Embed Size (px)
Citation preview

THERAPY AND PREVENTIONPHARMACOLOGY
Incidence of early tolerance to hemodynamic effectsof continuous infusion of nitroglycerin in patientswith coronary artery disease and heart failure
URI ELKAYAM, M.D., DANIEL KULICK, M.D., NANCY MCINTOSH, R.N., ARIE ROTH, M.D.,WILLA HSUEH, M.D., AND SHAHBUDIN H. RAHIMTOOLA, M.D.
ABSTRACT Sustained therapy with nitroglycerin (NTG) has been reported to provoke the devel-opment of early tolerance. Because continuous intravenous NTG infusion is commonly used in patientswith coronary artery disease and heart failure, we evaluated the incidence of early tolerance developedwithin the first 24 hr of therapy in 31 responders to NTG. After documentation of response to NTG,defined as a 10 mm Hg or greater or a 30% or greater reduction in mean pulmonary arterial wedgepressure (PAWP), 16 patients were blindly, randomly assigned to receive placebo and 15 patients werecontinued on same-dose NTG. Both groups showed an identical fall in PAWP at peak NTG titration(1 1 + 4 mm Hg). Discontinuation of NTG in the placebo group resulted in a rapid increase in PAWPto levels not significantly different from baseline (19 5 mm Hg at 2 hr vs 23 6 mm Hg at baseline;p = NS). In the NTG group, PAWP fell from 27 9 to 14 ± 7 mm Hg, was 16 ± 9 mm Hg at2 hr (p < .05 vs baseline), and continued to be significantly lower than baseline for 8 hr; however,due to attenuation of effect, PAWP values at 12, 20, and 24 hr were not significantly different fromplacebo or baseline values. Analysis of individual data showed there were eight patients (group A) whohad a persistent effect and seven patients (group B) who developed tolerance, which was defined as
an increase in PAWP to values within 10% of baseline or a greater than 34% increase (2 x coefficientof variation ofPAWP in the placebo group 2 to 24 hr after discontinuation ofNTG) from values measuredat the end ofNTG titration. These two groups differed only in their baseline systemic vascular resistance(2195 + 765 vs 1517 + 355 dyne-sec-cm-5; p < .05). No difference was found in any other baselinehemodynamic or hormonal variables or in the magnitude of hemodynamic change during peak NTGtitration and hormonal changes during the study. This study therefore provides further evidence for thedevelopment of early tolerance to the hemodynamic effects of continuous NTG administration.Tolerance is developed in approximately half of patients with coronary artery disease and heart failure.The development of tolerance cannot be predicted by baseline hemodynamic and hormonal values or
their changes during NTG therapy.Circulation 76, No. 3, 577-584, 1987.
SINCE THEIR INTRODUCTION over a century ago,organic nitrates have played an important role in thetreatment of ischemic heart disease.' Recent data dem-onstrating beneficial hemodynamic effect as well asimprovement in exercise capacity and survival havealso resulted in a widespread use of these drugs in thetreatment of acute and chronic congestive heartfailure 2-5
Since organic nitrates are easily absorbed from var-
From the Sections of Cardiology and Endocrinology, Department ofMedicine, LAC-USC Medical Center, University of Southern CaliforniaSchool of Medicine, Los Angeles.
Address for correspondence: Uri Elkayam, M.D., Director, InpatientCardiology, USC School of Medicine, 2025 Zonal Ave., Los Angeles,CA 90033.
Received March 24, 1987; revision accepted June 4, 1987.
ious body organs, many formulations have been devel-oped for sublingual, buccal, oral, and topicaladministration.6 Intravenous nitrate preparations havealso become available in the last several years. Thistherapeutic modality allows rapid onset of effect, easytitration, and a continuous and constant effect and hastherefore been used frequently for in-hospital treatmentof ischemic myocardial disease and heart failure.7Recent experience with transdermal nitroglycerin(NTG), however, has demonstrated the development ofearly and substantial attenuation of the cardiocircula-tory effects, 8,9 raising the possibility that sustainedplasma concentrations ofNTG may lead to early devel-opment of tolerance to the hemodynamic effects of thedrug. Such tolerance to NTG, if present with contin-
Vol. 76, No. 3, September 1987 577
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELKAYAM et al.
uous infusion of the drug, would impose an importantlimitation to its intravenous administration.The objectives of the present study were therefore to
evaluate the incidence and magnitude of tolerance tocontinuous intravenous infusion ofNTG and to attemptto determine potential hemodynamic or hormonal char-acteristics that could predict the development of thisphenomenon. Since patients with coronary artery dis-ease (CAD) and elevated left ventricular filling pressureare usually treated with NTG, we performed our eval-uation in such patients.
MethodsPatient selection. The study was designed to include patients
at least 21 years of age with clinical or angiographic evidenceof CAD and mean pulmonary arterial wedge pressure (PAWP)of 15 mm Hg or higher as a result of left ventricular systolicand/or diastolic failure. Angiographic evidence of CAD wasdefined as 70% or greater obstruction of a major epicardialcoronary artery, whereas clinical evidence of CAD was definedas a history of myocardial infarction documented by character-istic electrocardiographic and enzymatic changes.
Patients with the following conditions were not allowed in thestudy: (1) angiographic evidence of left main CAD, (2) unstableangina, (3) hypertension, (4) primary valvular disease, (5) pul-monary edema, (6) thyrotoxicosis, or (7) recent acute myocar-dial infarction within 30 days before the initiation study.
Forty patients were enrolled into the study, including 29 menand 11 women, aged 45 to 77 years (mean + SD 59 + 8). Thediagnosis of CAD was based on angiographic findings in 38patients and on history of myocardial infarction documented bytypical changes in the electrocardiogram and serum myocardialenzymes in two patients. Left ventricular ejection fraction wasmeasured in 36 patients and ranged from 0. 10 to 0.68 (mean 0.30± 0. 14). All patients had symptoms of heart failure for a periodof at least 1 month.Hemodynamic measurements and computations. Right
heart catheterization was performed with a balloon-tipped, tri-ple-lumen, Swan-Ganz catheter, which allowed the measure-ments or right atrial and pulmonary arterial pressure as well asPAWP. The reference point for the procedure was at the mid-chest level with the patient in a supine position. All pressureswere recorded on Electronics for Medicine AR 6 or VR 12recorders, and mean pressures were measured with the use ofelectronic integration. Heart rate was determined by electro-cardiographic recording and systemic blood pressure was mea-sured by the standard cuff method. Cardiac output was deter-mined by the thermodilution technique, as previouslydescribed. 10 Measurements were preformed in triplicate withice-cold 5% dextrose in water as the indicator. Mean arterialblood pressure, cardiac index, stroke volume index, left ven-tricular stroke work index, systemic vascular resistance, andpulmonary vascular resistance were calculated by standardformulas. 1' The determination of plasma levels of epinephrineand norepinephrine was performed with an isotope radioenzy-matic technique. 12 Plasma renin activity was measured byradioimmunoassay. 1 3 Plasma levels of nitroglycerin wereassayed by a method similar to that described by Settlage et al. 14using gas chromatography/negative ion mass spectrometry withon-column injection (Cal Lab East, Richmond, VA). The coef-ficient of variation was 4.08% for intra-assay and 13. 1 % forinterassay precision.
Study protocol. All patients were studied in a stable clinical
578
condition. Usual doses of digitalis, diuretic agents, and anti-arrhythmic drugs were continued throughout the study. Alllong-acting vasodilators were withheld for at least 24 hr beforethe initiation of the study. Because of reported spontaneoushemodynamic changes after insertion of the pulmonary arterialcatheter, '5 baseline hemodynamic values were measured at least24 hr after the performance of this procedure. Hemodynamicstability (less than 10% variation) was ensured by two consec-utive readings performed at approximately 30 min intervals;values obtained at the last measurement were used as baselinevalues. After baseline measurements, an intravenous infusion ofopen-label NTG was started at a rate of 20 ,ug/min throughspecial NTG polyethylene tubing. The infusion was regu!ated byan infusion pump (IVAC 530) and the rate was increased approx-imately every 5 min in increments of 30 to 60 gtg/min to achievea 30% or greater or a 10 mm Hg or greater reduction in meanPAWP or until a maximum dose of 560 gg/min was reached.After achieving the desired hemodynamic response, a constantinfusion rate of NTG was maintained, and stability of PAWP(< 10% variability) was ensured for at least 30 min. At that pointthe patients were assigned at random, according to a computer-generated schedule, to receive an infusion of either the same doseof NTG or an identical-appearing placebo infusion of NTGvehicle labeled to maintain the blinding. The infusion was thenmaintained at a constant rate for 24 hr. Hemodynamic mea-surements were repeated 2, 4, 8, 12. 20, and 24 hr later. At thatpoint the infusion of the study drug was discontinued andhemodynamic measurements were repeated 15, 30, and 60 minafter discontinuation.Measurements of plasma hormones. Blood samples for
catecholamines and renin were drawn at baseline, at the end ofNTG titration, at 24 hr of constant drug infusion, and 30 minafter discontinuation of the drugs.Measurements of plasma NTG level. Plasma NTG levels
were measured at the end ofNTG titration and at 24 hr of constantNTG infusion in a sample of five consecutive patients who werefound at the end of the study to have received NTG.
Statistical analysis. One-way repeated measures analysis ofvariance (ANOVA) and the Newman-Keuls test used to evaluatethe temporal hemodynamic effects of the study drugs in eachgroup, and single comparisons were performed with Student'st test. Coefficient of variation was calculated as standard devi-ation of the mean/mean x 100. Analyses were performed withthe use of the CLINFO system and the SAS statistical packageon the IBM 370 system at the University of Southern California.All values are expressed as mean + SD. A p value of less than.05 was considered statistically significant.
ResultsNineteen of 40 patients were initially assigned to be
treated with NTG, and the other 21 patients wereassigned to receive placebo. No significant differenceswere found between these two groups in age, durationof symptoms of heart failure, left ventricular ejectionfraction, and measured or calculated baseline hemody-namic values (table 1).
Five of the patients were excluded from the studybecause of failure to achieve the desired PAWPresponse to open-label NTG titrated to its maximumdose of 560 gg/min. Three of these patients wereassigned to receive NTG therapy and two were assignedto receive placebo. One patient who was assigned toreceive placebo was excluded because the baseline
CIRCULATION
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

THERAPY AND PREVENTION-PHARMACOLOGY
TABLE 1Comparison between patients receiving NTG and placebo
NTG Placebo p(n= 19) (n=21) value
Age (yr) 59±8 58+8 NSLeft ventricular ejection
fractionA 0.27 ±0.11 0.32 +0.17 NSDuration of CHF (mo) 29±38 15+16 NSHeart rate (beats/min) 88 ± 11 87 ± 17 NSMean blood pressure(mm Hg) 98+ 13 96+ 16 NS
Cardiac index(I/min/m2) 2.2+0.6 2.4+0.7 NS
Stroke volume index(ml/m2) 25 ± 7 29 + 9 NS
Mean right atrialpressure (mm Hg) 11 +6 8±4 NS
Mean pulmonary arterialpressure (mm Hg) 38 ± 9 35 + 10 NS
Mean PAWP (mm Hg) 26 ± 8 24 + 7 NSSystemic vascular resis-
tance (dynes-sec-cm-5) 1808 ± 648 1758 ± 612 NSPulmonary vascular resis-
tance (dyne-sec-cm 5) 240 ± 118 224 ± 130 NSLeft ventricular strokework index (g-m/m2) 25 ± 11 28 + 11 NS
AMeasured in 17 patients assigned to receive NTG and in 18 patientsassigned to receive placebo.
PAWP had declined to less than 15 mm Hg 24 hr afterthe insertion of the pulmonary catheter. Two patientsreceiving placebo dropped out of the study because ofworsening symptoms and one patient receiving NTGwas excluded because of inability to obtain adequatepressure tracings due to malfunction of the pulmonaryarterial catheter. Thirty-one patients therefore re-sponded to NTG, were blindly, randomly assigned toreceive the study drug, and completed the study. Six-teen of these patients received placebo and 15 receivedNTG.
Hemodynamic changes over timePlacebo group. Titration of open-labeled NTG re-
sulted in no statistically significant effects on heart rate,mean blood pressure, cardiac index, mean right atrialpressure, and systemic and pulmonary vascular resis-tance. NTG significantly reduced mean pulmonaryarterial pressure and PAWP. These pressures decreasedduring infusion of NTG from 34 ± 8 to 21 ± 5 mmHg and from 23 ± 6 to 12 ± 4 mm Hg, respectively,(p < .05). Both variables showed rapid increase aftersubstitution of NTG with placebo, and values at 2 hrwere 29 ± 6 and 19 ± 5 mm Hg, respectively; bothwere not significantly different from control. No furthersignificant changes were noted in both variables during
the study. The values of PAWP measured during thestudy are shown in figure 1. Coefficient of variation ofPAWP was measured in each patient between 2 and 24hr after discontinuation ofNTG; the mean value for theentire group was 17%.NTG group. As in the placebo group, NTG titration
resulted in a significant fall in mean pulmonary arterialpressure and PAWP without a statistically significantchange in other measured or calculated hemodynamicvalues. Mean pulmonary arterial pressure fell from 39± 10 to 24 ± 8 mm Hg (p < .05) and remainedsignificantly lower than baseline values for 12 hr. Val-ues measured at 20 and 24 hr of therapy were notstatistically different from baseline. Mean PAWPdemonstrated a similar change and fell from 27 ± 9 to14 ± 7 mm Hg at peak NTG titration. Although valuesremained lower than baseline for the entire study dura-tion, a gradual increase in PAWP was found and thedecrease in PAWP at 12 hr was no longer statisticallysignificant (figure 1).
Comparison of changes in PAWP between the two treat-ment groups. Figure 2 demonstrates the change inPAWPfrom control in the 16 patients receiving placeboand in the 15 patients receiving NTG. Both groupsshowed an identical fall in PAWP at peak NTG titration(1 1 ± 4 mm Hg). However, discontinuation of NTG
30 r
XIEE
w
Cl)
LJL
U)
a-W(90W
crW
crW
z0
a-zWwt
27±9
25 p
22t9
2020t6 20±9
15 .
I0
* PLACEBOo NTG
BL TITRATION1 2 4 6 8 10 12 14 16 18 20 22 24
TIME (HOURS)
FIGURE 1. ValuesofmeanPAWP as measured at baseline (BL) duringNTG titration and during the 24 hr of the study infusion. After titrationof NTG, 16 patients were randomly assigned to receive placebo and 15patients were assigned to receive NTG. *p < .05 vs BL.
Vol. 76, No. 3, September 1987 579
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELKAYAM et al.
PEAK NTG
o EFFECT-
6; -26l:E-64
_i _b0ir -10UA.
NS ---1 lp<O.O 1p<0.001
8 HRS 12 HRS 20HRS 24 HRS
PLACEBO GRO
. 93 NTG GROUP
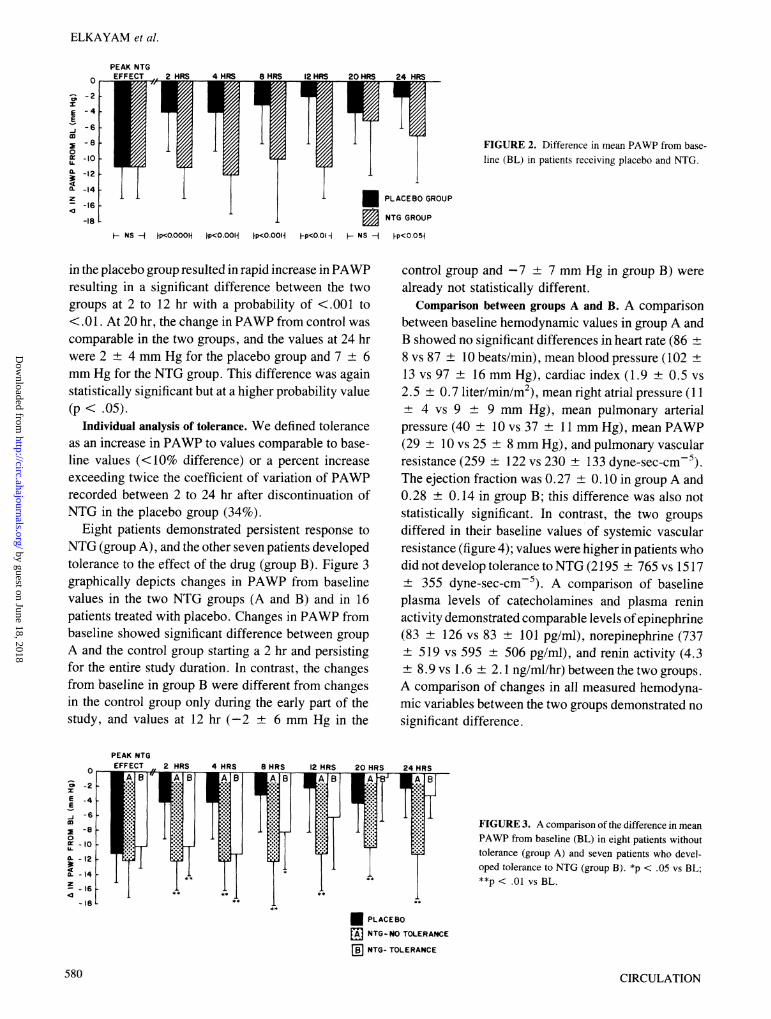
FIGURE 2. Difference in mean PAWP from base-line (BL) in patients receiving placebo and NTG.
UP
[p<O.OOH Fp<O.O H- NS -1 Fp<0.05
in the placebo group resulted in rapid increase in PAWPresulting in a significant difference between the twogroups at 2 to 12 hr with a probability of <.001 to<.01. At 20 hr. the change in PAWP from control wascomparable in the two groups, and the values at 24 hrwere 2 ± 4 mm Hg for the placebo group and 7 ± 6mm Hg for the NTG group. This difference was againstatistically significant but at a higher probability value(p < .05).
Individual analysis of tolerance. We defined toleranceas an increase in PAWP to values comparable to base-line values (<10% difference) or a percent increaseexceeding twice the coefficient of variation of PAWPrecorded between 2 to 24 hr after discontinuation ofNTG in the placebo group (34%).
Eight patients demonstrated persistent response toNTG (group A), and the other seven patients developedtolerance to the effect of the drug (group B). Figure 3graphically depicts changes in PAWP from baselinevalues in the two NTG groups (A and B) and in 16patients treated with placebo. Changes in PAWP frombaseline showed significant difference between groupA and the control group starting a 2 hr and persistingfor the entire study duration. In contrast, the changesfrom baseline in group B were different from changesin the control group only during the early part of thestudy, and values at 12 hr (-2 ± 6 mm Hg in the
control group and -7 ± 7 mm Hg in group B) werealready not statistically different.
Comparison between groups A and B. A comparisonbetween baseline hemodynamic values in group A andB showed no significant differences in heart rate (86 +8 vs 87 ± 10 beats/min), mean blood pressure (102 +13 vs 97 ± 16 mm Hg), cardiac index (1.9 ± 0.5 vs2.5 ± 0.7 liter/min/m2), mean right atrial pressure ( 11+ 4 vs 9 ± 9 mm Hg), mean pulmonary arterialpressure (40 ± 10 vs 37 ± 11 mm Hg), mean PAWP(29 ± 10 vs 25 ± 8 mm Hg), and pulmonary vascularresistance (259 ± 122 vs 230 + 133 dyne-sec-cm-5).The ejection fraction was 0.27 ± 0. 10 in group A and0.28 ± 0.14 in group B; this difference was also notstatistically significant. In contrast, the two groupsdiffered in their baseline values of systemic vascularresistance (figure 4); values were higher in patients whodid not develop tolerance to NTG (2195 ± 765 vs 1517± 355 dyne-sec-cm-5). A comparison of baselineplasma levels of catecholamines and plasma reninactivity demonstrated comparable levels ofepinephrine(83 ± 126 vs 83 ± 101 pg/ml), norepinephrine (737± 519 vs 595 ± 506 pg/ml), and renin activity (4.3± 8.9 vs 1.6 ± 2. 1 ng/ml/hr) between the two groups.A comparison of changes in all measured hemodyna-mic variables between the two groups demonstrated nosignificant difference.
PEAK NTG
FIGURE 3. A comparison of the difference in meanPAWP from baseline (BL) in eight patients withouttolerance (group A) and seven patients who devel-oped tolerance to NTG (group B). *p < .05 vs BL;**p < .01 vs BL.
* PLACEBO
m NTG-NO TOLERANCE
[ NTG- TOLERANCE
580
- -14 [z
-16-18 I
CIRCULATION
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

THERAPY AND PREVENTION-PHARMACOLOGY
SYSTEMIC VASCULARRESISTANCE
3800r
3400H
3000FIlE
C~
2600
2200
1800
1400
1000
0
0
0
0
--~-p-CO.05
S
S
--4
GROUP A GROUP BFIGURE 4. Individual and group values of systemic vascular resistancein patients with persistent effect of NTG on left ventricular fillingpressure (group A) and patients who developed tolerance to NTG(group B).
The change in plasma hormonal levels is demon-strated in figure 5 for the two groups. A tendency forelevation in plasma renin activity was seen at peakNTGtitration and at 24 hr in group A. The changes, however,were not significant when compared with baseline val-ues. Similarly, no significant changes were seen in thelevels of both epinephrine and norepinephrine duringthe infusion of NTG or after its discontinuation in thetwo groups of patients treated with this drug.
Plasma NTG levels. The measurements of plasmaNTG levels were preformed in a sample of five con-secutive patients treated with NTG during peak drugtitration and at 24 hr of NTG infusion (figure 6). MeanNTG plasma level was 21,200 + 6768 pg/ml at peakNTG titration and 20,299 + 7986 pg/ml at 24 hr ofNTG titration. These two values were not significantlydifferent. In spite of persistence of NTG in plasma, inthese patients PAWP was significantly higher (p < .05)
at 24 hr (27 ± 9 mm Hg) than at peak NTG titration(22 + 9 mm Hg).
DiscussionThese results clearly demonstrate the development
of tolerance to the hemodynamic effects of intravenousinfusion of NTG occurring within the first 12 hr oftherapy in approximately half of our patients. Thefindings of persistent NTG blood levels at the end ofthe study showed that the attenuation of the effects ofNTG was not caused by a reduction in drug concen-tration in the blood. These findings bear importantclinical implications and reemphasize the potentialtherapeutic limitations of NTG when given in a con-tinuous, uninterrupted fashion in patients with CADand heart failure. The relationship between continuityof exposure to organic nitrates and the development oftolerance to their vasodilatory effect was first demon-strated in animal experiments.16' 17 Recent investiga-tions of the effects of continuous NTG administrationvia transdermal systems have also demonstrated adevelopment of early tolerance to the hemodynamicand anti-ischemic effects in patients with angina pec-toris and heart failure.8 1821
Individual analysis of our data shows that not allpatients develop tolerance to the effects of NTG;approximately half of the patients maintained theirinitial response to the drug. This conclusion may belimited by the fact that the duration of the study wasrestricted to 24 hr and tolerance to NTG may occur laterin some patients. Although this possibility cannot beexcluded by our results, the findings in this study andothers suggest that tolerance to NTG when adminis-tered continuously is an early phenomenon that occurswithin several hours of therapy.21 22An ability to predict the development of tolerance in
patients treated with intravenous NTG would be ofobvious clinical importance. In this study, patients whodeveloped tolerance demonstrated a lower baseline sys-temic vascular resistance. The explanation for thisfinding in not readily apparent, especially since otherdifferences between the groups that may suggest milderhemodynamic impairment in patients with tolerancewere not statistically significant and no difference wasfound in baseline left ventricular function and levels ofcirculating catecholamines and renin. In addition, indi-vidual date showed overlap between the two groups,demonstrating that baseline values of systemic vascularresistance are a poor predictor of the effects in anindividual patient.
Previous reports suggested that tolerance to the effectof vasodilator drugs may result from activation of vaso-
Vol. 76, No. 3, September 1987
0
0
581
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELKAYAM et al.
PLASMA RENIN ACTIVITY(ng/mI/hr)
12 r
4
T1v----'I I
BL PE 24HR
900
600
120 r
80
40
NORE PINEPHRINE(pg/mi)
I
EPINEPHRINE(pg/mi)
BL PE 24 HR
FIGURE 5. Values of plasma renin activity, epi-nephrine, and norepinephrine as measured at baseline(BL), at peak NTG (PE), and at 24 hr of continuousNTG infusion, in eight patients who showed persis-tent effect (group A) and seven patients who devel-oped tolerance to NTG (group B). The differencebetween the two groups was not statistically signif-icant.
o GROUP A
*GROUP B
300 1
BL PE 24 HR
constrictor forces such as sympathetic nervous systemand the renin angiotensin system, which are mediatedby a fall in systemic blood pressure and may counteractthe initial vasodilatory effect.23 24 Our results cannotsupport such a mechanism, since no difference wasfound in the magnitude of hemodynamic changes withinitiation of NTG therapy and in the levels of cate-cholamines and renin during NTG administrationbetween patients who did and did not develop toler-ance. However, more frequent assessment of hormonal
PLASMA NTG LEVELS(pg/mi)
plasma levels or a direct functional assessment of theautonomous nervous systems during nitrate therapymay provide further understanding of the role of sym-pathetic nerve activity in the attenuation of vasodilatoryeffect of NTG.25
Five of our patients failed to demonstrate a reductionof PAWP in spite of titration of NTG to very largedoses. A similar finding is seen when NTG is givenintravenously to patients with heart failure caused byacute myocardial infarction26 or orally to patients with
PULMONARY ARTERYWEDGE PRESSURE
(mm Hg)36r
PEAK 24 HRSNTG
FIGURE 6. Values of NTG plasma levels and mean PAWP at peakdrug titration (open bars) and at 24 hr of NTG infusion (shaded bars)in five patients receiving NTG.
H- p<0.05-1
PEAK 24 HRSNTG
CIRCULATION
8
582
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

THERAPY AND PREVENTION-PHARMACOLOGY
chronic heart failure.27 Although failure to respond tohigh doses of NTG may be caused by resistance of thevascular system to the drug, early development oftolerance shortly after exposure to NTG due to nitrate-mediated oxidation of critical sulfhydryl groups in thenitrate receptors cannot be excluded. The depletion ofintracellular stores of sulfhydryl groups within vasculartissue has been suggested by Needleman and Johnson28as the mechanism of tolerance to organic nitrates.These sulfhydryl groups are needed for conversion oforganic nitrates to s-nitrosothiols in the smooth musclecell, which are believed to activate the enzyme guany-late cyclase. This enzyme leads to increased levels ofintracellular cyclic guanosine monophosphate, whichcauses vasodilation.29 Recent studies seemed to sup-port this assumption by demonstrating that NTG-in-duced peripheral and coronary dilatory effect could bepotentiated by N-acetylcysteine, a source of sulfhydrylgroups.30' 31 A recent preliminary report by Packer etal.32 has also shown reversal of tolerance to NTGshemodynamic effects in a group of patients with heartfailure after the administration of N-acetylcysteine.32More clinical data, however, are needed for furtherdefinition of the potential role of sulfhydryl donors inthe prevention of tolerance to organic nitrates.
Recent experimental data have demonstrated that,similar to NTG nitroprusside also appears to promotemuscle relaxation by increasing tissue levels of cyclicguanosine monophosphate.33 In an experiment in vitroby Axelsson et al.34 vascular smooth muscle madetolerant to NTG demonstrated some cross-tolerance to
nitroprusside with respect to its relaxant effect and theresponse of cyclic guanosine monophosphate. Otherinvestigators, however, failed to find cross-toleranceand postulated that the initial site of action in thevascular smooth muscle may be different for NTG andnitroprusside. Because of the obvious clinical impor-tance, further clinical investigation will be needed to
establish the presence or absence of cross-tolerancebetween these two drugs.The loss of NTG-mediated hemodynamic effect
within several hours after initiation of therapy inpatients with CAD demonstrated in our study empha-sizes the need for continuous monitoring of thehemodynamic effect of the drug. Although hemody-namic monitoring has been traditionally performed byinvasive methods, echocardiographic and Dopplertechniques35 36 may allow a noninvasive evaluation ofvolumetric and hemodynamic effects of nitrate therapyand assurance of their persistance.
Recent clinical investigations have demonstratedthat nitrate tolerance can be reversed or even prevented
by the use of intermittent dosing rather than continuousnitrate therapy.37-39Although the intravenous route forNTG administration is advantageous for the initial ther-apy of unstable ischemic disease or heart failure, anintermittent regimen seems to be preferred for pro-longed treatment with organic nitrates. Further studiesare needed, however, to determine the duration of thenitrate-free periods required to prevent or reverse tol-erance to the effect of nitrate therapy in patients withCAD and heart failure.
References1. Elkayam U, Aronow WS: Glyceryl trinitrate (nitroglycerin) oint-
ment and isosorbide dinitrate: a review of their pharmacologicalproperties and therapeutic use. Drugs 23: 165, 1982
2. Franciosa JA, Cohn JN: Sustained hemodynamic effects withouttolerance during long-term isosorbide dinitrate treatment of chronicleft ventricular failure. Am J Cardiol 45: 648, 1980
3. Leier CV, Huss P, Magorien RD, Unverferth DV: Improved exer-
cise capacity and differing arterial and venous tolerance duringchronic isosorbide dinitrate therapy for congestive heart failure.Circulation 67: 817, 1983
4. Cohn J, Archibald DG, Phil M, Ziesche S, Franciosa JA, HarstonWE, Tristani FE, Dunkman WB, JacobsW, Francis GS, FlohrKH,Goldman S, Cobb FR, Shah PM, Saunders R, Fletcher RD, LoebHS, Hughes VC, Baker B: Effect of vasodilator therapy on mortalityin chronic congestive heart failure: results of a Veterans Admin-istration cooperative study. N Engl J Med 314: 1547, 1986
5. Roth A, Weber L, Freidenberger L, Rahimtoola SH, Elkayam U:A comparison between hemodynamic effects of intravenous iso-sorbide dinitrate and nitroglycerin in acute myocardial infarctionand elevated pulmonary artery wedge pressure: a randomized trial.Chest 91: 190, 1987
6. Abrams J: Nitrate delivery system in perspective: a decade ofprogress. Am J Med 76(6A): 38, 1984
7. Herling IM: Intravenous nitroglycerin: clinical pharmacology andtherapeutic considerations. Am Heart J 108: 141, 1984
8. Jordan RA, Seth L, Casebolt P, Hayes MJ, Wilen MM, FranciosaJ: Rapidly developing tolerance to transdermal nitroglycerin incongestive heart failure. Ann Intern Med 104: 295, 1986
9. Flaherty JT: Hemodynamic attenuation and the nitrate-free interval:alternative dosing strategies for transdermal nitroglycerin. Am JCardiol 56: 321, 1985
10. Elkayam U, Berkley R, Azen S, Weber L, Geva B, Henry WL:Cardiac output by thermodilution technique: effect of inje-ctatevolume and temperature on accuracy and reproducibility in thecritically ill patient. Chest 84: 418, 1983
11. Elkayam U, Weber L, Torkan B, Berman D, Rahimtoola SH: Acutehemodynamic effects of oral nifedipine in severe chronic congestiveheart failure. Am J Cardiol 52: 1041, 1983
12. Goldstein DS, Feuerstein G, Izzo JL, Kopin IJ, Keiser HR: Validityand reliability of liquid chromatography with electromechanicaldetection for measuring plasma levels of norepinephrine and epi-nephrine in man. Life Sci 28: 467, 1981
13. Hsueh WA, Luetscher JA, Carlson EJ, Grislis G: Big renin inplasma of healthy subjects on high sodium intake. Lancet 1: 1281,1978
14. Settlage JA, Gielsdorf W, Jaeger: Femtogram level quantitativedetermination of nitroglycerin and metabolites in human plasma byGC-MS negative ion chemical ionization, single ion monitoring.Journal of High Resolution Chromatography and ChromatographyCommunications 179: 347, 1983
15. Packer M, Medina N, Yushak M: Hemodynamic changes mim-icking a vasodilator drug response in the absence of drug therapyafter right heart catheterization in patients with chronic heart failure.Circulation 71: 761, 1985
16. Needleman P, Blehm DJ, Harkey AB, Johnson GH Jr, Lang S: Themetabolic pathway in the degeneration of glyceryl trinitrate. JPharmacol Exp Ther 179: 347, 1971
17. Herman AG, Bogaert MG: Organic nitrates: tolerance at the level
583Vol. 76, No. 3, September 1987
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELKAYAM et al.
of the vascular smooth muscle. Arch Int Pharmacodyn Ther 192:200, 1971
18. Parker JO, Fung HL: Transdermal nitroglycerin in angina pectoris.Am J Cardiol 54: 471, 1984
19. Reichek N, Priest C, Zimrin D, Chandler T, Sutton MJ: Antianginaleffects of nitroglycerin patches. Am J Cardiol 54: 1. 1984
20. Thadani U, Hamilton SF, Olson E, Anderson J, Voyles W, PrasadR, Teague SM: Transdermal nitroglycerin patches in angina pec-toris: dose titration, duration of effect, and rapid tolerance. AnnIntern Med 105: 485, 1986
21. Packer M, Medina N, Yushak M, Lee WH: Hemodynamic factorslimiting the response to transdermal nitroglycerin in severe chroniccongestive heart failure. Am J Cardiol 57: 260, 1986
22. Jordan RA, Seth L, Henry DA, Wilen MM, Franciosa JA: Doserequirements and hemodynamic effects of transdermal nitroglycerincompared with placebo in patients with congestive heart failure.Circulation 71: 980, 1985
23. Manthey J, Dietz R, Leinberger H, Schmidt-Gagk H. Schoming A,Schwartz F, Kubler W: Vasodilator therapy in heart failure: limitedby activation of vasoconstrictor mechanisms? Circulation 62(supplIII): 111-259, 1980 (abst)
24. Colucci WS, Williams GH, Alexander RW, Braunwald E: Mech-anisms and implications of vasodilator tolerance in the treatment ofcongestive heart failure. Am J Med 71: 89, 1981
25. Leimback WN, Wallin BG, Victor RG, Aylward PE, Sundlof G,Mark AL: Direct evidence from intraneural recordings for increasedcentral sympathetic outflow in patients with heart failure. Circu-lation 73: 913, 1986
26. Elkayam U, Roth A, Weber L. Rahimtoola SH: Nitrate resistance:failure of intravenous nitrate to reduce elevated left ventricularfilling pressure in acute myocardial infarction: a common and unpre-dictable phenomenon. J Am Coll Cardiol 9: 23A, 1987 (abst)
27. Kulick D. Roth A, McIntosh N. Rahimtoola SH. Elkayam U:Resistance to isosorbide dinitrate in patients with chronic heartfailure: incidence and attempt at hemodynamic prediction. Clin Res35: 109A, 1987 (abst)
28. Needleman P, Johnson EM: Mechanism of tolerance developmentto organic nitrates. J Pharmacol Exp Ther 184: 709, 1973
29. Ignarro LJ, Lippton H, Edwards JC, Baricos WH, Hyman AL.Kadowitz PJ, Gruetter CA: Mechanism of vascular smooth musclerelaxation by organic nitrates, nitrites, nitroprusside, and nitricoxide: evidence for the involvement of s-nitrosothiols as activeintermediates. J Pharmacol Exp Ther 218: 739, 1981
30. Horowitz JD, Antman EM, Lorell BH, Barry WH, Smith TW:Potentiation of the cardiovascular effects of nitroglycerin by N-acetylcysteine. Circulation 68: 1247, 1983
31. Winniford MD, Kennedy PL, Wells PJ, Hillis LD: Potentiation ofnitroglycerin-induced coronary dilatation by N-acetylcysteine. Cir-culation 73: 138, 1986
32. Packer M, Lee WH, Kessler P, Medina N, Yushak M: Inductionof nitrate tolerance in heart failure by continuous intravenous infu-sion of nitroglycerin and reversal of tolerance by N-acetylcysteine,a sulfhydryl donor. J Am Coll Cardiol 7: 27A, 1985 (abst)
33. Keith RA, Burkman AM, Sokoloski TD, Fertel RH: Vasculartolerance to nitroglycerin and cyclic GMP generation in rat smoothmuscle. Pharmacol Exp Ther 221: 525, 1982
34. Axelsson KL. Anderson RGG, Wikberg JES: Vascular smoothmuscle relaxation by nitro compounds: reduced relaxation andcGNP elevation in tolerant vessels and reversal of tolerance bydithiothreitol. Acta Pharmacol Toxicol 50: 350, 1982
35. Abrams J. Kochukosky R: Hemodynamic effects of nitroglycerinointment and sublingual nitroglycerin: reduction in left ventricularvolume. Chest 70: 418, 1976
36. Elkayam U, Gardin JM. Berkley R, Hughes CA, Henry WC: Theuse of Doppler flow velocity measurement to assess the hemody-namic response to vasodilators in patients with heart failure. Cir-culation 67; 377, 1985
37. Rudolph W, Blasini R, Reiniger G, Brugmann U: Tolerance devel-opment during isosorbide dinitrate treatment: can it be circumvent-ed? Z Kardiol 72(suppl 3): 195, 1983
38. Silber S, Krause KH, Theisen K: Nitrate tolerance: dependence ofdosage intervals? Circulation 70(suppl II): 11-189, 1984 (abst)
39. Parker JO, Van Koughnett KA. Farrel B: Comparison of buccalnitroglycerin and oral isosorbide dinitrate for nitrate tolerance instable angina pectoris. Am J Cardiol 56: 724, 1985
CIRCULATION584
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from

U Elkayam, D Kulick, N McIntosh, A Roth, W Hsueh and S H Rahimtoolanitroglycerin in patients with coronary artery disease and heart failure.
Incidence of early tolerance to hemodynamic effects of continuous infusion of
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1987 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.76.3.577
1987;76:577-584Circulation.
http://circ.ahajournals.org/content/76/3/577the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 18, 2018http://circ.ahajournals.org/
Dow
nloaded from



























![Forat Negre[13]](https://img.pdfslide.net/doc/110x75/545e494caf795930708b476c/forat-negre13.jpg)
