Embed Size (px)
Citation preview
Tobacco, Alcohol and Drug Use in Childbearing
Families
Margaret H. Kearney, PhD, RN, FAAN
© 2007, March of Dimes
Substance Abuse During Pregnancy (SAMHSA, 2005)
Based on data collected from surveys of U.S. households in 2003 and 2004:
– 18.0 percent of pregnant women reported that they smoked cigarettes.
– 11.2 percent drank some alcohol.– 4.5 percent engaged in binge drinking.– 0.5 percent engaged in heavy drinking.– 4.6 percent used some kind of illicit
drug.
© 2007, March of Dimes
Substance Abuse During Pregnancy (SAMHSA, 2005) (Continued)
• Pregnant women are less likely to use substances than their peers.
• The exception is pregnant women aged 15 to 17; this substance use rate is 26 percent for pregnant women, compared with 19.6 percent for nonpregnant women.
© 2007, March of Dimes
Substance Abuse During Pregnancy (SAMHSA, 2005) (Continued)
• Rates of substance abuse in pregnancy have stayed constant.
• Pregnant women’s tobacco use decreased from 2002 to 2004, while alcohol and illicit drug use increased (SAMHSA, 2005).
© 2007, March of Dimes
Substance Abuse During Pregnancy (SAMHSA, 2005)
Women more prone to substance abuse:– Earn below poverty level – Were exposed to violence as a child– Have a history of domestic abuse – Suffer depression or other mental health
problems– Have less than a high school education– Are unmarried– Are unemployed– Are involved with the criminal justice
system
© 2007, March of Dimes
Substance Abuse During Pregnancy (SAMHSA, 2005)
• Substance use is highest in the first trimester.
• The most common form of substance use in pregnancy is smoking among White women.
• Because tobacco, alcohol and drug use in pregnancy occurs across all demographic groups, nurses should screen all women.
© 2007, March of Dimes
The Problem of Addiction
• Addiction does not occur unless psychological and social conditions promote continued drug use.
• Nurses are better able to provide support and nonjudgmental care if they respect substance users as reasonable and intelligent persons whose judgment has been impaired.
© 2007, March of Dimes
Genetic Contributions to Addiction• The propensity to specific
addictions has been linked to particular genes.
• Genetic differences may affect the seriousness of biological consequences of substance exposure in pregnancy.
© 2007, March of Dimes
Addiction as a Biopsychosocial Problem
• Addiction is produced when biological, psychological and social predispositions combine with exposure to substances and an environment that supports regular substance use.
• Nursing assessment should focus on a broad scope of personal, familial and social stressors and coping skills.
© 2007, March of Dimes
Women’s Treatment Issues
• Women may be more predisposed to addiction than men.
• Women are adversely affected by smaller amounts of alcohol and drugs than men.
• Women are more likely than men to lack resources to pay for drug treatment.
© 2007, March of Dimes
Women’s Treatment Issues (Roberts & Dunn, 2003) (Continued)
Women’s treatment programs must take a whole-life approach and address:
– Low self-esteem– The need for social services and
parenting support– Protection from violence– Training in relationship issues and
coping skills– Vocational and legal assistance
© 2007, March of Dimes
Ethical Challenges
• A conflict exists between the woman’s right to autonomy over her body and behavior and the nurse’s sense of obligation to prevent harm to the fetus.
• If nurses are part of an enforcement system instead of advocates for women’s needs, women may avoid prenatal care and social services.
© 2007, March of Dimes
The Nurse’s Role
• In prenatal and acute care settings, nurses should:– Thoroughly assess psychosocial risks– Conduct mutual goal-setting to
minimize harm associated with psychosocial risks
– Offer support and respect
• The sense of being valued can help drug users begin to make changes.
© 2007, March of Dimes
Tobacco Use in Pregnancy: Maternal Effects
Cigarette smoking is the most common form of substance abuse in pregnancy. It is linked to:
– Decreased fertility– Spontaneous abortion– Placenta previa– Placental abruption– Ectopic pregnancy– Preterm premature rupture of
membranes (PPROM)– Preeclampsia
© 2007, March of Dimes
Tobacco Use in Pregnancy: Fetal Effects
• Impaired transfer of oxygen and nutrition
• Long-term cognitive function and increased risk of brain damage
• Chronic low-level hypoxia• Intrauterine growth restriction (IUGR) • Preterm delivery• Low birthweight (LBW) in term infants
© 2007, March of Dimes
Tobacco Use in Pregnancy: Neonatal Effects
• Impaired respiratory function in premature infants
• Low neurobehavior scores and higher withdrawal-symptom scores
• Asthma, respiratory illness and pneumonia
• Infections of the middle ear• Increased risk of cancer and SIDS
© 2007, March of Dimes
Alcohol Use in Pregnancy
There is no safe amount of alcohol consumption during pregnancy (Jones & Chambers, 1999).
© 2007, March of Dimes
Alcohol Use in Pregnancy: Maternal Effects
• Cardiovascular and liver disease• Breast and gynecological cancer• Osteoporosis• Menstrual symptoms • Neurological and mental health
problems• Compromised ability to conceive • Spontaneous abortion
© 2007, March of Dimes
Alcohol Use in Pregnancy: Fetal Effects
• Abnormalities in brain and neuron development
• Growth deficiency • Structural changes• Prematurity• LBW • Decreased length and head
circumference
© 2007, March of Dimes
Alcohol Use in Pregnancy: Neonatal Effects
• Fetal alcohol syndrome (FAS)• Mental retardation• Developmental, learning and
behavior problems
© 2007, March of Dimes
Marijuana: Maternal Effects
• Is the illicit drug most commonly used during pregnancy, although only 3.6 percent of pregnant women report using it (SAMSHA, 2005)
• Does not cause a defined physical withdrawal syndrome
• Heavy use linked to lung problems
© 2007, March of Dimes
Marijuana: Fetal and Neonatal Effects
• Does not appear to cause anomalies or serious effects on the fetus
• Does not appear to decrease intelligence
• Newborns may show increased startle response, tremors, hand-to-mouth behavior and disturbed sleep patterns.
© 2007, March of Dimes
Cocaine: Maternal Effects
• Hypertension• Tachycardia • Cardiac events and maternal death • Spontaneous abortion• Placental abruption • Premature rupture of membranes
(PROM)
© 2007, March of Dimes
Cocaine: Fetal Effects
Fetal effects of cocaine are caused by the drug’s direct effects (vasoconstriction and neuroexcitation) and by lifestyle issues that maternal drug use brings, including poor nutrition and avoidance of prenatal care.
© 2007, March of Dimes
Cocaine: Neonatal Effects• Jitteriness• Hyperactivity• Inconsolability• Poor feeding and state regulation• No physiological withdrawal:
Neonates are not dependent on cocaine and do not need medication to lessen withdrawal.
© 2007, March of Dimes
Amphetamines: Maternal Effects• Stroke• Cardiac problems • Psychiatric emergencies• Growth restriction• Placental abruption• Preterm delivery
© 2007, March of Dimes
Amphetamines: Fetal and Neonatal Effects
• Similar effects to cocaine, with decreased fetal growth
• Some researchers expect that, like with cocaine (Wouldes et al., 2004), effects can be seen early in life but are quickly overpowered by environmental factors.
© 2007, March of Dimes
MDMA (Ecstasy): Maternal Effects• Anxiety• Twitching• Depression • Impaired cognitive processing and
memory performance

© 2007, March of Dimes
MDMA: Fetal and Neonatal Effects• Animal studies do not show an
increase in harmful fetal effects. • A small, uncontrolled, retrospective
study suggests a possible increase in ventricular septal defects (Bateman et al., 2004).
• Nurses should treat infants and families based on demonstrated health needs.
© 2007, March of Dimes
Heroin: Maternal Effects
Heroin can cause severe physiological withdrawal symptoms, including fatal seizures when withheld for 12 to 48 hours.
© 2007, March of Dimes
Heroin: Treatment
• Methadone– The most common treatment for
heroin abuse in pregnant women – During pregnancy, brings addicted
women into agencies that promote prenatal care
• Buprenorphine – Linked to better treatment adherence
with fewer side effects and overdoses than methadone
© 2007, March of Dimes
Heroin: Fetal Effects
• Opiates, such as heroin, methadone and buprenorphine, have not been linked to fetal anomalies.
• Fetal withdrawal responses include arrhythmias, seizure activity and fetal demise.
© 2007, March of Dimes
Heroin: Neonatal Effects
• Drug withdrawal • Suck-swallow difficulties • Central nervous system (CNS) irritability• Gastrointestinal upset• Yawning• Sneezing• Frantic sucking with uncoordinated
feeding• High-pitched cry• Increased or decreased muscle tone
© 2007, March of Dimes
Comprehensive Psychosocial Assessment: Setting the Stage• A woman should only have to
provide sensitive personal information once, in an environment most likely to produce support and appropriate follow-up.
• The nurse should provide privacy and a comfortable setting and view the session as the beginning of an important personal relationship with the woman.

© 2007, March of Dimes
Introducing Social Issues
The nurse should begin to explore the woman’s home situation, including:
– Stress related to work, finances, family and pregnancy
– Satisfaction with the amount and kind of support in her social network
– Feelings about self-esteem and ability to cope with stressors
© 2007, March of Dimes
Three-question Substance-use Screen
• Have you ever drunk alcohol?• How much alcohol did you drink in
the month before pregnancy?• How many cigarettes did you
smoke in the month before pregnancy?
© 2007, March of Dimes
Substance Abuse Assessment• In no case should urine or blood
testing be used without consent.• If a woman admits to substance
abuse, testing is not needed to confirm the presence of a problem.
© 2007, March of Dimes
Tobacco Use Assessment
• Women generally report their smoking status fairly accurately.
• The Fagerstrom Test for Nicotine Dependence is used to assess the level of addiction to tobacco (Heatherton et al., 1991).
© 2007, March of Dimes
The Fagerstrom Test for Nicotine Dependence• How soon after you wake up do you smoke
your first cigarette?• Do you find it difficult to refrain from
smoking in places where it is forbidden?• Which cigarette would you hate most to give
up?• How many cigarettes per day do you smoke?• Do you smoke more frequently in the first
hours after waking than during the rest of the day?
• Do you smoke if you are so ill that you are in bed most of the day?
© 2007, March of Dimes
Alcohol Use Assessment
• Women are quite reliable in reporting alcohol use in pregnancy (Jacobson et al., 2002).
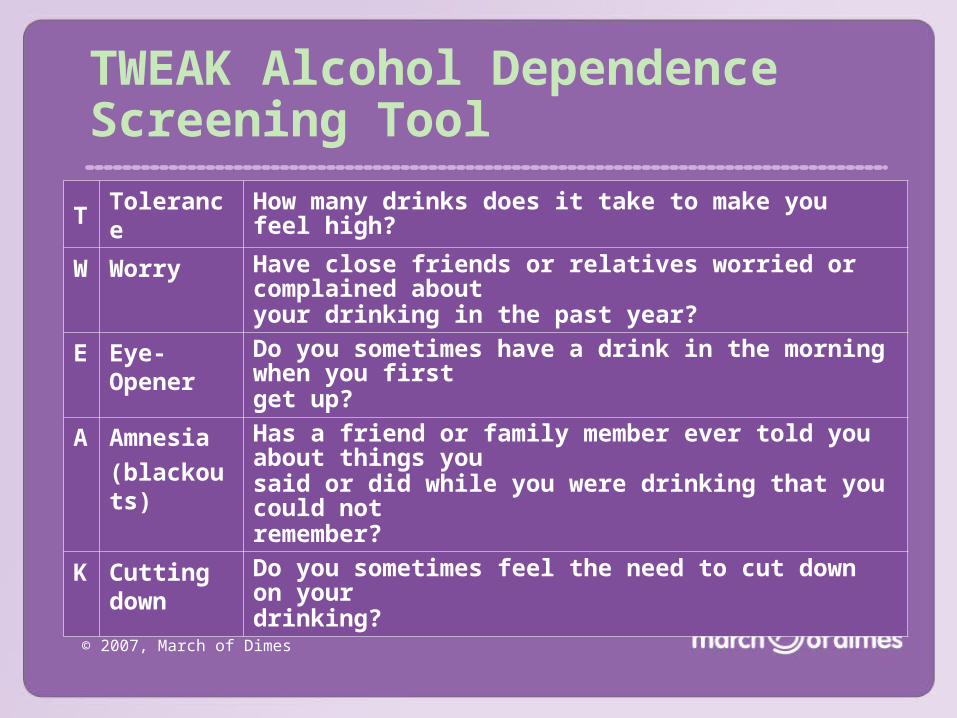
• The TWEAK is used to screen pregnant women for alcohol misuse.
© 2007, March of Dimes
TWEAK Alcohol Dependence Screening Tool
TTolerance
How many drinks does it take to make you feel high?
W Worry Have close friends or relatives worried or complained about your drinking in the past year?
E Eye-Opener
Do you sometimes have a drink in the morning when you firstget up?
A Amnesia(blackouts)
Has a friend or family member ever told you about things yousaid or did while you were drinking that you could notremember?
K Cutting down
Do you sometimes feel the need to cut down on yourdrinking?
© 2007, March of Dimes
Illicit Drug Use Assessment
• There is no standardized screening tool for illicit drug use in pregnancy.
• Most women are unlikely to admit the extent of drug use.
• Nurses should observe physical and behavioral signs that may indicate illicit drug use, and follow these over time.
© 2007, March of Dimes
Illicit Drug Use Assessment (Continued)
• Nursing assessment should focus on opening the door to further discussion and possible referral.
• Goals in prenatal settings:– To identify women at risk for
consequences of drug use– Offer continuing obstetric assessment – Provide support and resources for
further treatment
© 2007, March of Dimes
Principles of Brief Intervention:Problem Recognition and Goal-Setting1. Provide feedback on problems, symptoms
and historical events that suggest a substance abuse problem. Offer simple, realistic information about the effects on mother and baby.
2. Advise the woman to stop (or cut down) using substances.
3. Emphasize that any action taken is the woman’s choice.
4. Give options for treatment.5. Get agreement from the woman on at least
one action to take.
© 2007, March of Dimes
Follow-up During Pregnancy and Postpartum
At each visit, the nurse should:1. Ask the woman about psychosocial
issues.– Progress in reducing substance use– Use of treatment options– Health changes
2. Impart good news.
© 2007, March of Dimes
Harm Reduction
• Harm reduction is an important principle for care of substance users (MacMaster, 2004).
• When abstinence is not achieved, reducing the harm of substance use is an important goal.
© 2007, March of Dimes
Recognizing the Full Scope of the Problem
• Few substance users are able to quit on their first attempt.
• Nurses should view any progress as worthwhile and recognize that recovery is a lifelong process.
• Women need to develop entirely new social support systems.
© 2007, March of Dimes
Smoking Treatment: Stages of Change Model
1. Precontemplation: No intention of quitting
2. Contemplation: Considering quitting within 6 months
3. Action: Taking active steps to quit4. Maintenance: Maintaining
successful cessation for 6 months or more
© 2007, March of Dimes
Smoking Treatment: Self-Determination Model
• The nurse uses motivational interviewing or autonomy-promoting counseling to elicit the woman’s personal values and goals.
• The nurse and woman explore the aspects of unhealthy behavior, focusing on the discrepancy between the desired goals and the behavior.
© 2007, March of Dimes
Smoking: Brief Interventions
• Up to 40 percent of pregnant smokers quit on their own during pregnancy without intervention.
• A brief, 5-minute intervention can produce an additional 30 percent quit rate (Lerman et al., 2005).
© 2007, March of Dimes
Smoking Treatment: The Five A’s (Fiore et al., 2000)
1. Ask about tobacco use.2. Advise to quit.3. Assess willingness to quit.4. Assist in attempting to quit.5. Arrange follow-up.
The Five A’s are recommended for patients who
are willing to quit.
© 2007, March of Dimes
Smoking Treatment: The Five R’s (Fiore et al., 2000)
1. Relevance of quitting2. Risks of continued smoking3. Rewards of quitting4. Roadblocks to quitting5. Repetition
The Five R’s are recommended for patients who are unwilling to quit.
© 2007, March of Dimes
Smoking Treatment: Follow-up During Pregnancy
• One of the least expensive and most effective forms of follow-up is telephone contact.
• Follow-up should focus on how the effort is going; support and reinforcement for even small successes; suggestions to overcome obstacles; and health progress reports.
© 2007, March of Dimes
Smoking Treatment: Nicotine Replacement
• Use of nicotine replacement in pregnancy is controversial.
• Levels of nicotine in the mother’s body are lower with nicotine replacement than with smoking, and she does not ingest other toxins found in tobacco smoke.
© 2007, March of Dimes
Smoking Treatment: Bupropion (Zyban)
• Used as an antidepressant and as a smoking cessation aid
• Shows no harmful effects on pregnant women treated for depression (Kuller et al., 1996)
© 2007, March of Dimes
Smoking Treatment: Reducing Postpartum Relapse• Thirty percent to 70 percent of
smokers who quit during pregnancy relapse by 1 year postpartum (Secker-Walker et al., 1998).
• Postpartum follow-up is essential.• Nurses can offer the same tips they
gave to pregnant smokers, with emphasis on planning ahead to avoid excessive fatigue and isolation.
© 2007, March of Dimes
Alcohol and Illicit Drug Treatment: The Nurse’s Role• Work with the woman to identify
the problem and its risks.• Agree on initial steps to take.• Plan for follow-up, as needed.
© 2007, March of Dimes
Alcohol and Illicit Drug Treatment: Theoretical Frameworks• Psychodynamic insight-oriented
models• Cognitive-behavioral models • Relapse prevention
© 2007, March of Dimes
Alcohol and Illicit Drug Treatment: Treatment Formats• Outpatient counseling• Intensive outpatient treatment for 6
to 12 weeks or longer• Partial hospitalization or day
treatment• Inpatient treatment in a hospital
setting• Residential treatment for 28 days to
6 months or longer
© 2007, March of Dimes
Alcohol and Illicit Drug Treatment: Treatment Formats (Continued)
• Twelve-step and faith-based programs
• Home-visiting programs• Pharmacologic treatment• Women-oriented treatment
programs
© 2007, March of Dimes
Addiction Recovery (Kearney, 1998)
Recovery involves: – Abstinence– Self and psychological issues– Connections and relationships with
men and women, family, community and culture
© 2007, March of Dimes
Addiction Recovery (Continued)
The most intensive and woman-specific drug treatment programs have a 50 percent abstinence rate 1 year after program completion; a rate closer to 20 percent is not uncommon (Eisen et al., 1998).
© 2007, March of Dimes
Alcohol and Illicit Drug Treatment:Ongoing Support and Prenatal Care• Nurses should carefully observe
women on methadone or heroin for withdrawal symptoms and report any sudden changes in patterns of fetal movement.
• Fetal heart checks are important in the second and third trimesters.
• Providers should conduct fetal non-stress tests (NSTs) at each visit in the third trimester.
© 2007, March of Dimes
Care of the Chemically Dependent Woman in Labor
• The nurse can use the three-question substance-use screen when admitting a woman to a labor unit and ask follow-up questions, as needed.
• In general, epidural anesthesia is preferred for substance users if pain management is needed.
© 2007, March of Dimes
Interacting with Laboring Women Under the Influence of SubstancesNurses must:
– Have great patience and tolerance – Provide constant warmth and vigilance– Closely monitor maternal and fetal
well-being
© 2007, March of Dimes
Parenting Issues: Child CustodyNurses must:
– Provide accurate and realistic information to women about the risk of custody loss in the perinatal period
– Be familiar with local laws and practices
© 2007, March of Dimes
Handling Alcohol and Drug-exposed Infants
• Alcohol-exposed infants can be hypotonic or floppy and may have difficulty feeding and gaining weight.
• Cocaine-exposed infants may be rigid, irritable, resistant to holding and feeding and hard to soothe.
• Providers should use slow, gentle interactions when caring for these infants.
© 2007, March of Dimes
Feeding Alcohol and Drug-exposed Infants
Feedings should be slow and relaxed. If the baby sucks so vigorously that choking is a hazard, pause the feeding frequently, or use a bottle nipple with a smaller hole or a preemie nipple (Villarreal et al., 1992).
© 2007, March of Dimes
Soothing Alcohol and Drug-exposed Infants
• Excessive crying is a symptom of drug exposure. The infant may be soothed by:– Swaddling– Positioning on the side or back– Reducing room light and stimulation
gentle – Stroking or massage
• There may be times when nothing can be done for a crying infant.
© 2007, March of Dimes
Early Intervention and Respite Care• Providers should refer all alcohol- and
drug-exposed infants to early intervention programs.
• Social and financial services are important parts of discharge planning.
• Parents and caregivers may need respite; the nurse can help the mother arrange for alternate caregivers and support.
© 2007, March of Dimes
Promoting Positive Maternal-child Interaction
• Nurses can make a critically important contribution by working to improve the woman’s parenting knowledge and skills.
• A mother’s psychological state strongly influences her interaction with her infant (Fineman et al., 1997).
• Simple interventions can help mothers parent more effectively.
© 2007, March of Dimes
Summary
Nurses can:– Provide life-changing interventions for
vulnerable families– Advocate for increased funding for
women’s substance-abuse treatment– Work to reduce harmful stigma– Advocate for healthy environments that
reduce exposure to substances