Embed Size (px)
Citation preview

SINCOPE 2 0 1 5
www.gimsi.it
Tilt asistolico VASIS 2B Pro
Francesco Arabia U.O. Cardiologia – UTIC
Emodinamica e Cardiologia Interventistica Presidio Ospedaliero “A. Pugliese” Catanzaro
SINCOPE 2 0 1 5
www.gimsi.it
SINCOPE 2 0 1 5
www.gimsi.it
SINCOPE 2 0 1 5
www.gimsi.it
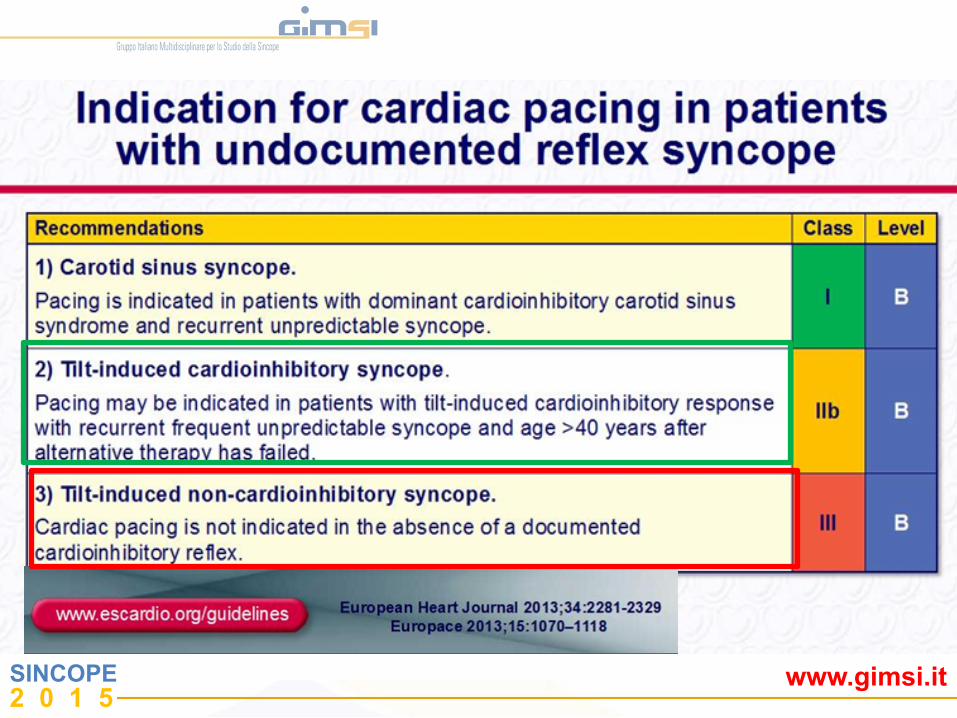
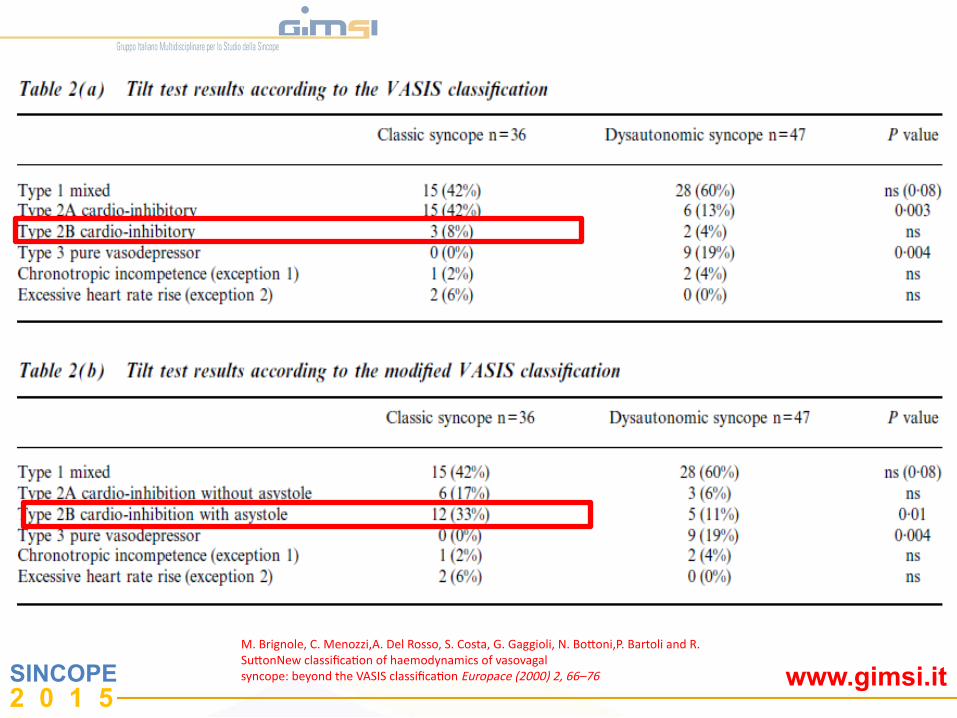
Tipo 2 A , cardioinibitoria senza asistolia:'la frequenza cardiaca scende a meno di 40 bpm per più di 10 s, ma non si verifica asistolia maggiore di 3 secondi. La pressione cala prima della diminuzione della frequenza cardiaca. Tipo 2 B , cardioinibitoria con asistolia: Si verifica asistolia maggiore di 3 secondi. Il calo pressorio coincide con la diminuzione della frequenza cardiaca o la precede
Tipo 2A : 'la frequenza cardiaca scende a meno di 40 bpm per più di 10 s o si verifica asistolia per più di 3 s; la pressione arteriosa scende prima della frequenza cardiaca Tpo 2B: la frequenza cardiaca scende a meno di 40 bpm per più di 10 s o si verifica asistolia per più di 3 s; la caduta della pressione arteriosa coincide con la caduta della frequenza cardiaca
Vasis 1992 Vasis 2000
SuJon R, Petersen M, Brignole M, Raviele A, Menozzi C, Giani P. Proposed classificaPon for Plt induced vasovagal syncope. Eur J Cardiac Pacing Electrophysiol 1992; 2: 180–3.
M. Brignole, C. Menozzi,A. Del Rosso, S. Costa, G. Gaggioli, N. BoJoni,P. Bartoli and R. SuJonNew classificaPon of haemodynamics of vasovagal syncope: beyond the VASIS classificaPon Europace (2000) 2, 66–76
SINCOPE 2 0 1 5
www.gimsi.it M. Brignole, C. Menozzi,A. Del Rosso, S. Costa, G. Gaggioli, N. BoJoni,P. Bartoli and R. SuJonNew classificaPon of haemodynamics of vasovagal syncope: beyond the VASIS classificaPon Europace (2000) 2, 66–76
SINCOPE 2 0 1 5
www.gimsi.it
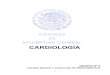
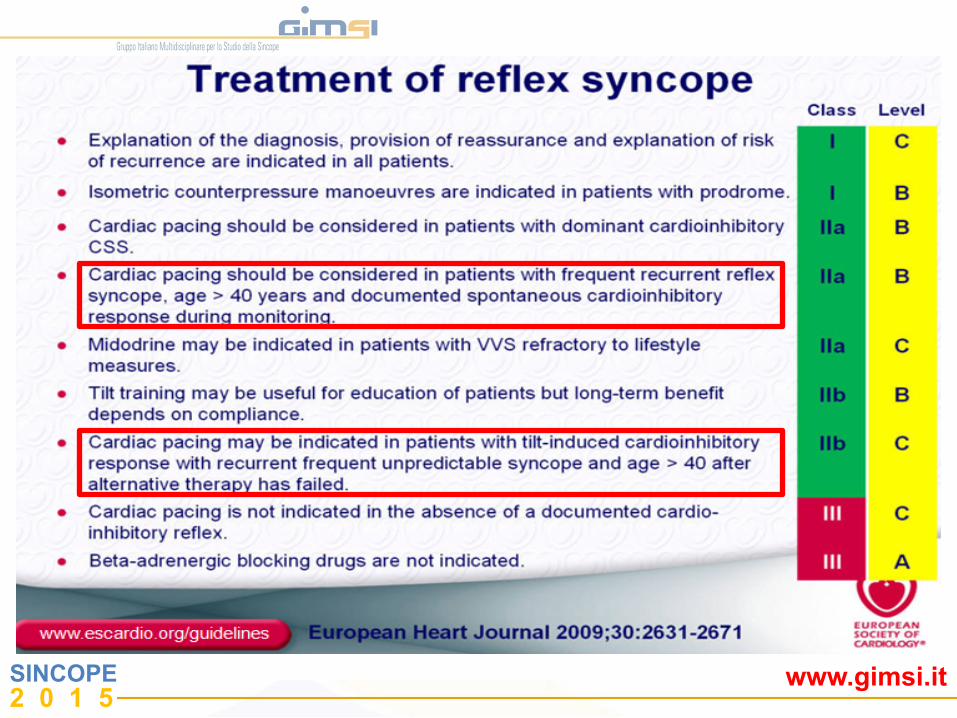
The Role of Pacing as Therapy for VVS VVS with +HUT and cardioinhibitory response: Class IIb indication for pacing Three randomized, prospective trials reported benefits of pacing in select VVS patients:
– VPS I
– VASIS
– SYDIT Subsequent study results less clear:
– VPS II
– Synpace
1Connolly SJ. J Am Coll Cardiol. 1999;33:16-20. 2Sutton R. Circulation. 2000;102:294-299. 3Ammirati F. Circ. 2001;104:52-57.
4Connolly 5Giada 6Occhetta E, et al. Europace. 2004;6:538-547.
Double blind
Open label
SINCOPE 2 0 1 5
www.gimsi.it
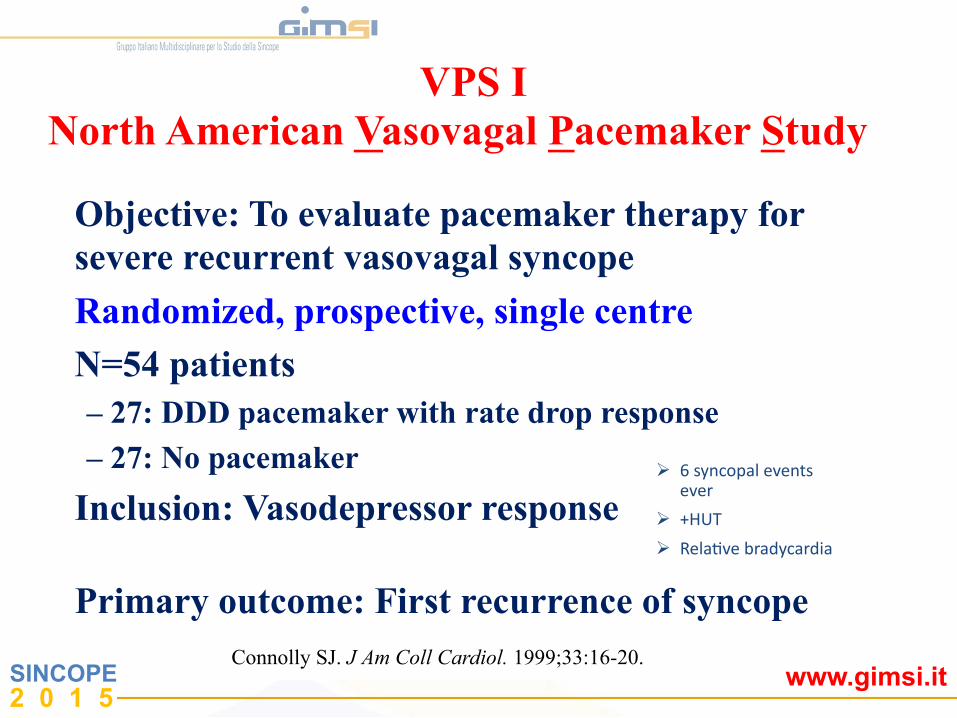
VPS I North American Vasovagal Pacemaker Study
Objective: To evaluate pacemaker therapy for severe recurrent vasovagal syncope
Randomized, prospective, single centre
N=54 patients – 27: DDD pacemaker with rate drop response
– 27: No pacemaker
Inclusion: Vasodepressor response
Primary outcome: First recurrence of syncope Connolly SJ. J Am Coll Cardiol. 1999;33:16-20.
! 6 syncopal events ever
! +HUT ! RelaPve bradycardia
SINCOPE 2 0 1 5
www.gimsi.it
Cum
ulat
ive
Ris
k (%
)
100 90 80 70 60 50 40 30 20 10 0
0 3 12 15 6 9 Time in Months
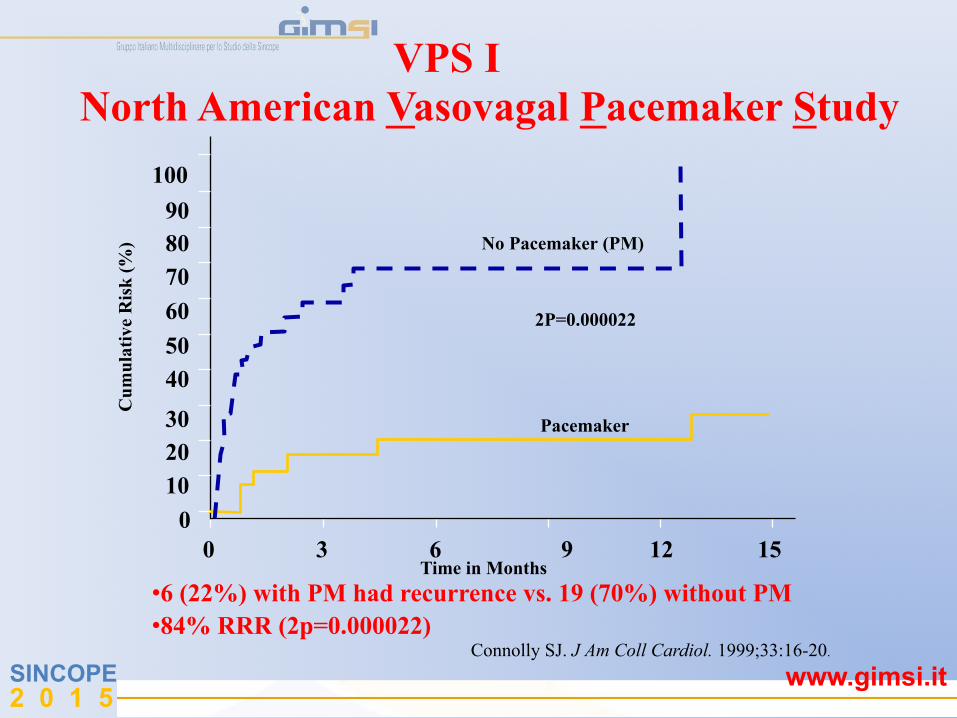
Connolly SJ. J Am Coll Cardiol. 1999;33:16-20.
• 6 (22%) with PM had recurrence vs. 19 (70%) without PM • 84% RRR (2p=0.000022)
VPS I North American Vasovagal Pacemaker Study
No Pacemaker (PM)
2P=0.000022
Pacemaker
SINCOPE 2 0 1 5
www.gimsi.it
VASIS Vasovagal Syncope International Study
Objective: To evaluate pacemaker therapy for severe cardioinhibitory tilt-positive neurally mediated syncope Randomized, prospective, multi-centre N=42 patients – 19: DDI pacemaker (80 bpm) with rate hysteresis (45 bpm) – 23: No pacemaker Inclusion: Positive cardioinhibitory response Primary outcome: First recurrence of syncopeope
Sutton R. Circulation. 2000;102:294-299.
! > 3 syncopal events in 2 years and last event occurring within 6 months of enrollment and,
! PosiPve VASIS type 2A or 2B cardioinhibitory response to HUT and, ! Age > 40 years or drug refractory if < 40 years
SINCOPE 2 0 1 5
www.gimsi.it
% S
ynco
pe-F
ree
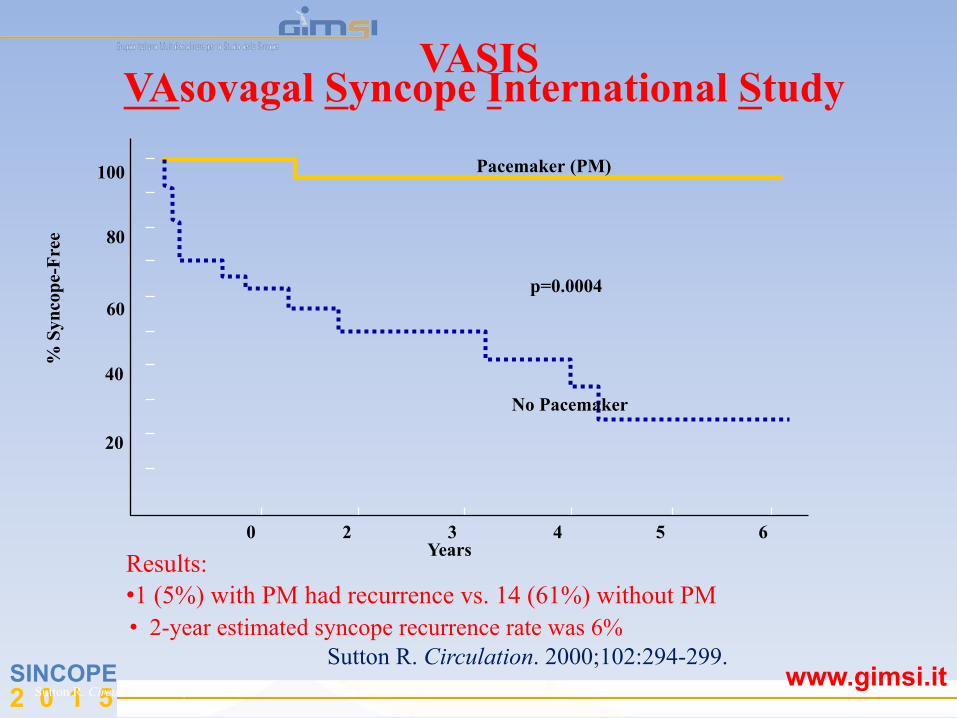
Sutton R. Circulation. 2000;102:294-299.
100 80 60 40 20
0 2 3 4 5 6 Years Results:
• 1 (5%) with PM had recurrence vs. 14 (61%) without PM
VASIS VAsovagal Syncope International Study
Pacemaker (PM)
p=0.0004
No Pacemaker
Sutton R. Circulation. 2000;102:294-299. • 2-year estimated syncope recurrence rate was 6%

SINCOPE 2 0 1 5
www.gimsi.it
SYDIT Syncope Diagnosis and Treatment
Objective: To compare the effects of cardiac pacing with pharmacological therapy in patients with recurrent vasovagal syncope Randomized, prospective, multi-centre N=93 patients – 46: DDD pacemaker with rate drop response – 47: Atenolol 100 mg/die Inclusion: Positive HUT with relative bradycardia Primary outcome: First recurrence of syncopee Ammirati F. Circulation. 2001;104:52-57.
> 55 yrs > 3 syncopal episodes in 2 years

SINCOPE 2 0 1 5
www.gimsi.it
% S
ynco
pe-F
ree
Ammirati F. Circulation. 2001;104:52-57.
1.0 0.9 0.8 0.7 0.6
0 100 200 300 400 500 600 700 800 900 1000
SYDIT Syncope Diagnosis and Treatment
Pacemaker (PM)
p=0.0032
Drug
Time (Days) • 2 (4%) with PM had syncope recurrence vs. 12 (26%) without PM • 2-year estimated syncope recurrence rate was 7,2%
SINCOPE 2 0 1 5
www.gimsi.it
VPS II Vasovagal Pacemaker Study II
Objective: To determine if pacing therapy reduces the risk of syncope in patients with vasovagal syncope Randomized, double-blind, prospective, multi-centre N=100 patients – 52: Only sensing without pacing – 48: DDD pacemaker with rate drop response Inclusion: Positive HUT with (HRxBP) < 6000/min x mmHg
! 6 syncope events ever or ! > 3 syncope events in 2 years or ! > 1 syncope event in 6 months
Primary outcome: First recurrence of syncope
Connolly S. JAMA. 2003;289:2224-2229.
SINCOPE 2 0 1 5
www.gimsi.it
Cum
ulat
ive
Ris
k
1.0 0.8 0.6 0.4 0.2 0
Months Since Randomization 6543 210
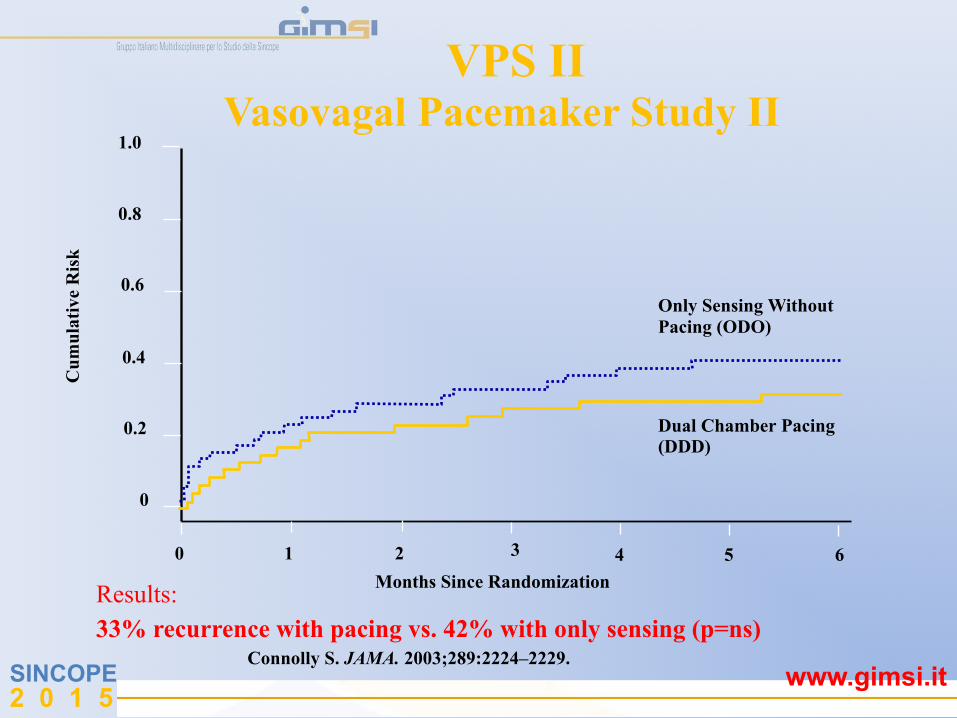
Connolly S. JAMA. 2003;289:2224–2229.
Results: 33% recurrence with pacing vs. 42% with only sensing (p=ns)
VPS II Vasovagal Pacemaker Study II
Only Sensing Without Pacing (ODO)
Dual Chamber Pacing (DDD)
SINCOPE 2 0 1 5
www.gimsi.it
SYNPACE Vasovagal Syncope and Pacing
Objective: To determine if pacing therapy will reduce syncope relapses in patients with recurrent vasovagal syncope, compared with those having a pacemaker programmed OFF Randomized, double-blind, prospective, multi-centre, placebo-controlled N=29 patients – 16: DDD PM with rate drop response programmed ON – 13: PM programmed OFF (OOO mode) Inclusion: Recurrent VVS and +HUT with asystolic or mixed response Primary outcome: First recurrence of syncope
Raviele A.. Europace. 2001;3:336–341. Raviele A, et al. Eur Heart J. 2004;25:1741-1748.
SINCOPE 2 0 1 5
www.gimsi.it
% S
ynco
pe-F
ree
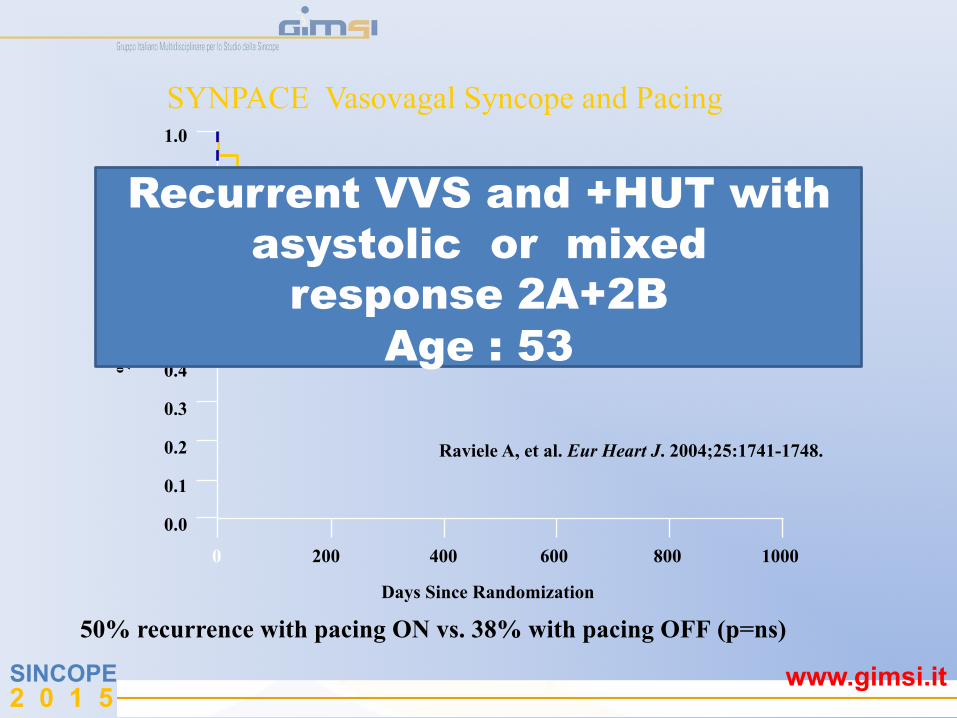
Raviele A, et al. Eur Heart J. 2004;25:1741-1748.
SYNPACE Vasovagal Syncope and Pacing 1.0
0 200 400 600 800 1000
0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0
p=0.58 Pacemaker OFF Pacemaker ON
Days Since Randomization 50% recurrence with pacing ON vs. 38% with pacing OFF (p=ns)
Recurrent VVS and +HUT with asystolic or mixed
response 2A+2B Age : 53
SINCOPE 2 0 1 5
www.gimsi.it
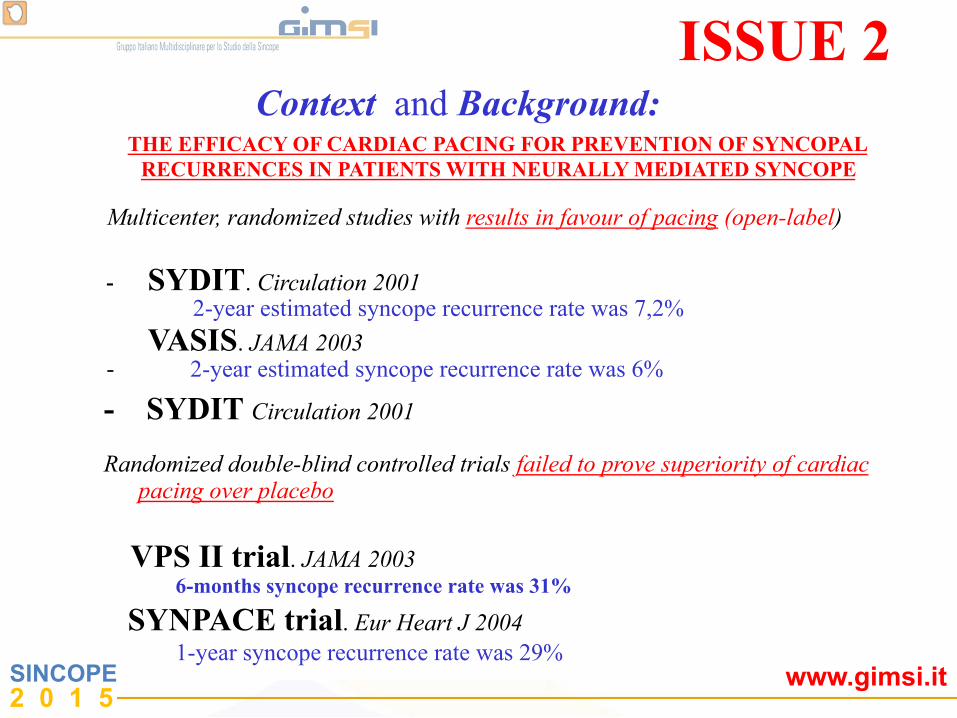
Context and Background: THE EFFICACY OF CARDIAC PACING FOR PREVENTION OF SYNCOPAL RECURRENCES IN PATIENTS WITH NEURALLY MEDIATED SYNCOPE
Multicenter, randomized studies with results in favour of pacing (open-label)
- -
SYDIT. Circulation 2001 2-year estimated syncope recurrence rate was 7,2%
VASIS. JAMA 2003 2-year estimated syncope recurrence rate was 6%
- SYDIT Circulation 2001 Randomized double-blind controlled trials failed to prove superiority of cardiac
pacing over placebo
VPS II trial. JAMA 2003 6-months syncope recurrence rate was 31%
SYNPACE trial. Eur Heart J 2004 1-year syncope recurrence rate was 29%
ISSUE 2
SINCOPE 2 0 1 5
www.gimsi.it
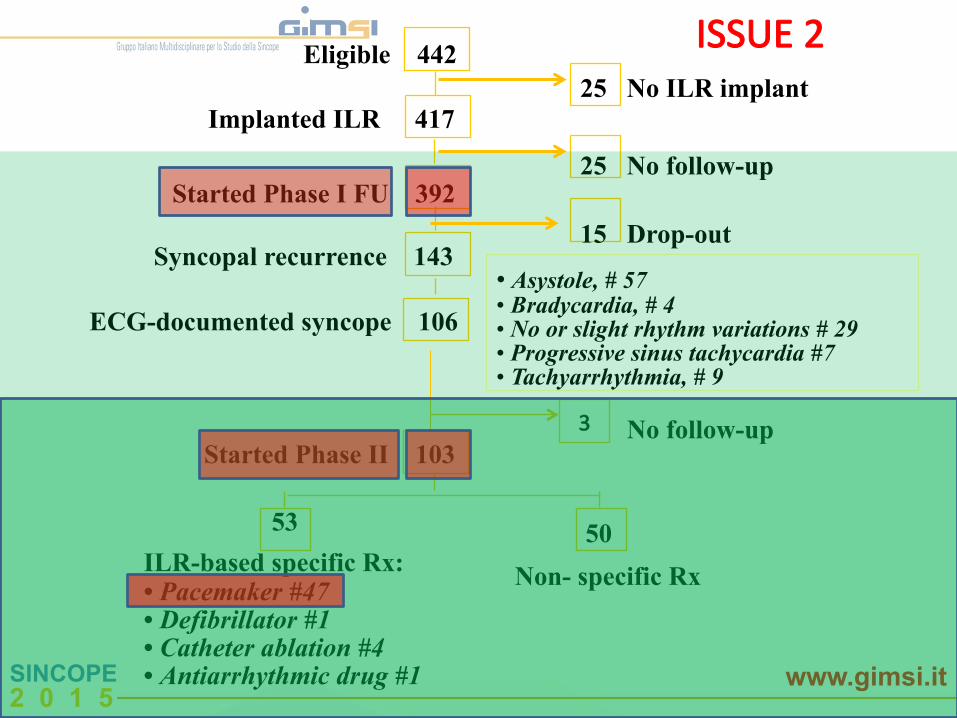
3
Implanted ILR
Eligible 442 25 No ILR implant
53 ILR-based specific Rx: • Pacemaker #47 • Defibrillator #1 • Catheter ablation #4 • Antiarrhythmic drug #1
50 Non- specific Rx
417
25 No follow-up
15 Drop-out • Asystole, # 57 • Bradycardia, # 4 • No or slight rhythm variations # 29 • Progressive sinus tachycardia #7 • Tachyarrhythmia, # 9
No follow-up Started Phase II 103
Started Phase I FU 392
Syncopal recurrence 143
ECG-documented syncope 106
ISSUE 2

SINCOPE 2 0 1 5
www.gimsi.it
ISSUE 2
1-year estimated syncope recurrence rate was 5% ( burden 0,05 ±0,15)
" Pacing potentially effective in patients with documented asystole " The mechanism of spontaneus NMS documentated by ILR was riproducible " Asystolic NMS treated with pacemaker showed a > 80% relative risk reduction of syncopal recurrence Studio mulPcentrico prospebco osservazionale
ISSUE-2 was not a formal controlled double-blind trial
Eur Heart J 2006; 27, 1085–1092
SINCOPE 2 0 1 5
www.gimsi.it
Europace. 2007 Jan;9(1):31-‐3. Pacing for neurally mediated syncope: is placebo powerless? Brignole M, SuJon R.
CONCLUSIONS:
Placebo is not an effecPve therapy for neurally mediated syncope. Different selecPon criteria in paPents who are candidates for cardiac pacing-‐for example, presence, absence, or severity of the cardioinhibitory reflex may separate posiPve from negaPve trials.
SINCOPE 2 0 1 5
www.gimsi.it
ISSUE 3"
SYNCOPE"
ISSUE 3 International Study on Syncope of Uncertain Etiology 3
Pacemaker therapy for paPents with
neurally-‐mediated syncope and documented asystole
A randomized controlled double-‐blind trial
Objective: to determine if pacing therapy reduces recurrences in patients with severe documented spontaneous asystolic NMS
SINCOPE 2 0 1 5
www.gimsi.it
ISSUE 3 International Study on Syncope of Uncertain Etiology 3
ISSUE 3"
SYNCOPE"
Total 29 centers
SINCOPE 2 0 1 5
www.gimsi.it
ISSUE 3 International Study on Syncope of Uncertain Etiology 3
Study hypothesis:
Pacing therapy is effecPve for prevenPng syncope recurrence in paPents with NMS and documented asystole
Background:
Two RCTs* failed to prove superiority of cardiac pacing over placebo of unselected NMS paPents with posiPve Plt tesPng
* VPS II trial. JAMA 2003; 289: 2224-‐2229 Synpace trial. Eur Heart J 2004: 25: 1741–1748
SINCOPE 2 0 1 5
www.gimsi.it
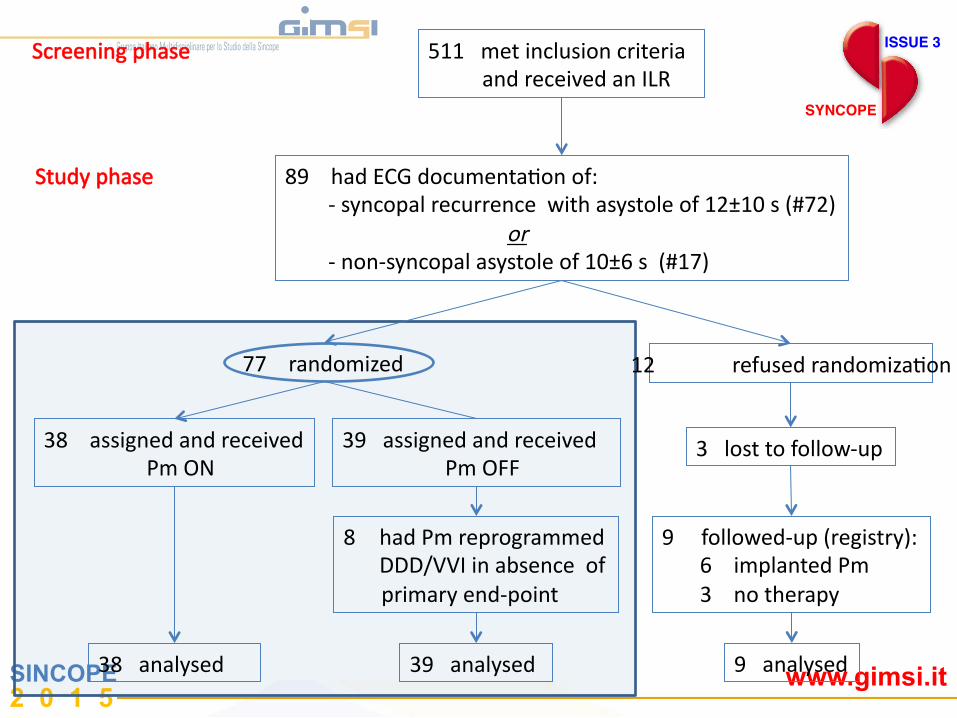
Screening phase
Study phase
77 randomized 12 refused randomizaPon
38 assigned and received Pm ON
39 assigned and received Pm OFF
511 met inclusion criteria and received an ILR
89 had ECG documentaPon of: -‐ syncopal recurrence with asystole of 12±10 s (#72) or -‐ non-‐syncopal asystole of 10±6 s (#17)
8 had Pm reprogrammed DDD/VVI in absence of
primary end-‐point
38 analysed 39 analysed
9 followed-‐up (registry): 6 implanted Pm 3 no therapy
9 analysed
3 lost to follow-‐up
ISSUE 3"
SYNCOPE"
ISSUE 3"
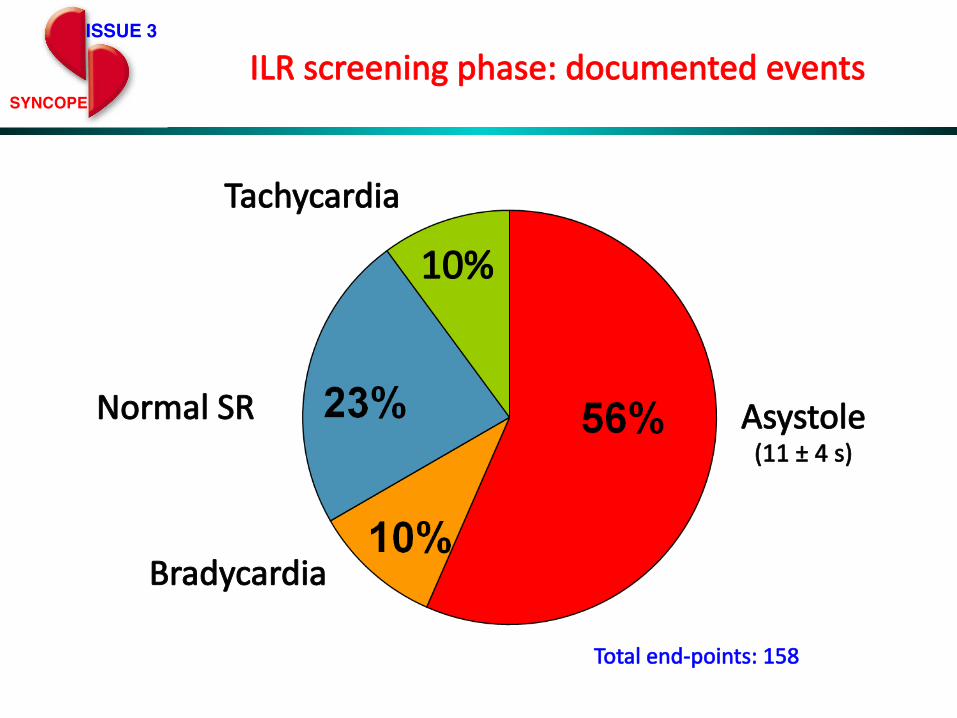
SYNCOPE"ILR screening phase: documented events
Asystole Normal SR
10%
Tachicardia
Asystole (11 ± 4 s)
Bradycardia
Normal SR
Tachycardia
Total end-‐points: 158
SINCOPE 2 0 1 5
www.gimsi.it
ISSUE 3"
SYNCOPE"
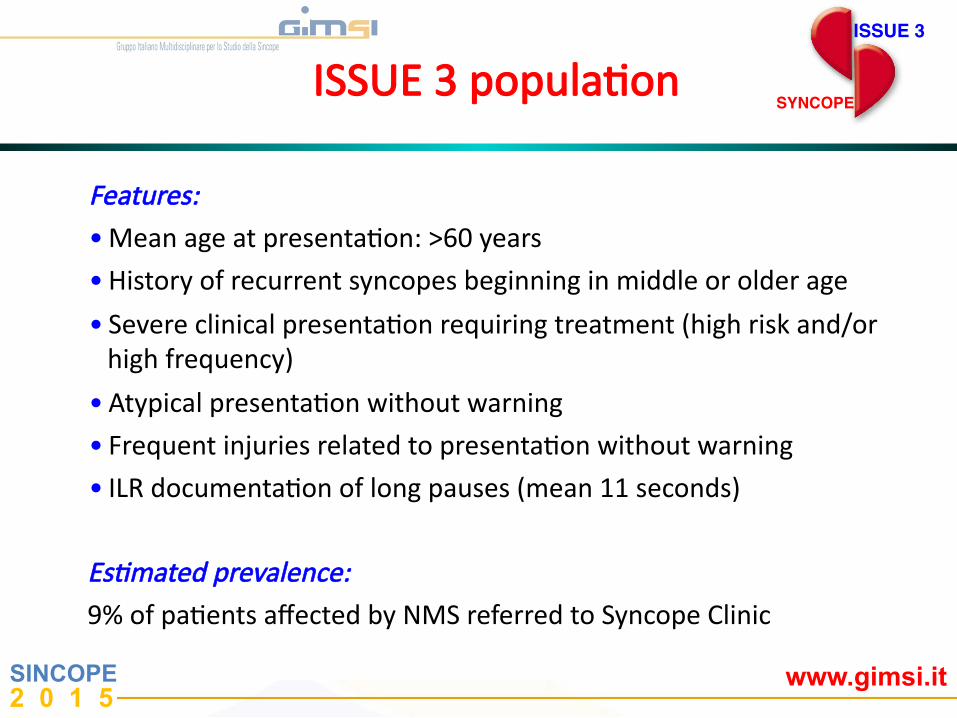
EsDmated prevalence: 9% of paPents affected by NMS referred to Syncope Clinic
ISSUE 3 populaPon
Features: • Mean age at presentaPon: >60 years
• History of recurrent syncopes beginning in middle or older age
• Severe clinical presentaPon requiring treatment (high risk and/or high frequency)
• Atypical presentaPon without warning • Frequent injuries related to presentaPon without warning • ILR documentaPon of long pauses (mean 11 seconds)
0
.1
.2
.3
.4
.5
.6
.7
.8
.9
1
Free
dom
from
syn
copa
l rec
urre
nce
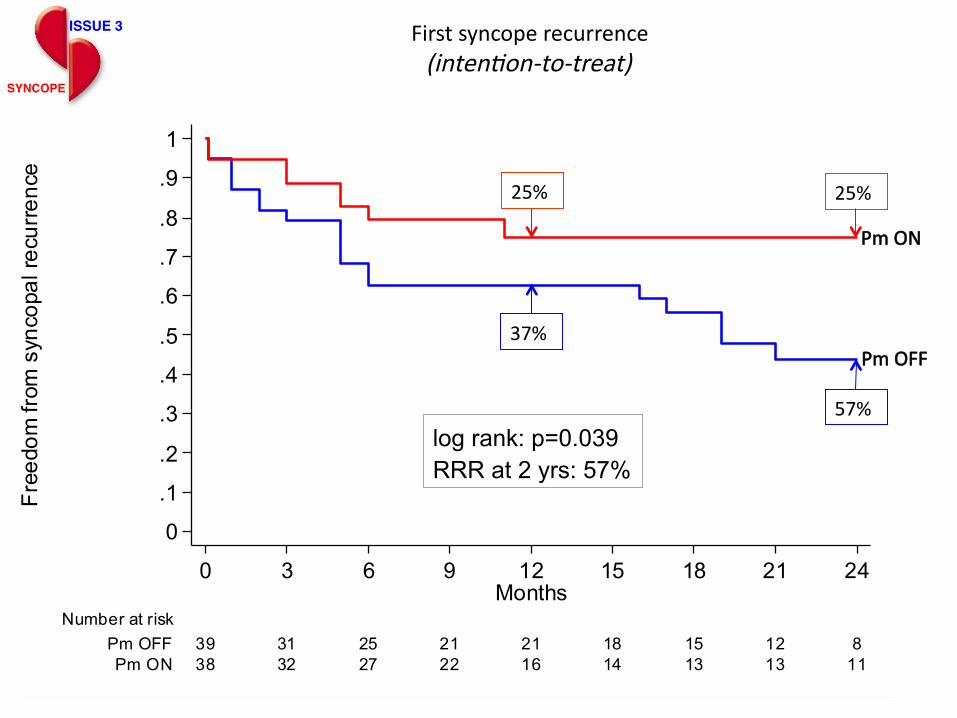
38 32 27 22 16 14 13 13 11Pm ON39 31 25 21 21 18 15 12 8Pm OFF
Number at risk
0 3 6 9 12 15 18 21 24Months
Kaplan-Meier survival estimates
log rank: p=0.039 RRR at 2 yrs: 57%
Pm ON
Pm OFF
First syncope recurrence (intenDon-‐to-‐treat)
ISSUE 3"
SYNCOPE"
25%
37%
25%
57%
SINCOPE 2 0 1 5
www.gimsi.it
ISSUE 3 International Study on Syncope of Uncertain Etiology 3
ISSUE 3"
SYNCOPE"
Conclusions
• Dual-‐chamber permanent pacing is effecPve in reducing recurrence of syncope in paPents ≥40 years with severe asystolic NMS.
• The observed 32% absolute and 57% relaPve syncope reducPon rate support the use of this invasive treatment for the relaPvely benign NMS.
• The overall strategy of using an ILR in order to determine indicaPon for pacing likely contributed to the posiPve findings and explains the discrepancy with the negaPve results of some previous report.
SINCOPE 2 0 1 5
www.gimsi.it Heart 2013;99:1825-‐1831 doi:10.1136/heartjnl-‐2013-‐304399
According to the ILR findings, the accuracy of the diagnosis of NMS made on iniPal evaluaPon was 87%. The diagnosPc accuracy of Plt table test was low: TT was posiPve in 56% NMS, 43% non-‐NMS; an asystolic response was present in 21% NMS and 0% non-‐NMS
SINCOPE 2 0 1 5
www.gimsi.it
ON-TREATMENT ANALYSIS The recurrence of syncope occurred in 10 paced patients (17%) 40 non-paced patients (46%). At 21 months, the estimated product-limit syncope recurrence rates were 27% and 54% respectevely. Risk of recurrence with cardiac pacing was reduced by 57%
SINCOPE 2 0 1 5
www.gimsi.it
-Positive TTT is more likely correlated with a higher frequency of recurrences of syncope in the group treated using a PM, while a negative response seems to predict the success of the pacing therapy. -The results of our study show the capacity of TTT to identify patients with a possible concomitant vasodepressive form ( !?!? ) Consequently PM is not sufficient in a group of patients with positive TTT response.
Circ Arrhythm Electrophysiol. 2014 Feb;7(1):10-‐6
SINCOPE 2 0 1 5
www.gimsi.it
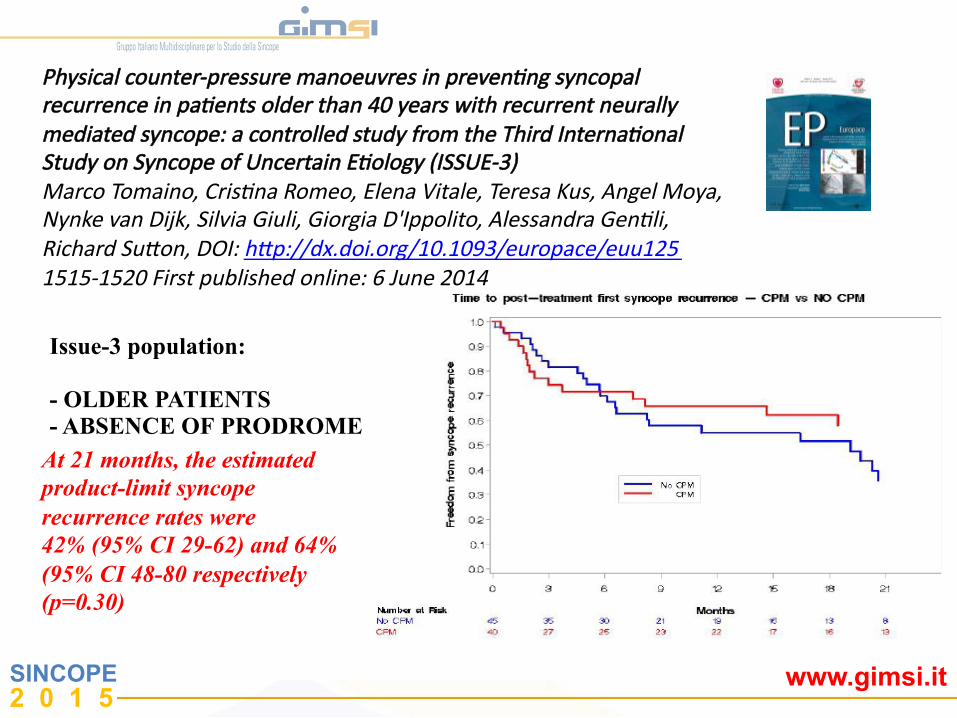
Physical counter-‐pressure manoeuvres in prevenDng syncopal recurrence in paDents older than 40 years with recurrent neurally mediated syncope: a controlled study from the Third InternaDonal Study on Syncope of Uncertain EDology (ISSUE-‐3) Marco Tomaino, CrisDna Romeo, Elena Vitale, Teresa Kus, Angel Moya, Nynke van Dijk, Silvia Giuli, Giorgia D'Ippolito, Alessandra GenDli, Richard Suaon, DOI: hap://dx.doi.org/10.1093/europace/euu125 1515-‐1520 First published online: 6 June 2014
Issue-3 population: - OLDER PATIENTS - ABSENCE OF PRODROME
At 21 months, the estimated product-limit syncope recurrence rates were 42% (95% CI 29-62) and 64% (95% CI 48-80 respectively (p=0.30)
SINCOPE 2 0 1 5
www.gimsi.it
Bolzano
SYNCOPE TAKE HOME MESSAGES
ISSUE 3 TRIAL
" Clinical evaluation " Diagnostic iter guided by ILR " Selection of patients who undergo to PM implantation " Reducing of recurrences and improvement of QOL by pacing DDD RDR
" PCM Therapy

SINCOPE 2 0 1 5
www.gimsi.it
SINCOPE 2 0 1 5
www.gimsi.it
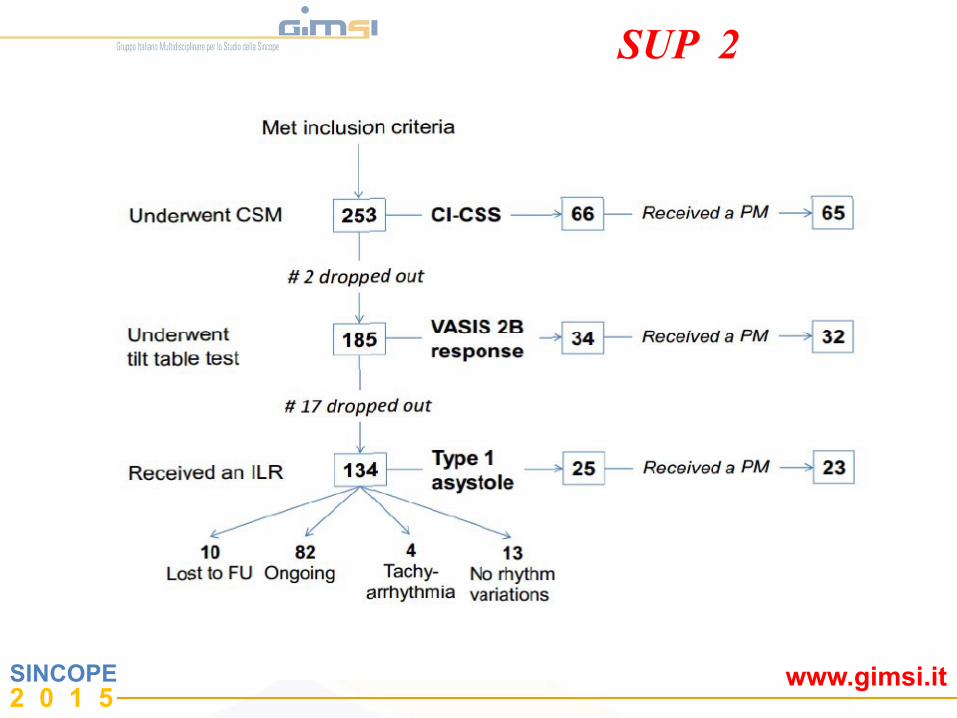
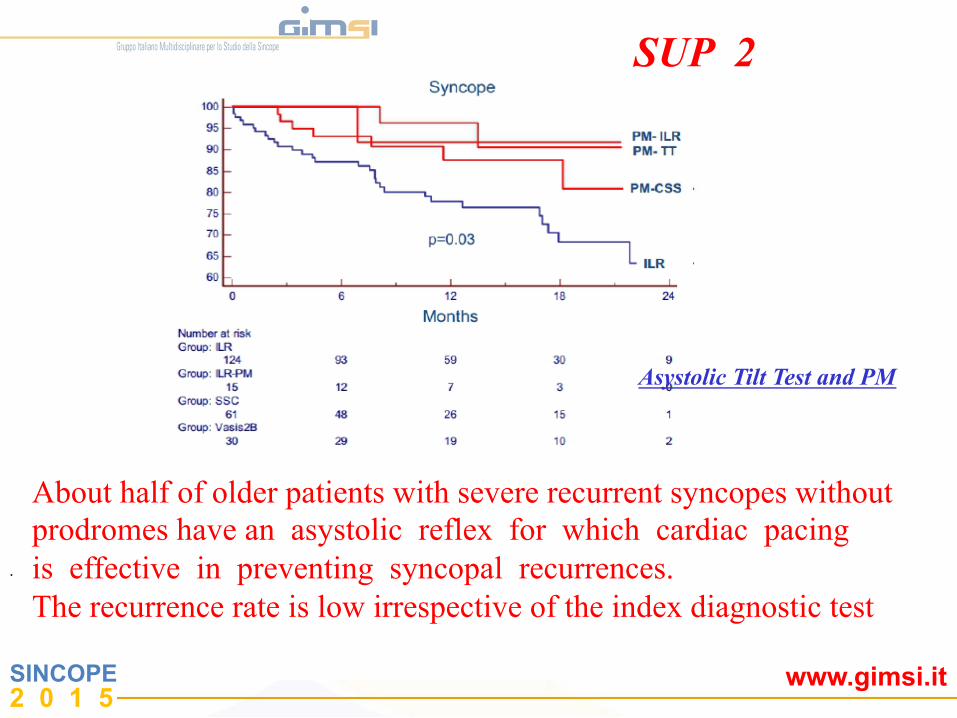
SUP 2
SINCOPE 2 0 1 5
www.gimsi.it
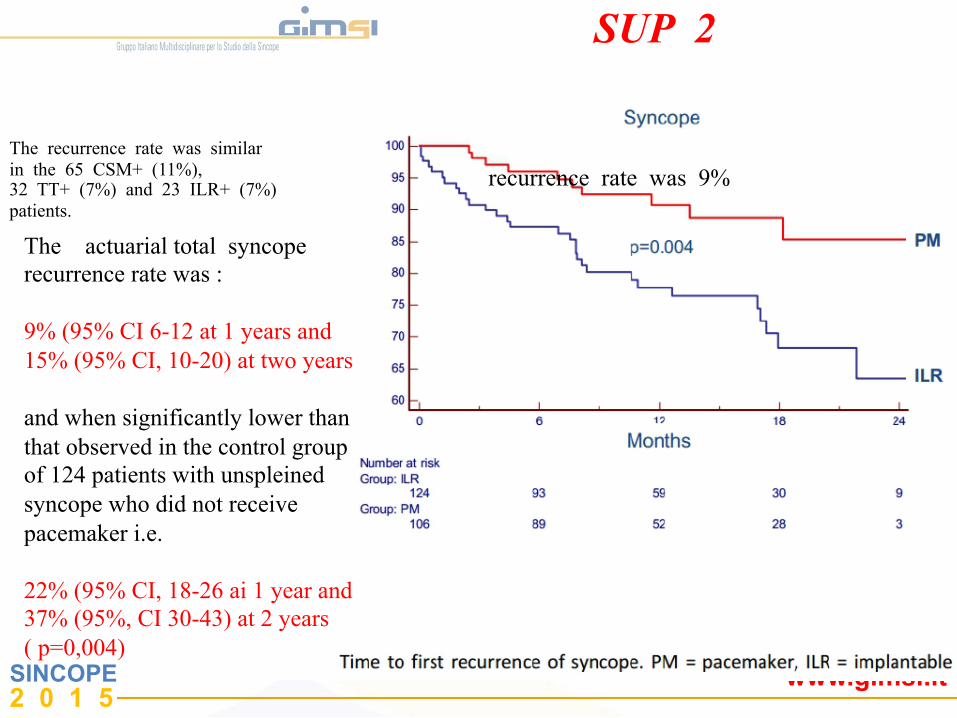
The recurrence rate was similar in the 65 CSM+ (11%), 32 TT+ (7%) and 23 ILR+ (7%) patients.
The actuarial total syncope recurrence rate was : 9% (95% CI 6-12 at 1 years and 15% (95% CI, 10-20) at two years and when significantly lower than that observed in the control group of 124 patients with unspleined syncope who did not receive pacemaker i.e. 22% (95% CI, 18-26 ai 1 year and 37% (95%, CI 30-43) at 2 years ( p=0,004)
recurrence rate was 9%
SUP 2
SINCOPE 2 0 1 5
www.gimsi.it
About half of older patients with severe recurrent syncopes without prodromes have an asystolic reflex for which cardiac pacing is effective in preventing syncopal recurrences. The recurrence rate is low irrespective of the index diagnostic test
.
Asystolic Tilt Test and PM
SUP 2
SINCOPE 2 0 1 5
www.gimsi.it
0
5
10
15
20
25
30
35
40 2008
2009
2010
2011
2012
2013
2014
Lineare (2008)
Lineare (2009)
Lineare (2010)
Lineare (2011)
Lineare (2012)
Lineare (2014)
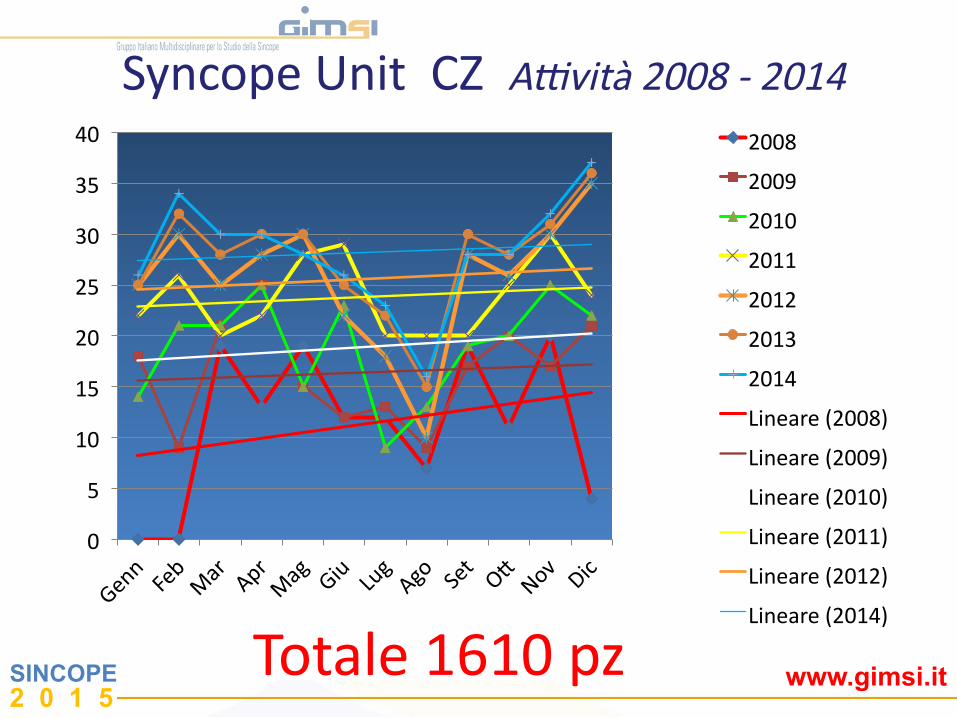
Syncope Unit CZ Aevità 2008 -‐ 2014
Totale 1610 pz
SINCOPE 2 0 1 5
www.gimsi.it
0
100
200
300
400
500
600
700
800
900
1000
NegaPvi Tipo I Tipo 2A Tipo 2B Tipo 3 MSC pos
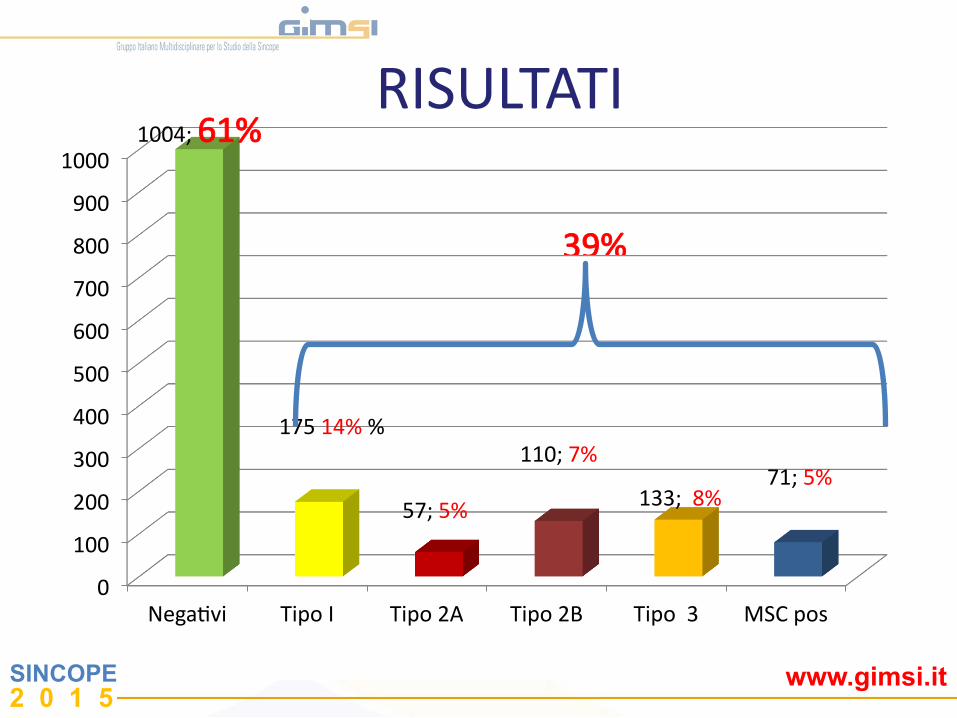
1004; 61%
175 14% %
57; 5%
110; 7%
133; 8% 71; 5%
39%
RISULTATI
SINCOPE 2 0 1 5
www.gimsi.it
0
20
40
60
80
100
120
140
160
180
Tipo I Tipo 2A Tipo 2B Tipo 3 MSC pos Altri
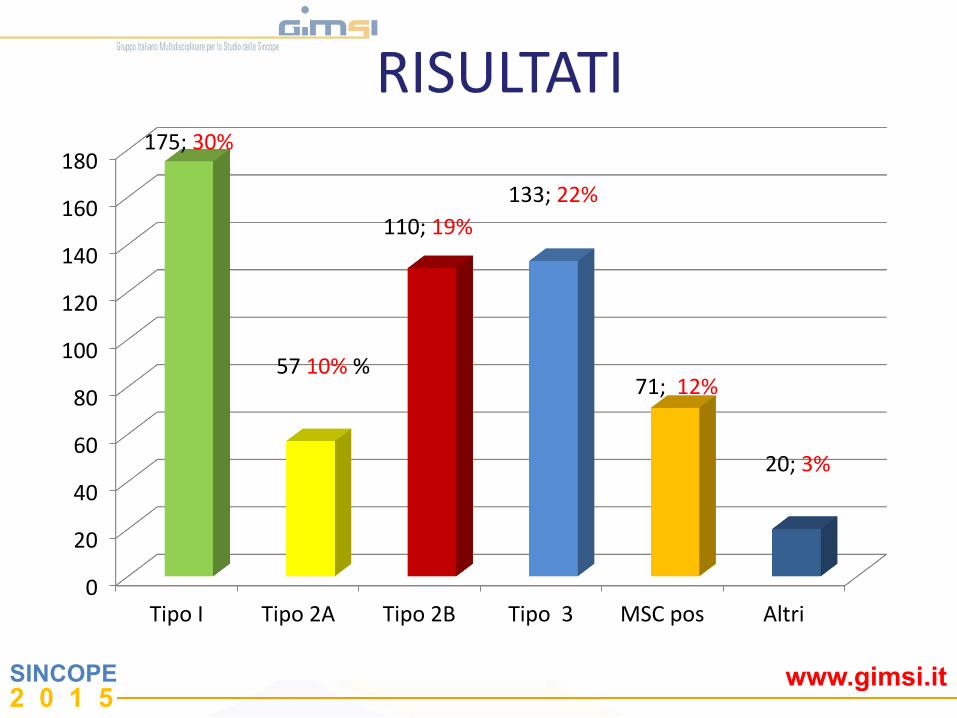
175; 30%
57 10% %
110; 19% 133; 22%
71; 12%
20; 3%
RISULTATI
SINCOPE 2 0 1 5
www.gimsi.it
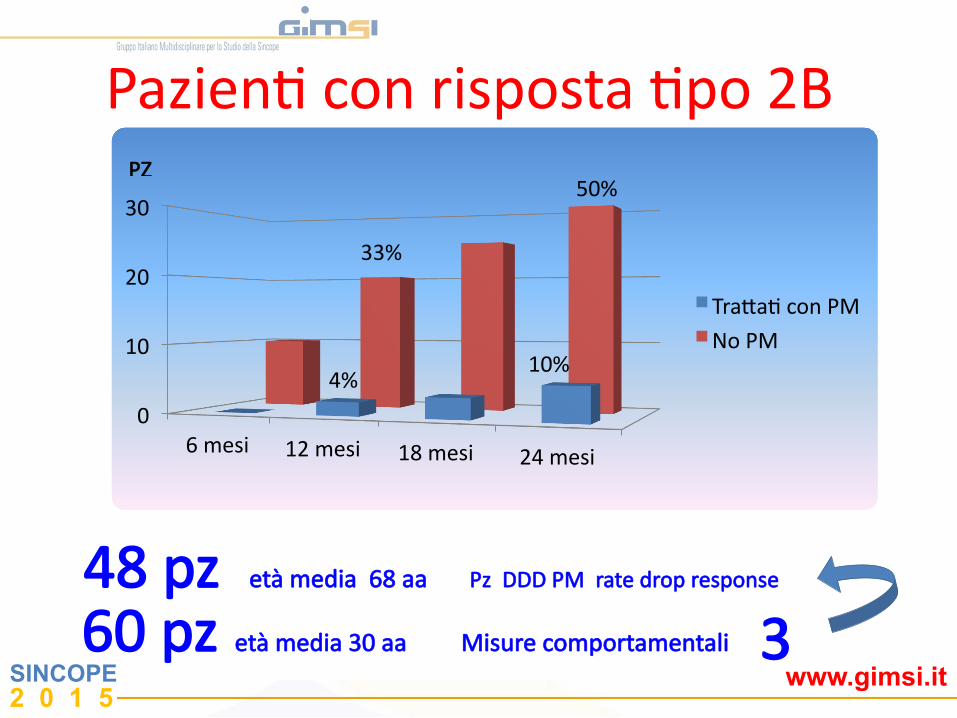
0
10
20
30
6 mesi 12 mesi 18 mesi 24 mesi
TraJaP con PM
No PM
PZ
PazienP con risposta Ppo 2B
33%
50%
4% 10%
48 pz età media 68 aa Pz DDD PM rate drop response
60 pz età media 30 aa Misure comportamentali 3

SINCOPE 2 0 1 5
www.gimsi.it
SINCOPE 2 0 1 5
www.gimsi.it
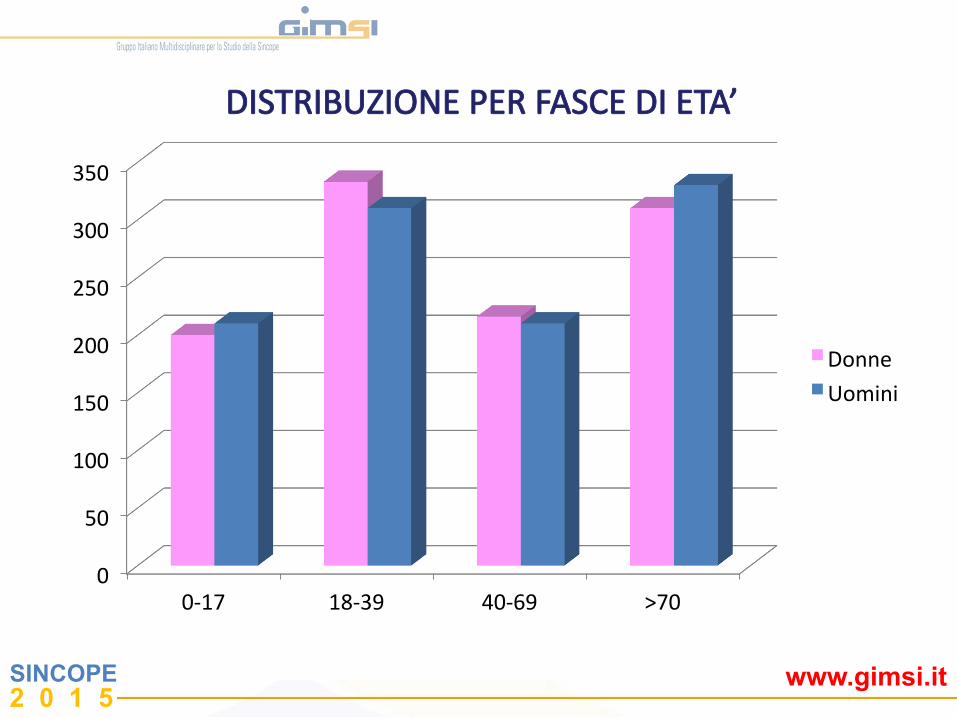
0
50
100
150
200
250
300
350
0-‐17 18-‐39 40-‐69 >70
Donne
Uomini
DISTRIBUZIONE PER FASCE DI ETA’