Embed Size (px)
Citation preview
Thyroid Disease in Pregnancy: The Essentials
Elizabeth N. Pearce, MD, MSc
Disclosures
• None
Case 1
A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy. She has no history of thyroid disease. She has no goiter. Exam findings are normal. Her serum TSH level is 1.9 mIU/L.
Which of the following should you recommend?A. Change to a diet containing animal productsB. Add twice-weekly kelp to current dietC. Start a daily prenatal supplement containing 150 µg iodineD. Change from iodized table salt to sea salt
U.S. and European GuidelinesWomen who are planning to be pregnant or are pregnant or breastfeeding shouldsupplement their diet with a daily oral supplement that contains 150 µg of iodine.
• Alexander EK, Pearce EN, et al. Thyroid 2017;27:315-389• De Groot L et al. J Clin Endocrinol Metab 2012;97:2543-65• SG Obican et al. Birth Defects Res A Clin Mol Teratol2012;94: 677-682• AAP Council on Environmental Health. Pediatrics2014;133:1163-6•JH Lazarus et al. Eur Thyroid J 2014;3:76-94.
Case 2
A 29 yo F presents at 9 weeks gestation. She has no history of thyroid disease. Her serum TSH is 3.4 mIU/L.
Is this a normal TSH value?
1st. Trimester 2nd. Trimester 3rd. Trimester
10 20 30weeks gestation
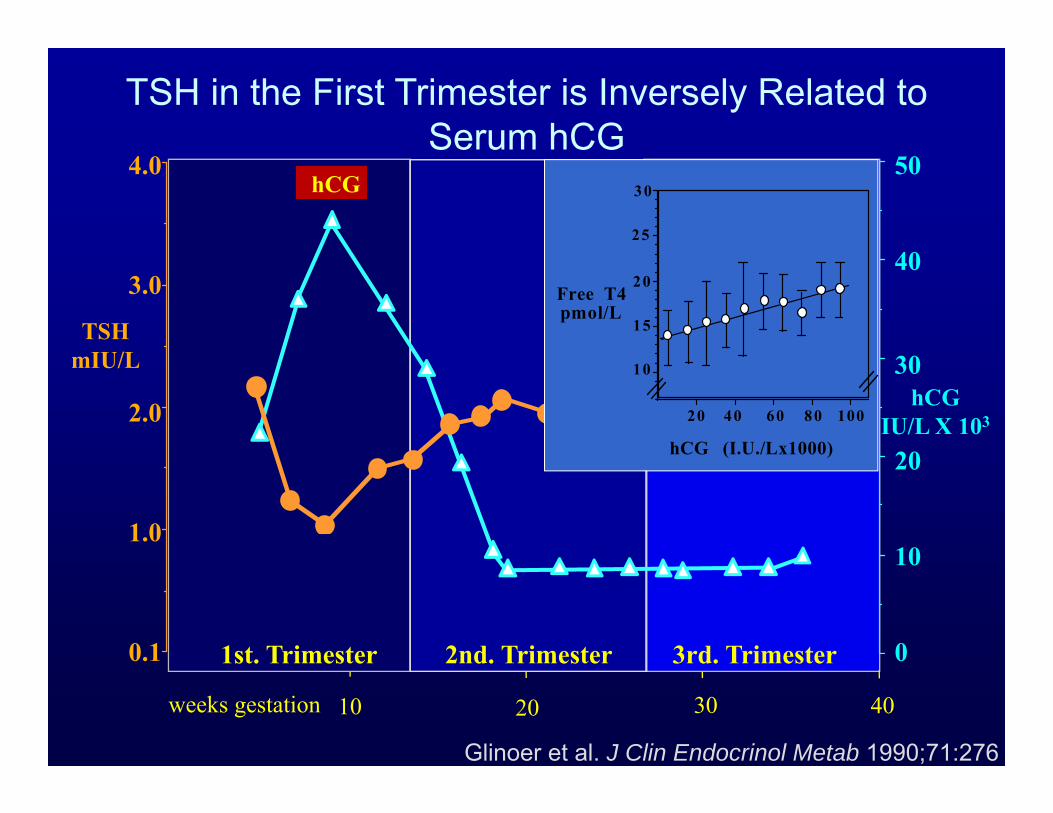
Glinoer et al. J Clin Endocrinol Metab 1990;71:276
hCG
10
15
20
25
10080604020
hCG (I.U./Lx1000)
Free T4pmol/L
30
hCGIU/L X 103
10
30
20
40
50
0
1.0
2.0
3.0
4.0
0.1
TSHmIU/L
40
TSH in the First Trimester is Inversely Related toSerum hCG
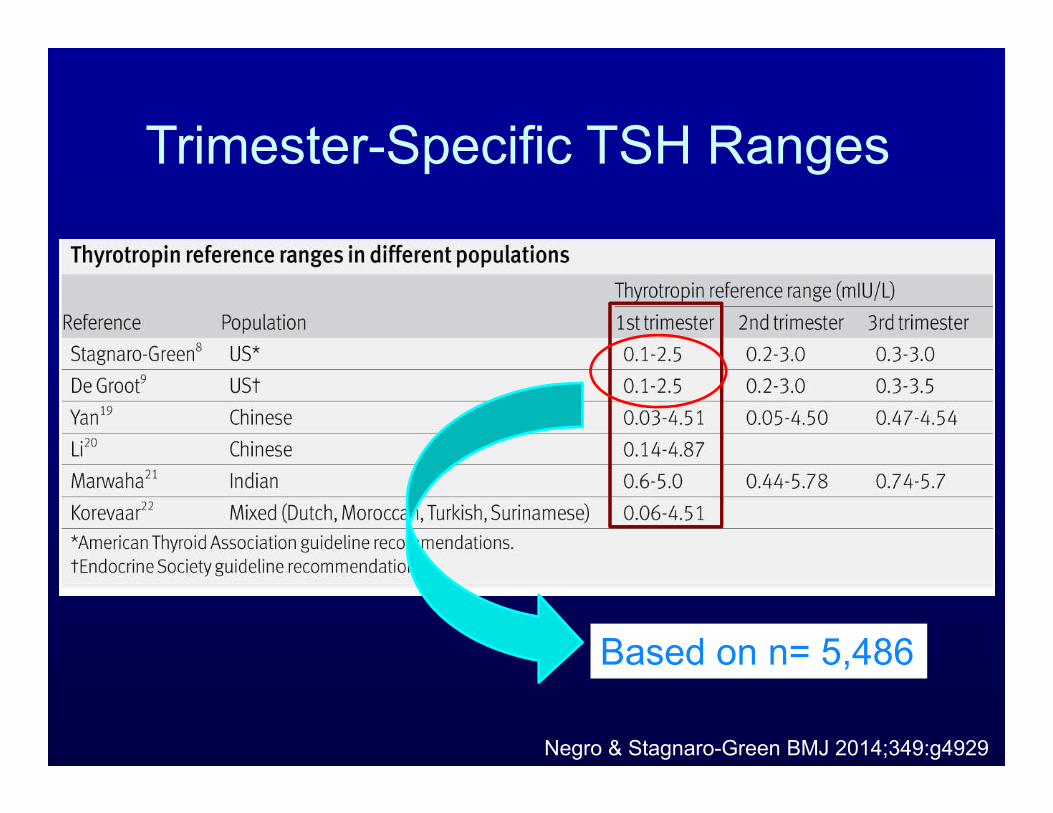
Negro & Stagnaro-Green BMJ 2014;349:g4929
Trimester-Specific TSH Ranges
Based on n= 5,486
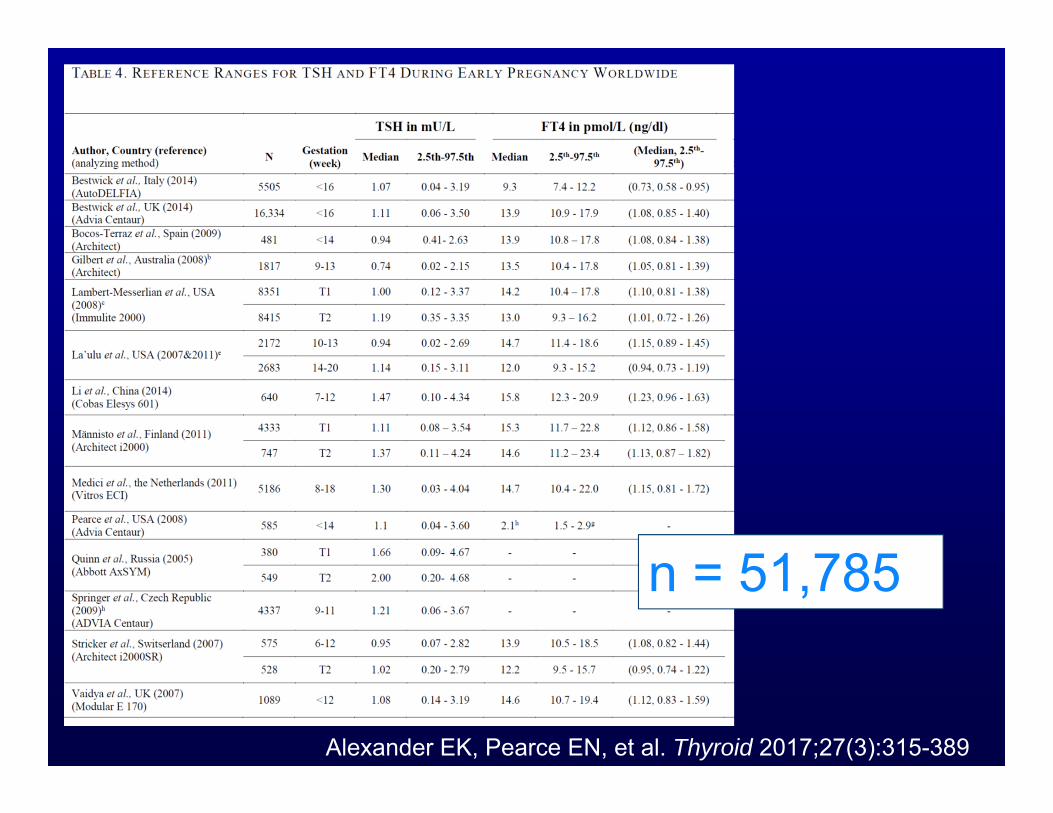
n = 51,785
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
When possible, trimester-specific reference ranges for serum TSH should be defined through assessment of local population data representative of a healthcare provider’s practice. Reference range determinations should only include pregnant women with no known thyroid disease, optimal iodine intake, and negative TPO Ab status. (Strong Recommendation, Moderate Quality Evidence)
ATA Guideline 2017
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
If internal or transferable pregnancy-specific TSH reference ranges are not available, an upper reference limit of ~ 4.0mU/l may be used. For most assays, this represents a reduction in the non-pregnant TSH upper reference limit of ~0.5mIU/L.
(Strong Recommendation, Moderate Quality Evidence)
ATA Guideline 2017
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
A 29 yo F presents at 10 weeks gestation. She has no history of thyroid disease. She has no goiter. Her serum TSH is 3.4 mIU/L.
What is the next best step?
A. Repeat the TSH in 4 weeksB. Check a TPO antibodyC. Start levothyroxine 50 mcg daily
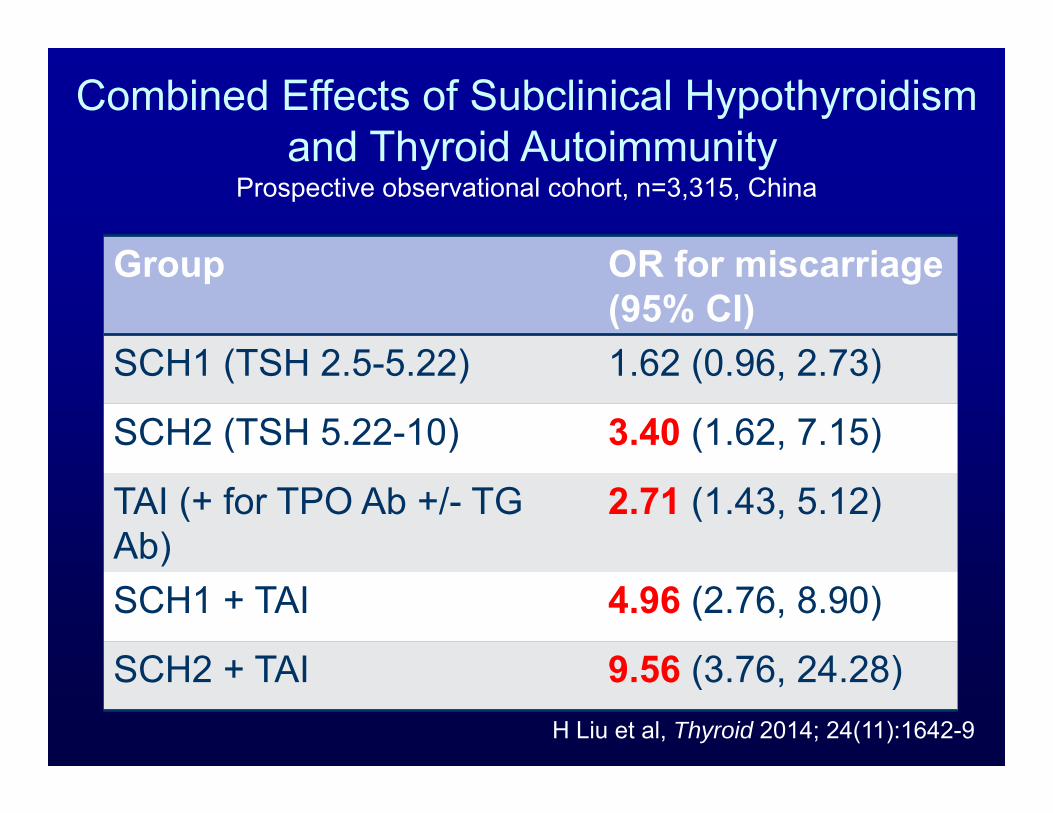
Group OR for miscarriage(95% CI)
SCH1 (TSH 2.5-5.22) 1.62 (0.96, 2.73)
SCH2 (TSH 5.22-10) 3.40 (1.62, 7.15)
TAI (+ for TPO Ab +/- TG Ab)
2.71 (1.43, 5.12)
SCH1 + TAI 4.96 (2.76, 8.90)
SCH2 + TAI 9.56 (3.76, 24.28)H Liu et al, Thyroid 2014; 24(11):1642-9
Combined Effects of Subclinical Hypothyroidismand Thyroid Autoimmunity
Prospective observational cohort, n=3,315, China
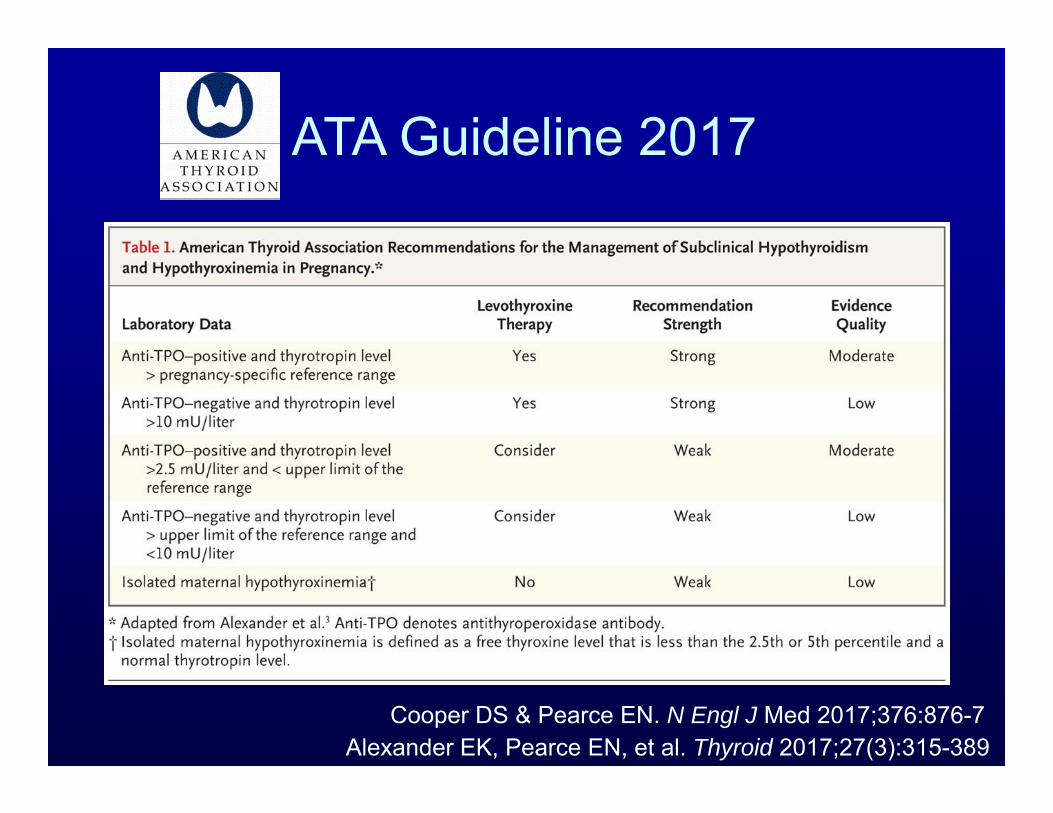
ATA Guideline 2017
Cooper DS & Pearce EN. N Engl J Med 2017;376:876-7Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
Case 3
A 37 yo woman presents with palpitations and tremor at 8 weeks gestation. She has no history of thyroid disease. She has no nausea, vomiting, or abdominal pain. Her heart rate is 106 beats/min, and she has no ophthalmopathy. The thyroid is nontender, upper limit of normal size, without bruit or palpable nodules. TSH 4 months ago: 0.54 mIU/LLabs now: TSH 0.014 mIU/L
free T4 1.59 ng/dL (ref 0.7-1.9 ng/dl)
What do you recommend:A. Start PTUB. Start methimazoleC. Repeat labs in 4 weeksD. Radioactive iodine uptake and scanE. Obtain a TRAb
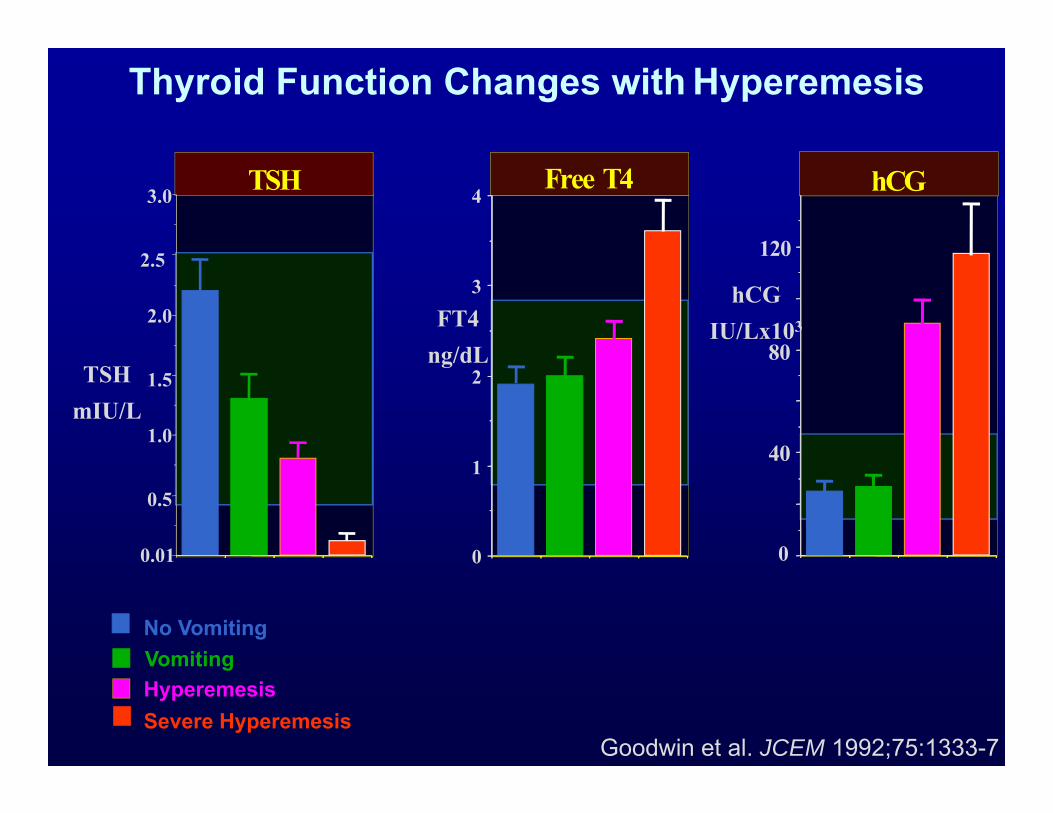
Thyroid Function Changes with Hyperemesis
Goodwin et al. JCEM 1992;75:1333-7
TSH
TSHmIU/L
No VomitingVomitingHyperemesisSevere Hyperemesis
3.0
2.5
2.0
1.5
1.0
0.5
0.01 0
1
2
3
4Free T4
40
80
120
hCG
0
hCGIU/Lx103FT4
ng/dL
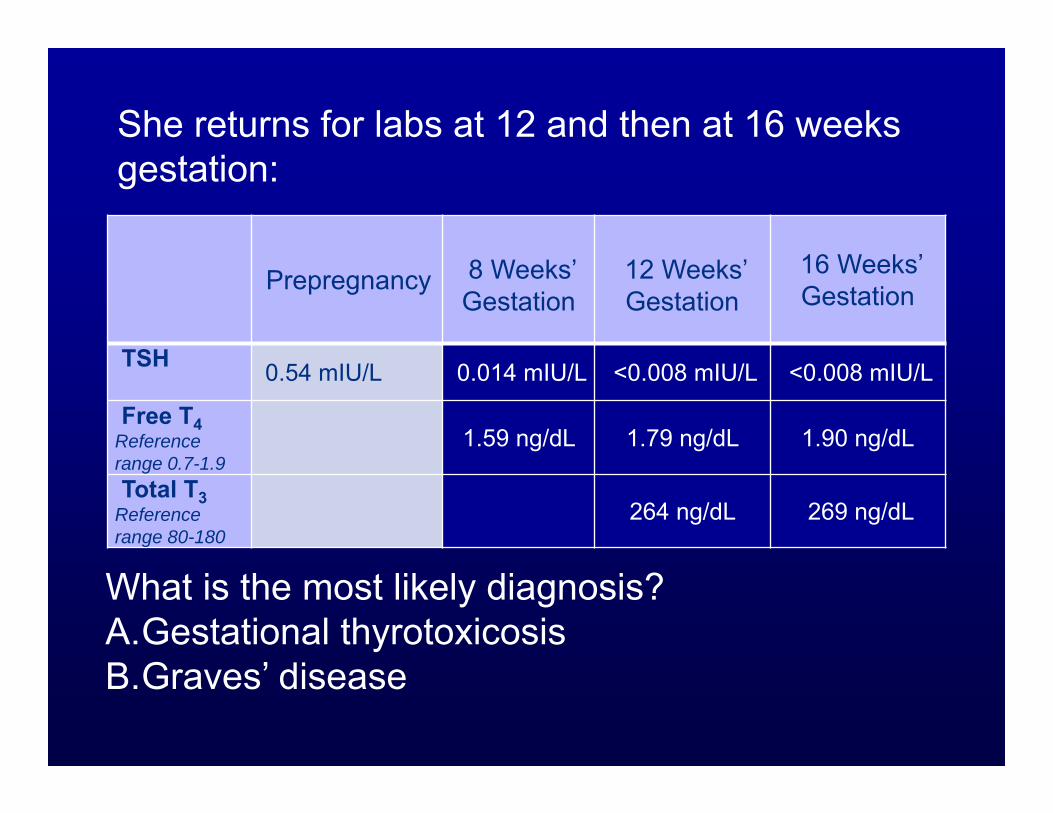
Prepregnancy 8 Weeks’ Gestation
12 Weeks’ Gestation
16 Weeks’ Gestation
TSH 0.54 mIU/L 0.014 mIU/L <0.008 mIU/L <0.008 mIU/L
Free T4Reference range 0.7-1.9
1.59 ng/dL 1.79 ng/dL 1.90 ng/dL
Total T3Reference range 80-180
264 ng/dL 269 ng/dL
She returns for labs at 12 and then at 16 weeks gestation:
What is the most likely diagnosis?A.Gestational thyrotoxicosisB.Graves’ disease
Prepregnancy 8 Weeks’ Gestation
12 Weeks’ Gestation
16 Weeks’ Gestation
TSH 0.54 mIU/L 0.014 mIU/L <0.008 mIU/L <0.008 mIU/L
Free T4Reference range 0.7-1.9
1.59 ng/dL 1.79 ng/dL 1.90 ng/dL
Total T3Reference range 80-180
264 ng/dL 269 ng/dL
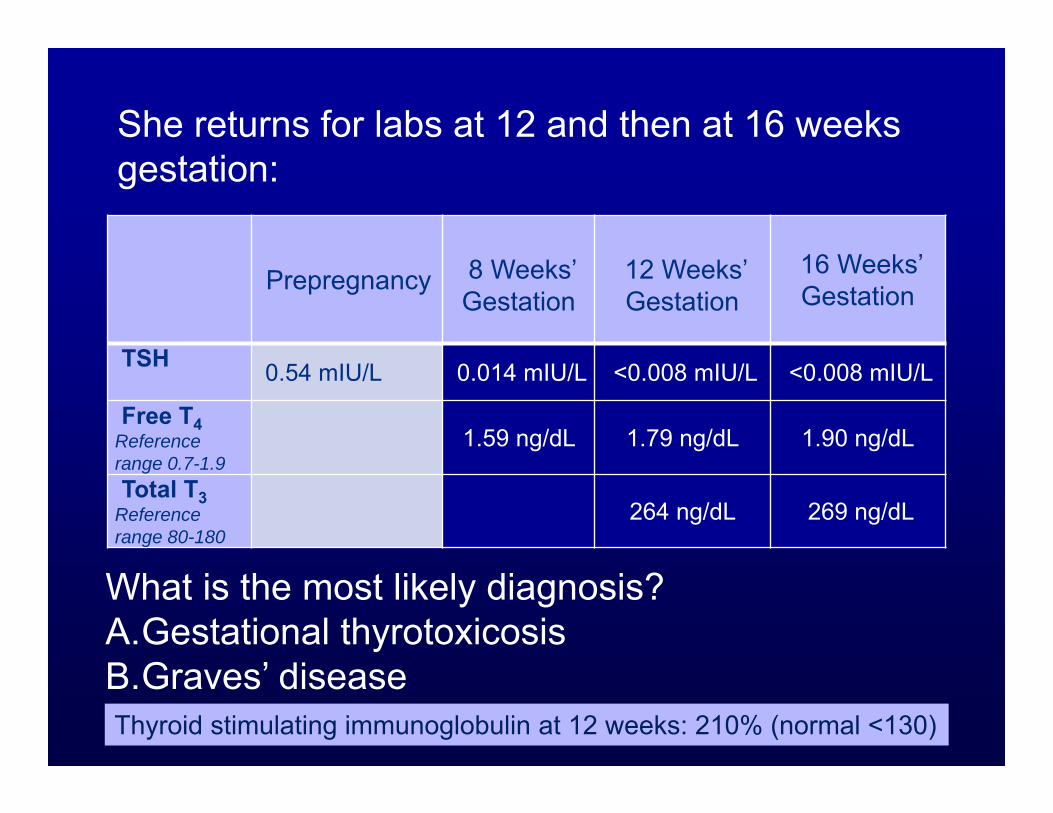
She returns for labs at 12 and then at 16 weeks gestation:
What is the most likely diagnosis?A.Gestational thyrotoxicosisB.Graves’ diseaseThyroid stimulating immunoglobulin at 12 weeks: 210% (normal <130)
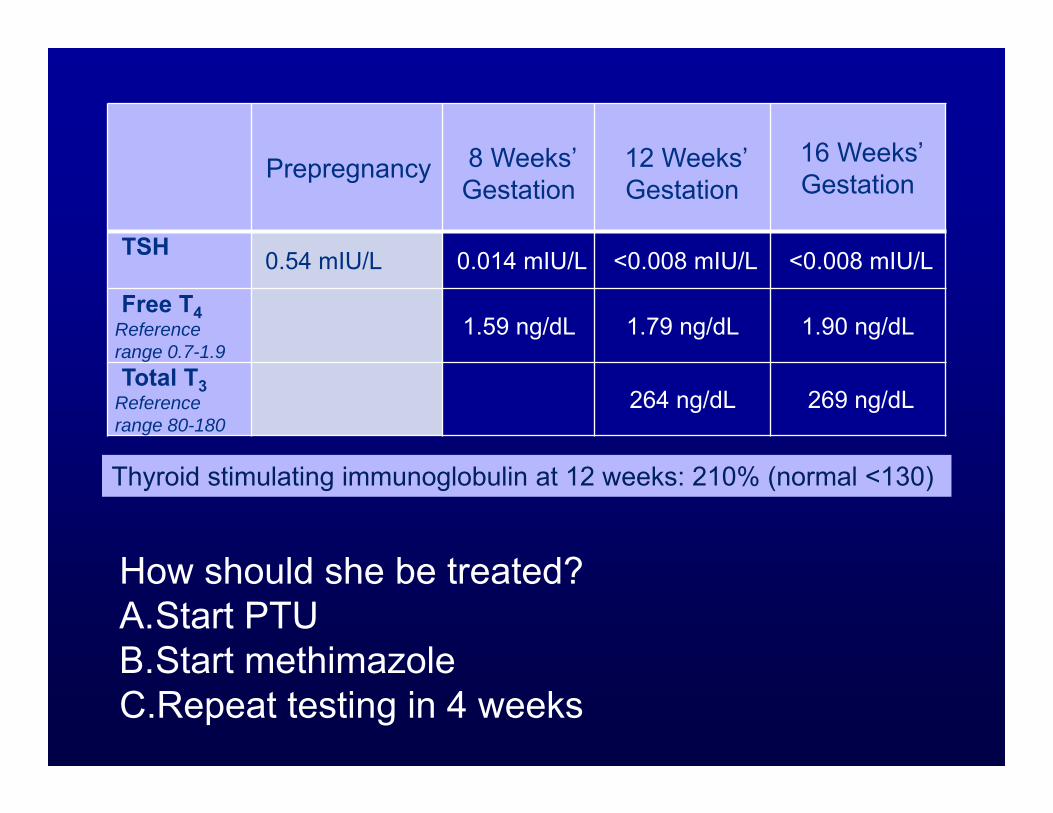
How should she be treated?A.Start PTUB.Start methimazoleC.Repeat testing in 4 weeks
Thyroid stimulating immunoglobulin at 12 weeks: 210% (normal <130)
Prepregnancy 8 Weeks’ Gestation
12 Weeks’ Gestation
16 Weeks’ Gestation
TSH 0.54 mIU/L 0.014 mIU/L <0.008 mIU/L <0.008 mIU/L
Free T4Reference range 0.7-1.9
1.59 ng/dL 1.79 ng/dL 1.90 ng/dL
Total T3Reference range 80-180
264 ng/dL 269 ng/dL
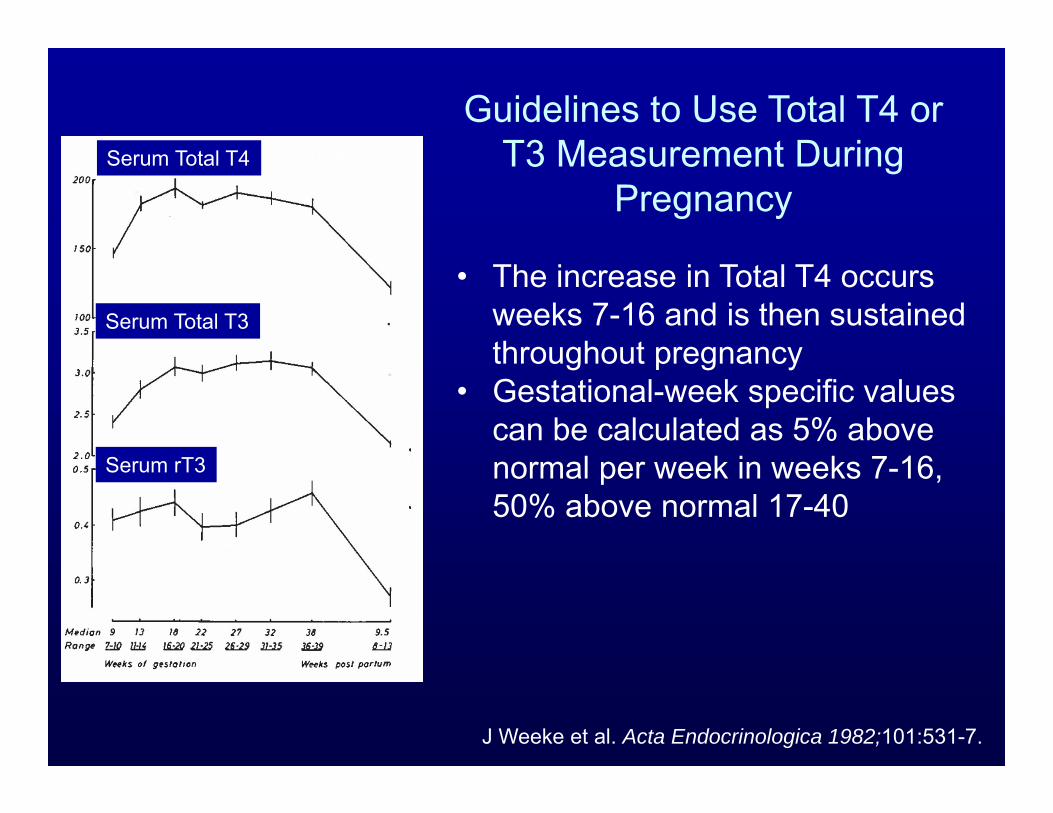
J Weeke et al. Acta Endocrinologica 1982;101:531-7.
Guidelines to Use Total T4 or T3 Measurement During
Pregnancy
• The increase in Total T4 occurs weeks 7-16 and is then sustained throughout pregnancy
• Gestational-week specific values can be calculated as 5% above normal per week in weeks 7-16, 50% above normal 17-40
Serum Total T4
Serum Total T3
Serum rT3
16 weeks
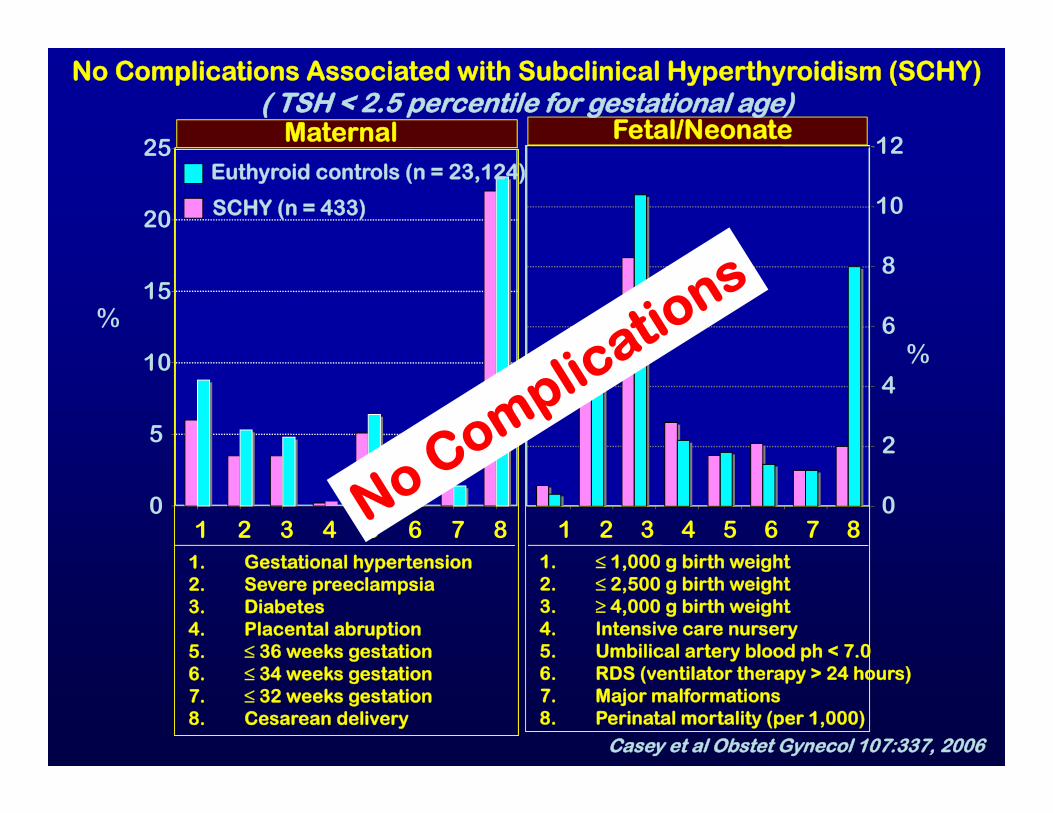
1. Gestational hypertension2. Severe preeclampsia3. Diabetes4. Placental abruption5. ≤ 36 weeks gestation6. ≤ 34 weeks gestation7. ≤ 32 weeks gestation8. Cesarean delivery
1. ≤ 1,000 g birth weight2. ≤ 2,500 g birth weight3. ≥ 4,000 g birth weight4. Intensive care nursery5. Umbilical artery blood ph < 7.06. RDS (ventilator therapy > 24 hours)7. Major malformations8. Perinatal mortality (per 1,000)
0
5
10
15
20
25
1 2 3 4 5 6 7 80
2
4
6
8
10
12
1 2 3 4 5 6 7 8
No Complications Associated with Subclinical Hyperthyroidism (SCHY)( TSH < 2.5 percentile for gestational age)
Maternal Fetal/Neonate
SCHY (n = 433)
Euthyroid controls (n = 23,124)
%%
Casey et al Obstet Gynecol 107:337, 2006
Case 4
A 27 year old woman with Graves’ hyperthyroidism is planning a pregnancy. She has been on methimazole for 9 months; her current dose is 5 mg/day. She is currently asymptomatic. Menses are regular. She has a 25 gm thyroid gland without nodules. No tremor. Heat rate 88 bpm.
Current labs:TSH 0.59 mIU/LFree T4 1.7 ng/dL (ref range 0.7-1.9)T3 156 ng/dL (ref range 80-180)TSI 190% (ref range <130)
What should you recommend?
A. ThyroidectomyB. Radioactive iodine treatmentC. Change now from methimazole to PTUD. Change from methimazole to PTU as soon as
pregnancy is diagnosedE. Discontinue anti-thyroid drug as soon as
pregnancy is diagnosed
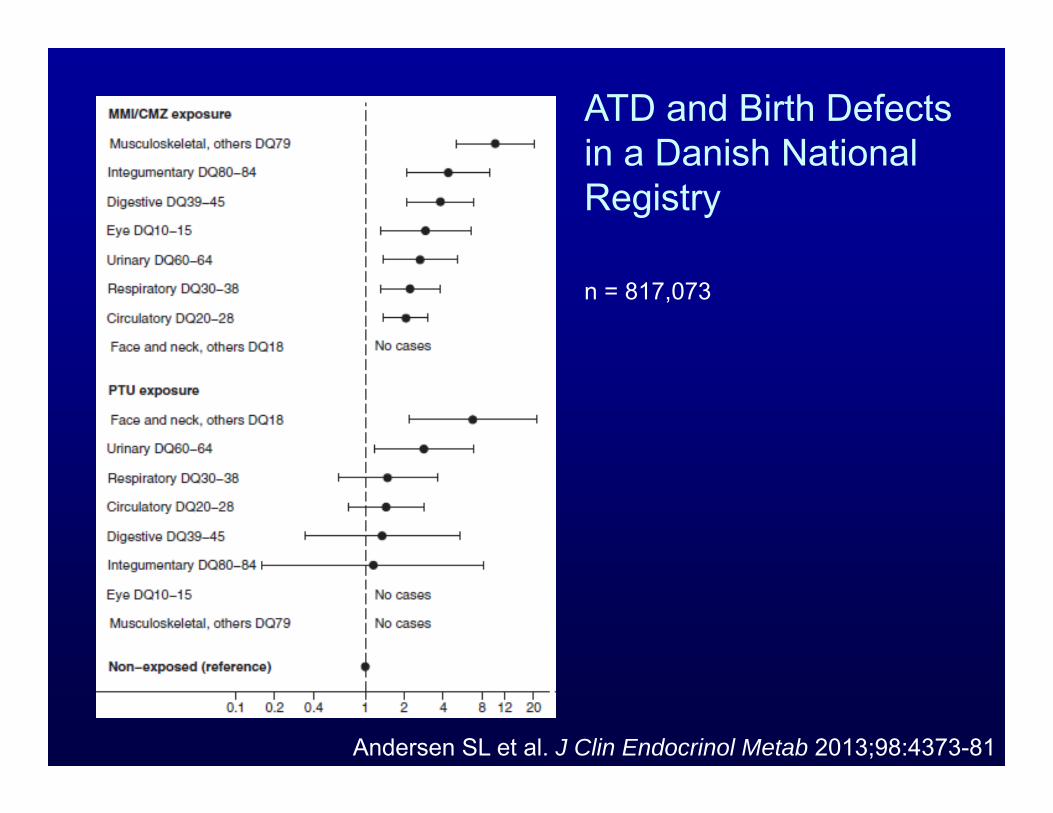
Andersen SL et al. J Clin Endocrinol Metab 2013;98:4373-81
ATD and Birth Defectsin a Danish National Registry
n = 817,073
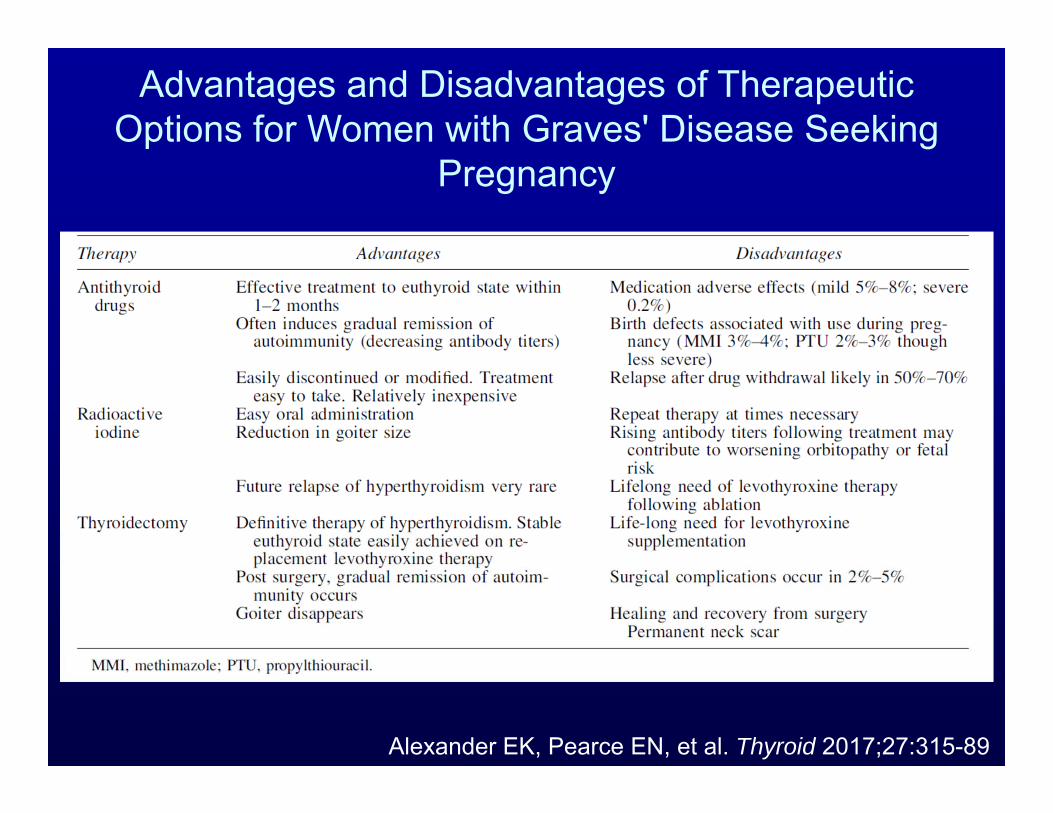
Advantages and Disadvantages of Therapeutic Options for Women with Graves' Disease Seeking
Pregnancy
Alexander EK, Pearce EN, et al. Thyroid 2017;27:315-89
Case 5
A 26 yo woman presents for routine antenatal care at 8 weeks gestation. This is her first pregnancy. She feels well apart from some fatigue and mild nausea. She has no history of thyroid disease.
What thyroid testing would you order?
A. NoneB. TSHC. TSH and free T4D. TSH, free T4, and TPO antibody
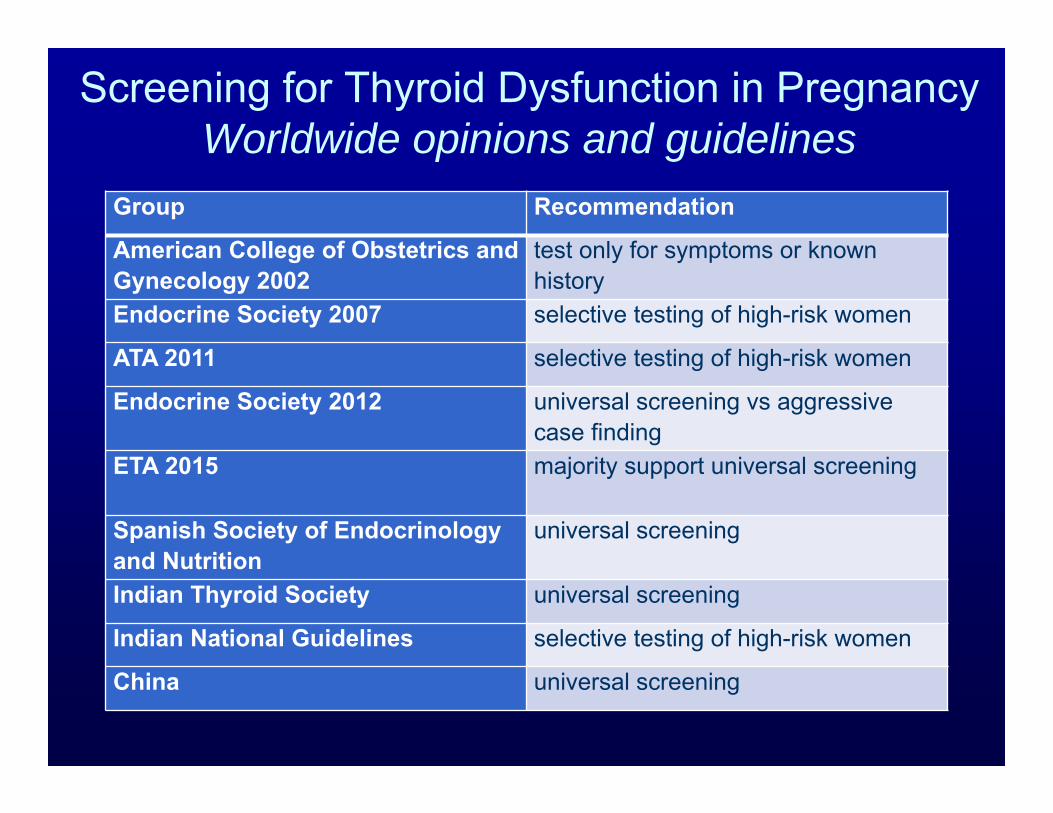
Screening for Thyroid Dysfunction in PregnancyWorldwide opinions and guidelines
Group Recommendation
American College of Obstetrics and Gynecology 2002
test only for symptoms or known history
Endocrine Society 2007 selective testing of high-risk women
ATA 2011 selective testing of high-risk women
Endocrine Society 2012 universal screening vs aggressive case finding
ETA 2015 majority support universal screening
Spanish Society of Endocrinology and Nutrition
universal screening
Indian Thyroid Society universal screening
Indian National Guidelines selective testing of high-risk women
China universal screening
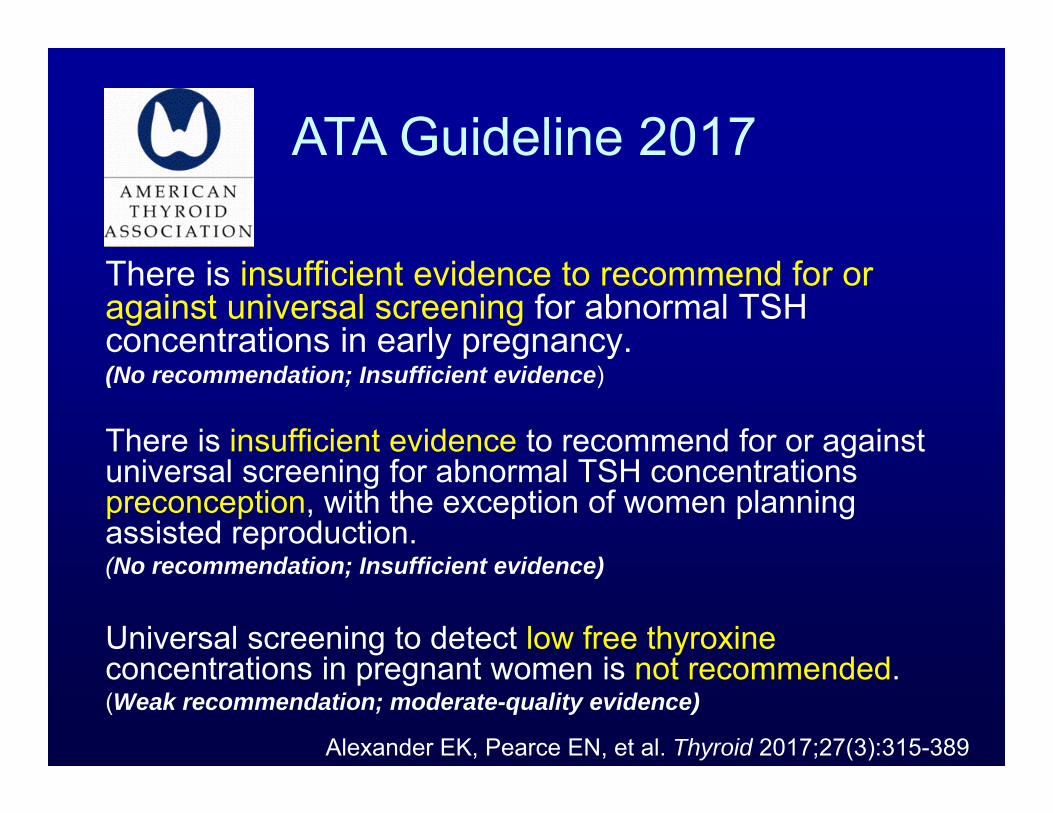
There is insufficient evidence to recommend for or against universal screening for abnormal TSH concentrations in early pregnancy. (No recommendation; Insufficient evidence)
There is insufficient evidence to recommend for or against universal screening for abnormal TSH concentrations preconception, with the exception of women planning assisted reproduction. (No recommendation; Insufficient evidence)
Universal screening to detect low free thyroxine concentrations in pregnant women is not recommended. (Weak recommendation; moderate-quality evidence)
ATA Guideline 2017
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
All patients seeking pregnancy, or newly pregnant, should undergo clinical evaluation. If any of the following risk factors are identified, testing for serum TSH is recommended as soon as pregnancy is confirmed.(Strong recommendation, moderate-quality evidence)
ATA Guideline 2017
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
1. History of hypothyroidism/hyperthyroidism or current symptoms/signs of thyroid dysfunction
2. Known thyroid antibody positivity or presence of a goiter3. History of head or neck radiation or prior thyroid surgery4. Age >30 years5. Type 1 diabetes or other autoimmune disorders 6. History of miscarriage, preterm delivery, or infertility7. Multiple prior pregnancies ( 2)8. Family history of autoimmune thyroid disease or thyroid
dysfunction9. Morbid obesity (BMI 40 kg/m2)10. Use of amiodarone or lithium, or recent administration of
iodinated radiologic contrast11. Residing in an area of known moderate to severe iodine
insufficiency
High Risk for Thyroid Dysfunction in Pregnancy
Case 6
A 23 year old woman presents at at 8 weeks gestation. She has previously miscarried twice. She is feeling well. She has no history of thyroid disease. The thyroid is 25 gm and firm. Labs obtained by her obstetrician include:
TSH 2.4 mIU/LTPO Antibody >1000 IU/mL (ref range <35)
What do you recommend?A. No treatmentB. Levothyroxine 50 µg dailyC. Selenium 200 mg daily
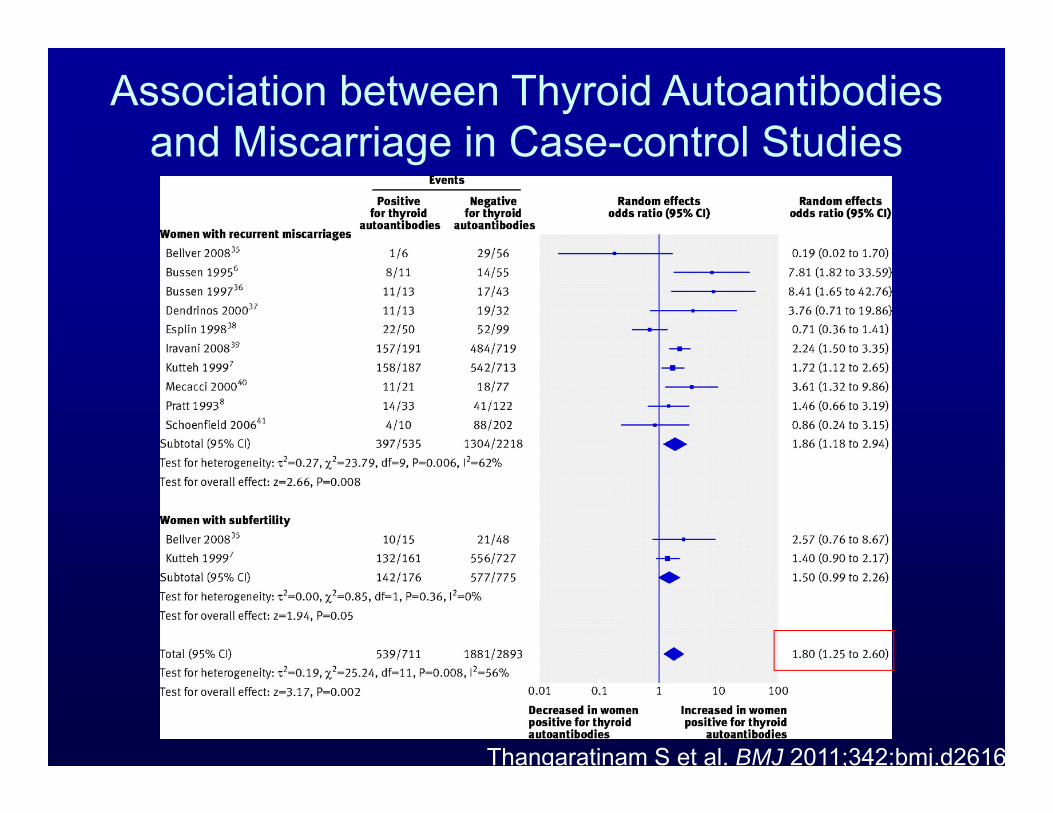
Association between Thyroid Autoantibodies and Miscarriage in Case-control Studies
Thangaratinam S et al. BMJ 2011;342:bmj.d2616
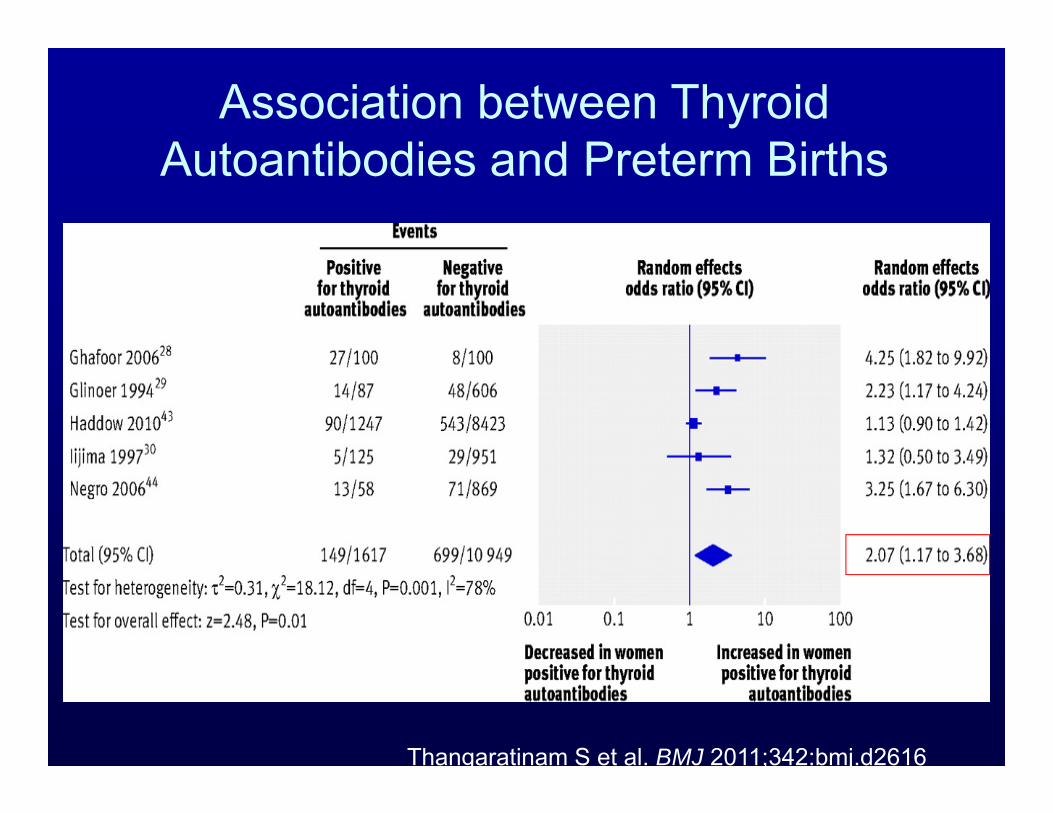
Association between Thyroid Autoantibodies and Preterm Births
Thangaratinam S et al. BMJ 2011;342:bmj.d2616
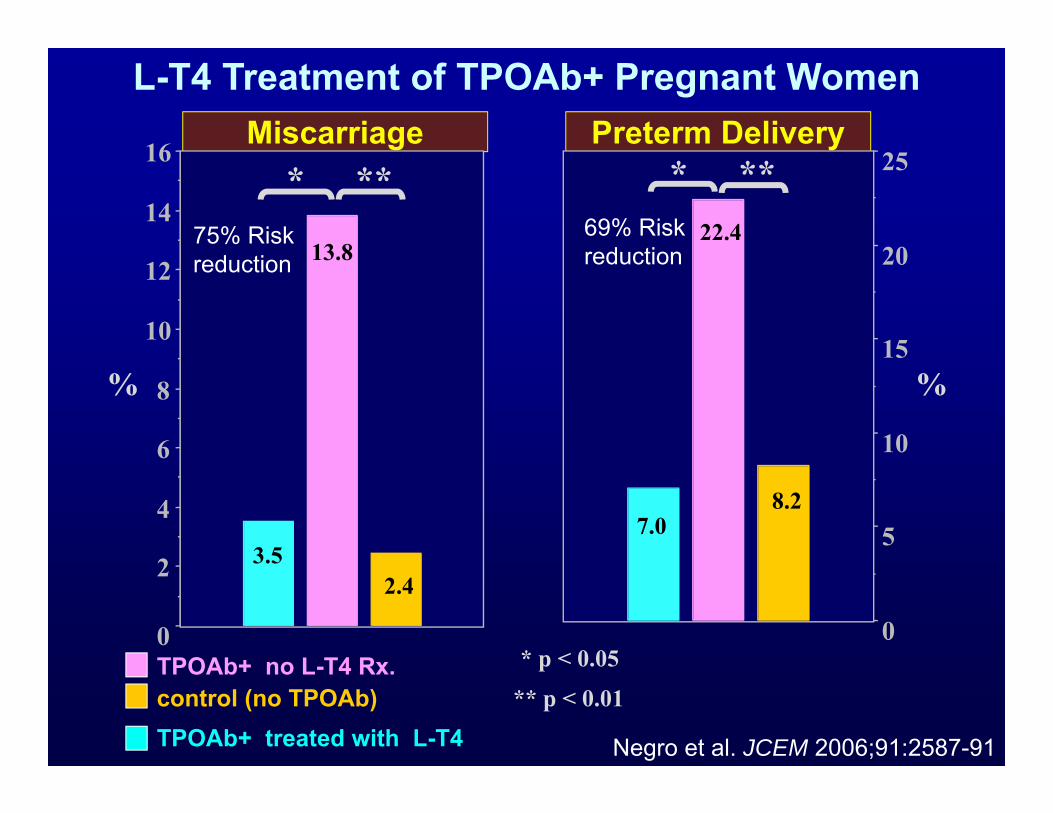
Miscarriage Preterm DeliveryL-T4 Treatment of TPOAb+ Pregnant Women
control (no TPOAb)TPOAb+ no L-T4 Rx.0
2
4
6
8
10
12
14
16
0
5
10
15
20
25
22.4
8.2
13.8
2.4
* p < 0.05
** p < 0.01
** **
7.03.5
TPOAb+ treated with L-T4
* *
% %
75% Riskreduction
69% Riskreduction
Negro et al. JCEM 2006;91:2587-91
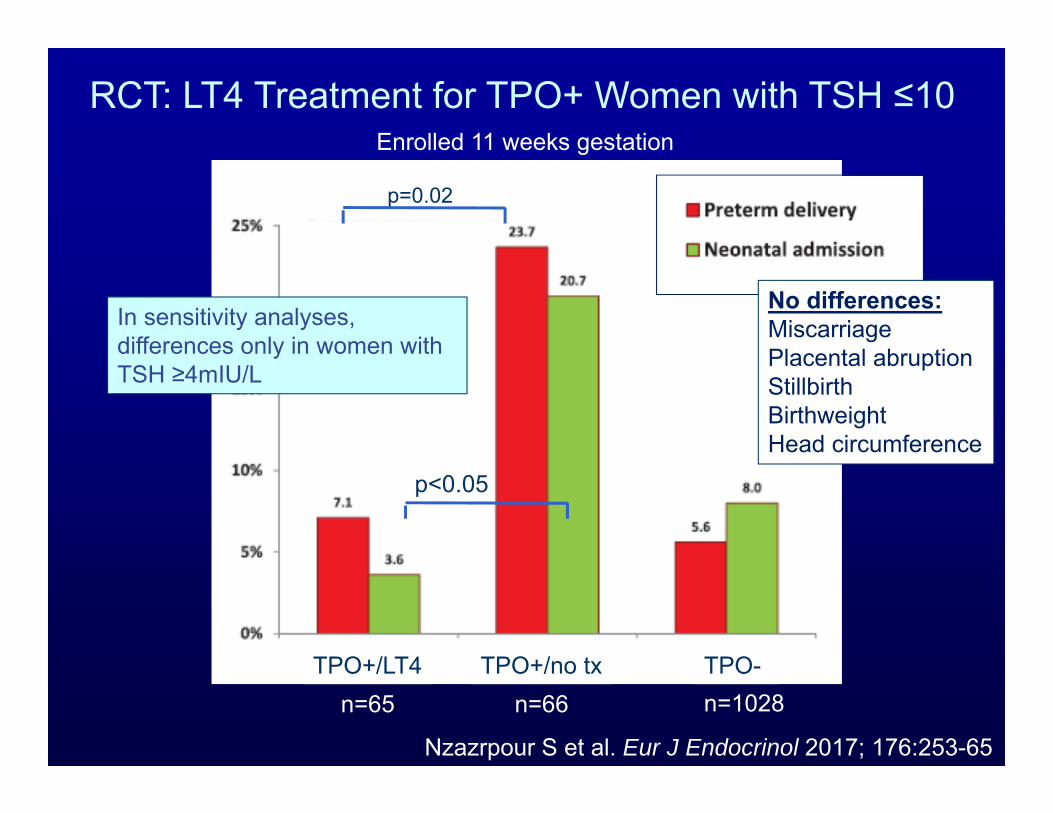
Nzazrpour S et al. Eur J Endocrinol 2017; 176:253-65
TPO+/LT4 TPO+/no tx TPO-n=65 n=66 n=1028
RCT: LT4 Treatment for TPO+ Women with TSH ≤10
p=0.02
p<0.05
No differences:MiscarriagePlacental abruptionStillbirthBirthweightHead circumference
Enrolled 11 weeks gestation
In sensitivity analyses, differences only in women with TSH ≥4mIU/L
Ongoing trials:
The TABLET trial - in the UK- randomizing euthyroid, TPO Ab positive women with a
history of infertility or miscarriage to either levothyroxine vs. placebo
- Outcome: live birth rates
The T4Life trial - in the Netherlands- Randomizing euthyroid, TPO Ab positive women with a
history of recurrent miscarriage to LT4 vs. placebo before conception.
- Outcome: live birth rates >24 weeks gestationhttp://www.birmingham.ac.uk/research/activity/mds/trials/bctu/trials/womens/tablet/index.aspxhttp://www.trialregister.nl/trialreg/admin/rctview.asp?TC=3364

There is insufficient evidence to conclusively determine whether levothyroxine therapy decreases miscarriage risk in TPO Ab positive, euthyroid women. However, administration of levothyroxine to TPO Ab positive, euthyroid women with a prior history of miscarriage may be considered given its potential benefits in comparison to its minimal risk. In such cases, 50 μg of levothyroxine is a typical starting dose. (Weak recommendation; Low-quality evidence)
ATA Guideline 2017
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
Selenium and the Thyroid in Pregnancy
Two Conflicting RCTs:.•200 mg selenium daily decreased postpartum thyroid dysfunction and lowered TPO Ab concentrations during gestation•60 mg selenium daily did not affect TPO concentrations or TPO positivity in pregnant women
Patients treated with selenium may be at higher risk for developing type 2 diabetes mellitus.
Negro et al. J Clin Endocrinol Metab 2007;92:1263–1268; Mao J et al. Eur J Nutr 2016;55:55–61; Stranges S et al. Ann Intern Med 147:217–223.
ATA Guideline 2017
Selenium supplementation is notrecommended for the treatment of TPOAb-positive women during pregnancy. Weak recommendation, moderate-quality evidence.
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
Case 7
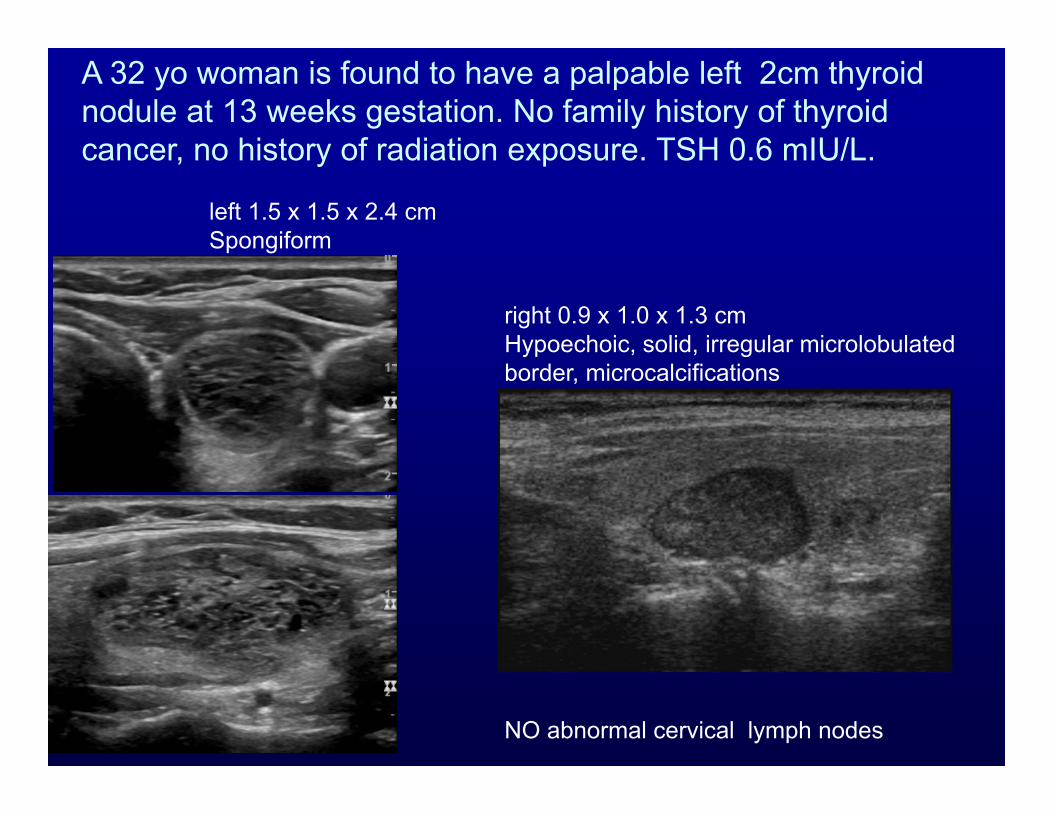
left 1.5 x 1.5 x 2.4 cmSpongiform
right 0.9 x 1.0 x 1.3 cmHypoechoic, solid, irregular microlobulated border, microcalcifications
NO abnormal cervical lymph nodes
A 32 yo woman is found to have a palpable left 2cm thyroid nodule at 13 weeks gestation. No family history of thyroid cancer, no history of radiation exposure. TSH 0.6 mIU/L.
What is the best next step?
A. Biopsy left (spongiform) 1.5 cm nodule nowB. Biopsy right (hypoechoic) 1.3 cm nodule nowC. Defer FNA biopsy until after delivery
ATA 2017 Guideline
Thyroid nodule FNA is generally recommended for newly detected nodules in pregnant women with a non-suppressed TSH. Determination of which nodules require FNA should be based upon the nodule’s sonographic pattern. The timing of FNA, whether during gestation or early postpartum, may be influenced by the clinical assessment of cancer risk, or by patient preference. (Strong recommendation, Moderate-quality evidence)
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389
The patient elects to undergo FNA biopsy at 14 weeks.
Cytopathology from her right nodule is read as Bethesda V (suspicious for papillary cancer).
What is the next best step?
A. Repeat FNA biopsy with molecular markersB. Thyroid surgery in the second trimesterC. Defer thyroid surgery until after delivery
Does pregnancy impact prognosis of newly diagnosed PTC?
• 3 retrospective studies have shown no differences in recurrence or survival rates in women diagnosed during pregnancy or within 1 year postpartum compared to nonpregnant women
• 2 recent reports of higher persistence/recurrent disease based upon either Tg, rising Tg Ab or structural neck disease– Small numbers of patients– Classification of recurrence – Recurrence rates of cancer DX during pregnancy discrepant between studies: 60% (Messuti) vs. 10% (Vanucchi)
Herzon Arch Otolaryngol Head Neck Surg 1994:120:1191; Moosa J Clin Endocrinol Metab 1997;82:2862;Yasmeen Int J Gynaecol Obstet 2005;91:15; Vannucchi Eur J Endocrinol 2010;162:145; Messuti Eur J Endocrinol 2014;170: 659;
ATA 2017 Guideline
PTC detected in early pregnancy should be monitored sonographically. If it grows substantially before 24-26 weeks gestation, or if cytologically malignant cervical lymph nodes are present, surgery should be considered during pregnancy. However, if the disease remains stable by midgestation, or if it is diagnosed in the second half of pregnancy, surgery may be deferred until after delivery. Weak recommendation, Low-quality evidence
Alexander EK, Pearce EN, et al. Thyroid 2017;27(3):315-389

Questions?





























