Embed Size (px)
Citation preview

TitleAlcohol Consumption and Multiple Dysplastic LesionsIncrease Risk of Squamous Cell Carcinoma in the Esophagus,Head, and Neck.
Author(s)
Katada, Chikatoshi; Yokoyama, Tetsuji; Yano, Tomonori;Kaneko, Kazuhiro; Oda, Ichiro; Shimizu, Yuichi; Doyama,Hisashi; Koike, Tomoyuki; Takizawa, Kohei; Hirao, Motohiro;Okada, Hiroyuki; Yoshii, Takako; Konishi, Kazuo;Yamanouchi, Takenori; Tsuda, Takashi; Omori, Tai;Kobayashi, Nozomu; Shimoda, Tadakazu; Ochiai, Atsushi;Amanuma, Yusuke; Ohashi, Shinya; Matsuda, Tomonari;Ishikawa, Hideki; Yokoyama, Akira; Muto, Manabu
Citation Gastroenterology (2016)
Issue Date 2016-08-01
URL http://hdl.handle.net/2433/216918
Right© 2016 by the AGA Institute. Published by Elsevier Inc. Thisis an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Type Journal Article
Textversion publisher
Kyoto University

Alcohol Consumption and Multiple Dysplastic LesionsIncrease Risk of Squamous Cell Carcinoma in the Esophagus,Head, and NeckQ2
Q23 Chikatoshi Katada,1 Tetsuji Yokoyama,2 Tomonori Yano,3 Kazuhiro Kaneko,3 Ichiro Oda,4
Yuichi Shimizu,5 Hisashi Doyama,6 Tomoyuki Koike,7 Kohei Takizawa,8 Motohiro Hirao,9
Hiroyuki Okada,10 Takako Yoshii,11 Kazuo Konishi,12 Takenori Yamanouchi,13
Takashi Tsuda,14 Tai Omori,15 Nozomu Kobayashi,16 Tadakazu Shimoda,17 Atsushi Ochiai,18
Yusuke Amanuma,19 Shinya Ohashi,19 Tomonari Matsuda,20 Hideki Ishikawa,21
Akira Yokoyama,22 and Manabu Muto19
1Department of Gastroenterology, Kitasato University School of Medicine, Sagamihara, Japan; 2Department of HealthPromotion, National Institute of Public Health, Wako, Japan; 3Department of Gastroenterology, Endoscopy Division, NationalCancer Center Hospital East, Kashiwa, Japan; 4Endoscopy Division, National Cancer Center Hospital, Tokyo, Japan;5Department of Gastroenterology, Hokkaido University Graduate School of Medicine, Sapporo, Japan; 6Department ofGastroenterology, Ishikawa Prefectural Central Hospital, Kanazawa, Japan; 7Division of Gastroenterology, Tohoku UniversityGraduate School of Medicine, Sendai, Japan; 8Division of Endoscopy, 17Division of Diagnostic Pathology, Shizuoka CancerCenter, Shizuoka, Japan; 9Department of Surgery, National Hospital Organization, Osaka National Hospital, Osaka, Japan;10Department of Gastroenterology and Hepatology, Okayama University Graduate School of Medicine, Dentistry andPharmaceutical Sciences, Okayama, Japan; 11Department of Gastroenterology, Kanagawa Cancer Center, Yokohama, Japan;12Division of Gastroenterology, Department of Medicine, Showa University School of Medicine, Tokyo, Japan; 13Department ofGastroenterology, Kumamoto Regional Medical Center, Kumamoto, Japan; 14Department of Clinical Oncology, St. MariannaUniversity School of Medicine, Kawasaki, Japan; 15Department of Endoscopy Center, Kawasaki Municipal Kawasaki Hospital,Kawasaki, Japan; 16Department of Diagnostic Imaging, Tochigi Cancer Center, Utsunomiya, Japan; 18Division of Pathology,National Cancer Center Hospital and Hospital East, Tokyo, Japan; 19Department of Therapeutic Oncology, Kyoto UniversityGraduate School of Medicine, Kyoto, Japan; 20Research Center for Environmental Quality Management, Kyoto University,Otsu, Japan; 21Department of Molecular-Targeting Cancer Prevention, Kyoto Prefectural University of Medicine, Kyoto, Japan;22Clinical Research Unit, National Hospital Organization Kurihama Medical and Addiction Center, Yokosuka, Japan
BACKGROUND & AIMS: Some patients develop multiplesquamous cell carcinomas (SCCs) in the upper aerodigestivetract, attributed to field cancerization; alcohol consumption hasbeen associated with this process. We examined the associationbetween multiple areas of dysplastic squamous epithelium withthe development of SCC of the esophagus or head and neckcancer, as well as alcohol consumption and smoking.METHODS: We examined 331 patients with early stageesophageal SCC using Lugol chromoendoscopy to evaluate thedysplastic squamous epithelium in the esophagus. Patients thenwere assigned to 3 groups, based on the number of Lugol-voiding lesions: A, no lesion; B, 1–9 lesions; or C, 10 or morelesions. Participants completed lifestyle surveys on their his-tory of drinking, smoking, and diet. All participants wereevaluated by laryngopharyngoscopy before registration; onlythose without head and neck cancer were included, except forpatients with superficial SCC limited to the subepithelial layer.Lesions detected in the esophagus and head and neck by sur-veillance were considered to be metachronous. The study endpoint was the cumulative incidence of metachronous SCCs inthe esophagus and head and neck after endoscopic resection ofesophageal SCC, according to the grade of Lugol-voiding lesions.At study entry, all patients were instructed to abstain fromalcohol and smoking. RESULTS: Over the 2-year study period,metachronous SCCs of the esophagus were detected in 4% ofpatients in group A, in 9.4% of patients in group B, and in24.7% of patients in group C (P < .0001 for patients in group Avs B or B vs C). Head and neck SCCs were detected in none of
the patients in group A, in 1.7% of the patients in group B, andin 8.6% of the patients in group C (P ¼ .016 for patients ingroup A vs C and P ¼ .008 for patients in group B vs C). SCC ofthe esophagus or head and neck developed in 4.0% of patientsin group A, in 10.0% of patients in group B, and in 31.4% ofpatients in group C (P < .0001 for group A vs B or A vs C).Alcohol abstinence decreased the risk of multiple SCCs of theesophagus (adjusted hazard ratio, 0.47, 95% confidence inter-val, 0.25–0.91; P ¼ .025), whereas smoking abstinence did not.CONCLUSIONS: Multiple dysplastic lesions in the esophagusincrease the risk of multiple SCCs. Alcohol abstinence reducesthe risk of metachronous SCCs. Clinical Trials registry:UMIN000001676 and UMIN000005466.
Keywords: Drinking Alcohol; Carcinogenesis; Risk Factor; Ge-netics Methods.
Abbreviations used in this paper: ALDH2, aldehyde dehydrogenase-2; CI,confidence interval; EMR, endoscopic mucosal resection; ESD, endo-scopic submucosal dissection; LVL, Lugol voiding lesion; RR, relative risk;SCC, squamous cell carcinoma.
© 2016 by the AGA Institute. Published by Elsevier Inc. This is an openaccess article under the CC BY-NC-ND license (http://creativecommons.
org/licenses/by-nc-nd/4.0/).0016-5085
http://dx.doi.org/10.1053/j.gastro.2016.07.040
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
Gastroenterology 2016;-:1–10
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
CLINICAL
AT

Q6 Q7Q8 Synchronous and metachronous development of
squamous cell carcinoma (SCC) in the upper aero-digestive tract including the esophagus and the headand neck region has been referred to as the phenomenonof “field cancerization”1 and adversely affects patient sur-vival.2 Recent endoscopic imaging technology such asnarrow-band imaging can detect early SCC, and minimallyinvasive endoscopic treatment can achieve cure andorgan preservation.3–6 Conversely, cancer survivors aftercurative treatment are at risk for the development ofmetachronous multiple SCCs in the preserved organ.However, little is known about the interval from the firstSCC to the metachronous SCC and the risk of metachronousSCC.
Squamous dysplasia has been believed to be a preneo-plastic lesion of SCC, and it is identified easily as Lugol-voiding lesions (LVL) on Lugol chromoendoscopy.7,8 Somepatients with esophageal SCCs have multiple LVLs in thebackground esophageal mucosa.9–13 However, prospectivedata on the association between the grade of LVL and therisk of metachronous SCC are lacking. In addition, mutationof the TP53 gene in the background esophageal mucosa wasshown as an early event of esophageal carcinogenesis.Moreover, TP53 gene mutations were detected even in themicroscopically normal epithelium.14 However, data on theassociation between the grade of LVL and TP53 status alsoare lacking. Follow-up data on LVL might provide importantinformation about the risk of metachronous SCC.
Although field cancerization is associated closely withalcohol consumption and insufficient alcohol meta-bolism,15,16 the benefit of alcohol abstinence on the fieldcancerization phenomenon remains unclear. In this study,we evaluated the cumulative incidence of metachronousmultiple SCCs in the esophagus and the head and neckregion according to the grade of LVL, as well as the riskfactors of metachronous multiple SCCs and the effect ofalcohol and smoking abstinence on field cancerization.
MethodsStudy Design
From September 2005 through May 2010, we prospectivelyrecruited patients from 16 hospitals throughout Japan. Thiscohort study was approved by the institutional review boardat each hospital, and we obtained written informed consentfrom all patients (UMINQ9 Clinical Trials Registry ID:UMIN000001676). The genetic analysis also was approvedby the Institutional Review Board of Kyoto University Hospital,and all participants provided written informed consent (UMINClinical Trials Registry ID: UMIN000005466).
Study PopulationInclusion criteria of this cohort study were as follows: (1)
newly diagnosed early SCC of the esophagus; (2) completeendoscopic resection by endoscopic mucosal resection (EMR)or endoscopic submucosal dissection (ESD); (3) tumor-negativevertical margins of resected specimens; (4) tumor invasionlimited to the mucosa on histopathologic examination ofresected specimens; (5) no additional treatment (surgical
resection, radiotherapy, chemotherapy, and so forth) immedi-ately after EMR or ESD; (6) no active head and neck cancer; (7)patients were evaluated by their attending physicians to be ingood general condition, allowing at least 2 years of follow-upevaluation; and (8) written informed consent obtained fromthe patient. Exclusion criteria were as follows: (1) a history ofchemotherapy for any other cancer or a history of surgicaltreatment or radiotherapy for head and neck cancer; (2) ahistory of iodine allergy; and (3) patients whom the investi-gator considered unsuitable as subjects.
We also prospectively examined TP53 mutations in thebackground esophageal mucosa in other patients with earlyesophageal SCC who were treated at Kyoto University Hospital.
Grading of LVLLVL was graded according to the number of LVLs per
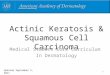
endoscopic view (A, no lesions; B, 1–9 lesions; C, �10 lesions)(Figure 1). Endoscopic images obtained from eligible patients atstudy entry were reviewed centrally in a blinded fashion by 3endoscopists to determine the grade of LVL.
Survey of Lifestyle and FlushingReaction After Drinking
At study entry, lifestyle surveys were conducted using aself-administered questionnaire (Supplementary Figure 1). Thehistories of drinking, smoking, and consumption of high-temperature foods, green-yellow vegetables, and fruit weredocumented carefully. The same questionnaire was used toobtain detailed information on each subject. Patient reports offacial flushing after drinking alcohol were presumed to bemarkers of insufficient alcohol metabolism owing to inactivealdehyde dehydrogenase-2 (ALDH2) genotype (present Q10andpast flushing and never flushing were indicative of activeALDH2).17
Definition of Synchronous andMetachronous Cancer
All candidates were surveyed by laryngoscopy by anotolaryngologist to confirm whether they had synchronousmultiple cancers in the head and neck region before registra-tion. The surveillance interval was within 6 months. Only pa-tients without active head and neck cancer were eligible, exceptfor patients with superficial SCCs limited to within the sub-epithelial layer. Lesions detected by surveillance before regis-tration and lesions including the esophagus were defined assynchronous lesions. After registration, all of the patients werefollowed up by a planned schedule according to the protocol. Ifa new lesion was detected at the first follow-up evaluation (3months after registration) or thereafter, such a lesion wasdefined as a metachronous lesion.
Follow-Up ExaminationsEndoscopic examinations of the head and neck, esophagus,
and stomach, as well as Lugol chromoendoscopy, were per-formed at 3-month intervals for up to 6 months after EMR orESD. Subsequently, these examinations were repeated every 6months. The head and neck region was examined by laryn-goscopy by an otolaryngologist at the time of EMR or ESD andat 1-year intervals thereafter.18 In addition to otolaryngologists,
2 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
CLINICALAT

gastrointestinal endoscopists also examined the oropharynxand hypopharynx during surveillance endoscopy.
Alcohol and Smoking AbstinenceAt study entry, the physicians in charge handed a document
describing the importance of alcohol and smoking abstinence toall patients and verbally instructed them to stop drinking andsmoking. At each examination, we surveyed smoking status(nonsmoker or smoker; for smokers, the number of cigarettessmoked per day) and drinking status (nondrinker or drinker;for drinkers, the drinking frequency and amount of alcoholconsumed) by self-reporting and instructed patients not todrink or smoke.
Histologic AnalysisAlthough the diagnosis of invasive SCC did not usually differ
among the pathologists, the diagnosis of high-grade intra-epithelial neoplasia sometimes was discordant. To control thesedifferences, lesions with a diagnosis of high-grade intra-epithelial neoplasia were reviewed centrally in a blindedfashion by 3 pathologists. Lesions present at enrollment as wellas new lesions were examined. Lesions not diagnosed to behigh-grade intraepithelial neoplasia or SCCs on central reviewwere excluded from this analysis.
TP53 Mutation in BackgroundEsophageal Mucosa
Biopsy specimens were taken from noncancerous back-ground esophageal mucosa. Genomic DNA was extracted usingthe Gentra Puregene Tissue Kit protocol (Qiagen, Inc, Hilden,Germany) with several modifications, and a low frequency ofTP53 mutations was detected by deep sequencing of theamplicons by using the TruSeq Amplicon Cancer Panel (Illu-mina, Inc, San Diego, CA) to sequence mutational hotspots. Thiscancer panel includes hotspots of TP53 mutation, but not allTP53 exons. The amplicon libraries were subjected to massivelyparallel sequencing using MiSeq (Illumina, Inc) with 170-bppaired-end reads. The sequencing data were imported to theCLC Genomics Workbench softwareQ11 (version 6.0.1), and
low-quality data were trimmed by a quality limit of 0.001. Thecleaned-up reads were mapped to the human genome(GRCh37_dbSNP135), and the somatic mutations were detectedby the Quality-based Variant Detection command.
Statistical AnalysisWe examined whether the grade of LVL was associated with
the development of metachronous multiple SCCs in theesophagus and head and neck region. The number of patientsrequired to detect a difference between grades A and B with astatistical power of 80% and a significance level of 5% wasestimated assuming that the cumulative rate of metachronousSCCs in grades A, B, and C, would be 1%, 10%, and 30%,respectively, with a patient ratio of 4:4:2 and a drop-out rate of10%. The total number of patients required was estimated tobe 292. Under these conditions, the statistical power to detect adifference between grades A and C would be 99% or greater(significance level, 5%). The planned number of enrolledpatients was set at 330, taking into account drop-outs andineligible patients.
The Kaplan–Meier method and the log-rank test wereperformed for the analysis of development of a second pri-mary SCC in the esophagus and the head and neck region. Wedefined the time to development from the day of endoscopictreatment to the day of endoscopic diagnosis of a secondprimary SCC. The person-year method was used to calculatethe total number of multiple cancers arising in the esophagusand head and neck per 100 person-years (ie, a patient couldhave multiple events); the Poisson regression analysis wasused to estimate the sex- and age-adjusted Q12relative risk (RR)of all arising events. A Cox proportional-hazards model wasused to estimate the sex- and age-adjusted hazard ratio (RR)and 95% confidence interval (CI) of the primary event. Theanalysis of end points was conducted after the completion ofat least 2 years of follow-up observation for all patients fromthe time of enrollment. Data on patients in whom follow-upexaminations were not completed were censored at the lastobservation. All data were analyzed with SAS Q13(version 9). Allauthors had access to the study data and reviewed andapproved the final manuscript.
print&
web4C=FPO
Figure 1.Grading of LVLs. The number of LVLs per endoscopic view was counted, and the grading was divided into thefollowing 3 categories: (A) group A, no lesions; (B) group B, 1–9 lesions; and (C) group C, 10 or more lesions.
Q1- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 3
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
CLINICAL
AT

ResultsStudy Population
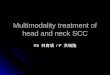
A total of 332 patients with early esophageal SCC wereenrolled. One patient refused to participate in this cohortstudy. The other 331 patients were registered and under-went the preplanned follow-up examinations. One patientwas excluded because the lesion was not diagnosed defini-tively as high-grade intraepithelial neoplasia or invasive SCCon central review of the pathologic assessment (Figure 2).Table 1 summarizes the baseline characteristics of the 330patients according to the grade of LVL. The median follow-up period was 49.4 months (range, 1.3–81.2 mo). The pro-portion of men was higher in the more severe LVL grades(62.0%, 85.1%, and 93.4%, respectively; P < .0001 for A orB vs C). The largest subgroup according to age was 60 to 69years in grade C and 70 years or older in grades A and B.After adjusting for sex and age, the LVL grade was associ-ated with progressively higher proportions of heavydrinkers (27.7%, 26.2%, and 52.8%, respectively; P < .0001for trend, vs others), heavy smokers (41.1%, 65.9%, and71.0%, respectively; P < .0001 for trend), not eating green-yellow vegetables almost every day (52.0%, 54.9%, and71.3%, respectively; P ¼ .021 for trend), and patients with alow body mass index (23.4%, 32.0%, and 37.4%, respec-tively; P ¼ .027 for trend).
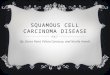
Primary and Secondary OutcomesLVL grade was associated with progressive increases in
the 2-year cumulative incidence of metachronous multipleSCCs (esophagus: 4.0%, 9.4%, and 24.7%, respectively;P < .0001 for A or B vs C; head and neck region: 0.0%, 1.7%,and 8.6%, respectively; P ¼ .016 for A vs C and P ¼ .008 forB vs C; both: 4.0%, 10.0%, and 31.4%, respectively; P <.0001 for A or B vs C) (Figure 3).
LVL grade was associated with progressive increases inthe total number of metachronous multiple SCCs per 100person-years (esophagus: RR, 1.91 and 7.41 for grades B andC, respectively, vs grade A; P < .0001 for trend; head andneck region: RR, 0.00 and 5.74 for grades A and C, respec-tively, vs grade B; P < .0001 for trend; both: RR, 2.19 and9.05 for grades B and C, respectively, vs grade A; P < .0001for trend) (Table 2). The frequency of events was notablyhigh in grade C (18.9, 5.8, and 24.7 per 100 person-years inesophagus, head and neck region, and both, respectively).
Grade C LVL was the most significant predictor ofmetachronous multiple SCCs on analysis with a univariateor multivariate Cox proportional-hazards model (esoph-agus: multivariate RR, 8.76; 95% CI, 3.02–25.5; for C vs. A;head and neck region: multivariate RR, 3.51; 95% CI,1.34–9.20; for C vs B; both: multivariate RR, 9.78; 95% CI,3.41–28.0; for C vs A) (Table 3). On multivariate analysis, analcohol flushing reaction after drinking was also a predictor
Figure 2. Enrollment andsubjects for analysis.
4 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
CLINICALAT

Table 1.Clinical Characteristics of Patients According to the LVL Grade
LVL grade
A (n ¼ 50) B (n ¼ 174) C (n ¼ 106) P
SexMale, % 62.0% 85.1% 93.4% <.0001Age, y
40–59 22.0% 17.2% 19.8%60–69 36.0% 36.8% 55.7%�70 42.0% 46.0% 24.5% .005 a
Means ± SD 66.4 ± 9.9 67.7 ± 8.6 64.8 ± 6.5 .018 a
Sex- and age-adjusted % or mean
Drinking alcoholb,c
Never/rare 25.9% 7.9% 4.7%Light 13.8% 21.4% 8.9%Moderate 27.8% 30.9% 25.5%Heavyd 27.7% 26.2% 52.8%Ex-drinker 4.7% 13.6% 8.2% <.0001 a
Means ± SEe 10.4 ± 1.8 13.1 ± 0.9 19.9 ± 1.2 <.0001 f
Strong alcoholic beveragesb
Frequently 6.7% 11.8% 12.2%Sometimes 15.1% 20.1% 23.2%Never 78.2% 68.1% 64.6% .17 f
Smoking, pack-yearsb
Never, 0 22.7% 14.8% 12.4%Light, <30 36.2% 19.3% 16.6%Heavy, �30 41.1% 65.9% 71.0% <.0001 f
High-temperature foodb
Likes very much 18.4% 20.8% 20.6%Likes somewhat 24.5% 25.1% 24.0%Neither likes nor dislikes 45.8% 41.8% 36.8%Dislikes somewhat 9.3% 9.9% 15.9%Dislikes very much 2.0% 2.3% 2.7% .81 f
Green-yellow vegetablesb
Seldom 0.0% 3.8% 2.1%1–2 d/mo 3.8% 5.7% 5.5%1–2 d/wk 20.5% 16.5% 35.3%3–4 d/wk 27.7% 29.0% 28.4%Almost every day 48.0% 45.1% 28.7% .021 f
Fruitb
Seldom 11.1% 9.6% 12.8%1–2 d/mo 5.2% 15.2% 12.6%1–2 d/wk 33.4% 22.9% 33.1%3–4 d/wk 26.2% 20.2% 17.0%Almost every day 24.1% 32.0% 24.5% .31 f
Body mass index, kg/m2g
<21.2 23.4% 32.0% 37.4%21.2–23.6 18.8% 37.1% 33.9%�23.7 57.8% 30.9% 28.7% .003 f
Means ± SE 23.5 ± 0.44 22.3 ± 0.24 22.1 ± 0.31 .027 f
Alcohol flushingb
Never flushing 35.2% 31.5% 40.6%Flushingh 64.8% 68.5% 59.4% .12 a
aP for trend across the 3 groups.bPercentage values were adjusted for sex and age by direct method (using all patients as the standard population) andstatistically tested by the Cochran–Mantel–Haenszel test. Mean values were adjusted for sex and age and were statisticallytested by analysis of covariance.cNever/rare, <1 U/wk; light, 1–8.9 U/wk; moderate, 9–17.9 U/wk; heavy, �18 U/wk (1 U ¼ 22 g ethanol).dP < .0001 for trend, vs others.eExcluding ex-drinkers.fP for homogeneity among the 3 groups.gCategorized by the overall tertile. Missing data for 1 patient.hPresent or past flushing.
- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 5
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
599
600
CLINICAL
AT

of metachronous esophageal SCC (RR, 1.07; 95% CI,1.02–2.82) and esophageal and head and neck SCC (RR,1.60; 95% CI, 1.00–2.57). Small or large body mass indexalso was associated with metachronous esophageal SCC (RR,2.09; 95% CI, 1.14–3.83; and RR, 1.86; 95% CI, 1.00–3.47,respectively) and esophageal and head and neck SCC (RR,1.73; 95% CI, 0.99–3.02; and RR, 1.55; 95% CI, 0.88–2.73,respectively).
TP53 Gene Alteration in BackgroundEsophageal Mucosa
To examine whether mutations of genes such as TP53occurred in the noncancerous esophageal mucosa withmultiple LVLs and whether the mutation frequency wasassociated with the severity of LVLs, we performed deepsequencing of the TP53 gene amplicon using biopsy speci-mens of noncancerous esophageal mucosa in patients withor without multiple LVLs. These samples were obtainedfrom 38 early esophageal SCCQ14 cases independent from ourpresent cohort study. The clinical characteristics are sum-marized in Supplementary Tables 1 and 2Q15 , and the detectedlow frequency of TP53 mutations (�2% of total reads) arelisted in Supplementary Table 3. Our study showed that thenumber of cases that had a TP53 mutation was 3 of 7(42.9%) in grade A, 5 of 9 (55.6%) in grade B, and 17 of 22(77.3%) in grade C (Supplementary Figure 2). Of note,several mutations (2–6 mutations) of the TP53 gene werefound simultaneously in biopsy specimens of noncancerousesophageal mucosa in patients with grade C LVL(Supplementary Figure 2). The median mutation frequencyof TP53 genes in biopsy specimens was 0%, 2.0%, and10.1% in grades A, B, and C, respectively. The median ingrade C was significantly higher than that in grade A(P ¼ .04) (Supplementary Figure 3).
Effect of Alcohol and Smoking Abstinence on theDevelopment of Metachronous SCC
As shown in Supplementary Figure 4, 69 (30.9%) of 223patients who drank 1 U/day (22 g of ethanol) or more atbaseline abstained from drinking alcohol, and 69 (53.5%) of129 patients who had smoked at baseline abstained fromsmoking. The cumulative incidence of metachronous
multiple SCCs in the esophagus was shown according to thestatus of drinking alcohol and smoking (Figure 4). Hazardratios were adjusted for sex, age, LVL grade, alcohol intakeat baseline, and alcohol flushing.
Alcohol abstinence decreased the risk of developingmetachronous multiple SCCs of the esophagus (adjustedhazard ratio, 0.47; 95% CI, 0.25–0.91; P ¼ .025) (Figure 4A).The risk reduction was especially large in grade C LVL(adjusted hazard ratio, 0.23; 95% CI, 0.09–0.60; P ¼ .003)(Figure 4B). In contrast, smoking abstinence did notdecrease the risk of developing metachronous multiple SCCsof the esophagus (all: adjusted hazard ratio, 0.59; 95% CI,0.29–1.18; P ¼ .13; grade C LVL: adjusted hazard ratio, 0.73;95% CI, 0.32–1.67; P ¼ .45) (Figure 4C and D, respectively).
DiscussionWe found that patients with grade C LVL were at sig-
nificant risk for the development of metachronous multipleSCCs in the esophagus and the head and neck region.Furthermore, TP53 mutation in the background esophagealmucosa was associated with an increased grade of LVL.These results clearly supported the theory of field cancer-ization in which genetic alteration in the backgroundsquamous epithelium might accumulate and increase thepotential to develop metachronous multiple SCCs. In addi-tion, alcohol abstinence significantly decreased the devel-opment of metachronous SCCs, especially in the patientswith grade C LVL. This result indicates that alcohol absti-nence should be encouraged to reduce the risk of meta-chronous multiple SCCs after curative treatment.
Although the field cancerization phenomenon in theupper aerodigestive tract has been well known for morethan half a century, it has been difficult to detect earlycancer in this region. A randomized controlled trial foundthat narrow-band imaging effectively can detect early SCC inthe esophagus and the head and neck region.3 In patientswith early SCC, organs can be preserved by endoscopiccurative treatment, but the preserved organs are affectedstrongly by the field cancerization phenomenon. Therefore,an effective surveillance strategy after treatment andmethods to prevent metachronous multiple SCCs are neededin survivors of esophageal SCC.
Figure 3. Cumulative incidence of metachronous multiple SCCs according to the LVL grade: (A) esophagus, (B) head and neckregion, and (C) esophagus and head and neck region.
6 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646
647
648
649
650
651
652
653
654
655
656
657
658
659
660
661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
717
718
719
720
CLINICALAT

Data on the interval from the first SCC to the develop-ment of a second primary metachronous SCC have beenlimited, largely because of dismal survival, completeesophageal resection on diagnosis, poor follow-up evalua-tion, and lack of effective surveillance programs. In thisstudy, we focused on patients with early esophageal SCCwho could achieve cure and organ preservation. The fre-quency of events was notably low in grade A. The 2-yearcumulative incidence of metachronous multiple SCCs andthe total number of metachronous multiple SCCs per 100person-years were 4.0%/2.8, 0.0%/0.0, and 4.0%/2.8 in theesophagus, head and neck region, and both, respectively. Onthe other hand, the frequency of events was notably high in
grade C. The 2-year cumulative incidence of metachronousmultiple SCCs and the total number of metachronous mul-tiple SCCs per 100 person-years were 24.7%/18.9, 8.6%/5.8, and 31.4%/24.7 in the esophagus, head and neckregion, and both, respectively. These results indicated thateffective surveillance programs according to the grade ofLVL or effective adjuvant strategies according to the gradeof LVL are required to detect metachronous SCC earlier.
There has been no effective biomarker for the risk of thefield cancerization phenomenon. In this study, we clearlyshowed that an increase in the grade of LVL is associatedclosely with the risk of metachronous SCC. In addition, gradeC LVL and a flushing reaction after drinking alcohol are
Table 2.Person-Years and Number of Primary and All Events According to the Grade of LVL
LVL grade
Total (n ¼ 330)A (n ¼ 50) B (n ¼ 174) C (n ¼ 106)
EsophagusPrimary eventsEvents, n 4 26 44 74Person-years 208.1 652.0 327.1 1187.2Per 100 person-years 1.9 4.0 13.5 6.2RRa 1 2.32 7.68 P < .000195% CI Referent 0.79–6.82 2.64–22.3 for trend
All eventsEvents, n 6 33 85 124Person-years 215.6 703.2 449.9 1368.6Per 100 person-years 2.8 4.7 18.9 9.1RRb 1 1.91 7.41 P < .000195% CI Referent 0.78–4.69 3.12–17.6 for trend
Head and neckPrimary eventsEvents, n 0 6 14 20Person-years 215.6 687.0 407.9 1310.4Per 100 person-years 0.0 0.9 4.1 1.5RRa 0.00 1 3.64 P ¼ .00295% CI Incalculable Referent 1.39–9.52 for trend
All eventsEvents, n 0 7 26 33Person-years 215.6 703.2 449.9 1368.6Per 100 person-years 0.0 1.0 5.8 2.4RRb 0.00 1 5.74 P < .000195% CI Incalculable Referent 0.08–0.40 for trend
Esophagus, head and neckPrimary eventsc
Events, n 4 29 50 83Person-years 208.1 640.0 306.0 1154.1Per 100 person-years 1.9 4.5 16.3 7.2RRa 1 2.48 8.52 P < .000195% CI Referent 0.85–7.19 2.97–24.4 for trend
All eventsd
Events, n 6 40 111 157Person-years 215.6 703.2 449.9 1368.6Per 100 person-years 2.8 5.7 24.7 11.5RRb 1 2.19 9.05 P < .000195% CI Referent 0.91–5.26 3.87–21.2 for trend
aSex- and age-adjusted hazard ratio by Cox proportional-hazards model.bSex- and age-adjusted relative risk by Poisson regression.cEsophagus or head and neck cancer.dEsophagus plus head and neck cancer(s).
- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 7
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736
737
738
739
740
741
742
743
744
745
746
747
748
749
750
751
752
753
754
755
756
757
758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
781
782
783
784
785
786
787
788
789
790
791
792
793
794
795
796
797
798
799
800
801
802
803
804
805
806
807
808
809
810
811
812
813
814
815
816
817
818
819
820
821
822
823
824
825
826
827
828
829
830
831
832
833
834
835
836
837
838
839
840
CLINICAL
AT

predictors of metachronous multiple SCCs. We previouslyreported that multiple LVLs in patients with SCC in theesophagus and the head and neck region was associatedwith ALDH2 inactive genotype and metachronous SCC in theesophagus and the head and neck region.13,19,20 These datamean that cancer survivors with flushing reaction afterdrinking alcohol or multiple LVLs in the background mu-cosa, or both, should be considered as having a higher riskof field cancerization.
A recent meta-analysis showed that the alcohol-relatedrisk of esophageal SCC is reversible after alcohol absti-nence, and 16 years are required until all increased riskdisappears.21 In our study, with a median follow-up periodof only 49.4 months (range, 1.3–81.2 mo), the risk ofmetachronous SCC significantly decreased after alcoholabstinence, especially among the patients with grade C LVL,in whom the hazard ratio decreased to 0.23. These data arevery important for reducing the risk of metachronous SCC incancer survivors who have received curative treatment.
The median follow-up time in our study was 49.4months, which might be too short to draw strong recom-mendations about the value of surveillance intervals.
However, even in this short period, the patients with gradeC LVL had a risk of metachronous multiple SCCs in theesophagus and the head and neck region. This means thatclose surveillance may be required for the patients withesophageal cancer who were treated successfully. Clinically,the grade of LVL on iodine staining of the backgroundmucosa should be evaluated initially. If the grade suggests arisk of cancer, narrow-band imaging should be performed assurveillance for the early detection of cancer.
We showed that the TP53 mutation was seen even innoncancerous lesions in patients with early esophageal SCC,and the frequency of the TP53 mutation was associated withthe severity of LVL grade. We believe these data help explainthe mechanisms of metachronous esophageal carcinogen-esis. In this study, we obtained biopsy samples from Lugol-stained lesions, in which glycogen granules are rich andstructural atypia is not seen. Such mucosa was assumed tobe “non Q16-cancerous” esophageal epithelium.22 However, wecould not exclude the possibility that the greater the num-ber of LVL lesions present in the patient, the more likely thepossibility that biopsy specimens from normal mucosa stillcontain cryptic dysplasia that would not have been detected
Table 3.Predictors of Metachronous Multiple Cancers by Cox Proportional-Hazards Model
Esophagus Head and neck Esophagus or head and neck
UnivariateRR (95% CI)a
MultivariateRR (95% CI)b
Univariate RR(95% CI)a
MultivariateRR (95% CI)b
UnivariateRR (95% CI)a
MultivariateRR (95% CI)b
Grade of LVLsA 1 (ref) 1 (ref) 0.00 (incalculable) 0.00 (incalculable) 1 (ref) 1 (ref)B 2.33 (0.79–6.85) 2.46 (0.84–7.24) 1 (ref) 1 (ref) 2.49 (0.86–7.23) 2.64 (0.91–7.68)C 7.66 (2.64–22.3) 8.76 (3.02–25.5) 3.61 (1.38–9.46) 3.51 (1.34–9.20) 8.51 (2.97–24.4) 9.78 (3.41–28.0)
Drinking alcohol, per þ1 U 1.12 (1.02–1.23) – 1.18 (1.01–1.38) – 1.11 (1.01–1.22) –
Alcohol flushingNever flushing 1 (ref) 1 (ref) 1 (ref) – 1 (ref) 1 (ref)Flushing 1.39 (0.84–2.29) 1.70 (1.02–2.82) 1.29 (0.49–3.37) – 1.30 (0.82–2.07) 1.60 (1.00–2.57)
Strong alcoholic beveragesSometimes/never 1 (ref) – 1 (ref–) – 1 (ref) –
Frequently 0.95 (0.45–1.99) – 1.17 (0.34–4.05) – 1.07 (0.55–2.08) –
Smoking, pack-yearsNever/light (<30) 1 (ref) – 1 (ref) – 1 (ref) –
Heavy (�30) 1.12 (0.66–1.92) – 1.80 (0.57–5.66) – 1.15 (0.69–1.91) –
High-temperature foodLikes very much 1.04 (0.57–1.90) – 0.93 (0.27–3.20) – 1.09 (0.62–1.92) –
Others 1 (ref) – 1 (ref) – 1 (ref) –
Green-yellow vegetablesAlmost every day 0.77 (0.46–1.26) – 0.59 (0.21–1.68) – 0.64 (0.39–1.03) –
Others 1 (ref) – 1 (ref) – 1 (ref) –
FruitAlmost every day 0.46 (0.24–0.87) 0.42 (0.22–0.82) 0.32 (0.07–1.45) 0.32 (0.07–1.43) 0.43 (0.23–0.81) 0.39 (0.21–0.74)Others 1 (ref) 1 (ref) 1 (ref) 1 (ref) 1 (ref) 1 (ref)
Body mass index, kg/m2
<21.2 2.06 (1.13–3.75) 2.09 (1.14–3.83) 1.29 (0.46–3.60) – 1.65 (0.95–2.85) 1.73 (0.99–3.02)21.2–23.6 1 (ref) 1 (ref) 1 (ref) – 1 (ref) 1 (ref)�23.7 1.59 (0.86–2.94) 1.86 (1.00–3.47) 0.67 (0.21–2.13) – 1.33 (0.76–2.33) 1.55 (0.88–2.73)
NOTE. One patient with missing data for body mass index was excluded (n ¼ 329).–, Not selected (P � .15). Sex and age also were adjusted but are not shown in the table.aSex- and age-adjusted RR for each variable.bVariables were selected from all the variables listed above Q18by the stepwise procedure with P < .15 for entry and removal, andthe relative risks were shown for the selected variables.
8 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
841
842
843
844
845
846
847
848
849
850
851
852
853
854
855
856
857
858
859
860
861
862
863
864
865
866
867
868
869
870
871
872
873
874
875
876
877
878
879
880
881
882
883
884
885
886
887
888
889
890
891
892
893
894
895
896
897
898
899
900
901
902
903
904
905
906
907
908
909
910
911
912
913
914
915
916
917
918
919
920
921
922
923
924
925
926
927
928
929
930
931
932
933
934
935
936
937
938
939
940
941
942
943
944
945
946
947
948
949
950
951
952
953
954
955
956
957
958
959
960
CLINICALAT

by Lugol staining alone. In addition, we could not addressthe difference regarding TP53 mutations between the pri-mary lesion and the noncancerous background esophagealmucosa because we did not obtain DNA samples from pri-mary lesions. Moreover, we could not assess whether thedifferent TP53 mutations identified in the same case werederived from monoclonal or polyclonal origin. These limi-tations should be clarified further in future studies.
In conclusion, the grade of LVL is a useful predictor ofthe risk of metachronous multiple SCCs arising in theesophagus and the head and neck region in survivors ofesophageal cancer. Alcohol abstinence is required to reducethe risk of metachronous multiple SCCs in the esophagus.
Supplementary MaterialNote: To access the supplementary material accompanyingthis article, visit the online version of Gastroenterology atwww.gastrojournal.org, and at http://dx.doi.org/10.1053/j.gastro.2016.07.040.
References1. Slaughter DP, Southwick HW, Smejkal W. “Field can-
cerization” in oral stratified epithelium. Cancer 1953;6:963–968.
2. Matsubara T, Yamada K, Nakagawa A. Risk of secondprimary malignancy after esophagectomy for squamouscell carcinoma of the thoracic esophagus. J Clin Oncol2003;21:4336–4341.
3. Muto M, Minashi K, Yano T, et al. Early detection ofsuperficial squamous cell carcinoma in the head andneck region and esophagus by narrow band imaging: amulticenter randomized controlled trial. J Clin Oncol2010;28:1566–1572.
4. Katada C, Tanabe S, Koizumi W, et al. Narrow bandimaging for detecting superficial squamous cell carci-noma of the head and neck in patients with esophagealsquamous cell carcinoma. Endoscopy 2010;42:185–190.
5. Higuchi K, Tanabe S, Azuma M, et al. A phase II study ofendoscopic submucosal dissection for superficialesophageal neoplasms (KDOG 0901). GastrointestEndosc 2013;78:704–710.
Figure 4. Cumulative inci-dence of metachronousmultiple esophageal SCCsaccording to the status ofdrinking alcohol andsmoking. (A) All patientsaccording to the status ofdrinking alcohol. (B) Pa-tients with grade C LVLaccording to the status ofdrinking alcohol. (C) Allpatients according to thestatus of smoking. (D) Pa-tients with grade C LVLaccording to the status ofsmoking.
- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 9
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
961
962
963
964
965
966
967
968
969
970
971
972
973
974
975
976
977
978
979
980
981
982
983
984
985
986
987
988
989
990
991
992
993
994
995
996
997
998
999
1000
1001
1002
1003
1004
1005
1006
1007
1008
1009
1010
1011
1012
1013
1014
1015
1016
1017
1018
1019
1020
1021
1022
1023
1024
1025
1026
1027
1028
1029
1030
1031
1032
1033
1034
1035
1036
1037
1038
1039
1040
1041
1042
1043
1044
1045
1046
1047
1048
1049
1050
1051
1052
1053
1054
1055
1056
1057
1058
1059
1060
1061
1062
1063
1064
1065
1066
1067
1068
1069
1070
1071
1072
1073
1074
1075
1076
1077
1078
1079
1080
CLINICAL
AT

6. Muto M, Satake H, Yano T, et al. Long-term outcome oftransoral organ-preserving pharyngeal endoscopicresection for superficial pharyngeal cancer. GastrointestEndosc 2011;74:477–484.
7. Muto M, Hitomi Y, Ohtsu A, et al. Association of aldehydedehydrogenase 2 gene polymorphism with multipleoesophageal dysplasia in head and neck cancer patients.Gut 2000;47:256–261.
8. Yokoyama A, Hirota T, Omori T, et al. Development ofsquamous neoplasia in esophageal iodine-unstainedlesions and the alcohol and aldehyde dehydrogenasegenotypes of Japanese alcoholic men. Int J Cancer2012;130:2949–2960.
9. Muto M, Hironaka S, Nakane M, et al. Association ofmultiple Lugol-voiding lesions with synchronous andmetachronous esophageal squamous cell carcinoma inpatients with head and neck cancer. Gastrointest Endosc2002;56:517–521.
10. Shimizu Y, Tsukagoshi H, Fujita M, et al. Head and neckcancer arising after endoscopic mucosal resection forsquamous cell carcinoma of the esophagus. Endoscopy2003;35:322–326.
11. Urabe Y, Hiyama T, Tanaka S, et al. Metachronousmultiple esophageal squamous cell carcinomas andLugol-voiding lesions after endoscopic mucosal resec-tion. Endoscopy 2009;41:304–309.
12. Hori K, Okada H, Kawahara Y, et al. Lugol-voidinglesions are an important risk factor for a second primarysquamous cell carcinoma in patients with esophagealcancer or head and neck cancer. Am J Gastroenterol2011;106:858–866.
13. Katada C, Muto M, Nakayama M, et al. Risk of superficialsquamous cell carcinoma developing in the head andneck region in patients with esophageal squamous cellcarcinoma. Laryngoscope 2012;122:1291–1296.
14. Mandard AM, Hainaut P, Hollstein M. Genetic steps inthe development of squamous cell carcinoma of theesophagus. Mutat Res 2000;462:335–342.
15. Secretan B, Straif K, Baan R, et al. A review of humancarcinogens-part E: tobacco, areca nut, alcohol, coalsmoke, and salted fish. Lancet Oncol 2009;10:1033–1034.
16. Lee YC, Wang HP, Wang CP, et al. Revisit of field can-cerization in squamous cell carcinoma of upper aero-digestive tract: better risk assessment with epigeneticmarkers. Cancer Prev Res 2011;4:1982–1992.
17. Yokoyama T, Yokoyama A, Kato H, et al. Alcohol flush-ing, alcohol and aldehyde dehydrogenase genotypes,and risk for esophageal squamous cell carcinoma inJapanese men. Cancer Epidemiol Biomarkers Prev 2003;12:1227–1233.
18. Katada C, Muto M, Tanabe S, et al. Surveillance afterendoscopic mucosal resection or endoscopic submu-cosal dissection for esophageal squamous cell carci-noma. Dig Endosc 2013;25(Suppl 1):S39–S43.
19. Muto M, Takahashi M, Ohtsu A, et al. Risk of multiplesquamous cell carcinomas both in the esophagus andthe head and neck region. Carcinogenesis 2005;26:1008–1012.
20. Katada C, Muto M, Tanabe S, et al. Risk for the devel-opment of multiple Lugol-voiding lesions of the esoph-ageal mucosa in patients with esophageal squamous cellcarcinoma. Dis Esophagus 2014;27:457–462.
21. Jarl J, Gerdtham UG. Time pattern of reduction in risk ofoesophageal cancer following alcohol cessation – ameta-analysis. Addiction 2012;107:1234–1243.
22. Mori M, Adachi Y, Matsushima T, et al. Lugol stainingpattern and histology of esophageal lesions. Am J Gas-troenterol 1993;88:701–705.
Received December 7, 2015. Accepted July 18, 2016.
Reprint requestsAddress requests for reprints to: Manabu Muto, MD, PhD, Department ofTherapeutic Oncology, Kyoto University Graduate School of Medicine, 54Kawaharacho, Shogoin, Sakyo-ku, Kyoto 606-8507, Japan. e-mail:[email protected]; fax: (81) 75-751-4594. Q3
AcknowledgmentsData were presented in part at Digestive Disease Week 2013 (abstract Su1486)in Orlando, FL. Q17
Chikatoshi Katada, Tetsuji Yokoyama, Hideki Ishikawa, Akira Yokoyama,Yusuke Amanuma, Shinya Ohashi, Tomonari Matsuda, and Manabu Mutowere responsible for the conception and design; Chikatoshi Katada, TetsujiYokoyama, Hideki Ishikawa, Yusuke Amanuma, Tomonari Matsuda, andManabu Muto were responsible for data analysis and interpretation; ManabuMuto and Kazuhiro Kaneko were responsible for financial support;Chikatoshi Katada and Manabu Muto provided administrative support; andall authors were responsible for the collection and assembly of data,manuscript writing, final approval of the manuscript, and provision of studymaterials or patients.
Conflicts of interestThe authors disclose no conflicts. Q4
FundingSupported by a grant from National Cancer Center Research and DevelopmentFund 36 by the Ministry of Health, Labour and Welfare of Japan. Q5
10 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
1081
1082
1083
1084
1085
1086
1087
1088
1089
1090
1091
1092
1093
1094
1095
1096
1097
1098
1099
1100
1101
1102
1103
1104
1105
1106
1107
1108
1109
1110
1111
1112
1113
1114
1115
1116
1117
1118
1119
1120
1121
1122
1123
1124
1125
1126
1127
1128
1129
1130
1131
1132
1133
1134
1135
1136
1137
1138
1139
1140
1141
1142
1143
1144
1145
1146
1147
1148
1149
1150
1151
1152
1153
1154
1155
1156
1157
1158
1159
1160
1161
1162
1163
1164
1165
1166
1167
1168
1169
1170
1171
1172
1173
1174
1175
1176
1177
1178
1179
1180
1181
1182
1183
1184
1185
1186
1187
1188
1189
1190
1191
1192
1193
1194
1195
1196
1197
1198
1199
1200
CLINICALAT

Supplementary Figure 1. A self-administered questionnaire for lifestyle surveys.
web4C=FPO
Supplementary Figure 2. TP53 mutations in biopsy speci-mens of noncancerous background esophageal mucosa.Deep sequencing of the TP53 gene amplicon was performedto detect small frequencies of mutations (�2% of total reads).A rectangle shows a biopsy specimen of each case. A redplot shows a mutation of TP53, and the plot size conforms tothe mutation frequency. The 38 cases are divided accordingto their LVL grade (grade A, 7 cases; grade B, 9 cases; andgrade C, 22 cases). ALDH2*1/*1 (ALDH2 wild-type homozy-gotes), ALDH2*1/*2 (ALDH2 heterozygotes), and ALDH2*2/*2(ALDH2 mutant homozygotes) are shown with blue rectan-gles, red rectangles, and yellow rectangles, respectively.
- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 10.e1
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
1201
1202
1203
1204
1205
1206
1207
1208
1209
1210
1211
1212
1213
1214
1215
1216
1217
1218
1219
1220
1221
1222
1223
1224
1225
1226
1227
1228
1229
1230
1231
1232
1233
1234
1235
1236
1237
1238
1239
1240
1241
1242
1243
1244
1245
1246
1247
1248
1249
1250
1251
1252
1253
1254
1255
1256
1257
1258
1259
1260
1261
1262
1263
1264
1265
1266
1267
1268
1269
1270
1271
1272
1273
1274
1275
1276
1277
1278
1279
1280
1281
1282
1283
1284
1285
1286
1287
1288
1289
1290
1291
1292
1293
1294
1295
1296
1297
1298
1299
1300
1301
1302
1303
1304
1305
1306
1307
1308
1309
1310
1311
1312
1313
1314
1315
1316
1317
1318
1319
1320

Supplementary Figure 3. Comparison of the TP53 mutationfrequency between LVL grades. A circle plot shows a sum-mation of TP53 mutation frequency in each case. The boxheight represents the interquartile range showing the lowerquartile (25th percentile values) and upper quartile (75thpercentile values) values. The line in the box represents themedian, and the whiskers represent the minimum andmaximum TP53 mutation frequencies. The P values werecalculated by the Wilcoxon signed-rank test.
10.e2 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
1321
1322
1323
1324
1325
1326
1327
1328
1329
1330
1331
1332
1333
1334
1335
1336
1337
1338
1339
1340
1341
1342
1343
1344
1345
1346
1347
1348
1349
1350
1351
1352
1353
1354
1355
1356
1357
1358
1359
1360
1361
1362
1363
1364
1365
1366
1367
1368
1369
1370
1371
1372
1373
1374
1375
1376
1377
1378
1379
1380
1381
1382
1383
1384
1385
1386
1387
1388
1389
1390
1391
1392
1393
1394
1395
1396
1397
1398
1399
1400
1401
1402
1403
1404
1405
1406
1407
1408
1409
1410
1411
1412
1413
1414
1415
1416
1417
1418
1419
1420
1421
1422
1423
1424
1425
1426
1427
1428
1429
1430
1431
1432
1433
1434
1435
1436
1437
1438
1439
1440

Supplementary Figure 4. Patient flow chart of alcohol and smoking abstinence according to the LVL grade. *P ¼ .90, †P ¼.61, and ‡P ¼ .98. (A) ¼ a, (B) ¼ j, (C) ¼ b, (D) ¼ k. Q19
- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 10.e3
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
1441
1442
1443
1444
1445
1446
1447
1448
1449
1450
1451
1452
1453
1454
1455
1456
1457
1458
1459
1460
1461
1462
1463
1464
1465
1466
1467
1468
1469
1470
1471
1472
1473
1474
1475
1476
1477
1478
1479
1480
1481
1482
1483
1484
1485
1486
1487
1488
1489
1490
1491
1492
1493
1494
1495
1496
1497
1498
1499
1500
1501
1502
1503
1504
1505
1506
1507
1508
1509
1510
1511
1512
1513
1514
1515
1516
1517
1518
1519
1520
1521
1522
1523
1524
1525
1526
1527
1528
1529
1530
1531
1532
1533
1534
1535
1536
1537
1538
1539
1540
1541
1542
1543
1544
1545
1546
1547
1548
1549
1550
1551
1552
1553
1554
1555
1556
1557
1558
1559
1560

Supplementary Table 1.Clinical Characteristics of 38 Esophageal SCC Patients Analyzed With TP53 Deep Sequencing Q20
Sample ID LVL grade ALDH2 genotype Age, y Sex Alcohol drinkinga Smoking, pack-year
S1 A *1/*1 74 Female Never 35.25S2 A *1/*2 60 Female Never 0S3 A *1/*1 85 Female Light 0S4 A *1/*1 57 Male Light 40S5 A *1/*1 64 Male Light 40S6 A *1/*2 68 Male Moderate 30S7 A *1/*1 60 Male Moderate 40S8 B *1/*1 67 Male Heavy 129S9 B *1/*2 69 Male Moderate 60S10 B *1/*2 75 Male Moderate 45S11 B *1/*2 72 Male Moderate 2.5S12 B *1/*1 55 Female Heavy 12.5S13 B *1/*1 68 Male Moderate 45S14 B *1/*1 64 Female Heavy 40S15 B *1/*2 75 Male Moderate 87S16 B *1/*1 72 Male Moderate 45S17 C *1/*2 75 Male Heavy 5S18 C *1/*2 71 Male Never 38S19 C *1/*2 53 Male Heavy 70S20 C *1/*1 62 Female Moderate 20S21 C *1/*2 67 Male Heavy 70.5S22 C *1/*2 61 Male Moderate 40S23 C *1/*2 64 Male Moderate 34.5S24 C *1/*2 71 Male Moderate 75S25 C *2/*2 58 Male Heavy 40S26 C *1/*2 61 Male Moderate 20S27 C *1/*1 69 Male Heavy 21.5S28 C *1/*1 59 Female Moderate 40S29 C *1/*2 67 Male Moderate 100S30 C *1/*2 59 Male Moderate 20S31 C *1/*2 59 Male Heavy 0S32 C *1/*2 73 Male Heavy 30S33 C *1/*2 64 Male Heavy 39.6S34 C *1/*2 68 Male Heavy 50S35 C *1/*2 71 Male Heavy 75S36 C *1/*2 69 Male Heavy 51S37 C *1/*2 66 Male Heavy 86S38 C *1/*2 50 Male Heavy 270
aNever/rare, <1 U/wk; light, 1–8.9 U/wk; moderate, 9–17.9 U/wk; heavy, �18 U/wk (1 U ¼ 22 g ethanol).
10.e4 Katada et al Gastroenterology Vol. -, No. -
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
1561
1562
1563
1564
1565
1566
1567
1568
1569
1570
1571
1572
1573
1574
1575
1576
1577
1578
1579
1580
1581
1582
1583
1584
1585
1586
1587
1588
1589
1590
1591
1592
1593
1594
1595
1596
1597
1598
1599
1600
1601
1602
1603
1604
1605
1606
1607
1608
1609
1610
1611
1612
1613
1614
1615
1616
1617
1618
1619
1620
1621
1622
1623
1624
1625
1626
1627
1628
1629
1630
1631
1632
1633
1634
1635
1636
1637
1638
1639
1640
1641
1642
1643
1644
1645
1646
1647
1648
1649
1650
1651
1652
1653
1654
1655
1656
1657
1658
1659
1660
1661
1662
1663
1664
1665
1666
1667
1668
1669
1670
1671
1672
1673
1674
1675
1676
1677
1678
1679
1680

Supplementary Table 2.Clinical Characteristics of 38Esophageal SCC PatientsAccording to the LVL Grade
LVL grade
A (n ¼ 7) B (n ¼ 9) C (n ¼ 22)
SexMale, % 57.1% 77.8% 91.0%
Age, yMeans ± SD 67 ± 10 69 ± 6 64 ± 6
Drinking alcohola
Never/rare 28.6% 0.0% 4.5%Light 42.9% 0.0% 0.0%Moderate 28.6% 66.7% 36.4%Heavy 0.0% 33.3% 59.1%
Heavy smoker, �30 pack-years 71.4% 77.8% 72.7%ALDH2 genotype
*1/*1 71.4% 55.6% 13.6%*1/*2 28.6% 44.4% 81.8%*2/*2 0.0% 0.0% 4.5%
aNever/rare, <1 U/wk; light, 1–8.9 U/wk; moderate, 9–17.9U/wk; heavy, �18 U/wk (1 U ¼ 22 g ethanol).
- 2016 Alcohol, Dysplastic Lesion, and Field Cancerization 10.e5
FLA 5.4.0 DTD � YGAST60613_proof � 29 September 2016 � 11:53 am � ce
1681
1682
1683
1684
1685
1686
1687
1688
1689
1690
1691
1692
1693
1694
1695
1696
1697
1698
1699
1700
1701
1702
1703
1704
1705
1706
1707
1708
1709
1710
1711
1712
1713
1714
1715
1716
1717
1718
1719
1720
1721
1722
1723
1724
1725
1726
1727
1728
1729
1730
1731
1732
1733
1734
1735
1736
1737
1738
1739
1740
1741
1742
1743
1744
1745
1746
1747
1748
1749
1750
1751
1752
1753
1754
1755
1756
1757
1758
1759
1760
1761
1762
1763
1764
1765
1766
1767
1768
1769
1770
1771
1772
1773
1774
1775
1776
1777
1778
1779
1780
1781
1782
1783
1784
1785
1786
1787
1788
1789
1790
1791
1792
1793
1794
1795
1796
1797
1798
1799
1800

Supplementary Table 3.Summary of TP53 Mutations in 38 Esophageal SCC Patients
Sample ID Mutation type Coverage Frequency Start position End position Reference allele Mutated allele Amino acid change Cosmic occurrence
S5 Nonsynonymous SNV 891 2.5 7578446 7578446 T A I162F Q2110S6 Nonsynonymous SNV 1243 2.7 7578532 7578532 A C M133R 6S6 Frameshift deletion 1030 2.0 7577572 7577572 T – 2S6 Nonsynonymous SNV 649 2.3 7579358 7579358 C A R110L 25S7 Nonsynonymous SNV 1571 2.2 7578394 7578394 T C H179R 114S7 Nonsynonymous SNV 1280 3.6 7578203 7578203 C A V216L 7S7 Nonsynonymous SNV 1280 2.7 7578191 7578191 A G Y220H 12S7 Nonsynonymous SNV 944 2.9 7577524 7577524 T G T253P 3S12 Nonsynonymous SNV 197 2.0 7579362 7579362 A G F70L 2S13 Nonsynonymous SNV 522 2.1 7579358 7579358 C G R110P 9S14 Nonsynonymous SNV 967 5.5 7578190 7578190 T C Y220C 231S15 Splicing 1055 2.2 7574035 7574035 T G 0S15 Nonframeshift deletion 986 2.9 7577580 7577585 TAGTGG – 0S15 Nonsynonymous SNV 987 3.7 7577530 7577530 T A I251F 8S15 Nonsynonymous SNV 989 2.2 7577547 7577547 C T G254D 110S16 Nonsynonymous SNV 1445 13.2 7578522 7578522 T A Q136H 1S16 Nonsynonymous SNV 880 2.6 7578396 7578396 G T H178Q 4S16 Nonsynonymous SNV 646 2.8 7577139 7577139 G A R267W 26S22 Nonsynonymous SNV 869 2.2 7577539 7577539 G A R248W 495S23 Nonsynonymous SNV 810 2.5 7577139 7577139 G A R267W 26S24 Nonsynonymous SNV 345 2.6 7579358 7579358 C A R71L 25S25 Frameshift deletion 1844 3.0 7579879 7579879 G – 0S26 Nonsynonymous SNV 936 4.1 7578260 7578260 C T V197M 10S26 Stopgain SNV 825 3.5 7574003 7574003 G A R342* Q2274S27 Splicing 950 9.8 7577610 7577610 T A 10S28 Nonsynonymous SNV 485 2.5 7578448 7578448 G T A29D 9S28 Nonsynonymous SNV 800 2.9 7578190 7578190 T C Y220 231S28 Stopgain SNV 372 5.1 7577100 7577100 T A R148X 10S29 Nonsynonymous SNV 1504 2.3 7578266 7578266 T A I195F 21S29 Nonsynonymous SNV 748 3.6 7578235 7578235 T C Y205C 66S29 Nonsynonymous SNV 877 6.6 7577565 7577565 T C N239S 21S29 Nonsynonymous SNV 879 4.9 7577539 7577539 G A R248W 495S30 Nonsynonymous SNV 356 11.2 7577121 7577121 G A R141C 474S30 Stopgain SNV 1091 5.7 7574021 7574021 C A E336* 4S31 Nonsynonymous SNV 1225 5.7 7578526 7578526 C T C135Y 52S31 Frameshift deletion 694 3.7 7577599 7577599 C – 0S31 Nonsynonymous SNV 702 5.0 7577536 7577536 T A R249W 34S31 Nonsynonymous SNV 502 2.4 7577124 7577124 C A V272L 23S32 Nonsynonymous SNV 1079 2.5 7577559 7577559 G A S241F 73S32 Nonsynonymous SNV 1080 4.8 7577570 7577570 C T M237I 68S32 Nonsynonymous SNV 537 4.8 7577098 7577098 T A R280S 11S32 Nonsynonymous SNV 538 3.0 7577094 7577094 G A R282W 395S32 Nonsynonymous SNV 1638 2.6 7578538 7578538 T C N131S 4S33 Splicing 1416 4.5 7578370 7578370 C T 21
10.e6Katada
etal
GastroenterologyVol.
-,No.
-
FLA
5.4.0
DTD
�YGAST60613_proof�
29Septem
ber
2016�
11:53am
�ce
1801
1802
1803
1804
1805
1806
1807
1808
1809
1810
1811
1812
1813
1814
1815
1816
1817
1818
1819
1820
1821
1822
1823
1824
1825
1826
1827
1828
1829
1830
1831
1832
1833
1834
1835
1836
1837
1838
1839
1840
1841
1842
1843
1844
1845
1846
1847
1848
1849
1850
1851
1852
1853
1854
1855
1856
1857
1858
1859
1860
1861
1862
1863
1864
1865
1866
1867
1868
1869
1870
1871
1872
1873
1874
1875
1876
1877
1878
1879
1880
1881
1882
1883
1884
1885
1886
1887
1888
1889
1890
1891
1892
1893
1894
1895
1896
1897
1898
1899
1900
1901
1902
1903
1904
1905
1906
1907
1908
1909
1910
1911
1912
1913
1914
1915
1916
1917
1918
1919
1920

Supplementary Table 3.Continued
Sample ID Mutation type Coverage Frequency Start position End position Reference allele Mutated allele Amino acid change Cosmic occurrence
S33 Nonsynonymous SNV 1393 4.5 7578406 7578406 C T R175H 818S33 Nonsynonymous SNV 339 5.0 7577124 7577124 C A V140L 23S33 Stopgain SNV 339 6.8 7577058 7577058 C A E162X 43S34 Nonsynonymous SNV 1394 13.8 7578190 7578190 T C Y220C 231S34 Nonsynonymous SNV 1346 9.2 7578536 7578536 T G K132Q 10S35 Nonsynonymous SNV 679 23.4 7577559 7577559 G A S241F 73S36 Nonsynonymous SNV 2181 2.5 7578395 7578395 G A H179Y 85S36 Nonsynonymous SNV 2181 4.4 7578393 7578393 A T H179Q 12S36 Nonsynonymous SNV 1147 4.3 7578271 7578271 T C H193R 81S36 Nonsynonymous SNV 674 9.5 7577538 7577538 C T R248Q 565S36 Nonsynonymous SNV 563 2.7 7577121 7577121 G A R273C 474S36 Frameshift deletion 583 2.2 7579391 7579391 G – 0S37 Nonsynonymous SNV 717 4.0 7578454 7578454 G A A159V 37S37 Nonsynonymous SNV 691 8.7 7577547 7577547 C A G245V 62S37 Nonsynonymous SNV 607 14.5 7577120 7577120 C T R273H 513S37 Nonsynonymous SNV 645 3.7 7579358 7579358 C A R110L 25S38 Splicing 896 6.5 7577609 7577609 C T 13S38 Frameshift insertion 899 6.3 7577530 7577530 – T I119fs 0S38 Nonsynonymous SNV 899 2.6 7577528 7577528 G C I251M 0S38 Nonsynonymous SNV 454 26.7 7577098 7577098 T G R148S 5
-2016
Alcohol,DysplasticLesion,and
FieldCancerization
10.e7
FLA
5.4.0
DTD
�YGAST60613_proof�
29Septem
ber
2016�
11:53am
�ce
1921
1922
1923
1924
1925
1926
1927
1928
1929
1930
1931
1932
1933
1934
1935
1936
1937
1938
1939
1940
1941
1942
1943
1944
1945
1946
1947
1948
1949
1950
1951
1952
1953
1954
1955
1956
1957
1958
1959
1960
1961
1962
1963
1964
1965
1966
1967
1968
1969
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
2037
2038
2039
2040