-
TORTICOLLISDiagnosis, Assessment, and Treatment of Infants and
Children
Krystle Chilibecki, MScPT
PresenterPresentation NotesWelcome participantsTell them where
bathrooms areTell no touching babiesSpeak about research issue: can
find something to support every opinion so this is based on our
clinical experience
-
Objectives
Provide an overview of the assessment and treatment of
torticollis
Provide a brief introduction to common head shape abnormalities
in infancy
-
Definition
Abnormal posturing of the neck
Lateral translation of the head on the trunk
Rotation and lateral head tilt
Most often affects sternocleidomastoid muscle
Not a diagnosis!
PresenterPresentation NotesNot a diagnosis-discribes a posture
only
-
Let’s review: Anatomy of the Neck
PresenterPresentation NotesDiscuss that many muscles can be
involved, does not only effect SCM
-
Types of Torticollis
Congenital
Acquired
-
Congenital Muscular Torticollis (CMT)
Etiology
Intrauterine crowding
Difficult labours and deliveries causing muscle damage
Ischemic injury due to abnormal vascular patterns (similar to
compartment syndrome)
PresenterPresentation NotesDifficult labours in up to 30 - 60%
casesMost cases no cause can be identified and that’s ok
-
CMT: A Three Dimensional Deformity
Affects growth and development of
Cranial facial system Vertebral column Shoulder girdle Pelvic
girdle Extremities Visual perceptual system
PresenterPresentation NotesWhy our assessment is 3 pages long,
needs to be extensiveTalk about new patient who has everything in
pictureNo concept of midline
-
Congenital Torticollis
Four categories
Congenital torticollis with abnormal spinal x-rays Postural
torticollis without muscle tightness or
pseudotumour Congenital muscular torticollis (CMT) with
muscle
tightness and pseudotumour (aka fibromatosis colli or SCM
tumour)
Muscular torticollis (MT) with muscle tightness and without
pseudotumour
PresenterPresentation NotesAbnormal xrays: Klippel-Feil
Syndrome, Scoliosis/Hemi-vertebrae, Unilateral atlanto-occipital
fusions, Unilateral absence of C1 facet, Sprengle’s
deformityWithout tightness or pseudotumour: will talk about what a
pseudotumour is on next slide. Often due to muscle weakness or
preference to look to one sideCan be impacted by vision
problemsPotential Causes:Benign Paroxysmal Torticollis, Congenital
absence of one or more cervical muscles, Congenital absence of
transverse ligament, Contracture of scalenes, omohyoids, Chiari
MalformationDescribe pseudotumour: normally size of pea, likely
hard, tends to become less noticable as patient grows as it stays
the same, typically diagnosed at birth and have US to rule out
pathology
-
Non-Congenital (Acquired) Torticollis
Three types
Traumatic
Painful
Non-traumaticOcular torticollis
PresenterPresentation NotesClavical fractureManual manipulation
of neck Painful: reflux, Sandifer Syndrome: haita hernia, abscess,
infections, osteoblastoma: cancer of bone, neck injury Non
traumatic: rotary subluxtion of c1 and c2 (caused by inflammation)
often resolves as inflammation resolves
-
Ocular Torticollis
Tilt to maintain binocularity and/or to optimize visual
acuity
Variety of conditions may be responsible Treatment may be
surgical Referral to developmental
optometrist necessary
-
Torticollis
Now you know what it is….but how do you use that knowledge?
-
Assessment
Infant should be undressed
Occurs in various age-appropriate positions.
PresenterPresentation NotesSupine, prone, sitting etc.Reminder:
infants should be able to hold head in midline in supine by 3-4
months of age. This is also when we expect to see righting
reactions emerging.Make friends with baby and parent, establish a
relationshipPull curtainsNeed a few fun toys or something to grab
attention
-
Assessment Form
PresenterPresentation NotesTake it or leave itCan be altered to
fit your clinic needssimple, fast and effectiveCan be done in
approx ½ hour
-
Hemihypoplasia
Enlargement of one side of the body or part of the body
Can be whole body or isolated to one body part CMT: Decreased
vertical dimension of face Can include: cheek, lip, nose, ear, eye,
tongue, jaw,
roof of the mouth, or teeth
PresenterPresentation NotesImportant to do a scan of rest of
body to ensure limbs are not affectedcan also affect internal
organsIf severe - Referral back to Dr. for further investigations
required, often need ortho consult
-
Hemihypoplasia
-
Using a Goniometer!
PresenterPresentation NotesNot necessary,We chart as a
percentage of full range, most important things is that staff
reports in the same way. Range is usually recorded as child will
move from 0-15
-
Muscle Function Scale for Infants
Ohman et al./physiotherapy theory and Practice 25 (2009)
129-137
PresenterPresentation NotesBaby should be tipped all the way to
vertical
-
Muscle Cording Upper Trap Tightness
Cording vs. Tautness
PresenterPresentation NotesDiscussion difference between cording
vs. tautness
-
Birthmarks and Dimples
Why check for them? May be linked to neurological conditions
Which ones are important? Coarse long hair Dimples in midline
where base is not easily visible Birthmarks in midline Webbing
between fingers or toes
Unsure? Refer back to doctor or to head shape clinic
PresenterPresentation NotesNeuro conditions: spina bifida,
tethered cord etc.
-
Birthmarks and Dimples
http://m1.wyanokecdn.com/0824c2d6499ca748a88aa1c6f638b568.jpghttp://m1.wyanokecdn.com/0824c2d6499ca748a88aa1c6f638b568.jpg
-
Now on to…
-
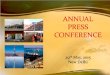
HEAD TILTPresent
↓ ROM
↓ PROMPreference: • games to
encourage rotation to opposite side
• environmental modifications
Weakness (↓ Righting Reactions)
Strengthening• diagonal
carry • righting rxns
↓ AROM
Improving
TOT Collar
Improving
Further Consults:• optometry• opthalmology• physician/
pediatrician• physiatry• request imaging• Neurosurgery•
Orthotist referral
Other Causes• occular• reflux • spasmodic
Try:• core/postural
pelvic stabilization
• other splinting positioning (ie: foam wedge cushion, kentucky
collar, over-correction with TOT collar)
Mild to Moderate (20o tilt or less or
75% – 100% PROM)
Stretches:• supine
stretches• sitting side
flexion• carry stretch• sub-occipital• 2 person
stretch
Improving
Severe (20o or more tilt or
less than 75% PROM)
Positioning:• foam collar• snug n’ go
Torticollis Flow ChartOctober 12, 2012
Examples of Improvement:
• equal righting reactions• active rotation to both sides•
increased time in midline
DDX:
• DDH• Clubfoot• Reflux• Strabismus/Occular
Problems• Chiari Malformation• Hemi-Vertebraes• Other
syndromes
NO
NO
YES
YES
YES
NO
NO
NO
YES
YESYES
Improving
Discharge
Discharge
Discharge
YES
NO
Criteria for Discharge:
• < 5o tilt• > 85% of time in midline• equal righting
reactions• full AROM rotation to both
sides
PresenterPresentation NotesTalk through this chart
-
Stretching
PresenterPresentation NotesMost common stretch is for SCM, done
in 2 separate stretches especially in young kids Too difficult to
maintain control of child and do both movements at the same
timeMention that we have lots of other stretches depending on what
muscle is effected, didn’t include them in this presentation due to
time but if you’d like more please email Krystle
-
Stretching Parameters
Hold 15-20 seconds Repeat 3 times; 5 times per day Ensure close
contact with baby Use whole hand
-
Strengthening
Righting Reactions
-
Strengthening Exercises
-
Other strengthening options:
http://www.google.ca/url?url=http://www.123rf.com/photo_19203382_mother-doing-gymnastics-with-baby-on-fitness-ball.html&rct=j&frm=1&q=&esrc=s&sa=U&ved=0ahUKEwjB_IyG2YbKAhWCLmMKHbxQCqsQwW4IHzAF&usg=AFQjCNFoQShWLeRSv2KEMf37xtpPi-AJSghttp://www.google.ca/url?url=http://fortheloveofpreschool.blogspot.com/2013/06/62-new-ways-to-play-with-exercise-ball.html&rct=j&frm=1&q=&esrc=s&sa=U&ved=0ahUKEwjB_IyG2YbKAhWCLmMKHbxQCqsQwW4IFzAB&usg=AFQjCNF31MOaMKSYRSZq_mHDpSVsZOUzDAhttp://www.google.ca/url?url=http://www.123rf.com/photo_19203382_mother-doing-gymnastics-with-baby-on-fitness-ball.html&rct=j&frm=1&q=&esrc=s&sa=U&ved=0ahUKEwjB_IyG2YbKAhWCLmMKHbxQCqsQwW4IHzAF&usg=AFQjCNFoQShWLeRSv2KEMf37xtpPi-AJSghttp://www.google.ca/url?url=http://fortheloveofpreschool.blogspot.com/2013/06/62-new-ways-to-play-with-exercise-ball.html&rct=j&frm=1&q=&esrc=s&sa=U&ved=0ahUKEwjB_IyG2YbKAhWCLmMKHbxQCqsQwW4IFzAB&usg=AFQjCNF31MOaMKSYRSZq_mHDpSVsZOUzDA
-
Treatment
Emphasize Neck and trunk strength and mobility Midline postural
control Symmetry of postural responses Symmetry of weight-bearing
and transitional movements Age-appropriate motor skill
development
-
Additional Treatment Options
TOT collar Alternative bracing Custom bracing Kinesiotape
Craniosacral therapy Myofascial therapy Osteopathy Massage
Acupuncture/Acupressure Surgery
PresenterPresentation NotesStudies suggest surgery seldom
necessary when treatment initiated early
-
Treating Older Children with Torticollis
Follow same general assessment and treatment
Thorough assessment is vital
Postural exercises Recognition of midline Consider cognitive
development Custom brace options
PresenterPresentation NotesPostural exercises, use visual
feedback, lights, mirrors, pt can participate and understandMidline
training, very important to reestablishOcular retrainingVestibular
retrainingTends to be a lengthy process, pt needs to be
dedicated.
-
Indicators for Surgical Intervention
Persistence of an intramuscular tumour Thickening of SCM muscle
at 6 months of age Plateau of improvement Increase in the deformity
Persistence of the deformity beyond 12 months of age
PresenterPresentation NotesDespite consistant intervention by
parents and therapistWe refer to our plastic surgeons Bipolar
release. Typically followed by TOT collar and stretches
-
Indications for Discharge
Full, symmetrical PROM of neck and trunk Active symmetrical head
rotation Active midline head to trunk alignment during static
and dynamic play Head righting reactions present bilaterally
Less than 5 degree tilt
PresenterPresentation NotesRoation of at least 80 degrees from
midline in both directions (without compensations)Head righting
reactions may be delayed to one side
Check midline during play in all positions
-
Post-Discharge
Infants are at risk for regression during Growth spurts Illness
TeethingAcquisition of new motor milestones
Regression should resolve in 10-14 days May require short period
of stretching
-
Normal Skull of the Newborn
-
Mal-Development
Primary = Synostotic Secondary = Positional Deformation
-
Positional Deformation
CausesProlonged external pressuresPositioning
In-UteroDeliveryAAP “Back to Sleep”
Campaign
PresenterPresentation NotesBack to sleep is now safe sleep
campaignPositioning: car seats, baby swings, bouncy
-
Plagiocephaly
FeaturesOne side of back of head is flatResults in
ipsilateralForehead bulgeEar forwardAppearance of Larger eye
-
Plagiocephaly
High risk of skull deformation with CMT Typically flattening is
on opposite side of tilt Treat with reposition strategies Improves
as the neck improves
PresenterPresentation NotesMod to severe torticollis and mod to
severe head shape may need helmet if repositioning does not work,
need to be seen by headshape clinic if querying helmetWorking
against a tight muscle
-
Plagiocephaly
-
Brachycephaly
Features Flatness across entire back of headBiparietal widening
Increased cranial vault heightProminent ears
-
PresenterPresentation NotesSubjective measurementNo magic number
that means they should have a helmet
-
Treatment of Plagiocephaly/Brachycephaly
Aggressive Repositioning Remodeling Helmet
-
Remodeling Helmet
Redistribution of forces to direct cranial growth
4 month commitment Wearing time: 23 hours/day Done by community
orthotist Follow up with orthotist every
1-3 weeks to adjust helmet $2500- $2700 cost
-
Craniosynostosis
Non-Syndromic No developmental or brain abnormalities May be
corrected with surgical intervention
Syndromic Associated anomalies Crouzon’s or Apert’s
SyndromesMuenke’s syndrome
PresenterPresentation NotesAperts: characterized by
malformations of the skull, face, hands and feet Muenke: early
synostosis of coronals often no intellectual delay but can be
-
Sagittal Synostosis
Clinical features Triangular shaped or closed anterior
fontanellePalpable ridging Long narrow headBilateral frontal
bossingProminent occiput
PresenterPresentation NotesMost common synostosisForehead wider
than back of headSurgical intervention then helmet
-
Coronal Synostosis
Can be unilateral or bilateral (rare) Clinical features
Same side as synostosis Palpable ridging Eye appears wider
Flattening of forehead
Prominent forehead on opposite side of synostosis
-
Bilateral Coronal
Clinical features Eyes are high Ears low setBilateral frontal
height Flattened foreheadPalpable ridging
bilaterally Eyes appear large
-
Metopic Synostosis
Clinical featuresNoticeable ridge
mid-forehead Eyes narrow set Triangular shaped
head when viewed from top
PresenterPresentation NotesIf not severe often not corrected
surgically
-
Lambdoid Synostosis
Clinical features Palpable ridge On same side as synostosis Ear
is back and down Prominent mastoid process Flattening in the
occipital region
Opposite side of synostosis Frontal bossingOccipital bossing
PresenterPresentation NotesOften mistaken for
torticollisRemember that flattening should push ear forward
-
Questions?
TorticollisObjectivesDefinitionLet’s review: Anatomy of the
NeckTypes of TorticollisCongenital Muscular Torticollis (CMT)CMT: A
Three Dimensional Deformity�Congenital TorticollisNon-Congenital
(Acquired) Torticollis Ocular
TorticollisTorticollisAssessmentAssessment
FormHemihypoplasiaHemihypoplasiaUsing a Goniometer!Muscle Function
Scale for Infants�Cording vs. Tautness�Birthmarks and
DimplesBirthmarks and DimplesNow on to…Slide Number
22Stretching�Stretching ParametersStrengtheningStrengthening
ExercisesOther strengthening options:TreatmentAdditional Treatment
OptionsTreating Older Children with TorticollisIndicators for
Surgical Intervention�Indications for DischargePost-DischargeSlide
Number 34Normal Skull of the NewbornMal-DevelopmentPositional
DeformationPlagiocephalyPlagiocephalyPlagiocephalyBrachycephalySlide
Number 42Treatment of Plagiocephaly/BrachycephalyRemodeling
HelmetCraniosynostosisSagittal SynostosisCoronal
SynostosisBilateral CoronalMetopic SynostosisLambdoid
SynostosisQuestions?