Embed Size (px)
Citation preview

9/19/2013
1
Daniel E. Cooper, M.D.
The Carrell Clinic
Dallas, Texas USA
Tibial Inlay Is My Preferred PCL
Reconstruction Technique
Vumedi Webinar 2013
DISCLOSURE:
• I, Daniel E. Cooper MD, have no financial
interest related to this topic.
• Consultant and Royalties – Stryker
Endoscopy
However….
• I prefer to not have to reconstruct
• I look for the opportunity to repair certain
acute PCL injuries
• ie. “Peel-off” lesions
9/19/2013
2
Arthroscopic PCL Primary Repair
Rationale for Tibial Inlay
Fixation Technique
• Marginal results of
tibial tunnel
techniques - open or
arthroscopic
• Early rigid fixation -
close to anatomic
• Approach - Burks
CORR 1990
• Early experience -
Berg Arthros. 1995
Current Problems with 2
Tunnel Technique
• Difficult arthroscopic
technique
• Vascular injury
when reaming?
• Fixation slippage or
creep / fixation
issues
• “Killer turn”
• ? long-term results
9/19/2013
3
Potential Advantages of
Tibial Inlay Fixation
• Eliminates potential for
anterior placement
• No “killer turn”
• Jung et al ISAKOS 99
(observed fraying)
• No tunnel erosion
• Ideal for revisions
• Allows large graft size
• Graft passage
• Secure initial fixation
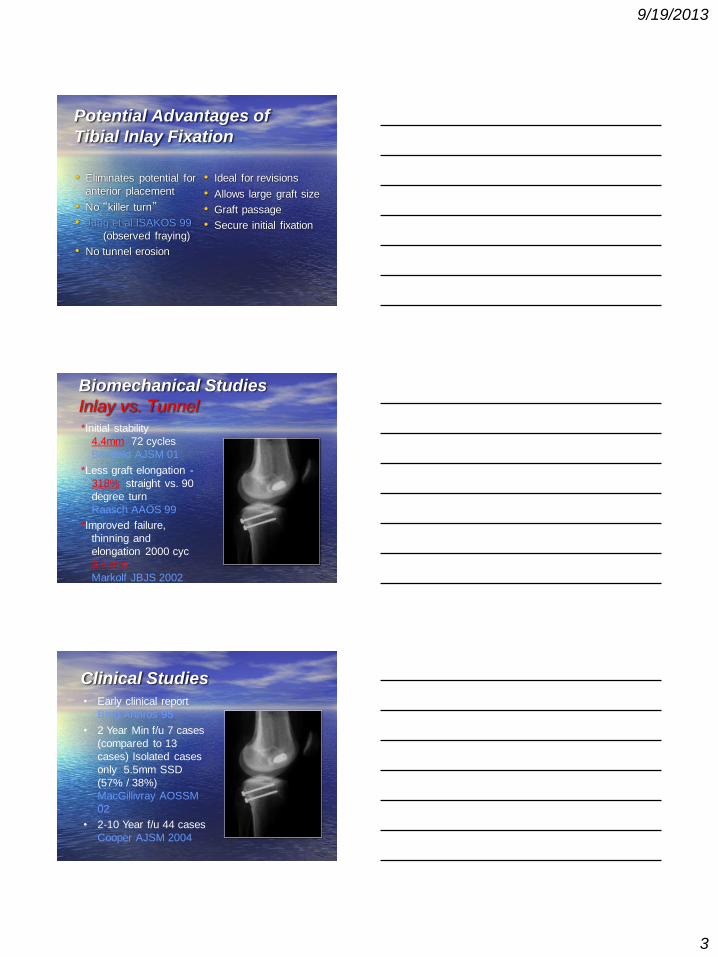
Biomechanical Studies
Inlay vs. Tunnel
*Initial stability
4.4mm 72 cycles
Bergfeld AJSM 01
*Less graft elongation -
318% straight vs. 90
degree turn
Raasch AAOS 99
*Improved failure,
thinning and
elongation 2000 cyc
3.9 mm
Markolf JBJS 2002
Clinical Studies
• Early clinical report
Berg Arthros 95
• 2 Year Min f/u 7 cases
(compared to 13
cases) Isolated cases
only 5.5mm SSD
(57% / 38%)
MacGillivray AOSSM
02
• 2-10 Year f/u 44 cases
Cooper AJSM 2004
9/19/2013
4
Tibial Inlay PCL Reconstruction
Technique
Supine Positioning
- The more unstable the knee, the easier the
positioning.
- Not well suited for the obese patient.
Graft Selection
• BTB Autograft
• BTB contralat Auto.
• BTB Allograft
• Achilles Allograft
• Quad Autograft
• Currently prefer
Allograft BTB
• X = 45 + 1mm for each
inch over 5’0” tall
• 6’0” = X-57
9/19/2013
5
Graft Preparation
• 1 or 2 grafts from whole construct (prefer male donor)
• 11mm femoral tunnel
• 12mm width inlay plug
• 18-20 soft tissue width
BTB Allograft:
Plan for appropriate length
Single Bundle Femoral Tunnel
Single Bundle Femoral Tunnel

9/19/2013
6
Double Bundle Femoral Tunnel
Double Bundle Femoral Tunnel
Posterior Exposure
9/19/2013
7
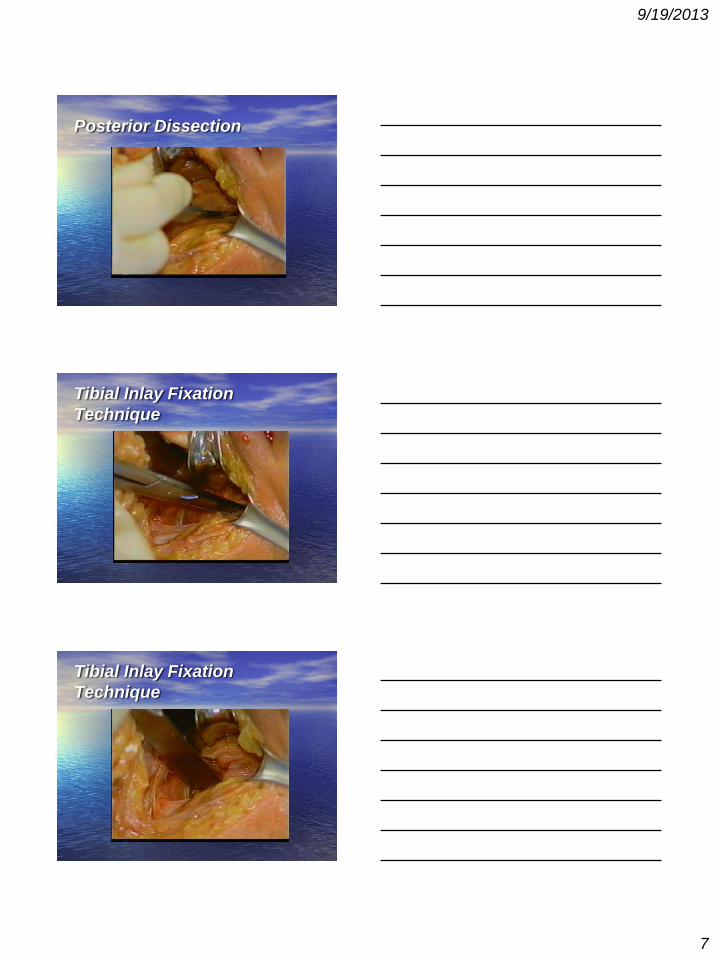
Posterior Dissection
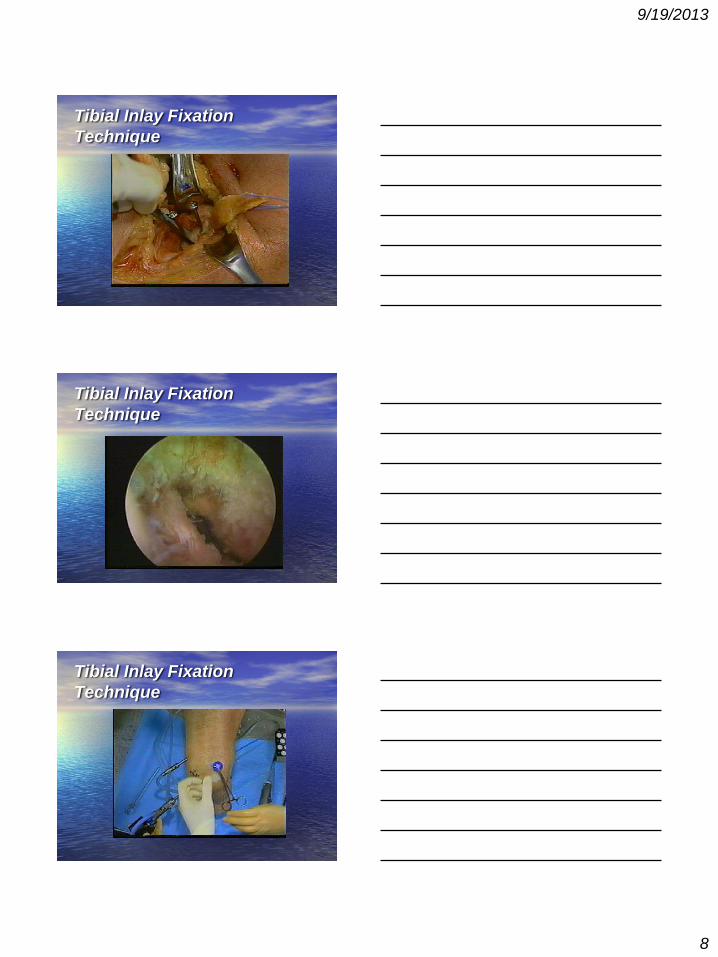
Tibial Inlay Fixation
Technique
Tibial Inlay Fixation
Technique
9/19/2013
8
Tibial Inlay Fixation
Technique
Tibial Inlay Fixation
Technique
Tibial Inlay Fixation
Technique
9/19/2013
9
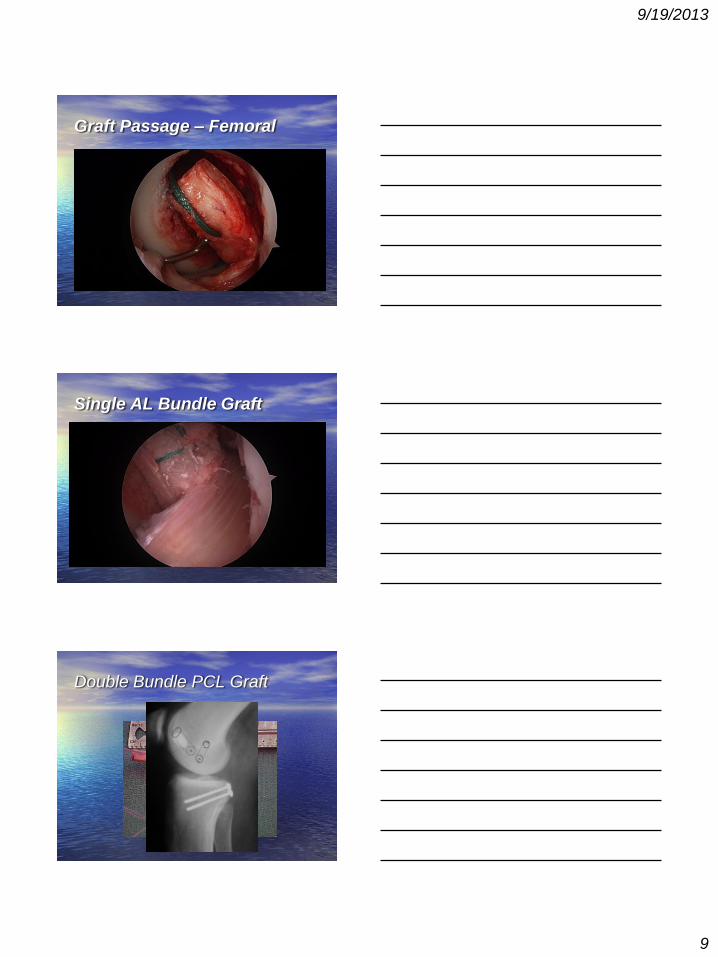
Graft Passage – Femoral
Single AL Bundle Graft
Double Bundle PCL Graft
9/19/2013
10
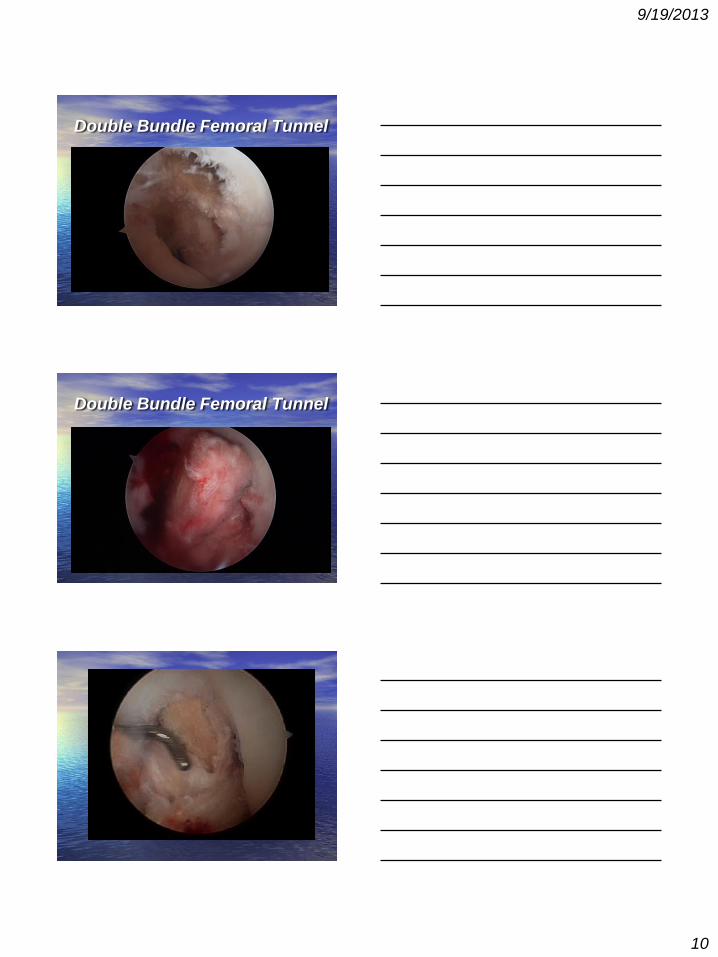
Double Bundle Femoral Tunnel
Double Bundle Femoral Tunnel
9/19/2013
11
Revision PCL Case
• Inlay, not onlay
• Screw - may create
stress riser in bone
plug leading to plug
fractrure
Example Cases
Inlay Revision - Telos
Evaluation
@ 2 yr.. postop
Control Study

9/19/2013
12
Revision PCL Case
Inlay PCL after Prior ACL
+ PCL primary repair
Control Preop Postop
2 yr po Telos
Final Telos Case Examples
9/19/2013
13
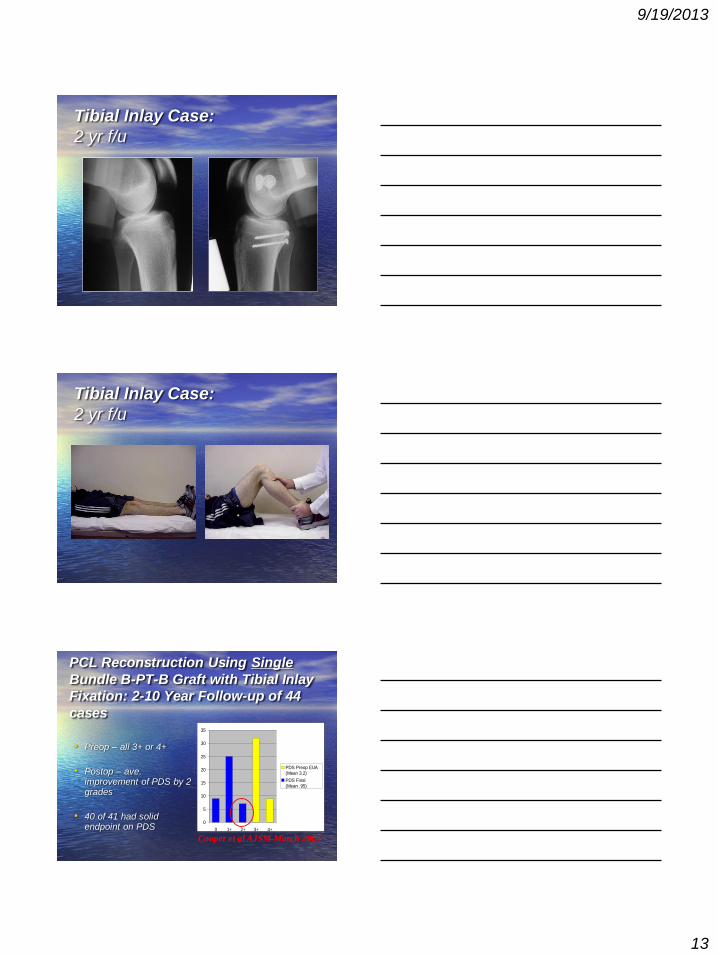
Tibial Inlay Case:
2 yr f/u
Tibial Inlay Case:
2 yr f/u
• Preop – all 3+ or 4+
• Postop – ave. improvement of PDS by 2 grades
• 40 of 41 had solid endpoint on PDS
0
5
10
15
20
25
30
35
0 1+ 2+ 3+ 4+
PDS Preop EUA
(Mean 3.2)
PDS Final
(Mean .95)
PCL Reconstruction Using Single
Bundle B-PT-B Graft with Tibial Inlay
Fixation: 2-10 Year Follow-up of 44
cases
Cooper et al AJSM March 2004

9/19/2013
14
• Ave. 4.1 mm –
whole study group
(-2 - 10mm)
• Ave. roughly 1+
PDS
• 20% - 8/41 cases
had 8-10 mm
Final Telos
0
2
4
6
8
10
12
14
16
18
-2 0 2 4 6 8 10
Final Telos
(Mean 4.11 mm)
Cooper et al AJSM March 2004
PCL Reconstruction Using Single
Bundle B-PT-B Graft with Tibial Inlay
Fixation: 2-10 Year Follow-up of 44
cases
-2 0 2 4
6 8 10
• Ave. 4.3 mm –
whole study group
(0-8 mm)
• Ave. roughly 1+
PDS
• 20% - 3/15 cases
had 8 mm PD
Cooper, unpublished 2007
PCL Reconstruction Using Double
Bundle B-PT-B Graft with Tibial Inlay
Fixation: 1 Year Follow-up of 15
cases
Conclusion
Tibial Inlay Technique:
• My initial experience with revision PCL reconstruction using inlay fixation technique led me to further use.
• Better endpoint to posterior translation
• Average SSD 4.2 mm - equates to average of < 1+ posterior drawer (Series with 70% combined ligament reconstruction)
9/19/2013
15
Conclusion
Tibial Inlay Technique: • Has advantages and
disadvantages (positioning)
• Useful in revision cases
• I think it is worth the hassle
• Need to compare 1 vs. 2 bundle techniques – with inlay not tibial tunnel !
• Is 2 bundle worth the hassle?
THANK YOU
Daniel E. Cooper, M.D.
W.B. Carrell Memorial Clinic
Dallas, Texas
10/7/2013
1
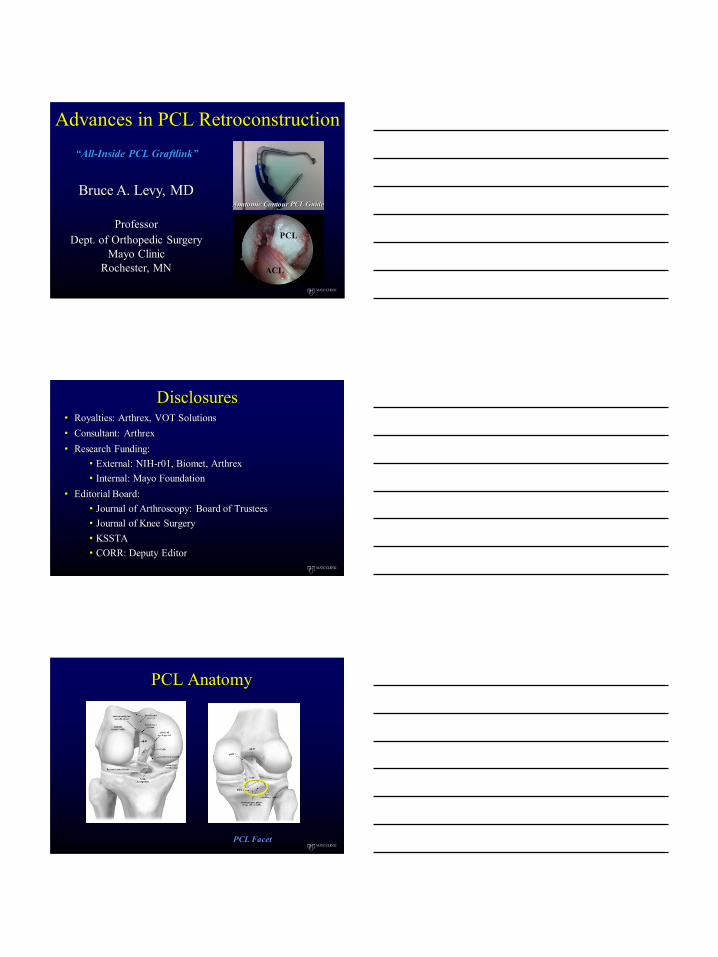
Advances in PCL Retroconstruction
Bruce A. Levy, MD
Professor
Dept. of Orthopedic Surgery
Mayo Clinic
Rochester, MN
PCL
ACL
Anatomic Contour PCL Guide
“All-Inside PCL Graftlink”
Disclosures
• Royalties: Arthrex, VOT Solutions
• Consultant: Arthrex
• Research Funding:
• External: NIH-r01, Biomet, Arthrex
• Internal: Mayo Foundation
• Editorial Board:
• Journal of Arthroscopy: Board of Trustees
• Journal of Knee Surgery
• KSSTA
• CORR: Deputy Editor
PCL Facet
PCL Anatomy

10/7/2013
2
Arthroscopic Inlay
Advances in PCL Retroconstruction
Arthroscopic Inlay
Achilles with bone block
ACL/PCL/MCL
10/7/2013
3
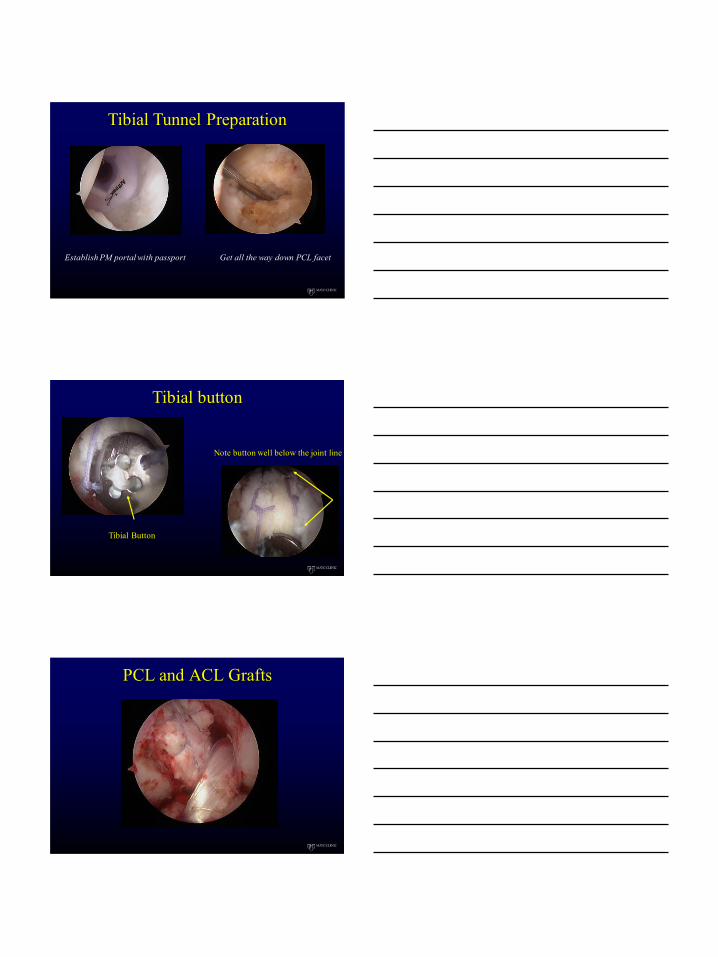
Tibial Tunnel Preparation
Establish PM portal with passport Get all the way down PCL facet
Tibial button
Tibial Button
Note button well below the joint line
PCL and ACL Grafts
10/7/2013
4
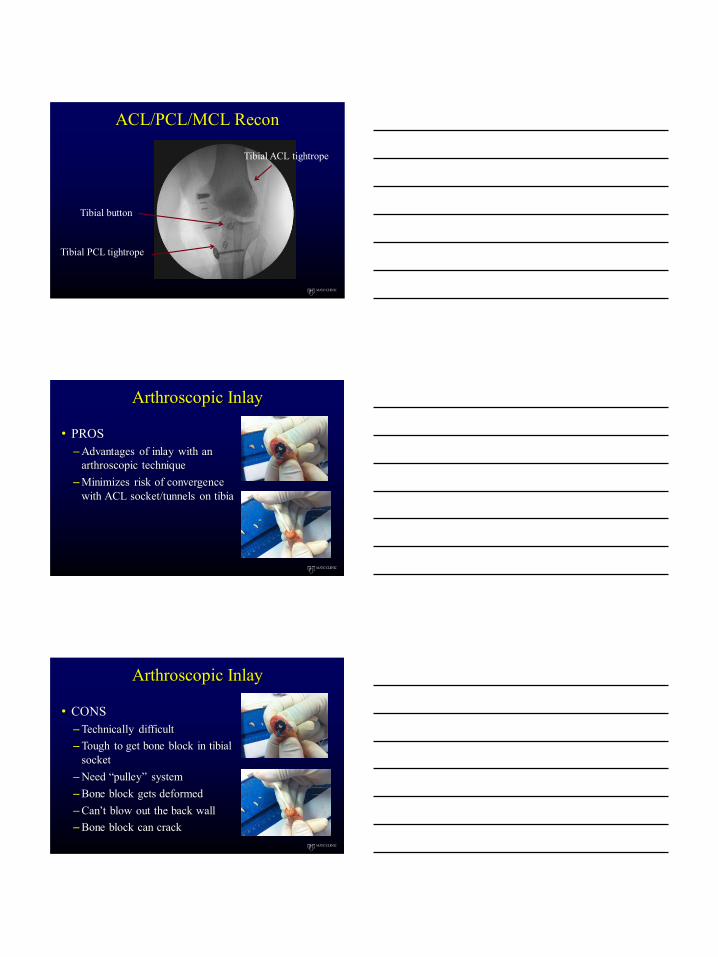
ACL/PCL/MCL Recon
Tibial button
Tibial PCL tightrope
Tibial ACL tightrope
Arthroscopic Inlay
• PROS
–Advantages of inlay with an
arthroscopic technique
–Minimizes risk of convergence
with ACL socket/tunnels on tibia
Arthroscopic Inlay
• CONS
–Technically difficult
–Tough to get bone block in tibial
socket
–Need “pulley” system
–Bone block gets deformed
–Can’t blow out the back wall
–Bone block can crack
10/7/2013
5
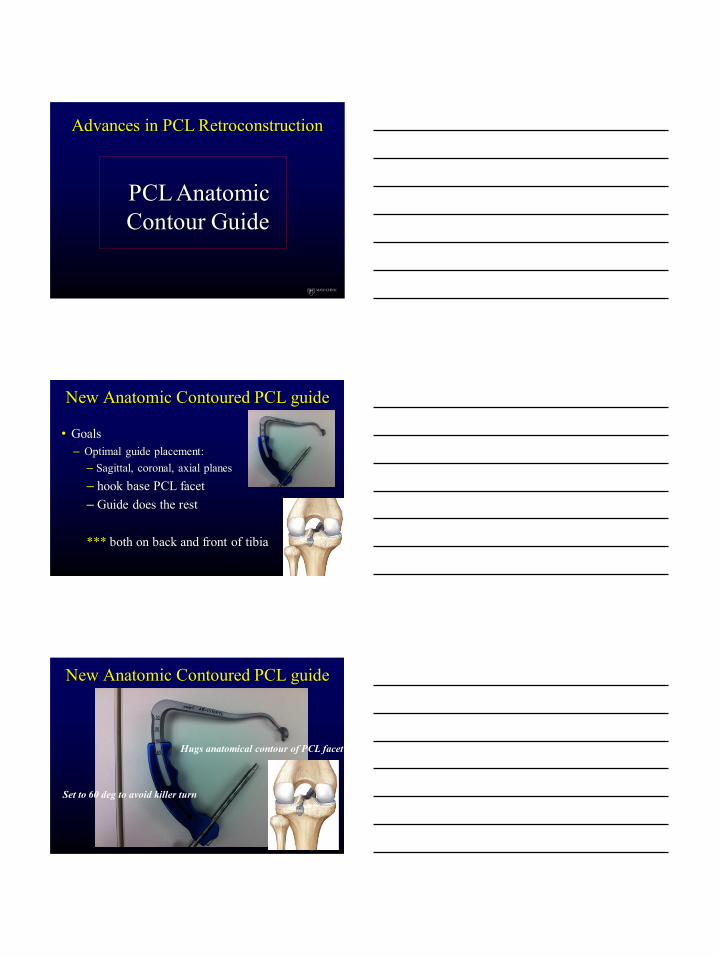
PCL Anatomic
Contour Guide
Advances in PCL Retroconstruction
New Anatomic Contoured PCL guide
• Goals
– Optimal guide placement:
– Sagittal, coronal, axial planes
– hook base PCL facet
– Guide does the rest
*** both on back and front of tibia
New Anatomic Contoured PCL guide
Hugs anatomical contour of PCL facet
Set to 60 deg to avoid killer turn
10/7/2013
6
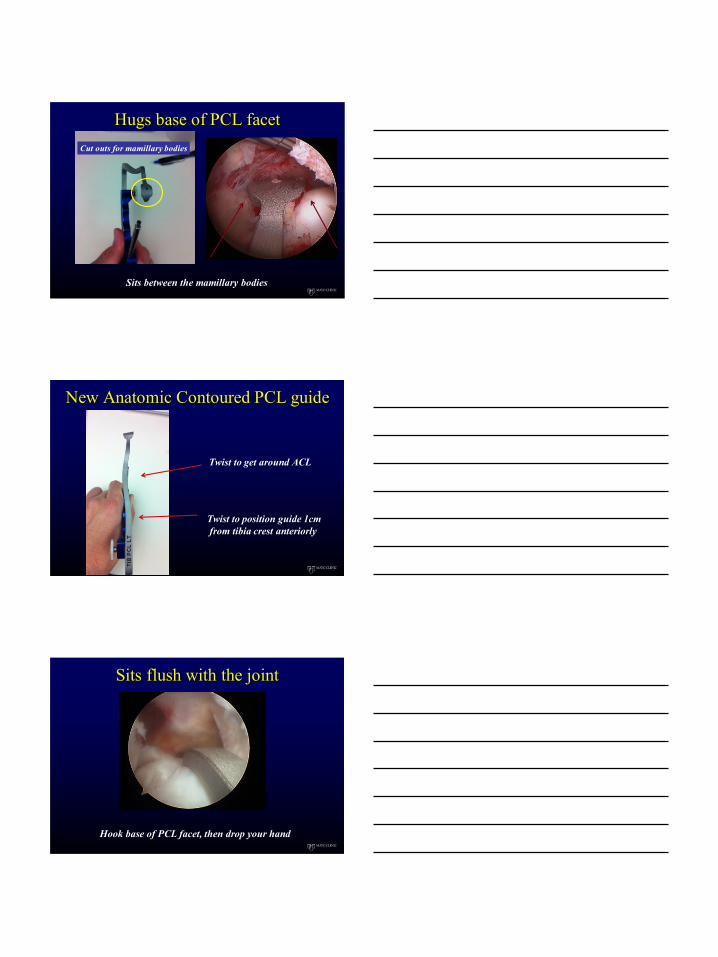
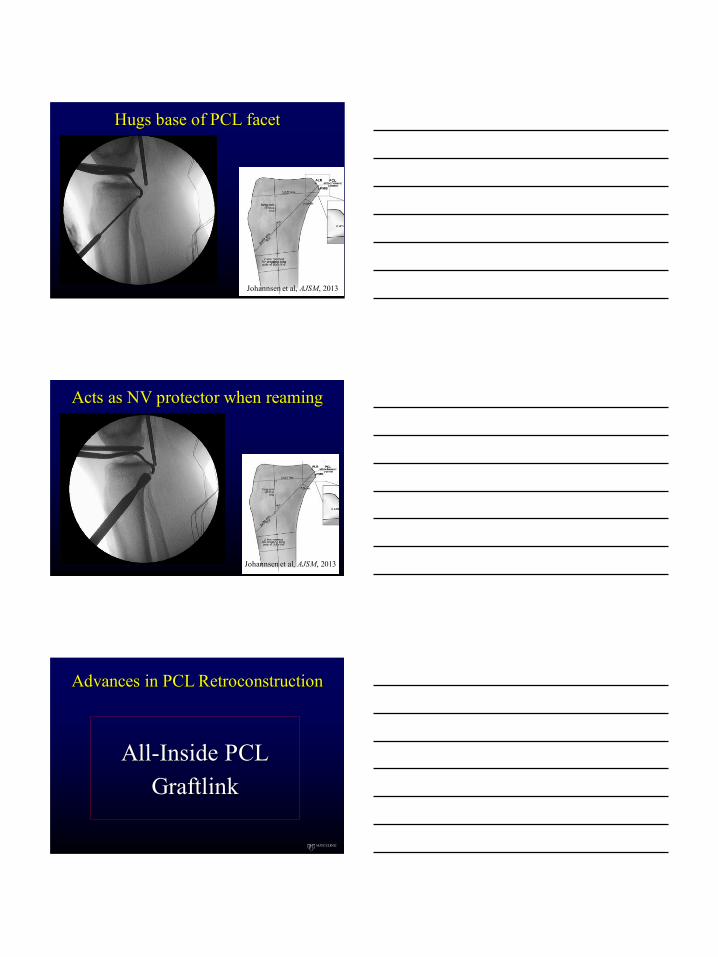
Hugs base of PCL facet
Sits between the mamillary bodies
Cut outs for mamillary bodies
New Anatomic Contoured PCL guide
Twist to get around ACL
Twist to position guide 1cm
from tibia crest anteriorly
Sits flush with the joint
Hook base of PCL facet, then drop your hand
10/7/2013
7
Hugs base of PCL facet
Johannsen et al, AJSM, 2013
Acts as NV protector when reaming
Johannsen et al, AJSM, 2013
All-Inside PCL
Graftlink
Advances in PCL Retroconstruction
10/7/2013
8
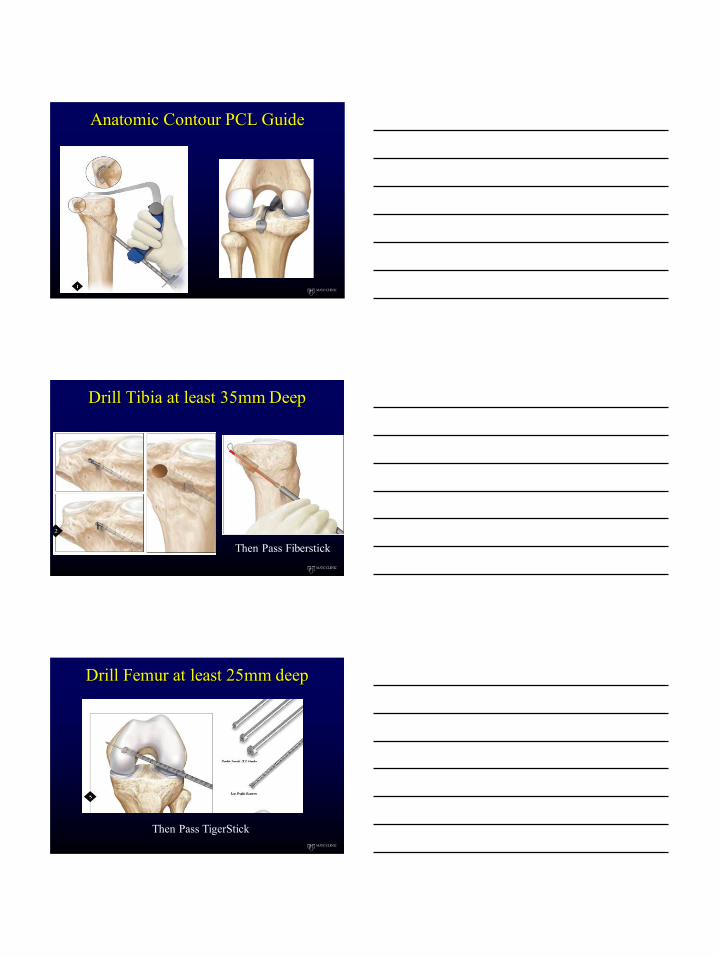
Anatomic Contour PCL Guide
Drill Tibia at least 35mm Deep
Then Pass Fiberstick
Drill Femur at least 25mm deep
Then Pass TigerStick

10/7/2013
9
Graft Passage – Tibia First
Tibia first Femur second
Final Step: Secure Tibia side
ABS Button END of procedure
CASE DS
Knee Dislocation
ACL/PCL/MCL/PMC
10/7/2013
10
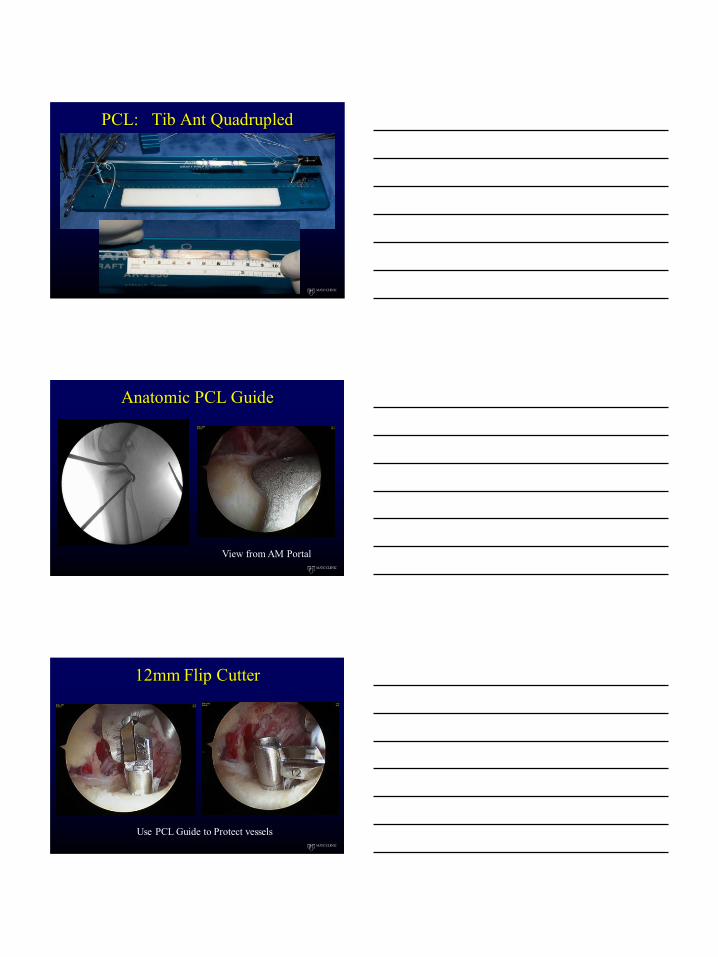
PCL: Tib Ant Quadrupled
Anatomic PCL Guide
View from AM Portal
12mm Flip Cutter
Use PCL Guide to Protect vessels
10/7/2013
11
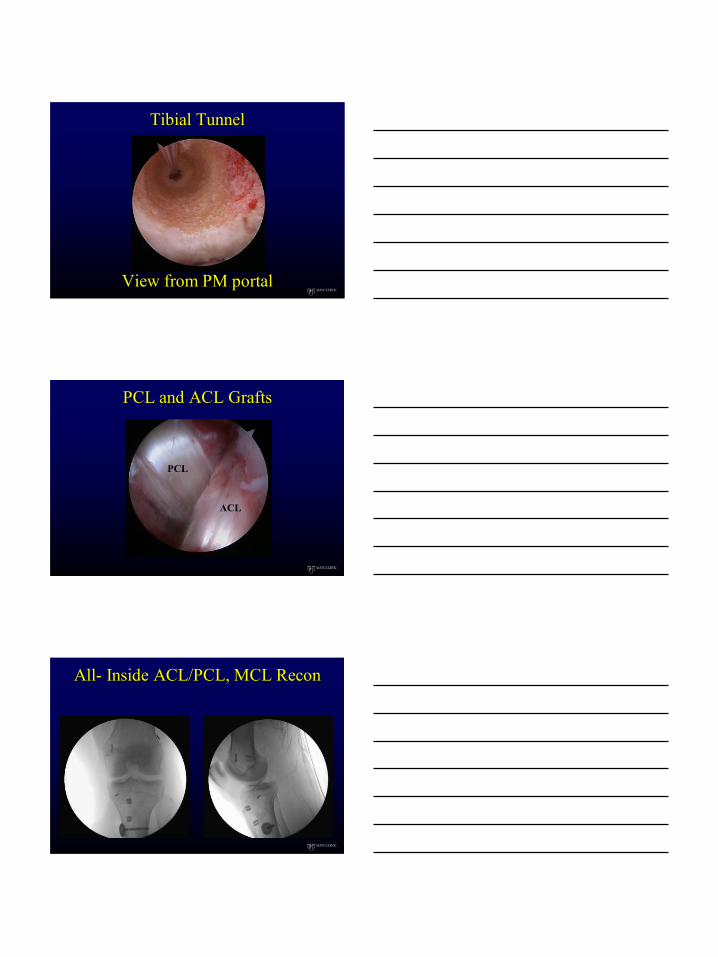
Tibial Tunnel
View from PM portal
PCL and ACL Grafts
PCL
ACL
All- Inside ACL/PCL, MCL Recon
10/7/2013
12
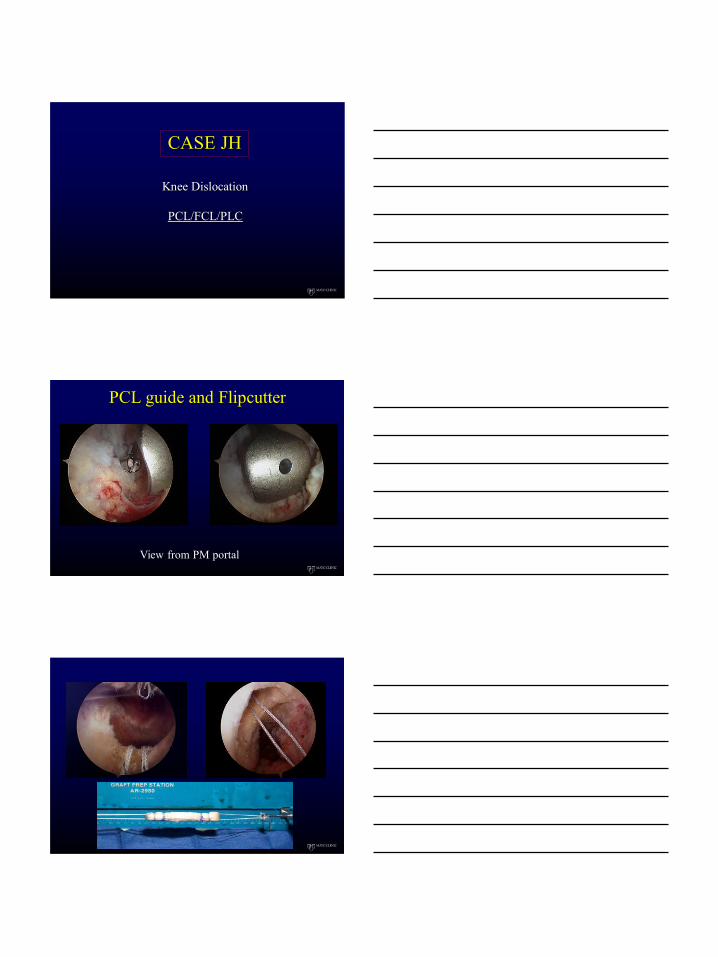
CASE JH
Knee Dislocation
PCL/FCL/PLC
PCL guide and Flipcutter
View from PM portal
10/7/2013
13
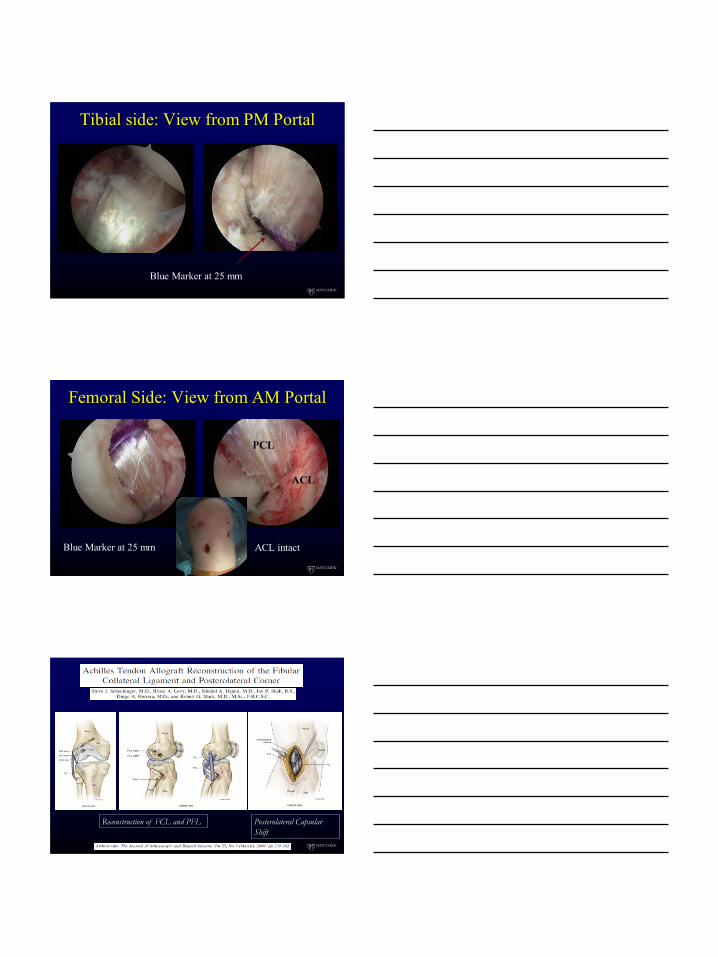
Tibial side: View from PM Portal
Blue Marker at 25 mm
Femoral Side: View from AM Portal
Blue Marker at 25 mm ACL intact
ACL
PCL
Reconstruction of FCL and PFL Posterolateral Capsular
Shift
10/7/2013
14
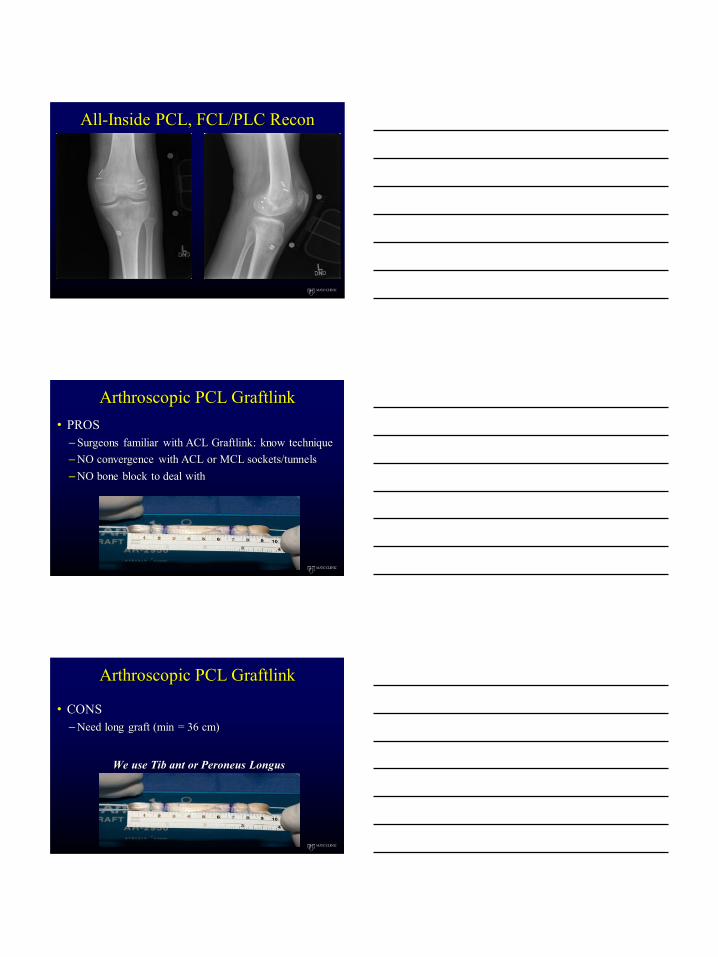
All-Inside PCL, FCL/PLC Recon
Arthroscopic PCL Graftlink
• PROS
–Surgeons familiar with ACL Graftlink: know technique
–NO convergence with ACL or MCL sockets/tunnels
–NO bone block to deal with
Arthroscopic PCL Graftlink
• CONS
–Need long graft (min = 36 cm)
We use Tib ant or Peroneus Longus
10/7/2013
15
THANK YOU

9/20/2013
1
GC Fanelli
PCL Reconstruction: Transtibial
Tunnel Surgical Technique
Gregory C. Fanelli, M.D.
115 Woodbine Lane
Danville, PA 17822-5212
570-271-6700
GC Fanelli
Disclosure • Royalties:
– Springer
• PCL Textbooks
• Multiple Ligament Injured Knee Textbooks
• Stock options: None
• Consultant:
– Biomet Sports Medicine
• PCL ACL Instrumentation System
– MTF
• Surgeon Advisory Board
• Research support: None
• Educational support: None
• Other support: None
GC Fanelli
Presentation Overview
• Surgical anatomy
• Graft selection
• Reasons for failure
• PCL reconstruction principles
– Applies to SB or DB reconstruction
• Surgical technique
• Postoperative rehabilitation
• Results
• Summary
9/20/2013
2
GC Fanelli
PCL Injuries In Trauma Patients: Part II G. Fanelli, C. Edson, 1995
Arthroscopy Vol. 11, No 5, 1995
• Acute Knee Injuries 222
• PCL Tears 85 (38.3%)
• Multiple Trauma Related 48 (56.5%)
• Sports Related 28 (32.9%)
• PCL/Multiple Ligaments 82 (96.5%)
• PCL/Isolated 3 (3.5%)
• Combined ACL/PCL 39 (45.9%)
• PCL/PLC 35 (41.2%)
• ACL/PCL (% total) 17.6%
GC Fanelli
Correct Diagnosis
• Planes of instability
• PCL ACL: anterior posterior translation
• Lateral and medial collateral ligament complex
– (A) axial rotation instability only
– (B) axial rotation instability + varus and/or valgus laxity
with firm end point
– (C) axial rotation instability + varus and/or valgus laxity
with no end point
• Fanelli, Operative Techniques Sports Medicine, 1999
• Fanelli, Techniques in Knee Surgery, 2007
• Recognition and correction of collateral instability is the
key to successful posterior and anterior cruciate ligament
surgery
GC Fanelli
Why do PCL surgeries fail?
9/20/2013
3
GC Fanelli
• Conclusions
– Associated ligament instabilities
• Missed or failed PLI reconstruction
– Sekiya, AJSM, 2005
• Don’t forget posteromedial reconstruction
– Robinson, AJSM, 2006
– Varus osseous malalignment
– Incorrect tunnel placement
PCL Revision Reconstruction Part I
Causes of Surgical Failure Noyes, Barber-Westin, AJSM, 2005, 33 (5)
GC Fanelli
PCL Reconstruction Principles
• Identify and treat all pathology
• Protect neuro-vascular structures
• Accurate tunnel placement
• Anatomic graft insertion sites
• Strong graft material
• Minimize graft bending
• Restore anatomic tibial step off
• Mechanical graft tensioning boot
• Secure primary and back up fixation
• Slow postoperative rehabilitation program
GC Fanelli
Graft Selection
Lee, Arthroscopy, 2004
Fulkerson, Arthroscopy, 1995
9/20/2013
4
GC Fanelli
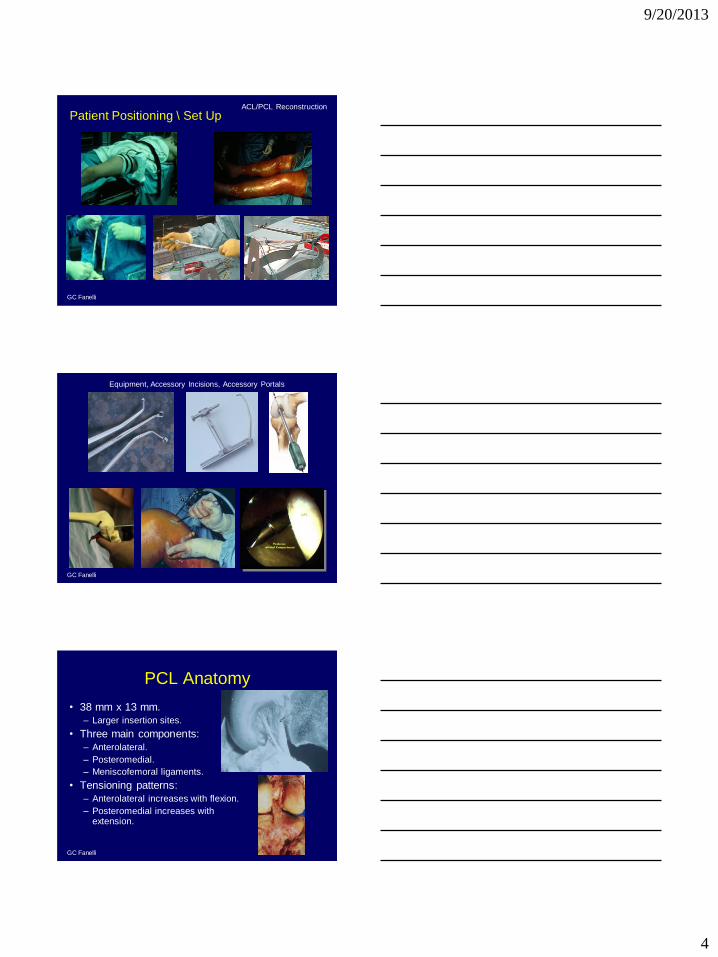
Patient Positioning \ Set Up ACL/PCL Reconstruction
GC Fanelli
Equipment, Accessory Incisions, Accessory Portals
GC Fanelli
PCL Anatomy
• 38 mm x 13 mm.
– Larger insertion sites.
• Three main components:
– Anterolateral.
– Posteromedial.
– Meniscofemoral ligaments.
• Tensioning patterns:
– Anterolateral increases with flexion.
– Posteromedial increases with extension.
9/20/2013
5
GC Fanelli
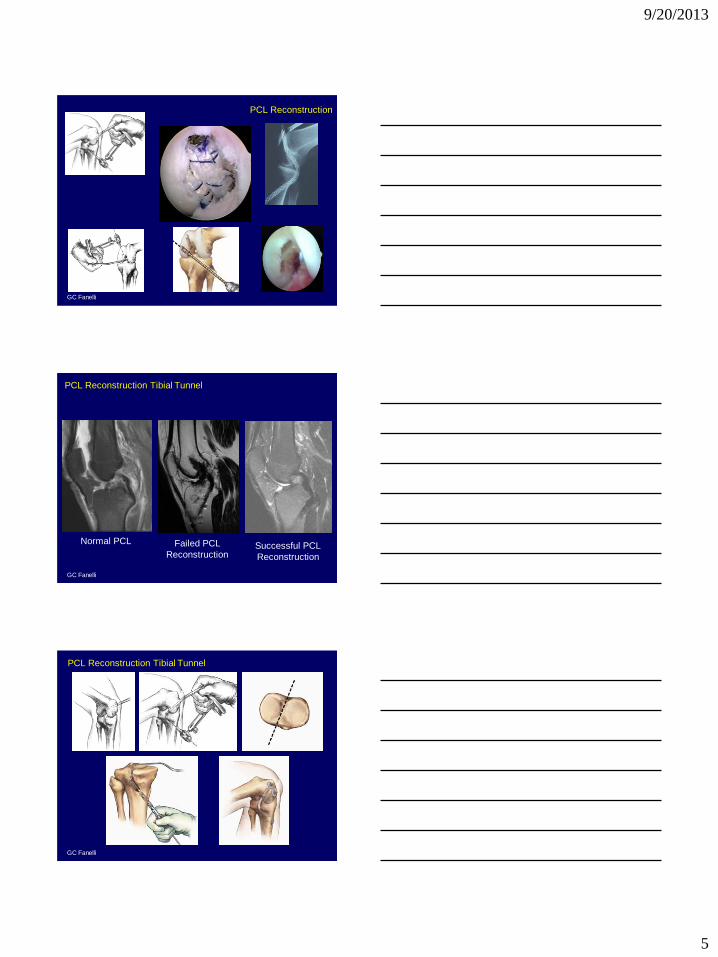
PCL Reconstruction
GC Fanelli
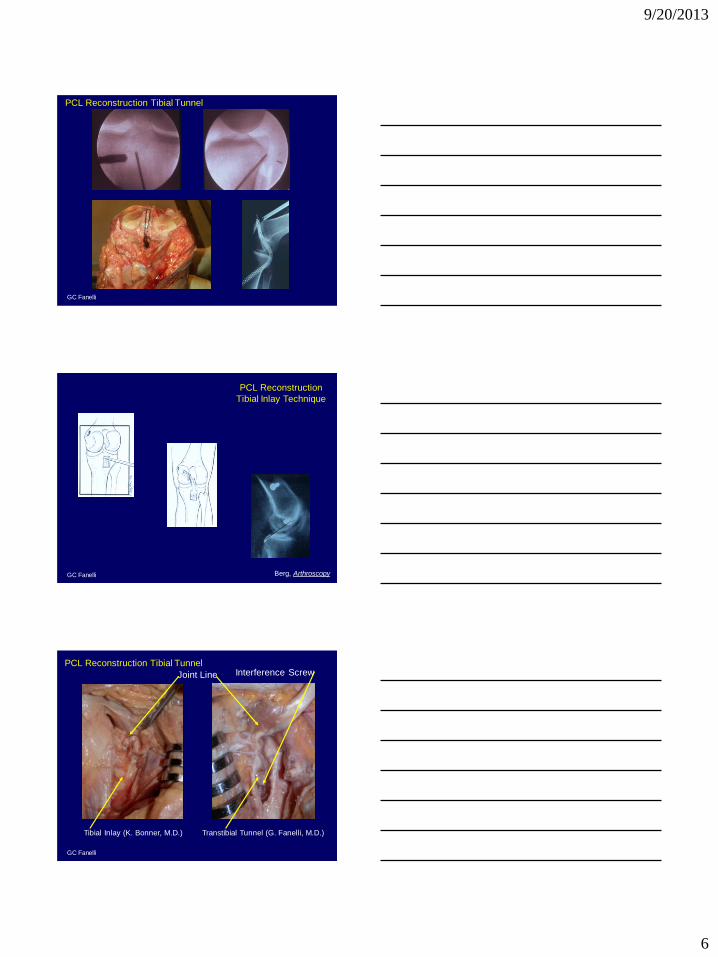
PCL Reconstruction Tibial Tunnel
Normal PCL Failed PCL
Reconstruction Successful PCL
Reconstruction
GC Fanelli
PCL Reconstruction Tibial Tunnel
9/20/2013
6
GC Fanelli
PCL Reconstruction Tibial Tunnel
GC Fanelli
PCL Reconstruction
Tibial Inlay Technique
Berg, Arthroscopy
GC Fanelli
Tibial Inlay (K. Bonner, M.D.) Transtibial Tunnel (G. Fanelli, M.D.)
PCL Reconstruction Tibial Tunnel
Joint Line Interference Screw
9/20/2013
7
GC Fanelli
GC Fanelli
GC Fanelli
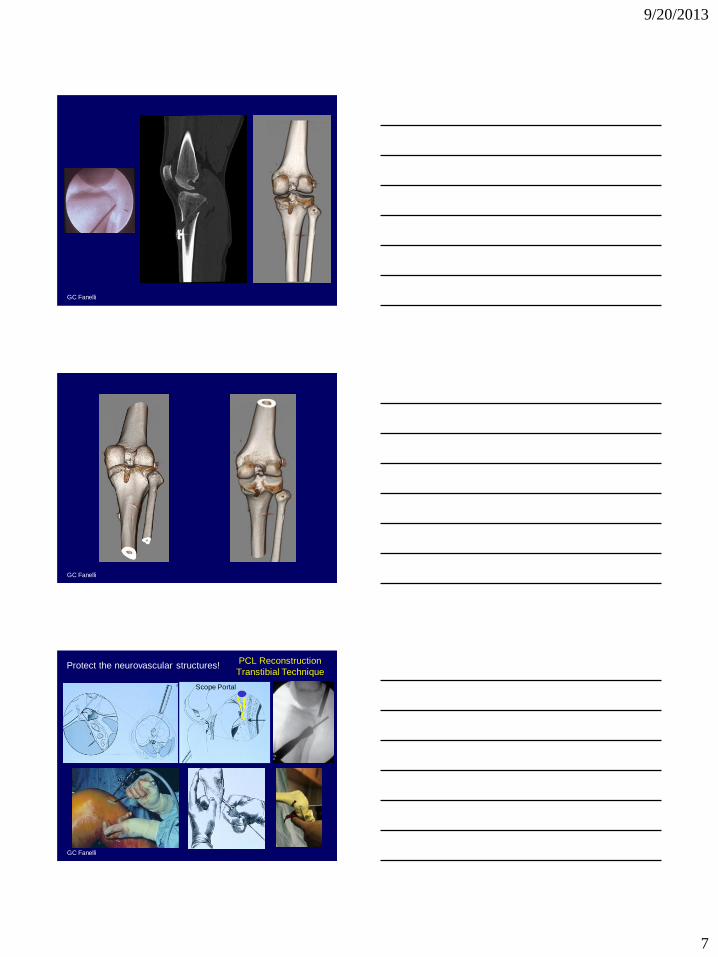
PCL Reconstruction
Transtibial Technique Protect the neurovascular structures!
Scope Portal
9/20/2013
8
GC Fanelli
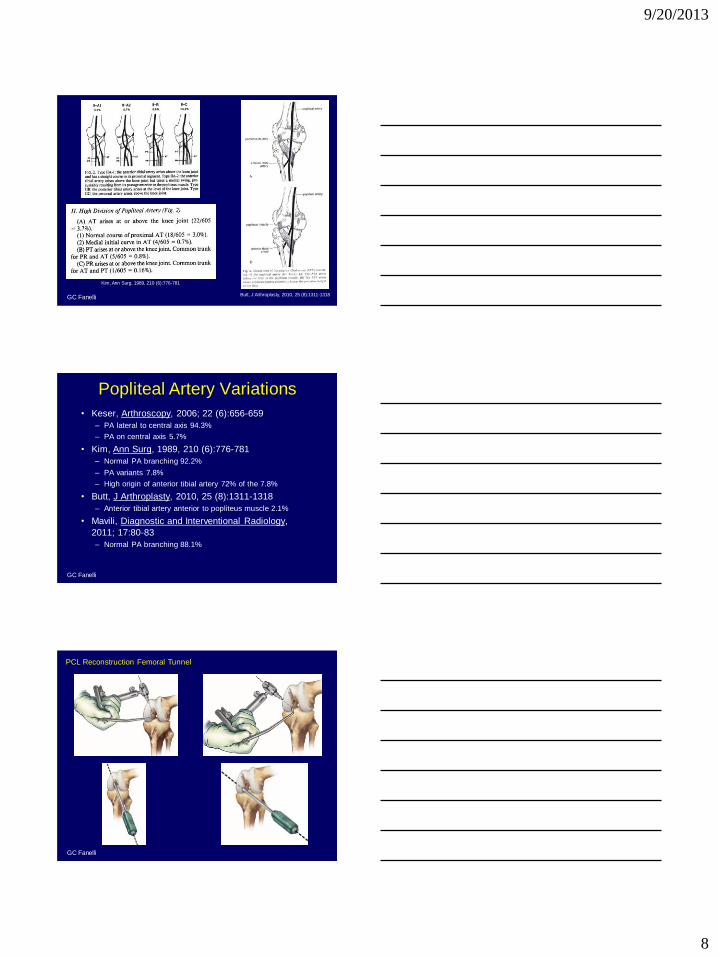
Kim, Ann Surg, 1989, 210 (6):776-781
Butt, J Arthroplasty, 2010, 25 (8):1311-1318
GC Fanelli
Popliteal Artery Variations
• Keser, Arthroscopy, 2006; 22 (6):656-659
– PA lateral to central axis 94.3%
– PA on central axis 5.7%
• Kim, Ann Surg, 1989, 210 (6):776-781
– Normal PA branching 92.2%
– PA variants 7.8%
– High origin of anterior tibial artery 72% of the 7.8%
• Butt, J Arthroplasty, 2010, 25 (8):1311-1318
– Anterior tibial artery anterior to popliteus muscle 2.1%
• Mavili, Diagnostic and Interventional Radiology,
2011; 17:80-83
– Normal PA branching 88.1%
GC Fanelli
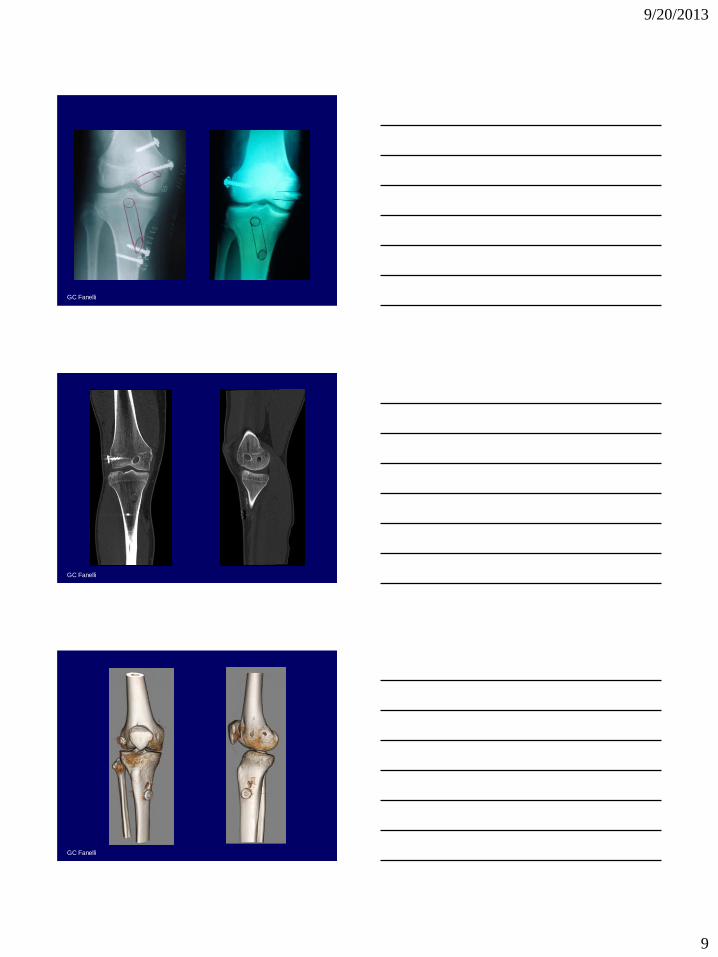
PCL Reconstruction Femoral Tunnel
9/20/2013
9
GC Fanelli
GC Fanelli
GC Fanelli
9/20/2013
10
GC Fanelli
GC Fanelli
GC Fanelli
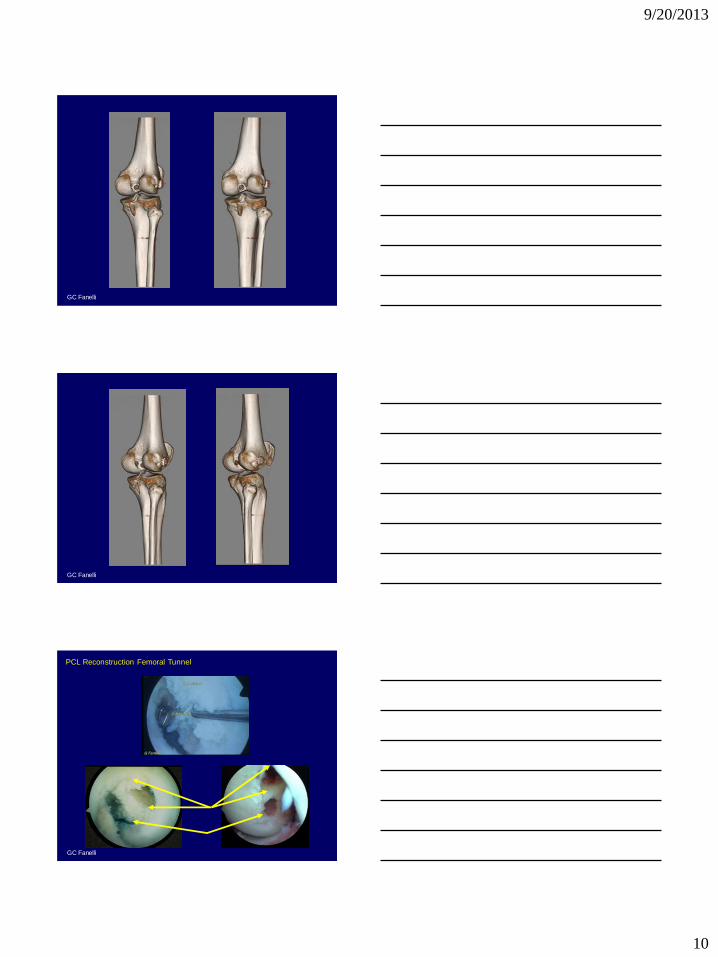
PCL Reconstruction Femoral Tunnel
9/20/2013
11
GC Fanelli
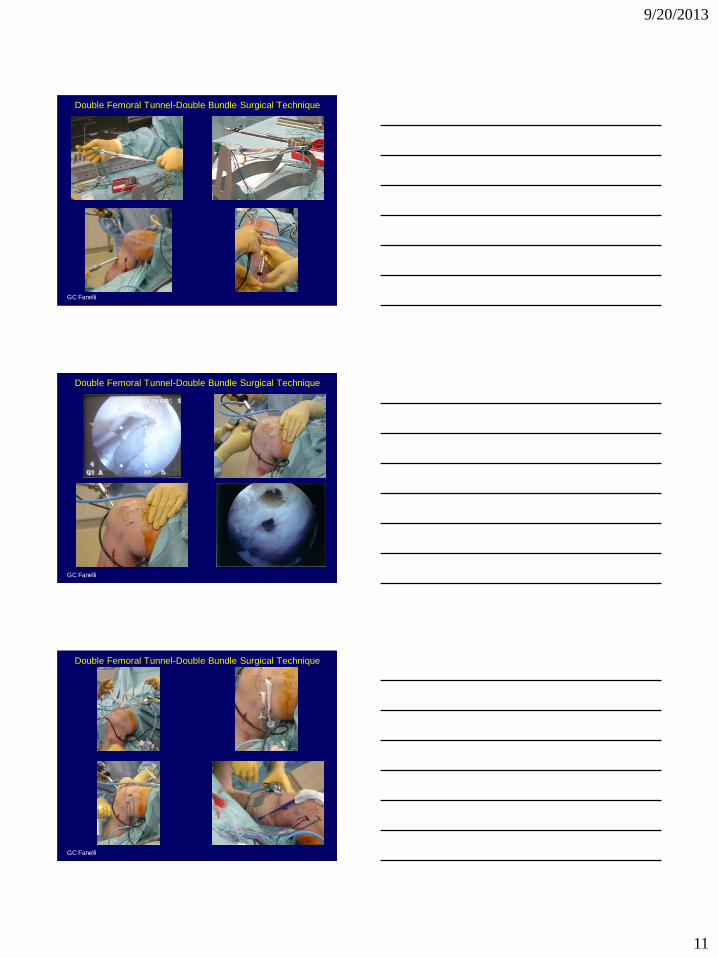
Double Femoral Tunnel-Double Bundle Surgical Technique
GC Fanelli
Double Femoral Tunnel-Double Bundle Surgical Technique
GC Fanelli
Double Femoral Tunnel-Double Bundle Surgical Technique
9/20/2013
12
GC Fanelli
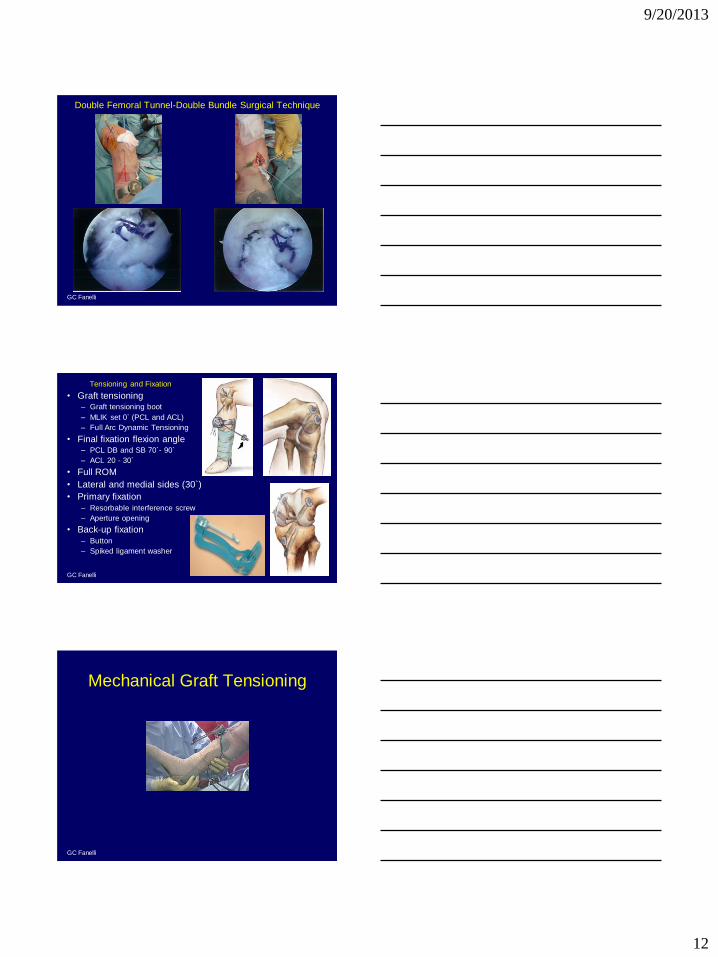
Double Femoral Tunnel-Double Bundle Surgical Technique
GC Fanelli
Tensioning and Fixation
• Graft tensioning – Graft tensioning boot
– MLIK set 0` (PCL and ACL)
– Full Arc Dynamic Tensioning
• Final fixation flexion angle – PCL DB and SB 70`- 90`
– ACL 20 - 30`
• Full ROM
• Lateral and medial sides (30`)
• Primary fixation – Resorbable interference screw
– Aperture opening
• Back-up fixation – Button
– Spiked ligament washer
GC Fanelli
Mechanical Graft Tensioning
9/20/2013
13
GC Fanelli
GC Fanelli
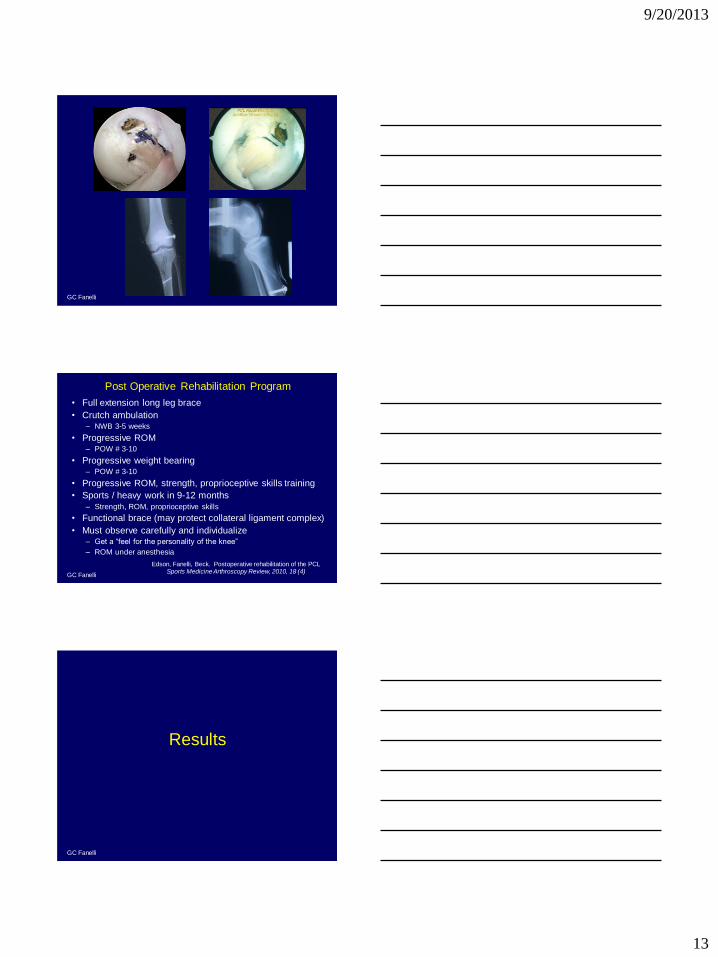
Post Operative Rehabilitation Program
• Full extension long leg brace
• Crutch ambulation – NWB 3-5 weeks
• Progressive ROM – POW # 3-10
• Progressive weight bearing – POW # 3-10
• Progressive ROM, strength, proprioceptive skills training
• Sports / heavy work in 9-12 months – Strength, ROM, proprioceptive skills
• Functional brace (may protect collateral ligament complex)
• Must observe carefully and individualize – Get a “feel for the personality of the knee”
– ROM under anesthesia
Edson, Fanelli, Beck. Postoperative rehabilitation of the PCL Sports Medicine Arthroscopy Review, 2010, 18 (4)
GC Fanelli
Results
9/20/2013
14
GC Fanelli
PCL Reconstruction Results
• Fanelli, Edson, Giannotti. AA combined ACL PCL reconstruction.
Arthroscopy, 1996
• Fanelli, Edson. AA PCL posterolateral reconstruction. 2-10 year
results. Arthroscopy, 2004
• Fanelli, Edson. AA assisted combined ACL PCL reconstruction. 2-10
year results. Arthroscopy, 2002
– No graft tensioning boot
• Fanelli, Edson, et al. Treatment of combined ACL PCL MCL PLC
injuries of the knee. J Knee Surgery, 2005
– Tensioning boot utilized
• Fanelli, Beck, Edson. Single compared to double bundle PCL
reconstruction using allograft tissue. J Knee Surgery, 2012
• Fanelli, Edson. Combined PCL ACL lateral and medial side (global
laxity) reconstruction. Technique and 2 to 18 year results. J Knee
Surgery , 2012
GC Fanelli
Fanelli GC, Giannotti B, Edson CJ. Arthroscopically assisted combined
ACL/PCL reconstruction. Arthroscopy, 1996; 12(1):5-14.
• 20 AA ACL/PCL reconstructions.
• Minimum 2 yr. f/u (24-48 months).
• 16 M, 4 F, 9 R, 11 L, 10 acute, 10 chronic.
• 14 AT allograft, 6 BTB autograft.
• PLC: Clancy BTT, primary repair prn.
• Tegner, Lysholm, HSS all improved preop to postop (p=0.0001)
• No SS difference auto-allo, acute-chronic
• KT 1000 Corrected anterior (p=0.0078)
• Lachman (15 Normal) Pivot shift (17 Normal)
• Posterior drawer/tibial step-off.
– Normal 9/20 Grade I 11/20
• All PLI corrected (ERTFA, PLD tests).
– 1 = Normal knee 11 < Normal knee
• All MCL tears corrected (30` vlagus stress).
– Brace (7) = Surgery (2)
GC Fanelli
AA PCL/PLC Reconstruction 2-10 Year Follow-Up
Fanelli, Edson, Arthroscopy 2004, 20 (4): 339-345
• Study type: case series
• 41 chronic PCL/PLC reconstructions
– 3 months to 20 years
– Follow-up rate 41/53 (77.4%)
• 31 M, 10 F, 24 L, 17 R
• Surgical Technique
– PCL AA, SFT, SB, TTT • FF-ATAL 41
– PLC BTT, PLC shift, primary repair. • CBTT 24
• SBTT 17
9/20/2013
15
GC Fanelli
AA PCL/PLC Reconstruction 2-10 Year Follow-Up Results
Fanelli, Edson, Arthroscopy 2004, 20 (4): 339-345
• Posterior Drawer-Tibial Step Off
– Normal 29/41 (70%)
– Grade 1 11/41 (27%)
– Grade 2 1/41 (3%)
• Biomet Tensioning Boot
– 12/41 (29.3%)
– Normal 11/12 (91.7%)
– Grade 1 1/12 (8.3%)
Effect of Graft Tensioning Boot: PCL Reconstruction
GC Fanelli
Combined PCL PLC reconstruction with ATAL and BFTT: 2-10
year follow-up.
GC Fanelli, CJ Edson, Arthroscopy 2004; 20 (4): 339-345
• 41 arthroscopic PCL PLC reconstructions
• PCL: 41 fresh frozen Achilles tendon allografts
• PLC: BFT transfer, PL capsular shift, primary repair
– CBTT 24
– SBTT 17
• ERTFA-Dial Test
– I < N 29/41 (71%)
– I = N 11/41 (27%)
– I > N 1/29 (2%)
• 30` Varus
– Normal 40/41 (97%)
– Grade 1 1/41 (3%)
GC Fanelli
• SS improvement pre op to post op
– All parameters (p = 0.001)
• No SS difference (p > 0.05)
– Acute-chronic, autograft-allograft
– Lysholm, Tegner, HSS, KT 1000, Telos
• Lachman/pivot shift negative (94%)
• Dial corrected (100%)
• Varus corrected (88%)
• Valgus corrected (S 100%), (B 87.5%)
• PD Normal (46%)
– No mechanical graft tensioning boot
• Telos SSD (21/35)
– 0-3 mm (52.3%), 4-5 mm (23.8%), 6-10 mm (19.0%)
AA Combined ACL/PCL Reconstruction
2-10 Year Follow-Up Results G. Fanelli, C. Edson, Arthroscopy, 2002; 18 (7)
9/20/2013
16
GC Fanelli
• Posterior drawer – Normal 13/15 (86.66%)
– 1+ 1/15 (6.66%)
– 2+ 1/15 (6.66%)
• Normal – Lachman 13/15 (86.6%)
– Pivot shift 14/15 (93.3%)
• Dial – 9/11 (81.8%) = NL
– 2/11 (18.2%) < NL
• Varus 30` – S=NS 11/11 (100%)
• Valgus 30` – S=NS 9/9 (100%)
• Telos Stress
Radiography
– SSD mm
– 0-3 mm 10/15 (66.66%)
– 0-4 mm 14/15 (93.3%)
– 4 mm 4/15 (26.66%)
– 7 mm 1/15 (6.66%)
• KT 1000 SSD mm
– PCL screen 1.6 (-3 to 7)
– CP 1.6 (-4.5 to 9)
– CA 0.5 (-2.5 to 6)
• 15 PCL ACL recon
– 2 year follow up
ACL PCL Reconstruction With Mechanical Graft Tensioner GC Fanelli, CJ Edson, Journal of Knee Surgery, July, 2005
GC Fanelli
• 90 consecutive PCL reconstructions (SB = DB = 45)
– KD SB 22, KD DB 25
• No SS difference SB vs. DB (p > 0.05)
• Static stability
– KT 1000 at 90`, 70`, 30` knee flexion
– Telos 90` stress radiography
• Acute SB vs. DB reconstructions
– Telos stress radiography
• 90` knee flexion, PTD force at TT
• No SS difference (p = 0.396)
• Chronic SB vs. DB reconstructions
– Telos stress radiography
• 90` knee flexion, PTD force at TT
• No SS difference (p = 0.416)
Single vs. Double Bundle PCL Reconstruction Fanelli, Beck, Edson. J Knee Surgery, 2012; 25(1):59-64
GC Fanelli
Overall Group
Single Bundle
34/45
75.6%
Double Bundle
30/45
66.7% p = 0.358
PCL Collateral
Ligament Group
Single Bundle 20/23 86.9%
Double Bundle 15/18 83.3% P = 0.756
Bi-cruciate Group
Single Bundle 17/22 73.3%
Double Bundle 21/25 84.0% P = 0.572
Single vs. Double Bundle PCL Reconstruction
Return to Pre-Injury Level of Function
No SS difference
9/20/2013
17
GC Fanelli
Fanelli, Edson. Combined PCL ACL lateral and medial side (global laxity) reconstruction.
Technique and 2 to 18 year results. J Knee Surgery, 2012; 25 (4)
• 40 combined PCL ACL lateral medial reconstructions (worst of the worst)
• 28/40 available 2 to 18 year follow up (70% follow up rate)
• Knee ligament rating scales Mean (Range)
– HSS 79.3/100 (56 to 95)
– Lysholm 83.8/100 (58 to 100)
– Tegner 4.0/10 (2 to 9)
• KT 1000 SSD mm Mean (Range)
– PCL 90 degree screen 2.02 (0 to 7)
– Corrected posterior 2.48 (0 to 9)
– Corrected anterior 0.28 (-3 to 7)
– 30 degree posterior to anterior 1.0 (-6 to 6)
• Telos stress radiography SSD to test PCL Mean (Range) – 90 degrees flexion posterior displacement force 2.35 (-2 to 8)
• Range of motion flexion loss SSD degrees Mean (Range) 14.0 (0 to 38)
– No flexion contractures
• Symmetrical: varus (93.3%), valgus (92.6%)
• Dial test: symmetrical (85.2%), tighter (11.1%), greater-lax (3.7%)
• Posttraumatic degenerative joint disease: Yes (29.6%) No (70.4%)
• Return to pre injury level of function: Yes (59.3%) No (40.7%)
GC Fanelli
• Identify and treat all pathology (PLI, PMI, alignment)
• Strong graft material
• Accurate tunnel placement
• Anatomic graft insertion sites
• Minimize graft bending
– Preserve PCL tibial remnant
• Mechanical graft tensioning boot
• Primary and back-up fixation
• Appropriate postoperative rehabilitation program
• Successful results SB and DB PCL reconstruction
– No statistically significant difference
– Stress x-ray
– KT 1000
– Knee ligament rating scales
– Patient satisfaction
– DB PCLR indications • Hyperextension
• Revision PCLR
Summary
GC Fanelli
Gregory C. Fanelli, M.D.
115 Woodbine Lane TYJ
Danville, PA 17822-5212
570-271-6700
2013
10/7/2013 10:48 AM
1
Christopher D. Harner, MD Blue Cross of Western Pennsylvania Professor
Medical Director, UPMC Center for Sports Medicine Head Team Physician, Pittsburgh Penguins
Overview
• General philosophy on treatment • My surgical approach
• Set up • Technique • Post op rehab
AL
ACL
PM
PCL Reconstruction AL Component
Observations/Facts
1). Not all PCL injuries are the same 2). Partial PCL injuries exist and the PCL (unlike the ACL) can heal 3). Isolated Grade II PCL injuries are not normal, but do function with minimal symptoms
10/7/2013 10:48 AM
2
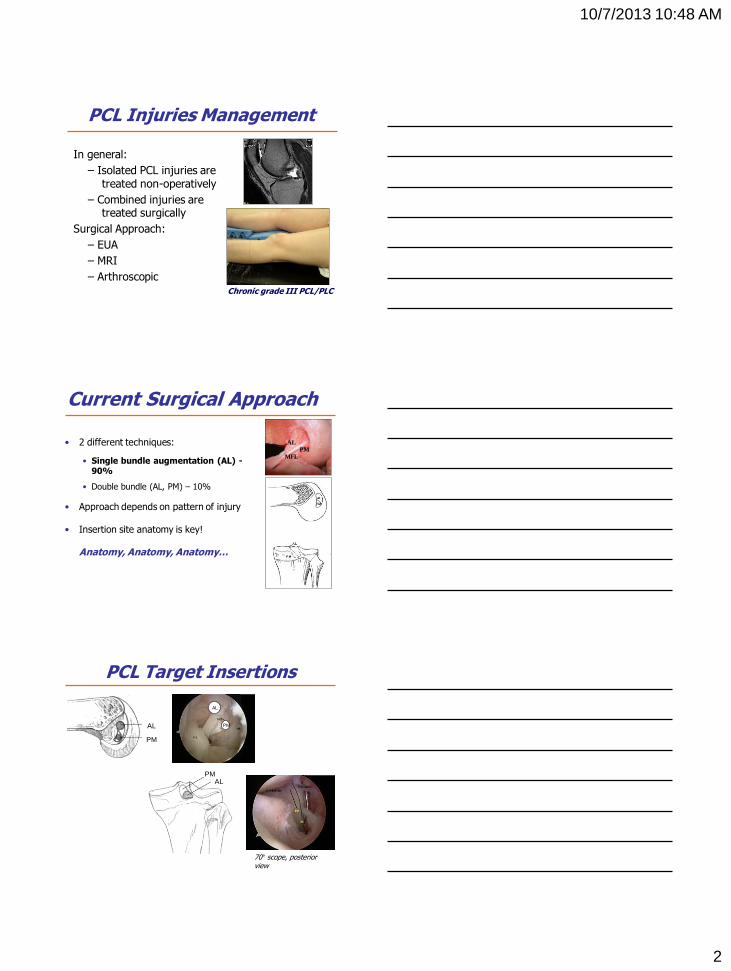
PCL Injuries Management
In general:
– Isolated PCL injuries are treated non-operatively
– Combined injuries are treated surgically
Surgical Approach:
– EUA
– MRI
– Arthroscopic Chronic grade III PCL/PLC
Current Surgical Approach
• 2 different techniques:
• Single bundle augmentation (AL) - 90%
• Double bundle (AL, PM) – 10%
• Approach depends on pattern of injury
• Insertion site anatomy is key!
Anatomy, Anatomy, Anatomy…
AL PM
MFL
AL
PM
AL PM
PCL Target Insertions
70° scope, posterior view
AL
PM
10/7/2013 10:48 AM
3
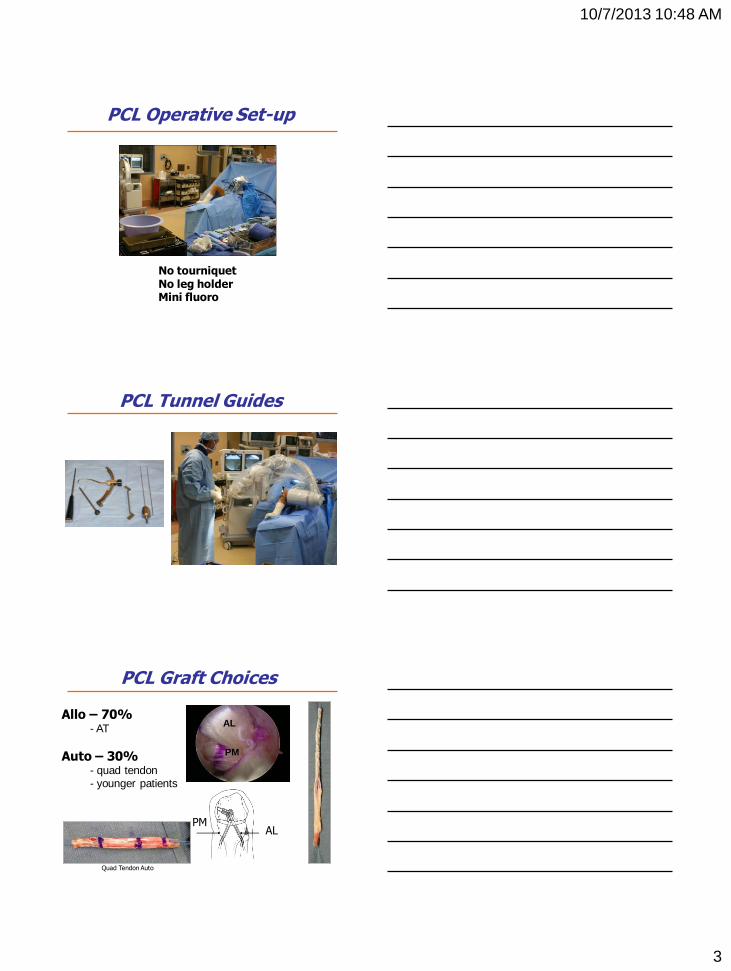
PCL Operative Set-up
No tourniquet No leg holder Mini fluoro
PCL Tunnel Guides
PCL Graft Choices
Allo – 70% - AT
Auto – 30% - quad tendon - younger patients
AL PM
AL
PM
Quad Tendon Auto
10/7/2013 10:48 AM
4
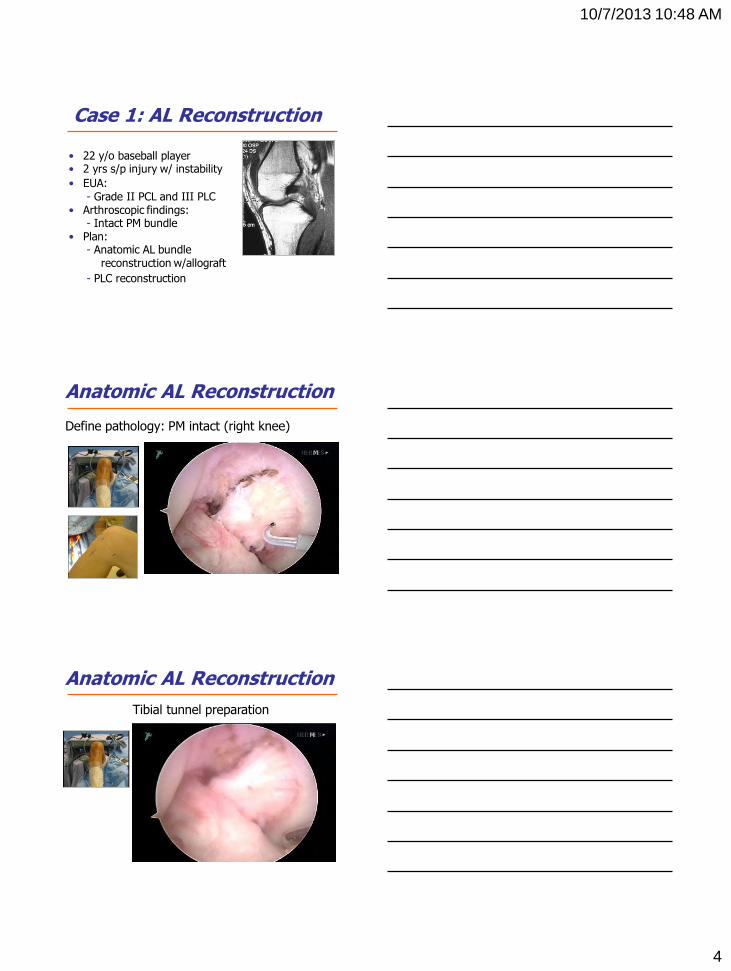
Case 1: AL Reconstruction
• 22 y/o baseball player • 2 yrs s/p injury w/ instability
• EUA: - Grade II PCL and III PLC
• Arthroscopic findings: - Intact PM bundle
• Plan: - Anatomic AL bundle reconstruction w/allograft
- PLC reconstruction
Anatomic AL Reconstruction
Define pathology: PM intact (right knee)
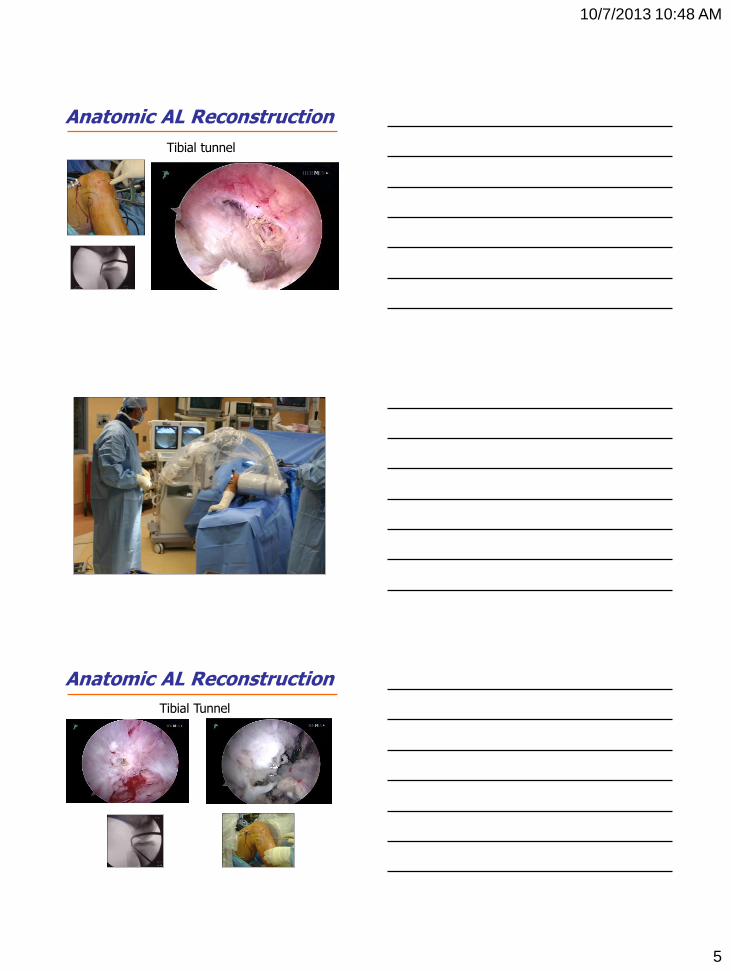
Anatomic AL Reconstruction
Tibial tunnel preparation
10/7/2013 10:48 AM
5
Anatomic AL Reconstruction
Tibial tunnel
Anatomic AL Reconstruction
Tibial Tunnel
10/7/2013 10:48 AM
6
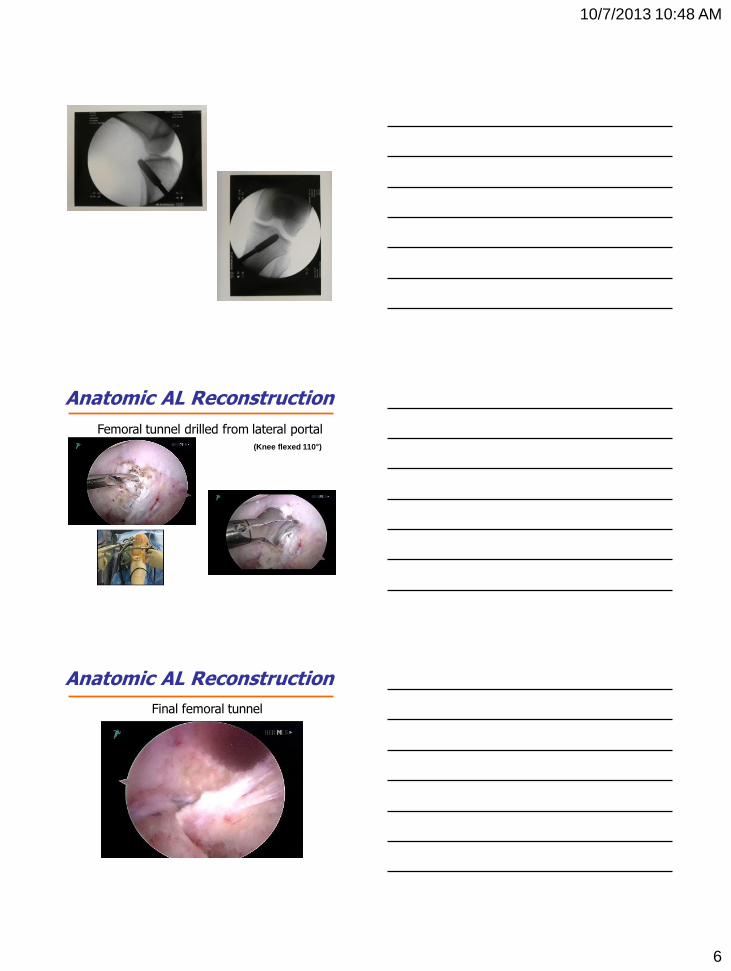
Anatomic AL Reconstruction
Femoral tunnel drilled from lateral portal
(Knee flexed 110°)
Anatomic AL Reconstruction
Final femoral tunnel
10/7/2013 10:48 AM
7
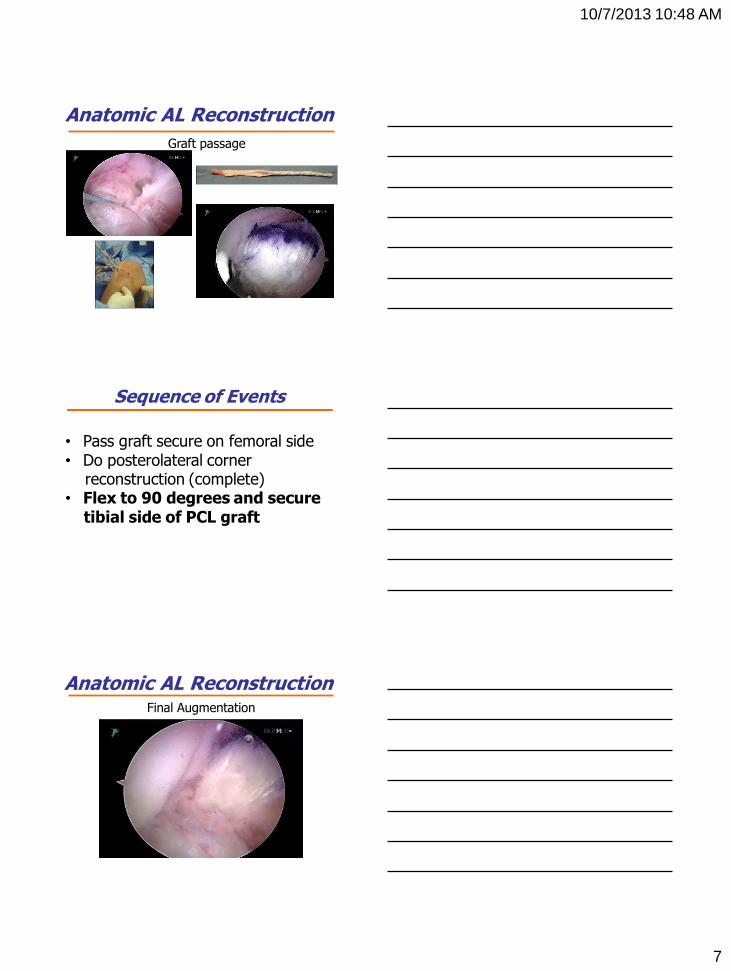
Anatomic AL Reconstruction
Graft passage
Sequence of Events
• Pass graft secure on femoral side • Do posterolateral corner reconstruction (complete) • Flex to 90 degrees and secure tibial side of PCL graft
Anatomic AL Reconstruction Final Augmentation
10/7/2013 10:48 AM
8
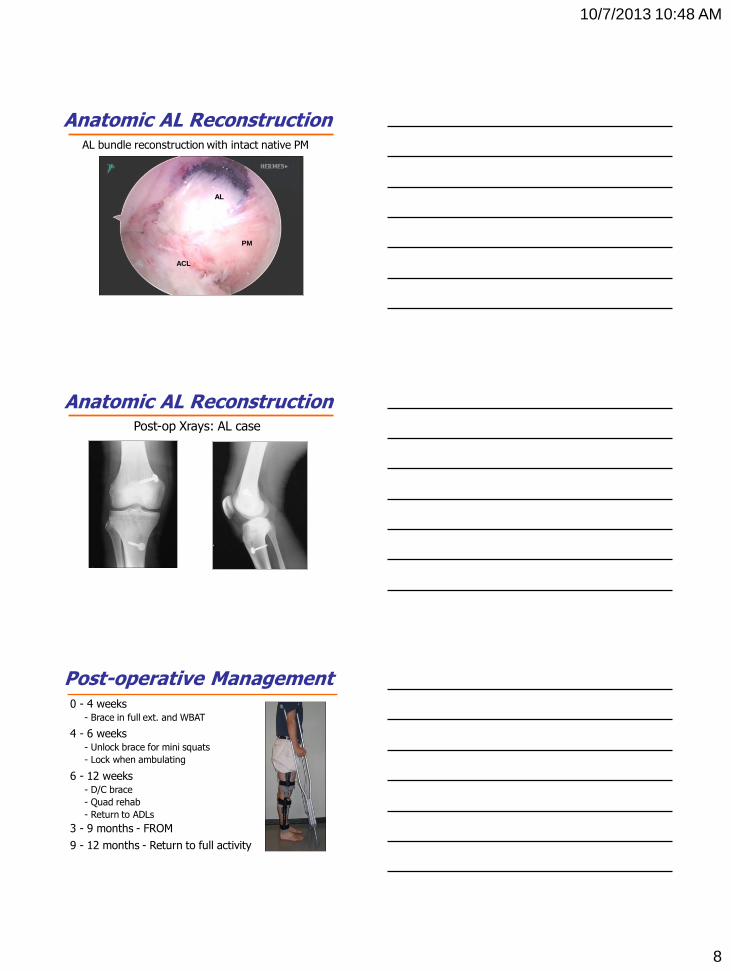
Anatomic AL Reconstruction AL bundle reconstruction with intact native PM
AL
PM
ACL
Anatomic AL Reconstruction Post-op Xrays: AL case
Post-operative Management 0 - 4 weeks
- Brace in full ext. and WBAT
4 - 6 weeks - Unlock brace for mini squats
- Lock when ambulating
6 - 12 weeks - D/C brace
- Quad rehab
- Return to ADLs
3 - 9 months - FROM
9 - 12 months - Return to full activity
10/7/2013 10:48 AM
9
Thank You
New High School Student New Driver
Case Examples – Non Op
I). 20 y/o college football player • Isolated Grade II PCL
II). 29 y/o soccer player
• 7 year follow up isolated Grade II-III PCL
PCL Injuries
III). 16 y/o female high school soccer player • Combined Grade II PCL, Grade III MCL (mid substance)
You must protect the injured PCL – it can heal!!
Case #1 Isolated PCL
Acute Grade II (III?) PCL
20 Year Old College Football Player
10/7/2013 10:48 AM
10
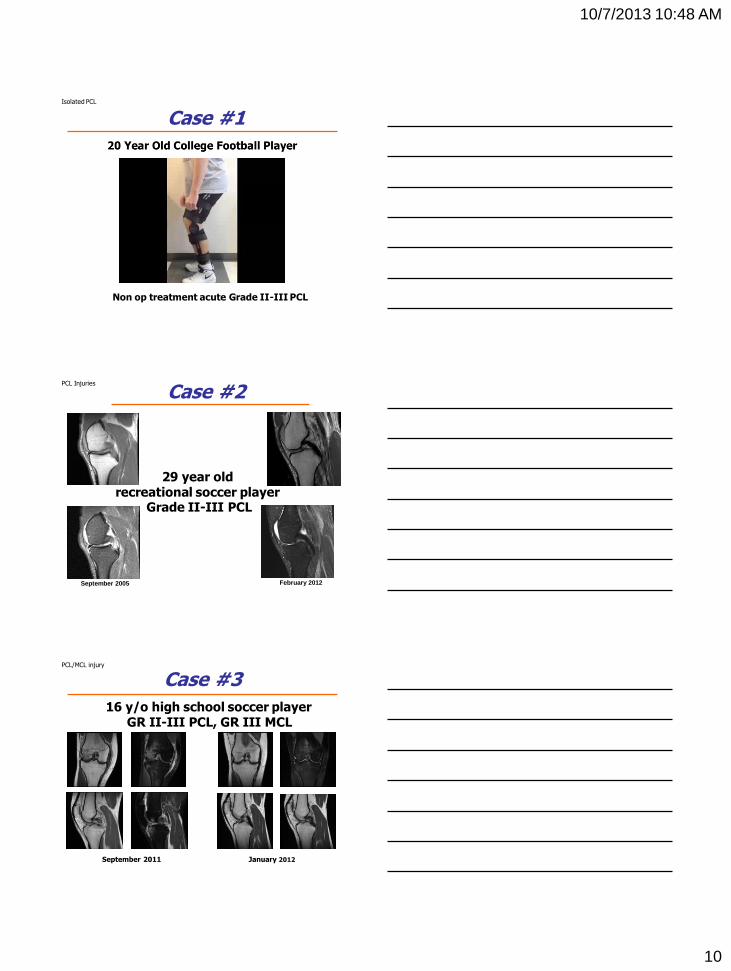
Case #1 Isolated PCL
Non op treatment acute Grade II-III PCL
Case #2 PCL Injuries
September 2005 February 2012
29 year old recreational soccer player
Grade II-III PCL
Case #3 PCL/MCL injury
September 2011 January 2012
16 y/o high school soccer player GR II-III PCL, GR III MCL

10/7/2013 10:48 AM
11
Case #3 PCL/MCL injury
Four months status post Grade II (III?) PCL/Grade III MCL





























