Embed Size (px)
Citation preview

3/27/2019
1/14
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e
Chapter 232: Chapter 232: Tests of HemostasisTests of Hemostasis Stephen John Cico; Robin R. Hemphill
THE BLEEDING PATIENTTHE BLEEDING PATIENT
Most bleeding seen in the ED is a result of trauma—local wounds, lacerations, or other structural lesions—and the
majority of traumatic bleeding occurs in patients with normal hemostatic mechanisms.1 In these patients, specificassessment of hemostasis is unnecessary. However, some ED patients have abnormal bleeding due to impaired
hemostasis. Identifying these patients requires attention to the history and physical findings.2,3,4 Generally speaking,when patients have spontaneous bleeding from multiple sites, bleeding from untraumatized sites, delayed bleedingseveral hours a�er trauma, and bleeding into deep tissues or joints, the possibility of a bleeding disorder should beconsidered.
Important historical data that aid in identifying a congenital bleeding disorder include the presence of unusual orabnormal bleeding in the patient and other family members and any occurrence of excessive bleeding a�er dental
extractions, surgical procedures, or trauma.5 Many patients with abnormal bleeding have an acquired disorder, suchas liver disease, renal disease, or drug use (particularly ethanol, aspirin, nonsteroidal anti-inflammatory drugs,
antiplatelet drugs, oral anticoagulants, antibiotics, and other salicylate-containing products).2,3,4 Many supplementsand herbal preparations, including garlic, ginseng, ginkgo biloba, ginger, and vitamin E, can also increase bleedingtendencies.
The site of bleeding may provide an indication of the hemostatic abnormality. Mucocutaneous bleeding, includingpetechiae, ecchymoses, epistaxis, GI or GU bleeding, or heavy menstrual bleeding, is characteristic of qualitative orquantitative platelet disorders. Purpura is o�en associated with thrombocytopenia and commonly indicates asystemic illness. Bleeding into joints and potential spaces, such as between fascial planes and into theretroperitoneum, and delayed bleeding are most commonly associated with coagulation factor deficiencies. Patientswho demonstrate both mucocutaneous bleeding and bleeding in deep spaces may have disorders such asdisseminated intravascular coagulation, in which both platelet abnormalities and coagulation factor abnormalitiesare present (see chapters 233, "Acquired Bleeding Disorders," 234, "Clotting Disorders," and 235, "Hemophilias andvon Willebrand's Disease").
Common laboratory tests for hemostasis have their limitations.6,7 They are generally useful and reliable foridentifying disorders of coagulation factor function and quantitative platelet availability. However, tests of qualitative
platelet function show a significant biologic variation, so that standardization has been di�icult to achieve.8,9 Inaddition, liver disease and renal failure—two conditions that increase the potential for abnormal hemorrhage—may
not give rise to consistent and measurable abnormal results on routine tests of hemostasis.10,11,12

3/27/2019
2/14
THE PATIENT WITH A THROMBUSTHE PATIENT WITH A THROMBUS
Presentation of a patient to the ED with a disorder due to an intravascular thrombosis, such as a deep venousthrombosis or pulmonary embolus, suggests the potential for an underlying hypercoagulable state (see chapter 234).Premature coronary artery disease and acute coronary syndrome in individuals as young as teenagers have also beenlinked to hypercoagulable conditions. However, many, if not most, occurrences of intravascular thrombosis are notdue to exaggerated hemostasis, but rather are due to local conditions, with blood vessel wall injuries, local
inflammation, or vascular stasis provoking the thromboembolic event.13,14
The susceptibility to hypercoagulation may be acquired or genetically transmitted. Common acquiredhypercoagulable disorders include essential thrombocythemia, polycythemia vera, paroxysmal nocturnalhemoglobinuria, antiphospholipid syndrome, and cancer (o�en occult at the time of acute thrombosis). Inheritedhypercoagulable disorders include factor V Leiden, prothrombin mutations, hyperhomocysteinemia, and deficienciesof protein C, protein S, and antithrombin. Patients with inherited hypercoagulable conditions tend to have venousthrombosis, whereas those with acquired disorders can have both arterial and venous clots.
Proteins C and S are vitamin K–dependent antihemostatic factors made in the liver, associated with disorders leadingto deficiencies of these proteins inherited in an autosomal manner. Protein C is activated by thrombin and functionswith protein S to stop fibrin formation and to stimulate the process of fibrinolysis. Antithrombin is also anantihemostatic protein that blocks activated coagulation factors. Elevated homocysteine level is also a known riskfactor for thromboembolism.
Laboratory tests for a hypercoagulable diathesis show wide biologic variation, and standardization amonglaboratories has been di�icult to achieve. The clinical utility of testing patients for suspected hypercoagulable
conditions is dependent on the specific disorder.13,14,15
NORMAL COAGULATIONNORMAL COAGULATION
The normal hemostatic system consists of a complex process that limits blood loss through the formation of aplatelet plug (primary hemostasis) and the production of cross-linked fibrin (secondary hemostasis), whichstrengthens the platelet plug. These reactions are counterregulated by the fibrinolytic system, which limits the size ofthe fibrin clot that is formed and thereby prevents excessive clot formation. Congenital and acquired abnormalitiesoccur in all these systems. The a�ected patient may have excessive hemorrhage, excessive thrombus formation, orboth.
PRIMARY HEMOSTASISPRIMARY HEMOSTASIS
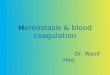
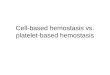
Primary hemostasis is the platelet interaction with the vascular subendothelium that results in the formation of aplatelet plug at the site of injury. Required components for this to occur are normal vascular subendothelium(collagen), functional platelets, normal von Willebrand factor (connects the platelet to the endothelium viaglycoprotein Ib), and normal fibrinogen (connects the platelets to each other via glycoprotein IIb and IIIa) (Figure 232-Figure 232-11). Primary hemostasis begins within 20 seconds of injury, is short-lived, and requires secondary hemostasis for clotstabilization.
FIGURE 232-1.FIGURE 232-1.

3/27/2019
3/14
Primary hemostasis. plt = platelet; vWF = von Willebrand factor.
SECONDARY HEMOSTASISSECONDARY HEMOSTASIS
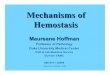
Secondary hemostasis consists of the tightly regulated reactions of the plasma coagulation proteins. The finalproduct is cross-linked fibrin, which is insoluble and strengthens the platelet plug formed in primary hemostasis(Figure 232-2Figure 232-2).
FIGURE 232-2.FIGURE 232-2.
Secondary hemostasis. Ca2+ = calcium; fibrinogen is factor I; PL = phospholipid surface (o�en platelets); prothrombinis factor II.

3/27/2019
4/14
Secondary hemostasis is also known as the coagulation cascade. The inactivated coagulation proteins (factors) areidentified by Roman numerals, and a�er activation, the activated factor is designated by a. There are twoindependent activation pathways. The contact system is known as the contact activation pathway or intrinsicpathway, and the tissue factor system is known as the tissue factor pathway or extrinsic pathway. The pathways
merge at the point of activation of factor X. Medications such as rivaroxaban (Xarelto®) and apixaban (Eliquis®) inhibitthe activity of factor Xa. The combination of factor Xa, factor Va, phospholipid, and calcium ("thrombinase complex")more e�iciently catalyzes the conversion of prothrombin to thrombin than free factor Xa. In turn, thrombin catalyzes
the conversion of fibrinogen to fibrin monomer. Medications such as bivalirudin (Angiomax®) or dabigatran (Pradaxa®)are direct thrombin inhibitors. The common pathway describes the steps from factor X activation to cross-linkedfibrin formation.
THE FIBRINOLYTIC SYSTEMTHE FIBRINOLYTIC SYSTEM
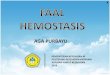
The fibrinolytic system regulates the hemostatic mechanism by limiting the size of the fibrin clots that are formed(Figure 232-3Figure 232-3). Tissue plasminogen activator (tPA), released from endothelial cells, is the principal physiologic triggerfor the fibrinolytic process, converting plasminogen, synthesized in the liver and adsorbed in the fibrin clot, to

3/27/2019
5/14
plasmin. Plasmin degrades fibrinogen and fibrin monomer into low-molecular-weight fragments known as fibrindegradation products and degrades cross-linked fibrin into d-dimers.
FIGURE 232-3.FIGURE 232-3.
The fibrinolytic system. FDP = fibrin degradation product; tPA = tissue plasminogen activator.
Other physiologic inhibitors of hemostasis with clinical relevance include antithrombin and the protein C–protein Ssystem. Antithrombin is a protein that forms complexes with all the serine protease coagulation factors (factors XIIa,XIa, Xa, IXa, and thrombin), thereby inhibiting their function. Heparin potentiates this interaction, and this is the basisfor its use as an anticoagulant. Proteins C and S are vitamin K–dependent factors that are produced in the liver.Activated protein C binds to the cell-surface-bound protein S, and this complex is capable of inactivating the twoplasma cofactors factors Va and VIIIa and inhibiting their participation in the coagulation cascade. A single amino acidsubstitution in factor V, a condition named factor V Leiden, prevents activated protein C from binding and inhibitingthe activity of factor Va. Thus, patients with this inherited condition have prolonged thrombogenic factor Va activity.Factor V Leiden, deficiency or defects in antithrombin, protein C, and protein S produce a potentially hypercoagulablecondition and predispose the patient to venous thromboses.
DIAGNOSISDIAGNOSIS
Before embarking on a sequence of hemostatic testing, evaluate the patient in three areas: (1) Is the bleedingabnormal? (2) Is there a current medical condition associated with increased hemorrhage? (3) Is there a structural
cause that explains the bleeding?13,14,15,16,17
The basic laboratory tests obtained for a patient with a suspected abnormal bleeding disorder are a CBC and plateletcount, prothrombin time, and activated partial thromboplastin time (Table 232-1Table 232-1). The results of these tests, coupled
with clinical evaluation, should enable formulation of a di�erential diagnosis.18 Additional studies are ordered asindicated (Table 232-2Table 232-2). Obtain hematologic consultation if the di�erential diagnosis or the laboratory approach isunclear. In patients with postoperative bleeding, the basic laboratory tests for coagulation are of little help in
assessment or management.19

3/27/2019
6/14
TABLE 232-1
Initial Tests of HemostasisInitial Tests of Hemostasis
Screening TestsScreening TestsReferenceReference
ValueValueComponent MeasuredComponent Measured Clinical CorrelationsClinical Correlations
Primary HemostasisPrimary Hemostasis
Platelet count 150–400/mm3
(150–400 ×
109/L)
Number of platelets per
mm3
Decreased platelet count (thrombocytopenia):
bleeding usually not a problem until platelet
count is <50,000/mm3 (50 × 109/L); high risk of
spontaneous bleeding, including CNS bleeding,
seen with count of <10,000/mm3 (10 × 109/L);
usually due to decreased production or
increased destruction of platelets
Elevated platelet count (thrombocytosis):
commonly a reaction to inflammation or
malignancy, and occurs in polycythemia vera;
can be associated with hemorrhage or
thrombosis
Bleeding time
(BT)
Variable Interaction between
platelets and the
subendothelium
Prolonged BT caused by:
Typically 2.5–
10.0 min using
a BT template
Thrombocytopenia (platelet count <50,000/mm3
or 50 × 109/L)
Abnormal platelet function (von Willebrand's
disease, antiplatelet drugs, uremia, liver disease)
Secondary HemostasisSecondary Hemostasis
Prothrombin
time (PT) and
international
normalized
ratio (INR)
PT: 11–13 s;
depends on
reagent
Extrinsic system and
common pathway—factors
VII, X, V, prothrombin, and
fibrinogen
INR = 1.7 corresponds to
approximately 30% activity
of coagulation factors as a
whole
Prolonged PT most commonly caused by:
INR: 1.0 Warfarin (inhibits production of vitamin K–
dependent factors II, VII, IX, and X)
Liver disease with decreased factor synthesis

3/27/2019
7/14
Screening TestsScreening TestsReferenceReference
ValueValueComponent MeasuredComponent Measured Clinical CorrelationsClinical Correlations
Antibiotics that inhibit vitamin K–dependent
factors (moxalactam, cefamandole, cefotaxime,
cefoperazone)
Activated
partial
thromboplastin
time (aPTT)
22–34 s Intrinsic system and
common pathway—factors
XII, XI, IX, VIII, X, V,
prothrombin, and
fibrinogen
Prolonged aPTT most commonly caused by:
Depends on
type of
thromboplastin
reagent used
Heparin therapy
"Activated"
with kaolin
Factor deficiencies (factor levels have to be <30%
of normal to cause prolongation)
Fibrinogen
level
Slightly
variable
according to
specific test
Protein made in liver;
converted to fibrin as part
of normal coagulation
cascade
Low levels seen in disseminated intravascular
coagulation
Elevated in inflammatory processes (acute-
phase reactant)
Typically 200–
400
milligrams/dL
(2–4 g/L)
Thrombin
clotting time
(TCT)
10–12 s Conversion of fibrinogen to
fibrin monomer
Prolonged TCT caused by:
Low fibrinogen level
Abnormal fibrinogen molecule (liver disease)
Presence of heparin, fibrin degradation
products, or a paraprotein (multiple myeloma);
these interfere with the conversion
Occasionally seen in hyperfibrinogenemia
"Mix" testing Variable Performed when results on
one or more of the above
screening tests is
prolonged; the patient's
plasma ("abnormal") is
If the mixing corrects the screening test result:
one or more factor deficiencies are present

3/27/2019
8/14
Screening TestsScreening TestsReferenceReference
ValueValueComponent MeasuredComponent Measured Clinical CorrelationsClinical Correlations
mixed with "normal"
plasma and the screening
test is repeated
If the mixing does not correct the screening test
result: a circulating inhibitor is present

3/27/2019
9/14
TABLE 232-2
Additional Hemostatic TestsAdditional Hemostatic Tests
TestTest Reference ValueReference Value Component MeasuredComponent Measured Clinical Correlations/CommentsClinical Correlations/Comments
Fibrin degradation
product (FDP) and d-
dimer levels
FDP: variable depending
on specific test, typically
<2.5–10 micrograms/mL
(2.5–10 milligrams/L)
FDP test: measures
breakdown products from
fibrinogen and fibrin
monomer
Levels are elevated in di�use
intravascular coagulation,
venous thrombosis, pulmonary
embolus, and liver disease, and
during pregnancyd-Dimer: variable
depending on specific
test, typically <250–500
nanograms/mL (250–
500 micrograms/L)
d-Dimer test: measures
breakdown products of
cross-linked fibrin
Factor level assays 60%–130% of reference
value (0.60–1.30
units/mL)
Measures the percent
activity of a specified factor
compared to normal
To identify specific deficiencies
and direct therapeutic
management
Protein C level Variable Level of protein C in the
blood
Vitamin K dependent
Typically 60%–150% of
reference value
Increases with age
Values higher in males than
females
Deficiency associated with
thromboembolism in people <50
y of age
Protein S level Variable Level of protein S in the
blood
Vitamin K dependent
Typically 60%–150% of
reference value
Increases with age
Values higher in males than
females
Deficiency associated with
thromboembolism in people <50
y of age

3/27/2019
10/14
TestTest Reference ValueReference Value Component MeasuredComponent Measured Clinical Correlations/CommentsClinical Correlations/Comments
Factor V Leiden (FVL) Variable Screening test looks for
activated protein C
resistance, and
confirmatory test analyzes
DNA sequence of factor V
gene
FVL not inactivated by activated
protein C
Screening assay uses
activated partial
thromboplastin time with
and without added
activated protein C
Heterozygotes have 7× and
homozygotes have a 20×
increased lifetime risk of venous
thrombosis
Mutation associated with
thromboembolism in people <50
y of age
Antithrombin level Variable depending on
specific test
Measures level of
antithrombin in the blood
Not vitamin K dependent;
patients with deficiency require
higher dosages of heparin for
anticoagulation therapy
Typically 20–45
milligrams/dL (200–450
milligrams/L)
Deficiency associated with
thromboembolism in people <50
y of age
Antiphospholipid
antibodies
IgG <23 GPL units/mL
and IgM <11 MPL
units/mL
Tests for antibodies that
bind to phospholipids
Lupus anticoagulant: elevated in
systemic lupus erythematosus
(SLE) and other autoimmune
diseases
Lupus anticoagulant Anticardiolipin antibody:
elevated in SLE, other
autoimmune diseases, syphilis,
and Behçet's syndrome
Anticardiolipin antibody Increased risk of spontaneous
abortions, fetal loss, and fetal
growth retardation

3/27/2019
11/14
TestTest Reference ValueReference Value Component MeasuredComponent Measured Clinical Correlations/CommentsClinical Correlations/Comments
Anti–factor Xa activity During therapeutic
anticoagulant use: 0.7–
1.1 units/mL
Inhibition of factor Xa
activity
Used to monitor low-molecular-
weight heparin therapy, and
newer anticoagulants such as
apixaban and rivaroxaban
During prophylactic
anticoagulant use: 0.2–
0.3 units/mL
May be elevated in renal
dysfunction
Platelet function assay 88–183 s Tests for platelet adhesion
and aggregation
A�ected by uremia, anemia,
thrombocytopenia, antiplatelet
medications, and von
Willebrand's disease
Variable Initial test done with
epinephrine. A prolonged test is
repeated using ADP, and if
normal <122 s, indicates
probable aspirin e�ect
Peripheral blood
smear
Qualitative and
quantitative based on
visualization
Estimates quantity and
appearance of platelets,
WBCs, and red blood cells
Allows identification of clumped
platelets, abnormal cells
interfering with coagulation
(leukemia)
Operator dependent
Dilute Russell viper
venom time
23–27 s Venom directly activates
factor X and converts
prothrombin to thrombin
when phospholipid and
factor V are present
Prolonged in the presence of
antiphospholipid antibodies
Inhibitor screens Variable Verifies the presence or
absence of antibodies
directed against one or
more of the coagulation
factors
Specific inhibitors: directed
against one coagulation factor,
most commonly against factor
VIII
Nonspecific inhibitors: directed
against more than one
coagulation factor; example is
lupus-type anticoagulant

3/27/2019
12/14
Abbreviations: ADP = adenosine diphosphate; GPL = 1 microgram of a�inity-purified immunoglobulin G anticardiolipin antibody
from an original index serum; IgM, immunoglobulin M; MPL = 1 microgram of a�inity-purified immunoglobulin M anticardiolipin
antibody from an original index serum.
1.
2.
3.
4.
5.
6.
7.
TestTest Reference ValueReference Value Component MeasuredComponent Measured Clinical Correlations/CommentsClinical Correlations/Comments
Des-γ-
carboxyprothrombin
or PIVKA II (protein
induced by vitamin K
absence or
antagonism) test
Variable Measures inactive under-
carboxylated form of
prothrombin
Increased in vitamin K–deficient
states, such as hemorrhagic
disease of the newborn
Increased in overdoses of
warfarin or cholestatic liver
diseases that can respond to
vitamin K therapy
REFERENCESREFERENCES
Noel P, Cashen S, Patel B: Trauma-induced coagulopathy: from biology to therapy. Semin Hematol 50: 259, 2013. [PubMed: 23953343]
Sallah S, Kato G: Evaluation of bleeding disorders. A detailed history and laboratory tests provide clues. PostgradMed 103: 209, 1998.
[PubMed: 9553596]
de Moerloose P, Levrat E, Fontana P, Boehlen F: Diagnosis of mild bleeding disorders. Swiss Med Wkly 139: 327,2009.
[PubMed: 19529990]
Greaves M, Watson HG: Approach to the diagnosis and management of mild bleeding disorders. Thromb Haemost5 (Suppl 1): 167, 2007.
[PubMed: 17635723]
Lippi G, Franchini M, Guidi GC: Diagnostic approach to inherited bleeding disorders. Clin Chem Lab Med 45: 2,2007.
[PubMed: 17243907]
Kamal AH, Te�eri A, Pruthi RK: How to interpret and pursue an abnormal prothrombin time, activated partialthromboplastin time, and bleeding time in adults. Mayo Clin Proc 82: 864, 2007.
[PubMed: 17605969]
Chee YL: Coagulation. J R Coll Physicians Edinb 44: 42, 2014. [PubMed: 24995447]

3/27/2019
13/14
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Hayward CP, Mo�at KA, Liu Y: Laboratory investigations for bleeding disorders. Semin Thromb Hemost 38: 742,2012.
[PubMed: 23011792]
Harrison P, Lordkipanidzé M: Testing platelet function. Hematol Oncol Clin North Am 27: 411, 2013. [PubMed: 23714306]
Ng VL: Liver disease, coagulation testing, and hemostasis. Clin Lab Med 29: 265, 2009. [PubMed: 19665678]
Northup PG, Caldwell SH: Coagulation in liver disease: a guide for the clinician. Clin Gastroenterol Hepatol 11:1064, 2013.
[PubMed: 23506859]
Galbusera M, Remuzzi G, Boccardo P: Treatment of bleeding in dialysis patients. Semin Dial 22: 279, 2009. [PubMed: 19573008]
Merriman L, Greaves M: Testing for thrombophilia: an evidence-based approach. Postgrad Med J 82: 699, 2006. [PubMed: 17099087]
Thachil J: A practical approach to thrombophilia testing. Br J Hosp Med (Lond) 74: C94, 2013. [PubMed: 24049827]
Chong LY, Fenu E, Stansby G, Hodgkinson S, Guideline Development Group: Management of venousthromboembolic diseases and the role of thrombophilia testing: summary of NICE guidance. BMJ 344: e3979, 2012.
[PubMed: 22740565]
James AH, Kouides PA, Abdul-Kadir R et al.: Evaluation and management of acute menorrhagia in women withand without underlying bleeding disorders: consensus from an international expert panel. Eur J Obstet GynecolReprod Biol 158: 124, 2011.
[PubMed: 21632169]
Franchini M, Frattini F, Crestani S, Bonfanti C: Bleeding complications in patients with hematologicmalignancies. Semin Thromb Hemost 39: 94, 2013.
[PubMed: 23247655]
Rydz N, James PD: Approach to the diagnosis and management of common bleeding disorders. Semin ThrombHemost 38: 711, 2012.
[PubMed: 22941792]
Haas T, Fries D, Tanaka KA, Asmis L, Curry NS, Schöchl H: Usefulness of standard plasma coagulation tests inthe management of perioperative coagulopathic bleeding: is there any evidence? Br J Anaesth 114: 217, 2015.
[PubMed: 25204698]
McGraw Hill

3/27/2019
14/14
Copyright © McGraw-Hill Education All rights reserved.
Your IP address is 99.53.251.15599.53.251.155 Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair