Embed Size (px)
Citation preview
Emergency Medicine Pearls
ASHP’s Section of Clinical Specialists and Scientists Section Advisory Group on Emergency Care
To the Moon and Back With a Bolus of Nicardipine
Nadia Awad, Pharm.D., BCPS
Clinical Assistant Professor, Emergency Medicine
Ernest Mario School of Pharmacy
Rutgers, The State University of New Jersey
Learning Objective:
• Describe the clinical indications and dosing recommendations of administration of bolus dosing of intravenous nicardipine in the emergency department.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 1
Cheung DG et al. Am Heart J 1990; 119:438‐442.
Cheung DG et al. Am Heart J 1990; 119:438‐442.
Decrease in SBP: 20 to 25 mmHg
Decrease in DBP: 15 to 44 mmHg
Onset within 3 minutes
Mean duration of action: 24 ± 5 minutes
Dose‐response relationship
Cheung AT et al. Anesth Analg 1999; 89:1116‐1123.
Cheung AT et al. Anesth Analg 1999; 89:1116‐1123.
Effects of Nicardipine Bolus Dosing on Measured Parameters
Parameter 0.25 mg 0.5 mg 1.0 mg 2.0 mg
Decrease in SBP (mmHg)
18 ± 2 32 ± 5 36 ± 4 51 ± 4
Decrease in MAP (mmHg)
15 ± 5 21 ± 3 24 ± 4 30 ± 2
Dose‐dependent effects
Two‐compartment pharmacokinetic model
Rapid redistribution
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 2

Kross RA et al. Anesth Analg 2000; 91:904‐909.
Zhang Y et al. Anesth Analg 2005; 100:378‐381.
Song D et al. Anesth Analg 1997; 85:1247‐1251.
Kovac AL et al. J Cardiothorac Vasc Anesth 2007; 21:45‐50. Tao P et al. Curr Ther Res Clin Exp 1998; 59:188‐195.
Nadia Awad, Pharm.D., BCPS
@Nadia_EMPharmD
Emergency Medicine PharmDhttp://empharmd.blogspot.com
iTunes: EMPOWER Podcast
How High Can You Go?Nitroglycerin Boluses for the Ailing Heart
Suprat S. Wilson, PharmD, BCPS
Pharmacy Coordinator, Emergency Medicine Services
Detroit Receiving Hospital
Detroit, MI
Learning Objective:
• To discuss the use of high dose nitroglycerin boluses in heart failure exacerbation.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 3
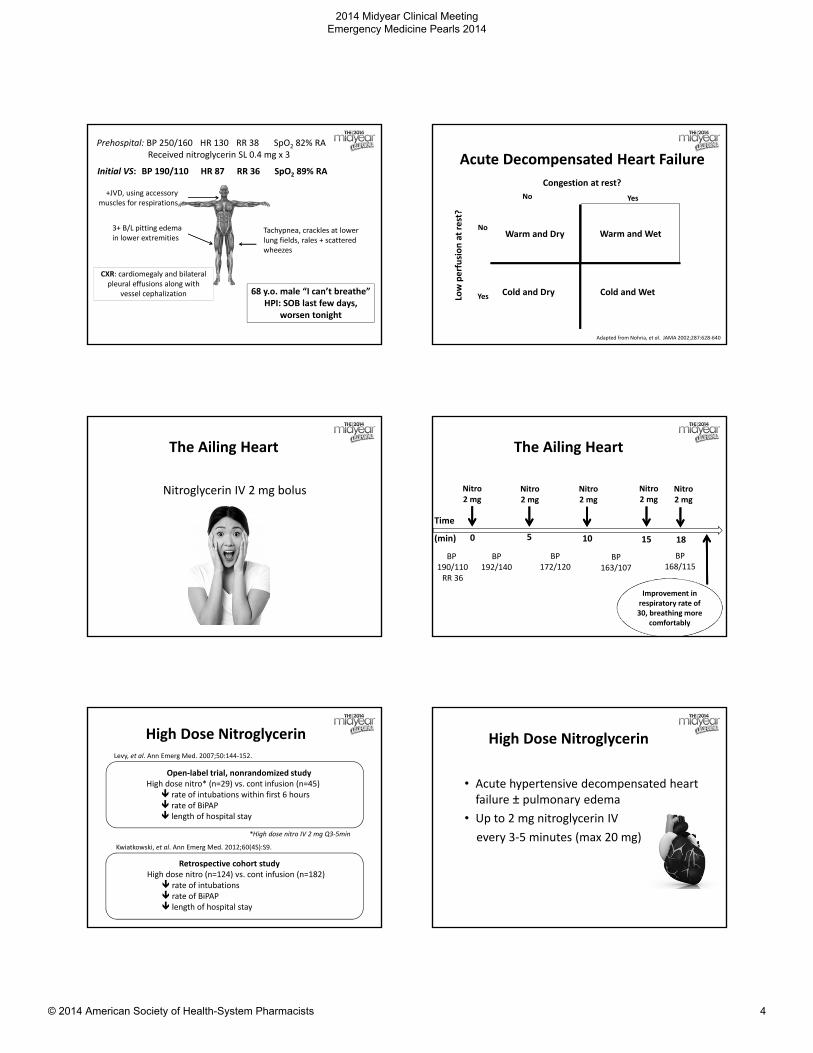
Prehospital: BP 250/160 HR 130 RR 38 SpO2 82% RAReceived nitroglycerin SL 0.4 mg x 3
+JVD, using accessory muscles for respirations
Tachypnea, crackles at lower lung fields, rales + scattered wheezes
3+ B/L pitting edema in lower extremities
68 y.o. male “I can’t breathe” HPI: SOB last few days,
worsen tonight
Initial VS: BP 190/110 HR 87 RR 36 SpO2 89% RA
CXR: cardiomegaly and bilateral pleural effusions along with
vessel cephalization
Acute Decompensated Heart Failure
Congestion at rest?
Low perfusion at rest?
No
No
Yes
Yes
Warm and Dry Warm and Wet
Cold and WetCold and Dry
Adapted from Nohria, et al. JAMA 2002;287:628‐640
The Ailing Heart
Nitroglycerin IV 2 mg bolus
The Ailing Heart
BP 190/110RR 36
Nitro2 mg
Nitro2 mg
Nitro2 mg
Nitro2 mg
Nitro2 mg
BP 192/140
BP 172/120
BP 163/107
BP 168/115
Time
(min) 0 5 10 15 18
Improvement in respiratory rate of 30, breathing more
comfortably
High Dose Nitroglycerin
Open‐label trial, nonrandomized studyHigh dose nitro* (n=29) vs. cont infusion (n=45) rate of intubations within first 6 hours rate of BiPAP length of hospital stay
*High dose nitro IV 2 mg Q3‐5min
Levy, et al. Ann Emerg Med. 2007;50:144‐152.
Retrospective cohort studyHigh dose nitro (n=124) vs. cont infusion (n=182) rate of intubations rate of BiPAP length of hospital stay
Kwiatkowski, et al. Ann Emerg Med. 2012;60(4S):S9.
High Dose Nitroglycerin
• Acute hypertensive decompensated heart failure ± pulmonary edema
• Up to 2 mg nitroglycerin IV
every 3‐5 minutes (max 20 mg)
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 4
How High Can You Go?Nitroglycerin Boluses for the Ailing Heart
Suprat S. Wilson, PharmD, BCPS
Pharmacy Coordinator, Emergency Medicine Services
Detroit Receiving Hospital
Detroit, MI
Who Nose How to Treat Epistaxis
Cole Sloan, Pharm.D.
PGY2 Resident, Emergency Medicine
University of Arizona Medical Center
Learning Objective
• Discuss therapies for treatment of epistaxis
• Focus on vasoconstrictors
Etiology
• Epistaxis digitorum
• Very cold or dry air
• Trauma
• Deviated septum
• Irritation (e.g., allergies, colds, chemicals)
• Overuse of nasal decongestants
Epistaxis
Anterior
• 90% of epistaxis episodes
• Kiesselbach's plexus
Posterior
• More difficult to treat
• May necessitate ENT consult or admission
Therapies for Epistaxis
• Address underlying cause
• Vasoconstrictors
• Topical hemostatic agents
• Chemical cautery
• Nasal packing
• Plasminogen activation inhibitors
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 5
Topical Vasoconstrictors
Mechanism of Action
• Oxymetazoline
• Phenylephrine
• Lidocaine + Epinephrine
• Cocaine Topical Solution• Note different concentrations (4%, 10%)
Comparative effectiveness studiesbetween these agents are lacking
Cocaine
Pros
• Potent anesthetic and vasoconstrictor
• Quick on, quick off
Cons
• Schedule II
• Cost has risen
• CV effects
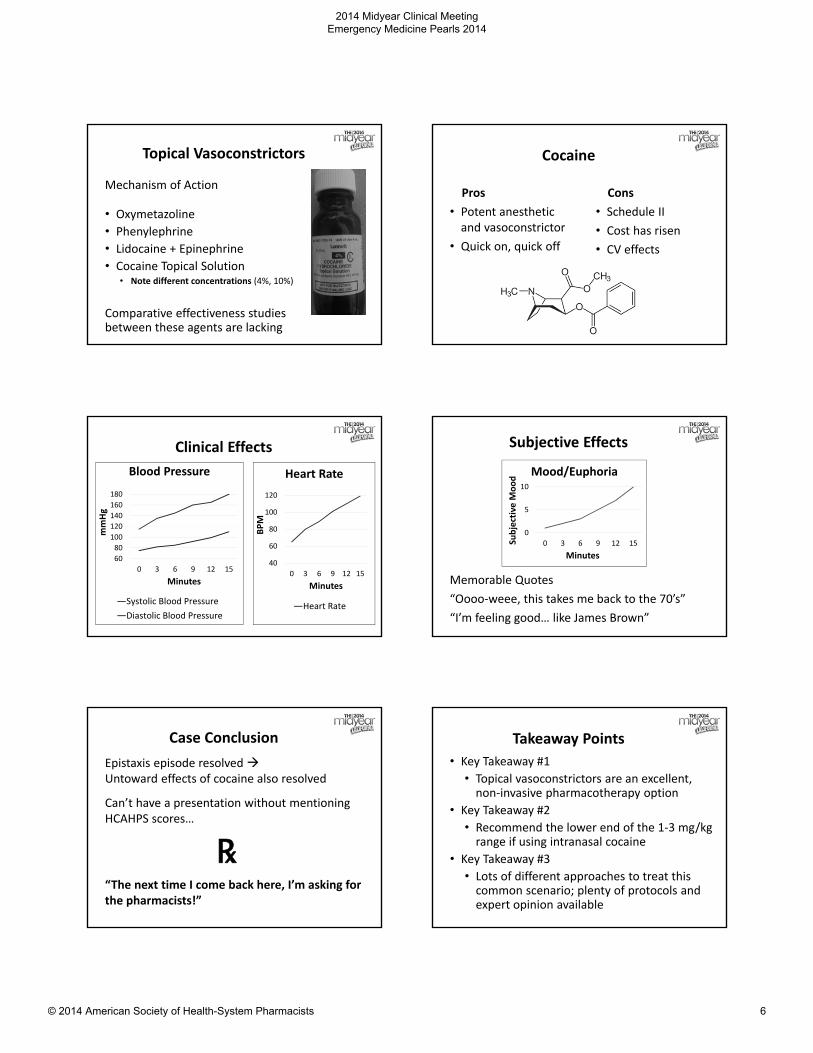
Clinical Effects
60
80
100
120
140
160
180
0 3 6 9 12 15
mmHg
Minutes
Blood Pressure
Systolic Blood Pressure
Diastolic Blood Pressure
40
60
80
100
120
0 3 6 9 12 15
BPM
Minutes
Heart Rate
Heart Rate
Subjective Effects
Memorable Quotes
“Oooo‐weee, this takes me back to the 70’s”
“I’m feeling good… like James Brown”
0
5
10
0 3 6 9 12 15Subjective M
ood
Minutes
Mood/Euphoria
Case Conclusion
Epistaxis episode resolved Untoward effects of cocaine also resolved
Can’t have a presentation without mentioning HCAHPS scores…
℞“The next time I come back here, I’m asking for the pharmacists!”
Takeaway Points
• Key Takeaway #1
• Topical vasoconstrictors are an excellent, non‐invasive pharmacotherapy option
• Key Takeaway #2
• Recommend the lower end of the 1‐3 mg/kg range if using intranasal cocaine
• Key Takeaway #3
• Lots of different approaches to treat this common scenario; plenty of protocols and expert opinion available
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 6
References• Katz RI, Hovagim AR, Finkelstein HS, et al. A comparison of cocaine,
lidocaine with epinephrine, and oxymetazoline for prevention of epistaxis on nasotracheal intubation. J Clin Anesth 1990. 2(1): 16‐20. PMID: 2310576
• Lannett Company, Inc (2012). Cocaine Hydrochloride, [product information]. Philadelphia, PA, Lannett Company, Inc.
• Therapeutic Intranasal Drug Delivery. “Epistaxis Therapy (Bloody Nose).” Retrieved September 8, 2014 from Therapeutic Intranasal Drug Delivery. http://intranasal.net/epistaxis/default.htm
• “Cocaine HCl”. Micromedex 2.0 [internet database]. Greenwood Village, CO, Thomson Reuters. Accessed September 15, 2013.
• “Kiesselbach’s Plexus and Tongue Depressors” – photo by Chris Edwards and Cole Sloan. Accessed September 23, 2014.
• "Kokain ‐ Cocaine" by NEUROtiker ‐ own work. Licensed under public domain via Wikimedia Commons – Accessed September 2, 2014.
Who Nose How to Treat Epistaxis
Cole Sloan, Pharm.D.
PGY2 Resident, Emergency Medicine
University of Arizona Medical Center
Sticking Its Nose in Another Indication: TXA for Epistaxis
Kristan E. Vollman, Pharm.D.Emergency Medicine Clinical Pharmacy Specialist
Owensboro Health Regional HospitalOwensboro, KY
Learning Objective:
• Discuss the use of tranexamic acid for treatment of epistaxis.
Patient Case
• 58yo male presents to the ED with recurrent epistaxis
Oxymetazoline Ice + pressureEpinephrine + lidocaine
Adapted from: arthrocareent.com
+ Antibiotics
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 7
Tranexamic Acid (TXA)
• Lysine analong reversible, competitive inhibition of plasminogen‐fibrin binding sites
• Indications• Labeled
• Tooth extractions• Menorrhagia
• Unlabeled• Cesarean sections• Hereditary angioedema• Traumatic hemorrhage• Perioperative bleeding
Adapted from: obgmanagement.com
TXA for Epistaxis
• Oral
• Local gel
• Duration of treatment
• Concern for thromboembolic complications with systemic use
Sabba C, et al. N Engl J Med 2001; 345(12):926.
White A, et al. Clin Otolaryngol Allied Sci 2007; 13(1):11‐6.
Tibbelin A, et al. J Otorhinolaryngol Relat Spec 1995; 57(4):207‐9.
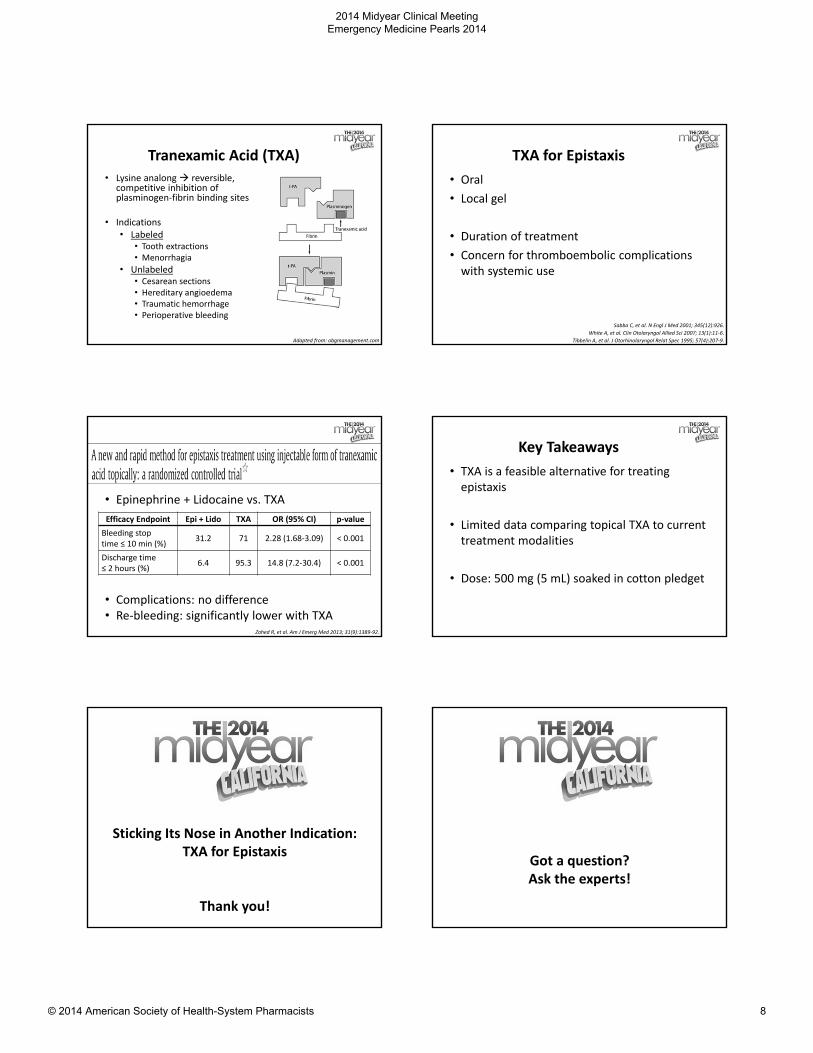
• Epinephrine + Lidocaine vs. TXA
• Complications: no difference• Re‐bleeding: significantly lower with TXA
Zahed R, et al. Am J Emerg Med 2013; 31(9):1389‐92.
Efficacy Endpoint Epi + Lido TXA OR (95% CI) p‐value
Bleeding stoptime ≤ 10 min (%)
31.2 71 2.28 (1.68‐3.09) < 0.001
Discharge time ≤ 2 hours (%)
6.4 95.3 14.8 (7.2‐30.4) < 0.001
Key Takeaways
• TXA is a feasible alternative for treating epistaxis
• Limited data comparing topical TXA to current treatment modalities
• Dose: 500 mg (5 mL) soaked in cotton pledget
Sticking Its Nose in Another Indication: TXA for Epistaxis
Thank you!
Got a question?Ask the experts!
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 8
Holy QT Batman!Isoproterenol for the treatment of refractory
Torsades de Pointes
Mason Bucklin, Pharm.D.
Emergency Medicine Pharmacist
University of Tennessee Medical Center
Learning Objective:
• Describe the mechanism of beta‐agonists in the treatment of refractory torsade de pointes.
Code Blue!
• 62 yo obese female, pale, diaphoretic, vomiting
• Airway is protected, breathing is labored
• Sinus bradycardia in the 50’s and blood pressure is normal
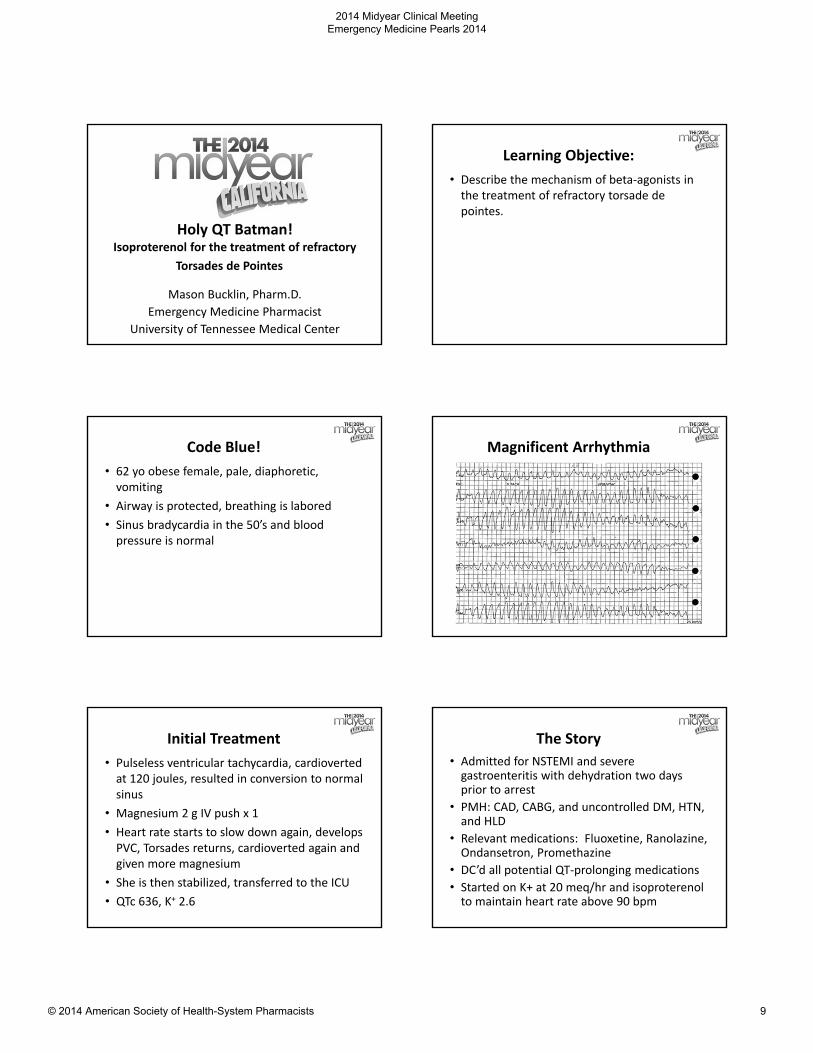
Magnificent Arrhythmia
Initial Treatment
• Pulseless ventricular tachycardia, cardiovertedat 120 joules, resulted in conversion to normal sinus
• Magnesium 2 g IV push x 1
• Heart rate starts to slow down again, develops PVC, Torsades returns, cardioverted again and given more magnesium
• She is then stabilized, transferred to the ICU
• QTc 636, K+ 2.6
The Story
• Admitted for NSTEMI and severe gastroenteritis with dehydration two days prior to arrest
• PMH: CAD, CABG, and uncontrolled DM, HTN, and HLD
• Relevant medications: Fluoxetine, Ranolazine, Ondansetron, Promethazine
• DC’d all potential QT‐prolonging medications
• Started on K+ at 20 meq/hr and isoproterenol to maintain heart rate above 90 bpm
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 9
Torsades de Pointes Etiologies
Congenital
• Mutations in Na and K channels
Acquired
• Drugs
• Low Mg2+/K+/Ca2+
• Bradycardia
• MI
• Autonomic neuropathy
• HIVOmar HR, et al. Am J Emerg Med 2014;32:683.e5‐7.
Khan IA, et al. Am Heart J 2002;143:7‐14
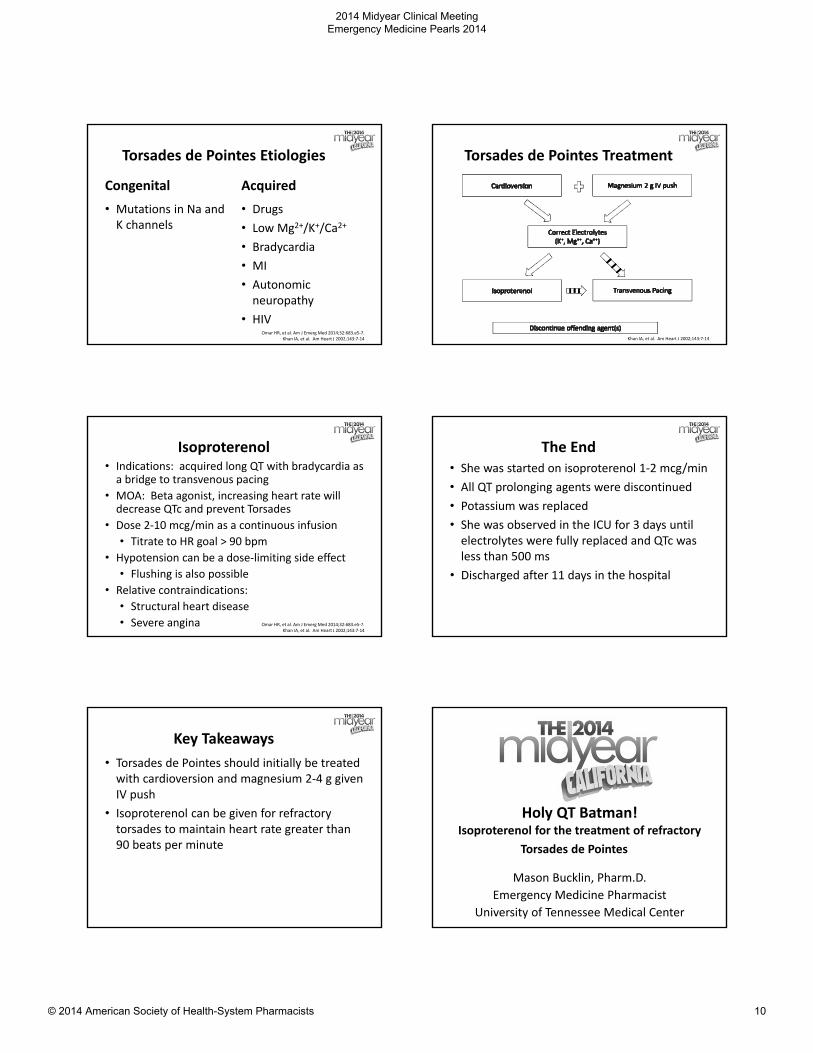
Torsades de Pointes Treatment
Khan IA, et al. Am Heart J 2002;143:7‐14
Isoproterenol• Indications: acquired long QT with bradycardia as a bridge to transvenous pacing
• MOA: Beta agonist, increasing heart rate will decrease QTc and prevent Torsades
• Dose 2‐10 mcg/min as a continuous infusion
• Titrate to HR goal > 90 bpm
• Hypotension can be a dose‐limiting side effect
• Flushing is also possible
• Relative contraindications:
• Structural heart disease
• Severe angina Omar HR, et al. Am J Emerg Med 2014;32:683.e5‐7.Khan IA, et al. Am Heart J 2002;143:7‐14
The End• She was started on isoproterenol 1‐2 mcg/min
• All QT prolonging agents were discontinued
• Potassium was replaced
• She was observed in the ICU for 3 days until electrolytes were fully replaced and QTc was less than 500 ms
• Discharged after 11 days in the hospital
Key Takeaways
• Torsades de Pointes should initially be treated with cardioversion and magnesium 2‐4 g given IV push
• Isoproterenol can be given for refractory torsades to maintain heart rate greater than 90 beats per minute
Holy QT Batman!Isoproterenol for the treatment of refractory
Torsades de Pointes
Mason Bucklin, Pharm.D.
Emergency Medicine Pharmacist
University of Tennessee Medical Center
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 10
Three ways to use a three‐way stopcock
Christopher B. Adams, Pharm.D.Emergency Medicine Clinical Pharmacist
University of California, Davis Medical Center
Learning Objective:
• Identify opportunities for improved efficiency by utilizing a three‐way stopcock.
Meet the Three‐Way Stopcock
• Commonly stocked in the ED
• Fluid directional control
• Male, female (x2)
Luer Lock system
Procedural Sedation
• Scenario:
• Preparation of multiple doses of sedation medication(s)
• Opportunity:
• Decrease waste
• Improve efficiency
Procedural Sedation Pediatric Cardiac Arrest
• Scenario:
• Expedited preparation of weight‐based unit dose medication(s)
• Opportunity:
• Simplify workflow
• Improved efficiency
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 11
Pediatric Cardiac Arrest Complex IV Administration
• Scenario
• patient requiring many simultaneous continuous infusion medications
• Opportunity
• Improved efficiency
Meet the Manifold
PatientFluids
Med 1 Med 2 Med 3
Summary
Thank You!
Christopher B. Adams, Pharm.D.Emergency Medicine Clinical Pharmacist
University of California, Davis Medical Center
A Case for Confusion: Valproic acid (VPA) induced hyperammonemic
encephalopathy (VHE)
Tony J. Casanova PharmDEmergency Department Pharmacist Specialist
Franciscan Health System
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 12
Learning Objective:
• To understand the symptoms of patients presentating with valproic acid induced hyperammonemic encephalopathy.
Consider:
A patient presents to your Emergency Department with the assistance of a local medic unit. The report given by the medics was that this individual is a “30 yr. old male, acting very strange, intoxicated, vomiting, tachycardic and probably high on something.”
…Everything is medication related until proven otherwise
VHE Signs and Symptoms
• Lethargy
• Impaired consciousness
• Focal neurological signs
• Disorientation
• Aggression
• Ataxia
• Vomiting
• Mental status changes
• Increased seizure frequency
• Sedation
• Confusion
• Somnolence
• Stupor
• Coma
• Death
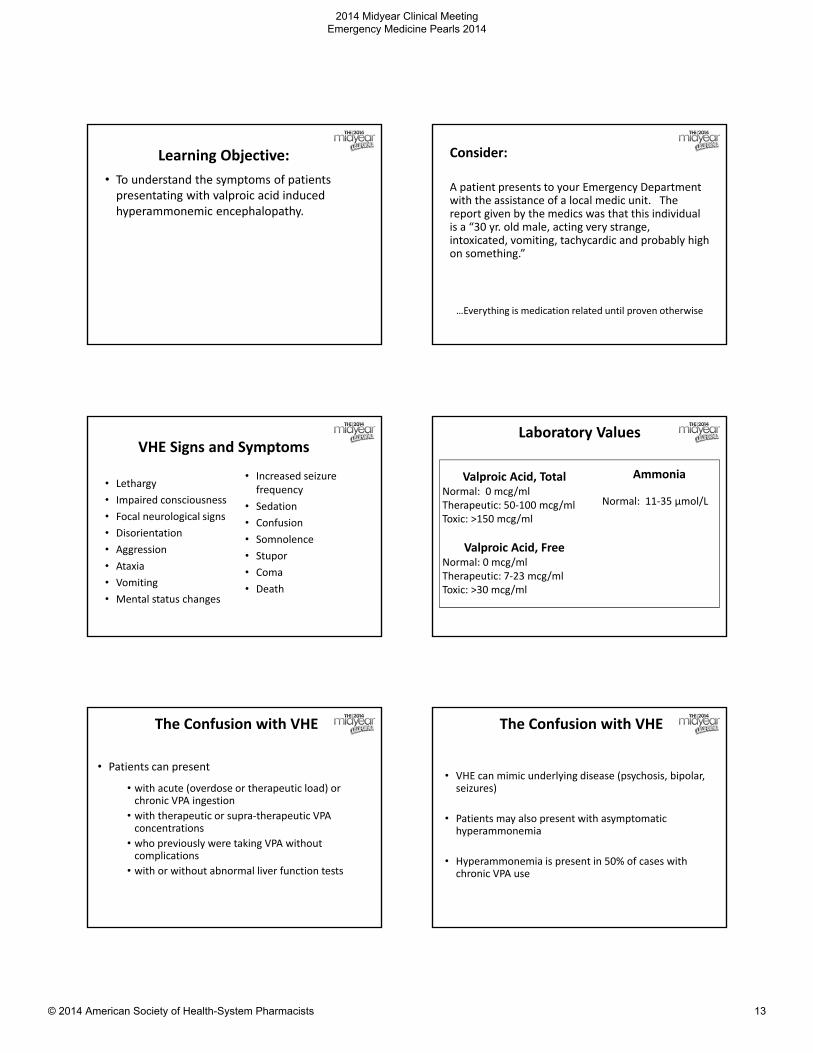
Laboratory Values
Valproic Acid, TotalNormal: 0 mcg/mlTherapeutic: 50‐100 mcg/mlToxic: >150 mcg/ml
Valproic Acid, FreeNormal: 0 mcg/mlTherapeutic: 7‐23 mcg/mlToxic: >30 mcg/ml
Ammonia
Normal: 11‐35 µmol/L
The Confusion with VHE
• Patients can present
• with acute (overdose or therapeutic load) or chronic VPA ingestion
• with therapeutic or supra‐therapeutic VPA concentrations
• who previously were taking VPA without complications
• with or without abnormal liver function tests
The Confusion with VHE
• VHE can mimic underlying disease (psychosis, bipolar, seizures)
• Patients may also present with asymptomatic hyperammonemia
• Hyperammonemia is present in 50% of cases with chronic VPA use
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 13
VHE Risk Factors
Non‐Medication Related
• Urea cycle disorders
• Malnourishment or catabolic state
• Renal failure
• Hypoalbuminemia
• L‐Carnitine deficiency
• Abnormal liver function
Medication Related
• Increased doses of VPA
• Concomitant
• Phenytoin
• Phenobarbital
• Topiramate
• Risperidone
• Clozapine
• Acetazolamide
VHE MOA
• Several proposed mechanisms…
• Multifactorial
• Renal
• VPA increases uptake of glutamine (leading to ammonia production)
• Hepatic
• VPA and its metabolites decrease free carnitine, acetyl CoA, and coenzyme A, as well as decrease and inhibit N‐acetyl glutamate and carbamoyl phosphate synthetase, which both play a role in the urea cycle
• Metabolic disorders (urea cycle disorders)
• Underlying hepatic disease
VHE Key Takeaways
1) Altered mental status from VHE can be multifactorial and can often masquerade as underlying disease or substance abuse.
2) When in doubt, check a serum ammonia level.
3) Know your patients medications, everything is medication related until proven otherwise.
A Case for Confusion: Valproic acid (VPA) induced hyperammonemic
encephalopathy (VHE)
Tony J. Casanova PharmDEmergency Department Pharmacist Specialist
Franciscan Health System
Valproic Acid: The Not‐So‐Good, The Bad, and The UglyAimee Mishler, PharmDMaricopa Medical Center
Emergency Medicine Pharmacist
Learning Objective:
• Discuss therapeutic treatment for valproic acid overdose.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 14
Case• “30 yr. old male, acting very strange, intoxicated, vomiting, tachycardic and probably high on something.”
• Confused, lethargic, able to protect airway, responsive with verbal and painful stimuli, GCS 14
• Vitals: BP: 138/72, HR: 83, O2 sat: 100%
• Labs:• AST/ALT: 35/42 units/L
• Albumin: 3.4 g/dL
• INR: 1
• Ammonia: 150µg/dL
• Valproic acid: 103mcg/mL
Lab Findings in VHE
• Hyperammonemia: serum ammonia >80µg/dL
• AST/ALT and markers of hepatic synthetic function can be normal
• Valproic acid levels can be within normal range
VHE Treatment
• Stop and wait• Immediate discontinuation of VPA
• Time
• Supplementation with L‐Carnitine for serum ammonia metabolism
• Decrease GI ammonia production, absorption & increase elimination• Consider lactulose, rifaximin, metronidazole
• Other Therapy
• Consider naloxone
VHE Treatment
• Lactulose• Inhibits diffusion of NH3 into blood by causing NH3NH4
+
which draws NH3 from tissue
• Osmotic effect on colon promoting peristalsis
• Rifaximin or metronidazole• Target ammonia producing bacteria in GI tract
• Naloxone• May act as a GABA antagonist or inhibit postsynaptic
GABA transport
Valproic Acid and Carnitine
• VPA depletes carnitine stores
• Valproylcarnitine and valproyl‐CoA formed
• Valproylcarnitine decreases reabsorption of free carnitine
• Decreases synthesis of carnitine
• Blocks carnitine transport into the cell
• Low carnitine ω‐oxidation
• Carnitine deficiency impairs urea cycle accumulation of ammonia
L‐Carnitine Supplementation
• Recommend supplementation in exposure to VPA:
– Ammonia >100µg/dL with no symptoms
– Ammonia >80µg/dL with symptoms
– Pediatrics presenting with VPA overdose
• Symptomatic patients
– 100mg/kg IV (6g max) over 30min
– Maintenance dose: 15mg/kg IV q4h over 10‐30min
• Asymptomatic patients
– 100mg/kg/day (3g/d max) PO divided q6h
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 15
Valproic Acid: The Not‐So‐Good, The Bad, and The UglyAimee Mishler, PharmDMaricopa Medical Center
Emergency Medicine Pharmacist
Time for another brief Q&A session!
A Chilling Debate - Medication Use in Hypothermic Arrest
Gabrielle L. Procopio, PharmD
Emergency Medicine Clinical Pharmacist
Hackensack University Medical Center
Learning Objective:
• Discuss medication use during hypothermic cardiac arrest
Physiologic Effects of Mild to Moderate Hypothermia by System
95
System Temp Effect
Endocrine < 35°C ↓ insulin sensi vity, ↓ insulin secre on,↑ fat metabolism
Musculoskeletal 34 ‐ 36°C Shivering
Metabolic < 35°C ↓ metabolism,↓ oxygen consump on
Hematologic ≤ 35°C Impaired platelet aggrega on, ↑ clo ng mes
Renal/electrolytes < 35°C ↑ urine output, ↑ loss of electrolytes, ↓ CrCl,tubular dysfunction
Cardiovascular < 30°C< 34°C< 34°C< 35°C
Ventricular tachycardia (VT), VF, atrial fibrillation Prolonged PR, QRS, and QT intervalsSinus bradycardia↓ Cardiac output
Arpino PA, et al. Pharmacotherapy. 2008 Jan;28(1):102‐11.
Cardiac Arrest Medications in Hypothermia
96
Medication PK Properties Potential Effects
Epinephrine Metabolism• Hepatically metabolized by MAO and
catechol‐O‐methyl transferase (COMT)Excretion
• Excreted through urine as mainly inactive metabolites
‐May accumulate due to decreasedmetabolism
Vasopressin Metabolism• Hepatically and really metabolized
Excretion• Excreted ~5 ‐ 15% through urine unchanged
‐May accumulate due to decreasedmetabolism
Amiodarone Distribution• Vd ~60 L/kg
Metabolism• Hepatically – extensive with CYP3A4 / 2C8
Excretion• Primarily biliary
‐May accumulate due to decreasedmetabolism‐Large Vd, may heighten action if cannot distribute
Lexicomp Online, Pediatric and Neonatal Lexi‐Drugs Online, Hudson, Ohio: Lexi‐Comp, Inc.; 2014; March 20, 2014.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 16
Guideline Comparison
97
Intervention American Heart
Association
European Resuscitation
Council
Basic life support Same as
normothermic algorithm
Same as
normothermic algorithm
Drug administration
• Initiation Same as
normothermic algorithm
Withhold cardioactive drugs
until temp > 30˚C
• Interval between
doses
Same as
normothermic algorithm
Doubled for temp 30 ‐ 35˚C
• Standard protocol
use
Same as
normothermic algorithm
Once temp > 35˚C
Defibrillation Same as
normothermic algorithm
If VT/VF persists after 3 shocks,
delay further attempt until temp
> 30˚C
Soar J, et al. Resuscitation. 2010 Oct;81(10):1400‐33. VandenHoek TL, et al. Circulation. 2010 Nov 2;122(18 Suppl 3):S829‐61.
What’s the Data?!
• Data is mostly limited to case reports and animal studies, which don’t talk about the drugs
• Most case reports and studies have not evaluated effect of continuous doses of ACLS drugs
• 2014 case report 8mg epinephrine over ~2 hours
• Clinical evidence to support holding arrest drugs until a certain temperature is reached is lacking
WARM THEM UP!
98Meyer M, et al. J Thorac Cardiovasc Surg. 2014 Jan;147(1):e1‐2.
Key Takeaway Points
• Remember hypothermia is your H aggressive rewarming
• There may be a potential for drug accumulation due to decreased enzymatic activity during the hypothermic state
• Normothermic ACLS treatment algorithm should be followed per AHA guidelines, as clinical evidence to support holding arrest drugs until a certain temperature is reached is lacking
99
A Chilling Debate - Medication Use in Hypothermic Arrest
Gabrielle L. Procopio, PharmD
Emergency Medicine Clinical Pharmacist
Hackensack University Medical Center
The Errors We Make…
Zlatan Coralic, PharmD, BCPS
University of California San Francisco
Learning Objective:
• Discuss the most common cognitive errors clinical pharmacist are prone to when working in the emergency department.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 17
Good diagnostics
Best available evidence
Search for cognitive errors
The reasonable decision
+ +
Emergency Medicine Decision Making: Critical Choices in Chaotic Environments
Cognitive Errors
• Commission bias
• Omission bias
• Instant gratification bias
Heuristics Skill Errors
• Slips
• Memory Lapses
“Clinical decision making is built on experience ‐foundation of experience is the mistakes we made”
– S. Weingart, P. Wyer
The Errors We Make…
Zlatan Coralic, PharmD, BCPS
University of California San Francisco
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 18
"Adventures in drug diversion: What you can get in five minutes or less"
Philippe Mentler PharmD BCPSPharmacy Implementation Manager
VHA Inc.
Learning Objective:
• The audience will be able to discuss different methods of drug diversion in the ED including ways to spot, monitor and prevent it.
Drug Diversion in Health Care
• Up to 15% Healthcare workers misuse during career
• Opioid and benzodiazepine abuse is more common than in general population
• Easy access and constant exposure
• Presumed “knowledge” of medications
• Job stress and dissatisfaction
Crit Care Med 2007:35(2):S106-116, PharmD Purch Prod 2012;11(7):10--14
Drug Diversion in Health Care
• Drug diversion carries significant risks
• Impaired healthcare worker
• Inadequate pain control for patients
• Infection Risk
• 2012: 45 patients contract Hepatitis C from worker siphoning fentanyl
Mayo Clin Proc. n July 2014;89(7):878‐887
Diversion tactics
• Pocketing waste
• Stealing from Sharps Bin
• Siphoning IV drug and replacing with other solution
• Other tactics…
Drug Diversion
• Limit Automated Dispensing Machine (ADM) access
• Actually following waste/witness policies
• Education
• Camera surveillance
• Specialty disposal bins
• Create a Diversion Response teamhttp://www.health.state.mn.us/patientsafety/drugdiversion/divroadmap
041812.pdf
Preventing diversion
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 19
Recognizing Diversion
• Anyone could be diverting
• Think outside the box
• Consider this case…
CASE: “Those aren’t the 512’s”
• Frequent flyer presents with abd pain
• Oxycodone/APAP prescribed
• RN gives the patient this tablet
• Highly skilled RN with 8+ years at the index hospital. A favorite of the staff.
• Pt complains, “I want the 512’s, that pill doesn’t work”
• Meanwhile…
http://pillbox.nlm.nih.gov/pillimage/search.php
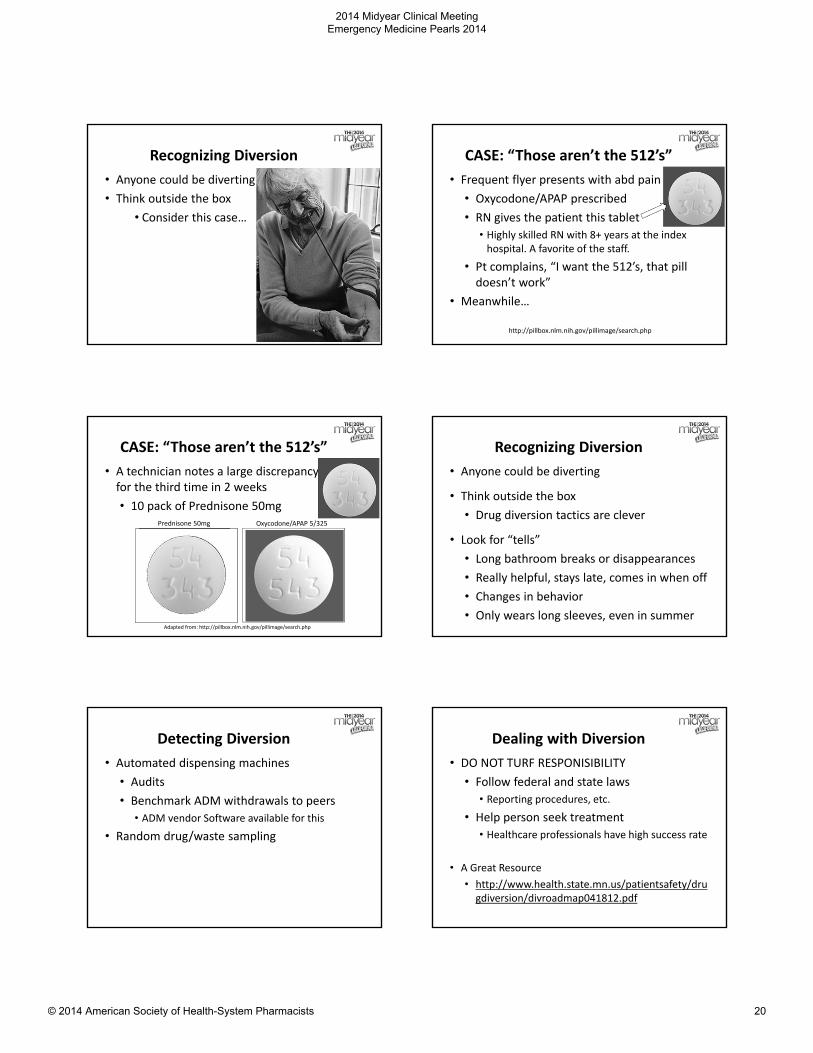
CASE: “Those aren’t the 512’s”
• A technician notes a large discrepancy for the third time in 2 weeks
• 10 pack of Prednisone 50mg
Adapted from: http://pillbox.nlm.nih.gov/pillimage/search.php
Prednisone 50mg Oxycodone/APAP 5/325
Recognizing Diversion
• Anyone could be diverting
• Think outside the box
• Drug diversion tactics are clever
• Look for “tells”
• Long bathroom breaks or disappearances
• Really helpful, stays late, comes in when off
• Changes in behavior
• Only wears long sleeves, even in summer
Detecting Diversion
• Automated dispensing machines
• Audits
• Benchmark ADM withdrawals to peers
• ADM vendor Software available for this
• Random drug/waste sampling
Dealing with Diversion
• DO NOT TURF RESPONISIBILITY
• Follow federal and state laws
• Reporting procedures, etc.• Help person seek treatment
• Healthcare professionals have high success rate
• A Great Resource
• http://www.health.state.mn.us/patientsafety/drugdiversion/divroadmap041812.pdf
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 20
References• Knight JR. A 35‐Year‐Old Physician With Opioid Dependence. JAMA.
2004;292(1):1351‐1357
• Baldisseri MR. Impaired healthcare professional Crit Care Med 2007;35(2):S106‐116
• Risks of Healthcare‐associated Infections from Drug Diversion. Accessed from: http://www.cdc.gov/injectionsafety/drugdiversion/index.html
• Berge KH, Dillon KR, Sikkink KM, Taylor TK, Lanier WL Diversion of Drugs Within Health Care Facilities, a Multiple‐Victim Crime: Patterns of Diversion, Scope, Consequences, Detection, and Prevention. MayoClinProc. 2012;87(7):674‐682
• Schaefer MH, Perz JF. Outbreaks of infections associated with drug diversion by US health care personnel. Mayo Clin Proc. June 1, 2014.
• Cross W. Addressing substance abuse in the pharmacy. Pharmacy Purchasing and Products. July 2014: 10‐14
"Adventures in drug diversion: What you can get in five minutes or less"
Philippe Mentler PharmD BCPSPharmacy Implementation Manager
VHA Inc.
When fat is your friend: Intravenous lipid emulsion in local anesthetic
toxicity
Jackie O’Connor, PharmD
PGY2 Emergency Medicine Resident
Detroit Receiving Hospital
Learning Objective
• Describe the role of intravenous lipid emulsion in the management of local anesthetic toxicity.
http://3.imimg.com/data3/CC/SY/MY‐6793224/intralipid‐100ml‐500x500.jpg
The Surprise Arrest• 50 y/o M presents to the ED after cardiac arrest during an
outpatient surgery
• PMH: diabetes
• Labs: pH 6.85, K 4.4, Ca 7.2, AST 422, ALT 413, trop <0.05
• No response from the patient
• Epi x3, vasopressin x3, atropine, dopamine given, followed by sodium bicarb, calcium gluconate
• Still no signs of ROSC…
• 2 boluses of 250mL 20% Intralipid given, followed by an IV infusion of 15 mL/kg/hr
• ROSC after the first bolus!
What Did Intralipid Do?
• Two theories for mechanism
• “Lipid sink” – Intralipid sequesters lipophilic toxins to reduce concentration in the blood
• Reversal of carnitine acylcarnitine translocase (CACT) enzyme inhibition
Am J Health‐Syst Pharm. 2011;68:125‐9.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 21
Intralipid with Local Anesthetics
• Reversal of cardiovascular or CNS toxicity
• Circulatory collapse in approximately 1/1000 peripheral nerve blocks
• First studies by Weinberg et al. in rats and dogs
• Pretreatment with Intralipid increased the lethal dose of bupivicaine
• Speeds loss of bupivicaine from cardiac tissue and accelerated recovery from asystole
Reg Anesth Pain Med. 2006;31:296‐303.
What Dose Should I Give?
• Various doses reported in case studies
• Association of Anaesthetists of Great Britain and Ireland guidelines from 2007
• 1.5 mL/kg bolus 20% ILE over 1 min
• May repeat two boluses q5min
• 15 mL/kg/hr infusion 20% ILE
• Max rate 30 mL/kg/hr
Assc Anaesthetists of Great Britain & Ireland – Safety Guideline. 2010.
Can I Fix More Things with Intralipid?
• Recent review by Cave et al. found 42 published case reports of Intralipid success
• 19 local anesthetic toxicity
• 9 sedative/hypnotic toxicity
• 5 calcium channel blocker overdose
• 6 beta blocker overdose
• 3 tricyclic antidepressant overdose
• Primary indication of cardiovascular collapse or arrest refractory to other therapies
Emerg Med Australasia. 2011;23:123‐141.
Administration Considerations
• May cause false elevation of hemoglobin and methemoglobin
• Infection risk
• Thrombophlebitis
• Hypersensitivity reactions
• Consider source of lipid emulsion (egg products, etc)
J Intensive Care Med. 2014;29:59‐70.
Key Takeaways
• Intralipid can save lives in acute toxicity
• Give 1.5 mL/kg bolus over 1 min, then 15 mL/kg/hr infusion of 20% Intralipid
• Documented safety and efficacy for local anesthetic toxicity
• Likely safe and effective for other lipophilic drug overdoses Now a word from our sponsors…
And questions from you!
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 22
Reality Bites: Pharmacist Driven Rabies Protocol in the ED
Christi Jen, PharmD, BCPSClinical Pharmacist – Emergency Medicine
Banner Boswell Medical Center
Objective
• Outline a pharmacist‐driven rabies protocol in the emergency department.
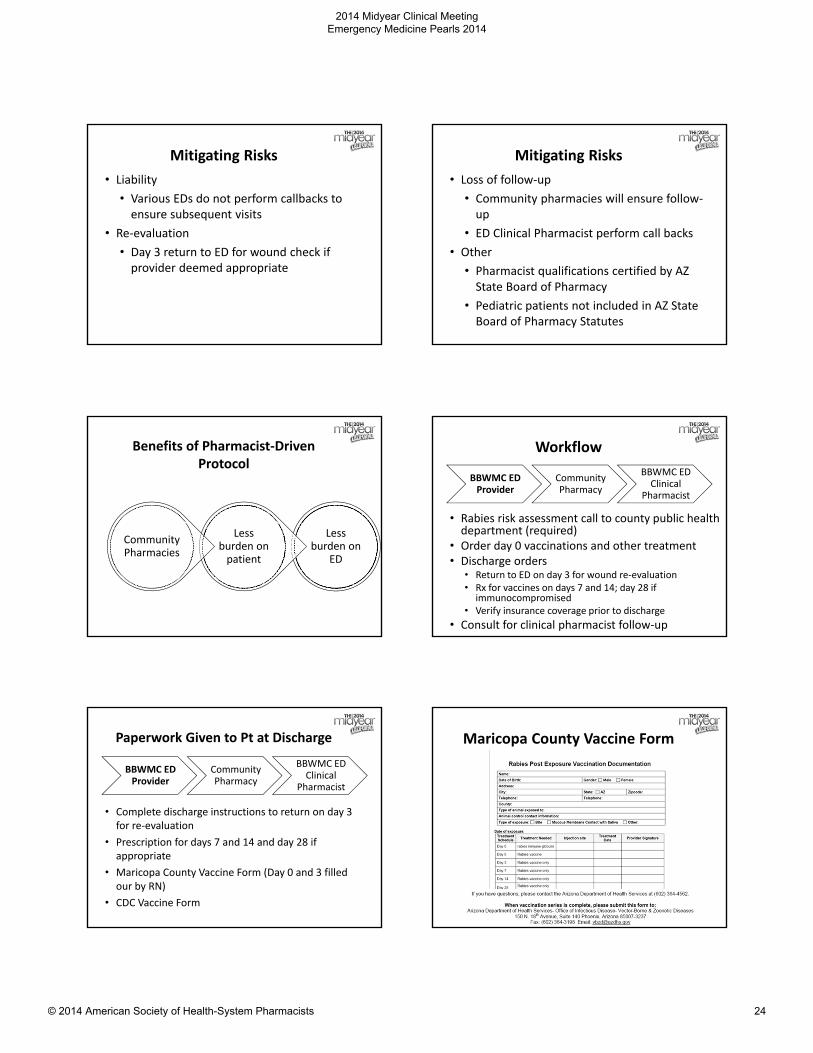
Patient Case
• CC: 68 yo female presents to the ED s/p bobcat bite
• HPI: sunbathing and fell asleep
• Woke up
• Bobcat bite to chest area
Rabies
• Virus from Mononegavirales
• Exposure to saliva or brain tissue
• Bite from a rabid animal
• Epidemiology
• Wild carnivores and bats
• > 90% wildlife
• Human cases involved organ transplant pts
• Rare
http://www.cdc.gov/rabies/location/usa/index.html
Management
Rabies immune globulin on day 0
Rabies vaccine on day 0, 3, 7, 14, 28* if immunocompromised
Tetanus vaccine
Wound management
http://www.cdc.gov/rabies/location/usa/index.html
Risks of Current Rabies Process
LiabilityRe‐
Evaluation
Loss of Follow‐Up
Other
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 23
Mitigating Risks
• Liability
• Various EDs do not perform callbacks to ensure subsequent visits
• Re‐evaluation
• Day 3 return to ED for wound check if provider deemed appropriate
Mitigating Risks
• Loss of follow‐up
• Community pharmacies will ensure follow‐up
• ED Clinical Pharmacist perform call backs
• Other
• Pharmacist qualifications certified by AZ State Board of Pharmacy
• Pediatric patients not included in AZ State Board of Pharmacy Statutes
Benefits of Pharmacist‐Driven Protocol
Less burden on
ED
Less burden on patient
Community Pharmacies
Workflow
BBWMC ED Provider
Community Pharmacy
BBWMC ED Clinical
Pharmacist
• Rabies risk assessment call to county public health department (required)
• Order day 0 vaccinations and other treatment• Discharge orders
• Return to ED on day 3 for wound re‐evaluation• Rx for vaccines on days 7 and 14; day 28 if
immunocompromised• Verify insurance coverage prior to discharge
• Consult for clinical pharmacist follow‐up
Paperwork Given to Pt at Discharge
BBWMC ED Provider
Community Pharmacy
BBWMC ED Clinical
Pharmacist
• Complete discharge instructions to return on day 3 for re‐evaluation
• Prescription for days 7 and 14 and day 28 if appropriate
• Maricopa County Vaccine Form (Day 0 and 3 filled our by RN)
• CDC Vaccine Form
Maricopa County Vaccine Form
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 24
Workflow
BBWMC ED Provider
Community Pharmacist
BBWMC ED Clinical
Pharmacist
• Receives faxed copy of the Rx for day 7 and 14
• Sets up future appointments with patient & performs reminder calls
• Performs required patient assessment via patient questionnaire
Workflow
BBWMC ED Provider
Community Pharmacist
BBWMC ED Clinical
Pharmacist
• Pharmacist administers the vaccine
• Patient education on:
• Follow‐up
• When to go to the ER
• How to report adverse drug reaction
• After each dose given & completion of series, staff to fax vaccine form to Maricopa County & BBWMC ED
Workflow
BBWMC ED Provider
Community Pharmacy
BBWMC ED Clinical
Pharmacist
• Receives pharmacy consult and documents in chart
• Calls the patient to remind for future vaccine appointments as part of Daily Microbiology Follow‐Up
• Receives faxed vaccine completion report and scan into patient’s medical record
Assessment
• Call AZ Public Health or Maricopa County Disease Line
• Obtain authorization to provide vaccine
• Fax Bite Report
Treatment
• Provide vaccine and immune globulin for day 0 and 3• Provider to write Rx for day 7 and 14 for vaccine only
• Fax Rx’s to participating pharmacies on day 0
• Pt may return on day 3 for wound re‐check
Follow‐up
• Pt to follow‐up with pharmacy for subsequent vaccinations
• Clinical pharmacist to follow‐up on completion of vaccinations and document in the chart
Reality Bites: Pharmacist Driven Rabies Protocol in the ED
Christi Jen, PharmD, BCPSClinical Pharmacist – Emergency Medicine
Banner Boswell Medical Center
PharmDs Read EKGs?: Pointers to Identify the Toxicologic Patient
Libby Giesler Johnson, PharmD, BCPS
Clinical Specialist – Emergency Medicine/ Critical Care
John Peter Smith Hospital, Fort Worth, TX
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 25
Learning Objective:
• Describe key EKG changes associated with toxic ingestions.
Patient Case #1
56 year old female56 year old female
• Chief complaint: altered mental status
PMHPMH
• Depression, HTN
VitalsVitals
• BP 112/74 HR 85 RR 13
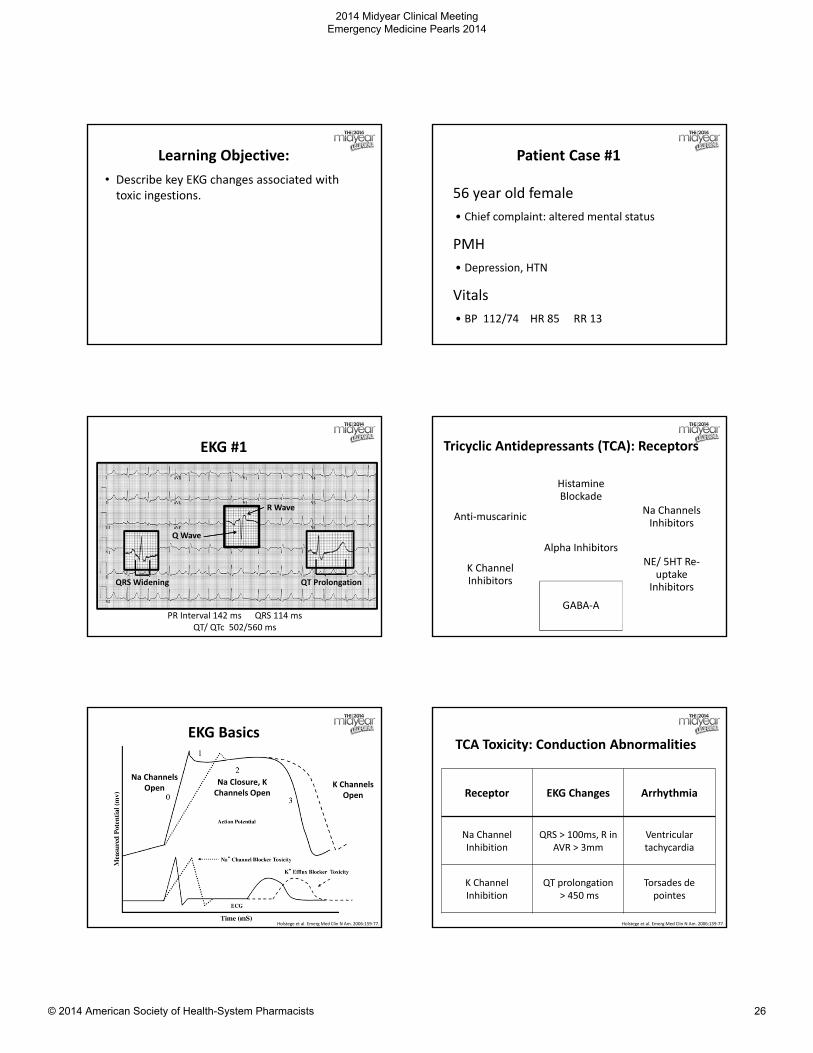
EKG #1
PR Interval 142 ms QRS 114 msQT/ QTc 502/560 ms
Q Wave
R Wave
QT ProlongationQRS Widening
Tricyclic Antidepressants (TCA): Receptors
Anti‐muscarinic
Histamine Blockade
Na Channels Inhibitors
K Channel Inhibitors
Alpha InhibitorsNE/ 5HT Re‐
uptake Inhibitors
GABA‐A
EKG Basics
Holstege et al. Emerg Med Clin N Am. 2006:159‐77.
Na Channels Open K Channels
Open
Na Closure, K Channels Open
TCA Toxicity: Conduction Abnormalities
Receptor EKG Changes Arrhythmia
Na ChannelInhibition
QRS > 100ms, R in AVR > 3mm
Ventricular tachycardia
K Channel Inhibition
QT prolongation> 450 ms
Torsades de pointes
Holstege et al. Emerg Med Clin N Am. 2006:159‐77.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 26
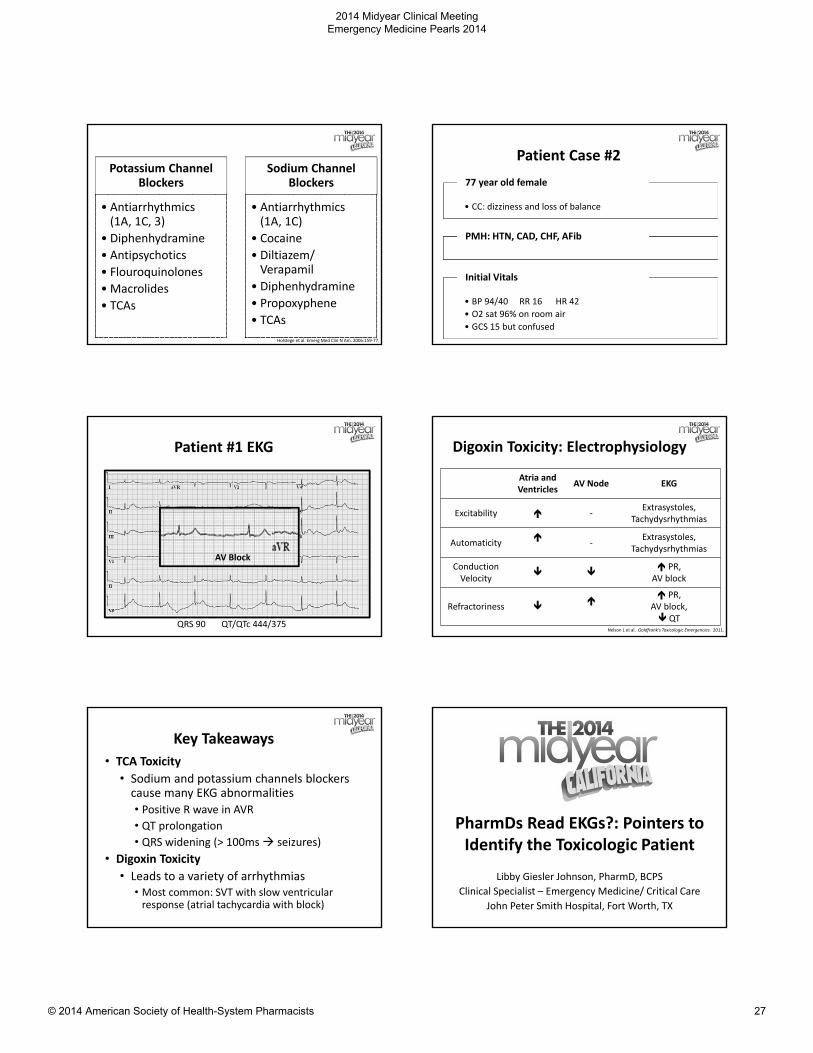
Potassium Channel Blockers
• Antiarrhythmics(1A, 1C, 3)
• Diphenhydramine
• Antipsychotics
• Flouroquinolones
• Macrolides
• TCAs
Sodium Channel Blockers
• Antiarrhythmics(1A, 1C)
• Cocaine
• Diltiazem/ Verapamil
• Diphenhydramine
• Propoxyphene
• TCAs
Holstege et al. Emerg Med Clin N Am. 2006:159‐77.
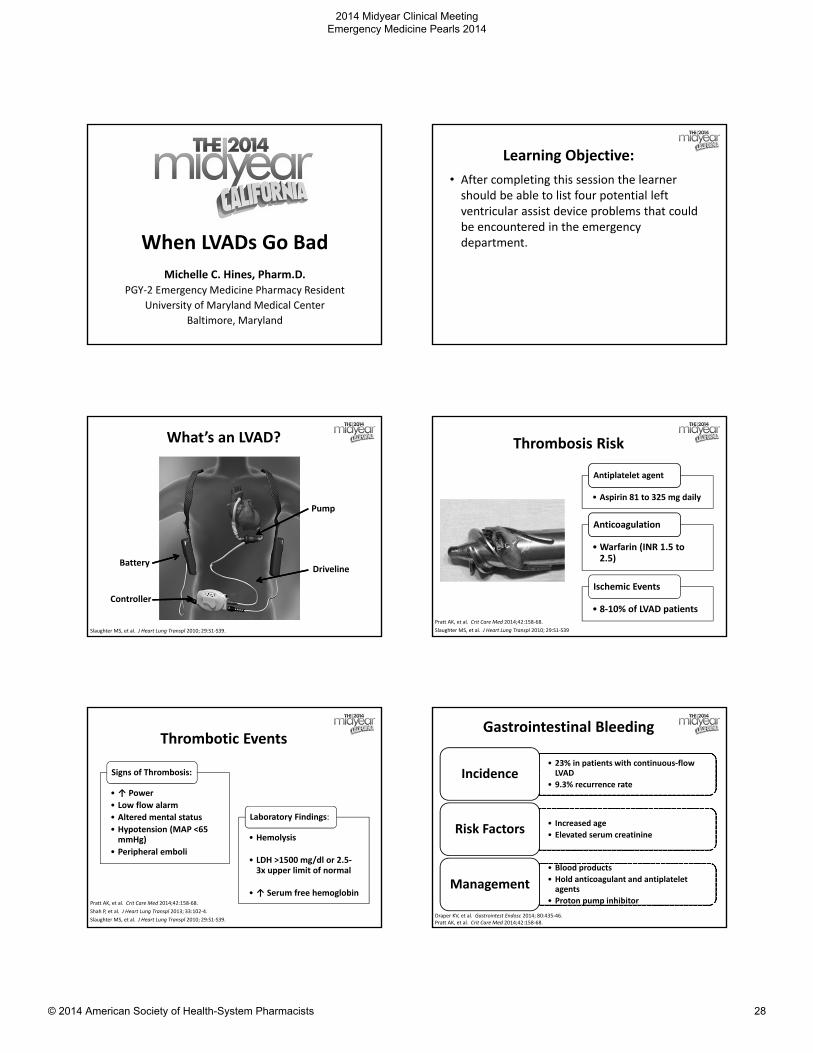
Patient Case #2
• CC: dizziness and loss of balance
77 year old female
PMH: HTN, CAD, CHF, AFib
• BP 94/40 RR 16 HR 42
• O2 sat 96% on room air
• GCS 15 but confused
Initial Vitals
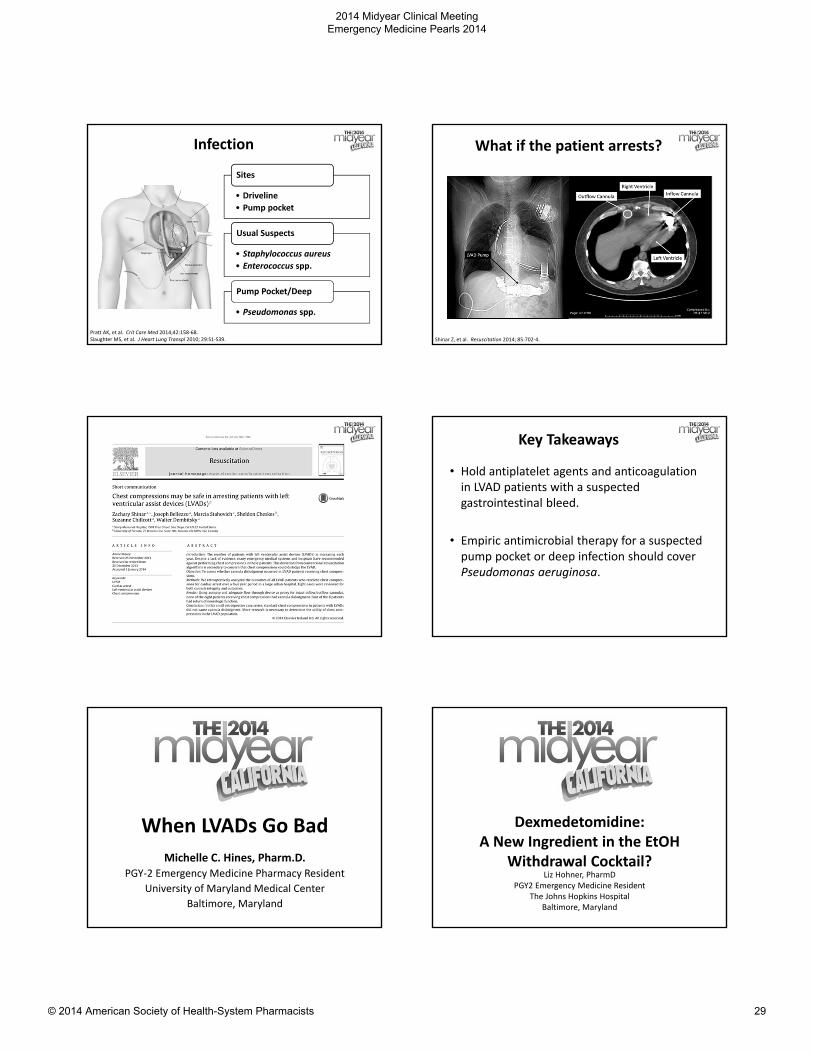
Patient #1 EKG
QRS 90 QT/QTc 444/375
AV Block
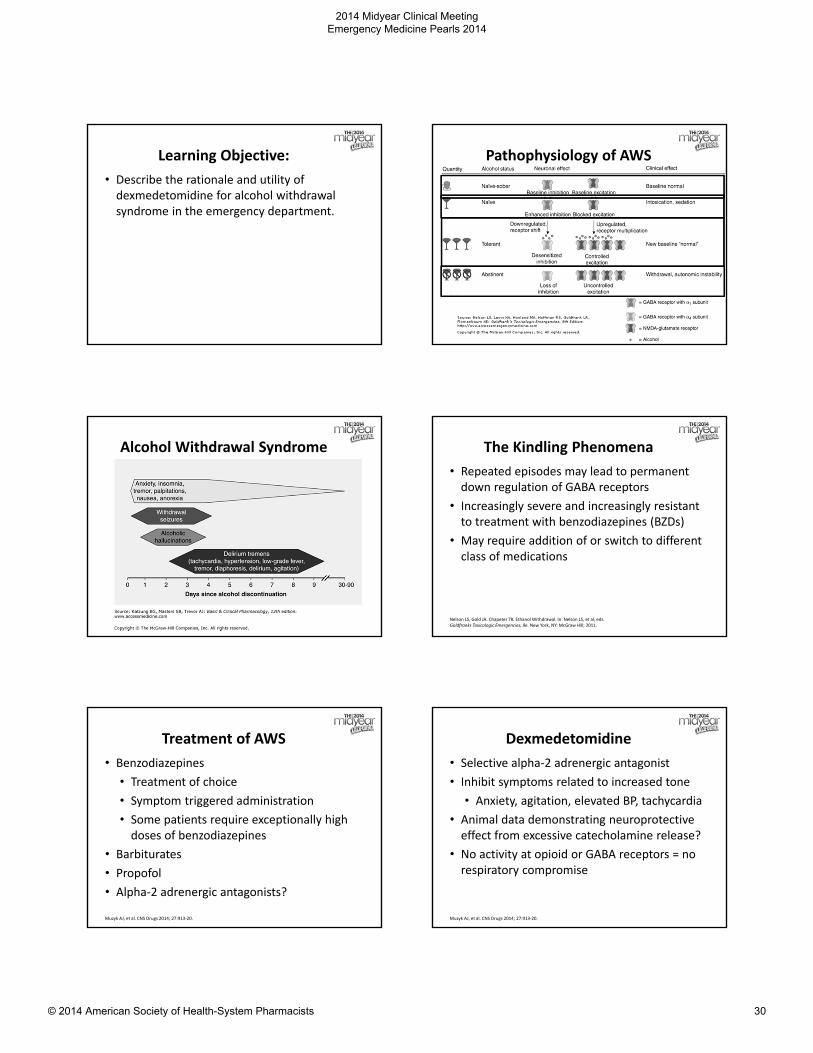
Digoxin Toxicity: Electrophysiology
Nelson L et al. Goldfrank’s Toxicologic Emergencies. 2011.
Atria and Ventricles
AV Node EKG
Excitability ‐Extrasystoles,
Tachydysrhythmias
Automaticity
‐Extrasystoles,
Tachydysrhythmias
Conduction Velocity
PR,
AV block
Refractoriness
PR, AV block, QT
Key Takeaways
• TCA Toxicity
• Sodium and potassium channels blockers cause many EKG abnormalities
• Positive R wave in AVR• QT prolongation • QRS widening (> 100ms seizures)
• Digoxin Toxicity
• Leads to a variety of arrhythmias• Most common: SVT with slow ventricular response (atrial tachycardia with block)
PharmDs Read EKGs?: Pointers to Identify the Toxicologic Patient
Libby Giesler Johnson, PharmD, BCPS
Clinical Specialist – Emergency Medicine/ Critical Care
John Peter Smith Hospital, Fort Worth, TX
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 27
When LVADs Go Bad
Michelle C. Hines, Pharm.D.PGY‐2 Emergency Medicine Pharmacy Resident
University of Maryland Medical Center
Baltimore, Maryland
Learning Objective:
• After completing this session the learner should be able to list four potential left ventricular assist device problems that could be encountered in the emergency department.
What’s an LVAD?
Slaughter MS, et al. J Heart Lung Transpl 2010; 29:S1‐S39.
Battery
Pump
Driveline
Controller
Thrombosis Risk
Pratt AK, et al. Crit Care Med 2014;42:158‐68.
Slaughter MS, et al. J Heart Lung Transpl 2010; 29:S1‐S39
• Aspirin 81 to 325 mg daily
Antiplatelet agent
•Warfarin (INR 1.5 to 2.5)
Anticoagulation
• 8‐10% of LVAD patients
Ischemic Events
Thrombotic Events
• ↑ Power
• Low flow alarm
• Altered mental status
• Hypotension (MAP <65 mmHg)
• Peripheral emboli
Signs of Thrombosis:
• Hemolysis
• LDH >1500 mg/dl or 2.5‐3x upper limit of normal
• ↑ Serum free hemoglobin
Laboratory Findings:
Pratt AK, et al. Crit Care Med 2014;42:158‐68.
Shah P, et al. J Heart Lung Transpl 2013; 33:102‐4.
Slaughter MS, et al. J Heart Lung Transpl 2010; 29:S1‐S39.
Gastrointestinal Bleeding
• 23% in patients with continuous‐flow LVAD
• 9.3% recurrence rateIncidence
• Increased age
• Elevated serum creatinineRisk Factors
• Blood products
• Hold anticoagulant and antiplateletagents
• Proton pump inhibitor
Management
Draper KV, et al. Gastrointest Endosc 2014; 80:435‐46.Pratt AK, et al. Crit Care Med 2014;42:158‐68.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 28
Infection
• Driveline
• Pump pocket
Sites
• Staphylococcus aureus
• Enterococcus spp.
Usual Suspects
• Pseudomonas spp.
Pump Pocket/Deep
Pratt AK, et al. Crit Care Med 2014;42:158‐68. Slaughter MS, et al. J Heart Lung Transpl 2010; 29:S1‐S39.
What if the patient arrests?
Shinar Z, et al. Resuscitation 2014; 85:702‐4.
Key Takeaways
• Hold antiplatelet agents and anticoagulation in LVAD patients with a suspected gastrointestinal bleed.
• Empiric antimicrobial therapy for a suspected pump pocket or deep infection should cover Pseudomonas aeruginosa.
When LVADs Go Bad
Michelle C. Hines, Pharm.D.PGY‐2 Emergency Medicine Pharmacy Resident
University of Maryland Medical Center
Baltimore, Maryland
Dexmedetomidine: A New Ingredient in the EtOH
Withdrawal Cocktail?Liz Hohner, PharmD
PGY2 Emergency Medicine ResidentThe Johns Hopkins Hospital
Baltimore, Maryland
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 29
Learning Objective:
• Describe the rationale and utility of dexmedetomidine for alcohol withdrawal syndrome in the emergency department.
Pathophysiology of AWS
Alcohol Withdrawal Syndrome
Muzsyk
The Kindling Phenomena
• Repeated episodes may lead to permanent down regulation of GABA receptors
• Increasingly severe and increasingly resistant to treatment with benzodiazepines (BZDs)
• May require addition of or switch to different class of medications
Nelson LS, Gold JA. Chapeter 78. Ethanol Withdrawal. In: Nelson LS, et al, eds. Goldfranks Toxicologic Emergencies, 9e. New York, NY: McGraw Hill; 2011.
Treatment of AWS
• Benzodiazepines
• Treatment of choice
• Symptom triggered administration
• Some patients require exceptionally high doses of benzodiazepines
• Barbiturates
• Propofol
• Alpha‐2 adrenergic antagonists?
Muzyk AJ, et al. CNS Drugs 2014; 27:913‐20.
Dexmedetomidine
• Selective alpha‐2 adrenergic antagonist
• Inhibit symptoms related to increased tone
• Anxiety, agitation, elevated BP, tachycardia
• Animal data demonstrating neuroprotectiveeffect from excessive catecholamine release?
• No activity at opioid or GABA receptors = no respiratory compromise
Muzyk AJ, et al. CNS Drugs 2014; 27:913‐20.
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 30
Dexmedetomidine• Mostly case reports and retrospective cohorts; few prospective randomized trials
• Conducted in non‐emergency department settings
• May impair ability to administer appropriate BZD treatment as DEX blunts symptomatic assessment
• Large range of infusion rates reported:
• 0.2 – 4.6 mcg/kg/min
• No clear benefit in decreasing rates of intubation or improving outcomes
Foster C, et al, Crit Care Med 2012; 40: Suppl 1.Tolonen J, et al. Eur J Emerg Med 2013; 20:425‐7.Mueller SW, et al. Crit Care Med 2014; 42:1131‐9.Crispo AL, er al. Pharmacother 2014; 34:910‐7.
Dexmedetomidine vs. Placebo
Mueller
Study Design
In addition to CIWA‐triggered lorazepam: ‐ DEX 1.2 mcg/kg/hr (high dose)‐ DEX 0.4 mcg/kg/hr (low dose) ‐ Placebon = 24
Results ‐ No significant difference in:• 7 day lorazpam requirements• Patients with severe CIWA score at 24 hrs
‐ Four patients with DEX experience bradycardia
Conclusion Adjunctive DEX may help to controls symptoms of AWS but has no significant effect on long‐term lorazepamrequirements with a CIWA‐triggered protocol.
. Mueller SW, et al. Crit Care Med 2014; 42:1131‐9.
Clinical Outcomes with DEX Study Design
Continuous infusion BZD (lorazepam or midazolam) or DEX in addition to standard medical therapyn = 61
Results ‐ No significant differences in:• Respiratory distress requiring intubation• Alcohol withdrawal seizures• Intermittent BZD requirements
‐ Significantly more patients with DEX experienced bradycardia and hypotension
Conclusion DEX did not result in decreased rates of intubation or alcohol withdrawal seizures. DEX may decrease BZD requirements which could put patients at risk for alcohol withdrawal seizures.
.Crispo AL, er al. Pharmacother 2014; 34:910‐7.
Key Takeaways• Key Takeaway #1
• Benzodiazepines are the backbone of therapy for AWS
• Key Takeaway #2
• Dexmedetomidine has limited data in AWS that does not suggest any improvement in outcomes
• Key Takeaway #3
• Use of dexmedetomidine is discouraged until further data is available
Last minute questions? Thank you!
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 31
Tarred and Feathered
Christopher J. Edwards, PharmD, BCPS
Clinical Pharmacy Specialist – Emergency Medicine
The University of Arizona Medical Center – Tucson AZ
What is Hot Tar
• Mixture of organic compounds
• Primarily 3 to 40 ringed polynucleararomatic hydrocarbons
• Used often for roofing and paving
• Viscosity decreases at higher temperatures
• Industrial applications often maintain temperatures up to 560oF
Options for Removal?
• Manual removal using a scrub brush and forceps
• PAINFUL!
• Non‐polar organic solvents
• What do we have in the hospital?
• Various ointments and creams
• Light mineral oil
• Soap and water• Emulsifying agents
• Polysorbates (e.g. Tween‐80)
Case
• 38 year old male was carrying a bucket of hot tar to a roof when he tripped.
• Both arms coated with a thick layer of black tar except for the areas where burned skin had begun to peel
Time for Science!
• N of 1, unblinded, parallel, cross over study
• Used light mineral oil, then soap and water on the right arm
• Thick layer of bacitracin, then soap and water on the left arm
• No statistical analyses were performed
• Both agents were effective at removing tar from the patient
• Subjectively, mineral oil worked faster and with less effort in application
Aftercare
• After the tar has been removed, the extent of injury secondary to burns should be assessed
• Patient will likely need to follow up in burn clinic
2014 Midyear Clinical Meeting Emergency Medicine Pearls 2014
© 2014 American Society of Health-System Pharmacists 32