Embed Size (px)
DESCRIPTION
Tick Borne Illness in Virginia. Thomas M. Kerkering, M.D. Professor of Medicine & Professor Virginia Tech Program of Public Health Chief, Section of Infectious Diseases VTCSOM & Carilion Clinic. 71 year old WM presents with three day hx “heavy chest - PowerPoint PPT Presentation
Citation preview

Tick Borne Illness inVirginia
Thomas M. Kerkering, M.D.Professor of Medicine & Professor
Virginia Tech Program of Public HealthChief, Section of Infectious Diseases
VTCSOM & Carilion Clinic
Map data © OpenStreetMap (and) contributors, CC-BY-SA.
24651
24531
24523
24426
24184
24179
24175
24151
24122
24121
24115
24102
24101
24095
24090
24085
24066
24065
24055
24018
24016
2401524014
24013


8/28/20108/31/201
0Hgb 14.2 13.8WBC 8.3 8.1
Platelets 77 111Sodium 131 136
BUN 23 15Creatinin
e 1.31 0.8Total Bili 1.5 1
AST 98 56ALT 101 72
71 year old WM presents with three day hx “heavy chest sensation”, fever, chills, fatigue, dull headache & dyspnea. B/P 199/70, P =102, T = 102.3, R = 20. EKG, troponins notindicative of cardiac ischemia. Tick bites “all the time”; last one 7 days ago. Lyme screening antibody = 3.47 (normal < 0.9)
What is yourDiagnosis?

28-Aug-10 11-Oct-10Lyme Disease Ab IgG, WB: Lyme Disease Ab IgG, WB:
Negative PositiveLyme Disease 18 KD IgG: Lyme Disease 18 KD IgG:Non-Reactive Non-ReactiveLyme Disease 23 KD IgG: Lyme Disease 23 KD IgG:Non-Reactive ReactiveLyme Disease 28 KD IgG: Lyme Disease 28 KD IgG:Non-Reactive Non-ReactiveLyme Disease 30 KD IgG: Lyme Disease 30 KD IgG:Non-Reactive Non-ReactiveLyme Disease 39 KD IgG: Lyme Disease 39 KD IgG:Non-Reactive ReactiveLyme Disease 41 KD IgG: Lyme Disease 41 KD IgG:
Reactive ReactiveLyme Disease 45 KD IgG: Lyme Disease 45 KD IgG:Non-Reactive Non-ReactiveLyme Disease 58 KD IgG: Lyme Disease 58 KD IgG:Non-Reactive ReactiveLyme Disease 66 KD IgG: Lyme Disease 66 KD IgG:Non-Reactive ReactiveLyme Disease 93 KD IgG: Lyme Disease 93 KD IgG:Non-Reactive Non-ReactiveLyme Disease Ab IgM, WB Lyme Disease Ab IgM, WBPositive PositiveLyme Disease 23 KD IgM: Lyme Disease 23 KD IgM:Reactive ReactiveLyme Disease 39 KD IgM: Lyme Disease 39 KD IgM:Non-Reactive ReactiveLyme Disease 41 KD IgM: Lyme Disease 41 KD IgM:Reactive Reactive
28-Aug-2010Ehrilichia chaffeensis
IgM < 1:20(negative < 1:20)

Morulae

28-Aug-10 11-Oct-10Lyme Disease Ab IgG, WB: Lyme Disease Ab IgG, WB:
Negative PositiveLyme Disease 18 KD IgG: Lyme Disease 18 KD IgG:Non-Reactive Non-ReactiveLyme Disease 23 KD IgG: Lyme Disease 23 KD IgG:Non-Reactive ReactiveLyme Disease 28 KD IgG: Lyme Disease 28 KD IgG:Non-Reactive Non-ReactiveLyme Disease 30 KD IgG: Lyme Disease 30 KD IgG:Non-Reactive Non-ReactiveLyme Disease 39 KD IgG: Lyme Disease 39 KD IgG:Non-Reactive ReactiveLyme Disease 41 KD IgG: Lyme Disease 41 KD IgG:
Reactive ReactiveLyme Disease 45 KD IgG: Lyme Disease 45 KD IgG:Non-Reactive Non-ReactiveLyme Disease 58 KD IgG: Lyme Disease 58 KD IgG:Non-Reactive ReactiveLyme Disease 66 KD IgG: Lyme Disease 66 KD IgG:Non-Reactive ReactiveLyme Disease 93 KD IgG: Lyme Disease 93 KD IgG:Non-Reactive Non-ReactiveLyme Disease Ab IgM, WB Lyme Disease Ab IgM, WBPositive PositiveLyme Disease 23 KD IgM: Lyme Disease 23 KD IgM:Reactive ReactiveLyme Disease 39 KD IgM: Lyme Disease 39 KD IgM:Non-Reactive ReactiveLyme Disease 41 KD IgM: Lyme Disease 41 KD IgM:Reactive Reactive

10/11/2010Ehrilichia chaffeensis IgM = 1:80
(negative < 1:20)
Morulae

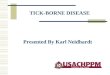
Deer tick, black legged tick, Ixodes scapularis(ehrlichiosis, Lyme disease, babesiosis)

Male & Female Black Legged Tick Deer tick, Ixodes scapularis(ehrlichiosis, Lyme disease, babesiosis)


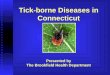
Male & Female American Dog Tick, (Dermacentor variabilis) Rocky Mountain Spotted Fever

Male & Female Lone Star Tick, (Amblyomma americanum)Ehrilichia chaffeensis, STARI



Anaplasmosis is caused by the bacterium Anaplasma phagocytophilum. This organism used to be known by other names, including Ehrlichia equi and Ehrlichia phagocytophilum, and the disease caused by this organism has been previously described as human granulocytic ehrlichiosis (HGE).

The areas from which cases are reported correspond with the known geographic distribution of the lonestar tick (Amblyomma americanum), which is associated with transmission of both E. chaffeensis and E. ewingii.


RMSF
The primary tick that transmits R. rickettsii in these states is the American dog tick (Dermacentor variabilis Dermacentor andersoni).

RMSF


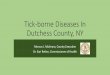
Percent of RMSF Cases Reported by Month

Tick Borne Diseases in Virginia Babesiosis Ehrlichiosis Lyme Disease Rocky Mountain Spotted Fever STARI Tick Paralysis Tularemia

Cases of Ehrlichiosis / AnaplasmosisBy Year in Virginia
Significance of Trend p = 0.0001
Source: VDH

Cases of Spotted FeverBy Year
In Virginia
Significance of Trend p = 0.01
Source: VDH

Source: VDH
Significance of Trend p = 0.0002
Cases of Lyme DiseaseBy Year in Virginia

Significance of Trend p = 0.5
Source: VDH
Cases of TularemiaBy Year in Virginia

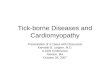
Ehrlichiosis/Anaplasmosis
Lyme Spotted Fever Tularemia0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
447
6,376
1,046
16
Total cases of each disease for the 10 years2002-2011

Map data © OpenStreetMap (and) contributors, CC-BY-SA.
24651
24531
24523
24426
24184
24179
24175
24151
24122
24121
24115
24102
24101
24095
24090
24085
24066
24065
24055
24018
24016
2401524014
24013

0
1
2
3
4
5
6
7
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005
2006
2007
2008
2009
2010
Rickettsial Infections at CRMH 2005-2010

01
23
1
13
15
4 4
0 0 00
2
4
6
8
10
12
14
16
Jan
Feb Mar AprMay Ju
n Jul
Aug Sep Oct NovDec
Total Rickettsial Infections at CRMH by Month 2005-2010

Babesiosis
B. microti on peripheral smear


• incubation period of 1 to 4 weeks
• the disease can last several weeks.
• more severe in patients who are immunosuppresed, splenectomized, and/or elderly
• infections caused by B. divergens tend to be more severe (frequently fatal if not appropriately treated) than those due to B. microti, where clinical recovery usually occurs.
Babesiosis

• Most infections are probably asymptomatic
• Manifestations of disease include - Fever- Chills- Sweating- Myalgias- Fatigue- Hepatosplenomegaly- Hemolytic anemia
Clinical Features of Babesiosis

Diagnosis of Babesia infection Made by detection of parasites in patients' blood
smears. Antibody detection tests are useful for:
- detecting infected individuals with very low levels of parasitemia (such as asymptomatic blood donors in transfusion-associated cases),
- for diagnosis after infection is cleared by therapy, and for discrimination between Plasmodium falciparum and Babesia infection in patients whose blood smear examinations are inconclusive and whose travel histories cannot exclude either parasite.
The indirect fluorescent antibody test (IFA) 88-96% of patients with B. microti infection. Patients' titers generally rise to >1:1024 during the first weeks of illness and decline gradually over 6 months to titers of 1:16 to 1:256 but may remain detectable at low levels for a year or more.

PCR Testing for the presence of B. microti DNA is available.

Treatment of Babesiosis

Ehrlichia chaffeensis primarily infects mononuclear leukocytes (predominantly monocytes and macrophages),
The pathogen that causes human granulocytic ehrlichiosis (HGE) (Anaplasmosis) primarily infects granulocytes (neutrophils and rarely eosinophils).

Ehrlichia ewingii primarily infects neutrophils and occasionally eosinophils and produces a disease clinically similar to HME and HGE. Most patients with this form of ehrlichiosis have also had other medical conditions causing immunosuppression (e.g., HIV infection, splenectomy, transplantation,

Lone star tick (Amblyomma americanum)
Ehrlichia chaffeensis is principally transmitted by the lone star tick (Amblyomma americanum) White-tailed deer are a major host of lone star ticks and appear to represent one natural reservoir for E. chaffeensis.

Blacklegged tick(Ixodes scapularis)
The HGE agent (Anaplasmosis) has been associated with the blacklegged tick (Ixodes scapularis). Deer, elk, and wild rodents are likely reservoirs.

• Initial symptoms generally include - fever- headache- malaise- myalgias
Ehrlichiosis
• incubation period of about 5-10 days after the tick bite
• Patients with ehrlichiosis generally visit a physician in their first week of illness

• Other signs and symptoms may include - nausea- vomiting- diarrhea- cough- joint pains- confusion- occasionally rash.
In contrast to Rocky Mountain spotted fever, rash is relatively uncommon in adult patients with HME, and is rarely reported with HGE. However, rash has been described in approximately 60% of pediatric patients infected with E. chaffeensis.
Ehrlichiosis

Laboratory findings indicative of ehrlichiosis include - leukopenia- thrombocytopenia- elevated liver enzymes
If a lumbar puncture is performed the CSF is abnormal- a few to 100-200 WBC (predominately lymphs)- a few RBCs- normal glucose- normal to slightly elevated protein
Ehrlichiosis

Ehrlichiosis can be a severe illness, especially if untreated, and as many as half of all patients require hospitalization. Severe manifestations of the disease may include:
- prolonged fever- renal failure- disseminated intravascular coagulopathy
- meningoencephalitis- adult respiratory distress syndrome -- seizures, or coma
It is estimated that 2%-3% of patients may die from the infection. Preliminary evidence suggests that E. chaffeensis infection may become more severe than other Ehrlichia infections.
Ehrlichiosis

The severity of ehrlichiosis may be related in part to the immune status of the patient. Persons with compromised immunity caused by immunosuppressive therapies e.g.,
- corticosteroids- cancer chemotherapy- HIV infection- splenectomy
appear to develop more severe disease, and case-fatality ratios for these individuals are characteristically higher than case-fatality ratios reported for the general population.
Ehrlichiosis

The organisms can be demonstrated in blood smears by staining with Diff-Quik or Giemsa stains
Ehrlichiosis

Although IFA remains the principal diagnostic tool for the detection of ehrlichial infection, there is no standardized antigen, conjugate, or agreement on what constitutes a positive result among the various laboratories providing these tests
Most patients demonstrate increased IgM or IgG titers by the second week of the illness. However, patients may lack diagnostic IgG antibody titers in the first 7 days of illness. This is an important consideration, because patients seek health care at a median of 3 days after onset of the illness.
Ehrlichiosis

PCR is the next most frequently used method for detecting infection. This test is available through CDC and some state health laboratories, as well as a number of research and commercial laboratories. PCR tests remain unstandardized, and analytical and diagnostic sensitivity and specificity may vary among individual assays.
Direct isolation of the organism remains the gold standard for confirmatory diagnosis, but is the most difficult and time-consuming approach. Both E. chaffeensis and the HGE agent have been recovered from the blood of acutely ill patients by using a variety of cell lines.
Ehrlichiosis

Doxycycline
100 mg twice daily for adults 4.4 mg/kg body weight per day in two divided doses for children under 45.4 kgs (100 lbs)
treat for at least 3 days after the fever subsides and until evidence of clinical improvement, for a minimum total course of 5 to 7 days
severe or complicated disease may require longer treatment courses.
rifampin has been used successfully in a limited number of pregnant women with documented HGE.
Ehrlichiosis


R. rickettsii in cell culture

American dog tick (Dermacentor variabilis)
Dogs and medium-sized mammals are the preferred hosts of adult D. variabilis, although it feeds readily on other large mammals, including humans. This tick is the most commonly identified species responsible for transmitting R. rickettsii to humans.

The frequency of reported cases of Rocky Mountain spotted fever is highest among males, Caucasians, and children. Two-thirds of the Rocky Mountain spotted fever cases occur in children under the age of 15 years, with the peak age being 5 to 9 years old Individuals with frequent exposure to dogs and who reside near wooded areas or areas with high grass may also be at increased risk of infection.


Initial symptoms may include:
fever nausea vomiting severe headache muscle pain lack of appetite
Later signs and symptoms include:
rash abdominal pain joint pain diarrhea
Rocky Mountain Spotted Fever

rash appears 2-5 days after the onset of fever
often not present or very subtle when the patient is initially seen
younger patients usually develop the rash earlier than older patients
most often it begins as small, flat, pink, non-itchy spots (macules)
on the wrists, forearms, and ankles
macules turn pale when pressure is applied and eventually become raised on the skin
Rocky Mountain Spotted Fever

the characteristic red, spotted (petechial) rash of Rocky
Mountain spotted fever is usually not seen until the sixth day or later after onset of symptoms, and this type of rash occurs in only 35% to 60% of patients with Rocky Mountain spotted fever
the rash involves the palms or soles in as many as 50% to 80% of patients; however, this distribution may not occur until later in the course of the disease
as many as 10% to 15% of patients may never develop a rash.
Rocky Mountain Spotted Fever





Abnormal laboratory findings seen in patients with Rocky Mountain spotted fever may include:
- thrombocytopenia- hyponatremia- elevated liver enzyme levels - abnormal CSF
Rocky Mountain Spotted Fever

severe manifestations of this disease may involve:
- respiratory system- central nervous system- gastrointestinal system- renal system.
Rocky Mountain Spotted Fever
Due to infection of the endothelial cells and resulting vasculitis

Host factors associated with severe or fatal Rocky Mountain spotted fever include:
- advanced age- male sex- African-American race- chronic alcohol abuse- glucose-6-phosphate dehydrogenase (G6PD)
deficiency.
Deficiency of G6PD is a sex-linked genetic condition affecting approximately12% of the U.S. African-American male population; deficiency of this enzymeis associated with a high proportion of severe cases of Rocky Mountainspotted fever. This is a rare clinical course that is often fatal within 5 days of onset of illness.
Rocky Mountain Spotted Fever

Long-term health problems following acute Rocky Mountain spotted fever infection include:
- partial paralysis of the lower extremities - gangrene requiring amputation of fingers, toes, or arms or legs- hearing loss- loss of bowel or bladder control- movement disorders- language disorders
These complications are most frequent in persons recovering from severe, life-threatening disease, often following lengthy hospitalizations.
Rocky Mountain Spotted Fever

Laboratory Detection
There is no widely available laboratory assay that provides rapid confirmation of early Rocky Mountain spotted fever.
Therefore, treatment decisions should be based on epidemiologic and clinical clues, and should never be delayed while waiting for confirmation by laboratory results.
Fundamental understanding of the signs, symptoms, and epidemiology of the disease is crucial in guiding requests for tests for Rocky Mountain spotted fever and interpretation of results.
Rocky Mountain Spotted Fever

The indirect immunofluorescence assay (IFA) is generally considered the reference standard in Rocky Mountain spotted fever serology.
Blood samples taken early (acute) and late convalescent) in the disease are the preferred specimens for evaluation.
Most patients demonstrate increased IgM titers by the end of the first week of illness. Diagnostic levels of IgG antibody generally do not appear until 7-10 days after the onset of illness.
Rocky Mountain Spotted Fever

It is important to consider the amount of time it takes for antibodies to appear when ordering laboratory tests, especially because most patients visit their physician relatively early in the course of the illness, before diagnostic antibody levels may be present.
The value of testing two sequential serum or plasma samples together to show a rising antibody level is considerably more important in confirming acute infection with rickettsial agents because antibody titers may persist in some patients for years after the original exposure.
Rocky Mountain Spotted Fever

Immunostaining is used by taking a skin biopsy of the rash from an infected patient prior to therapy or within the first 48 hours after antibiotic therapy has been started.
Because rickettsiae are focally distributed in lesions of Rocky Mountain spotted fever, this test may not always detect the agent. The sensitivity is only about 70% on biopsied tissues.
This assay may also be used to test tissues obtained at autopsy and has been used to confirm Rocky Mountain spotted fever in otherwise unexplained deaths

Chloramphenicol is an alternative drug that can be used to treat Rocky Mountain spotted fever;
Doxycycline
100 mg twice daily for adults 4.4 mg/kg body weight per day in two divided doses for children under 45.4 kgs (100 lbs)
treat for at least 3 days after the fever subsides and until evidence of clinical improvement, for a minimum total course of 5 to 10 days
Rocky Mountain Spotted Fever

Southern Tick-Associated Rash Illness

In 2001, a patient with evidence of B. lonestari infection was reported in the medial literature. This patient had exposure to ticks in Maryland and North Carolina and developed a rash indistinguishable from erythema migrans after an A. americanum tick bite. DNA analysis indicated the presence of B. lonestari in a skin biopsy taken at the leading edge of the rash and in the tick removed by the physician. Serologic testing for Lyme disease was negative. The patient was treated with an oral antibiotic and returned to normal health.
Southern Tick-Associated Rash Illness

A rash similar to the rash of Lyme disease has been described in humans residing in southeastern and south-central states and is associated with the bite of the lone star tick, Amblyomma americanum. This Lyme disease-like rash has been named Southern tick-associated rash illness (STARI).

Research indicates that live spirochetes are observed in only 1-3% of A. americanum.
Even though spirochetes have been seen in A. americanum ticks by microscopy, attempts to culture it in the laboratory have consistently failed. Modified BSK (Barbour-Stoenner-Kelly) is the best medium for cultivating the Lyme disease spirochete, B. burgdorferi, but is apparently not suitable for cultivating the spirochete found in A. americanum. However, a spirochete has been detected in A. americanum by DNA analysis and was given the name Borrelia lonestari.
Southern Tick-Associated Rash Illness

Reported cases of tularemia, United States, 2001-2010

Tularemia is a disease of animals and humans caused by the bacterium Francisella tularensis. Rabbits, hares, and rodents are especially susceptible and often die in large numbers during outbreaks. Humans can become infected through several routes, including:
Tick and deer fly bitesSkin contact with infected animalsIngestion of contaminated waterLaboratory exposureInhalation of contaminated dusts or aerosols

Steps to prevent tularemia include:
Use of insect repellent
Wearing gloves when handling sick or dead animals
Avoiding mowing over dead animals
In the United States, naturally occurring infections have been reported from all states except Hawaii.

Ulceroglandular This is the most common form of tularemia and usually occurs following a tick or deer fly bite or after handing of an infected animal. A skin ulcer appears at the site where the organism entered the body. The ulcer is accompanied by swelling of regional lymph glands, usually in the armpit or groin.
Glandular Similar to ulceroglandular tularemia but without an ulcer. Also generally acquired through the bite of an infected tick or deer fly or from handling sick or dead animals.
Oculoglandular This form occurs when the bacteria enter through the eye. This can occur when a person is butchering an infected animal and touches his or her eyes. Symptoms include irritation and inflammation of eye and swelling of lymph glands in front of the ear.

Oropharyngeal This form results from eating or drinking contaminated food or water. Patients with orophyangeal tularemia may have sore throat, mouth ulcers, tonsillitis, and swelling of lymph glands in the neck.
Pneumonic This is the most serious form of tularemia. Symptoms include cough, chest pain, and difficulty breathing. This form results from breathing dusts or aerosols containing the organism. It can also occur when other forms of tularemia (e.g. ulceroglandular) are left untreated and the bacteria spread through the bloodstream to the lungs.


1. Avoiding ticks - whenever possible, stay out of weedy areas. Use paths in wooded areas. Wear light-colored clothing. If you are wearing long pants, tuck them into your socks Spray repellents on your socks and pants legs. Never use repellents on skin covered by clothing.
2. Routine inspection - inspection of yourself and other family members, particularly if anyone has spent significant time outdoors in areas where ticks are likely to be found.
The recommended approach to preventing tick-borne illness is quite simple.

3. Prompt removal of ticks - use tweezers to gently pull the tick loose. Do not apply vaseline, kerosene, nail polish or other similar products.
4. Monitoring - if you find a tick on yourself or someone else, circle the date on the calendar and watch for the symptoms of tick-borne illness (i.e., flu-like symptoms) which typically develop within 10 to 14 days. If these symptoms develop, contact your physician immediately. Do not rely solely on watching for the expected physical signs of the rash (Rocky Mountain Spotted Fever) or the Bull's eye for Lyme disease.
The recommended approach to preventing tick-borne illness is quite simple.