Embed Size (px)
Citation preview

THE RELATION OF SERUMBICARBONATECONCENTRATIONTOMUSCLECOMPOSITION1
By DANIEL C. DARROW,ROBERTSCHWARTZ,JOHN F. IANNUCCI,AND FRANCESCOVILLE
(From the Department of Pediatrics, Yale University School of Medicine, New Haven)
(Received for publication September 2, 1947)
Knowledge which enables one to predict thecomposition of intracellular as well as extra-cellular fluids is necessary for rational therapy ofdisturbances in body water and electrolyte. Thepresent paper shows that, when the kidneys reachadjustment in the presence of a deficit of sodiumor chloride or potassium, there is a predictable re-lationship between the concentration of bicar-bonate in serum and the composition of rat mus-cle. At present, treatment of acidosis is guidedchiefly by information that low concentration ofbicarbonate in serum is explained by an absoluteor relative deficiency of the sodium in extracellularfluids. Similarly, the therapy of alkalosis is basedon knowledge that relative or absolute deficiencyof chloride in extracellular fluids leads to high con-centration of bicarbonate in serum. Although thechanges in body electrolyte are not confined toextracellular electrolyte, knowledge of the quan-titative aspects of the changes in intracellular fluidsis just beginning to be developed. Darrow (1)has presented some of the known changes in com-position of intracellular and extracellular fluidsin a form which permits quantitative comparisonof the changes in the two chief categories of bodyfluid and has discussed some of the implicationsof these quantitative relationships. The presentpaper expands and defines these relationships atbiological equilibrium.
The experiments were designed to show thechanges in composition of both serum and musclewhich accompany certain types of deficit of po-tassium, in acidosis produced by deficit of sodiumand in alkalosis produced by deficit of chloride.In each type of experiment, the analyses presentthe compositions after the kidneys have reachedthe adjustment which is attained in the presenceof a deficit of one of the ions-sodium, chloride
1Aided by a Grant from the Fluid Research Fund,Yale University School of Medicine, New Haven.
or potassium-and are suitable to demonstrate therelation of the concentration of bicarbonate inserum to the composition of muscle.
EXPERIMENTALMETHODS
All experiments were carried out on white rats of bothsexes, weighing about 300 grams. Before being used inthe studies, the rats were fed Purina Fox Chow. Duringthe experimental period three diets were used. The lowpotassium diet was made up as follows: Lactalbumin 18,Crisco 22, Dextrin 32, Sucrose 25, cod liver oil 1, pow-dered yeast 2, bone ash 2, NaCl 1 gram. In additionto the above, the normal potassium diet had 2 gramsKH2PO,. The rats with acidosis received the same dietwithout bone ash or sodium chloride. The analyses ofthe diets are shown in Table I.
TABLE I
Composition of diets per 100 grams
Type of diet N C1 Na K
grams mM mM mMLow Cl 2.95 1 30 13Low Na 2.95 1 1 1Low K 2.95 17 34 1Normal 2.95 17 34 13
One group of rats was adrenalectomized and kept alivefor three to four days by administration of salt solutionuntil they had recovered from the effects of the operation.Other rats were subjected to similar dietary and experi-mental procedures except that no operation was per-formed. The experimental period of three weeks wasthen begun by giving them the synthetic diets, but theexperiments on the adrenalectomized rats were terminatedin two weeks, when the rats seemed unlikely to survive.
During the experimental period the rats were sub-divided into groups of four, which received daily subcu-taneous injections of desoxycorticosterone acetate, desoxy-corticosterone acetate in conjunction with cortical extract,cortical extract or no hormones, as is indicated in TableII. The desoxycorticosterone acetate . was prepared so
that about 2 mg. were given in 1 cc. of a suspension ofcrystals. The cortical extract was Upjohn's lipo-extractwhich contains 40 rat growth-survival units per cubiccentimeter and is equivalent per cubic centimeter to 2
198

RELATION OF SERUMBICARBONATETO MUSCLECOMPOSITION19
TABLE II
Adre- Muscle composition per 100 grams fat-free solids Serum concentrations per literGroup Rat Pe- Diet* Injec- nal ______ __-_____-__
No.N~riod tion ctomyFat HiOj N Cl Na KJP (Na)i HsOJHCO:S Cl Na K pH PCOs
13daysI
N
3 21 1 N
4
4
2
4
4
4
3
3
3
3
5
4
211 N
21 1 N
21 LK(
21 1 LK
21 1 LK
21 1 LK
0
CE
D
DCE
0
CE
D
DCE,
14 LK IO0
14 LK CE
14 LK D
14 LK
2
6
DCEJ
LNaI 0
LCI 0
0
0
0
0
0
0
0
0
0
0
* N = Normal diet.
LK = Low potassium diet.
grams
3.00.8
4.11.0
3.01.1
11.81.3
8.11.0
7.91.0
11.50.6
11.8
6.51.9
11.3
grams340
6
3433
3253
3268
31424
3275
3268
3349
350
3358
3314
6.8 338
1.3 4
11.0
1.0
341
5
337
6
grams15.3
0.3
14.20.2
14.00.3
13.20.4
15.30.1
15.00.3
15.00.2
15.60.4
16.6
15.60.8
15.70.4
15.70.3
14.10.1
14.70.1
mm7.1i0.5
5.70.2
5.40.2
5.70.3
5.60.5
5.50.7
5.50.3
5.60.3
6.6
5.70.3
4.50.9
6.00.6
4.90.2
5.00.41
mm10.0
0.6
8.80.4
14.90.8
16.61.4
8.50.2
11.40.4
19.81.0
18.51.2
10.9
15.91.0
20.82.1
20.92.6
6.60.3
15.20.6
mm48.9
0.6
46.40.5
36.31.7
35.51.4
39.90.6
43.60.5
34.01.1
34.31.1
46.9
33.53.3
34.42.3
33.51.4
49.51.0
38.22.01
mm32.4
1.5
31.70.2
30.40.8
30.10.9
31.50.5
28.01.8
26.50.9
31.30.5
32.9
26.60.5
30.40.7
30.31.0
33.70.4
31.70.8
mm3.1
3.40.4
8.70. 7
9.81.3
6.70.8
5.90.9
13.21.6
13.10.6
4.1
9.40.9
15.72.6
13.81.0
1.30.6
9.50.6
LNa = Low sodium diet.
LCl = Low chloride diet.
grams933
S
9358
9302
9324
9283
9432
9368
9398
9446
9463
9432
9433
9102
9351
mm20.9
2.4
22.01.5
30.22.0
30.02.4
30.31.0
26.31.4
38.14.0
40.02.5
22.11.0
31.64.0
39.21.2
38.22.2
14.62.3
32.84.0
mm102.6
0.6
108.82.6
92.14.5
97.44.7
94.05.0
100.81.2
85.32.4
86.04.0
99.95.9
96.43.9
88.35.5
93.03.2
93.62.4
79.52.1
mm143
2.9
1382.7
1444.4
1471
147.51.5
1382.5
1411.7
1436
1344.8
1452.6
1392.9
1431.4
138.82.5
142.70.51
.mm5.40.3
7.20.6
7.81.3
5.00.2
5. 10.03
6.60.3
5.81.2
5.10.3
7.40.5
4.41.9
6.11.5
6.52.5
6.80.5
4.30.6
7.280.03
7.230.03
7.430.02
7.480.03
7.440.03
7.320.06
7.340.02
7.400.08
7.430.03
CE = Adrenal cortical extract.
D = Desoxycorticosterone acetate.
mg. compound E or 4 mg. of corticosterone. The daily
dose of extract was 0.1 cc.
Acidosis was produced in rats by injecting into the
peritoneal cavity a 5 per cent solution of glucose contain-
ing about 60 mMof NH4C1 per liter. About 100 cc. per
kilogram of rat were injected and the fluid remaining
after four hours was removed through a small abdominal
incision. The rats were kept on the synthetic diet with-
out added bone ash or sodium chloride for two days.
This procedure removed about 10 mMof sodium and 5
mMof chloride per kilogram of rat and at the end of
the experiments the serum concentration of bicarbonate
varied from 11 to 18 mMper liter. The details of the
acidosis experiments are recorded in the thesis of Robert
Schwartz (2).
The alkalosis experiments were reported previously as
Group 4 (3) and are represented in the present paper as
Group 14. In these experiments a glucose solution con-
taining 150 mMof NaHCOaper liter was injected into
the peritoneal cavity and withdrawn after four hours.
The rats were permitted to survive on a diet deficient
only in chloride for six days.
At the end of the experimental period, the rats were
anesthetized with ether, and as much blood as possible
was withdrawn from the abdominal aorta by inserting a
needle attached to a syringe containing mineral oil. The
rats were then immediately killed by excising the heart.
The muscles of the legs were removed, freed from exces-
sive amounts of fat and nerves, and analyzed by the
methods used previously in this laboratory (4). The
estimation of pH was done with a glass electrode at
380 C. The determinations of pH were carried out on
1
2
3
4
5
6
7
8
9
10
11
12
13
14
MM.Hg44
48
37
52
59
44
60
60
62
199

200 DANIEL C. DARROW,ROBERTSCHWARTZ,JOHN F. IANNUCCI, AND FRANCESCOVILLE
serum, when sufficient blood was obtained. Unfortunately,the pH was not estimated in the later experiments, be-cause the apparatus was out of order.
Four rats were started in each experimental group, butin some groups one rat died or blood was not obtainedin sufficient quantity. Some groups are, therefore, rep-resented by analyses of only two or three animals. TableII shows the average + the standard deviation. Atten-tion is directed to the fact that the muscle analyses arecalculated per 100 grams of fat-free solids. This methodof presentation (3) was used because the fat-free solidsare chiefly intracellular and hence the values for intra-cellular constituents are practically unaffected by changesin the volume of extracellular water. Furthermore, thedata show no close relation of the volume of intracellularwater or the concentration of intracellular electrolyte tothe concentration of extracellular sodium. Hence thechanges in intracellular electrolyte are most simply rep-resented in terms of fat-free solids.
The intracellular sodium was calculated as follows:
(CDl- = (H20).
(Na) - (H20).[Na]. = (Na)i
in which (Cl) and (Na) are total tissue chloride andsodium per 100 grams of fat-free solids; (H2O), is theextracellular water per 100 grams of fat-free solids;(Na), is the intracellular sodium per 100 grams of fat-free solids. [Cl] e and [Na]. are the concentration ofchloride and sodium in an ultrafiltrate of serum calcu-lated from the serum concentrations and the serum waterand an average Donnan factor of 0.96. In the first equa-tion the 1 represents an average correction for non-extracellular chloride (4).
RESULTS
As shown in Group 1, the usual value for themuscle potassium of normal rats on a normal dietis 49 mMper 100 grams of fat-free solids. Thestandard deviation is somewhat deceiving, sinceMiller and Darrow (5) found that essentiallynormal rats may show values as low as 44 mM,but potassium in muscle probably does not go be-low this figure in normal rats. In adrenalecto-mized rats muscle potassium is 52, when the ratsare fed a diet of the usual salt content (6). There-fore the two different sets of values for normaland adrenalectomized rats should be used in de-termining changes in muscle composition broughtabout by either the diet or the injections of corticalextract or desoxycorticosterone acetate.
The results in unoperated rats fed the normaldiet are shown in Groups 1 through 4. The in-jection of cortical extract (Group 2) did not
change the muscle composition unmistakablythough the concentration of chloride in serum isa little high (109 mMper liter). However,- theinjection of desoxycorticosterone acetate aloneor in conjunction with cortical extract (Groups3 and 4) lowered the muscle potassium to 36 mMper 100 grams of fat-free solids and increased theintracellular sodium to about 9 mMper 100 gramsof fat-free solids. The decrease in muscle potas-sium and the increase in intracellular sodium fol-lowing injections of desoxycorticosterone ace-tate have been previously demonstrated (5, 7to 9). The present experiments show that themuscle changes are accompanied by an increasein concentration of bicarbonate in serum to 30 mMper liter. The rise in serum bicarbonate wasmissed in the previous work since this determina-tion was omitted. However, the previous workshowed a decrease in serum chloride and normalor high serum sodium. These findings almostcertainly indicate that high concentration of bi-carbonate in serum could have been demonstrated.
The results on unoperated rats fed a diet low inpotassium are shown in Groups 5 through 8.Group 5 shows that diets low in potassium de-crease muscle potassium to 40 and increase intra-cellular sodium to 6.7 mMper 100 grams offat-free solids. Accompanying the changes in mus-cle, the concentration of bicarbonate in serum in-creased to 30 mMper liter and the concentrationof chloride in serum decreased to 94 mMper liter.Though less marked, these changes are similar tothose produced by injections of desoxycortico-sterone acetate in rats fed a normal diet. The in-jection of cortical extract in rats fed a diet lowin potassium (Group 6) was. not followed by asgreat a lowering of muscle potassium or as greata rise in serum bicarbonate. However, the in-jection of desoxycorticosterone acetate alone or inconjunction with cortical extract (Groups 7 and8) decreased muscle potassium to 34 and in-creased intracellular sodium to 13 mMper 100grams of fat-free solids. The most striking changein these groups is the increase in serum bicarbon-ate to about 39 mMper liter and the reduction ofserum chloride to about 85 mMper liter.
Groups 9 through 12 show the results in ad-renalectomized rats on a diet low in potassium.If one recalls that a diet of normal potassium con-

RELATION OF SERUMBICARBONATETO MUSCLECOMPOSITION
tent is likely to produce high muscle potassium andmay lead to early death, the diet low in potas-sium (Group 9) did produce an effect in pre-serving muscle composition at approximately nor-
mal concentrations. However, serum sodium isdefinitely low despite normal bicarbonate andchloride. The adrenalectomized rats receivingcortical extract (Group 10) were more vigorousthan the untreated ones of Group 9. It is, there-fore, interesting to observe that the muscle com-
position is more abnormal in Group 10. The po-
tassium is as much reduced as in normal rats on a
normal diet receiving desoxycorticosterone acetate(Groups 3 and 4) or the normal rats on a diet lowin potassium receiving desoxycorticosterone acetate(Groups 7 and 8). Accompanying the change inmuscle composition, serum bicarbonate is 32, serum
chloride 96, and serum sodium 145 mMper liter.While the cortical extract did not produce com-
pletely normal functions in the adrenalectomizedrats, the changes demonstrated are of the same
type as was seen in- normal rats on a diet low inpotassium. For this reason, the dose of corticalextract is adequate to produce an effect in animalsproducing no cortical hormone, i.e., the dose isadequate to produce an effect in adrenalectomizedrats. The injections of desoxycorticosterone ace-
tate alone or in conjunction with cortical extract(Groups 11 and 12) probably produce essentiallythe same effect in adrenalectomized rats as thesame injections in normal rats (Groups 3, 4, 7and 8). The higher value for intracellular so-
dium in Group 11 is dependent on the one aber-rant intracellular sodium mentioned later. Thelowering of muscle potassium and increase inserum bicarbonate are striking in these two groups.
The rats suffering from acidosis (Group 13)show changes in muscle composition which fit inwith the above findings. Lowering of serum bi-carbonate decreased the intracellular sodium whilemuscle potassium remained normal or slightlyhigh.
The rats suffering from alkalosis produced bydeficit of chloride (Group 14) resemble the rats on
a diet deficient in potassium or receiving desoxy-corticosterone acetate. Muscle potassium is 38 andthe intracellular sodium is 9.5 mMper 100 grams
of fat-free solids. The serum bicarbonate andchloride were 33 and 80 mMper liter.
The data have been analyzed for relationshipsbetween the concentration of serum sodium andthe total intracellular water per 100 grams of fat-free solids and the apparent concentration of so-dium plus potassium in intracellular water. Al-though there are striking variations in these twovalues, no correlation is found with the concentra-tion of sodium in serum. In acute experiments adecrease in concentration of sodium in serum leadsto an increase in intracellular water and a decreasein the concentration of univalent cations in intra-cellular water (4). In the present experiments inwhich the rats have reached a biological equilib-rium no such relationship is found. The lack ofcorrelation between the concentration of sodium inserum and the concentration of univalent cationsin intracellular water is supported by findings inpatients and experimental animals (10).
There are striking decreases in muscle phos-phorus in Groups 6, 7 and 10, and somewhatsmaller decreases in some other groups. These.changes are not associated consistently with anytype of change in the serum or other constituentsof the muscle. Since the values for muscle phos-phorus include all muscle phosphorus, studies of
TABLE III
Statistical data on relationships of serumand muscle compositions
Average and standarddeviation Correlation coefficients
(K) mM 40.22-6.21 (K) (Na)i -0.90(Na)i mM 7.91i4.48 (K) (HCO), -0.90(HCOM ). mM 28.6548.04 (K) (Cl) 0.47(Cl), mM 94.3948.10 (Na)i (HCOs)s 0.94
(Nai (CGi -0.57(HCO). (Cl), -0.59
(K) is total muscle potassium and (Na)i is intracellularmuscle sodium per 100 grams of fat-free solids. (HCOS).and (Cl). are the respective concentrations per liter ofserum.
Regression equations cakulated from Table III(K) = 50.1 - 1.25 (Na)i 4 2.7(Na)i = 34.0 - 0.65 (K) i 1.9
(K) = 60.1 - 0.696 (HCO)), 2.7(HCO,), = 75.6 - 1.165 (K) 4 3.5
(K) = 0.36 (Cl), + 6.0 4 5.5(Cl). = 0.61 (K) + 68.7 4 7.1
(Na)i = 0.52 (HCO3)s - 7.1 1.5(HCO3), =. 1.69 (Na)j + 15.3 4 2.6
(Na)1 = 37.7 - 0.32 (Cl). ± 3.6(Cl), = 102.5 - 1.026 (Na)i h 6.6
(Cl), = 111.4 - 0.59 (HCOs), i 3.4(HCO)s = 93.9 - 0.59 (Cl). i 3.4
201

202 DANIEL C. DARROW,ROBERTSCHWARTZ,JOHN F. IANNUCCI, AND FRANCESCOVILLE
Serum HC03 mMper L
40
35
i30
25
20
15
1030 35 40 45 50 55 0 5 10 IS 20
Km M per 100 gm F F Solids [No]I mMper 100 gm FF Solids
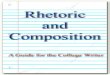
FIG. 1. RELATION OF THE CONCENTRATIONOF BICARBONATE IN SERUMTOTHE TOTAL POTASSIUMAND INTRACELLULAR SODIUM OF RAT MUSCLEPER 100GRAMSOF FAT-FREE SOLIDS
the various types of compounds might throw lighton the decreases in total phosphorus.
Table III shows the correlation coefficients ofcertain values of the serum and muscle. The chiefinterest is the interrelationship between serum bi-carbonate, muscle potassium 2 and intracellularsodium which are defined in the regression equa-tions and illustrated in Figures 1 and 2. The cor-relations between serum chloride and serum bi-carbonate, serum chloride and muscle potassium,and serum chloride and intracellular sodium aredefinite, but not as precise as the correlations be-tween serum bicarbonate and intracellular cations.For this reason the fundamental correlation of in-tracellular cations and serum concentrations isregarded as dependent on serum bicarbonate ratherthan serum chloride. The relation of muscle po-tassium and intracellular sodium to serum chlorideis secondary relationship dependent on the in-verse relationship between serum chloride andserum bicarbonate.
2 It is realized that equilibrium would be theoreticallymore accurately stated in terms of intracellular potas-sium. Since the correction for extracellular potassium issmall and approximately the same in all groups, the totalmuscle potassium was used.
As is indicated by the correlation coefficients,there are few aberrant values. In the largest de-viation (one of the values in Group 11), the in-tracellular sodium is 19 mm. per 100 grams offat-free solids, when the serum bicarbonate wouldpredict a value of 14. In this case muscle po-tassium is essentially that predicted by serum bi-carbonate. Either the determination of musclesodium or chloride is erroneous in this case or oc-casional values deviate considerably from thepredicted value. With this exception, the con-centration of serum bicarbonate predicts the com-position of muscle with respect to potassium andintracellular sodium with surprising accuracy inthis series of animals. The values for the rats withacidosis fall along the lines. More values in thegroup with acidosis might bring out a resistanceto lowering of intracellular sodium below 1 mm.per 100 grams of fat-free solids. Previous workhas indicated that muscle potassium seldom risesover 50 mm. per 100 grams of fat-free solids ex-cept when serum potassium is increased (5, 7).For this reason acidosis may not lead to greatincrease in muscle potassium unless serum po-tassium rises. Doubtless other variables are in-volved in the relationship between intracellular

RELATION OF SERUMBICARBONATETO, MUSCLECOMPOSITION
50
"45 ;
E>e40
0
06
(3)5
E450
25. . X5 10 15 20
i mM per 100 gm F F SolidsFIG. 2. RELATION OF TOTAL POTASSIUM TO JNTRA-
CELLULAR SODIUM IN RAT MUSCLEPER 100 GRAMSOFFAT-FREE SOLIDS
composition and serum concentrations, but theconcentration of bicarbonate in serum is one ofthe most important factors.
Normal serum bicarbonate is 21 mm. per literand the pH is 7.28 when the blood is taken as inthese experiments. Owing to the fact that the ratswere anesthetized and bled from the abdominalaorta after opening the abdomen, the pH and car-bon d ioxide tensions are probably unreliable asmeasurements of undisturbed animals. It will benoticed that the carbon dioxide pressures are highin the cases with high concentration of bicarbonatein serum. Since the carbon dioxide pressure isrelatively normal in the rats with normal concen-trations of bicarbonate in serum, the increase incarbon dioxide pressure in the rats with highserum bicarbonate is evidence of some respiratorycompensation, but not sufficient to produce thesame pH as was obtained in the normal group.
Sections of the heart were examined for thelesions associated with low muscle potassium.There was no striking difference in the extent ofthe lesions except as associated with loss of muscle
potassium. In this respect the normal and adren-alectomized rats are alike. These observationswere made because heart symptoms have seemedunduly prominent in cases of Addison's diseasetreated with desoxycorticosterone acetate. It wasfelt that cortical extract might provide some pro-tection from the lesions produced by desoxycorti-costerone acetate, but the histological sections donot support this supposition. Since the intakeof sodium chloride was about the same in theseexperiments, this finding is in agreement withrecent work which indicates that renal and heartlesions require the combined effect of sodiumchloride and desoxycorticosterone acetate (11).
DISCUSSION
The experimental demonstrations of the cor-relation between the serum bicarbonate, musclepotassium and intracellular sodium have been ob-tained by four methods of producing changeseither in the serum or muscle. First the diets lowin potassium produce loss of potassium from thecells owing to inability of the kidneys to preventloss of potassium when the diets contain little po-tassium and considerable sodium chloride. Theimportance of sodium chloride was brought outin unpublished observations on rats fed a diet sim-ilar to the low potassium diet of the present ex-periments except that no sodium chloride wasadded. This diet did not produce striking changein muscle composition or serum bicarbonate.Second, desoxycorticosterone acetate augments theexcretion of potassium so that deficit of musclepotassium develops on normal diets. Desoxy-corticosterone acetate also aggravates the effectof diets low in potassium. Third, the experimentspreviously published (3) produced alkalosis byinjecting sodium bicarbonate in 5 per cent glu-cose into the peritoneal cavity. If a diet deficientin chloride was given for six days after removingthe fluid equilibrated in the peritoneal cavity, themuscles lost potassium and gained intracellular
-sodium, and the concentration of bicarbonate inserum remained high. Fourth, acidosis pro-duced by deficit of sodium induced the oppositeeffect on muscle. Thus, it seems clear thatthere is a biological equilibrium or biologicalsteady state in which these three variables bearpredictable relationships to each other, when renal
203

204 DANIEL C. DARROW,ROBERTSCHWARTZ,JOHN F. IANNUCCI, AND FRANCESCOVILLE
function is carried out in the presence of deficit ofone of the ions-sodium, chloride or potassium.The biological equilibrium may be initiated eitherby a primary change in serum bicarbonate or mus-cle potassium and is the same in normal andadrenalectomized rats.
The equilibrium must be regarded as biologicalrather than chemical because of the relatively longtime required to reach the relationships. Afteran interval of four hours, Hastings and Eichel-berger (12) found increase in cell water, but didnot measure intracellular base in their experi-ments on alkalosis. Yannet (13) did not findshifts of electrolyte in cats with alkalosis after aninterval of about 24 hours. Flexner and others(14) found equal distribution of deuterium oxideand radioactive isotopes of sodium and potassiummuch more rapidly.
Whatever the mechanism for bringing about theeffect of serum bicarbonate on the composition ofcells, the relationships must be maintained and lim-ited by the ability of the kidneys to regulate ex-tracellular concentrations. The development ofpotassium deficit on a diet low in potassium canbe explained by the fact that urine is never com-pletely devoid of potassium. When potassium islost from the cells, it is not difficult to understandthat sodium replaces the lost cation. However, itis not easy to understand why this change is ac-companied by high bicarbonate and low chloridein the serum. It would seem that, if the mainten-ance of extracellular concentrations were the chiefrenal function, the kidneys could maintain normalextracellular concentrations. The effect of des-oxycorticosterone acetate is brought about by achange in the excretion of sodium and potassiumby the kidneys and the end result is analogous tothe effect of diets low in potassium. When highserum bicarbonate was produced by deficit ofchloride, it is clear that extracellular concentra-tions and volumes cannot both be restored with-out replacement of chloride, but it is not easy toexplain why these changes in extracellular con-centrations lead to loss of potassium and retentionof sodium in the cells. Since cell membranes areconsidered permeable to sodium and potassium,high bicarbonate in serum must either facilitate thetransfer of potassium out of the cells or increasethe entrance of sodium. The other possible ex-planation would be that alkalosis increases the rate
of potassium excretion. This explanation is un-likely, since the change in the cells takes placein the presence of abundant potassium in thediet. We are forced to conclude that the threevariables are dependent and tend to adjust one toanother so as to preserve the relationships ex-hibited in the regression equations and Figures1 and 2.
There is considerable evidence that this biologi-cal equilibrium is exhibited by patients. In thecases of Cushing's syndrome with high serum bi-carbonate, low chloride and low potassium (15,16), the alkalosis responded to potassium chlo-ride but not sodium chloride or ammonium chlo-ride. Power and Kepler (17) found low potas-sium and high sodium in muscle taken at biopsyfrom one of these cases. Furthermore, the anal-ogy with the effects of desoxycorticosterone ace-tate is supported by the fact that the alkalosis dis-appeared when an adrenal cortical tumor wasremoved and recurred when metastatic growths de-veloped. The present data provide an explanationof the persistent alkalosis in cases of Cushing'ssyndrome-developing deficit of potassium.
Observations have shown that the alkalosis ofvomiting is sometimes accompanied by low con-centration of potassium in serum (18). One ofthe authors has observed one case of gastric tetanywhich persisted despite administration of abundantamounts of physiological saline. He also has ob-served a balance of sodium, potassium and chlorideduring recovery from dehydration following vom-iting that indicated the presence of a large amountof intracellular sodium and a deficit of potassium.If these evidences of changes in cell composition ingastric alkalosis can be confirmed, gastric alka-losis must be considered'to lead to deficit of po-tassium and excessive retention of sodium in thecells, and treatment of these disturbances withpotassium chloride as well as sodium chloride islikely to prove as advantageous as the introduc-tion of potassium chloride in the treatment of diar-rhea (19, 20).
The observation of persistent high serum bi-carbonate in certain lung diseases is also probablyaccompanied by the characteristic changes in thecells. Darrow and Sarason found high intracellularsodium and low potassium in rats subjected to lowatmospheric pressure for seven days (21). Al-though the authors did not attribute the change in

205RELATION OF SERUMBICARBONATETO MUSCLECOMPOSITION
muscle composition to alkalosis, nor measure theserum bicarbonate, it is likely that compensatedrespiratory alkalosis explains the change.
The first evidence of the dependence of tissuecomposition on serum bicarbonate was recognizedin a case of "congenital alkalosis with diarrhea"(22). In this patient the stools were always vol-uminous and watery and contained more chloridethan sodium. As the boy developed' more alka-losis, potassium in excess of nitrogen was lost inthe stools or urine, and sodium was retained inthe cells. During recovery from profound alka-losis, administration of potassium chloride facili-tated partial restoration of serum bicarbonate;the retentions of electrolyte indicated that largeamounts of sodium left the cells as potassium was
retained, but potassium and sodium chloride were
unable entirely to overcome the alkalosis. Theauthor felt that the excessive loss of chloride inthe stools was the fundamental difficulty. Instudying a similar case, Gamble and others (23)postulated that there might be a fundamental diffi-culty in which the body adjusted preferentially toalkalosis. The present study makes this hypothe-sis tenable, if one could prove that the muscles andperhaps all tissues preferentially contained ex-
cessive amounts of intracellular sodium. Such a
disturbance in intracellular composition is more
difficult for one of the authors to visualize than a
peculiar defect in intestinal absorption leadingto alkalosis. In any case, the demonstration ofthe dependent relationship between alkalosis andmuscle composition explains the excretion of po-tassium in the urine despite a deficit of muscle po-tassium. It also explains the therapeutic failure
of acid salts and the refractoriness of the cases toall forms of treatment.
It must be kept in mind that the relationshipsunder discussion may be expected to be found onlywhen renal function has made the appropriate ad-justment. Thus, we know that there are varia-tions in one or more of the variables without thepredicted changes in the others, when there is de-hydration. One may be permitted to call thesetypes of disorders unstable states with respect tothe relationship between the composition of intra-cellular and extracellular fluids. For instance, thestudies on diarrhea (19) show that this type ofacidosis and dehydration is practically always ac-
companied by a considerable deficit of potassium,
but intracellular sodium may be low or high. Theregression equations predict high muscle potas-sium and low intracellular sodium in acidosis.The low intracellular sodium is contrary to theexpectation of high intracellular sodium accom-panying loss of muscle potassium. The high in-tracellular sodium is predicted by the potassiumloss, but is contrary to the prediction from lowserum bicarbonate. Diabetic coma (24, 25, 26)probably shows similar changes in the cells ac-companying acidosis and in this sense also ex-hibits an unstable state in the relationship betweenextracellular fluids and tissue composition.
One may speculate that the lack of a relativelystable equilibrium in these usually dependent vari-ables explains some of the findings in these cases.It is obvious that deficit of potassium explains thelarge doses of sodium bicarbonate necessary toovercome acidosis if sodium chloride and sodiumbicarbonate are administered without potassium.It is not so clear how acidosis and dehydrationrapidly become manifest in some cases. The au-thors have in mind babies with diarrhea who sud-denly manifest marked symptoms of acidosis. anddehydration despite no increase in watery stools.In these cases, if deficit of potassium developsgradually and intracellular sodium remains low ornormal, an unstable state develops. Under thesecircumstances, acidosis and dehydration of ex-tracellular fluids could suddenly be aggravated ifsodium were rapidly transferred to the cells in con-sequence of the unstable state. If the transfer ofsodium is equivalent to 5 per cent of the intra-cellular potassium, the decrease in extracellularsodium would be equivalent to one-half of thenormal extracellular bicarbonate or one-tenthof the normal extracellular sodium. Since the ex-tracellular fluids are already depleted in a patientwith diarrhea, a very small shift in sodium wouldproduce a marked aggravation of extracellulardehydration and acidosis.
On the other hand, the relationship of musclecomposition to serum bicarbonate must be con-sidered in treating disturbances in body electrolytefrom the point of view of the ultimate equilibriumdependent on the tissue deficit. In diarrhea andprobably also in diabetic coma (24, 25, 26), ifrestoration of serum bicarbonate becomes the chiefcriterion of successful treatment, biological equi-librium will not be obtained with a normal serum

206 DANIEL C. DARROW,ROBERTSCHWARTZ,JOHN F. IANNUCCI, AND FRANCESCOVILLE
bicarbonate, but with a high serum bicarbonate ifdeficit of potassium is not restored. For instance,a rat with a muscle potassium of 30 mMper 100grams of fat-free solids (about two-thirds of nor-mal figure) is in a biological state of equilibriumwhen serum bicarbonate is 40 mMper liter andintracellular sodium is 14 mMper 100 grams offat-free solids. If a baby behaves like a rat in thisrespect, the sodium in the muscle cells would beabout 14 mMper kilogram of body weight. Thisamount of intracellular sodium would be about threetimes the normal value and would be equivalentto over twice the normal amount of bicarbonate inextracellular fluids. Looking at the state of equi-librium from the point of view of the serum, pro-found alkalosis would be produced if administra-tion of sodium chloride and sodium bicarbonatewere forced until the kidneys reached biologicalequilibrium in the presence of potassium deficit.Alkalotic tetany is, therefore, not the result of afailure of renal function when there is deficit ofmuscle potassium, but alkalosis may be anticipatedas the actual result which the kidneys tend tomaintain. Since alkalosis often leads to low serumcalcium, high concentration of serum bicarbonatemay precipitate low calcium tetany.
Some such course of events probably explainsthe high incidence of tetany reported by Rapoportand others (27) in babies treated by prolonged in-travenous therapy with solutions of glucose, so-dium chloride and sodium bicarbonate. Sinceadministration of calcium chloride would be effec-tive in low calcium tetany and would tend to pro-duce acidosis, the favorable effects of calcium saltswhen used in conjunction with sodium chlorideand sodium bicarbonate are readily explained (27,28). In contrast to their results, however, theauthors have seldom observed low calcium tetanyand have not encountered alkalosis when usingpotassium chloride as well as sodium chloride andsodium bicarbonate in treating infantile diarrhea.
The relationship of serum concentrations tomuscle composition are also relevant to the prac-tice of using the concentration of chloride in serumas an index of therapy. If deficit of potassium ispresent, serum chloride tends to be low at biologi-cal equilibrium. Administration of sodium chlo-ride will not overcome the abnormality in serumand will probably aggravate the deficit of potas-sium in the muscles. In the treatment of Ad-
dison's disease with desoxycorticosterone acetate,low serum chloride may indicate that too largerather than too small a dose of the drug is beingused.
As in previous studies on rats, the serum po-tassium bears no precise relation to muscle po-tassium. In part, this finding may be dependenton changes in the level of serum potassium ac-companying anesthesia. However, high serumpotassium has been the rule when treatment isbegun in patients suffering from dehydration dueto diarrhea (19) and in diabetic coma (26). Rob-inson (29) and Larguia and Vidal (30) foundthat the concentration of potassium was frequentlylow in babies with intestinal intoxication. Duringtreatment, the potassium concentration oftenreached extremely low values and if there was notendency to return to normal, such patients died(29). Although many conditions accompaniedby deficit of body potassium show low serum po-tassium, the exceptions are so many that the levelof serum potassium cannot be relied upon as anindex of the state of intracellular potassium.Nevertheless, the authors do not believe the po-tassium concentrations of this study should beaccepted without reservations, since rats are un-suitable animals for demonstrating the relationof the concentration of potassium in serum to mus-cle composition owing to the difficulty in obtainingblood under resting conditions. Clinical studiesmust be made to evaluate the value of serum po-tassium as an index of deficit of potassium in tis-sues in various conditions.
SUMMARY
The composition of serum and muscle was de-termined in normal and adrenalectomized rats sub-jected to conditions leading to adjustment of bodyelectrolyte in the presence of a deficit of one of theions-sodium, chloride or potassium. Deficit of po-tassium was maintained by a diet low in potassiumor injections of desoxycorticosterone acetate. Def-icit of sodium was produced by injecting NH4C1in glucose into the peritoneal cavity and with-drawing the fluid, and maintaining the rats on adiet deficient in sodium. Deficit of chloride wasproduced by injecting a solution of NaHCO8 inglucose into the peritoneal cavity and withdrawingthe fluid, and maintaining the rats on a diet defi-cient in chloride.

RELATION OF SERUMBICARBONATETO MUSCLECOMPOSITION
The data demonstrate a high degree of cor-relation between the concentration of bicarbonatein serum, muscle potassium and intracellular so-dium. Thus, serum bicarbonate varies directlywith intracellular sodium and inversely with mus-cle potassium. Muscle potassium and intracellularsodium show inverse relationships. These re-latronships may be considered a biological equi-librium which is attained when renal adjustmentis made in the presence of a deficit of sodium orchloride or potassium.
Adrenalectomized rats show the same relation-ships as normal rats.
The therapeutic implications of these findingsare briefly discussed. First, the relationship isknown not to be maintained in dehydration and insuch states we may term the lack of relationshipan unstable state with respect to the relationshipbetween extracellular and intracellular fluids.Second, patients with dehydration accompaniedby deficit of potassium may be expected to developalkalosis when they are treated solely with sodiumand chloride. Third, alkalosis may be expected tobe relatively refractory to treatment with sodiumchloride, if a deficit of potassium persists. Fourth,the dose of sodium bicarbonate necessary to over-come low serum bicarbonate is always uncertain,since sodium may enter or leave the cells depend-ing on the presence or absence of an excess of in-tracellular sodium and the presence or absenceof a deficit of potassium.
BIBLIOGRAPHY
1. Darrow, D. C., Medical progress: body-fluid physiol-ogy: the relation of tissue composition to prob-lems of water and electrolyte balance. New Eng-land J. Med., 1945, 233, 91.
2. Schwartz, R., Electrolyte studies of metabolic acido-sis in the rat. Thesis submitted to the Faculty ofthe Yale University School of Medicine, 1947.
3. Darrow, D. C., Changes in muscle composition inalkalosis. J. Chin. Invest., 1946, 25, 324.
4. Yannet, H., and Darrow, D. C., The effect of deple-tion of extracellular electrolytes on chemical com-position of skeletal muscle, liver and cardiac mus-cle. J. Biol. Chem., 1940, 134, 721.
5. Miller, H. C., and Darrow, D. C., Relation of muscleelectrolyte to alterations in serum potassium andto the toxic effects of injected potassium chloride.Am. J. Physiol., 1940, 130, 747.
6. Harrison, H. E., and Darrow, D. C., The distribu-tion of body water and electrolytes in adrenal in-sufficiency. J. Clin. Invest., 1938, 17, 77.
7. Miller, H. C., and Darrow, D. C., The relation ofserum and muscle electrolyte, particularly potas-sium, to voluntary exercise. Am. J. Physiol.,1941, 132, 801.
8. Darrow, D. C., and Miller, H. C., The productionof cardiac lesions by repeated injections of desoxy-corticosterone acetate. J. Clin. Invest., 1942, 21,601.
9. Ferrebee, J. W., Parker, D., Carnes, W. H., Gerity,M. K., Atchley, D. W., and Loeb, R. F., Certaineffects of desoxycorticosterone: development of"diabetes insipidus" and replacement of musclepotassium by sodium in normal dogs. Am. 3.Physiol., 1941, 135, 230.
10. Elkinton, J. R., Winkler, A. W., and Danowski, T. S.,Inactive cell base and measurement of changes incell water. Yale J. Biol. & Med., 1944, 17, 383.
11. Knowlton, A. I., Loeb, E. N., Stoerk, H. C., andSeegal, B. C., Desoxycorticosterone acetate. Thepotentiation of its activity by sodium chloride. J.Exper. Med., 1947, 85, 187.
12. Hastings, A. B., and Eichelberger, L., The exchangeof salt and water between muscle and blood. I.The effect of increase in total body water pro-duced by the intravenous injection of isotonic saltsolutions. J. Biol. Chem., 1937, 117, 73.
13. Yannet, H., The effect of alkalosis on the chemicalcomposition of brain, skeletal muscle, liver andheart. J. Biol. Chem., 1940, 136, 265.
14. Flexner, L. B., Gellhorn, A., and Merrell, M., Studieson the rates of exchange of substances betweenblood and extravascular fluid. I. The exchangeof water in the guinea pig. J. Biol. Chem., 1942,144, 35.
15. McQuarrie, I., Johnson, R. M., and Ziegler, M. R.,Plasma electrolyte disturbance in a patient withhypercorticoadrenal syndrome contrasted with thatfound in Addison's disease. Endocrinology, 1937,21, 762.
16. Willson, D. M., Power, M. H., and Kepler, E. J.,Alkalosis and low plasma potassium in case ofCushing's syndrome: metabolic study. J. Clin.Invest., 1940, 19, 701.
17. Power, M. H., and Kepler, E. J., Personal commu-nication.
18. Allott, E. N., and McArdle, B., Further observa-tions on familial periodic paralysis. Chin. Sc.,
.1938, 3, 229.1
19. Darrow, D. C., The retention of electrolyte duringrecovery from severe dehydration due to diarrhea.J. Pediat., 1946, 28, 515.
20. Govan, C. D., Jr., and Darrow, D. C., The use ofpotassium chloride in the treatment of dehydrationof diarrhea in infants. J. Pediat., 1946, 28, 541.
21. Darrow, D. C., and Sarason, E. L, Some effects oflow atmospheric pressure on rats. J. Clin. Invest.,1944, 23, 11.
22. Darrow, D. C., Congenital alkalosis with diarrhea.J. Pediat., 1945, 26, 519.
207

208 DANIEL C. DARROW,ROBERTSCHWARTZ,JOHN F. IANNUCCI, AND FRANCESCOVILLE
23. Gamble, J. L., Fahey, K. R., Appleton, J., and Mac-Lachlan, E., Congenital alkalosis with diarrhea.J. Pediat., 1945, 26, 509.
24. Atchley, D. W., Loeb, R. F., Richards, D. W., Jr.,Benedict, E. M., and Driscoll, M. E., On diabeticacidosis. A detailed study of electrolyte balancesfollowing withdrawal and reestablishment of in-sulin therapy. J. Clin. Invest., 1933, 12, 297.
25. Holler, J. W., Potassium deficiency occurring duringtreatment of diabetic acidosis. J. A. M. A., 1946,131, 1186.
26. Martin, H. E., and Wertman, M., Serum potassium,magnesium and calcium levels in diabetic acidosis.J. Clin. Invest., 1947, 26, 217.
27. Rapoport, S., Dodd, K., Clark, M., and Syllm, I.,Postacidotic state in infantile diarrhea: symptomsand chemical data. Postacidotic hypocalcemia andassociated decreases in levels of potassium phos-phorus and phosphatase in plasma. Am. J. Dis.Children, 1947, 73, 391.
28. Minot, A. S., and Dodd, K., The correction of dis-torted fluid equilibrium in the presence of vascularinjury. J. Pediat., 1940, 17, 571.
29. Robinson, P.,. Potassium in acute gastro-enteritis.Ann. Pediat., 1939, 153, 157.
30. Larguia, A. E., and Vidal, J. D., Desmineralizacione hipopotasemia. Medicina, Buenos Aires, 1945, 5,240.
ASSOCIATION ANNOUNCEMENT
The 40th annual meeting of the American Society for ClinicalInvestigation will be held at the Chalfonte-Haddon Hall, AtlanticCity, N. J., on Monday, May 3, 1948, at 9 a.m.
For those who may be interested, the annual meeting of the Ameri-can Association for Research in Psychosomatic Problems will be heldat the same hotel on Saturday, May 1, at 9 a.m., and
The annual meeting of the Association of American Physicians willbe held on Tuesday and Wednesday, May 4 and 5, also at theChalfonte-Haddon Hall.