Embed Size (px)
Citation preview

THYROID PATHOLOGYTHYROID PATHOLOGY

Thyroid glandThyroid gland
Normal anatomyNormal anatomy
Congenital abnormalitiesCongenital abnormalities
ThyroiditisThyroiditis
HyperplasiaHyperplasia
TumorsTumors

THYROID-ANATOMY THYROID-ANATOMY Butterfly-two lateral lobes-isthmusButterfly-two lateral lobes-isthmus15-20 g15-20 gA thin fibrous capsuleA thin fibrous capsuleRed-brownRed-brownFollicleFollicleRound oval-single layer of epithelial cells Round oval-single layer of epithelial cells (Flattened-cuboidal-columnar)-on basement (Flattened-cuboidal-columnar)-on basement membranemembraneC-cells-NE cells-calcitoninC-cells-NE cells-calcitoninLumen of the follicle-kolloidLumen of the follicle-kolloid




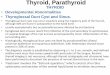
Homeostasis in the hypothalamus-pituitary-thyroid axis and mechanism of action of thyroid hormones. Secretion of thyroid hormones (T3 Homeostasis in the hypothalamus-pituitary-thyroid axis and mechanism of action of thyroid hormones. Secretion of thyroid hormones (T3 and T4) is controlled by trophic factors secreted by both the hypothalamus and the anterior pituitary. Decreased levels of T3 and T4 and T4) is controlled by trophic factors secreted by both the hypothalamus and the anterior pituitary. Decreased levels of T3 and T4
stimulate the release of thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormone (TSH) from the stimulate the release of thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormone (TSH) from the anterior pituitary, causing T3 and T4 levels to rise. Elevated T3 and T4 levels, in turn, suppress the secretion of both TRH and TSH. This anterior pituitary, causing T3 and T4 levels to rise. Elevated T3 and T4 levels, in turn, suppress the secretion of both TRH and TSH. This
relationship is termed a negative-feedback loop. TSH binds to the TSH receptor on the thyroid follicular epithelium, which causes relationship is termed a negative-feedback loop. TSH binds to the TSH receptor on the thyroid follicular epithelium, which causes activation of G proteins, and cyclic AMP (cAMP)-mediated synthesis and release of thyroid hormones (T3 and T4). In the periphery, T3 activation of G proteins, and cyclic AMP (cAMP)-mediated synthesis and release of thyroid hormones (T3 and T4). In the periphery, T3
and T4 interact with the thyroid hormone receptor (TR) to form a hormone-receptor complex that translocates to the nucleus and binds to and T4 interact with the thyroid hormone receptor (TR) to form a hormone-receptor complex that translocates to the nucleus and binds to so-called thyroid response elements (TREs) on target genes initiating transcription.so-called thyroid response elements (TREs) on target genes initiating transcription.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

Congenital abnormalitiesCongenital abnormalitiesThyroglossal duct anomaliesThyroglossal duct anomaliesLocalized-persistence of the throglossal ductLocalized-persistence of the throglossal duct
Thyroglossal duct cystThyroglossal duct cyst
Midline of the neckMidline of the neck
Mic:cyst: Pseudostratified-squamous epiteliumMic:cyst: Pseudostratified-squamous epitelium
Heterotopic thyroid tissueHeterotopic thyroid tissueTongue,sublingual,lingual,prelaringeal,substernalTongue,sublingual,lingual,prelaringeal,substernal

ThyroiditisThyroiditis
Acute thyroiditisAcute thyroiditis
Granulomatous (de Ouervain’s) Granulomatous (de Ouervain’s) ThyroditisThyroditis
Other granulomatous inflammationsOther granulomatous inflammations
Autoimmune (lymphocytic and Autoimmune (lymphocytic and Hashimoto’s) thyroiditisHashimoto’s) thyroiditis
Riedel’s Thyroiditis Riedel’s Thyroiditis

Acute thyroiditisAcute thyroiditisInfectious nature-pharyngitis,tonsillitisInfectious nature-pharyngitis,tonsillitis
St. Haemolyticus, Staph aureus, St. Haemolyticus, Staph aureus, PneumoccusPneumoccus
Mic:neutrophilic infiltration,tissue necrosisMic:neutrophilic infiltration,tissue necrosis

Granulomatous(de Ouervain’s) Granulomatous(de Ouervain’s) ThyroditisThyroditis
Ages:Ages:3030-- 50 50 ,F/M:,F/M:3:1 to 5:13:1 to 5:1 Clinical CourseClinical Course
The presentation of subacute thyroiditis The presentation of subacute thyroiditis may be sudden or gradual. may be sudden or gradual. It is characterized by pain in the neck, It is characterized by pain in the neck, which may radiate to the upper neck, jaw, which may radiate to the upper neck, jaw, throat, or ears, particularly when throat, or ears, particularly when swallowingswallowingNearly all patients have high serum T4 Nearly all patients have high serum T4 and T3 levels and low serum TSH levels.and T3 levels and low serum TSH levels.

PathogenesisPathogenesis
Subacute thyroiditisSubacute thyroiditis- - viral infectionviral infection or a postviral or a postviral inflammatory processinflammatory process-- a history of an upper a history of an upper respiratory infection respiratory infection
AA viral infection that provides an antigen, either viral infection that provides an antigen, either viral or a thyroid antigen that is released viral or a thyroid antigen that is released secondary to virus-induced host tissue damage. secondary to virus-induced host tissue damage. This antigen stimulates This antigen stimulates cytotoxic T lymphocytescytotoxic T lymphocytes, , which then damage which then damage thyroid follicular cells. thyroid follicular cells.

MorphologyMorphology The gland may be unilaterally or bilaterally The gland may be unilaterally or bilaterally enlarged and firm, with an intact capsule.enlarged and firm, with an intact capsule.On cut section, the involved areas are firm and On cut section, the involved areas are firm and yellow-white and stand out from the more yellow-white and stand out from the more rubbery, normal brown thyroid substance. rubbery, normal brown thyroid substance.
Histologically.Histologically. EarlyEarly in the active inflammatory phase, scattered in the active inflammatory phase, scattered folliclesfollicles-- replaced by neutrophils forming replaced by neutrophils forming microabscesses.microabscesses.Later, Later, aggregations of lymphocytes, histiocytes, aggregations of lymphocytes, histiocytes, and plasma cells about collapsed and damaged and plasma cells about collapsed and damaged thyroid follicles. thyroid follicles. Multinucleate giant cellsMultinucleate giant cells enclose naked pools enclose naked pools or fragments of colloid , hence the designation or fragments of colloid , hence the designation granulomatous thyroiditisgranulomatous thyroiditis..

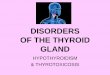
Subacute thyroiditis. The thyroid parenchyma contains a chronic inflammatory infiltrate with a
multinucleate giant cell (above left) and a colloid follicle (bottom right).Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier


Other granulomatous Other granulomatous inflammationsinflammations
Palpation thyroiditisPalpation thyroiditis
TuberculosisTuberculosis
SarcoidosisSarcoidosis
MycosesMycoses
Postoperattive necrotizing granulomasPostoperattive necrotizing granulomas

Autoimmune (lymphocytic and Hashimoto’s) Autoimmune (lymphocytic and Hashimoto’s) thyroiditisthyroiditis
Some authors use terms lymphocytic and Some authors use terms lymphocytic and Hashimoto thyroiditis synonymouslyHashimoto thyroiditis synonymously
Another autoimmune -Graves’ diseaseAnother autoimmune -Graves’ disease
Mechanism: Humoral and cellular natureMechanism: Humoral and cellular nature
Circulating autoab-TG-follicular cell Ag-TSH Circulating autoab-TG-follicular cell Ag-TSH receptorreceptor
Follicle epithelial cell- agFollicle epithelial cell- ag
Morphological common finding autoimmune Morphological common finding autoimmune thyroiditis: extensive lymphocytic infiltration with thyroiditis: extensive lymphocytic infiltration with gland associated-germinal center formation.gland associated-germinal center formation.

Lymphocytic thyroiditisLymphocytic thyroiditisChildrenChildren
Juvenil form lymphocytic thyroiditisJuvenil form lymphocytic thyroiditis
Silent-painless thyroiditis with hyperthyroidism Silent-painless thyroiditis with hyperthyroidism
Grossly:Grossly: Diffusely enlarged-nodular, white, Diffusely enlarged-nodular, white, nodular cut surface.nodular cut surface.
Mic: lymphocytic nodules with germinal Mic: lymphocytic nodules with germinal centers,follicles centers,follicles

Hashimoto’s thyroiditisHashimoto’s thyroiditisHashimoto thyroiditis (or chronic Hashimoto thyroiditis (or chronic lymphocytic thyroiditis) is the most lymphocytic thyroiditis) is the most common cause of hypothyroidism in areas common cause of hypothyroidism in areas of the world in 45 and 65 years of age of the world in 45 and 65 years of age
A female predominance of 10:1 to 20:1A female predominance of 10:1 to 20:1
Epidemiologic studies have demonstrated Epidemiologic studies have demonstrated a significant a significant genetic componentgenetic component to to Hashimoto thyroiditisHashimoto thyroiditis
Specifically the HLA-DR3 and HLA-DR5 Specifically the HLA-DR3 and HLA-DR5 alleles, are linked to Hashimoto thyroiditisalleles, are linked to Hashimoto thyroiditis

PathogenesisPathogenesis Hashimoto thyroiditis is an autoimmune Hashimoto thyroiditis is an autoimmune disease.disease.
The overriding feature of Hashimoto The overriding feature of Hashimoto thyroiditis is progressive depletion of thyroiditis is progressive depletion of thyroid epithelial cells (thyrocytes)thyroid epithelial cells (thyrocytes)--ggradually replaced by mononuclear cell radually replaced by mononuclear cell infiltration and fibrosis.infiltration and fibrosis.
Multiple immunologic mechanisms may Multiple immunologic mechanisms may contribute to the death of thyrocytes contribute to the death of thyrocytes

CD8CD8+ + cytotoxic T cell-mediated cell deathcytotoxic T cell-mediated cell death
Cytokine-mediated cell deathCytokine-mediated cell death
Binding of antithyroid antibodies (anti-TSH Binding of antithyroid antibodies (anti-TSH receptor antibodies, antithyroglobulin, and receptor antibodies, antithyroglobulin, and antithyroid peroxidase antibodies) followed antithyroid peroxidase antibodies) followed by antibody-dependent cell-mediated by antibody-dependent cell-mediated cytotoxicity cytotoxicity

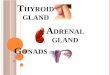
Pathogenesis of Hashimoto thyroiditis. Three proposed models for mechanism of thyrocyte destruction in Hashimoto disease. Sensitization of autoreactive CD4+ T
cells to thyroid antigens appears to be the initiating event for all three mechanisms of thyroid cell death.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

MorphologyMorphology
The thyroid is often diffusely enlargedThe thyroid is often diffusely enlarged The capsule is intact, and the gland is well The capsule is intact, and the gland is well demarcated from adjacent structures. The cut demarcated from adjacent structures. The cut surface is pale, yellow-tan, firm, and somewhat surface is pale, yellow-tan, firm, and somewhat nodular.nodular. MicMic::extensive infiltration of the parenchyma by a extensive infiltration of the parenchyma by a mononuclear inflammatory infiltratemononuclear inflammatory infiltrate containing small lymphocytes, plasma cells, and containing small lymphocytes, plasma cells, and well-developed well-developed germinal centersgerminal centers The thyroid follicles are atrophic The thyroid follicles are atrophic -- lined in many lined in many areas by epithelial cells distinguished by the areas by epithelial cells distinguished by the presence of abundant eosinophilic, granular presence of abundant eosinophilic, granular cytoplasm, termed cytoplasm, termed HHuurthlerthle cells cells-- metaplastic metaplastic cellscells. .


Hashimoto thyroiditis. The thyroid parenchyma contains a dense lymphocytic infiltrate with germinal centers. Residual thyroid follicles lined by deeply eosinophilic
Hurthle cells are also seen.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier


Clinical CourseClinical Course HHypothyroidism develops gradually.ypothyroidism develops gradually.IIt may be preceded by transient thyrotoxicosis t may be preceded by transient thyrotoxicosis caused by disruption of thyroid follicles, with caused by disruption of thyroid follicles, with secondary release of thyroid hormones secondary release of thyroid hormones ("hashitoxicosis"). ("hashitoxicosis"). Patients with Hashimoto thyroiditis are at Patients with Hashimoto thyroiditis are at increased risk for developing other concomitant increased risk for developing other concomitant autoimmune diseases, both endocrine (type 1 autoimmune diseases, both endocrine (type 1 diabetes, autoimmune adrenalitis), and diabetes, autoimmune adrenalitis), and nonendocrine (systemic lupus erythematosus, nonendocrine (systemic lupus erythematosus, myasthenia gravis, and Sjögren syndromemyasthenia gravis, and Sjögren syndrome
**IIncreased risk for the development of ncreased risk for the development of B-cell non-Hodgkin lymphomas. B-cell non-Hodgkin lymphomas.

SUBACUTE LYMPHOCYTIC (PAINLESS) SUBACUTE LYMPHOCYTIC (PAINLESS)
THYROIDITISTHYROIDITIS Subacute lymphocytic thyroiditisSubacute lymphocytic thyroiditis, which is also , which is also referred to as referred to as painless thyroiditis or silent painless thyroiditis or silent thyroiditisthyroiditis, is an uncommon cause of , is an uncommon cause of hyperthyroidism.hyperthyroidism.MMiddle-aged adults and is more common in iddle-aged adults and is more common in women, especially during the postpartum period women, especially during the postpartum period ((postpartum thyroiditispostpartum thyroiditis), than in men), than in men The pathogenesis of this disorder is unknown. The pathogenesis of this disorder is unknown. An autoimmune basis has been suggested An autoimmune basis has been suggested because some patients have elevated levels of because some patients have elevated levels of antibodies to thyroglobulin and thyroid antibodies to thyroglobulin and thyroid peroxidase or a family history of thyroid peroxidase or a family history of thyroid autoimmune diseaseautoimmune disease

MorphologyMorphology
MMild symmetric enlargement, the thyroid ild symmetric enlargement, the thyroid appears normal on gross inspection. appears normal on gross inspection.
The most specific histologic features The most specific histologic features consist of lymphocytic infiltration with consist of lymphocytic infiltration with hyperplastic germinal centers within the hyperplastic germinal centers within the thyroid parenchyma and patch disruption thyroid parenchyma and patch disruption and collapse of thyroid follicles. and collapse of thyroid follicles.

Clinical CourseClinical Course
The principal clinical manifestation of The principal clinical manifestation of painless thyroiditis is hyperthyroidism. painless thyroiditis is hyperthyroidism. Symptoms usually develop over 1 to 2 Symptoms usually develop over 1 to 2 weeks and last from 2 to 8 weeks weeks and last from 2 to 8 weeks
Laboratory findings during periods of Laboratory findings during periods of thyrotoxicosis include thyrotoxicosis include elevated levels of T4 elevated levels of T4 and T3and T3 and and depressed levels of TSHdepressed levels of TSH. .

Riedel thyroiditisRiedel thyroiditisAA rare disorder of unknown etiology rare disorder of unknown etiology characterized by extensive fibrosis involving the characterized by extensive fibrosis involving the thyroid and contiguous neck structures. thyroid and contiguous neck structures.
The presence of a hard and fixed thyroid mass The presence of a hard and fixed thyroid mass clinically simulates a thyroid carcinoma. clinically simulates a thyroid carcinoma.
Grossly: asymmetric-stony hardGrossly: asymmetric-stony hard
Mic:Fibrous tissue involves glandMic:Fibrous tissue involves gland
Inflammatory fibrosclerosis-idiopathic disordersInflammatory fibrosclerosis-idiopathic disorders

PalpationPalpation thyroiditisthyroiditis, caused by vigorous , caused by vigorous clinical palpation of the thyroid gland, clinical palpation of the thyroid gland, results in multifocal follicular disruption results in multifocal follicular disruption associated with chronic inflammatory cells associated with chronic inflammatory cells and occasional giant cell formationand occasional giant cell formation. .
Unlike De Quervain thyroiditis, Unlike De Quervain thyroiditis, abnormalities of thyroid function are not abnormalities of thyroid function are not presenpresent t

HyperplasiaHyperplasia
Dyshormonogenetic goiterDyshormonogenetic goiter
Graves’ Disease(Diffuse toxic goiter)Graves’ Disease(Diffuse toxic goiter)
Diffuse nontoxic goiterDiffuse nontoxic goiter
Multinodular-goiter-Nodular Multinodular-goiter-Nodular hyperplasiahyperplasia

NameName MechanismMechanism PathologyPathology Functional Functional statusstatus
DyshormonoDyshormonogenetic genetic goitergoiter
GeneticallyGenetically Nodular or Nodular or less diffuse less diffuse hyperplasiahyperplasia
HypotyhroidHypotyhroid
Graves’ Graves’ diseasedisease
AutoimmuneAutoimmune Diffuse Diffuse hyperplasiahyperplasia
HyperthyroidHyperthyroid
Nodular –Nodular –difuse difuse hyperplasiahyperplasia
-Endemic -Endemic goitergoiter
Iodine Iodine deficiencydeficiency
Nodular Nodular hyperplasiahyperplasia
Usually Usually eutyroid; eutyroid; sometimes sometimes hypothyroidhypothyroid
Sporadic Sporadic goitergoiter
UnknownUnknown Nodular Nodular hyperplasiahyperplasia
Usually euthyroid: Usually euthyroid: sometimes hyper sometimes hyper or hypoor hypo

Dyshormonogenetic goiterDyshormonogenetic goiter
Enzyme defects in hormone synthesisEnzyme defects in hormone synthesis
Genetic mutationsGenetic mutations
Grossly:enlarged-multinodularGrossly:enlarged-multinodular
Mic:Hyperplastic follicles are lined by Mic:Hyperplastic follicles are lined by marked nuclear pleomorphism, fibrosis.marked nuclear pleomorphism, fibrosis.

Graves’ DiseaseGraves’ Disease(Diffuse toxic goiter)(Diffuse toxic goiter)
Graves disease is the most common cause of Graves disease is the most common cause of endogenous hyperthyroidism.endogenous hyperthyroidism. It is characterized It is characterized by a by a triadtriad of clinical findings: of clinical findings:
HyperthyroidismHyperthyroidism owing to hyperfunctional, owing to hyperfunctional, diffuse enlargement of the thyroid diffuse enlargement of the thyroid
Infiltrative Infiltrative ophthalmopathyophthalmopathy with resultant with resultant exophthalmos exophthalmos
Localized, infiltrative Localized, infiltrative dermopathydermopathy,, sometimes sometimes called called pretibial myxedemapretibial myxedema,, which is present in a which is present in a minority of patientsminority of patients

Ages Ages of 20 and 40, of 20 and 40, F/M:7/1F/M:7/1HLA-B8 and -DR3HLA-B8 and -DR3
PathogenesisPathogenesis Graves disease is an autoimmune disorderGraves disease is an autoimmune disorder in which a in which a variety of antibodies may be present in the serum, variety of antibodies may be present in the serum, including antibodies to the TSH receptor, thyroid including antibodies to the TSH receptor, thyroid peroxisomes, and thyroglobulin.peroxisomes, and thyroglobulin. Thyroid-stimulating immunoglobulin (TSI):Thyroid-stimulating immunoglobulin (TSI): Almost 50 Almost 50 years ago, serum from patients with Graves disease was years ago, serum from patients with Graves disease was found to contain a long-acting thyroid stimulator (LATS)found to contain a long-acting thyroid stimulator (LATS) Thyroid growth-stimulating immunoglobulinsThyroid growth-stimulating immunoglobulins ((TGITGI):): TSH-binding inhibitor immunoglobulinsTSH-binding inhibitor immunoglobulins ( (TBIITBII): These anti-): These anti-TSH receptor antibodies prevent TSH from binding TSH receptor antibodies prevent TSH from binding normally to its receptor on thyroid epithelial cellsnormally to its receptor on thyroid epithelial cells resulting resulting in the stimulation of thyroid epithelial cell activity.in the stimulation of thyroid epithelial cell activity.

MorphologyMorphology
SSymmetrically enlarged because of ymmetrically enlarged because of diffuse hypertrophy diffuse hypertrophy and hyperplasiaand hyperplasia of thyroid follicular epithelial cells. of thyroid follicular epithelial cells.Cut surface:Cut surface: meaty appearance resembling normal meaty appearance resembling normal muscle. muscle. Histologically, too many cells. The follicular epithelial Histologically, too many cells. The follicular epithelial cells in untreated cases are tall and more crowded than cells in untreated cases are tall and more crowded than usual. usual. TThe formation of small papillae,he formation of small papillae,Lymphoid infiltrates, consisting predominantly of T cells, Lymphoid infiltrates, consisting predominantly of T cells, with fewer B cells and mature plasma cells, are present with fewer B cells and mature plasma cells, are present throughout the interstitium; germinal centers are throughout the interstitium; germinal centers are commoncommon

Diffusely hyperplastic thyroid in a case of Graves disease. The follicles are lined by tall, columnar epithelium. The crowded, enlarged epithelial cells
project into the lumens of the follicles. These cells actively resorb the colloid in the centers of the follicles, resulting in the scalloped appearance of the
edges of the colloid.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier


Clinical CourseClinical CourseThe clinical findings in Graves disease The clinical findings in Graves disease include changes referable to include changes referable to thyrotoxicosisthyrotoxicosis as well as those associated uniquely with as well as those associated uniquely with Graves disease: Graves disease: diffuse hyperplasia of the diffuse hyperplasia of the thyroidthyroid,, ophthalmopathyophthalmopathy, and , and dermopathydermopathy. . Laboratory findingsLaboratory findings::EElevated free T4 and T3levated free T4 and T3 levels levelsDDepressed TSHepressed TSH levels. levels. RRadioactive iodine uptake is increased, adioactive iodine uptake is increased, and radioiodine scans show a diffuse and radioiodine scans show a diffuse uptake of iodine.uptake of iodine.

DDiffuse non-toxiciffuse non-toxic Goiter Goiter
This disorder occurs in both an endemic and a This disorder occurs in both an endemic and a sporadic distribution.sporadic distribution.
Endemic goiterEndemic goiter - -occurs in geographic areas where occurs in geographic areas where the soil, water, and food supply contain only low the soil, water, and food supply contain only low levels of iodine. levels of iodine.
The lack of iodine leads to decreased synthesis The lack of iodine leads to decreased synthesis of thyroid hormone and a compensatory of thyroid hormone and a compensatory increase in TSH, leading to follicular cell increase in TSH, leading to follicular cell hypertrophy and hyperplasia and goitrous hypertrophy and hyperplasia and goitrous enlargementenlargement-diffuse or nodular colloid goiter.-diffuse or nodular colloid goiter.

Sporadic goiterSporadic goiter
OOccurs less frequently than does endemic ccurs less frequently than does endemic goiter.goiter.
There is a striking female preponderance and a There is a striking female preponderance and a peak incidence at puberty or in young adult life. peak incidence at puberty or in young adult life.
Mild dietary deficiency of iodineMild dietary deficiency of iodine
Slight impairment of hormone synthesisSlight impairment of hormone synthesis
Increased iodide clearance by kidneysIncreased iodide clearance by kidneys

MorphologyMorphology Two phases can be identified in the Two phases can be identified in the evolution of diffuse non-toxic goiter: evolution of diffuse non-toxic goiter: the the hyperplastic phasehyperplastic phase and the phase of and the phase of colloid involution.colloid involution. D Diffusely and iffusely and symmetrically enlarged, although the symmetrically enlarged, although the increase is usually modest, and the gland increase is usually modest, and the gland rarely exceeds 100 to 150 gm. rarely exceeds 100 to 150 gm. The follicles are lined by crowded columnar The follicles are lined by crowded columnar cells, which may pile up and form cells, which may pile up and form projections similar to those seen in Graves projections similar to those seen in Graves disease. The accumulation is not uniform disease. The accumulation is not uniform throughout the gland, and some follicles are throughout the gland, and some follicles are hugely distended, whereas others remain hugely distended, whereas others remain small. small.

If dietary iodine subsequently increases or If dietary iodine subsequently increases or if the demand for thyroid hormone if the demand for thyroid hormone decreases, the stimulated follicular decreases, the stimulated follicular epithelium involutes to form an enlarged, epithelium involutes to form an enlarged, colloid-rich gland colloid-rich gland (colloid goiter).(colloid goiter). In these In these cases, the cut surface of the thyroid is cases, the cut surface of the thyroid is usually brown, somewhat glassy, and usually brown, somewhat glassy, and translucent. translucent. Histologically, the follicular epithelium is Histologically, the follicular epithelium is flattened and cuboidal, and colloid is flattened and cuboidal, and colloid is abundant during periods of involution.abundant during periods of involution.

Clinical CourseClinical Course
The vast majority of patients with simple The vast majority of patients with simple goiters are clinically euthyroid. goiters are clinically euthyroid.
TThe clinical manifestations are primarily he clinical manifestations are primarily related to related to mass effectsmass effects from the enlarged from the enlarged thyroid gland thyroid gland
SSerum T3 and T4 levels are normal, the erum T3 and T4 levels are normal, the serum TSH is usually elevated or at the serum TSH is usually elevated or at the upper range of normalupper range of normal

MULTINODULAR GOITERMULTINODULAR GOITER ––Nodular hyperplasiaNodular hyperplasia
RRecurrent episodes of hyperplasia and involution ecurrent episodes of hyperplasia and involution combine to produce a more irregular combine to produce a more irregular enlargement of the thyroid, termed enlargement of the thyroid, termed multinodular multinodular goitergoiter..-Nodular hyperplasia-Nodular hyperplasia
They may be nontoxic or may induce They may be nontoxic or may induce thyrotoxicosis (toxic multinodular goiter).thyrotoxicosis (toxic multinodular goiter).
Multinodular goiters produce the most extreme Multinodular goiters produce the most extreme thyroid enlargements thyroid enlargements -- mistaken for neoplastic mistaken for neoplastic involvementinvolvement

MMultinodal goiters may arise because of ultinodal goiters may arise because of variations among follicular cells in responses to variations among follicular cells in responses to external stimuli, such as trophic hormones.external stimuli, such as trophic hormones.
If some cells in a follicle have a growth If some cells in a follicle have a growth advantage, perhaps because of intrinsic genetic advantage, perhaps because of intrinsic genetic abnormalities similar to those abnormalities similar to those that give rise to that give rise to adenomas,adenomas, those cells will develop into clones of those cells will develop into clones of proliferating cells. proliferating cells.
This may result in the formation of a nodule This may result in the formation of a nodule whose continued growth could even be whose continued growth could even be autonomous,autonomous, without the external stimulus. without the external stimulus.

MorphologyMorphology Multinodular goiters are multilobulated, Multinodular goiters are multilobulated, asymmetrically enlarged glands that can achieve asymmetrically enlarged glands that can achieve a weight of more than 2000 gm.a weight of more than 2000 gm.The pattern of enlargement is quite The pattern of enlargement is quite unpredictable and may involve one lobe far unpredictable and may involve one lobe far more than the other, producing lateral pressure more than the other, producing lateral pressure on midline structures, such as the trachea and on midline structures, such as the trachea and esophagus. esophagus. TThe goiter grows behind the sternum and he goiter grows behind the sternum and clavicles to produce the so-called clavicles to produce the so-called intrathoracicintrathoracic or or plunging goiter.plunging goiter.



Nodular goiter. The gland is coarsely nodular and contains areas of fibrosis and cystic change.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier


OOne nodule may so stand out as to impart the ne nodule may so stand out as to impart the clinical appearance of a solitary nodule.clinical appearance of a solitary nodule.On cut section, irregular nodules containing On cut section, irregular nodules containing variable amounts of brown, gelatinous colloid variable amounts of brown, gelatinous colloid are present.are present.Regressive changesRegressive changes occur frequently, occur frequently, particularly in older lesions, and include areas of particularly in older lesions, and include areas of hemorrhage, fibrosis, calcification, and cystic hemorrhage, fibrosis, calcification, and cystic change.change. The microscopic appearance includes colloid-The microscopic appearance includes colloid-rich follicles lined by flattened, inactive rich follicles lined by flattened, inactive epithelium and areas of follicular epithelial epithelium and areas of follicular epithelial hypertrophy and hyperplasia, accompanied by hypertrophy and hyperplasia, accompanied by the degenerative changes noted previously.the degenerative changes noted previously.

Clinical CourseClinical Course The dominant clinical features of goiter are those The dominant clinical features of goiter are those caused by the caused by the mass effectsmass effects of the enlarged gland. of the enlarged gland.CCosmetic effects of a large neck mass, goiters osmetic effects of a large neck mass, goiters may cause airway obstruction, dysphagia, and may cause airway obstruction, dysphagia, and compression of large vessels in the neck and compression of large vessels in the neck and upper thorax.upper thorax. Most patients are Most patients are euthyroid,euthyroid, but in a substantial but in a substantial minority of patients, a hyperfunctioning nodule may minority of patients, a hyperfunctioning nodule may develop within a long-standing goiter, resulting in develop within a long-standing goiter, resulting in hyperthyroidismhyperthyroidism (toxic multinodular goiter). (toxic multinodular goiter). Hyperfunctioning nodules concentrate radioiodine Hyperfunctioning nodules concentrate radioiodine and appear "hot.“and appear "hot.“Goiters are also of clinical significance because of Goiters are also of clinical significance because of their ability to mask or to mimic neoplastic their ability to mask or to mimic neoplastic diseases arising in the thyroiddiseases arising in the thyroid

Thyroid TumorsThyroid TumorsEpithelial Tumors-specific typesEpithelial Tumors-specific typesA-Follicular adenomaA-Follicular adenoma-Hyalinizing trabecular adenoma and related lesions-Hyalinizing trabecular adenoma and related lesionsB-Papillary carcinomaB-Papillary carcinomaC-Follicular carcinomaC-Follicular carcinomaD-Clear cell tumorsD-Clear cell tumorsE-Squmaous cell, mucinous, and related tumorsE-Squmaous cell, mucinous, and related tumorsF-Poorly differentiated carcinomaF-Poorly differentiated carcinomaG-Undiferentiated carcinomaG-Undiferentiated carcinomaH-Medullary carcinoma and related NE lesionsH-Medullary carcinoma and related NE lesionsLymphoid tumors and tumorlike conditionsLymphoid tumors and tumorlike conditionsMesencymal tumorsMesencymal tumorsOther primary tumors and tumorlike conditionsOther primary tumors and tumorlike conditionsMetastatic tumorsMetastatic tumors

Neoplasms of the ThyroidNeoplasms of the Thyroid Several clinical criteria might provide a clue to the nature Several clinical criteria might provide a clue to the nature of a given thyroid nodule: of a given thyroid nodule: 1-1-Solitary nodules,Solitary nodules, in general, are more likely to be in general, are more likely to be neoplastic than are multiple nodules. neoplastic than are multiple nodules. 2-2-Nodules in younger patientsNodules in younger patients are more likely to be are more likely to be neoplastic than are those in older patients. neoplastic than are those in older patients. 3-3-Nodules in malesNodules in males are more likely to be neoplastic than are more likely to be neoplastic than are those in females. are those in females. 4-4-A history of A history of radiationradiation treatment to the head and neck treatment to the head and neck region is associated with an increased incidence of region is associated with an increased incidence of thyroid malignancy. thyroid malignancy. 5-5-Nodules that take up radioactive iodine in imaging Nodules that take up radioactive iodine in imaging studies (studies (hot noduleshot nodules) are more likely to be benign than ) are more likely to be benign than malignantmalignant

ADENOMASADENOMAS Adenomas of the thyroid are typically discrete, Adenomas of the thyroid are typically discrete, solitary massessolitary massesMMost of these benign tumors are nonfunctionalost of these benign tumors are nonfunctional Simple colloid adenomas (macrofollicular Simple colloid adenomas (macrofollicular adenomas), a common form, resemble normal adenomas), a common form, resemble normal thyroid tissue; thyroid tissue; OOthers recapitulate stages in the embryogenesis thers recapitulate stages in the embryogenesis of the normal thyroid (fetal or microfollicular, of the normal thyroid (fetal or microfollicular, embryonal or trabecular). embryonal or trabecular). Hormone production in functional adenomas Hormone production in functional adenomas ("toxic adenomas") occurs independent of TSH ("toxic adenomas") occurs independent of TSH stimulation and represents another example of stimulation and represents another example of thyroid autonomythyroid autonomy, analogous to toxic , analogous to toxic multinodular goiters. multinodular goiters.

Pathogenesis.Pathogenesis.The The TSH receptor signaling pathwayTSH receptor signaling pathway plays an plays an important role in the pathogenesis of toxic important role in the pathogenesis of toxic adenomas.adenomas.Activating ("gain of function") somatic mutations Activating ("gain of function") somatic mutations in one of two components of this signaling in one of two components of this signaling systemsystem-most often the TSH receptor itself or the -most often the TSH receptor itself or the α-subunit of Gs-cause chronic overproduction of α-subunit of Gs-cause chronic overproduction of cAMP, generating cells that acquire a growth cAMP, generating cells that acquire a growth advantage advantage This results in clonal expansion of follicular This results in clonal expansion of follicular epithelial cells that can autonomously produce epithelial cells that can autonomously produce thyroid hormone and cause symptoms of thyroid thyroid hormone and cause symptoms of thyroid excessexcess

MorphologyMorphology The typical thyroid adenoma is a solitary, The typical thyroid adenoma is a solitary, spherical, encapsulated lesion that is well spherical, encapsulated lesion that is well demarcated from the surrounding thyroid demarcated from the surrounding thyroid parenchyma. parenchyma. Follicular adenomas average about 3 cm in Follicular adenomas average about 3 cm in diameter, but some are smaller and others are diameter, but some are smaller and others are much larger (up to 10 cm in diameter). much larger (up to 10 cm in diameter). The neoplastic cells are demarcated from the The neoplastic cells are demarcated from the adjacent parenchyma by a well-defined, adjacent parenchyma by a well-defined, intact intact capsulecapsule. . These features are important in These features are important in making the distinction from multinodular making the distinction from multinodular goitersgoiters, , Areas of hemorrhage, fibrosis, calcification, and Areas of hemorrhage, fibrosis, calcification, and cystic change, similar to those encountered in cystic change, similar to those encountered in multinodular goiters, are common in follicular multinodular goiters, are common in follicular adenomas, particularly within larger lesions.adenomas, particularly within larger lesions.

MicroscopicallyMicroscopicallyThe follicular growth pattern within the The follicular growth pattern within the adenoma is usually quite distinct from the adenoma is usually quite distinct from the adjacent non-neoplastic thyroid. adjacent non-neoplastic thyroid.
The epithelial cells composing the follicular The epithelial cells composing the follicular adenoma reveal little variation in cell and adenoma reveal little variation in cell and nuclear morphology. nuclear morphology.
Mitotic figures are rare, and extensive Mitotic figures are rare, and extensive mitotic activity warrants careful mitotic activity warrants careful examination of the capsule to exclude examination of the capsule to exclude follicular carcinoma.follicular carcinoma.

Similar to endocrine tumors at other Similar to endocrine tumors at other anatomic sites, even benign follicular anatomic sites, even benign follicular adenomas may, on occasion, exhibit adenomas may, on occasion, exhibit focal nuclear pleomorphism, atypia, focal nuclear pleomorphism, atypia, and prominent nucleoli (endocrine and prominent nucleoli (endocrine atypia); this by itself does not atypia); this by itself does not constitute a feature of malignancyconstitute a feature of malignancy..

Follicular adenoma of the thyroid. A solitary, well-circumscribed nodule is seen.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier


Follicular adenoma. The photomicrograph shows well-differentiated follicles resembling normal thyroid parenchyma.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

Follicular adenoma. A high-power view showing that the tumor is composed of cells with abundant eosinophilic cytoplasm and small regular nuclei.
(Courtesy of Dr. Mary Sunday, Brigham and Women's Hospital, Boston, MA.)
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

AAtypical follicular typical follicular aadenomasdenomas::IIncreased cellularity, more extensive variation in ncreased cellularity, more extensive variation in cellular size and nuclear morphology, and even cellular size and nuclear morphology, and even mitotic activity. mitotic activity.
The hallmark of all follicular adenomas is the The hallmark of all follicular adenomas is the presence of an intact, well-formed capsule presence of an intact, well-formed capsule encircling the tumor. encircling the tumor.
Careful evaluation of the integrity of the Careful evaluation of the integrity of the capsule is therefore critical in distinguishing capsule is therefore critical in distinguishing follicular adenomas from follicular follicular adenomas from follicular carcinomascarcinomas , , which demonstrate capsular which demonstrate capsular and/or vascular invasionand/or vascular invasion

Clinical FeaturesClinical Features unilateral painless mass, unilateral painless mass, cold nodules relative to the adjacent thyroid cold nodules relative to the adjacent thyroid tissuetissue Owing to the need for evaluating capsular Owing to the need for evaluating capsular integrity, the definitive diagnosis of integrity, the definitive diagnosis of adenomas can be made only after careful adenomas can be made only after careful histologic examination of the resected histologic examination of the resected specimen.specimen.Suspected adenomas of the thyroid are Suspected adenomas of the thyroid are therefore removed surgically to exclude therefore removed surgically to exclude malignancy.malignancy.Thyroid adenomas, including atypical Thyroid adenomas, including atypical adenomas, have an excellent prognosis and adenomas, have an excellent prognosis and do not recur or metastasize.do not recur or metastasize.

OTHER BENIGN TUMORSOTHER BENIGN TUMORS
Additional benign Additional benign lesions lesions include dermoid include dermoid cysts, lipomas, hemangiomas, and cysts, lipomas, hemangiomas, and teratomas (seen mainly in infants).teratomas (seen mainly in infants).

CARCINOMASCARCINOMAS
1.5% of all cancers1.5% of all cancers(in United States)(in United States)Most cases occur in adults, although some forms, Most cases occur in adults, although some forms, particularly papillary carcinomas, may present in particularly papillary carcinomas, may present in childhood.childhood. A female predominance A female predominance The major subtypes of thyroid carcinoma: The major subtypes of thyroid carcinoma: Papillary carcinoma (75% to 85% of cases) Papillary carcinoma (75% to 85% of cases) Follicular carcinoma (10% to 20% of cases) Follicular carcinoma (10% to 20% of cases) Medullary carcinoma (5% of cases) Medullary carcinoma (5% of cases) Anaplastic carcinoma (<5% of cases)Anaplastic carcinoma (<5% of cases)

Most thyroid carcinomas are derived from Most thyroid carcinomas are derived from the follicular epithelium, except for the follicular epithelium, except for medullary carcinomas; the latter are medullary carcinomas; the latter are derived from the parafollicular or C cellsderived from the parafollicular or C cells
PathogenesisPathogenesis There are several factors, genetic and There are several factors, genetic and environmental, implicated in the environmental, implicated in the pathogenesis of thyroid cancers. pathogenesis of thyroid cancers.

PathogenesisPathogenesis GGeneticenetic
Follicular Thyroid CarcinomasFollicular Thyroid Carcinomas - -Approximately Approximately half of follicular thyroid carcinomas harbor half of follicular thyroid carcinomas harbor mutations in the mutations in the RASRAS family of oncogenes family of oncogenes ((HRASHRAS, , NRASNRAS, and , and KRASKRAS Papillary Thyroid CarcinomasPapillary Thyroid Carcinomas-- One pathway One pathway involves rearrangements of the tyrosine kinase involves rearrangements of the tyrosine kinase receptors receptors RETRET or or NTRK1NTRK1 (neurotrophic tyrosine (neurotrophic tyrosine kinase receptor 1) and another involves activating kinase receptor 1) and another involves activating mutations in the mutations in the BRAFBRAF oncogene. A third pathway oncogene. A third pathway involves involves RASRAS mutations (10% to 20% of papillary mutations (10% to 20% of papillary carcinomas), suggesting that some of these carcinomas), suggesting that some of these cancers are related to follicular adenomascancers are related to follicular adenomas

Environmental FactorsEnvironmental Factors The major risk factorThe major risk factor--ionizing radiationionizing radiation, , particularly during the first two decades of life. particularly during the first two decades of life. In the past, In the past, radiation therapyradiation therapy was liberally was liberally employed in the treatment of a number of head employed in the treatment of a number of head and neck lesions in infants and children, and neck lesions in infants and children, including reactive tonsillar enlargement, acne, including reactive tonsillar enlargement, acne, and tinea capitis.and tinea capitis.Up to 9% of peopleUp to 9% of people-t-thyroid malignancieshyroid malignancies Long-standing multinodular goiterLong-standing multinodular goiter--areas with areas with iodine deficiency-related endemic goiter have a iodine deficiency-related endemic goiter have a higher prevalence of higher prevalence of follicular carcinomasfollicular carcinomasTThyroid lymphomashyroid lymphomas may may arise from pre-existing arise from pre-existing Hashimoto thyroiditisHashimoto thyroiditis..

Papillary CarcinomaPapillary Carcinoma
Papillary carcinomas are the most Papillary carcinomas are the most common form of thyroid cancercommon form of thyroid cancer
Young-middle age adultsYoung-middle age adults. .

MorphologyMorphology
Papillary carcinomas are solitary or multifocal Papillary carcinomas are solitary or multifocal lesions. lesions. WWell-circumscribed and even encapsulated; ell-circumscribed and even encapsulated; others may infiltrate the adjacent parenchyma others may infiltrate the adjacent parenchyma with ill-defined margins.with ill-defined margins.The lesions may contain areas of fibrosis and The lesions may contain areas of fibrosis and calcification and are often cystic. calcification and are often cystic. On the cut surface, they may appear granular On the cut surface, they may appear granular and may sometimes contain grossly discernible and may sometimes contain grossly discernible papillary foci. The definitive diagnosis of papillary foci. The definitive diagnosis of papillary carcinoma can be made only after papillary carcinoma can be made only after microscopic examinationmicroscopic examination

Papillary carcinoma of the thyroid. A, The macroscopic appearance of a papillary carcinoma with grossly discernible papillary structures. This particular example
contains well-formed papillae
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier


Microscopic examinationMicroscopic examinationPapillary carcinomas can contain Papillary carcinomas can contain branching branching papillaepapillae having a fibrovascular stalk covered by a single to having a fibrovascular stalk covered by a single to multiple layers of cuboidal epithelial cells.multiple layers of cuboidal epithelial cells. The nuclei of papillary carcinoma cells contain finely The nuclei of papillary carcinoma cells contain finely dispersed chromatin, which imparts an dispersed chromatin, which imparts an optically clearoptically clear or or emptyempty appearance, giving rise to the designation appearance, giving rise to the designation ground glassground glass or or Orphan Annie eyeOrphan Annie eye nuclei. nuclei. intranuclear inclusionsintranuclear inclusions ("pseudo-inclusions") or ("pseudo-inclusions") or intranuclear grooves. intranuclear grooves.
Concentrically calcified structures termed Concentrically calcified structures termed psammoma psammoma bodiesbodies are often present within the lesion, usually within are often present within the lesion, usually within the cores of papillae.the cores of papillae.
Foci of lymphatic invasion by tumor are often present, Foci of lymphatic invasion by tumor are often present, but involvement of blood vessels is relatively uncommon, but involvement of blood vessels is relatively uncommon, particularly in smaller lesions. particularly in smaller lesions.
Metastases to adjacent cervical lymph nodes are Metastases to adjacent cervical lymph nodes are estimated to occur in up to half the cases. estimated to occur in up to half the cases.

Papillary carcinoma of the thyroid. This particular example contains well-formed papillae (B), lined by cells with characteristic empty-appearing
nuclei, sometimes termed "Orphan Annie eye" nucleiDownloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier



Papillary carcinoma of the thyroid. lined by cells with characteristic empty-appearing nuclei, sometimes termed "Orphan Annie eye" nuclei (C).
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

Papillary carcinoma of the thyroid. D, Cells obtained by fine-needle aspiration of a papillary carcinoma. Characteristic intranuclear inclusions
are visible in some of the aspirated cells.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

Clinical CourseClinical Course Most papillary carcinomas present as Most papillary carcinomas present as asymptomatic thyroid nodules, but the first asymptomatic thyroid nodules, but the first manifestation may be a mass in a cervical lymph manifestation may be a mass in a cervical lymph node.node.In a minority of patients, hematogenous In a minority of patients, hematogenous metastases are present at the time of diagnosis, metastases are present at the time of diagnosis, most commonly in the lung. most commonly in the lung. Most papillary lesions are Most papillary lesions are coldcold masses on masses on scintiscans.scintiscans.CCytologic analysis have made fine-needle ytologic analysis have made fine-needle aspiration cytology a reliable test for aspiration cytology a reliable test for distinguishing between benign and malignant distinguishing between benign and malignant nodules. nodules. The nuclear features are often nicely The nuclear features are often nicely demonstrable in aspirated specimens. demonstrable in aspirated specimens.

Follicular CarcinomaFollicular Carcinoma
TThe second most common form of thyroid he second most common form of thyroid cancer, accounting for 10% to 20% of all cancer, accounting for 10% to 20% of all thyroid cancers.thyroid cancers.
They tend to present in women, and at an They tend to present in women, and at an older age than do papillary carcinomas, older age than do papillary carcinomas, with a peak incidence in the forties and with a peak incidence in the forties and fifties. fifties.
The incidence of follicular carcinoma is The incidence of follicular carcinoma is increased in areas of dietary iodine increased in areas of dietary iodine deficiency, deficiency,

MorphologyMorphology
Follicular carcinomas are single nodules Follicular carcinomas are single nodules -- well circumscribed or widely infiltrative well circumscribed or widely infiltrative
Sharply demarcated lesions may be Sharply demarcated lesions may be exceedingly exceedingly difficult to distinguish from difficult to distinguish from follicular adenomas by gross examination.follicular adenomas by gross examination.
Degenerative changes, such as central Degenerative changes, such as central fibrosis and foci of calcification, are fibrosis and foci of calcification, are sometimes present.sometimes present.

Follicular carcinoma. Cut surface of a follicular carcinoma with substantial replacement of the lobe of the thyroid. The tumor has a
light-tan appearance and contains small foci of hemorrhage.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

MicroscopicallyMicroscopicallyMMost follicular carcinomas are composed ost follicular carcinomas are composed of fairly uniform cells forming small follicles of fairly uniform cells forming small follicles containing colloid, quite reminiscent of containing colloid, quite reminiscent of normal thyroidnormal thyroidTThe nuclei lack the features typical of he nuclei lack the features typical of papillary carcinoma, and psammoma papillary carcinoma, and psammoma bodies are not present.bodies are not present.DDistinctionistinction from from follicular adenomasfollicular adenomas requires extensive requires extensive histologic sampling of histologic sampling of the tumor-capsule-thyroid interface to the tumor-capsule-thyroid interface to exclude capsular and/or vascular invasionexclude capsular and/or vascular invasion

Capsular integrity in follicular neoplasms. Evaluating the integrity of the capsule is critical in distinguishing follicular adenomas from follicular carcinomas. In adenomas (A), a fibrous capsule, usually thin but occasionally more prominent, circumferentially
surrounds the neoplastic follicles and no capsular invasion is seen (arrowheads); compressed normal thyroid parenchyma is usually present external to the capsule
(top of the panel). Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 12 February 2007 05:41 PM)
© 2007 Elsevier

Clinical CourseClinical CourseFollicular carcinomas present as slowly Follicular carcinomas present as slowly enlarging painless nodules. enlarging painless nodules.
Most frequently, they are Most frequently, they are coldcold nodules on nodules on scintigramsscintigrams
VVascular invasion is common, with spread to ascular invasion is common, with spread to bone, lungs, liver, and elsewherebone, lungs, liver, and elsewhere
The prognosis is largely dependent on the The prognosis is largely dependent on the extent of invasion and stage at presentation.extent of invasion and stage at presentation.
Most follicular carcinomas are treated with total Most follicular carcinomas are treated with total thyroidectomy followed by the administration of thyroidectomy followed by the administration of radioactive iodineradioactive iodine. .

Medullary CarcinomaMedullary Carcinoma Medullary carcinomas of the thyroid are Medullary carcinomas of the thyroid are neuroendocrineneuroendocrine neoplasms neoplasms derived from the derived from the parafollicular cells, or C cells, of the thyroidparafollicular cells, or C cells, of the thyroid The cells of medullary carcinomas, similar to The cells of medullary carcinomas, similar to normal C cells, secrete normal C cells, secrete calcitonincalcitonin, , In some instances, the tumor cells elaborate In some instances, the tumor cells elaborate other polypeptide hormones, such as other polypeptide hormones, such as somatostatin, serotonin, and vasoactive somatostatin, serotonin, and vasoactive intestinal peptide (VIP).intestinal peptide (VIP). The tumors arise sporadically in about 80% of The tumors arise sporadically in about 80% of cases.cases. The remainder occurs in the setting of The remainder occurs in the setting of MEN syndrome 2A or 2B or as familial tumors MEN syndrome 2A or 2B or as familial tumors without an associated MEN syndrome without an associated MEN syndrome

MorphologyMorphology
Medullary carcinomas can arise as a Medullary carcinomas can arise as a solitary nodule or may present as multiple solitary nodule or may present as multiple lesions involving both lobes of the thyroid.lesions involving both lobes of the thyroid.The sporadic neoplasms tend to originate The sporadic neoplasms tend to originate in one lobe in one lobe BBilaterality and ilaterality and multicentricitymulticentricity are are common in familial cases. common in familial cases. The tumor tissue is firm, pale gray to tan, The tumor tissue is firm, pale gray to tan, and infiltrative.and infiltrative.

MicroscopicallyMicroscopicallyMMedullary carcinomas are composed of edullary carcinomas are composed of polygonal to spindle-shaped cells, which may polygonal to spindle-shaped cells, which may form nests, trabeculae, and even follicles. form nests, trabeculae, and even follicles.
Small, more anaplastic cells are present in some Small, more anaplastic cells are present in some tumors and may be the predominant cell type. tumors and may be the predominant cell type.
Acellular Acellular amyloid depositsamyloid deposits,, derived from derived from altered calcitonin molecules, are present in the altered calcitonin molecules, are present in the adjacent stroma in many cases adjacent stroma in many cases ..
Calcitonin is readily demonstrable within the Calcitonin is readily demonstrable within the cytoplasm of the tumor cellscytoplasm of the tumor cells--immunohistochemical methods.immunohistochemical methods.


Clinical CourseClinical Course
Sporadic cases of medullary carcinoma Sporadic cases of medullary carcinoma come to medical attention most often as acome to medical attention most often as a mass in the neckmass in the neck
In some instances, the initial In some instances, the initial manifestations are those of a manifestations are those of a paraneoplastic syndrome, caused by the paraneoplastic syndrome, caused by the secretion of a peptide hormone (e.g., secretion of a peptide hormone (e.g., diarrhea owing to the secretion of VIP). diarrhea owing to the secretion of VIP).

Anaplastic CarcinomaAnaplastic Carcinoma
Anaplastic carcinomas of the thyroid are Anaplastic carcinomas of the thyroid are undifferentiated tumorsundifferentiated tumors of the thyroid of the thyroid follicular epitheliumfollicular epithelium AAnaplastic carcinomas are aggressive naplastic carcinomas are aggressive tumors, with a mortality rate approaching tumors, with a mortality rate approaching 100%.100%. Patients with anaplastic carcinoma are Patients with anaplastic carcinoma are older than those with other types of thyroid older than those with other types of thyroid cancer, with a mean age of 65 years. cancer, with a mean age of 65 years.

MorphologyMorphology Microscopically, these neoplasms are composed Microscopically, these neoplasms are composed of highly anaplastic cells, which may take one of of highly anaplastic cells, which may take one of several histologic patterns: several histologic patterns:
(1) large, pleomorphic (1) large, pleomorphic giantgiant cells, including cells, including occasional osteoclast-like multinucleate giant occasional osteoclast-like multinucleate giant cells; cells;
(2) (2) spindlespindle cells with a sarcomatous cells with a sarcomatous appearance; appearance;
(3) (3) mixedmixed spindle and giant cells; and (4) spindle and giant cells; and (4) smallsmall cells resembling those seen in small cell cells resembling those seen in small cell carcinomas arising at other sites. carcinomas arising at other sites.

Clinical CourseClinical CourseAnaplastic carcinomas usually present as Anaplastic carcinomas usually present as a rapidly enlarging bulky neck mass.a rapidly enlarging bulky neck mass. In most cases, spread beyond the thyroid In most cases, spread beyond the thyroid capsule into adjacent neck structures or capsule into adjacent neck structures or has metastasized to the lungs at the time has metastasized to the lungs at the time of presentation. Compression and invasion of presentation. Compression and invasion symptoms, such as dyspnea, dysphagia, symptoms, such as dyspnea, dysphagia, hoarseness, and cough, are common.hoarseness, and cough, are common.There is There is no effective therapyno effective therapy for anaplastic for anaplastic thyroid carcinoma, and the disease is thyroid carcinoma, and the disease is almost uniformly fatal. almost uniformly fatal.