y, et al: Adenocarcinoma of thethymus: mucinous subtype. Hum Pathol 36:219-223, 2005
0. Matsuno Y, Mukai K, Noguchi M, et al: Histochemical and immuno-histochemical evidence of glandular differentiation in thymic carci-noma. Acta Pathol Jpn 39:433-438, 1989
1. Chuang MT, Barba FA, Kaneko M: Adenocarcinoma arising in anintrathoracic duplication cyst of foregut origin: a case report withreview of the literature. Cancer 47:1887-1890, 1981
2. Suster S, Moran CA: Thymic carcinoid with prominent mucinousstroma. Report of a distinctive morphologic variant of thymic neu-roendocrine neoplasm. Am J Surg Pathol 19:1277-1285, 1995
3. Suster S, Moran CA: Pleomorphic large cell lymphomas of the medi-astinum. Am J Surg Pathol 20:224-232, 1996
4. Moran CA, Suster S: Primary mediastinal choriocarcinomas. A clini-copathologic and immunohistochemical study of 8 cases. Am J SurgPathol 21:1007-1012, 1997
5. Hsu C-P, Chen C-Y, Chen C-L, et al: Thymic carcinoma. Ten years’experience in twenty patients. J Thorac Cardiovasc Surg 107:615-620,1994
6. Nonaka D, Rodriguez J, Rollo JL, et al: Undifferentiated large cellcarcinoma of the thymus associated with Castleman disease-like reac-tion. A distinctive type of thymic neoplasm characterized by an indo-lent behavior. Am J Surg Pathol 29:490-495, 2005
7. Falconieri G, Moran CA, Pizzolito S, et al: Intrathoracic rhabdoidcarcinoma: a clinicopathological, immunohistochemical and ultra-structural study of 6 cases. Ann Diagn Pathol 9:279-283, 2005
8. Franke A, Strobel P, Fackeldey V, et al: Hepatoid thymic carcinoma.Report of a case. Am J Surg Pathol 28:250-256, 2004
9. Moreira deq Ueiroga E, Chikota H, Bacchi CE, et al: Rhabdomyo-matous carcinoma of the thymus. Am J Surg Pathol 28:1245-1250,2004
0. Hishima T, Fukayama M, Fujisawa M, et al: CD5 expression in thymiccarcinoma. Am J Pathol 145:268-275, 1994
1. Hishima T, Fukayama M, Hayashi Y, et al: CD70 expression in thymiccarcinoma. Am J Surg Pathol 24:742-746, 2000
2. Datta MW, Shahsafaei A, Nadler LM, et al: Expression of MHC classII-associated invariant chain (Ii;CD74) in thymic epithelial neoplasms.Appl Immunohistochem Mol Morph 8:210-215, 2000
3. Berezowski K, Grimes MM, Gal A, et al: CD5 immunoreactivity ofepithelial cells in thymic carcinoma and CSTLE using paraffin-em-
bedded tissue. Am J Clin Pathol 106:483-486, 1996
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
212 Seminars in Diagnostic Pathology, Vol 22, No 3
4. Dorfman DM, Shahsafaei A, Chan JKC: Thymic carcinomas, but notthymomas and carcinomas of other sites, show CD5 immunoreactivity.Am J Surg Pathol 21:936-940, 1997
5. Kornstein MJ, Rosai J: CD5 labeling of thymic carcinomas and othernonlymphoid neoplasms. Am J Clin Pathol 109:722-726, 1998
6. Tateyama H, Eimoto T, Tada T, et al: Immunoreactivity of a new CD5antibody with normal epithelium and malignant tumors includingthymic carcinoma. Am J Clin Pathol 111:235-240, 1999
7. Lauriola L, Erlandson RA, Rosai J: Neuroendocrine differentiation isa common feature of thymic carcinoma. Am J Surg Pathol 22:1059-1066, 1995
8. Hishima T, Fukayama M, Hayashi Y, et al: Neuroendocrine differ-entiation in thymic epithelial tumors with special reference tothymic carcinoma and atypical thymoma. Hum Pathol 29:330-338,1998
9. Nino H, Kondo K, Miyoshi T, et al: High frequency of p53 proteinexpression in thymic carcinoma but not in thymoma. Br J Cancer76:1361-1366, 1997
0. Pan CC, Chen PC, Chieng H: Kit (CD117) is frequently overexpressedin thymic carcinomas but is absent in thymomas. J Pathol 202:375-381, 2004
1. Henley JD, Cummins OW, Loehrer PJ Sr: Tyrosine kinase receptorexpression in thymomas. J Cancer Res Clin Oncol 130:222-224,2004
2. Linden MD, Miller ML, Katzin WE, et al: The role of Ki-67 and T6(CD1) in differentiating thymic carcinomas and thymomas. Am J ClinPathol 90:497A, 1988
3. Pomplun S, Wotherspoon AC, Shah G, et al: Immunohistochemicalmarkers in the differentiation of thymic and pulmonary neoplasms.Histopathology 40:152-158, 2002
4. Pan C-C, Chen P C-H, Chou T-Y, et al: Expression of calretinin andother mesothelioma-associated markers in thymic carcinoma and thy-moma. Hum Pathol 34:1155-1162, 2003
5. Sonobe H, Takeuchi T, Ohtsuki Y, et al: A thymic squamous cellcarcinoma with complex chromosome abnormalities. Cancer GenetCytogenet 103:83-85, 1998
6. Zettl A, Strobel P, Wagner K, et al: Recurrent genetic aberrations inthymoma and thymic carcinoma. Am J Pathol 157:257-266, 2000
7. Kees UR, Mulcahy MT, Willoughby MLN: Intrathoracic carcinoma inan 11 year-old girl showing a translocation t(15;19). Am J Ped He-matol Oncol 13:459-464, 1991
8. Kubonishi I, Takehara N, Iwata J, et al: Novel t(15;19)(q15;p13)chromosome abnormality in a thymic carcinoma. Cancer Res 51:3327-3328, 1991
9. Lee ACW, Kwong Y-I, Fu KH, et al: Disseminated mediastinalcarcinoma with chromosomal translocation (15;19). A distinctive clin-icopathologic syndrome. Cancer 72:2273-2276, 1993
0. French CA, Miyoshi I, Aster JC, et al: BRD4 bromodomain generearrangement in aggressive carcinoma with translocation t(15;19).Am J Pathol 159:1987-1992, 2001
1. Vargas SO, French CA, Faul PN, et al: Upper respiratory tract carci-noma with chromosomal translocation 15;19. Evidence for a distinctdisease entity of young patients with a rapidly fatal course. Cancer92:1195-1203, 2001













![Inflammation and cancer: How hot is the link? · carcinoma [30], colon carcinoma, lung carcinoma, squamous cell carcinoma, pancreatic cancer [31,32], ovarian carcinoma biochemical](https://img.pdfslide.net/doc/110x75/5fcdd6c81c76a34db570e7e6/iniammation-and-cancer-how-hot-is-the-link-carcinoma-30-colon-carcinoma.jpg)














