Embed Size (px)
Citation preview

230 BRIEF REPORTS
FIGURE 2. Apical view of the mitral prosthesis in systole (left) and diastole (right) just before the patient’s death. Note the clear separation of the valve from the anulus (arrow) during systole. LA = left atrium; LV = left ventricle; S = stent.
weeks before the 2-D study revealed abnormal stent motion. Second, in addition to the detection of systolic
regurgitant flow, the Doppler study confirmed pros- thetic MR by showing a calculated increase in mitral valve are&, which is most likely due to diastolic flow around the dehisced stent and through the prosthesis:
Analysis of Doppler flow pattern changes in diastole as well as systole may provide useful information in evaluation of prosthetic mitral valvular dysfunction.
References 1. Abbasi A, Allen M, DeCristofaro D, Ungar I. Detection and estimation of the
degree of mitral regurgitation by range-gated pulsed Doppler echocardiog- raphy. Circulation 1980;61:143-147.
2. Hatle L, Angelsan 6, Tromsdal A. Noninvasive assessment of atrioventricular pressure half-time by Doppler ultrasound. Circulation 1979;60:1096- 1104.
3. Hatle L, Angelsen B. Doppler ultrasound in cardiology: Physical principles and clinical applications. Philadelphia: Lea & Febiger, 1982:121-128.
4. Kotler MN, Mink GS, Panidis I, Morganroth J, Segal BL, Ross J. Noninvasive evaluation of normal and abnormal prosthetic valve function. JACC 1983; 2:151-173.
5. Caputo G, Pearlman A, Namay D, Dooley T. Detection of prosthetic valve incompetence using pulsed Doppler echocardiography (abstr). Circulation 1980;62:suppl lll:lll-252.
Tissue Characterization by Magnetic Resonance Imaging in Hypertrophic
Cardiomyopathy
DONALD FARMER, MD CHARLES B. HIGGINS, MD
EDWARD YEE, MD MARTIN J. LIPTON, MD
DENNIS WAHR, MD THOMAS PORTS, MD
A method for providing tissue characterization of the myocardium has been sought for years. Magnetic res- onance imaging (MRI) has demonstrated excellent soft tissue differentiation and has been proposed as a method for tissue characterization. This capability of MRI is suggested from previous studies that showed changes in signal intensity of ischemic compared with normal myocardium in experimental preparations.lJ Measurement of magnetic relaxation times, Tl and T2, in animal studies have verified a difference in these times between normal and ischemically damaged myocardium.l-3 Recently, we encountered a patient with hypertrophic cardiomyopathy (HC) in whom MRI provided more accurate anatomic depiction of the condition than other imaging techniques. MRI also re- vealed differences in signal intensity at various sites in the left ventricular (LV) myocardium due to fibrosis and myocardial ischemia.
From the Departments of Radiology, Medicine and Surgery, University of California, San Francisco, California 94143. Manuscript received May 23, 1984; revised manuscript received August 16, 1984, accepted August 23, 1984.
A62-year-old man was admitted for evaluation of refrac- tory recurrent ventricular tachycardia. Cardiac catheter- ization at age 48 years yielded findings consistent with HC. A subsequent echocardiogram in 1982 showed an LV aneu- rysm and a prolapsing mitral valve. During the current ad- mission, 2-dimensional echocardiography showed a dyski- netic apex and an extremely hypertrophied proximal portion and midportion of the left ventricle with systolic cavity obliteration. Cardiac angiography was interpreted as asymmetric encroachment of the cardiac walls upon the LV cavity with division of the chamber into a small-volume, hyperdynamic proximal chamber and a distal akinetic chamber. The 2 major cavities were separated by a wide ring of thickened myocardium in the midportion of the ventricle. The proximal and distal cavities were connected by a narrow
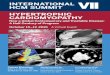
FIGURE 1. Systolic frame of the left ventricular cineangiogram (right anterior oblique projection). There is severe midventricular narrowing producing a small channel (arrows), which leads into a small akinetic apical chamber (arrowhead).

January 1, 1985 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 55 231
tunnel coursing through the ring of hypertrophied muscle (Fig. 1). A rare form of HC of the midventricular type was considered, although a cardiac tumor causing the segmen- tation could not be excluded. The coronary arteriogram re- vealed no fixed obstruction lesions, but did reveal severe systolic narrowing of an intramyocardial left anterior de- scending coronary artery.
MRI was performed with a 0.35-tesla superconductive type (Diasonics, Inc.), which gave a resonance frequency for hy- drogen of 15 MHz. The multislice imaging technique was used whereby 5 adjacent but not contiguous 7.0-mm-thick tissue sections (2.5-mm gap between slices) were pulsed at lOO-ms intervals during each repetition interval (TR). Thus, the imaging period for all 5 sections was approximately 500 ms. This duty cycle of 500 ms was accommodated within the RR interval for this patient. With this technique, the slices are not in the same phase of the cardiac cycle. The sectional (plane) images were reconstructed with the 2-dimensional Fourier transform technique. The reconstruction matrix comprised 128 vertical and 256 horizontal pixels. It was displayed in 256 gray levels, with the brightest area repre- senting the tissue with the greatest MRI signal intensity. Spatial resolution was 1.6 mm. The TR was determined by the RR interval of the electrocardiogram when gated to every heart beat and double the RR interval when gated to every second heart beat. The echo delay times (TE) were 28 and 56 ms.
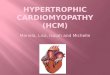
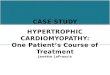
Magnetic resonance images showed obliteration of the LV cavity by marked thickening of the anterior, anteroseptal and anterolateral walls of the LV myocardium (Fig. 2). At the midventricular level, only the inflow portion was patent, with an anteriorly situated aneurysmal cavity at the apex, connected only by a narrow channel to the residual inflow cavity. This appearance was similar to that shown by left ventriculography (Fig. 1). In addition to.defining the ana- tomic configuration of the ventricle, the images also dem- onstrated inhomogeneity of the myocardial signal intensity. The upper septum had normal intensity, whereas the an- teroseptal region had low intensity. Additionally, there was a region of high signal intensity involving the subendocardial
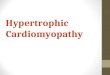
layer of the apical segment (Fig. 2). There was a greater in- crease in signal intensity of the apical subendocardial layer on the TE 56-ms image than on the TE 28-ms image. This finding is consistent with a long T2 relaxation time of the subendocardial myocardium. High signal intensity and prolonged T2 time were observed in dogs with acute myo- cardial infarctions lv2. these experimental data were the basis of interpretation of dhe MR study in this case. The observa- tions in the present case and the prior experimental results suggested that the variability of the signal intensity in the myocardium represented fresh ischemic damage in the high-intensity region, while the low intensity region was fi- brosis at the site of remote myocardial ischemia injury. In view of the mass effect on the ventricular cavity, the possi- bility of a myocardial tumor was also considered. The mag- netic resonance images (Fig. 3) also provided evidence of stasis of flow in the narrowed LV cavity. Comparison of first (TE = 28 ms) and record (TE = 56 ms) images showed filling of the chamber with high-intensity signal on the second echo image. This finding is consistent with experimental data indicating that this pattern is consistent with flow stasis.4
At surgery, a LV apical aneurysm was resected and the apical scar was plicated. Gross examination of the ventricle during bypass revealed areas of tough, fibrous myocardium adjacent to edematous myocardium in the subendocardial layer of the mass of myocardium that nearly obliterated the midportion and distal portion of the left ventricle. Extreme hypertrophy of the myocardium at the base of the papillary muscles was noted. Pathologic examination of the resected portion of the left ventricle revealed marked interstitial fi- brosis separating sparse myocardial fibers. The regions found to be edematous by inspection were not biopsied.
A wide spectrum of distribution of HC exists within the left ventricle.536 While asymmetric septal hyper- trophy is the most frequent type, several variations of this disease have been uncovered in the past decade, of which the midventricular type is apparently very rare.5 MRI provided an accurate anatomic assessment in this
FIGURE 2. Sequential but not contiguous transverse magnetic resonance image in the region of the cardiac apex. The lefl and middle panels were produced from the first spin echo (TE = 28 ms); the right panel was from the second spin echo (TE = 56 ms). Three areas of signal intensity can be seen within the myocardium (left). The upper septum (open white arrow) has normal signal intensity, whereas the anteroseptal portion (white arrow) shows diminished signal intensity and corresponded to regions of fibrosis at surgery. The region of high signal intensity (black arrow) adjacent to the area of anteroseptal fibrosis suggests soft tissue edema secondary to acute myocardial ischemic damage near the apex. In the image on the right, which was obtained during ventricular systole, the left ventricular cavity is nearly obliterated in its midportion (arrowhead), corresponding to the left ventricular cineangiogram in Figure 1. The small akinetic apical chamber (arrow) is rimmed by high signal intensity, suggesting subendocardial edema. There are regions of high signal intensity in the anterior myocardium on all images, suggesting that the area of ischemic damage involves a wide region.

232 BRIEF REPORTS
FIGURE 3. Transverse magnetic resonance images at the apical portion of the left ventricle showing obliteration of the inferior portion of the ventricular cavity, leaving only the small akinetic apical chamber. The image produced from the first spin-echo (left) (TE = 28 ms) reveals the high-signal intensity rim around the chamber (arrow), corresponding to subendocardial edema. In the second spin-echo image (rigM, TE = 56 ms), the chamber is filled with signal secondary to extremely sluggish flow in the akinetic region (arrowhead).
unusual case. Previous reports have also indicated that gated MRI provides clear anatomic depiction of cardiac7 and pericardial abnormalities? because it provides high natural contrast between the blood pool and the walls of the heart as a consequence of the virtual absence of magnetic resonance signal from blood flowing at normal velocity.
Perhaps more important in this patient was the variability in myocardial signal intensity, which corre- sponded to differences in the nature of the tissue in the LV wall. The ability of MRI to discern tissue water content1*2 and suggest fibrous change in tissues9 due to alterations in magnetic relaxation times (Tl and T2 times) has been proposed. The current report suggests that this sensitivity to variations in the composition of tissues can provide myocardial tissue characterization in patients.
References 1. Higgins CB, Herfkens R, Lipton MJ, Sheldon P, Kaufman L, Crooks LE.
Nuclear magnetic resonance imaging of acute myocardial infarctions: Al- terations in magnetic relaxation times. Am J Cardiol 1983;52:184-188.
2. Wesbey G, Higgins CB, Lanzer P, Botvinick E, Lipton MJ. Imaging and characierization-of acute myocardial infarction in viva by gated nuclear maanetic resonance. Circulation 1984:69:125-130.
3. Williams ES, Kaplan JI, thatcher F, Zimmerman G, Knabel SB. Prolongation of proton spin lattice relaxation times in regionally ischemic tissues from dog hearts. J Nucl Med 1980;21:449-453.
4. Kaufman L, Crooks LE, Sheldon PE, Hrlcak H, Herfkens R, Bank W. The potential impact of nuclear magnetic resonance imaging on cardiovascular diagnosis. Circulation 1983;67:251.
5. Maron BJ, Gottdiener MS, Epstein SE. Patterns and significance of distri- bution of left ventricular hypertrophy in hypertrophic cardiomyopathy. Am J Cardiol 1981;48:418-428.
6. Falicoo RE, Resnekov L, Bharatl S, Lev M. Midventricular obstruction: a variant of obstructive cardiomyopathy. Am J Cardiol 1976;37:432-437.
7. Higgins CB, Lanzer P, Stark D, et al. Imaging by nuclear magnetic resonance in patients with chronic ischemic heart disease. Circulation 1983;69: 523-531.
6. Stark D, Higgins CB, Lanzer P, et al. Magnetic resonance imaging of the rrcardium: normal and pathologrc frndmgs. Radiology 1984;150:469-
9. Davis PR, Kaufman L, Crooks LE, Margulis AR. NMR characteristics of normal and abnormal rat tissue. In: Nuclear Magnetic Resonance Imaging in Medicine. Tokyo, Igaku-Shoin, 1981:71.
Origin of the Right Coronary Artery from the Pulmonary Trunk: Diagnosis by
Two-Dimensional Echocardiography
CLIFTON WORSHAM, MD STEPHEN P. SANDERS, MD
BRUNO M. BURGER, MD
Anomalous origin of the right coronary artery (RCA) from the pulmonary trunk (PT) is rare. Fewer than 20 cases have been rep0rted.i Most have been incidental findings at autopsy or during surgery for other rea- sons.2-4 Rarely, diagnosis has been made by angiogra- phy.596 We report here a patient with the RCA from the
From the Department of Pediatrics, Harvard Medical School, and the Department of Cardiology, The Children’s Hospital, Boston, Massa- chusetts 02115. Dr. Worsham’s present affiliation: Cigna Health Plan, Division of Pediatrics, Phoenix, Arizona. Dr. Burger’s present affiliation: Centro Medico Docente La Trinidad, Caracas, Venezuela. Manuscript received August 13, 1984; revised manuscript received August 27, 1984, accepted August 29, 1984.
PT, diagnosed by 2-dimensional echocardiography (2-D echo). /
T.A., a 6.5year-old asymptomatic girl, was referred be- cause of precordial murmur. Examination disclosed a grade Z/6 blowing midsystolic ejection murmur at the left lower sternal border without radiation. The electrocardiogram showed a QRS axis of +50° without evidence of left ventric- ular hypertrophy or repolarization abnormalities, The car- diac silouette was minimally enlarged on chest radiograph. A 2-D echocardiogram disclosed a dilated left coronary artery arising from the aorta (Fig. IA). The right coronary artery, seen in parasternal short-axis view, also was dilated and appeared to course anterior to the aorta to join the PT (Fig. 1B). Doppler examination revealed a diastolic flow distur- bance in the PT adjacent to the origin of the RCA. Both ventricles were of normal size and appeared to function normally. Origin of the RCA from the PT was subsequently documented by cineangiography (Fig. 2). A left-to-right shunt (&p/&s = 1.4:1) was demonstrated. The end-diastolic pressure was 1 to 4 mm Hg in both ventricles before angiog- raphy, but the left ventricular end-diastolic pressure in- creased to 20 mm Hg after angiography.
Dilatation of the coronary arteries is a distinctive echocardiographic finding that suggests an anomalous