Embed Size (px)
Citation preview

Tissue-engineered intervertebral discs producenew matrix, maintain disc height, and restorebiomechanical function to the rodent spineRobby D. Bowlesa, Harry H. Gebhardb,1, Roger Härtlb, and Lawrence J. Bonassara,c,2
aDepartment of Biomedical Engineering, Cornell University, 151 Weill Hall, Ithaca, NY 14853; bDepartment of Neurosurgery, Weill Cornell MedicalCollege, 525 East 68th Street, New York, NY 10065; and cSibley School of Mechanical and Aerospace Engineering, Cornell University, 149 Weill Hall,Ithaca, NY 14853
Edited* by Robert Langer, Massachusetts Institute of Technology, Cambridge, MA, and approved June 20, 2011 (received for review May 5, 2011)
Lower back and neck pain are leading physical conditions for whichpatients see their doctors in the United States. The organ com-monly implicated in this condition is the intervertebral disc (IVD),which frequently herniates, ruptures, or tears, often causing painand limiting spinal mobility. To date, approaches for replacement ofdiseased IVD have been confined to purely mechanical devicesdesigned to either eliminate or enable flexibility of the diseasedmotion segment. Herewe present the evaluation of a living, tissue-engineered IVD composed of a gelatinous nucleus pulposus sur-rounded by an aligned collagenous annulus fibrosus in the caudalspine of athymic rats for up to 6 mo. When implanted into the ratcaudal spine, tissue-engineered IVD maintained disc space height,produced de novo extracellular matrix, and integrated into thespine, yielding an intact motion segment with dynamic mechanicalproperties similar to that of native IVD. These studies demonstratethe feasibility of engineering a functional spinal motion segmentand represent a critical step in developing biological therapies fordegenerative disc disease.
regenerative medicine ∣ total disc replacement ∣ biomaterials ∣ discarthroplasty ∣ image-based
Among the most common physical conditions for whichpatients see their doctors are back and neck pain, which carry
an estimated annual cost to society up to $100 billion (1). Currentconservative and operative treatment options are mostly pallia-tive in nature and fail to restore function to the spine. The mostcommon target for treatment of back and neck pain is the inter-vertebral disc (IVD) (2–5). IVD degeneration is characterized byloss of proteoglycan, loss of disc height, annulus fibrosus (AF)damage and tears, spondylolisthesis, spinal stenosis, herniateddiscs, neoinnervation, hypermobility, and inflammation (6–8).Conservative treatments including medication and physiotherapyare the first line of defense in treating these disorders. Despitethese treatments, it is estimated that between 1.5 and 4 millionpatients in the United States await surgical intervention (9).
Such surgical interventions may involve the removal of her-niated tissue or the entire IVD and replacing it with a mechanicaldevice designed to either fuse the adjacent vertebrae or to pre-serve some motion. Regardless of approach, motion segmentmobility is altered, often precipitating degeneration in adjacentmotion segments (10). Nonbiological total disc replacement im-plants were developed to avoid this loss of motion at the operatedlevel, and as a result, reduce the incidence of adjacent segmentdisease. The efficacy of such implants is a matter of much debate(11–13); however, it is clear that nonbiological total disc replace-ment implants suffer from failure modes commonly associatedwith traditional metal/polyethylene arthroplasty, such as mechan-ical failure, dislodgement, polyethylene wear, and associated osteo-lysis and implant loosening.More recently, increasing attention hasbeen turned toward creating tissue engineering strategies to restorefunction to the diseased or injured IVD.
The intervertebral disc is composed of two distinct regions, theAF and the nucleus pulposus (NP). The NP is a gelatinous tissue,rich in proteoglycan and type II collagen that is surrounded bythe AF, a highly organized fibrocartilage predominantly made oftype I collagen and proteoglycans. A number of tissue engineeringstrategies have focused on creating either the AF or NP separately(14), but much interest has recently been focused on creating acomposite tissue-engineered total disc replacement (TE-TDR)implant that contains both AFand NP tissue (15–19). The success-ful replication of spinal motion and function in human IVD allo-graft transplantation (20) suggests that a properly engineered IVDimplant could be an important tool for clinical spine care.
Despite the promise of tissue engineering approaches fordesign of IVD implants (15–19) and preliminary reports of theirtransplantation into the spine (21), to date none have demon-strated the ability to restore the structure and function of a motionsegment in vivo. Here we show that our previously documentedapproach to producing TE-TDR implants with circumferentiallyaligned collagen fibrils in the AF (15), combined with image-baseddesign techniques to reproduce precise anatomy (22–26) yieldedimplants that integrated with the rat caudal spine, reproduced ap-propriate tissue structure, and generated a mechanically functionalmotion segment in the rat caudal spine.
ResultsEngineered IVDs Reproduce Native Shape and Composite Structureover 6_ Mo of Implantation. To study the function of tissue-engi-neered IVD implants, we chose to replace healthy IVD in the ratcaudal spine. The rat caudal spine was chosen for ease of surgicalaccess, repeatability of the surgery, and the levels of stress andstrain imposed on caudal discs (27–29). We constructed compo-site TE-TDR implants seeded with ovine AF and NP cells andinserted them into the caudal 3∕4 disc space of athymic rats. Sam-ples were harvested at 6 wk and 6 mo along with separate groupscontaining no implant (discectomy) and native discs reimplantedinto the caudal spine, analogous to an allograft (30).
Microcomputed tomography (μCT) andMRI images of the cau-dal 3∕4 disc space were obtained and used to produce a TE-TDRimplant with native dimensions (Fig. 1A). μCT images allowedthe outer boundaries of the IVD to be determined from the bonyends of the neighboring vertebrae and the NP dimensions from theMRI data. Using these clinically relevant imaging techniques to
Author contributions: R.D.B., H.H.G., R.H., and L.J.B. designed research; R.D.B. and H.H.G.performed research; R.D.B., H.H.G., R.H., and L.J.B. analyzed data; and R.D.B., H.H.G., R.H.and L.J.B. wrote the paper.
The authors declare no conflict of interest.
*This Direct Submission article had a prearranged editor.1Present address: Clinic of Trauma Surgery (BG), Schnarrenbergstrasse 95, 72076Tuebingen, Germany.
2To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1107094108/-/DCSupplemental.
13106–13111 ∣ PNAS ∣ August 9, 2011 ∣ vol. 108 ∣ no. 32 www.pnas.org/cgi/doi/10.1073/pnas.1107094108
Dow
nloa
ded
by g
uest
on
Mar
ch 5
, 202
1

design the engineered disc and combining them with the collagencontracted-AF/alginate-NP engineered disc construction we re-ported previously (15), we constructed anatomically shaped discs(Fig. 1E) that were surgically implanted into the native caudal 3∕4disc space (Fig. 1C).
The imaging and fabrication technique produced discs thatmimicked the native morphology (Fig. 1 E and F). These anato-mically shaped engineered discs were implanted into the nativecaudal disc space and the MRI demonstrated hydrated tissuein the disc space post operatively at 6 wk and at 6 mo that weresimilar to the native adjacent levels (Fig. 1D). Upon explantationat 6 mo, the tissue had a distinct composite cartilaginous appear-ance and IVD shape upon explantation (Fig. 1 E and F).
Engineered IVD Integrated with Neighboring Vertebrae and ProducedExtracellular Matrix with Native Levels of Collagen and Proteoglycanin the AF and NP. It was hypothesized that our composite engi-neered IVD would produce an ECM in the native caudal discspace that was rich in collagen and proteoglycans, similar to thenative IVD, and would integrate with the vertebral bodies. To testthis hypothesis, we performed histological staining for collagenand proteoglycans in the disc space, as well as quantitative bio-chemical analysis on the explanted tissue at 6 mo for collagen,proteoglycan, and DNA (31–33). In the discectomy group, inwhich the native disc had been removed and nothing implantedin its place, the disc space collapsed with no production of col-lagen and proteoglycans (Fig. 2 C andD). In contrast, engineereddiscs contained properly distributed collagen and proteoglycan inthe AF and NP by 6 mo (Fig. 2 E, F, and I). Similar to the nativeIVD, increased collagen was observed in the AF compared tothe NP at 6 mo as indicated by both the hydroxyproline contentand picrosirius red staining (Fig. 2 E and I). Collagen type I wasdistributed throughout the disc whereas type II collagen demon-strated some localization in the NP region (Fig. S1). Proteogly-
cans were seen in both the AF and NP regions, but with increasedproteoglycan content in the NP region compared to the AF region,as seen by histology and biochemical analysis (Fig. 2 F and I).Overall, biochemical analysis showed no significant differences incollagen or proteoglycan content between the engineered andnative AF and NP after 6 mo in the disc space. In contrast, thereimplanted IVD showed significantly more collagen (p < 0.05)in the AF and significantly less proteoglycan (p < 0.05) in theNP after 6 mo. DNA content indicated that robust cell prolifera-tion occurred within the disc space in both the engineered andreimplanted groups. Collectively the analysis of the ECM pro-duced by TE-TDR indicates phenotypically appropriate spatialdeposition of collagen and proteoglycans, which resulted in thecomposite structure observed in the engineered tissue (Fig. 1E).
In addition to appropriate composition and arrangement ofECM, a critical requirement for a tissue-engineered IVD is inte-gration with neighboring vertebrae.
Analysis of the implant-end plate interface by histologydemonstrated progressive integration over 6 mo. At 6 wk integra-tion was apparent, but small discontinuities were observed atthe end plate and engineered tissue boundaries (Fig. 2 J and K).At 6 mo, the boundary was integrated completely with no largediscontinuities observed at this interface (Fig. 2 L andM). Underpolarized light microscopy, collagen bundle networks can be ob-served crossing the boundary between the end plate/bone inter-face and the engineered tissue (Fig. S2). This integration suggeststhat the proteoglycan and collagen-rich matrix produced by theengineered disc can function as a unit with the native spine.
Engineered IVD Produced Functional Tissue that Maintained DiscHeight and had Similar Mechanical Properties to Native IVD.To deter-mine whether tissue-engineered IVD implants generated a func-tional motion segment, we analyzed the disc height and thedynamic mechanical properties of the motion segments. Mainte-
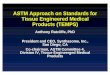
Fig. 1. Anatomical TE-TDR, designed from MRI and CT, survives in disc space for 6 mo. (A) CT and MRI design procedure for obtaining TE-TDR dimensions.(B) Fabrication of TE-TDR. (i) NP dimensions used to design injection molds via computer-aided design. (ii) Injection mold 3-D printed out of acrylonitrilebutadiene styrene plastic. (iii) Cell-seeded alginate was injected into mold, removed, (iv) placed in center of 24 well plate, and cell-seeded collagen was pouredaround alginate NP. (v) After 2 wk of culture, cell-seeded collagen contracts around the NP to form composite TE-TDR. (C) Intraoperative images showingexposed caudal 3∕4 disc space and implanted TE-TDR. (D) T2-weighted MRI of implanted disc space (marked by yellow arrows) and adjacent native levelsimmediately postoperative, at 1 mo, and 6 mo after implantation. (E) History of TE-TDR in native disc space. Intraoperative photo showing explanted nativeIVD next to the TE-TDR (day 0) that was implanted in its place and TE-TDR after being implanted into native disc space for 6 mo. (F) Size of engineered IVDcompared to native IVD. Measurements were taken along the lateral and ventral-dorsal planes of the engineered and native IVD. Engineered IVD measure-ments were taken at day 0 prior to implantation (n ¼ 12) and compared to explanted native discs (n ¼ 12). Engineered IVDmeasurements were also taken after6 mo of implantation (n ¼ 12).
Bowles et al. PNAS ∣ August 9, 2011 ∣ vol. 108 ∣ no. 32 ∣ 13107
BIOPH
YSICSAND
COMPU
TATIONALBIOLO
GY
ENGINEE
RING
Dow
nloa
ded
by g
uest
on
Mar
ch 5
, 202
1

nance of vertebral spacing is a critical role of the IVD and is aprimary clinical indicator of IVD health. As such, maintenance ofdisc height is a critical indicator of the performance of a tissue-engineered IVD. Tissue-engineered IVD implants maintained79� 18% of the disc height at 6 wk and 83� 13% at 6 mo, whereasthe discectomy group collapsed (37� 3%) (Fig. 3A). At 6 wk andat 6 mo the engineered disc was comparable to the reimplantednative disc at maintaining caudal disc space (Fig. 3A).
The ability to properly sustain axial loads is a key function ofthe IVD (34). To investigate how the engineered discs restoredthis function of the spine, we analyzed the dynamic mechanicalproperties of motion segments of native caudal spines and those
receiving implants by imposing sinusoidal strains of 3% ampli-tude (3% tensile strain to 3% compressive strain) at frequenciesranging from 0.01 to 10 Hz. Intact motion segments were testedto assess effects of integration of the IVD tissue with the endplate and vertebrae, and the mechanical performance of tissue-engineered IVD was compared to that of native caudal motionsegments and of spines that received reimplanted healthy discs(Fig. 3 B and C). Motion segments with engineered tissue hada moderately larger modulus than the native motion segment(p ¼ 0.020) over the full range of frequencies tested. This mod-ulus was maintained over both the compressive and tensile strainregions of the test, demonstrating the integration observed within
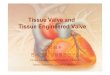
Fig. 2. TE-TDR produces integrated tissue with IVD-like collagen and proteoglycan content in the native disc space. Picrosirus red collagen staining for(A) native IVD, (C) discectomy group, (E) TE-IVD at 6 mo, and (G) reimplanted IVD at 6 mo. Alcian blue staining for (B) native IVD, (D) discectomy group,(F) TE-IVD at 6 mo, and (H) reimplanted IVD at 6 mo. (I) Biochemical analysis of glycosaminoglycan (proteoglycans), hydroxyproline (collagen), and DNA (cells)content for the native disc (n ¼ 6), engineered TE-TDR (n ¼ 6), and reimplanted IVD (n ¼ 6) broken down by region of the disc (� ¼ p < :05 compared to native;# ¼ p < :05 compared to all groups). Histology of TE-TDR and native tissue interface (VB, vertebral bodies; EP, end plate) at (J, K) 6 wk and (L, M) 6 mo de-monstrates progressive integration of TE-TDR with native tissue (arrows point to small disruptions of integration at 6 wk, absent at 6 mo).
Fig. 3. TE-TDR produces a mechanically functional tissue in the native disc space. (A) Percentage of disc space height maintained at 6 wk and 6 mo for dis-cectomy group (n ¼ 12), reimplant group (n ¼ 12), and TE-TDR group (n ¼ 12). (B) Dynamic mechanical properties at 6 mo for TE-TDR implanted motionsegments (n ¼ 6), intact native motion segments (n ¼ 6), and reimplant motion segments (n ¼ 6) showing representative stress-strain curves at 1 Hz and ap-parent moduli from 0.01–10 Hz. (C) Equilibrium modulus, hydraulic permeability, and percent hysteresis (energy dissipation) for intact native motion segments(n ¼ 6), TE-TDR implanted motion segment (n ¼ 6), and reimplant motion segments (# ¼ p < 0.05 compared to discectomy) (� ¼ p < 0.05 compared to native).
13108 ∣ www.pnas.org/cgi/doi/10.1073/pnas.1107094108 Bowles et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 5
, 202
1

the histology was mechanically functional at the levels of tensilestrain imposed here. The capacity of the engineered IVD todissipate mechanical energy, as indicated by the hysteresis inthe stress-strain curve, was similar to that of the native motionsegment (32% compared to 41%) (Fig. 3C). The reimplanted discshowed no significant difference in apparent modulus comparedto the native disc but dissipated significantly less energy(p < 0.05) than both the engineered and intact native motionsegment. The ability to dissipate mechanical energy is a criticalfunction of the IVD, and the lack of this function may contributeto adjacent segment disease seen after fusion or total disc arthro-plasty (12, 13). In this way, tissue-engineered IVD may restorethe energy damping capacity of the spine in a way that is not avail-able with current treatment options.
In addition to dynamic mechanical testing, the motion seg-ments were subjected to stress-relaxation testing to determine thestatic compressive equilibrium modulus and the hydraulic perme-ability of the tissue (35). The equilibrium modulus and hydraulicpermeability of the engineered disc were not significantly differ-ent from the intact native disc (Fig. 3C) or reimplanted disc.Overall, both the dynamic and quasi-static compressive data in-dicates the engineered discs restored compressive mechanicalfunction to the caudal spine by producing a tissue with similarproperties to the native IVD.
DiscussionThe production of a TE-TDR implant for use in the treatment ofdiscogenic back and neck disorders, as well as for use in studyingIVD pathology and structure-function relationships has been arecent area of scientific interest. Yet, the successful creation of afunctional engineered IVD in the native disc space had yet to beachieved (15–19). The ability to replace an IVD with a living andmechanically functional engineered IVD provides great promisein the treatment and understanding of spinal disease. However,the implantation of a TE-TDR implant into the native disc spaceprovides a number of challenges to the disc that had yet to beaddressed because of the lack of in situ studies.
The main challenges in developing and delivery of a tissue-engineered IVD implant are thought to be (i) generating func-tional tissue in the disc space (36), (ii) securing the implants inthe spine to ensure that they will integrate with the neighboringvertebrae (15–18, 37), and (iii) developing an implant that canwithstand the complex mechanical loading of the disc space (38).Here we demonstrated that our tissue-engineered IVD implantswere able to meet all three of these challenges in the rat caudalspine by producing a collagen and proteoglycan-rich, well-inte-grated, and mechanically functional tissue in the native disc space.This study provides unique evidence that a tissue-engineered IVDimplant can replace the native IVD in the spine.
A critical piece of enabling technology involved the use ofclinically relevant imaging modalities, MRI and CT, to designtissue-engineered IVD. This technique allowed the creation ofa TE-TDR implant in the size and shape of the native IVD (Fig. 1)and was integral to producing a disc that fit properly into thenative disc space (Fig. 1C). MRI and CTwere used to design thedisc because it is easily translatable to clinical practice and makespatient-specific TE-TDR implant design possible. Patient-specificdesign is likely to be important for TE-TDR, as proper sizematching is essential for IVD transplantation success (30). After6 mo of implantation, a hydrated tissue was produced withinthe disc space (Fig. 1D) that maintained the overall shape of theimplanted TE-TDR implant and disc space (Fig. 1 E and F).
The production of proteoglycans and collagen in quantitiessimilar to the native disc demonstrated that the cells survivedin the caudal disc space and successfully produced tissue de novo.In previous work in vitro, a proteoglycan content of only approxi-mately 25% was obtained in vitro for both AF and NP (18)whereas a proteoglycan content on the order of the native NP
and approximately 33% of the AF was obtained in subcutaneousimplantations (17). In general, in vitro studies have not yieldedIVD tissue with collagen and proteoglycan similar to that ofnative tissue (14, 17–19). Together with the current data, theseresults suggest that the caudal intervertebral disc space providessufficient nutrient supply in our model to enable the productionand maintenance of robust ECM by IVD implants.
There are likely a number of contributing factors to the successof this TE-TDR implant in producing a robust ECM in the discspace. These factors may include the increased cytokine signalinglikely experienced in an in vivo environment and the anaboliceffect that mechanical stimulation, which would be present in thenative disc space, has been shown to have on IVD cells (39, 40).However, the disc space is known to have limited nutrient avail-ability (i.e., glucose and oxygen) and poor waste product trans-port (e.g., lactate) out of the disc (41). The high permeability ofthe collagen/alginate TE-TDR construct at implantation mayincrease the availability of nutrients throughout the engineeredIVD in the disc space and promote ECM production. At thistime, it is unclear which of these effects, or others, are promotingsuch a robust ECM development, but it will be important infuture work to further elucidate these mechanisms, as they willbe important for the future design principles of TE-TDR implants.It is important to note that despite the similarities in ECM contentbetween the native and engineered disc, a number of differencesdid exist. These included a lack of lamellar structure in the AF,differences in collagen I and II distribution, and larger variancesin ECM content in the engineered discs than observed in the nativediscs. It is currently unclear how these differences will affect thelong-term viability and function of TE-TDR, but will become im-portant to understand as work in TE-TDR moves forward.
In addition to the ECM production, the ability of the TE-TDRimplant to integrate with the end plates of the neighboring ver-tebral bodies and produce a functional motion segment is a keyfinding of this work. Although the arrangement of lamellar col-lagen in TE-IVD implants is not the same as native tissue, polar-ized light microscopy shows large, organized fiber bundles fromthe implants inserting into neighboring vertebrae (Fig. S2c).Furthermore, this integrated ECM produced by the TE-TDR im-plant is mechanically functional within the motion segment, asindicated by the ability of the motion segment to withstand tensilestresses imposed during dynamic mechanical tests (Fig. 3B). Thismechanical data is consistent with the histology that shows pro-gressive integration of the implants into the spine over the courseof 6 mo (Fig. 2 L and M).
Despite the successful replacement of the native IVD with anengineered IVD composite in the caudal rat model, it is impor-tant to note the challenges that remain before TE-TDR can be-come a reality in the clinic. The engineered IVD demonstrated anability to produce functional tissue in the caudal disc space of therat. However, a number of important differences exist betweenthe rat caudal disc space and the human cervical and lumbar discspace that may provide additional hurdles to clinical translation.First, the larger size of the human IVD and decreased permeabil-ity of the degenerated end plate will provide decreased nutri-tional availability in clinical patients compared to the rat caudaldisc space (36). It will be important to investigate how the chal-lenge of the nutrient-deprived human disc space environment willaffect tissue development and integration of engineered IVD withnative tissues. In addition, although there is evidence that the me-chanical loading environment of the rodent tail shares some simi-larities with the human spine (27–29), the loading environmentsare undoubtedly different and will likely provide additional me-chanical challenges to an engineered disc beyond that seen inthe caudal disc space. Furthermore, only axial mechanical proper-ties were investigated within this study. It will be important infuture work to investigate how such composites perform in the full6° of freedom experienced in the human spine, including bending
Bowles et al. PNAS ∣ August 9, 2011 ∣ vol. 108 ∣ no. 32 ∣ 13109
BIOPH
YSICSAND
COMPU
TATIONALBIOLO
GY
ENGINEE
RING
Dow
nloa
ded
by g
uest
on
Mar
ch 5
, 202
1

and torsion.. Finally, ovine AFand NP cells were used in this study,but because of senescence observed in aged and degenerated AFand NP cells (7), an alternative cell source such as mesenchymalstem cells will likely be necessary in the clinic and may performdifferently than the cells chosen for this study. Furthermore, it isunclear how these cells will respond when implanted into the in-flammatory environment of the degenerated disc space (42), whichis not replicated in the current model. Despite these challenges,this work demonstrates important and promising advancementsin our understanding of how engineered IVD develops, integrates,and functions in the native disc space. Furthermore, this model ofTE-TDR has immediate applications in the investigation of howvarious IVD properties (e.g., composition, architecture, perme-ability, cell type, stiffness, energy dissipation, etc.) affect structure-function relationships and pathology in vivo. The ability to intro-duce tissues with controllable AFand NP properties into the nativedisc space, in vivo, allows relationships to be studied that are notcurrently possible in traditional animal or in vitro models.
In summary, this data demonstrates that a tissue-engineeredIVD can be implanted into the caudal spine, remain in place,withstand the mechanical loads, and survive and produce an inte-grated and mechanically functional ECM similar to the nativeIVD. These findings provide support for the development of tis-sue-engineered IVD technologies and evidence that the challengesassociated with TE-TDRmay be overcome. Translating the successof studies in rats to larger animal models will be a key step in mov-ing this technology closer to clinical applications, whereas exploit-ing the rat model can provide valuable insight into in vivo IVDstructure-function relationships and pathology. Overall, this studydemonstrates promising advancements toward the therapeutic ap-plication of TE-TDR and develops a platform to better investigateand understand the IVD and its associated pathology.
MethodsCell Preparation. Cell preparation was based on previously described techni-ques (15, 16). IVDs were dissected out of lumbar region of skeletally mature(∼14 months) Finn/Dorset cross male sheep (Cornell University Sheep Pro-gram). Tissue was washed in PBS (Dulbecco’s PBS; Gibco BRL) and then sepa-rated into AF and NP region. Tissue was dissected into small pieces anddigested in 200 mL of 0.3% wt∕vol collagenase type II at 37 °C for 9 h for AFtissue and 6 h for NP tissue. Digested tissue was filtered through 100 μmnylonmesh (BD Biosciences) and centrifuged at 936 g for 7 min. Cells were countedand seeded at 2;500 cells∕cm2 in culture flasks with Ham’s F-12 media (GibcoBRL) that contained 10% fetal bovine serum, penicillin (Gemini Bio Products),(100 units∕mL), streptomycin (100 μg∕mL), amphotericin B (250 ng∕mL),and ascorbic acid (25 μg∕mL). Cells were cultured at 37 °C, 5% CO2, andnormoxia to confluence with media changes every 3 d. At confluence, cellswere removed from flasks with 0.05% trypsin (Gibco BRL) and counted with ahemocytometer. Cells were then seeded into TE-TDRs.
IVD Fabrication. T2 weighted MRI images and μCT images were obtained ofcaudal 3∕4 disc level (imaging specifics in imaging section). T2 weighted MRIimages were imported in DICOM format to slicOmatic v4.3 (TomoVision) andthe NP was manually segmented and converted to point cloud images ofthe NP. Point cloud images were converted to surface and solid models inStudio 4.0 (Geomagic Inc.). This process resulted in a model containing thedimensions and shape of the NP (Fig. 1A).
μCT images were converted to DICOM format and imported into slicO-matic v4.3 (TomoVision) where the boney surfaces of the vertebral bodieswere segmented to obtain the overall shape and dimensions of the caudal3∕4 disc space. The μCT-derived dimensions of the disc space were thencombined with the MRI-derived NP model to obtain the target dimensionsof the TE-TDR implant (Fig. 1A).
TE-TDR implant of target dimensions was created using contracted col-lagen (AF)/alginate (NP) technique (Fig. 1B) (15). MRI-derived NP surfaceand solid model was transferred into SolidWorks to create an injection moldof NP. The Injection mold was 3-D printed of acrylonitrile butadiene styreneplastic on FDM 3,000 machine (Stratasys).
Three percent (wt∕vol) low viscosity grade alginate (FMC BioPolymer)seeded with 25 × 106 NP cells∕mL was mixed with 0.02 g∕mL CaSO4 (Sigma-Aldrich) to crosslink the alginate, and injected into the NP mold. Cell-seededalginate NP was then removed from molds and placed in the center of a well
of a 24 well plate. Collagen type I was obtained from rat-tail tendon (SpragueDawley, 7–8-wk old) (Pel-Freez Biologicals) using established protocols (15,43). One or two milligrams per millileter collagen gel solution seeded with1 × 106 AF cells∕mL was subsequently poured and gelled around the alginateNP. Constructs were cultured for 2 wk in previously described media whilecollagen gel contracted around aliginate NP to the proper AF dimensions.
Surgery. After 2 wk of in vitro culture, TE-TDR constructs were implantedinto the caudal spine of athymic rats (n ¼ 18). All animal procedures wereperformed in accordance with the guidelines of the Institutional Animal Careand Use Committee of the Hospital for Special Surgery. Rats were anesthe-tized using ketamine (Ketaset, 100 mg∕mL) 80–90 mg∕kg, and xylazine(Rompun, 20 mg∕mL) 5 mg∕kg, which were mixed together and adminis-tered intraperitoneally. If necessary, anesthesia was prolonged by administra-tion of isoflurane via nose cone. A unique method was established to removethe native disc and to prepare the disc space for implant insertion in the tail.The vertebral column was exposed and the native IVD (caudal 3∕4) removed.Upon removal, the caudal 3 and caudal 4 vertebral bodies were minimallyretracted to allow the insertion of the engineered disc into the disc space.The disc space was released to press-fit the implant in place and woundclosure was performed in layers. An initial dose of 0.01–0.05 mg∕kg bupre-norphine (Buprenex) was administered intraoperatively or immediately post-operatively prior to anesthetic recovery. Buprenorphine treatments wereperformed for 2 d postoperatively.
In addition to TE-TDR implants, two control groups were studied. Thediscectomy group followed the above procedure and removed the native discbut implanted nothing back into the disc space (n ¼ 12). The reimplantationgroup followed the above procedure, removed the native IVD and thenreimplanted that native IVD back into the disc space (n ¼ 12).
After implantation, rats were maintained up to 6 mo. MRI images weretaken of all three groups at 6 wk (n ¼ 12∕group) and 6 mo (n ¼ 12∕group)and analyzed for disc height. In the TE-TDR group, 12 animals were sacrificedat 6 mo and analyzed for histology (n ¼ 6), mechanics (n ¼ 6), and biochem-istry (n ¼ 6). In addition, a smaller cohort of six animals was sacrificed at6 wk for histology. The two control groups were taken out to 6 mo. The re-implantation group was analyzed for histology (n ¼ 6), mechanics (n ¼ 6), andbiochemistry (n ¼ 6). The discectomy group was analyzed for histology (n ¼ 6)but not biochemistry and mechanics due to the lack of tissue in the disc space.
Imaging. μCT images of rat caudal spine were obtained from caudal 3 tocaudal 5 vertebrae on a Scanco μCT 35 system (Scanco Medical) with an iso-tropic resolution of 30 μm.
MRI images were obtained on a 7.0 Tesla Bruker 70∕30 MagneticResonance Imaging (Bruker Biospin) system. Rats were anesthetized with1.5% Isoflurane during imaging procedures. A high-resolution T1-weightedflash sequence (resolution: 78.1 um × 58.6 um × 1 mm) was obtained for discspace measurements at 6 wk and 6 mo and a T2-weighted sequence (resolu-tion: 104.2 um × 78.1 um × 1 mm) was obtained for implant design and at6 wk and 6 mo post implantation.
Histology. Spines and bone samples were cleaned of muscle and preservedin 10% phosphate-buffered formalin and were fixed at room temperaturefor 2 d. After an overnight running water rinse, samples were decalcifiedin 10% EDTA in 0.05 M Tris buffer, pH 7.4, until bone was soft and flexible.An overnight running water rinse was conducted in a VIP tissue processor toparaffin. Embedded samples were sectioned at 5 μm thickness and subse-quently stained with alcian blue for proteoglycans, picrosirius red stainingfor collagen, and hemotoxylin and eosin.
Biomechanics. TE-TDR motion segments and intact native motion segmentswere both cleaned of surrounding tissue to result in bone-disc-bone motionsegments after sacrificing the animals at 6 mo. Prepared motion segmentswere mounted on ELF 3,200 mechanical testing frame (EnduraTech) usingmodified microvices (McMaster-Carr) (27). Unconfined stress-relaxation testswere performed at 5% strain incremental steps to a total of 20% strain. Equi-librium modulus and permeability were calculated by fitting resulting stres-ses to a poroelastic model (35). In addition, motion segments were subjectedto a sinusoidal dynamic frequency sweep from 0.01–10 Hz at �3% strainaround zero strain. Apparent modulus and percent hysteresis were calculatedfrom dynamic data. All data analysis was performed using Matlab software.
Biochemistry. Native IVD and TE-TDR tissue were both dissected out of discspace using a scalpel. For the native IVD, NP and AF tissue were separated andtested individually. For the TE-TDR tissue, the representative NP region at thecenter of the tissue was removed using a 2-mm biopsy punch and tested as NP
13110 ∣ www.pnas.org/cgi/doi/10.1073/pnas.1107094108 Bowles et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 5
, 202
1

and the surrounding AF region was tested as AF. Tissues were analyzed forglycosaminoglycan content using a modified dimethylmethylene blue assay(31), total collagen using the hydroxyproline assay (33), and DNA using theHoechst dye assay (32). All data were normalized to wet weight.
Disc Measurements. Images were taken of all engineered IVD immediatelyprior to implantation along with pictures of the fully intact explanted nativeIVD being replaced. Size measurements along the lateral and ventral-dorsalplane of both the engineered and native IVD were calculated using Image Jsoftware (National Institutes of Health). Measurements of engineered IVD at6 mo after implantation were calculated from MRI images.
Statistical Analysis. All statistical analysis was performed using two-factorANOVA and Tukey post hoc test. Data represented as mean� standarddeviation. P values <0.05 are considered statistically significant.
ACKNOWLEDGMENTS We thank Stephen Doty, PhD for his technical supporton the histology and immunohistochemistry. We also thank Jonathan Dyke,PhD and Douglas Ballon, PhD for their technical support on the MRI aspectsof this work. Finally, we thank Tatianna Saleh for her help with daily animalcare and logistics. This work is supported by a grant through AOSpineNorth America, AO Research Fund Grant F-08-10B, the AOSpine InternationalHansjörg Wyss Focus Award 2010, and a grant from NFL Medical Charities.
1. Ehrlich GE (2003) Low back pain. Bull WHO 81:671–676.2. Kelsey JL, White AA, III (1980) Epidemiology and impact of low-back pain. Spine
5:133–142.3. Yasuma T, Koh S, Okamura T, Yamauchi Y (1990) Histological changes in aging lumbar
intervertebral discs. Their role in protrusions and prolapses. J Bone Jt Surg 72:220–229.4. Kuslich SD, Ulstrom CL, Michael CJ (1991) The tissue origin of low back pain and
sciatica: A report of pain response to tissue stimulation during operations on thelumbar spine using local anesthesia. Orthop Clin N Am 22:181–187.
5. O’Neill CW, Kurgansky ME, Derby R, Ryan DP (2002) Disc stimulation and patterns ofreferred pain. Spine 27:2776–2781.
6. Lotz JC, Ulrich JA (2006) Innervation, inflammation, and hypermobility may character-ize pathologic disc degeneration: Review of animal model data. J Bone Jt Surg 88(Suppl 2):76–82.
7. Gruber HE, Ingram JA, Norton HJ, Hanley EN, Jr. (2007) Senescence in cells of the agingand degenerating intervertebral disc: Immunolocalization of senescence-associatedbeta-galactosidase in human and sand rat discs. Spine (Philadelphia) 32:321–327.
8. Hadjipavlou AG, Tzermiadianos MN, Bogduk N, Zindrick MR (2008) The pathophysiol-ogy of disc degeneration: A critical review. J Bone Jt Surg Br Vol 90-B:1261–1270.
9. Masuda K, Lotz JC New challenges for intervertebral disc treatment using regenera-tive medicine. Tissue Eng Part B 16:147–158.
10. Chiu JC, Clifford T, Princenthal R, Shaw S (2005) Junctional disc herniation syndrome inpost spinal fusion treated with endoscopic spine surgery. Surg Technol Int 14:305–315.
11. Harrop JS, et al. (2008) Lumbar adjacent segment degeneration and disease afterarthrodesis and total disc arthroplasty. Spine (Philadelphia) 33:1701–1707.
12. Botelho RV, Moraes OJ, Fernandes GA, Buscariolli Ydos S, Bernardo WM A systematicreview of randomized trials on the effect of cervical disc arthroplasty on reducingadjacent-level degeneration. Neurosurg Focus 28:E5.
13. Bartels RH, Donk R, Verbeek AL No justification for cervical disk prostheses in clinicalpractice: Ameta-analysis of randomized controlled trials.Neurosurgery 66:1153–1160.
14. O’Halloran DM, Pandit AS (2007) Tissue-engineering approach to regenerating theintervertebral disc. Tissue Eng 13:1927–1954.
15. Bowles RD, Williams RM, Zipfel WR, Bonassar LJ (2010) Self-assembly of alignedtissue-engineered annulus fibrosus and intervertebral disc composite via collagengel contraction. Tissue Eng 16:1339–1348.
16. Mizuno H, et al. (2004) Tissue-engineered composites of anulus fibrosus and nucleuspulposus for intervertebral disc replacement. Spine 29:1290–1297.
17. Mizuno H, et al. (2006) Biomechanical and biochemical characterization of compositetissue-engineered intervertebral discs. Biomaterials 27:362–370.
18. Nerurkar NL, Sen S, Huang AH, Elliott DM, Mauck RL Engineered disc-like angle-plystructures for intervertebral disc replacement. Spine (Philadelphia) 35:867–873.
19. Nesti LJ, et al. (2008) Intervertebral disc tissue engineering using a novel hyaluronicacid-nanofibrous scaffold (HANFS) amalgam. Tissue Eng 14:1527–1537.
20. Ruan D, et al. (2007) Intervertebral disc transplantation in the treatment of degenera-tive spine disease: A preliminary study. Lancet 369:993–999.
21. Bowles RD, et al. (2011) Image-based tissue engineering of a total intervertebraldisc replacement for restoration of function to the rat lumbar spine. NMR Biomed,10.1002/nbm.1651.
22. Ballyns JJ, et al. (2009) An optical method for evaluation of geometric fidelity foranatomically shaped tissue engineered constructs. Tissue Eng Part C 16:693–703.
23. Ballyns JJ, et al. (2008) Image-guided tissue engineering of anatomically shapedimplants via MRI and micro-CT using injection molding. Tissue Eng 14:1195–1202.
24. Cheah CM, Chua CK, Leong KF, Cheong CH, NaingMW (2004) Automatic algorithm forgenerating complex polyhedral scaffold structures for tissue engineering. Tissue Eng10:595–610.
25. Sun W, Starly B, Darling A, Gomez C (2004) Computer-aided tissue engineering:Application to biomimetic modeling and design of tissue scaffolds. Biotechnol ApplBiochem 39:49–58.
26. Van Cleynenbreugel T, Van Oosterwyck H, Vander Sloten J, Schrooten J (2002) Trabe-cular bone scaffolding using a biomimetic approach. J Mater Sci 13:1245–1249.
27. Elliott DM, Sarver JJ (2004) Young investigator award winner: Validation of the mouseand rat disc as mechanical models of the human lumbar disc. Spine (Philadelphia)29:713–722.
28. Stokes IA, Aronsson DD, Spence H, Iatridis JC (1998) Mechanical modulation of inter-vertebral disc thickness in growing rat tails. J Spinal Disord 11:261–265.
29. Espinoza Orias AA, Malhotra NR, Elliott DM (2009) Rat disc torsional mechanics: Effectof lumbar and caudal levels and axial compression load. Spine J 9:204–209.
30. Luk KD, Ruan DK (2008) Intervertebral disc transplantation: A biological approach tomotion preservation. Eur Spine J 17(Suppl 4):504–510.
31. Enobakhare BO, Bader DL, Lee DA (1996) Quantification of sulfated glycosamino-glycans in chondrocyte/alginate cultures, by use of 1,9-dimethylmethylene blue. AnalBiochem 243:189–191.
32. Kim YJ, Sah RL, Doong JY, Grodzinsky AJ (1988) Fluorometric assay of DNA in cartilageexplants using Hoechst 33258. Anal Biochem 174:168–176.
33. Neuman RE, Logan MA (1950) The determination of hydroxyproline. J Biol Chem184:299–306.
34. Broberg KB (1983) On the mechanical behavior of intervertebral discs. Spine8:151–165.
35. Kim YJ, Bonassar LJ, Grodzinsky AJ (1995) The role of cartilage streaming potential,fluid flow and pressure in the stimulation of chondrocyte biosynthesis during dynamiccompression. J Biomech 28:1055–1066.
36. Shirazi-Adl A, Taheri M, Urban JP Analysis of cell viability in intervertebral disc: Effectof end plate permeability on cell population. J Biomech 43:1330–1336.
37. Iatridis JC (2009) Tissue engineering: Function follows form. Nat Mater 8:923–924.38. Nerurkar NL, Elliott DM, Mauck RL Mechanical design criteria for intervertebral disc
tissue engineering. J Biomech 43:1017–1030.39. Hutton WC, et al. (1999) The effect of hydrostatic pressure on intervertebral disc
metabolism. Spine 24:1507–1515.40. Wang DL, Jiang SD, Dai LY (2007) Biologic response of the intervertebral disc to static
and dynamic compression in vitro. Spine 32:2521–2528.41. Bibby SR, Jones DA, Lee RB, Yu J, Urban JPG (2001) The pathophysiology of the
intervertebral disc. Jt Bone Spine 68:537–542.42. Le Maitre CL, Hoyland JA, Freemont AJ (2007) Catabolic cytokine expression in degen-
erate and herniated human intervertebral discs: IL-1beta and TNFalpha expressionprofile. Arthritis Res Ther 9:R77, doi: 10.1186/ar2275.
43. Elsdale T, Bard J (1972) Collagen substrata for studies on cell behavior. J Cell Biol54:626–637.
Bowles et al. PNAS ∣ August 9, 2011 ∣ vol. 108 ∣ no. 32 ∣ 13111
BIOPH
YSICSAND
COMPU
TATIONALBIOLO
GY
ENGINEE
RING
Dow
nloa
ded
by g
uest
on
Mar
ch 5
, 202
1