Embed Size (px)
Citation preview
THYROTOXICOSIS: A RETROSPECTIVE STUDY OF CASES SEEN
AT NUCLEAR MEDICINE UNIT (NEMROCK)
Thesis
Submitted for the fulfillment of master degree
In nuclear medicine
By
Amira Hodhod Elsayed
M.B.B.CH
Under Supervision of
Professor Dr. Shawky Ibrahim El.Haddad
Professor of Radiotherapy and Nuclear Medicine
Faculty of medicine –Cairo University
Dr. Gehan Ahmed Yuonis
Lecturer of Nuclear Medicine
Faculty of medicine –Cairo University
Faculty of medicine
Cairo University
2013
Acknowledgments
First, I would like to thank all my professors who allowed me to quote
their work.
I particularly grateful to professor Dr/ Shawky El.hadad for his
encouragement and generosity in dealing with science and Dr/ Gehan
Younis, this study would be much poorer without her help.
I am grateful to everyone in Nuclear Medicine department, Cairo
University.
A special thanks to Dr/ Ahmed Sabrey who helped me in the statistical
part of the study.
I am deeply indebted to my dear husband Dr/ Hisham Aboelnasr, who
was encouraging and supportive throughout.
This list would not be completed without mentioning the role of my
great mother in supporting me.
And last but not least, to my family and my friends for patiently
persevering with me.
Index
List of figures……………………………………………….…….…………………I
List of tables………………………………………………………………………….III
List of abbreviations………………………………………..………………..….V
Introduction and aim of the study………………………..…………….…1
Review of literature……………………………………….………..……………5
Material, methods and data collection…………………………….….49
Results………………………………………………………………………………..52
Discussion……………………………………………………………………….….69
Conclusion…………………………………………………………………..……..78
References……………………………………………….…………..……..…….81
Arabic summary…………………………………………..………..…………….1
�� درا�� �� ��ددة ا��ر��� ا���ة ا��از ز��دة ���ت ��� ر� ��� ا�
ا�$#وى ا�! و��ة
��� �����ل�� ا���وى ا��� ��
� درا�����
����� ��
��� ا� �� ه�ه� أ��ة / ا������
ا"اف ��
ا���اد ا��اه�� ���� /د.أ
ا�!�وى وا��� ا�ورام أ���ذ
ا�&�ه�ة %�$� – ا��� آ"��
,�+* أ(�� %�)�ن /د
ا�!�وى ا��� �رس
ا�&�ه�ة %�$� -ا��� آ"��

� ا���هة ��$�-ا��� آ�
٢٠١3
I
List of Figures
Figure (1) iodine -123 thyroid scan in patient with Graves'
disease …………………............................................................…….19
Figure (2) iodine-123 scan in patient with a toxic multinodular
goiter ……………………………………………………………………..….…………20
Figure (3) iodine-123 scan in a patient with a toxic
adenoma.……..………………………………………………………………….…..20
Figure (4) Tc 99m
thyroid scan of toxic adenoma …….……………..22
Figure (5) Tc 99m
thyroid scan of Graves' disease …….…………….22
Figure (6) Tc 99m
thyroid scan of toxic multi nodular goiter ……23
Figure (7) color flow ultrasonogram in a patient with Graves'
disease ………………………………………………………………..…………….…25
Figure (8) Comparison between age group and percentage of
cases of each type of thyrotoxicosis………………….…………………..54
Figure (9) Figure showing sex and percentage of cases of each
type of thyrotoxicosis …………………………………………..………………55
Figure (10) Treatment frequency according to the type of
thyrotoxicosis and percentage of cases received medical
treatment ….…………………………………………….…………….……….…..56
Figure (11) Thyrotoxicosis and percentage of cases with
previous surgery …………………………………………………….……………57
II
Figure (12) Relationship between response of primary type and
dose value of radio-active iodine……………………..……………………63
Figure (13) Secondary type response and dose value of radio-
active iodine……………………………………………………..…………………..65
Figure (14) Percent of cases received one or more dose of
radio-active iodine …………………………………………………..…………...66
Figure (15) Relationship between onset of hypothyroidism and
dose value of radio-active iodine.………………………………..………..68
III
List of tables
Table (1) lists clinical manifestation of hyperthyroidism ….....14
Equation (1) calculation of I131 dose based on goiter size and
radioactive iodine uptake …………………………………………………....32
Table (2) Relationship between the different age group in each
type of thyrotoxicosis…………………………………………………………53
Table (3) Relationship between sex and percentage of cases of
each type of thyrotoxicosis…………………………………………………55
Table (4) Frequency table of those received medical treatment
in the two groups of patients.………………………………………………56
Table (5) Cases with previous surgery ……………………………………57
Table (6) The predominant symptoms in each type of
thyrotoxicos…………………………………………………………………………..58
Table (7) Relation between TSH levels and type of
thyrotoxicosis……………………………………………………………………….59
Table (8) Relation between T3 levels and type of
thyrotoxicosis…………………………………………………………………….…60
Table (9) Relation between T4 levels and type of
thyrotoxicosis……………………………………………………………………….60
Table (10) The relation between the percent of thyroid gland
uptake and the response to radio-active iodine treatment….61
IV
Table (11) Relationship between response of primary type to
different dose values of radio-active iodine during 2 years of
follow up. ………………………………………………………………………….….62
Table (12) Response of secondary type thyrotoxicosis and
different dose values of radio-active iodine……………………….64
Table (13) Percentage of cases received one or more than one
dose of radio-active iodine…………………………………………………65
Table (14) Relationship between the dose value of radio-active
iodine and the onset of hypothyroidism……………………………..67
V
List of abbreviations
B
Bpm: beat per minute.
C
CI: THE CURIE (symbol CI) is a non-SI unit of radioactivity, named after
Marie and Pierre Curie. One curie is roughly the activity of 1 gram of
Radium isotope Ra226 a substance studied by Curies. 1 Ci =3.7x 1010
Bq=37 GBq.
E
EUGOGO: European Group on Graves' orbitopathy
F
FSH: follicle- stimulating hormone.
FT3: free triiodothyronine
FT4: free thyroxine
G
GnRH: Gonadotropin- Releasing Hormone
Graves' disease: primary diffuse toxic goiter
GY : gray is the unit of the International System of Units(SI) of absorbed
radiation dose , defined as transfer of 1 joul of energy per kilogram of
absorbing material (1 J/Kg); 1 gray equal 100 rads.
VI
H
HCG: Human Chorionic Gonadotropin.
I
I123
: Radioactive Iodine isotope 123.
I 131
: Radioactive Iodine isotope 131.
L
LH: luteinizing hormone.
N
NEMROCK: Kasr- El.Aini- Center of Radiotherapy and Nuclear Medicine.
M
MBq: The Becquerel is the International System of Units(SI) derived
unit of radioactivity . One Bq is defined as the activity of a quantity of
radioactive material in which one nucleus decays per second.
mg: milligram
mIU/L: milli International Unit per Liter
mm: micro meter
R
Rad: The rad is deprecated unit of absorberd radiation dose, defined as
1 rad = 0.01 Gy = 0.01 J/kg.
RAIU%: Radioactive Iodine Uptake percent.
VII
Rem: Is deprecated unit used to measure the biological effect of
ionizing radiaton . The rem is defined as equal to 0.01 sievert.
rhTSH: Recombinant Human thyroid -Stimulating Hormone.
S
SV: The Sievert (symbol: SV) is the International System of Units (SI)
derived unit of equivalent radiation dose, effective dose, committed
dose.
T
TAO: Thyroid-associated orbitopathy.
T3: Triiodothyroxine.
T4: Thyroxine.
Tc 99m
: Technetium Pertechnetate.
TMNG: Toxic multinodular goiter.
TRAb: Thyroid – Stimulating Hormone receptor antibodies.
TSAb: Thyroid Stimulating Antibodies.
TSbAB: Thyroid Stimulating blocking Antibodies.
TSH: Thyroid Stimulating Hormone.
TSI: Thyroid Stimulating Immunoglobulin.
U
uci=1x10-6
ci
VIII
U.K: United Kingdom.
U.S: United States.
1
Introduction & aim of the study
Thyrotoxicosis is the hypermetabolic condition associated
with elevated levels of thyroxin (FT4) and free triiodothyronine
(FT3). (Lee and Ananthakrishnan,2009).
Graves’ disease: Graves’ disease is the most common cause of
hyperthyroidism. It accounts for 60% to 80% of the total reported cases
of hyperthyroidism in the U.S. (Weetman, 2000).
Patients younger than 40 years are the highest risk for the
development of Graves’ disease. (Davies and Larsen, 2003).
Women have a higher reported incidence of Graves’ disease than
men, with a female to male incidence ratio of approximately 7:1 to
10:1. (Nayak and Hodak, 2007).
Graves’ disease is an autoimmune disorder where antibodies
mistakenly attack the thyroid gland, particularly the TSH receptor sites.
The attack stimulates the gland to synthesize and overproduce thyroid
hormone. (Werner, et al, 2000).
Toxic Multinodular Goiter and Toxic Adenomas: Toxic multinodular
goiter (TMNG), also known as Plummer’s disease, is a condition in
which the thyroid gland contains multiple nodules or lumps that are
hyper functional, causing an overproduction of thyroid hormones.
(Werner, et al, 2000).
TMNG usually occurs in patients who are more than 40 years old and
accounts for 5% of the total cases of hyperthyroidism in the U.S. The
incidence of TMNG is increased in iodine-deficient regions. (Werner, et
al, 2000).
2
Toxic adenomas are independently functioning thyroid nodules that
produce excessive amounts of thyroid hormones. Toxic adenomas are
most commonly found in younger patients who live in iodine-deficient
regions. (Slatosky, et al, 2000).
Thyroiditis: Thyroiditis is a condition where the thyroid gland becomes
inflammed. Inflammation of thyroid causes excess thyroid hormone
stored in the gland to leak into the systemic circulation. (Slatosky, et al,
2000).
Other causes of thyrotoxicosis:-
Iodide -induced hyperthyroidism is classified in two different types.
Type 1 Iodide -induced hyperthyroidism manifested with a low level of
TSH and high levels of T3 and T4. It is caused by uncontrolled excessive
production of T3 and T4 by the solitarily functioning thyroid in response
to iodine (Jod-Basedow phenomenon). (Baskin, et al, 2002).
Type 2 Iodide -induced hyperthyroidism is the destructive
inflammation of the thyroid (thyroiditis). (Baskin, et al, 2002).
Some of the tumors that can lead to a thyrotoxic state is struma
ovarii, Human Chorionic Gonadotropin (HCG)-producing and TSH
receptor-activating trophoblastic tumors, and TSH-secreting
adenomas. (Tierny, et al, 2005).
Laboratory investigations:
Serum Hormonal Level is diagnostic findings show that 95% of
patients with hyperthyroidism have a combination of suppressed serum
TSH levels of <0.05 mIU/L and an elevated serum free T4 level. (Dabon-
Almirante, et al, 1998 and Ladenson, 2005).
The levels of T3 and T4 should subsequently be assessed. (Braverman,
et al, 2005).
3
Imaging Tests:
In addition to clinical evaluation and blood tests, imaging techniques
are used to confirm diagnosis of hyperthyroidism.
The thyroid radioactive iodine uptake test with scanning is a key
diagnostic tool in the evaluation of hyperthyroidism.The average 6-hour
radioiodine uptake reference range is 5% to 15%, whereas the normal
24-hour uptake ranges from 5% to 25 %. (Intenzo and dePapp, 2003
and Meier and Kaplan, 2001).
Thyroid scintigraphy usually performed with technetium-99m
pertechnetate or radioiodine. (Meller and Becker, 2002; Summaria, et
al, 1999 and Smith and Oates, 2004).
Advantages of technetium-99m pertechnetate Lower radiation dose, better image quality, less waiting time after
administration, wider availability, lower cost and images can be
obtained while the patient is taking anti-thyroid medications. (Meller
and Becker, 2002; Summaria, et al, 1999 and Smith and Oates, 2004).
Treatment of thyrotoxicosis includes:
Symptoms relief by Beta-blocker therapy, Anti-thyroid drugs
(e.g.Propylthiouracil,Methimazole) leading to gradual reduction of
thyroid hormone level over 2-8 weeks or longer. (Cooper, 2005)
Radioactive Iodine: The desired outcomes are not seen immediately in
radioactive iodine therapy, endocrinologists often require patients to
continue anti-thyroid drug treatment until positive results are
established. Often patients start to manifest signs and symptoms of
euthyroidism within 2 to 3 months of ablative radioactive iodine
therapy. If complete ablation is not achieved 6 months after the
4
radioactive iodine therapy, repeated treatment is recommended
(Burman, 2006).
Surgical Intervention: Thyroidectomy is reserved for special
circumstances such as intolerance to anti-thyroid drugs or patient
refusal to undergo radioactive iodine therapy. Other candidates for
thyroidectomy are pregnant women with hyperactive thyroid who
cannot tolerate anti-thyroid drugs. (Wilson, et al, 1998).
Aim of the study:-
Review of cases of thyrotoxicosis: presentation, types (Graves’
disease, toxic nodular goiter, subacute thyroiditis and toxic adenoma),
laboratory findings, imaging picture, treatment, follow up and the
differences in between.
5
Hyperthyroidism
Introduction
Thyrotoxicosis is the hyper metabolic condition associated with
elevated levels of free thyroxine (FT4) and/or free triiodo -thyronine
(FT3) caused by excess synthesis and secretion of thyroid hormone by
the thyroid not associated with exogenous thyroid hormone intake .
(Lee and Ananthakrishnan, 2009)
The most common cause of thyrotoxicosis is Graves’ disease. Other
common causes are toxic multinodular goiter (TMNG), solitary toxic
adenoma, and thyroiditis. (Larsen, et al , 2002).
Rare causes of thyrotoxicosis include thyroid-stimulating hormone
(TSH)–secreting pituitary adenoma, struma ovarii, metastatic
functioning differentiated thyroid cancer, and metastatic tumors
within the thyroid gland causing destruction -induced thyrotoxicosis.
(Larsen, et al , 2002).
Specific thyrotoxic state
Graves’ disease:-
The most common cause of thyrotoxicosis is Graves’ disease (50-60%).
(Lee and Ananthakrishnan, 2010).
Graves’ disease is an autoimmune disease caused by an activating
autoantibody that targets the TSH receptor. (Larsen, et al, 2002).
Patients younger than age 40 years are the highest risk for the
development of Graves’ disease. (Davies , Larsen, 2003).
6
Graves’ disease is more common in women, with a female to- male
incidence ratio of approximately 7 to 10:1 (Larsen, et al, 2002).
Thyroid-stimulating antibodies (TSAb) bind to the TSH receptor,
activating adenylate cyclase, causing increased production of thyroid
hormone as well as increased thyroid growth and vascularity. Patients
with hyperthyroidism attributable to Graves’ disease may have (TSAb)
and thyroid stimulation-blocking antibodies (TSBAb) simultaneously.
(Takasu, et al, 1990).
Physical examination findings of Graves’ disease present in various
organ systems. The patient with Grave’s disease can have thyroid gland
findings of goiter and bruit. Ophthalmic findings can include proptosis,
ophthalmoplegia, and conjunctival irritation. (Bahn, 2000).
The proptosis and ophthalmoplegia seen in Graves’ disease are
attributable to infiltrative orbitopathy. Thyroid-stimulating hormone
receptor antibodies (TRAb) are thought to target the retro-orbital
tissues by binding to a TSH receptor antigen, which initiates a
subsequent T-cell inflammatory infiltrate. Fibroblasts stimulated by
cytokines produce glycosaminoglycans causing ophthalmopathy as a
result of mass effect in 20% to 40% of patients who have Grave’s
disease. (Bahn, 2000).
Graves’ disease may also present with multiple dermatologic findings.
Localized dermal myxedema can occur in 0.5% to 4.3% of patients with
Graves’ disease. (Fatourechi. 2005).
Because myxedema of Graves’ disease usually occurs in the anterior
leg, it has been called ‘‘pretibial myxedema’’. (Fatourechi, 2005).
7
Subacute thyroiditis
Subacute thyroiditis is the inflammation of the thyroid gland following
a viral infection of the upper respiratory tract. It is a self-limiting
inflammation of the thyroid characterized by an abrupt inception of
thyrotoxic signs and symptoms that are usually resolved within 8
months. (Slatosky, et al, 2000).
The inflammation of subacute thyroiditis is characterized by an
infiltration of mononuclear cells in affected regions of the thyroid
gland. Histopathologic examination can reveal the classic finding of a
central core of colloid surrounded by multi -nucleated giant cells, which
can progress to form a granuloma. (Farwell, 2005).
Subacute thyroiditis is the next most common cause of thyrotoxicosis
is (approximately 15-20%), due to a destructive release of preformed
thyroid hormone. (Lee and Ananthakrishnan, 2011).
Subacute thyroiditis has a peak incidence in the fourth and fifth
decades of life. It is rare in the first decade and relatively infrequent in
people older than 50 years, although it has been reported in extreme
age groups. (Ogawa, et al, 2003).
Anterior localized neck pain with or without fever is the hallmark of
the clinical presentation of subacute thyroiditis. The pain may also
radiate to the jaw or ear. Patients may report having hoarseness or
dysphagia. (Pearce, et al, 2003).
Thyrotoxic symptoms, including palpitations, nervousness, and
emotional liability, may also occur in up to 50% of patients (Pearce, et
al, 2003).

8
Physical examination findings include a tender thyroid gland, with
pain frequently localized to one side of the gland more than to the
other side. (Pearce, et al, 2003).
Laboratory evaluation of subacute thyroiditis demonstrates
suppressed TSH, elevated T4 and T3, elevation of the erythrocyte
sedimentation rate, leukocytosis, and an elevated thyroglobulin level.
(Pearce, et al, 2003).
In the initial phase of thyroiditis, inflammation destroys thyroid
tissue, which releases stored thyroid hormone and causes
thyrotoxicosis. This leads to suppression of TSH and a decrease of new
hormone synthesis, causing low uptake on radioactive iodine uptake
scanning. During the recovery phase of thyroiditis, the thyroid gland
can enter a ‘‘rebound’’ phase during which thyroid hormone
production is increased, with evidence of increased radioactive iodine
uptake (Intenzo and dePapp, 2003).
Toxic multinodular goiter Toxic multinodular goiter (TMNG), also known as Plummer’s disease,
is a condition in which the thyroid gland contains multiple nodules or
lumps that are hyperfunctional, causing an overproduction of thyroid
hormones. (Werner, et al. 2000).
TMNG accounts for 5% of the total cases of hyperthyroidism in the
U.S. The incidence of TMNG is increased in iodine-deficient regions.
(Werner, et al, 2000).
TMNG usually presents in individuals older than 50 years of age who
have had a long previous history of multinodular goiter. (Larsen, et al,
2002).
9
Toxic nodular goiter occurs more commonly in women than men. In
women and men older than 40 years the prevalence rate of palpable
nodule is 5-7 % and 1-2 % respectively. (Basaria and Salvatori, 2004).
The clinical presentation of the thyrotoxicosis is usually mild. Because
of the presentation in older age groups, however, TMNG often presents
with cardiovascular manifestations of thyrotoxicosis, such as
palpitations, tachycardia, and atrial fibrillation. (Larsen, et al, 2002).
Diagnosis of TMNG is made through laboratory evaluation that
demonstrates suppressed TSH and elevated levels of thyroxine (T4) and
triiodothyronine (T3). (Larsen, et al. 2002).
Radioactive iodine uptake and scanning reveals normal to increased
uptake and a heterogeneous pattern, with focal areas of increased
uptake corresponding to the hyperfunctioning nodules. (Larsen, et al,
2002).
Toxic adenoma
Toxic adenoma is caused by a single hyper functioning follicular
thyroid adenoma. Patients with a toxic thyroid adenoma comprise
approximately 3-5% of patients who are thyrotoxic. (Larsen, et al,
2002).
Like toxic multinodular goiter (TMNG), the pathogenesis is thought
to be attributable to a mutation in the TSH receptor gene, causing
constitutive receptor activation. The course of the disease, like TMNG,
generally evolves slowly; with frank nodule autonomy occurring only
after the nodule has been present for many years. (Larsen, et al, 2002).
Unlike TMNG, which occurs in older patients, the clinical presentation
of solitary toxic nodules usually occurs in the third and fourth decades.
(Larsen, et al, 2002).
10
Laboratory evaluation of a toxic adenoma demonstrates suppressed
TSH and elevation of T4 and T3. (Larsen, et al, 2002).
Solitary toxic adenoma is one of the most frequent causes of isolated
T3 toxicosis, however. In this situation, T4 may be normal with isolated
elevation of T3. (Larsen, et al, 2002).
Imaging with ultrasound should reveal a nodule. Radioactive iodine
uptake and scanning should demonstrate increased uptake over the
nodule, with evidence of suppressed uptake throughout the remainder
of the gland. (Larsen, et al, 2002).
Other causes of thyrotoxicosis
Iodide -induced hyperthyroidism is classified in two different types.
Type 1 Iodide -induced hyperthyroidism is similar to iodine-induced
hyperthyroidism and is manifested with a low level of TSH and high
levels of T3 and T4. It is caused by uncontrolled excessive production of
T3 and T4 by the solitarily functioning thyroid in response to iodine (Jod-
Basedow phenomenon). (Baskin, et al, 2002).
Type 2 Iodide -induced hyperthyroidism is the destructive
inflammation of the thyroid (thyroiditis). (Baskin, et al, 2002).
An excess of iodine in the diet can also have a devastating effect on
human health, as it can cause excessive production of thyroid
hormones leading to hyperthyroidism, especially in older patients with
pre-existing multinodular goiter. (Fitzgerald, 2005).
Other iodine-related contributing factors include medications and
radiographic contrast media exposure. (Fitzgerald, 2005).
Tumors are one of the rare causes of hyperthyroidism. Some of the
tumors that can lead to a thyrotoxic state are struma ovarii (tumor of
the ovary where predominantly or entirely existing thyroid cells in the
ovary produce thyroid hormones), Human Chorionic Gonadotropin
11
(HCG)-producing and TSH receptor-activating trophoblastic tumors, and
TSH-secreting adenomas. (Tierny, et al, 2005).
Factitious hyperthyroidism is characterized by higher than normal
thyroid hormone levels brought about by taking too many thyroid
hormone medications for hypothyroidism. (Reid, et al, 2005).
Another cause of factitious hyperthyroidism is intentional intake of
thyroid hormone preparation for weight loss. (Reid, et al, 2005).
12
Clinical presentation of thyrotoxicosis:-
Thyrotoxicosis causes a hypermetabolic state resulting in an
imbalance of energy metabolism in which energy production exceeds
energy expenditure. This may cause increased heat production,
resulting in perspiration, heat intolerance, and even fever. (Dabon-
Almirante, et al, 1998).
The signs and symptoms of hyperthyroidism are dependent on age,
duration of illness, extent of the overproduction of thyroid hormones,
and existence of a disease condition not related to hyperthyroidism.
(Reid and Wheeler, 2005).
Tri iodothyronine (FT3) exerts its effects directly on the heart. The
manifestations of these changes include increased heart rate, cardiac
contractility,and cardiac output. (Klein and Ojama, 2001) .
Tachycardia is the most common cardiovascular sign of
thyrotoxicosis. Thyrotoxic patients may also experience palpitations
attributable to increased force of cardiac contraction. (Larsen, et al,
2002).
Thyroid hormone decreases systemic vascular resistance through a
direct vasodilator action on the smooth muscle, which is mediated by
endothelial release of nitric oxide and other endothelial-derived
vasodilators. (Ojamaa, et al, 1996).
Physical findings in thyrotoxicosis can include a strong apical
impulse, increased pulse pressure, and a hyperdynamic precordium.
Heart sounds can include the ‘‘Means-Lerman scratch’’ heard at the
apex, which is thought to be attributable to the hyperdynamic
precordium rubbing against the pleura. (Larsen, et al, 2002 and Dabon-
Almirante, et al, 1998).
13
Thyrotoxic patients can experience chest pain that may mimic
ischaemic angina pectoris. (Dabon-Almirante, et al, 1998).
Older individuals may present with atypical clinical manifestations of
thyrotoxicosis. ‘‘Apathetic hyperthyroidism’’ is a common presentation
in the elderly and is characterized by weight loss, weakness,
palpitations, dizziness, or memory loss and physical findings of sinus
tachycardia or atrial fibrillation. (Dabon-Almirante, et al, 1998).
Thyrotoxicosis causes neuropsychiatric changes resulting in
restlessness, agitation, anxiety, emotional liability. (Wartofsky,2005).
Gastrointestinal manifestations of thyrotoxicosis include increased
frequency of bowel movements caused by increased motor contraction
of the small bowel, resulting in more rapid transit of intestinal contents.
(Dabon-Almirante, et al, 1998).
Thyrotoxicosis can affect the menstrual cycle in women, resulting in
oligomenorrhea or amenorrhea. The etiology of the menstrual
irregularity is unclear but may be attributable to the effects of thyroid
hormone on gonadotropin-releasing hormone (GnRH) causing
disruption of normal luteinizing hormone (LH)/follicle-stimulating
hormone (FSH) pulsatility. (Larsen, et al, 2002).
Approximately 10% of male patients with hyperthyroidism may
experience symptoms of decreased libido or gynecomastia and
development of spiderangiomas. (Dabon-Almirante, et al, 1998).
14
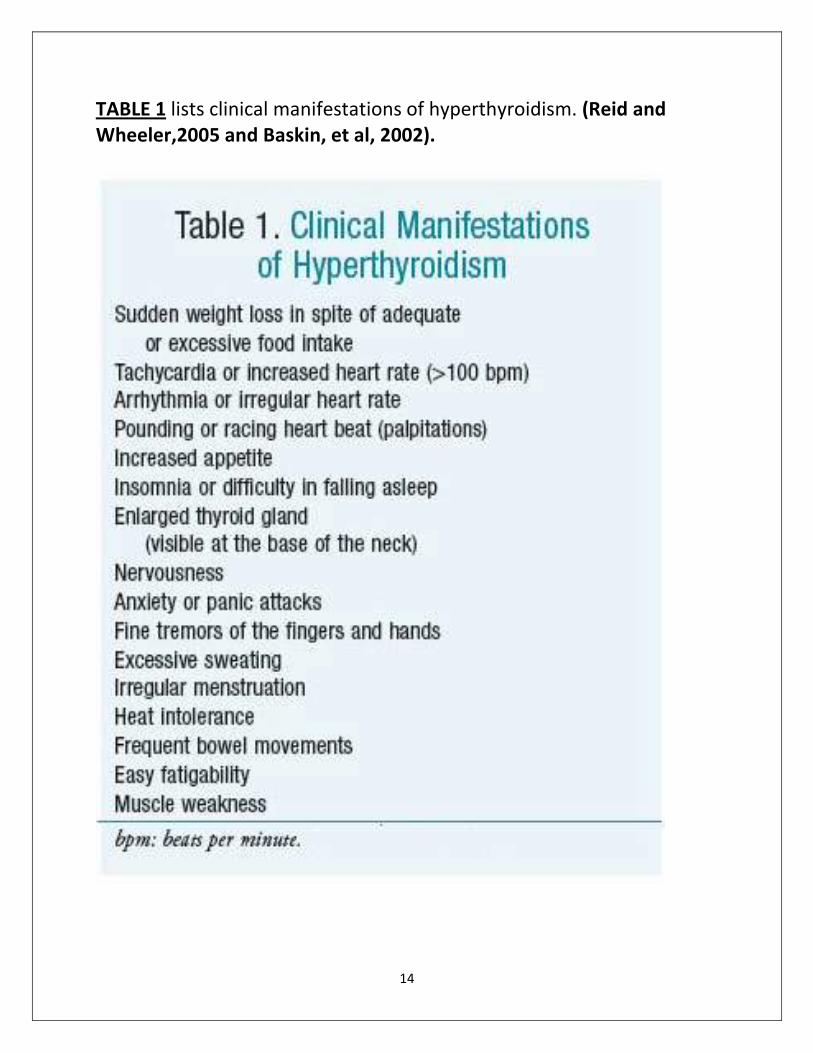
TABLE 1 lists clinical manifestations of hyperthyroidism. (Reid and
Wheeler,2005 and Baskin, et al, 2002).
15
Diagnosis of hyperthyroidism:-
(A) Laboratory diagnosis:-
T3 ,T4 and TSH level A suppressed TSH level (<0.05 mU/mL) in combination with an
elevated serum free T4 level occurs in 95% of patients with clinically
evident thyrotoxicosis. (Dabon-Almirante, et al,1998 and Ladenson.
2005).
Although a TSH assessment alone may be appropriate for routine
screening in an asymptomatic patient, the suspicion of thyrotoxicosis
warrants the additional assessment of T4 and T3. In cases in which
subclinical hyperthyroidism is suspected, TSH measurement may be
used as a first diagnostic step, with subsequent T4 and T3 assessment if
TSH is suppressed.
(Dabon-Almirante, et al,1998 and Ladenson. 2005).
Free hormone concentrations are preferable in the diagnosis of
thyrotoxicosis because of the possible interference of protein binding
with total thyroid hormone levels. (Baloch, et al, 2003).
Thyroid-stimulating hormone receptor antibodies
The measurement of Thyroid-stimulating hormone receptor
antibodies (TRAb) may occasionally be helpful in the diagnosis and
management of Grave’s disease. A second generation of this assay
using recombinant TSH receptor has been developed and has a
reported sensitivity of 98.6%. (Costagliola, et al, 1999).
TRAb measurements are particularly useful in the prediction of
postpartum Grave’s thyrotoxicosis and neonatal thyrotoxicosis.
(Hidaka, et al, 1994).
16
Thyroxine/triiodothyronine ratio
The ratio of T4 to T3 frequently has a characteristic pattern in different
thyrotoxic states. Evaluation of the T4/T3 ratio may be a useful tool in
the initial diagnosis of thyrotoxicosis when radio -active iodine uptake
testing is not readily available or is contra -indicated. (Ladenson,
2005).
Grave’s disease and toxic nodular goiter typically present with
increased T3 production, with a T3/T4 ratio greater than 20.
(Yanagisawa, et al, 2005).
With thyrotoxicosis caused by thyroiditis, iodine exposure, or
exogenous levothyroxine intake T4 is the predominant hormone and
the T3/T4 ratio is usually less than 20.
(Ladenson. 2005).
Other laboratory findings
Thyrotoxicosis may also cause hyperglycemia, hypercalcemia,
elevated alkaline phosphatase, leukocytosis, and elevated liver
enzymes. (Wartofsky, et al, 2005 and Pimental, Hansen, 2005 ).
17
(B) Imaging:-
Multiple imaging modalities may assist in the determination of the
etiology of thyrotoxicosis. These include thyroid nuclear imaging
studies and anatomic studies like thyroid ultrasound.
Nuclear imaging studies:-
A key diagnostic tool in the evaluation of thyrotoxicosis is radioactive
iodine uptake and scanning. Radioactive iodine uptake and scanning
uses a radioactive isotope of iodine, typically I123
or I131
. (Meier and
Kaplan, 2001).
After ingestion of the tracer, the normal values for the24-hour
radioiodine uptake range between 5% and 25%, and the average6-hour
uptake reference range is between 5% and 15% (Meier and Kaplan,
2001).
The differential diagnosis of thyrotoxicosis may be divided into
categories based on whether increased or decreased uptake of
radiotracer is observed during thyroid scanning.
Increased nuclear tracer uptake
May be seen in toxic multi-nodular goiter, toxic solitary nodule, or
Grave’s disease. (Cakir, 2005).
Graves’disease generally demonstrates homogeneous uptake
throughout the gland. With markedly increased thyroid hormone
synthesis and turn over in Graves’ disease, there can be a paradoxical
finding of elevated uptake at 4 or 6 hours after radioiodine dosing but a
normal uptake at 24 hours as a result of accelerated clearance of the
radioactive iodine. (Cavalieri, 1991).
18
TMNG generally has a heterogeneous pattern of uptake with
hyperfunctioning nodules that demonstrate increased radionuclide
uptake on scan. These nodules appear on a background of partially or
completely suppressed uptake in the uninvolved areas of the thyroid
gland. (Cavalieri, 1991).
Solitary toxic nodules have a radioactive iodine scan pattern
demonstrating increased uptake in the hyperfunctioning nodule and
decreased uptake in the remainder of the gland. When the uptake in
the uninvolved parts of the thyroid is completely suppressed, such a
nodule is frequently referred to as an autonomous or ‘‘hot’’ nodule. If
the uninvolved parts of the thyroid are not completely suppressed, the
nodule is frequently referred to as a ‘‘warm’’ nodule to differentiate
this type of radiographic pattern. (Cavalieri, 1991).
Paradoxically, increased radioactive iodine uptake may also be found
in Hashimoto’s thyroiditis. This finding usually occurs with early or
relatively mild disease. (Meier and Kaplan, 2001).
Decreased nuclear tracer uptake
Thyrotoxic conditions typically associated with decreased radioactive
iodine uptake include exogenous thyroid hormone intake, thyroiditis,
and iodine intoxication. The main cause of the decreased isotope
uptake in all these conditions is suppression of TSH. (Intenzo and
dePapp , 2003).
In the initial phase of thyroiditis, inflammation destroys thyroid
tissue, which releases stored thyroid hormone and causes
thyrotoxicosis. This leads to suppression of TSH and a decrease of new
hormone synthesis, causing low uptake on radioactive iodine uptake
scanning. (Intenzo and dePapp, 2003).
During the recovery phase of thyroiditis, the thyroid gland can enter
a ‘‘rebound’’ phase during which thyroid hormone production is

19
increased, with evidence of increased radioactive iodine uptake
(Intenzo and dePapp, 2003).
Iodine-rich agents, such as amiodarone, radiographic contrast
agents, or increased oral iodine intake are a frequent cause of iodine
intoxication. Iodine intoxication decreases radioiodine uptake. (Intenzo
and dePapp, 2003 and Cavalieri, 1991).
Figure (1) Iodine-123 thyroid scan in a patient with Grave’s disease: Tracer
uptake is uniform throughout the gland. The 5-hour iodine uptake was high at
53%. (Piga , et al, 2008).
20
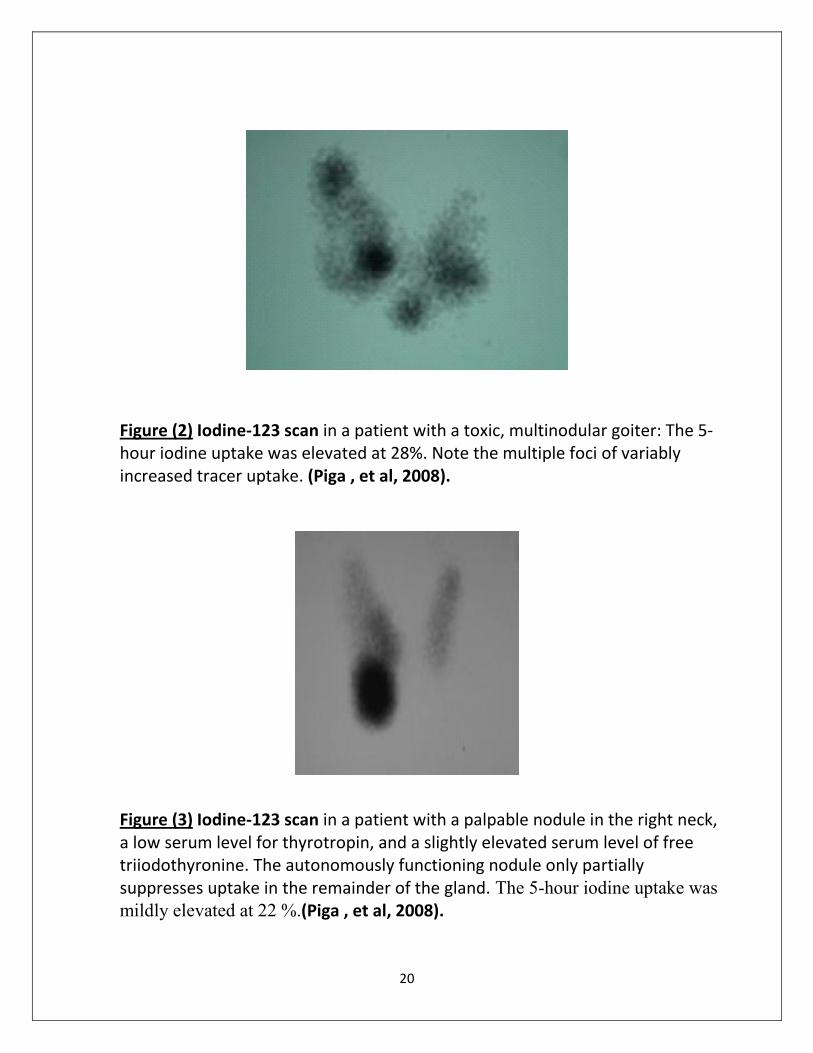
Figure (2) Iodine-123 scan in a patient with a toxic, multinodular goiter: The 5-
hour iodine uptake was elevated at 28%. Note the multiple foci of variably
increased tracer uptake. (Piga , et al, 2008).
Figure (3) Iodine-123 scan in a patient with a palpable nodule in the right neck,
a low serum level for thyrotropin, and a slightly elevated serum level of free
triiodothyronine. The autonomously functioning nodule only partially
suppresses uptake in the remainder of the gland. The 5-hour iodine uptake was
mildly elevated at 22 %.(Piga , et al, 2008).
21
Technetium-99m pertechnetate imaging
Thyroid scintigraphy usually performed with technetium-99m
pertechnetate or radioiodine. (Meller and Becker, 2002 ; Summaria, et
al, 1999 and Smith and Oates, 2004).
:m pertechnetate99-vantages of technetiumAd
• Lower radiation dose
• Better image quality
• Less waiting time after administration
• Wider availability
• Lower cost
• Images can be obtained while the patient is taking anti-thyroid
medications.
(Meller and Becker, 2002 ; Summaria, et al, 1999 and Smith and
Oates, 2004).
: active iodine-Advantages of radio
• Has lower levels of vascular background activity which is useful when
assessing retrosternal masses.
• Has some advantages in the evaluation of thyroid nodules, although
these are rarely of clinical significance
• Oral administration
(Intenzo, et al, 2003; Naik and Bury, 1998 and Smith and Oates, 2004)
Scintigraphy is particularly useful for distinguishing Graves' disease
from conditions such as subacute, silent and post -partum thyroiditis
and factitious hyperthyroidism. (Meier and Kaplan, 2001).
Scintigraphy is also useful for demonstrating toxic adenomas.
(Intenzo, et al , 2003).
22
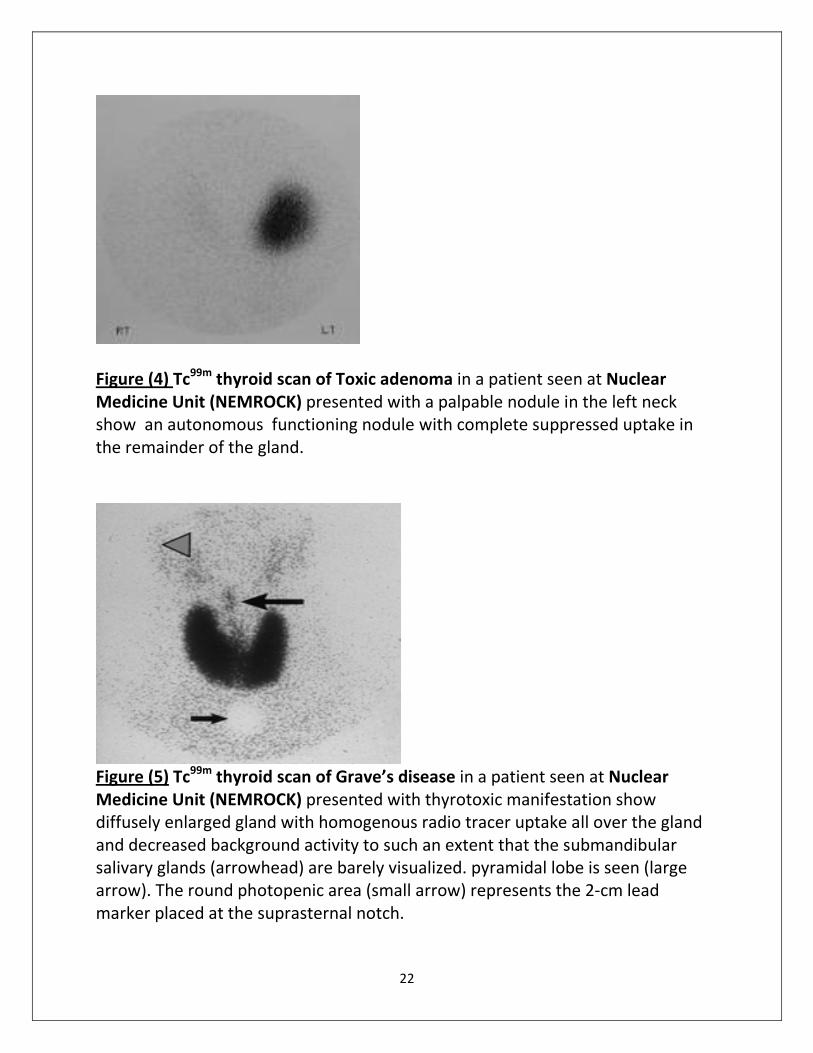
Figure (4) Tc99m
thyroid scan of Toxic adenoma in a patient seen at Nuclear
Medicine Unit (NEMROCK) presented with a palpable nodule in the left neck
show an autonomous functioning nodule with complete suppressed uptake in
the remainder of the gland.
Figure (5) Tc
99m thyroid scan of Grave’s disease in a patient seen at Nuclear
Medicine Unit (NEMROCK) presented with thyrotoxic manifestation show
diffusely enlarged gland with homogenous radio tracer uptake all over the gland
and decreased background activity to such an extent that the submandibular
salivary glands (arrowhead) are barely visualized. pyramidal lobe is seen (large
arrow). The round photopenic area (small arrow) represents the 2-cm lead
marker placed at the suprasternal notch.
23
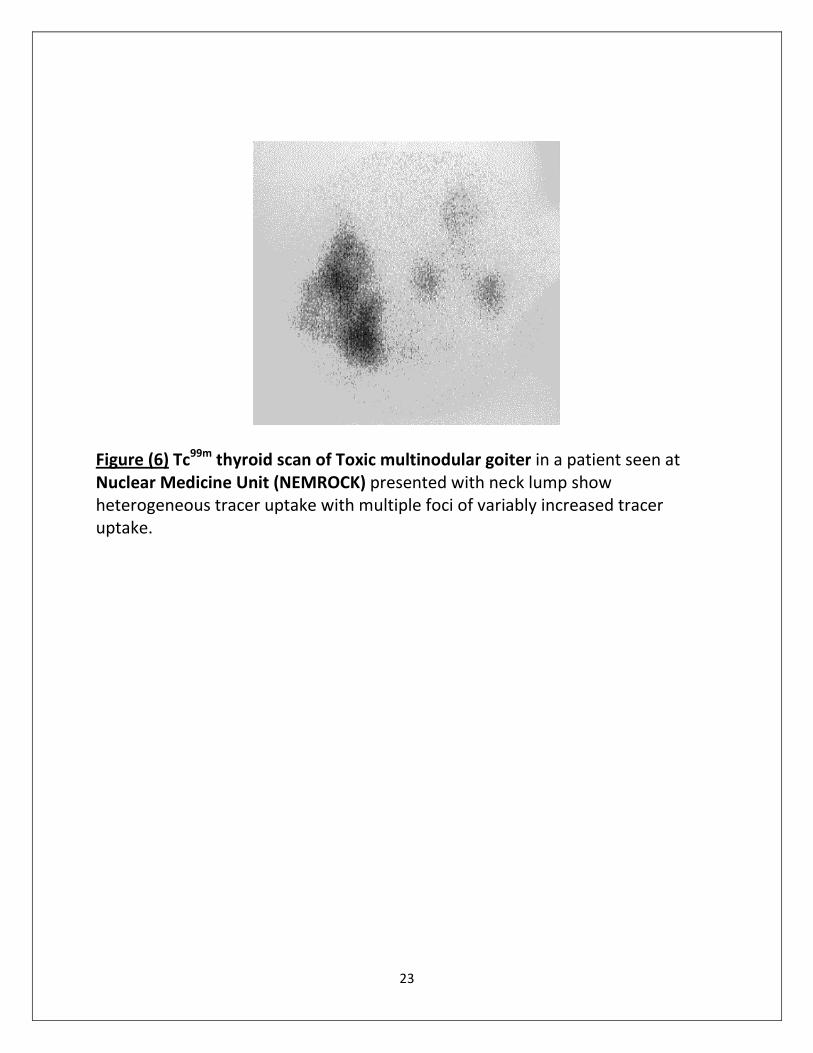
Figure (6) Tc99m
thyroid scan of Toxic multinodular goiter in a patient seen at
Nuclear Medicine Unit (NEMROCK) presented with neck lump show
heterogeneous tracer uptake with multiple foci of variably increased tracer
uptake.
24
Thyroid ultrasonography in the evaluation of
hyperthyroidism
Thyroid sonography may be useful in the diagnostic evaluation of
thyrotoxicosis. Sonographic assessment can identify thyroid nodules
and goiter that may not be readily apparent on examination. (Kurita, et
al, 2005).
Additionally, sonographic Doppler flow assessment may provide
particularly useful information about several thyrotoxic states.
Kurita and colleagues used an index measurement of thyroid blood
flow per unit area to distinguish between Graves’ disease and
thyrotoxicosis caused by non hypermetabolic destructive thyroiditis.
(Kurita, et al, 2005).
Using a thyroid blood flow area of 8% or greater had a sensitivity of
95% and a specificity of 90% for the prediction of Graves’ disease.
(Kurita, et al, 2005).
Ultrasound can detect the presence of nodules and goiter that may
favor the diagnosis of type I Iodide –Induced thyrotoxicosis. (Bogazzi, et
al, 1997).
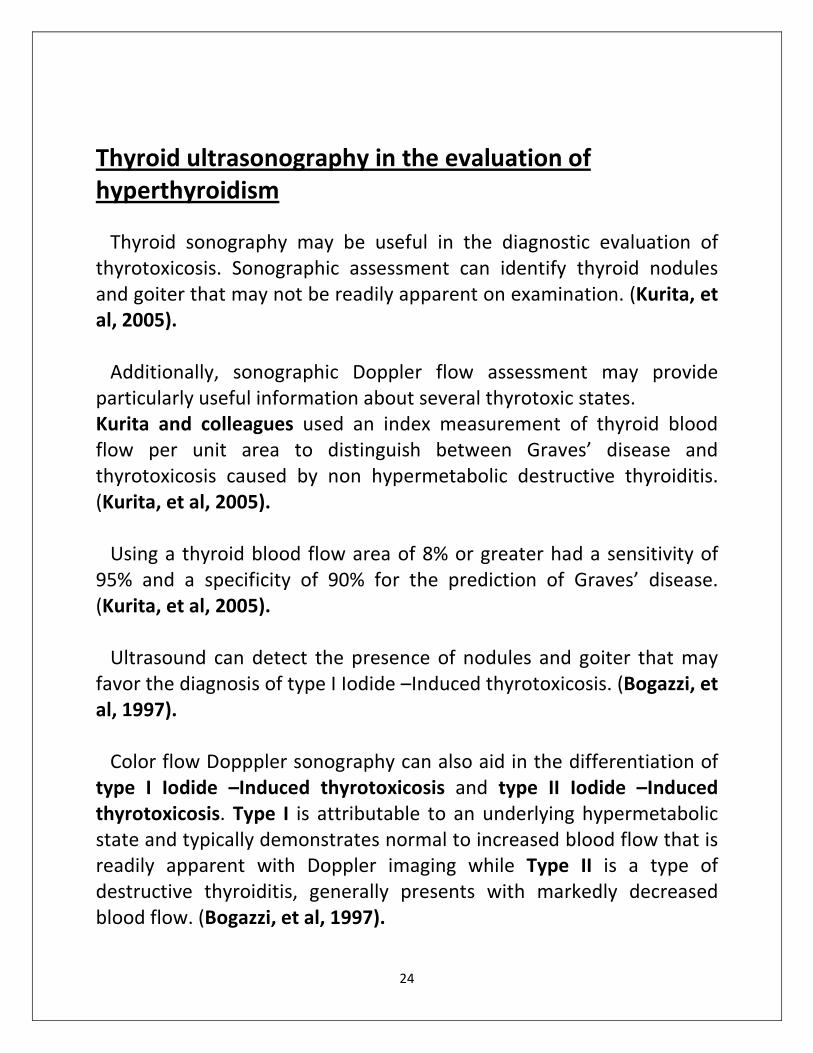
Color flow Dopppler sonography can also aid in the differentiation of
type I Iodide –Induced thyrotoxicosis and type II Iodide –Induced
thyrotoxicosis. Type I is attributable to an underlying hypermetabolic
state and typically demonstrates normal to increased blood flow that is
readily apparent with Doppler imaging while Type II is a type of
destructive thyroiditis, generally presents with markedly decreased
blood flow. (Bogazzi, et al, 1997).

25
Figure( 7): Color flow ultrasonogram in a patient with Grave’s disease.
Generalized hypervascularity is visible throughout the gland, which often can be
heard as a hum or bruit with a stethoscope. (Loy, et al, 2007).
26
Differential Diagnosis of Hyperthyroidism
Graves’ disease there is cases where in elevated levels of free thyroid
hormones (T3 and T4) despite a normal-sized thyroid gland. There are
also circumstances wherein patients would only develop T3 toxicosis, as
manifested by sole elevation of triiodothyronine hormone levels.
Sensitive assay testing reveals depressed levels of TSH in Graves’
disease, whereas radioactive scans reveal diffused uptake of radioactive
isotopes and, in some cases, a pyramidal lobe. (Baskin, et al, 2002).
Thyroid adenoma (toxic adenoma) also known as hot nodule is
manifested by suppressed levels of TSH, with or without elevated levels
of free thyroid hormones. Thyroid scanning reveals a normally
functioning thyroid nodule and decreased iodine uptake in the
surrounding extranodular and contralateral thyroid tissue. The same is
true of toxic multinodular goiter where thyroid gland variably enlarged
with multiple nodules. (Baskin, et al, 2002).
Subacute thyroiditis, silent thyroiditis, iodine-induced
thyrotoxicosis, and factitious thyroxine-induced thyrotoxicosis are
characterized by a low radioiodine uptake and poor thyroid gland
imaging in scintigraphic scan. These conditions are often accompanied
by increased levels of thyroid hormones during the hyperactive thyroid
state. (Baskin, et al, 2002).
Classic subacute thyroiditis is a thyroid condition that is manifested
by painful inflammation of the thyroid gland accompanied by fever. It
has a triphasic clinical pathway consisting of: hyperthyroid phase,
hypothyroid phase and resolution phase. (Baskin, et al. 2002).
Silent thyroiditis is an autoimmune disorder characterized by painless
inflammation of the thyroid gland. It has a clinical course similar to that
of classic subacute thyroiditis. It is common in women, especially during
the postpartum period. (Baskin, et al, 2002).
27
Iodine-induced thyrotoxicosis more often affects elderly patients. It
can also be seen in patients with pre-existing autonomously functioning
thyroid nodules. (Baskin, et al, 2002).
Factitious thyrotoxicosis has the same clinical presentation as iodine-
induced thyrotoxicosis. In contrast to all types of thyroiditis, the
thyroglobulin level is very low and sometimes nonexistent. (Baskin, et
al, 2002).
28
Treatment of thyrotoxicosis
Disease’ Treatment of Graves
Antithyroid medications
Those in current use are methimazole (carbimazole in the U.K. and
countries influenced by British medicine) and propylthiour -acil. The
longer half-life of methimazole allows for once-daily intake, which is a
considerable advantage over the dosage schedule for propylthiouracil,
which generally has to be taken 2 or 3 times daily (Cooper, 2005)
Propylthiouracil is preferred during pregnancy to avoid teratogenic
effect of methimazole. (Zweig, et al, 2006).
The main action of these drugs is to interfere with the iodination of
tyrosine within the colloid of the thyroid follicle. The drugs have a
minor immunologic effect that is not entirely attributable to the
normalization of thyroid function. The inhibition of the conversion of T4
to T3 by Propylthiouracil is of minor significance. (Zweig, et al, 2006).
Both medications are introduced in a loading dose for about 4–6
weeks. As the patient’s condition improves symptomatic -cally and
biochemically, the dose can usually be reduced. Daily loading doses of
10–30 mg of methimazole or 100–300 mg of propylthiouracil,
Maintenance doses of 5–10 mg of methimazole or 50–100 mg of
propylthiouracil twice daily keep most patients euthyroid. (Zweig, et al,
2006).
Medication is prescribed for 12–18 months with the hope
that the disease will remit.(Abraham, et al, 2005).
An alternative medical approach is to continue the larger loading dose
for 18 months and to add thyroid hormone (block and-replace therapy).
29
This approach was thought to increase the percentage of patients
whose disease would remit (Abraham, et al, 2005).
Mild complications include maculopapular and urticarial skin rashes,
nausea, dislike of the taste of the medications, and arthoropathy.
(Koornstra, et al, 1999).
More serious complications is agranulocytosis, which occurs most
often within weeks of starting either medication and usually presents
as a sore throat with fever. Patients must be warned to stop the drug
and have an immediate differential white cell count test. (Koornstra, et
al, 1999).
When the granulocyte count is less than 1,500/mm the medication
should not be restarted and an alternative medication should be used.
(Koornstra, et al, 1999).
Anti-thyroid medication has a significant role in rendering patients
euthyroid before treatment with I131
or thyroidectomy (Koornstra, et
al, 1999).
For radioiodine, this process is advised for older patients, very
thyrotoxic patients, and patients with cardiac problems.Patients being
treated by surgery should be euthyroid first. (Imseis, et al, 1998 and
Santos, et al, 2004).
Propylthiouracil is discontinued for 3 days and methimazol is
discontinued for 5 days before testing and therapy. (Razvis, et al, 2004;
Walter, et al,2006 and Weaver and Razvis, 2005).
30
Surgery
Indications for surgery include a coexisting nonfunctioning nodule or a
nodule suggestive of cancer on fine-needle aspiration.
One indication for surgery is a patient who desires to become
pregnant and who is not convinced that it is safe to be treated with I131
before conception or to take anti-thyroid medication during pregnancy
(England, et al, 2006).
The procedure should be a nearly total thyroidectomy with the
expectation for lifelong thyroid hormone replacement. (Gurleyik, et al,
2005).
The incidence of recurrence after subtotal thyroidectomy is high and
this almost always should be treated with I131
.Thus, the patient receives
radioiodine treatment which, for one reason or another, was originally
believed to be less desirable complications, such as hypoparathyroidism
and damage to the recurrent and superior laryngeal nerves, should be
uncommon. (Gurleyik, et al, 2005).
Surgery provides a more rapid outcome and should be considered in
a patient who wishes an early conception or is concerned about
radiation(Kang, et al, 2002).

31
CTIVE IODINEA- TREATMENT WITH RADIO
There has never been any debate that the goal of I131
treatment is to
cure the thyrotoxic condition. (Cooper, 1996 and Franklyn, 1994).
Radioactive iodine is the treatment of choice for most patients with
Graves’ disease and toxic nodular goiter. It is inexpensive, highly
effective, easy to administer, and safe.
(American Academy of Clinical Endocrinologists, 2002 and
Harper and Mayeaux, 2003).
The treatment of hyperthyroidism in children remains controversial,
but radioactive iodine is becoming more acceptable in this group.
(Rivkees , 2001) .
HOW IS ADMINISTERED DOSE DETERMINED?
There are 2 common approaches for determining the administered
dose (Kalinyak and McDougall, 2003).
One is to prescribe a fixed dose for all patients. The other is to
calculate a dose based on the size of the thyroid and its percentage
uptake at 24 h. Fixed doses vary but are commonly in the range of 185–
555 MBq (5–15 mCi). (Kalinyak and MC Dougall, 2003).
A variation on the fixed-dose is to add an incremental dose of I131
when the gland is large or when the uptake is relatively low. (Kalinyak
and MC Dougall, 2003).
A gland-specific dosage based on the estimated weight of the gland
and the 24-hour uptake may allow a lower dosage and result in a lower
incidence of hypothyroidism but may have a higher recurrence rate.
(Harper and Mayeaux, 2003).
Higher-dose ablative therapy increases the chance of successful
treatment and allows the early hypothyroidism
32
(Weetman , 2000 and Allahabadia, et al, 2001).
CALCULATING ADMINISTERED DOSE
Many use a formula that is based on gland size and 24 hour
radioactive iodine uptake % for calculating the administered dose.
Generally, large glands require a relatively higher therapeutic dose and
patients with higher %RAIU require a lower dose.
I131
administerated dose =
24 hour % RAIU
Equation (1) calculation of I131
dose based on goiter size and radioactive iodine
uptake. (Burmank, et al, 2006).
Therefore, a 40-g gland with 50% uptake would be treated with 474
MBq (12.8 mCi). This method has a high probability of cure with a single
dose of I131
and less than 10% of patients needing to be retreated
(Alexander and Larsen, 2002).
The administration of a quantity of I131
on the basis of the size of the
thyroid implies that the exact size is known. This size can be
determined with some accuracy by ultrasound. (Alexander and Larsen,
2002).
CALCULATING ABSORBED DOSE
33
Controversies exist with regard to the radiation dose to the thyroid
needed to successfully treat Graves’ disease. A study comparing doses
of 150, 300, and greater than 300 Gy to the thyroid found no significant
difference in the rates of recurrent hyperthyroidism whereas the rates
of hypothyroidism in the 3 groups were significantly correlated with
doses. (Howarth, et al, 2001).
FAILURE OF THERAPY
The need for retreatment indicates that insufficient I131
was
administered. This situation could result because a fixed dose was too
small relative to the size of the gland or because the thyroid was less
able to trap iodine than expected (Erem, et al, 2004) or because the
size of the gland was underestimated when a dose per gram corrected
for uptake was administered. A rapid turnover of iodine must be
considered and can be adjusted for by measuring 24-h uptake rather
than uptake at 4–6 hours (Venulakonda, et al, 1996).
Another rare cause of failure was described: a patient ‘‘spat up’’ the
capsule and also had a high level of serum iodine (Kinuya, et al, 2004).
When a patient is not rendered euthyroid or hypothyroid, a second
treatment is advised. Some authorities advise a second treatment after
3 months, some prefer a delay of 6 months or more because a
proportion of patients respond later. (Kinuya, et al, 2004).
34
TREATMENT OF SINGLE HYPERFUNCTIONING AUTONOMOUS
NODDULE
In few cases necrosis of the center of the nodule result in
euthyroidism however, that remission is not long-lasting. As a result,
the decision to remove the nodule by lobectomy or to ablate it with I131
is generally accepted. Each treatment has benefits and drawbacks.
(Vidal, et al, 2004 and Gurleyik, et al, 2005).
Indications for surgery include a coexisting nonfunctioning nodule or
a nodule suggestive of cancer on fine-needle aspiration. (England, et al,
2006).
One indication for surgery is a patient who desires to become
pregnant and who is not convinced that it is safe to be treated with I131
before conception or to take anti-thyroid medication during pregnancy
(England, et al, 2006).
Lobectomy is undertaken after the patient is rendered euthyroid by
anti-thyroid medications. It produces a speedy cure, there is no
radiation, but it requires surgery, usually under general anesthesia.
(Vidal, et al, 2004 and Gurleyik, et al, 2005).
I131
treatment avoids surgery and anesthesia but requires radiation
safety education and planning. (Vidal, et al, 2004 and Gurleyik, et al,
2005).
35
I131
takes several weeks to have its full effect, and the nodule will not
dissolve completely; therefore, the patient must be advised that
physicians may want to perform follow up examinations. (Vidal, et al,
2004 and Gurleyik, et al, 2005).
Ceccarelli et al 2005. administered 7.4 MBq (200 UCi) of I131
per gram
corrected for uptake had a success rate of 94%, and 60% of their
patients were hypothyroid by 20 years .
The volume can be determined by ultrasound and the uptake can be
determined with a I123
tracer. (Reiners and Schneider, 2002).
A total of 66% of the patients were adequately treated with a single
calculated dose; in comparison, 27% were adequately treated with a
single empiric dose. Thus, calculated doses appear to be preferable to
fixed doses. (Huysmans, et al, 1993).
Finally, the administered dose can be calculated to deliver a specific
dose defined in rads or grays to the nodule. A recent study of 425
treated patients demonstrated that doses of 300–400 Gy delivered to
the nodule were successful in 90%–94% of patients (Reinhardt, et al,
2006).
Other therapeutic options for autonomous hyperfunctioning thyroid
nodules include ultrasound-guided laser thermal ablation and
percutaneous ethanol injection (Pacella, et al. 2004).
Several injections of alcohol are administered to the nodule by use of
ultrasound to localize the appropriate site. Free hormone levels fall,
TSH levels rise, and the volume of the nodule decreases. The
advantages include no surgery or exposure to radiation. The
disadvantages are multiple visits (occasionally more than 10), pain and,
in rare cases, serious local complications, such as necrosis of the larynx
(Mauz, et al, 2004).
36
TOXIC MULTINODULAR GOITERS
The American Thyroid Association and American Association of
Clinical Endocrinologists have released guidelines for the management
of hyperthyroid and other causes of thyrotoxicosis, including the use of
radioactive iodine or surgery to treat toxic multinodular goiter
(TMNG).(Bahn Chair, et al, 2011).
Because the affected patients are usually older, it is important to
render them euthyroid with antithyroid medications before definitive
therapy. (Giovanella, et al, 2000 and Nygaard, et al, 1999).
In the United States and Europe, radioactive iodine is considered the
treatment of choice for TMNG. Except for pregnancy, there are no
absolute contraindications to radioiodine therapy.
( Allahabadia , et al, 2001).
Much debate exists regarding optimal dosing of radioactive iodine.
Patients with TNG tend to have less uptake than patients with Grave’s
disease; therefore, they are generally considered to need higher doses
of I131
. However, studies by Allahabadia and colleagues suggest that
fixed doses of radioiodine do not demonstrate any difference in
response in these 2 groups of patients (patients with Grave’s and
patients with TNG) using a fixed dose of 10 mci. (Allahabadia , et al,
2001).
One approach is to deliver 7.4MBq (200 uCi) per gram, a dose
calculated from the 24-h uptake and the volume determined by
ultrasound. (Duick and Baskin, 2003 and Rubio, et al, 2005).
A single dose of radioiodine therapy has a success rate of 85-100% in
patients with TNG. Radioiodine therapy may reduce the size of the
goiter by up to 40%. (Zingrillo, et al, 2007).
37
Failure of initial treatment with radioactive iodine has been
associated with increased goiter size and higher T3 and free T4 levels,
which suggests that these factors may present a need for higher doses
of I131
. ( Albino, et al , 2005 and Duick and Baskin, 2003).
A positive correlation exists between radiation dose to the thyroid
and decrease in thyroid volume. ( Albino, et al , 2005 and Duick and
Baskin, 2003).
In patients with uptake of less than 20%, pretreatment with lithium or
recombinant TSH can increase the effectiveness of iodine uptake and
treatment. ( Albino, et al , 2005 and Duick and Baskin, 2003).
Hypothyroidism occurs in 10-20% of patients; this is similar to the
incidence rate after surgery and is substantially less than in the
treatment of Graves' disease. (Adamali, et al, 2007).
surgery A subtotal thyroidectomy is performed most commonly. This surgery
preserves some of the thyroid tissue and reduces the incidence of
hypothyroidism to 25 percent, but persistent or recurrent
hyperthyroidism occurs in 8 percent of patients. (Alsanea, et al, 2000).
38
Side effects and complications of radio-active iodine I131
treatment and how to overcome:-
Acute radiation thyroiditis
Is very rare after I131
therapy of Graves’ disease. It is painful and
similar to subacute thyroiditis, with referral of the pain to the jaws and
ears. Anti-inflammatory medication or a short course of corticosteroids
is of value. (Kadman, et al, 2001).
Thyroid storm
Can occur several days after therapy and is more common in older
patients and those with severe disease—hence, the recommendation
for the pretreatment of these patients with anti-thyroid drugs.
(Kadman, et al, 2001).
There are rare reports of a thyroid crisis in children (Kadman, et al,
2001).
These data further support the argument for first rendering severely
thyrotoxic patients and those at most risk euthyroid by medical
therapy. (Ron, et al, 1998).
Salivary Gland Dysfunction
Sialoadenitis is a direct result of radiation injury from active iodine
uptake into the gland 20 to 100 times that of plasma. (Mandel, et al,
2003).
The incidence of acute radiation sialoadenitis with swelling and pain is
widely variable, reported in between 12% and 67% of patients after RAI
treatment. (Caglar, et al, 2002).
39
Sialoadenitis can be prevented with lower activities of prescribed I
131,
good hydration, and use of sialogogues. (Van Nostrand , et al, 2009).
Quantitative studies have shown that radiation within the parotid
decreased rapidly after induction of salivary gland secretion with lemon
juice. (Van Nostrand , et al, 2009).
Stomatitis
Occasionally acute stomatitis is seen, which is thought to be the
result of mucosal radiation from the I131
secreted into saliva. many
experts have seen this complication 5 to 7 days after therapy.
Symptoms can be controlled with an elixir mouthwash containing
dexamethasone, viscous lidocaine, diphenhydramine, and aluminum
and magnesium hydroxide. (Mandel, et al, 2003).
Taste Changes
Loss of taste or altered taste is thought to be caused by radiation
destruction of lingual taste buds from the RAI secreted into saliva. (
Mendoza, et al, 2004 and Kita, et al, 2004).
Gastrointestinal Complications
Nausea is the most common gastrointestinal symptom of RAI therapy
but is rarely accompanied by emesis. ( Mendoza, et al, 2004).
Studies have shown that 50% to 67% of patients complain of nausea
starting as early as 2 hours after treatment and lasting up to 2 days
after therapy. (Maenpaa, et al, 2008).
Antiemetics can be given intravenously to patients with severe
symptoms to prevent emesis and allow oral hydration. (Lassmann, et
al, 2010).
40
Gonadal Radiation and Fertility
The gonads receive radiation from the free and iodinated proteins
circulating in blood and from the urinary excretion of the RAI. Gonadal
exposure in the first 3 days after RAI treatment can be reduced with
good hydration and frequent urination. (Hyer, et al, 2002).
The biochemical abnormalities (elevated luteinizing hormone, low
testosterone) usually resolved within 18 months after I131
treatment
with less than 150 mCi, but the risk for persistent gonadal dysfunction
increased after a repeated or high cumulative dose of RAI, male fertility
is not significantly affected by a single lower dose of RAI. (Sawka, et al,
2008).
RAI effects on female fertility have been examined carefully. Transient
amenorrhea or oligomenorrhea has been reported after RAI. (Vini, et
al, 2002).
Additional small clinical observational studies confirm that female
fertility, pregnancies, and babies’ health are not affected by prior high-
dose radioiodine treatment. (Bal, et al, 2005).
Bone Marrow Suppression
Asymptomatic transient drops in white blood cell, red blood cell, and
platelet counts are seen with usual doses of I131
. (Sisson, et al, 2001).
41
LITHIUM AS ADJUVANT TO I131
Lithium reduces the release of thyroid hormones from the thyroid
and has been used alone to treat hyperthyroidism.
Lithium has also been used as an adjuvant to I131
by retaining the
radionuclide within the gland and delivering more radiation with a
smaller administered dose. (Bogazzi, et al, 1999).
RADIATION SAFETY
When a patient is treated with I131
and released, it is important that
members of the public, including the family, are not exposed to
significant radiation.
Family members have confirmed that simple measures, such as
sleeping in a separate bedroom and remaining more than 2 meters
from family members for a few days, ensure that the regulations are
fulfilled (Cappelen, et al, 2006).
In 1 investigation, the maximum exposure to a family member from
the treatment of Grave’s disease was 2.4 mSv (240 mrem); when
detailed instructions were given, this exposure was reduced to 1.9 mSv
(190mrem) (Pant, et al, 2006).
42
SPECIAL SITUATIONS
Children
Most thyrotoxic children have Graves’ disease (Hung and Sarlis,
2004).
Children are less likely to have infiltrative orbitopathy but
there have been reports of eye disease.(Hung and Sarlis, 2004 and
Wiersinga, 2004).
The incidence of side effects from anti-thyroid medications is higher
in children, and they can be serious (Rivkees, et al, 1998; Birrell and
Cheetham, 2004 and Segni and Gorman, 2001).
Children are less consistent in taking the medications, and the
remission rates are lower. (Barrio, et al, 2005).
When high doses of anti-thyroid medications are required for a long
time, remission is unlikely (Barrio, et al, 2005).
Thyroidectomy is technically more difficult in young children, and
few surgeons are trained in this procedure. As a result, there has been
increasing experience in the role and value of I131
treatment in pediatric
patients (Rivkees, 2003).
Several authorities have promoted the administration of I131
earlier in
the management of pediatric patients and even as the primary
treatment. Children as young as 3 years can be treated (Rahman, et al,
2003).
Some children have relatively large goiters, and the size can be
calculated from length, width, and depth measurements obtained by
43
ultrasound. This calculation provides a more exact size for treatment
based on a dose per gram corrected for percentage uptake. (Rahman,
et al, 2003).
Pregnancy
Graves’ disease occurs in young women, and a patient may become
pregnant before, coincidentally with, or after the diagnosis (Chen and
Khoo, 2002 and Perros, 2005).
The maternal thyroid dysfunction, the presence of TSI (thyroid
stimulating immunoglobulin), and the management of the condition
can all affect the fetus. Usually, the treatment consists of anti-thyroid
medications, but maternal allergy to the medications presents a
difficult management problem (Cho and Shon, 2005).
Methimazole administered to the mother has been reported to cause
aplasia cutis (a scar like lesion of the scalp) and recently was linked to
choanal atresia in offspring. (Barbero, et al, 2004 and Foulds, et al,
2005).
Therefore, propylthiouracil is preferred. (Luton, et al, 2005)
It is very important to ensure that the mother does not receive
diagnostic or therapeutic radioiodine when pregnant. There should be a
mechanism to ensure that all women about to be tested with radio
nuclides of iodine are asked about the possibility of pregnancy and that
all women who are to be treated have a negative pregnancy test. (Cho
and Shon, 2005).
After 11 weeks, the fetal thyroid concentrates iodine, and if the fetus
is exposed, it will be born a thyrotic (Cho and Shon, 2005).
44
Exposure of the fetus also reduces the intelligence quotient by 30
points per gray (100 rads) and introduces a slightly increased cancer
risk. (Mc Dougall, 2006).
When exposure occurs in the first trimester, the risk of neonatal
hypothyroidism is reduced considerably however; every effort should
be made to ensure that such exposure does not occur. (Berlin, 2001).
Thyroid Eye Disease
Eye disease is seen only in patients with autoimmune thyroid disease,
such as Graves’ disease. (Wiersinga, 2005; Bartalena, et al, 2005 and
Wiersinga, 2004).
Correction of both hyperthyroidism and hypothyroidism is important
for the ophthalmopathy. Anti-thyroid drugs and thyroidectomy do not
influence the course of the ophthalmopathy, whereas radioiodine
treatment may exacerbate preexisting ophthalmopathy but can be
prevented by glucocorticoids. In the long term, thyroid ablation may be
beneficial for ophthalmopathy because of the decrease in antigens
shared by the thyroid and the orbit in the autoimmune reactions. In
general, treatment of hyperthyroidism is associated with an
improvement of ophthalmopathy, but hypothyroidism must be avoided
because it worsens ophthalmopathy.( Bartalena, et al, 2004).
For mild-to-moderate ophthalmopathy, local therapeutic measures
(e.g., artificial tears and ointments, sunglasses, eye patches, nocturnal
taping of the eyes, elevating the head at night) can control symptoms
and signs.
45
If the disease is active, the mainstays of therapy are high-dose
glucocorticoids. (Macchia, et al, 2001).
The antioxidant selenium (200 mcg daily) was shown in one study to
help patients with mild Grave's orbitopathy. (Marcocci, et al, 2011).
Systemic steroids are usually reserved for patients with severe
inflammation or compressive optic neuropathy in thyroid-associated
orbitopathy (TAO). The consensus statement of the European Group on
Grave's orbitopathy (EUGOGO) suggests intravenous glucocorticoids for
patients with advanced thyroid-associated orbitopathy. (Bartalena, et
al, 2008).
If no response to therapy occurs in the inflammatory phase, orbital
radiotherapy with or without steroids may be tried. (Wakelkamp, et al,
2004).
Orbital irradiation is sometimes prescribed for moderate to severe
inflammatory symptoms, diplopia, and visual loss in patients with
thyroid-associated orbitopathy (TAO). The radiation (1500-2000 cGy
fractionated over 10 days) is usually administered via lateral fields with
posterior angulation. Radiation is believed to damage orbital fibroblasts
or perhaps lymphocytes. (Gorman, et al, 2001).
The radiation requires several weeks to take effect, and it may
transiently cause increased inflammation. Thus, most patients are
maintained on steroids during the first few weeks of treatment. In
addition, better response to radiation is observed in patients with
active inflammation who are treated within 7 months of the onset of
thyroid-associated orbitopathy. Radiation may be more effective if
combined with steroid treatment. (Gorman, et al, 2001).
46
Orbital radiotherapy does not increase the risk for radiation-induced
tumors, cataract, and retinopathy, except in patients with diabetes with
possible or definite retinopathy. (Wakelkamp, et al, 2004).
Orbital decompression by resecting orbital fat was found to reduce
proptosis in patients with disfiguring Grave's ophthalmopathy.
(Wakelkamp, et al, 2004)
A study by Liao and Huang 2011 evaluated the correlation of retro
bulbar volume change, resected orbital fat volume, and proptosis
reduction after surgical decompression in patients with Grave's
ophthalmopathy.
Orbital irradiation, orbital decompression & glucocorticoids at 40
mg/d (usual dose) may be tried in severe or progressive disease. The
drug should be continued until evidence of improvement and disease
stability is observed. The dosage is then tapered over 4-12 weeks. High-
dose pulse glucocorticoid therapy has also been used with good results.
(Liao, et al, 2011).
Gamma knife surgery has been attempted with success in a limited
number of patients, but further studies are needed to validate this
approach. ( Dickinson, et al, 2004; Wemeau, et al. 2005 and Stan, et
al, 2006).
Surgical management is generally performed in the fibrotic phase,
when the patient is euthyroid. ( Dickinson, et al, 2004; Wemeau, et al.
2005 and Stan, et al, 2006).
Novel treatments such as somatostatin analogs or intravenous
immunoglobulins are under evaluation. Studies with octreotide LAR
(long-acting, repeatable) show conflicting or marginal therapeutic
47
benefit for patients with Grave's ophthalmopathy. ( Dickinson, et al,
2004; Wemeau, et al. 2005 and Stan, et al, 2006).
Infliximab, an anti-tumour necrosis factor alpha (TNF-α) antibody, has
been reported to successfully treat a case of sight-threatening Grave's
ophthalmopathy. (Durrani, et al, 2005).
Chronic Renal Failure and Dialysis Patients
Administered iodine that is not trapped in the thyroid gland is cleared
from the body largely by renal excretion.
Thus, the selection of a dose for I131
therapy can be a challenging
decision in patients with impaired renal function.
Holst et al 2005. reviewed the medical literature and concluded that
the I131
dose does not need to be adjusted in patients who have end-
stage renal disease and who are referred for the therapy of
hyperthyroidism.
However, they recommended I131
administration as soon as possible
after dialysis and a delay in subsequent dialysis until the maximum I131
uptake has occurred in the thyroid. (Holst, et al, 2005).
The radiation dose to the technician in the dialysis unit should be
monitored, and the patient should undergo dialysis in a private room.
(Mello, et al, 1994).
Equipment and fluid disposed from the dialysis unit should be
monitored by radiation safety personnel, but they did not find any
contamination in a patient treated for thyroid cancer (Mello, et al,
1994).

48
Care after radioactive Iodine ablation Follow-up examination at 4- to 6-week intervals is advised for patients
after the completion of radioactive iodine therapy. These checkups
should be continued until patients return to their euthyroid state and
their condition stabilizes. (Wilson, et al, 1998 and Franklyn, 1994).
Since the adverse effect of radioactive iodine therapy is permanent
hypothyroidism, patients may require lifelong thyroid hormone
replacement therapy. (Wilson, et al, 1998 and Franklyn, 1994).
Even though signs and symptoms of hypothyroidism begin to appear
3 months after the initiation of radioactive iodine therapy, thyroid
hormone replacements of levothyroxine should be initiated in the
second month of radioactive iodine therapy. (Wilson, et al, 1998 and
Franklyn, 1994).
The decision to initiate hormonal replacement should be based on
clinical evaluation and laboratory testing. This is because during the
second month of radioactive therapy, the thyroid gland quickly changes
from a euthyroid to a hypothyroid state. At this stage, the TSH level is
not a good tool to use in determining hypothyroidism, as it takes about
2 weeks to several months to recover and increase TSH concentration
in response to hypothyroidism. (Wilson, et al, 1998 and Franklyn,
1994).
During this period, free thyroid hormone estimates are more accurate
than TSH values. Once the patient’s condition stabilizes, the frequency
of clinic visits can be decreased and intervals of examination can be
extended and modified per the physician’s judgment. Usually, the
follow-up consultations are conducted every 3 months, 6 months, and
yearly. (Wilson, et al, 1998 and Franklyn, 1994).
49
PATIENT METHODS& DATA COLLECTION
• Case selection:-
The study population consisted of 200 cases with previous
thyroid gland troubles seen at Nuclear Medicine Unit (NEMROCK),
Cairo University during the period of January 2008 till December
2010.They were 120 female and 80 male.
Inclusion criteria
• Primary and secondary type of thyrotoxicosis.
• Different sex.
• Different age groups.
• Different duration of symptoms.
• Different methods& duration of treatment.
• Different responses to treatment.
-:They all were subjected to
• History taking:
Including age, sex, symptoms, duration of illness, type and
response to treatment.
• Clinical examination:-
Looking for gland size, consistency, nodularity & other neck swellings,
Eye signs examination.
50
• Laboratory investigations:-
Including T3, T4, TSH levels and antibodies.
• Neck ultrasound:-
To detect size, nodularity & other neck swellings.
• Radio –nuclear imaging :-
technetium-99m pertecnetate (Tc 99m
) thyroid scan to detect
size ,nodules , gland uptake & Radio-active iodine( I 131
)scan to
detect retrosternal extension before treatment.
• Treatment :-
Either in the form of medical treatment, surgery, or Radio-active
Iodine treatment.
• Follow up:-
By measuring T3, T4, and TSH levels recently after treatment then
after 3 months, 6 months then every year till patient becomes
euthyroid.
• Data collection
Retrospective data analysis of 200 cases of thyrotoxicosis with
primary and secondary types, age groups, sex, duration of illness,
methods of treatment and response to treatment seen at Nuclear
Medicine Unit between January 2008 to December 2010.
-:and conclude the relationship between
• Age group and type of thyrotoxicosis.
51
• Sex of patient and type of thyrotoxicosis.
• Percentage of thyroid uptake and response to Radio- active iodine
dose.
• Most predominant symptoms in each type of thyrotoxicosis.
• Thyroid hormone levels and the type of thyrotoxicosis.
• Type of treatment of each type of thyrotoxicosis.
• Response to different dose values of Radio- active iodine.
• Relationship between dose value of Radio -active iodine and onset
of hypothyroidism.
52
Statistical analysis
Statistical analysis was done using the Statistical Package of Social
Sciences (SPSS) version 17.00.
Data were assigned as parametric, nonparametric , parametric data
were analyzed using the Independent sample T test if it were two
groups, and one way analysis of variance ANOVA if more than two
groups.
Non parametric data were analyzed using the non parametric Man
Whtney U test, and Kruskal Wallis test for more than two groups.
Nominal data were analyzed using the Chi Square analysis.
Correlation analysis were conducted using the spearman correlation
coefficient where stated.
A P value of < 0.05 was considered significant in some instances, and
<0.001 in other instances.
53
RESULTS
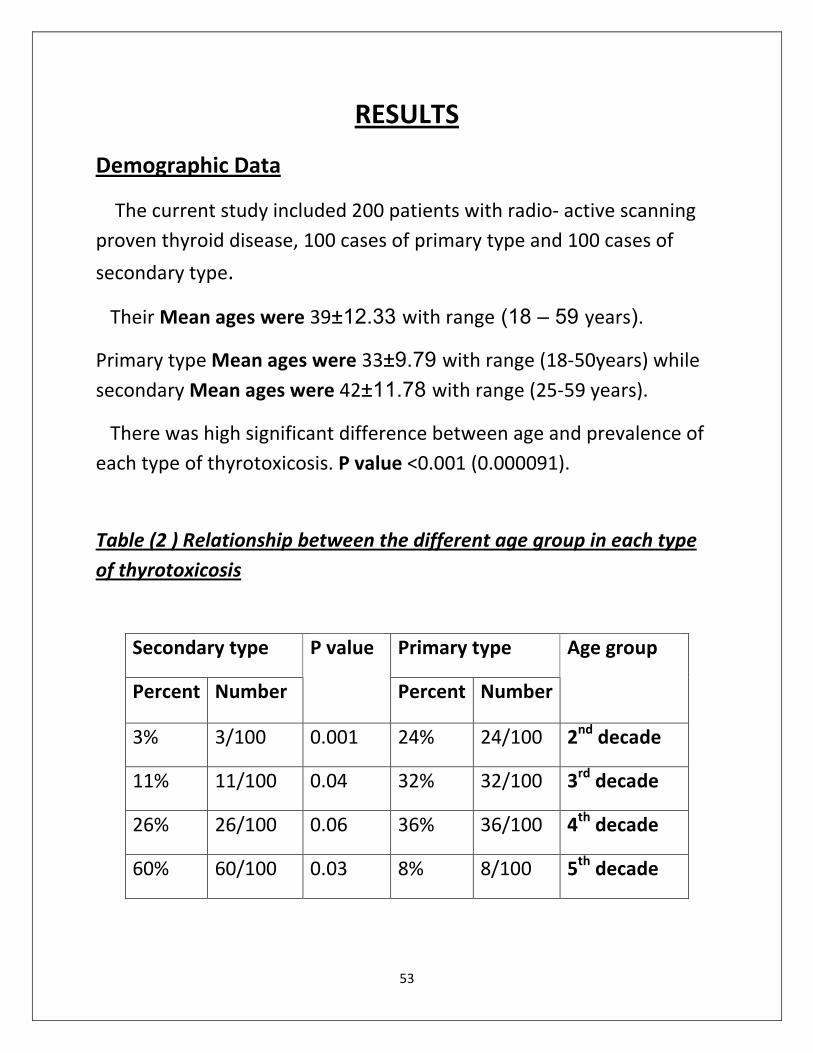
Demographic Data
The current study included 200 patients with radio- active scanning
proven thyroid disease, 100 cases of primary type and 100 cases of
secondary type.
Their Mean ages were 39±12.33 with range (18 – 59 years).
Primary type Mean ages were 33±9.79 with range (18-50years) while
secondary Mean ages were 42±11.78 with range (25-59 years).
There was high significant difference between age and prevalence of
each type of thyrotoxicosis. P value <0.001 (0.000091).
Relationship between the different age group in each type ) 2 (Table
of thyrotoxicosis
Secondary type Primary type
Percent Number
P value
Percent Number
Age group
3% 3/100 0.001 24% 24/100 2nd
decade
11% 11/100 0.04 32% 32/100 3rd
decade
26% 26/100 0.06 36% 36/100 4th
decade
60% 60/100 0.03 8% 8/100 5th
decade
54
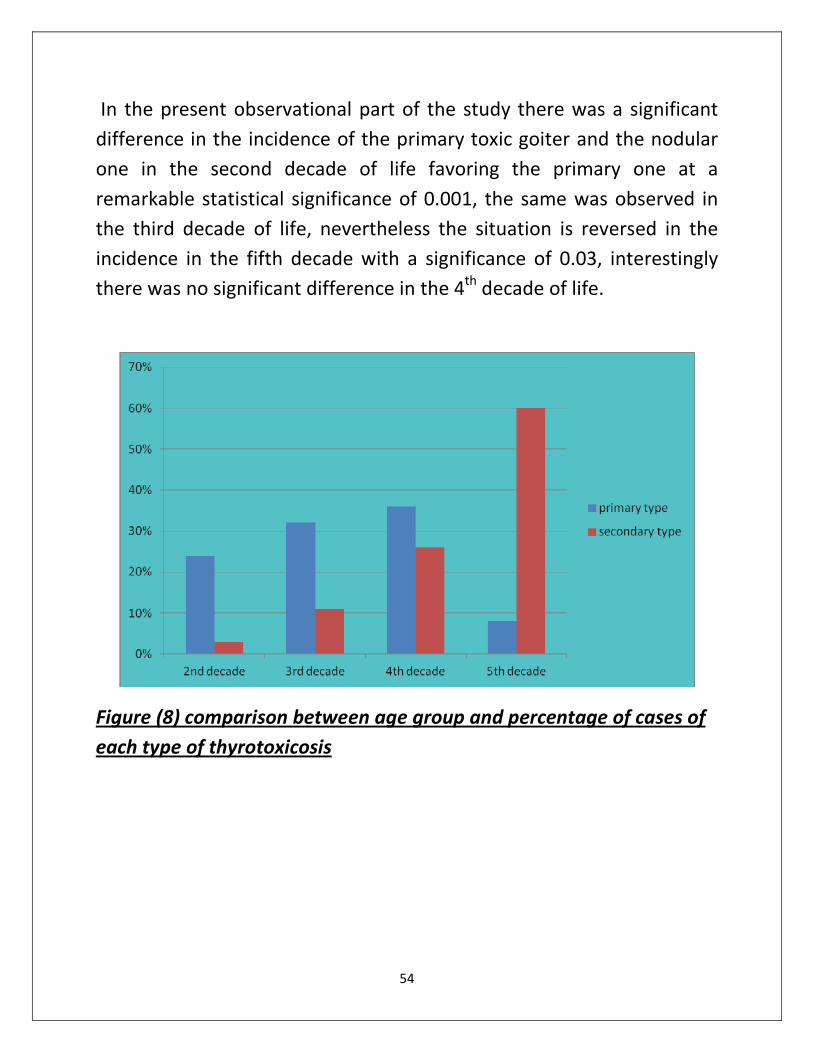
In the present observational part of the study there was a significant
difference in the incidence of the primary toxic goiter and the nodular
one in the second decade of life favoring the primary one at a
remarkable statistical significance of 0.001, the same was observed in
the third decade of life, nevertheless the situation is reversed in the
incidence in the fifth decade with a significance of 0.03, interestingly
there was no significant difference in the 4th
decade of life.
Figure (8) comparison between age group and percentage of cases of
each type of thyrotoxicosis
55
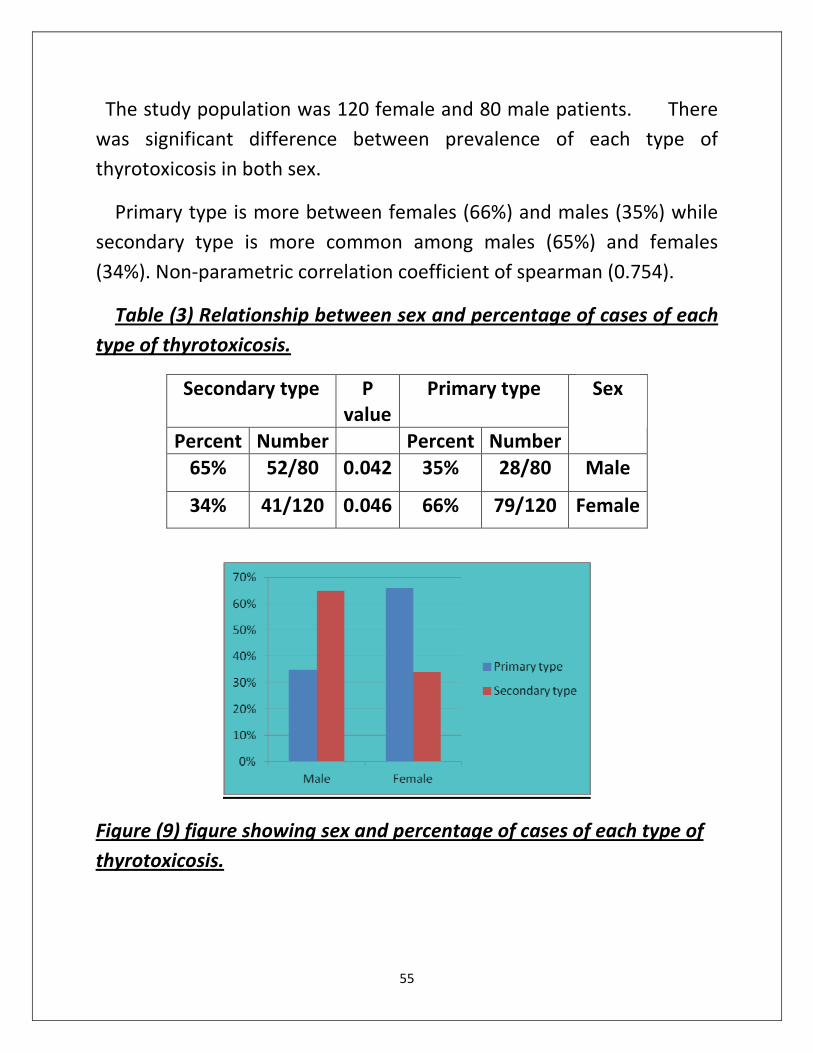
The study population was 120 female and 80 male patients. There
was significant difference between prevalence of each type of
thyrotoxicosis in both sex.
Primary type is more between females (66%) and males (35%) while
secondary type is more common among males (65%) and females
(34%). Non-parametric correlation coefficient of spearman (0.754).
Table (3) Relationship between sex and percentage of cases of each
type of thyrotoxicosis.
Secondary type P
value
Primary type
Percent Number Percent Number
Sex
65% 52/80 0.042 35% 28/80 Male
34% 41/120 0.046 66% 79/120 Female
figure showing sex and percentage of cases of each type of ) 9(Figure
.thyrotoxicosis
56
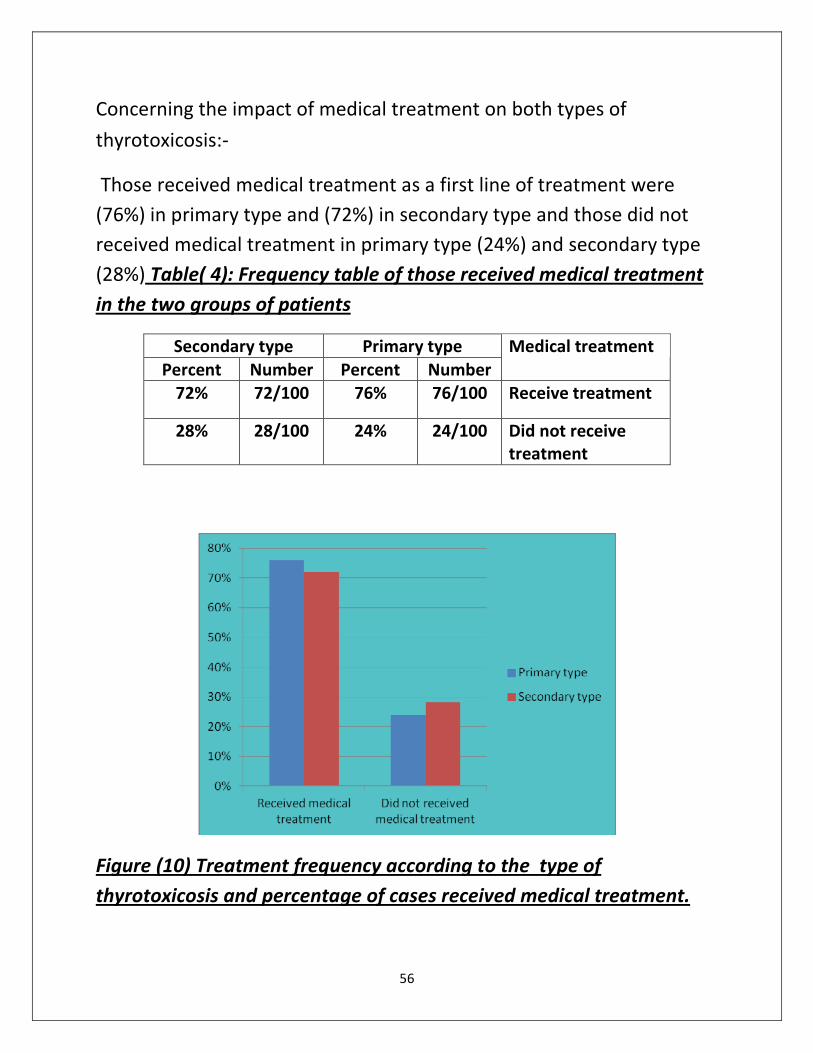
Concerning the impact of medical treatment on both types of
thyrotoxicosis:-
Those received medical treatment as a first line of treatment were
(76%) in primary type and (72%) in secondary type and those did not
and secondary type %) 24(received medical treatment in primary type
al treatment Frequency table of those received medic): 4( Table %)28(
in the two groups of patients
Secondary type Primary type
Percent Number Percent Number
Medical treatment
72% 72/100 76% 76/100 Receive treatment
28% 28/100 24% 24/100 Did not receive
treatment
Figure (10) Treatment frequency according to the type of
thyrotoxicosis and percentage of cases received medical treatment.
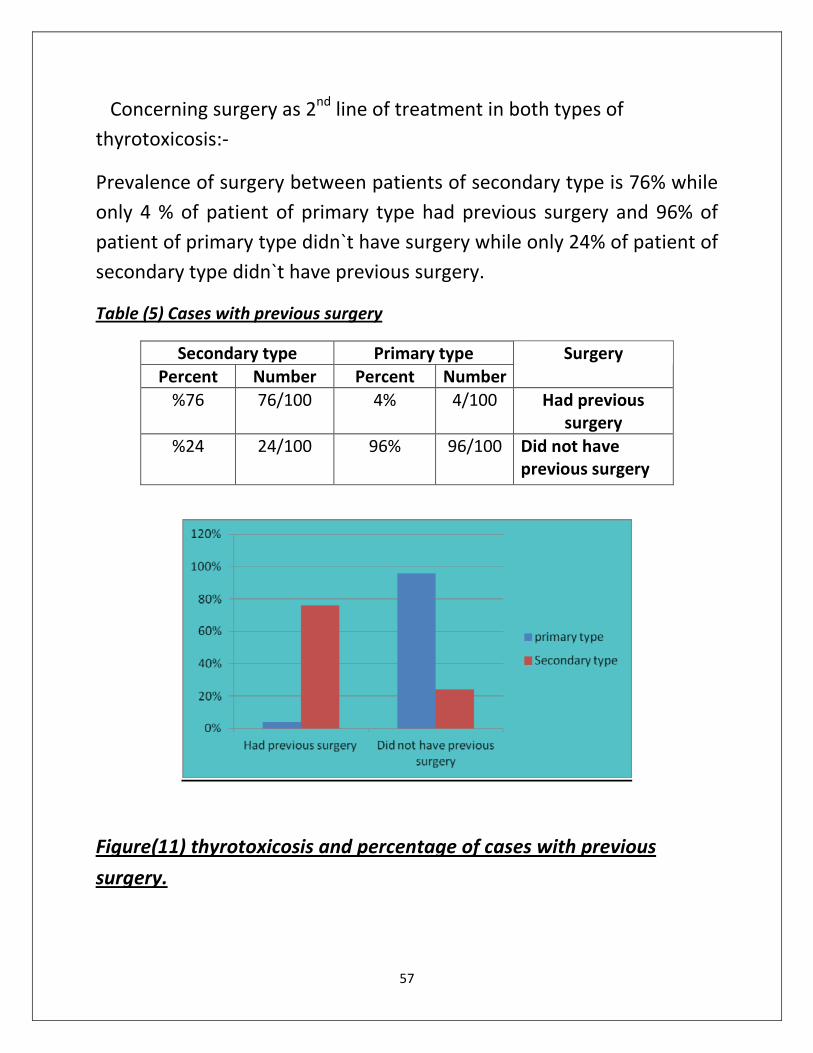
57
Concerning surgery as 2nd
line of treatment in both types of
thyrotoxicosis:-
Prevalence of surgery between patients of secondary type is 76% while
only 4 % of patient of primary type had previous surgery and 96% of
patient of primary type didn`t have surgery while only 24% of patient of
secondary type didn`t have previous surgery.
Cases with previous surgery) 5(Table
Secondary type Primary type
Percent Number Percent Number
Surgery
%76 76/100 4% 4/100 Had previous
surgery
%24 24/100 96% 96/100 Did not have
previous surgery
thyrotoxicosis and percentage of cases with previous ) 11(Figure
.surgery
58
The most common symptoms were palpitation, tachycardia, loss of
weight, tremors, nervousness, heat intolerance and neck swelling.
The most common symptoms in Graves' disease were tachycardia,
anxiety, loss of weight, tremors, heat intolerance and neck swelling.
The most common symptoms in Toxic nodular type were tachycardia,
palpitation and dyspnea.
Table (6) shows the predominant symptoms in each type of
thyrotoxicosis
The most common symptoms Type of
thyrotoxicosis
Tachycardia, anxiety, loss of weight,
tremors, heat intolerance and neck
swelling.
Graves' disease
Tachycardia, palpitation and dyspnea Toxic nodular type
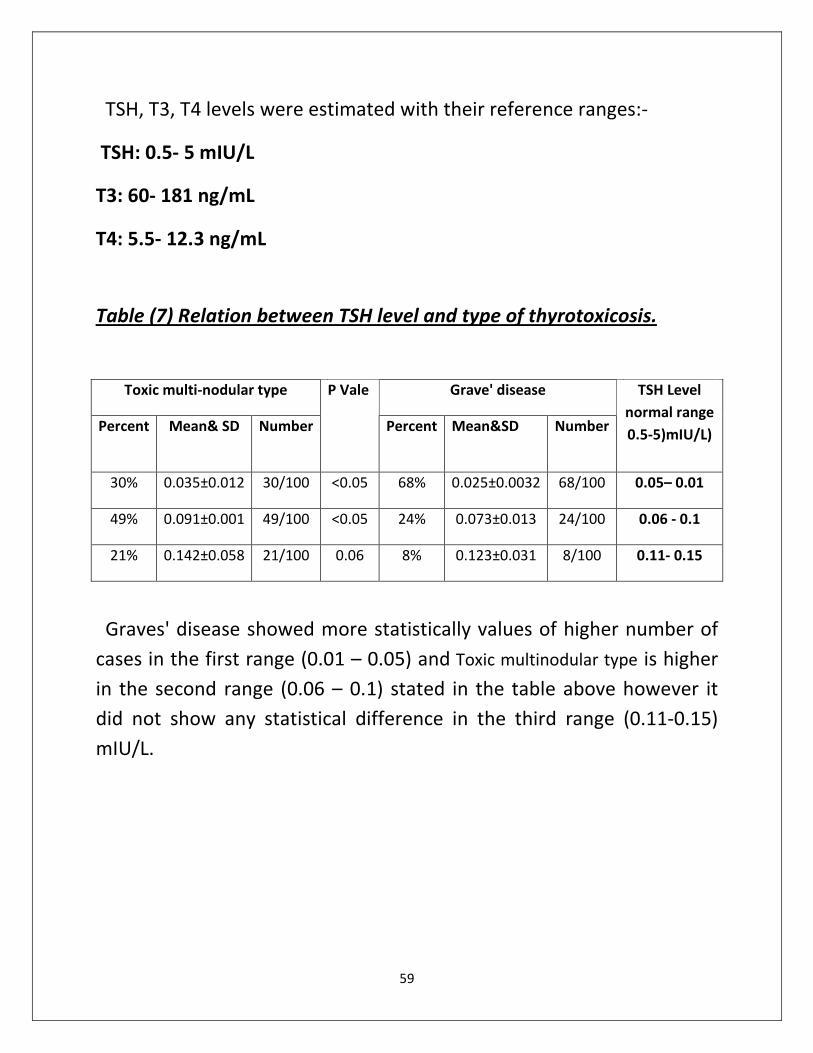
59
TSH, T3, T4 levels were estimated with their reference ranges:-
TSH: 0.5- 5 mIU/L
T3: 60- 181 ng/mL
T4: 5.5- 12.3 ng/mL
.Relation between TSH level and type of thyrotoxicosis) 7(Table
Toxic multi-nodular type Grave' disease
Percent Mean& SD Number
P Vale
Percent Mean&SD Number
TSH Level
normal range
0.5-5)mIU/L)
30% 0.035±0.012 30/100 <0.05 68% 0.025±0.0032 68/100 0.05– 0.01
49% 0.091±0.001 49/100 <0.05 24% 0.073±0.013 24/100 0.06 - 0.1
21% 0.142±0.058 21/100 0.06 8% 0.123±0.031 8/100 0.11- 0.15
Graves' disease showed more statistically values of higher number of
cases in the first range (0.01 – 0.05) and Toxic multinodular type is higher
in the second range (0.06 – 0.1) stated in the table above however it
did not show any statistical difference in the third range (0.11-0.15)
mIU/L.
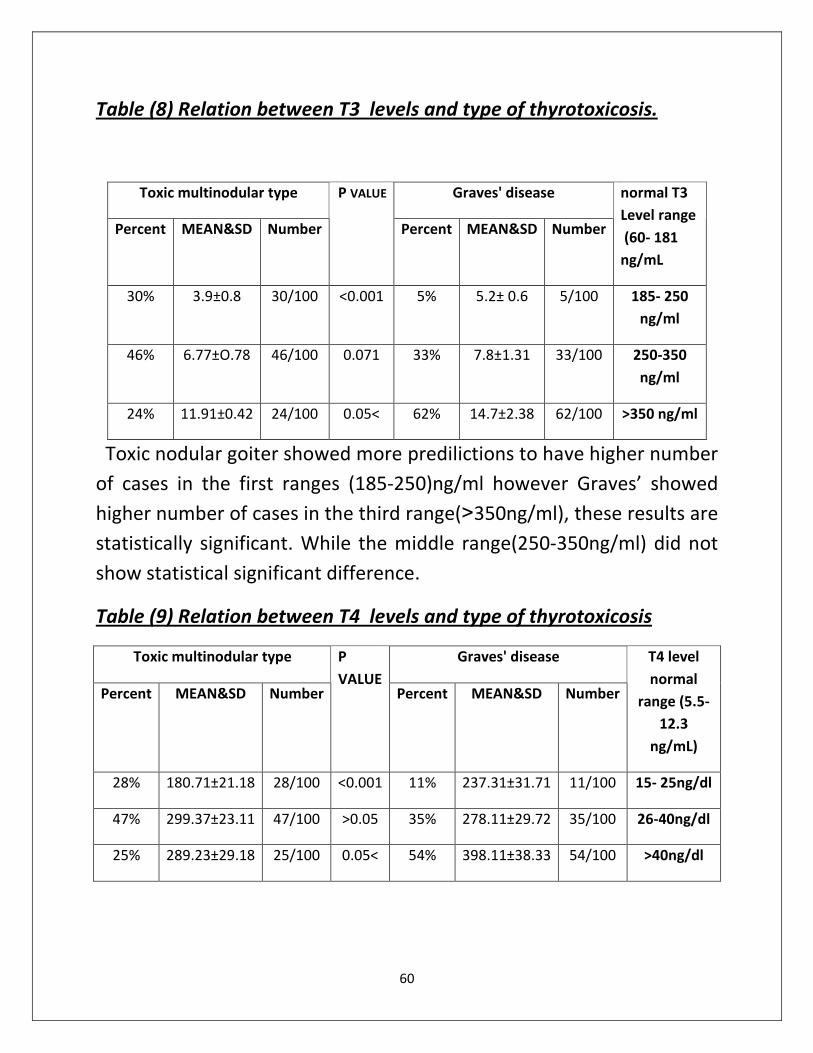
60
Table (8) Relation between T3 levels and type of thyrotoxicosis.
Toxic multinodular type Graves' disease
Percent MEAN&SD Number
P VALUE
Percent MEAN&SD Number
normal T3
Level range
(60- 181
ng/mL
30% 3.9±0.8 30/100 <0.001 5% 5.2± 0.6 5/100 185- 250
ng/ml
46% 6.77±O.78 46/100 0.071 33% 7.8±1.31 33/100 250-350
ng/ml
24% 11.91±0.42 24/100 0.05< 62% 14.7±2.38 62/100 >350 ng/ml
Toxic nodular goiter showed more predilictions to have higher number
of cases in the first ranges (185-250)ng/ml however Graves’ showed
higher number of cases in the third range(>350ng/ml), these results are
statistically significant. While the middle range(250-350ng/ml) did not
show statistical significant difference.
Table (9) Relation between T4 levels and type of thyrotoxicosis
Toxic multinodular type Graves' disease
Percent MEAN&SD Number
P
VALUE Percent MEAN&SD Number
T4 level
normal
range (5.5-
12.3
ng/mL)
28% 180.71±21.18 28/100 <0.001 11% 237.31±31.71 11/100 15- 25ng/dl
47% 299.37±23.11 47/100 >0.05 35% 278.11±29.72 35/100 26-40ng/dl
25% 289.23±29.18 25/100 0.05< 54% 398.11±38.33 54/100 >40ng/dl
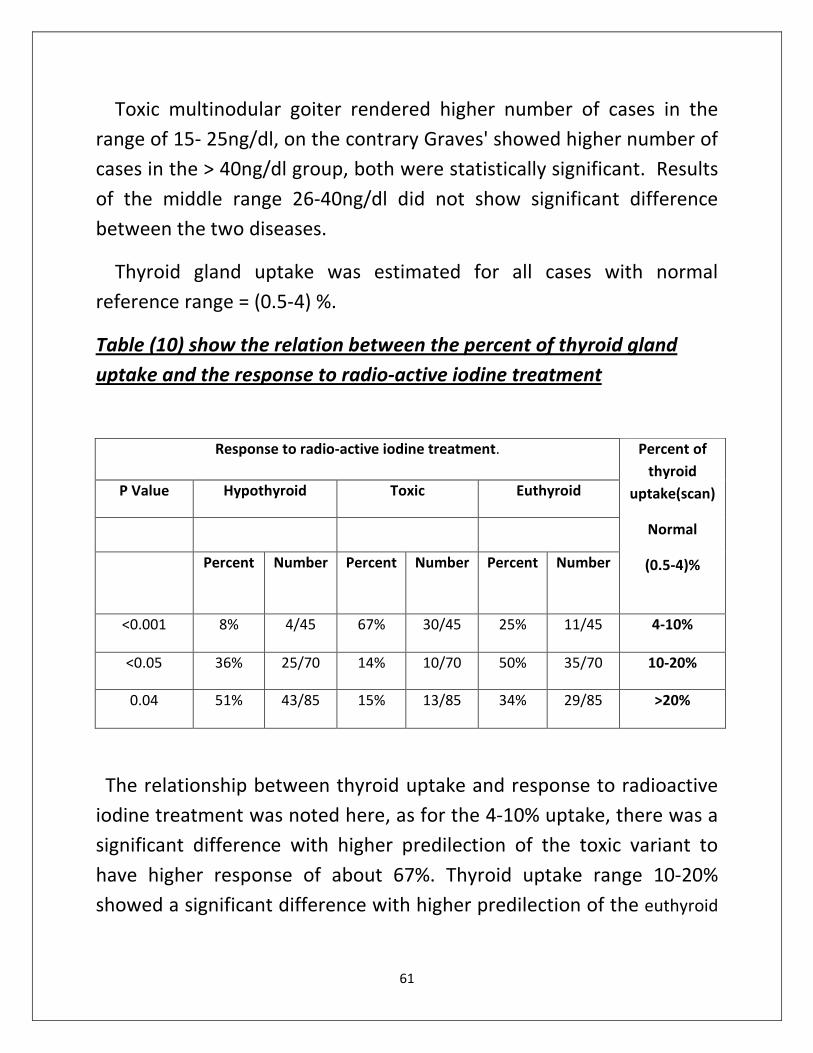
61
Toxic multinodular goiter rendered higher number of cases in the
range of 15- 25ng/dl, on the contrary Graves' showed higher number of
cases in the > 40ng/dl group, both were statistically significant. Results
of the middle range 26-40ng/dl did not show significant difference
between the two diseases.
Thyroid gland uptake was estimated for all cases with normal
reference range = (0.5-4) %.
show the relation between the percent of thyroid gland) 10(Table
active iodine treatment-uptake and the response to radio
Response to radio-active iodine treatment.
P Value Hypothyroid Toxic Euthyroid
Percent Number Percent Number Percent Number
Percent of
thyroid
uptake(scan)
Normal
(0.5-4)%
<0.001 8% 4/45 67% 30/45 25% 11/45 4-10%
<0.05 36% 25/70 14% 10/70 50% 35/70 10-20%
0.04 51% 43/85 15% 13/85 34% 29/85 >20%
The relationship between thyroid uptake and response to radioactive
iodine treatment was noted here, as for the 4-10% uptake, there was a
significant difference with higher predilection of the toxic variant to
have higher response of about 67%. Thyroid uptake range 10-20%
showed a significant difference with higher predilection of the euthyroid
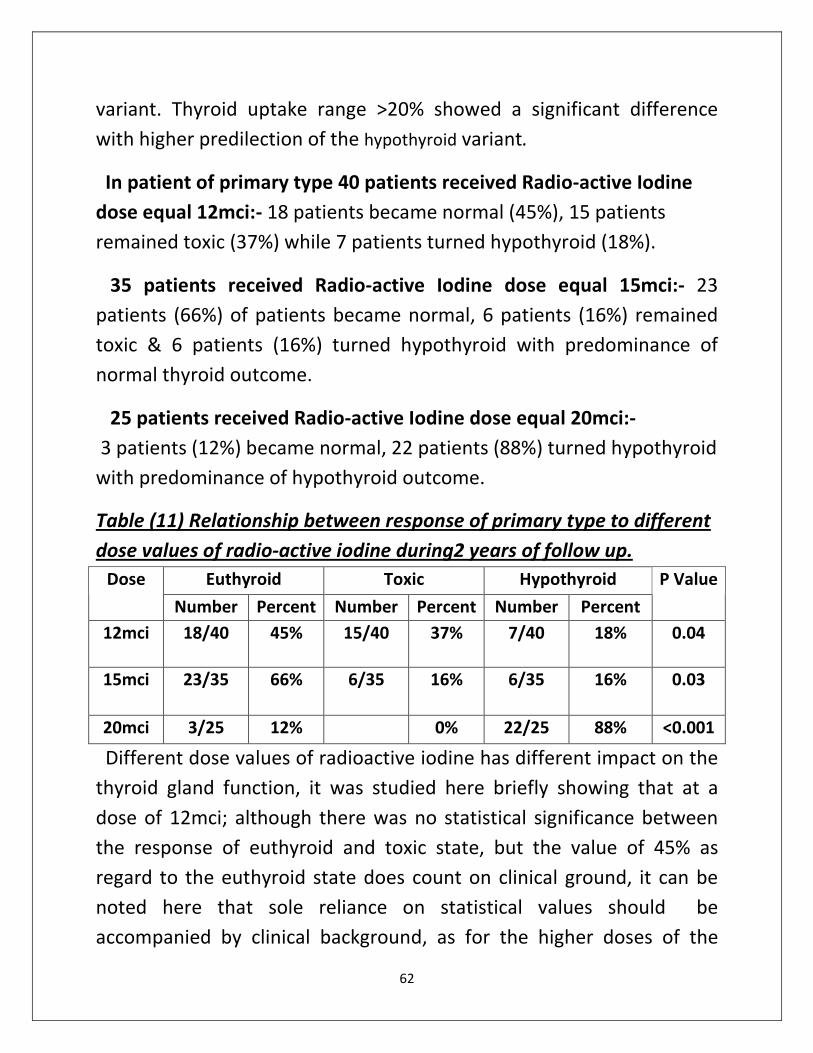
62
variant. Thyroid uptake range >20% showed a significant difference
with higher predilection of the hypothyroid variant.
In patient of primary type 40 patients received Radio-active Iodine
dose equal 12mci:- 18 patients became normal (45%), 15 patients
remained toxic (37%) while 7 patients turned hypothyroid (18%).
35 patients received Radio-active Iodine dose equal 15mci:- 23
patients (66%) of patients became normal, 6 patients (16%) remained
toxic & 6 patients (16%) turned hypothyroid with predominance of
normal thyroid outcome.
25 patients received Radio-active Iodine dose equal 20mci:-
3 patients (12%) became normal, 22 patients (88%) turned hypothyroid
with predominance of hypothyroid outcome.
Table (11) Relationship between response of primary type to different
dose values of radio-active iodine during2 years of follow up.
Euthyroid Toxic Hypothyroid Dose
Number Percent Number Percent Number Percent
P Value
12mci 18/40 45% 15/40 37% 7/40 18% 0.04
15mci 23/35 66% 6/35 16% 6/35 16% 0.03
20mci 3/25 12% 0% 22/25 88% <0.001
Different dose values of radioactive iodine has different impact on the
thyroid gland function, it was studied here briefly showing that at a
dose of 12mci; although there was no statistical significance between
the response of euthyroid and toxic state, but the value of 45% as
regard to the euthyroid state does count on clinical ground, it can be
noted here that sole reliance on statistical values should be
accompanied by clinical background, as for the higher doses of the
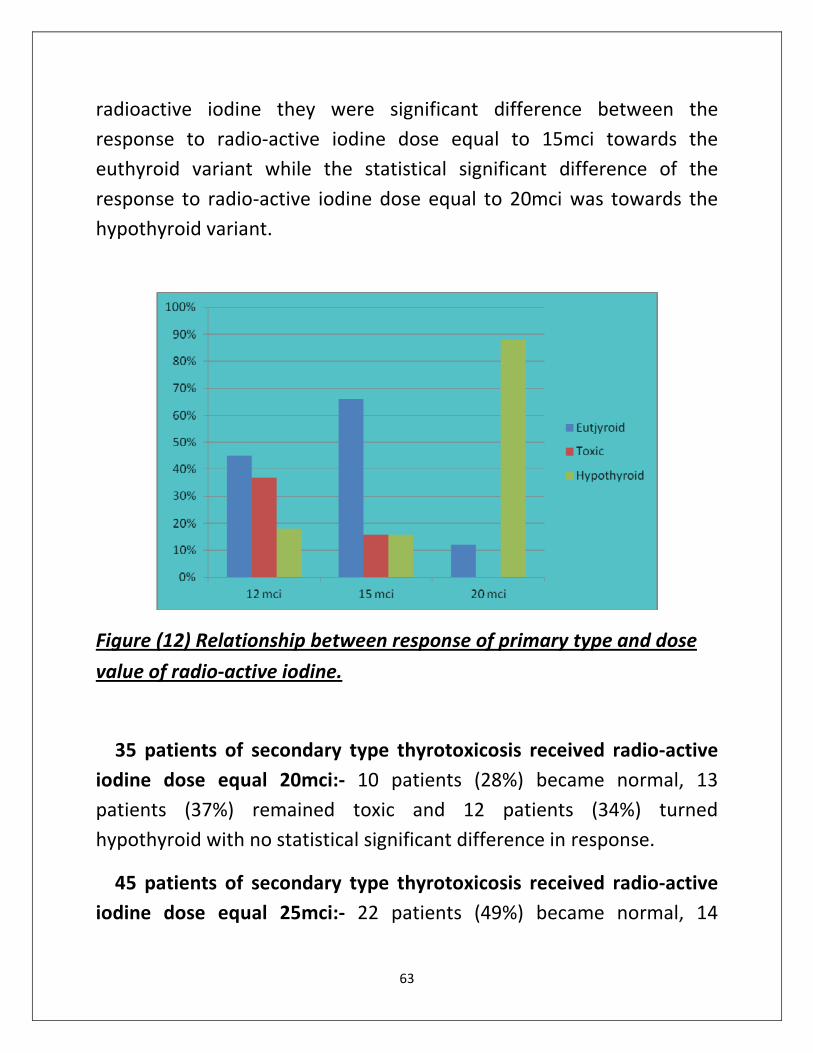
63
radioactive iodine they were significant difference between the
response to radio-active iodine dose equal to 15mci towards the
euthyroid variant while the statistical significant difference of the
response to radio-active iodine dose equal to 20mci was towards the
hypothyroid variant.
Figure (12) Relationship between response of primary type and dose
value of radio-active iodine.
35 patients of secondary type thyrotoxicosis received radio-active
iodine dose equal 20mci:- 10 patients (28%) became normal, 13
patients (37%) remained toxic and 12 patients (34%) turned
hypothyroid with no statistical significant difference in response.
45 patients of secondary type thyrotoxicosis received radio-active
iodine dose equal 25mci:- 22 patients (49%) became normal, 14
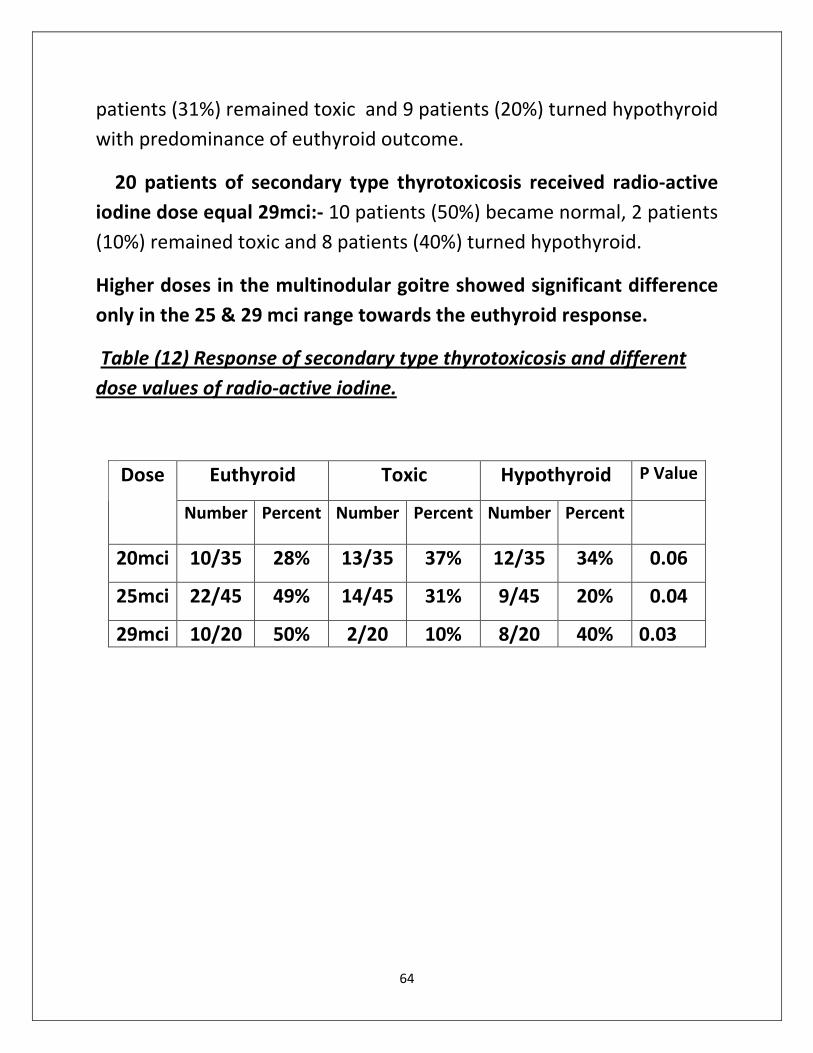
64
patients (31%) remained toxic and 9 patients (20%) turned hypothyroid
with predominance of euthyroid outcome.
20 patients of secondary type thyrotoxicosis received radio-active
iodine dose equal 29mci:- 10 patients (50%) became normal, 2 patients
(10%) remained toxic and 8 patients (40%) turned hypothyroid.
Higher doses in the multinodular goitre showed significant difference
only in the 25 & 29 mci range towards the euthyroid response.
Table (12) Response of secondary type thyrotoxicosis and different
dose values of radio-active iodine.
Euthyroid Toxic Hypothyroid P Value Dose
Number Percent Number Percent Number Percent
20mci 10/35 28% 13/35 37% 12/35 34% 0.06
25mci 22/45 49% 14/45 31% 9/45 20% 0.04
29mci 10/20 50% 2/20 10% 8/20 40% 0.03
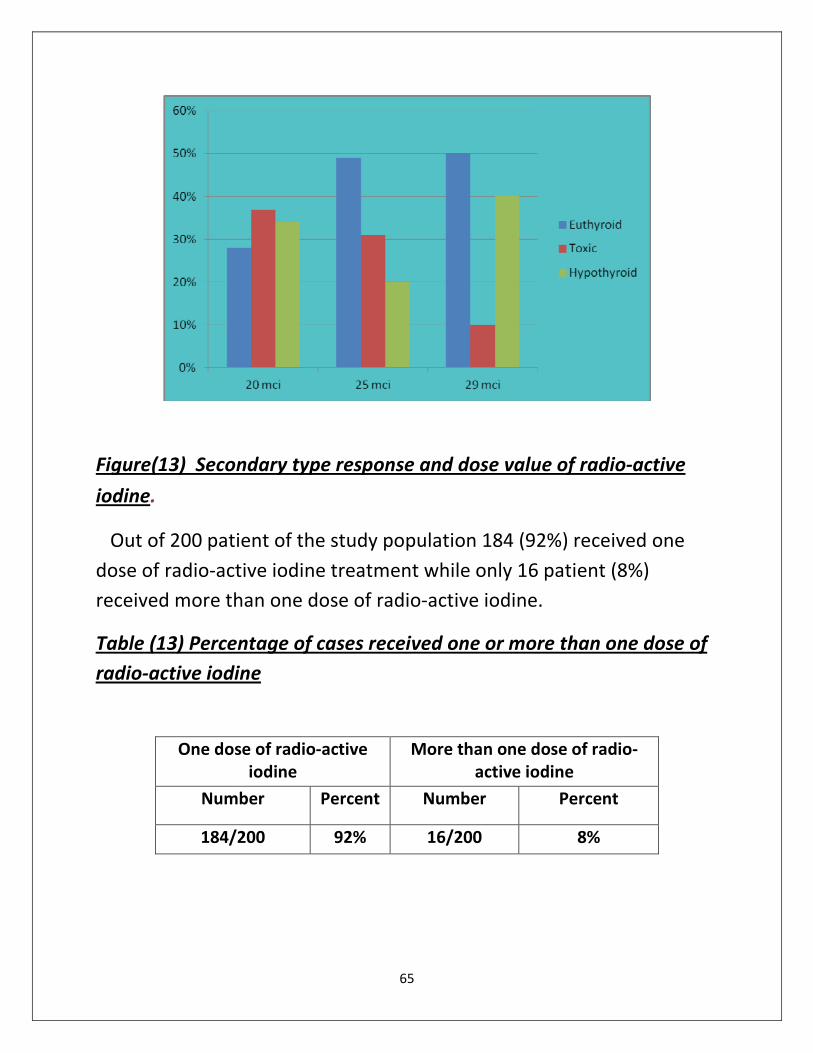
65
Figure(13) Secondary type response and dose value of radio-active
iodine.
Out of 200 patient of the study population 184 (92%) received one
dose of radio-active iodine treatment while only 16 patient (8%)
received more than one dose of radio-active iodine.
Percentage of cases received one or more than one dose of ) 13(Table
active iodine-radio
One dose of radio-active
iodine
More than one dose of radio-
active iodine
Number Percent Number Percent
184/200 92% 16/200 8%
66
active -Percent of cases received one or more dose of radio) 14(Figure
.iodine
Patients turned hypothyroid after radio-active iodine treatment
during 2 years follow up period were:-
7 patients received radio-active iodine of 12mci:- 1 patient (14%)
developed hypothyroid after 6 month, 2 patients (29%) developed
hypothyroid after 12 months& 4 patients (57%) developed hypothyroid
after more than 12 months.
6 patients received radio-active iodine of 15 mci:-1 patient (17%)
developed hypothyroid after 6 month, 2 patients (33%) developed
hypothyroid after 12 months& 3 patients (50%) developed hypothyroid
after more than 12 months.
34 patients received radio-active iodine of 20mci:- 13 patients (38%)
developed hypothyroid after 6 month, 8 patients (24%) developed
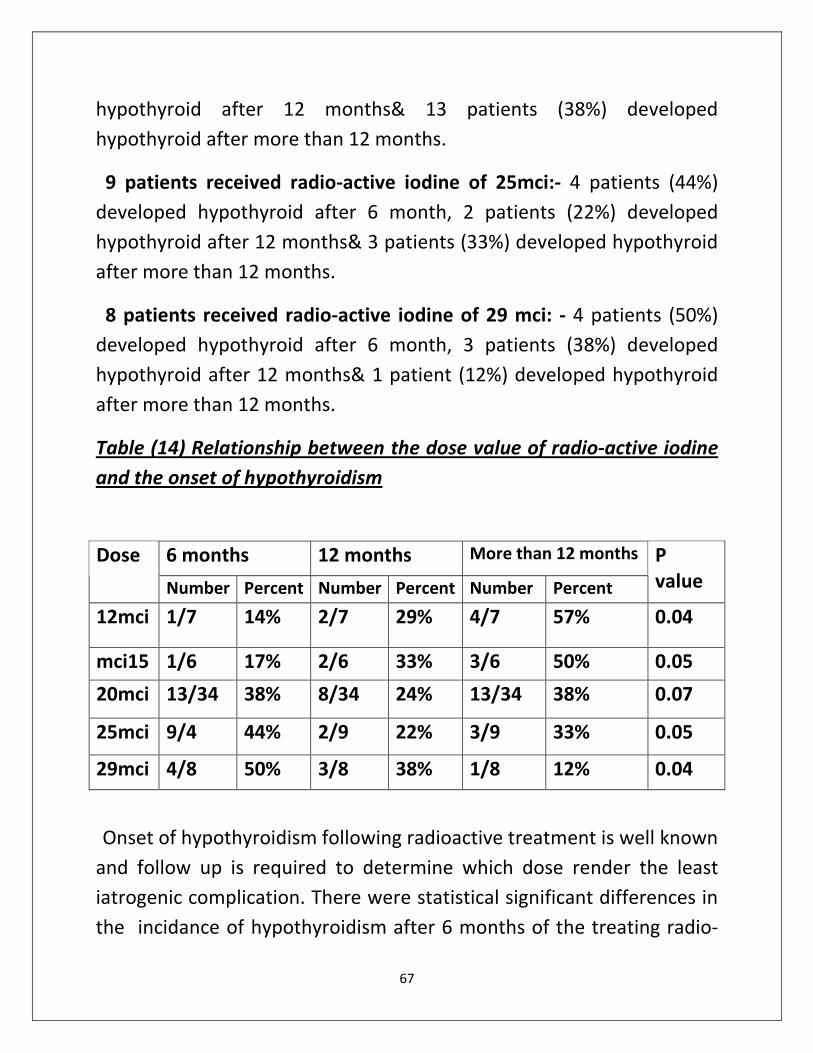
67
hypothyroid after 12 months& 13 patients (38%) developed
hypothyroid after more than 12 months.
9 patients received radio-active iodine of 25mci:- 4 patients (44%)
developed hypothyroid after 6 month, 2 patients (22%) developed
hypothyroid after 12 months& 3 patients (33%) developed hypothyroid
after more than 12 months.
8 patients received radio-active iodine of 29 mci: - 4 patients (50%)
developed hypothyroid after 6 month, 3 patients (38%) developed
hypothyroid after 12 months& 1 patient (12%) developed hypothyroid
after more than 12 months.
Table (14) Relationship between the dose value of radio-active iodine
and the onset of hypothyroidism
6 months 12 months More than 12 months Dose
Number Percent Number Percent Number Percent
P
value
12mci 1/7
14% 2/7 29% 4/7 57% 0.04
mci15 1/6 17% 2/6 33% 3/6 50% 0.05
20mci 13/34 38% 8/34 24% 13/34 38% 0.07
25mci 9/4 44% 2/9 22% 3/9 33% 0.05
29mci 4/8 50% 3/8 38% 1/8 12% 0.04
Onset of hypothyroidism following radioactive treatment is well known
and follow up is required to determine which dose render the least
iatrogenic complication. There were statistical significant differences in
the incidance of hypothyroidism after 6 months of the treating radio-
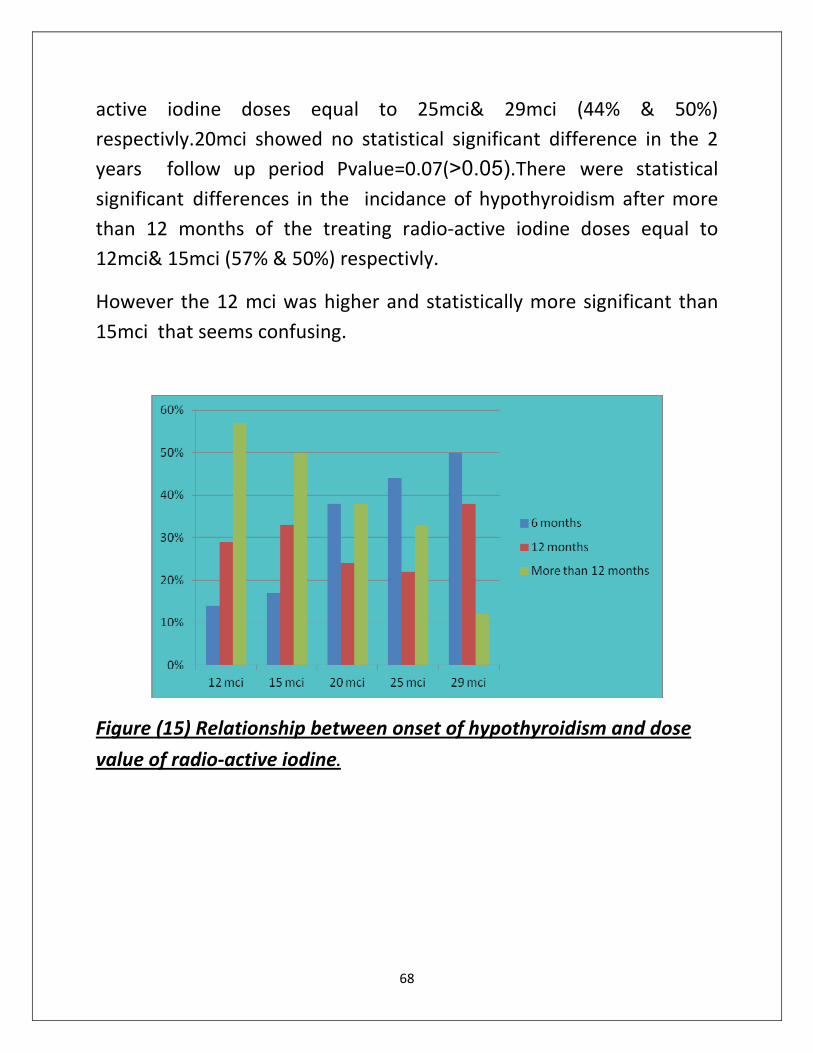
68
active iodine doses equal to 25mci& 29mci (44% & 50%)
respectivly.20mci showed no statistical significant difference in the 2
years follow up period Pvalue=0.07(>0.05).There were statistical
significant differences in the incidance of hypothyroidism after more
than 12 months of the treating radio-active iodine doses equal to
12mci& 15mci (57% & 50%) respectivly.
However the 12 mci was higher and statistically more significant than
15mci that seems confusing.
Figure (15) Relationship between onset of hypothyroidism and dose
value of radio-active iodine.
69
Discussion
The current study included 200 patients with laboratory data and
radio- active scanning proven thyrotoxic, 100 cases of primary type and
100 cases of secondary type. Their Mean ages were 39 ± 12.33 with
range (18 – 59 years).
Primary type Mean ages were 33± 9.79 with range (18-50) while
secondary type Mean ages were 42±11.78 with range (25-59 years).
There was high significant difference between age and prevalence of
each type of thyrotoxicosis. (P value < 0.001(0.000091)).
In the present observational part of the study there was a significant
difference in the incidence of the primary toxic goiter and the nodular
one in the second decade of life favoring the primary one at a
remarkable statistical significance of 0.001, the same was observed in
the third decade of life, nevertheless the situation is reversed in the
incidence in the fifth decade with a significance of 0.03, interestingly
there was no significant difference in the 4th
decade of life.
The peak age-specific incidence of Graves' disease was between 20
and 49 years in two studies, (Zimmerman, 2009).
The incidence of thyrotoxicosis increased with age, and women were
affected two to eight times more than men across the age range.
Recent further analysis suggested that the incidence of thyrotoxicosis
was increasing in women but not in men between 1997 and 2001.
(Leese, et al, 2008).
The study population was 120 female and 80 male patients; Primary
type is more between females (66%) and males (35%) while secondary
70
type is more common among males (65%) and females (34%). Non-
parametric correlation coefficient of spearman (0.754)
Women have a higher reported incidence of Graves’ disease than
men, with a female to male incidence ratio of approximately 7:1 to 10:1
as confirmed by (Nayak and Hodak, 2007).
According to (Basaria and Salvatori, 2004), toxic nodular goiter
occurs more commonly in women than men. In women and men older
than 40 years the prevalence rate of palpable nodules is 5-7% and 1-2%
respectively.
Patients of both types of thyrotoxicosis received medical treatment
in the form of anti-thyroid medications as first line of treatment for
period ranged from 3 months to more than 1 year before asking for
other lines of treatment were 76% of primary type and 72% of
secondary type while only 24% of primary type and 28% of secondary
type did not receive medical treatment.
As confirmed in (Zweig, et al, 2006), maintenance doses of 5–10 mg of
methimazole or 50–100 mg of propylthiouracil twice daily keep most
patients euthyroid. For patients who cannot take medications by
mouth, propylthiouracil has been administered rectally.
koornstra, et al,(1999). see that Antithyroid medication has a
significant role in rendering patients euthyroid before treatment with
I131
or thyroidectomy.
Alexander, et al, (2002). treated 261 patients with hyperthyroidism
caused by Graves’ disease with I131
[mean dose, 14.6 mCi (540 MBq)].
Patients pretreated with antithyroid medication for greater than 4
months were at higher risk for treatment failure.
On the other hand, Braga, et al. demonstrated that methimazole
pretreatment has no effect on the final result, the time required for
71
cure, or the 1-year success rate of I131
therapy. (Braga, et al, 2002 and
Andrade, et al , 2001).
In contrast, Ahmad, et al, (2002). demonstrated that the frequency of
hypothyroidism was lower in patients treated with antithyroid drugs
prior to RAI compared with patients who did not received antithyroid
drugs. Ahmed et al 2002. studied risk factors that allow estimates of
the probability of developing hypothyroidism following radioactive
iodine treatment.
Concerning surgery as line of treatment in both types of
thyrotoxicosis prevalence of surgery between patients as 2nd
line of
treatment are more in multi-nodular patients76% than in diffuse type
4% .while 96% of cases of diffuse type and 24% of multi-nodular
patients did not have previous surgery.
Some surgeons promote thyroidectomy as the treatment of choice for
Graves’ disease (Lal, et al, 2005). However, at present very few patients
with uncomplicated Graves’ disease are treated by surgery, as
confirmed by (Wartofsky, et al, 1991).
Lal, et al, (2005). reported on 103 surgical patients for whom the
indications were patient preference (26%), cold nodule (24%), eye
symptoms (20%), large goiter size (18%), allergy to anti-thyroid
medications (15%), and young age (14%) .
In another series, eye involvement was also used as an indication for
thyroidectomy, and there was improvement in 130 of 500 patients
(Bhansali and Chandalia, 2002).
The most common symptoms were palpitation, Tachycardia, loss of
weight, tremors, nervousness, heat intolerance, thyroid opthalmopathy
and neck swelling.
72
Tachycardia, anxiety, loss of weight, tremors, heat intolerance, thyroid
opthalmopathy and neck swelling were common in patients of Graves'
disease while tachycardia, palpitation and dyspnea were the
predominant in Toxic nodular type.
Tachycardia is the most common cardiovascular sign of
thyrotoxicosis. Thyrotoxic patients may also experience palpitations
attributable to increased force of cardiac contraction. (Larsen, et al,
2002).
Apathetic hyperthyroidism is a common presentation in the elderly
and is characterized by weight loss, weakness, palpitations, dizziness, or
memory loss and physical findings of sinus tachycardia or atrial
fibrillation. (Dabon-Almirante, et al, 1998).
Thyrotoxicosis causes neuropsychiatric changes resulting in
restlessness, agitation, anxiety, emotional liability, psychosis, and even
coma. (Wartofsky, 2005).
The clinical presentation of the thyrotoxicosis of TMNG is usually mild.
Because of the presentation in older age groups, however, TMNG often
presents with cardiovascular manifestations of thyrotoxicosis, such as
palpitations, tachycardia, and atrial fibrillation. (Larsen, et al, 2002).
Graves' disease showed more statistically values of number of cases in
the first range (0.01 – 0.05) and Toxic multinodular type is higher number
of cases in the second range (0.06 – 0.1) however it did not show any
statistical difference in the third range (0.11-0.15) mIU/L.
Toxic nodular goiter showed more predilections to have higher
number of cases in the first range (185- 250 ng/ml) however Graves'
showed higher number of cases in the third range(>350 ng/ml), these
results are statistically significant. while the middle range (250-350
ng/ml) did not show statistical significant difference.
73
Toxic multinodular goiter rendered higher number of cases in the
range of 15- 25ng/dl, on the contrary Graves' showed higher number of
cases in the range > 40ng/dl group, both were statistically significant.
Results of the middle range 26-40ng/dl did not show significant
difference between the two diseases.
Low TSH level accompanied by raised free T3& T4 levels, indicates
primary hyperthyroidism, most commonly caused by Grave's disease,
multinodular goiter, or toxic adenoma. In these cases clinical criteria
can usually separate the three common causes of primary
hyperthyroidism. (Coles, et al, 1999).
Thyroid opthalmopathy and diffuse thyroid uptake of thyroid scanning
make the diagnosis of Graves' disease likely. (Coles, et al, 1999).
Low TSH, normal free T3& T4 are usually seen in thyroxin ingestion or
in subclinical primary hyperthyroidism, typically seen in elderly people.
Further investigations reavels multinodular goiter. (Ross, 1994).
The relationship between thyroid uptake and response to radioactive
iodine treatment: for the 4-10% uptake, there was a significant
difference with higher predilection of the toxic variant.Thyroid uptake
range 10-20% showed a significant difference with higher predilection
of the euthyroid variant. Thyroid uptake range >20% showed a
significant difference with higher predilection of the hypothyroid
variant.
Most dosimetric methods have the benefit of including a measure of
thyroid size in their formulas, thereby administering a dose of RAI
proportional to size of the gland. This theoretically increases the
74
probability of cure. In addition, the use of isotope uptake
measurements, as part of the dose calculation protocol, can confirm
the absence of thyroiditis and identify patients with extremes of
isotope uptake or turnover, which may predict failure of RAI treatment.
(Meier, et al, 2001).
Different dose values of radioactive iodine has different impact on
the thyroid gland function, showing that at a dose of 12mci; although
there was no statistical significance between the response of euthyroid
and toxic state, but the value of 45% as regard to the euthyroid state
does count on clinical ground, it can be noted here that sole reliance on
statistical values should be accompanied by clinical background, as for
the higher doses of the radioactive iodine they were significant
difference between the response to radio-active iodine dose equal to
15mci towards the euthyroid variant, while the statistical significant
difference of the response to radio-active iodine dose equal to 20mci
was towards the hypothyroid variant.
Leslie, et al, (2003). studied 88 patients with Graves’ hyperthyroidism
who had not previously been treated with radioactive iodine. The
patients were randomized to one of four dose-calculation methods:
low-fixed, 235 MBq (6mci); high-fixed, 350 MBq (9mci); low-adjusted,
2.96 MBq (80uCi)/g thyroid adjusted for 24 h RAI uptake; and high-
adjusted, 4.44 MBq (120uCi)/g thyroid adjusted for 24-hour RAI uptake.
Subjects were followed for a mean of 63 months to assess clinical
outcomes. Mean treatment doses were similar in the different outcome
groups.
Leslie, et al, (2003).. could not demonstrate any advantage to using
an adjusted dose method. Survival analysis did not demonstrate any
75
difference in the time to outcome between the fixed and adjusted dose
methods .
Mazzaferri, et al, (2001). in their study on 813 hyperthyroid patients,
divided them into two groups. The first group received 185 MBq(5 mci),
and the second group received 370 MBq (10 mci). At the end of their
study period, the first group had an incidence of hypothyroidism of
41.3%, and the second group had an incidence of 60.8 %.
35 patients of secondary type thyrotoxicosis received radio-active
iodine dose equal 20mci:- 10 patients (28%) became normal, 13
patients (37%) remained toxic and 12 patients (34%) turned
hypothyroid with no statistical significant difference in response.
45 patients of secondary type thyrotoxicosis received radio-active
iodine dose equal 25mci:- 22 patients (49%) became normal, 14
patients (31%) remained toxic and 9 patients (20%) turned hypothyroid
with predominance of euthyroid outcome.
20 patients of secondary type thyrotoxicosis received radio-active
iodine dose equal 29mci:- 10 patients (50%) became normal, 2 patients
(10%) remained toxic and 8 patients (40%) turned hypothyroid.
Higher doses in the multinodular goitre showed significant difference
only in the 25 & 29 mci range towards the euthyroid response.
In 1 study (7- 15mci) were administered to patients of toxic nodular
goiter; 92% of 146 patients became euthyroid within 3 months, and
97% became euthyroid at 1 year. 3% became clinically or biochemically
hypothyroid. (Giovanella, et al, 2000).
A similar study of 130 patients also found that 92% were cured, but a
high proportion needed a second treatment. (Nygaard, et al, 1999).
76
In the population study 100 case of primary type of thyrotoxicosis
were followed up for one year after the first dose of radio-active iodine
treatment. 92% of cases became euthyroid or turned hypothyroid thus
no more doses of radio-active iodine is needed. While only 8% of cases
remained toxic and asked for second dose of radio-active iodine.
Retrospective review of I131
for thyrotoxicosis at Waikato Hospital,
during the 3 year period prior to 1 December 2010.
Results: A total of 326 doses of I131 were given to 285 patients. Follow
up data were available on 283 patients. Median follow-up was 2.3 years
. The diagnosis was GD for 61.1% and TMNG for 34.3%. Most patients
(98.2%) received a fixed dose of 15mci I131. At last follow up cure had
been achieved in 72.1% after the first dose. ( Allahabadia, et al,2001;
Allahabadia, et al,2000; Metso, et al, 2004 and Boelaert, et al, 2009).
Onset of hypothyroidism following radioactive treatment is well
known and follow up is required to determine which dose render the
least iatrogenic complication. There were statistical significant
differences in the incidance of hypothyroidism after 6 months of the
treating radio-active iodine doses equal to 25mci& 29mci (44% & 50%)
respectivly. 20mci showed no statistical significant difference in the 2
years follow up period (P value >0.05). There were statistical significant
differences in the incidance of hypothyroidism after 12 months of the
treating radio-active iodine doses equal to 12mci& 15mci (57% & 50%)
respectivly.
About 20% of all cases treated with radio-active iodine I131
became
hypothyroid after one year of treatment on further follow up
investigations.
77
Howarth, et al, (2001). compared low radiation doses to the thyroid
(60 vs. 90 Gy), trying to minimize the number of patients requiring
thyroid hormone replacement after I131
therapy .Euthyroidism was
achieved in 46% of the patients and 47% were rendered hypothyroid at
the final follow-up 3 years.
A dose of 60 Gy yielded a 39% response rate at 6 months while
minimizing early hypothyroidism, but no significant advantage in the
response rate was gained with a dose of 90 Gy. For a more rapid
therapeutic effect, the authors recommended doses in excess of 120
Gy, recognizing that there will be an increased rate of hypothyroidism.
Ceccarelli, et al, (2005). administered 7.4 MBq (200 uCi) of I131
per
gram corrected for uptake. As a single dose had a success rate of 94%,
and60% of their patients were hypothyroid by 20 years.
By comparison, (Ahmad, et al, 2002).reported that the cumulative
incidence of hypothyroidism following RAI treatment was 38.2% after 6
months. The incidence increased to 55.8% after 1 year and to 86.1% at
10 years.
78
:Conclusion
There are two main types of thyrotoxicosis : primary diffuse toxic
type and secondary multinodular type
There was significant difference between age and prevalence of each
type of thyrotoxicosis. P value < 0.001
Primary type Mean ages were 33 ± 9.79 with range (18-50) while
secondary Mean ages were 42 ±11.78with range (25-59 years).
Primary type is more between females (66%) than males (35%) while
secondary type is more common among males (65%) than females
(34%). Non-parametric correlation coefficient of spearman (0.754)
The most common symptoms were palpitation, Tachycardia, loss of
weight, tremors, nervousness, heat intolerance and neck swelling.
Thyroid hormones levels are higher in primary type than secondary
type thyrotoxicosis with no overall significant difference.
Graves' disease show higher percent of thyroid uptake affecting the
response to radio-active iodine treatment clinically but not in the point
of view of statistical significance.
Most patients prefer medical treatment in the form of symptoms
relief and anti-thyroid medications as first line of treatment before
asking for surgery or radio-active iodine treatment.
On other hand more patients avoid the risk of surgery as a line of
treatment in primary type while physicians prefer surgery as a line of
treatment of toxic nodular type.
79
Radio-active iodine treatment has a very important role in
treatment of both types of thyrotoxicosis and many patients prefer it as
a main line of treatment.
Doses of Radio-active iodine varies according to type of
thyrotoxicosis, size of the gland, level of thyroid hormones, percent of
gland uptake and even the general conditions of the patient.
Radio-active iodine is safe, effective in both types of thyrotoxicosis,
its effect appears shortly after the first dose and very small percent
need a second dose.
Single high dose of radio-active iodine is better to avoid the risk of
re-exposure to second dose.
Different dose values of radioactive iodine has different impact on the
thyroid gland function, it was studied here briefly showing that at a
dose of 12mci; although there was no statistical significance between
the response of euthyroid and toxic state, but the value of 45% as
regard to the euthyroid state does count on clinical ground.
Higher doses in the multinodular goitre showed significant
difference of response only in the 25 & 29 mci range.
Hypothyroidism is a common outcome after radio-active iodine
treatment that should be considered. Hypothyroidism should be
diagnosed clinically and biochemically and thyroxin replacement
therapy should be started once the diagnosis is confirmed.
Onset of hypothyroidism following radioactive treatment is well
known and follow up is required to determine which dose render the
least iatrogenic complication. There were statistical significant
differences in the incidance of hypothyroidism after 6 months of the

80
treating radio-active iodine doses equal to 25mci& 29mci (44% & 50%)
respectivly. Twenty (20mci) showed no statistical significant difference
in the 2 years follow up period (P value >0.05). There were statistical
significant differences in the incidance of hypothyroidism after 12
months of the treating radio-active iodine doses equal to 12mci& 15mci
(57% & 50%) respectivly.
81
References
A
Abraham P, Avenell A, Park CM, Watson WA and Bevan JS. (2005); A systematic
review of drug therapy for Graves’ hyperthyroidism.Eur J Endocrinal. 153: 489–
498.
Adamali HI, Gibney J, O'Shea D, et al(2007);. The occurrence of hypothyroidism
following radioactive iodine treatment of toxic nodular goiter is related to the TSH
level. Ir J Med Sci. Sep 176(3):199-203.
Ahmad, A.F., Ahmad, M., and Young, E.T. 2002: Objective estimates of the
probability of developing hypothyroidism following radioactive iodine treatment
of thyrotoxicosis. Eur. J. Endocrinol., 146 767–775,.
Albino CC, Mesa CO Jr, Olandoski M, et al(2005). Recombinant human
thyrotropin as adjuvant in the treatment of multinodular goiters with radioiodine.
J Clin Endocrinol Metab. May;90(5):2775-80.
Alexander E and Larsen PR. (2002)High dose of (131) I therapy for the treatment
of hyperthyroidism caused by Graves’ disease. J ClinEndocrinolMetab.;87: 1073–
1077.
Allahabadia A, Daykin J, Sheppard MC, Gough SC and Franklyn JA.
(2001);Radioiodine treatment of hyperthyroidism-prognostic factors for outcome.
J Clin Endocrinol Metab86:3611-7.
82
Allahabadia, et al. (2000). Age and gender predict the outcome of treatment for
Graves' hyperthyroidism. J Clin Endocrinol Metab ;85:1038-42.
Alsanea O and Clark OH. (2000); Treatment of Graves’ disease: the advantages of
surgery. Endocrinol Metab Clin North Am 29:321-37.
American Academy of Clinical Endocrinologists. (2002); American Association of
Clinical Endocrinologists medical guidelines for clinical practice for the evaluation
and treatment of hyperthyroidism and hypothyroidism Endocr Pract 8:457-69.
Andrade, V.A., Gross, J.L., and Maia, A.L.: 2001 The effect of methimazole
pretreatment. On the efficacy of radioactive iodine therapy in Graves’
hyperthyroidism. J. Clin. Endocrinal. Metab.,86(8):3488-3493,.
B
Bahn Chair RS, Burch HB, Cooper DS, et al. (2011);Hyperthyroidism and other
causes of thyrotoxicosis: management guidelines of the American Thyroid
Association and American Association of Clinical Endocrinologists. Thyroid.Jun
21(6):593-646.
Bahn RS. (2000); Understanding the immunology of Graves’ ophthalmopathy: is it
an autoimmune disease? Endocrinol Metab Clin North Am 29:287–96).
Bal C, Kumar A, Tripathi M, et al. (2005); High-dose radioiodine treatment for
differentiated thyroid carcinoma is not associated with change in female fertility
or any genetic risk to the offspring. Int J Radiat Oncol Biol Phys 63:449–455.
Baloch Z, Caryon P, Conte-Devolx B, et al. (2003);Laboratory medicine practice
guidelines: laboratory support for the diagnosis and monitoring of thyroid
disease. Thyroid 13(1): 3–126.
Barbero P, Ricagni C, Mercado G, Bronberg R and Torrado M. (2004);Choanal
atresia associated with prenatal methimazole exposure: three new patients. Am J
Med Genet A. 129:83–86.
83
Barrio R, Lopez-Capape M, Martinez-Badas I, Carrillo A, Moreno JC and Alonso
M.( 2005) Graves’ disease in children and adolescents: response to long-term
treatment.Acta Paediatr.;94:1583–1589.
Bartalena L, Baldeschi L, Dickinson A, Eckstein A, Kendall-Taylor P and Marcocci
C. (Mar 2008) Consensus statement of the European Group on Graves'
orbitopathy (EUGOGO) on management of GO. Eur J Endocrinol.;158(3):273-85.
Bartalena L, Tanda ML, Bogazzi F, Piantanida E, Lai A and Martino E. (2005);An
update on the pharmacological management of hyperthyroidism due to Graves’
disease.Expert OpinPharmacother. 6:851–861.
Bartalena L, Marcocci C, Tanda ML, et al. (2005);An update on medical
management of Graves’ ophthalmopathy. J Endocrinol Invest. 28:469–478.
Bartalena L, Tanda ML, Piantanida E, Lai A and Pinchera A. ( 2004);Relationship
between management of hyperthyroidism and course of the ophthalmopathy. J
Endocrinol Invest. Mar27(3):288-94.
Basaria S and Salvatori R. (2004); Images in clinical medicine. Pembertons sign N
Engl JMed. Mar25 350(13):1338.
Baskin HJ, Cobin RH, Duick DS, et al. (2002); American Association of Clinical
Endocrinologists medical guidelines for clinical practice for the evaluation and
treatment of hyperthyroidism and hypothyroidism. Endocr Pract. 8:457-469.
Berlin L .(2001); Iodine-131 and the pregnant patient.AJR176:869–871.
Bhansali SK and Chandalia HB. (2002); Thyrotoxicosis: surgical management in
the era of evidence-based medicine—experience in western India with 752 cases.
Asian J Surg. 25:291–299.
Birrell G and Cheetham T. (2004); Juvenile thyrotoxicosis: can we do better? Arch
Dis Child. 89:745–750.
84
Boelaert et al. (2009). Prediction and cure of risk of hypothyroidism in patients
receiving 131I for hyperthyroidism. Clin Endocrinol (Oxf) ;70:129-38.
Bogazzi F, Bartalena L, Brogioni S, et al .(1999); Comparison of radioiodine with
radioiodine plus lithium in the treatment of Graves’ hyperthyroidism.
JClinEndocrinolMetab,84:499–503.
Bogazzi F, Bartalena L and Brogiani S. (1997);Color flow Doppler sonography
rapidly differentiates type I and type II amiodarone-induced thyrotoxicosis.
Thyroid 7:541–5.
Braga, M.,Walpert, N., Burch, H.B., et al. 2002: The effect of methiamazole on
cure rate after radioiodine treatment for graves’ hyerthyroidisdm. Thyroid,
12(2):135-139.
Braverman LE, Utiger RD and Werner and Ingbar’s (2005):The Thyroid. 9th ed.
Philadelphia, PA: Lippincott, Williams & Wilkins; 660-664.
Burman K. (2006):Hyperthyroidism. In: Rakel R, Bope E, eds. Conn’s Current
Therapy. Philadelphia, PA: Saunders;( 806-811
C
Caglar M, Tuncel M and Alpar R. (2002); Scintigraphic evaluation of salivary gland
dysfunction in patients with thyroid cancer after radioiodine treatment. Clin Nucl
Med27:767–771.
Cakir M. 2005); Marine-Lenhart syndrome. J Natl Med Assoc(97(7):1036–8.
Cappelen T, Unhjem JF, Amundsen AL, Kravdal G and Folling I( 2006);. Radiation
exposure to family members of patients with thyrotoxicosis treated with iodine-
131. Eur J Nucl Med Mol Imaging. 33:81–86.
Cavalieri RR. (1991). In vivo isotopic tests and imaging. In: Braverman LE, Utiger
R, editors. Werner’s and Ingbar’s the thyroid. 6th edition. Philadelphia: Lipincott-
Ranen; p. 437–45.
85
Ceccarelli C, Bencivelli W, Vitti P, Grasso L and Pinchera A. (2005);Outcome of
radioiodine-131 therapy in hyperfunctioning thyroid nodules: a 20 years’
retrospective study. ClinEndocrinol (Oxf). 62:331–335.
Chen YT and Khoo DH. (2002);Thyroid diseases in pregnancy.Ann Acad Med
Singapore. 31:296–302.
Cho YY, Shon HS and Yoon HD. (2005);Management of a pregnant patient with
Graves’ disease complicated by propylthiouracil induced agranulocytosis. Korean J
Intern Med. 20:335–338.
Coles AJ, Wing M, Smith S, et al.(1999). Pulsed monoclonal antibody treatment
and autoimmune thyroid disease in multiple sclerosis;354:1691-95.
Cooper DS. (2005); Antithyroid drugs. N Engl J Med. 352:905–917.
Cooper DS. (1996):Treatment of thyrotoxicosis. In: Braverman LE, Utiger RD, eds.
Werner and Ingbar’s The Thyroid: A Fundamental and Clinical Text. 7th ed.
Philadelphia, Pa: JB Lippincott Co; 713-743.
Costagliola S, Morgenthaler NG, Hoermann R, et al. (1999); Second generation
assay for thyrotropin receptor antibodies has superior diagnostic sensitivity for
Graves’ disease. J Clin Endocrinol Metab 84(1):90–7.
D
Dabon-Almirante CL and Surks M. (1998);Clinical and laboratory diagnosis of
thyrotoxicosis. Endocrinol Metab Clin North Am 27(1):25–35.
Davis TF and Larsen PR. (2003) Thyrrotoxicosis In: Williams RH , Larsen PR,
Kronenberg HM, et al. editors. Williams text. Book of endocrinology.10th
ed.
Philadelphia : Saunders ;: 379.J
Dickinson AJ, Vaidya B, Miller M, Coulthard A, Perros P and Baister E. (2004);
Double-blind, placebo-controlled trial of octreotide long-acting repeatable (LAR)
in thyroid-associated ophthalmopathy. J Clin Endocrinol Metab. Dec 89(12):5910-
5.
86
Duick DS and Baskin HJ. (2003);Utility of recombinant human thyrotropin for
augmentation of radioiodine uptake and treatment of nontoxic and toxic
multinodular goiters. Endocr Pract. 9:204–209.
Durrani OM, Reuser TQ and Murray PI. (2005);. Infliximab: a novel treatment for
sight-threatening thyroid associated ophthalmopathy. Orbit. Jun 24(2):117-9.
E
England RJ, Kamath MB, Jabreel A, Dunne G and Atkin SL. (2006); How we do it:
surgery should be considered equally with I131 and thionamide treatment as first-
line therapy for thyrotoxicosis. ClinOtolaryngol. 31:160–162.
Erem C, Kandemir N, Hacihasanoglu A, Ersoz HO, Ukinc K and Kocak M.
(2004);Radioiodine treatment of hyperthyroidism: prognostic factors affecting
outcome. Endocrine. 25:55–60.
F
Fatourechi V. (2005); Pretibial myxedema: pathophysiology and treatment
options. Am J Clin Dermatol 6(5):295–309.
Fitzgerald PA. ( 2005); Endocrinology. In: Tierny LM, McPhee SJ, Papadakis MA,
eds. Current Medical Diagnosis and Treatment. 44th ed. New York, NY: McGraw-
Hill; 1102-1110.
Foulds N, Walpole I, Elmslie F and Mansour S. (2005); Carbimazole
embryopathy: an emerging phenotype. Am J Med Genet A. 132:130–135.
Franklyn JA. (1994); The management of hyperthyroidism.N Engl J Med.
330:1731-1738
87
G
Giovanella L, De Palma D, Ceriani L, et al. (2000)Radioiodine treatment of
hyperthyroidism using a simplified dosimetric approach: clinical results [in Italian].
Radiol Med (Torino).;100:480–483.
Gorman CA, Garrity JA, Fatourechi V, et al. (2001) A prospective, randomized,
double-blind, placebo-controlled study of orbital radiotherapy for Graves'
ophthalmopathy. Ophthalmology.;108(9):1523-34.
Gurleyik E, Pehlivan M and Gokpinar I. (2005); Surgery is the procedure of choice
for the treatment of patients with toxicadenoma in an endemic goitre area.
ActaChir Belg. 105:373–377.
H
Harper MB and Mayeaux EJ Jr. (2003)Thyroid disease. In: Taylor RB. Family
medicine: principles and practice. 6th ed. New York: Springer,:1042-52.
Hidaka Y, Tamaki H, Iwatani Y, et al. (1994 )Prediction of post-partum Graves’
thyrotoxicosis by measurement of thyroid stimulating antibody in early
pregnancy. Clin Endocrinol (Oxf);41:15–20.
Holst JP, Burman KD, Atkins F, Ulmans JG and Jonklaas J. (2005)Radioiodine
therapy for thyroid cancer and hyperthyroidism in patients with end-stage renal
disease on hemodialysis. Thyroid.;15:1321–1331.
Howarth D, Epstein M, Lan L, Tan P and Booker J. (2001) Determination of the
optimal minimum radioiodine dose in patients with Graves’ disease: a clinical
outcome study. Eur J Nucl Med.;28:1489–1495.
Hung W and Sarlis NJ. (2004) Autoimmune and non-autoimmune
hyperthyroidism in pediatric patients: a review and personal commentary on
management. PediatrEndocrinol Rev.;2:21–38.

88
Huysmans DA, Hermus AR, Corstens FH and Kloppenborg PW.( 1993) Long-term
results of two schedules of radioiodine treatment for toxic
multinodulargoitre.EurJ Nucl Med.;20:1056–1062.
Hyer S, Vini L, O’Connell M, et al. (2002) Testicular dose and fertility in men
following I(131) therapy for thyroid cancer. Clin Endocrinol (Oxf);56:755–758.
I
Imseis RE, Vanmiddlesworth L, Massie JD, Bush AJ and Vanmiddlesworth
NR.(1998 ) Pretreatment with propylthiouracil but not methimazole reduces the
therapeutic efficacy of iodine-131 in hyperthyroidism. J
ClinEndocrinolMetab.;83:685–687.
Intenzo CM and dePapp AE. (2003) Scintigraphic manifestations of
thyrotoxicosis.Radiographics.;23:857-869."
K
Kadmon PM, Noto RB, Boney CM, Goodwin G and Gruppuso PA. (2001) Thyroid
storm in a child following radioactive iodine (RAI) therapy: a consequence of RAI
versus withdrawal of antithyroid medication. J ClinEndocrinolMetab.; 86:1865–
1867.
Kang AS, Grant CS, Thompson GB and van Heerden JA. ( 2002) Current
treatment of nodular goiter with hyperthyroidism (Plummer’s disease): surgery
versus radioiodine. Surgery.;132:916–923.
Kalinyak JE and McDougall IR. (2003) How should the dose of iodine-131 be
determined in the treatment of Graves’ hyperthyroidism? J
ClinEndocrinolMetab.;88:975–977.
Kinuya S, Michigishi T, Nakajima K, et al. (2004) Failure of radioiodine treatment
in Graves’ disease intentionally caused by a patient: suspected Munchausen
syndrome. Ann Nucl Med.;18:631-632.
89
Kita T, Yokoyama K, Higuchi T, et al. (2004) Multifactorial analysis on the short-
term side effects occurring within 96 hours after radioiodine-131 therapy for
differentiated thyroid carcinoma. Ann Nucl Med;18:345–349.
Klein I and Ojama K. (2001) Thyroid hormone and the cardiovascular system. N
Engl J Med; 344(7):501–8.
Koornstra JJ, Kerstens MN, Hoving J, et al. (1999) Clinical and biochemical
changes following 131I therapy for hyperthyroidism in patients not pretreated
with antithyroid drugs. Neth J Med.;55:215–221.
Kloos RT. (2009 ) Protecting thyroid cancer patients from untoward effects of
radioactive iodine treatment. Thyroid;19:925–928.
Kurita S, Sakurai M and Kita Y.( 2005). Measurement of thyroid blood flow area is
useful for diagnosing the cause of thyrotoxicosis. Thyroid;15(11):1249–52.
L
Ladenson P.( 2005) Diagnosis of thyrotoxicosis. In: Braverman LE, Utiger RD,
editors.Werner’s and Ingbar’s the thyroid. 9th edition. Philadelphia: Lipincott,
Williams & Wilkins;. p. 660–4.
Lal G, Ituarte P, Kebebew E, Siperstein A, Duh QY and Clark OH. (2005) Should
total thyroidectomy become the preferred procedure for surgical management of
Graves’ disease? Thyroid.;15:569–574.
Larsen PR, Davies TF, et al. (2002) Thyrotoxicosis. In: Larsen PR, Kronenberg
HM,Melmed S,et al, editors. Williams’ textbook of endocrinology. 10th edition.
Philadelphia: WB SaundersCo;. p. 374–421.
Lassmann M, Reiners C and Luster M.( 2010) Dosimetry and thyroid cancer: the
individual dosage of radioiodine. Endocr Relat Cancer;17:R161–172.
Lee SL and Ananthakrishnan S (2009). Hyperthyroidism.Available at
http://emedicine.medscape.com/article/121865-overview.
90
Leese GP, Flynn RV, Jung RT, et al. (2008) Increasing prevalence and incidence of
thyroid disease in Tayside, Scotland: The Thyroid Epidemiology, Audit and
Research Study (TEARS). Clin Endocrinol (Oxf);68:311-16.
Leslie WD, Ward L, Salamon EA, et al. (2003 ) A randomized comparison of
radioiodine doses in Graves' hyperthyroidism. J
ClinEndocrinolMetab. Mar ;88(3):978-83.
Liao SL and Huang SW. (2011) Correlation of retrobulbar volume change with
resected orbital fat volume and proptosis reduction after fatty decompression for
Graves ophthalmopathy. Am J Ophthalmol. Mar;151(3):465-9.
Loy M, Perra E, Melis A, Cianchetti ME, Piga M, Serra A, Pinna G and Mariotti S.
(2007) Color-flow Doppler sonography in the differential diagnosis and
management ofamiodarone-induced thyrotoxicosis.Acta Radiol. Jul;48(6):628-34.
Luton D, Le Gac I, Vuillard E, et al. (2005); Management of Graves’ disease during
pregnancy: the key role of fetal thyroid gland monitoring. J ClinEndocrinolMetab.
90:6093–6098.
M
Macchia PE, Bagattini M, Lupoli G, et al. (2001) High-dose intravenous
corticosteroid therapy for Graves' ophthalmopathy. J Endocrinol Invest.;24:152-8.
Maenpaa HO, Heikkonen J, Vaalavirta L, et al. (2008) Low vs. high radioiodine
activity to ablate the thyroid after thyroidectomy for cancer: a randomized study.
PLoS One;3:e1885.
Mandel SJ and Mandel L.( 2003) Radioactive iodine and the salivary glands.
Thyroid;13:265–271.
Marcocci C, Kahaly GJ, Krassas GE, et al. (2011) Selenium and the course of mild
Graves' orbitopathy. N Engl J Med. May 19;364(20):1920-31.
91
Mauz PS, Maassen MM, Braun B and Brosch S. (2004) How safe is percutaneous
ethanol injection for treatment of thyroid nodule? Report of a case of severe toxic
necrosis of the larynx and adjacent skin.ActaOtolaryngol.;124:1226– 1230.
Mazzeferri, E.L. and Lorraine, A. (2001): Year book of Endocrinology. North
America, Mosby,
McDougall IR.( 2006) Management of Thyroid Cancer and Related Nodular
Disease. London, England: Springer;.
Meier DA and Kaplan MM.( 2001) Radioactive iodine uptake and thyroid
scintiscanning.Endocrinol Metab Clin North Am.;30:291-313.
Meller J and Becker W. (2002) The continuing importance of thyroid scintigraphy
in the era of high-resolution ultrasound. Eur J Nucl Med Mol Imaging;29:425-38.
Mello AM, Isaacs R, Petersen J, Kronenberger S and McDougall IR. (1994)
Management of thyroid papillary carcinoma with radioiodine in a patient with end
stage renaldisease on hemodialysis.ClinNucl Med.;19:776–781.
Mendoza A, Shaffer B, Karakla D, et al. (2004) Quality of life with well-
differentiated thyroid cancer: treatment toxicities and their reduction.
Thyroid;14:133–140.
Metso et al. (2004). Long-term follow-up study of radioiodine treatment of
hyperthyroidism. Clin Endocrinol (Oxf)2004;61:641-8.
N
Naik KS and Bury RF. Review: Imaging the thyroid. (1998) Clinical
Radiology;53:630-9.
Nayak B and Hodak SP. (2007) Hyperthyroidism. Endocrinol Metab Clin North
Am.;36:617-656.
Nygaard B, Hegedus L, Ulriksen P, Nielsen KG and Hansen JM. (1999) Radioiodine
therapy for multinodular toxic goiter. Arch Intern Med.;159:1364–1368.
92
O
Ogawa E, Katsushima Y, Fujiwara I and Iinuma K. (2003) Subacute thyroiditis in
children: patient report and review of the literature. J Pediatr Endocrinol Metab.
Jul-Aug;16(6):897-900.
Ojamaa K, Klemperer JD and Klein I.( 1996) Acute effects of thyroid hormone on
vascular smooth muscle. Thyroid;6(5):505–12.
P
Pacella CM, Bizzarri G, Spiezia S, et al. (2004)Thyroid tissue: US-guided
percutaneous laser thermal ablation. Radiology.;232:272–280.
Pant GS, Sharma SK, Bal CS, Kumar R and Rath GK. (2006) Radiation dose to
family members of hyperthyroidism and thyroid cancer patients treated with
131I. RadiatProtDosimetry.;118:22.
Pearce EN, Farwell AP and Braverman LE.( 2003) Thyroiditis. N Engl J
Med;348(26):2646–55.
Perros P. (2005) Thyrotoxicosis and pregnancy.PLoS Med.;2:e370.
Piga M, Cocco MC, Serra A, Boi F, Loy M and Mariotti S. (2008) The usefulness of
99mTc-sestaMIBI thyroid scan in the differential diagnosis and management of
amiodarone-induced thyrotoxicosis. Eur J Endocrinol. Oct;159(4):423-9.
Pimental L and Hansen K. (2005) Thyroid disease in the emergency department:
a clinical and laboratory review. J Emerg Med;28:201–9.
93
R
Rahman MA, Birrell G, Stewart H, Lucraft H and Cheetham TD. (2003) Successful
radioiodine treatment in a 3 year old child with Graves’ disease following
antithyroid medication induced neutropenia. Arch Dis Child.;88:158–159.
Razvi S, Basu A, McIntyre EA, Wahid ST, Bartholomew PH and Weaver JU.
((2004) Low failure rate of fixed administered activity of 400 MBq 131I with pre-
treatment with carbimazole for thyrotoxicosis: the Gateshead Protocol. Nucl Med
Commun.;25:675–682.
Reid JR and Wheeler SF.( 2005) Hyperthyroidism: diagnosis and treatment. Am
Fam Physician.;72:623-630.
Reinhardt MJ, Biermann K, Wissmeyer M, et al. (2006 ) Dose selection for
radioiodine therapy of borderline hyperthyroid patients according to thyroid
uptake of (99m)Tc-pertechnetate: applicability to unifocal thyroid autonomy? Eur
J NuclMed Mol Imaging.;33:608–612.
Reiners C and Schneider P. (2002) Radioiodine therapy of thyroid autonomy. Eur
J Nucl Med Mol Imaging.;29(suppl 2):S471–S478.
Rivkees SA, Sklar C and Freemark M. (1998) Clinical review 99: the management
of Graves’ disease in children, with special emphasis on radioiodine treatment. J
ClinEndocrinolMetab.;83:3767–3776.
Rivkees SA. (2003) The management of hyperthyroidism in children with
emphasis on the use of radioactive iodine.PediatrEndocrinol Rev.;1(suppl 2):212–
221. 109.
Ron E, Doody MM, Becker DV, et al. (1998) Cancer mortality following treatment
for adult hyperthyroidism: Cooperative Thyrotoxicosis Therapy Follow-up Study
Group. JAMA.;280:347–355.
Ross DS, (1994) Hyperthyroidism, thyroid hormone therapy and bone.
Thyroid;4:319-26.
94
Rubio IG, Perone BH, Silva MN, Knobel M and Medeiros-Neto G. (2005) Human
recombinant TSH preceding a therapeutic dose of radioiodine for multinodular
goiters has no significant effect in the surge of TSH-receptor and TPO antibodies.
Thyroid.;15:134–139.
S
Santos RB, Romaldini JH and Ward LS.( 2004) Propylthiouracil reduces the
effectiveness of radioiodine treatment in hyperthyroid patients with Graves’
disease. Thyroid.;14:525–530.
Sawka AM, Lea J, Alshehri B, et al. (2008) A systematic review of the gonadal
effects of therapeutic radioactive iodine in male thyroid cancer survivors. Clin
Endocrinol (Oxf);68:610–617.
Segni M and Gorman CA. (2001) The aftermath of childhood hyperthyroidism.J
PediatrEndocrinolMetab.;14(suppl 5):1277–1282.
Sisson JC and Carey JE. (2001) Thyroid carcinoma with high levels of function:
treatment with (131)I. J Nucl Med;42:975–983.
Slatosky J, Shipton B and Wahba H. (2000) Thyroiditis: differential diagnosis and
management. Am Fam Physician.;61:1047-1052.
Smith JR and Oates E. (2004) Radionuclide imaging of the thyroid gland: patterns,
pearls, and pitfalls. Clin Nucl Med;29:181-93.
Stan MN, Garrity JA, Bradley EA, Woog JJ, Bahn MM and Brennan MD. (2006)
Randomized, double-blind, placebo-controlled trial of long-acting release
octreotide for treatment of Graves' ophthalmopathy. J Clin Endocrinol Metab.
Dec;91(12):4817-24.
Summaria V, Salvatori M, Rufini V, et al. (1999) Diagnostic imaging in
thyrotoxicosis.Rays;24:273-300.
95
T
Takasu N, Yamada T, Sato A, et al. (1990) Graves’ disease following
hyperthyroidism due to Hashimoto’s disease: studies of eight cases. Clin
Endocrinol (Oxf);33(6):687–98.
Tierny LM, McPhee SJ and Papadakis MA, eds. (2005) Current Medical Diagnosis
and Treatment. 44th ed. New York, NY: McGraw-Hill;:1102-1110.
V
Van Nostrand D, Atkins F, Bandaru VV, et al. (2009) Salivary gland protection
with sialagogues: a case study. Thyroid;19:1005–1008.
Vemulakonda US, Atkins FB and Ziessman HA. (1996) Therapy dose calculation
in Graves’ disease using early I-123 uptake measurements.ClinNucl Med.; 21:102–
105.
Vidal-Trecan GM, Stahl JE and Eckman MH.( 2004) Radioiodine or surgery for
toxic thyroid adenoma: dissecting an importantdecision—a cost-effectiveness
analysis. Thyroid.;14:933.
Vini L, Hyer S, Al-Saadi A, et al. (2002) Prognosis for fertility and ovarian function
after treatment with radioiodine for thyroid cancer. Postgrad Med J;78:92–93.
W
Wakelkamp IM, Tan H, Saeed P, et al.( 2004) Orbital irradiation for Graves'
ophthalmopathy: Is it safe? A long-term follow-up study. Ophthalmology.
Aug;111(8):1557-62.
Walter MA, Christ-Crain M, Schindler C, Muller-Brand J and Muller B. (2006)
Outcome of radioiodine therapy without, on or 3 days off carbimazole: a
prospective interventional three-group comparison. Eur J Nucl Med Mol
Imaging.; 33:730–737.
96
Wartofsky L. (2005) Thyrotoxic storm. In: Braverman LE, Utiger RD, editors.
Werner’s and Ingbar’s the thyroid. 9th edition. Philadelphia: Lipincott,
Williams&Wilkins;. p. 660–4, 652–7.
Wartofsky L, Glinoer D, Solomon B, et al. (1991) Differences and similarities in
the diagnosis and treatment of Graves’ disease in Europe, Japan, and the United
States.Thyroid.;1:129–135.
Weaver JU and Razvi S. (2005) Dose of anti-thyroid drugs can effect remission in
Grave’s disease [comment]. Endocr J.;52:159
Weetman AP.( 2000) Graves' disease. N Engl J Med. Oct 26 ;343(17):1236-48.
Wemeau JL, Caron P, Beckers A, et al. (2005) Octreotide (long-acting release
formulation) treatment in patients with graves' orbitopathy: clinical results of a
four-month, randomized, placebo-controlled, double-blind study. J Clin Endocrinol
Metab.;90:841-8.
Werner SC, Ingbar SH, Braverman LE, Utiger RD, eds. Werner and
Ingbar’s(2000) The Thyroid: A Fundamental and Clinical Text. 8th ed.
Philadelphia, PA: Lippincott Williams &Wilkins;:564-572.
Wiersinga WM. (2005) The philosophy of Graves’ ophthalmopathy
.Orbit.;24:165–171.
Wiersinga WM. (2004) Thyroid associated ophthalmopathy: pediatric and
endocrine aspects. PediatrEndocrinol Rev.;1(suppl3):513–517.
Wilson ID, Foster DW, Kronenberg HM, et al. (1998) Williams Textbook of
Endocrinology. 9th ed. Philadelphia, PA: WB Saunders Co;:389-515
Y
Yanagisawa T, Sato K and Takano K. (2005) Rapid differential diagnosis of
Graves’ disease and painless thyroiditis using T3/T4 ratio, TSH, and total alkaline
phosphatase activity. Endocr J;52(1):29–36.
97
Z Zimmerman MB. (2009) Iodine deficiency. Endocr Rev;30:376-408.
Zingrillo M, Urbano N, Suriano V, et al. (2007) Radioiodine treatment of
Plummer and multinodular toxic and nontoxic goiter disease by the first
approximation dosimetry method. Cancer Biother Radiopharm. Apr;22(2):256-60.
Zweig SB, Schlosser JR, Thomas SA, Levy CJ and Fleckman AM. (2006) Rectal
administration of propylthiouracil in suppository form in patients with
thyrotoxicosis and critical illness: case report and review of literature.
EndocrPract.;12:43–47.