Embed Size (px)
Citation preview
L I S A A . C I C O , M S N , N P U P S T A T E M E D I C A L U N I V E R S I T Y B R E A S T & E N D O C R I N E S U R G E R Y
C O O R D I N A T O R T H Y R O I D C A N C E R P R O G R A M S U R G I C A L C O O R D I N A T O R B R E A S T C A N C E R
P R O G R A M
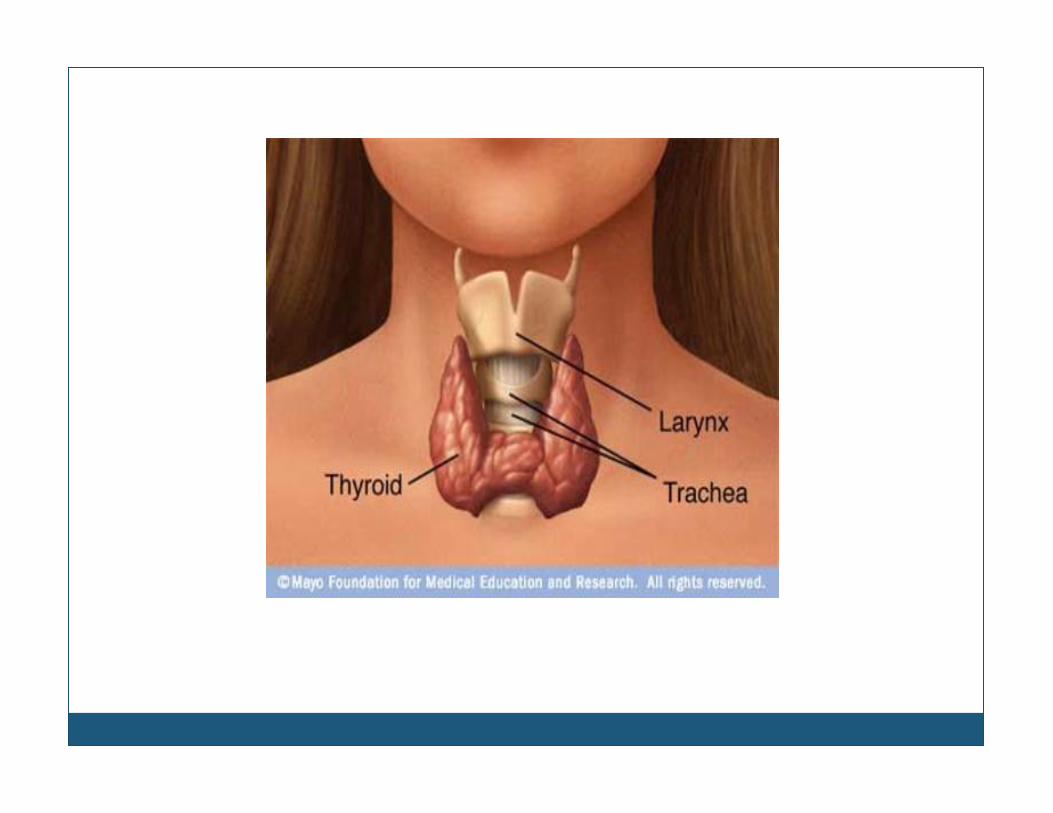
THYROID NODULES
OBJECTIVES Describe tools / diagnostic testing for assessment of the patient with a thyroid nodule(s)
*Utilize national guidelines developed for patients with thyroid nodules
*Describe some of the common symptoms of patients with thyroid nodules
Comprehensive review of current diagnostic tools and imaging to assess thyroid nodules
Review American Thyroid Association, & National Comprehensive Cancer Network Guidelines for patients who develop thyroid nodules
Review common symptoms of patients with thyroid nodule
OBJECTIVES Identify which patients can safely be followed by PCP
*Describe imaging/diagnostic modalities for following the patient with thyroid nodules
*Identify those patients requiring referral to specialty
*Identify which specialty to make an appropriate referral based on diagnostic, objective and symptomatic findings
Obtaining appropriate imaging/diagnostic testing, and frequency
Overview of ultrasonographic thyroid terminology
Overview of Betheseda thyroid nodule pathology terminology
Obtaining appropriate personal and family history
Identify what patients require referral and to endocrine or surgery?
Briefly discuss appropriate follow up for the patient with thyroid cancer
Definition of Thyroid Nodule
“A discrete lesion within the thyroid gland that is palpably and/or ultrasonographically distinct from surrounding thyroid parenchyma”
*ATA Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer (2006 & 2009 Task Force)
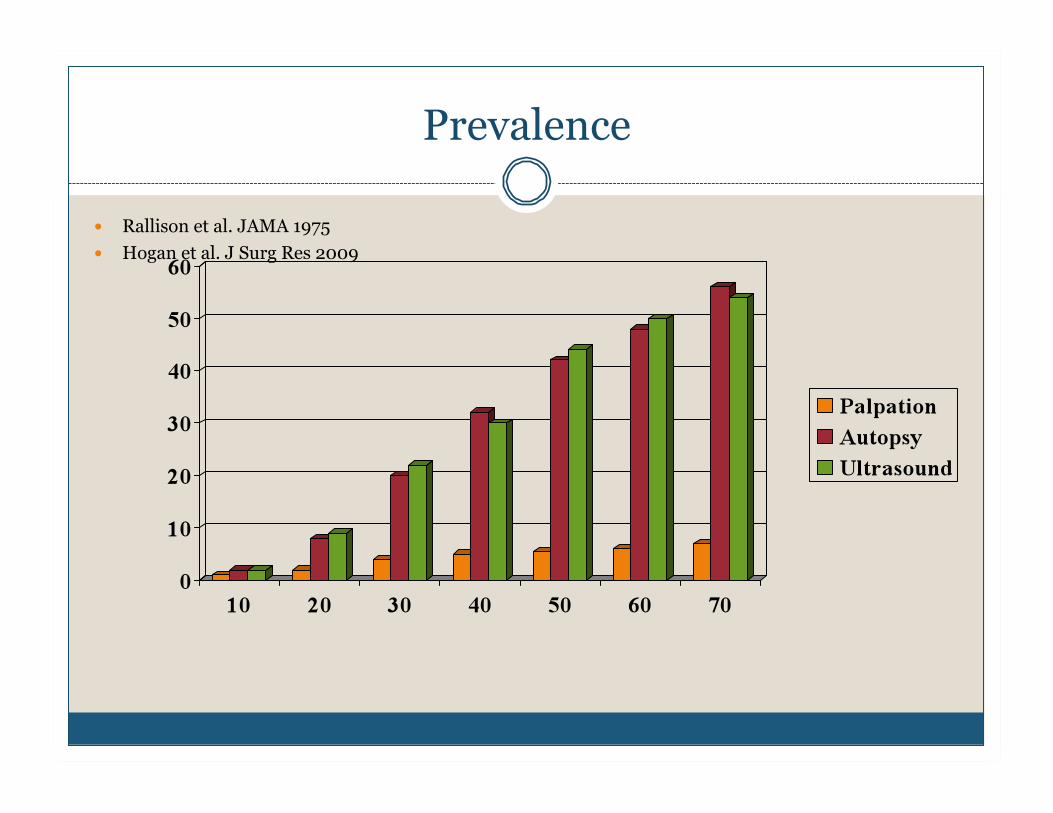
Prevalence
Rallison et al. JAMA 1975 Hogan et al. J Surg Res 2009
“How was this nodule found?”
Palpation with a physical exam Incidental finding on diagnostic work up Self detection Surveillance Work up for symptoms of hyper/hypothyroidism
How was found is it clinically relevant?
Physical Examination of Thyroid Gland
Visual inspection Palpation of thyroid, neck nodes, and supraclavicular
nodes Fixed, mobile, soft, tender? Reflexes why? HR, BP, weight
Symptoms
Usually NONE!! Occasionally painful, quick onset (cyst) Difficulty swallowing Hoarseness OR change in voice Shortness of breath (or difficulty swallowing) usually
while supine OR hands raised over head (Pemberton’s Sign)
Choking sensation hyper/hypo thyroid
Nodules Hyper/Hypo thyroid
Difficulty swallowing
Globus sensation
Choking sensation
Hyper-functioning nodule
Hashimoto’s
Symptoms?
History Physical Findings
Head & neck irradiation
Whole body irradiation Nuclear fallout Family history of
thyroid malignancy Heredity
Rapid growth Hoarseness Cervical /supraclavicular
lymphadenopathy Fixation of nodule or
gland > 4 cm Solitary
Pertinent History & PE in Evaluation of TNs
Differential Diagnosis
Multinodular Goiter Hashimoto’s Thyroiditis Cancer Lymphoma
Solitary Thyroid Nodule Substernal Goiter
C O W D E N ’ S S Y N D R O M E F A M I L I A L P O L Y P O S I S
C A R N E Y C O M P L E X M E N 2
W E R N E R S Y N D R O M E T H Y R O I D M A L I G N A N C Y
Family History of
Hereditary Diseases
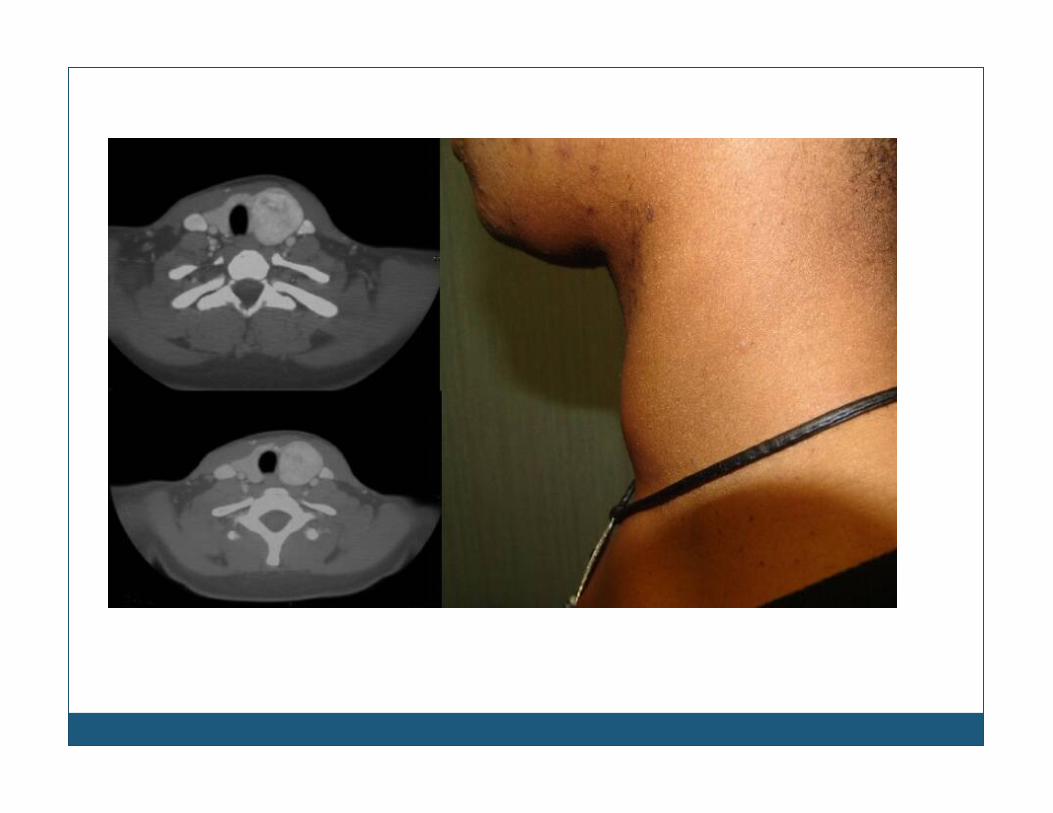
Substernal Goiters
Short neck Stocky build
Usually incidental finding by CXR or CT Many times treated unsuccessfully for asthma
Ultrasound: The Gold Standard
Anyone found to have, OR is suspected of having a nodule evaluate by ultrasound!!
BENIGN CHARACTERISTICS
Pure cystic (relatively rare)
Spongiform appearance in >50% of nodule volume (aggregration of multiple microcystic components)
Multiple (?)
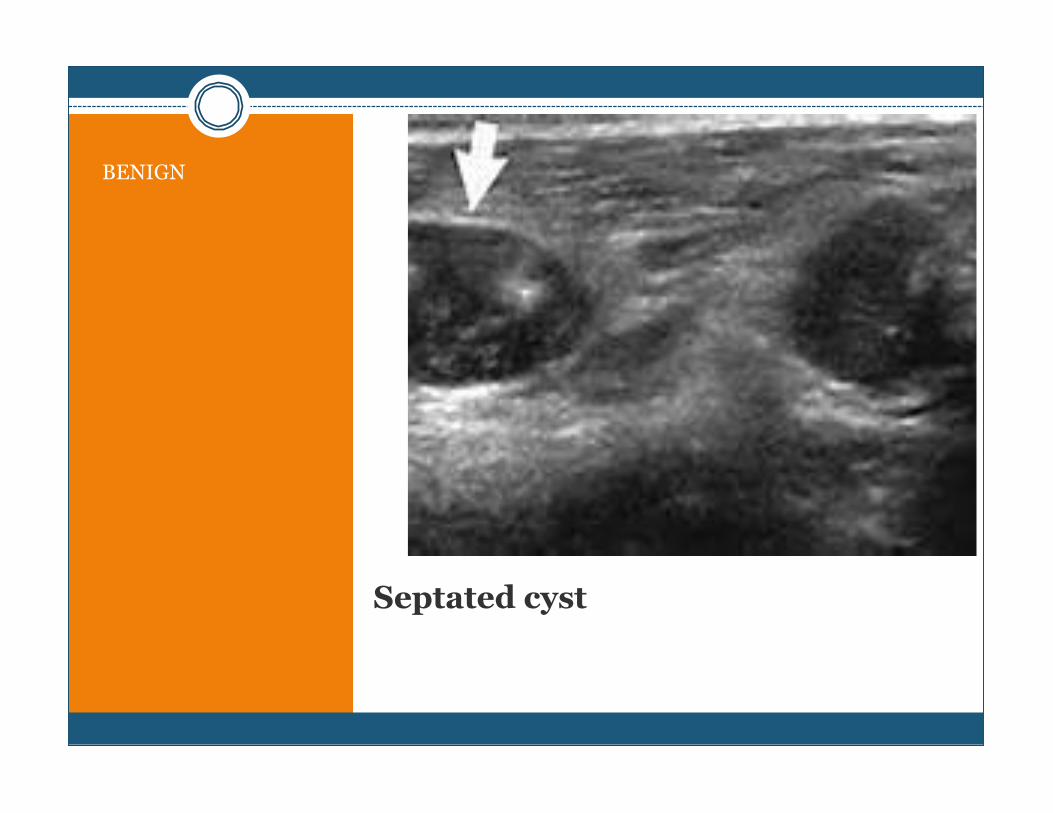
Septated cyst
BENIGN
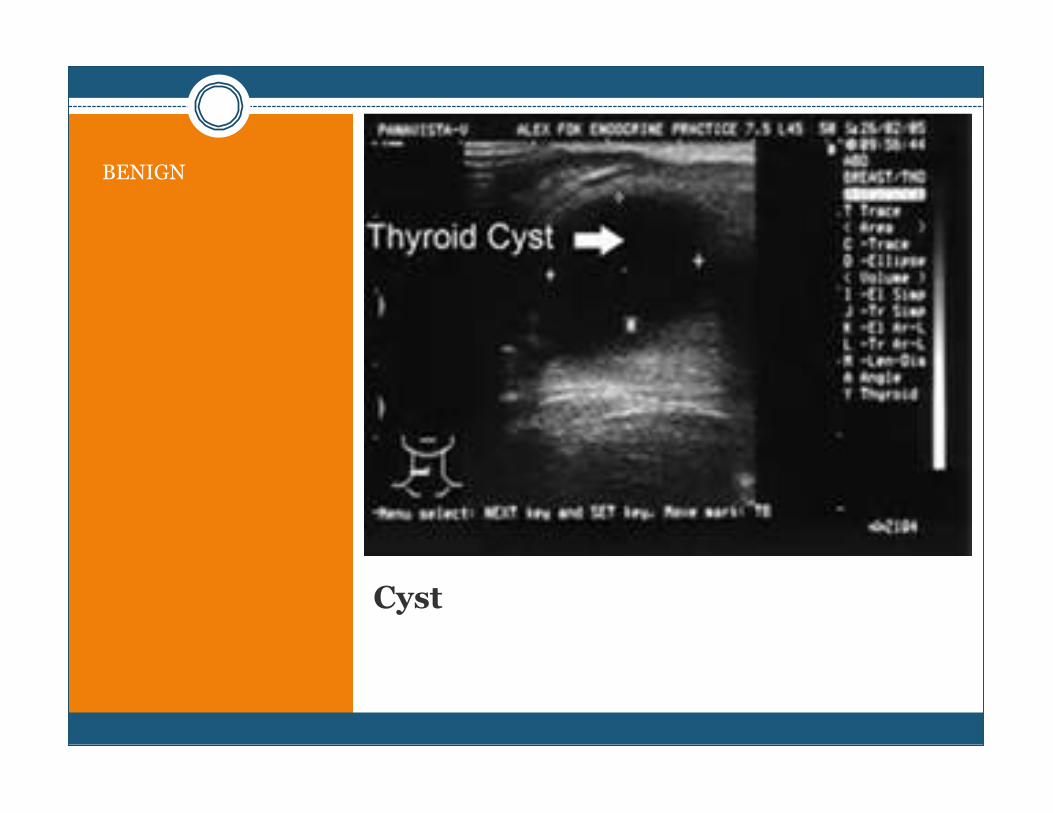
Cyst
BENIGN
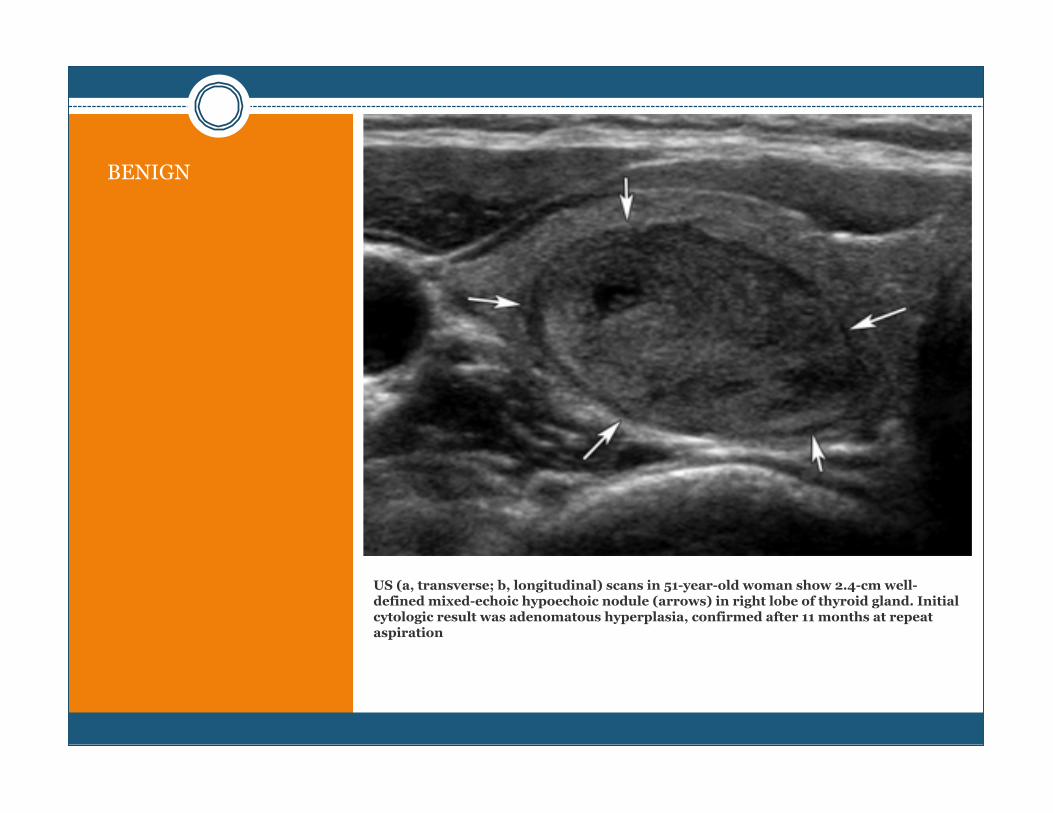
US (a, transverse; b, longitudinal) scans in 51-year-old woman show 2.4-cm well-defined mixed-echoic hypoechoic nodule (arrows) in right lobe of thyroid gland. Initial cytologic result was adenomatous hyperplasia, confirmed after 11 months at repeat aspiration
BENIGN
ULTRASOUND CHARACTERISTIC
CONSIDERATIONS
High-risk history: History of thyroid cancer in one or more first degree relatives; history of external beam radiation as a child; exposure to ionizing radiation in childhood or adolescence; prior hemithyroidectomy with discovery of thyroid cancer, 18FDG avidity on PET scanning; MEN2/FMTC-associated RET protooncogene mutation, calcitonin >100 pg/mL. MEN, multiple endocrine neoplasia; FMTC, familial medullary thyroid cancer.
Suspicious features: microcalcifications; hypoechoic; increased nodular vascularity; infiltrative margins; taller than wide on transverse view.
FNA cytology may be obtained from the abnormal lymph node in lieu of the thyroid nodule.
Sonographic monitoring without biopsy may be an acceptable alternative
SUSPICIOUS CHARACTERISTICS
Hypo-echogenicity compared to normal thyroid parenchyma
Increased intra-nodular vascularity Irregular infiltrative margins Presence of micro-calcifications Absent halo Shape taller than width in transverse
dimension Nodules > 4 cm Solitary Difficulty swallowing
ATA Guidelines 2009
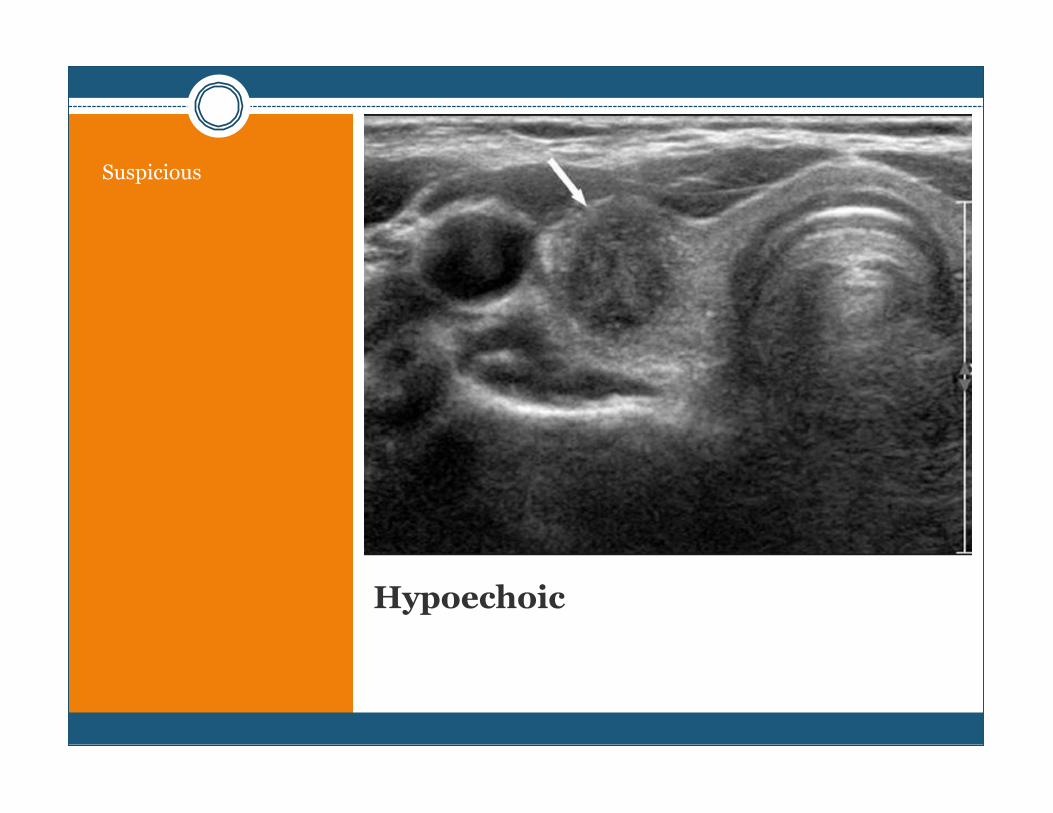
Hypoechoic
Suspicious
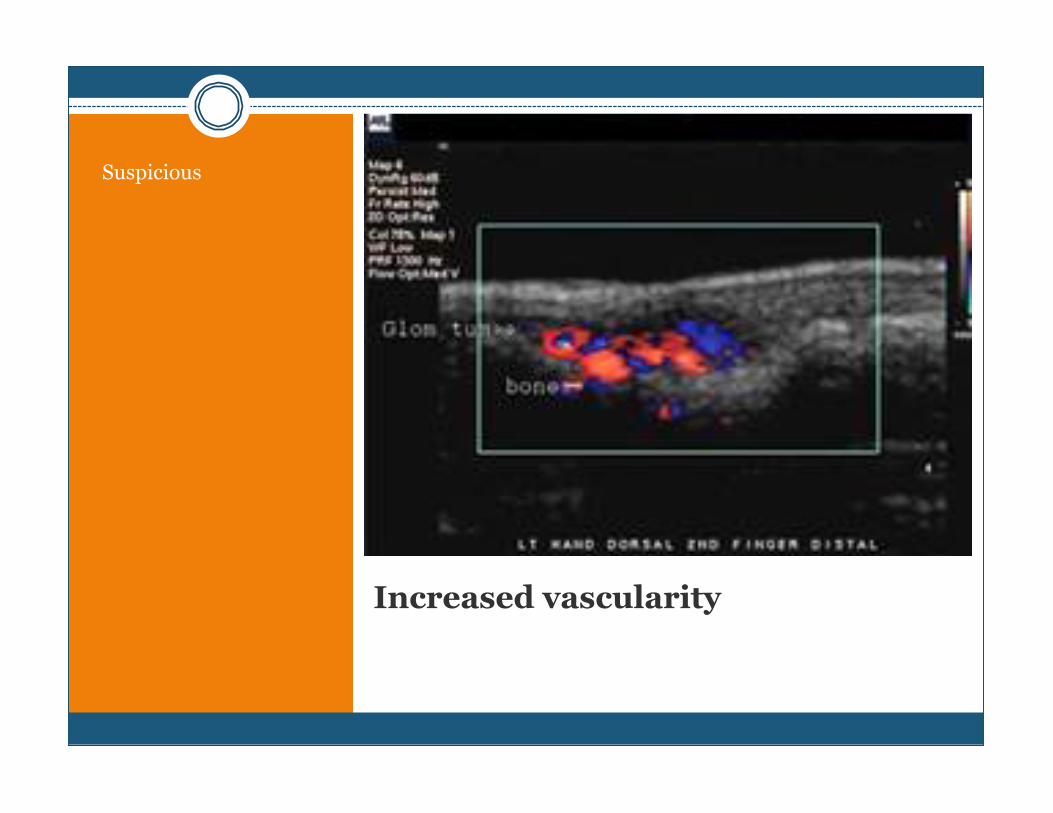
Increased vascularity
Suspicious
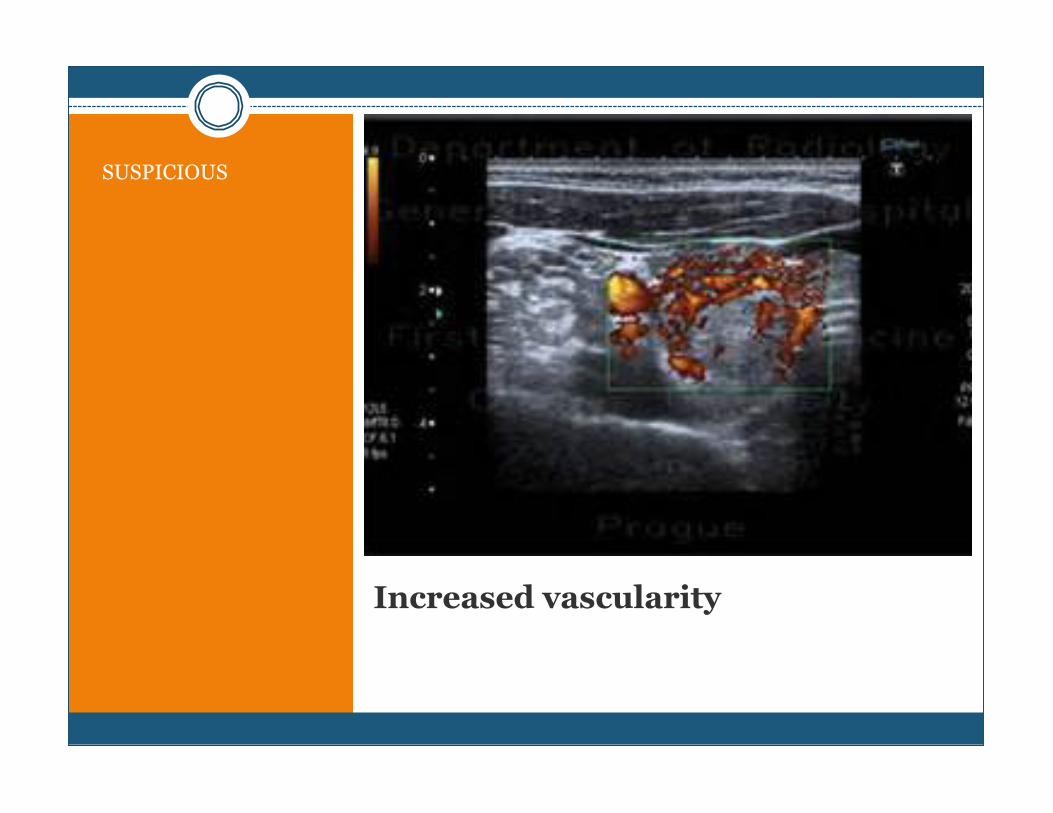
Increased vascularity
SUSPICIOUS
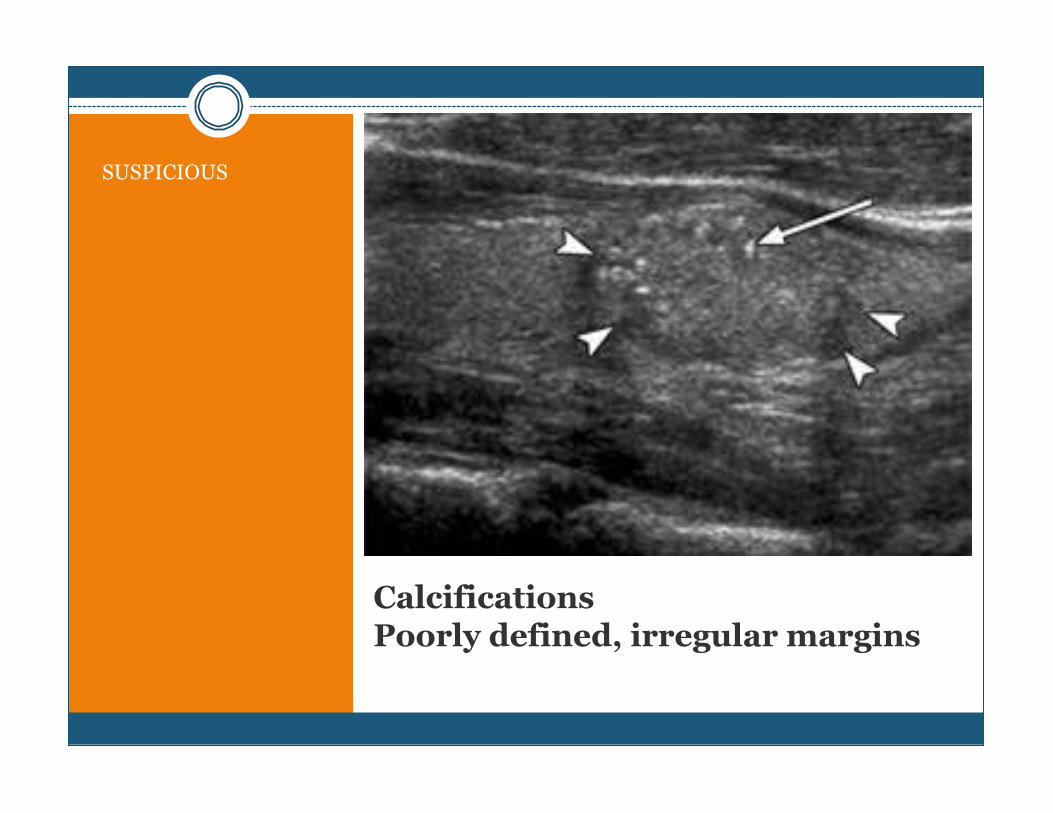
Calcifications Poorly defined, irregular margins
SUSPICIOUS
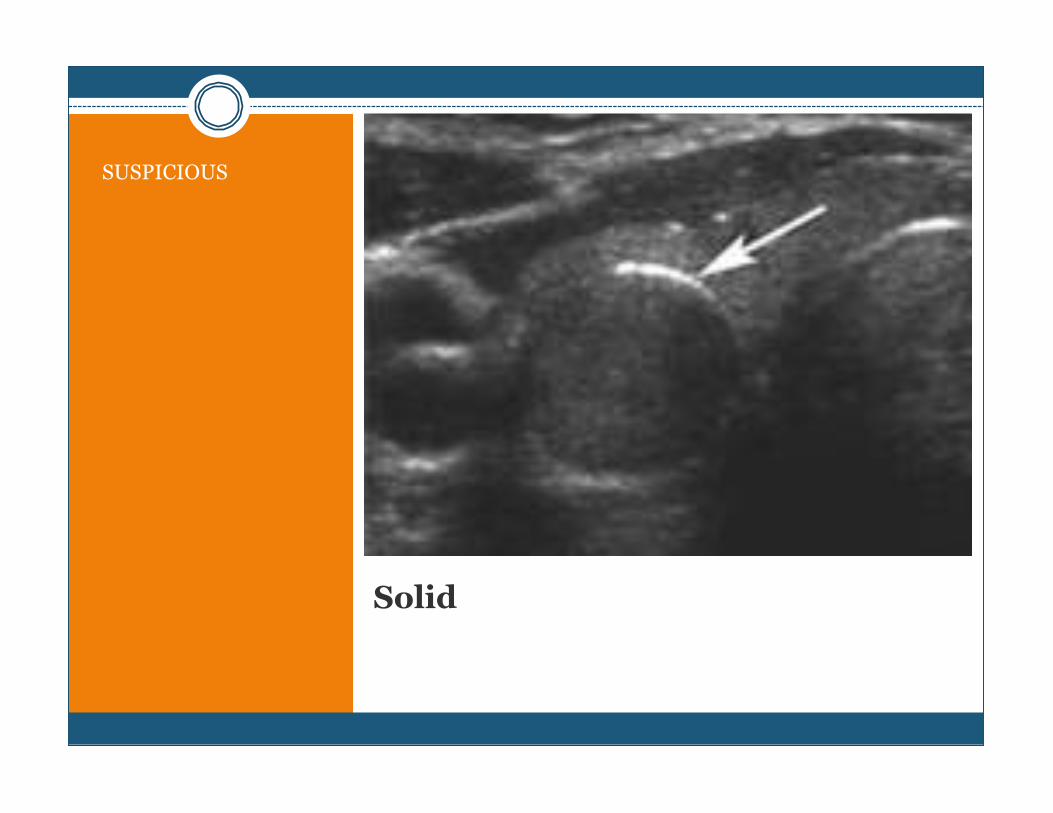
Solid
SUSPICIOUS
Multiple Thyroid Nodules
FNA what nodule?? > 1 cm Suspicious features Dominant / largest one
Palpation? Ultrasound?
What nodule(s) do you FNA?
What nodule(s) do you FNA?
FNA of Palpable Nodule
TN with suppressed TSH
UPTAKE SCAN to assess autonomous nodule
Compare to U/S what is the correlation with Uptake
FNA consider in non - functioning or isofunctioning with suspicious features
FNA
Only GOLD standard for proof of malignancy without surgical pathology
False Negative False Positive
false-negative rate of up to 5% with FNA which may be even higher with nodules >4 cm
??
FNA
< 1 cm > 1 cm
NO
ATA Guidelines 2009
NO
Is Size a Predictor of Malignancy?
FNA Results
Nondiagnostic Benign Atypia of Undetermined Significance (AUS) Suspicious for a Follicular Neoplasm/Follicular
Neoplasm Suspicious for Malignancy Malignant
Bethesda System for Reporting Thyroid Cytopathology
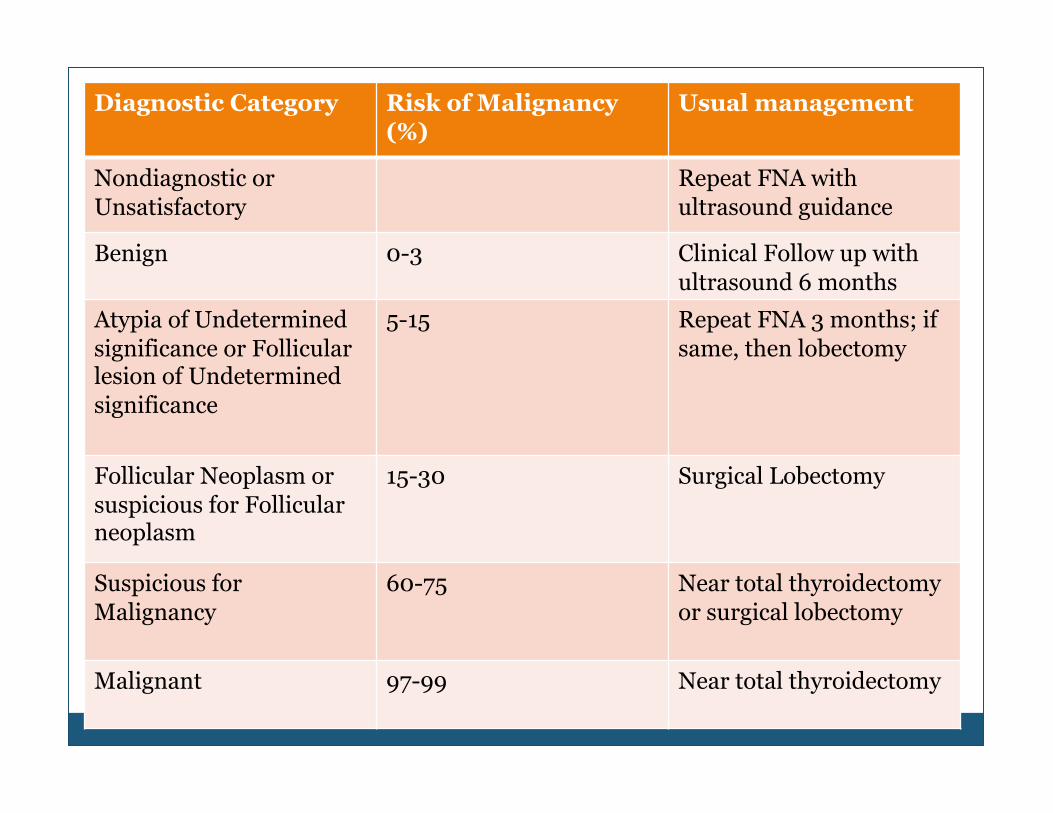
Diagnostic Category Risk of Malignancy (%)
Usual management
Nondiagnostic or Unsatisfactory
Repeat FNA with ultrasound guidance
Benign 0-3 Clinical Follow up with ultrasound 6 months
Atypia of Undetermined significance or Follicular lesion of Undetermined significance
5-15 Repeat FNA 3 months; if same, then lobectomy
Follicular Neoplasm or suspicious for Follicular neoplasm
15-30 Surgical Lobectomy
Suspicious for Malignancy
60-75 Near total thyroidectomy or surgical lobectomy
Malignant 97-99 Near total thyroidectomy
Lab Work
TSH Free T4
TPO in suspected thyroiditis
TG tumor marker in PTC, FTC, HTC
Calcitonin suspected MTC or in follow up of MTC
TSH
Free T4
T4
T3
Free T3
TPO
Thyroglobulin (TG)
Calcitonin
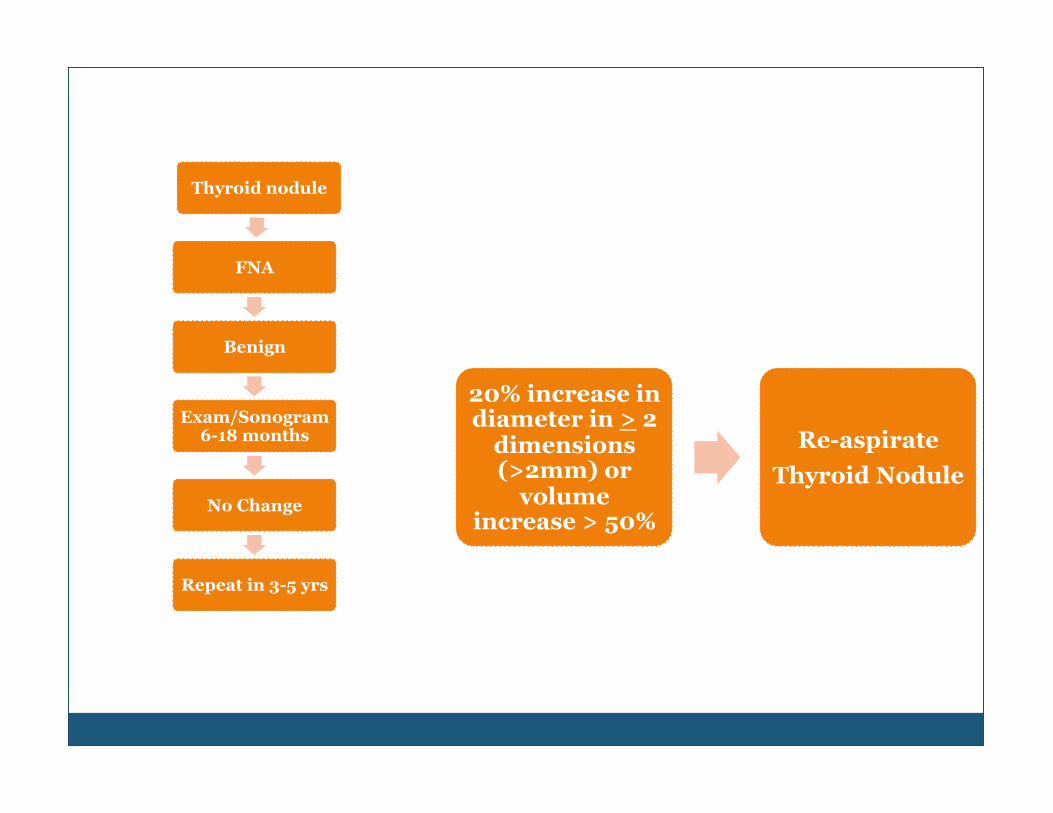
Thyroid nodule
FNA
Benign
Exam/Sonogram 6-18 months
No Change
Repeat in 3-5 yrs
20% increase in diameter in > 2
dimensions (>2mm) or
volume increase > 50%
Re-aspirate Thyroid Nodule
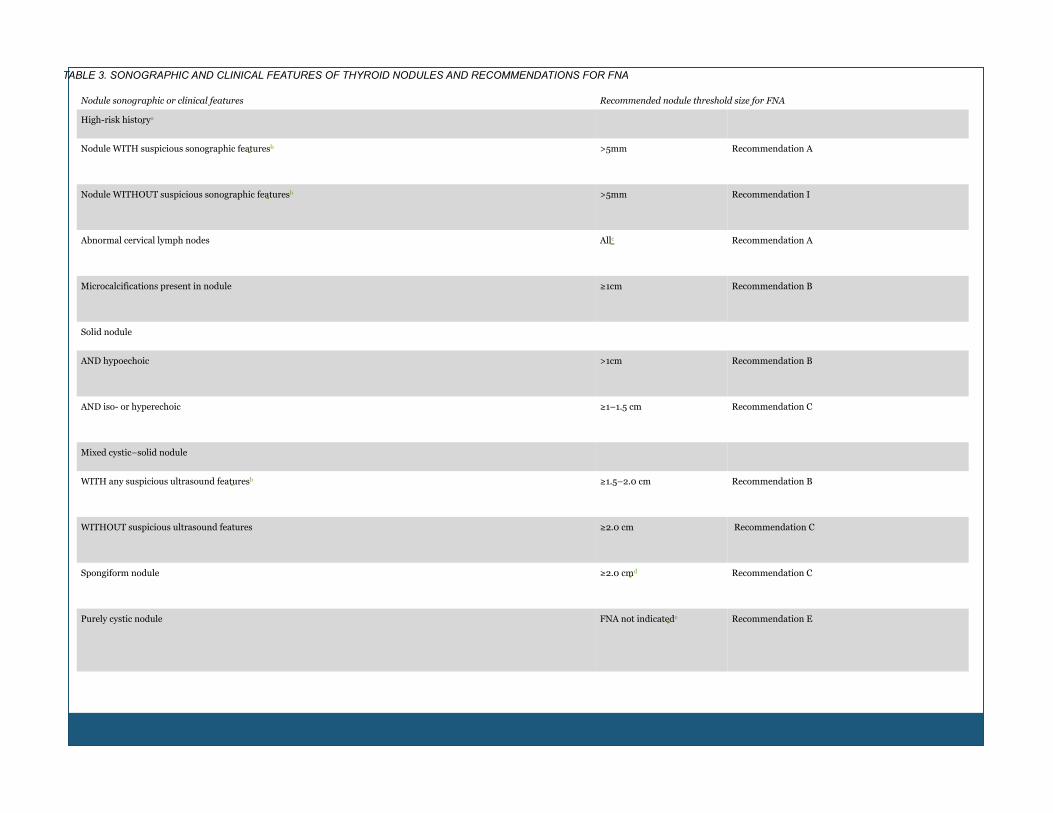
Nodule sonographic or clinical features Recommended nodule threshold size for FNA
High-risk historya
Nodule WITH suspicious sonographic featuresb >5mm Recommendation A
Nodule WITHOUT suspicious sonographic featuresb >5mm Recommendation I
Abnormal cervical lymph nodes Allc Recommendation A
Microcalcifications present in nodule ≥1cm Recommendation B
Solid nodule
AND hypoechoic >1cm Recommendation B
AND iso- or hyperechoic ≥1–1.5 cm Recommendation C
Mixed cystic–solid nodule
WITH any suspicious ultrasound featuresb ≥1.5–2.0 cm Recommendation B
WITHOUT suspicious ultrasound features ≥2.0 cm Recommendation C
Spongiform nodule ≥2.0 cmd Recommendation C
Purely cystic nodule FNA not indicatede Recommendation E
TABLE 3. SONOGRAPHIC AND CLINICAL FEATURES OF THYROID NODULES AND RECOMMENDATIONS FOR FNA
RAI Uptake Scan
ONLY IN HYPERTHYROID
Cold Nodule - 10% incidence of being CA
From 2005 to 2009, incidence rates increased by 5.6% per year in men and 7.0% per year in women, making thyroid cancer the fastest increasing cancer in both men and women
Most common endocrine cancer
Thyroid Cancers
Projected Cases of Thyroid Cancer
60, 220 new cases are estimated for 2013 45, 310 female 14, 910 male
1,850 deaths projected for 2013 1,040 female 810 male Death rate 0.5 per 100,000 in both male and females
AGE & INCIDENCE AMCERICAN CANCER SOCIETY / NCCN/ SEER
Diagnosed at a younger age then most adult cancers Median age at diagnosis was 50 years from 2005-2009 2 out of 3 cases are < 55 years old
Thyroid cancer in the pediatric population Pediatric Incidence 2.0 per 1 million in children <15 yrs and
17.6 per 1 million in children 15-19 yrs 2% occur in children and teens
TREATMENT FOR
THYROID
CANCER
Surgery
Radioactive Iodine Ablation
Levothyroxine
Monitor with WBS / ultrasound
CHILDREN &
PREGNANT WOMEN
W H E N D O Y O U O P E R A T E ? ? ?
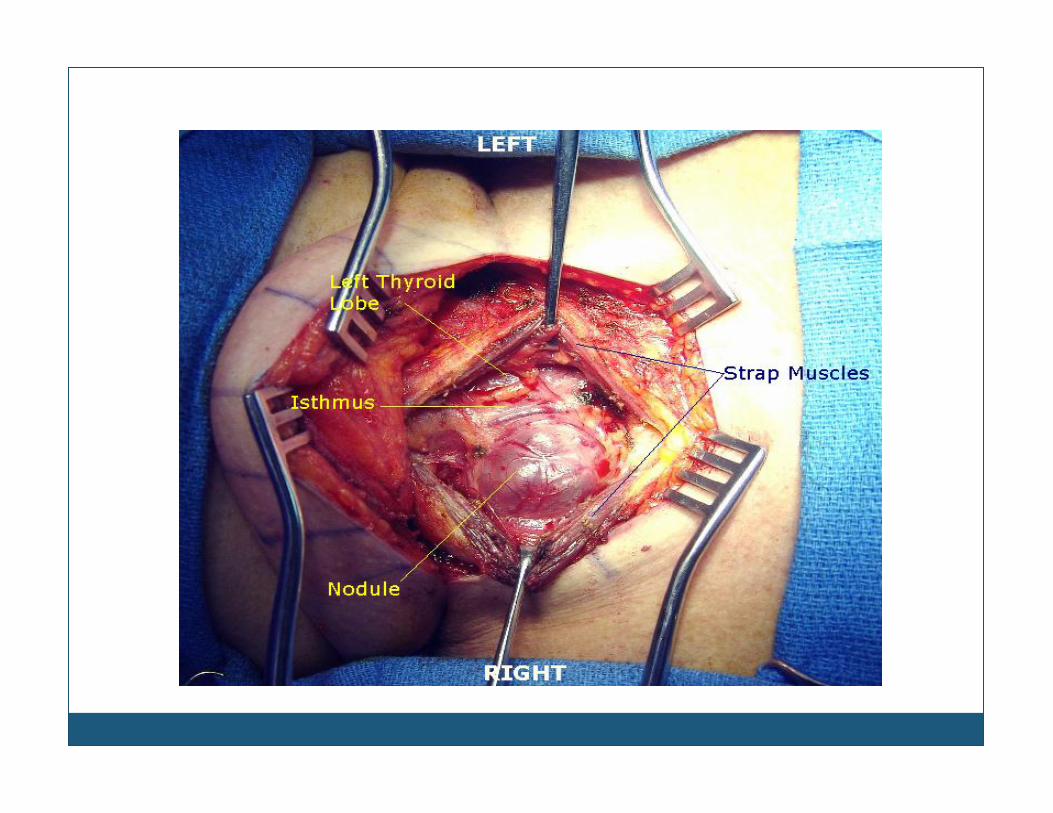
Complications of Thyroid Surgery
Recurrent laryngeal nerve injury
Hypo parathyroidism
Bleeding
Infection
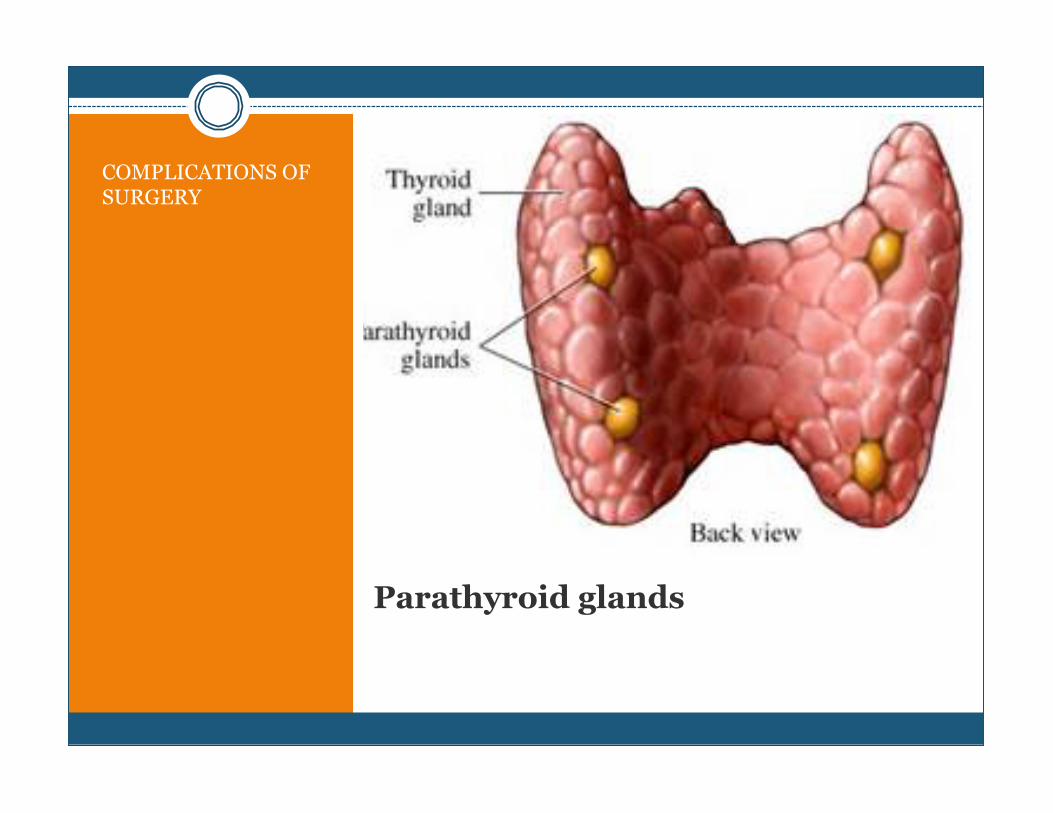
Parathyroid glands
COMPLICATIONS OF SURGERY
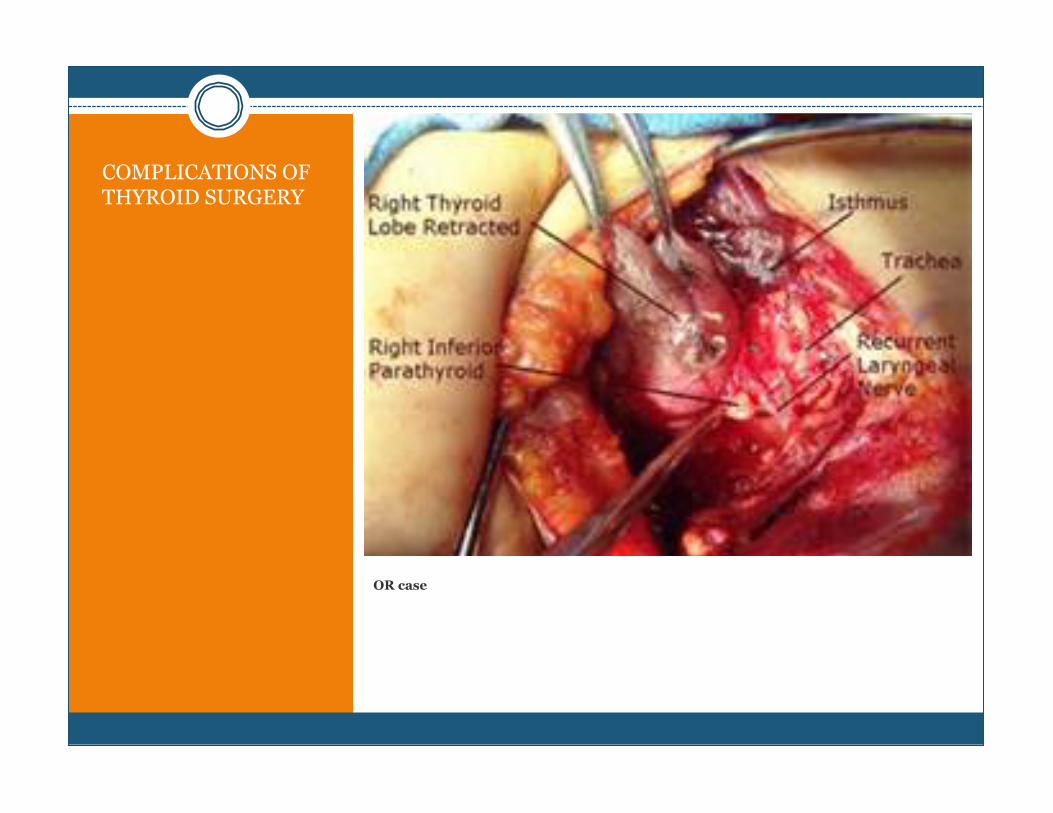
OR case
COMPLICATIONS OF THYROID SURGERY
Surgery and TC
Low MORTALITY
Thyroid cancers LOW Mortality!! Rod Stewart, Julie Andrews, Joe Piscopo
Always exceptions to the rules : Roger Ebert, Supreme Court Justice
Reinquist
Should be LOW MORBIDITY too!!
IF surgery is required, always refer to someone who does at least > 50 / year
NO drains!!
NO RR tracks!!
Dermabond is ulgy on the neck, and often opens a bit…
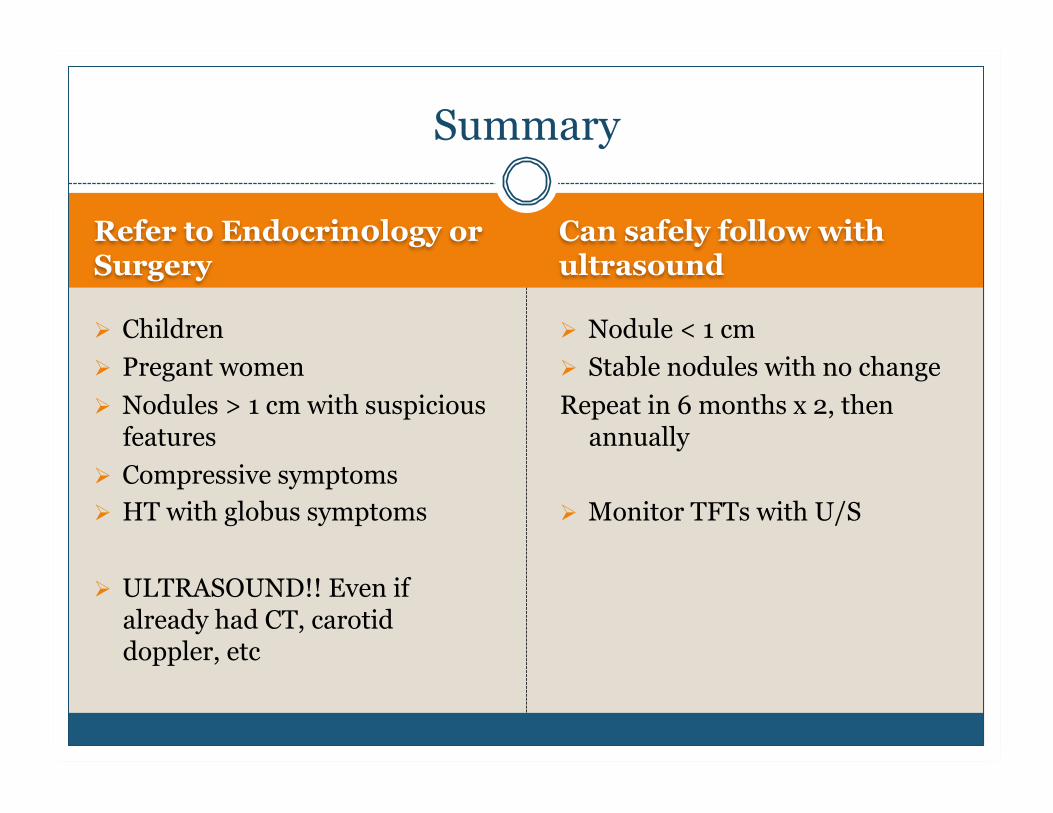
Summary
Refer to Endocrin0logy or Surgery
Children Pregant women Nodules > 1 cm with suspicious
features Compressive symptoms HT with globus symptoms
ULTRASOUND!! Even if already had CT, carotid doppler, etc
Can safely follow with ultrasound
Nodule < 1 cm Stable nodules with no change Repeat in 6 months x 2, then
annually
Monitor TFTs with U/S
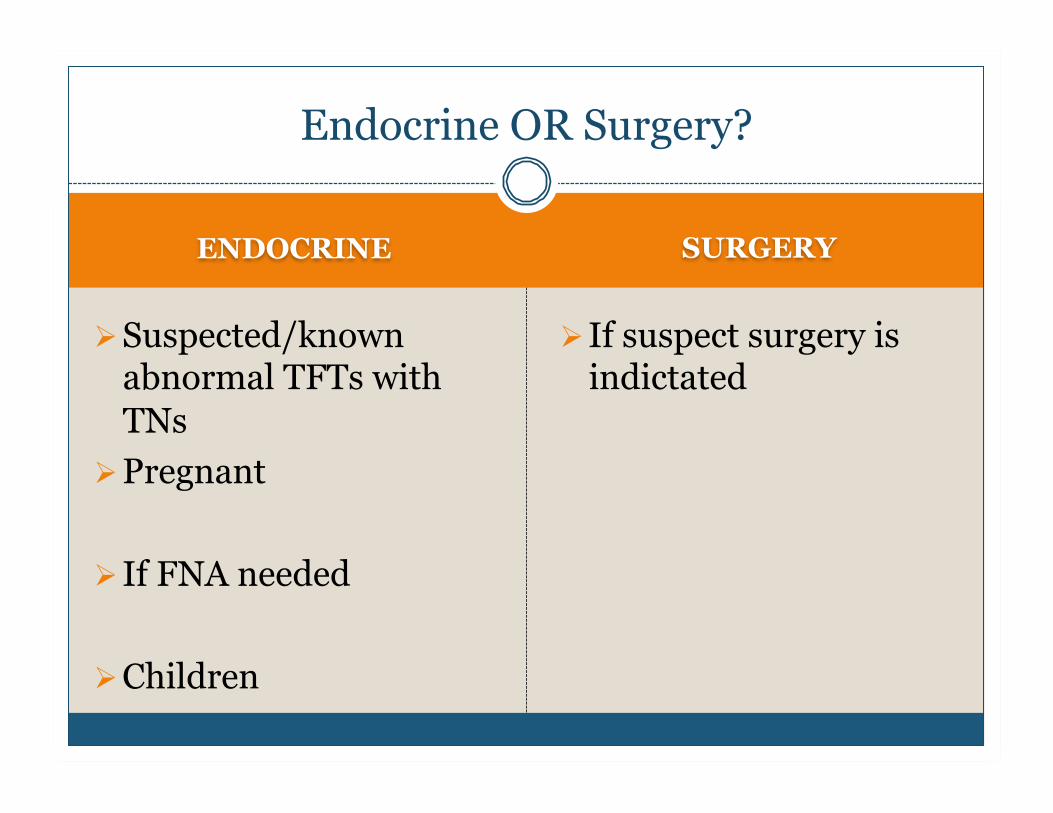
ENDOCRINE SURGERY
Suspected/known abnormal TFTs with TNs
Pregnant
If FNA needed
Children
If suspect surgery is indictated
Endocrine OR Surgery?
Q U E S T I O N S ?
Thank You