Embed Size (px)
Citation preview
Title Lyme disease - a brief review and report of a case in Hong Kong
Author(s) Hodgkiss, IJ; Wong, YC; Chan, BSS
Citation Hong Kong Practitioner, 1995, v. 17 n. 8, p. 370-378
Issued Date 1995
URL http://hdl.handle.net/10722/44717
Rights This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
DISCUSSION PAPER
Lyme Disease - A Brief Review And Report Of A Case InHong Kong
I.J. Hodgkiss*, BSc, PhD, FLS, CBiol, FIBiol,FCIWEMReaderDepartment of Ecology & BiodiversityThe University of Hong Kong
Y.C. Wong, BLabTechScientific Officer/SupervisorDepartment of Clinical PathologyHong Kong Central Hospital
Ben S.S. Chan, BSc, PhDLecturerBiology DepartmentHong Kong Baptist University
Abstract
In a search for the spirochetes responsible forLyme disease in Hong Kong, a sixty year old female,with a clinical diagnosis of arthritis, was found tohave a rising antibody litre against Borreliaburgdorferi by indirect immunofluorescent assay(IFA).
This paper presents a brief review of Lymedisease, its epidemiology, clinical features, diagnosis,prevention and treatment, followed by a report ofthis first case of Lyme disease in Hong Kong.
Key words: Borrelia burgdorferi, indirectimmunofluorescent antibody (IFA),Lyme disease, rheumatoid factor,Treponema pallidum haemag-lutination assay (TPHA).
History
For Americans, a discussion of the history ofLyme borreliosis usually begins with the story oftwo persevering women, Polly Murray and JudithMensch of Old Lyme, Connecticut. In the early1970s, they were concerned about the occurrenceof arthritis in members of their families and infamilies of the neighbouring towns of Lyme andEast Haddam. Severe headaches, skin lesions,and subsequent recurring arthritic and neurologicsymptoms suggested to them that the physicians*diagnosis of "juvenile rheumatoid arthritis" waswrong. Their suspicion that something unusualwas happening was made known to theConnecticut State Health Department, whichsought help from Dr. Allen Steere of theRheumatology Department at Yale UniversityMedical School. In October 1975, he started aretrospective study that eventually led to thedescription of Lyme arthritis,1 which was laterchanged to Lyme disease,2 a new complexmultisystem disorder of unknown etiology.
Unknown to most Americans, however, is theearliest reference to manifestations of what todayis known as Lyme borreliosis. In as early as 1909,the Swedish physician, Dr. Arvid Afzelius,reported an elderly woman who had a ringlikeskin lesion where she had been bitten by thesheep tick, Ixodes ricinus? This characteristicexpanding skin lesion, erythema chronicummigrans (ECM), has long been associated withsheep tick bites,4-5 and with tick-bornemeningopolyneuritis in Europe.6'7 The association,between Lyme Disease and Ixodid ticks is nowwell recognized in Europe and the United States
"Address for correspondence:
370
Dr. I.J. Hodgkiss, Reader in Ecology & Biodiversity, The University of Hong Kong, Pokfulam Road, HongKong.

Hong Kong Practitioner 17 (8) August 1995
of America;8 it is noted as the most prevalent tick-borne illness in the coastal regions of NorthAmerica;9 and is of world-wide distribution,including China.10'11 These syndromes are nowoften subsumed under the name Lyme disease.
Although many theories have been proposedto explain its etiology,12"17 the causative agent ofLyme disease remained elusive until 1982, whenBurgdorferi and associates18 isolated thespirochete that bears his name Borrelia burgdorferifrom Ixodes dammini in New York, and linked itserologically to patients with Lyme disease. In thefollowing few years, numerous workers confirmedthe spirochete nature of the disease.19"23 Becauseit is infectious in origin but inflammatory or"rheumatic" in expression, Lyme disease, beyondits intrinsic interest as a new nosologic entity,presents a unique human model for an infectiousetiology of rheumatic disease.
during biting, or by infective tick faecal matterthat is deposited on the skin and rubbed intothe bite. The spiral organisms of medicalsignificance include Leptospira, which causeshuman leptospirosis; Treponema, responsible forthe diseases known as treponematoses, such assyphilis;24 and Borrelia, which causes relapsingfever.25
Tick Vectors
Ticks are not insects, but related to spiders,scorpions and mites, and placed in the classArachnida.26 There are two families of ticks, theIxodidae (hard-bodied ticks) and the Argasidae(soft-bodied ticks), which differ morphologicallyand behaviourally. Ixodes is one of the thirteengenera of Ixodidae, and the principal vector of B.burgdorferi worldwide.27
Epidemiology
Lyme disease has now been recognized as aworldwide tickborne borreliosis of public healthimportance. It has become the leadingvectorborne infectious disease in the UnitedStates, with more than 40,000 cases reported tothe Centers for Disease Control in the 10-yearperiod 1982 to 1991.
The Hosts
The Ixodes vectors of B. burgdorferi that feedon humans as incidental hosts also parasitize alarge number of small, medium and large wild anddomestic animals, including hundreds of species ofmammals, reptiles and birds.28"30
Global Distribution
The Pathogen
Borrelia burgdorferi, the causative agent ofLyme disease,18 is a newly discoveredmicroaerophilic spirochete that is 2 to 20 \imlong but only 0.18 to 0.25 um wide, belonging tothe family Spirochaetaceae. B. burgdorferi occursmainly in wild white-footed mice, in deer, and inticks of the genus Ixodes. The ticks can transmitthe spirochete to humans by bites at any stageof the tick's life cycle (i.e. larval, nymph andadult). B. burgdorferi is injected into the skin ofan human victim either by infective tick saliva
Lyme disease is endemic in North America,across Europe to Asia, including the British Isles,western Europe and Russia (from the Baltic Statesto the Pacific Coast),31'33 China and Japan. 1W1'34'35
Although not yet confirmed by isolation, thedisease has also been reported from Africa, SouthAmerica, Australia and India.33'36"38
Clinical Features
Lyme disease is an illness having proteanmanifestations with symptoms that include:
371

Lyme Disease
(1) an erythematous expanding red annular rashwith central clearing;
(2) fever, headache, stiff neck, nausea, andvomiting;
(3) neurologic complications such as facial nerve(Bell's) palsy and meningitis; and
(4) arthritis in about 50% of untreated patients.
These symptoms occur most frequentlyfrom May to November, when ticks are activeand numerous, and people are engaged in manyoutdoor activities. The most characteristicfeature of early Lyme disease is a skin rash,often referred to as erythema chronicummigrans (ECM), which appears shortly (3-32days) after a bite from an infected tick. Thelesion typically expands almost uniformly fromthe centre of the bite and is usually flat orslightly indurated with central clearing andreddening at the periphery. It is noteworthy,however, that many Lyme disease victims donot recall being bitten by a tick or do notdevelop classic ECM. Indeed one third of thepatients may not develop ECM. On the otherhand, at various intervals after the initial rash,some patients develop similar but smallermultiple secondary annular skin lesions that lastfor several weeks to months. In approximatelyhalf of the patients, the first sign to appear isa slowly expanding red rash at the site of thebite. Beginning as a small flat or raisedlesion, the rash increases in diameter in acircular pattern and over a period of weeks thediameter may reach 10-15 inches. It has anintense red border and a red centre resemblinga bull's eye. It can vary in shape and isusually hot to touch. The initial tick bite maybe distinguished from a mosquito bite becausethe latter itches, while a tick bite does not.39
Biopsy of these skin lesions reveals lymphocyticand plasmacytic infiltrates. Various flulikesymptoms such as malaise, fever, headache, stiffneck and arthralgias are often associated withECM. The spirochete eventually reaches thebrain, and within several weeks or months
about 15% of the patients develop meningitis,which may be accompanied by excruciatingheadaches and neck pain. There may beabnormalities of the nervous system that lastfor years, ranging from a mild tingling sensationin the limbs to encephalomyelitis, partialparalysis, or even mental deterioration. Withinseveral weeks after the onset of the disease,approximately 8% of patients show cardiacinvolvement indicated by heartbeat irregularity,dizziness or shortness of breath. Within 2weeks to 2 years after the beginning of thedisease, 80% of patients develop recurrentarthritis, and eventually the knees or otherlarge joints may become swollen and painful.
Much of the damage to the body causedby B. burgdorferi has been attributed to theendotoxin in the outer membrane of thespirochete. The endotoxin is believed tostimulate macrophages to produce interleukin-1,a regulator of the body's immune response.Over-production of this regulator accounts forthe fever, skin rash and recurrent arthritis thatare characteristics of Lyme disease/0 The latemanifestations of Lyme disease may includemigratory and polyarticular arthritis, neurologicand cardiac involvement with cranial nervepalsies and radiculopathy, myocarditis andarrhythmias. Lyme arthritis typically involves aknee or other large joint. It may enter achronic phase, leading to destruction of boneand joints if left untreated. Interestingly, Lymearthritis is less common in Europe than in theUSA, but neurologic complications are moreprevalent in Europe. Unique strain variationsexpressing antigenic subtypes between Europeanand North American isolates of B. burgdorferiprobably explain these dissimilarities.
Diagnosis
Like syphilis, Lyme disease produces adiverse number of clinical symptoms that canbe confused with many other disease entities.
372
Hong Kong Practitioner 17 (8) August 1995
In many cases the clinical differential is oftencomplex resulting in heavy reliance on thelaboratory to provide diagnostic evidence.1'2-41-42
However, successful isolation and culture of B.burgdorferi from skin lesions, blood and jointand cerebrospinal fluid in suspected cases ofLyme disease is rare,19'42 and most commonnonspecific laboratory tests are not helpful inthe differential diagnosis. Thus, serologic testsprovide the most important confirmatoryevidence of all stages of Lyme disease and maybe the only way of diagnosing atypical cases.The most commonly used serologic tests are theenzyme-linked immunosorbent assay (ELISA)and indirect fluorescent-antibody assay (IFA)which detect the specific antibody against B.burgdorferi. Since antibodies to otherspirochetes, including Treponema pallidum, cancross-react, differential diagnosis must beundertaken using tests such as VDRL, TPHAor RPR for all specimens showing a positivereaction towards 8. burgdorferi.
In serum, specific IgM antibody titresagainst B. burgdorferi usually reach a peakbetween the third and sixth week after theonset of disease; specific IgG antibody titresrise more slowly and are generally highestmonths later when arthritis is present.
On 19 October 1990, the CDC definedcase criteria for reportable disease.43 Lymedisease is one of the diseases for which theCDC established diagnostic clinical and
'laboratory criteria, as follows:
Clinical case definition - Erythema migrans,or at least one late manifestation.
Laboratory criteria for diagnosis - isolationof B. burgdorferi from clinical specimen, ordemonstration of diagnostic levels of IgM andIgG antibodies to the spirochete in serum ofCSF, or significant change in IgM or IgGantibody response to B. burgdorferi in pairedacute and convalescent-phase serum samples.
Treatment and Prevention
For early stage treatment, in order ofpreference, oral tetracycline 250mg four timesa day, phenoxy-methyl penicillin 5OOmg fourtimes a day, or erythromycin 250mg four timesa day each for 10 to 20 days depending on theresponse, is suggested.44
For meningitis and cranial or peripheralneuropathies, intravenous penicillin G 20 millionU a day in six divided doses for 10 days iseffective therapy.43
For established Lyme arthritis, treatmentwith intra-muscular benzathine penicillin 2.5million U weekly for 3 weeks has been provento be successful.46 The affected joint should beat rest, and accumulated fluid should beremoved by needle aspirations.
In vitro and in vivo susceptibility tests havesuggested that cefuroxime may be an effectivealternative therapy for Lyme disease.47
A few simple precautions will help reducepossible exposure to Borrelia-infected ticks andincrease protection against Lyme disease.These include wearing clothing that fullyprotects the body and using repellents thatcontain DEET (diethyltoluamide).48 Peopleshould be made aware of the typical earlysymptoms of infection, such as the characteristicskin rash. The potential for human contactwith Ixodes ticks as a cause of occasional casesof locally acquired spotted fever must not beoverlooked.
The Current Investigation
The incidence of Lyme disease has beenincreasing considerably world-wide since 1975, butit has never been documented in Hong Kong; andthe local situation regarding the disease isunknown. In an attempt to investigate its
373
Lyme Disease
occurrence in Hong Kong, since August 1992, asurvey of seroprevalence has been conducted inpatients with a clinical diagnosis of arthritis.
Blood samples of patients with a clinicaldiagnosis of arthritis were collected from tendifferent clinical laboratories in Hong Kong.Whole blood specimens were centrifuged to obtainsera for assay by indirect immunofluorescentantibody (IFA) titre to Borrelia burgdorferi (Lyme-spot IF, Ref. 75941 Bio Merieux, France); torheumatoid factor by agglutination of IgG coatedlatex particles (RA80, Eiken Chemical, Japan);and for antibodies against Treponema pallidum byhaemaglutination assay (TPHA, Fujirebio Inc.,Japan) and the rapid plasma reagin card test(RPR reditest, Biokit, Spain) following themanufacturers' instructions. Other clinical andlaboratory data relating to the patients were alsocollected and recorded as additional information.
For a potential patient to be defined aspositive for antibody to Borrelia burgdorferi, thepatient had to have a clinical diagnosis of arthritis,
a titre of 1:160 or greater for antibody to Borreliaburgdorferi by indirect immunofluorescent antibody(IFA), together with non-reactive results in theremaining three assays, namely: (a) rheumatoidfactor (RA), (b) Treponema pallidumhaemaglutination assay (TPHA) as well as (c)rapid plasma reagin (RPR).49
Case Report
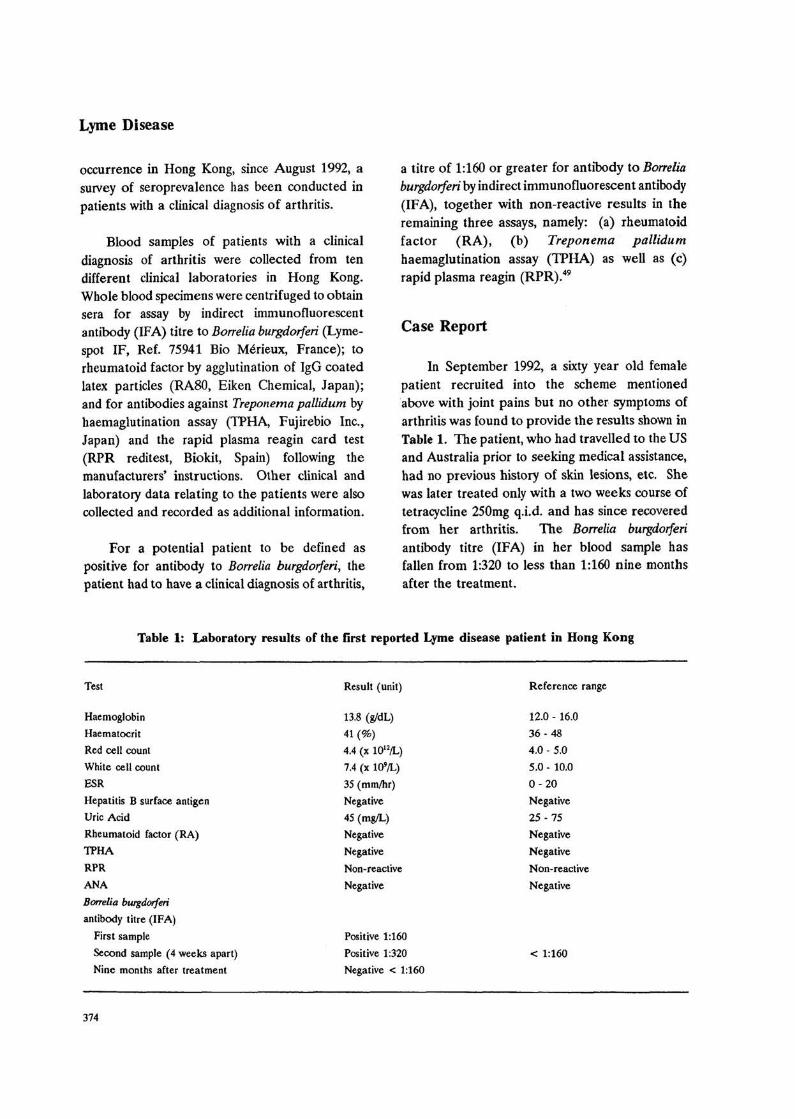
In September 1992, a sixty year old femalepatient recruited into the scheme mentionedabove with joint pains but no other symptoms ofarthritis was found to provide the results shown inTable 1. The patient, who had travelled to the USand Australia prior to seeking medical assistance,had no previous history of skin lesions, etc. Shewas later treated only with a two weeks course oftetracycline 250mg q.i.d. and has since recoveredfrom her arthritis. The Borrelia burgdorferiantibody titre (IFA) in her blood sample hasfallen from 1:320 to less than 1:160 nine monthsafter the treatment.
Table 1: Laboratory results of the first reported Lyme disease patient in Hong Kong
Test
Haemoglobin
Haematocrit
Red cell count
White cell count
ESRHepatitis B surface antigen
Uric Acid
Rheumatoid factor (RA)
TPHA
RPRANABorrelia burgdorferi
antibody titre (IFA)
First sample
Second sample (4 weeks apart)
Nine months after treatment
Result (unit)
13.8 (g/dL)
41(%)
4.4 (x 1012/L)
7.4 (x lO'/L)
35 (mm/hr)
Negative
45 (mg/L)
Negative
Negative
Non-reactive
Negative
Positive 1:160
Positive 1:320
Negative < 1:160
Reference range
12.0 - 16.0
36-48
4.0 - 5.0
5.0 - 10.0
0-20Negative25-75NegativeNegativeNon-reactiveNegative
< 1:160
374
Discussion
The situation regarding Lyme disease in HongKong is unclear. Although little is known aboutthe prevalence of the Ixodes ticks in this area,there are several possible routes for Lyme diseaseto gain entrance into Hong Kong.
1. Domestic animals, such as dogs and cats, arefound to be commonly infested by B.burgdorferi carrying Ixodes ticks in endemicareas.50"52 But pets imported into Hong Kongare not known to have been de-ticked beforeentrance. Ixodes ticks have been noted inpets visiting local veterinarians.53
2. 49 species of birds have been found to beinfested by Ixodes ticks,29 and migrating birdshave already been suspected to be a route oftransmitting Lyme disease.54
3. Other than Ixodes ticks, possible transmissionof B. burgdorferi to humans by blood-suckinginsects such as fleas, mosquitoes and horseflies has been reported.55136
4. The tremendously high volume of visitors, re-immigrants, and travellers to and fromendemic areas each year has increased largelythe possibility of Lyme disease infection.
Like syphilis, Lyme disease has been called a"great imitator" and is often difficult to diagnoseclinically. Less than one third of patientspresenting with ECM recall having been bitten byticks.57-58 Up to 50% of patients presenting withLyme arthritis may not recall the pathognomonicECM rash, flulike illness, or tick bite.59 The ECMrash may be unrecognized or mistaken for anotherannular dermatosis. Even in endemic areas of theUnited States, such as eastern New York and
Hong Kong Practitioner 17 (8) August 1995
Connecticut, ECM went unrecognized by mostphysicians until the early 1980s. In children, therash can be totally missed, when occurring in thescalp area or other unobserved locations.2-60
In almost all clinical bacteriologicalinvestigations, laboratory culture of causativemicroorganisms is the prime tool for diagnosis;however, for the screening of Lyme disease,laboratory culture is not a practical option.Isolation of Borrelia burgdorferi from blood serum,joint fluid, cerebrospinal fluid, or tissue hasproven to be very difficult, if not impossible.Successful positive cultures have been reported inless than 5% of patients with otherwise provenLyme disease.22
Nearly all patients with Lyme arthritis haveantibodies to Borrelia burgdorferi detectable intheir sera. Antibody screening, therefore, remainsthe most practical method for the detection of thedisease, pending the discovery of a better, morereliable, faster methodology. False-positiveresults, attributable to antibodies cross-reactive toBorrelia burgdorferi, can also be seen, however, inthe serum of patients with other spirochetalinfections.57 Thus, confirmation of the diagnosisof Lyme disease is only possible if results obtainedfrom the TPHA and RPR test are negative.
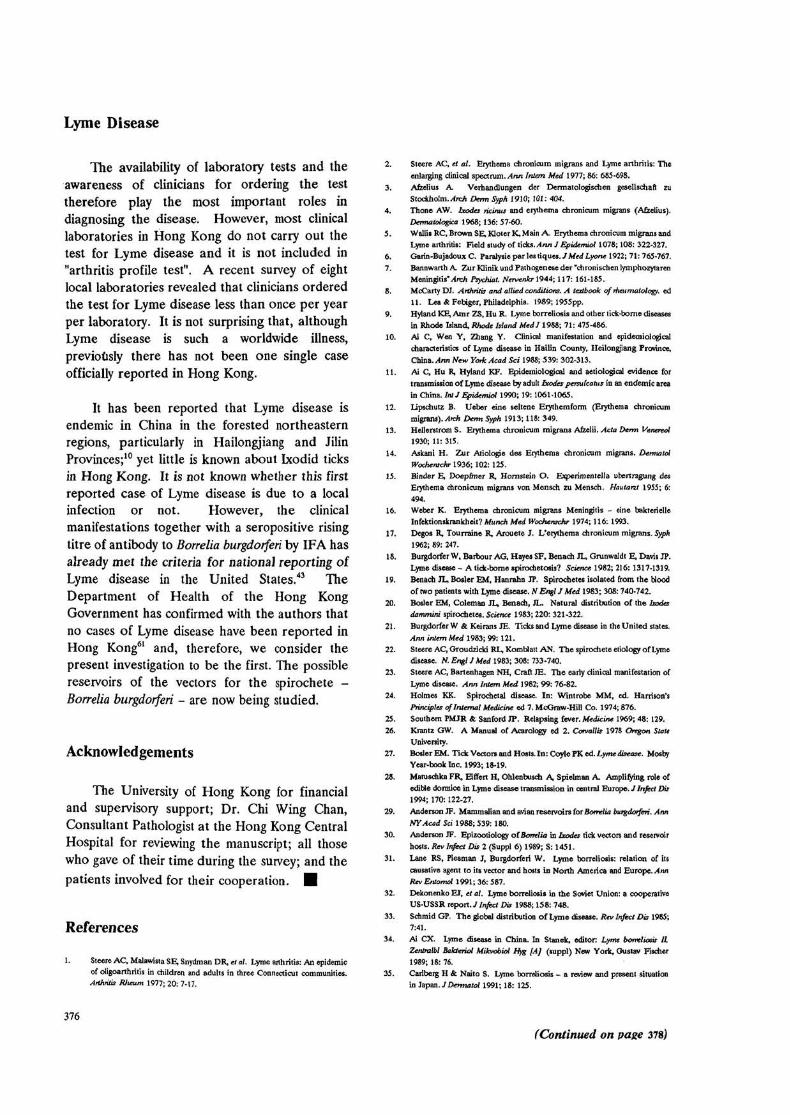
Routine laboratory testing is often not helpfulin the differential diagnosis of Lyme disease, sincesome patients with Lyme disease may not havelaboratory abnormalities. Table 2 summarizeslaboratory findings during early Lyme disease,where rheumatoid factor (RF) and ANA aretypically absent from the sera of Lyme diseasepatients1 and, as can be seen from the results, lessthan 60% showed any abnormality.
Table 2: Laboratory Findings in Early Lyme disease.23
Test Number of patients (%) with abnormal values* Median (range) of abnormal values
HaematocritLeukocytes >10 cells x lO'/mm3
ESR >20 mm/hrIgM >250 mg/dL
37 (12)24 (8)
166 (53)104 (33)
35 (31 - 36)12 (11 - 18)35 (21 - 68)
310 (252 - 930)
'Total number of patients = 314
375
Lyme Disease
The availability of laboratory tests and theawareness of clinicians for ordering the testtherefore play the most important roles indiagnosing the disease. However, most clinicallaboratories in Hong Kong do not carry out thetest for Lyme disease and it is not included in"arthritis profile test". A recent survey of eightlocal laboratories revealed that clinicians orderedthe test for Lyme disease less than once per yearper laboratory. It is not surprising that, althoughLyme disease is such a worldwide illness,previously there has not been one single caseofficially reported in Hong Kong.
It has been reported that Lyme disease isendemic in China in the forested northeasternregions, particularly in Hailongjiang and JilinProvinces;10 yet little is known about Ixodid ticksin Hong Kong. It is not known whether this firstreported case of Lyme disease is due to a localinfection or not. However, the clinicalmanifestations together with a seropositive risingtitre of antibody to Borrelia burgdorferi by IFA hasalready met the criteria for national reporting ofLyme disease in the United States.43 TheDepartment of Health of the Hong KongGovernment has confirmed with the authors thatno cases of Lyme disease have been reported inHong Kong61 and, therefore, we consider thepresent investigation to be the first. The possiblereservoirs of the vectors for the spirochete -Borrelia burgdorferi - are now being studied.
Acknowledgements
The University of Hong Kong for financialand supervisory support; Dr. Chi Wing Chan,Consultant Pathologist at the Hong Kong CentralHospital for reviewing the manuscript; all thosewho gave of their time during the survey; and thepatients involved for their cooperation. •
References
1. Steere AC, Malawista SE, Snydman DR, a at. Lyme arthritis: An epidemicof oligoarthritis in children and adults in three Connecticut communities.Arthritis Rheum 1977; 20: 7-17.
2. Steere AC, et at. Erythema chronicutn migrans and Lyme arthritis: Theenlarging clinical spectrum. Ann Intern Med 1977; 86: 685-698.
3. Afzelius A Verhandlungen der Dermatologischen gesellschaft zuStockholm./Arch Derm Syph 1910; 101: 404.
4. Thone AW. Ixodes ricinus and erythema chronicum migrans (Afzelius}.Dematologxa 1968; 136: 57-60.
5. Wallis RC, Brown SE, Kloter K, Main A. Erythema chronicum migrans andLyme arthritis: Field study of ticks. Ann ] Epidemiol 1078; 108: 322-327.
6. Garin-Bujadoux C. Paralysie par les tiques.J Med Lyone 1922; 71: 765-767.7. Bannwarth A Zur Klinik und Pathogenese der "chronischen lymphozytaren
Meningitis 'Arch Psychiat. Nervenkr 1944; 117: 161-185.8. McCarty DJ. Arthritis and allied conditions. A textbook of rheumatology, ed
11. Lea & Febiger, Philadelphia. 1989; 1955pp.9. Hyland KE, Amr ZS, Hu R. Lyme borreliosis and other lick-borne diseases
in Rhode Island, Rhode Island MedJ 1988; 71: 475-486.10. Ai C, Wen Y, Zhang Y. Clinical manifestation and epidemiological
characteristics of Lyme disease in Hailin County, Heilongjiang Province,China. Ann New York Acad Sci 1988; 539: 302-313.
11. Ai C, Hu R, Hyland KF. Epidemiological and aetiologjcal evidence fortransmission of Lyme disease by adult bodes persulcatus in an endemic areain China. IntJ Epidermal 1990; 19: 1061-1065.
12. Lipschutz B. Ueber eine seltene Erythemform (Erythema chronicummigrans). Arch Derm Syph 1913; 118: 349.
13. Hellerstrom S. Erythema chronicum migrans Afzelii. Acta Derm Venereal1930; 11: 315.
14. Askani H. Zur Atiologie des Erythema chronicum migrans. DermatolWocherachr 1936; 102: 125.
15. Binder E, Doepfmer R, Hornstein O. Experimentella ubertragung desErythema chronicum migrans von Mensch zu Mensch. Hautarzt 1955; 6:494.
16. Weber K. Erythema chronicum migrans Meningitis - eine bakterielleInfektionskrankheit? Munch Med Wocherachr 1974; 116: 1993.
17. Degos R, Tourraine R, Arouete J. L'erythema chronicum migrans. Syph1962; 89: 247.
18. Burgdorfer W, Barbour AG, Hayes SF, Benach JL, Grunwaldt E, Davis JP.Lyme disease - A tick-borne spirochetosis? Science 1982; 216: 1317-1319.
19. Benach JL, Bosler EM, Hanrahn JP. Spirochetes isolated from the bloodof two patients with Lyme disease. N Engl J Med 1983; 308:740-742.
20. Bosler EM, Coleman JL, Benach, JL. Natural distribution of the bodesdammini spirochetes. Science 1983; 220: 321-322.
21. Burgdorfer W & Keirans JE. Ticks and Lyme disease in the United states.
Ann intern Med 1983; 99: 121.22. Steere AC, Groudzicki RL, Komblatt AN. The spirochete etiology of Lyme
disease. N. Engl J Med 1983; 308: 733-740.23. Steere AC, Bartenhagen NH, Craft JE. The early clinical manifestation of
Lyme disease. Arm Intern Med 1982; 99: 76-82.24. Holmes KK. Spirochetal disease. In: Wintrobe MM, ed. Harrison's
Principles of Internal Medicine ed 7. McGraw-Hill Co. 1974; 876.25. Southern PMJR & Sanford JP. Relapsing fever. Medicine 1969; 48: 129.26. Krantz GW. A Manual of Acarology ed 2. Corvallis 1978 Oregon State
University.27. Bosler EM. Tick Vectors and Hosts. In: Coyle FK ed. Lyme disease. Mosby
Year-book Inc. 1993; 18-19.
28. Matuschka FR, Eiffert H, Ohlenbusch A, Spielman A. Amplifying role ofedible dormice in Lyme disease transmission in central Europe. J I n f e c t Dis1994; 170:122-27.
29. Anderson JF. Mammalian and avian reservoirs for Borrelia burgdorferi. AnnNY Acad Sci 1988; 539: 180.
30. Anderson JF. Epizootiology of Borrelia in Ixodes tick vectors and reservoirhosts. Rev Infect Dis 2 (Suppl 6) 1989; S: 1451.
31. Lane RS, Piesman J, Burgdorferi W. Lyme borreliosis: relation of itscausative agent to its vector and hosts in North America and Europe. AnnRev Entomol 1991; 36: 587.
32. Dekonenko EJ, et al. Lyme borreliosis in the Soviet Union: a cooperativeUS-USSR report. J Infect Dis 1988; 158: 748.
33. SchmidGP. The global distribution of Lyme disease. Rev Infect Dis 1985;7:41.
34. Ai CX. Lyme disease in China. In Stanek, editor: Lyme borreliosis II,Zentralbl Baktaiol Mikvobiol Hyg [A] (suppl) New York, Gustav Fischer1989; 18: 76.
35. Carlberg H & Naito S. Lyme borreliosis - a review and present situationin Japan. J Dermatol 1991; 18: 125.
376
(Continued on page 378)

Lyme Disease
36. Schafrank SN, Kurba AK, Martone G. Lyme disease acquired in South 48.
Africa. Arch Dermalol 1990; 126: 6S5.
37. Stewart A, a al. Lyme arthritis in the Hunter Valley. MedJ Aust 1982; 1: 49.
139.38. Patial RK, el al. Lyme disease in a Shimla \xiy.JAP India 1990; 38(7): 503-
4. 50.39. Schmltz I. After the bite. Hippocrates May, 1989.
40. Barbour AG & Fish D. The biological and social significance of Lyme
disease. Science 1993; 260:1610-1616. 51.
41. Gologhty M Dattwyler. Lyme disease vs. meumatic disease.
Immunopathology 1986; 10: 4. 52.
42. Steere AC, Grodzicki MS, Komblatt AN. The spirochetal etiology of Lyme
disease. N EngI J Med 1983; 308: 733. 53.
43. Anonymous. Lyme disease surveillance United States 1989-1990. MMWR; 54.
1991; 40: 417. 55.
44. Steere AC, el al. Treatment of the early manifestations of Lyme disease.Ann Intern Med 1983; 99: 22-26. 56.
45. Steere AC, Pachner AR, and Malawista SE. Neurologic abnormalities ofLyme disease: Successful treatment with high-dose intravenous penicillin. 57.
Ann Intern Med. 1983; 99: 767-772.
46. Steere AC, a al. Successful parenleral antibiotic therapy of established 58.
Lyme arthritis. N Engl J Med 1985; 312: 869-874
47. Johnson RC, et al. Comparative in vitro and in vivo susceptibilities of the 59.
Lyme disease spirochete Bomlia burgdorferi to cefuroxime and other 60.antimicrobial agents. Antimicrobial Agents and Chemotherapy. 1990; 34(11): 61.
2133-6.
Anderson JF. Preventing Lyme disease. Rheum Clin North Am 1989: 15:
757.Magnarelli LA, Anderson JF, Johnson RC. Cross-reactivity in serological
tests for Lyme disease and other spirochetal infections. J Infect Dis 1987;156: 183.
Serologic studies of the occurrence of Borrelia burgdorferi in domestic
animals in Berlin. Berl-Murch-Tierarztl-Wocherachr. 1990 Nov 1; 103(11):
374-8.
Antibodies to Bomlia burgdorferi in dogs in Hokkaido. Microbiollummd
1990; 34(12): 1005-12.
Eng TR, et al. Greater risk of Borrelia burgdorferi infection in dogs than
people. J infect Dis 1988; 158: 1410.
Personal communication. Dr. E Leong DVM. 1994.
Lord R. (In press).
Luger SW. Lyme disease transmitted by a biting fly. N Engl J Med 1990;
322: 1752.Magnarelli LA, Anderson JF, Barbour AG. The etiologic agent of Lyme
disease in deer, horse and mosquitoes. J Infect Dis 1986; 154: 355.
Asbrink E ft Olsson I. Clinical manifestations of erthyema chronicum
migrans Afzelius in 161 patients.Acta Dem Venereol (Stockh) 1985; 65; 43.
Steere AC, et. al. The early clinical manifestations of Lyme disease. Ann
Intern Med 1983; 99:76.
Steere AC, et. al. Lyme disease. N Bngl J Med 1989; 321: 586.
Lyme disease - Connecticut. MMWR 15, 1988; 37(1): 1.
Hong Kong Government, Department of Health. Statistics on Lyme
Disease - Personal Communication, 20 November 1992.
378