Embed Size (px)
Citation preview

Time to First Disease Progression, But Not b2-Microglobulin, Predicts Outcome in Myeloma PatientsWho Receive Thalidomide as Salvage Therapy
Antonio Palumbo, MD1
Sara Bringhen, MD1
Patrizia Falco, MD1
Federica Cavallo, MD1
Maria Teresa Ambrosini, MD1
Ilaria Avonto, MD1
Francesca Gay, MD1
Tommaso Caravita, MD2
Benedetto Bruno, MD1
Mario Boccadoro, MD1
1 Division of Hematology, University of Torino,San Giovanni Battista Hospital, Turin, Italy.
2 Division of Hematology, University Tor Vergata,St. Eugenio Hospital, Rome, Italy.
BACKGROUND. Baseline parameters that may be predictive of outcome after thali-
domide treatment have been investigated to identify which myeloma patient sub-
groups will most benefit from this drug.
METHODS. Thalidomide has been used as a salvage regimen at the study institu-
tion since 1999. A total of 102 myeloma patients who were diagnosed between
January 1999 and February 2005 were evaluable for intention-to-treat analysis; 78
patients received thalidomide (at a dose of 100 mg/day continuously) and dexa-
methasone (at a dose of 40 mg/day on Days 1–4 each month) (TD) as salvage
treatment whereas 24 patients died or were lost to follow-up before the initiation
of TD. Several parameters such as serum b2-microglobulin, serum C-reactive
protein, immunoglobulin A isotype, hemoglobin, stage of disease, bone marrow
plasmacytosis, age, serum creatinine, gender, stem cell transplantation at the
time of diagnosis, and time to first disease progression were analyzed in associa-
tion with overall survival (OS).
RESULTS. The OS from the time of diagnosis was 43.8 months. Using univariate
analysis, factors found to be associated with a shorter OS were a creatinine level
�2 mg/dL (P 5 .05), stage III (P 5 .04), and time to first disease progression �12
months (P < .0001). The only factor that remained significantly associated with a
shorter OS in multivariate models was time to first disease progression �12
months (P 5 .0006). Elevated serum b2-microglobulin was not found to be pre-
dictive of poor OS.
CONCLUSIONS. Time to first disease progression >12 months was found to be
the best indicator of OS. Elevated serum b2-microglobulin, generally considered
to be a poor prognostic factor, was not found to be predictive of outcome.
Cancer 2007;110:824–9. � 2007 American Cancer Society.
KEYWORDS: thalidomide, prognostic factors, b2-microglobulin, multiple myeloma,survival.
B ecause of the high heterogeneity of the disease, survival for
patients with multiple myeloma (MM) varies from <6 months
to >10 years. Several clinical and laboratory parameters have been
described as independent predictors of survival. Hemoglobin and
serum calcium, albumin, and creatinine levels as well as serum b2-microglobulin and C-reactive protein levels and the proliferative ac-
tivity of bone marrow plasma cells have emerged as the most
powerful independent prognostic factors.1–6 Recently, the negative
prognostic role of specific chromosomal translocations such as
t(4;14), t(14;16), t(14;20), or deletion 17q13 has been established.7–9
Chromosome 13 deletion is the most commonly reported prognostic
abnormality.8,9 The magnitude of M-protein reduction and time to
Address for reprints: Antonio Palumbo, MD, Divi-sione di Ematologia dell’Universita di Torino,Azienda Ospedaliera S. Giovanni Battista, ViaGenova 3, 10126 Torino, Italy; Fax: (011) 30-011-6963737; E-mail: [email protected]
Supported by Associazione Italiana Leucemie,Compagnia di S. Paolo, Associazione per lo Studioe la Cura delle Malattie del Sangue, FondazioneNeoplasie Sangue Onlus, Fondazione Cassa di Ris-parmio di Torino, Ministero Universita RicercaScientifica e Tecnologica (MIUR), and ConsiglioNazionale delle Ricerche (CNR).
We thank the patients, nurses, and the ClinicalTrial Office staff (Tiziana Marangon, FedericaLeotta, Antonella Bono, Maria Jose Fornaro, andBarbara Marchese).
Received February 1, 2007; revision receivedMarch 27, 2007; accepted March 30, 2007.
ª 2007 American Cancer SocietyDOI 10.1002/cncr.22855Published online 26 June 2007 in Wiley InterScience (www.interscience.wiley.com).
824

the first disease progression have been used as surro-
gate markers of survival and/or treatment benefit. In
a large survey of 1555 untreated patients, time to first
disease progression >12 months, rather than the
magnitude of response, emerged as the best indica-
tor of survival.10
In the last decade, thalidomide, a potent immu-
nomodulatory drug with antiangiogenesis properties,
has been introduced in the treatment of MM. Thali-
domide was found to synergistically enhance the ac-
tivity of dexamethasone in preclinical studies11 and
their combination induced partial responses in 41%
to up to 55% of patients, with a median progression-
free survival of 1 year in patients with advanced
MM.12,13 The combination of thalidomide and dexa-
methasone (TD) has been proven effective in a large
cohort of pretreated patients and their 3-year survival
was significantly increased compared with historic
controls treated with conventional chemotherapy
(P < .0016).14 The TD combination currently repre-
sents one of the most widely used salvage regimens
for MM.
Prognostic factors may help to select patients
who will benefit the most from different therapies. In
the current study, we evaluated baseline demographic
and clinical parameters to determine their value in
predicting the outcome of patients with recurrent or
refractory MM who were treated with TD.
MATERIALS AND METHODSPatientsAt our institution, all myeloma patients have received
salvage therapy with TD as per the center guidelines
since 1999. A total of 102 patients were diagnosed
between January 1999 and February 2005 and were
evaluated by intention-to-treat analysis. Seventy-
eight of these patients received TD salvage therapy
between June 2000 and December 2005, whereas 24
patients either died or were lost to follow-up before
the initiation of TD therapy. Inclusion criteria were
previously treated MM, age >18 years with no upper
limits, and measurable disease. The staging system
of Durie and Salmon was used.15 Patients agreed to
use contraception, and women of childbearing age
were given a pregnancy test before study enrollment.
Exclusion criteria were a second malignancy, psychi-
atric disease, and any grade 2 peripheral neuropathy
according to Common Toxicity Criteria 2.0. Abnormal
cardiac function, chronic respiratory disease, and
abnormal liver or renal function were not considered
to be criteria for exclusion. The study was approved
by the local Institutional Review Board. Written
informed consent was obtained at the time of study
entry in accordance with the Declaration of Helsinki.
Treatment and Evaluation of OutcomeThalidomide (Grunenthal GmbH, 52222 Stolberg)
was administered at a dose of 100 mg/day continu-
ously and oral dexamethasone was administered at a
dose of 40 mg/day on Days 1–4 each month until
evidence of recurrence or refractory disease. Re-
sponses were categorized according to the criteria of
the European Group for Blood and Marrow Trans-
plantation with the addition of a very good partial
response (VGPR) category.16 Briefly, a complete
response (CR) required the disappearance of serum/
urine myeloma protein and negative immunofixa-
tion. A partial response (PR) required at least a 50%
reduction in serum myeloma protein and a 90%
decrease in urine myeloma protein. Near-complete
remission (nCR), a subcategory of PR, required the
disappearance of serum/urine myeloma proteins
with positive immunofixation. VGPR, a subcategory
of PR, required a reduction of 90% in serum my-
eloma proteins. Minimal response (MR) was defined
as a reduction in serum myeloma protein of 25% to
49% and a reduction in urine myeloma protein of
50% to 89%. Disease progression was defined as an
increases in serum or urine myeloma protein
of >25%. Responses were confirmed after 6 weeks.
Bone marrow plasmacytosis and skeletal disease
were included in the response evaluation. Event-free
survival (EFS) was calculated from the initiation of
thalidomide treatment until the date of disease pro-
gression, relapse death from any cause, or the date
the patient was last known to be in disease remis-
sion. Overall survival (OS) was calculated from the
time of diagnosis until the date of death from any
cause or the date the patient was last known to be
alive.
Eleven potentially relevant predictors of outcome
were evaluated. Chromosome 13 deletion and albu-
min were not included because data regarding these
2 variables were not available for a large number of
patients. Age, time to first disease progression, and
laboratory variables were dichotomized with the usu-
ally reported cutoff points. For OS, the following fac-
tors were assessed: age (<65 years vs �65 years),
gender, stage of disease (Durie and Salmon stage I,
II, or III), previous stem cell transplantation, percent-
age of plasma cells in bone marrow biopsy (<40%
vs �40%), hemoglobin concentration (�10 g/dL
vs >10 g/dL), creatinine (<2 mg/dL vs �2 mg/dL),
M-protein isotype (immunoglobulin [Ig] A, IgG, light
chain), serum b2-microglobulin (<3.5 mg/L vs �3.5
mg/L), C-reactive protein (<6 mg/L vs �6 mg/L),
Prognostic Factors With Thalidomide Therapy/Palumbo et al. 825

and time to first disease progression (�12 months
vs >12 months). Hemoglobin, creatinine, serum b2-microglobulin, and C-reactive protein levels were
measured at the time of diagnosis.
Statistical AnalysesAll 102 patients were entered into the intention-to-
treat analysis. Data were analyzed as of April 1, 2006.
Survival data were analyzed using the Kaplan-Meier
method17 and differences were tested by the log-rank
test. In the univariate analysis assessing OS, Cox pro-
portional hazards regression was performed to detect
clinically relevant interactions between outcome and
each prognostic factor.18 The Cox proportional hazards
model was used to estimate the hazards ratios (HR)
and the 95% confidence intervals (95% CI). An HR >1
indicated an increased risk, whereas an HR <1 indi-
cated a decreased risk.
In the multivariate analysis assessing OS, the Cox
proportional hazards model was used to analyze all
factors to identify independent variables that were
predictive of survival. A P value <.05 was considered
statistically significant. All statistical tests were
2-sided. Statistical analyses were performed using SAS
software (version 8.2; SAS Institute Inc, Cary, NC).
RESULTSThe study group was comprised of 102 patients (60 of
whom were male) with median age of 63.7 years
(range, 31.3–83.7 years). Patient characteristics are
illustrated in Table 1. At the time of diagnosis, 53
patients were treated with autologous stem cell trans-
plantation (41 patients received tandem melphalan at
a dose of 100 mg/m2 and 12 patients received tandem
melphalan at a dose of 200 mg/m2), and 49 patients
were treated with conventional chemotherapy (38
patients received oral melphalan and prednisone and
11 patients were treated with the combination of
dexamethasone, doxorubicin, and vincristine). The
median time to first disease progression was 20.1
months in patients treated with autologous stem cell
transplantation and 9.9 months in patients treated
with conventional chemotherapy. The median OS
from the time of diagnosis was 43.8 months.
Patients Receiving TDSeventy-eight patients received TD (63 after first-line
therapy, 10 after 2-line therapy, and 5 after third-line
therapy, respectively). TD was administered a median
of 19.5 months from the time of diagnosis. The me-
dian follow-up from the initiation of TD therapy was
27.5 months (range, 3.9–65.7 months). CRs or PRs
were observed in 39 of the 78 patients (50%). A nCR
or CR were achieved in 11 patients (14.1%) and
VGPR or CR were observed in 16 patients (20.5%).
Fifty-two of the 78 patients (67%) experienced dis-
ease progression, recurrence, or death and 38
patients died (49%). The median EFS from the time
of the initiation of TD therapy and the OS from the
time of diagnosis were 15.7 months and 57.4 months,
respectively. The achievement of at least a VGPR did
not appear to affect either the EFS (HR of 1.29; 95%
CI, 0.53–3.15 [P 5 .58]) or OS of patients treated with
TD (HR of 0.86; 95% CI, 0.31–2.35 [P 5 .77]).
Prognostic Factors Affecting OutcomeFactors associated with OS from the time of diagno-
sis were assessed by univariate analysis. Gender, age,
TABLE 1Patient Characteristics
Characteristics N 5 102
Age, y
Median (range) 63.7 (31.3–83.7)
�65 45 (44.1)
�75 13 (12.7)
Sex
Male 60 (58.8)
Female 42 (41.2)
M-protein class, no. (%)
IgG 51 (50.0)
IgA 25 (24.5)
Bence Jones protein 24 (23.5)
Other 2 (2.0)
Stage, no. (%)
I 4 (3.9)
II 22 (21.6)
III 76 (74.5)
Bone marrow plasma cells, %
Median (range) 50 (1–95)
�40%, no. (%) 57 (55.9)
b2-microglobulin, mg/L
Median (range) 3.6 (1.0–37.5)
�3.5, no. (%) 36 (35.3)
Plasma c-reactive protein, mg/L
Median (range) 3.4 (0.1–40)
�6, no. (%) 18 (17.6)
Hemoglobin, g/dL
Median (range) 10.2 (5.1–15.5)
�10, no. (%) 41 (40.2)
Serum creatinine, mg/dL
Median (range) 1.1 (0.4–8.4)
�2, no. (%) 15 (14.7)
Previous therapy
SCT 53 (52.0)
CC 49 (48.0)
Duration of first remission, mo
>12, no. (%) 60 (58.8)
�12, no. (%) 42 (41.2)
Ig indictes immunoglobulin; SCT, stem cell transplantation; CC, conventional chemotherapy.
826 CANCER August 15, 2007 / Volume 110 / Number 4

hemoglobin, serum b2-microglobulin, serum C-reac-
tive protein, previous autologous stem cell transplan-
tation, bone marrow plasma cell infiltration, and IgA
isotype did not appear to affect patient outcome,
whereas a serum creatinine �2 mg/dL (P 5 .05),
stage III disease (P 5 .04), and time to first disease
progression �12 months (P < .0001) were found to
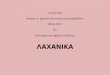
be associated with shorter OS (Table 2). The median
OS of patients who developed disease progression �and >12 months from the time of diagnosis were
19.6 months and 59.1 months, respectively. Disease
progression >12 months from the time of diagnosis
was associated with significantly longer survival
(P < .0001). Kaplan-Meier survival curves are shown
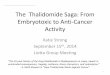
in Figure 1. The median OS of patients with serum
b2-microglobulin <3.5 mg/L and those with serum
b2-microglobulin �3.5 mg/L were 43.8 months and
45.0 months, respectively. Low serum b2-microglobu-
lin was not found to be associated with significantly
longer survival (P 5 .96), as shown in Figure 2.
The only factor that remained significantly as-
sociated with a shorter OS on multivariate models
was a time to first disease progression �12 months
(P 5 .0006) (Table 3).
DISCUSSIONThalidomide in combination with corticosteroids
has been widely used as a salvage regimen for
patients with recurrent and refractory MM. In the
current study, the results of multivariate analysis
indicated that a time to first disease progression >12
months is the best predictor of prolonged survival,
whereas both elevated serum b2-microglobulin
and C-reactive protein levels do not appear to affect
outcome.
It has previously been shown that the best inde-
pendent indicator of survival duration is time to first
disease progression.10 In some studies, the achieve-
ment of a CR has been reported to be an excellent
predictor of outcome,19–21 whereas in other reports,
TABLE 2Effect of Demographic Variables, Disease Characteristics, PreviousTreatment, and Time to First Disease Progression on Overall Survivalon Univariate Analysis
P HR 95% CI
Sex, M vs F .56 0.86 0.52–1.43
Age, <65 y vs �65 y .98 1.00 0.61–1.67
b2-microglobulin, <3.5 mg/L vs �3.5 mg/L .12 1.71 0.87–3.35
C-reactive protein, <6 mg/L vs �6 mg/L .50 1.29 0.61–2.69
Hemoglobin, >10 g/dL vs �10 g/dL .18 1.45 0.85–2.49
SCT at diagnosis, yes vs no .29 1.31 0.79–2.16
Bone marrow plasma cells, <40% vs �40% .38 1.25 0.76–2.07
Creatinine, <2 mg/dL vs �2 mg/dL .05 1.90 1.01–3.65
IgA, yes vs no .95 1.02 0.58–1.80
Stage, I–II vs III .04 2.74 1.40–5.36
Time to first disease progression,
�12 mo vs >12 mo < .0001 3.00 1.81–4.99
HR indicates hazards ratio; 95% CI, 95% confidence interval; M, male; F, female; SCT, stem cell trans-
plantation; IgA, immunoglobulin A.
Boldface type represents statistical significance.
FIGURE 1. Overall survival according to time to first disease progression.The difference was found to be statistically significant (P < .0001).
FIGURE 2. Overall survival according to b2-microglobulin. The difference
was not found to be statistically significant (P 5 .96).
TABLE 3Effect of Disease Characteristics and Time to First DiseaseProgression on Overall Survival on Multivariate Analysis
P HR 95% CI
b2-microglobulin, <3.5 mg/L vs �3.5 mg/L .65 1.18 0.57–2.46
Creatinine, <2 mg/dL vs �2 mg/dL .46 1.30 0.65–2.61
Stage, I–II vs III .07 1.88 0.95–3.74
Time to first disease progression,
�12 mo vs >12 mo .0006 2.65 1.52–4.60
HR indicates hazards ratio; 95% CI, 95% confidence interval.
Boldface type represents statistical significance.
Prognostic Factors With Thalidomide Therapy/Palumbo et al. 827

the magnitude of response as an independent vari-
able did not predict survival.10,22–24 Major determi-
nants of survival most likely are related to 1) the
number and intrinsic biology of the resistant my-
eloma cells remaining after induction therapy25,26
and 2) host factors responsible for myeloma cell
growth regulation.27,28 This may explain why the du-
ration of disease remission rather than the mag-
nitude of response, which does not necessarily
reflect these 2 biologic factors, is a better predictor
of survival. In the light of these results, clinicians
and investigators should be particularly aware of
response duration rather than single M-protein
decrements in assessing the usefulness and clinical
benefit of a given treatment in patients with MM.
The results of the current study demonstrate that
patients with a particularly good prognostic marker,
such as longer time to first disease progression, are
those who will benefit the most from TD salvage
therapy. This may lead physicians to consider more
aggressive approaches such as the combination of
melphalan and/or doxorubicin and/or cyclophospha-
mide with thalidomide in patients with a short dura-
tion of response. Previous experiences were derived
from patients treated with standard-dose or high-
dose chemotherapy only, whereas in the current
study, the impact of time to first disease progression
was evaluated in patients who received a new, biolo-
gically based treatment with thalidomide.
Serum b2-microglobulin level is one of the most
widely used prognostic factors in MM. The impor-
tance of prognostic factors in the pretreatment
evaluation of MM patients has gained even more sig-
nificance with the creation of the new International
Staging System.6 This system uses only 2 simple fac-
tors for staging newly diagnosed patients: serum albu-
min as an indicator of rapid myeloma growth and b2-microglobulin as a marker of tumor burden. In the
current study, both b2-microglobulin and C-reactive
protein were not found to be predictive of outcome.
New drugs such as thalidomide and bortezomib may
reduce the impact of these factors even though to our
knowledge the reasons for this have not yet been fully
elucidated. In 1 report, an increased baseline b2-microglobulin level was associated with poor OS on
univariate analysis but not on multivariate analysis in
patients with recurrent and refractory MM who were
treated with bortezomib.29 In another study in which
thalidomide was included in a double autologous
stem cell transplantation program for newly diag-
nosed MM patients, the probability of EFS was found
to be significantly lower in patients with high levels of
b2-microglobulin. However, this parameter failed to
predict OS on multivariate analysis.21
Patients with a poor prognosis remain an
unsolved therapeutic challenge. New drugs, highly
effective as salvage treatments, have been shown to
be more effective in good-risk patients.21,30,31
Patients with aggressive disease recurrence and
those at poor risk also may benefit less from the
TD combination.
It should be emphasized that the analyses and
models used in the current study should be consid-
ered exploratory and our conclusions are subject to
confirmation by further clinical studies. However,
although these precautions are mandatory, there is
growing evidence that major prognostic factors such
as serum b2-microglobulin and chromosome 13 de-
letion may have a smaller impact on OS after therapy
with thalidomide and/or bortezomib. Such evidence
calls for the better identification of newer prognostic
factors that may better define those patients who
would benefit the most from salvage regimens with
new drugs.
REFERENCES1. Bataille R, Durie BGM, Grenier J, et al. Prognostic factors
and staging in multiple myeloma: a reappraisal. J Clin
Oncol. 1986;4:80–87.
2. Merlini G, Waldenstrom JG, Jayakar SD. A new improved
clinical staging system for multiple myeloma based on
analysis of 123 treated patients. Blood. 1980;55:1011–1019.
3. Bataille R, Durie BGM, Grenier J. Serum beta-2 microglo-
bulin and survival duration in multiple myeloma: a simple
reliable marker for staging. Br J Haematol. 1983;55:439–
447.
4. Bataille R, Boccadoro M, Klein B, et al. C-reactive protein
and beta-2 microglobulin produce a sample and powerful
myeloma staging system. Blood. 1992;80:733–737.
5. Greipp PR, Lust JA, O’Fallon WM, et al. Plasma cell label-
ing index and beta-2 microglobulin predict survival inde-
pendent of thymidine-kinase and C-reactive protein in
multiple myeloma. Blood. 1993;81:3382–3387.
6. Greipp PR, San Miguel J, Durie BGM, et al. International
staging system for multiple myeloma. J Clin Oncol. 2005;
23:3412–3420.
7. Jaksic W, Trudel S, Chang H, et al. Clinical outcomes in
t(4;14) multiple myeloma: a chemotherapy-sensitive dis-
ease characterized by rapid relapse and alkylating agent re-
sistance. J Clin Oncol. 2005;23:7069–7073.
8. Chng WJ, Santana-Davila R, Van Wier SA, et al. Prognostic
factors for hyperdiploid-myeloma: effects of chromosome
13 deletions and IgH translocations. Leukemia. 2006;20:
807–813.
9. Jagannath S, Richardson PG, Sonneveld P, et al. Bortezomb
appears to overcome the poor prognosis conferred by
chromosome 13 deletion in phase 2 and 3 trials. Leukemia.
2007;21:151–157.
10. Durie BGM, Jacobson J, Barlogie B, et al. Magnitude of
response with myeloma frontline therapy does not predict
outcome: importance of time to progression in Southwest
Oncology Group Chemotherapy Trials. J Clin Oncol. 2004;
22:1857–1863.
828 CANCER August 15, 2007 / Volume 110 / Number 4

11. Hideshima T, Chauhan H, Shima Y, et al. Thalidomide and
its analogs overcome drug resistance of human multiple
myeloma cells to conventional therapy. Blood. 2000;96:
2943–2950.
12. Dimopoulos MA, Zervas K, Kouvatseas G, et al. Thalido-
mide and dexamethasone combination for refractory mul-
tiple myeloma. Ann Oncol. 2001;12:991–995.
13. Palumbo A, Giaccone L, Bertola A, et al. Low-dose thali-
domide plus dexamethasone is an effective salvage ther-
apy for advanced myeloma. Haematologica. 2001;86:399–
403.
14. Palumbo A, Bertola A, Falco P, et al. Efficacy of low-dose
thalidomide and dexamethasone as first salvage regimen in
multiple myeloma. Hematol J. 2004;5:318–324.
15. Durie BG, Salmon SE. A clinical staging system for multiple
myeloma. Correlation of measured myeloma cell mass
with presenting clinical features, response to treatment,
and survival. Cancer. 1975;36:842–854.
16. Blade J, Samson D, Reece D, et al., on behalf of the My-
eloma Subcommittee of the EBMT (European Group for
Blood and Marrow Transplant). Criteria for evaluating dis-
ease response and progression in patients with multiple
myeloma treated by high-dose therapy and haemopoietic
stem cell transplantation. Br J Haematol. 1998;102:1115–
1123.
17. Kaplan EL, Meier P. Non parametric estimation from
incomplete observations. J Am Stat Assoc. 1958;53:457–
481.
18. Cox DR. Regression model and life-tables (with discussion).
J R Stat Soc B. 1972;34:187–220.
19. Attal M, Harousseau JL, Stoppa AM, et al. A prospective,
randomised trial of autologous bone marrow transplanta-
tion and chemotherapy in multiple myeloma. N Engl J
Med. 1996;335:91–97.
20. Child JA, Morgan GJ, Davies FE, et al. High-dose chemo-
therapy with hematopoietic stem-cell rescue for multiple
myeloma. N Engl J Med. 2003;348:1875–1883.
21. Barlogie B, Tricot G, Anaissie E, et al. Thalidomide and
hematopoietic-cell transplantation for multiple myeloma.
N Engl J Med. 2006;354:1021–1030.
22. Anderson JR, Cain KC, Gelber RD. Analysis of survival by
tumor response. J Clin Oncol. 1983;1:710–719.
23. Palmer M, Belch A, Hanson J, et al. Reassessment of the
relationship between M-protein decrement and survival in
multiple myeloma. Br J Cancer. 1989;59:110–112.
24. Durie BGM. Is magnitude of initial response predictive for
survival in multiple myeloma? Ann Oncol. 1991;2:166.
25. Boccadoro M, Gavarotti P, Fossati G, et al. Low plasma cell
3(H) thymidine incorporation in monoclonal gammopathy of
undetermined significance (MGUS) smouldering myeloma
and remission phase myeloma: a reliable indicator of patients
not requiring therapy. Br J Haematol. 1984;58:689–696.
26. Durie BGM, Russell DH, Salmon SE. Reappraisal of plateau
phase in myeloma. Lancet. 1980;2:65–68.
27. Brown RD, Pope B, Yuen E, et al. The expression of T cell
related co-stimulatory molecules in multiple myeloma.
Leuk Lymphoma. 1998;31:379–384.
28. Brown RD, Pope B, Murray A, et al. Dendritic cells from
patients with myeloma are numerically normal, but func-
tionally defective as they fail to up regulate CD80 (B7-1)
expression after huCD40LT stimulation due to inhibition
by transforming growth factor-beta1 and interleukin-10.
Blood. 2001;98:2992–2998.
29. Richardson PG, Barlogie B, Berenson J, et al. Clinical fac-
tors predictive of outcome with bortezomib in patients
with relapsed, refractory multiple myeloma. Blood. 2005;
106:2977–2981.
30. Richardson PG, Schlossman RL, Weller E, et al. Immuno-
modulatory drug CC-5013 overcomes drug resistance and
is well tolerated in patients with relapsed multiple my-
eloma. Blood. 2002;100:3063–3067.
31. Richardson PG, Barlogie B, Berenson J, et al. A phase 2
study of bortezomib in relapsed, refractory myeloma. N
Engl J Med. 2003;348:2609–2617.
Prognostic Factors With Thalidomide Therapy/Palumbo et al. 829