Embed Size (px)
Citation preview

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neuroimmunomodulation 2007;14:243–247
DOI: 10.1159/000112049
Thyroid Function Changes and Cytokine Alterations following Major Surgery
Ioannis Ilias a Marinella Tzanela b Irini Mavrou d Evangelia Douka d
Petros Kopterides d Apostolos Armaganidis d Stylianos Orfanos d
Georgia Kostopanagiotou d Anastasios Macheras e Stylianos Tsagarakis c
Ioanna Dimopoulou d
Departments of Endocrinology, a Elena Venizelou Hospital, b Evagelismos Hospital and c Athens Polyclinic, and
d Second Department of Critical Care Medicine and e Third Department of Surgery, University of Athens School of
Medicine, Attikon Hospital, Athens , Greece
Introduction
Proinflammatory cytokines are implicated in alter-ations in thyroid function and particularly in cases of thyroiditis or hyperthyroidism [1] . Furthermore, pro- and anti-inflammatory cytokines are elevated during pe-riods of somatic stress [2] . Conditions that compromise the body’s integrity (such as surgery) activate the cyto-kine cascade, producing large quantities of tumor necro-sis factor (TNF)- � , interleukin (IL)-1, IL-6, IL-8 and IL-12 (the key components of an inflammatory response). Most cytokines are produced by specific cell types in re-sponse to specific stimuli, whereas IL-6 is produced by almost all cells in response to any type of stimulation [3–5] . Although thyroid function changes and cytokine alterations associated with surgery are well documented [6–12] , the interaction among them has not been fully evaluated [13, 14] and is even refuted [15] .
The current work describes the sequential evaluation of serum thyroid hormone levels in relation to changes in cytokine concentrations in patients following elective major abdominal operations. The aim of this study was to establish whether cytokine release is implicated in thy-roid hormone changes during surgical stress.
Key Words
Cytokine levels � Surgical stress � Thyroid hormones
Abstract
To establish whether cytokine release is implicated in thy-
roid hormone changes during surgical stress we studied 36
adult patients (20 men; mean age 8 SD: 68.5 8 10.5 years)
undergoing elective major abdominal operations. We mea-
sured tumor necrosis factor (TNF)- � , interleukin (IL)-6, IL-8
and IL-10 and thyrotropin (TSH), free thyroxine (FT 4 ) and tri-
iodothyronine (T 3 ) before scheduled non-emergency sur-
gery, immediately postoperatively, on the 1st postoperative
day (post-1) and on the 2nd postoperative day (post-2). TNF-
� , IL-6 and IL-8 peaked on day post-1 whereas IL-10 peaked
immediately postoperatively. Fourteen of 36 patients had
low T 3 levels after surgery, indicating non-thyroidal illness
(NTI). Significant negative correlations were noted among
TNF- � , IL-6 and IL-8 against T 3 and FT 4 . Cytokines are respon-
sible, at least in part, for NTI following major operations.
Copyright © 2007 S. Karger AG, Basel
Received: April 18, 2007
Accepted: September 5, 2007
Published online: December 10, 2007
Dr. Ioannis Ilias 129, Kifisias Avenue GR–11524 Athens (Greece) Tel. +30 693 258 7674, Fax + 30 210 699 7507 E-Mail [email protected]
© 2007 S. Karger AG, Basel1021–7401/07/0145–0243$23.50/0
Accessible online at:www.karger.com/nim

Ilias et al.
Neuroimmunomodulation 2007;14:243–247244
Patients and Methods
We studied 36 adult patients (20 men; mean age 8 SD: 68.5 8 10.5 years) undergoing elective major abdominal operations, such as colectomy (n = 17), total gastrectomy (n = 7), abdominal aorta aneurysm repair (n = 7) and Whipple’s pancreatectomy (n = 5). Median duration of surgery was 145 min. Exclusion criteria were: neutropenia ( ̂ 500 neutrophils/mm 3 ); HIV infection; periopera-tive administration of corticosteroids, etomidate, dopamine and amiodarone; a history of an endocrine disorder, and pre- and perioperative liver or renal dysfunction judged by routine labora-tory tests. All patients were in good general condition.
Informed written consent was obtained from all patients who participated in the present study.
We measured TNF- � , IL-6, IL-8, IL-10, thyrotropin (TSH), free thyroxine (FT 4 ) and triiodothyronine (T 3 ) before scheduled non-emergency surgery, immediately postoperatively, and on the 1st (post-1) and 2nd postoperative days (post-2). IL-6, IL-8, IL-10 and TNF- � were determined using the LINCOplex assay (Linco Research, St. Charles, Mo., USA). This assay relies on the use of polystyrene beads, each with a unique signature mix of fluores-cent dyes that can be discriminated by a laser-based detection in-strument, the Luminex 100 (Luminex, Austin, Tex., USA). Each bead type is coated with a specific antibody to the cytokine of in-terest. The cytokine antibody pairs in this multiplex assay do not cross-react with other analytes in the panel. The assay sensitivity is 0.64 pg/ml. The intra-assay coefficients of variation are 6.3% for IL-6, 6.0% for IL-8, 5.4% for IL-10 and 5.8% for TNF- � , while the interassay coefficients of variation are 10.4% for IL-6, 9.0% for IL-8, 11.2% for IL-10 and 9.4% for TNF- � [16, 17] . TSH, FT 4 and T 3 were measured with electrochemiluminescence (Elecsys Sys-tems, Roche Diagnostics, Mannheim, Germany). The assay sen-sitivity is 0.014 � IU/l for TSH, 0.02 ng/dl for FT 4 and 0.02 pg/dl for T 3 . The intra- and interassay coefficients of variation are ! 5.1% for TSH, FT 4 and T 3 .
Normal distributions in thyroid hormones and cytokines were assessed with the Kolmogorov-Smirnov test. Following the as-
sessment of normality, differences in thyroid hormones among the four sampling times were evaluated with analysis of variance (ANOVA) for repeated measures and two-way ANOVA and post hoc tests, whereas differences in cytokine levels were evaluated with the Kruskal-Wallis test. Interactions among cytokines and thyroid function parameters as well as with the patients’ age were evaluated with a linear regression correlation matrix.
Results
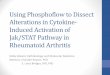
All but 4 patients survived and were discharged from hospital. Gastrointestinal bleeding and/or sepsis were the causes of death for the 4 patients. Regarding cytokine ki-netics, TNF- � , IL-6 and IL-8 peaked on post-1 whereas IL-10 peaked immediately postoperatively (except for TNF- � , all the other observed variations were statisti-cally significant, p ! 0.05, Kruskal-Wallis test, table 1 ). As far as perioperative thyroid hormone changes are con-cerned, TSH and FT 4 peaked immediately postoperative-ly, whereas T 3 was the highest before surgery and then dropped continuously (only variations in TSH and T 3 were statistically significant, p ! 0.05, ANOVA for re-peated measures; fig. 1 ). Overall, 14 patients (39%) had low serum T 3 levels after surgery, indicating non-thyroi-dal illness (NTI). Low T 3 occurred immediately postop-eratively (n = 2), on day post-1 (n = 9) and on day post-2 (n = 3). Although T 3 was negatively correlated with age (with r ranging from –0.095 to –0.525 and p ranging from 0.58 to 0.01), there was no appreciable effect of older age on the decrease in T 3 immediately postoperatively and on post-1 (two-way ANOVA p 1 0.10); however, older pa-
Table 1. Comparison of cytokine levels before scheduled non-emergency surgery (pre), immediately postop-eratively (im-post), and on post-1 and post-2
Cytokines pre im-post post-1 post-2
TNF-�, pg/mlMedian 4.595 4.72 6.2 5.21Q25/Q75 3.195/8.225 3.2/8.87 3.2/10.35 3.2/8.17
IL-6, pg/mlMedian 8.735* 127.5* 379.13* 108*Q25/Q75 0.68/26.095 57.545/2,093.2025 147.97/782.08 70.03/300.5225
IL-8, pg/mlMedian 3.2* 13.3* 20.315* 11.4*Q25/Q75 0.64/12.275 5.62/27.9925 14.39/28.645 4.925/17.8085
IL-10, pg/mlMedian 3.2* 36.33* 16.585* 6.3*Q25/Q75 0.64/5.41 12.265/134.69 10.4/27.68 4.82/8.1675
* p < 0.05, Kruskal-Wallis test.

Thyroid Function, Cytokines and Surgery
Neuroimmunomodulation 2007;14:243–247 245
tients more often had low T 3 on post-2 (two-way ANOVA p = 0.03). Significant negative correlations were noted among TNF- � , IL-6 and IL-8 against T 3 and FT 4 ( ta-ble 2 ).
Discussion
In this study, an interplay (albeit without definitive causality) was seen between pro- and anti-inflammatory cytokines and thyroid function. The changes noted were within a narrow time frame and are in agreement with known observations of NTI (or ‘euthyroid sick syn-drome’). Older patients more often showed low T 3 only on post-2 (however, the small number of patients with low T 3 does not point to a consistent effect in the patients that were studied).
During the acute phase reaction in humans, TNF- � rises almost immediately and peaks at 1.5 h. At 3 h, IL-6 and IL-8 were also increased. At 5 h, IL-10 secretion is maximal (counteracting the production, release or activ-ity of the proinflammatory cytokines IL-1, IL-6 and TNF- � ) [18, 19] .
9
8
7
6
5
4
3
2
1
0
TS
H (
µIU
/l)
Prea Im-post Post-1 Post-2
2.0
1.8
1.6
1.4
1.2
1.0
0.8
0.6
FT
4 (
ng
/dl)
Preb Im-post Post-1 Post-2
200
180
160
140
120
100
80
60
40
20
0
T3 (
ng
/dl)
Prec Im-post Post-1 Post-2
Fig. 1. Plots of TSH ( a ), FT 4 ( b ) and T 3 ( c ) before scheduled non-emergency surgery (pre), immediately postoperatively (im-post), and on post-1 and post-2. Horizontal lines indicate means 8 SD; unshaded areas indicate normal ranges.
Table 2. Correlation coefficients (r) of cytokines versus thyroid function parameters for values immediately postoperatively (im-post), and on post-1 and post-2 (only significant correlations are presented)
T3 post-1 T3 post-2 FT4 post-1
TNF-�im-post –0.336post-1 –0.350post-2 –0.345
IL-6im-post –0.378post-1 –0.430 –0.371post-2 –0.370 –0.370
IL-8im-post –0.365post-2 –0.340

Ilias et al.
Neuroimmunomodulation 2007;14:243–247246
During the course of any severe NTI, profound alter-ations in serum concentrations and in the metabolism of thyroid hormones may occur. A reduction in serum total T 3 and FT 3 characterizes NTI. It is still controversial whether the reduction in serum T 3 is a beneficial adapta-tion resulting in the protection against metabolism or whether it is a maladaptation contributing to a worsening of the disease and to a poor outcome [20–23] . The patho-genesis of thyroid function abnormalities in acute illness remains to be elucidated to date. Elevated blood levels of catecholamines, glucose or glucocorticoids, along with major changes in the peripheral metabolism of thyroid hormones, all known to follow critical states, have been implicated [20–23] . With hourly sampling, in a study of operated, mostly morbidly obese subjects, the FT 3 nadir was observed 2–4 h postoperatively and preceded the peak in serum IL-6 by 2–5 h postoperatively (casting doubt on the causative effects of IL-6 production on se-rum T 3 /FT 3 secretion) [24] . On the other hand, in exper-imental studies on human hepatoma cells (HepG2), TNF- � was found to activate the transcription factor NF- � B, leading to inhibition of T 3 -dependent induction of the type I 5 � -deiodinase gene [25] . Thus TNF- � may contrib-ute to the pathogenesis of NTI [25] . Although it seems certain that NTI is associated with an increased produc-tion and release of cytokines, the degree of cytokine in-volvement and their specific role in the pathogenesis of NTI remain to be clarified [13] . In the present study since
sampling was only done on a daily basis, the aforemen-tioned rapid changes that occur in the cytokine cascade were not observed. Nevertheless, a shift in the correla-tions of cytokines and thyroid function parameters was evident: TNF- � (which is secreted earlier in the proin-flammatory response cascade) was negatively correlated with T 3 (with no lag and a lag of 1–2 days) whereas IL-6 and IL-8 (which are secreted later in the pro- and anti-inflammatory response) were negatively correlated with T 3 (with a lag of 1–2 days). There was also a negative cor-relation between FT 4 on post-1 versus IL-6 on post-2. (We have no firm explanation for this finding; it may be at-tributed to central hypothalamic-pituitary-thyroid activ-ity, or changes in the T 3 /T 4 ratio; analogous correlations have been observed in patients treated for Hashimoto’s thyroiditis [26] .)
Taken together our data indicate that the euthyroid sick syndrome is not uncommon following major opera-tions and that cytokines are associated, at least in part, with this finding. More frequent blood sampling in the early postoperative period in large patient cohorts would better clarify these relationships.
Acknowledgment
This work was supported by a grant from the University of Athens (ELKE).
References
1 Martocchia A, Falaschi P: Role of genetic predisposition, cytokines, and neuroendo-crine response in development of thyroid au-toimmunity; in Plotnikoff NP, Faith RE, Murgo AJ, Good RA (eds): Cytokines, Stress and Immunity, ed 2. Boca Raton, CRC-Tay-lor & Francis, 2007, pp 359–370.
2 Berczi I, Quintanar-Stephano A, Kovacs K: Immunoconversion in acute phase response; in Plotnikoff NP, Faith RE, Murgo AJ, Good RA (eds): Cytokines, Stress and Immunity, ed 2. Boca Raton, CRC-Taylor & Francis 2007, pp 216–254.
3 Imamura M, Hashino S, Kobayashi H, et al: Serum cytokine levels in bone marrow trans-plantation: synergistic interaction of inter-leukin-6, interferon-gamma, and tumornecrosis factor-alpha in graft-versus-host disease. Bone Marrow Transplant 1994; 13: 745–751.
4 Schwaighofer H, Herold M, Schwarz T, et al: Serum levels of interleukin 6, interleukin 8, and C-reactive protein after human alloge-neic bone marrow transplantation. Trans-plantation 1994; 58: 430–436.
5 Castell JV, Gomez-Lechon MJ, David M, et al: Interleukin-6 is the major regulator of acute phase protein synthesis in adult hu-man hepatocytes. FEBS Lett 1989; 242: 237–239.
6 Khatri VP, Shah MH, Petrelli NJ, et al: Type-2 dominant cytokine gene expression fol-lowing hepatic surgery. J Hepatobiliary Pan-creat Surg 2006; 13: 442–449.
7 Kremen J, Dolinkova M, Krajickova J, et al: Increased subcutaneous and epicardial adi-pose tissue production of proinflammatory cytokines in cardiac surgery patients: pos-sible role in postoperative insulin resis-tance. J Clin Endocrinol Metab 2006; 91: 4620–4627.
8 Duggan E, Caraher E, Gately K, et al: Tumor necrosis factor-alpha and interleukin-10 gene expression in peripheral blood mono-nuclear cells after cardiac surgery. Crit Care Med 2006; 34: 2134–2139.
9 Poitou C, Lacorte JM, Coupaye M, et al: Re-lationship between single nucleotide poly-morphisms in leptin, IL6 and adiponectin genes and their circulating product in mor-bidly obese subjects before and after gastric banding surgery. Obes Surg 2005; 15: 11–23.
10 Wellby ML, Kennedy JA, Barreau PB, Roedi-ger WE: Endocrine and cytokine changes during elective surgery. J Clin Pathol 1994; 47: 1049–1051.
11 Juma AH, Ardawi MS, Baksh TM, Serafi AA: Alterations in thyroid hormones, cortisol, and catecholamine concentration in patients after orthopedic surgery. J Surg Res 1991; 50: 129–134.

Thyroid Function, Cytokines and Surgery
Neuroimmunomodulation 2007;14:243–247 247
12 Tsuchiya A, Goretzki PE, Gramse M, Joseph K, Wahl RA: Low T3 syndrome in patients following major surgery. Jpn J Surg 1985; 15: 285–290.
13 Papanicolaou DA: Euthyroid sick syndrome and the role of cytokines. Rev Endocr Metab Disord 2000; 1: 43–48.
14 Mastorakos G, Pavlatou M: Exercise as a stress model and the interplay between the hypothalamus-pituitary-adrenal and the hypothalamus-pituitary-thyroid axes. Horm Metab Res 2005; 37: 577–584.
15 Van der Poll T, Van Zee KJ, Endert E, et al: Interleukin-1 receptor blockade does not af-fect endotoxin-induced changes in plasma thyroid hormone and thyrotropin concen-trations in man. J Clin Endocrinol Metab 1995; 80: 1341–1346.
16 Cook EB, Stahl JL, Lowe L, et al: Simultane-ous measurement of six cytokines in a single sample of human tears using microparticle-based flow cytometry: allergics vs. non-al-lergics. J Immunol Methods 2001; 254: 109–118.
17 Hildesheim A, Ryan RL, Rinehart E, et al: Simultaneous measurement of several cyto-kines using small volumes of biospecimens. Cancer Epidemiol Biomarkers Prev 2002; 11: 1477–1484.
18 Moore KW, O’Garra A, de Waal Malefyt R, Vieira P, Mosmann TR: Interleukin-10. Annu Rev Immunol 1993; 11: 165–190.
19 de Waal Malefyt R, Yssel H, de Vries JE: Di-rect effects of IL-10 on subsets of human CD4+ T cell clones and resting T cells. Spe-cific inhibition of IL-2 production and pro-liferation. J Immunol 1993; 150: 4754–4765.
20 Fliers E, Alkemade A, Wiersinga WM, Swaab DF: Hypothalamic thyroid hormone feed-back in health and disease. Prog Brain Res 2006; 153: 189–207.
21 De Groot LJ: Non-thyroidal illness syn-drome is a manifestation of hypothalamic-pituitary dysfunction, and in view of current evidence, should be treated with appropriate replacement therapies. Crit Care Clin 2006; 22: 57–86, vi.
22 DeGroot LJ: ‘Non-thyroidal illness syn-drome’ is functional central hypothyroid-ism, and if severe, hormone replacement is appropriate in light of present knowledge. J Endocrinol Invest 2003; 26: 1163–1170.
23 Umpierrez GE: Euthyroid sick syndrome. South Med J 2002; 95: 506–513.
24 Michalaki M, Vagenakis AG, Makri M, Kalfarentzos F, Kyriazopoulou V: Dissocia-tion of the early decline in serum T 3 concen-tration and serum IL-6 rise and TNF � in nonthyroidal illness syndrome induced by abdominal surgery. J Clin Endocrinol Metab 2001; 86: 4198–4205.
25 Nagaya T, Fujieda M, Otsuka G, Yang JP, Okamoto T, Seo H: A potential role of acti-vated NF- � B in the pathogenesis of euthy-roid sick syndrome. J Clin Invest 2000; 106: 393–402.
26 Papanas NP, Papazoglou DP, Papatheodorou KP, et al: Thyroxine replacement dose in pa-tients with Hashimoto disease: a potential role for interleukin-6. Endocrine Abstracts 2006; 11:P844.