Embed Size (px)
Citation preview
ANTICOAGULANT TOOLKIT
Reducing Adverse Drug Events &
Potential Adverse Drug Events with
Unfractionated Heparin,
Low Molecular Weight Heparins
and Warfarin

ii |
ANTICOAGULANT TOOLKIT
Reducing Adverse Drug Events & Potential Adverse Drug Events with Unfractionated Heparin, Low Molecular Weight Heparins
and Warfarin
Developed by Purdue University PharmaTAP in collaboration with the Indiana Patient Safety Center (IPSC), Indiana Hospital Association (IHA) and VHA Central.
Copyright © 2008 Purdue University PharmaTAP. All Rights Reserved.
Permission to use, copy, modify, and distribute all or portions of this toolkit without fee and without written agreement is hereby granted by Purdue University PharmaTAP.
Purdue University PharmaTAP, 6640 Intech Blvd., Suite 120, Indianapolis, IN 46278‐2012. www.purdue.edu/pharmatap

iii | A n t i c o a g u l a n t T o o l k i t
Thank you to the many individuals who have contributed their time, expertise and creativity for the development of this toolkit. Their generosity has made this toolkit possible. Specifically, we’d like to thank:
Carol Birk, M.S., R.Ph. Director Purdue University, PharmaTAP Indianapolis, IN Frank Federico Content Director Institute for Healthcare Improvement Cambridge, MA Jan Kirsch, M.S.N., Ed.D., R.N. Senior Director Performance Improvement, VHA Central Indianapolis, IN
Betsy Lee, R.N., M.S.P.H.Director Indiana Patient Safety Center Indianapolis, IN Steve Meisel, Pharm.D. Director, Medication Safety Fairview Health Services Minneapolis, MN Erin Moore, M.A. Communications Specialist, Regenstrief Center for Healthcare Engineering at Purdue University West Lafayette, IN
Gloria Sachdev, Pharm.D.Clinical Assistant Professor Pharmacy Practice, Purdue University School of Pharmacy and Pharmaceutical Sciences West Lafayette, IN Ellen Schellhase, Pharm.D. Assistant Professor Pharmacy Practice, Purdue University School of Pharmacy and Pharmaceutical Sciences West Lafayette, IN
Tool Kit Resource Contributors
Kristi Williams, Pharm.D. Pharmacy Clinical Services Manager Union Hospital Terre Haute, IN
Brian Wolfe, Pharm.D.Clinical Pharmacy Coordinator Ball Memorial Hospital Muncie, IN
Additionally, thank you to the Institute for Healthcare Improvement (IHI) and VHA Central for their materials.
Acknowledgements

iv |
Chapter 1: Introduction ........................................................................................... 1 Chapter 1 Resources .................................................................................................................... 5
Chapter 2: Self Assessment ...................................................................................... 10 Chapter 2 Resources .................................................................................................................... 12
Chapter 3: Improving Anticoagulant Processes .................................................. 53 Chapter 3 Resources .................................................................................................................... 60
Chapter 4: Measuring Performance ...................................................................... 70 Chapter 4 Resources .................................................................................................................... 73
Chapter 5: Spreading and Sustaining Improvement .......................................... 77 Chapter 5 Resources .................................................................................................................... 79
Chapter 6: Additional References ......................................................................... 82
Table of Contents

1 | A n t i c o a g u l a n t T o o l k i t
Ch t 1 I t d ti

2 | C h a p t e r 1 : I n t r o d u c t i o n
Anticoagulants, such as Unfractionated Heparin, Low Molecular Weight Heparins, and Warfarin, are considered high risk drugs for “adverse drug events” (ADE)1, defined by the Agency for Healthcare Research and Quality (AHRQ) as expected adverse drug reactions (or "side effects") and events due to error2. Preventable adverse drug events are associated with 1 of 5 injuries or deaths and are a result of poorly designed systems, which often lack independent redundancies3.
Numerous studies describe the high risks associated with use of anticoagulants. As a drug category, anticoagulants are one of the top five drug types associated with patient safety
incidents4 Heparin ranks 3rd in reported products involved in harmful errors. Warfarin ranks 6th and enoxaparin ranks
9th5 7.2% of medication errors reported in a hospital were due to anticoagulants. Furthermore, 6.2% of these
required medication intervention6 Warfarin and insulin caused an estimated one in every seven adverse drug events treated in emergency
departments, and more than a quarter of all hospitalizations7 Insulin, Warfarin, and digoxin (all narrow therapeutic index medications) were responsible for one in every
three adverse drug events treated in an emergency department in patients 65 years and older7 32.2% of preventable adverse drug events in a teaching hospital involved anticoagulants. This was double
the amount caused by any other medication8 Anticoagulants were responsible for 121 of the 1,523 adverse drug events, a third of which were
preventable9
Anticoagulants are included on the Institute for Safe Medication Practice’s (ISMP) high alert medication list due to the significant risk of causing life‐threatening bleeding or thrombosis if the appropriate safe practices are not in place. The Institute for Healthcare Improvement’s (IHI) “Save 5 Million Lives from Harm” campaign has focused in part on harm associated with the use of anticoagulants10. This high risk is due to the complexity of administering this therapy:
Selecting the appropriate agent and determining the appropriate dose,
Individual patient variability in response to therapy,
Timing of and use of the appropriate laboratory measures to monitor response,
Proper adjustment of dose based upon the laboratory parameters and/or clinical response,
The transition of patients from Heparin therapy to Warfarin,
Ensuring patient education and compliance,
Use of these agents in a variety of settings, by various practitioners, and within differing patient populations, and
Interdisciplinary coordination needed between lab, pharmacy, nursing, medical staff, and dietary.
Introduction

3 | A n t i c o a g u l a n t T o o l k i t
TABLE 1 Common Risks and Safe Practices Associated with Anticoagulants
ISMP Medication Safety Alert, January 11, 2007, Volume 12 Issue 1
Common Risks Safe Practices to Reduce or Eliminate Adverse Drug Events
Duplicate or concurrent therapy Accidental stoppage of therapy Look-alike vials or syringes Look-alike names Dosing errors Calculation errors Monitoring problems Food and drug interactions Spinal hematoma Adverse drug reactions Confusion between insulin and Heparin; between LMWHs and UFH
Avoid reliance on memory.
- Use protocols/checklists
- Automate
- Develop built-in reminders Simplify tasks.
- Decrease steps in the process
- Decrease number of staff involved in the process
- Reduce need for calculations Reduce or eliminate handoffs. Standardize.
- Develop practice guidelines, order sets, and pathways Use constraints and forcing functions.
- Ensure use of required computer fields
- Remove outdated forms
- Utilize free flow pump protection Improve access to information.
- Ensure that up-to-date, accurate information is available when needed
Use redundancy.
- Create double checks at critical steps in the process Provide adequate training.
- Use drills, practice, simulation Manage fatigue.
- Offer reasonable work schedules
- Ensure adequate staff Design useful, clear, concise policies.
The Solution
Adverse drug events associated with anticoagulants can be reduced by implementing recognized safe practices in high risk areas, redesigning care processes, partnering with patients and families, and maximizing communications within and across the care continuum. Table 1 outlines common risks and suggested safe practices to reduce or eliminate risks that could lead to adverse drug events.
The Institute for Healthcare Improvement’s Getting Started Kit entitled “Prevent Harm from High Alert Medications: How to Guide” lists safe practices specific to Heparin and Warfarin use in inpatient and outpatient settings.10 The ISMP, whose goal is to educate the healthcare community about safe medication practices, featured anticoagulants in their January 2007 Medication Safety Alert11 which listed risks associated with anticoagulants and recommended safety improvements.

4 | C h a p t e r 1 : I n t r o d u c t i o n
Additional evidence‐based support for safe practices with anticoagulants includes the Seventh American
College of Chest Physicians (ACCP) Conference on Antithrombotic and Thrombolytic Therapy: Evidence‐Based Guidelines. Published on a periodic basis, the “CHEST Guidelines” are well referenced, provide graded recommendations, and cover a variety of different anticoagulant indications and clinical practice areas.12
The Joint Commission emphasizes and promotes safe use of medications throughout its Standards and National Patient Safety Goals (NPSGs). National Patient Safety Goal (NPSG) 3E was developed with a specific focus on safe use of anticoagulants13 in hospital and ambulatory settings that provide anticoagulant therapy.
The Joint Commission established a one‐year implementation timeline for planning, development and testing changes to meet the intent of the goal. Following this one‐year transition it is expected that compliance includes continued evaluation of the anticoagulation use processes for Unfractionated Heparins, Low Molecular Weight Heparins (LMWH), and Warfarin. Compliance with the goal is based on review of documents (e.g. patient records, policies and procedures and performance monitors), interviews with patients and staff, and direct observation of processes.
In this Toolkit This anticoagulant toolkit is intended for use by healthcare providers and institutions to provide effective and safe anticoagulation therapy in all care settings. The toolkit consists of six chapters designed to offer information and solutions to improve anticoagulant practices. Chapter 1 serves as an introduction to the problems associated with anticoagulants and describes support for evaluating and improving the medication process for anticoagulant management. Chapter 2 is a resource for evaluation and assessment of safe medication practices for anticoagulation. Example tools have been included to assist institutions in developing their own resources for safe anticoagulant use. Chapters 3, 4, and 5 outline strategies for implementing change. Chapter 6 contains additional resources for further knowledge regarding anticoagulation. The following model of care is used throughout the toolkit and is intended to assist organizations with identification and self assessment of safe practices by specific care environment.
Includes a variety of providers
(physicians, pharmacists, nurses, dieticians) who provide care related to the utilization of anticoagulants.
Includes providers from both in‐patient and out‐patient settings. Focus is two‐fold: (1) preparing a
patient for continued care with out‐patient providers (2) establishing a
source of outpatient care. Communication is a key aspect.
Includes a provider(s) responsible for continued and long‐term care of patients receiving anticoagulants.
Inpatient
Transitional
Outpatie
nt
Joint Commission National Patient Safety Goal 3E Reduce the likelihood of patient harm associated with the use of

5 | A n t i c o a g u l a n t T o o l k i t
References 1. Psnet.ahrq.gov/glossary 2. For example, a serious allergic reaction to penicillin in a patient with no prior history is an ADE, and so is the
same reaction in a patient who does have a known allergy history but receives penicillin due to a prescribing oversight. An example of an anticoagulant ADE is a major hemorrhage from Heparin due to a dosing error.
3. Pronovost P, et al. medication Reconciliation: a Practical Tool to Reduce the Risk of Medication Errors, Journal of Critical Care, Volume 18, Issue 4, December 2003, Pages 201‐205
4. Cousins D, et al. 2006. Rick Assessment of Anticoagulation. National Patient Safety Association. United Kingdom.
5. USP MedMarx Data, 2005 6. Fanikos J, et al. Medication Errors Associated with Anticoagulant Therapy in the Hospital. American Journal
Cardiol. 2004 August 15:94:532‐5. 7. Budnitz, et al. National Surveillance of Emergency Department Visits for Outpatient Adverse Drug Events,
JAMA 2006;295(15):1585‐1866. 8. Winterstein, et al. Identifying Clinically Significant Preventable Adverse Drug Events through a Hospital’s
Database of Adverse Drug Reaction Reports, American Journal of Health‐System Pharmacy. 59 (18): 1742‐1749, September 15, 2002
9. Gurwitz JH, et al. Incidence and Preventability of Adverse Drug Events Among Older Persons in Ambulatory Setting, JAMA. 289:1107‐1116, March 5, 2003.
10. www.IHI.org 11. ISMP Medication Safety Alert, January 11, 2007, Volume 12 Issue 1 12. http://www.chestjournal.org/content/vol126/3_suppl/index.shtml 13. www.jointcommission.org
A. Inpatient Case Study
B. Transition Case Study
C. Outpatient Case Study
D. Joint Commission National Patient Safety Goal 3E Implementation Expectations
E. Incorporating NPSG 3E into Medication Process Steps
Chapter 1 Resources

6 | C h a p t e r 1 : I n t r o d u c t i o n
CHAPTER 1 RESOURCE TOOL A Inpatient Case Study
A 68‐year‐old female is hospitalized for a Congestive Heart Failure exacerbation. Upon admission, the patient is continued on her home medication regimen determined only from her prescription bottles (including Warfarin) and without any communication with the patient or family. The INR was ordered on day 3 of admission instead of the day of admission. On day 3, the INR report indicated a higher than normal result of 5. The physician reduced the Warfarin dose and continued to monitor.
Case Commentary
It is likely that this patient was seen in an outpatient clinic on several occasions where Warfarin dose adjustments were made without changes to the labeling on the prescription container. This resulted in an incorrect Warfarin dose ordered upon admission since only the prescription container label was used for medication reconciliation purposes. The lack of an INR on admission, or within the first day of hospitalization prevented the practitioner from identifying the elevated INR and adjusting the Warfarin therapy earlier in the hospital stay.
Suggested Safe Practices - Medication reconciliation process includes appropriate communications with patients and families to verify
patient medications and dosages.
- A policy to include timing for obtaining and reporting initial and ongoing lab results is utilized (i.e. INR for Warfarin and aPTT for Unfractionated Heparin).
CHAPTER 1 RESOURCE TOOL B Transition Case Study
A 48‐year‐old male patient was discharged from the hospital following a new onset Deep Venous Thrombosis (DVT). During the brief hospitalization, the patient was started on a Low Molecular Weight Heparin (LMWH). On Friday, day 1 of discharge from the hospital, the patient was provided with 10 doses of LMWH or enough doses for 4 days. The patient was also started on Warfarin therapy which is used in combination with LMWH to achieve a therapeutic INR. The patient was instructed to contact the outpatient anticoagulant management clinic for a follow‐up visit. On day 4 of therapy (Monday) and upon taking the last dose of LMWH, the patient contacted the outpatient clinic and scheduled an appointment for Thursday (day 6) of therapy. During clinic on Thursday (day 6) the INR was 1.4 or sub‐therapeutic, and the patient informed the practitioner that his last dose of LMWH was Monday evening (day 4).
Case Commentary
This case highlights the need for identified staff to take responsibility for the follow‐up care of a patient. This patient may not have had the knowledge (or appropriate education) to know that he needed a follow‐up appointment before Thursday. The sub‐therapeutic INR resulting from the omitted doses of LMWH may have placed the patient at risk for another DVT.
Suggested Safe Practices
- Inpatient staff accountable for coordinating the patients’ anticoagulation management from hospital discharge to the outpatient clinic assures that the appropriate quantity of medication is prescribed and that the follow‐up appointment with the next provider of care is scheduled prior to discharge.
- Patients remain on combination LMWH/Warfarin therapy until the INR remains within therapeutic range for 2 consecutive days (consider adding one refill).

7 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 1 RESOURCE TOOL C Outpatient Case Study
A 79‐year old female patient with atrial fibrillation, maintained on a 2.5mg daily dose of Warfarin had an INR of 1.6. The prescriber gave the patient a new prescription for 5mg Warfarin tablets and verbal instructions to change the regimen to 5mg MWF and 2.5 TRSS. No follow‐up written information was provided to the patient. At her next visit, two weeks later, her INR was 7.8 indicating that her dose was too high. The patient interview revealed that she had added 5mg MWF to her previous regimen of 2.5 mg daily, increasing the dose by 15mg per week rather than by 7.5mg per week.
Case Commentary
The error occurred for several reasons; no written information was provided to the patient and the patient was given an additional tablet strength which complicated the dosing regimen.
Suggested Safe Practices
- Tablets are split or doubled to make the appropriate dose to avoid prescribing multiple tablet strengths of Warfarin.
- Written anticoagulant dosing changes and lab appointments are provided. When verbal communication is necessary (via phone), the patient reads back for verification.
- Provide and document anticoagulant patient education.

8 | C h a p t e r 1 : I n t r o d u c t i o n
CHAPTER 1 RESOURCE TOOL D Joint Commission National Patient Safety Goal 3E
Implementation Expectations 1. The organization implements a defined anticoagulant management program to individualize the care provided
to each patient receiving anticoagulant therapy.
2. To reduce compounding and labeling errors, the organization uses ONLY oral unit dose products and pre‐mixed infusions, when these products are available.
3. When pharmacy services are provided by the organization, Warfarin is dispensed for each patient in accordance with established monitoring procedures.
4. The organization uses approved protocols for the initiation and maintenance of anticoagulation therapy appropriate to the medication used, to the condition being treated and to the potential for drug interactions.
5. For patients being started on Warfarin, a baseline International Normalized Ration (INR) is available, and for all patients receiving Warfarin therapy, a current INR is available and is used to monitor and adjust therapy.
6. When dietary services are provided by the organizations, the service is notified of all patients receiving Warfarin and responds according to its established food/drug interaction program.
7. When Heparin is administered intravenously and continuously, the organization uses programmable infusion pumps.
8. The organization has a policy that addresses baseline and ongoing laboratories tests that are required for Heparin and Low Molecular Weight Heparin therapies.
9. The organization provides education regarding anticoagulation therapy to prescribers, staff, patients and families.
10. Patient/family education includes the importance of follow‐up monitoring, compliance issues, dietary restrictions, and potential for adverse drug reactions and interactions.
11. The organization evaluates anticoagulation safety practices.1
Additional Joint Commission Expectations Pertaining to Anticoagulants
- The organization has a standardized list of abbreviations, acronyms, symbols, and dose designations that are not to be used throughout the organization (“U” for units must be on the list).2
- Standardize and limit the number of drug concentrations used.3
- Accurately and completely reconcile medications across the continuum of care. A complete list of medications is communicated to the next provider and is provided to the patient on discharge from the facility.4
- Identify and at a minimum annually review a list of look‐alike/sound‐alike drugs used in the organization and take action to prevent errors involving the interchange of these drugs.5
- Implement a standardized approach to hand off communications including an opportunity to ask and respond to questions.6
- Measure, assess and if appropriate, take action to improve the timeliness of reporting and the timeliness of receipt by the responsible licensed caregiver of critical tests and critical results and values.7
- Encourage patients’ active involvement in their own care as a patient safety strategy.8
References
1. Medication Management Standard, 8.10 2. National Patient Safety Goal, 2B 3. Medication Management Standard, 2.20 4. National Patient Safety Goal, 8A, 8B
5. National Patient Safety Goal, 3C 6. National Patient Safety Goal, 2E 7. National Patient Safety Goal, 2C 8. National Patient Safety Goal, 13A

9 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 1 RESOURCE TOOL E Incorporating NPSG 3E into Medication Process Steps
Organizations should consider developing safer processes beyond what is expected under NPSG 3E. Project goals should include improved prescribing, reduced adverse effects and an improvement in patient outcomes. The 11 expectations are listed in the table below by medication process step to assist with prioritizing activities associated with gathering data, identifying gaps between actual and expected practice, developing action plans, implementing changes for improvement, and monitoring for sustainability.
Anticoagulant Medication Process Steps JC NPSG 3E Implementation Expectations
Formulating Plan of Care
1. Defined anticoagulant management program that individualizes care 6. Dietary services notified of patients on Warfarin and responds according to
its established food/drug interaction program 11. Evaluates anticoagulation safety practices
Prescribing 4. Use approved protocols for the initiation and maintenance of anticoagulation therapy appropriate to the medication used, to the condition being treated and to the potential for drug interactions.
Dispensing 2. Use ONLY oral unit dose products and pre-mixed infusions
Administration 7. Programmable infusion pumps are used when Heparin is administered intravenously and continuously
Monitoring 3. Warfarin is dispensed for each patient in accordance with established monitoring procedures.
5. Patients on Warfarin require:
- Baseline International Normalized Ration (INR)
- Current INR to monitor and adjust therapy 8. Policy addresses baseline and ongoing laboratory tests that are required for
Heparin and low molecular weight Heparin therapies.
Patient Education 9. Education provided to prescribers, staff, patients and families. Patient/family education includes follow-up monitoring, compliance issues, dietary restrictions and potential for adverse drug reactions and interactions.

10 | C h a p t e r 2 : S e l f - A s s e s s m e n t
Ch t 2 S lf

11 | A n t i c o a g u l a n t T o o l k i t
This chapter discusses specific recommendations to assist organizations with implementation of safe anticoagulation practices as outlined in the Joint Commission National Patient Safety Goal 3E (NPSG 3E) Expectations. Assuring safe practices for anticoagulants requires developing standardized processes in the in‐patient, transition and outpatient care settings. Joint Commission recommends that hospital leadership assign responsibility for oversight, coordination of development, testing, and implementation of these expectations which should be completed prior to conducting self assessments.
Organizations should complete a self assessment(s) to determine if they have safe practices in place for each Joint Commission Expectation in one or all three care settings. This can be accomplished by printing and using the following tables as self assessment tools: Table 1: Inpatient Care; Table 2: Transition Care; and Table 3: Outpatient Care. Validation of the compliance score for each safe practice should be done through direct observation and/or interview.
Through use of the self assessment tools, one may find that some safe practices are in place, but may not be performed as intended and/or may not be consistently applied to all patients. In these situations, it may be beneficial to address the level of difficulty of change required to meet the Joint Commission Expectations. Depending on available resources, the implementation level of difficulty will vary. An organization may wish to assess the level of difficulty of change required for each targeted opportunity for improvement as either “low”, “intermediate”, or “high” using the definitions provided on each table. Once the organization has completed their self‐assessment(s) and prioritized safe practice recommendations by level of implementation difficulty, they should begin to address their process improvement opportunities as defined in Chapters 3‐5 of the toolkit.
Organizations that wish to pursue use of a highly detailed anticoagulation self assessment tool are referred to the Institute for Safe Medication Practices (ISMP) Medication Safety Self Assessment for Antithrombotics.1
Organizations are also encouraged to conduct a Failure Mode and Effects Analysis (FMEA). A FMEA is an ongoing quality improvement process that is carried out in healthcare organizations by a multidisciplinary team to determine points of potential failure and what their effect would be. FMEA is a proactive process used to look more carefully and systematically at vulnerable areas or processes.2
References 1. www.ismp.org/selfassessments/asa2006/Intro.asp 2. www.ismp.org/Tools/FMEAofanticoagulants.pdf
Self Assessment

12 | C h a p t e r 2 : S e l f - A s s e s s m e n t
The hard copy and web resources listed below are referenced in the Inpatient, Transition and Outpatient Care tables starting on page 14. These example tools are utilized by various institutions and are noted for the purposes of providing a template regarding format and function only, not as specific recommendations.
Hard Copy (alphabet designation)
A. Policy and Procedure for Warfarin Monitoring and Dosing Protocol
B. Measures for Adverse Drug Event Related to Warfarin, Heparin, Enoxparin, and other Anticoagulants
C. Med Watch Form
D. Weight Based Heparin Protocol Order Form
E. Physician Order form for Heparin and Enoxaparin
F. Warfarin Dosing Protocol
G. Pharmacy Heparin Dosing Service ‐ flow sheet for tracking Heparin and Warfarin
H. Warfarin Monitoring ‐ Warfarin Flow Sheet
I. Warfarin Flow Sheet
J. Anticoagulation Review
K. Warfarin Management Test (with key)
L. Annual Education ‐ Anticoagulation (with key)
M. Wishard Hospital Outpatient Anticoagulation Flow Sheet
N. Wishard Hospital Outpatient Warfarin Dosing Card
Web Resources (numeric designation)
1. Bristol‐Myers Squibb, manufacturers of brand Coumadin has numerous tools: www.coumadin.com (at the time of this publication, this website was being updated)
2. PTINR.com America’s Anticoagulation Resource: www.ptinr.com has a link to Improve your Warfarin Safety with links to tools: “Using Warfarin Safely at Home” (also available in Spanish), “Patient INR Test Results Diary”
3. American College of Clinical Pharmacy recognizes anticoagulation training program through the University of Texas and The Anticoagulation Clinics of North America: www.accp.com/frontiers/research.php
4. Clot Care Online Resource has links to numerous anticoagulation training programs: www.clotcare.com/clotcare/anticoagtrainingprograms.aspx
5. Spectrum Health, West Michigan’s largest integrated health care system, has developed an online anticoagulation toolkit: http://spectrum‐health.org/cs/Satellite?c=eHA_Content_ C&cid=1158780505675&pagename=Spectrum_Health_Core%2FSpectrum_Core_Central_Template#doc
a. Warfarin Patient Education Booklet
b. Patient Dosing Sheet for Warfarin
i. Recommended Frequency of INR Testing
j. Guidelines for Warfarin Reversal with Vitamin K
Chapter 2 Resources

13 | A n t i c o a g u l a n t T o o l k i t
c. Patient Dosing Sheet for Warfarin (inpatient and outpatient)
d. Patient Dosing Card (Warfarin)
e. Recommendations for Target INR Range and Duration of Therapy for Warfarin Therapy
f. Recommendations for Initiation of Warfarin Therapy
g. Managing Oral Anticoagulation during Invasive Procedures
h. Guidelines for Warfarin Maintenance
k. Warfarin Interactions with Drugs, Herbals, Food, and Labs
l. Anticoagulation Management Face Sheet
m. Warfarin Monitoring Sheet
n. Anticoagulation Patient Education Note
o. Patient Questionnaire for Warfarin Therapy
p. Anticoagulation Management Note
q. Health Care Professional Anticoagulation Competency
6. American College of CHEST Physicians publishes The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Chest, Sept 2004;126:163S – 696S., full text available free on‐line at www.chestjournal.org/
7. Best Practices Preventing Deep Vein Thrombosis and Pulmonary Embolism: A Practical Guide to Evaluation and Improvement hosted by University of Massachusetts Medical School: www.ourcomes‐umassmed.org then, click on VTE Education to get to www.dvt.org
8. Anticoagulation Forum has numerous links to assist in developing indication‐specific anticoagulation algorithms: www.acforum.org/links.html
9. Warfarin dosing website, supported by the Barnes‐Jewish Hospital and the NIH, provides initial Warfarin dosing recommendations: www.Warfarindosing.org
10. The University of Washington Venus Thromboembolism site, funded by AHRQ, contains recommendations for safe practice interventions for patients at risk for or who are diagnosed with VTE: http://vte.son.washington.edu/
11. Iowa Healthcare Collaborative Anticoagulation Toolkit: www.ihconline.org/toolkits/anticoagulation.cfm
a. Step 1 Policies and Procedures link to intake/indication for long‐term anticoagulation, several tools including “A patient admission intake form” of Madison County Healthcare System, Winterset, IA
b. Step 1 Policies and Procedures “target INR range and dosing policies”
c. Step 1 Policies and Procedures “duration of long‐term anticoagulation and/or a review date”
d. Step 1 Policies and Procedures “timing of next INR appointment
e. Step 3 Reliable patient schedule and tracking “A patient Coumadin dosing and INR schedule” of Central Community Hospital, Elkader, IA (appointment card)
f. Step 5 Discharge Planning “Discharge form” of Central Community Hospital, Elkader, IA
12. Institute for Healthcare Improvement Medication Safety Reconciliation Tool Kit: www.ihi.org/IHI/topics/patientsafety/medicationsystems/tools/,medicationsafetyreconciliationtoolkit.htm

14 | C h a p t e r 2 : S e l f - A s s e s s m e n t
TABLES 2-4 Inpatient, Transition and Outpatient Care - Instructions
Column 1:
The 11 Joint Commission NPSG 3E Implementation Expectations are addressed within the context of medication process steps to which they apply. Specifically these process steps have been designated as Formulating a Plan of Care, Prescribing, Dispensing, Administration, Monitoring, and Patient Education.
Column 2:
Safe Practice recommendations are provided for implementation of each NPSG 3E expectation.
Column 3:
Example Tools for Safe Practices, such as protocols, algorithms, and forms, are listed. These example tools are utilized by various institutions and are noted for the purposes of providing a template regarding format and function only, not as specific recommend-ations. Tools are referenced from:
- Hard copy (alphabet design-nation*)
- Websites (numeric designation*)
Column 4:
Self Assessment of Safe Practices involves self scoring utilizing the key listed below.
.
Column 5:
Level of Implementation Difficulty involves self scoring utilizing the key listed below.
L= Low
I = Intermediate
H = High
*Lists of referenced tools with numeric and alphabet designations on pages 12-13. Hard copy tools begin on page 25.
Key:
*Self Assessment of Safe Practices Self-Scoring Scale **Level of Implementation Difficulty
1. There is no discussion around this activity
2. This activity is under discussion, but there is no implementation plan
3. This activity is partially implemented in some or all areas of the organization
4. This activity is fully implemented in some areas of the organization
5. This activity is implemented in all areas of the organization
n/a This activity is not applicable
Low = Safe practice recommendation is in place with few adjustments needed to meet expectation. No additional resources are required with practitioners continuing in their current role.
Intermediate = Safe practice recommendation may or not be in place. No additional resources are required as existing practitioners will assume new responsibilities to meet expectation.
High = Safe practice recommendation is not in place. Additional resources will be needed to meet expectation.

15 | A n t i - C o a g u l a n t T o o l k i t
TABLE 2 Inpatient Care
JC NPSG 3E Implementation Expectation Safe Practices Tools^
Self Assessment
Score*
Level of Implementation
Difficulty**
Form
ulat
ing
A P
lan
of C
are
1. The organization implements a defined anticoagulant management program to individualize the care provided to each patient receiving anticoagulant therapy
Identify inpatient personnel to coordinate anticoagulation management responsibilities (consider clinical pharmacy services as available)
A
6. When dietary services are provided by the organizations, the service is notified of all patients receiving Warfarin and responds according to its established food/drug interaction program.
Daily printout of patients receiving Warfarin provided to nutrition services
---
11. The organization evaluates anticoagulation safety practices (see MM.8.10).
Complete a Self Assessment ---
Interdisciplinary team organized to analyze safe anticoagulant use process
---
Interdisciplinary team evaluates anticoagulant protocols, pathways, order sets, flow sheets and checklists for accuracy and updates
---
Methods defined for reporting medication errors (internally and externally)
---
Methods defined for reporting adverse effects associated with anticoagulation
B, C
Pre
scrib
ing
4. The organization uses approved protocols for the initiation and maintenance of anticoagulation therapy appropriate to the medication used, to the condition being treated and to the potential for drug interactions.
A list of error prone abbreviations (i.e.; “U” for units) is established and implemented on all forms, order sets, and pharmacy storage
--
Medication reconciliation process in place to verify patient medications and dosages
12
Utilize standard protocols for: 6
- New starts D,F,5f,9
- Prophylaxis E
- UFH dosing D, E

16 | C h a p t e r 2 : S e l f - A s s e s s m e n t
Table 2 Continued: Inpatient Care
JC NPSG 3E Implementation Expectation
Safe Practices
Tools^
Self Assessment
Score*
Level of Implementation
Difficulty**
Pre
scrib
ing
4. Continued A list of error prone abbreviations (i.e.; “U” for units) is established and implemented on all forms, order sets, and pharmacy storage
--
- LMWH dosing E
- Warfarin dosing F, 5h, 9
- Bridging from LMWH to Warfarin F, 5g
- Vitamin K reversal F, 5j
Disease state protocols (atrial fibrillation, DVT…) 7,8,10
Dis
pens
ing
2. To reduce compounding and labeling errors, the organization uses ONLY oral unit dose products and pre-mixed infusions, when these products are available
Utilize unit dose Warfarin (nurses do not split Warfarin tablets)
---
Consider warning labels ---
All strengths of Warfarin are purchased from a single manufacturer
---
Limit concentrations of Heparin stored in Automated Dispensing Machines and as floor stock
---
Utilize commercially prepared, pre-mixed IV solutions of UFH in limited concentrations and vial sizes
---
Utilize standard dose concentrations throughout the facility ---
Utilize unit dose LMWH (round to the nearest strength if using a pen)
---
Provide physical separation by product and strength when storing products (may use warning labels)
---
Utilize machine readable coding to verify patient identity prior to anticoagulant administration
---
Adm
inis
tratio
n 7. When Heparin is administered intravenously and continuously, the organization uses programmable infusion pumps.
Utilize programmable pump, such as Smart Pumps, with both standard rates and weight based rates
---
Require a second nurse to double check when initiating Heparin drips, changing rates or changing bag
---
Separate Heparin and insulin to reduce mix-ups ---

17 | A n t i - C o a g u l a n t T o o l k i t
Table 2 Continued: Inpatient Care
M
onito
ring
3. When pharmacy services are provided by the organization, Warfarin is dispensed for each patient in accordance with established monitoring procedures
Protocol for test results available in a timely manner ---
Warfarin is administered at the same time each day after INR results are available (e.g. afternoon / evening)
---
5. For patients being started on Warfarin, a baseline International Normalized Ration (INR) is available, and for all patients receiving Warfarin therapy, a current INR is available and is used to monitor and adjust therapy.
A policy for initial and ongoing lab results is utilized (i.e.; INR for Warfarin and aPTT for UFH)
11 b-d 5e, 5i
8. The organization has a policy that addresses baseline and ongoing laboratories tests that are required for Heparin and low molecular weight Heparin therapies.
Tracking form for managing anticoagulant patients is used (and provided upon patient transfer)
G, H, I,
Obtain baseline tests (e.g. Hgb, Hct, SCr, Platelet, INR, aPTT) before prescribing anticoagulant
---
An aPTT is obtained no sooner than 6-8 hours after UFH initiated
---
Utilize standard guidelines for laboratory monitoring for LMWH, including monitoring special populations (i.e. morbid obesity, renal insufficiency, pregnancy, etc.)
---
Pat
ient
Edu
catio
n
9. The organization provides education regarding anticoagulation therapy to prescribers, staff, patients and families.
Document anticoagulant patient education ---
Annually, at minimum, provides staff education about anticoagulants (for providers who prescribe, dispense, administer or monitor anticoagulants)
J, 3, 4
Providers complete annual competency evaluation for anticoagulants
K, L
10. Patient/family education includes the importance of follow-up monitoring, compliance issues, dietary restrictions, and potential for adverse drug reactions and interactions.
Provide pre-approved written patient and family education (audio-visual material may be considered in addition to written material) to include indication, symptoms for monitoring indication, dietary issues, drug interactions, disease interactions, monitoring requirements, duration of therapy, potential adverse effects, etc.
1, 5a-d 5k, 5o
Have low literacy patient education material available ---
Have patient education material available in other languages (e.g. Spanish)
2
Utilize standard log sheet for LMWH injections to include time of dosing, site of injection, missed doses, etc.
---
JC NPSG 3E Implementation Expectation Safe Practices Tools^
Self Assessment
Score*
Level of Implementation
Difficulty**

18 | C h a p t e r 2 : S e l f - A s s e s s m e n t
TABLE 3 Transition Care
JC NPSG 3E Implementation Expectation Safe Practices Tools^
Self Assessment
Score*
Level of Implementation
Difficulty**
Form
ulat
ing
A P
lan
of C
are
1. The organization implements a defined anticoagulant management program to individualize the care provided to each patient receiving anticoagulant therapy
Identify inpatient personnel to coordinate anticoagulation management transitional care responsibilities (consider clinical pharmacy services as available)
A
11. The organization evaluates anticoagulation safety practices (see MM.8.10).
Complete a Self Assessment ---
Interdisciplinary team organized to analyze safe anticoagulant use process
---
Interdisciplinary team routinely evaluates anticoagulant protocols, pathways, order sets, flow sheets and checklists for accuracy and updates
---
Methods defined for reporting medication errors (internally and externally)
---
Methods defined for reporting adverse effects associated with anticoagulation
B, C
Pre
scrib
ing
4. The organization uses approved protocols for the initiation and maintenance of anticoagulation therapy appropriate to the medication used, to the condition being treated and to the potential for drug interactions.
A list of error prone abbreviations (i.e.; “U” for units) is established and implemented on all forms, order sets, and pharmacy storage
---
Medication reconciliation process in place to verify patient medications and dosages
12
Utilize standard protocols for: - New start
6, E, F 5f, 9
- Prophylaxis E, F
- LMWH dosing E
- Warfarin dosing F 5h
- Bridging from LMWH to Warfarin F, 5g
- Vitamin K reversal F, 5j
- Disease state protocols (e.g. atrial fibrillation, DVT, etc) 7, 8, 10
For patients on combination LMWH/Warfarin, provide enough LMWH until INR expected to be therapeutic for 2 consecutive days (consider adding one refill)
---

19 | A n t i - C o a g u l a n t T o o l k i t
Table 3 Continued: Transition Care
JC NPSG 3E Implementation Expectation Safe Practices Tools^ Self
Assessment Score*
Level of Implementation
Difficulty**
Dis
pens
ing
2. To reduce compounding and labeling errors, the organization uses ONLY oral unit dose products and pre-mixed infusions, when these products are available
Utilize unit dose LMWH (round to nearest dosing strength if using a pen)
---
Not recommended for patient to administer partial dosing of LMWH pens
---
3. When pharmacy services are provided by the organization, Warfarin is dispensed for each patient in accordance with established monitoring procedures
Limit concentrations of Heparin stored in Automated Dispensing Machines and as floor stock
---
Utilize standard protocol for Warfarin monitoring and dosing
F, 5h, 5i, 9
Adm
inis
tratio
n
9. The organization provides education regarding anticoagulation therapy to prescribers, staff, patients and families.
Document anticoagulant patient education ---
Annually, at minimum, provides staff education about anticoagulants (for providers who prescribe, dispense, administer or monitor anticoagulants)
J, 3, 4
Providers complete annual competency evaluation for anticoagulants
K, L, 5q
Mon
itorin
g
5. For patients being started on Warfarin, a baseline International Normalized Ration (INR) is available, and for all patients receiving Warfarin therapy, a current INR is available and is used to monitor and adjust therapy.
Implement a policy for ordering INR prior to Warfarin initiation
11 b-d
Utilize standard guideline for INR monitoring and subsequent Warfarin dosing adjustment.
F, 5g
INR scheduled in out-patient setting by in-patient personnel ---
Inpatient personnel to notify outpatient provider responsible for following up INR of lab date and patient’s current contact information
---
Tracking form for managing anticoagulant patients is used (and provided to patient and/or outpatient anticoagulation provider upon patient discharge)
G, H, I, 5c, 11f
8. The organization has a policy that addresses baseline and ongoing laboratories tests that are required for Heparin and low molecular weight Heparin therapies.
Obtain baseline tests (Hgb, Hct, SCr, Platelet, INR, aPTT) before prescribing anticoagulants as appropriate
---
Utilize standard guidelines for laboratory monitoring for LMWH, including monitoring special populations (i.e. morbid obesity and renal insufficiency)
---

20 | C h a p t e r 2 : S e l f - A s s e s s m e n t
Table 3 Continued: Transition Care
JC NPSG 3E Implementation Expectation Safe Practices Tools^ Self
Assessment Score*
Level of Implementation
Difficulty**
Pat
ient
Edu
catio
n
9. The organization provides education regarding anticoagulation therapy to prescribers, staff, patients and families.
Document anticoagulant patient education ---
Annually, at minimum, provides staff education about anticoagulants (for providers who prescribe, dispense, administer or monitor anticoagulants)
J, 3, 4
Providers complete annual competency evaluation for anticoagulants
K, L, 5q
10. Patient/family education includes the importance of follow-up monitoring, compliance issues, dietary restrictions, and potential for adverse drug reactions and interactions.
Written anticoagulant dosing changes and lab appointments date/time provided to patient
11e, 5d, N
Patient provided outpatient provider’s contact information ---
Consider providing patient with free LMWH patient education kits as available from manufacturers
---
Provide pre-approved written patient education (audio-visual material may be considered in addition to written material) to include indication, symptoms for monitoring indication, dietary issues, drug interactions, disease interactions, monitoring requirements, duration of therapy, potential adverse effects, etc. Have low literacy patient education material available
1, 5a-d 5k, 5o
Have patient education material available in other languages (e.g. Spanish)
2
Provide patient with contact name/number should questions/concerns arise prior to their next out-patient visit.
---
Inpatient personnel to demonstrate to patient (or care giver) appropriate self-administration technique of LMWH
---
Utilize standard log sheet for LMWH injections to include time of dosing, site of injection, missed doses, etc.
---

21 | A n t i - C o a g u l a n t T o o l k i t
TABLE 4
Outpatient Care
JC NPSG 3E Implementation Expectation Safe Practices Tools^ Self
Assessment Score*
Level of Implementation
Difficulty**
Form
ulat
ing
A P
lan
of C
are
1. The organization implements a defined anticoagulant management program to individualize the care provided to each patient receiving anticoagulant therapy
Identify out-patient personnel to coordinate anticoagulation management (consider clinical pharmacy services as available)
A
2. To reduce compounding and labeling errors, the organization uses ONLY oral unit dose products and pre-mixed infusions, when these products are available
Utilize unit dose LMWH (round to nearest dosing strength if using a pen)
---
Not recommended for patient to administer partial dosing of LMWH pens
---
Consider warning labels ---
11. The organization evaluates anti- coagulation safety practices (see MM.8.10).
Complete a Self Assessment ---
Interdisciplinary team organized to analyze safe anticoagulant use process
---
Interdisciplinary team evaluates anticoagulant protocols, pathways, order sets, flow sheets and checklists for accuracy and updates
---
Methods defined for reporting medication errors (internally and externally)
---
Methods defined for reporting adverse effects associated with anticoagulation
C
Pre
scrib
ing
4. The organization uses approved protocols for the initiation and maintenance of anticoagulation therapy appropriate to the medication used, to the condition being treated and to the potential for drug interactions.
A list of error prone abbreviations (i.e.; “U” for units) is established and implemented on all forms, order sets, and pharmacy storage
---
Medication reconciliation process in place to verify patient medications and dosages
12
Utilize standard protocols for: - New starts
6 F, 5f, 9
- Prophylaxis ---
- LMWH dosing ---
- Warfarin dosing F, 5h, 9

22 | C h a p t e r 2 : S e l f - A s s e s s m e n t
Table 4 Continued: Outpatient Care
Pre
scrib
ing
4. The organization…cont. - Bridging from LMWH to Warfarin F, 5g
- Vitamin K reversal F, 5j
- Disease state protocols (e.g. atrial fibrillation, DVT, etc) 7, 8, 10
For patients on combination LMWH/Warfarin, provide enough LMWH until INR expected to be therapeutic for 2 consecutive days (consider adding one refill)
---
Avoid prescribing multiple tablet strengths of Warfarin ---
Utilize standard directions noting, as an example, “to take as directed per anticoagulation clinic”
---
Dis
pens
ing
2. To reduce compounding and labeling errors, the organization uses ONLY oral unit dose products and pre-mixed infusions, when these products are available
Utilize unit dose LMWH (round to nearest dosing strength if using a pen)
---
Not recommended for patient to administer partial dosing of LMWH pens
---
Consider warning labels ---
3. When pharmacy services are provided by the organization, Warfarin is dispensed for each patient in accordance with established monitoring procedures
Protocol for test results available in a timely manner ---
Limit number of Warfarin tablet strengths available ---
Use a medication box reminder if patient missing Warfarin doses
---
Provide pill cutter as needed ---
Avoid switching from brand to generic or from one generic to another (if this does occur, notify anticoagulation provider).
---
Adm
inis
tratio
n
9. The organization provides education regarding anticoagulation therapy to prescribers, staff, patients and families
Document anticoagulant patient education ---
Annually, at minimum, provides staff education about anticoagulants (for providers who prescribe, dispense, administer or monitor anticoagulants)
J, 3, 4
Providers complete annual competency evaluation for anticoagulants
K, L
JC NPSG 3E Implementation Expectation Safe Practices Tools^ Self
Assessment Score*
Level of Implementation
Difficulty**

23 | A n t i - C o a g u l a n t T o o l k i t
Table 4 Continued: Outpatient Care
Mon
itorin
g
5. For patients being started on Warfarin, a baseline International Normalized Ration (INR) is available, and for all patients receiving Warfarin therapy, a current INR is available and is used to monitor and adjust therapy.
Implement a policy for ordering INR prior to Warfarin initiation
---
Utilize standard guideline for INR monitoring and subsequent Warfarin dosing adjustment
F,11b-d
Personnel to contact patients who no-show for scheduled INR the same day as missed lab appointment and reschedule them
---
Monitor INR closely if patient is switched from Warfarin brand to generic or from one generic to another
---
Utilize standard flow sheets to monitor INR and dosing changes
5m, 5n, 5p, M, 11a
8. The organization has a policy that addresses baseline and ongoing laboratories tests that are required for Heparin and low molecular weight Heparin therapies.
Obtain baseline tests (Hgb, Hct, SCr, Platelet, INR, aPTT) before prescribing anticoagulants as appropriate
---
Utilize standard guidelines for laboratory monitoring for LMWH, including monitoring special populations (i.e. morbid obesity and renal insufficiency)
---
Pat
ient
Edu
catio
n
9. The organization provides education regarding anticoagulation therapy to prescribers, staff, patients and families.
Document anticoagulant patient education ---
Annually, at minimum, provides staff education about anticoagulants (for providers who prescribe, dispense, administer or monitor anticoagulants)
J, 3, 4
Providers complete annual competency evaluation for anticoagulants
K, L, 5q
10. Patient/family education includes the importance of follow-up monitoring, compliance issues, dietary restrictions, and potential for adverse drug reactions and interactions.
Written anticoagulant dosing changes and lab appointments preferred; however, if verbal (via phone) then patient to read back for verification
11e, N, 5d
Patient provided outpatient anticoagulation provider’s contact information
---
Consider providing patient with free LMWH patient education kits as available from manufacturers
---
JC NPSG 3E Implementation Expectation Safe Practices Tools^
Self Assessment
Score*
Level of Implementation
Difficulty**

24 | C h a p t e r 2 : S e l f - A s s e s s m e n t
Table 4 Continued: Outpatient Care
Pat
ient
Edu
catio
n
10. Patient/family education…cont.
Provide pre-approved written patient education (audio-visual material may be considered in addition to written material) to include indication, symptoms for monitoring indication, dietary issues, drug interactions, disease interactions, monitoring requirements, duration of therapy, potential adverse effects, etc.
1, 5a-d 5k, 5o
Have low literacy patient education material available ---
Have patient education material available in other languages (e.g. Spanish)
2
Patient to carry wallet ID card or wear ID noting s/he is on anticoagulants
---
Personnel to demonstrate to patient appropriate self-administration technique of LMWH
---
Utilize standard log sheet of LMWH injections including time of dosing, site of injection, missed doses, etc.
---
JC NPSG 3E Implementation Expectation Safe Practices Tools^
Self Assessment
Score*
Level of Implementation
Difficulty**

25 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL A Policy and Procedure for Warfarin monitoring and dosing protocol
SUBJECT: Warfarin (Coumadin) Monitoring and Dosing Protocol FILE NO.: VI-6 PAGE: 1 OF 1
SPONSORING DEPARTMENT/COMMITTEE Pharmacy Services SCOPE: BMH, BMH Rehab Unit, BMH Transitional Care Unit APPROVED (COMMITTEE, DATE): Pharmacy and Therapeutics Committee 10/02 DATE EFFECTIVE: 10/02
REVIEW/REVISION DATES: 10/03, 10/05, 01/06, 4/07
KEY WORDS: Warfarin, Coumadin, Protocol, Dosing, Monitoring
PURPOSE: To optimize safety, dosing, monitoring, and appropriateness of Warfarin therapy.
POLICY: Pursuant to a physician’s order, pharmacists shall initiate and monitor Warfarin therapy on a daily basis, according to a protocol that has been approved by the medical staff. Such Warfarin monitoring will be provided by licensed pharmacists who have been certified in Warfarin dosing and monitoring by the Department of Pharmacy Services. Such certification is done by successfully completing the Warfarin dosing training program.
PROCEDURE/TECHNIQUE/GUIDELINES:
1. Pursuant to a physician’s order, a certified pharmacist shall initiate, dose, and monitor Warfarin therapy on a daily basis, according to protocol approved by the medical staff.
2. The pharmacist shall review the patient’s laboratory data, age, physical characteristics, signs and symptoms of bleeding, current and past drug therapy, and assessments made by other healthcare professionals before formulating a plan of action. The pharmacist shall determine the Warfarin dose, dosing frequency, route of administration, and needed laboratory monitoring.
3. Pharmacists shall be certified in Warfarin dosing and monitoring by the Department of Pharmacy Services. Pharmacists shall complete a training program, including reading materials, demonstrated competency as determined by the Clinical Coordinator and supervising certified Warfarin pharmacists, and successfully completing a written assessment test.
4. Certified pharmacists’ competency will be reassessed on an annual basis by the Clinical Coordinator.

26 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL B Measures for Adverse Drug Event Related to
Warfarin, Heparin, Enoxparin, and other Anticoagulants See Chapter 4.

27 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL C Med Watch Form (Page 1 of 2)

28 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL C Med Watch Form (Page 2 of 2)

29 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL D Weight Based Heparin Protocol Order Form
Date ______________________________________ 1. Patient’s weight:________________kg
• Maximum dosing weight—100kg • (Dose any patients > 100kg at 100kg
2. Bolus Heparin: 80 units/kg = _________________ units • Maximum 8,000 units bolus •
3. Heparin Infusion: 25,000 unites/250 ml D5W or NS (100 units/ml) Initial infusion rate 18 units/kg/hr = ______________ units/hr (____________ ml/hr) • Maximum 1,800 units/hr •
4. Laboratory: • PTT, CBC NOW • STAT PTT 6 hours after initial bolus (and 6 hours after any change) • PTT every 24 hours (once therapeutic) • CBC every other day while on Heparin
5. Adjust Heparin infusion based on sliding scale below:
PTT Bolus Dose
Stop Infusion
for minutes
Rate/Change Repeat ATT
< 35 sec
80 u/kg 0 + 4 u/kg/hr 6 hrs
36-45 sec
40 u/kg 0 + 2 u/kg/hr 6 hrs
46-70 0 0 0 (no change)
next AM
71-90 0 0 - 2 u/kg/hr 6 hrs > 90 sec 0 60 - 4 u/kg/hr 6 hrs
6. Order a PTT 6 hours after any dosing change, adjusting Heparin infusion by the sliding scale until
PTT is therapeutic (46-70 seconds). When 2 consecutive PTT’s are therapeutic, order PTT every 24 hours, and readjust Heparin drip as needed.
7. In the event that an IV Heparin infusion should infiltrate, the following guidelines shall be used. If the IV has been infiltrated less than 4 hours, rebolus with the amount that would have infused during the time (units per hour x approximate hours infiltrated). If the IV has been infiltrated for more than 4 hours, the physician must be contacted for a restart order.
Please make changes as promptly as possible and round off to the nearest ml/hr (100 units/hr) M.D./D.O. Signature: _________________________________________________
Courtesy of St. Vincent Charity Hospital, Cleveland, Ohio

30 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL E Physician Order form for Heparin and Enoxaparin (Page 1 of 2)

31 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL E Physician Order form for Heparin and Enoxaparin (Page 2 of 2)

32 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL F Warfarin Dosing Protocol (Page 1 of 5)
Ball Memorial Hospital
Department of Pharmacy Services
Warfarin Dosing Protocol Updated April 12, 2007
Patient Inclusion Criteria (new addition 4/12/07): Patients included in this protocol are adults 18 years of age or older.
Exclusion Criteria (new edition 4/12/07): The following patients are excluded form this protocol: patients younger than 18 years of age, active bleeding, have an epidural catheter in place, have or will undergo a ventriculostomy, lumbar puncture within 24 hours.
Initiating a request for Pharmacist management of Warfarin therapy per pharmacy protocol (new addition 4/12/07): The physician must write or give a verbal order for “pharmacist to dose Warfarin per protocol”. The order shall also include the desired target INR and the indication for Warfarin.
Initiation of Therapy: Physicians may request pharmacists to dose Warfarin (Coumadin®) according to this protocol, stating in their order the indication for Warfarin and the target International Normalized Ratio (INR). Upon receiving such an order, a pharmacist certified in Warfarin dosing will review the patient’s chart for indication, conditions affecting Warfarin sensitivity, coagulation labs, potential drug interactions with Warfarin, and other medical information pertinent to Warfarin dosing. The pharmacist will dose Warfarin and order INRs as appropriate. The pharmacist will write a daily progress note in the chart pertaining to the patient’s anticoagulation therapy. All Warfarin doses will be administered at 8pm. When requests for pharmacists to dose Warfarin per protocol are received after 11 PM, the pharmacist will inform the physician that the physician will need to order the first dose of Warfarin. In such instances, the pharmacist will begin dosing of Warfarin the next day.
Unless otherwise specified by the physician, the targeted INRs used to guide Warfarin therapy will be those recommended by the most recent American College of Chest Physicians (ACCP) Consensus Conference on Antithrombotic Therapy (1). Thus, targeted INRs are:
Indication INR
Prophylaxis of venous thrombosis (orthopedic surgery) 1.5 – 2.2*
Prophylaxis of venous thrombosis (other than high-risk surgery) 2.0 – 3.0
Treatment of Deep Vein Thrombosis/Pulmonary Embolism 2.0 – 3.0
Prevention of systemic embolism
Tissue heart valves 2.0 – 3.0
Acute Myocardial Infarction (to prevent systemic embolism) 2.0 – 3.0
AMI (to prevent recurrent MI) 2.5 – 3.5
Valvular heart disease 2.0 – 3.0
Atrial Fibrillation 2.0 – 3.0
Bileaflet mechanical valve in aortic position 2.0 – 3.0
Mechanical prosthetic valves (high risk) 2.5 – 3.5
Presence of Lupus Anticoagulant or Antiphospholipid Antibodies 2.5 – 3.5
* deviates from ACCP guidelines at the request of the BMH orthopedic surgeons

33 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL F Warfarin Dosing Protocol (Page 2 of 5)
Guidelines for Selecting Initial Warfarin Doses:
If a patient is admitted on a maintenance dose of Warfarin, check the INR. If the INR is therapeutic, continue that maintenance dose. Added 4/12/07.
Otherwise, the initial starting doses of Warfarin will be those listed in the following table. Pharmacists may select a lower or higher starting dose of Warfarin as the patient’s condition or medical history warrants.
Patient Condition Suggested Daily Warfarin Dose
Previously on Warfarin Continue previous regimen if INR is in target range
69 years or younger 5 mg
DVT prophylaxis following joint replacement 5 mg per total joint pathway
70 years old or older 4 mg
Impaired nutritional status 4 mg
Acute or exacerbation of Congestive Heart Failure 4 mg
High Risk of Bleeding 4 mg or less
Selecting a Warfarin maintenance dose:
For patients 70 years of age or older, the method of Siguert et al (4) suggests giving a fixed initial dose for the first two days of Warfarin therapy and then obtaining an INR the next morning to guide the selection of a maintenance dose as outlined in the following table.
Suggested algorithm for selecting a Warfarin maintenance dose in inpatients 70 years old and older when the target INR is 2.0to 3.0
If day 3 INR result is: Suggested maintenance dose is:
Less than 1.3 5 mg
1.3 to 1.4 4 mg
1.5 to 1.6 3 mg
1.7 to 1.8 2 mg
1.9 to 2.4 1 mg
2.5 and higher Measure INR daily and omit Warfarin doses until INR is less than or equal to 2.4
Adapted from Siguret V, Gouin I, Debray M, et al. Initiation of Warfarin therapy in elderly medical inpatients: a safe and accurate regimen. Amer J Med 2005;118:137-42.
For patients younger than 70 years old, the following table may be used to guide dosing (added 4/12/07)
Day of Warfarin therapy INR Value Dose of Warfarin to give
Day 3 < 1.5 1.5 – 1.9 2.0 – 2.5 2.6 – 3.0 > 3.0
Between 5 and 10 mg (should this between 5 and 7.5 mg??) 2.5 – 5 mg 0 – 2.5 mg 0 – 2 mg No dose

34 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL F Warfarin Dosing Protocol (Page 3 of 5)
Day of Warfarin therapy INR Value Dose of Warfarin to give
Day 4 < 1.5 1.5 – 1.9 2.0 – 3.0 > 3.0
10 mg 5 – 7.5mg 0 – 5 mg No dose
Day 5 < 1.5 1.5 – 1.9 2.0 – 3.0 > 3.0
10 mg 7.5 – 10 mg 0 – 5 mg No dose
Day 6 < 1.5 1.5 – 1.9 2.0 – 3.0 > 3.0
7.5 – 12.5 mg 5 – 10 mg 0 - 5mg No dose
Management of Elevated INRs Post-Operative Patients (including orthopedic surgery patients) – The following guidelines will be used in recommending to physicians doses of vitamin K to reverse excessive anticoagulation.
Warfarin Reversal Guidelines (Adapted from 7th ACCP Consensus Conference on Antithrombotic Therapy) INR Symptoms/Situation Treatment < 5.0 no clinically significant bleeding
and rapid reversal for surgery is unnecessary
Lower dose or omit the next dose and resume at a lower dose. If only minimally above therapeutic range, no dose reduction may be required.
5.0 - 9.0 no clinically significant bleeding and rapid reversal for surgery is unnecessary no clinically significant bleeding but rapid reversal for surgery is required
If no additional risk factors for bleeding: Omit next 1-2 doses, re-check INR, and resume Warfarin at a reduced dose. If at increased risk of bleeding: Omit next dose of Warfarin and give vitamin K1 (≤5mg)* po. Give vitamin K1 2-4mg* po (to reduce INR within 24 hrs). If INR remains high after 24 hrs, an additional 1-2mg* of vitamin K1 may be given.
≥ 9.0 no clinically significant bleeding Hold Warfarin and give vitamin K1 5-10mg* po (to reduce INR within 24-48 hrs). Monitor INR closely. May repeat vitamin K1 if necessary. Resume therapy at lower dose when INR therapeutic.
Any serious bleeding Hold Warfarin and give vitamin K1 10mg by slow IV infusion and supplement with fresh plasma transfusion or prothrombin complex concentrate. Recombinant factor VIIa may be considered as alternative to prothrombin complex concentrate. (Note: Factor VIIa (NovoSeven ® is available from BMH Blood Bank) May repeat vitamin K1 q12h as necessary.
Any life-threatening bleeding Hold Warfarin and give prothrombin complex concentrate and supplement with vitamin K1 10mg given by slow IV infusion. Recombinant factor VIIa may be considered as alternative to prothrombin complex concentrate. May repeat as necessary.
* Only 5mg scored tablets commercially available (2.5mg is possible but other strengths are not) If Warfarin is discontinued for any reason the patient is no longer a Warfarin protocol patient. The physician must re-order for the pharmacist to dose Warfarin per protocol if s/he wants Warfarin managed per pharmacy protocol.(added 4/12/07)

35 | A n t i - C o a g u l a n t T o o l k i t
RESOURCE TOOL F Warfarin Dosing Protocol (Page 4 of 5)
If Warfarin is discontinued and re-started using the Warfarin protocol, the pharmacist may restart on the previous dose of Warfarin if the INR was in the desired therapeutic range prior to being discontinued.(added 4/12/07) If a patient requires an invasive procedure that necessitates Warfarin being held or anticoagulation reversal, the patient will no longer be treated using the protocol. (added 4/12/07)
Management of Warfarin During Invasive Procedures For emergent invasive procedures, vitamin K can be used to reverse effects of Warfarin (see above). The following recommendations are from ACCP1:
Risk of thromboembolism Recommended procedure
Low risk (no thromboembolism for > 3 months, atrial fibrillation patients without a history of stroke or other risk factors, and bileaflet mechanical cardiac valve in aortic position)
Stop Warfarin approximately 4 days before surgery, allow INR to return to near-normal level, briefly administer post-op prophylaxis (if the intervention itself creates a higher risk of thrombosis) using Heparin 5,000 units SC or a prophylactic dose of enoxaparin and simultaneously begin Warfarin therapy; alternatively, a low dose of UFH or a prophylactic dose of LMWH can also be used preoperatively.
Intermediate risk of thromboembolism Stop Warfarin approximately 4 days before surgery, allow the INR to fall, cover the patient with Heparin 5,000 units SC beginning 2 days before surgery or with a prophylactic dose of LMWH, and then commence low-dose Heparin (or LMWH) and Warfarin postoperatively; some individuals would recommend a higher dose of Heparin or a full dose of LMWH in this setting
High risk of thromboembolism (patients with recent [< 3 months] history of DVT, or mechanical cardiac valve in the mitral position or an old model of cardiac valve [ball/cage])
Stop Warfarin therapy approximately 4 days before surgery, allow INR to return to normal, begin therapy with full-dose Heparin or full-dose LMWH as the INR falls (approx 2 days before surgery). Heparin infusion should be discontinued 5 hours before surgery with the expectation that the anticoagulant effect will have worn off at the time of surgery; it is also possible to continue with SC Heparin or LMWH and to stop 12-24 hours before surgery with the expectation that the anticoagulant effect will be very low or have worn off at the time of surgery
Low risk of bleeding
Continue Warfarin therapy at a lower dose and operate at an INR or 1.3 to 1.5, an intensity that has been shown to be safe in gynecologic and orthopedic surgical patients; the dose of Warfarin can be lowered 4 or 5 days before surgery; Warfarin therapy can then be restarted postoperatively, supplemented with a low dose of UFH (5000 units SC) or a prophylactic dose of LMWH (enoxaparin) if necessary
Adapted from Table 8 in: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004 (suppl) 126:214S-215S. Management of enoxaparin (Lovenox ®), fondaparinux (Arixtra ®) or unfractionated Heparin (UFH) when used in combination with Warfarin. New addition 8/12/05

36 | C h a p t e r 2 : S e l f - A s s e s s m e n t
RESOURCE TOOL F Warfarin Dosing Protocol (Page 5 of 5)
It is commonplace to use either unfractionated Heparin (UFH) or a low molecular weight Heparin (LMWH) (e.g. enoxaparin (Lovenox ®), fondaparinux (Arixtra ®)) in combination with Warfarin in order to provide an immediate anticoagulant effect until the Warfarin regimen reaches a target therapeutic INR. This protocol authorizes the pharmacist to discontinue any concurrent UFH or LMWH once the INR has been in the desired target range for 2 consecutive days and the patient has received at least five total days of Heparin or LMWH therapy and Heparin or LMWH will not be discontinued before three days of bridge therapy (new addition 4/12/07)
Frequency of INR Monitoring INRs will be obtained daily. Once the INR is in the desired target range for two or more consecutive days, the frequency of INR monitoring may be reduced.
Frequency of Pharmacists leaving Warfarin dosing notes in patient’s charts (new addition 4/12/07) Requirements for pharmacists leaving Warfarin notes for dosing per protocol in patient charts: (added 4/12/07) Initial notes to include: Patient’s age, weight, allergies, presence or absence of liver disease, baseline/initial PT/INR, Baseline/initial hematocrit, indication for Warfarin, goal INR, list any known interacting medications, list any concomitant anticoagulation (e.g. Heparin, LMWH), statement regarding plan of action, dose, whether or not patient was on Warfarin prior to admission, was therapeutic, etc Subsequent notes shall be left daily until INR has been in the desired INR range for 2 or more consecutive days whereupon, notes may then be left every third day or more frequently if needed. These notes shall include the following information: indication, goal INR, PT/INR, hematocrit, dose, statement regarding plan f action, any complications, interacting medications and any other pertinent information. References: 1. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: The Seventh ACCP
Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126 (suppl):204S-233S. 2. American Geriatrics Society. The use of oral anticoagulants (Warfarin) in older people. J of the Amer Geriatrics Society
2002;50:1439-1445. 3. Garcia D, Regan S, Crowther M, et al. Warfarin maintenance dosing patterns in clinical practice: implications for safer
anticoagulation in the elderly population. Chest 2005;127:2049-2056 4. Siguret V, Gouin I, Debray M, et al. Initiation of Warfarin therapy in elderly medical inpatients: a safe and accurate regimen.
Amer J Med 2005;118:137-42. Originally developed by: Kelly Wolfe, Pharm.D., December 2002 Approved by: Pharmacy & Therapeutics Committee, January 28, 2003
Revised and Updated by: R. Brian Wolfe, Pharm.D., BCPS, January 12, 2006; April 12, 2007

37 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL G Pharmacy Heparin Dosing Service (Page 1 of 3)
Flow Sheet for Tracking Heparin and Warfarin
MD ___________________________________ PTT Parameters ________________________
Started in ER
Transferred from other Institution
GP IIb/IIIa inhibitor ___________________
Received Lovenox in past 8 hr
Taking Coumadin Prior to Admission HT _____________ ABW _____________ LBW _____________ DW _____________
Cardiovascular / Vascular Protocol *Follow thrombolytic protocol if patient has received TNK DVT / PE Protocol
Stroke Prosthetic valve
Unstable angina/MI Vascular surgery
Post coronary intervention
Other_________________________________________
DVT
PE
Vascular alteplase with Heparin
DATE
TIME
PTT
BOLUS DOSE/
HOLD TIME INFUSION
RATE PLT
COUNT RPH
WARFARIN
DOSE INR

38 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL G Pharmacy Heparin Dosing Service (Page 2 of 3)
Flow Sheet for Tracking Heparin and Warfarin
A. If the physician specifies a desired PTT range different from the pharmacy standard, the sliding scale protocol will be altered.
B. Notify MD if: 1. Two consecutive PTTs are > 200 or < 31 2. If the platelet count decreases to < 100,000 or decreases by > 50% from baseline
C. Round all infusion doses to nearest 50 Units/hour D. TPA for PE
1. TPA dose = 100 mg IV over 2 hours 2. TPA may be given up to 14 days following diagnosis of PE (not MI or stroke) 3. Heparin is not recommended to be given concomitantly with TPA.
a. If Heparin has been started before TPA, discontinue Heparin for 1-2 hours and restart when PTT < 2 x normal.
b. If Heparin has not been initiated, start at the completion of the TPA infusion. 4. Upon initiation of Heparin, follow DVT/PE protocol. The first 24h should be more conservative with PTT
range of 60-80. E. TPA for Stroke
Do not start Heparin for 24 hours after the completion of TPA Upon initiation of Heparin, follow the cardiovascular protocol NOT the thrombolytic protocol
F. LBW male = 50 kg + 2.3 (Ht” – 60”) LBW female = 45.5 kg + 2.3 (Ht” – 60”) Dosing Weight = {(ABW – LBW) x 0.4} + LBW
G. Pharmacist may use clinical judgment for protocol adjustments
C-V / Vascular Protocol Load: 60 Units/kg
Initial Infusion: 12 Units/kg/hr
PTT (sec)
BOLUS DOSE (units/kg)
STOP INFUSION (minutes)
RATE CHANGE (units/kg/hr)
NEXT PTT
< 31
50 0 + 4
6 hrs
31-47
30 0 + 2
6 hrs 48-66
0 0 No change
Next AM
67-78 67-78 on Coumadin
0 0
0 0
- 2
- 3
6 hrs
6 hrs
79-95 79-95 on Coumadin
0 0
30
30
- 3
- 4
6 hrs
6 hrs
96-160 96-160 on Coumadin
0 0
60
60
- 4
- 5
6 hrs
6 hrs
> 160
0 60 - 5
6 hrs

39 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL G Pharmacy Heparin Dosing Service (Page 3 of 3)
Flow Sheet for Tracking Heparin and Warfarin
DVT/PE Protocol Load: 80 Units/kg
Initial Infusion: 18 Units/kg/hr PTT (sec)
BOLUS DOSE (units/kg)
STOP INFUSION (minutes)
RATE CHANGE (units/kg/hr)
NEXT PTT
< 31
50 0 + 4
6 hrs
31-47
30 0 + 2
6 hrs 48-66
0 0 No change
Next AM
67-78 67-78 on Coumadin
0 0
0 0
- 2
- 3
6 hrs
6 hrs

40 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL H Warfarin Monitoring Flow Sheet
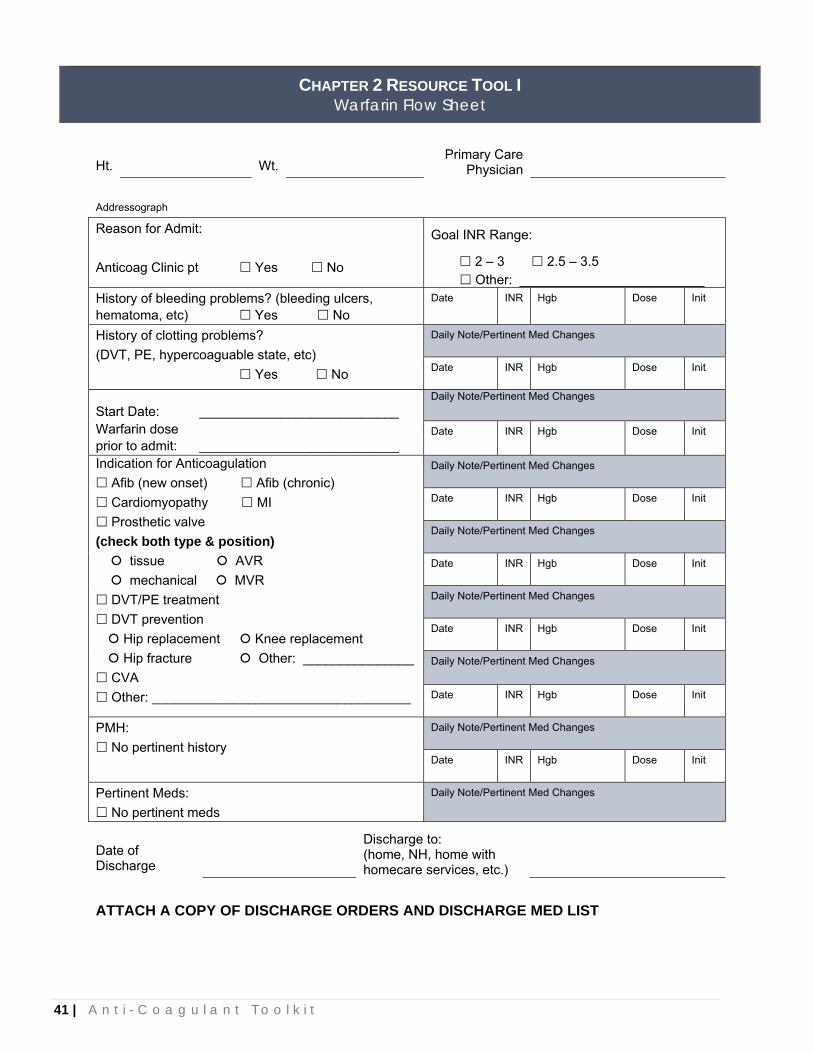
41 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL I Warfarin Flow Sheet
Ht. Wt. Primary Care
Physician Addressograph Reason for Admit: Anticoag Clinic pt Yes No
Goal INR Range:
2 – 3 2.5 – 3.5 Other: _________________________
History of bleeding problems? (bleeding ulcers, hematoma, etc) Yes No
Date INR Hgb Dose Init
History of clotting problems? (DVT, PE, hypercoaguable state, etc) Yes No
Daily Note/Pertinent Med Changes Date INR Hgb Dose Init
Start Date: ___________________________ Daily Note/Pertinent Med Changes
Warfarin dose prior to admit: ___________________________
Date
INR Hgb Dose Init
Indication for Anticoagulation Afib (new onset) Afib (chronic) Cardiomyopathy MI Prosthetic valve
(check both type & position) tissue AVR mechanical MVR
DVT/PE treatment DVT prevention
Hip replacement Knee replacement Hip fracture Other: _______________
CVA Other: ___________________________________
Daily Note/Pertinent Med Changes Date INR Hgb Dose Init
Daily Note/Pertinent Med Changes Date INR Hgb Dose Init
Daily Note/Pertinent Med Changes Date INR Hgb Dose Init
Daily Note/Pertinent Med Changes Date INR Hgb Dose Init
PMH:
No pertinent history Daily Note/Pertinent Med Changes Date INR Hgb Dose Init
Pertinent Meds:
No pertinent meds Daily Note/Pertinent Med Changes
Date of Discharge
Discharge to: (home, NH, home with homecare services, etc.)
ATTACH A COPY OF DISCHARGE ORDERS AND DISCHARGE MED LIST

42 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL J Anticoagulation Review (Page 1 of 3)
Unfractionated Heparin Rapid-acting parenteral anticoagulant. Uses: Prophylaxis of DVT/PE, Treatment of DVT/PE, Thrombosis due to atrial fibrillation, and Acute
Coronary Syndrome/MI. The prophylaxis dose is 5000 units Subcu every 8 – 12 hours. This dose is not high enough to elevate
aPTT, therefore aPTT does not need to be monitored. Treatment doses are administered by continuous IV infusion and are based on actual body weight (when
calculating the dose do not exceed 100 Kg total body weight. A bolus dose is required to more quickly achieve therapeutic level. The initial dose is an 80 units/kg bolus, and then 18 units/kg/hour.
Patient’s aPTT should be monitored every 6 hours for 24 hours and then until stable. Once the aPTT is stable, it should be monitored once daily. Dose changes should be based on the patient’s aPTT according to the hospital’s Heparin continuous IV infusion algorithm.
Adverse effects include: bleeding, thrombocytopenia, osteoporosis (with long-term use), and hyperkalemia.
Heparin-induced thrombocytopenia (HIT) is a drop in platelets to less than 100,000/mm3 or by greater than 50%. It is antibody mediated and has a delayed onset of 5-14 days. When a patient experiences HIT, all forms of Heparin should be stopped and the patient should never receive Heparin again. HIT can cause venous and arterial thrombosis and leads to amputation in 25% of cases and death in 25-30% of cases.
Contraindications include: History of HIT, Active bleeding, and Hypersensitivity. The effects of Heparin can be reversed by holding the infusion, transfusions with fresh frozen plasma or
whole blood, or protamine.
Low Molecular Weight Heparin (i.e. Lovenox®) Derived from unfractionated Heparin. Uses: Prophylaxis of DVT/PE, Treatment of DVT/PE, and Acute MI/Unstable Angina. The prophylaxis dose is 40 mg subcu daily for patients with normal renal function, or 30 mg subcu
daily for patients with impaired renal function (CrCl < 30 ml/min). The treatment dose is 1 mg/Kg subcu BID for patients with normal renal function, or 1 mg/Kg subcu
daily for patients with impaired renal function (CrCl < 30 ml/min). Low molecular weight Heparin does not elevate aPTT. Anti-factor Xa concentrations can be monitored,
but therapeutic monitoring is not beneficial in most patients. Adverse effects include: bleeding, thrombocytopenia, and pain at the injection site. Low molecular weight Heparin does carry a black box warning for risk of epidural/spinal hematoma. Contraindications include: History of HIT, Active bleeding, and Hypersensitivity. The effects of Heparin can be reversed by holding doses, transfusions with fresh frozen plasma or whole
blood, or protamine. The advantages of low molecular weight Heparin over unfractionated Heparin include: longer half-life,
lower incidence of HIT, less routine laboratory monitoring, patient can self-administer and can potentially be treated outpatient.

43 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL J Anticoagulation Review (Page 2 of 3)
Coumadin® (Warfarin) Interferes with the hepatic synthesis of vitamin K dependent clotting factors II, VII, IX, and X, as well as
endogenous anticoagulant proteins C and S. Uses: DVT/PE Treatment, DVT/PE Prophylaxis, and Prevention of thromboembolic events with Prosthetic
heart valves, Acute MI, Atrial fibrillation, and Inherited clotting disorders. The onset of action is 36-72 hours, and full antithrombotic effect may take up to 15 days. Warfarin may
even increase the risk of clotting for a few days. Therefore, when treating a thromboembolic event, Warfarin and Heparin are started simultaneously.
The gold standard for monitoring Warfarin therapy is the International Normalized Ratio (INR). INR should be monitored daily while in the hospital.
Adverse effects include: bleeding, skin necrosis, and purple toe syndrome. Contraindications include: Pregnancy, Active bleeding, and Hypersensitivity. Warfarin has numerous interactions with food and drugs.
- An increase intake of vitamin K (green leafy vegetables) will decrease the effectiveness of Warfarin. Smoking, alcohol, phenytoin, rifampin, carbamazepine, and barbiturates will also decrease the effectiveness of Warfarin by increasing its elimination.
- Drugs such as amiodarone, fluconazole, metronidazole, sulfamethoxazole, cimetidine, ciprofloxacin, clarithromycin, erythromycin, fluoxetine, and grapefruit juice can increase the effects of Warfarin by decreasing the metabolism.
- Aspirin, clopidogrel, and NSAIDs can increase the risk of bleeding associated with Warfarin. Patient education for Warfarin should include: signs and symptoms of bleeding, signs and symptoms of a
clot, possible drug interactions, need for consistency in Vitamin K foods, importance of monitoring INR, what to do when a dose is missed, and knowing which strength and color of tablet they use.
Vitamin K (phytonadione) Because Warfarin interferes with the hepatic synthesis of vitamin K dependent clotting factors, giving vitamin
K can reverse the effects of Warfarin. When using vitamin K, the lowest dose possible to reverse the effects should be given. If a patient has an INR ≥ 5 but < 9 with no significant bleeding, give vitamin K 1-2.5 mg orally. If a patient has an INR ≥ 9 with no significant bleeding, give vitamin K 3-5 mg orally. If INR is not
significantly improved in 24 – 48 hours, additional vitamin K can be given. If a patient has an INR > 20 or serious bleeding regardless of the INR, give vitamin K 10 mg by slow IV
infusion. If a patient has life-threatening bleeding, give vitamin K 10 mg by slow IV infusion along with prothrombin
complex concentrate.

44 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL J Anticoagulation Review (Page 3 of 3)
Initial Coumadin Dosing Protocol:
Goal INRs are based on patient diagnosis:
• Acute myocardial infarction: 2 – 3 • Atrial fibrillation: 2 – 3 • Mechanical heart valve: 2.5 – 3.5 • Cardioembolic cerebral ischemic events: 2 – 3 • Thromboembolism: 2 – 3
References: Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In Dipiro JP, et al, eds. Pharmacotherapy, A Pathophysiologic Approach, 6th ed. New York, NY: McGraw-Hill; 2005. p. 373-410. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126:163S-696S.
Day INR Dose 1 < 1.5
≥ 1.5 5 mg Determine patients current regimen
2 < 1.5 1.5 – 1.9 2.0 – 2.5 2.5 – 3.0 > 3.0
5 mg 5 mg 2.5 mg 1 mg Hold dose
3 < 1.5 1.5 – 1.9 2.0 – 2.5 2.5 – 3.0 > 3.0
5 mg 5mg 2.5 mg 1 mg Hold dose
4 < 1.5 1.5 – 1.9 2.0 – 2.5 2.5 – 3.0 > 3.0
5 mg 5 mg 5 mg 2.5 mg Hold dose
5 < 1.5 1.5 – 1.9 2.0 – 2.5 2.5 – 2.9 3.0 – 3.5 > 3.5
5 mg 5 mg 5 mg 2.5 mg 1 mg Hold dose
6 < 1.5 1.5 – 1.9 2.0 – 2.9 3.0 – 3.5 > 3.5
7.5 mg 7.5 mg 5 mg 2.5 mg Hold dose
Dosing Protocol for Maintenance Coumadin: INR Dose Adjustment for Goal INR 2-3< 2 Increase dose by 5-15% 3.1 – 3.5 Decrease dose by 5-15% 3.6 – 4.0 Hold 1 dose, then decrease dose by 10-
15% 4.1 – 5.9 Hold 2 doses, then decrease dose by 10-
15% > 6 Hold and follow daily INRs
INR Dose Adjustment for Goal INR 2.5 – 3.5< 2.5 Increase dose by 5-15% 3.6 – 4.0 Decrease dose by 5-15% 4.1 – 4.5 Hold 1 dose, then decrease dose by
10-15% 4.6 – 5.9 Hold 2 doses, then decrease dose by
10-15% > 6 Hold and follow daily INRs

45 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL K Warfarin Management Test (with Key) (Page 1 of 4)
Pharmacist Name: ___________________________ Date: _________________________________ 1. Which of the following are Vit K dependent? (1 point)
a) Protein C b) Protein S c) Factors II, VII, IX d) Both a & b
2. Which statement is false as to why the elderly typically require lower maintenance doses of Warfarin? (1 point)
a) Lower body weight b) Renal dysfunction c) Multiple medications and disease states d) Lower albumin concentrations
3. What is the rationale for over-lapping Heparin and Warfarin n therapy? (1 point)
a) Delayed antithrombotic effect of Warfarin b) Warfarin may induce a transient hyper-
coagulable state c) Heparin and Warfarin do not need to be
overlapped d) Both a and b e) None of the above
4. VG received a St. Jude mitral valve replacement. Pharmacy has been consulted to dose the Warfarin. Which of the following statements are true? (1 point)
a) The goal INR is 2.5-3.5 b) The goal INR is 2.0-3.0 c) Patients with a mitral valve are less at risk of
thromboembolism than patients with an aortic valve
d) Therapy should be continued indefinitely e) Both a and d
5. KC is a 45 year old, 310 lb male who just had an anterior wall myocardial infarction with an urgent CABG. Pharmacy has been consulted to dose the Warfarin. His medications include atenolol, lisinopril and nitroglycerin prn. Which of the following statements are true? (1 point) a) The goal INR is 2.5-3.5 b) Therapy should be continued indefinitely c) Most mural thrombi form within 1 week of the infarction d) A reasonable starting dose would be 15mg e) Both a and c 6. DS is a 70 year old, 180 lb male who just had a total hip arthroplasty for osteoarthritis. Dr. Anderson has checked Coumadin per Pharmacy. Which of the following statement is false? (1 point) a) The goal INR is 2.0-3.0 b) The optimal duration of therapy is 4-5 weeks c) The risk of venous thromboembolism persists for 2 weeks postoperatively d) A reasonable starting dose for this patient would be 5mg 7. Which of the following statement is false regarding atrial fibrillation? (1 point) a) Risk of stroke increases with age, diabetes, history of previous stroke or TIA, and hypertension b) Patients >75 years old with atrial fibrillation should be treated with Warfarin c) Normal atrial contractility resumes immediately following return to normal sinus rhythm d) Coumadin should be given three weeks prior a (unless TEE reveals no thrombi) and 4 weeks after direct-current cardioversion

46 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL K Warfarin Management Test (with Key) (Page 2 of 4)
8. Indicate whether the following statements are True (T) or False (F) (1/2 point each) T Protein C and S are body’s own natural anticoagulants and are inhibited by coumadin F The R-enantiomer of Warfarin is 5x more potent than the S-enantiomer T The initial prolongation of the prothrombin time is to due factor VII depletion F Amiodarone, cotrimoxazole, and glyburide are major Warfarin interactions T With high doses of Vit. K, Warfarin resistance occur for up to one week F Coumadin is contraindicated in pregnancy and nursing T Warfarin drug interactions may involve CYP P450 2C9. 2C19, and 3A4 inhibitors F Vit. K is useful when the INR needs to be
decreased urgently 9. Indicate whether the following would be expected to Increase (I) or Decrease (D) the effectiveness of Warfarin (1/2 point each) I Liver disease I Congestive heart failure D Hypothyroidism I Diarrhea I Amiodarone I Cimetidine D Carbamazepine I Metronidazole
10. A.G. is a 45 y/o female who presents to the E.R. with c/o progressive SOB and some minor irregularity in heart rate but no sustained dysrhythmia. The patient was admitted to the hospital and MI was ruled out yet was newly diagnosed with A.fib. On the fifth day of hospital stay you review the patient’s Warfarin therapy and recommend: (1 point)
Day INR Dose
Day 1 1.0 7.5mg
Day 2 1.2 7.5mg
Day 3 1.4 7.5mg
Day 4 1.8 5mg
Day 5 2.1
a) 7.5mg b) 5mg c) 10mg d) 2mg

47 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL K Warfarin Management Test (with Key) (Page 3 of 4)
11-13. For the following case examples please indicate what dose of Warfarin you would give based on the patient’s indication, medical history, concurrent medications and laboratory values. Please explain the rationale you used in determining the dose (i.e. patient elderly; interacting medications; INR has risen significantly in 1 day). 1 point for each day. 11. JK is a 71 year old, 5'9", 94 kg, male s/p aortic bioprosthetic valve insertion. His PMH includes COPD, hypothyroidism (stable), and CVA. The physician has checked Warfarin per pharmacy and indicated an INR range of 2.0-2.5.
Current Medications: Levothyroxine 100 mcg daily Lansoprazole 30 mg daily
Triamcinolone MDI Combivent MDI Propoxyphene/APAP prn Heparin gtts
Day
INR
Recommended Dose
Rationale
Day 1 --- 5-7.5 mg Patient is 94 kg so 7.5 mg probably ok, but 5 mg probably better. Thyroid is not an issue since this is stable.
Day 2 1.05 5-7.5 mg Less than 0.3 increase and less than 1.2 so give same dose as the day before.
Day 3 1.81 2-3 mg Greater than 0.5 increase in two days so need to decrease the dose.
Day 4 2.03 4 mg This dose may vary based on what the initial two doses were. The dose should be increased from the day before due to the slowdown in the rise of the INR.
12. MT is a 75yo, 5'6", 84 kg female admitted to FSH because of new onset a. fib. with an uncontrolled ventricular rate. Her PMH includes CAD with history MI and stenting, GERD, and glaucoma. The Minnesota Heart Clinic has consulted pharmacy to dose the Warfarin.
Current Medications: Digoxin 0.125 mg daily Metoprolol XL 50 mg daily
Linsinopril 10 mg daily Atorvastatin 40 mg hs
Day
INR
Recommended Dose
Rationale
Day 1 --- 5 mg No interacting meds, elderly female of larger size.
Day 2
1.00 IV amiodarone load started
5 mg Less than 0.3 increase and not greater than 1.2, so give the same dose as the day before. Slight lowering of dose probably okay. IV amiodarone tends to have an earlier effect on Warfarin so monitor closely.
Day 3
1.21 5 mg Less than 0.3 increase in two days, but it is close and IV amiodarone has been started so give 5 mg again.
Day 4
1.90 2-3 mg Significant jump in INR and greater than 0.5 INR increase in two days, so decrease dose.
Day 5
2.08 3-4 mg INR rise has slowed down and full effects of the 2 mg dose has not been realized.

48 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL K Warfarin Management Test (with Key) (Page 4 of 4)
13. EJ is an 82 year old, 5'8", 178 lb, male admitted for a left leg deep vein thrombosis. His PMH includes history of PE, peptic ulcer disease (without history of bleeding), and degenerative joint disease. Pharmacy has been consulted to dose the Warfarin.
Current medications: Metoprolol 25 mg bid Fenofibrate 200 mg daily
Lansoprazole 30 mg daily Heparin gtt
Day INR Recommended Dose Rationale
Day 1 1.13 5-7.5 mg Although patient is elderly and of average size, he is a high risk due to his history of PE so will error on the high side.
Day 2 1.02 5-7.5 mg Less than 0.3 increase in the INR and less than 1.2 so give the same dose.
Day 3 1.32 5-7.5 mg 0.3 increase over two days, so give the same dose.
Day 4 2.06 2.5-3 mg INR has risen rapidly and > 0.5 increase over two days so decrease the dose. 3 mg is still fairly aggressive, but we want to assure he does not fall below 2.0.
Day 5 3.57 1-2 mg INR is greater than therapeutic range and 1.5 increase in one day, but patient is high risk and we have not seen the full effects of the 3 mg dose so DO NOT HOLD.

49 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL L Annual Education (Page 1 of 2)
Anticoagulation (with key)
1. Treatment doses of unfractionated Heparin should be administered by which of the following methods?
a. IM injections. b. Continuous IV infusion. c. Subcutaneous injection. d. Orally.
2. Which of the following can be sued to reverse the effects of Heparin?
a. Protamine. b. Vitamin K. c. Fresh frozen plasma. d. Both a & c.
3. In regards to Heparin-induced thrombocytopenia (HIT), which of the following statements is not true?
a. If a patient experiences HIT, Heparin or low molecular weight Heparin can be used again in this patient after a year.
b. HIT is defined by a drop in platelets to less than 100,000/mm3 or a drop in platelets by greater than 50%.
c. When a patient experiences HIT, all sources of Heparin must be stopped immediately.
d. Death will occur in about 25-30% of cases with HIT.
4. Which of the following is an advantage of low molecular weight Heparin (i.e. Lovenox®) over unfractionated Heparin?
a. Low molecular weight Heparin has a lower incidence of thrombocytopenia (HIT).
b. Low molecular weight Heparin requires less routine laboratory monitoring.
c. Low molecular weight Heparin can be self-administered by patients.
d. All of the above are advantages of low molecular weight Heparin over unfractionated Heparin.
5. What is the appropriate dose of Lovenox® (enoxaparin) for prevention of Deep Vein Thrombosis in a patient who weighs 70 Kg and has a reduced creatinine clearance of 15 ml/min?
a. 40 mg Subcu daily. b. 70 mg Subcu daily. c. 30 mg Subcu daily. d. 70 mg Subcu BID.
6. What is the rationale for over-lapping Heparin and Coumadin® (Warfarin) therapy?
a. Delayed antithrombotic effect of Warfarin. b. Warfarin may induce a transient
hypercoagulable state (increased risk of clotting).
c. Heparin and Warfarin do not need to be overlapped.
d. Both a & b.
7. For a patient who has just received a St. Jude mitral valve replacement, which of the following statements is true?
a. The goal INR is 2.5 – 3.5. b. The goal INR is 2 – 3. c. The goal INR is 1.5 – 2.5.
8. Which of the following medications will increase the effectiveness of Coumadin® (Warfarin) (increase the INR)?
a. Rifampin b. Phenytoin c. Bactrim d. Carbamazepine
9. Which of the following medications is a Pregnancy Category X?
a. Coumadin® (Warfarin) b. Unfractionated Heparin c. Low molecular weight Heparin (i.e.
Lovenox®) d. All of the above

50 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL L Annual Education (Page 2 of 2)
Anticoagulation (with key) Please use the information in question #10 to answer #10 – 12.
10. Patient JD is a 50 year old male who has just been diagnosed with a deep vein thrombosis. The physician would like to treat him with Lovenox® (enoxaparin). He weighs 80 Kg and his renal function is normal. What would be an appropriate treatment dose for JD?
a. 30 mg Subcu BID. b. 40 mg Subcu daily. c. 80 mg Subcu daily. d. 80 mg Subcu BID.
11. The physician would also like to start patient JD on Coumadin® (Warfarin). The goal INR for
patient JD is 2 – 3. What would be an appropriate starting dose?
a. 5 mg PO daily. b. 10 mg PO daily. c. 5 mg PO BID. d. Do not start Coumadin® (Warfarin) at this time.
11. Patient JD has now been on Coumadin® (Warfarin) for several weeks. His INR today is 3.8.
According to the hospital’s Dosing Protocol for Maintenance Coumadin Adjustments, what adjustments need to be made?
a. No adjustments need to be made. Continue current dose. b. Hold one dose, and then decrease the dose by 10 – 15%. c. Hold the Coumadin until INR is within range, and then resume the current dose. d. Decrease the dose by 50%.
12. Patient JD has an INR of 9.2, but does not have any significant bleeding. What would be an appropriate dose of Vitamin K for this patient?
a. No Vitamin K is needed. b. Vitamin K 3-5 mg PO. c. Vitamin K 20 mg IV infusion
13. Which of the following are important points to include when counseling a patient who has just been started on Coumadin® (Warfarin)?
a. Signs and symptoms of bleeding. b. Consistency of Vitamin K in the diet. c. Possible interactions including OTCs,
herbals, and alcohol. d. The importance of monitoring INR e. All of the above

51 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 2 RESOURCE TOOL M Wishard Hospital Outpatient Anticoagulation Flow Sheet
Wishard Health Services, North Arlington Clinic Indianapolis, Indiana
Patient’s Name MRN
Phone Physician
Indication Duration INR goal
Date PT/INR
POC/venous Current
Regimen New
Regimen Next Lab
MD Notified/ Initials

52 | C h a p t e r 2 : S e l f - A s s e s s m e n t
CHAPTER 2 RESOURCE TOOL N Wishard Hospital Outpatient Warfarin Dosing Card
ANTICOAGULATION CLINIC Wishard Health Services
Your Warfarin dose has been changed. You should now take:
1 mg Red
2 mg Purple
2.5 mg Green
4 mg Blue
5 mg Peach
6 mg Blue-Grn
7.5 mg Yellow
10 mg White
Number of tablets to take each day
Strength
Color
Sun Mon Tues Wed Thur
Fri Sat
Date: Name:
Next Appointment: ANTICOAGULATION CLINIC Wishard Health Services
Your Warfarin dose has been changed. You should now take:
1 mg Red
2 mg Purple
2.5 mg Green
4 mg Blue
5 mg Peach
6 mg Blue-Grn
7.6 mg Yellow
10 mg White
Number of tablets to take each day
Strength
Color
Sun Mon Tues Wed Thur
Fri Sat
Date: Name:
Next Appointment:

53 | A n t i c o a g u l a n t T o o l k i t
Chapter 3: Improving Anticoagulant Processes

54 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
Getting Started
A variety of team members are needed to drive improvement projects. Team composition will vary depending on where a team is in testing and implementation of changes. Use of a Project Team and Testing Teams are described below.
The Project Team should include a champion, a local leader, a data manager, someone with quality improvement experience among others. The team must have an executive sponsor or senior leader who is accountable for the success of the improvement. In turn, this individual holds the rest of the team accountable for testing and keeping to a time line.
The right team is critical to the success of the improvement effort. It is key to choose individuals who are willing to drive improvement, maintain focus on team goals, and develop support necessary for success. Choose the team based on their knowledge of and involvement in anticoagulation management processes and their desire to improve the overall care process. The team members will serve as advocates for rapid improvement in the organization. It is ideal to include representatives from the following areas on the team: Medical Staff, Nursing, Pharmacy, Risk/Quality Management, Nutrition Services, and Administration. Others, such as Information Technology staff and Case Managers, should be included as needed.
See Resource Section: Project Team Member Roles and Responsibilities list
During the project, the team should meet regularly (every other week minimum). The team will develop strategies to drive change through various work processes within the organization, and will confer regularly on team progress. The team will have authority to adjust their process to maximize their efforts. The team will take responsibility for completing project assignments on time, communicate obstacles that prevent completion of assignments, use facts and data in decision making, listen to stakeholder feedback, and communicate project updates and outcomes to all stakeholders.
The agenda items for the initial meetings of the Project Team should include a review of this toolkit to develop a common understanding among the team members of anticoagulant safe practices. Development of a project charter and project plan will help to define the scope of work for the team.
See Resource Section: Project Team Meeting Agenda template
Testing Teams Designing and carrying out tests of change can be completed by a small group; one doctor, one nurse, one pharmacist. Testing Teams are supported by the Project Team. The testing team should meet at the end of each testing phase to discuss what was learned, what changes are needed and plan for the next test. These meetings should be limited to no more than the time needed to answer the test questions. Limiting these meetings to 5 to 10 minutes standing up with a very specific agenda will not only ensure that the project moves forward quickly but also prevent the loss of momentum that takes place with long and scheduled meetings.
The right team is
critical to the success of the improvement
effort.
Improving Anticoagulant Processes

55 | A n t i c o a g u l a n t T o o l k i t
The Project Charter The team should develop a project charter which specifies the project start and length, project members, problem statement, what success will look like, and key measurements. The Joint Commission National Patient Safety Goal on Anticoagulant therapy outlines the rationale and implementation expectations that should be included in the Project Charter.
See Resource Section: Project Charter for reducing likelihood of Patient Harm with Anticoagulation Therapy
The Project Plan The project team should develop a timeline to include the following activities:
Project Timeline- Activity Month 1
Month 2
Month 3
Month 4
Month 5
Review Entire Toolkit
Understand Anticoagulant Safe Practices (Chapter 1)
Conduct Assessment of Current Practices (Chapter 2)
Assess your current processes (FMEA; Self Assessment)
Validate assessment results by observation and/or interview
Review baseline data if available
Improving Anticoagulant Processes (Chapter 3)
Select Project Team members
Develop the Project Plan
Develop Communications Plan for project milestones
Formulate AIMS Statements for identified gaps in performance
Determine ongoing measures to support the AIMS Statements
Develop ideas to test change or create new processes
Evaluate need for Testing Teams and identify key team members
Select test areas (a unit, floor, etc.)
Run Tests of Change using PDSA Worksheets
Measuring Performance (Chapter 4)
Collect and display data/results for Self Assessments, FMEAs, Tests of Changes tried, overall AIMs for improvement
Use Percent Protocol Compliance tool and display results
Use tool for Measuring Harm from ADE’s and display results
Spreading and Sustaining Improvement (Chapter 5)
Complete Spreading Improvement worksheet and determine plan
Complete Sustaining Changes Worksheet

56 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
Formulating Your AIMs Statements
The system or process the team wants to improve depends upon the AIM. The AIM answers the first question in the Model for Improvement, “What are we trying to accomplish?” The team should select specific AIMs for improvement based upon current information available within the organization on anticoagulation practices and completion of the FMEA and/or results of the self assessment/personal observations described in Chapter 2 of the toolkit.
Improving the Process Improvement can be accelerated by intense focus on a specific area and by sustaining support for rapidly conducted, small‐scale “tests of change” using the Plan‐Do‐Study‐Act cycles. These cycles are the methodology for improving care delivery. This accelerated effort is designed around the Model for Improvement and the Plan‐Do‐Study‐Act Cycle.
Model for Improvement Model developers Tom Nolan and his colleagues (Langley, Nolan, Nolan, Norman, Provost, The Improvement Guide, 1996) observed that organizations that are able to make rapid advances seem to have a rudimentary capacity to answer three questions and to set in place small‐scale tests of change that are guided by their answers to these three questions:
1. What are we trying to accomplish? (Establish AIM statements) 2. How will we know that a change is an improvement? (Set criteria for measurement)
State the Team AIMs. - Be clear, concise, targeted. The team will make better progress if the AIM is specific.
Include Numerical Goals.
- A numerical goal will help the team measure improvement and progress. Quantify the AIM by marrying the AIM to a Baseline Measure, which over time will indicate improvement and progress toward achieving successful outcomes. The quantifiable nature of the AIM will assist with planning rapid tests of change using the PLAN‐DO‐STUDY‐ACT cycle mentioned below.
- Do not accept minimal improvement ‐ strive for success. - Maintain focus on the goal - Fifty‐percent improvement can easily slip to 40% or 30% or 20%, but only if the team chooses to accept less.
Examples:
Increase the percent of orthopedic patients receiving Warfarin on Unit A whose treatment was ordered, administered, and managed according to protocol by X % within 2 months.
Reduce the number of adverse drug events associated with heparin use per 100 admissions to Unit B by X % within 6 months.
Increase the percent of patients where a heparin nomogram/protocol is initiated in the ICU by X% within 2 months.
Guidelines for AIM statement development

57 | A n t i c o a g u l a n t T o o l k i t
3. What changes can we make that will result in improvement? (Plan and test changes that may lead to improvement)
Plan, Do, Study, Act Cycle The PDSA Cycle is applied to the PDSA framework to develop tests and implement changes.
Plan: Decide upon the test of change and how it is to be tested. Do: Test the changes, collect data, observe and document effects of the test of change. Study: Analyze and determine what was learned from the tests that were tried. Act: Decide whether the test of change is to be made permanent, modified, or abandoned.
Several tests of change leading to improvement can be successfully applied using the Plan‐Do‐Study‐Act cycle (see Figure 1). Test Cycles include detailed plans to carry out one anticoagulant safe practice. Each test cycle includes the objective of the test, the plan for the test (who, what, where, and when), the data to know if the test worked. The test may need to be rerun more than once as the team improves the process. Tests are generally done on a small scale (one nurse, one unit, one patient), and then expanded if successful. Each test of change should take no more than 30‐60 minutes to plan, and should be completed within 1‐2 weeks. Just enough data is collected to know if the process is working or needs to be changed. Each cycle, when properly done, is informative and provides a basis for further improvement. The model is repeatedly used for each short cycle of change targeted to reaching the aim or goal. Think about this question: “What is the most informative test of a change that you can run or implement by next week related to improving the safe use of anticoagulants? The size of the test is negotiable; “next week” is not. As you discover better ideas or practices that are known to work and you quickly test that change, the more likely you are to identify those changes that can be implemented for sustained improvement.
See Resource Section: Project Team Model for Improvement Checklist
Figure 1: PDSA Cycle
Do Carry out the plan
Document problems and unexpected
observations
Begin data analysis
Study Complete data analysis
Compare data to predictions
Summarize what was learned
Plan Objective
Questions and predictions (why?)
Plan to carry out cycle (who, what, when, where?)
Act What changes are to
be made?
Next cycle?

58 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
Specif
ic Tes
t Cyc
les
A PD
AP
SD
D S
P A
A P
S D
Overall AIM: 75% Reduction of Anticoagulant-Related ADEs
A P
S D
A PSD
AP
SD
APS
D
D S
P A
A P
S D
A P
SD
APS
D
Weight-Based
HeparinProtocol
Pre-mixedSolutions
PTTresults atbedside
NutritionServices
Informed ofWarfarinPatients.
BridgingTherapy
AS
PD
SD
AP
D S
P A
A P
S D
D S
P A
A P
S D
D S
P A
Anticoagulant Safe Practices
Figure 2: Use of test cycles for multiple anticoagulant safe practices
Figure 3: Use of test cycles specific to improving the use of a Heparin Weight Based Protocol.

59 | A n t i c o a g u l a n t T o o l k i t
Tests of Change
Tests of change involving use of approved protocols may include:
1. Copy a protocol from another organization or select one from your own if you have more than one.
2. Ask one doctor, one pharmacist and one nurse to simulate the use of the protocol on one patient.
3. Ask “What will be different if we make this change?”
Examples:
a. Is the protocol easy to use?
b. Did the doctor or nurse fill in all of the required elements?
4. Ask “what worked and what did not?” Modify the protocol based on that feedback.
5. Test the protocol with another doctor, nurse, one patient and pharmacist. If you have a small staff, consider testing with the same people.
6. Modify again if needed.
7. Test the protocol with 3 doctors.
8. Test under different conditions, such as weekends and off‐shifts.
9. If no other changes are needed, introduce the protocol to all other physicians, pharmacists and nurses who are involved in the unit where you have tested the protocol.
10. Once implemented on one unit, consider testing the same protocol on another unit. Because you have already completed testing, the tempo on the second unit should be much quicker and few if any changes will be needed.
11. Test with one, three, and five doctors. Unless changes are needed, you can consider implementing the protocol on the second unit.
12. You can now consider increasing the tempo by testing on several other units at one time.
For safe practices involving “use of approved protocols” teams are encouraged to complete one worksheet for each test cycle. Use of approved protocols implies that there is opportunity for standard processes.
“WHAT?” ‐ The protocol that our patients should receive is based on science.
“HOW?” ‐ The process that supports the delivery of evidence‐based care should be based on systems thinking and can be supported by standardized processes.
Although it may be necessary to have more than one protocol, this need should be based on patient centered care not on the individual preferences of care givers. The goal should be to standardize the processes that deliver the care we believe our patients should receive.
Resource Section: Example PDSA test cycle worksheets for tests cycles 1-3.
Test under different
conditions, such as weekends and
off-shifts.

60 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
Engaging Others
In order to improve the systems we work in, we must engage those who do the work. Generally, there is a small group of individuals who are trained in quality improvement, and they are expected to lead and complete testing and measurement. The reality is that all must be involved.
We must also recognize that asking people to change the way that they do work is difficult. For some, it may be fear of change, for others, it may be that they have invested much in the status quo and are not willing to give it up; and, for some it may be that they do not know how to make improvements or fear consequences if the changes tested are not perfect.
In order to engage all staff (physicians, nurses, pharmacists and all other stakeholders), one must build will. In order to build will convey the importance of quality improvement.
Share data and stories about the present state of the system and the future desired state. Organize educational activities that help staff understand quality improvement and build capacity by
teaching improvement methodologies. Select people who are willing to work with the team. Carve out time from daily duties for testing and analyzing the results. This also demonstrates the
organization’s commitment to quality improvement. Provide support; recognize staff for their QI efforts; provide food and celebrate successes; use friendly
competition to inspire people to action; encourage transparency.
Share successes and be open about what is not working well.
The focus should always be on what is best for the patient. Yet also consider: What is in it for me? Will this new procedure make my life more difficult or take more time?
Make it easy for staff to participate in meetings by scheduling when it is most convenient for staff, respect that time is valuable by being prompt and keeping meetings short (i.e., hallway meetings with all standing).
A. Project Team Member Roles and Responsibilities
B. Project Team Meeting Agenda
C. Project Charter
D. Project Team Model for Improvement Checklist
E. Example completed PDSA Worksheets for Tests of Change for use of approved protocols
Chapter 3 Resources
We must
recognize that asking people to
change is difficult.

61 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 3 RESOURCE TOOL A Project Team Member Roles and Responsibilities
Create a project team that will meet the aim (goals). Teams will vary in size and composition, but the team should have representation from each of the categories below. There may be one or more individuals on the team who fit into each category, or may fill more than one role; but each should be represented in order to successfully drive change within the organization. The project team composition may have 6-10 people.
1. Team Leader Role: Is an integral and working member of the team. The person filling this role should have good organizational skills, credibility and the ability to collaborate with peers and those at higher levels to support the team. Responsibilities: - Conducts effective team meetings - Keeps the team focused on their goals - Coordinate communication among team members, and within the organization
2. Physician Role: Is the resident subject matter expert, actively engaged in the care delivery process with the ability and desire to support the improvement effort. Experience with multidisciplinary improvement teams is preferred along with a collaborative leadership style. Responsibilities: - Provide expert recommendations for tests of change - Support the changes within the organization, the physician community and administration.
3. Data Manager Role: Is responsible for ongoing measurement for the project. Should have familiarity with web-based tools and understanding of measurement applications such as run charts. Responsibilities: - Assures ongoing data collection - Develops reports
4. Executive Leadership Role: Has the authority to institute change and support the team. Authority to institute rapid change should extend across all areas affected by the change. Responsibilities: - Allocates time and resources necessary to achieve the project goals - Assures linkage of the project efforts to organizational strategies and priorities - Communicates project updates and outcomes as appropriate throughout the organization - Assures timely decisions are made at key decision points - Assumes role of “Barrier Buster”
5. Technical Expertise Role: Knows the process intimately and understands the entire system of care. Responsibilities: - Embraces change and supports the team - Has good working relationships with colleagues - Helps drive system change.
6. Day-to-Day Leadership Role: Works on a daily basis in the system that is being improved and advocates changes needed. Responsibilities: - Understands the details of the daily processes and the effects of making change - Assures that data is being collected and changes are being tested
- May also function as the Team Leader
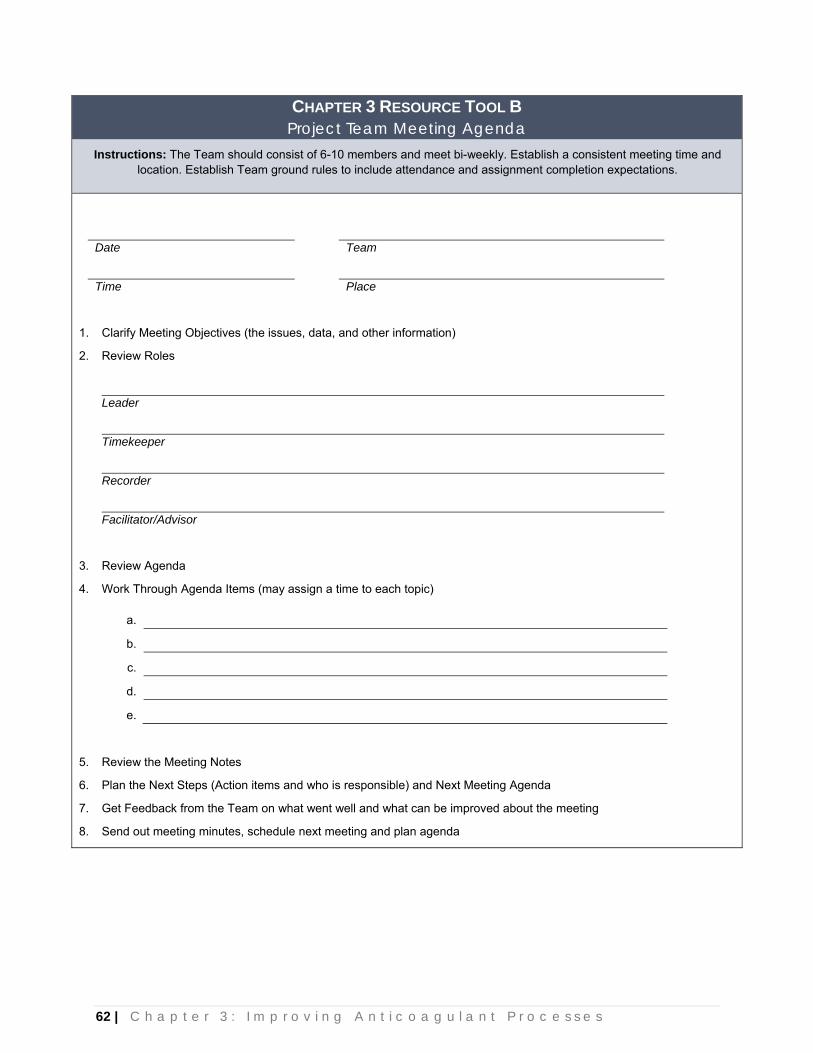
62 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
CHAPTER 3 RESOURCE TOOL B Project Team Meeting Agenda
Instructions: The Team should consist of 6-10 members and meet bi-weekly. Establish a consistent meeting time and location. Establish Team ground rules to include attendance and assignment completion expectations.
Date Team
Time Place
1. Clarify Meeting Objectives (the issues, data, and other information)
2. Review Roles
Leader
Timekeeper
Recorder
Facilitator/Advisor
3. Review Agenda
4. Work Through Agenda Items (may assign a time to each topic)
a.
b.
c.
d.
e.
5. Review the Meeting Notes
6. Plan the Next Steps (Action items and who is responsible) and Next Meeting Agenda
7. Get Feedback from the Team on what went well and what can be improved about the meeting
8. Send out meeting minutes, schedule next meeting and plan agenda

63 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 3 RESOURCE TOOL C Project Charter
Reducing Likelihood of Patient Harm with Anticoagulation Therapy Project Start: 2008 Project Length: One Year Team Members: Project Leader: Physician: Executive: Data Manager: Technical Expert: Day to Day Leaders: Problem: Anticoagulation is a high risk treatment which commonly leads to adverse drug events due to complex dosing, monitoring, and patient compliance issues. (It may be helpful to add current measures such as harm rate or compliance rate with protocols here) What will success look like: 1. Use of standardized practices that include patient involvement. 2. There will be a reduction in harm associated with use of Unfractionated Heparin, Low Molecular
Weight Heparins (LMWH) and Warfarin. Project Scope: One Year implementation period with full implementation January 1, 2009. Must Do: 1. April 1, 2008 – Responsibility assigned for oversight and coordination of Anticoagulant safe practices
development, testing, and implementation 2. July 1, 2008 – Implementation plan (who, what, when, where) 3. October 1, 2008 – Pilot testing 4. January 1, 2009 – Full implementation Must Have: Full compliance with all anticoagulant safe practices. Key Measurements Met: 1. Reduced harm from anticoagulation therapy 2. Implementation of all National Patient Safety Goal Expectations and Joint Commission Standards
applicable to anticoagulation therapy. 3. Ongoing monitoring measures to assure compliance.

64 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
CHAPTER 3 RESOURCE TOOL D Project Team Model for Improvement Checklist
Focus on a Specific Aim 1. Specify an aim for the improvement project.
Must be able to answer, “What are we trying to improve?” This may be a process or an indicator (e.g., # ADEs). If a process
is selected, indicators that reflect the performance of the process will need to be selected as well (e.g., percent protocol compliance).
2. Set a numerical target for improvement that is significantly beyond current performance. Aim for at least 30%-50% improvement.
Set an aggressive timeframe for the completion of the project.
3. Secure the necessary resources. Secure an executive sponsor with the ability to remove obstacles.
Look for content expertise on site or elsewhere to provide
improvement suggestions and guidance for the project.
Make sure the day-to-day leader is on the project.
Staff the project with at least some early adopters, and proper representation of skills, functions, and stakeholders.
Have an aggressive plan to inform key power groups.
Supply the project with ample facilitation; both process improvement expertise and data collection and analysis support.
Provide backup so people can devote ample time to the project.
Communicate, communicate, communicate throughout the project.
Analyze Basic Data 1. Select and gather data for baseline measurement.
Must be able to answer, “How will we know a change is an improvement?”
Establish clear operational definitions.
Seek usefulness, not perfection.
Use small samples. This is not research.
Don’t wait for information system changes.
Use sampling for speed and efficiency.
Use qualitative and quantitative data.
Project Notes
65 | A n t i c o a g u l a n t T o o l k i t
Look at outcome and process measures.
Plot data over time on run charts.
2. Compare baseline data with the target. 3. Determine key causes (if necessary).
If someone has a reasonable change to test, move straight to Test phase.
Think 20/80, i.e., what 20% of the work is creating 80% of the problems?
Select Potential Changes 1. Generate process changes to test.
Look at improvements others have made and test for replication.
Review literature.
Consult content experts.
Review change strategies and brainstorm ideas.
Think 20 / 80. What few changes will give us the greatest gain?
Review self assessment or FMEA results.
Look for improvement opportunities.
2. Decide on changes to be made. Select changes that are “do-able”, changes you can test by next
week.
Do not try to be perfect the first time. This is an opportunity to learn.
Don’t waste too much time trying to get consensus or “buy in”.
Start testing rapidly and let the data tell you what changes are improvements.
Consider effect of changes on system downstream processes. Test the Proposed Changes
PLAN the test (P) 1. Determine whether to test single changes or changes in combination.
2. Plan, sequence, and schedule the tests. Test on a small scale.
Stratify and sample.
Test under varying conditions.
Project Notes

66 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
Use multiple cycles.
Compress testing time - “By next week.”
Communicate what you are doing and why to everyone potentially
affected. DO the test (D) 1. Make the changes, following your plan.
2. Collect data on the measure(s). STUDY to see the effect of the test (S) 1. Study effect of each test on the measure(s). ACT on the knowledge gained (A) 1. Decide on need for further improvement (additional PDSA cycles). 2. Decide on actions to hold the gains.
Develop a plan to audit compliance and discuss changing conditions.
Decide how often you will measure the indicator. Take steps to ensure that new staff will be trained to follow the improved processes.
Project Notes

67 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 3 RESOURCE TOOL E Model for Improvement
CYCLE FOR LEARNING AND IMPROVEMENT Cycle: 1 Date: _________________________________
Objective: Determine if protocol obtained from Hospital A can be used in our hospital.
PLAN Ask questions:
Will protocol be acceptable for use at this hospital? Will physicians find the protocol easy to use? Will nurses be able to carry out the treatment plan outlined in the protocol? Will pharmacists be able to distribute medications based on the protocol?
Make predictions: Physicians will find the protocol easy to use. Y or N Nurses will find that they can execute the treatment plan as out lined in the protocol. Y or N Pharmacists will find that the protocol clearly describes the medications and doses to be dispensed? Y or N
Plan for change or test: Who? What? When? Where?
Obtain a copy of a protocol from Hospital A. As first test: Simulate the use of the protocol on one patient. Select one physician, one nurse and one pharmacist to walk through the protocol as if taking care of a
patient.
Plan for collection of data: Who? What? When? Where?
Request a meeting of the involved staff and select one patient’s chart. Debrief those involved in the test.
DO Carry out the change or test; collect data and begin analysis.
Team asks one physician, one nurse, and one pharmacist to simulate use of the protocol on one patient by next Tuesday.
Nurse, pharmacist, and physician meet together to review patient chart and protocol and list recommended modifications to protocol on flipchart.
STUDY Complete analysis of data; summarize what was learned. There were 8 minor recommendations for protocol modifications.
ACT Determine if you are ready to make a change. Plan for the next cycle.
The protocol is modified and another test is scheduled for later that day or the next day.
Act Plan
Study Do

68 | C h a p t e r 3 : I m p r o v i n g A n t i c o a g u l a n t P r o c e s s e s
CHAPTER 3 RESOURCE TOOL E Model for Improvement
CYCLE FOR LEARNING AND IMPROVEMENT Cycle: 2 Date: _________________________________
Objective: Modify protocol based on cycle 1 test.
PLAN Ask questions:
What modifications to Hospital A protocol need to occur?
Make predictions: Minor modifications are needed based on 8 recommendations suggested in cycle 1 test.
Plan for change or test: Who? What? When? Where?
Meet as a team on Wednesday to review list of advantages and disadvantages from cycle 1 test and modify proposal on Wednesday.
Plan for collection of data: Who? What? When? Where?
As a team, consider what worked and what did not and modifies proposal based on feedback from cycle 1 test.
DO Carry out the change or test; collect data and begin analysis.
The test is carried out. The steps are documented.
STUDY Complete analysis of data; summarize what was learned.
Did the test answer our questions? If the revised protocol did not meet our expectations, what changes are needed?
ACT Determine if you are ready to make a change. Plan for the next cycle.
All recommendations are addressed via minor modifications to proposal which are made by pharmacy department staff by Friday.
Plan an actual test of the modified proposal with the same staff from cycle 2 for a patient on Unit 5N by next Wednesday (see cycle 3).
Act Plan
Study Do

69 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 3 RESOURCE TOOL E Model for Improvement
CYCLE FOR LEARNING AND IMPROVEMENT Cycle: 3 Date: _________________________________
Objective: Test the revised protocol with one nurse, one pharmacist, and one physician on one patient on Unit 5N by next Wednesday.
PLAN Request a meeting of the involved staff and select one patient’s chart. Debrief those involved in the test. Ask questions:
Are additional modification to protocol needed?
Make predictions: No additional modifications needed.
Plan for change or test: Who? What? When? Where?
Team contacts same nurse, pharmacist, and physician involved in cycle 2 test and requests an actual test of protocol on one patient.
Team generates instruction sheet on how, when, where test should occur. Team develops instruction sheet for test outlining process flow. Team contacts those involved in test and establishes test date of next Tuesday.
Plan for collection of data: Who? What? When? Where?
Team will convene meeting of those involved in test to discuss protocol modifications and any operational process issues.
DO Carry out the change or test; collect data and begin analysis.
Involved staff carry out test on Tuesday with one patient on Unit 5N at 2:00 pm. Document steps.
STUDY Complete analysis of data; summarize what was learned. Team holds stand-up meeting with test staff on Unit 5N immediately following the test to discuss any protocol modifications and process issues. Team determines that slight modifications to the process are needed with no modifications to protocol.
ACT Determine if you are ready to make a change. Plan for the next cycle.
Team develops a plan to test the protocol with 3 additional doctors next week on same unit.
Act Plan
Study Do

70 | C h a p t e r 4 : M e a s u r i n g P e r f o r m a n c e
Chapter 4: Measuring Performance

71 | A n t i c o a g u l a n t T o o l k i t
Tests of Change
The ability to define and measure performance is critical to understanding the dynamics of change and sustaining long‐term clinical quality improvement. The data collected should help to clarify the improvement AIM. The data should be simple to collect, and easy to display (use graph, table, run chart). Use sampling to make measurement efficient, and integrate measurement into the daily routine. Data results should be plotted over time and displayed so staff can see progress. The project team should base their decisions on the data and continue to monitor using data after changes are made to ensure that the changes were effective. Anticoagulants measures can be grouped into two broad categories. Process Measures. Process measures track if the process as designed is in place. One example process measure is Percent Protocol Compliance which is used to determine the reliability of the protocol process in place. The goal of this measure is to assure that all patients eligible for treatment are treated according to the protocol. Additional process measures can be developed and used to measure small tests of change using simple data collection methodologies.
Measuring Performance
Percentage of Warfarin patients receiving correct meal plan (to assure that Nutrition Services are informed of all patients on Warfarin therapy)
Percentage of eligible patients placed on new Bridging Protocol (to measure physician compliance with new protocol policy)
Heparin flush solution dollar purchases over time (if replace peripheral heparin flush solutions with normal saline)
Number of IV anticoagulant products admixed by pharmacy over time (if replaced by premixed solutions)
Time frame for receipt of lab results by care providers over time.
Time to therapeutic levels
Reduction in error potential over time (analysis of Smart Pump data for near misses)
Percentage of INRs > 4‐5 or other measures of super‐therapeutic levels
Percentage of patients receiving anticoagulants with INR and/or aPTT outside protocol limits
Example Process Measures

72 | C h a p t e r 4 : M e a s u r i n g P e r f o r m a n c e
The figure below displays the impact of multiple process related interventions over time on the overall AIM of reducing Heparin Related ADE’s.
Figure 4: Measurement: Reduction in Heparin Related ADEs
Outcome Measures
The purpose of this measure is to determine the overall impact of the process changes on patient care. An example of an anticoagulation therapy outcome measure is “Reduction in Harm”.
Tracking harm versus medication errors associated with anticoagulant therapy is a more effective way for hospitals to identify events that do cause harm to patients. Harm is defined as “an unintended physical injury resulting from or contributed to by medical care that requires additional monitoring, treatment or hospitalization, or results in death”. The Institute for Healthcare Improvement (IHI) recommends that hospitals use the IHI Global Trigger tool which focuses on use of ADE triggers to identify harm. The IHI Global Trigger tool measures harm (not error) and events associated with commission rather than omission. It does not distinguish between preventable and non‐preventable harm. The trigger tool allows categorization of harm by severity using the National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP) index.
A modified version of the IHI Trigger tool developed by Fairview Health Services is attached at the end of this chapter. When using this tool it is recommended that the data collection be done as follows:
Identify and train a review team to include a physician advisor and two reviewers
Read and discuss the IHI Global Trigger tool guide found at www.IHI.org
Review all charts where the suggested triggers indicate a potential adverse drug event with Heparin and/or Warfarin. The “triggers” are defined below. The review process is done in two steps.
- The reviewers independently review charts and then reach consensus on the presence of harm from the perspective of the patient and then assign a category of harm.

73 | A n t i c o a g u l a n t T o o l k i t
- A physician reviews the consensus decision of the reviewers
Charts are selected by using the following suggested “triggers.”
- INR>4 and PTTs>upper limit of therapeutic range x 2
- Daily review of the use of Protamine, Argatroban, Lepiriudin, and Fondaparinux
The precise INR or PTT to use as the “trigger” may be arbitrary and is a balance between false‐ positives and false‐negatives. The higher the level, the less likely there will be false‐positives. However, the higher trigger point may exclude ADEs that occur at lower or normal INR/PTT values. Lower trigger points will create more records to review that do not have ADEs, thereby increasing workload, but are less likely to miss ADEs. Hospitals should examine what data are available, assess workload demands, and determine their own INR/PTT trigger values.
Measurement of harm should include all patients who are admitted to the hospital with an adverse event including patients admitted through the Emergency Department. Hospitals may elect to stratify and track harm by source.
In summary, the Trigger Tool establishes a baseline of adverse events for a hospital and categorizes them by severity so that resources can focus on those events causing the greatest harm. The adverse event rate is measured over time so that the effects of the interventions can be monitored.
A. Percent Protocol Compliance (Process Measure) B. Measuring Harm resulting from ADEs (Outcome Measure)
Chapter 4 Resources

74 | C h a p t e r 4 : M e a s u r i n g P e r f o r m a n c e
CHAPTER 4 RESOURCE TOOL A Percent Protocol Compliance (Process Measure)
Percent of Patients Receiving IV or SQ Heparin(s) or Warfarin with Treatment Managed According to Protocol
Purpose: This measure is used to determine the reliability of the process in place. It is intended to be used in those situations where a hospital has already adopted a protocol for the management of anticoagulants. Definition: The percentage of patients receiving an anticoagulant whose treatment was ordered, received, and managed according to protocol or for whom the protocol was not followed due to a documented contraindication as defined in the protocol. A single treatment may include multiple doses, and does not only include the initial ordering and delivery of the medication, but extends through the entire management of the treatment, until discontinuation. Instructions: Review 20 charts per month for Heparin patients and 20 charts per month for Warfarin patients where protocols are in place. HEPARIN: # Yes responses / total # charts reviewed for Heparin = % protocol compliance WARFARIN: # Yes responses / total # charts reviewed for Warfarin = % protocol compliance Goal = 100%
CHART # HEPARIN(S): Treatment Managed According to Protocol (Y/N)?
WARFARIN: Treatment Managed According to Protocol (Y/N)?
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.

75 | A n t i c o a g u l a n t T o o l k i t
CHAPTER 4 RESOURCE TOOL B Measuring Harm resulting from ADEs (Outcome Measure)
Measuring Harm resulting from Warfarin, Heparin, Enoxaparin, and
Other Anticoagulants Adverse Drug Event(s)
I. Identify patient charts for further review according to the following suggested triggers:
Note: Hospitals may also identify patient charts for further review that were reported through their voluntary Risk Management System.
Exclude patients where duration of anticoagulant therapy is less than 24 hours
Daily review of INRs > 4 and PTTs > upper limit of therapeutic range x 2 (i.e. if upper limit is 100, then use trigger of 200) as identified by the laboratory.
Daily review of the use of Protamine, Argatroban, Lepirudin and Fondaparinux (for Heparin) as identified by the pharmacy computer system or automated dispensing cabinet. Exception(s): Newborn nursery, emergency department unless patient is experiencing an adverse event, operating rooms, cardiac cath labs.
II. Identify and review all charts where “triggers” exist.
III. Complete Section A of this tool to Screen for an Adverse Drug Event (ADE).
IV. Complete Section B of this tool for those charts where an ADE has been identified based on results of the Screen completed in Section A.
Section 1: Screening for an ADE
Date: Trigger(s)*: Warfarin: INR > 4
Heparin: PTT at upper limit of therapeutic range x 2 &/or use of protamine, argatroban, lepirudin, fondaparinux
Patient Name:
MR#:
Room #: Reviewer:
Y N Example/Comment
Legitimate screen? Example of an illegitimate screen: a bedside PTT = 210 mg/dl but a subsequent PTT = 155 mg/dl. If N, stop.
Associated with anticoagulant? Example: a high INR may be related to malnutrition or liver disease. If N, stop.
Clinical intervention? A clinical intervention could be the administration of vitamin K, or fresh frozen plasma. A clinical intervention could be holding a dose of Warfarin or reducing the dose of Heparin if a problem is suspected. The intentional administration of vitamin K pre-procedure is not a clinical intervention. Holding the dose because the patient is undergoing a test is not a clinical intervention. If N, stop.
If the answer to all 3 questions is “Yes”, this is an adverse drug event (ADE). Complete SECTION B for ONLY those charts with an ADE.

76 | C h a p t e r 4 : M e a s u r i n g P e r f o r m a n c e
Section 2: ADE Analysis Warfarin-related bleeding resulting from outpatient services or a prior hospital discharge will count as an ADE. It is possible that a given patient may have more than one adverse event. If harm is part of a sequence of events, there should be one incident reported and rated as the highest level of harm.
If the same dose of an anticoagulant resulted in multiple laboratory abnormalities or multiple doses of antidotes, it would be considered a single adverse drug effect.
a. Specific drug involved
b. Dose/route/time of administration
c. Drug/dose/timing of clinical intervention(s)
d. Follow-up lab measurements (time & results)
e. Was there a mediation error? □ Yes □ No
f. Circle the degree of injury (see below). E F G H I g. Did any of the following risk factors play a
role? □ Starting and stopping antibiotics, anti-epilepsy drugs, or other
interacting drugs
□ Major dietary changes □ Malnutrition or other chronic illness
□ Other. Describe the risk factor(s) and other suggestions for future prevention.
Harm Category Description Example
E An event contributed to or resulted in temporary harm to the patient
Reversal was successful with no further action warranted.
Reversal was successful but recovery was complicated by one or more co-morbid medical conditions.
Additional assistance from medical or nursing staff needed, such as the rapid response team.
F
An event contributed to or resulted in temporary harm to the patients and prolonged hospitalization
Increase in hospitalization from prolonged or repeated treatment with protamine, fresh frozen plasma, or vitamin K.
Transfer to an intensive care unit for observation and monitoring.
Use of argatroban due to Heparin-induced thrombocytopenia
G An event contributed to or resulted in permanent patient harm
Permanent injury or disability, such as a myocardial infarction, resulting from hemorrhage.
H An event which required intervention to sustain life
Event resulted in Code Blue.
I An event which contributed to the patient’s death
Death resulting from prolonged hemorrhage or a secondary medical condition, such as acute MI, that was related to the hemorrhage.

77 | A n t i c o a g u l a n t T o o l k i t
Chapter 5: Spreading and Sustaining Improvement
78 | C h a p t e r 5 : S p r e a d i n g a n d S u s t a i n i n g I m p r o v e m e n t
Spreading Changes The “Spread Team” may not necessarily contain the same individuals as the “Testing Team.” Spread skills are different from testing skills. It may take a different set of team members who will bring the change to another unit for testing and then implementation. Changes should be implemented, stabilized, and measured for improvement locally before spreading across the organization. The Spread Team should assess “readiness for change” prior to spreading the changes beyond the current location.
Prior to the spread team introducing the process to the new location, the following questions should be considered:
Is there a team dedicated to testing the process in this new location?
Will there be staff time made available to participate in test cycles?
Is there local leadership commitment and support for the process?
Is there will among the staff to make changes?
Will an improvement methodology be used?
There should be a YES response to all these questions prior to spreading the process to a new location.
Changes that spread easily have the following characteristics:
There is a clear advantage to the change compared to current way of doing things especially for those directly impacted by the change
The change is compatible with the current system and values
The change is simple, easy to implement and easy to test
The impact of the change was observable (can place on a Storyboard)
There is leadership support to promote the change making spread easier
There is measurement to track outcomes of the changes and rate of the spread
There is feedback for accountability, to encourage and support those involved in making changes, and to refine the process changes if needed
Sustaining Changes Changes that are sustainable have the following characteristics:
The change is based on a robust and reliable process
The change is based on a position and not a person
The process put in place will withstand changes in staff and will adapt as changes occur on the unit
The team is open to new ideas to make process changes as needed
How to use the process can be taught in a short time frame
The tools/forms associated with a new process are easy to use
Readiness for
change should be assessed prior to
spreading changes beyond the current
location.
Spreading and Sustaining Improvement

79 | A n t i c o a g u l a n t T o o l k i t
NOTE: do not fall back on use of training and education as this approach does not result in sustainable change.
Role of the “Process Owner” A process owner is a person responsible for periodically reviewing process and outcome measures. This person does not have to be the one who collects the data. The role of this person is to bring to the attention of the team when the process is no longer working as designed or the outcomes are no longer achieved as expected. Fear of having to deal with all of the elements of this improvement will cause many to hesitate from taking on this role. The purpose of this role is to ensure that the system and processes continue to perform as designed. All systems degrade over time. Appropriate monitoring/auditing is needed to sustain the changes. The following outlines key success factors in sustaining organizational changes implemented:
Management Support: changes should be constantly championed and monitored. Leadership should hold project teams accountable for success, communicate measurable improvement goals, and celebrate successful attainment of those goals.
Fool‐proofing Changes: include changes in guidelines and training materials, use pre‐assembled kits in applying interventions (supply kits), use differentiation to separate look‐alikes (vials vs. syringes), use computers to edit and cross check order entry, use bar coding, alarms, and use run charts to monitor patients INRs over time.
Public display of data: to effectively provide feedback and communicate progress towards goals Culture of Improvement: all staff know current performance improvement activity and can explain their
role in it, staff view quality improvement work as part of their job, improvement responsibilities are included in job descriptions, staff ideas are freely shared and concerns expressed.
Project Teams Core Competencies: ongoing training in quality improvement methods occurs to enhance the skill base of teams
A. Spreading Improvement Worksheet B. Sustaining Changes Worksheet
Chapter 5 Resources
All systems degrade
over time. Monitoring is
needed to sustain changes.

80 | C h a p t e r 5 : S p r e a d i n g a n d S u s t a i n i n g I m p r o v e m e n t
CHAPTER 5 RESOURCE TOOL A Spreading Improvement Worksheet (Example)
Spread should take place only after the initial change has been well tested and implemented in the pilot unit.
We Wish to Spread: Use of approved Protocols for Inpatient Warfarin Therapy for Orthopedic Patients on Unit A
Organization Team:
Area for Spread
Readiness to Change*
(H, M, L) “Opinion Leaders” who can aid spread
Communication Plan with “Opinion Leaders”
List Spread Barriers and Support Needed to Overcome Action Plan for Spread
Ortho Unit A H Dr. Smith, Orthopedic Surgeon Nurse Manager, Unit A Clinical Nurse Specialist, Unit A
See at meeting Invite to lunch Friendship Relationship
Time to educate staff nurses. Obtain support from Nurse Manager to educate nurses during shift change
Schedule time for staff nurses on Unit A to meet with opinion leaders from Unit A Arrange for Education staff to assist with material development Share measures of increased compliance with Unit A nurses that were achieved by other units Share changes implemented successfully on other units with Unit A staff
*Rating Staff Receptivity to Change (High, Medium, Low) Terms
There is a clear advantage to the change compared to current way of doing things especially for those directly impacted by the change The change is compatible with the current system and values The change is simple and easy to implement The change was easy to test The impact of the change was observable (can place on a Storyboard) There is leadership support to promote the change making spread easier There is a measurement to track outcomes of changes and rate of spread There is feedback for accountability, to encourage and support those involved in making changes, and to refine the process if needed
Testing A change to determine if the change is an improvement. There may be four or five cycles of testing needed. Test with three patients or three physicians. Test under different circumstances, e.g. evenings, nights and weekends. Implementation Takes place when testing is completed and the team agrees that the change will be how care is provided. Spread Taking a tested and implemented intervention from the original test area or pilot unit to a new area. Spread should not be from a pilot unit/ population to the entire hospital. The change should be tested in each area to determine if adjustments are needed. In some cases, adjustments made on a spread unit may be an improvement for all areas.

81 | A n t i - C o a g u l a n t T o o l k i t
CHAPTER 5 RESOURCE TOOL B Sustaining Changes Worksheet (Example)
Improvement Topic: Nutrition Services is notified of patients receiving Warfarin
Organization/Team:
The main changes made were …
(describe briefly)
Sustainable? *** (H, M, L)
Plans for enhancing sustainability of changes(s)
Susie Jones calls Nutrition services for
each new Warfarin patient.
L The task should be delegated to a position not a person.
Pharmacy sends a printout of all patients on Warfarin to Nutrition Support Services
M The pharmacy computer system generates a list of all
patients on Warfarin. The list is faxed to the NS service by a pharmacy technician.
As a fail safe, NS services contacts
pharmacy if a list of patients is not faxed by a specified time.
H A NS staff person contacts pharmacy requesting a list of patients on Warfarin if a list is not received by X time.
*** Rate your perception of sustainability of each change listed (High, Medium, Low) based on the presence of the following characteristics of sustainable changes:
The change is based on a robust and reliable process The change in place will with stand changes in staff The process is based on a position and not a person The process put in place will adapt as changes occur on the unit The team is open to new ideas to make process changes as needed How to use the process can be taught in a short time frame The tools/forms associated with a new process are easy to use

82 | C h a p t e r 6 : A d d i t i o n a l R e s o u r c e s
Chapter 6: Additional Resources
83 | A n t i - C o a g u l a n t T o o l k i t
Web Resources Bristol‐Myers Squibb manufacturer of brand Coumadin: www.coumadin.com (at the time of this publication, this website was being updated)
PTINR.com America’s Anticoagulation Resource: www.ptinr.com
American College of Clinical Pharmacy: www.accp.com
Clot Care Online Resource: www.clotcare.com
Spectrum Health, West Michigan's largest integrated health care system, online anticoagulation toolkit: http://www.spectrum‐health.org/cs/Satellite?c=eHA_Content_C&cid=1158780505675&pagename= Spectrum_Health_Core%2FSpectrum_Core_Central_Template#doc
Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Chest, Sep 2004; 126:163S ‐ 696S: www.chestjournal.org/
University of Massachusetts Medical School, VTE education: www.outcomes‐umassmed.org
The Joint Commission: www.jointcommission.org
The Institute for Safe Medication Practices (ISMP): www.ismp.org/
Anticoagulation Forum: www.acforum.org/links.html
Warfarin Dosing: www.Warfarindosing.org
Iowa Healthcare Collaborative Anticoagulation Toolkit: www.ihconline.org/toolkits/anticoagulation.cfm
Institute for Healthcare Improvement: www.ihi.org
VTE Toolkit ‐ www.vte.washington.edu/
IHI Mentor Hospitals for Anticoagulants Fairview Health Services – Minneapolis, MN Steven Meisel [email protected], 612‐672‐7061 Missouri Baptist Medical Center – St. Louis, MO Nancy Kimmel [email protected], 314‐966‐5066 OSJ Saint James – John W. Albrecht Medical Center – Pontiac, IL Bill Wightkin, Pharm.D. [email protected], 815‐842‐4926 St. Luke’s Hospital – Cedar Rapids, IA Pat Thies [email protected] 319‐368‐5861
Page 2
Caption describing picture or graphic.
Additional Resources