Embed Size (px)
Citation preview

Timing of Dialysis Initiation in the Geriatric Population:Toward a Patient-centered Approach
Kathryn Treit,* Daniel Lam,* and Ann M. O’Hare*†*Department of Medicine, Division of Nephrology, University of Washington, Seattle, Washington, and †VAPuget Sound Healthcare System, Seattle, Washington
ABSTRACT
Over the last 10–15 years, the incidence of treated end-stage renal disease (ESRD) among older adults hasincreased and dialysis is being initiated at progressivelyhigher levels of estimated glomerular filtration rate(eGFR). Average life expectancy after dialysis initiationamong older adults is quite limited, and many experiencean escalation of care and loss of independence after start-ing dialysis. Available data suggest that treatment deci-sions about dialysis initiation in older adults in the UnitedStates are guided more by system- than by patient-levelfactors. Stronger efforts are thus needed to ensure thattreatment decisions for older adults with advanced kidneydisease are optimally aligned with their goals and prefer-ences. There is growing interest in more conservativeapproaches to the management of advanced kidney diseasein older patients who prefer not to initiate dialysis andthose for whom the harms of dialysis are expected to out-weigh the benefits. A number of small single center studies,mostly from the United Kingdom report similar survival
among the subset of older adults with a high burden ofcomorbidity treated with dialysis vs. those managed con-servatively. However, the incidence of treated ESRD inolder US adults is several-fold higher than in the UnitedKingdom, despite a similar prevalence of chronic kidneydisease, suggesting large differences in the social, cultural,and economic context in which dialysis treatment decisionsunfold. Thus, efforts may be needed to adapt conservativecare models developed outside the United States to opti-mally meet the needs of US patients. More flexibleapproaches toward dialysis prescription and better integra-tion of treatment decisions about conservative care withthose related to modality selection will likely be helpful inmeeting the needs of individual patients. Regardless of thechosen treatment strategy, time can often be a critical allyin centering care on what matters most to the patient, anda flexible and iterative approach of re-evaluation andredirection may often be needed to ensure that treatmentstrategies are fully aligned with patient priorities.
Over the last decade, there has been an increaseboth in the number of older adults initiating chronicdialysis and in the level of estimated glomerularfiltration rate (eGFR) at which dialysis is initiated(1,2). This trend may translate into meaningfuldifferences in the timing of dialysis initiationbecause loss of eGFR is often slow in older adultswith advanced kidney disease (2). Life expectancyafter initiation of dialysis in older adults may bequite limited, and kidney transplant is not an optionfor most (1,3). Thus, for many older adults, deci-sions about whether and when to initiate dialysisoften have broader implications on how they willspend the final phase of their lives.
A recent study from Alberta, Canada found thatolder adults were much more likely than their youn-ger counterparts to develop untreated end-stagerenal disease (ESRD), which the authors defined as
a sustained eGFR<15 ml/minute/1.73 m2 in apatient who did not initiate dialysis (4). At olderages, the number of patients with untreated ESRDgreatly exceeded the number treated with dialysis,suggesting that the burden of advanced kidneydisease among older adults may be more substantialthan previously realized, and that there may be arelatively large “reservoir” of older adults with verylow levels of eGFR who do not receive chronicdialysis. The data sources for this project wereinsufficiently granular to determine whether patientswith a sustained eGFR<15 ml/minute/1.73 m2 whowere not treated with dialysis had indications fordialysis and either were not offered or chose not toreceive dialysis, or whether these patients did notdevelop clinical indications for initiation of dialysisduring follow-up. Nevertheless, the results of thisstudy are consistent with a growing number of smallsingle-center studies in Europe and Australia,suggesting that a substantial number of older adultswith advanced kidney disease are managedconservatively (5–11).Several lines of indirect evidence suggest that in
the United States also, not all older adults withadvanced kidney disease initiate dialysis. Registry
Author correspondence to: Ann M. O’Hare, MA MD, 1660South Columbian Way, Seattle, WA 98108, Tel.: (206) 277-3192, Fax: (206) 764-2022, or e-mail [email protected].
Seminars in Dialysis—2013DOI: 10.1111/sdi.12131© 2013 Wiley Periodicals, Inc.
1
TRANSITION TO DIALYSIS:CONTROVERSIES IN ITS TIMING AND MODALITY

data show that the crude incidence of treated ESRDplateaus and then declines in the very elderly,despite a linear increase in the overall prevalence ofCKD with increasing age (1). Similar patterns havebeen reported for the incidence of acute kidneyinjury treated with dialysis among hospitalizedpatients (12). There is also marked regional varia-tion in the incidence of treated ESRD in olderadults, with the highest incidence observed inhospital referral regions with the highest levels ofMedicare spending for beneficiaries in their final6 months of life (13).
Available data seem to suggest that patient goalsand preferences probably play only a limited role inshaping decisions about dialysis initiation in theUnited States. Qualitative work in outpatientnephrology clinics suggests that dialysis is oftenpresented more as a “necessity” than as a truetreatment “choice” and patients may be left feelingthat they have little choice but to prepare for andultimately initiate dialysis (14). Trends in eGFR atinitiation and in the incidence of treated ESRD alsosupport the possibility that dialysis initiationpractices are shaped more by societal and healthsystem factors than by individual patient character-istics. For example, an upward trend in eGFR atinitiation seems to have occurred across all patientgroups, irrespective of differences in prognosis afterinitiation (2,15). If anything, differences in timing ofinitiation and regional differences in the incidenceof ESRD seem to be most pronounced in the veryelderly—a group for whom there may be the great-est degree of uncertainty about the benefits ofchronic dialysis (1,2,13).
Disease-based Vs. Patient-CenteredApproach to Dialysis Initiation
Traditional approaches to dialysis initiation basedon level of renal function and the presence of classicclinical indications provide an example of a disease-based approach to care (16). Disease-based modelsof care assume a direct connection between underly-ing pathophysiologic processes and observed signsand symptoms and clinical outcomes (17). However,in older patients with complex comorbidities, theremay be a less direct connection between underlyingdisease processes, observed signs and symptoms,and the effects of treatments targeted at underlyingpathophysiologic processes. Often there can be atension between what would be recommended undera disease-based approach and what matters most tothe individual patient. Treatments targeted at theunderlying disease process may do little to addressthe symptoms that are most bothersome to thepatient if these do not result directly from thisprocess. For this reason, a more individualizedpatient-centered approach is often favored incomplex older patients (17). Under this approach,interventions are targeted at modifiable processes
that matter most to the patient, and signs andsymptoms are recognized as potential treatmenttargets in and of their own right, even if they donot result from a single underlying disease process.A common challenge in older adults with
advanced kidney disease lies in disentangling thosesymptoms that are due to the patient’s underlyingkidney disease and those that are due to otherdisease processes, perhaps in concert with theirunderlying kidney disease. Many of the signs andsymptoms of advanced kidney disease are relativelynonspecific, especially in older adults with othercomorbid conditions that may cause similarsymptoms. This often leads to uncertainty aboutwhether and to what degree a particular symptomor constellation of symptoms will improve withdialysis initiation and whether dialysis is the optimalapproach for addressing those symptoms inindividual patients.
Available Evidence to Guide Timing ofDialysis Initiation
Available trial data seem to suggest that it is safeto delay dialysis initiation until the development ofsigns and symptoms of advanced kidney disease,but provide little guidance on the comparativeeffectiveness of dialysis and more conservativeapproaches in symptomatic patients (18,19). Partici-pants in the Diet and Dialysis trial were 70 years ofage or older with an eGFR 5–7 ml/minute and wererandomized to receive a very low protein diet vs.dialysis (18). There was an approximately 9-monthdifference in median time to dialysis initiationbetween trial arms. Mortality was similar in botharms, and rates of hospitalization were lower in thediet arm. However, patients with signs andsymptoms of uremia were excluded from this trial,as were those with diabetes.Participants in the Initiating Dialysis Early and
Late (IDEAL) trial were randomized to initiatedialysis at an eGFR of 10–14 (“early start”) vs. 5–7 ml/minute/1.73 m2 (“late start”) (19). The “latestart” patients were followed monthly in nephrologyclinic. On average, patients randomized to the “latestart” arm initiated dialysis nearly 6 months laterthan those randomized to the “early start” arm.However, the vast majority of patients randomizedto the “late start” arm initiated dialysis beforereaching the target eGFR, in most instances due tothe development of “uremic symptoms” or “physi-cian preference.” There were no differences betweenarms in a wide range of clinical outcomes, and thiswas true both for older and younger patients, aswell as all sub-groups examined.Thus, the IDEAL trial seems to support the
safety of delaying dialysis initiation until thedevelopment of uremic signs and symptoms inpatients followed closely by a nephrologist.However, neither of these trials provided evidence
2

to guide decision making in older adults with signsand symptoms of advanced kidney disease or aboutthe impact of dialysis initiation vs. more conserva-tive approaches on symptom management and otheroutcomes (20).
Conservative Treatment Strategies
Patients with chronic kidney disease as well asthose receiving dialysis often have a high symptomburden. Although uremic symptoms are consideredindications for dialysis and we often assume thatthese symptoms will improve after dialysis initia-tion, very little is known about the impact of dialy-sis on symptom control (21). Murtagh andcolleagues found that the symptom burden inpatients with stage V CKD managed conservativelywas very similar to that reported for patients receiv-ing chronic dialysis (22). Over the last 5 years, therehas been growing interest in positive alternatives todialysis that focus on managing the signs and symp-toms of advanced kidney disease without initiatingdialysis. In several countries, formal conservative orsupportive care pathways have been developed toaccommodate patients who choose not to receivedialysis or for whom dialysis is not recommended.A recent observational study in Australia evaluatedpatients who chose conservative therapy over dialy-sis and found that one in seven patients with stageV CKD did not plan to initiate dialysis (23).
In recent years, several observational studieshave compared survival and other outcomes amongpatients managed conservatively vs. those treatedwith dialysis. Most studies were conducted at singlecenters and none has been conducted within theUnited States, with the majority taking place in theUnited Kingdom (Table 1). In general, patientstreated conservatively tend to be older, but notnecessarily sicker as defined by comorbidity scores.In general, patients treated with dialysis survivedlonger than those treated conservatively. However,in several studies, older patients with a high burdenof comorbidity experienced similar survivalregardless of treatment strategy (7,24). In addition,compared with patients treated with dialysis, thosemanaged conservatively spend significantly less timein hospitalized settings and they are more likely todie at home (25). Outcomes such as time spent in amedical setting, time spent traveling to and fromdialysis and life expectancy have been identified asimportant considerations by patients making thedecision to undergo dialysis vs. conservativetherapy (23).
The National Service Framework for Renal Ser-vices in the United Kingdom identifies several keyelements of conservative care described in Table 2(26). However, there appear to be some differencesin how conservative care programs are implementedat each center. At Lister Hospital, Smith and DaSilva Gane described a multidisciplinary group that
meets to develop a treatment recommendation forrenal replacement therapy or conservative manage-ment (7). This recommendation is presented to thepatient who provides his/her input and a treatmentplan is then agreed upon. If a patient choosesconservative care, he/she continues to be followedin the renal clinic for ongoing medical care and sup-port. The degree to which patients are free to movebetween treatment strategies is not explicitlydescribed, but there is an emphasis on the dynamicnature of this program to ensure that patient goalsare periodically re-evaluated (26).Burns and Davenport describe a similar approach
at the Royal Free Hospital in London, includinghome visits by a renal social worker or counselor toensure that patients opting for conservative manage-ment understand the nature of their decision(27,28). Conservatively managed patients in thisprogram were offered ongoing specialist support inclinic and hospitalization as needed. Patientsfollowed in clinic continued to receive maximalmedical management including erythropoietin foranemia and medications to optimize blood pressureand cholesterol as needed. Interventions to optimizecalcium and phosphorus are primarily titrated tocontrol symptoms such as pruritis rather than toattain traditional guideline-based targets. Dietaryinterventions are limited to control of potassiumand general dietary support. End-of-life care includ-ing access to hospice and palliative care is discussedwith all patients who chose not to receive dialysis,and referrals made based on patient preferences.Murtagh described outcomes among patients
aged 75 and older managed at four major renalunits in the South Thames Region in the UnitedKingdom (9). Patients expected to need dialysiswithin 18 months were referred to a dedicatedmultidisciplinary predialysis care team of physicians,specialist nurses, counselors, and dieticians. Thefinal decision about dialysis was made jointlybetween the patient and their nephrologist based onthe patient’s wishes and suitability for dialysis. Thedecision for or against dialysis was based on theanticipated benefit/burden of receiving dialysis, withparticular consideration of quality of life and sur-vival. It is not always clear in published reports ofobservational studies comparing outcomes amongpatients treated with dialysis vs. those managedconservatively, whether and how often treatmentdecisions are re-evaluated with the development ofnew health events or changing preferences, theapproach taken to ensure that treatment decisionsreflect patient preferences vs. provider recommenda-tions, and the extent to which discussions aboutconservative management were integrated intobroader discussions about treatment modality(Table 1).Large differences in survival between patients
receiving conservative care across different studiessuggest that there may be differences in the selec-tion process and how conservative care is
3

TABLE
1.Studiescomparingsurvivalbetweenconservative
care
andrenalreplacementtherapy
Study
Study
design
Studypopulation
(n=subject
#)
Age
Location
Conservativecare
model
components
Outcome
Chandna
etal.(11)
Retrospective
survival
analysis
CM:n=155
RRT:n=689
CM
meanage=
77.5
RRTmeanage58.5.
UK
1.Ongoingsupport
bymultidisciplinary
team
2.Liaisonwithcommunity,primary
care,hospice
3.fullmedicaltreatm
entcontinued
includingEPO
1.Mediansurvivalwas67monthsin
RRT
comparedto
21monthsin
CM.
2.Survivalin
age>75andlow
comorbidities36.8
comparedto
29.4
monthswithCM.High
comorbidities.
3.When
correctedforgender,ageDM,andhigh
comorbidities,nosurvivaladvantage
Murtagh
etal.(9)
Retrospective
Survival
Analysis
CM:n=
77
RRT:n=52
CM
75–7
9years
=15%
RRT75–79years
=46%
CM
80–8
4years
=47%
RRT80–84years
=44%
CM
85–8
9years
=31%
RRT85–89years
=10%
CM
>89years
=7%
RRT>89years
=0%
UK
1.Noclearconservativecare
model
described
2.PredialysisMultidisciplinary
team
forall
patients
enrolled—
physician,nursespecialist,
dieticians,counselor,socialandpsychological
support—
increaseddecision-m
akingsupport
comparedwithusualcare
1.One-yearsurvivalof84%
inRRTcomparedto
68%
inCM.
2.Two-yearsurvivalof76%
inRRTvs47%
inCM.
3.Nodifference
betweenpts
withhigh
comorbidities.
4.Nodifference
inthose
withischem
icheart
disease
Carson
etal.(28)
Prospective
cohort
study
CM:n=29
RRT:n=173
CM
medianage=81.6
RRTmedianage=76.4
UK
1.Allpatients
received
care
from
multidisciplinary
team
2.Conservativemanagem
entreceived
one
homevisitbysocialwork
3.Allpatients
offered
ongoingspecialtycare
4.Anem
iaandcholesteroltreatedin
both
5.Ca/Phosmanagem
entwassymptomaticonly
inCM
group
6.End-of-life
planningincludinghospice/home
palliativecare
discussed
1.CM
survivalmedian=13.9
months
RRTmediansurvival=37.8
months
2.Hospitalizationsin
CM
16days/patient/year
RRThospitalizations25days/patient/year
Smith(7)
Prospective
Cohort
Study
CM:n=63
RRTn=258
Allpatients
meanage=61.5
CM
meanage=71
RRTmeanage=59
UK
Model
ofMultidisplinary
team
inpredialysis
1.Followed
byliaisonteam
withseniornurse,
counselor,socialworker
2.Team
Rolesincluded:education,assessm
ent
ofptunderstandingofillnessandconsequences,
functionalstatus,socialsupport,needsand
expectations
3.M
ultidisciplinary
team
meets
withphysician
andmakes
recommendationfordialysisorCM
4.Those
pursuingCM
received
support
by
multidisciplinary
team
andhospice.
5.Fullmedicaltreatm
entincludingEPO
was
continued
1.palliativeRRTgroupsurivial=8.6
months
2.Palliativenondialysissurvivalof6.3
months
3.80%
ofRRTpatients
stillaliveat5years
Joly
(6)
Prospective
Cohort
Study
CM:n=37
RRT:n=107
CM
meanage=84.1
RRTmeanage=83.2
France
1.Multidisciplinary
team
madedecision
regardingconservativecare
2.Ultrafiltrationwasallowed
forfluid
managem
entifnecessary
3.Focusonpsychologic,social,andspiritual
concerns
4.Comanagem
entwithfamilyphysician
1.MediansurvivalRRTgroup=28.9
months
2.Two-yearsurvivalwas60%
inRRTgroupvs
15%
inconservativemanagem
ent
3.Mediansurvivalconservativemanagem
ent=
8.9
months
Seow
(29)
Prospective
Cohort
Study
CM:n=63
RRT:n=38
CM
meanage=78
RRTmeanage=71
Singapore
Nodescription
available
1.Two-yearsurvivalof86.8%
inRRTgroup
vs.38.1%
inconservativemanagem
ent
2.RRTdid
notim
provephysical
componentscore
orkidney-specificsymptoms
CM:conservativemanagem
ent;RRT:renalreplacementtherapy.
4

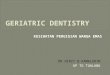
operationalized across centers. Without a detailedunderstanding of how conservative care modelsare operationalized in the clinical setting, it is dif-ficult to know how acceptable this approachwould be to US patients and providers. Large dif-ferences in the incidence of treated ESRD betweenthe United States vs. Europe despite a similarprevalence of CKD suggest that there are largeinternational variations in treatment practices forESRD even among developed countries (29).Figure 1 compares the crude incidence of treatedESRD in the United Kingdom (where most stud-ies of conservative care have been conducted) andin the United States (30,31).
Although the crude incidence of treated ESRD ishigher in the United States than in the UnitedKingdom for all age groups, differences are espe-cially pronounced at older ages. There appears tobe an approximately 5-year difference in the age atwhich the incidence of ESRD begins to decline,with the peak ESRD incidence occurring in the 75–79 age group in the United Kingdom, as comparedwith the 80–84 age group in the United States.Common themes identified by conservatively man-aged patients in the United Kingdom as beingimportant in shaping their treatment decisioninclude an acceptance of the inevitability of death, afeeling that dialysis is more appropriate for youngerpeople, feeling well on medication, and a desire not
to be a burden or a nuisance (32). Whether thesethemes would resonate for US patients and to whatextent care models developed outside the UnitedStates would be acceptable to US patients and pro-viders is not known. Taken together, large interna-tional differences in the incidence of treated ESRDand the heterogeneity in survival across conserva-tively managed cohorts suggest that it may beimportant to explicitly consider whether and howconservative care models outside the United Statesmight need to be adapted to meet the needs of USpatients, providers, and other stakeholders.
How to Promote Patient-centered TreatmentDecisions for Older Adults with Advanced
Kidney Disease
Given the very limited life expectancy of manyolder adults with advanced kidney disease and thedearth of available evidence to support decisionsabout whether and when to initiate dialysis in olderadults with symptomatic advanced kidney disease inthe United States, it is especially important thatpatients and their families play a central role inshaping these decisions. Shared decision makingrefers to a process for making medical decisionsthat includes both patient preferences and physicianexperience and expertise (33), and is foundational to
0.0
200.0
400.0
600.0
800.0
1000.0
1200.0
1400.0
1600.0
1800.0
20-29 30-39 40-49 50-59 60-64 65-69 70-74 75-79 80-84 85+
Inci
denc
e pe
r M
illio
n
Age Group
US
England
Fig 1. Crude incidence of ESRD in the United Kingdom vs. United States, 2008. Sources: USRDS Annual Data Report; UK Renal
Registry (30,31).
TABLE 2. Key elements of conservative care
Access to a multiskilled renal team with expertise in communication, shared decision making, and symptom managementPrognostic assessmentTimely information about the choices available to them and a palliative care planOngoing medical treatmentDignity in death, and where possible to die in their preferred place of careCulturally appropriate bereavement support
5

patient-centered models of care (34,35). The RenalPhysicians Association has recommended the use ofthe shared decision-making model to support deci-sions about dialysis initiation and discontinuation(36,37), and the importance of shared decision mak-ing around dialysis initiation has been highlightedin the American Board of Internal Medicine’sChoosing Wisely campaign (38).
Although a high proportion of patients reportwanting to be actively involved in their medicaldecisions, the clinical adoption of shared decisionmaking has been disappointing (39). Barriers toshared decision making cited by physicians includetime constraints, a belief that shared decisionmaking is not applicable to particular clinical situa-tions, and that patients do not favor shared deci-sion-making models (40). An additional barrier toshared decision making may be the patient’s readi-ness to participate in this process. Patients may bereluctant to discuss the severity of their illness andthe difficult decisions that lie ahead. Asking permis-sion to discuss prognosis and treatment preferencesmay be a useful way to gauge patient readiness toenter into these discussions, and for preparingpatients for future discussions (41).
A realistic understanding of life expectancy andfuture illness trajectory is often critical in support-ing treatment decisions in patients with advancedkidney disease. There is substantial heterogeneity inlife expectancy and illness trajectories amongpatients of similar ages with similar levels of renalfunction (1). Several prognostic models have beendeveloped for patients receiving chronic dialysis.The surprise question: ‘Would I be surprised if thispatient died in the next year’ was strongly associ-ated with observed survival among patients receiv-ing chronic dialysis (42). The surprise question hasalso been incorporated into a prediction model thatincludes older age, dementia, peripheral vasculardisease, and low albumin (43). It is not knownwhether this question has similar prognosticaccuracy in patients not yet receiving dialysis.
In addition to life expectancy, patients often wantto know about the expected course of their illness.Prior studies in older adults have described substan-tial heterogeneity in functional trajectories aspatients approach death (44). Disability in the lastyear of life remains highly unpredictable and mayoften not be correlated with underlying disease pro-cesses (45). Murtagh and colleagues described pat-terns of functional status, as defined by theKarnofsky Performance Scale, among 75 elderlypatients with stage V CKD who chose conservativetherapy (24,44). The dominant pattern of functionaldecline most closely resembled the pattern of a ter-minal illness described by Lunney et al., with arapid decline in functional status in the last monthof life (44). Less is known about patterns of func-tional decline after dialysis initiation and towardthe end of life among older adults receiving chronicdialysis, and how dialysis initiation might beexpected to modify illness trajectories. Among a
national cohort of nursing home residents initiatingchronic dialysis, there was a sharp decline in func-tional status immediately following dialysis initia-tion, followed by a slower sustained decline. Evenamong community dwelling older adults, most expe-rienced some loss of independence during the yearafter dialysis initiation (46). However, the degree ofheterogeneity in functional trajectories after dialysisinitiation among older adults with advanced kidneydisease has not been described.Nephrologists often struggle to effectively com-
municate the complexities of chronic kidney diseasewith patients and their families (47). Not all treat-ment options will be relevant, realistic, or possiblefor each patient; thus, it is important to tailor dis-cussions about treatment options to the realities ofthe patient’s situation, prognosis, and illness trajec-tory (48). In addition, treatment decisions mustoften be dynamic to accommodate changes in signsand symptoms, clinical situation, priorities, andpreferences that may occur during each patient’sillness trajectory (49–51).A discrete choice experiment by Morton and col-
leagues suggests that pragmatic details may often beimportant in shaping treatment choices foradvanced kidney disease (52). These authors foundthat practical considerations related to dialysistreatment such as number of visits per week,whether there would be travel restrictions, time ofday of dialysis treatments, and the availability ofsubsidized transport influenced whether patientsfavored dialysis over a more conservative approach,with some patients being willing to accept a shorterlife expectancy to prioritize other goals such asbeing able to travel without restrictions. Currentlyavailable data do not provide guidance regarding a“better” dialysis option for elderly patients, butpatient preferences and assessment of feasibility ofhome modalities should be addressed.In addition to providing patients with informa-
tion on a range of relevant treatment options, amore flexible approach to prescribing dialysis mightalso be useful in promoting a more patient-centeredapproach to care for older adults with advancedkidney disease—perhaps moving away from conven-tional dialysis prescriptions that emphasize metricsthat address the underlying disease process (e.g.,dialysis adequacy and control of laboratory values)in favor of those that best support individualpatient priorities (e.g., symptom management, timeat home, independence).In part because of the high degree of uncertainty
that often surrounds treatment decisions forpatients with advanced kidney disease, time canoften be a great ally in centering care on whatmatters most to the patient (53). Regardless of thechosen treatment strategy, a flexible approach ofre-evaluation and redirection and ongoing commu-nication is often needed to ensure that treatmentstrategies are fully aligned with patient priorities. Inmany instances, neither patients nor clinicians maybe certain about whether a given sign or symptom
6

will be best addressed by initiating dialysis vs. amore conservative approach or about what theexperience of dialysis treatment will be like for indi-vidual patients. A trial approach with subsequentre-evaluation can often be helpful in clarifying thebenefits vs. burdens of different treatment strategiesfor individual patients.
It is also important to keep in mind that the bal-ance of benefits and harms associated with dialysisis often a moving target that may change over time,particularly after key health and life events. In thisrespect, many treatment decisions do not occur at adiscrete point in time, but are better characterizedas a “process” that unfolds over time. While chang-ing goals of care may frustrate some physicians, byits nature, addressing what matters most to thepatient must often be a dynamic process to capturechanging circumstances, evolving experience ofillness, and changing priorities (49,54).
Conclusion
For older adults with advanced kidney disease,life expectancy is often quite limited. Many of thosewho initiate dialysis can expect to spend a greaterproportion of their remaining lifetime in a health-care setting and may not regain their previousfunctional status (25,46). Relatively little is knownabout treatment practices for advanced kidney dis-ease in the United States, and how frequentlypatients with this condition choose not to receivedialysis or are not offered this therapy. Availabletrial evidence does not provide guidance on theoptimal timing of dialysis initiation in older adultswith symptomatic advanced kidney disease. Thegeneralizability of study results and acceptability ofconservative care models developed outside theUnited States to patients and providers within theUnited States has not been evaluated.
Given the very limited life expectancy of manyelderly patients with advanced kidney disease, thepaucity of high-quality evidence to guide clinical deci-sion making, and the intensive nature of dialysistreatment, it is especially important that patients andtheir families play a central role in shaping treatmentdecisions. While some patients may prefer not toreceive dialysis regardless of how their illness unfolds,other patients may wish to delay dialysis for as longas possible, initiating dialysis only when symptomsbecome intolerable and cannot be adequately man-aged without dialysis. Other patients may wish tobegin dialysis, but may benefit from an individualizeddialysis prescription tailored to meet their own treat-ment goals. For some patients, the substantial differ-ences between different models of dialysis care (e.g.,peritoneal dialysis, vs. home hemodialysis vs. centerhemodialysis) and the practical realities of thesetreatment options may critically shape decisionsabout whether a patient chooses to receive dialysisvs. pursue a more conservative approach.
A more complete understanding of the acceptabil-ity of conservative care models developed outsidethe United States to older adults with advanced kid-ney disease in the United States will be helpful indeveloping strong positive alternatives to dialysis inthis country and supporting a more flexibleapproach to the care of older adults with advancedkidney disease. A trial approach to chosen treat-ment strategies may help patients to develop a dee-per more personal understanding of the balancebetween benefits and harms and the acceptability ofa given treatment option (including but not limitedto dialysis), with iterative re-evaluation and redirec-tion as needed to meet individual patient goals.Time can be a critical ally in understanding patientgoals and the benefits and burdens of differenttreatment strategies for individual patients thatshould be fully leveraged in efforts to optimize carefor older adults with advanced kidney disease.
References
1. Kurella M, Covinsky KE, Collins AJ, Chertow GM: Octogenariansand nonagenarians starting dialysis in the United States. Ann InternMed 146(3):177–183, 2007
2. O’Hare AM, Choi AI, Boscardin WJ, Clinton WL, Zawadzki I, He-bert PL, Kurella Tamura M, Taylor L, Larson EB: Trends in timingof initiation of chronic dialysis in the United States. Arch Intern Med171(18):1663–1669, 2011
3. Wachterman MW, Marcantonio ER, Davis RB, Cohen RA, WaikarSS, Phillips RS, McCarthy EP: Relationship between the prognosticexpectations of seriously ill patients undergoing hemodialysis and theirnephrologists. JAMA Intern Med 173(13):1206–1214, 2013
4. Hemmelgarn BR, James MT, Manns BJ, O’Hare AM, Muntner P,Ravani P, Quinn RR, Turin TC, Tan Z, Tonelli M: Rates of treatedand untreated kidney failure in older vs younger adults. JAMA 307(23):2507–2515, 2012
5. Ellam T, El-Kossi M, Prasanth KC, El-Nahas M, Khwaja A:Conservatively managed patients with stage 5 chronic kidney disease–outcomes from a single center experience. QJM 102(8):547–554, 2009
6. Joly D, Anglicheau D, Alberti C, Nguyen AT, Touam M, GrunfeldJP, Jungers P: Octogenarians reaching end-stage renal disease: cohortstudy of decision making and clinical outcomes. J Am Soc Nephrol 14(4):1012–1021, 2003
7. Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R,Farrington K: Choosing not to dialyse: evaluation of planned non-dialytic management in a cohort of patients with end-stage renal fail-ure. Nephron Clin Pract 95(2):c40–c46, 2003
8. Wong CF, McCarthy M, Howse ML, Williams PS: Factors affectingsurvival in advanced chronic kidney disease patients who choose notto receive dialysis. Ren Fail 29(6):653–659, 2007
9. Murtagh FE, Marsh JE, Donohoe P, Ekbal NJ, Sheerin NS, HarrisFE: Dialysis or not? A comparative survival study of patients over75 years with chronic kidney disease stage 5. Nephrol Dial Transplant22(7):1955–1962, 2007
10. Hirsch DJ, West ML, Cohen AD, Jindal KK: Experience with notoffering dialysis to patients with a poor prognosis. Am J Kidney Dis23(3):463–466, 1994
11. Chandna SM, Da Silva-Gane M, Marshall C, Warwicker P, Green-wood RN, Farrington K: Survival of elderly patients with stage 5CKD: comparison of conservative management and renal replacementtherapy. Nephrol Dial Transplant 26:1608–1614, 2011
12. Hsu CY, McCulloch CE, Fan D, Ordonez JD, Chertow GM, Go AS:Community-based incidence of acute renal failure. Kidney Int 72(2):208–212, 2007
13. O’Hare AM, Rodriguez RA, Hailpern SM, Larson EB, Kurella TamuraM: Regional variation in health care intensity and treatment practicesfor end-stage renal disease in older adults. JAMA, 304(2):180–186, 2010
14. Kaufman SR, Shim JK, Russ AJ: Old age, life extension, and thecharacter of medical choice. J Gerontol B Psychol Sci Soc Sci 61(4):S175–S184, 2006
15. Molnar MZ, Ojo AO, Bunnapradist S, Kovesdy CP, Kalantar-ZadehK: Timing of dialysis initiation in transplant-naive and failed trans-plant patients. Nat Rev Nephrol 8(5):284–292, 2012
7

16. Bowling CB, O’Hare AM: Managing older adults with CKD: individ-ualized versus disease-based approaches. Am J Kidney Dis 59(2):293–302, 2012
17. Tinetti ME, Fried T: The end of the disease era. Am J Med 116(3):179–185, 2004
18. Brunori G: Treatment of chronic kidney disease in the elderly: diet orconservative management. J Nephrol 25(19):S28–S31, 2012
19. Cooper BA, Branley P, Bulfone L, Collins JF, Craig JC, FraenkelMB, Harris A, Johnson DW, Kesselhut J, Li JJ, et al.: A randomized,controlled trial of early versus late initiation of dialysis. N Engl J Med363(7):609–619, 2010
20. Abra G, Kurella Tamura M: Timing of initiation of dialysis: timefor a new direction? Curr Opin Nephrol Hypertens 21(3):329–333,2012
21. Abdel-Kader K, Unruh ML, Weisbord SD: Symptom burden, depres-sion, and quality of life in chronic and end-stage kidney disease. ClinJ Am Soc Nephrol 4(6):1057–1064, 2009
22. Murtagh FE, Addington-Hall JM, Edmonds PM, Donohoe P, CareyI, Jenkins K, Higginson IJ: Symptoms in advanced renal disease: across-sectional survey of symptom prevalence in stage 5 chronic kid-ney disease managed without dialysis. J Palliat Med 10(6):1266–1276,2007
23. Morton RL, Snelling P, Webster AC, Rose J, Masterson R, JohnsonDW, Howard K: Factors influencing patient choice of dialysis versusconservative care to treat end-stage kidney disease. CMAJ 184:E277–E283, 2012
24. Murtagh FE, Marsh JE, Donohoe P, Ekbal NJ, Sheerin NS, HarrisFE: Dialysis or not? A comparative survival study of patients over75 years with chronic kidney disease stage 5. Nephrol Dial Transplant22:1955–1962, 2007
25. Carson RC, Juszczak M, Davenport A, Burns A: Is maximum conser-vative management an equivalent treatment option to dialysis forelderly patients with significant comorbid disease? Clin J Am SocNephrol 4:1611–1619, 2009
26. Da Silva-Gane M: Supportive Care for the Renal Patient, 2nd edn.Oxford University Press; 2010
27. Burns A, Davenport A: Maximum conservative management forpatients with chronic kidney disease stage 5. Hemodial Int 14(Suppl 1):S32–S37, 2010
28. Carson RC, Juszczak M, Davenport A, Burns A: Is maximum conser-vative management an equivalent treatment option to dialysis forelderly patients with significant comorbid disease? Clin J Am SocNephrol 4(10):1611–1619, 2009
29. Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S,Hallan HA, Lydersen S, Holmen J: International comparison of therelationship of chronic kidney disease prevalence and ESRD risk.J Am Soc Nephrol 17(8):2275–2284, 2006
30. United States Renal Data System Annual Data Report ReferenceTables: Incidence. Available at http://www.usrds.org, accessed June2013
31. Byrne C, Ford D, Gilg J, Ansell D, Feehally J: UK Renal Registry12th Annual Report (December 2009): chapter 3: UK ESRD incidentrates in 2008: national and centre-specific analyses. Nephron Clin Pract115(Suppl 1):c9–c39, 2010
32. Johnston S, Noble H: Factors influencing patients with stage 5 chronickidney disease to opt for conservative management: a practitionerresearch study. J Clin Nurs 21(9–10):1215–1222, 2012
33. Towle A, Godolphin W: Framework for teaching and learninginformed shared decision making. BMJ 319(7212):766–771, 1999
34. Weston WW: Informed and shared decision-making: the crux ofpatient-centered care. CMAJ 165(4):438–439, 2001
35. Makoul G, Clayman ML: An integrative model of shared decisionmaking in medical encounters. Patient Educ Couns 60(3):301–312, 2006
36. Association RP: Shared Decision-Making in the Appropriate Initiationof and Withdrawal from Dialysis: Clinical Practice Guidelines. Mary-land: Rockville, 2010
37. Moss AH: Shared decision-making in dialysis: the new RPA/ASNguideline on appropriate initiation and withdrawal of treatment. Am JKidney Dis 37(5):1081–1091, 2001
38. Williams AW, Dwyer AC, Eddy AA, Fink JC, Jaber BL, Linas SL,Michael B, O’Hare AM, Schaefer HM, Shaffer RN, et al.: Criticaland honest conversations: the evidence behind the “Choosing Wisely”campaign recommendations by the American Society of Nephrology.Clin J Am Soc Nephrol 7(10):1664–1672, 2012
39. Kiesler DJ, Auerbach SM: Optimal matches of patient preferences forinformation, decision-making and interpersonal behavior: evidence,models and interventions. Patient Educ Couns 61(3):319–341, 2006
40. L�egar�e F, Witteman HO: Shared decision making: examining key ele-ments and barriers to adoption into routine clinical practice. HealthAff (Millwood) 32(2):276–284, 2013
41. Schell JO, Arnold RM: Nephrotalk: communication tools to enhancepatient-centered care. Semin Dial 25(6):611–616, 2012
42. Moss AH, Ganjoo J, Sharma S, Gansor J, Senft S, Weaner B, DaltonC, MacKay K, Pellegrino B, Anantharaman P, et al.: Utility of the“surprise” question to identify dialysis patients with high mortality.Clin J Am Soc Nephrol 3(5):1379–1384, 2008
43. Cohen LM, Ruthazer R, Moss AH, Germain MJ: Predicting six-month mortality for patients who are on maintenance hemodialysis.Clin J Am Soc Nephrol 5(1):72–79, 2010
44. Lunney JR, Lynn J, Foley DJ, Lipson S, Guralnik JM: Patterns offunctional decline at the end of life. JAMA 289(18):2387–2392, 2003
45. Gill TM, Gahbauer EA, Han L, Allore HG: Trajectories of disabilityin the last year of life. N Engl J Med 362(13):1173–1180, 2010
46. Kurella Tamura M, Covinsky KE, Chertow GM, Yaffe K, LandefeldCS, McCulloch CE: Functional status of elderly adults before andafter initiation of dialysis. N Engl J Med, 361(16):1539–1547, 2009
47. Schell JO, Green JA, Tulsky JA, Arnold RM: Communication skillstraining for dialysis decision-making and end-of-life care in nephrol-ogy. Clin J Am Soc Nephrol 8(4):675–680, 2013
48. Lamas D, Rosenbaum L: Freedom from the tyranny of choice–teachingthe end-of-life conversation. N Engl J Med 366(18):1655–1657, 2012
49. Schell JO, O’Hare AM: Illness trajectories and their relevance to thecare of adults with kidney disease. Curr Opin Nephrol HypertensMarch 20, 2013 [Epub ahead of print]
50. Rosansky SJ: Renal function trajectory is more important thanchronic kidney disease stage for managing patients with chronic kid-ney disease. Am J Nephrol 36(1):1–10, 2012
51. Schell JO, Patel UD, Steinhauser KE, Ammarell N, Tulsky JA: Dis-cussions of the kidney disease trajectory by elderly patients and neph-rologists: a qualitative study. Am J Kidney Dis 59(4):495–503, 2012
52. Morton RL, Snelling P, Webster AC, Rose J, Masterson R, JohnsonDW, Howard K: Factors influencing patient choice of dialysis versusconservative care to treat end-stage kidney disease. CMAJ 184(5):E277–E283, 2012
53. Sweet V: God’s Hotel: A Doctor, a Hospital, and a Pilgrimage to theHeart of Medicine. New York: Riverhead Books, 2012
54. Russ AJ, Kaufman SR: Discernment rather than decision-makingamong elderly dialysis patients. Semin Dial 25(1):31–32, 2012
8