Embed Size (px)
Citation preview

Totsion Dvstonia in Israel 4
Amos D. Korczyn, MD, MSc, Esther Kahana, MD, Nelly Zilber, D k s Sc, Max Streifler, MD, Raphael Carasso, MD, and Milton Alter, MD
~
A country-wide search for idiopathic torsion dystonia (ITD) in Israel between 1969 and 1975 revealed 42 patients (41 Jewish and 1 Druze Arabr Prevalence of ITD per million population, age-adjusted to the United States popula- tion in 1970, was 10.8 in the total Jewish potmldon (22.0 among Jews of European extraction contrasted with 1.5 among Jews with Afro-Asian forebears). Among Europeans, the highest prevalence was among Jews from Eastern Europe.
The average age-adjusted annual incidence rates per million population were 0.43 in the total Jewish population, 0.98 in the Europeans, and 0.1 1 in the Afro-Asians. Ainong the 40 patients for whom familial data were available, the majority of cases (26) were sporadic. The other 14 belonged to four unrelated European 'f'gmilies, all of Russian-Polish origin. The pattern of inheritance in these four families fits an autosomal dominant model with incomplete penetrance.
Korczyn AD, Kahana E, Zilber N, et al: Torsion dystonia in Israel. Ann Neurol8:387-391, 1980
Idiopathic torsion dystonia (ITD) is a movement dis- order characterized by irregular, sustained involun- tary movements, often resulting in abnormal pos- tures [9]. The onset of symptoms is preceded by a period of normal neurological and intellectual devel- opment. The disorder is not accompanied by other organ system disease. Although there is still no general agreement as to the nosology, pathology, or treatment [ 2 ] , some evidence exists that disturbance of brain catecholamine function may be the pathophysiological basis of dystonia [ 101.
The possibility that ITD might be an inherited dis- order was considered in the earliest reports, and the likelihood that the Jewish ethnic group might have a higher frequency of the disorder than other groups was supported by observations of familial aggregates of ITD in Jews [ 2 , 33. Recently, extensive family studies by Eldridge et al[4, 51 have provided a larger clinical material, from which they conclude that there might be two genetic forms of ITD. About one-third of the families with typical dystonia studied by El- dridge et a1 were Jewish, and a recessive pattern of inheritance was thought to be more common in this group. Onset occurred between 4 and 16 years of age, limbs were involved earlier and more severely than the axial musculature, and clinical deterioration was rapid in the early stages of the disease. However, after adolescence, symptoms often tended to sta- bilize. It was suggested that the recessive form of
ITD might be due to a gene occurring with unusual frequency in Jews who have immigrated to America from Eastern Europe.
Ih the series of Eldridge et al[3-5], the autosomal dominant form of ITD was thought to occur mostly in non-Jewish families. In this form of dystonia, age at onset was more variable but onset usually occurred in adulthood, there was earlier involvement of the axial musculature, torticollis was frequently the pre- senting complaint, and the clinical course was slowly progressive. The gene postulated to cause the domi- nant form of ITD appeared to have no geographical selectivity. The disease was rare in some ethnic groups, such as blacks in the United States [7].
Previously we reported the results of a nationwide survey of hospital records for ITD in Israel [ l l and measured the levels of dopamine P-hydroxylase [l 1, 121. In the present study, we were able to extend and enlarge the clinical material available for analysis. By studying a well-defined population, we minimized bias in case selection and were able to present a more complete epidemiological analysis of ITD among Jews.
Methods In the present study, the National Registry of Neurological Diseases, maintained by the Uri Leibowitz Neuroepi- demiology Unit of Hadassah University Hospital, Jeru- salem, served as a major source for case finding. The
From the Sackler School of Medicine, Tel Aviv University, and Beilinson Hospital. Petah Tikva, Hadassah University Hospital,
Received Nov 19, 1979, and in revised form Feb 7 , 1980. Ac- cepted for publication Feb 10, 1980. Address reprint requests to A. D. Korczyn, MD, Department of Physiology and Pharmacology, Tel Aviv University Medical School, Ramat Aviv, Israel.
Jerusalem, Ba&iai Hospital, Ashkeion, Ichilov Hospital,. Tel Aviv, Israel, and Temple University Hospital, Philadelphia, PA.
0364-5134/80/100387-05$01.25 @ 1979 by Amos D. Korctyn 387

registry receives data on every patient with a neuro- logical disorder discharged from any hospital in Israel.
Demographic data about the general population of Israel are available from detailed reports published annually by the Central Bureau of Statistics [13]. The population is ethnically diverse, consisting of native-born Jews and Arabs as well as immigrants from Europe, Africa, Asia, and America [8]. In publications of the Central Bureau of Statistics, ethnic origin is based on the individual's place of birth or, if born in Israel, on the father's place of birth [13]. Hence we accepted this convention as well.
In the present study we retrieved from the registry names of patients hospitalized during the period 1969 through 1975 and suspected of having ITD. All cases covered in the previous study of I T D in Israel [ I ] were included in the present study, and additional names were obtalned through notification by other neurologists as well as through data gathered from patients about affected rela- tives. All suspected cases of ITD, spasmodic torticollis, blepharospasm, and graphospasm were identified. These patients were visited by a trained field worker. Patients who had not recently been hospitalized in a neurological department were reexamined by one of us (A. D. K. or E. K.). Information pertaining to ethnic origin and fam- ily pedigree was systematically collected on a specially designed form. Family data were obtained for all but 1 pa- tient.
Only patients who satisfied all five of the following clini- cal criteria were accepted as having ITD: (1) dystonic pos- ture or movement; (2) a progressive clinical course at some time; (3) normal perinatal history and no other abnormal neurological signs (intellectual, sensory, pyramidal, or cerebellar); ( 4 ) no history of encephalitis or brain trauma; and ( 5 ) no metabolic disorder (e.g., Wilson disease o r ab- normal calcium levels) that could account for the condition.
Results A total of 137 names were collected of patients ten- tatively considered to have ITD. Of these, 95 were excluded for various reasons: 5 1 had other disorders such as cerebral palsy or signs incompatible with
ITD; 19 had only focal abnormalities such as tor- ticollis; and 25 could not be located despite intensive efforts (2 of these are known to have died and 3 were living abroad). Forty-two patients were accepted as having ITD. There were 2 5 males and 17 females, a nonsignificant difference. One subject was an Arab of the Drute sect; the others were Jewish. Of the 42 patients, 35 were known to be alive and in Israel on December 31, 1977, which was designated the prevalence day.
Prevalence data are summarized in Table 1. The crude point-prevalence rate of ITD in Israel on that day was 9.6 per million population. In the Jewish population it was 1 1.1 per million. The prevalence of ITD in European Jews was 23.8 per million, com- pared with only 1.1 per million in Afro-Asian Jews. The highest prevalence among Europeans (27.0) was observed in East Europeans, compared with Central Europeans and Jews from elsewhere in Europe (2 1.2 and 13.5, respectively). The prevalence among non- Jews was 1.7 per million population, which was simi- lar to that of Afro-Asian Jews but was based on a single Arab case.
Populations of different origins living in Israel vary considerably in age distribution. Therefore, preva- lence rates were adjusted to a standard population (United States population in 1970 [6]). However, even after standardization for age differences, Euro- pean Jews-in particular those of Eastern European origin-had the highest prevalence of ITD (see Table 1).
The age-specific prevalence rates among various ethnic groups are shown in Table 2. No patient was younger than 15 years of age. The prevalence rate was significantly higher for younger individuals among people of Eastern European origin than among other ethnic groups (p < 0.001).
The average annual incidence rate of ITD was cal- culated for the period January l , 1969, through De-
Table 1 , Prevalence Rates of I T D among Ethnic Groups in IJrael on December 31, 1977, per Million Population
Prevalence No. of Population Group Patients (X 103) Crude Age-ad justed"
Total in Israelb 35 3,653 9.6 9.8 Non-Jewish 1 576 1.7 2.2 Jewish 34 3,077 11.1 10.8
European 31 1,300 23.8 22.0 East EuropeanC 24 889 27.0 25.8 Central Europeand 4 189 21.2 17.9 Other 3 222 13.5 14.5
Afro- Asian 2 1,777 1 .1 1.5 Uncertain 1 . . . . . . . . .
aUnited States population in 1970. "Seven patients were deceased or not living in Israel on prevalence day (12/3 1/77). cLatvia, Lithuania, Russia, Poland, and Rumania. dGerrnany, Ausrria, Czechoslovakia, and Hungary.
388 Annals of Neurology Vol 8 No 4 October 1980
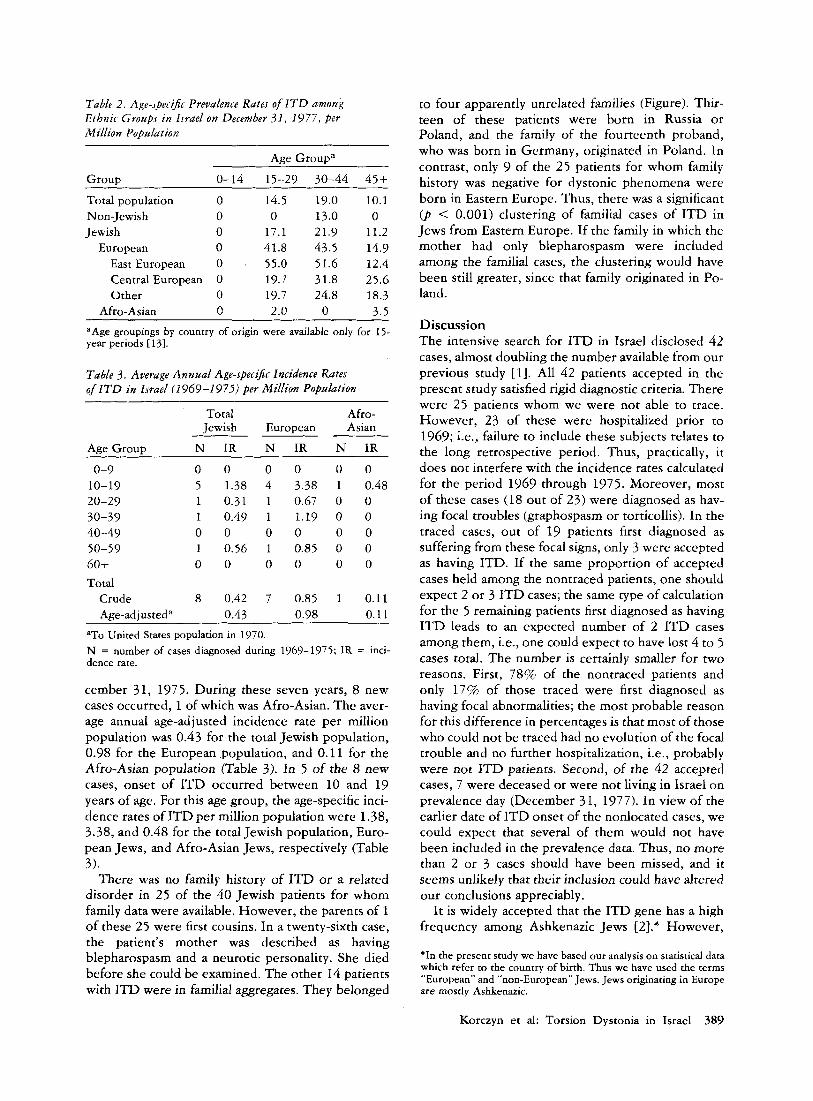
Table 2. Age-specz$r Prevalence Rates of I T D among Ethnic Groups in Israel on December 31, 1977, per Million Population
Group
Total population Non-Jewish Jewish
European East European Central European Other
Afro-Asian
Age Groupa 0-14 15-29 30-44 45+
0 14.5 19.0 10.1 0 0 13.0 0 0 17.1 21.9 11.2 0 41.8 43.5 14.9 0 . 55.0 51.6 12.4 0 19.7 31.8 25.6 0 19.7 24.8 18.3 0 2.0 0 3.5
~~~ ~ ~~
aAge groupings by country of origin were available only for 15- year periods 1131.
Table 3. Average Annual Age-specific Incidence Rates of ITD in Israel (1969-1975) per Million Population
~ ~~~~ ~
Total Afro- Jewish European Asian
Age Grout, N IR N IR N IR
0-9 0 0 0 10-19 5 1.38 4 20-29 1 0.31 1 30-39 1 0.49 1 40-49 0 0 0 50-59 1 0.56 1 60-t 0 0 0 Total
Crude 8 0.42 7 Age-ad i usteda 0.43
0 3.38 0.67 1.19 0 0.85 0
0.85 0.98
0 0 1 0.48 0 0 0 0 0 0 0 0 0 0
1 0.11 0.11
aTo United States population in 1970. N = number of cases diagnosed during 1969-1975; IR = inci- dence rate.
cember 31, 1975. During these seven years, 8 new cases occurred, 1 of which was Afro-Asian. The aver- age annual age-ad justed incidence rate per million population was 0.43 for the total Jewish population, 0.98 for the European population, and 0.11 for the Afro-Asian population (Table 3). In 5 of the 8 new cases, onset of ITD occurred between 10 and 19 years of age. For this age group, the age-specific inci- dence rates of ITDper million population were 1.38, 3.38, and 0.48 for the total Jewish population, Euro- pean Jews, and Afro-Asian Jews, respectively (Table 3).
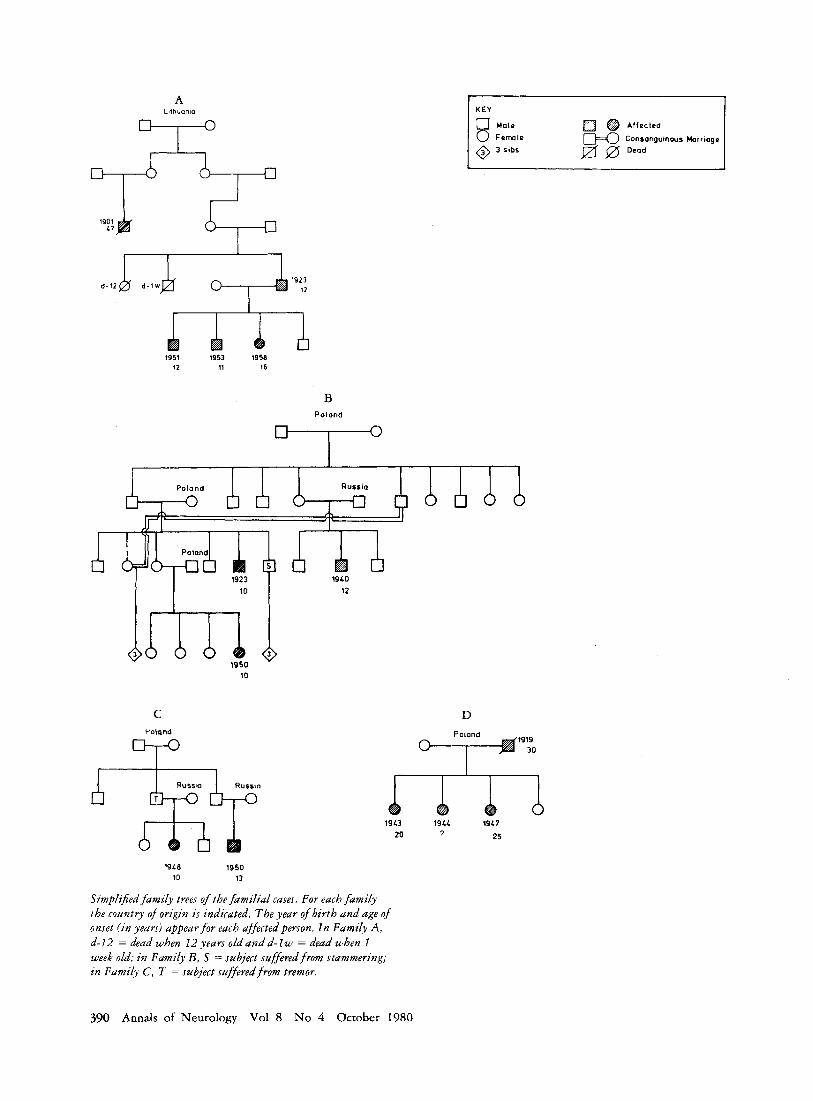
There was no family history of ITD or a related disorder in 25 of the 40 Jewish patients for whom family data were available. However, the parents of 1 of these 25 were first cousins. In a twenty-sixth case, the patient’s mother was described as having blepharospasm and a neurotic personality. She died before she could be examined. The other 14 patients with ITD were in familial aggregates. They belonged
to four apparently unrelated families (Figure). Thir- teen of these patients were born in Russia or Poland, and the family of the fourteenth proband, who was born in Germany, originated in Poland. In contrast, only 9 of the 25 patients for whom family history was negative for dystonic phenomena were born in Eastern Europe. Thus, there was a significant ( p < 0.001) clustering of familial cases of ITD in Jews from Eastern Europe. If the family in which the mother had only blepharospasm were included among the familial cases, the clustering would have been still greater, since that family originated in Po- land.
Discussion The intensive search for ITD in Israel disclosed 4 2 cases, almost doubling the number available from our previous study [l]. All 42 patients accepted in the present study satisfied rigid diagnostic criteria. There were 25 patients whom we were not able to trace. However, 23 of these were hospitalized prior to 1969; i.e., failure to include these subjects relates to the long retrospective period. Thus, practically, it does not interfere with the incidence rates calculated for the period 1969 through 1975. Moreover, most of these cases (18 out of 23) were diagnosed as hav- ing focal troubles (graphospasm or torticollis). In the traced cases, out of 19 patients first diagnosed as suffering from these focal signs, only 3 were accepted as having ITD. If the same proportion of accepted cases held among the nontraced patients, one should expect 2 or 3 ITD cases; the same type of calculation for the 5 remaining patients first diagnosed as having ITD leads to an expected number of 2 ITD cases among them, i.e., one could expect to have lost 4 to 5 cases total. The number is certainly smaller for two reasons. First, 78% of the nontraced patients and only 17% of those traced were first diagnosed as having focal abnormalities; the most probable reason for this difference in percentages is that most of those who could not be traced had no evolution of the focal trouble and no further hospitalization, i.e., probably were not ITD patients. Second, of the 42 accepted cases, 7 were deceased or were not living in Israel on prevalence day (December 31, 1977). In view of the earlier date of ITD onset of the nonlocated cases, we could expect that several of them would not have been included in the prevalence data. Thus, no more than 2 or 3 cases should have been missed, and it seems unlikely that their inclusion could have altered our conclusions appreciably.
It is widely accepted that the ITD gene has a high frequency among Ashkenazic Jews [2].* However,
*In the present study we have based our analysis on statistical data which refer to the country of birth. Thus we have used the terms “European” and “non-European” Jews. Jews originating in Europe are mostly Ashkenazic.
Korczyn et al: Torsion Dystonia in Israel 389
A Lilhuonia
1951 1953 1958 12 11 16
K E Y
@ Affected
Consonguinws Horrwge a 0 Dead 8 :::Ie
@ 3 sibs
B Polond
C Poland
D
1919 30
1948 1950 10 13
Simplified family trees of the familial cases. For each family the country of origin is indicated. The year of birth and age of onset ( in years) appear for euch affected person. In Family A, d-I2 = dead when 12 years old and d - l w = dead when I week old; in Family B , S = subject suferedfrom stammering; in Family C , T = subject suffered from tremor.
19L3 194L 19L7 25 20 7
390 Annals of Neurology Vol 8 No 4 October 1980

previous studies of ITD among Jews were performed in populations with very few non-Ashkenazic Jews. The present country-wide survey in Israel, where non-European Jews comprise a large and well-defined segment of the population, showed that European Jews had a much higher prevalence and incidence of ITD than non-European Jews. Since all segments of the population in Israel have ready access to medical care, including hospitalization, selection artifact can- not explain this difference. In addition, our study confirmed that the disease is particularly common in Jews of Eastern European ancestry (see Table 1).
Eldridge et a1 estimated the frequency of ITD among Jews in the United States as 25 per million population initially IS], and later [ 3 ] as 59 per million. These rates are based on a denominator which is the assumed number of Jewish births in the United States. Our estimate of 22 per million population for European Jews in Israel is, however, the point- prevalence rate, age-adjusted to the United States population in 1970, i.e., it is based on a denominator which is the corresponding population living in Israel on prevalence day. Between 1949 and 1959, 190,544 Jewish live births were recorded in Israel from mothers of European or American origin (i.e., mothers born in these continents or born in Is- rael from parents of Euro-American origin). Ten of our Jewish ITD patients were born in Israel during this period, giving a rate of 52.5 per million live births, a figure closer to that of Eldridge and Gottlieb [31.
Our results, based on the exact demographic data available in Israel not only for the general population but for different ethnic groups, enable us for the first time to give accurate prevalence and incidence rates. In general, these figures confirm the previous as- sumption that ITD is more common among Ash- kenazic Jews, particularly those originating in East- ern Europe (see Tables 1-3).
Eldridge and Gottlieb’s [ 3 ] conclusion that ITD in Jews is usually inherited as an autosomal recessive disorder may be questioned on the basis of the re- sults of our Israeli study. In all families in which more than one member was affected, ITD appeared in more than one generation, suggesting autosomal dominant transmission with incomplete penetrance (see the Figure). In recessive inheritance of a rela- tively rare disorder, one would expect to find fre- quent parental consanguinity. In our material this oc- curred only once, not exceeding the rate in the general population [8 ] . In addition, contrary to what would be expected for recessive inheritance, in the familial cases siblings were never affected unless a parent was also affected.
A first approximation to test the hypothesis of re-
cessive inheritance can be based on the number of ITD patients who are offspring from rnatings of nonaffected parents as compared to matings in which one of the parents also suffered from ITD. Assuming recessive inheritance, the expected number of af- fected individuals from normal parents should be much smaller. In the four ITD families, 7 patients were products of phenotypically normal parents, and in each of 6 cases one parent was affected. In ad- dition, it should be noted that the patients with sporadic ITD had 57 nonaffected siblings, an unlikely occurrence for a recessive mode of transmission. Thus the results of our survey make it more likely that in Jews, as in non-Jews, transmission of ITD is dominant, although the penetrance rate is low.
Supported in part by a grant from the Israel-United States Bina- tional Science Foundation.
N . Zilber, on leave from the Laboratoire de Neurobiologie Cel- lulaire, 91 19O-Gif-sur-Yvette, France, received support from the Centre National de la Rcchcrche Scientifique, France.
References 1. Alter M, Kahana E, Feldman S: Differences in torsion dys-
tonia among Israeli ethnic groups. Adv Neurol 14115-120, 1975
2. Eldridge R: The torsion dystonias: literature review and ge- netic and clinical studies. Neurology (Minneap) 20: 1-78, 1970
3. Eldridge R, Gottlieb R: The primary hereditary dystonias. Adv Neurol 14:457-474, 1976
4. Eldridge R, Harlan A, Cooper IS, Riklan M: The hereditary torsion dystonias (dystonia musculorum deformans): geo- graphical distribution and IQ in dominant and recessive forms. Trans Am Neurol Assoc 94:248-250, 1969
5. Eldridge R, Koerbet T: The torsion dystonias: some genetic and psychiatric implications. Psychiatr Forum 3:27-33, 197 1
6. General Population Characteristics, U.S. Summary, U.S. De- partment of Commerce, Bureau of the Census. Washington, DC, Government Printing Office, 1970
7. Golden GS: Dystonia in the Black and Puerto Rican popula- tion. Adv Neurol 14:121-124, 1976
8. Goodman RM: Various genetic traits and diseases among the Jewish ethnic groups. Birth Defects 10:205-219, 1974
7. Hertz E: Dystonia 1. Historical review; analysis of dystonic symptoms and physiologic mechanisms involved. Arch Neurol Psychiatry 51305-355, 1944
10. Korczyn AD: The pathophysiology of dystonia. J Neural Transm 42:245-250, 1978
11. Korczyn AD, Kahana E, Alter M, et al: Dopamine-beta- hydroxylase and pupiltary sympathetic activity in idiopathic torsion dystonia. In Usdin E, Kopin IJ, Barchas I (eds): Cate- cholamines: Basic and Clinical Frontiers. New York, Perga- mon, 1979, pp 1631-1633
12. Rabinowitz R, Korczyn AD, Kahana E, et al: Serum levels of dopamine-beta-hydroxylase in dystonia. Isr J Med Sci 15:290, 1979
13. Statistical Abstract of Israel, nos. 20-29, Central Bureau of Statistics. Jerusalem, Israel, The Government Printer, 1969- 1975
Korczyn et al: Torsion Dystonia in Israel 391













![J. Irwin J. Schwartzmanl Study Design: Case Report Wall Dystonia and CRPS.pdfforms of dystonia can occur that involve all limbs [7,8]; however dystonia of axial muscles (intercostal,](https://img.pdfslide.net/doc/110x75/60277a5699a9ad280a71f846/j-irwin-j-schwartzmanl-study-design-case-report-wall-dystonia-and-crpspdf-forms.jpg)













