Embed Size (px)
Citation preview
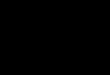
T O : T H E S U P E R I N T E N D E N TN A T A L S P R U I T H O S P I T A L
C O N S E N T T O S U P P L Y C O N F I D E N T I A L M E D I C AL R E P O R T
N A M E O F P A T I E N T
H O S P I T A L R E F E R E N C E N O
D A T E OF T R E A T M E N T
I, the u n d e r E i g n e d i
do h e r e b y r e q u e s t and a u t h o r i z e y o u to g i v e a m e d i c a l r e p o r t o n the i n j u r i e s s u s t a i n e d and t r e a t m e n t r e c e i v e d by me, and to s u p p l y c o p i e s of all m e d i c a l r e c o r d s , x - r a y s and r e c o r d s of any o t h e r f o r m o f t r e a t m e n t to : -
T H E S T A T E A T T O R N E Y 8 8 8 R O Y A L S T . M A R Y’S B U I L D I N G
8 5 E L O F F S T R E E T P R I V A T E B A G X9 J O H A N N E S B U R G
as a m a t t e r of u r g e n c y .
I h a v e f u l l y c o n s i d e r e d the i m p l i c a t i o n s of m y a c t i o n s and a u t h o r i z e y o u to g i v e all my m e d i c a l r e c o r d s to my legal r e p r e s e n t a t i v e s or a n y p r i v a t e d o c t o r t h e y m a y a d v i s e m e to see,
S I G N E D at this the ^ ' ^ d a y of
A S W I T N E S S E S : -
S .
'J ) js J s ± v ± d i^O F C O N S E N T E E
OR R I G H T H A N D T H U M B
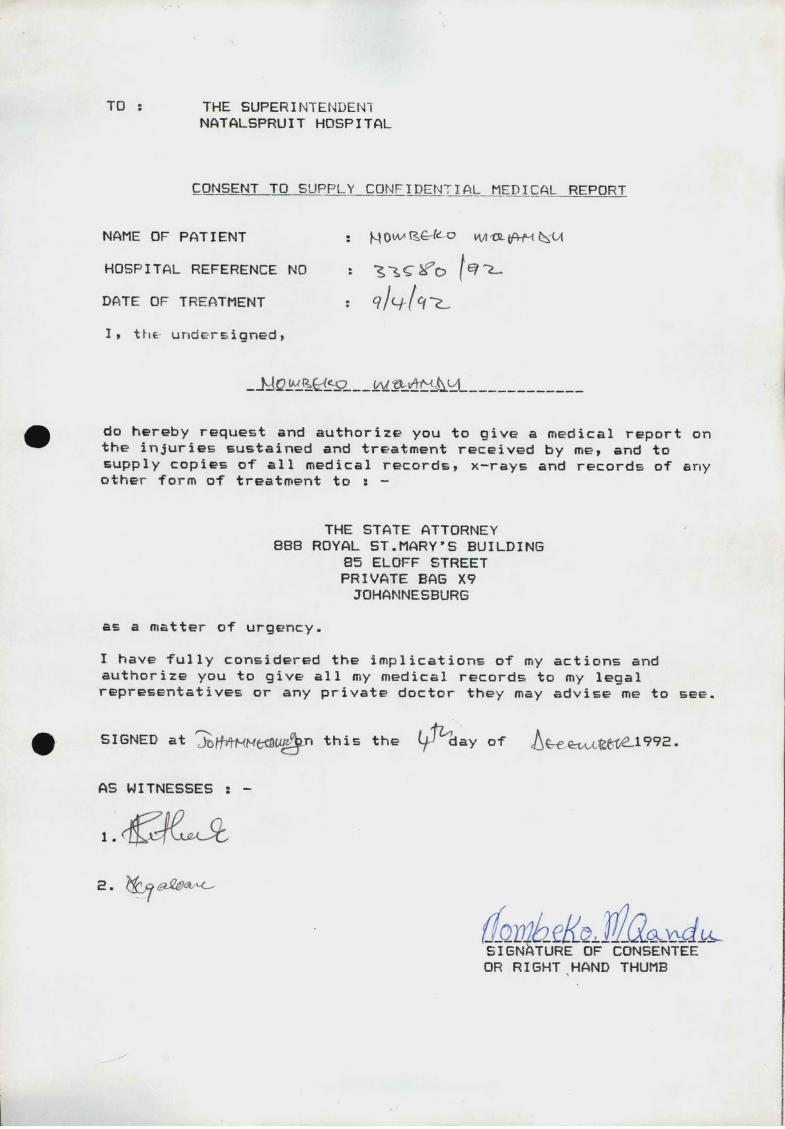
PH 466 IN THE SUPREME COURT OF SOUTH AFRICA (UITUATERSRAND LOCAL DIVISION)
In the matter between t -
MNQANDU, Nombeko
AND
THE MINISTER OF LAW AND ORDER
REPLY TO NOTICE IN TERMS OF RULE 36<4>
BE PLEASED TO TAKE NOTICE that the P l a i n t i f f h e r e b y a t t a c h e s
r e l e v a n t m e d i c a l r e c o r d s as r e q u e s t e d by the D e f e n d a n t .
day of D E C E M B E R 1992.
N fC H O L L S 7~C AMBAN f B i S U D A N OP L A I N T I F F S’ A T T O R N E Y S 2 3 R D FLOOR, K I N E C E N T R E 1 +1 C O M M I S S I O N E R S T R E E T J O H A N N E S B U R G REF : V S / P P / 4 6
A N D TO : S T A T E A T T O R N E YD E F E N D A N T’S A T T O R N E Y S8 T H F L O O R , R O Y A L S T .M A R Y ’S BLD G8 5 E L O F F S T R E E TJ O H A N N E S B U R GM R .B O W E N / 6 6 7 5 / 9 2 /P5
: . R e c e i v e d c o p y h e r e o f on thisthe r^^-V^lay o f /DEC E M B E R 1992.
F O R : D E F E N D A N T’S A T T O R N E Y SU R E U R I
D A T E D at J O H A N N E S B U R G on th i s the
TO : T H E R E G I S T R A R OF THE A B O V E H O N O U R A B L E C O U R T J O H A N N E S B U R G
CASE NO « 95/56575
Plaintiff
Defendant
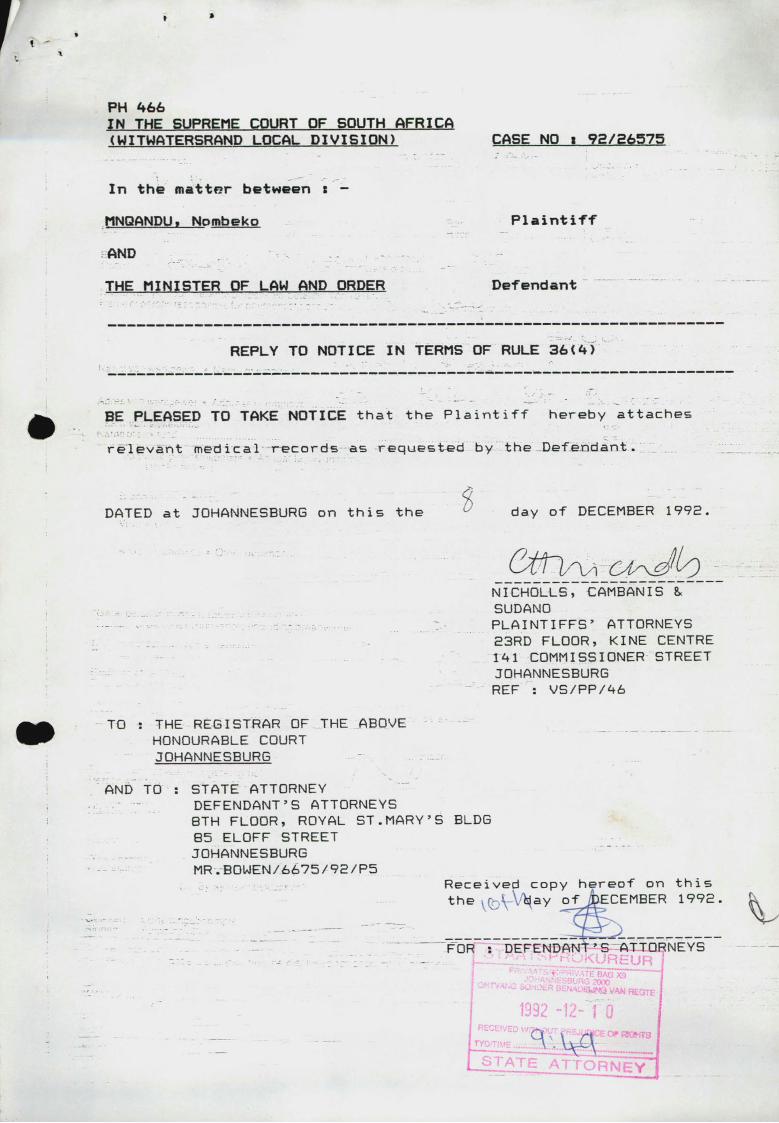
G P -S 0C-0162T.P.H. 25B
B U ITE P A S IE N TE EN /O F O N G E V A L L E AFD. • O U TP A TIE N T A N D /O R CASUALTY DEPT.
' - ........... ..................HOSPITAAL • HOSPITAL PASl£NT • PATIENT No.....
Naam voluit Name in full... \ \ W i C o
Huisadres Residential address.........”TT
/ /£- 'Z ' Foon ........................ Phone No..
g s s r . ^ M P '0 ...........................& f > . ;
Naam van persoon verantwoordelik vir betaling van rekening Name of person responsible for payment of account......................
Volgno. Serial No. %
OpgeneemAdmitted
Datum • Date VM.A.M.
NM.P.M.
M
Indeling Classification. U p
Dr..
Sy/Haar adres • His/Her address........................................................................
Naam van werkgewer • Name of employer...
Adres van werkgewer • Address of employer....
|a a m van siekefonds Kame of sick fund.......... S/F
S /FN o..'Jaarlikse gesinsinkomste • Annual family income
Uit alle bronne From all sources
Broodwinner • Breadwinner.
Vrou • Wife.
Ander afhanklikes • Other dependants..
Totaal • Total RS I M c S b , c - / &
*Getal persone fn gesin (brooowinner ingesluit)Number of persons in household (including breadwinner)
Meld ouderdomme van afhanklikes—. . whw.w .iHmg van omariM^Kb q •---State ages of dependants................................................. . 'T '.S / ^ \ %Rede vir afhanklikheid \ / C cReason for dependence..................................................
m
* rM innfrhrw eS va«n, I 6 )aar en ouer wal selfonderhoudend is, moet uitgesluit word) J Minor cNdren 01 16 Vears and o'der who are self-supporting must be'excluded)
atum van ongelukfoesering Date of accident/injury
Persoon wat beseerde inaebring het Person who brought in theTnjured,Sy/Haar adres His/Her addressSy/Haar handtekening . .His/Her signature en v°ertuig No.. . . . — ..................................................................................... . ........................................................... and vehicle No.was beseerde: (i) Onder die invloed van drank?was injured: Underthe influence of liquor?.....................................
(ii) By sy/haar bewussyn?Conscious?......................
Geteken: Opnemingsbeampte Signed: Admitting'bfficer........
van, (J'e PaS'ent se siekte mag vir rekeningdoeleindes vrygestel word The nature of the patient’s illness may be disclosed for accounting purposes
Getuie W itness.......
DatumDate....
GetekenSigned....
{?•
KlagteComplaint..
Huidige siekte Present illness..
SLE G S VIR AFSKEURSTRO KIES FO R CO UN TER FO ILS ONLY
T.P.H. 2Z£
DatumDate Betalngs • Payments Datum
Date Betalmgs • Payments Betalings • Payments
i
< r - -
V\ \\
I»1
ili
j
11j
• r ~ ;, ( 1
i, _ - v " ■ " ‘ ii
Rekenings • Accounts
0
-
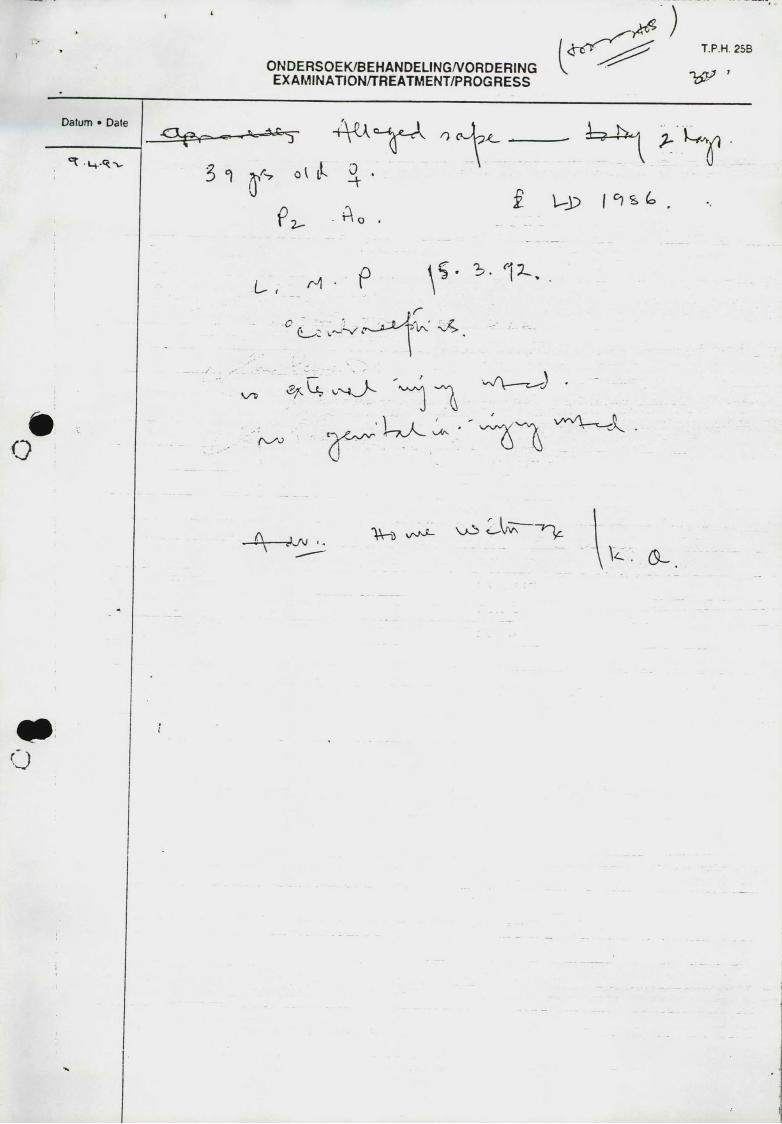
O N D E R SO EK /B EH A N D ELIN G /V O R D ER IN GE X A M IN A TIO N /TR EA TM EN T/PR O G R E SS
T.P.H. 25B
? • i - 12-.
K/T>
(L ^ :
r
~ n
w \ ------r_ < )
■ I " 7 < ~ A ~
i \ ---- ^"W-a va^ > - L . U r “’"k
t . 0 -
“ *?-r
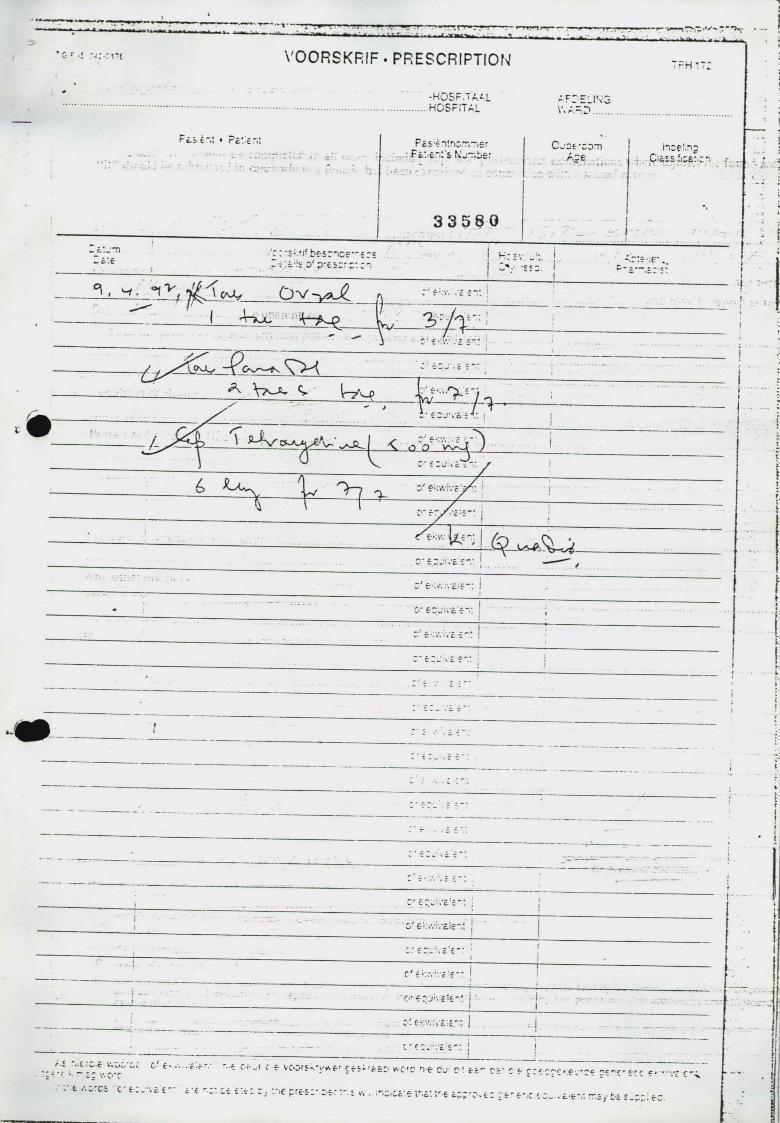
’ Gr< V O O R S K F .IF . P R E S C R IP T IO N TPH 17:
- -HbSF.TAi.LHOSriTA1 af: eli'v3
r c.S 6T»t « Pc'. c."it FcS;4i!riDTi~,er a F£.:.ev.'s Nj~bsr Cjcie'com
Aceshce!irg
• J r Cle?££:JC£:Cn f
3 3 5 8 0 : : i__t._,-n 'r: •;•.'!? be-sr"ice"£rE - c-c r-s;.s*!s p' p*esrr:p: n
<r. / r,
! H;gv 1
! .£52 i P- i
»i»
- ■ ^ V ^0' e^wiva >*
. c-‘ £:ji.c
o'e<>\\vc.-e-: \
O' ecjivc f “:
' --------------------------------------------------------- - »* I
ft
--------------- _ : * e r u ' . = ‘ r - :• ' r
T|
_ , :■ f - . = r " . —If
* t
- ’ r C *. v c £ “ . . . . . . . - r t .
c ’ (
i c ; t > ’c !£ 1 f - -
i Gr 6 * ’. * v iv £ l6 ~ t i ■ 1
eli|i- - ... . c r 5z~:\c.rz~:
•• 1 ■* * 1 •
C 'r— ------------------------------------- ------------------------------------
. * i • - * . ' * ..... " r ” " ' • <•? f T > \ r 1€ ~ * - •
...j - - - - - - - _____: .............. ' c f 6 • v 2 e r -1................................................................................. - C - f j ! . _
/ . £ . . £ . 0 . c V .C ^ C.V C-' 6 ' . . . f . r v '•■£ C r u l 0 6 V C O fS*sfV vV £ * C fS '» , f * i c W O T '
r c D * c r c n -e C J c l 7 j r P ' £ £- r- •"C C ? C * .6 . ' 'C ? 0 £ ' 'C ' £- r r f ►" " ’,*£■ r
• • '•~ r CS C ’ K w 'V c £ " c * € *"C* £.6 €\rl Z , *.ri£ p r t S C M 'S T £ v\ ' “C 'C .c '6 : lh £ * . *ir 6 c .pp o * e : r e ' e r .c ;
I 0P:5 “ “ “ ' / r f > y r,
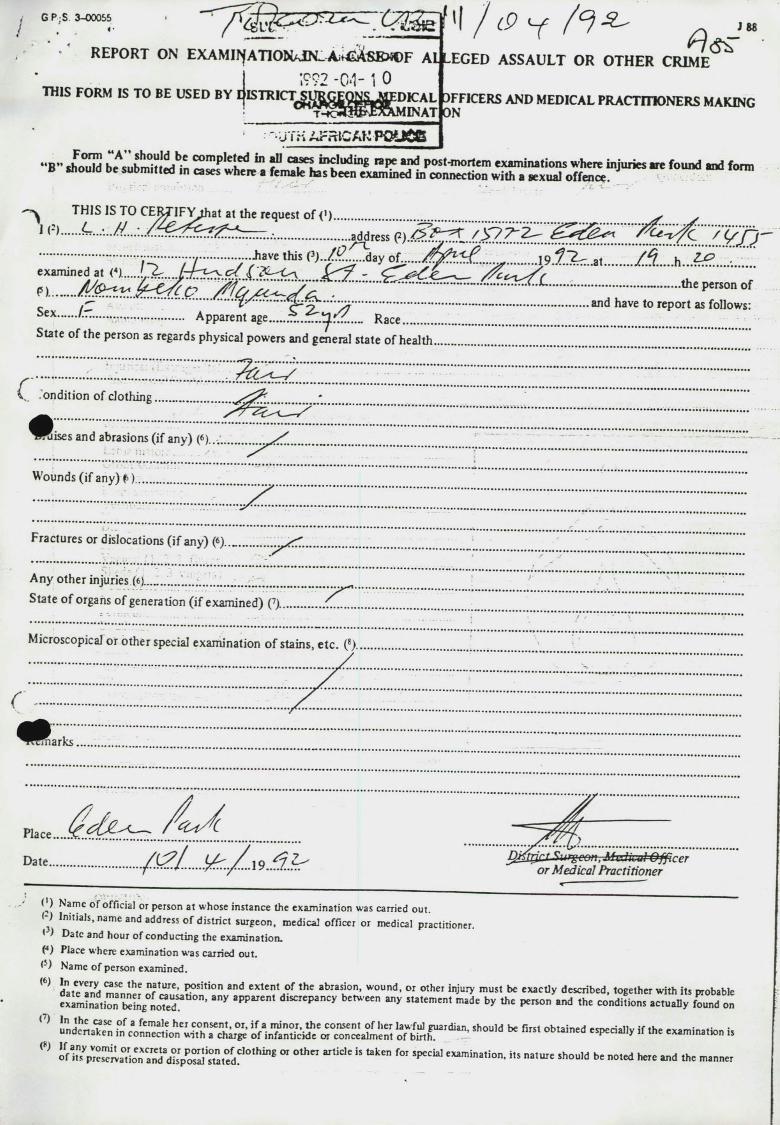
, • ‘ REPORT ON E X A M II^A T IO N A lN ^A ffiA SK W F A ^ -------- ------------------------- ^_ I ; ? ? 2 - 0 4 - 1 oTHIS FORM IS TO BE USED BY DISTRICT SURGFONSAIEDICAL
INATS i n A F n iC A K P 0 U S 6
J 88
EGED A SSA U L T OR OTHER CRIME
OFFICERS AND MEDICAL PRACTITIONERS MAKINGON
“B” should be^submined^in C L ! nf*u< ^ raPe a?^ post-mortem examinations where injuries «re found and form snou,(3 De sut,m,« « 3 ,n cases where a female has been examined in connection with a sexual offence.i • V . f T 'r‘ * • : ,'■*£. "7 "
^ THIS IS TO CER^TIFYthat at the request of <>).................................... ^ .
..... ...........................................................................
..............................y~*...... •;••/••......... ••••■have this 0 . . / £ ^ ay of.......................................... 19 .^“?— at Z f? . h •
examined at ...../ % cZ f( ' ........
P I .......■ .................................................................................................... ....................... ............................. .......... the person ofc f'Z ............* .............................................................................................................and have to report as follows:ex....../— ...... ........... ....... Apparent age.....Z..Z. R a c e ...............................................................................
State of the person as regards physical powers and general state of health................
.......................: Z : : : : : Z Z Z : Z 3 E V Z
V ondition o f clothing............— ...... .
^Ri:Rises and abrasions ( if any) («)f . : r H i " - ; . .
W ounds ( if a n y )£ ) ................................
F ractures or dislocations ( if any) (6).._ ..........
A ny o th er injuries («j....... ............................;S tate o f organs o f generation ( if exam ined) (7).. "7 ^ ‘
PlaceD a te / C ^ 7/ U ' / \ o gXtrjrt V m g ro /i , i f u c f l i u / f l / j ^ c e r ..............................i * ...... .JSm.j/....]9 ..../„... or Medical Practitioner
<’) N am « o f official or person a t w hose in stance the ex am ina tion was carried out.H Initials, name and address of district surgeon, medical officer or medical practitioner.• ) D ate and hou r o f con du ctin g th e exam ination .(4) Place where exam ination was carried ou t.
Nam e o f person exam ined.d a te T n d m anner n “ d e x te " ‘ ° f ,h e abras,>o n . w o u n d . o r o ther injury m ust be ex actly described, together w ith its probable exam ination te in g noted * d,SCrepanC>' be,w een ^ !ta tem en t m^ e by th e person and th e conditions ac tu a lly found on
undertaken ? S S f c " ^ ^ ^ “ *“ «*»» is<V) of1,7pVr° ^ ^ 7 io ^ a n d ad?s7osI]\Ta«fdCl0thlI’g “ * * * “ f° T *** '“ eX2mil'ation- “ » *hould be noted here and the manner
<6)
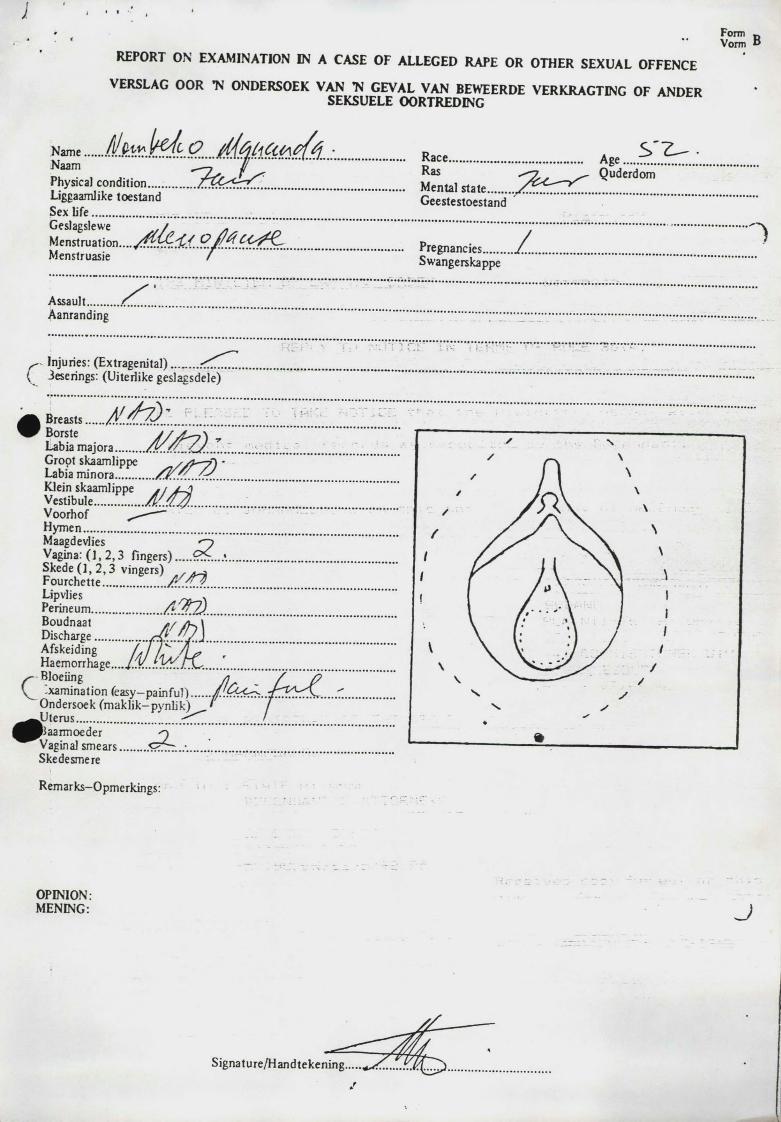
REPORT ON EXAMINATION IN A CASE OF ALLEGED RAPE OR OTHER SEXUAL OFFENCE VERSLAG OOR TC ONDERSOEK VAN TM GEVAL VAN BEWEERDE VERKRAGTING OF ANDER
SEKSUELE OORTREDING
oNaam j
Physical condition...... Ras QuderdomLiggaamlike toestand Sex Life....................... Geestestoestand
M enstruation. ® '//$Menstruasie / Swangerskappe
Assault...........r...................... • - ---- * - • ------- ----- ‘ - -
Injuries: (E xtragenital).........
B reasts......Borste j / — \
Labia majora Groot skaamlippe / /y~y) *Labia m inora.............Klein skaamlippe */ j-J)Vestibule................. /I'.'U/.............V oorhof -----Hymen MaagdevliesVagina: ( 1 , 2 ,3 fingers).....S k ed e (] , 2 ,3 vingers) , . 3F ourchette ......................Lipvlies .Perineum.........................Boudnaat / / /h>\Discharge..................Afskeiding Haemorrhage
C Bloeiing.xamination (easy—painful)
Ondersoek (m ak lik -p y n lik )J J te ru s ....................................Jiaarm oeder oVagina] sm ears.........SkedesmereRem arks-Opm erkings:
OPINION:MENING: J
Signature/Handtekening.....
TO T H E S U P E R 1 NTEUDEI'TiN A T A L S P R U I T H O S P I T A L
C O N S E N T T O S U P P L Y C O N F I D E N TI A L M E D I C AL R E P O R T
do h e r e b y r e q u e s t and a u t h o r i z e y o u to g i v e a m e d i c a l r e p o r t on the i n j u r i e s s u s t a i n e d a n d t r e a t m e n t r e c e i v e d by me, a n d to s u p p l y c o p i e s o f all m e d i c a l r e c o r d s , x - r a y s and r e c o r d s of any o t h e r f o r m of t r e a t m e n t to s -
T H E S T A T E A T T O R N E Y 8 8 8 R O Y A L S T . M A R Y’S B U I L D I N G
8 5 E L O F F S T R E E T P R I V A T E B A G X9 J O H A N N E S B U R G
as a m a t t e r of u r g e n c y .
I h a v e f u l l y c o n s i d e r e d t h e i m p l i c a t i o n s of m y a c t i o n s and a u t h o r i z e y o u to g i v e all m y m e d i c a l r e c o r d s to my legal r e p r e s e n t a t i v e s or a n y p r i v a t e d o c t o r th e y m a y a d v i s e m e to see.
N A M E OF P A T I E N T
D A T E O F T R E A T M E N T
H O S P I T A L R E F E R E N C E N O
1, tht u n d e r s i g n e d ,
S I G N E D a
A S W I T N E S S E S
S I G N A T U R E OF C O N S E N T E E O R R I G H T H A N D T H U M B
O.P.-S. 003-0055 / 0 / e © C ' K
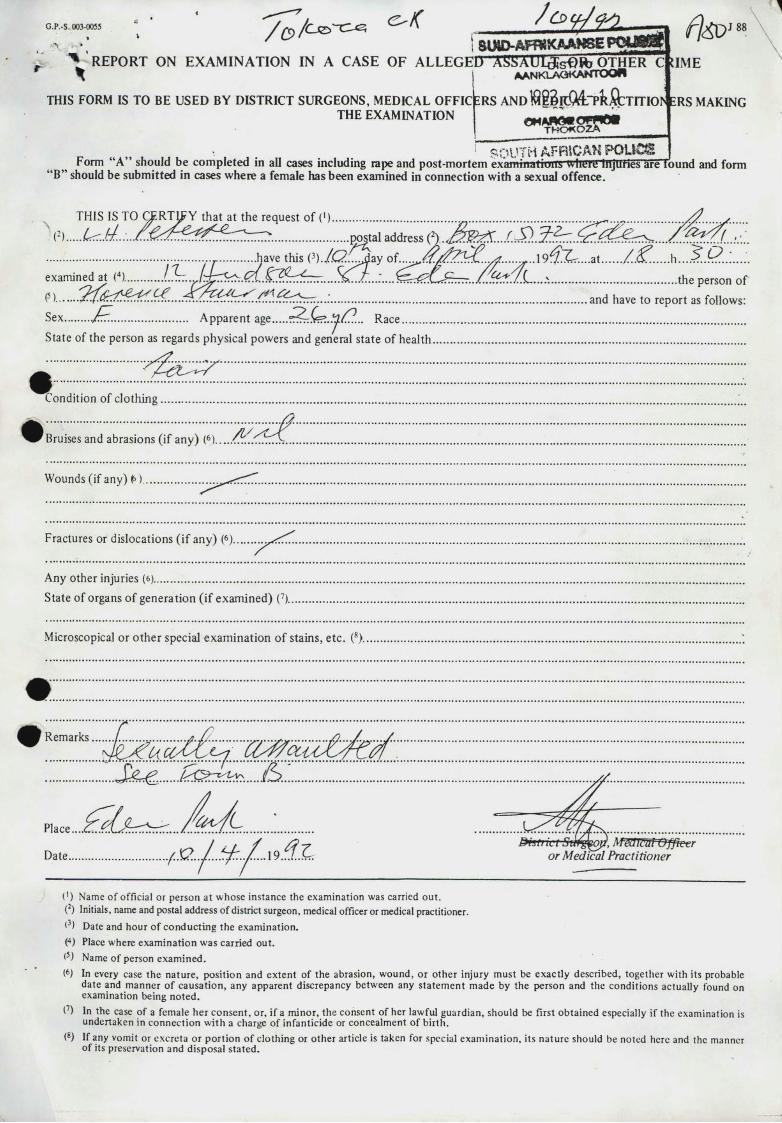
SlMD-AFf^XAAWSE P O ^ S S t\ REPORT ON EXAM INATION IN A CASE OF ALLEGED A ^A U I<*st>K > OTHER C UME
THIS FORM IS TO BE USED BY DISTRICT SURGEONS, MEDICAL OFFICTHE EXAMINATION
A A N K L A O K A N T O O f l
ERS AN D K) B l d A i " p k O l T ITIO R S MAKINGeM« £ s s s r (*
SOUTH AFRiCAK POUCS5 jForm “A” should be com pleted in all cases including rape and post-m ortem exanrinatiuns Where MjUHes are'found and form ‘B” should be subm itted in cases where a female has been examined in connection with a sexual offence.
THIS IS TO C^RTTpY that at the request o f ( ') ........................................... ........................................ ..................................(2).................................................................................................... postal address
examined at (4)............. /..Tt.. ^ .........T i . .................... .............................
Sex........ J~7............................ A pparent age.....R ace.........................................State of the person as regards physical powers and general state o f health
■posts
.................... have this ay o f . . . . ^ ^ ^ / ^ r ^ ' . y/ . . . . . .^ . .1 9 ^ Z r . . . .a t .......U+' ............................... the person of
and have to report as follows:
Condition of c lo th ing .
'Bruisesand abrasions (if any) (6) A-y
Wounds (if any) £)
Fractures or dislocations ( if any) (6)..
Any other injuries (6).................................................State of organs o f generation ( if exam ined) (7)..
Microscopical or o ther special exam ination o f stains, etc. (8)..
Remarks
S £ ^ ....................................................................
&isti a I Si&g^Ofi, M&Ilc'til Offtetr or Medical Practitioner
( ') Name o f official or person a t whose instance the exam ination was carried out.(:) Initials, name and postal address o f district surgeon, medical officer or medical practitioner.<3) Date and hour o f conducting th e exam ination.(4) Place where exam ination was carried out.Is) Name o f person exam ined.(6) In every case th e natu re , position and ex ten t o f the abrasion, w ound, o r o th er injury m ust be exactly described, together with its probable
date and m anner o f causation , any apparen t discrepancy between any sta tem en t m ade by the person and the conditions actually found on exam ination being no ted .
I1) In the case o f a female her consen t, o r, if a m inor, the consent o f her lawful guardian, should be first obtained especially if the exam ination is undertaken in connection w ith a charge o f in fanticide or concealm ent o f b irth .
(8) If any vomit or excreta o r p ortion o f clothing or o ther article is taken for special exam ination , its natu re should be noted here and the manner o f its preservation and disposal s ta ted .
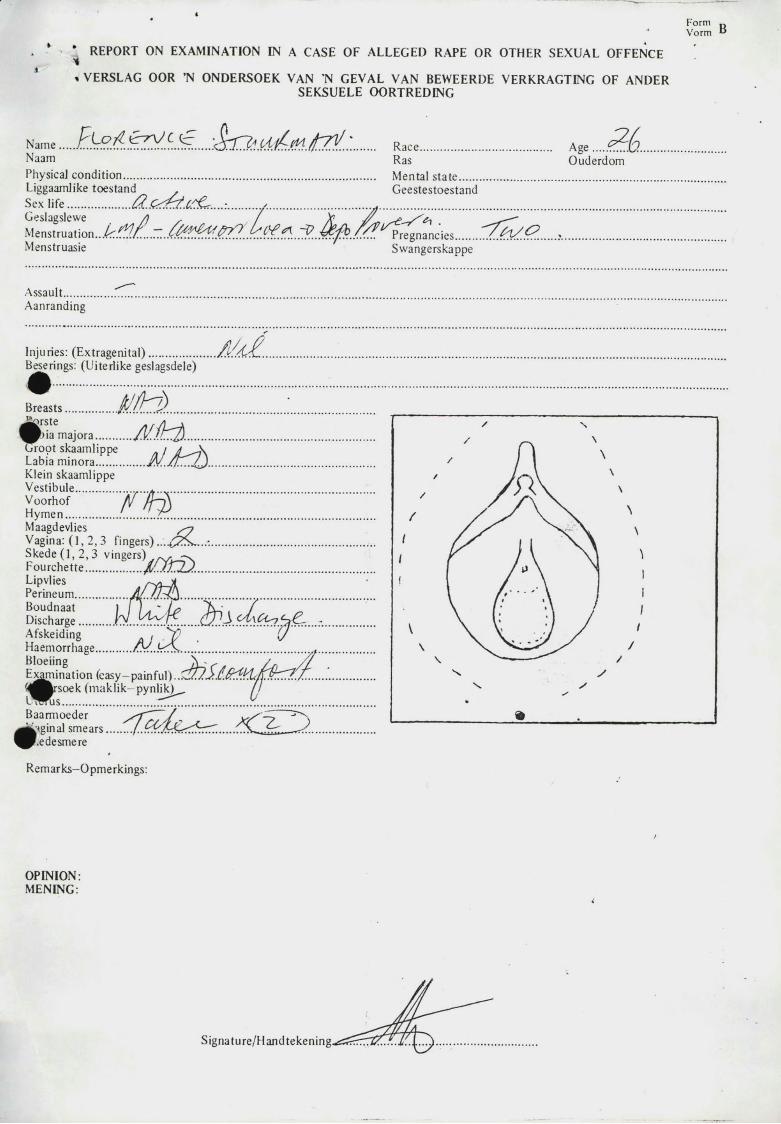
. * ’ REPORT ON EXAMINATION IN A CASE OF ALLEGED RAPE OR OTHER SEXUAL OFFENCE» VERSLAG OOR ’N ONDERSOEK VAN N GEVAL VAN BEWEERDE VERKRAGTING OF ANDER
SEKSUELE OORTREDING
* Form RVorm
N am e..... ........................................................................................................... Race............................................... AgeNaam Ras OuderdomPhysical condition.......................................................................................... Mental s ta te ..................................................................Liggaamlike toestand GeestestoestandSex life ....................../2..Q± t !.C.CC....:...........y................................... ...................................................................................................
M e n s t T u a t i o n . . . ^ . f ^ / ^ . Z . . ^ ^ ^ ^ ^ ^ . ! ^ f ^ . f ^ . . T ? . . ^ ^ . . / ^ /^ re g M n c ie s ................................... >..............................Menstruasie Swangerskappe
Assault........Aanranding
i M . .Injuries: (E xtragenital)......................^ j^ ring s: (Uiterlike geslagsdele)
Breasts.................. ................................A K V a ..........m H . ......
Groot skaamlippe /Labia m inora.................Klein skaamlippeVestibule.................... t ..............Voorhof /if If—AH ym en.................. ................................MaagdevliesVagina: ( 1 , 2 ,3 fingers) ...£ Z s....'.Skede (1, 2 ,3 vingers)Fourchette................
...............A / M ...................
£ £ £ ........ir T U k k .....h id *Afskeiding , Y 1
Ha emorrhage............BloeiingExamination (easy-painful)...'( ^ ^ « s o e k (m aklik— pynlik)
i S . T S L f e : ... . < £ 2 .^^ .e d e sm e reRemarks-Opmerkings:
OPINION:MENING:
i
Signature/Handtekening.
G.P.-S. C -005*< * 9 / 9 ^ ?;u u > a f w k a a k s e p o u s i e
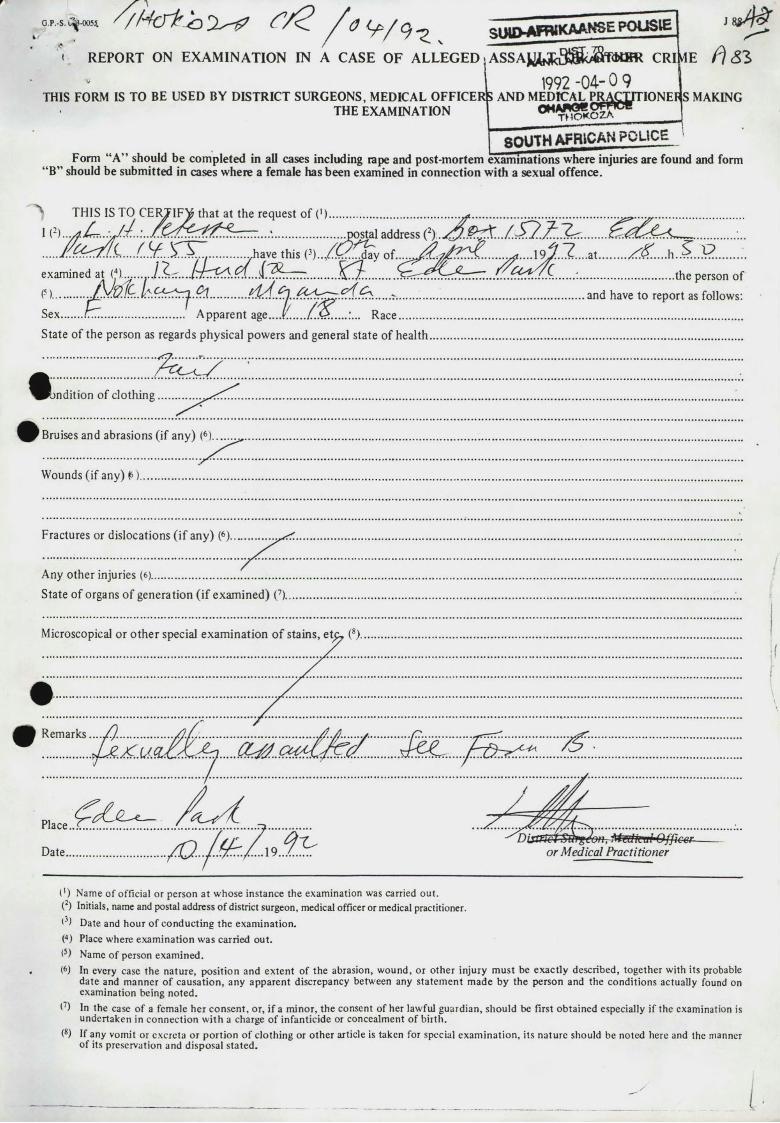
<. REPORT ON EXAM INATION IN A CASE OF ALLEGED A S S A J ^ y ^ ^ ^ K H R CRI1992 -04- 0 9
FICER|S AND MTHE EXAMINATION
THIS FORM IS TO BE USED BY DISTRICT SURGEONS, MEDICAL OFFICERS AND MEDICAL PRACTITIONERS MAKINGO M A W W p F n c t
Form “A” should be com pleted in all cases including rape and post-m ortem
T M O K O Z A
SOUTH AFRICAN POLICE
“ B” should be subm itted in cases where a female has been examined in connection w ith a sexual offence.exam inations where injuries are found and form
^ THIS IS TO C E O I F ^ tha t at the request o f ( ') ............................................. ....................................................... ...................................... 1....................................................................................................... .^postal address (2) . &?%... / .........................................................................
.......... ....,have this..................... dav o f..... .................................. J? ....a t.............................................................. ..have this (3) . . / £ _ d a y o f....^ ..u ;> « ........ ................................0 . ....................examined at (4). .y. . . .Srr..4 ' t ^ S . . Jl. .^ T T T .......... .................... ^rr:^r^r^7... ....... '...................................the person of
P)............Jy.v.iSex....... t ...............................’ A pparent age.State o f the person as regards physical powers and general state of health.
................................................................ - ...... ...........................................................and have to report as follows:........... A pparent age....r...... /..<£......:... R ace...........................................................................................................................
Fractures or dislocations ( if any) (6).
Any other injuries (6).State of organs o f generation (if exam ined) (7).
( ') Name o f official or person a t w hose instance the exam ination was carricd out.(2) Initials, name and postal address of district surgeon, medical officer or medical practitioner.t3) Date and hour o f conducting th e exam ination.(4) Place where exam ination was carried out.(5) Name o f person exam ined.(6) In every case th e natu re , position and ex ten t o f the abrasion, w ound, o r o th er in jury m ust be exactly described, together with its probable
date and m anner o f causation , any apparen t discrepancy between any sta tem en t m ade by the person and the conditions actually found on examination being noted .
(7) In the case o f a female h er consen t, or, i f a m inor, th e consent o f her lawful guardian , should be first obtained especially if the examination is undertaken in connection w ith a charge o f infanticide or concealm ent o f b irth .
(8) If any vomit or excreta or po rtio n o f c lothing or o th er article is taken for special exam ination , its natu re should be noted here and the manner o f its preservation and disposal sta ted .
I
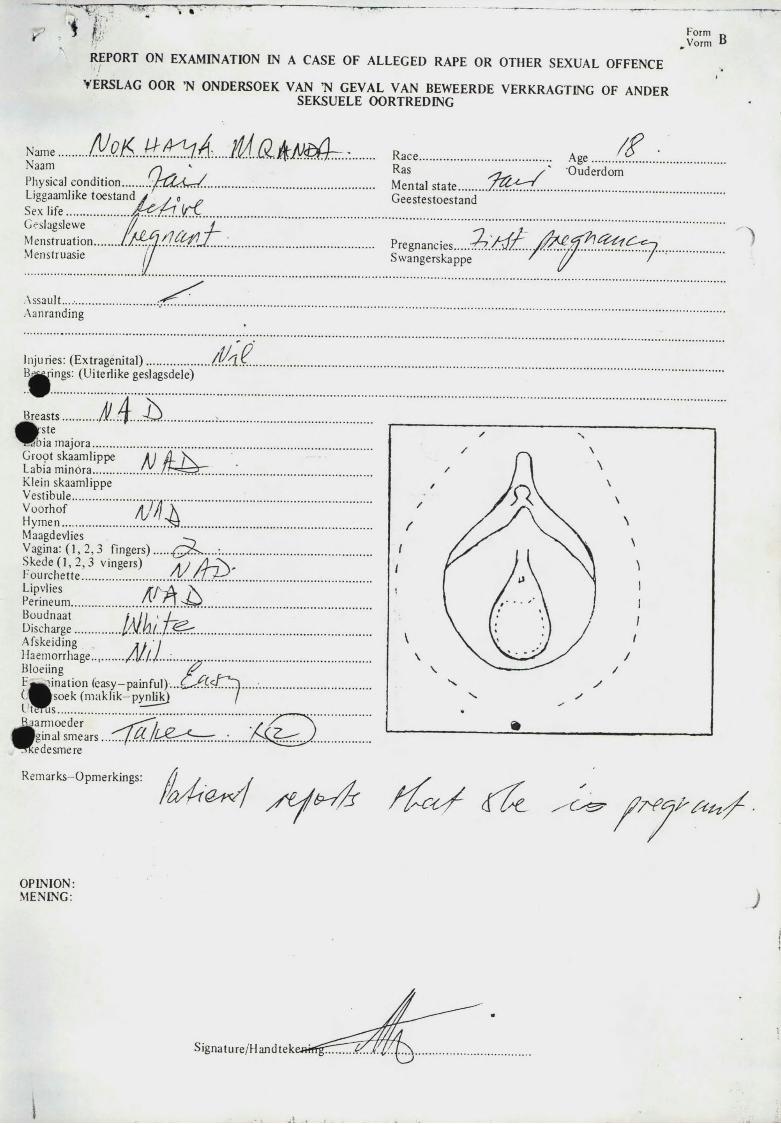
REPORT ON EXAMINATION IN A CASE OF ALLEGED RAPE OR OTHER SEXUAL OFFENCE YERSLAG OOR ’N ONDERSOEK VAN ’N GEVAL VAN BEWEERDE VERKRAGTING OF ANDER
SEKSUELE OORTREDING
Form DVorm “
N ajue..........M t A .
Q a L / ........................................
T M sjcL .......
NaamPhysical condition Liggaamlike toestand Sex life ......Ceslagslewe // /M enstruation.........Menstruasie J
Race...............................................RaS /Mental s ta te ..........Geestestoestand
Age Ouderdom
■
Pregnancies.....?.Swangerskappe
A ssault.........Aanranding
Injuries: (E xtragenital).................B ^pings: (Uiterlike geslagsdele)
Breastsf kste
lb
J M i.
& r ) . .J y .............
...........I I S I
Ml
5Dia majora.......Groot skaamlippeLabia m inora.......Klein skaamlippeVestibule...............VoorhofHym en..................MaagdevliesVagina: ( 1 , 2 ,3 fingers).............................Skede ( 1 ,2 ,3 vingers) / L S \ .Fourchette...............................LipvliesPerineum............Boudnaat l. II < /Discharge................Afskeiding / / IHaemorrhage...........All-)—-...BloeiingF j^ in a t io n (easy-painful).C .'^^so ek (m aklik -pynlik )U tm is ............................................l^iarmoeder
inal sm ears....... f.kis.Hedesmerem
Remarks-Opmerkings:
/ ^/ _ \/ j 1 \
// / A \
\\
/ N1 A s \1 r j \ V \< / ii \ ' 1
1fV I j y
//
\ ///« /
•
V \ \
OPINION:MENING:
S ig n a tu r e /H a jid te k e w f l^ T ^ T ^ ^ ^ X ^ .
I
Collection Number: AK2702 Goldstone Commission of Enquiry into PHOLA PARK Records 1992-1993 PUBLISHER: Publisher:-Historical Papers, University of the Witwatersrand Location:-Johannesburg ©2012
LEGAL NOTICES:
Copyright Notice: All materials on the Historical Papers website are protected by South African copyright law and may not be reproduced, distributed, transmitted, displayed, or otherwise published in any format, without the prior written permission of the copyright owner.
Disclaimer and Terms of Use: Provided that you maintain all copyright and other notices contained therein, you may download material (one machine readable copy and one print copy per page) for your personal and/or educational non-commercial use only.
People using these records relating to the archives of Historical Papers, The Library, University of the Witwatersrand, Johannesburg, are reminded that such records sometimes contain material which is uncorroborated, inaccurate, distorted or untrue. While these digital records are true facsimiles of the collection records and the information contained herein is obtained from sources believed to be accurate and reliable, Historical Papers, University of the Witwatersrand has not independently verified their content. Consequently, the University is not responsible for any errors or omissions and excludes any and all liability for any errors in or omissions from the information on the website or any related information on third party websites accessible from this website.
This document is part of a private collection deposited with Historical Papers at The University of the Witwatersrand by the Church of the Province of South Africa.