Embed Size (px)
Citation preview
EUROPEAN FORUM
*** * * * * * * ***
of tlrt IIISlIrtlnCt IIBII"'st «ccldents tlf wo,,,
lI11d occlIPtlflOIlIl' dlse«ses
"' DGUV Deutsche Gesetzliche Unfallversicherung Spitzenverband
Adding Value through International Cooperation Conference, Dresden June 21 to 22, 2011
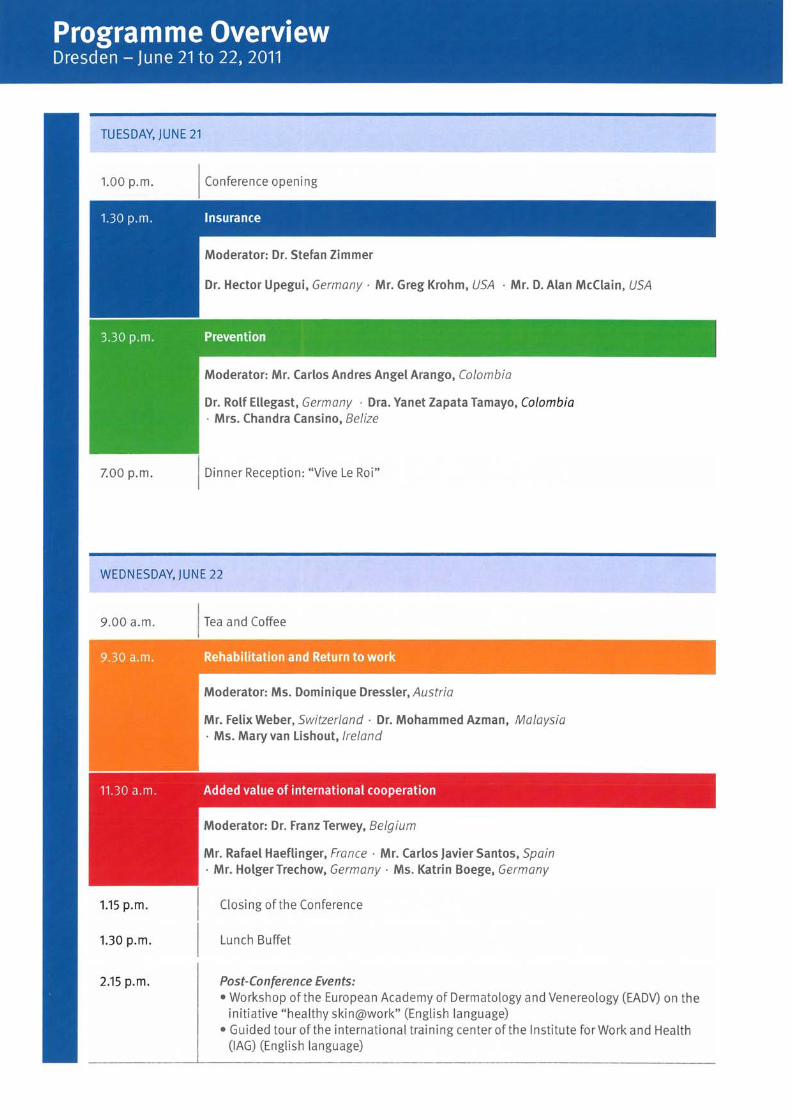
TU ESDAY, jUNE 21
1.00 p.m .
7.00 p.m.
Conference opening
Moderator: Mr. Carlos Andres Angel Arango, Ca/ambia
Dr. Rolf Ellegast, Germany . Dra. Yanet Zapata Tamayo, Ca/ambia · Mrs. Chandra Cansino, Be/ize
Dinner Reception: "Vive Le Roi"
WEDNESDAY, jUNE 22
9.00 a.m.
1.15 p.m .
1.30 p.m.
2.15 p.m.
Moderator: Ms. Dominique Dressler, Austria
Mr. Felix Weber, Switzer/and . Dr. Mohammed Azman, Ma/aysia · Ms. Mary van lishout, Ire/and
Moderator: Dr. Franz Terwey, Be/gium
Mr. Rafael Haeflinger, France . Mr. Carlos javier Santos, Spain · Mr. HolgerTrechow, Germany . Ms. Katrin Boege, Germany
Closing ofthe Conference
Lunch Buffet
Post-Conference Events: • Workshop ofthe European Academy of Dermatology and Venereology (EADV) on the
initiative "healthy skin@work" (English language) • Guided tour ofthe international training center of the Institute for Work and Health
(lAG) (English language)
tt • • AddingValue through
International Cooperation Conference, Dresden June 21 10 22, 2011
14:00-18:00
15:00-17:00
18:00-18:30
18:30-19:30
19:30
21,06,2011
9:00-17:00
9:00-10:00
10:00-12:00
12:00-13:00
13:00-13:30
13:30-15:00
15:00-15:30
15:30-17:30
19:00
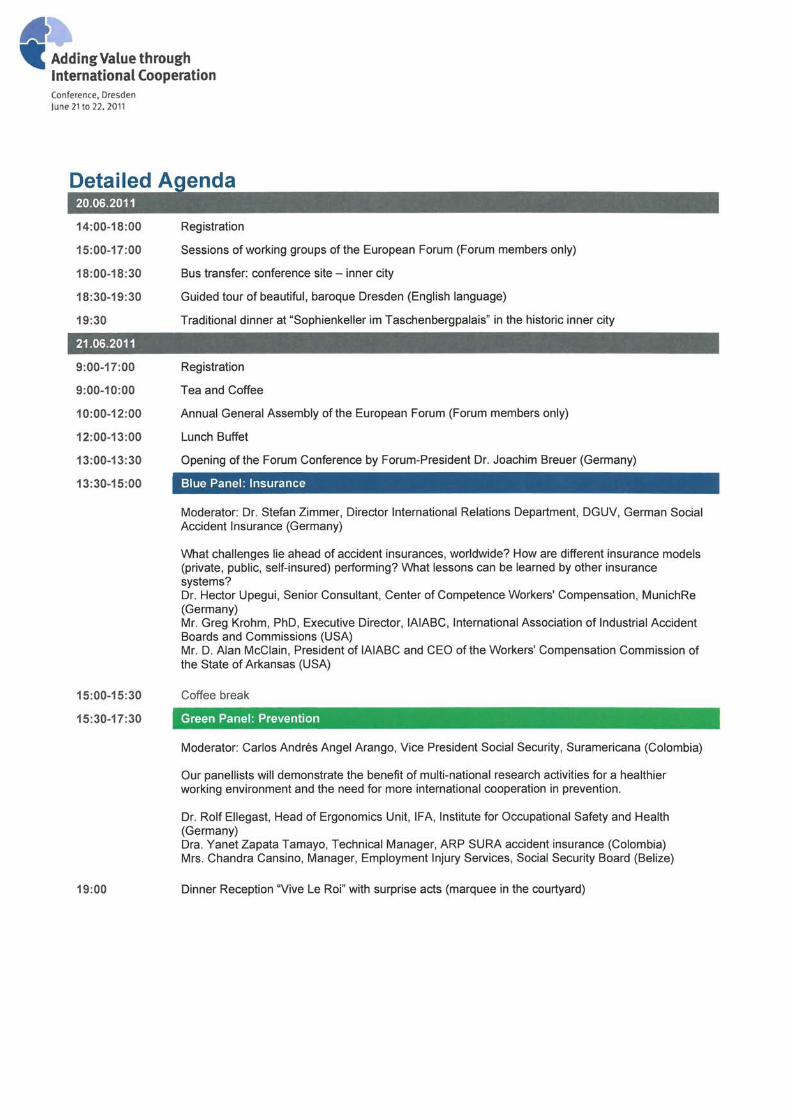
Registration
Sessions of working groups of the European Forum (Forum members only)
Bus transfer: conference site - inner city
Guided tour of beautiful, baroque Dresden (English language)
Traditional dinner at "Sophienkeller im Taschenbergpalais" in the historie inner city
Registration
T ea and Coffee
Annual General Assembly of the European Forum (Forum members only)
Lunch Buffet
Opening of the Forum Conference by Forum-President Dr. Joachim Breuer (Germany)
Blue Panel: Insurance
Moderator: Dr. Stefan Zimmer, Director International Relations Department, DGUV, German Social Accident Insurance (Germany)
What challenges lie ahead of accident insuranees, worldwide? How are different insurance models (private, public, self-insured) performing? What lessons can be learned by other insurance systems? Dr. Hector Upegui, Senior Consultant, Center of Competence Workers' Compensation, MuniehRe (Germany) Mr. Greg Krohm, PhD, Executive Director, lAIABC, International Association of Industrial Accident Boards and Commissions (USA) Mr. D. Alan McClain, President of lAIABC and CEO ofthe Workers' Compensation Commission of the State of Arkansas (USA)
Coffee break
Green Panel: Prevention
Moderator: Carlos Andres Angel Arango, Vice President Social Security, Suramericana (Colombia)
Our panellists will demonstrate the benefit of multi-national research activities for a healthier working environment and the need for more international cooperation in prevention.
Dr. Rolf Ellegast, Head of Ergonomies Unit, IFA, Institute for Occupational Safety and Health (Germany) Dra. Yanet Zapata Tamayo, Technical Manager, ARP SURA accident insurance (Colombia) Mrs. Chandra Cansino, Manager, Employment Injury Services, Social Security Board (Belize)
Dinner Reception "Vive Le Roi" with surprise acts (marquee in the court yard)
I!I • AddingValue through
International Cooperation Conference. Dresden /une 21 to 22. 2011
22.06.2011
9: 00-09:30
9:30-11:00
11 :00-11 :30
11:30-13:00
13:15-13:30
13:30-14:15
14:15-15:30
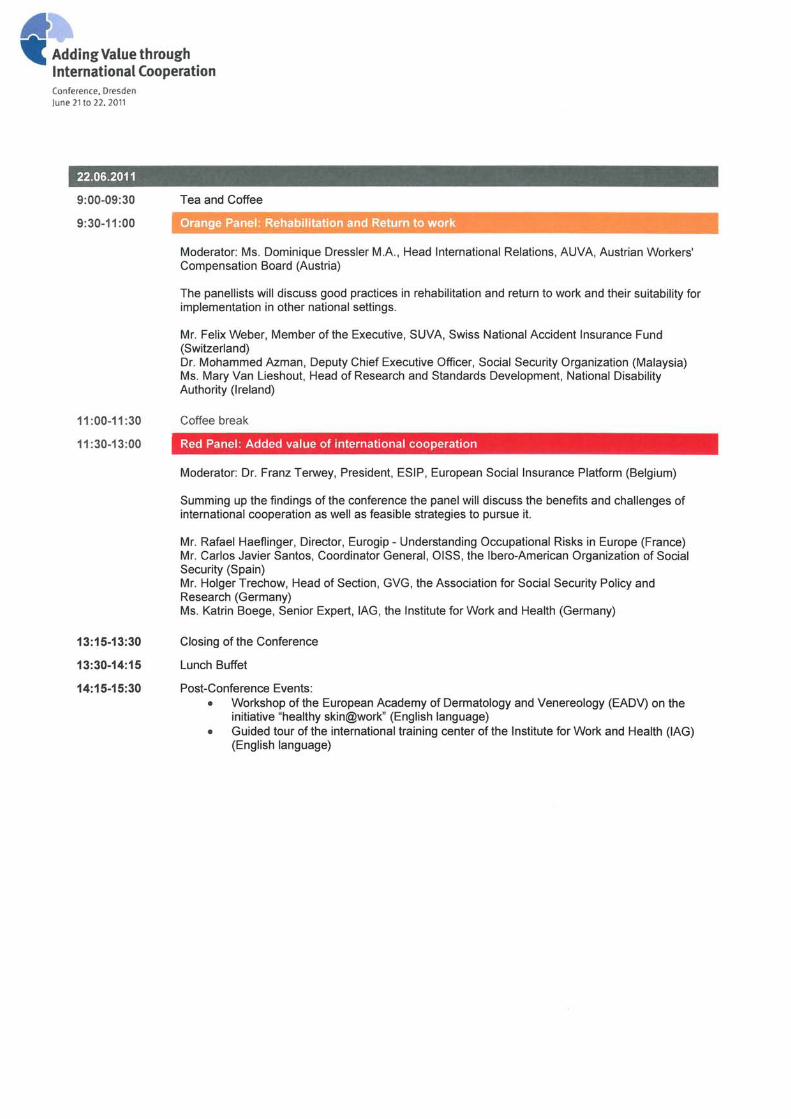
Tea and Coffee
Orange Panel: Rehabilitation and Return to work
Moderator: Ms. Dominique Dressler MA, Head International Relations, AUVA, Austrian Workers' Compensation Board (Austria)
The panellists will discuss good practices in rehabilitation and return to work and their suitability for implementation in other national settings.
Mr. Felix Weber, Member of the Executive, SUVA, Swiss National Accident Insurance Fund (Switzerland) Dr. Mohammed Azman, Deputy Chief Executive Officer, Social Security Organization (Malaysia) Ms. Mary Van Lieshout, Head of Research and Standards Development, NationalDisability Authority (Ireland)
Coffee break
Red Panel: Added value of international cooperation
Moderator: Dr. Franz Terwey, President, ESIP, European Sociallnsurance Platform (Belgium)
Summing up the findings of the conference the panel will discuss the benefits and challenges of international cooperation as weil as feasible strategies to pursue it.
Mr. Rafael Haeflinger, Director, Eurogip - Understanding Occupational Risks in Europe (France) Mr. Carlos Javier Santos, Coordinator General, OISS, the Ibero-American Organization of Social Security (Spain) Mr. Holger Trechow, Head of Section, GVG, the Association for Social Security Policy and Research (Germany) Ms. Katrin Boege, Senior Expert, lAG, the Institute for Work and Health (Germany)
Closing of the Conference
Lunch Buffet
Post-Conference Events: • Workshop of the European Academy of Dermatology and Venereology (EADV) on the
initiative "healthy skin@work" (English language) • Guided tour of the international training center of the Institute for Work and Health (lAG)
(English language)
European Forum Of The Insurance Against Accidents At Work
And Occupational Diseases
Abstract: RTW ‐ The Malaysian Perspective ‐ Is it an investment?
By Dr. Mohammed Azman Bin Aziz Mohammed
The presenter will give a brief overview of the Social Security Organisation of Malaysia and its
benefits under social insurance schemes. The main topic of this presentation would be the
Return to Work (RTW) Program, which was introduced by SOCSO to rehabilitate workers who
have been injured during work; and also those seeking invalidity pension. The RTW program is
basically a disability management program; which is a collaborative process that facilitates
recommended efficient treatment plans to assure that the appropriate medical care is provided
to disabled, ill or injured individuals. It is also about planning and coordination of health care
services appropriate to achieve the goal of medical rehabilitation. The program may include,
but is not limited to, care assessment, including personal interview with the client, and
assistance in developing, implementing and coordinating a medical care plan with healthcare
providers, as well as the clients and his/her family, and evaluation of treatment results while
promoting cost‐effective care. The presenter will also share experience in terms of socio‐
economic benefits and how it has impacted the related stakeholder due to disability of an injury
or a disease.

Social Security Organisation of Malaysia
European Forum Of The Insurance Against Accidents At Work And Occupational Diseases
Adding Value Through International Cooperation
RTW ‐
The Malaysian Perspective ‐
Is it an investment?
DR. MOHAMMED AZMAN BIN AZIZ MOHAMMED
Deputy Chief Executive Officer
SOCIAL SECURITY ORGANIZATION MALAYSIA (SOCSO)
21‐22 June 2011
Dresden, Germany
1
Social Security Organisation of Malaysia
2
• Overview on SOCSO
• SOCSO’s RTW Program– Chronology– Concept– Legal Mandate
• Returns? Investment?
• Conclusion
Scope of Presentation
Social Security Organisation of Malaysia
Malaysia
Capital: Kuala Lumpur
Land Area: 329,845sqm
Population: 28million (approx.)
Climate: Tropical (avrg. 33 degrees Celsius), Rain and shine all year round.
Social Security Organisation of Malaysia
Social Security Organisation of Malaysia
Overview of the Social Security Organisation, Malaysia
(SOCSO)

Social Security Organisation of Malaysia
• Statutory Organisation governing
Employment Injury Insurance Scheme &
Invalidity Pension Scheme in Malaysia.
• CORPORATE GOAL ‐
To provide
comprehensive social security
protectionprotection
for Malaysians.
• CORPORATE OBJECTIVE ‐
To ensure
and guarantee the timely and adequate
provision of benefits in a socially just
manner and to promote occupational to promote occupational
health and safetyhealth and safety.
SOCSO
Social Security Organisation of Malaysia
• Currently insuring 13.2 million workers & 727,744 employers
(All workers with income of RM3000 (≈
€700) and below).• Contribution of 2.25% of the average salary
(1.25% Employment Injury Scheme –
Funded by Employer & 1% for Invalidity Pension scheme –
Equally Shared by Employer &
Employee)• Manage over 78,000 Claims/per year
• Over 55,000 accidents • Over 13,000 permanently disabled• Over 10,000 Claiming for invalidity (≈3000 certified invalid)
SOCSO
Social Security Organisation of Malaysia
SOCSO’s Return to Work Program
Social Security Organisation of Malaysia
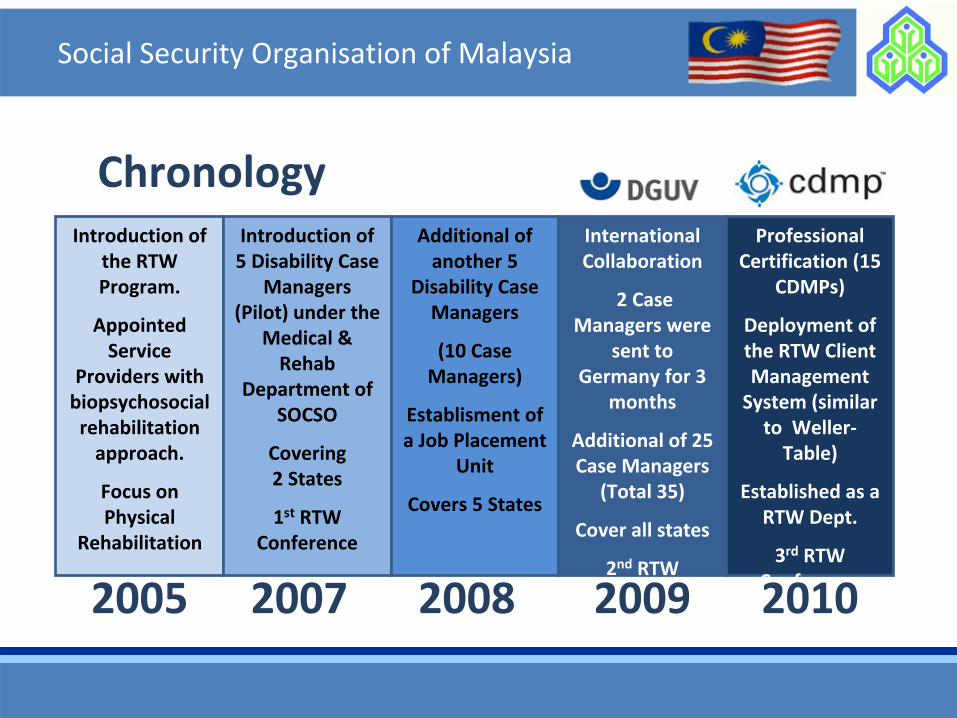
ChronologyIntroduction of
the RTW
Program.
Appointed
Service
Providers with
biopsychosocial
rehabilitation
approach.
Focus on
Physical
Rehabilitation
Introduction of
5 Disability Case
Managers
(Pilot) under the
Medical &
Rehab
Department of
SOCSO
Covering 2 States
1st
RTW
Conference
Additional of
another 5
Disability Case
Managers
(10 Case
Managers)
Establisment of
a Job Placement
Unit
Covers 5 States
International
Collaboration
2 Case
Managers were
sent to
Germany for 3
months
Additional of 25
Case Managers(Total 35)
Cover all states
2nd
RTW
Conference
Professional
Certification (15
CDMPs)
Deployment of
the RTW Client
Management
System (similar
to Weller‐
Table)
Established as a
RTW Dept.
3rd
RTW
Conference2005 2007 2008 2009 2010
Social Security Organisation of Malaysia
Case Management is a collaborative process that facilitates
recommended efficient treatment plans to assure the
appropriate medical care is provided to disabled, ill or injured
individuals.
Planning and coordination of health care services appropriate to
achieve the goal of medical rehabilitation. Medical case
management may include, but is not limited to, care
assessment, including personal interview with the client, and
assistance in developing, implementing and coordinating a
medical care plan with healthcare providers, as well as the
clients and his/her family evaluation of treatment results while
promoting cost‐effective care.
Concept of Case ManagementCase Management is a collaborative process that facilitatesfacilitates
recommended efficientefficient
treatment plans to assure the
appropriate medical careappropriate medical care
is provided to disabled, ill or injured
individuals.
Planning and coordination of health care services appropriate to
achieve the goal of medical rehabilitationachieve the goal of medical rehabilitation. Medical case
management may include, but is not limited to, care care
assessmentassessment, including personal interview with the client, and
assistance in developingin developing, implementingimplementing
and coordinating a coordinating a
medical care planmedical care plan
with healthcare providershealthcare providers, as well as the
clientsclients
and his/her familyhis/her family
evaluation of treatment resultsevaluation of treatment results
while
promoting costpromoting cost‐‐effective careeffective care.
Social Security Organisation of Malaysia
RTW
Service Providers
Coordinating Treatment/Rehabilitation
Related Stakeholders
(employers, family, etc
Insurer (SOCSO)Facilitate
Social Security Organisation of Malaysia
Section 40 (1) The Organization may, in addition to the scheme of
benefits specified in this Act, promote measures or co‐ operate with existing institutions for the improvement of the health, occupational safety and welfare of
insured persons and for the rehabilitationfor the rehabilitation
and rere‐‐ employmentemployment
of insured persons who have been
disabled or injured and may incur in respect of such measures expenditure from the funds of the
Organization within such limits as may be prescribed by the Minister.
Legal Mandate
Social Security Organisation of Malaysia
Section 57 (1) An insured person suffering from or claiming to
suffer from invalidity or permanent disablement may be provided by the Organization, free of charge facilities free of charge facilities
forforphysicalphysical
or vocational rehabilitationvocational rehabilitation.
(2) Facilities under subsection (1) shall be of such nature nature and scaleand scale
and shall be provided to such insured persons
and on such conditions as may be specified by theregulations.
Legal Mandate

Social Security Organisation of Malaysia
Returns? Investment? You decide
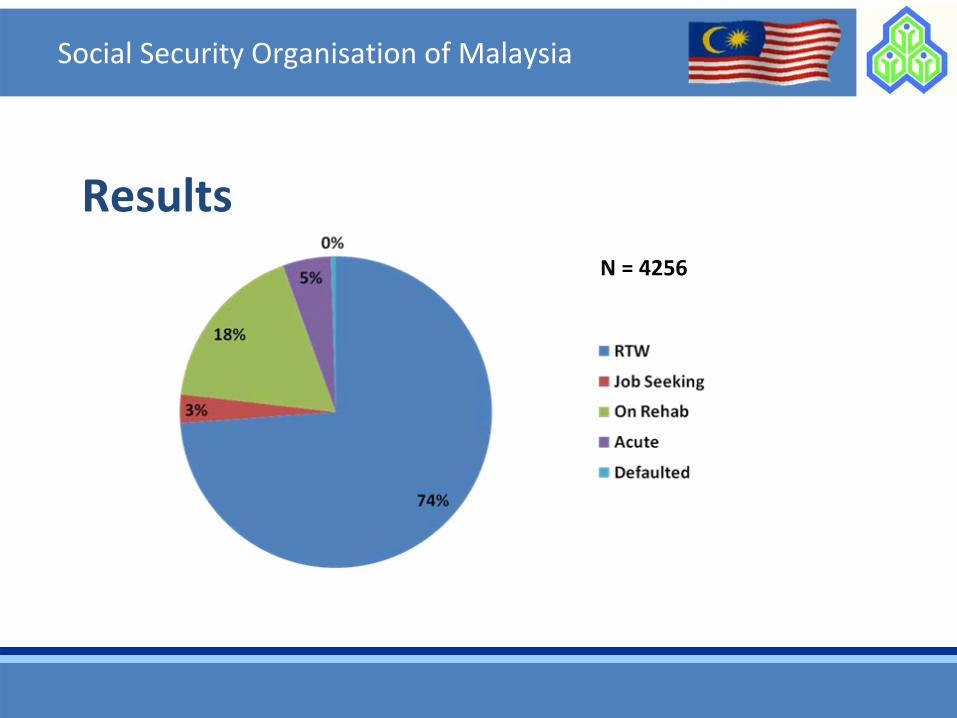
Results
Social Security Organisation of Malaysia
N = 4256
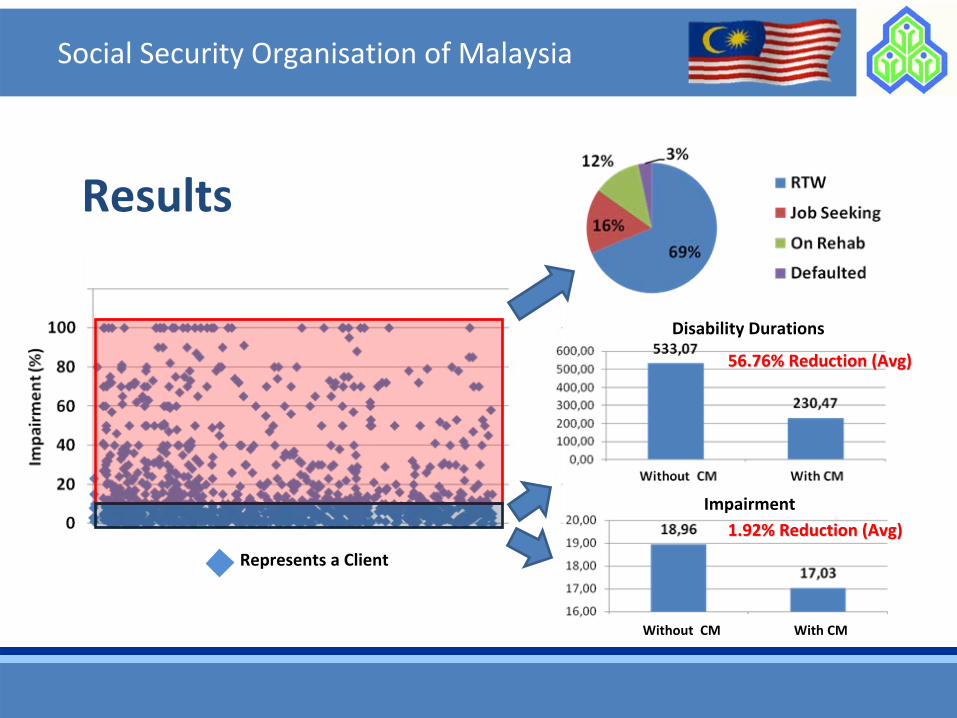
Results
Social Security Organisation of Malaysia
Represents a Client
Disability Durations
56.76% Reduction (Avg)56.76% Reduction (Avg)
Impairment
1.92% Reduction (Avg)1.92% Reduction (Avg)
Without CM With CM
Social Security Organisation of Malaysia
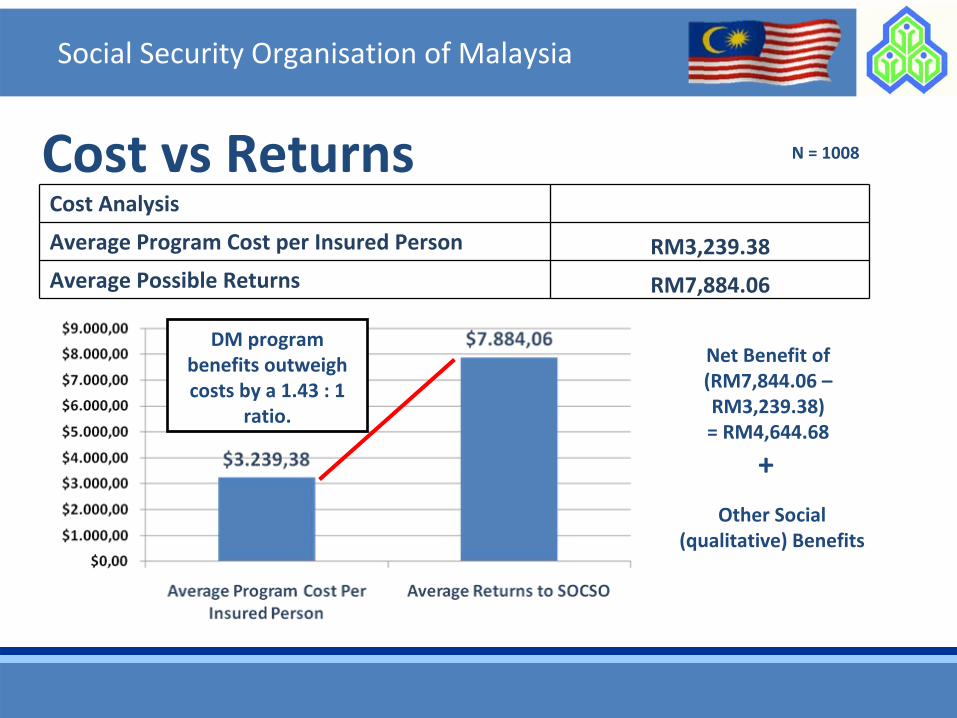
Cost vs ReturnsCost Analysis
Average Program Cost per Insured Person RM3,239.38
Average Possible Returns RM7,884.06
Net Benefit of(RM7,844.06 –
RM3,239.38)= RM4,644.68
Other Social
(qualitative) Benefits
+
DM program
benefits outweigh
costs by a 1.43 : 1
ratio.
N = 1008
Social Security Organisation of Malaysia
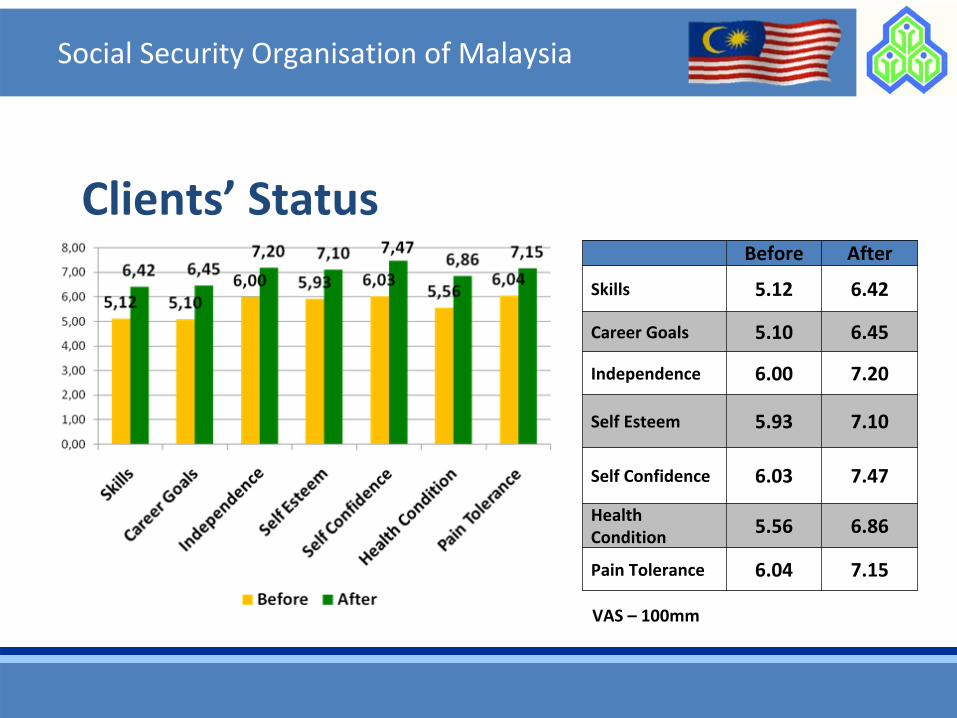
Before After
Skills 5.12 6.42
Career Goals 5.10 6.45
Independence 6.00 7.20
Self Esteem 5.93 7.10
Self Confidence 6.03 7.47
Health Condition
5.56 6.86
Pain Tolerance 6.04 7.15
VAS –
100mm
Clients’
Status
Social Security Organisation of Malaysia
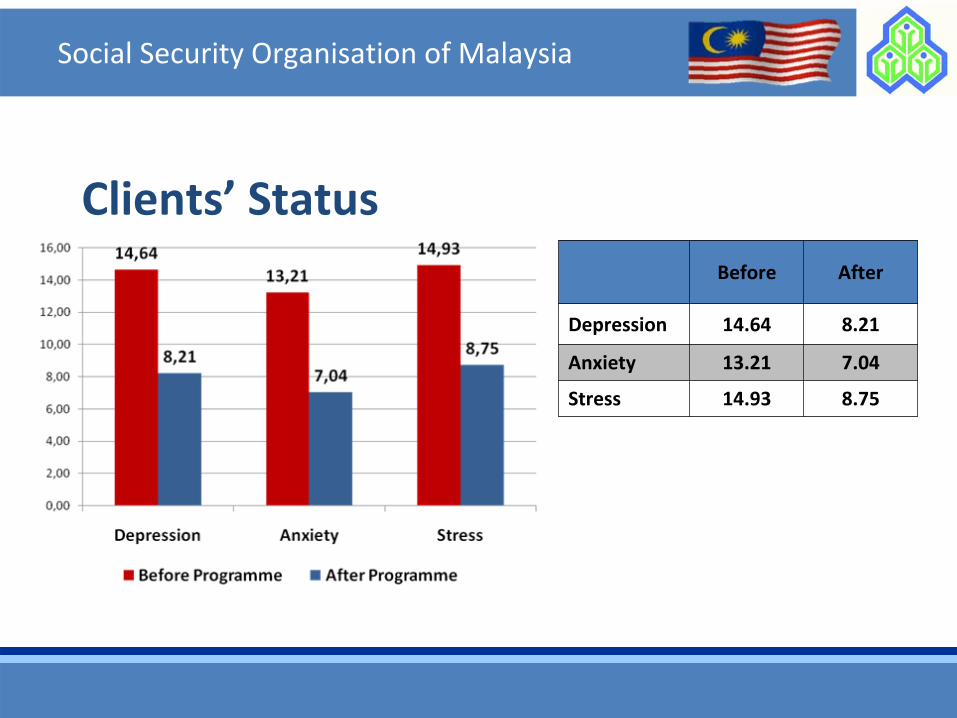
Before After
Depression 14.64 8.21
Anxiety 13.21 7.04
Stress 14.93 8.75
Clients’
Status
Social Security Organisation of Malaysia
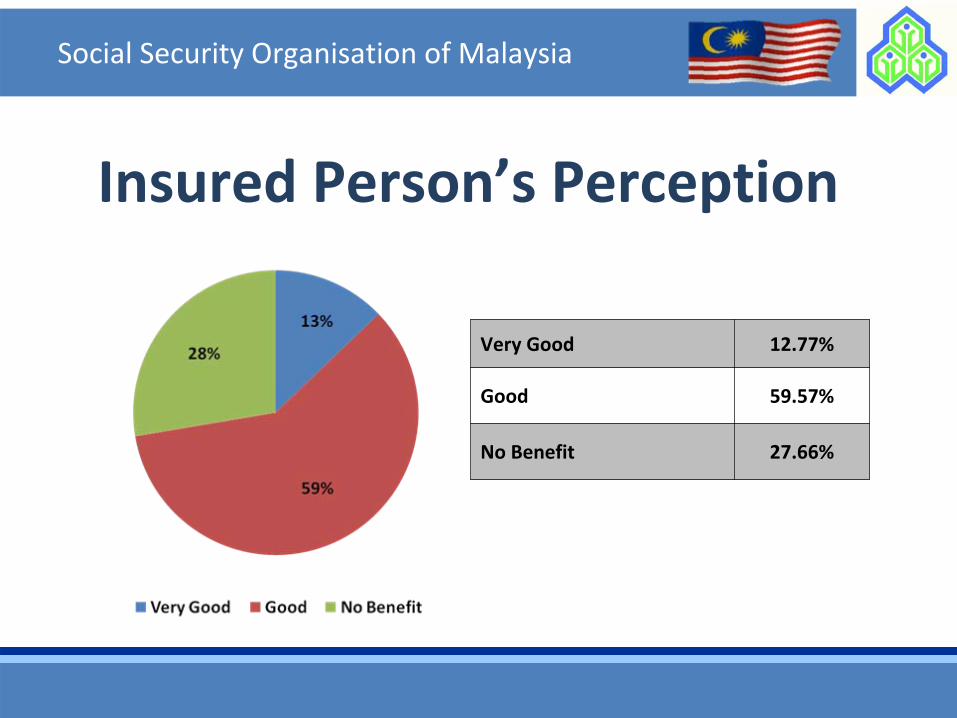
Insured Person’s Perception
Very Good 12.77%
Good 59.57%
No Benefit 27.66%
Social Security Organisation of Malaysia
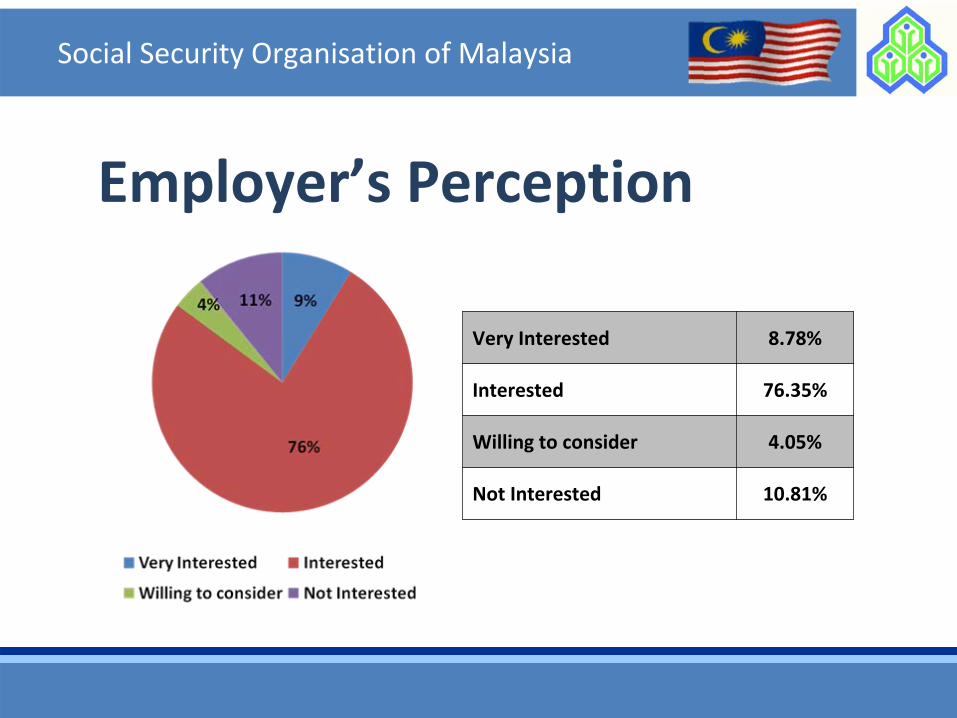
Employer’s Perception
Very Interested 8.78%
Interested 76.35%
Willing to consider 4.05%
Not Interested 10.81%

Social Security Organisation of Malaysia
• Fiscal Aspects• Addressing Health/Disability• Psychosocial Improvements• Employees’ Perception• Employers’ Perception
Returns of RTW/DM Strategies
Conclusion
• Work is a social right!
• The ultimate objective of social security systems is to honour benefits when they are due ‐
First of all, the
Social Security System must be sustainable.
• A Social Security System which include
and not exclude.
• Investing in People – Creating Opportunities, not sympathy.
Social Security Organisation of Malaysia
Yes – Oui – Sí – Ya ‐ (Shi)
Social Security Organisation of Malaysia
Returns? Is it an investment?
Thank you
Social Security Organisation of Malaysia
Social Security Organisation
+6 03 4264 5480

www.perkeso.gov.my
Breaking Down Barriers and Moving ForwardBreaking Down Barriers and Moving ForwardReturn to Work Conference Return to Work Conference ––
Kuala Lumpur 2011Kuala Lumpur 2011
Venue: Putra World Trade Centre (PWTC), 4Venue: Putra World Trade Centre (PWTC), 4thth
––
55thth
July 2011July 2011www.rtwmalaysia.com
PERKESOPERKESO

International OSH Seminars at the Institute for Work and Health, Dresden
Katrin Boege, Senior Expert
International Cooperation, IAG

In the area of globalization
Safety and Health not only a national issue
DGUV cooperates at international levelDGUV cooperates at international level
IAG received delegations from Russia, Turkey, Italy, Korea,
Singapore..

IAG expertise
Training courses for:
Labour inspectorsLabour inspectorsSafety officersOccupational physiciansTrainers in occupational safety and health

Increasing international cooperation
leads to growing demand for international
seminars

International Seminars
•OSH Management Systems
•Labour Inspection•Labour Inspection
•Basic Occupational Health
•Risk Assessment
•Train-the-Trainer
International Seminars
• Modules last 1 – 2 days
International Seminars
•In English
•In other languages translated from German •In other languages translated from German

Practical facilities
Ergonomics
Noise Woodwork
Metalwork

Why International Seminars?
DGUV's policy of internationalizing prevention work
OSH standards may be exported in the medium term
DGUV´s autonomous administration's objective:
Making the world of work more humane

Questions? Interested? Contact us
Katrin Boege
International Cooperation and International Trainings International Cooperation and International Trainings
Institute Work and Health
01099 Dresden
Email: [email protected]
Phone: +49 351 4571124
Fax: +49 351 457201124

Katrin Boege
Short Abstract:
In the era of globalization, safety and health at the workplace are not merely a
national issue. For this reason, the DGUV and its institutes co-operate with numerous
institutions and organizations at international level. The IAG has already trained OSH
experts from Russia, Italy and Turkey, just to name a few. Delegations from Korea,
Singapore and China have also sought information on the IAG's training provision.
This led to the idea of offering training which is tailored specifically to the needs of
prevention experts in other countries. In this presentation, the international seminar
programme will be presented together with some of the ideas underlying the rationale
of this form of international cooperation.
Chandra Cansino
My presentation will give an overview of Accident Insurance for work related accidents in Be-lize. Since I fall more in the category of need for more international cooperation, the presenta-tion will highlight the areas that my country needs or can use some collaboration as well as dis-cuss some of the things we already have in place. I will also share a little information on Beli-ze.
09.06.2011L:\CONITZER\FORUMDresdenJun2011\Redner_Abstract\green_panel_prevention\Cansino\Cansino_abstract.doc
Accident Insurance The Belize experience
1
Adding Value through International Cooperation
Conference, DresdenJune 21 to 22, 2011
Presentation Overview
1.
Some quick facts about Belize2.
Accident Insurance in Belize – Overview
3.
Qualifying conditions4.
Coverage
5.
Prevention Strategies6.
Limitations
7.
Recommendations8.
What we have
9.
What we need
2
3
Quick facts about Belize
•
Population: approx. 310,000 people•
Size: 8866 sq. miles or 22,963 sq. km.
•
Belize is both Caribbean and Central American•
Multi‐ethnic
•
Climate : Sub‐Tropical (55F or 12C to 100F or 36C)•
Government: Parliamentary Democracy
•
Language: Official –
English over 50% speak Spanish•
Largest unbroken; second largest unbroken barrier reef
in the world.
World Map
4
5
Map of Belize
6
Accident Insurance
•
All Belizeans have the option to purchase private insurance
•
Private insurance companies do not cover work‐ related accidents
•
Social Security covers all registered workers for accidents that occur on the job
•
In most case this amounts to 100% coverage in both private and public medical institutions after the
claim is allowed
Who qualifies for on‐the‐job Accident Insurance?
•
Any registered person from age 14 (this is the age a person can legally join the workforce in Belize)
•
Both employed and self‐employed persons
7
What are the conditions to qualify?
•
Be registered with Social Security
•
Employers are legally bound to hire only registered workers and pay contributions on their behalf (Not so
with self‐employed – voluntary)
•
Person has to have been injured during
and in the course of insurable employment
•
Qualifies as of Day 1
8
Coverage
All Medical care recommended by treating Doctor until person can return to work including:
•Hospitalization•Pharmaceuticals•Labs•Diagnostic testing •Rehabilitation (physical and psychological therapy)•Other medical needs such as wheelchairs, specialized
beds, walkers, etc.
9
Coverage cont’d
•
The injured person has the right to request a second opinion
•
While on leave from work the person is paid 80% of his insurable earnings
•
Every injured person is entitled to claim for Disablement benefit
10
Prevention Strategy
Some done by SSB as much as possible including:•Investigation and identification of hazards•Recommendations for recurrence•Documentation to Employers•Employer and Employee education on good
Occupational Safety and Health practices
11
Limitations
•
The OSH Legislation has yet to be passed by Cabinet•
SSB OSH Inspectors can make recommendations but
cannot enforce •
VERY little training and VERY little expertise in the
country•
SSB can educate the workers but cannot obligate them
to practice OSH•
SSB is bound by law to allow all claims whether or not it
was caused by employer or employee negligence •
There are no incentives for lowering the amount and/or
severity of work accidents (exception for those companies who have to meet international standards)
12
Recommendations
•
Organization and guidance of the NOSH/Working Committee
•
Aggressive lobbying by SSB for passage of the OSH Law•
Develop an incentive system to “award”
both workers
and employers who make efforts in OSH•
Training, training, training! Needed at all levels in the
area of OSH and accident prevention and investigation
13
What we have
•
Commitment – 10 years of writing and revising the present Legislation draft
•
Representation – Tri‐partite representation including workers’
unions on the NOSH/Working Committee
•
Some expertise
•
Some support from CARICOM and other international groups
14
What we need
Training at ALL levels including: •Medical – Eg. Occupational medicine (presently GP’s and other general
Specialists diagnose Occupational illnesses) •Inspectorate •Management
OSH Information System
Expertise in utilizing the available information to develop Accident Prevention in Belize
Consultancies to assist with the organization of National Committees
15
What does Belize have to offer you?
•
Most beautiful place on earth
•
Belize has a very functional National Health Insurance system still in its pilot phase instrumental in ensuring
better primary health care (also under Social Security)
16
Why should you come to Belize?
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
Thank you and see you soon!
33
34
PREVENTION OF WORK-RELATED MSDS – THE BENEFIT OF INTERNATIONAL COOPERATIONS
Dr. Rolf Ellegast
Institute for Occupational Health and Safety of the German Social Accident Insurance (IFA), Sankt Augustin, Germany
Musculoskeletal disorders (MSDs) are frequently described as a "national disease", since one person in two complains of problems in this comprehensive and complex area. MSDs are of immense importance in the occupational sphere. In Germany and many countries in Europe work-related musculoskeletal disorders are those causing the highest direct costs (costs of treatment) and indirect costs (loss of production owing to sick leaves), and for many years have led the statistics for working days lost owing to incapacity for work broken down by diagnostic group.
International cooperations of accident insurances can help to find preventive measures to tackle work-related MSDs. The presentation will give examples of
common strategies to prevent occupational diseases, joint research programs and technical developments and cooperation approaches to cope with new emerging risks.

1
Prevention of work-related MSDs –The benefit of international cooperations
Dr. Rolf Ellegast
IFA – Institute for Occupational Health and Safety of theGerman Social Accident Insurance, Germany
Outline
� Introduction: Work-related MSDs in Europe and German y
� International cooperation on work-related MSD preve ntion
� Common strategies to prevent occupational diseases
� Joint research programs and technical developments
� Coping with new emerging risks
� Conclusions
� Benefits of international cooperation on MSD prevention
� Future offers and needs
2
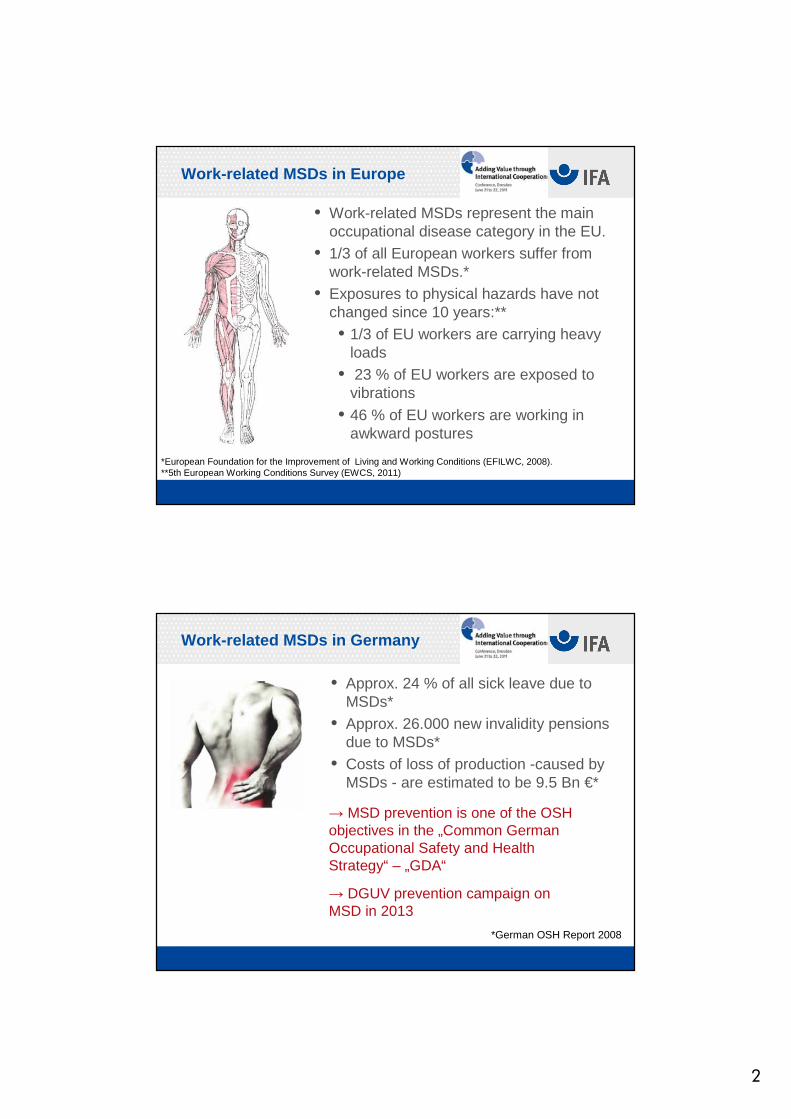
Work-related MSDs in Europe
• Work-related MSDs represent the main occupational disease category in the EU.
• 1/3 of all European workers suffer from work-related MSDs.*
• Exposures to physical hazards have not changed since 10 years:**• 1/3 of EU workers are carrying heavy
loads• 23 % of EU workers are exposed to
vibrations
• 46 % of EU workers are working in awkward postures
*European Foundation for the Improvement of Living and Working Conditions (EFILWC, 2008).**5th European Working Conditions Survey (EWCS, 2011)
Work-related MSDs in Germany
• Approx. 24 % of all sick leave due to MSDs*
• Approx. 26.000 new invalidity pensions due to MSDs*
• Costs of loss of production -caused by MSDs - are estimated to be 9.5 Bn €*
→ MSD prevention is one of the OSH objectives in the „Common German Occupational Safety and Health Strategy“ – „GDA“
→ DGUV prevention campaign on MSD in 2013
*German OSH Report 2008

3
MSDs as occupational diseases in Germany
• Upper limb:• Diseases due to overstraining tendon
sheaths, peritendineum or muscular and tendonous insertions (2101)
• Osteoarticular diseases of the hands and wrists caused by mechanical vibration (2103)
• Carpal Tunnel Syndrome CTS (21XX)
• Spine:• Intervertebral disc-based diseases of the
lumbar or cervical spine (2108, 2109, 2110)
• Lower limb:• Meniscus lesions (2102 )• Knee osteoarthritis (2112)
International cooperation on work-relatedMSD prevention
Common strategies to prevent occupational diseases
•CTS was introduced as occupational disease in Columbia since several years.
• 45 % of all MSDs are due to CTS.• Experiences with associated risk factors and affected professions/tasks exist.
• Ongoing prevention activities in Colombian companies
4
International cooperation on work-relatedMSD prevention
Common strategies to prevent occupational diseases
•Cooperation project in the Colombian Floriculture Sector with
• > 90.000 employees in the Colombian Floricultural sector
• Ergonomic intervention study to improve workplaces and the understanding of CTS risk factors
• Application of common risk assessment tools, e. g. CUELA measurements
→ Presentation of Yanet Zapata Tamayo
International cooperation on work-relatedMSD prevention
Common strategies to prevent occupational diseases
•Future aim: Development of common international exposure data bases
• Cooperation with Lund University Hospital, Sweden
• Similar structure of risk factors and associated tasks
• Interfaces to other MSD exposure databases, e. g. vibrations, spinal loads
CTS Database

5
International cooperation on work-relatedMSD prevention
Common strategies to prevent occupational diseases
•Spinal workloads: cooperation with Canadian accident insurances, IRSST, Montreal, Quebec
•Project “911”: Assessment of spinal exposures of emergency medical assistants
•Application of common risk assessment tools, e. g. CUELA measurements
• Development of preventive measures
International cooperation on work-relatedMSD prevention
Joint research programs and technical developments
• International cooperation with accident insurances and university institutes to develop biomechanical models within joint research
• Aim: Calculation of internal muskuloskeletal loads during the performance of work tasks
• On basis of the results better task specific prevention measures can be derived

6
International cooperation on work-relatedMSD prevention
Joint research programs and technical developments
•Development and calibration of measurement systems for long-term physical exposure assessment
•Cooperation with Canadian University of Sherbrooke und IRSST
• Aim: quality control of ergonomic workplace assessments
International cooperation on work-relatedMSD prevention
Joint research programs and technical developments
•Technical developments to tackle combined physical risks
•Cooperation with Loughborough University and INRS in France to develop and test a measuring system for combined assessment of whole body vibration and awkward postures
• Use of research results in international standardization
7
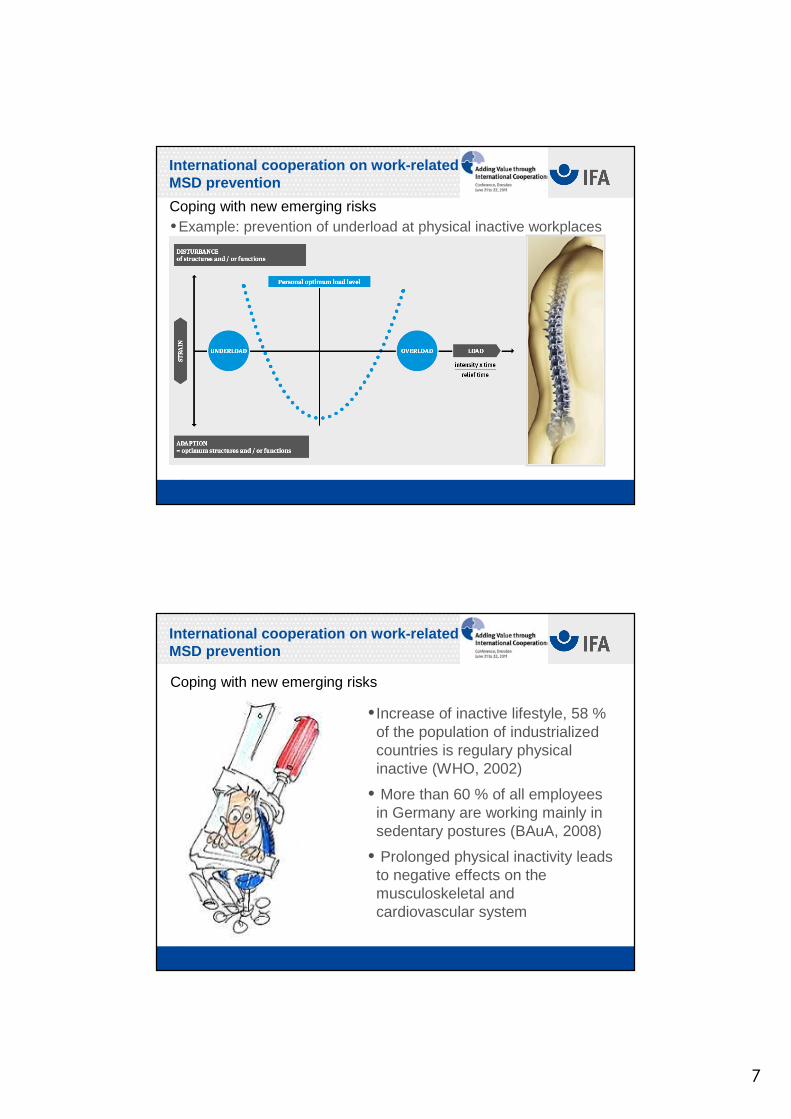
International cooperation on work-relatedMSD prevention
Coping with new emerging risks•Example: prevention of underload at physical inactive workplaces
International cooperation on work-relatedMSD prevention
Coping with new emerging risks
• Increase of inactive lifestyle, 58 % of the population of industrialized countries is regulary physical inactive (WHO, 2002)
• More than 60 % of all employees in Germany are working mainly in sedentary postures (BAuA, 2008)
• Prolonged physical inactivity leads to negative effects on the musculoskeletal and cardiovascular system
8
International cooperation on work-relatedMSD prevention
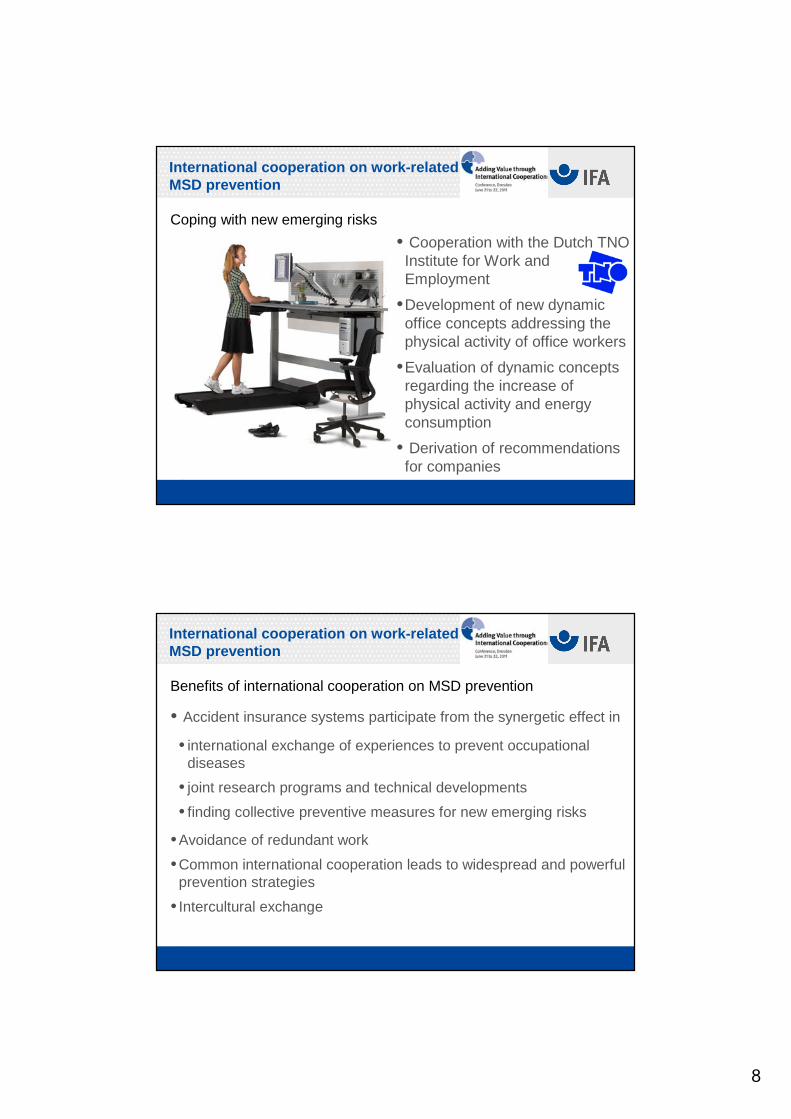
Coping with new emerging risks
• Cooperation with the Dutch TNO Institute for Work and Employment
•Development of new dynamic office concepts addressing the physical activity of office workers
•Evaluation of dynamic concepts regarding the increase of physical activity and energy consumption
• Derivation of recommendations for companies
International cooperation on work-relatedMSD prevention
Benefits of international cooperation on MSD prevention
• Accident insurance systems participate from the synergetic effect in
• international exchange of experiences to prevent occupational diseases
• joint research programs and technical developments
• finding collective preventive measures for new emerging risks
•Avoidance of redundant work
•Common international cooperation leads to widespread and powerful prevention strategies
• Intercultural exchange

9
International cooperation on work-relatedMSD prevention
Future offers and needs
• Invitation to accident insurers to
• share our national knowledge on MSD prevention and occupational diseases
• use common exposure databases and technical equipment
• Need in exchange of experiences in
• coping with new occupational diseases, e.g. lower limb disorders
• conducting a prevention campaign on MSD/LBP
THANK YOU for your attention !
Further information:
www.dguv.de/ifawww.dguv.de/d/ifa/fac/ergonomie/index.html
Contact details:Dr. Rolf EllegastInstitute for Occupational Health and Safety ofthe German Social Accident Insuarance – IFAAlte Heerstraße 111, 53757 Sankt Augustin, Germany www.dguv/ifa.de [email protected]: 02241-231-2605 Fax: 02241-231-2234
EUROPEAN FORUM Dresde - 21-22 juin 2011 Speaker : Raphaël HAEFLINGER, EUROGIP
Name: Raphaël HAEFLINGER
Name of Organisation: EUROGIP
Title of Presentation: Échange de connaissances et d'expertises sur les risques professionnels en Europe : l'expérience d’EUROGIP
The presentation will be given in French
No Power Point Presentation Abstract Échange de connaissances et d'expertises sur les risques professionnels en Europe : l'expérience d’EUROGIP La coopération européenne est à la base même de la mission d'EUROGIP depuis sa création en 1991. Les formes de coopération sont variées : bilatérale sur des sujets spécifiques ou multilatérale à travers le Forum européen par exemple. EUROGIP agit selon ces deux approches, complémentaires, qu'il privilégie en fonction des objectifs poursuivis. À travers différents exemples seront présentées les principales activités d’EUROGIP dans le domaine de l’assurance AT/MP qui mettent en œuvre des coopérations avec d’autres pays ou organismes. En termes de bilan, l’échange de connaissances et d’expériences sur l’assurance AT/MP se révèle indispensable dans un processus de convergence des différents systèmes et approches assurancielles. Malgré les nombreuses différences selon les pays, des problématiques d’intérêt commun existent en Europe et au-delà, sur divers aspects (juridique, statistiques, prévention…). Si la multiplication des lieux et des niveaux d’échanges est indispensable, il serait indéniablement utile d’optimiser la mise à disposition et la circulation des connaissances existantes.
EUROGIP EUROGIP est un groupement d'intérêt public (GIP) constitué en 1991 par la Caisse nationale de l'assurance maladie des travailleurs salariés (CNAMTS) et l’Institut national de recherche et de sécurité (INRS). Ses activités se concentrent sur les aspects européens des accidents du travail et des maladies professionnelles (AT-MP). À ce titre, EUROGIP :
réalise des enquêtes comparatives sur les risques professionnels en Europe ;
publie des lettres d'information électroniques, des rapports d’enquêtes, des notes thématiques... ;
organise des conférences, les Débats d’EUROGIP, sur des thématiques européennes de sécurité et santé au travail ;
participe à des projets d’intérêt communautaire ;
coordonne un réseau d’experts (Branche AT-MP) qui participent à l’élaboration des normes européennes et internationales ;
assure le secrétariat des Coordinations françaises des organismes notifiés pour la certification réglementaire des équipements de protection individuelle et des machines (par délégation des ministères chargés du Travail et de l’Agriculture) ainsi que le secrétariat technique de la Coordination européenne "Machines" (contrat avec la Commission européenne).
Facing Future Challenges in Workers’ Compensation: Private
Insurance– the US ExampleGregory Krohm
Executive DirectorInternational Association of Industrial Accident Boards and Commissions (IAIABC)
Conference of the European Forum Dresden, GermanyJune 21-22, 2011
US Private Insurance
• History of development• Strengths • Weakness• Applicability of the US model elsewhere
Development
• From its advent in 1911, private funding of benefits was the norm for the US workers’ comp system– Only six states established single payer
government funds• Private WC insurance became a highly
standardized/uniform across states– Much different than other property/liability
insurance in the US
How Did Standards Develop?
• Private insurance in the US has similarity and uniformity in:– Insurance agreements– Rate classifications– Rate making methods– Experience rating– Reporting of claims and premium– Reporting proof of coverage to regulators
• This uniformity is largely due to the establishment of a national statistical agent/rate making organization
NCCI: statistical agent & rate maker
• The National Council on Compensation Insurance (NCCI) was founded in 1922
• From its founding the NCCI worked with insurance regulators for approval business practices:– The insurance agreement– How class and individual experience rates would be
set– Rules for auditing premium and other adjustments to
the insurance contract• Originally served 10 states; now working in 40
states
Strengths
• Less political involvement in administration, particularly rate making
• Strong solvency standards– No deficits or liability to general public
• Guaranty funds pay insurance benefits of insolvent insurers and spread the cost to other insurers
• Wide range of choice of carriers– Carriers differ somewhat on rate levels,
underwriting, and policyholder service
Weaknesses
• High administrative expense– Profit, marketing, and agent commission
• Insurance rating cycle– Seemingly irrational ups and downs in pricing
• No strong commitment to safety and loss control
• Mixed performance on rehabilitation and return to work
Downside of Competition
• Competitive insurance defeats the goal of universal coverage– Very high risk employers will not be able to find
coverage, or only at “excessive” rates • In the US, the solution to lack of availability is
a government mandated market of last resort– Assigned risk plan– Risk pool
• Aggressive competition also leads to unsustainable price cutting
Applicability
• Worldwide, there seems to be a very slow expansion of private insurance as the funding source for WC benefits
• In the US, the move to private insurance seems to be as a reprisal for a public system that has failed to meet stakeholder expectations or has run up large deficits
Applicability
• The US system cannot be fully imitated because it requires a very expensive infrastructure– Rating/statistical agencies need to be
authorized, regulated and funded– If more than one rating agency is to exist, there
must be close coordination
Other Barriers to Applicability
• US system is distributed by professional insurance agents, which may not be available
• Private carriers in the US are closely regulated by:– State insurance departments (solvency)– State industrial commissions (benefit payments)
Summary
• Private insurance in the US is strongly entrenched as the delivery and financing system for WC
• Private insurance seems to cost more than publicly funded systems
• Unfunded deficits and administrative breakdowns are less widespread among private insurers– Unsuccessful insurers disappear from the market
• US model is not readily applicable elsewhere
About the IAIBC The IAIABC is a not-for-profit association that represents government agencies charged with the administration of workers’ compensation programs. There are more than 60 jurisdictional members, primarily in the US and Canada. The IAIABC engages in research and educational programs for its members. Contact information: International Association of Industrial Accident Boards and Commissions 5610 Medical Circle, Suite 24 Madison, WI 53719 608-663-6355 email: [email protected] Web: www.iaiabc.org
Neither public nor private: Self- insurance in workers
compensationAlan McClain
Outline
• General concept of “self insurance”• Benefits of self insurance• Core regulatory features in the US• Variations on US model in Canada and
Australia
General Concept of Self Insurance
• Not really “insurance” because there is no spreading of risk over a pool of entities
• In reality this is self funding of benefits• Must be selective approval to self fund
– Risk of default on payment can be very high
Benefits
• Companies want to self insure for a variety of reasons
• Dissatisfaction with private insurers– Pricing, service, etc
• Belief that an actuarilly fair rate would overcharge them because of their better loss experience
• More control over claim handling
US Self Insurance
• All but two states allow self insurance• Requirements are generally more liberal
for government entities• The typical state may have 200 or so self
insured employers• Group self insurance is allowed in 26
states
Core Regulatory Feature in US
• Screening mechanism for would-be self insured employers
• Setting financing security levels as a backstop against default
• Reviewing periodic financial/operating reports for licensed self insurers
• Curtailing right to self insurer is standards are not met
• Dealing with bankruptcy of self insured
Variations: Canada
• Self insurance in Canada is much less common than in the US
• Governments of Canada and individual province/territory are self insured
• Several provinces do not allow non government self insurance
Australia: General
• Six states (New SouthWales, Queensland, South Australia, Tasmania, Victoria andWestern Australia)
• Two territories (Australian Capital Territory and Northern Territory).
Variations: Australia
• Self-Insurance is permitted in all 6 states• Subject to state specific requirements
Australia: Common Requirements
• Financial Capability• Health & Safety Provisions• Return To Work Emphasis• Capacity to administer claims process
Federal Government Self Funding
• Compulsory workers' compensation program for employees of the commonwealth - Australian federal government and national agencies
• Central fund, but both self insurance and self administration is permitted.
QUESTIONS?
1 Director Ejecutivo OISS
2

3
Perfil diferencial
17,5 millones de niños trabajan y 22.000 mueren anualmente.
50% trabajadores informales (+120 m).1
Otros Colectivos desfavorecidos: mujeres, migrantes, indígenas …
2
3
Intensidad del
fenómeno
Subregistro de AT (20%) y de EP (1-5%).
30 millones AT y 240.000 muertes relacionadas con el trabajo.
Construcción, agricultura y minería: 140.000 muertes
La siniestralidad compromete el 10% del PIB de la Región.
1
2
3
4
Diagnóstico de la Región Iberoamericana:
4
Adaptada a realidad Posibilista Consensuada
Proceso de elaboración:
Encomienda a la OISS Ministros y Máximas Autoridades
Respaldo Máximas Autoridades:
VII Conferencia Ministros y Máximos responsables de Seguridad Social
XIX Cumbre Iberoamericana de Jefes de Estado y de Gobierno
Aprobación definitiva: Declaración de Santiago
5
Aborda objetivos concretos y posibilistas, estableciendo diferentes niveles de intervención que han de plasmarse en Estrategias Nacionales.
Características de la Estrategia:
Se configura como un documento dinámico, no reactivo.
Pretende diseñar un marco común y compartido.
Estructura:Diagnóstico (mercado laboral, siniestralidad, protección social).
5 objetivos generales: principios programáticos.
8 objetivos específicos: en niveles adaptables.
Plan de Acción y seguimiento.
6
Concebidos como principios programáticos o rectores de las políticas de seguridad y salud en la Región
Avanzar en la mejora de las condiciones de trabajo en la Región. .
Objetivos Generales
Avanzar en el protagonismo de los agentes sociales en el establecimiento de Políticas públicas de Seguridad y Salud.
Lucha contra el Dumping social.
Generar mejoras efectivas en la cultura preventiva.
2
1
3
Mejorar los sistemas de información y registro de accidentes y enfermedades profesionales. Homogeneidad y elaboración estadísticas. Creación del Observatorio de Riesgos profesionales.
Incrementar la cooperación y colaboración regional en la materia:
4
5
7
Incluyen acciones concretas y un planteamiento de seguimiento y evaluación a través de indicadores.
Se diferencian los Estados en función del desarrollo de su estructura preventiva.
Objetivos Específicos
Reforzar el marco normativo de cada Estado.
Conocer situación nacional. Diagnóstico situacional. Encuestas de condiciones de trabajo.
Reforzar los Órganos Técnicos de Seguridad y Salud.
Reforzar las instituciones nacionales de Inspección y Control.
2
1
3
4
Avanzar en investigación y estudio de la multicausalidad.
Promover programas de apoyo en PYMES y autónomos.
Mejorar capacitación de agentes implicados.
Promoción de Políticas Públicas de Responsabilidad Social.
6
5
7
8
8
Informes específicos (Disponibles 9: Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua, Panamá, Chile, Ecuador y Colombia. (Apoyo en la red SALTRA)
Ultimado y validado cuestionario de encuesta de condiciones de trabajo. Previsión primera aplicación en Centroamérica en el 2º semestre de 2011.
Informe actividades realizadas:
Análisis de situación de las condiciones de trabajo y las políticas de seguridad y salud
Constitución Cátedra de salud laboral: J. Andalucía/Univ. Almería
Asistencia técnica a países:Presencial: Gobierno de Chile, CODELCO, Argentina,
Remota (on line): Compromiso respuesta técnica en 72 horas. Web OISS - Serviprevencia
Sensibilización y formación: cursos cortos, divulgación…
Investigacion: Estudio trabajo infancia y mujeres
9
Acuerdo tripartito de apoyo a la EISSTDeclaración de Granada: especial referencia al escenario
económico y las políticas de seguridad y saludDeclaración de GranadaFINAL.doc
Informe actividades realizadas:
IV Congreso Iberoamericano de Prevención de Riesgos laborales en Iberoamérica PREVENCIA 2010:
Observatorio de Seguridad y Salud:
Estrategias / Planes Nacionales de concreción de objetivos:
Argentina (firmado), Chile (Comisión de Gobierno), Colombia (PNSO 2010-2012), España y Portugal (U.E.) en tramite C. Rica, Panamá, Dominicana, Salvador y Guatemala.
•Ultimado soporte informático y estructura
10
OIT/CSA: Formación representantes de los trabajadores, Argentina (febrero/marzo 2011)
UGT-España/Universidad de Uruguay: formación y apoyo al desarrollo de encuesta de condiciones de trabajo .
Mutuas Españolas: 6 trabajos de investigación. INSHT España: entrega de materiales de autoevaluación
de riesgos, estudios técnicos, material didáctico.RED SALTRA, U. Pompeu Fabra, ISTAS-CCOO España
Informe actividades realizadas:
Programas de trabajo en colaboración:
Disponible plataforma on line y programas comprometidos con agentes sociales: prevención básica, dialogo social, relaciones laborales
Máster superior tres especialidades. Multitud de Materiales autodidácticos: formación, fichas técnicas,
autoevaluación de riesgos, soportes especiales PYMES, recomendaciones preventivas sectoriales, actividades sensibles…
Formación / divulgación: www.oiss.org /EISST/Serviprevencia
11
…les esperamos en Cartagena de Indias el próximo 29 de junio
Gracias por su atención y….
12
Informe actividades realizadas:
CONSIDERANDO
3.Que en el presente Congreso se ha puesto de manifiesto el riesgo de que los ciclos económicos bajos y, en particular, la situación de crisis mundial que se vive en la actualidad, incidan en el deterioro de las condiciones de trabajo y en el incremento del empleo informal, en la recesión de las inversiones en medios preventivos y en el estancamiento del desarrollo de políticas de Seguridad y Salud laborales.
4.Que dicho proceso vendría a incrementar los ya elevados ratios de siniestralidad de la Región y agravar los efectos perniciosos sobre las personas en términos de salud, discapacidad y muerte.
DECLARACIÓN PREVENCIA 2010En Granada (España) a veintiuno de mayo de 2010, en el seno del
IV Congreso de Prevención de Riesgos Laborales en Iberoamérica “PREVENCIA 2010”, los participantes en el mismo, ………
13
Informe actividades realizadas:
DECLARAQUINTO:El Congreso expresa su convicción de que el desarrollo de políticas de Seguridad y Salud, lejos de ser un obstáculo a los procesos de reactivación económica, coadyuvan al incremento de la productividad y la competitividad y reducen, de manera trascendente, los costes derivados de la siniestralidad laboral y la enfermedad profesional, así como los daños a la salud y a la vida de los trabajadores.Por ello, es preciso tomar conciencia y evitar el riesgo de recesión de las inversiones en Seguridad y Salud en los periodos más bajos del ciclo económico.
Director Ejecutivo OISS

Diagnosis of the Latin-American Region:
30 million Accident at Work and 240.000 fatalities related to work.
Subregistration of Accident at Work (20%) and of Occupational Disease (1-5%).
Construction, agriculture y mining: 140.000 fatalities
Iberoamerican Strategy
Production Process:
Iberoamerican Strategy
Characteristics of the Strategy
Iberoamerican Strategy
It sets specific and achievable targets, establishing different levels of intervention

General Objectives
Iberoamerican Strategy
Knowledge of the National Situation. Situational diagnosis. Working conditions Surveys.
Iberoamerican Strategy
Promote supporting programs in PYMES and Autónomos (Small bussiness And Self-employed).
Situational analysis of working conditions and health and safety policies
Creation of the Department of Occupational Health: University of Almería (Spain)
Technical assistance to other countries(onsite and remote/on line)
Training and Awareness: ( www.oiss.org/EISST/Servipreventia )
Iberoamerican Congress of occupational risk prevention: PREVENCIA 2010
National Plans to consolidate goals
Work programs in collaboration with other organizations:
Activity Report:
Iberoamerican Strategy

Thanks
Abstract of the Presentation: International Co-operation in OHS – Impacts, Sustainabiliy and Challenges Holger Trechow, Head of Section OHS, GVG – Gesellschaft für Versicherungswissenschaft und -gestaltung GVG comprises the key actors of the German Social Security System. In its national and international work, GVG covers all the five branches of social insurance. In its international project work, GVG works closely with and largely relies on the DGUV and the BG system at large, as well as on the state authorities for occupational health and safety. Projects in OHS funded by the EU, World Bank or other Donors, as well as Study Projects (e.g. funded by DG EMPL) on a variety of Health and Safety related topics are to a large extent donor-driven. The designing phase of such projects is highly important as it defines the objectives and mandatory results based on an outline of the project activities. The example of Turkey, at least at a first glance, may highlight how international co-operation may support the long-term process of establishing a national safety culture. But is continuity between the different development stages ensured both in the national process and in Technical Assistance? Further examples will be provided to critically discuss the impact of international co-operation, its shortcomings and challenges. Resuming, it can be stated that international co-operation in Technical Assistance projects and beyond does not only provide an arena for various forms of exchange and a strong impetus for the harmonisation of social security in the world of labour, but it is an important tool to support the safeguarding of the workforce from any threats to their health and safety.

GVG – Short Portrait The GVG’s international activities are an extension of our contribution to the social policy discussion in Germany. Conferences and workshops offer our partners both inside and outside the European Union a forum for exchanging ideas and sharing experience within the context of the international social policy debate. On behalf of German and foreign Ministries and International Organisations, we advise Governments, Social Security Institutions and other Clients on social security issues. Our projects provide support at various levels. We offer consultation on reorientation and restructuring processes in the social security sector, we give practical support in the drafting of legislation, we provide longer-term consultation and support for the administrative reorganisation of social security systems and institution building and we design training courses for specialist staff. The assessment and evaluation of social policy measures is also part of our work.
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
EUROPEAN FORUM - Adding Value through
International Cooperation
Conference, Dresden
June 21 to 22, 2011
International Co-operation on OHS -Impacts, Sustainability and Problems
Perceived
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
2
Speaker
Holger Trechow
Head of Section OHS / Project Manager eHealth
M.A. Political Sciences (Cologne)
Master in Humanitarian Assistance (Bochum / Uppsala)
Working e.g. for CARE (in BiH), BMZ, gtz/giz in the areas of Social Security Policy / Poverty Reduction
Kontakt: [email protected]
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
3
GVG Members
GVGHealth Care Providers
Associations of: Doctors / Dentists / Physiotherapists
Hospitals / Rehab ClinicsIndustry (Pharma, Med. Aids)
Social PartnersEmployers‘ Organizations
Trade Unions
Scienceand
Research
Companypension and health
schemes
StatutoryInsurances
Pension / Health /Long-Term Care / Accident
Private InsurancesLife / Health /
Long-Term Care /Accident
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
4
Mandate: Maintain and strengthen the basic consensus on the fundamental principles of the German social security system:
- Solidarity: Provide society‘s support to individuals in need
- Subsidiarity: bottom-up approach – first, the lower or more immediate level shall deal with matters in their area; higher levels get involved only in case of need
- Enforce individual risk coping (problem solving) capacities
- Diversity: Ensure a pluralistic system with a variety of institutions to take care of the specific needs of diverse population groups
- Ensure access of all members of society to a liberal and pluralistic system of social security and a broad scope of high-quality coverage for the major risks in life
- Based on the principle of self-government
Basis of our national Work
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
5
International consultancy answering the large need in Eastern European Countries
Basic requirement: modernise the OHS systems and adaptthem to EU / ILO requirements
Focus of international OHS projects clearly on prevention!
Close co-operation with DGUV and German State and Federal State Authorities
Only one project on the Accident Insurance System (Ukraine, EuropeAid114778: Support to the Development of the Accident Insurance system in Ukraine)
What do we do internationally?
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
6
In the following slides, some examples of our work are presented:
- To give an outline of possible interventions
- To demonstrate the variety of (also high orlow) impacts of international co-operation
- To show some problems that may befaced in this field of work
What do we do internationally?
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
7
Basic project interventions:
• OHS Policy / Strategy
• Capacities
• Training
• Social Dialogue
• Setting up institutions / infrastructure (e.g. OHS
Centre, OHS Laboratory)
Five basic interventions
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
8
A – Turkey
Turkey 1: large-scale TA (Technical Assistance) project2004-2006 with DGOHS on policies, strategies, capacitybuilding / training, public awareness + OHS laboratory
Turkey 2: Twinning Project with LIB (Labour InspectionBoard) providing training in key risk areas (2008-09)
Ongoing:
Turkey 3: (but not implemented by GVG): introduction of pilot OHS management systems at enterprise level, parallel OHS Lab project (start 2010)
Turkey 4: PPE lab for market surveillance (start 2011)
Turkey 5: SEVESO II (still in forecast) …
Exemplary projects I
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
9
B – Others
Azerbaijan 1: Worldbank (WB) project on Enhancing State Labour Inspectorat Service (SLIS) Capacities (2010–13)
Azerbaijan 2: EU Twinning on Support to SLIS for OHS Enhancement (2011-12)
Russian Federation: EU - TA on Approximation of OHS Legislation (2006-07)
Latvia: EU Twinning Occupational Health and Safety system (with Labour Inspectorate, 2006-07)
Ukraine: EU TA Support to Development of the Accident Insurance System (2004-05)
Exemplary projects II
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
10
Key features of work on projects
1) Design by the Beneficiary and Donor is very important
2) Continuity: how are project results taken on board and furtherelaborated
3) Political support: a strategy may be developed as an instrument to achieve ownership at all levels
4) Training: is it enough to evaluate training sessions? How cantrainings (mainly for state officials) be improved
5) Exchange: - between experts
- at enterprise level
- on methodologies (training, awarenessraising etc.)
OHS projects - Assessment
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
11
Worldbank
- Macedonia: Feasibility study on strengthening
enforcement capacity of the state labour inspectorate
DG EMPL
- Proposal for commission practical guidelines for training
of workers involved in work with asbestos (2009-10)
- Impact on OHS in EU of the increasing use of portable
computing and communications devices (2009-10)
- Report on ... OD systems in EU Member States …, in
particular relative to Recommendation 2003/670/EC concerning European Schedule of OD (start 2011)
Exemplary studies
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
12
Key features of work on studies:
1) Contribution to health and safety of the workforce and the population (e.g. asbestos)
2) Harmonisation process with EU and international standards (Macedonia)
3) International institutional co-operation4) Preparation of political decisions at EU level
5) Topics with potentially strong political impact6) Are interventions well-targeted? Asbestos Guidelines
vs. Standards e.g. regarding demolition works(asbestos roofs etc.)
OHS studies: Assessment
GVG e.V. - Hansaring 43 - 50670 Köln
www.gvg.org
13
International Co-operation:
- Paves the way for economic co-operation
- Helps harmonise the social security systems
(core labour standards, access to markets,
competitiveness)
- Provides exchange of experts at even level
- Helps to reflect the own system
- Supports the safeguarding of the workforce!
Resume and Outlook
Issue 04 Future challenges in workers’ compensation
A discussion paper by the Munich Re Centre of Competence for Workers’ Compensation
Issue 04
Contents
Executive summaryWorkers’ compensation at a crossroads
Workers’ compensation insuranceA pillar of social and fi nancial security
Future challengesIs today’s system fi t for tomorrow’s working world?
ConclusionsAwareness, dialogue and cooperation are called for
References
The Munich Re Group operates worldwide, turning risk into value. In the fi nancial year 2008, it achieved a profi t of €1,528m on premium income of around €38bn. The Group operates in all lines of business, with around 44,000 employees at over 50 locations throughout the world and is character-ised by particularly pronounced diversifi cation, client focus and earnings stability. With premium income of around €22bn from reinsurance alone, it is one of the world‘s leading reinsurers.
About the Centre of Competence for Workers’ CompensationActing on its keen awareness of the special role – and global importance – of workers’ compensation insurance, the Munich Re Group established the Centre of Competence for Workers’ Compensation in 1998. Since then, the highly specialised and dedicated team of experts has been monitoring and analysing developments in this complex type of social insurance on a world-wide scale. Today, the Centre of Competence is an internationally valued and respected source of advice and information regarding systems with state and/or private-sector involvement.
2
4
6
14
16
1Munich Re Future challenges in workers‘ compensation
Dear Reader,
The Munich Re Centre of Competence for Workers’ Compensation has been closely monitoring international developments in this extremely complex area of risk man-agement for more than ten years. In addition, we have been listening to the views and experiences of diverse stakeholders from all over the world. One of the main con-clusions we have reached as a result of our research and knowledge-gathering can be summed up as follows: the demands on workers’ compensation are changing.
Due to its key role in society, workers’ compensation is far too important to be put at risk. And the only way to guar-antee that it remains fi t for the future is through an open exchange of views among all involved parties. This is why we have compiled some thought-provoking information on future challenges. By no means comprehensive or conclusive, the brief overview in the following pages is designed to offer insights and foster discussion.
Regardless of your personal level of direct or indirect involvement in workers’ compensation, your thoughts are important – and you can make a valuable contribution. We wish you interesting and informative reading.
With best regards,
Victor Schultheiss Head of Centre of Competencefor Workers’ Compensation
2 Munich Re Future challenges in workers‘ compensation
Executive summary Workers’ compensation at a crossroads
All over the world, workers’ compensation systems face new challenges – with more looming on the horizon. The Munich Re Centre of Competence for Workers’ Compensation has gath-ered information on a number of issues with possible repercus-sions for this important form of social insurance.
The main challenges are identifi ed as follows (listed alphabet-ically): chronic diseases, climate change, demographic shift (greying workforce), legal confl ict, migration, musculoskeletal disorders, obesity, psychological disorders, use and abuse of prescription drugs. Each of the factors – individually and/or in combination with others – could potentially put signifi cant pres-sure on a workers’ compensation system. For the sake of brevity and clarity, this paper looks at four examples that underscore the importance of closely monitoring these developments.
Climate Global climate change is now widely accepted as scientifi c fact. Rising water levels are already rendering some coastal and island regions uninhabitable, triggering migration. Experts fore-cast an increase in the frequency and/or intensity of heat waves and droughts in southern regions and milder winters with more precipitation in northern geographies. The probable impacts on occupational disease include increased risk of heat-related dis-orders, respiratory disease due to pollens and cancers caused by ultraviolet radiation.
Demographics Higher life expectancies and the increasing average age in most countries suggest that tomorrow’s workforces will contain a bigger share of older employees. A greying future workforce will be more prone to accidents and diseases associated with ageing. In addition, more long-latency illnesses must be expected.

3Munich Re Future challenges in workers‘ compensation
Drugs More and more professionals use prescription drugs to boost performance. Taking any medication for a purpose other than that for which it has been approved is inherently risky, and many such stimulants and antidepressants have lists of known side effects, including addiction. Some amphetamine-based drugs, designed to treat attention-defi cit hyperactivity disorder (ADHD), are already in use as cognitive enhancers in signifi cant numbers. And a new generation of pharmaceuticals aimed at treating cognitive decline – with considerable potential as so-called neuroenhancers – is emerging. Workers who over-estimate capabilities, become euphoric and lose sleep could represent a higher accident risk.
Obesity Obesity, defi ned as a body mass index (BMI) of more than 30, is already considered a global epidemic – and it continues to increase. Excessive body fat is linked not only to a large number of common health problems, but also to occupational accidents and diseases. Signifi cantly overweight employees have been shown to suffer more on-the-job accidents.
What this means for workers’ compensation These changes are real. Precisely how they will unfold and inter-act to compound one another is impossible to forecast. Very probable results include sharp increases in the complexity of attributing disorders to occupational causes as well as in the frequency of litigation. For this reason, risk carriers and policy-makers must be prepared to take steps to stabilise the delicate balance between the four basic components of social insurance – defi nitions, benefi ts, coverage, fi nancing. The shifting risk landscape and what it means for the defi nition of events that trigger claims (triggers) and premiums must be closely moni-tored. All workers’ compensation systems are well advised to subject current reserves – notably IBNR (incurred but not reported) and IBNER (incurred but not enough reserved) – to a stress test in order to determine whether they are suffi cient to meet the challenges ahead. A very close look at the logic used to defi ne premiums (loadings) might be useful. The categorical pricing approach used in many countries might not be valid in tomorrow’s world. At the same time, it should be noted that the world’s workers’ compensation systems have overcome many obstacles over the past 125 years. Based on transparency, co-operation and dialogue, these future challenges can be mastered as well.
Executive summary

4 Munich Re Future challenges in workers‘ compensation
Since its inception in the late nineteenth century, workers’ compensation insurance has developed into one of the most important cornerstones of social justice and welfare.
Its immediate effect was to largely free workers and their fam-ilies of the often tortuous task of litigation against employers to gain compensation in the event of occupational disease or acci-dent. But it was also welcomed by many companies, which had previously faced court cases with uncertain outcomes. Workers’ compensation insurance required employees to forgo the right to sue for damages due to a covered claim. By providing a clear framework of covered risks and benefi ts in cash or in kind, work-ers’ compensation has served as a pillar of fi nancial security.
Today’s systems vary widely, with many countries maintaining public monopolistic programmes while others include private participation. The solutions also differ in terms of which risks are recognised as occupational. The laws governing attribution of disease or accident to work-related causes are anything but uniform. Carpal tunnel syndrome, which affects the wrist and hand, causing symptoms including numbness and a tingling or burning sensation, is one example of a disorder that is cat-egorically excluded in some countries and included in others – in some as an occupational accident while in others as an occu-pational disease. In other words, defi nitions are in fact a purely political matter.
Stakeholders throughout society But as multifaceted as the approaches to workers’ compensa-tion insurance are, all markets share a number of characteris-tics. They all involve a complex matrix of stakeholders (see Fig-ure 1, The stakeholder matrix): alongside the primarily affected parties – employer, employee and dependants, the state – the risks and benefi ts have direct or indirect bearing on many other elements. Customers and suppliers of employers, for example, would feel the consequences should a system fail to provide the necessary fi nancial stability and planning security to keep a company solvent. Without insurance, entire families would be at risk of having to compromise their lifestyles should bread-winners fall ill, which would in turn impact the communities in
Workers’ compensation insurance A pillar of social and fi nancial security
Defi nitions Benefi ts
Financing Coverage
Figure 2: Social insurance in balance
The four basic elements must be kept in perfect balance
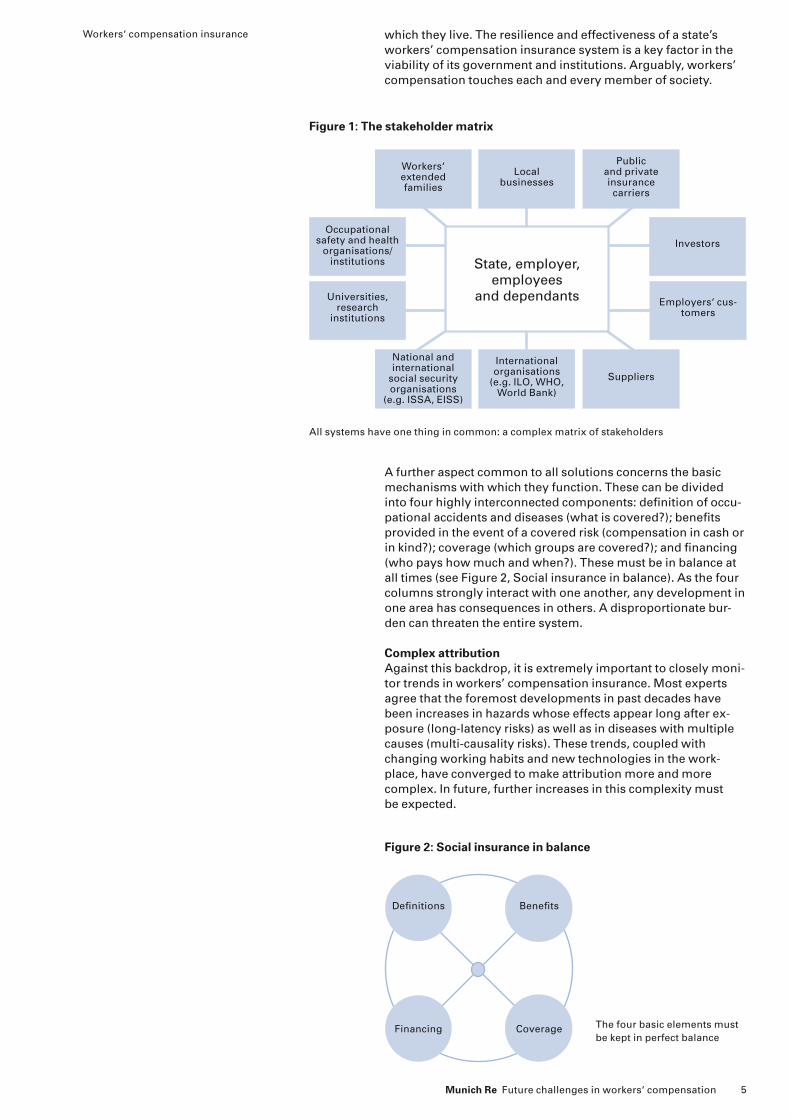
Figure 1: The stakeholder matrix
State, employer, employees
and dependants
Workers‘ extended families
Local businesses
Public and private insurance carriers
National and international
social security organisations
(e.g. ISSA, EISS)
International organisations
(e.g. ILO, WHO, World Bank)
Suppliers
Occupational safety and health
organisations/institutions
Universities,research
institutions
Investors
Employers‘ cus-tomers
All systems have one thing in common: a complex matrix of stakeholders
5Munich Re Future challenges in workers‘ compensation
which they live. The resilience and effectiveness of a state’s workers’ compensation insurance system is a key factor in the viability of its government and institutions. Arguably, workers’ compensation touches each and every member of society.
A further aspect common to all solutions concerns the basic mechanisms with which they function. These can be divided into four highly interconnected components: defi nition of occu-pational accidents and diseases (what is covered?); benefi ts provided in the event of a covered risk (compensation in cash or in kind?); coverage (which groups are covered?); and fi nancing (who pays how much and when?). These must be in balance at all times (see Figure 2, Social insurance in balance). As the four columns strongly interact with one another, any development in one area has consequences in others. A disproportionate bur-den can threaten the entire system.
Complex attribution Against this backdrop, it is extremely important to closely moni-tor trends in workers’ compensation insurance. Most experts agree that the foremost developments in past decades have been increases in hazards whose effects appear long after ex-posure (long-latency risks) as well as in diseases with multiple causes (multi-causality risks). These trends, coupled with changing working habits and new technologies in the work-place, have converged to make attribution more and more complex. In future, further increases in this complexity must be expected.
Workers‘ compensation insurance
6 Munich Re Future challenges in workers‘ compensation
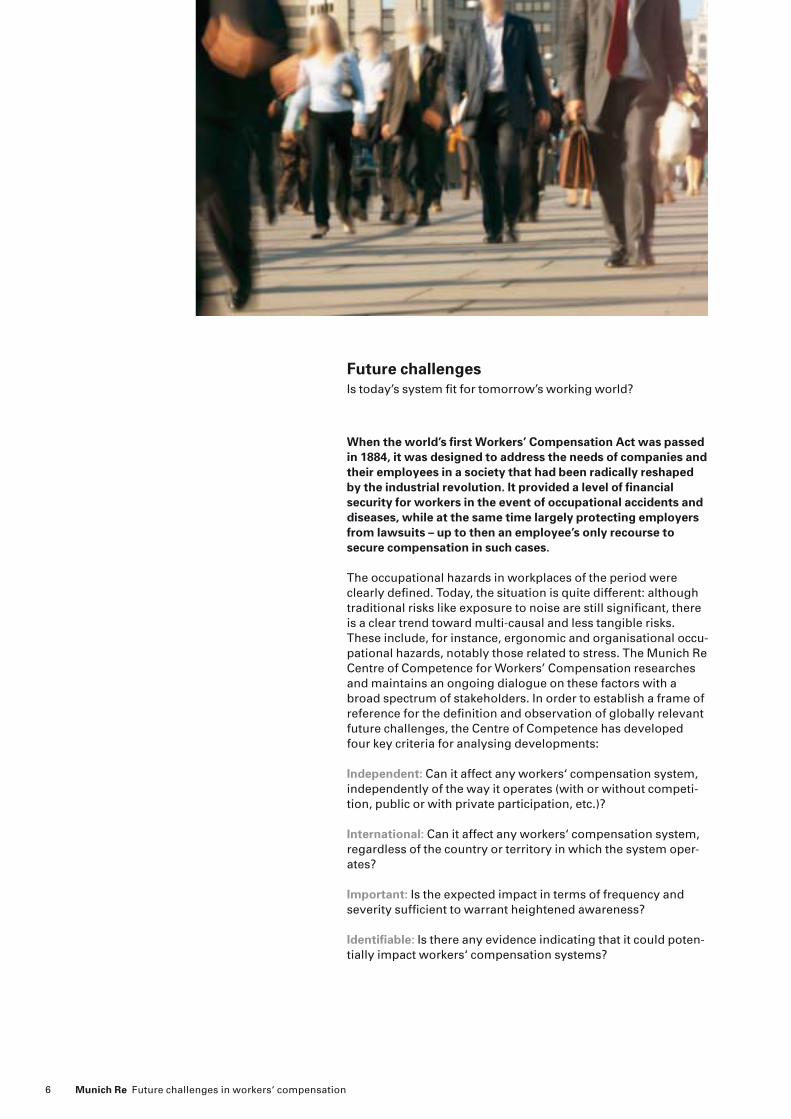
When the world’s fi rst Workers’ Compensation Act was passed in 1884, it was designed to address the needs of companies and their employees in a society that had been radically reshaped by the industrial revolution. It provided a level of fi nancial security for workers in the event of occupational accidents and diseases, while at the same time largely protecting employers from lawsuits – up to then an employee’s only recourse to secure compensation in such cases.
The occupational hazards in workplaces of the period were clearly defi ned. Today, the situation is quite different: although traditional risks like exposure to noise are still signifi cant, there is a clear trend toward multi-causal and less tangible risks. These include, for instance, ergonomic and organisational occu-pational hazards, notably those related to stress. The Munich Re Centre of Competence for Workers’ Compensation researches and maintains an ongoing dialogue on these factors with a broad spectrum of stakeholders. In order to establish a frame of reference for the defi nition and observation of globally relevant future challenges, the Centre of Competence has developed four key criteria for analysing developments:
Independent: Can it affect any workers‘ compensation system, independently of the way it operates (with or without competi-tion, public or with private participation, etc.)?
International: Can it affect any workers‘ compensation system, regardless of the country or territory in which the system oper-ates? Important: Is the expected impact in terms of frequency and severity suffi cient to warrant heightened awareness? Identifi able: Is there any evidence indicating that it could poten-tially impact workers‘ compensation systems?
Future challenges Is today’s system fi t for tomorrow’s working world?

7Munich Re Future challenges in workers‘ compensation
Based on these “4 Is”, nine future challenges have been defi ned. These issues, which have been the subject of height-ened research and information-gathering efforts by the Centre of Competence over the past two years, are listed alphabetically below:
– Chronic diseases– Climate change– Demographic shift (greying workforce)– Legal confl ict– Migration – Musculoskeletal disorders – Obesity– Psychological disorders– Use and abuse of prescription drugs
In March 2009, the Centre of Competence hosted its fourth Workers’ Compensation Symposium, focusing on future chal-lenges. The gathering of international experts – including high-ranking representatives from research institutes and interna-tional organisations as well as decision-makers and researchers from various healthcare and insurance markets – confi rmed the relevance of the nine global issues defi ned above.
The nine factors can be expected to impact workers’ compensa-tion to varying degrees at different times. In some cases, with climate change for example, many potential effects can only be roughly estimated at this point. Interactions between the issues – such as how the increasing frequency of heat waves due to global climate change might affect the growing number of clinic-ally obese workers in many countries – represent an additional major variable. Together, the nine challenges may well compli-cate the attribution process and lead to increased litigation. To gain a better understanding of the current and emerging issues workers’ compensation systems will have to deal with in future, it is helpful to look at the most important challenges in more detail. Although all nine are signifi cant, below we have outlined four examples. These details underscore the impor-tance of heightened awareness.
Climate change The future repercussions of global climate change on workers’ compensation are diffi cult to judge. However, there is wide-spread agreement that climatic zones will shift, with conse-quences for vegetation, agriculture and fauna. In addition, the melting of glaciers – which can already be observed – is expected to result in fl ooding of coastal regions. And experts forecast an increase in the frequency and/or intensity of heat waves and droughts in southern regions and milder winters with more precipitation in northern geographies. The probable impacts on human health and thus on occupational accidents and diseases – at least as aggravating factors – are manifold (see Figure 3, Global climate change and its impacts).
Future challenges
An aggregate 1°C increase in monthly mean tempera-ture may increase total, respiratory and cardiovas-cular mortality by 1.4%, 10.4% and 1.6% respec-tively if the temperature exceeds the comfort range.W.J.M. Martens, Health Impacts of Climate Change and Ozone Depletion: An Ecoepide-miologic Modeling Approach
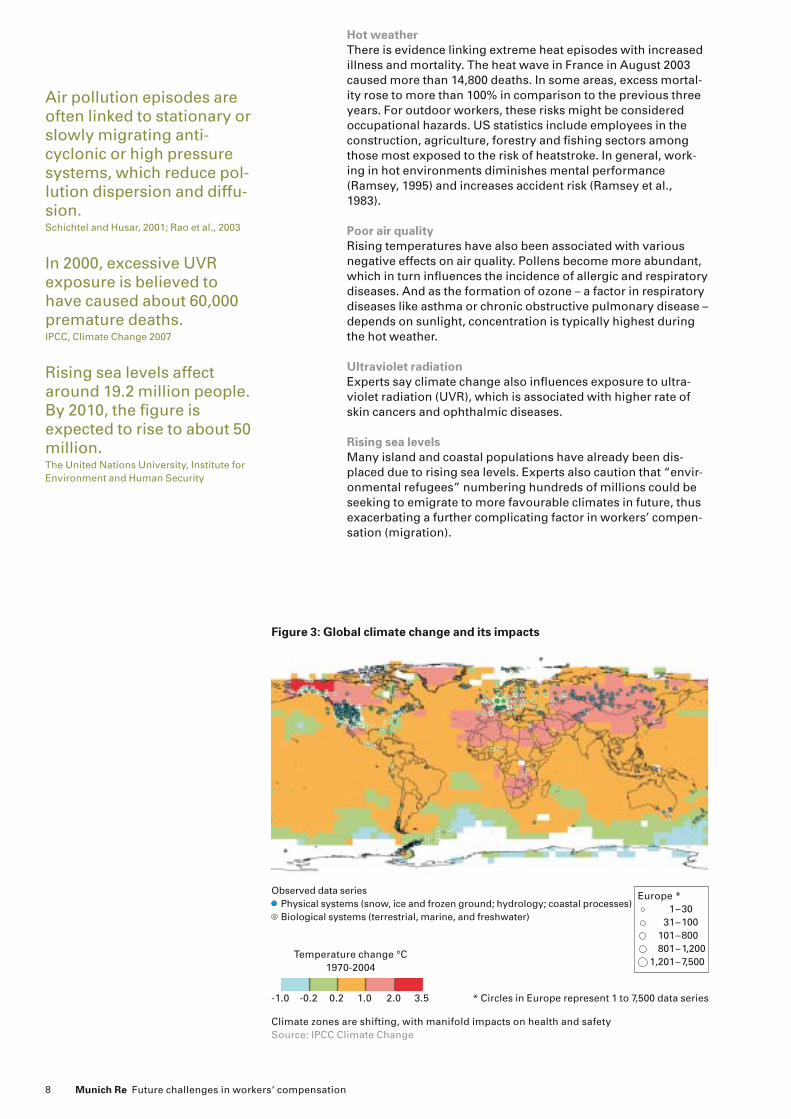
Observed data series Physical systems (snow, ice and frozen ground; hydrology; coastal processes) Biological systems (terrestrial, marine, and freshwater)
* Circles in Europe represent 1 to 7,500 data series
Temperature change °C1970-2004
-1.0 -0.2 0.2 1.0 2.0 3.5
Figure 3: Global climate change and its impacts
Europe * 1–30 31–100 101–800 801–1,200 1,201–7,500
Climate zones are shifting, with manifold impacts on health and safetySource: IPCC Climate Change
8 Munich Re Future challenges in workers‘ compensation
Hot weather There is evidence linking extreme heat episodes with increased illness and mortality. The heat wave in France in August 2003 caused more than 14,800 deaths. In some areas, excess mortal-ity rose to more than 100% in comparison to the previous three years. For outdoor workers, these risks might be considered occupational hazards. US statistics include employees in the construction, agriculture, forestry and fi shing sectors among those most exposed to the risk of heatstroke. In general, work-ing in hot environments diminishes mental performance (Ramsey, 1995) and increases accident risk (Ramsey et al., 1983).
Poor air quality Rising temperatures have also been associated with various negative effects on air quality. Pollens become more abundant, which in turn infl uences the incidence of allergic and respiratory diseases. And as the formation of ozone – a factor in respiratory diseases like asthma or chronic obstructive pulmonary disease – depends on sunlight, concentration is typically highest during the hot weather.
Ultraviolet radiation Experts say climate change also infl uences exposure to ultra-violet radiation (UVR), which is associated with higher rate of skin cancers and ophthalmic diseases.
Rising sea levels Many island and coastal populations have already been dis-placed due to rising sea levels. Experts also caution that “envir-onmental refugees” numbering hundreds of millions could be seeking to emigrate to more favourable climates in future, thus exacerbating a further complicating factor in workers’ compen-sation (migration).
Air pollution episodes are often linked to stationary or slowly migrating anti-cyclonic or high pressure systems, which reduce pol-lution dispersion and diffu-sion. Schichtel and Husar, 2001; Rao et al., 2003
In 2000, excessive UVR exposure is believed to have caused about 60,000 premature deaths. IPCC, Climate Change 2007
Rising sea levels affect around 19.2 million people. By 2010, the fi gure is expected to rise to about 50 million. The United Nations University, Institute for Environment and Human Security
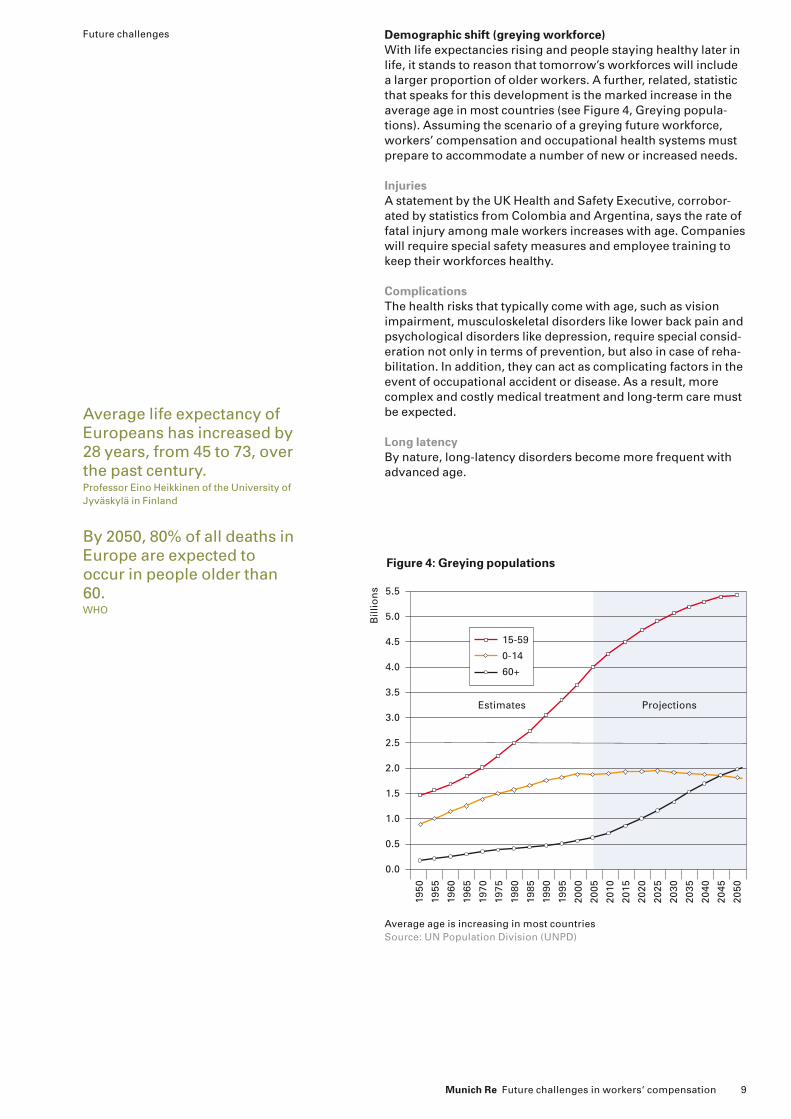
Figure 4: Greying populations
Average age is increasing in most countries Source: UN Population Division (UNPD)
5.5
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
2005
2010
2015
2020
2025
2030
2035
2040
2045
2050
15-59
0-14
60+
Bill
ion
s
Estimates Projections
9Munich Re Future challenges in workers‘ compensation
Demographic shift (greying workforce) With life expectancies rising and people staying healthy later in life, it stands to reason that tomorrow’s workforces will include a larger proportion of older workers. A further, related, statistic that speaks for this development is the marked increase in the average age in most countries (see Figure 4, Greying popula-tions). Assuming the scenario of a greying future workforce, workers’ compensation and occupational health systems must prepare to accommodate a number of new or increased needs.
Injuries A statement by the UK Health and Safety Executive, corrobor-ated by statistics from Colombia and Argentina, says the rate of fatal injury among male workers increases with age. Companies will require special safety measures and employee training to keep their workforces healthy.
Complications The health risks that typically come with age, such as vision impairment, musculoskeletal disorders like lower back pain and psychological disorders like depression, require special consid-eration not only in terms of prevention, but also in case of reha-bilitation. In addition, they can act as complicating factors in the event of occupational accident or disease. As a result, more complex and costly medical treatment and long-term care must be expected.
Long latency By nature, long-latency disorders become more frequent with advanced age.
Average life expectancy of Europeans has increased by 28 years, from 45 to 73, over the past century. Professor Eino Heikkinen of the University of Jyväskylä in Finland
By 2050, 80% of all deaths in Europe are expected to occur in people older than 60. WHO
Future challenges

Figure 5: Weighing in on obesity
5 10 15 20 25 30 35 40%
Authorities consider obesity a global epidemic Population with BMI > 30 Source: Global Database on Body Mass Index World Health Organization
Saudi ArabiaUSAUnited KingdomMexicoNew ZealandChileSouth AfricaGermanyAustraliaPeruMoroccoCanadaFinlandColombiaSpainBelgiumBrazilSwedenPortugalSingaporeNorwayMalaysiaChina
10 Munich Re Future challenges in workers‘ compensation
Obesity Global authorities including the International Obesity Task Force and the World Health Organisation already consider obesity a global epidemic (see Figure 5, Weighing in on obesity). Defi ned as a body mass index (BMI) of more than 30 (see Figure 6, How BMI is calculated), obesity is widespread in many countries – and it continues to increase. Excessive body fat is linked not only to a large number of common health problems, but also to occupational accidents and diseases. Tackling the problem of obesity calls for heightened cooperation among employers, employees, risk carriers and regulatory bodies aimed at foster-ing awareness of healthier lifestyles and eating habits.
Accidents and diseases Signifi cantly obese workers have been shown to suffer more frequent and severe on-the-job accidents. A general lack of physical fi tness coupled with the increased strain that the excess weight places on the musculoskeletal system can cause and exacerbate accidents. At the same time, obese employees are believed to be more susceptible to some toxins, which are absorbed through the skin. And it has been argued that work-places and personal protective equipment are not adjusted to this specifi c working population. For example, protective suits and fall-arrest equipment are not designed for the extremely obese.
The next generation Studies in a number of countries point to alarming rates of obes-ity among children. That means future workforces are likely to be even heavier on average than those of today – and that the health issues associated with obesity will be with us for a long time.
Employees in obesity class III (BMI 40) had 11.65 claims per 100 full-time employ-ees, while recommended-weight employees had 5.80; the effect on lost workdays (183.63 vs. 14.19 lost work-days per 100 full-time employees), medical claims costs (US$ 51,091 vs. US$ 7,503 per 100 full-time employees ), and indemnity claims costs (US$ 59,178 vs. US$ 5,396 per 100 full-time employees) was even stronger. Archives of Internal Medicine, April 2007
In 2002, 30.3% of boys and 30.7% of girls in England were overweight; 16% were clinically obese. British Medical Association
In 2004, 31.1% of males and 33.2% of females over the age of 20 in the USA classi-fi ed as clinically obese. WHO
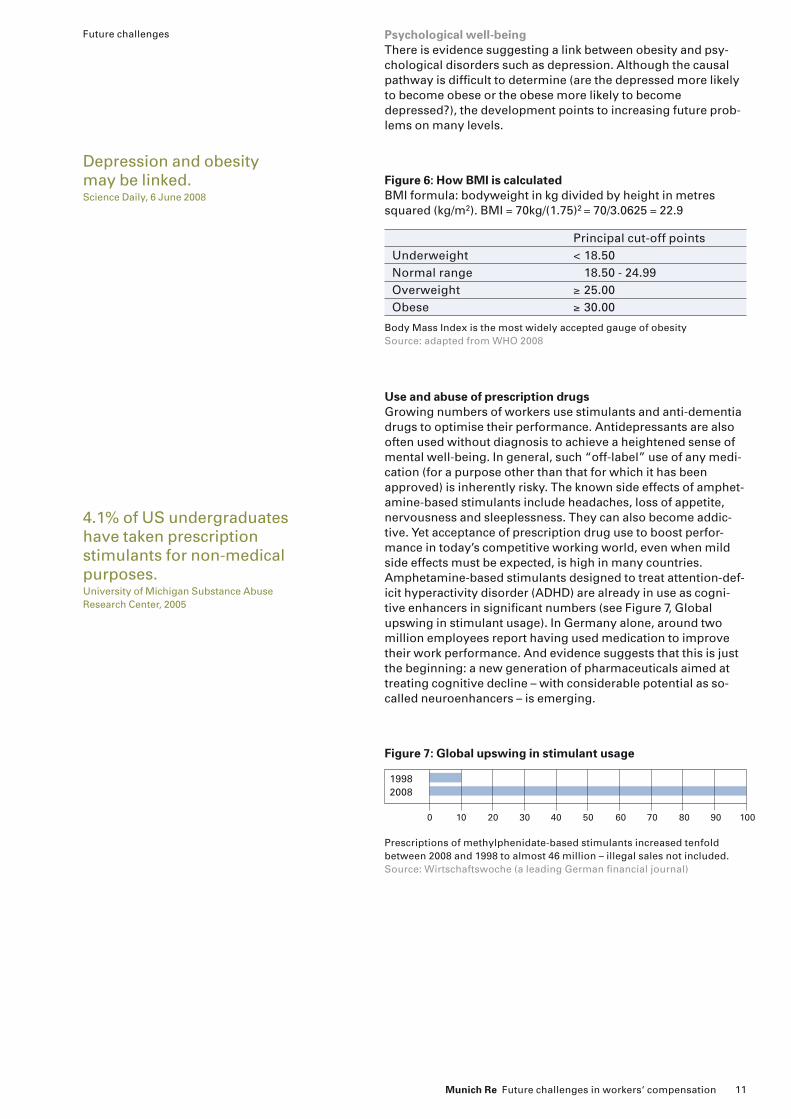
Figure 7: Global upswing in stimulant usage
19982008
10 30 40 50 60 70 80 90 100200
Prescriptions of methylphenidate-based stimulants increased tenfold between 2008 and 1998 to almost 46 million – illegal sales not included. Source: Wirtschaftswoche (a leading German fi nancial journal)
Principal cut-off pointsUnderweight < 18.50Normal range 18.50 - 24.99Overweight ≥ 25.00Obese ≥ 30.00
Body Mass Index is the most widely accepted gauge of obesitySource: adapted from WHO 2008
Figure 6: How BMI is calculatedBMI formula: bodyweight in kg divided by height in metres squared (kg/m2). BMI = 70kg/(1.75)2 = 70/3.0625 = 22.9
11Munich Re Future challenges in workers‘ compensation
Psychological well-being There is evidence suggesting a link between obesity and psy-chological disorders such as depression. Although the causal pathway is diffi cult to determine (are the depressed more likely to become obese or the obese more likely to become depressed?), the development points to increasing future prob-lems on many levels.
Use and abuse of prescription drugs Growing numbers of workers use stimulants and anti-dementia drugs to optimise their performance. Antidepressants are also often used without diagnosis to achieve a heightened sense of mental well-being. In general, such “off-label” use of any medi-cation (for a purpose other than that for which it has been approved) is inherently risky. The known side effects of amphet-amine-based stimulants include headaches, loss of appetite, nervousness and sleeplessness. They can also become addic-tive. Yet acceptance of prescription drug use to boost perfor-mance in today’s competitive working world, even when mild side effects must be expected, is high in many countries. Amphetamine-based stimulants designed to treat attention-def-icit hyperactivity disorder (ADHD) are already in use as cogni-tive enhancers in signifi cant numbers (see Figure 7, Global upswing in stimulant usage). In Germany alone, around two million employees report having used medication to improve their work performance. And evidence suggests that this is just the beginning: a new generation of pharmaceuticals aimed at treating cognitive decline – with considerable potential as so-called neuroenhancers – is emerging.
Depression and obesity may be linked. Science Daily, 6 June 2008
Future challenges
4.1% of US undergraduates have taken prescription stimulants for non-medical purposes. University of Michigan Substance Abuse Research Center, 2005

12 Munich Re Future challenges in workers‘ compensation
Overdoing it Experts agree that many stimulants can lead workers to over-estimate capabilities, become euphoric and develop sleeping disorders. Although it is currently diffi cult to quantify their im-pact on occupational accidents, these factors clearly have the potential to cause dangerous situations – especially where machines or vehicles are involved.
Under pressure As can be expected, use of cognitive enhancers is most preva-lent in high-pressure occupations. In some cases, employees have felt compelled to begin using neurological medication just to keep up. This could result in an “arms race” that would fur-ther increase pressure to perform – an important factor in many physical illnesses and psychological disorders.
Unknowns As the development pipeline produces new neurological phar-maceuticals, increased off-label use must be expected. Precisely how this will affect health and safety in the workplace remains to be seen. Although no direct comparison can be made with alcohol or illicit drug use, it is interesting to note that alcohol has been shown to increase the likelihood of an occupational accident by a factor of two or even three (United Nations 1993).
The sum total The total effect of these issues must be expected to add up to far more than the sum of their individual parts. It is important to note that the four aspects discussed above represent only a lim-ited view of the overall future workers’ compensation world. A brief look at the fi ve other factors reveals – among other things – that compounded effects involving multiple scenarios can play a major role. Migration, for example, not only puts workers in situations where they are unfamiliar with the language as well as local working habits (notably safety and health procedures), it also tends to place them in positions outside of their actual occupations – a source of accidents and heightened on-the-job stress. Chronic diseases and musculoskeletal disorders increase signifi cantly with both age and excessive body mass. Psycho-logical disorders encourage use of prescription neurological drugs, and have been linked to weight gain. And all of these fac-tors are likely to strain regulatory frameworks and contribute to increasingly frequent and complex litigation.
20% of German employees consider medication to boost on-the-job perfor-mance justifi able, even without medical indication. Recent survey by the German health insurer DAK
The majority of “Nature” readers say healthy adults should be permitted to use neuroenhancers. Recent poll by the scientifi c journal Nature
Legal sales of prescription drugs containing methyl-phenidates (group of amphetamines), mainly used for ADHD treatment has increased tenfold since 1998. Toennesmann, 2008
Use of prescription antide-pressants with the active ingredient fl uoxetin has increased by 43% between 2005 and 2007. Recent survey by the German health insurer DAK

13Munich Re Future challenges in workers‘ compensation
Jarmo Jacobsson (left) and Andrés Angel (right) speaking at the Workers‘
Compensation Symposium
In March 2009, the Munich Re Centre of Competence for Workers’ Compensation hosted an international symposium to look at the future challenges facing different systems all over the world. While at the three-day event, two decision-makers with major workers’ compensation organisations commented on the role of the Centre of Competence in tackling the challenges that lie ahead.
“We have a relationship of nearly ten years with the Centre of Competence. And I think it’s a unique unit, worldwide. There are a lot of organisations studying health and prevention strategies and how to reduce medical costs or whatever, but not many dealing with the insurance part.”
“So I think that’s the main benefi t of the centre. If you take into account that they are always trying to understand what’s happening all around the world, and actually when they go, for example, to a country like Colombia, people listen to them. The govern-ment listens to the centre, because it’s been studying developments all around the world. If, for example, they’re thinking of changing a new defi nition in the laws, well the Centre of Competence has a lot of information that helps those governments or those companies to do a better job.”
“And it helps to have a good partner, which is how we see Munich Re and the Centre of Competence; as a partner, a long-term partner for our reinsurance programme. Basically, you feel better when you know your partner knows at least as much if not more than you know. Because you have a good and strong relationship and good discussion of the prob-lems of the future and how we can tackle those chal-lenges. Or we can ask whether there are situations anywhere else in the world like the ones we face in Colombia.”
Andrés AngelVice-PresidentInversura SAInversura SA is the holding company of Susalud (HMO) and Suratep, Colombian workers’ compensa-tion insurer.
“I have worked for this organisation for eight years, but I have a long history in the Finnish insurance industry and I’ve been involved in the workers’ com-pensation system. We have a kind of market pool in Finland, and I know that Munich Re has been a leader in this pool since the 1960s – quite a long time. A long-standing relationship, as it used to be in reinsur-ance. As I think it should be, even though of course we have competition.”
“But I think it’s very important that this kind of market player brings together all different players and also the public sector, because it’s very inspiring to hear different views, and this is the kind of line that always involves the public sector – occupational health, occupational diseases – so it’s fantastic that this com-petent international player is actually organising this kind of forum. Of course I understand that there’s a long-term business idea behind it – and there has to be.”
“To be honest, this is a very, very diffi cult line of insurance and it’s good to understand how it is done in other countries. Of course we offer our experience too, because this is a long-term investment: if you give something, you’re going to get something. It’s a normal situation. So it’s fantastic to have this kind of forum – this is unique. We have casualty seminars, property or D&O seminars, but workers’ compensa-tion is very special.”
Jarmo JacobssonChief Actuary, DirectorFederation of Accident Insurance Institutions (FAII), FinlandThe FAII coordinates all organisations involved in Finland’s statutory accident insurance.

14 Munich Re Future challenges in workers‘ compensation
Conclusions Awareness, dialogue and cooperation are called for
This paper does not intend to provide actual forecasts or solu-tions to future challenges, but rather to inspire lively dialogue and information sharing. At the same time, it seeks to present thoughts and fi ndings that should become part of the discus-sion on the future of workers’ compensation.
The developments looked at here are real and for the most part unstoppable. Some are in their infancy, like the use of cognitive enhancers, while others, such as musculoskeletal disorders, have been with us for many decades, yet are taking on new dimensions. It cannot be stressed enough that no single chal-lenge can be isolated. They all have considerable potential to compound one another, leading in many cases to occupational diseases and accidents of greater frequency and/or severity as well as to unprecedented legal complexity. It will become more and more diffi cult to determine whether claims are linked directly or indirectly to work. Increasing migration will mean multiple workers’ compensation systems and policies in differ-ent countries will often be involved in a single case. How can it be proved or disproved, for example, that a worker of advanced age suffers from lower back pain as a result of work? And how can labour histories of workers moving between countries, sys-tems and regulatory frameworks – and often changing occupa-tions on the way – be suffi ciently documented?
To ensure that workers’ compensation insurance can continue to fulfi l its intended role – to protect workers and their families from fi nancial burden in the event of an occupational accident and/or a disease and to give employers clear cost frameworks – it is time to think about how much the world in which it must function is changing. Systems should operate as smoothly and fairly as possible, with a maximum degree of openness to work-ers and a minimum of litigation.
Stability built on perfect balance Above all, the four basic mechanisms of social insurance – defi -nitions, benefi ts, coverage, fi nancing – must be kept in perfect balance to ensure future stability. The needs of all directly involved parties including employees, employers and the state as well as indirect stakeholders – in a broader sense, all of society – must be met. This calls for a heightened spirit of co-operation and transparency among all involved in the world’s

15Munich Re Future challenges in workers‘ compensation
workers’ compensation systems. In general, claims management will play a more prominent role, as will knowledge management and a more technical approach to understanding insured risks. Sharing methods and technologies that enhance effi ciency – examples include state-of-the-art data capture and manage-ment systems, discussed at the Fourth Workers’ Compensation Symposium hosted by the Munich Re Centre of Competence for Workers’ Compensation in March 2009 – is a good start. In addition, the challenges looming on the horizon will compel risk carriers and lawmakers to closely monitor the shifting risk landscape and what it means for the defi nition of events and conditions that trigger claims (triggers) and premiums.
The time is ripe for all workers’ compensation systems to sub-ject current reserves – notably IBNR (incurred but not reported) and IBNER (incurred but not enough reserved) – to a stress test in order to determine whether they are suffi cient to meet the challenges ahead. Especially in light of the fact that most emerging risks affect multiple groups including traditionally low-risk groups like offi ce workers, a very close look at the logic used to defi ne premiums (loadings) might be useful. The cat-egorical pricing approach, the allocation of industry types to specifi c or recommended tariffs or tariff ranges used in many countries, might not be valid in tomorrow’s world.
For 125 years, workers’ compensation insurance has been serv-ing as an anchor of fi nancial security and social stability. During that time, it has seen war and economic crises come and go. Entirely new industries and technologies have emerged, and previously unknown occupational diseases have appeared. Throughout all these developments, the concept of workers’ compensation insurance has endured. Provided stakeholders maintain an awareness of new developments and engage in open dialogue aimed at fi nding the best possible solutions for all parties, workers’ compensation systems can master the chal-lenges of the 21st century too.
Conclusions
“I expect future pressure on premiums. On the claims side, there will be pressure from private medical providers seeking profi t. Among claimants relapses or demands for permanent incapacity revi-sions will increase. And more regulatory control from supervisors and less reliability on fi nancial income from technical provisions will cause com-bined ratio fi gures to climb.”
“Although we have a fi xed price, my perception is that in the near future there will be adjustments in the pricing formula to accommodate the increase in
claims, but not in the recalculation algorithm. The inclusion of new diagnoses which are borderline with non-job-related diseases will impose a further burden on claims and costs.”
“With the current fi nancial crisis, major factors like weakening wage and salary growth and the overall reduction in investment are expected to slow growth in workers’ compensation insurance. At the same time, medical costs continue to rise. This trend threatens to cause higher combined ratios for both the public social security administrator and private insurers writing workers‘ compensation business.”
Francisco de Bras OliveirasCaixa Seguros é Saúde, Portugalspeaking at the workers’ Compensation Symposium 2009 in Munich.
Alejandro MoralesMutual de Seguridad, Chilespeaking at the workers’ Compensation Symposium 2009 in Munich.
Jawad JanebJordan Insurance Companyspeaking at the workers’ Compensation Symposium 2009 in Munich.

16 Munich Re Future challenges in workers‘ compensation
European Agency for Safety and Health at Work. European Union [http://europe.osha.eu.int].
4th Workers’ Compensation Symposium: Future Challenges, Munich 2009 [http://www.munichre.com/wcs/en/homepage/default.aspx].
Kappos, A.D., P. Bruckmann, T. Eikmann, N. Englert, U. Heinrich, P. Hoppe, E. Koch, G.H.M. Krause, W.G. Kreyling, K. Rauchfuss, P. Rombout, V. Schulz-Klemp, W.R. Thiel and H.E.Wichmann, 2004: “Health effects of particles in ambient air”. Int. J. Hyg. Envir. Heal., 399–407.
Martens, W.J.M., “Health Impacts of Climate Change and Ozone Depletion: An Ecoepidemiologic Modeling Approach”– Environmental Health Perspectives * Vol. 106, Supplement 1, February 1998.
Munich Re: “Workers’ Compensation: Analysis of private and public systems”. Germany, 2000.Occupational Safety & Health Administration (OSHA). USA. [http://www.osha.gov].
Pope, C.A., R.T. Burnett, M.J. Thun, E.E. Calle, D. Krewski, K. Ito and G.D. Thurston, 2002: “Lung cancer, cardiopulmonarymortality, and long-term exposure to fi ne particulate air pollution”. J. Am. Med. Assoc., 1132–1141.
Ramsey, J., 1995: “Task performance in heat: a review”. Ergonomics, 154–165.
Ramsey, J., C. Burford,M. Beshir and R. Hensen, 1983: “Effects of workplace thermal conditions on safe working behavior”. J. Safety Res., 105–114.
Randolph, S.E., 2001: “The shifting landscape of tick-borne zoonoses: tick-borne encephalitis and Lyme borreliosis in Europe”. Philos. T. Roy. Soc. Lond. B, 1045–1056.
Rao, S., J. Ku, S. Berman, D. Zhang and H.Mao, 2003: “Summertime characteristics of the atmospheric boundary layer and relationships to ozone levels over the eastern United States”. Pure Appl. Geophys., 21–55.
Rosenzweig, C., G. Casassa, D.J. Karoly, A. Imeson, C. Liu, A. Menzel, S. Rawlins, T.L. Root, B. Seguin, P. Tryjanowski, 2007: “Assessment of observed changes and responses in natural and managed systems”. Climate Change 2007: Impacts, Adaptation and Vulner-ability. Contribution of Working Group II to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change, M.L. Parry, O.F. Canziani, J.P. Palutikof, P.J. van der Linden and C.E. Hanson, Eds., Cambridge University Press, Cambridge, UK, 79–131.
Schichtel, B. and R. Husar, 2001: “Eastern North Ameri-can transport climatology during high- and low-ozone days”. Atmos. Environ., 1029–1038.
The National Institute for Occupational Safety and Health (NIOSH). USA. [http://www.cdc.gov/niosh/homepage.html].
Toennesmann, J. In Wirtschaftswoche, 20.10.2008, Nr. 43, p.138–143.
United Nations University, Institute for Environment and Human Security.
United Nations. Narcotics Bulletin Issue 2, 1993.
References:
© 2009Münchener Rückversicherungs-GesellschaftKöniginstrasse 10780802 MünchenGermanyTel.: +49 (0) 89/38 91-0Fax: +49 (0) 89/39 90 56http://www.munichre.com
Responsible for contentGlobal Clients/North AmericaCentre of Competence for Workers’ Compensation
ContactDr. med. Héctor Upegui-GarcíaTel.: +49 (0) 89/38 91-24 02Fax: +49 (0) 89/38 91-7 24 02E-mail: [email protected]
Ertl ChristineTel.: +49 (0) 89/38 91-92 62Fax: +49 (0) 89/38 91-792 62E-mail: [email protected]
Victor SchultheissTel.: +49 (89) 38 91-22 38Fax: +49 (89) 38 91-7 22 38E-mail: [email protected]
Picture creditsCover: Getty images/David Ellisp. 2: Getty images/Will & Deni McIntyrep. 4: Getty images/Eric Audrasp. 6: Getty images/Ciaran Griffi npp. 13-15: Oliver Soulas, München
Printed by: Color Offset GmbHGeretsrieder Strasse 1081379 MünchenGermany
© 2009Münchener Rückversicherungs-GesellschaftKöniginstrasse 10780802 MünchenGermany
Order number 302-06153

FUTURE CHALLENGES IN WORKERS‘
COMPENSATION INSURANCE AN OPPORTUNITY FOR INTERNATIONAL COOPERATION
21 June 2011
Dr. Hector Upegui, MD
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Our Unit -
History and Main Activities
MR WORKERS’
COMPENSATION UNIT WAS ESTABLISHED IN 1998 ASCENTRE OF COMPETENCE
Observe and accompany private participation and/or reform processes
Develop worldwide opinion leadership position for comparing and developing
systems either with private participation &/or public Workers’
Comp. Systems
Provide advice and service on both insurance and reinsurance questions, from
legislative to operational
Exchange know how and expertise with Munich Re America
Generate substantial reinsurance business for Munich Re
Concentrate and amplify expertise within the Munich Re Group
2
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Introduction –
General Characteristics
Workers‘
compensation insurance provides coverage in order to help the insured and the families to overcome the burden of an occupational injury or an
occupational disease
Some major characteristics of WC systems:
No fault
Compulsory
Highly regulated
Employer pays
Links to Social Security systems
3
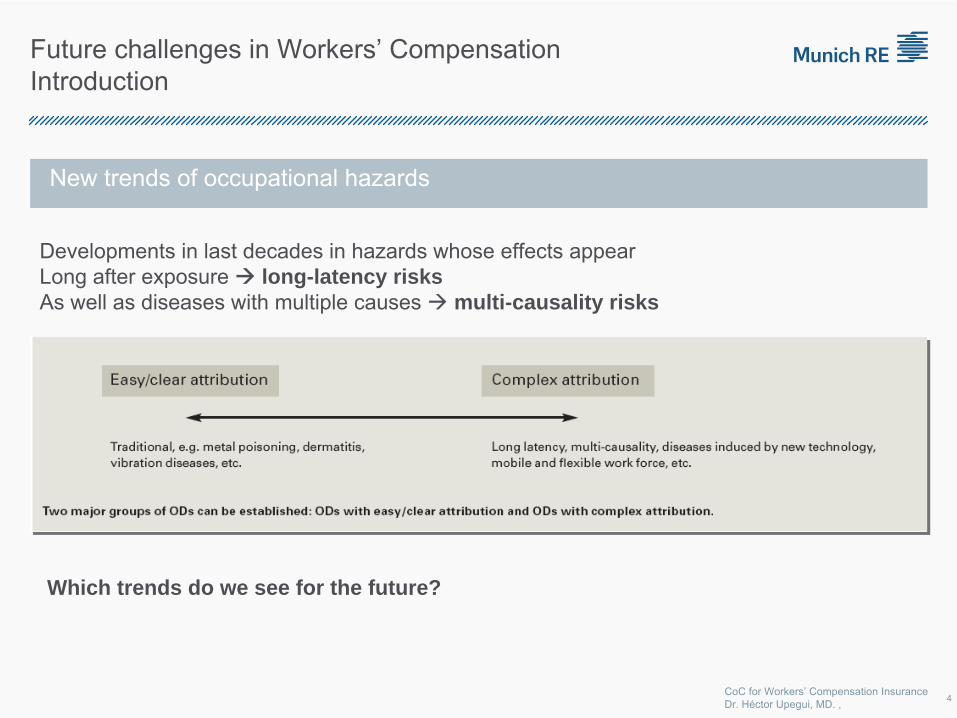
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
New trends of occupational hazards
Developments in last decades in hazards whose effects appear Long after exposure long-latency risksAs well as diseases with multiple causes multi-causality risks
Which trends do we see for the future?
Future challenges in Workers’
Compensation Introduction
4
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Definition: Any condition that might affect the performance of a
Workers'
Compensation System
The condition/challenge must follow the following criteria :
Independent: should be able to affect any workers' compensation system, independently of the way in which it operates (under competition, without competition, public, with private participation, etc.)
International: should be able to affect any workers' compensation system, independently of the country or territory where the system operates
Important: where the expected impact in terms of frequency and severity is important enough to raise awareness
Identifiable: there should be evidence to show that the risk/condition might cause an impact on the workers' compensation insurance
Future challenges in Workers’
Compensation
5
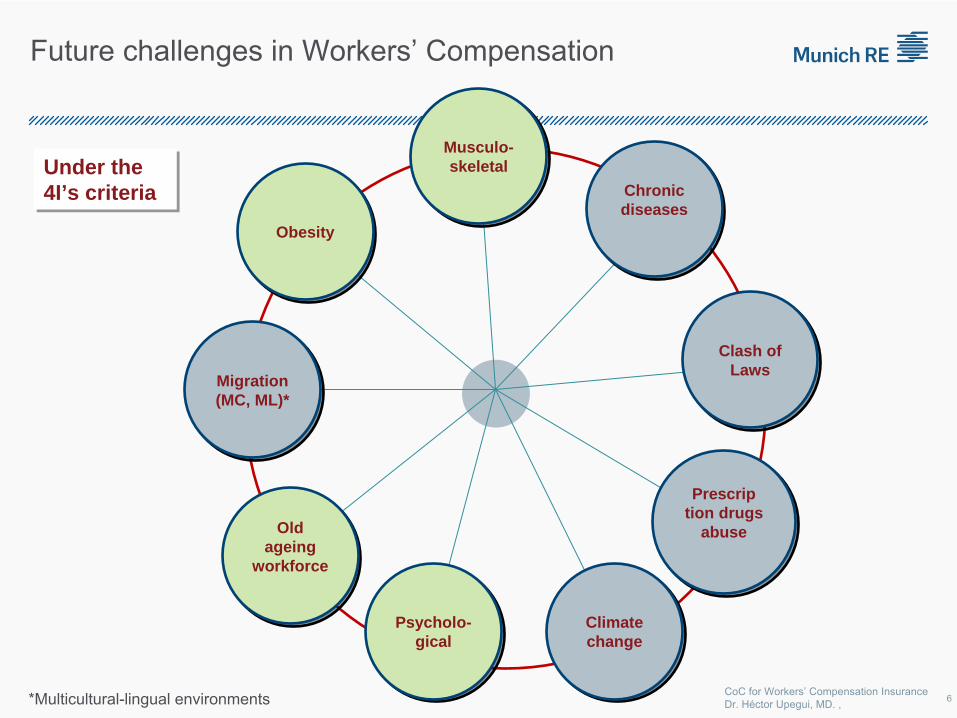
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. , 6
Under the 4I’s criteria Under the 4I’s criteria
*Multicultural-lingual environments
Obesity Obesity
Migration (MC, ML)* Migration (MC, ML)*
Psycholo- gical
Psycholo- gical
Climate change Climate change
Old ageing
workforce
Old ageing
workforce
Musculo- skeletal
Musculo- skeletal
Prescrip tion drugs
abuse
Prescrip tion drugs
abuse
Clash of Laws
Clash of Laws
Chronic diseases Chronic diseases
Future challenges in Workers’
Compensation
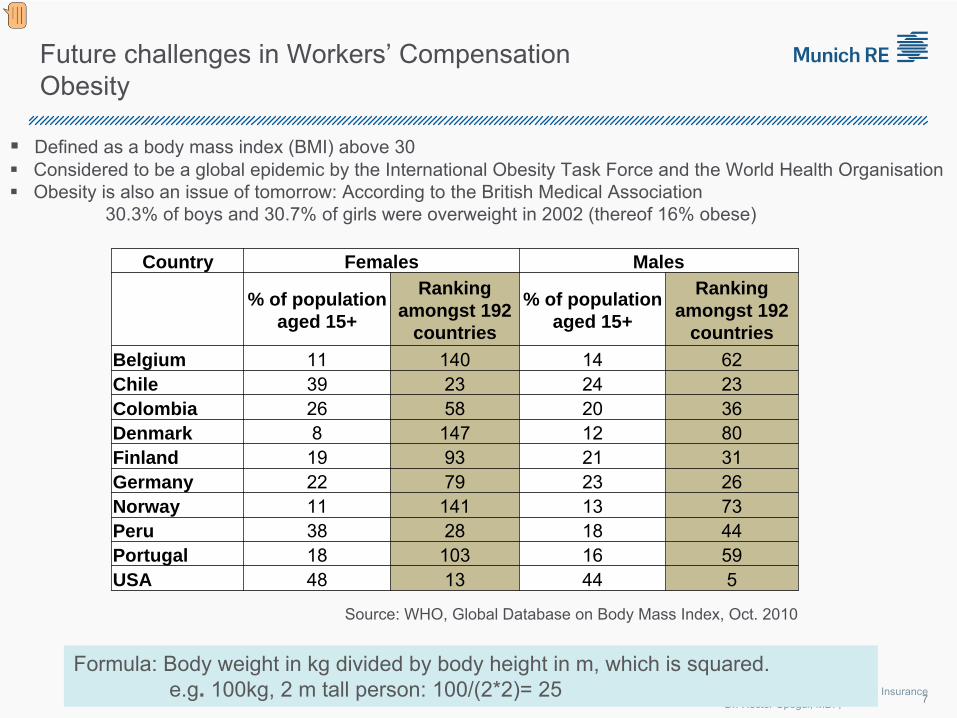
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Defined as a body mass index (BMI) above 30
Considered to be a global epidemic by the International Obesity
Task Force and the World Health Organisation
Obesity is also an issue of tomorrow: According to the British Medical Association 30.3% of boys and 30.7% of girls were overweight in 2002 (thereof 16% obese)
Future challenges in Workers’
Compensation Obesity
7
Source: WHO, Global Database on Body Mass Index, Oct. 2010
Country Females Males
% of population aged 15+
Ranking amongst 192
countries
% of population aged 15+
Ranking amongst 192
countries
Belgium 11 140 14 62Chile 39 23 24 23Colombia 26 58 20 36Denmark 8 147 12 80Finland 19 93 21 31Germany 22 79 23 26Norway 11 141 13 73Peru 38 28 18 44Portugal 18 103 16 59USA 48 13 44 5
Formula: Body weight in kg divided by body height in m, which is
squared. e.g. 100kg, 2 m tall person: 100/(2*2)= 25
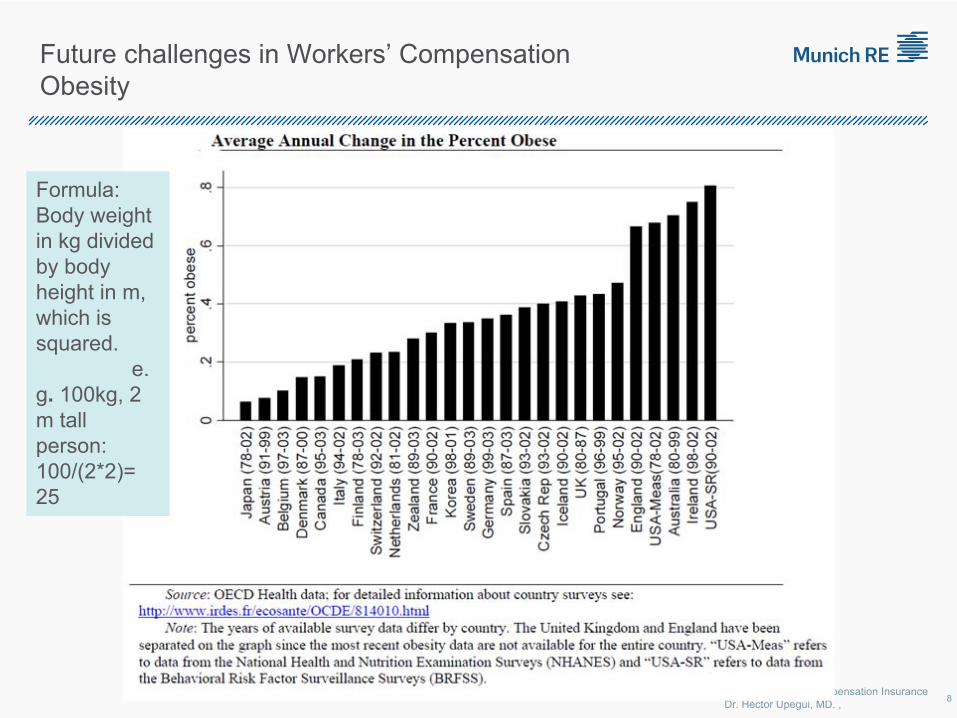
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Future challenges in Workers’
Compensation Obesity
8
Formula: Body weight in kg divided by body height in m, which is squared.
e.
g. 100kg, 2 m tall person: 100/(2*2)= 25
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Obesity Research
NCCI Research Brief –
Nov 2010:
“
RESERVING IN THE AGE OF OBESITY”
Some Key Findings:
Obese claims are more expensive than non-obese claims, and the differences in costs are magnified as the claims mature
Obese claims are 2.8 times more expensive at the 12-month maturity
Obese claims are 4.5 times more expensive at the 36-month maturity
Obese claims are 5.3 times more expensive at the 60-month maturity
The cost difference (at the five year maturity) is less for females than for males.
Mandatory utilization review and, in particular, mandatory bill review significantly reduce the cost difference between obese and non-obese claims.
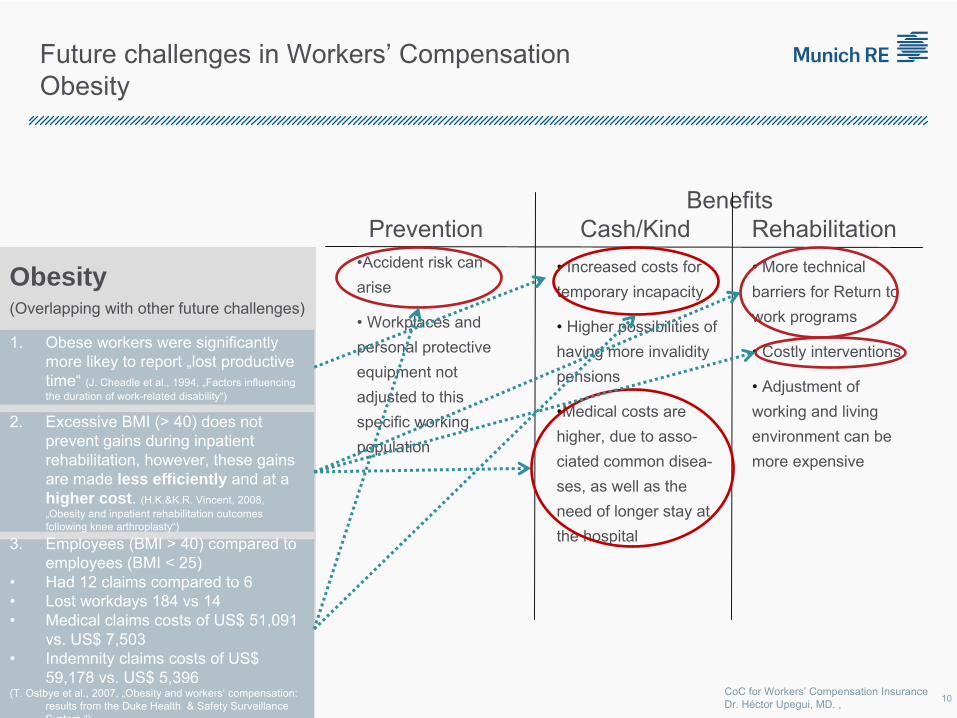
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Obesity(Overlapping with other future challenges)
BenefitsPrevention Cash/Kind
Rehabilitation
•Accident risk can arise
•
Workplaces and personal protective equipment not adjusted to this specific working population
•
Increased costs for temporary incapacity
•
Higher possibilities of having more invalidity pensions
•Medical costs are higher, due to asso-
ciated common disea-
ses, as well as the need of longer stay at the hospital
•
More technical barriers for Return to work programs
• Costly interventions
•
Adjustment of working and living environment can be more expensive
Future challenges in Workers’
Compensation Obesity
1.
Obese workers were significantly more likey to report „lost productive time“
(J. Cheadle et al., 1994, „Factors influencing the duration of work-related disability“)
2.
Excessive BMI (> 40) does not prevent gains during inpatient rehabilitation, however, these gains are made less efficiently and at a higher cost. (H.K.&K.R. Vincent, 2008, „Obesity and inpatient rehabilitation outcomes following knee arthroplasty“)
3.
Employees (BMI > 40) compared to employees (BMI < 25)
•
Had 12 claims compared to 6•
Lost workdays 184 vs 14•
Medical claims costs of US$ 51,091 vs. US$ 7,503
•
Indemnity claims costs of US$ 59,178 vs. US$ 5,396
(T. Ostbye et al., 2007, „Obesity and workers‘
compensation: results from the Duke Health & Safety Surveillance System
“)
10
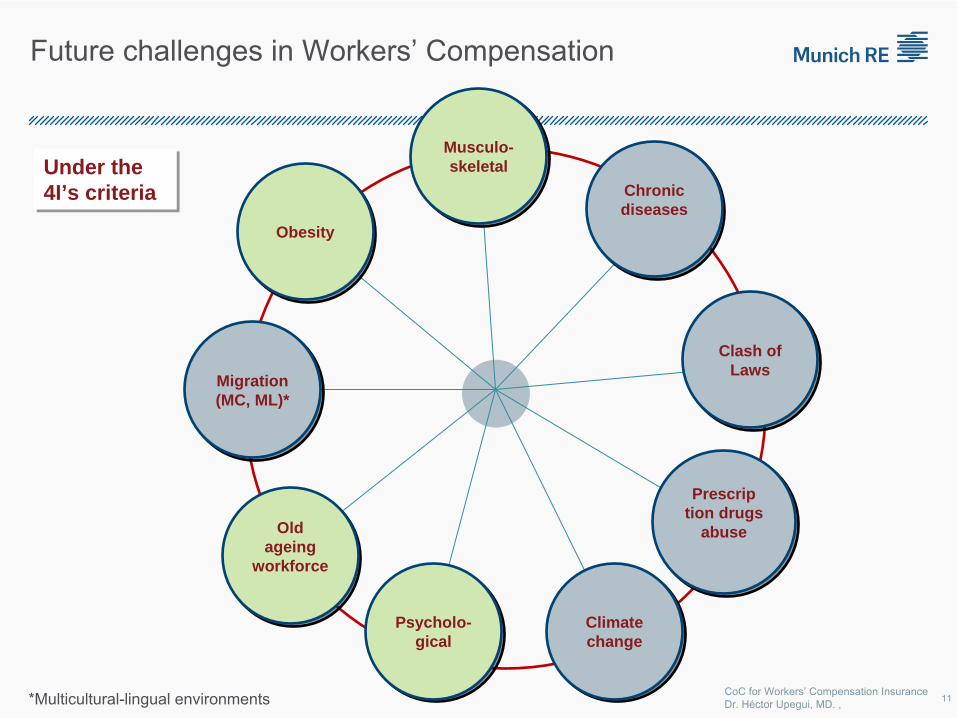
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. , 11
Under the 4I’s criteria Under the 4I’s criteria
*Multicultural-lingual environments
Obesity Obesity
Migration (MC, ML)* Migration (MC, ML)*
Psycholo- gical
Psycholo- gical
Climate change Climate change
Old ageing
workforce
Old ageing
workforce
Musculo- skeletal
Musculo- skeletal
Prescrip tion drugs
abuse
Prescrip tion drugs
abuse
Clash of Laws
Clash of Laws
Chronic diseases Chronic diseases
Future challenges in Workers’
Compensation
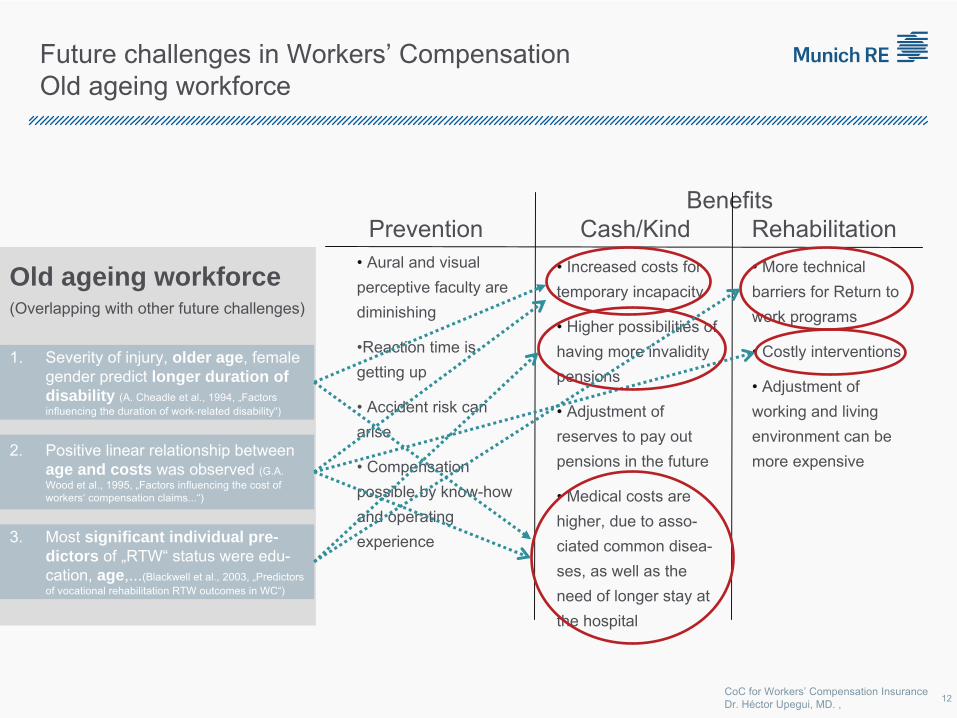
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Old ageing workforce(Overlapping with other future challenges)
BenefitsPrevention Cash/Kind
Rehabilitation
•
Aural and visual perceptive faculty are diminishing
•Reaction time is getting up
•
Accident risk can arise
•
Compensation possible by know-how and operating experience
•
Increased costs for temporary incapacity
•
Higher possibilities of having more invalidity pensions
•
Adjustment of reserves to pay out pensions in the future
•
Medical costs are higher, due to asso-
ciated common disea-
ses, as well as the need of longer stay at the hospital
•
More technical barriers for Return to work programs
• Costly interventions
•
Adjustment of working and living environment can be more expensive
Future challenges in Workers’
Compensation Old ageing workforce
1.
Severity of injury, older age, female gender predict longer duration of disability (A. Cheadle et al., 1994, „Factors influencing the duration of work-related disability“)
2.
Positive linear relationship between age and costs was observed (G.A. Wood et al., 1995, „Factors influencing the cost of workers‘
compensation claims...“)
3.
Most significant individual pre- dictors of „RTW“
status were edu-
cation, age,...(Blackwell et al., 2003, „Predictors of vocational rehabilitation RTW outcomes in WC“)
12
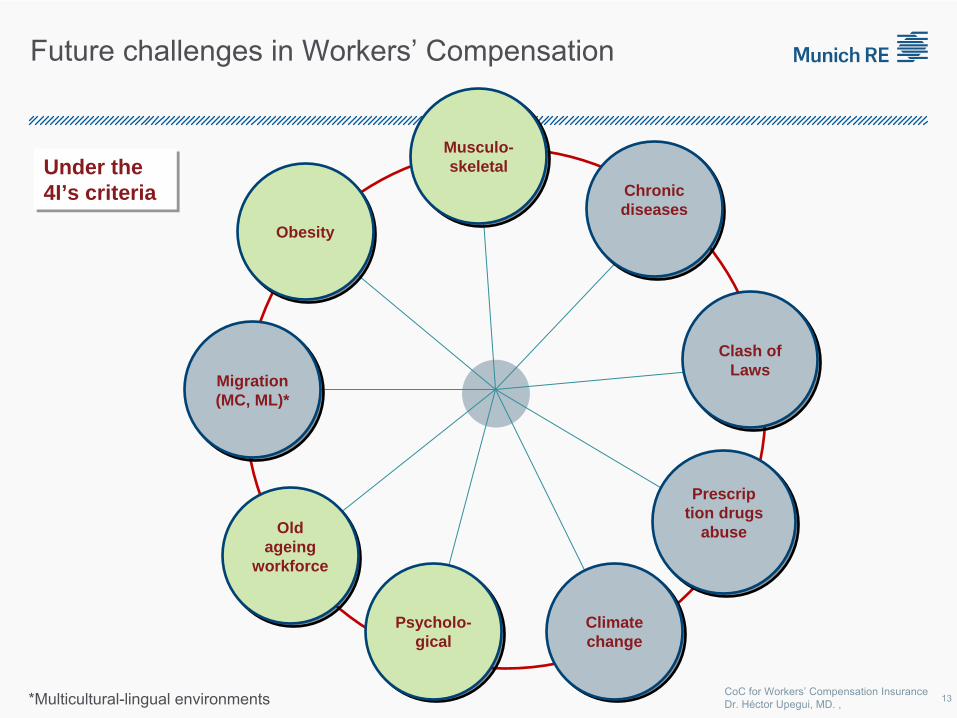
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. , 13
Under the 4I’s criteria Under the 4I’s criteria
*Multicultural-lingual environments
Obesity Obesity
Migration (MC, ML)* Migration (MC, ML)*
Psycholo- gical
Psycholo- gical
Climate change Climate change
Old ageing
workforce
Old ageing
workforce
Musculo- skeletal
Musculo- skeletal
Prescrip tion drugs
abuse
Prescrip tion drugs
abuse
Clash of Laws
Clash of Laws
Chronic diseases Chronic diseases
Future challenges in Workers’
Compensation
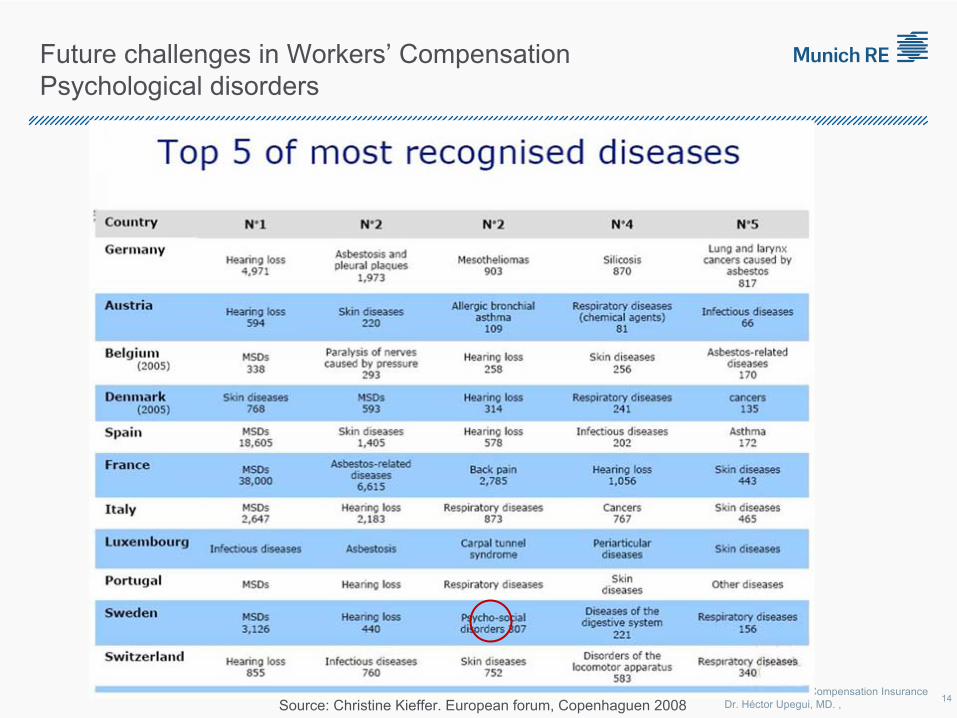
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,Source: Christine Kieffer. European forum, Copenhaguen 2008
Future challenges in Workers’
Compensation Psychological disorders
14
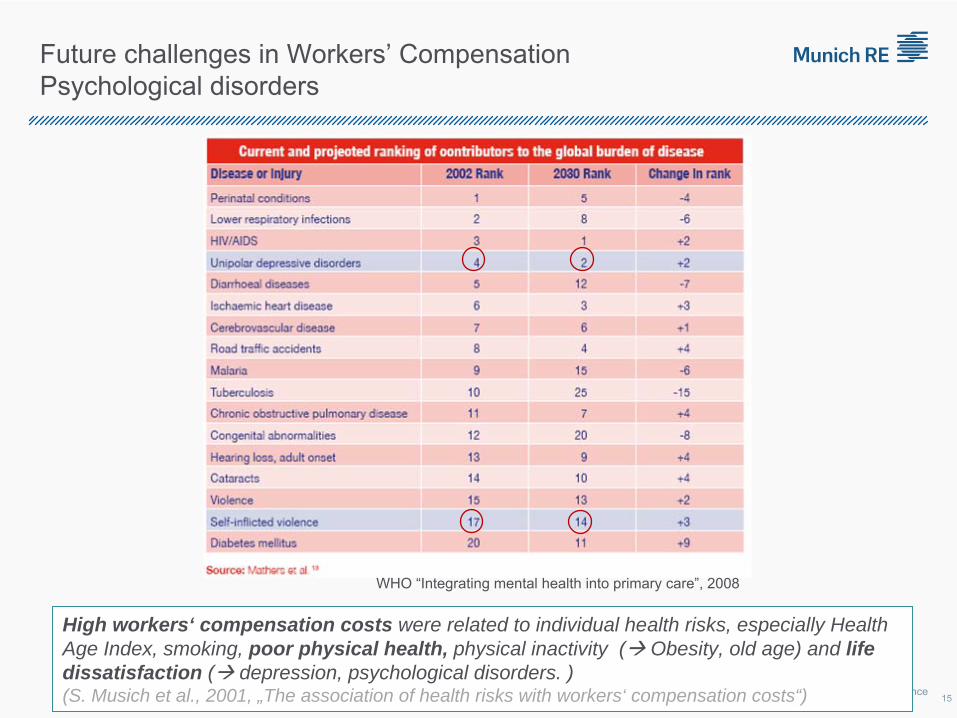
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
WHO “Integrating mental health into primary care”, 2008
Future challenges in Workers’
Compensation Psychological disorders
High workers‘ compensation costs were related to individual health risks, especially Health Age Index, smoking, poor physical health, physical inactivity ( Obesity, old age) and life dissatisfaction ( depression, psychological disorders. )(S. Musich et al., 2001, „The association of health risks with workers‘ compensation costs“) 15
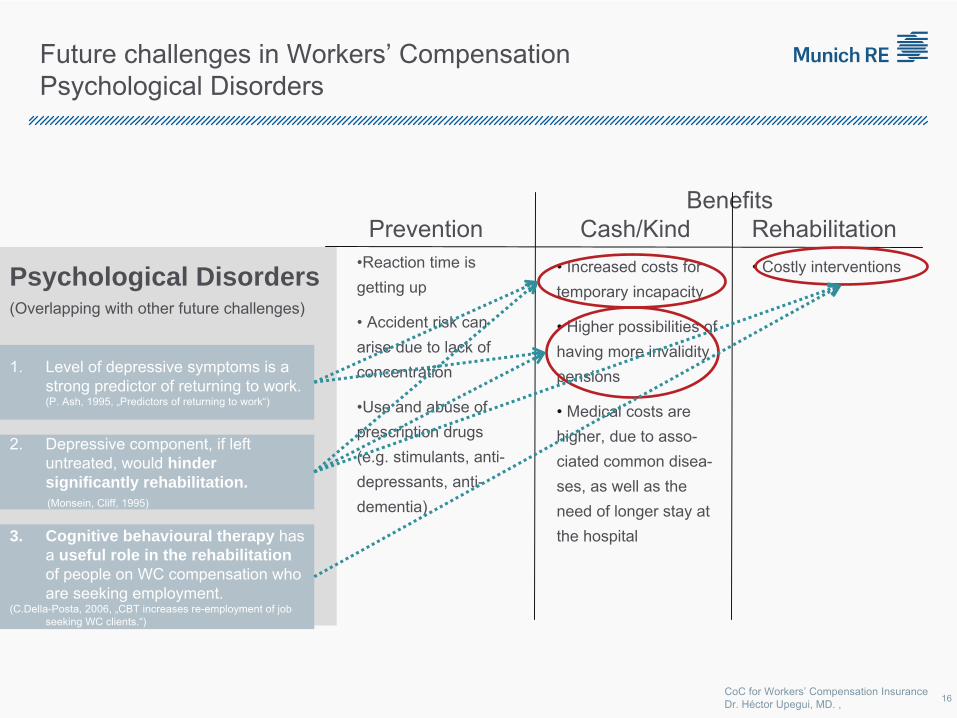
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
Psychological Disorders(Overlapping with other future challenges)
BenefitsPrevention Cash/Kind
Rehabilitation
•Reaction time is getting up
•
Accident risk can arise due to lack of concentration
•Use and abuse of prescription drugs (e.g. stimulants, anti-
depressants, anti-
dementia)
•
Increased costs for temporary incapacity
•
Higher possibilities of having more invalidity pensions
•
Medical costs are higher, due to asso-
ciated common disea-
ses, as well as the need of longer stay at the hospital
• Costly interventions
Future challenges in Workers’
Compensation Psychological Disorders
1.
Level of depressive symptoms is a strong predictor of returning to work. (P. Ash, 1995, „Predictors of returning to work“)
2.
Depressive component, if left untreated, would hinder significantly rehabilitation.(Monsein, Cliff, 1995)
3. Cognitive behavioural therapy has a useful role in the rehabilitation of people on WC compensation who are seeking employment.
(C.Della-Posta, 2006, „CBT increases re-employment of job seeking WC clients.“)
16
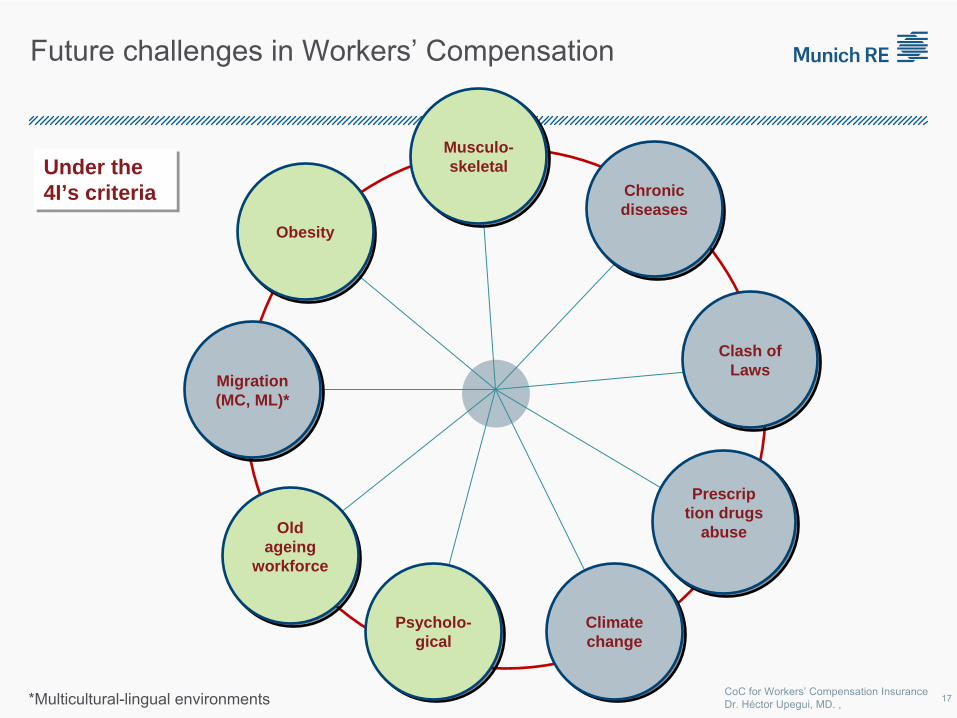
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. , 17
Under the 4I’s criteria Under the 4I’s criteria
*Multicultural-lingual environments
Obesity Obesity
Migration (MC, ML)* Migration (MC, ML)*
Psycholo- gical
Psycholo- gical
Climate change Climate change
Old ageing
workforce
Old ageing
workforce
Musculo- skeletal
Musculo- skeletal
Prescrip tion drugs
abuse
Prescrip tion drugs
abuse
Clash of Laws
Clash of Laws
Chronic diseases Chronic diseases
Future challenges in Workers’
Compensation
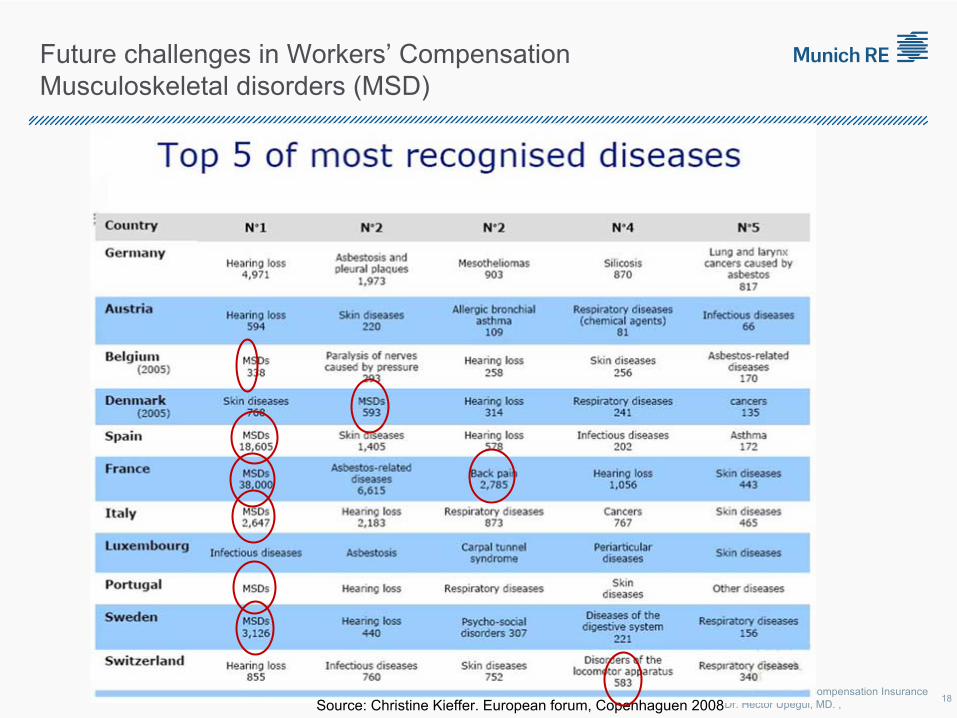
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,Source: Christine Kieffer. European forum, Copenhaguen 2008
Future challenges in Workers’
Compensation Musculoskeletal disorders (MSD)
18
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
FUTURE CHALLLENGES
Old ageing workforce ObesityMusculoskeletal Migration PsychologicalClimate change Chronic diseasesPrescription Drugs abuse Clash of laws
Future challenges in Workers’
Compensation Conclusions
19
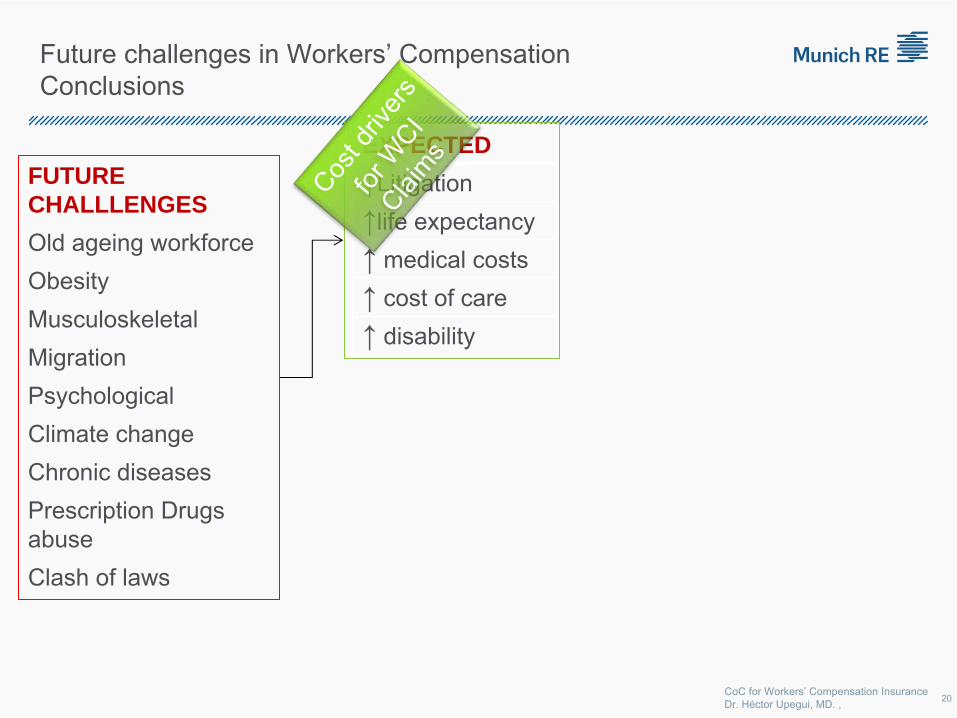
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
FUTURE CHALLLENGES
Old ageing workforce ObesityMusculoskeletal Migration PsychologicalClimate change Chronic diseasesPrescription Drugs abuse Clash of laws
EXPECTED
↑Litigation↑life expectancy↑ medical costs↑ cost of care↑ disability
Cost d
river
s
for W
CI Clai
ms
Future challenges in Workers’
Compensation Conclusions
20
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
FUTURE CHALLLENGES
Old ageing workforce ObesityMusculoskeletal Migration PsychologicalClimate change Chronic diseasesPrescription Drugs abuse Clash of laws
EXPECTED
↑Litigation↑life expectancy↑ medical costs↑ cost of care↑ disability
CONSEQUENCES
↑ reserves. Especially, IBNER & IBNR
↑ investment in claims management (health care and care)
↑ return to Work programs↑ investment in knowledge
management
Cost d
river
s
for W
CI Clai
ms
Press
ure o
n
the pr
emium
Future challenges in Workers’
Compensation Conclusions
21
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
FUTURE CHALLLENGES
Old ageing workforce ObesityMusculoskeletal Migration PsychologicalClimate change Chronic diseasesDrugs/Medicaments abuse Clash of laws
EXPECTED
↑Litigation↑life expectancy↑ medical costs↑ cost of care↑ disability
CONSEQUENCES
↑ reserves. Especially, IBNER & IBNR
↑ investment in claims management (health care and care)
↑ return to Work programs↑ investment in knowledge
management
Cost d
river
s
for W
CI Clai
ms
Press
ure o
n
the pr
emium
ACTIONS AND SOLUTIONS
Macrolevel: More lobby, improve contact with social policy makers and decision takers
Generate platforms, forums, to foster the exchange of knowledge (Risk knowledge) transform the risk (Claims management, RTW, etc.)
Create new scenariosRethink triggers
Future challenges in Workers’
Compensation Conclusions
22
CoC for Workers’ Compensation Insurance Dr. Héctor Upegui, MD. ,
THANK YOU VERY MUCH!
Dr. Héctor
Upegui, MDSenior Consultant
Employment of People with Disabilities in Ireland: Research and Strategy
Mary Van Lieshout
What the National Disability Authority does
• Provides policy advice to the Irish Government and public bodies
• Undertakes, commissions and collaborates in disability research and assists
in the development of statistical information
• Advises on standards and guidelines in services to people with disabilities
• Develops standards, education and awareness of Universal Design
Data on employment of people with disabilities• In the 2006 Census, the employment rate of people with disabilities was less
than half that of those without, at 21.6% to 57.2%
• In the same census, people with disabilities made up 4% of the total number
of those in employment
• According to a 2006 survey for the National Physical and Sensory Disability
Database, 57.1% of respondents experienced participation restriction in the
area of employment and job seeking
• Approximately 70% of people with disabilities acquired them since birth
(QNHS 2002)
Researching the employment of people with disabilities in Ireland• Disability and Labour Market Participation, a 2004 report produced by the
ESRI for the Equality Authority, notes that such surveys as currently exist are
better at measuring levels of labour and employment than they are at
measuring gradations of disability
• Different datasets such as the Census, the QNHS and the Living in Ireland
Survey vary in their definitions of both employment and disability
• The NDA, on behalf of the CSO, has represented Ireland in the work of the
Washington City Group on setting global standards of disability statistics
Employment policies for people with disabilities• The relevant chapter in Disability and Social Policy in Ireland (2003),
identifies three modes of policy in operation:
– Obligatory non-discrimination and actions to reasonably accommodate: legislation
including the 1998 Employment Equality Act and the 2005 Disability Act
– Voluntary positive action: including sheltered, supported and rehabilitative
employment
– Voluntary targets: the 3% quota for employment in the civil and public service
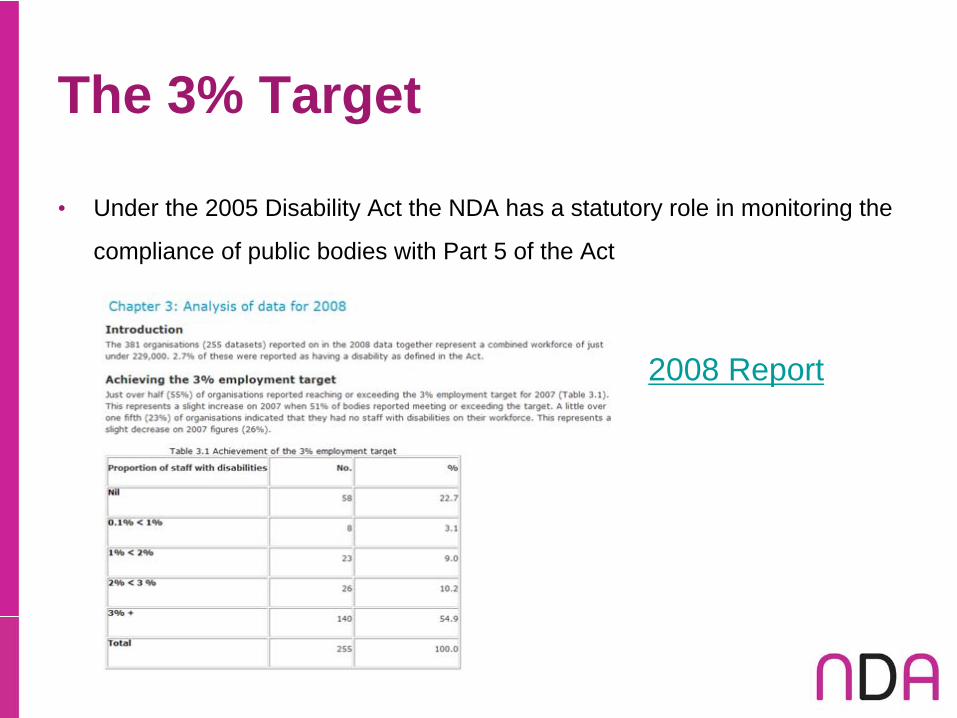
The 3% Target
• Under the 2005 Disability Act the NDA has a statutory role in monitoring the
compliance of public bodies with Part 5 of the Act
2008 Report
Welfare entitlements relating to disability and employment• The main social welfare payments for people with long-term illness or
disabilities are the invalidity pension, the means-tested disability allowance,
and the blind pension
• Upon written approval, people receiving disability payments can engage in
rehabilitative or therapeutic work while keeping their payments
• In addition, there are a range of secondary benefits due to those who are
receiving social welfare disability payments, which may be retained according
to earnings
Difficulties
• A Strategy for Engagement: Towards a Comprehensive Employment
Strategy for People with Disabilities (NDA, 2006) identifies persistent
inequality both in the area of educational qualifications and dependency on
welfare payments
• It also describes the pre-existing experience of people with disabilities in
Ireland as one of ‘unequal treatment’ and the current system of welfare and
employment measures as ‘an outdated model’
Challenges
• Further challenges observed in the Strategy for Engagement include:
– The ‘moving on’ of the employment market towards more high-skilled jobs
– Relatively few companies have experience in accommodating workers with less
restrictions, and even fewer those with more severe restrictions (the demand side
of employment of people with disabilities)
– The heterogeneity of the population of people with disabilities in terms of their
circumstances, needs and abilities, which must be taken into account in policy
– Whether it is a voluntary choice to work fewer hours, in part-time or self-
employment, or if it is an effect of the welfare system or the workplace

Pillars of a Strategy of Engagement
• Six pillars are identified on which to base a comprehensive strategy:
1. Removing benefit traps and disincentives towards working in the welfare system
2. Enhancing the effectiveness of education and training to ensure that people with
disabilities can compete in the current and future labour markets
3. Ensuring demand-side awareness of disabilities in the labour market
4. Devising preventative strategies to reduce early school-leaving, and to improve
retention in employment following adult-onset disability
5. Engaging with people with disabilities and their employment aspirations
6. Ensuring that the provision of the above is sufficiently diverse to meet the needs
of all people with disabilities, especially those experiencing severe disabilities
Benefiting from the Irish experience
• From a recent speech by the Minister for Health, Dr. James Reilly
– “Under the new Universal Health Insurance system everyone will have health
insurance from their choice of insurance company. This insurance will guarantee
every citizen equal access to a comprehensive range of hospital and medical
services. Moreover, it will offer greater transparency for people by directly linking
their payments on health insurance to an associated level of benefits or service
entitlements.
The core purpose of universal health insurance is to achieve equity of access to
healthcare. Similarly, the concept of equity will inform the internal design of the
insurance system which will be based on community rating and a robust risk
equalisation scheme, governed by a new Regulator – the Hospital Insurance
Fund.”
Accident insurance systems
• Ireland is keen to learn from international best practice in
this area
• In order to advise our government, the NDA is keen to
have access to further details on systems, costs, and
outcomes for people for disabilities of such schemes

suva
Die Suva ist mehr als eine Versicherung Kurzporträt Die Schweizerische Unfallversicherungsanstalt (Suva1) ist die wichtigste Trägerin der obligatorischen Unfallversicherung in der Schweiz. Gut die Hälfte der Schweizer Berufstätigen (rund 2 Millionen Versicherte in 115 000 Unternehmen) sind bei ihr gegen die Folgen von Unfällen in Beruf und Freizeit sowie gegen Be-rufskrankheiten versichert. Die Suva ist ein selbständiges, nicht gewinnorientier-tes Unternehmen des öffentlichen Rechts (Non-Profit-Organisation). Sie arbeitet selbstragend, ohne öffentliche Gelder und gibt Gewinne in Form von tieferen Prämien an die Versicherten zurück. Im Verwaltungsrat sind die Sozialpartner - Arbeitgeber und Arbeitnehmer - und der Bund vertreten. Die Suva bietet ihren Versicherten einen ganzheitlichen Gesundheitsschutz. Ihre Dienstleistungen umfassen Prävention, Versicherung und Rehabilitation. Im Auf-trag des Bundes führt sie seit 2005 auch die Militärversicherung. Rund 3000 Mit-arbeiterinnen und Mitarbeiter stehen für die Versicherten im Einsatz, davon 600 in ihren beiden Rehabilitationskliniken. Luzern, Mai 2011
1 www.suva.ch

Felix Weber
Suva, Member of Business Management
Rehabilitation and Return to Work/Dresden 22 June 2011
Suva claims management: a quality programme designed to contain rehabilitation costs
Bild ?
AGENDA
1 Suva at a glance
2 Occupational reintegration – a key concern for Suva
3 Suva’s claims management
Goals
Three processes
Focus on complex cases
4 Experiences and results
2
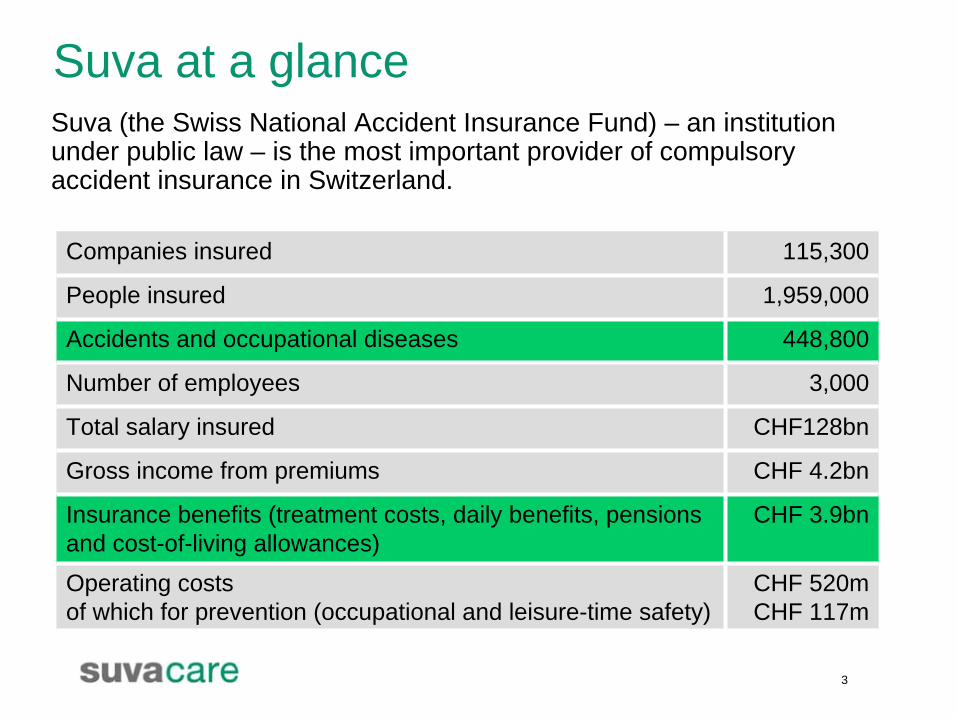
Suva at a glance
Companies insured 115,300
People insured 1,959,000
Accidents and occupational diseases 448,800
Number of employees 3,000
Total salary insured CHF128bn
Gross income from premiums CHF 4.2bn
Insurance benefits (treatment costs, daily benefits, pensions and cost-of-living allowances)
CHF 3.9bn
Operating costs of which for prevention (occupational and leisure-time safety)
CHF 520m CHF 117m
Suva (the Swiss National Accident Insurance Fund) – an institution under public law – is the most important provider of compulsory accident insurance in Switzerland.
3
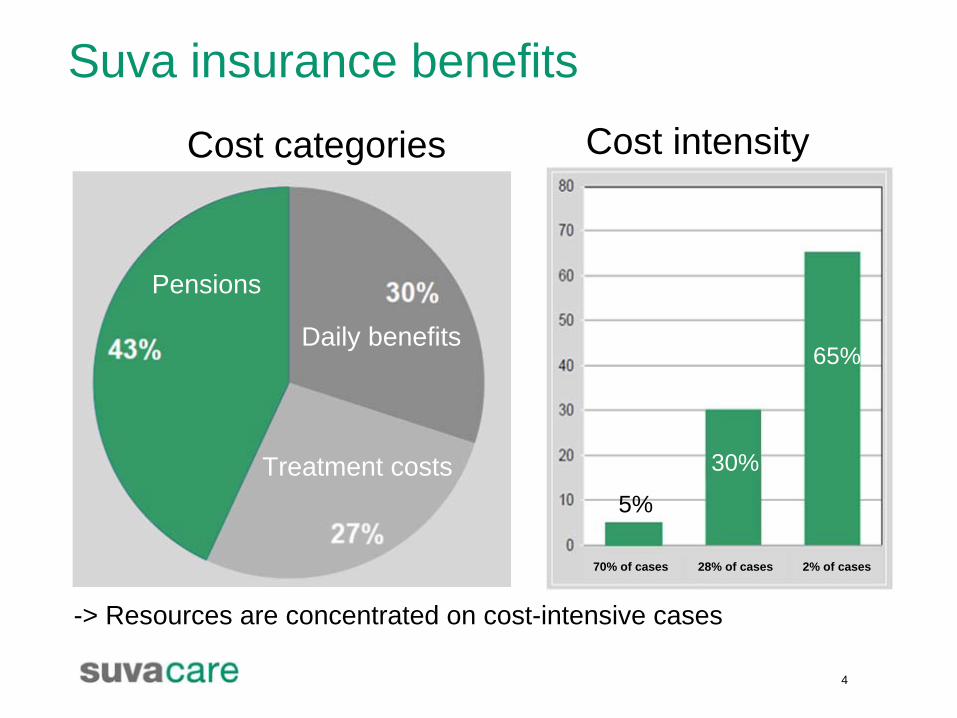
Suva insurance benefits
-> Resources are concentrated on cost-intensive cases
Cost categories Cost intensity
Pensions
Daily benefits
Treatment costs5%
30%
65%
4
70% of cases 28% of cases 2% of cases

Occupational rehabilitation - a key concern for Suva
5
Suva – more than just insurance:A combination of prevention, insurance and rehabilitation.
Occupational reintegration - benefits for everyone
6
Personal benefits for accident victims•They regain their independence•They participate in everyday working life•They are not socially excluded
Financial benefits for insurers and insurees• Reduction in cost-intensive pension benefits lower premiums
Social benefits• Advantages for society in general
Occupational reintegration - what Suva offers:
7
• Comprehensive care and support for seriously injured insurees
• Work-oriented rehabilitation at Suva clinics
• Occupational reintegration initiative: an incentive system for employers
• Cooperation with other insurers (mainly concerning disability insurance) and institutions
• Cooperation with employment agencies
The emphasis is placed on a return to the previous workplace. Occupational reorientation as far as this is necessary.
AGENDA
1 Suva in brief
2 Occupational reintegration – a key concern for Suva
3 Suva’s claims management
Goals
The part-processes
Focus on complex cases
4 Experiences and results
8

Goals of claims management
9
High-quality, customer-friendly, effective and economical claims management
The part-processes
Normal
Complex
Standard
10
Severely injured victims (e.g. people with cerebral injuries, serious multiple injuries)
Cervical spine injury victims unable to work > 4 weeks
Psychological complaints
Cases of anticipated disability
Workplace at risk or even the loss of a workplace
Foreseeable or existing reintegration problems
Difficult social environments
.......
Management of complex cases (1)
A vital role is played not only by the injuries themselves, but also by the “soft factors” as they are known. These are the accident victims’ personal and, in particular, occupational backgrounds.
11
Komplex
Management of complex cases (2)
“Case Management” does not mean that the accident victims are managed. Instead, it is the extraordinary situation in which the victims find themselves that is managed.
Timely, comprehensive and intensive care as well as the specific promotion of victims’ occupational reintegration with full regard for their personal resources (“encourage + expect”).
Coordination of medical and occupational rehabilitation measures.
Goal-oriented assistance and care from “A – Z” by one case manager right from the time of the accident itself if possible.
12
Case Managers:• Insurance specialists with high-level specialist, social,
communication and leadership skills• Practice-oriented training in in-house suva workshops• Regular specialist and behavioural further training
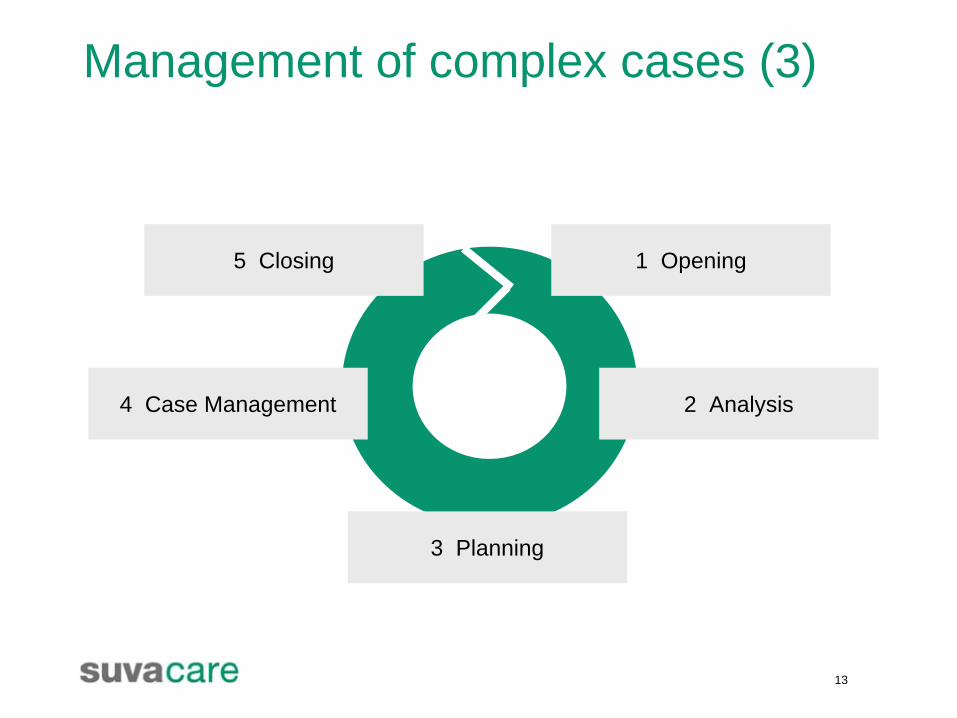
Management of complex cases (3)
1 Opening
2 Analysis
3 Planning
4 Case Management
5 Closing
13
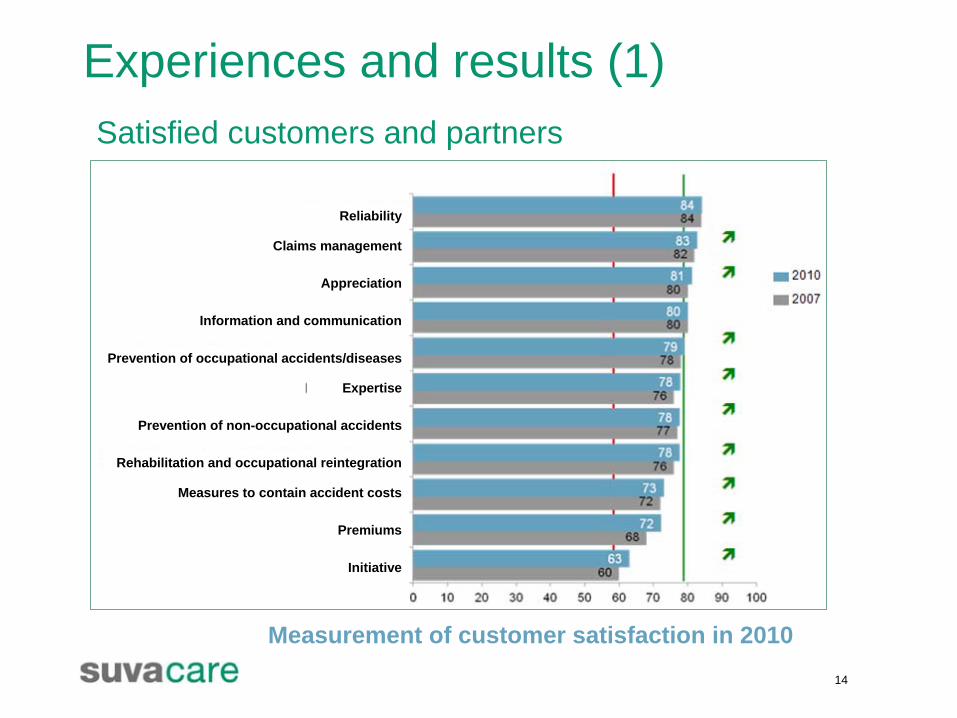
Experiences and results (1)
14
Satisfied customers and partners
Measurement of customer satisfaction in 2010
Reliability
Information and communication
Prevention of non-occupational accidents
Premiums
Rehabilitation and occupational reintegration
Claims management
Prevention of occupational accidents/diseases
Appreciation
Expertise
Measures to contain accident costs
Initiative
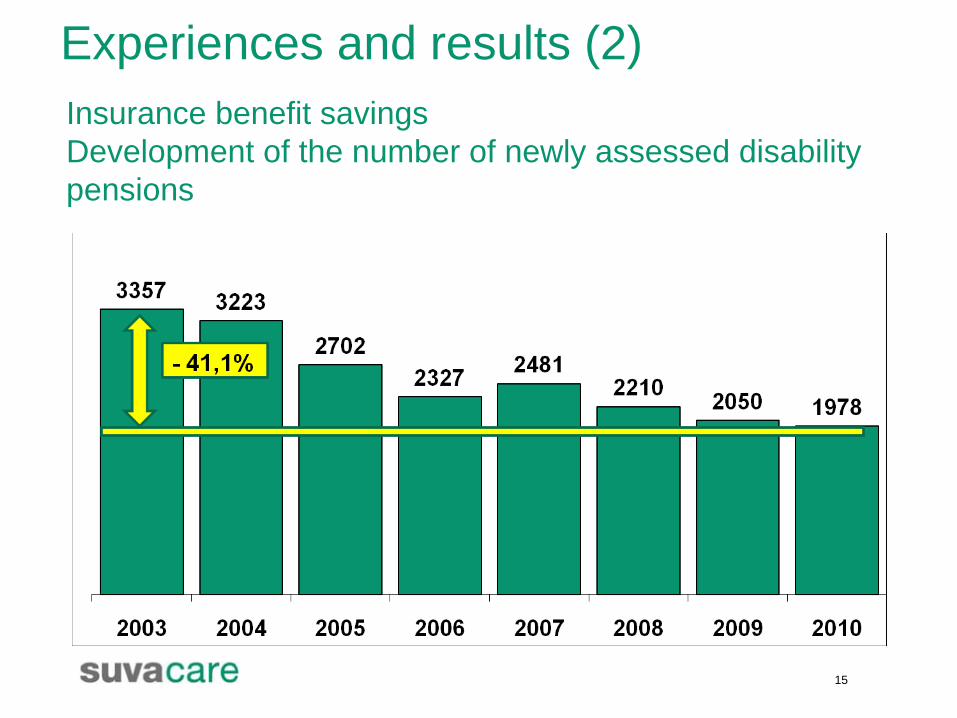
Experiences and results (2)
15
Insurance benefit savingsDevelopment of the number of newly assessed disability pensions
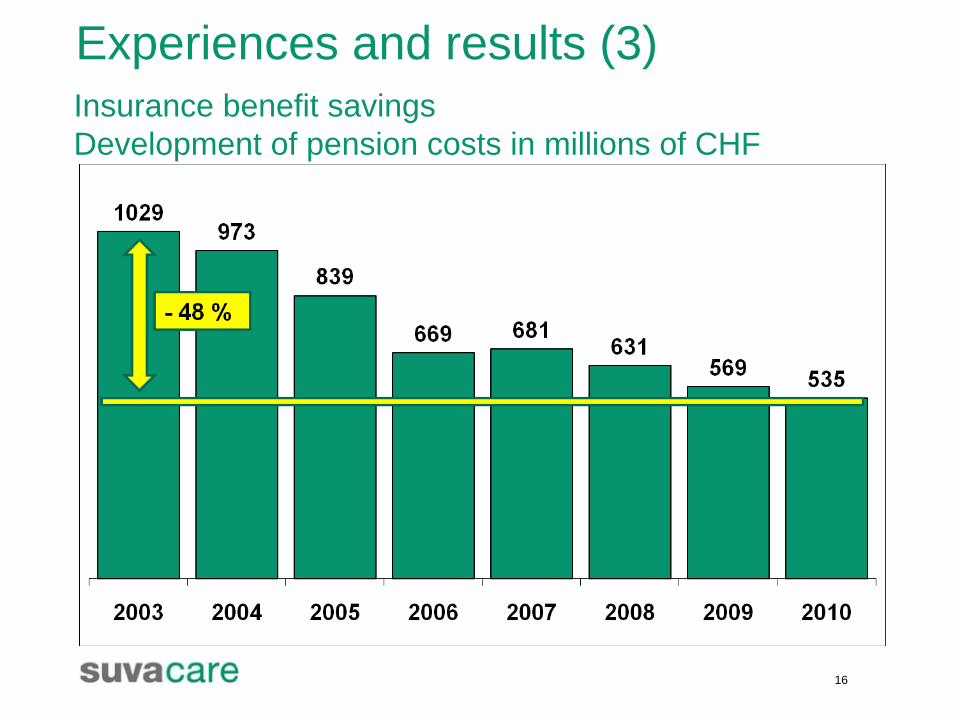
Experiences and results (3)
16
Insurance benefit savingsDevelopment of pension costs in millions of CHF

www.suva.ch
18
Factsheets• Das Schadenmanagement der Suva• New Case Management• Berufliche Reintegrationhttp://www.suva.ch/startseite-suva/service-suva/informationsmittel-suva/factsheets-unfall-suva.htm
• La gestion des cas de la Suva• New Case Management• Réintegration professionellehttp://www.suva.ch/fr/startseite-suva/service-suva/informationsmittel-suva/factsheets-unfall-suva.htm
• La gestione dei casi alla Suva• New case management• Reinserimento professionalehttp://www.suva.ch/it/startseite-suva/service-suva/informationsmittel-suva/factsheets-unfall-suva.htm
lic. oec. HSG Felix WeberMitglied der GeschäftsleitungSuvaCH 6002 Luzern, [email protected] www.suva.ch
Europäisches Forum der Versicherungen gegen Arbeitsunfälle und Berufskrankheiten Konferenz Dresden 21. - 22. Juni 2011
Rehabilitation and Return to Work
Beispiel eines kostendämpfenden Qualitätsprogramms in der Rehabilitation: Das Schadenmanagement der Suva
Abstract
Die Suva Die Suva (Schweizerische Unfallversicherungsanstalt) - eine selbständige öffentlich rechtliche Institution - ist die wichtigste Trägerin der obligatorischen Unfallversicherung in der Schweiz. Gut die Hälfte aller Arbeitnehmer der Schweiz (rund 2 Mio. Versicherte) sind bei ihr gegen die Folgen von Unfällen und Berufskrankheiten versichert. Die Suva wird von den Sozialpartnern geführt. Sie ist selbsttragend; sie erhält keine öffentlichen Gelder. Die Suva ist mehr als eine Versicherung: sie vereint Prävention, Versicherung und Rehabilitation (www.suva.ch). Jährlich melden die Betriebe rund 450 000 Unfälle und Berufskrankheiten der Suva. Dabei führen 70 % der Schadenfälle lediglich zu 5 % der Versicherungskosten. 2 % der gemeldeten Fälle hingegen verursachen fast zwei Drittel der gesamten Versicherungsleistungen. Es han-delt sich dabei um komplexe Unfälle mit einem schwierigen Heilungsverlauf. Schadenmanagement Ziel der Suva ist, Verunfallten und deren Arbeitgebern ein qualitativ hochstehendes, kunden-freundliches und wirtschaftliches Schadenmanagement zu bieten. Damit alle Beteiligten den grösstmöglichen Nutzen haben, bearbeitet die Suva die Schadenfälle in drei verschiedenen Fallkategorien: Standard-, Normal- und Komplexfälle. Als Standardfälle gelten Bagatellunfälle ohne Taggeldanspruch sowie Fälle mit kurzfristigem Taggeldanspruch. Bei dieser weit überwiegenden Anzahl der Fälle steht für die Kunden die Entschädigungsfrage im Vordergrund und eine Beratung ist kaum gewünscht. Diese Fälle werden aus wirtschaftlichen Überlegungen mit minimalstem administrativem Aufwand und möglichst automatisiert verarbeitet. Ein wirkungsvolles Schadenmanagement kann hier ohne-hin kaum angesetzt werden, da die Schadenmeldungen vielfach erst nach Wiederaufnahme der Arbeit bei der Suva eintreffen. Normalfälle sind Schadenfälle, bei denen versicherungsrechtliche Probleme zu klären sind, sowie Fälle mit einer Arbeitsunfähigkeit von mehr als acht Wochen, die zu keinen Schwierig-keiten bei der Wiedereingliederung führen und voraussichtlich ohne Dauerschaden abheilen. Durch die persönliche Betreuung der Verunfallten wird die Rückkehr an den angestammten Arbeitsplatz gefördert und Komplexfälle werden vermieden. Dies erfordert unter anderem ei-nen guten Kontakt zu den Arbeitgebern der Verunfallten. Primäre Ansprechpersonen bei Ver-sicherungsfragen sind die Suva-Sachbearbeitenden. Im Zentrum des Schadenmanagements stehen die Komplexfälle, d.h. Unfälle und Berufs-krankheiten mit erschwerter Wiedereingliederung. Ziel ist es, diese kostenintensiven Scha-denfälle so früh wie möglich zu erkennen, um schnell mit einer umfassenden und individuellen Beratung und Betreuung der Verunfallten hinsichtlich medizinischer, sozialer und beruflicher Reintegration beginnen zu können. Die Verunfallten werden in enger Zusammenarbeit mit den Case Managern, Komplexschadenspezialisten, Kreisärzten und den eigenen Rehabilitati-onskliniken der Suva betreut. Je nach Bedarf werden weitere Suva-Experten und externe Spezialisten (z. B. Stellenvermittler) beigezogen. Ausgesprochen wichtig ist auch die Koordi-nation mit anderen Versicherungen wie z. B. mit der Invalidenversicherung.
Schadenmanagement bringt Mehrwert Kostenzahlen und Kundenbefragungen zeigen, dass die Suva mit der Gliederung ihres Scha-denmanagements auf dem richtigen Weg ist. Es bringt sowohl den Verunfallten, deren Arbeit-gebern und der Suva Vorteile. Die Anzahl und die Kosten der Neurenten konnten in den letz-ten Jahren massiv gesenkt und die Zufriedenheit der Verunfallten und deren Arbeitgeber ge-steigert werden. Lic. oec. HSG Felix Weber Mitglied der Geschäftsleitung Leiter des Departementes Versicherungsleistungen und Rehabilitation
INFORMATION ABOUT ARP SURA ARP SURA: A Colombian Workers’ Compensation Insurance Company History Law 100 of 1993 and specifically the Law decree 1295 de 1994, were the
basis for the restructuring of the Workers’ Compensation System. Suramericana de Seguros decided then to become part of the Social
Security System in Colombia. Starting studies and later creating ARP SURA as a Workers’ Compensation Administrator.
Since 1996 until now, ARP SURA has been the leader among privates ARP’s. In order to guarantee its quality service ARP Sura has developed a quality system certified by ICONTEC under ISO 9001:2000.
The Business ARP SURA is a Worker Compensation Insurance Company (ARP),
subsidiary of SURAMERICANA. ARP SURA main function is to prevent, assist and protect all workers from
the effects caused by accidents or illnesses that may occur during the development of their work.
ARP SURA has 552 employees and 1.611.224 Affiliated Workers One main office located in Medellín.
Branches: Antioquia and Eje Cafetero: Offices in Medellín, Manizales and Pereira. Centro: Offices in Bogotá and Bucaramanga. Occidente Office in Cali. Norte: Offices in Barranquilla and Cartagena. Coverage in more than 1.000 cities and towns of Colombia

ARP SURA
MSD interventions in the Colombian Floriculture Sector - Practical application of
CUELA
Dr. Yanet Zapata Tamayo M.D.
Technical Manager
Prevention & Health Services
Dresden, June 2011
ARP SURA
AGENDA
• Current situation of Occupational Diseases in Colombia
• Integral approach: – How the problems were dealt with and what was the
contribution of CUELA in the overall approach
• Learning perspectives:– How to continue improving the knowledge acquired
and increase its impact
ARP SURA
CURRENT SITUATION

ARP SURA
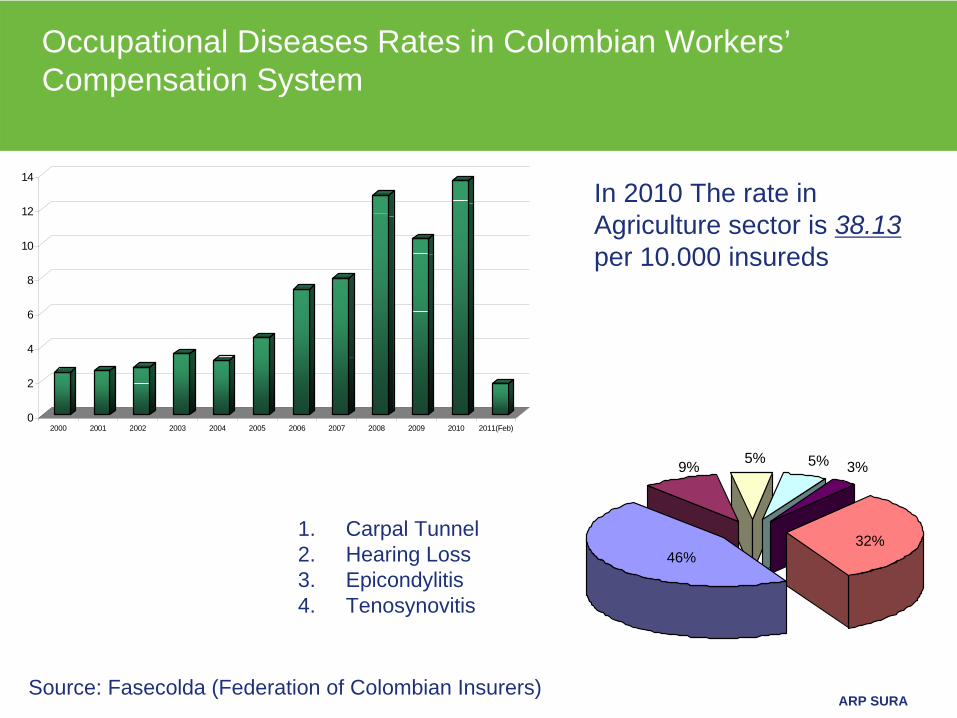
ARP SURA
Occupational Diseases Rates in Colombian Workers’ Compensation System
0
2
4
6
8
10
12
14
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011(Feb)
5% 5% 3%9%
46%32%
In 2010 The rate in Agriculture sector is 38.13 per 10.000 insureds
1. Carpal Tunnel2. Hearing Loss3. Epicondylitis4. Tenosynovitis
Source: Fasecolda (Federation of Colombian Insurers)

ARP SURA
INTEGRAL APPROACH

ARP SURA
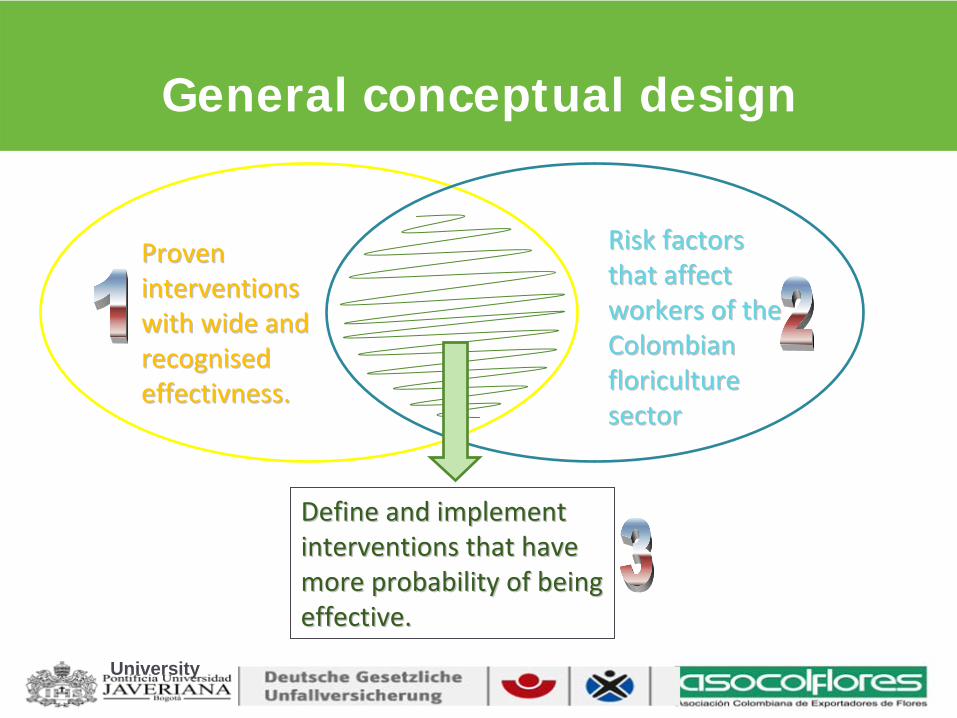
ARP SURA
General conceptual design
Proven Proven
interventions interventions
with wide and with wide and
recognised recognised
effectivness.effectivness.
Risk factors Risk factors
that affect that affect
workers of the workers of the
Colombian Colombian
floriculture floriculture
sectorsector
Define and implement Define and implement
interventions that have interventions that have
more probability of being more probability of being
effective.effective.
University
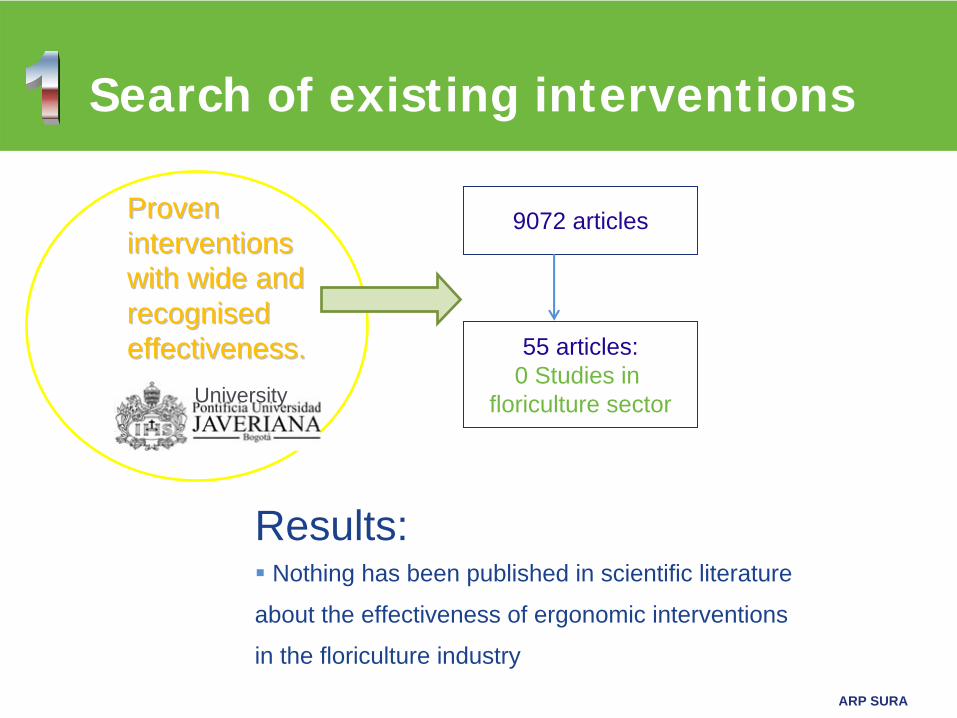
ARP SURA
Search of existing interventions
Proven Proven interventions interventions with wide and with wide and recognised recognised effectiveness.effectiveness.
9072 articles
55 articles:0 Studies in
floriculture sector
Results:
Nothing has been published in scientific literature
about the effectiveness of ergonomic interventions
in the floriculture industry
University
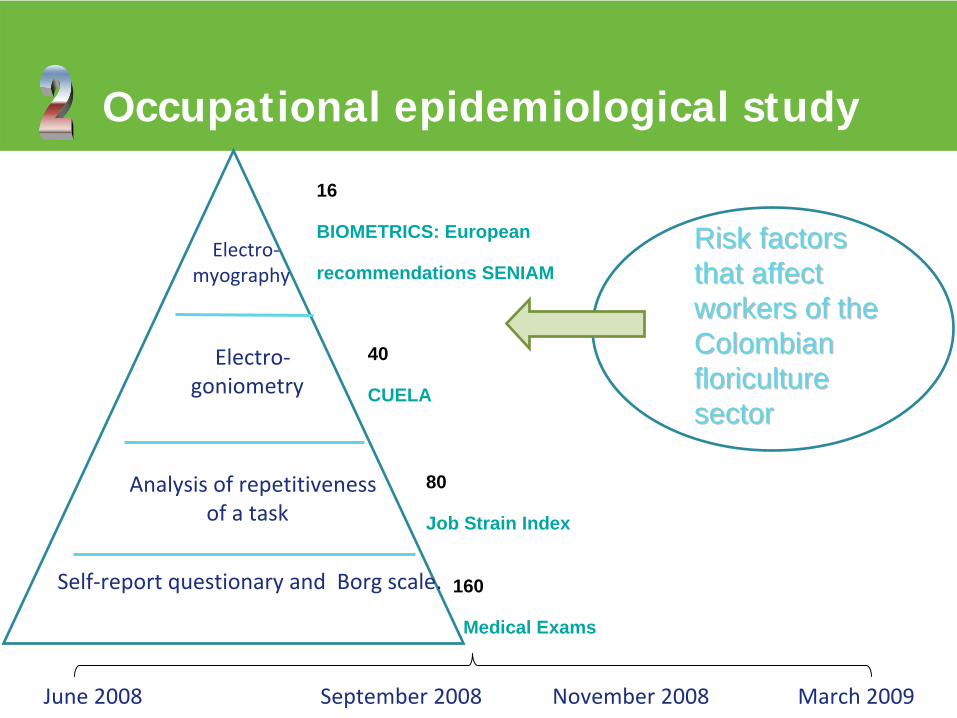
ARP SURA
Occupational epidemiological study
Risk factors Risk factors that affect that affect workers of the workers of the Colombian Colombian floriculture floriculture sector sector
Self‐report questionary and Borg scale.
Analysis of repetitiveness
of a task
Electro‐
goniometry
Electro‐myography
16
BIOMETRICS: European
recommendations SENIAM
40
CUELA
80
Job Strain Index
160
Medical Exams
June
2008 September 2008 November
2008 March
2009
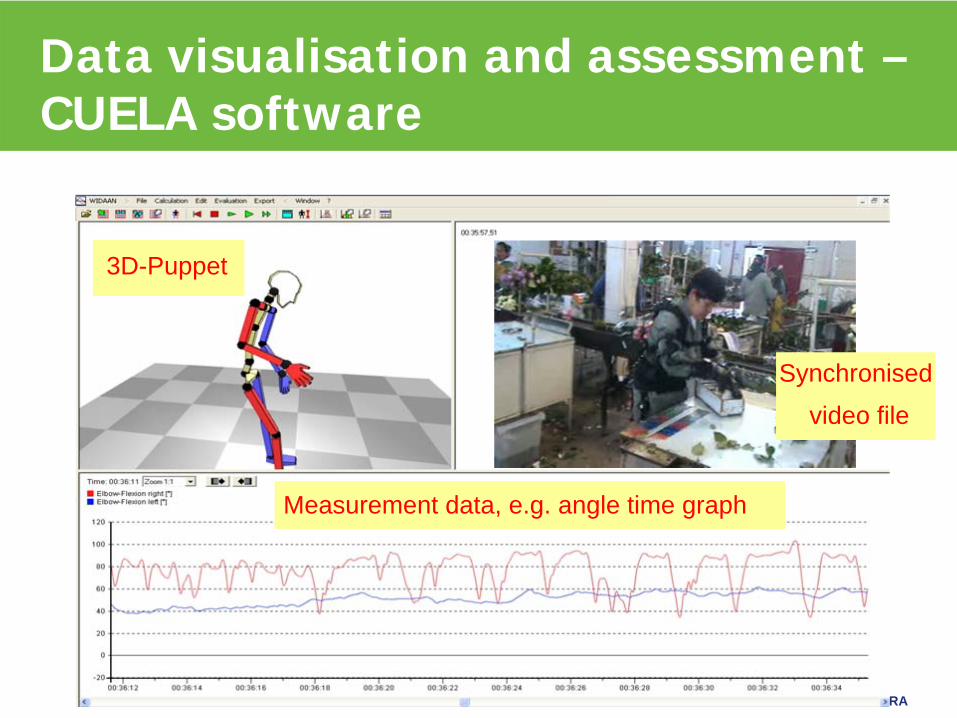
ARP SURA
Data visualisation and assessment – CUELA software
3D-Puppet
Synchronised
video file
Measurement data, e.g. angle time graph
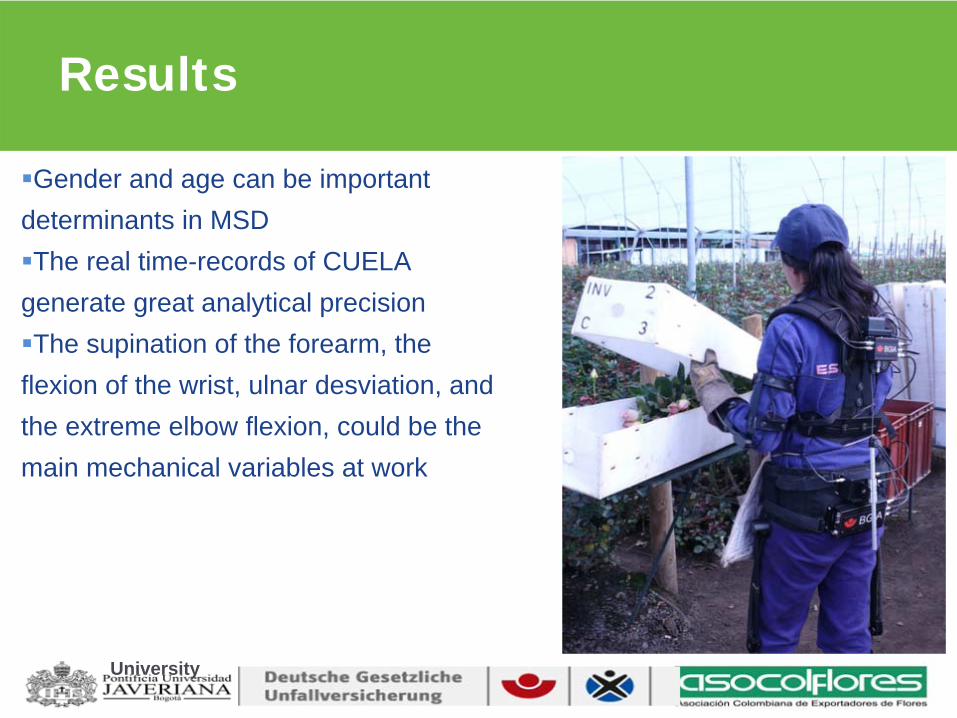
ARP SURA
Results
Gender and age can be important determinants in MSDThe real time-records of CUELA generate great analytical precisionThe supination of the forearm, the flexion of the wrist, ulnar desviation, and the extreme elbow flexion, could be the main mechanical variables at work
University
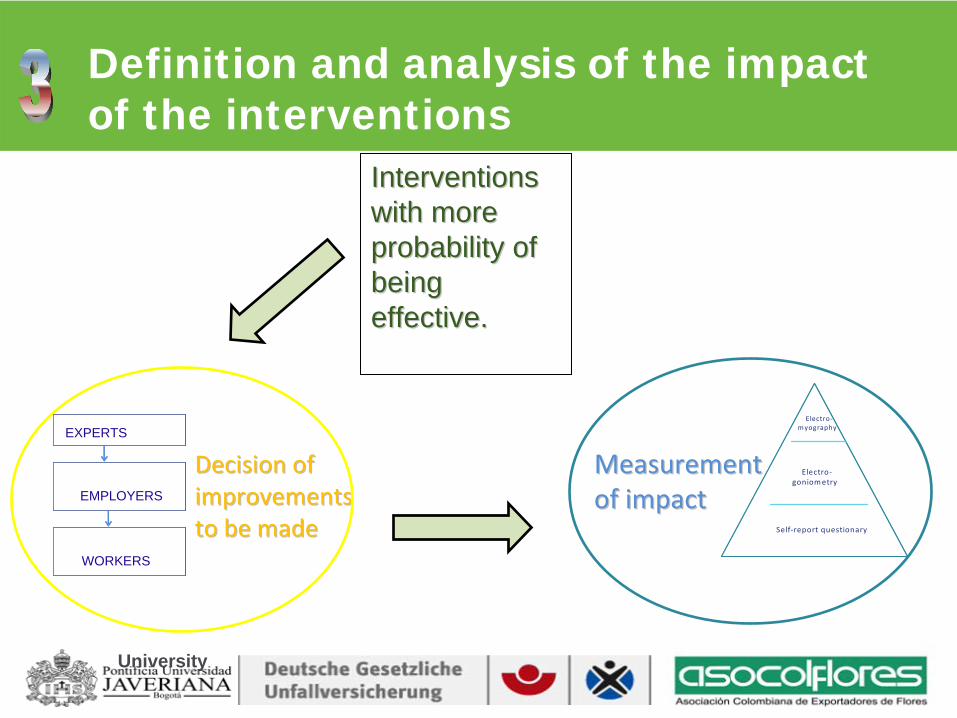
ARP SURA
Definition and analysis of the impact of the interventions
Interventions Interventions with more with more probability of probability of being being effective.effective.
Decision of Decision of
improvements improvements
to be madeto be made
Measurement Measurement of impactof impact
Taller de expertos
Revisión conempleadores
Implementación contrabajadores
EXPERTS
EMPLOYERS
WORKERS
University
Self‐report questionary
Electro‐goniometry
Electro‐myography
Self‐report questionary
Electro‐goniometry
Electro‐myography
ARP SURA
Results
The real-time records of CUELA generated great confidence therefore the companies will participate in the most complex areas of the sector
Postures change in critical activities (post harvest and “poncheo”) as well as improved maintenance of scissors demonstrated a reduction of the risk in the short term (3 months after the intervention)
Have the technology and specialized advice generated the confidence within the floricultor sector, and allowed the impruvements and the possibility to make changes
University
ARP SURA
LEARNING PERSPECTIVES

ARP SURA
ARP SURA
This study was the first experience in the floricultor sector, and is the base for others investigations and publicationsThis knowledge will be available to the sector throught of simples toolsThe experience will be replicated in other economic sectors with significant prevalence of these types of occupational diseases
The design of the investigation could be apply with other
countries in the region such as Chile and Argentina
How to continue improving the knowledge
acquired and increase its impact.