Embed Size (px)
Citation preview
1
Title: SEVERE OBSTRUCTIVE SLEEP APNEA TREATMENT WITH ORAL 1
APPLIANCE: THE IMPACT ON OBSTRUCTIVE, CENTRAL AND MIXED 2
EVENTS 3
4
Authors: Maria de Lourdes Rabelo Guimarães1, Ana Paula Hermont1, Pedro Guimarães 5
de Azevedo2, Poliana Lima Bastos3, Millena Teles Portela de Oliveira4, Iracema Matos 6
de Melo5, Guilherme Salles Ottoboni6, Gabriela Vedolin7, Jorge Machado Caram1 7
8
Affiliation: 9
1 Universidade Federal de Minas Gerais, Av. Pres. Antônio Carlos, 6627 - Pampulha, Belo Horizonte - MG, 31270-901, Brazil. 10 2 Pontifícia Universidade Católica de Minas Gerais, Av: Dom José Gaspar, 500 Coração Eucaristíco - Belo Horizonte – MG, 11 30535-901, Brazil. 12 3 Department of Prosthesis and Occlusion, Universidade Federal do Ceará, Av. da Universidade, 2853 - Benfica, Fortaleza - CE, 13 60020-181, Brazil. 14 4 Universidade Federal do Ceará, Universidade Federal do Ceará, Av. da Universidade, 2853 - Benfica, Fortaleza - CE, 60020-15 181, Brazil. 16 5 Department of Physiology and Pharmacology, Universidade Federal do Ceará, Universidade Federal do Ceará, Av. da 17 Universidade, 2853 - Benfica, Fortaleza - CE, 60020-181, Brazil. 18 6 Faculdade de Odontologia de Piracicaba, Unicamp, Av. Limeira, 901 - Bairro Areião, Piracicaba – SP, 13414-903, Brazil. 19 7 Pontificia Universidade Catolica do Rio Grande do Sul, Av. Ipiranga, 6681 - Partenon, Porto Alegre - RS, 90619-900, Brazil. 20 21
Corresponding author: 22 23
Maria de Lourdes Rabelo Guimarães 24 Faculty of Dentistry, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil 25 Benvinda de Carvalho, 105/101, Santo Antônio, Belo Horizonte, Minas Gerais, 26
BRAZIL, 30330-180 27 Phone: +55 31 3342-3949 28
Fax number: +55 3132273825 29 E-mail: [email protected] 30
31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
2
Abstract: 1
Purpose Evaluate the effectiveness of two types of oral appliance (OA) in the treatment 2
of severe obstructive sleep apnea syndrome (OSAS) and their impact on the reduction 3
of obstructive, central and mixed apneas. 4
Methods Forty-eight patients suffering from severe OSAS with a history of 5
nonadherence to positive airway pressure therapy were treated with OA (lingual 6
orthosis and combined orthosis). Polysomnography exams were performed before and 7
after treatment. Computed tomography and cephalometric radiography were requested 8
for all patients to evaluate the titrated position of the OA and the airspace obtained. 9
Statistical tests used the Minitab, version 17, program. The level of statistical 10
significance was 5%. 11
Results Before treatment the mean AHI was 56.3 ± 19.1 events/ hour. It decreased to 8.1 12
± 5.2 after the OA titration (p <0.001). There was a significant reduction in obstructive 13
events from 43.0 ± 20.2 events/ hour to 7.1 ± 4.6 events/ hour (p <0.001). The reduction 14
in central events after OA treatment was also significant (from 5.1 ±9.3 events/ hour to 15
0.8 ±1.9 events/ hour p <0.001) whereas mixed events decreased from 6.4 ±9.5 events/ 16
hour to 0.1±0.3 events/ hour (p <0.001). The minimum oxygen saturation also showed 17
significant improvement after treatment (p<0.001). There was no statistically significant 18
difference between both OA with respect to central events (p=0.22) or mixed events 19
(p=0.98). 20
Conclusion The treatment was effective in reducing obstructive events which were 21
evaluated through the AHI and minimum oxygen saturation. The oral appliances also 22
normalized central and mixed events among patients with severe OSAS. 23
24
Key-words Oral appliances, Obstructive sleep apnea, Sleep disordered breathing, 25 Orthotic Devices 26
27
28
29

3
Introduction 1
Sleep-related breathing disorders are divided into four main categories: central 2
sleep apnea (CSA), obstructive sleep apnea (OSA), hypoventilation disorders related to 3
sleep and hypoxemia disorders related to sleep [1]. 4
CSA is a disorder characterized by repetitive cessation or reduction of both the 5
airflow and the respiratory effort during sleep [2]. When symptomatic it is called central 6
sleep apnea syndrome (CSAS) and appears to be more prevalent among elderly people, 7
males or persons who present certain medical or neurological comorbidities [3, 4]. 8
Unlike CSA, OSA is characterized by a respiratory effort against a closed upper 9
airway, showing that patients with OSA have anatomical or functional deficits in the 10
upper airway [5]. When associated with clinical signs and symptoms such as excessive 11
daytime sleepiness, cognitive impairment, decreased quality of life and increased 12
cardiovascular morbidity, it is called obstructive sleep apnea syndrome (OSAS) [6-8]. 13
In clinical practice patients, rarely present pure OSAS, and most of them exhibit 14
some central and/ or mixed events. The coexistence of more than one type of apnea 15
disorders indicates more complex underlying disorders than just the increased upper 16
airway resistance. In fact, unstable respiratory control has been implicated in the 17
pathogenesis of both central and obstructive sleep apnea [5]. 18
The treatment of sleep-related breathing disorder is mainly based on greater 19
ventilation during sleep with positive airway pressure (PAP) devices [9]. Medication is 20
rarely used, but patients suffering from CSAS may need it [1]. Oral appliances (OAs) 21
are recommended only for OSAS treatment. The literature points out three major groups 22
of intraoral appliances: the soft palate elevators, tongue-retaining devices and 23
mandibular advancement devices. The latter category is by far the most currently used 24
type of oral appliance [10]. According to the American Academy of Dental Sleep 25
Medicine (AADSM) the term ‘oral appliances’ refers to mandibular advancement 26
devices (MADs), since these are the most effective and widely used devices in clinical 27
practice. Nevertheless, such definition will be reviewed and revised as new methods and 28
evidences become available [11]. 29
Although OAs are indicated only for treatment of obstructive sleep apnea, a 30
study published in 1991 showed two cases of patients with central apnea treated with 31
OAs [12]. The pathophysiology of central sleep apnea syndrome is not fully understood, 32
4
but the obstruction of the upper airway might be a possible correlated cause [13]. The 1
relationship between central sleep apnea and partial obstruction of the upper airways 2
was suggested in a study in which not only did CPAP improve respiratory events during 3
sleep but also eliminated central sleep apnea events in patients who had narrow upper 4
airways. However, CPAP did not present positive effects on central apnea patients with 5
brainstem lesions [14]. 6
Innovations related to OAs and the OSA treatments have been discussed in the 7
literature [15, 16]. This novel type of oral appliance (the lingual orthosis proposed by 8
Caram) was first described in the literature in 2013 and it was designed to prevent the 9
obstruction of the oropharynx through a tongue control mechanism [16]. The appliance 10
can be used in combination with or as an alternative to the conventional MADs and it 11
was developed to address limitations of mandibular advancement devices, such as the 12
occurrence of temporomandibular disorders, teeth absence, severe periodontal problem, 13
patients with extensive prostheses, patients newly discharged from orthodontic 14
appliances, young patients (less than 19 years old) [15]. Although observed side effects 15
include: difficulty in swallowing, gagging, vomiting and injury to the mucosa, the 16
lingual orthosis has shown satisfactory results in cases of OSAS and has improved 17
obstructive, mixed and central events [15,16]. 18
Lingual control devices may have a mechanism similar to the lingual retainers, 19
such as neutralizing genioglossus muscle activity [17]. In addition, a lingual control 20
mechanism based on proprioceptive information acquired with tongue surface receptors 21
can help patients to maintain a tongue position preventing oropharyngeal obstruction 22
and, consequently, preventing OSA [15]. 23
The aim of this study was to evaluate the effectiveness of the OAs using 24
Caram’s lingual and combined orthoses in the treatment of OSAS and its impact on the 25
reduction of the obstructive, central and mixed apneas among patients suffering from 26
severe OSAS. 27
28
29
30
31
32
33

5
Material and Methods 1
2
Participants 3
4
Forty-eight patients referred by sleep specialists for dental clinic specialized in 5
the treatment of OSAS with OAs were recruited for the study. All selected patients had 6
a history of nonadherence to PAP. To be included in the study the patient had to present 7
a diagnosis of severe obstructive sleep apnea-hypopnea syndrome (AHI above 30 8
events/hour) with central and/or mixed components. No cutoff values were established 9
for the minimum number of central or mixed apneas for patients to be included in the 10
research. The main complaints were: snoring, daytime sleepiness and mood swings. The 11
sample presented severe OSAS (AHI above 30 events/hour), with central and / or mixed 12
components. These individuals were referred by sleep medicine centers in the city of 13
Belo Horizonte, southeastern Brazil. Informed consent forms were obtained from all the 14
participants. 15
16
Research instruments 17
18
▪ Polysomnography 19
20
The diagnosis of OSAS was accomplished through a polysomnography (PSG) 21
exam performed in a sleep laboratory. Polysomnography included 22
electroencephalography recording, right and left electro-oculogram, electromyography 23
of the genioglossus and tibialis anterior muscle, electrocardiogram and oxygen 24
saturation measured by a finger pulse oximeter. The respiratory variables were 25
recorded, including the nasal air flow by means of a thermistor and a pressure nasal 26
cannula. Respiratory effort was measured using a respiratory inductance 27
plethysmography. Snoring was recorded by a microphone and body position was 28
monitored using a piezoelectric sensor. 29
Polysomnographic recordings were scored according to the guidelines of the 30
American Academy of Sleep Medicine [18]. Obstructive apnea was defined as a ≥10-31
second cessation of airflow on the pressure nasal cannula, associated with an oronasal 32
thermal sensor. Hypopnea was defined as a ≥50% reduction in airflow, or a reduction of 33
6
airflow <50% on the nasal pressure cannula accompanied by a decrease ≥3% in oxygen 1
saturation (SpO2) or an arousal. Central apnea was defined by the absence of respiratory 2
effort throughout the entire period of absent air flow; and mixed apnea was defined by 3
the onset of the respiratory event with no airflow and no respiratory effort during the 4
first half of the event and, at the second half of the event, the absence of airflow 5
persisted even after a resumption of inspiratory effort. The minimum SpO2 (SpO2 6
nadir) was also recorded [18]. 7
All patients were subjected to two full night polysomnography recordings: the 8
first PSG was performed to diagnose sleep-related breathing disorders, it was the 9
baseline recording. Once the OA was optimally titrated resulting in symptoms 10
resolution or the titration had achieved individual tolerance, the patient was referred to 11
the sleep laboratory for polysomnography monitoring with the OA in situ. These exams 12
allowed the therapeutic effect of the titrated OA to be objectively assessed by 13
comparing the PSG results. 14
Complete response to the treatment (treatment success) was defined by an AHI 15
cut-off values of < 5/h or < 10/h. Sleep and respiratory parameters were recorded during 16
sleep at baseline and the follow-up visit using PSG recordings which were manually 17
scored according to the American Academy of Sleep Medicine (AASM) guidelines 18
[18]. The therapy was considered suboptimal when AHI decreased < 50% and/or patient 19
presented persistent symptoms. 20
21
▪ Oral appliance 22
23
The treatment for controlling obstructive apnea was performed by OA using the 24
lingual orthosis proposed by Caram [16]. This technique is applied through two devices: 25
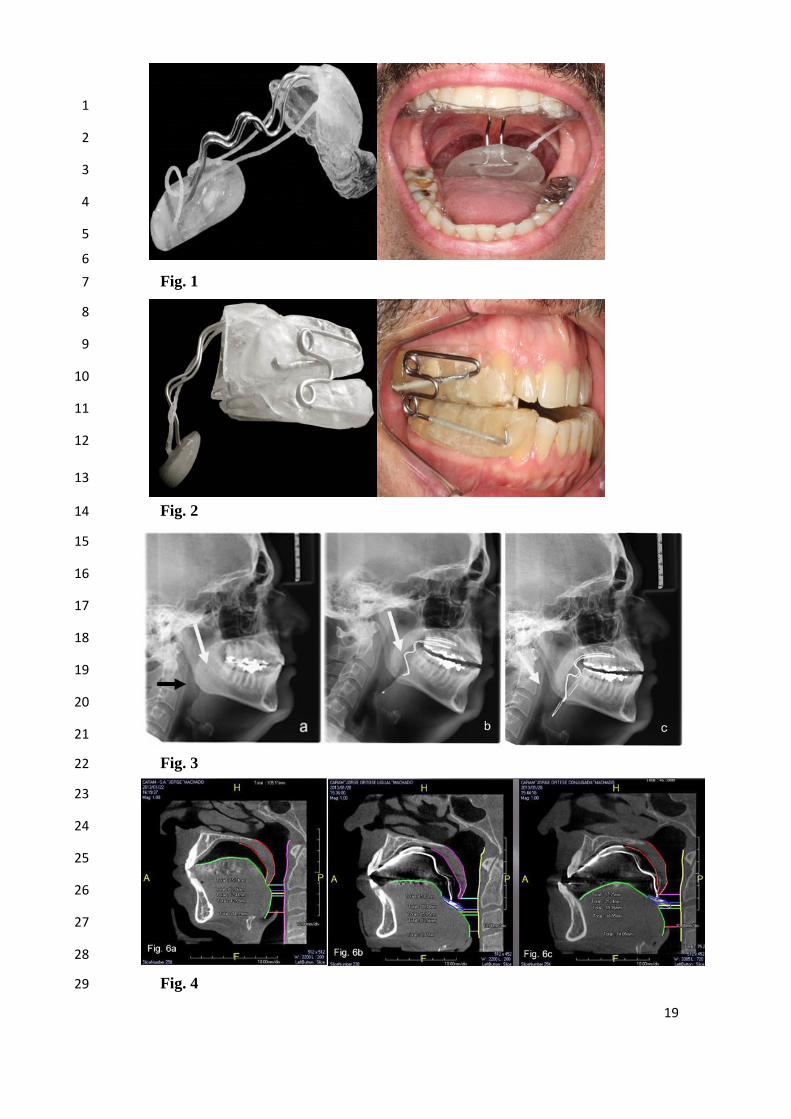
the first is designated as ‘lingual orthosis’ or ‘spring’ and it consists of a jaw fitting 26
single plate in which is attached an acrylic lingual control device (Figure 1). The second 27
device consists of an acrylic block, articulated by means of helical vestibular arcs, 28
providing mandibular advancement associated with direct mechanical action on the 29
tongue [16]. This OA is designated as ‘combined orthosis’ (Figure 2). 30
The combined orthosis was used to enhance the spring action through the 31
protrusion mechanism and stabilization of the jaw. The patients were not randomly 32
allocated to the treatment with lingual orthosis or combined orthosis. If the patient had a 33
7
history of temporomandibular disorders (TMD) or if there was no minimum number of 1
teeth for retention of the combined mandibular advancement device, the patient was 2
referred to treatment with the lingual orthosis. Thirty-six patients were treated with the 3
combined orthosis and twelve with the lingual orthosis. During titration, the mandibular 4
advancement and the lingual control device were adjusted according to the sleep dentist 5
criteria in order to provide the best risk-benefit ratio. 6
The oral appliance titration protocol consists of an initial mandibular 7
advancement set to advance the mandible between 50% to 70% of the patient’s 8
maximum protrusion. After two weeks, if the patient presents no signs or symptoms 9
related to pain or discomfort, the appliance is titrated again until it reaches 80% of 10
maximum protrusion. Once this titration has been made and the patient adhered/adapted 11
to the OA treatment, a second phase is started which consists of attaching a spring to the 12
body of the oral device. 13
The titration of the spring is done weekly or according to the patient’s adaptation 14
(biweekly or monthly). Initially, a small spring is placed and juxtaposed to the palate, 15
and during the titration it undergoes a process of stretching in which it is directed 16
towards the base of the tongue. The device is composed of two wires (caliber 1.0 mm) 17
which are stretched (titrated) in a ratio of 1 to 2 mm during each dental appointment. 18
Approximately 2 months after the oral appliance has been fitted, the wires are fully 19
extended and are supporting the acrylic retainer which must be in close contact with the 20
base of the tongue. In most cases this position achieved by the combined orthosis is 21
sufficient to treat patients with mild and moderate OSAS in whom solely the 22
mandibular advancement has no effect or who presents persistent snoring even after the 23
mandibular advancement. 24
When treating cases of severe OSAS, after the wire caliber 1.0 mm is completely 25
distended, it is replaced by a wire caliber 1.2 mm. The titration process continues to be 26
gradually conducted aiming to place the acrylic retainer towards the oropharynx and 27
pressuring the base of the tongue. The titration limit is achieved when the wire caliber 28
1.2 mm is fully extended or according to the patient’s tolerance. During the treatment, a 29
monitoring polysomnography is requested by the dentist to check if the respiratory and 30
sleep parameters improved. The exam is requested when the patient reports no 31
symptoms related to the OSAS. 32
33

8
▪ Imaging 1
In order to evaluate the titrated position of the OA and the airspace obtained 2
using the OA both computed tomography and cephalometric radiography were 3
requested for all patients (Figures 3 and 4). The images were requested after the oral 4
appliances final adjustments aiming to evaluate the positioning of the spring in relation 5
to the oropharynx tissues and avoid possible traumas to the tissues. 6
7 Statistical analysis 8
9
Statistical tests used univariate analysis by Minitab 17 © program. In order to 10
verify the requirements for parametric or nonparametric statistics Anderson Darling test 11
was used. The level of statistical significance was 5%. Mean and standard deviation 12
were the measures used for data following normal distribution. 13
Comparisons between parametric and dependent continuous variables used 14
paired t-test, and in cases of non-parametric data it was used the Wilcoxon test. 15
Comparisons between parametric and independent continuous variables used the two-16
sample t-test, and non-parametric data was compared by Mann-Whitney test. 17
18 19 Results 20 21
22 Forty-eight patients took part in this study. The sample’s age varied from 21 to 23
84 years (mean ± SD age was 53.7 ± 10.8 years), being 6 women and 42 men. At least 24
two months were required to achieve the optimal OA titration in 86% of participants; 25
and 25% of the patients required additional titration after the first monitoring PSG. The 26
mean total amount of mandibular advancement in the combined orthosis was 7.3 ± 2.1 27
mm. The time interval between fitting the OA and the monitoring PSG exam with the 28
OA in situ was 5 ± 3 months. 29
When comparing the final AHI with the baseline parameters, all patients reduced 30
their AHI by more than 50%, and the majority of them presented a complete response to 31
the treatment (72.9% achieved an AHI <10/h and 35.4% achieved an AHI <5/h). Before 32
treatment the mean AHI of the sample was 56.3 ± 19.1 events/ hour and it decreased to 33
8.1 ± 5.2 after the OA titration (p <0.001). There was a significant reduction in 34
obstructive events from 43.0 ±20.2 events/ hour to 7.1 ±4.6 events/ hour (p <0.001). 35

9
The reduction of central events after OA treatment was also significant when 1
compared to baseline events (from 5.1 ± 9.3 events/ hour to 0.8 ± 1.9 events/ hour; p 2
<0.001) whereas mixed events decreased from 6.4 ± 9.5 events/ hour to 0.1 ± 0.3 3
events/ hour (p <0.001). The minimum oxygen saturation also showed significant 4
improvement after OA treatment (71.0 ± 13.9 to 84.7 ± 4.9, p <0.001). These results are 5
summarized in Table 1. 6
The baseline AHI among patients who used lingual orthosis and combined 7
orthosis was 57.4 ± 18.4 events/ hour and 53.0 ± 21.8 events/ hour, respectively. After 8
treatment, a significant reduction in the AHI was observed among patients with lingual 9
orthosis (8.4 ± 5.5 events/ hour) and with the combined device (7.0 ± 4.2 events/ hour; p 10
= 0.42). Table 2 shows that there was no statistically significant difference between both 11
devices with respect to the AHI <5 and AHI <10 (p> 0.05). 12
Central events decreased from 3.8 ± 6.7 to 0.5 ±1.3 events/ hour among patients 13
using lingual orthosis and among patients using the combined orthosis it decreased from 14
5.6 ±10.0 to 0.9 ±2.0 events/ hour. There was no statistically significant difference 15
between both OAs (p=0.22). With respect to mixed events, after treatment both orthosis 16
showed significant improvements and there was no statistically significant difference 17
between the two types of devices (p=0.98) (Table 2). 18
Treatment with both devices significantly improved minimum oxygen saturation 19
from 71.0 ± 13.9 to 84.7 ± 4.9 (p <0.001), but there was no statistically significant 20
difference between the two types of devices (p> 0.05) (Table 1 and Table 2). In one 21
case, the AHI was reduced from 64.5 events/hour to 19.5 events/ hour, the central 22
events increased from 0.5 to 2.8 events/hour and mixed events slightly decreased from 23
9.8 to 7.0 events/hour. In a single case, in which the AHI decreased from 66.4 to 16.8 24
events/ hour, there was a simultaneous worsening in central apneas, which increased 25
from 0.2 to 3.2 events/hour, and mixed apneas that increased from 0 to 1.8 events/hour. 26
27
28 29 Discussion 30
31
In this study, the sample consisted of patients noncompliant with CPAP who had 32
severe OSA. The sample presented predominantly obstructive apnea events, but they 33
also suffered from central and mixed apnea events. There was no control group, but the 34
10
main objective of the present research was to evaluate the short-term effectiveness of 1
the OA using Caram’s lingual orthosis and combined orthosis in patients with severe 2
OSA who dropped out the CPAP treatment. Treatment with these OAs aimed to 3
improve obstructive apneas, but the results also showed an equally effective control of 4
mixed and central events, as well as in the minimum oxygen saturation. 5
The phenotypes that have current treatment options for central sleep apnea are 6
upper airway collapsibility, chemoreflex activation level and sleep fragmentation 7
propensity [19]. We believe that the results of the present study using Caram’s lingual 8
and combined orthosis may have been achieved due to the patient’s collapsibility 9
phenotype. 10
Thirty-six patients used the combined orthosis which was composed of a lingual 11
control device associated with plaques embedded in the upper and lower arches for 12
mandibular advancement. The use of a combined orthosis aimed to potentiate the action 13
of the spring mechanism allowing the protrusion and stabilization of the mandible in 14
order to maintain a patent upper airway during sleep. Radiographs showed a greater 15
increase in the upper airway with the combined orthosis. However, the lingual orthosis 16
showed a higher number of patients with AHI <5 and AHI <10, although this difference 17
was not significant. After treatment both devices, lingual and combined orthoses, 18
significantly improved the AHI. Central and mixed events also improved significantly 19
with both OAs, with no statistically significant difference between them. 20
Mandibular advancement devices are the most widely used type of oral 21
appliance and those with greater scientific evidence of effectiveness, but as more 22
evidence becomes available, new devices may be considered in the treatment of OSAS. 23
Furthermore, clinical judgment (such as the individual requirements of patients that may 24
dictate alternative methods) must be respected. The definition established by AADSM 25
related to mandibular advancement appliances should serve as a clinically relevant 26
standard for the selection of oral appliances by sleep dental practitioners and as a guide 27
to facilitate development of the next generation of OAs design [11]. 28
The intraoral devices with lingual controls used in this study were developed by 29
one of the authors (JMC) and were designed to prevent further slip of the tongue and the 30
consequent oropharynx obstruction. Devices using similar lingual control mechanisms 31
have already been discussed in the literature [15]. 32
11
The OAs using Caram’s lingual technique have a lingual control accessory or 1
"spring" that allows an activation to ensure complete resolution of obstructive 2
respiratory events [16]. Adjustments in the spring depend on each case. It may be mild 3
and limited up to the base of the tongue, or may be more vigorous and deep enough to 4
reach the area of the epiglottis. Clinical success is evaluated by a lack or reduction of 5
snoring and improvements in the sleep quality. Polysomnography is performed to 6
objectively evaluate the OAs effectiveness. It is conducted after a positive report of the 7
patient with respect to his symptomatology. The average period of treatment to achieve 8
clinical success is 4 to 6 months. 9
In this study, some patients presented worsening in central and mixed events 10
after the treatment. We realized that patients with mixed apneas tend to respond more 11
easily to the obstructive apnea control, even in the few cases in which the central events 12
worsen. By analyzing the possible causes of this worsening we could not find any 13
explanation related to the clinical aspects of OAs. All OAs were checked a week before 14
the PSG examination. 15
Treatment-emergent central sleep apnea has been described especially after the 16
positive airway pressure (PAP) therapy. Moreover, it is important to be aware that 17
central apneas may also arise from treatment with OAs [20]. However, these devices 18
have been used with reasonable success in patients with complex sleep apnea who are 19
intolerant to PAP. Residual AHI can occur with OAs requiring adjuvant therapy. Once 20
OAs are less likely to induce hypocapnia but treatment of obstructions is less precise, 21
‘cocktails’ have been currently used and they include oral appliance + benzodiazepine 22
or acetazolamide, or supplemental oxygen [19]. 23
In our clinical practice, we observe that the polysomnography of patients with 24
OSA often do not exhibit central and mixed events in the reports. We believe that this 25
happens once scores of respiratory events in patients with sleep apnea have traditionally 26
been directed to an obstructive phenotype, even with the update of the 2007 American 27
Academy of Sleep Medicine guidelines, which has criteria for scoring central 28
hypopneas and short sequences of periodic breathing / Cheyne-Stokes respiration [21]. 29
The rules for scoring respiratory events state that central hypopneas should not 30
be marked in the presence of flow limitation, although the obstruction is a common 31
feature of central events [19]. Direct visualization of the upper airway often shows 32
collapse at the nadir of the cycle, even in polysomnographic "central" disease [22]. 33

12
Expiratory pharyngeal narrowing occurs during central during central hypocapnic 1
hypopnea, supporting the concept that the presence of flow limitation alone cannot be 2
used to distinguish obstructive and central hypopneas [23, 24]. 3
We consider that a score of central and mixed events in polysomnography is 4
important not only to evaluate baseline events in sleep-related breathing disorders, but it 5
should also be taken into consideration when analyzing the criteria used to estimate 6
therapies success. 7
In the present study, there was a 100% response rate, which means that no 8
patient discontinued the treatment. The side effects and possible treatment 9
abandonment/ non-adherence were not analyzed. However, the main complaints pointed 10
out by the patients related to the treatment were recorded and divided into 4 categories: 11
A) Swallowing difficulty. We understand that the swallowing physiology includes 12
lifting the back of the tongue, which suffers a movement limitation due to the spring 13
retainer. However, the tongue is a functional and elastic muscle capable of adapting to 14
this restriction and it can develop alternative movements. After 2 weeks using the oral 15
appliance, nearly 90% of the patients reported they were not having trouble swallowing 16
(dysphagia). B) Gagging. This initial tongue restriction may cause an accumulation of 17
saliva and it can trigger eventual gagging. In the present study, this side effect was 18
rarely reported; C) Vomiting. It may emerge from a physiological cause such as an 19
exaggerated gag reflex related to the appliance being placed deep into the throat and 20
often happens just after fitting the oral appliance. This side effect is reported by nearly 21
80% of patients. 22
Furthermore, sometimes it is necessary to place the spring in a position far 23
below the oropharynx and the deeper the appliance is placed, the more the patient may 24
use the vomiting as a defense mechanism. All the side effects mentioned before may 25
occur when initially fitting the oral appliance but they are transitory events; D) Injury to 26
the mucosa. Although it is not supposed to happen, the spring may traumatize the 27
tongue, palate and/or the throat tissues if the device itself or the appliance titration is 28
incorrectly conducted. Therefore, it is of paramount importance an image 29
(cephalometric radiograph) to verify the spring positioning. 30
Moreover, by analyzing the computed tomography and the cephalometric 31
radiography the dentist can conduct a more detailed adjustment/ titration, providing a 32
perfect juxtaposition of the spring and the tongue retainer. In several cases, the 33
13
cephalometric radiography demonstrated that the space in the oropharynx had been 1
reduced by the action of the spring. However, the result on PSG parameters did not 2
worsen, probably due to the action of the spring preventing the tongue and soft palate 3
falling back against the posterior pharyngeal wall, and thereby preserving the airway 4
patency. 5
The present study has some limitations. Some patients underwent the baseline 6
and after-treatment polysomnography in different sleep laboratories. However, the 7
laboratories used the same polysomnographic parameters and the same guidelines of the 8
American Academy of Sleep Medicine (AASM) for the elaboration of the reports, 9
allowing the parameters standardization and comparison of results. 10
Furthermore, there was no control group and the participants were not 11
randomized, therefore it is not possible to state whether the analyzed appliances 12
improve treatment beyond mandibular advancement alone. Nevertheless, the main 13
objective of the present study was to evaluate the efficacy of the lingual and combined 14
orthoses in patients with severe OSAS who dropped out CPAP treatment and required 15
mandatory treatment. Further studies, such as randomized clinical trials, should be 16
conducted to compare this novel appliance to the existing mandibular advancement 17
devices which have already proven their efficacy by the scientific evidence. 18
19
20
Conclusions 21
22
It was observed that treatments using Caram’s lingual and combined OAs were 23
effective in reducing obstructive events which were evaluated through the AHI and 24
minimum oxygen saturation. It was also observed a significant effectiveness in 25
normalizing central and mixed events among patients with severe OSAS. 26
More studies are needed to better understand and clarify the relationship 27
between obstructive, central and mixed events and the impact of OAs on sleep-related 28
breathing disorders. 29
30
Funding 31
No funding was received for this research. 32
33
14
Conflict of Interest 1
All authors certify that they have no affiliations with or involvement in any 2
organization or entity with any financial interest (such as honoraria; educational grants; 3
participation in speakers' bureaus; membership, employment, consultancies, stock 4
ownership, or other equity interest; and expert testimony or patent-licensing 5
arrangements), or non-financial interest (such as personal or professional relationships, 6
affiliations, knowledge or beliefs) in the subject matter or materials discussed in this 7
manuscript. 8
9
Ethical approval 10
All procedures performed in studies involving human participants were in accordance 11
with the ethical standards of the institutional and/or national research committee and 12
with the 1964 Helsinki declaration and its later amendments or comparable ethical 13
standards. 14
15
Informed consent 16
Informed consent was obtained from all individual participants included in the study. 17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
15
References 1
2
1. Thorpy M (2015) Classification of sleep disorders. In: Guglietta A (ed) Drug 3
Treatment of Sleep Disorders, 1st edn. Springer, New York, pp 71-83 4
2. American Academy of Sleep Medicine (2014) International Classification of 5
Sleep Disorders, 3rd edn. Darien, IL : American Academy of Sleep Medicine 6
3. Bixler EO, Vgontzas AN, Ten HT, Tyson K, Kales A (1998) Effects of age on 7
sleep apnea in men: I. Prevalence and severity. Am J Respir Crit Care Med. doi: 8
10.1164/ajrccm.157.1.9706079 9
4. Guilleminault C, van den Hoed J, Mitler M (1978) Clinical overview of the sleep 10
apnea syndromes. In: Guilleminault C, Dement W (eds) Sleep apnea 11
syndromes. Alan R Liss, New York, pp 1-11 12
5. Xie A, Bedekar A, Skatrud JB, Teodorescu M, Gong Y, Dempsey JA (2011) 13
The heterogeneity of obstructive sleep apnea (predominant obstructive vs pure 14
obstructive apnea). Sleep. doi: 10.5665/SLEEP.1040. 15
6. American Academy of Sleep Medicine Task Force (1999) Sleep-related 16
breathing disorders in adults: recommendations for syndrome definition and 17
measurement techniques in clinical research. Sleep 22: 667-689 18
7. Barbé, Pericás J, Muñoz A, Findley L, Antó JM, Agustí AG (1998) Automobile 19
accidents in patients with sleep apnea syndrome. An epidemiological and 20
mechanistic study. Am J Respir Crit Care Med 158:18-22 21
8. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V 22
(2005) Obstructive sleep apnea as a risk factor for stroke and death. N Engl J 23
Med 353:2034-2041 24
9. Aurora RN, Chowdhuri S, Ramar K et al (2012) The treatment of central sleep 25
apnea syndromes in adults: practice parameters with an evidence-based 26
literature review and meta-analyses.Sleep 35:17-40. 27
10. Hoffstein V (2007) Review of oral appliances for treatment of sleep-disordered 28
breathing. Sleep Breath 11:1-22. 29
11. Scherr SC, Dort LC, Almeida FR et al (2014) Definition of an effective oral 30
appliance for the treatment of obstructive sleep apnea and snoring: a report of 31
the American Academy of Dental Sleep Medicine. J Dent Sleep Med 1:39-50 32
16
12. Farrow SJ (1991) Successful treatment of central sleep apnea with an oral 1
prosthesis. Chest 100:1461-1462 2
13. Bradley TD, McNicholas WT, Rutherford R, Popkin J, Zamel N, Phillipson EA 3
(1986) Clinical and physiologic heterogeneity of the central sleep apnea 4
syndrome. Am Rev Respir Dis 134:217-21 5
14. Guilleminault C, Quera-Salva MA, Nino-Murcia G, Partinen M (1987) Central 6
sleep apnea and partial obstruction of the upper airway. Ann Neurol 21:465-469 7
15. Singh GD, Keropian B, Pillar G (2009) Effects of the full breath solution 8
appliance for the treatment of obstructive sleep apnea: a preliminary study. 9
Cranio 27:109-117 10
16. Caram JM, Quintela MM (2013) The lingual orthosis - a new proposed oral 11
appliance for severe sleep apnea – case reports. Ortho Sci 6:110-117 12
17. Ono T, Lowe AA, Ferguson KA, Fleetham JA (1996) A tongue retaining 13
device and sleep-state genioglossus muscle activity in patients with obstructive 14
sleep apnea. Angle Orthod 66:273-280 15
18. Iber C, Ancoli-Israel S, Chesson AL, Jr., Quan SF (2007) The AASM Manual 16
for the Scoring of Sleep and Associated Events: Rules, Terminology, and 17
Technical Specifications, 1st edn. Westchester, IL: American Academy of Sleep 18
Medicine. 19
19. Thomas RJ (2014) Alternative approaches to treatment of Central Sleep Apnea. 20
Sleep Med Clin 9:87-104 21
20. Mohan A, Henderson J, Mador MJ (2016) Mandibular Advancement Device-22
Emergent Central Sleep Apnea Can Resolve Spontaneously: A Case Report. J 23
Clin Sleep Med 12:137-138 24
21. Berry RB, Budhiraja R, Gottlieb DJ et al (2012) Rules for scoring respiratory 25
events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and 26
Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of 27
the American Academy of Sleep Medicine. J Clin Sleep Med 8:597-619 28
22. Badr MS, Toiber F, Skatrud JB, Dempsey J (1995) Pharyngeal 29
narrowing/occlusion during central sleep apnea. J Appl Physiol (1985) 78:1806-30
1815 31
17
23. Thomas RJ, Tamisier R, Boucher J et al (2007) Nocturnal hypoxia exposure 1
with simulated altitude for 14 days does not significantly alter working memory 2
or vigilance in humans. Sleep 30:1195-1203 3
24. Sankri-Tarbichi AG, Rowley JA, Badr MS (2009) Expiratory pharyngeal 4
narrowing during central hypocapnic hypopnea. Am J Respir Crit Care Med 5
179:313-319 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
18
Fig. 1 Caram’s lingual orthosis 1
Fig. 2 Caram’s combined orthosis 2
Fig. 3 (a) Baseline: the sagittal plane shows the close relationship between the soft 3 palate and tongue. Note that both structures are in contact (white arrow) and oropharynx 4 is narrow (black arrow), (b) The sagittal plane shows the change related to the soft 5 palate and the tongue position when Caram’s lingual orthosis is in situ. It can be 6 observed a space between both structures promoted by Caram’s lingual orthosis (white 7
arrow), (c) The sagittal plane shows a change in the soft palate and tongue relationship 8 after the lingual orthosis titration. It can be observed an increase in the oropharynx 9 caliber (white arrow) 10 11 Fig. 4 (a) Baseline: the sagittal plane shows the soft palate and tongue in normal 12
occlusion without the lingual orthosis, (b) shows the change related to the soft palate 13 and the tongue position when Caram’s lingual orthosis is in situ, (c) The sagittal plane 14 shows a change in the soft palate and tongue relationship when Caram’s combined 15
orthosis is in situ. It can be observed an increase in the caliber of the oropharynx with 16 both orthoses, but the increase was even higher when the combined orthosis was used. 17
18
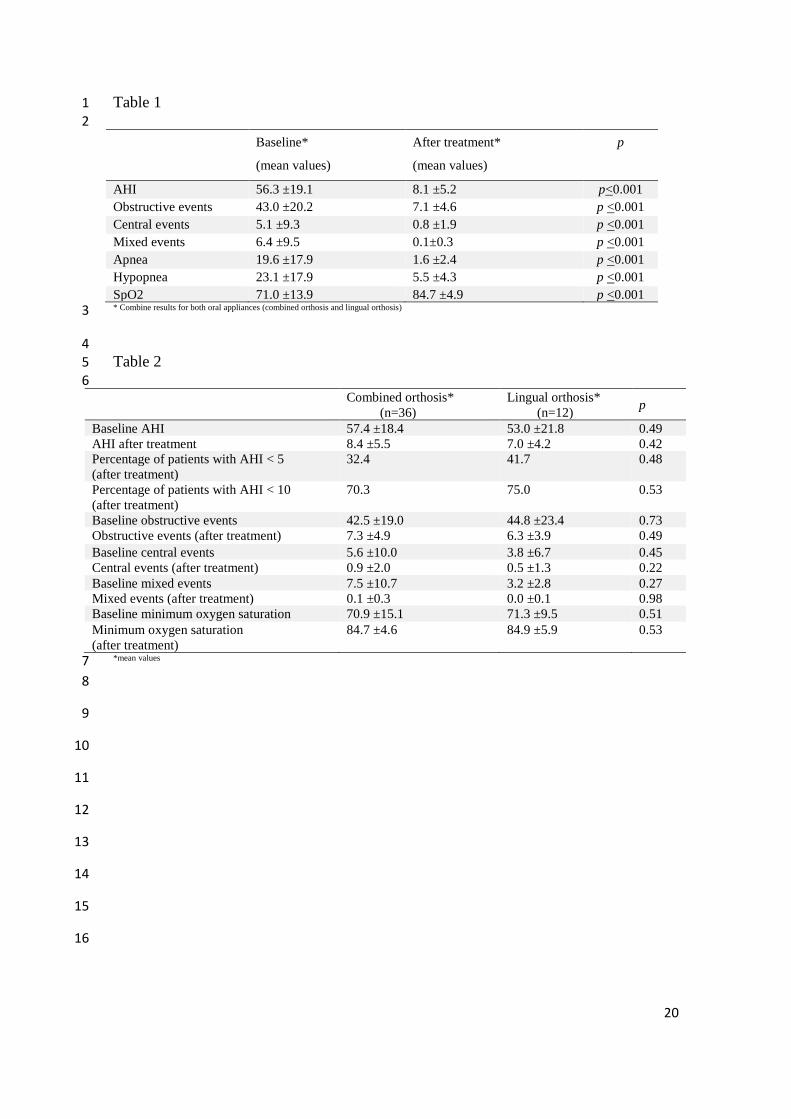
Table 1 Polysomnographic respiratory parameters after lingual orthosis and combined 19 orthosis titration 20
21 Table 2 Effects of lingual orthosis and combined orthosis on respiratory parameters 22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
19
1
2
3
4
5
6
Fig. 1 7
8
9
10
11
12
13
Fig. 2 14
15
16
17
18
19
20
21
Fig. 3 22
23
24
25
26
27
28
Fig. 4 29
20
Table 1 1
2
Baseline*
(mean values)
After treatment*
(mean values)
p
AHI 56.3 ±19.1 8.1 ±5.2 p<0.001
Obstructive events 43.0 ±20.2 7.1 ±4.6 p <0.001
Central events 5.1 ±9.3 0.8 ±1.9 p <0.001
Mixed events 6.4 ±9.5 0.1±0.3 p <0.001
Apnea 19.6 ±17.9 1.6 ±2.4 p <0.001
Hypopnea 23.1 ±17.9 5.5 ±4.3 p <0.001
SpO2 71.0 ±13.9 84.7 ±4.9 p <0.001 * Combine results for both oral appliances (combined orthosis and lingual orthosis) 3
4 Table 2 5
6
Combined orthosis*
(n=36)
Lingual orthosis*
(n=12) p
Baseline AHI 57.4 ±18.4 53.0 ±21.8 0.49
AHI after treatment 8.4 ±5.5 7.0 ±4.2 0.42
Percentage of patients with AHI < 5
(after treatment)
32.4 41.7 0.48
Percentage of patients with AHI < 10
(after treatment)
70.3 75.0 0.53
Baseline obstructive events 42.5 ±19.0 44.8 ±23.4 0.73
Obstructive events (after treatment) 7.3 ±4.9 6.3 ±3.9 0.49
Baseline central events 5.6 ±10.0 3.8 ±6.7 0.45
Central events (after treatment) 0.9 ±2.0 0.5 ±1.3 0.22
Baseline mixed events 7.5 ±10.7 3.2 ±2.8 0.27
Mixed events (after treatment) 0.1 ±0.3 0.0 ±0.1 0.98
Baseline minimum oxygen saturation 70.9 ±15.1 71.3 ±9.5 0.51
Minimum oxygen saturation
(after treatment)
84.7 ±4.6 84.9 ±5.9 0.53
*mean values 7
8
9
10
11
12
13
14
15
16





























