Embed Size (px)
Citation preview
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 1
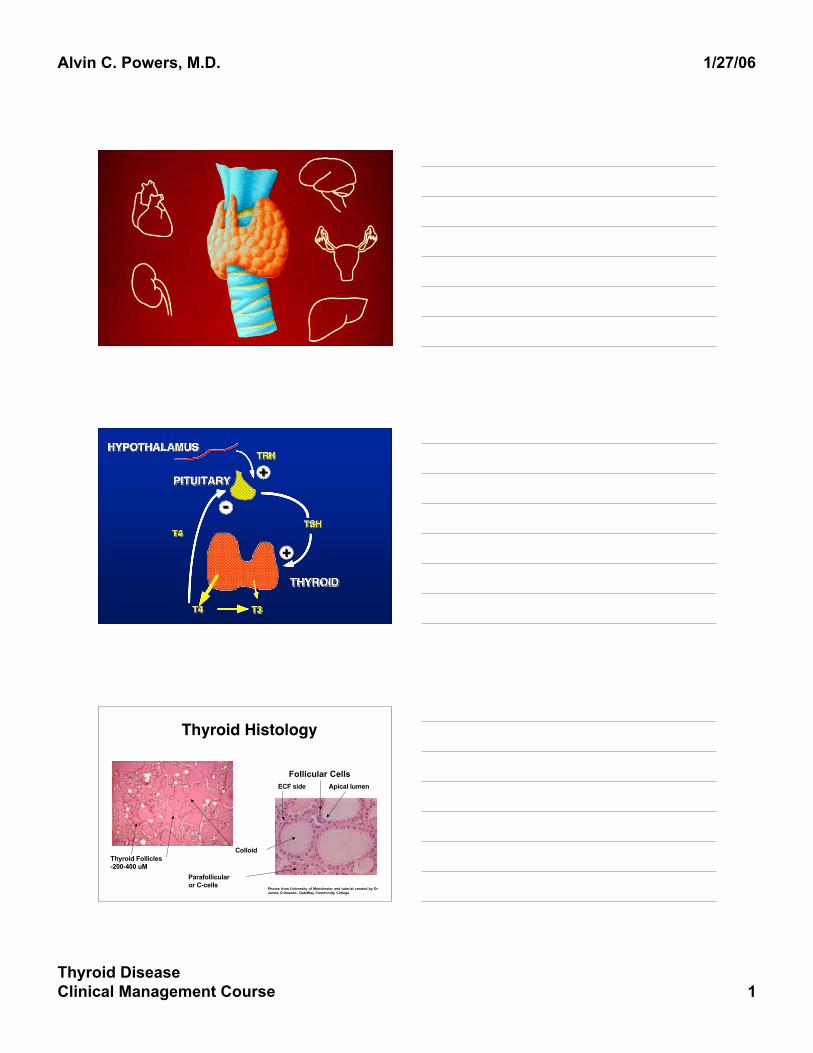
Thyroid Histology
Photos from University of Manchester and tutorial created by Dr.James Crimando, GateWay Community College
ColloidThyroid Follicles-200-400 uM
Parafollicularor C-cells
Follicular CellsApical lumenECF side
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 2
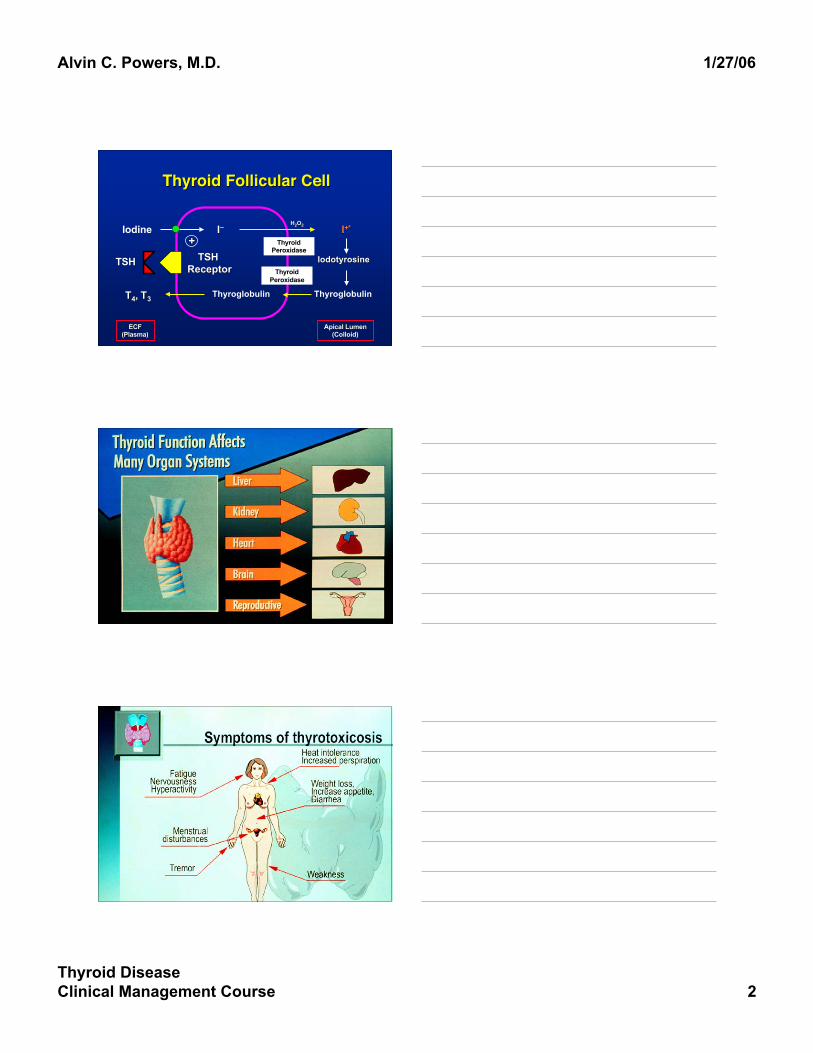
Thyroid Follicular CellThyroid Follicular Cell
TSHTSH TSH TSH ReceptorReceptor
TT44, T, T33 Thyroglobulin Thyroglobulin
ThyroidPeroxidase
Iodine++
II__
Apical LumenApical Lumen(Colloid)(Colloid)
ECFECF(Plasma)(Plasma)
IodotyrosineIodotyrosine
ThyroidPeroxidase
II+*+*HH22OO22
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 3

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 4
21 year old female is referred from her21 year old female is referred from hercardiologist for treatment of hyperthyroidism.cardiologist for treatment of hyperthyroidism.She is followed for asymptomatic aorticShe is followed for asymptomatic aorticinsufficiency.insufficiency.
Total T4 = 15.6 (Total T4 = 15.6 (nl nl = 4-12)= 4-12) Free T4 = 1.35 (Free T4 = 1.35 (nl nl = 0.8-1.9)= 0.8-1.9) TSH = 1.2 (TSH = 1.2 (nl nl = 0.4-5.0)= 0.4-5.0)
Thyroid Function TestsThyroid Function Tests
Total TTotal T44
Total TTotal T33
Free TFree T44
TSHTSH
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 5
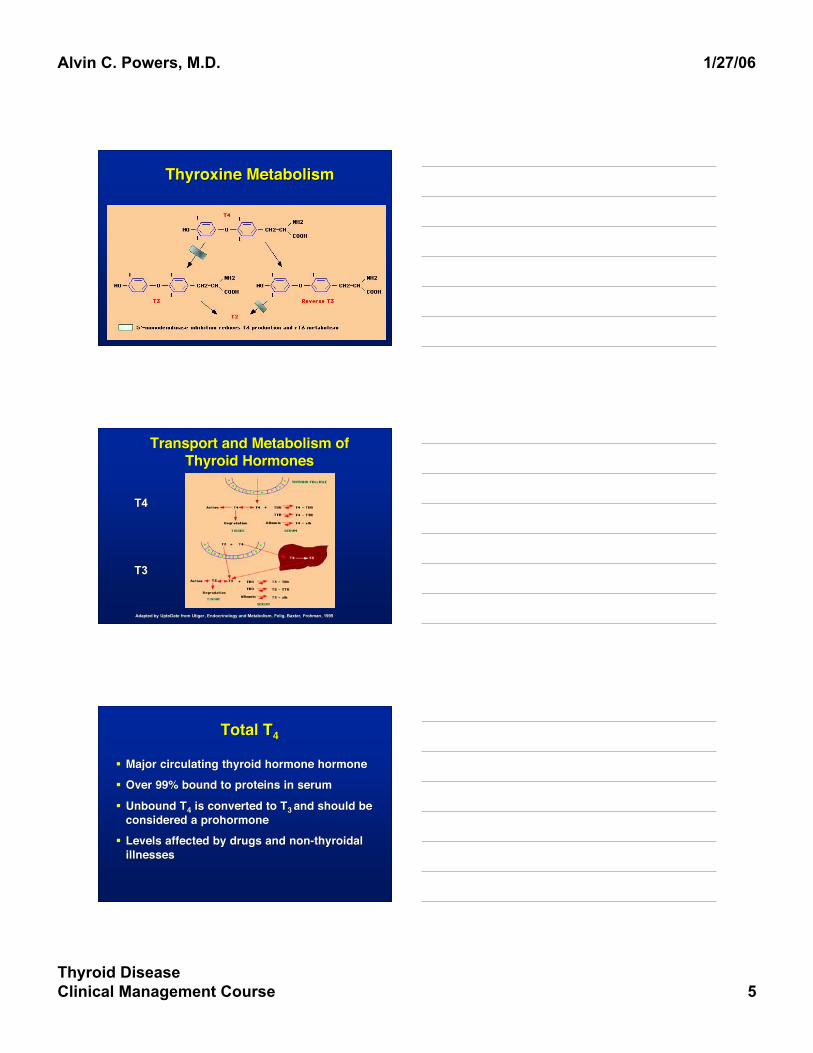
Thyroxine MetabolismThyroxine Metabolism
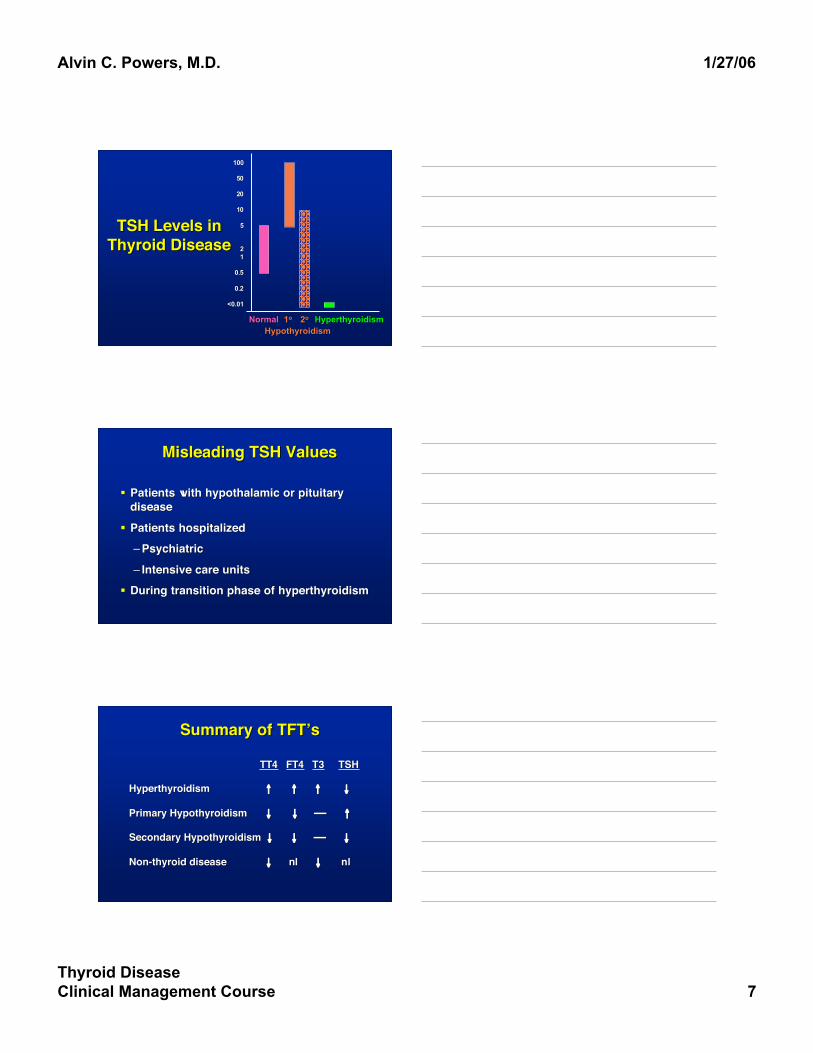
Transport and Metabolism ofTransport and Metabolism ofThyroid HormonesThyroid Hormones
Adapted by Adapted by UptoDate UptoDate from from UtigerUtiger, Endocrinology and Metabolism, , Endocrinology and Metabolism, FeligFelig, Baxter, , Baxter, FrohmanFrohman, 1995, 1995
T4T4
T3T3
Total TTotal T44
Major circulating thyroid hormone hormoneMajor circulating thyroid hormone hormone Over 99% bound to proteins in serumOver 99% bound to proteins in serum
Unbound TUnbound T44 is converted to T is converted to T3 3 and should beand should beconsidered a prohormoneconsidered a prohormone
Levels affected by drugs and non-thyroidalLevels affected by drugs and non-thyroidalillnessesillnesses

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 6
Free T4Free T4
Reflection of bioactive hormoneReflection of bioactive hormone Either measured directly or calculatedEither measured directly or calculated Calculated Free T4 (using Total T4 and an estimateCalculated Free T4 (using Total T4 and an estimate
of thyroid hormone binding capacity, the resin T3of thyroid hormone binding capacity, the resin T3uptake) is called a Free T4 indexuptake) is called a Free T4 index
Should order a Free T4 and not a total T4.Should order a Free T4 and not a total T4.
Total TTotal T33
Results from peripheral conversion from TResults from peripheral conversion from T4 4 andandthyroid production of Tthyroid production of T33
Bioactive hormone and is the major ligand for theBioactive hormone and is the major ligand for thethyroid hormone receptorthyroid hormone receptor
Always elevated in hyperthyroidismAlways elevated in hyperthyroidism Often normal in hypothyroidismOften normal in hypothyroidism
Thyroid Stimulating HormoneThyroid Stimulating Hormone
Gold standard-best overall indicator ofGold standard-best overall indicator ofthyroid diseasethyroid disease
Capable of separating hyperthyroid,Capable of separating hyperthyroid,euthyroid, and hypothyroid stateseuthyroid, and hypothyroid states
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 7
TSH Levels inTSH Levels inThyroid DiseaseThyroid Disease
11oo
HypothyroidismHypothyroidism22oo HyperthyroidismHyperthyroidismNormalNormal
100100
5050
2020
1010
55
2211
0.50.5
0.20.2
<0.01<0.01
Misleading TSH ValuesMisleading TSH Values
Patients with hypothalamic or pituitaryPatients with hypothalamic or pituitarydiseasedisease
Patients hospitalizedPatients hospitalized––PsychiatricPsychiatric
–– Intensive care unitsIntensive care units During transition phase of hyperthyroidismDuring transition phase of hyperthyroidism
Summary of Summary of TFTTFT’’ss
TT4TT4 FT4FT4 T3T3 TSHTSH
HyperthyroidismHyperthyroidism ↑↑ ↑↑ ↑↑ ↓↓
Primary HypothyroidismPrimary Hypothyroidism ↓↓ ↓↓ ↑↑
Secondary HypothyroidismSecondary Hypothyroidism ↓↓ ↓↓ ↓↓
Non-thyroid diseaseNon-thyroid disease ↓↓ nlnl ↓↓ nlnl
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 8
Suggested Use of ThyroidSuggested Use of ThyroidFunction TestsFunction Tests
Suspect thyroid diseaseSuspect thyroid disease -Free T4 and TSH -Free T4 and TSH Monitor T4 replacementMonitor T4 replacement -TSH -TSH If pituitary disease is presentIf pituitary disease is present -Free T4 -Free T4
48 year old man from Shelbyville is referred48 year old man from Shelbyville is referredby his primary care physician for weightby his primary care physician for weightloss, tachycardia, and tremor.loss, tachycardia, and tremor.
Free T4 = 4.2 (Free T4 = 4.2 (nl nl = 0.8-1.9)= 0.8-1.9)
TSH < 0.001 (TSH < 0.001 (nl nl = 0.4-5.0)= 0.4-5.0)
How would you evaluate him?How would you evaluate him?
Normal Thyroid ScanNormal Thyroid Scan

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 9
Thyroid Scan in GravesThyroid Scan in Graves’’ Disease Disease
Graves DiseaseGraves Disease
HyperthyroidismHyperthyroidism OphthalmopathyOphthalmopathy
Dermopathy Dermopathy (pre-(pre-tibial tibial myxedema)myxedema)
TSHTSHTSHReceptorTSHReceptor
IodineIodine IodineIodine IodotyrosineIodotyrosine
ThyroglobulinThyroglobulin T4T4
Thyroid PeroxidaseThyroid Peroxidase
++TSITSI
Thyroid Follicular CellThyroid Follicular Cell

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 10
A 34 year old woman, who is 4 months post-A 34 year old woman, who is 4 months post-partum (twin boys), reports a month longpartum (twin boys), reports a month longhistory of trouble sleeping, emotionalhistory of trouble sleeping, emotionallability, fatigue, and neck swelling. Onlability, fatigue, and neck swelling. Onexamination, she is mildly tachycardiac andexamination, she is mildly tachycardiac andhas a diffusely enlarged thyroid. She has nohas a diffusely enlarged thyroid. She has noeye findings to suggest Graveseye findings to suggest Graves’’ Disease. Disease.
Free T4 = 2.8 (normal 0.9 - 1.9)Free T4 = 2.8 (normal 0.9 - 1.9)
TSH = <0.05 (normal 0.3 - 4.0)TSH = <0.05 (normal 0.3 - 4.0)HOW WOULD YOU EVALUTE HER?HOW WOULD YOU EVALUTE HER?
Low Uptake on Thyroid ScanLow Uptake on Thyroid Scan
Causes of ThyrotoxicosisCauses of Thyrotoxicosis Normal or Increased Activity on Thyroid ScanNormal or Increased Activity on Thyroid Scan–– Graves DiseaseGraves Disease–– Multinodular Multinodular Goiter or Hot NoduleGoiter or Hot Nodule
Decreased Activity on Thyroid ScanDecreased Activity on Thyroid Scan–– ThyroiditisThyroiditis–– Iodine-induced thyrotoxicosis (Iodine-induced thyrotoxicosis (amiodaroneamiodarone))–– Exogenous thyroid hormone useExogenous thyroid hormone use

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 11
Multinodular Multinodular GoiterGoiter
A 71 year old man comes for theA 71 year old man comes for theevaluation of weight loss, poor appetite,evaluation of weight loss, poor appetite,and new-onset congestive heart failureand new-onset congestive heart failure(mild). His thyroid function tests show:(mild). His thyroid function tests show:
Free T4 = 1.9 (normal 0.9 - 1.9)Free T4 = 1.9 (normal 0.9 - 1.9)
TSH = <0.05 (normal 0.2 - 4.0)TSH = <0.05 (normal 0.2 - 4.0)
IS HE HYPERTHYROID?IS HE HYPERTHYROID?
TSHTSH
TT44
NormalNormal
NormalNormalBA
B = Develops hypothyroidismB = Develops hypothyroidismB
A
A = Develops hyperthyroidismA = Develops hyperthyroidism
Individualized Set Point for TIndividualized Set Point for T44

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 12
Treatment of HyperthyroidismTreatment of Hyperthyroidism
Antithyroid Antithyroid DrugsDrugs
Radioactive Radioactive IodineIodine
SurgerySurgery
74 year old woman is brought74 year old woman is broughtby her son who has noticed:by her son who has noticed:
Decreased memoryDecreased memory FatigueFatigue
ConstipationConstipation
She has the heat on in her house in theShe has the heat on in her house in thesummer.summer.
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 13
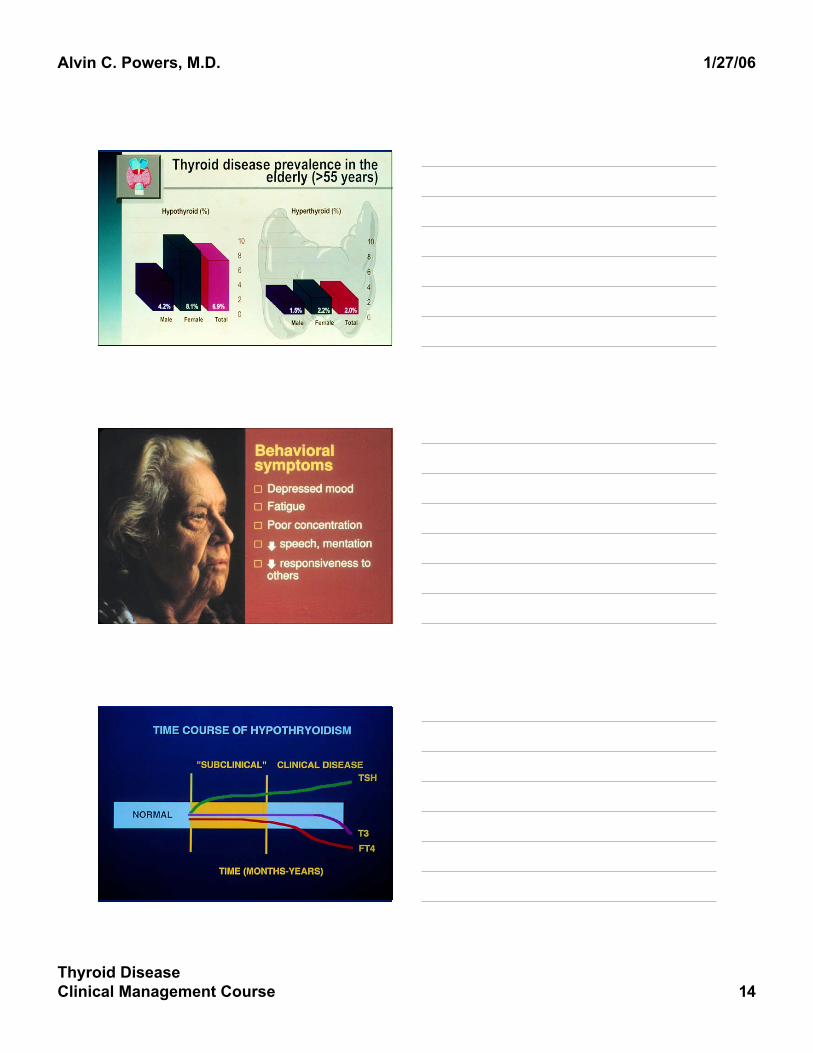
Patient withPatient withHypothyroidismHypothyroidism
HypothyroidismHypothyroidism
TSH is best indicatorTSH is best indicator May or may not have a goiterMay or may not have a goiter
Thyroid scanning or ultrasound is notThyroid scanning or ultrasound is notnecessarynecessary
Autoimmune or post-surgical are the mostAutoimmune or post-surgical are the mostcommon causescommon causes
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 14
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 15
““You know the thyroid gland in your throat-theYou know the thyroid gland in your throat-theone that stokes the engine and keeps the oldone that stokes the engine and keeps the oldbrain working. In some people the thingbrain working. In some people the thingdoesndoesn’’t work properly and they turn out to bet work properly and they turn out to becretinous imbecilescretinous imbeciles…….., but feed .., but feed ‘‘em the stuffem the stuffand they come out absolutely all rightand they come out absolutely all right……....””
Lord Peter Wimsey in Dorothy SayersLord Peter Wimsey in Dorothy Sayers’’ HangmanHangman’’s Holidays Holiday, 1933, 1933
Treatment of HypothyroidismTreatment of Hypothyroidism
Thyroid Hormone SupplementsThyroid Hormone Supplements Well-tolerated; well-absorbed from GI tractWell-tolerated; well-absorbed from GI tract One of most commonly prescribed medicationsOne of most commonly prescribed medications Current preparations consist of synthetic TCurrent preparations consist of synthetic T44
((EuthyroxEuthyrox, , LevothyroidLevothyroid, , LevoxylLevoxyl, Synthroid,, Synthroid,UnithroidUnithroid) and/or T) and/or T33
New evidence does not support replacement withNew evidence does not support replacement withTT44 and T and T33
TT33 results from T results from T44 metabolism and is not routinely metabolism and is not routinelyprescribed.prescribed.
Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 16
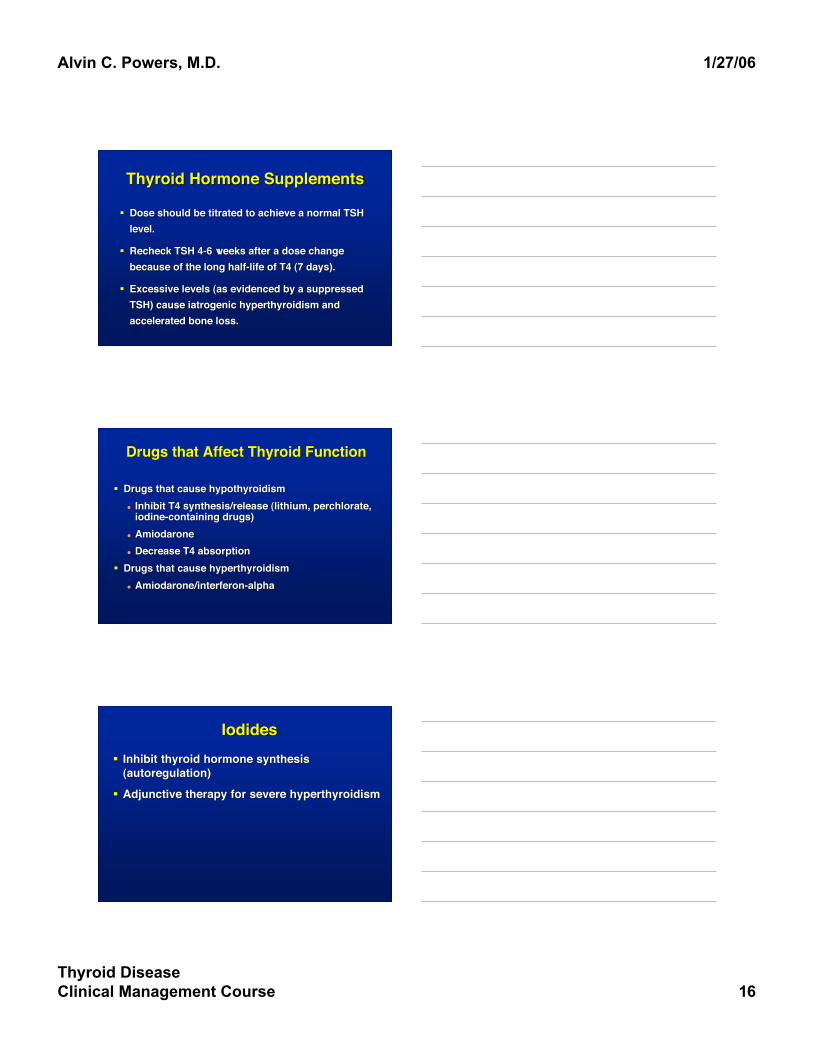
Thyroid Hormone SupplementsThyroid Hormone Supplements
Dose should be titrated to achieve a normal TSHDose should be titrated to achieve a normal TSHlevel.level.
Recheck TSH 4-6 weeks after a dose changeRecheck TSH 4-6 weeks after a dose changebecause of the long half-life of T4 (7 days).because of the long half-life of T4 (7 days).
Excessive levels (as evidenced by a suppressedExcessive levels (as evidenced by a suppressedTSH) cause iatrogenic hyperthyroidism andTSH) cause iatrogenic hyperthyroidism andaccelerated bone loss.accelerated bone loss.
Drugs that Affect Thyroid FunctionDrugs that Affect Thyroid Function
Drugs that cause hypothyroidismDrugs that cause hypothyroidism Inhibit T4 synthesis/release (lithium, perchlorate,Inhibit T4 synthesis/release (lithium, perchlorate,
iodine-containing drugs)iodine-containing drugs) AmiodaroneAmiodarone Decrease T4 absorptionDecrease T4 absorption
Drugs that cause hyperthyroidismDrugs that cause hyperthyroidism AmiodaroneAmiodarone/interferon-alpha/interferon-alpha
IodidesIodides Inhibit thyroid hormone synthesisInhibit thyroid hormone synthesis
(autoregulation)(autoregulation)
Adjunctive therapy for severe hyperthyroidismAdjunctive therapy for severe hyperthyroidism

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 17
SSaturated aturated SSolutions ofolutions ofPPotassium otassium IIodideodide(SSKI) is most(SSKI) is mostcommon preparation;common preparation;some countries havesome countries haveemergency stores ofemergency stores ofthis in case of athis in case of anuclear accident.nuclear accident.
IodidesIodides
19 year old Vanderbilt undergraduate is19 year old Vanderbilt undergraduate isreferred for a left sided thyroid nodule thatreferred for a left sided thyroid nodule thatwas found in Student Health when she waswas found in Student Health when she wasseen for a sore throat.seen for a sore throat.
TFTTFT’’s s normalnormal
Thyroid NodulesThyroid Nodules
Most are benign.Most are benign. Hot nodules are benign; thyroid cancer is coldHot nodules are benign; thyroid cancer is cold
on scanning.on scanning. Most are cold on thyroid scanningMost are cold on thyroid scanning Ultrasound cannot confirm or excludeUltrasound cannot confirm or exclude
malignancy.malignancy. FNA is required for all cold nodules.FNA is required for all cold nodules.

Alvin C. Powers, M.D. 1/27/06
Thyroid DiseaseClinical Management Course 18