Embed Size (px)
Citation preview

Towards
evidence-based physiotherapy
for patients with stroke
Roland PS van Peppen

Towards evidence-based physiotherapy for patients with stroke Thesis, Utrecht University & Hogeschool Utrecht, The Netherlands ISBN 978-90-7138225-3 © 2008, Roland PS van Peppen No part of this thesis may be reproduced, stored or transmitted in any way or by any means, without prior permission of the author The printing of this thesis was financially supported by: Stichting Steunfonds Faculteit Gezondheidszorg Hogeschool Utrecht, Divisie Hersenen (UMC Utrecht), Netherlands Heart Foundation (Nederlandse Hartstichting), Stimuleringsfonds Wetenschappelijk College Fysiotherapie (WCF), Nederlandse Vereniging voor Fysiotherapie in de Geriatrie (NVFG), Boehringer Ingelheim BV, Livit Orthopedie, Abakus BV, Berkman & Van der Steeg, Electro Medico, VanP&D Professional Development in de gezondheidszorg Printed by: Gildeprint Drukkerijen, Enschede, The Netherlands © Original Artwork cover: Arno Overdevest © Cover design: Roland van Peppen

Towards
evidence-based physiotherapy
for patients with stroke
Op weg naar
evidence-based fysiotherapie
bij patiënten met een beroerte (met een samenvatting in het Nederlands)
PROEFSCHRIFT
ter verkrijging van de graad van doctor aan de Universiteit Utrecht
op gezag van de rector magnificus, prof. dr. J.C. Stoof, ingevolge het besluit van het college voor promoties
in het openbaar te verdedigen op vrijdag 30 mei 2008 des middags te 2.30 uur
door
Rolandus Petrus Stephanus van Peppen
geboren op 15 maart 1961 te Delft

Promotor: Prof. dr. E. Lindeman Co-promotoren: Dr. G. Kwakkel
Dr. N.L.U. van Meeteren
Dr. M.J. Schuurmans

Voor Coby & Martin, mijn lieve ouders


Contents Chapter 1
Introduction
9
Chapter 2 The impact of physiotherapy on functional outcome after stroke: What’s the evidence?
23
Chapter 3 Effects of augmented exercise therapy time after stroke: A meta‐analysis
67
Chapter 4 Effects of visual feedback therapy on postural control in bilateral standing after stroke: A systematic review
91
Chapter 5 The development of a clinical practice stroke guideline for physiotherapists in The Netherlands: A systematic review of available evidence
107
Chapter 6 Outcome measures in physiotherapy management of patients with stroke: A survey into self‐reported use, and barriers to and facilitators for use
137
Chapter 7 Feasibility and effectiveness of an educational program to promote the use of measurement instruments by physiotherapists involved in stroke rehabilitation: An RCT on tutor expertise
155
Chapter 8 General discussion 177
Summary 201
Nederlandse samenvatting 209
Dankwoord 219
Publications 229
About the author 235

CHAPTER
Introduction

Chapter 1
10
Introduction Stroke in the Netherlands Stroke (or cerebrovascular accident) is defined as ‘a clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hours or leading to death, with no apparent causes other than of vascular origin’.1 Depending on the location of the vascular defect(s), different functions are disturbed leading to temporary or permanent impairments, activity limitations and participation restrictions.1 Stroke is the leading cause of severe long term disability in adults in the Western world, with high societal costs due to its increasing prevalence and the long‐term disability it generally causes. For instance, in the Netherlands, the incidence of cerebrovascular accidents is estimated at about 34,500 per year (~2.2/1000/year) and the prevalence at 190,000 (~1.2% of Dutch population) patients and this prevalence will increase with 27% over the next decade.2
In the Netherlands, stroke is a highly disabling disease; about 70% of the stroke surviving patients experience long term problems in their activities of daily living (ADL) and social participation. Of these, 44% experienced mild consequences of stroke, 21% moderate, 16% severe and 19% very severe consequences of stroke.3 Physiotherapy as a part of stroke care In the absence of any cure for the initial pathology, rehabilitation is the most universally adopted treatment strategy to improve quality of life in patients with stroke.4 Rehabilitation, as described by Stucki et al5 can be defined as ‘the health strategy that aims to enable people with health conditions experiencing or likely to experience disability to achieve and maintain optimal functioning in interaction with the environment’.5,p39 The main aim of organised‐stroke rehabilitation is to achieve a level of functional independence that enables patients to return home and reintegrate into community life that lives up to their own expectations and desires as much as possible.4 In the Netherlands patients with stroke generally rehabilitate in different settings, usually started in an acute stroke‐unit care and continued in a rehabilitation centre, a nursing home, or in the community by physiotherapists employed in health centres or in private practices.6
In the Netherlands 55%‐61% of patients with a first‐ever stroke were admitted to an acute care hospital. Recent studies showed that 40%‐68% of surviving patients with stroke in Dutch acute care hospitals were discharged home, 25%‐31% to a nursing home, 9% to 15% to a rehabilitation centre.7‐9

Introduction
11
Physiotherapy is perceived as one of the key disciplines in providing organised‐stroke care.10 Physiotherapists involved in the management of patients with stroke have to: 1) deal with establishing diagnosis of functioning,11 and determine the factors for predicting functional outcome,4,12,13 2) start remedial interventions to restore motor control in gait and gait‐related activities and to improve upper limb activities, as well as to learn to cope with existing deficits in ADL and to enhance participation in general,14,15 and 3) monitor patients’ (progress in) functional health with help of outcome measures.11,16,17 Physiotherapists involved in stroke‐management often apply physical exercises and assistive devices for gait (canes and walkers). Besides they employ other equipment such as treadmills and electronic devices as therapeutic treatment interventions.6 In addition, advice and instructions are provided to the patient, family and other members of the in general interdisciplinary stroke team regarding treatment and prevention of complications such as falls and shoulder pain.14,15 Functioning, Disability and Health In 2001, the World Health Organization (WHO)18 published the International Classification of Functioning, Disability and Health (ICF) as a model to describe in a standardised language concerning human functioning in the context of health and health related issues. The ICF holds the following components: body functions and structures, activities, participation, and environmental and personal factors (Figure 1). Meanwhile, this model is widely used as a structuring framework for describing functioning of man and related outcome research.5 The ICF and recently formulated linking rules can be used for classifying the type of outcome measures in general,19 and in stroke‐management20‐22, and has been proven to be applicable in physiotherapy‐management.23,24 Figure 1. International Classification of Functioning, Disability and Health (ICF)18
PersonalFactors
Activities Participation
Health Condition(disorder or disease)
Body Functions& Structures
EnvironmentalFactors

Chapter 1
12
Evidence‐Based Practice Evidence Based Practice (EBP) is proclaimed to be a ‘new paradigm’ in which evidence from health care research is the best basis for decisions for individual patients and health systems.25 Evidence‐Based Medicine, introduced in 1991 by Guyatt and colleagues,26 has evolved over the years and was redefined recently as Evidence Based Practice in the ‘Sicily Statement’.27 EBP demands that decisions in health care, in this thesis in physiotherapy, are based on the best available, current, valid and relevant evidence combined with optimal clinical experience. These decisions should be made by those receiving care ‐the patients‐, informed by the care providers, within the context of available resources.27 In the most recent model for evidence‐based clinical decision making four aspects are considered to be of importance: 1) best research evidence, 2) patientsʹ circumstances, 3) patientsʹ preferences and actions, and 4) clinical expertise to integrate the previous components (Figure 2).27,28 Figure 2. Model of the key elements for evidence‐based clinical decision making25
Clinical expertise
Clinical stateand circumstances
Patient preferencesand actions
Research evidence

Introduction
13
Based on the model of Haynes concerning evidence‐based decision‐making, available evidence ought to guide the clinical decision‐making process of health care professionals,25 i.e. physiotherapists, dealing with the rehabilitation of patients with stroke. As of recent years, the importance of EBP, as a guide for the clinical decision making process, is increasingly being recognised by physiotherapists.29,30 Although EBP is the standard in this century and many interventions were underpinned with evidence, there are a number of gaps in the research area of stroke rehabilitation.
Lack of evidence for treatment approaches Before the 1950’s, physiotherapy for patients with neurological diseases was considered to be a muscle re‐education technique with an ‘orthopedic’ point of view. Since the advances of science in recent decades and the gradual understanding of neurophysiological principles in movement control, new concepts about the optimal physical treatment strategy for movement disorders in patients with brain damage have been developed resulting in new approaches. One of these approaches was the Bobath‐concept developed by Bertha and Karl Bobath, later known as the neuro‐developmental treatment (NDT). More than 50 years later, the revolutionary ideas of ‘the Bobaths’ have become, in the Western world, the most common approach for the treatment of neurologically impaired patients.31 Due to the increasing knowledge about functional recovery after stroke.4 and the lack of evidence for the training strategies used,32 the NDT developed and evolved over the years and included new insights into the concept. The main change was the awareness of therapists that effects of training focused on restitution of body functions hardly generalises to activities that are not directly trained in the treatment programme. Specificity of treatment effects includes also the context specificity33 suggesting that treatment effects hardly generalise beyond the environment in which the training is applied. This latter finding suggests that exercise training regimes should preferably be applied in patients own everyday surroundings.
Since the introduction of the Bobath approach there has been much criticism on the effectiveness of the concept.32,34,35 A recent Cochrane systematic review (14 trials; N=886 patients)32 critically appraised and reviewed the literature about the effects of treatment approaches aimed at promoting postural control and lower limb function, such as Bobath / NDT, Brunnstrom, Proprioceptive Neuromuscular Facilitation (PNF) and Motor Relearning Programme (MRP). They explored whether there was any difference in functional independence depending on which physiotherapy the patients with stroke received. Pollock and colleagues concluded that

Chapter 1
14
currently no evidence exists that one physiotherapy approach is superior in promoting recovery of disability after stroke. A mix of components from different approaches, an eclectic approach, seems to be more effective than no treatment or placebo control in attaining functional independence following stroke.32 Physiotherapists should therefore be encouraged to find ways of integrating these findings into their daily practice. To date, about 80% of Dutch physiotherapists in stroke management treat patients based on the principles of the NDT approach36, which is also comparable to that of colleagues in Sweden37, Australia38 and the UK39,40. In the near future the underpinning of physiotherapy stroke management has to be focused on existing evidence rather than philosophies of different approaches.
Clinical practice guidelines on stroke care Recently, the ‘best evidence’ for stroke management, derived from methodologically sound clinical research, has been collected in systematic reviews and converted into several multidisciplinary stroke guidelines.6,41‐47 However, these clinical practice guidelines, commonly defined as ‘systematically developed statements to assist practitioners and patient decisions about appropriate health care for specific clinical circumstances’,48 do not review in depth all available evidence with regard to physiotherapy practice. Physiotherapists still need to have more detailed information to foster and enrich their clinical decisions where it concerns valid functional prognosis and diagnosis, designing the most effective intervention programme, and selecting the most appropriate measures to evaluate functional outcome. These aspects have to be an integrated part of everyday practice. International physiotherapy associations already stated that assessing and monitoring the health status of patients is considered an aspect of good clinical practice in physiotherapy.49,50 However, up to 2005, no specific guidelines for physiotherapy in the management of patients with stroke were published, even though physiotherapy accounts for a substantial proportion of the total therapy time provided by stroke rehabilitation services ranging from 44 to 90%.14,51 In other words, a detailed, evidence‐based clinical practice guideline for physiotherapy‐management of patients with stroke is needed.
Guideline implementation The main benefit of clinical practice guidelines is to improve the quality of care and change behaviour of professionals. In general, clinical practical guidelines should recommend evidence based and feasible procedures to determine: 1) prognostic factors; 2) therapeutic interventions and 3)

Introduction
15
evaluative outcome measures. Clinical practice guidelines are meant to be combined with clinical experience,52,53 and are not to be seen as a magic solution which resolves problems of effectiveness of health care. Up and above, guidelines do not implement themselves spontaneously. Experts in the field recommend explicit multifactor dissemination, implementation, and audit strategies in order to integrate guidelines into daily practice of health care professionals.54 Implementation can be described as ‘a planned process and systematic introduction and/or change of proven value, with the aim to give these a structural place in professional practice, in the functioning of organisations or in the health care structure’.55,p10 In the Netherlands a standard method of implementation for clinical practice physiotherapy guidelines was developed.56 In the standard procedure of implementing the clinical practice guidelines for physiotherapy a hard‐copy of the guideline was disseminated to all members of the professional organisation of physiotherapists, the Royal Dutch Society for Physical Therapy (‘Koninklijk Nederlands Genootschap voor Fysiotherapie’: KNGF). Besides, the physiotherapists were attended to the clinical practice guidelines by publications in professional journals and platform presentations at national conferences.57
There are many different strategies to change the behaviour of practitioners in health care, and all strategies claimed to be effective.54 The literature on implementation strategies of innovations in health care is large, diverse, and complex.58 The majority of the implementation strategies, such as audit and feedback, reminder systems, and educational meetings, has been targeted at the individual professionals, particularly their knowledge, attitude and behaviour.59 Multifaceted implementation interventions (i.e., combination of interventions) were recommended for many years,54 but recently the advise about such composite‐interventions was criticised.59 Up until today, mixed effects were found for educational strategies aiming at knowledge transfer of evidence into daily practice. With respect to interactive sessions, the change in clinical practice, and with that the effectiveness of the implementation will increase.54 Jonathan Lomas described an implementation model which integrates an educational strategy in the process getting research evidence into daily practice.60,61 This implementation model can be used to structure the complex process of changing professional behaviour of physiotherapists (Figure 3).60,61 Lomas mentioned that the implementation of research information in an educational environment for practitioners and patients is a complex process, influenced by several contextual factors (administrative environment), processes (i.e. public pressure) and external factors (i.e. media).61 According

Chapter 1
16
to this model, evidence has to be disseminated in all its complexity by using educational implementation strategies, by which health care professionals have to be trained to integrate evidence into their clinical decision making process. Hereby, the interactive sessions have to integrate the debate between tutors and practitioners,54 in small group teaching‐sessions or workshops based on problem‐based learning.62
Figure 3. The implementation model described by Lomas61
Research information
Credible dissemination
Educationalenvironment
Practitioner
Patient
Economicenvironment
Administrativeenvironment
Personal Communityenvironment
context
context
Aims of the present thesis
The first aim of the present thesis was to collect and review systematically, and to appraise critically the available evidence stemming from physiotherapy and physiotherapy‐related studies in patients with stroke. On the basis of these findings, recommendations were to be made, that permitted guidance of the clinical decision‐making process of physiotherapists involved in the (interdisciplinary) care of such patients. The results of these review‐activities will be presented as a clinical practice guideline on physiotherapy management of patients with stroke.
The second aim was to integrate the recommendations of the guideline into daily physiotherapists’ practice. Subsequently, one part of the clinical practice guideline related with using the core set of outcome measures was implemented. The use of outcome measures by professionals can be seen as

Introduction
17
a useful indicator of guideline adherence.16 Based on an analysis of barriers and facilitators of implementation, an educational programme was performed to implement the recommendations into daily practice in a selected group of physiotherapists who were dedicated to the management of patients with stroke. Emphasis was given to the selection of outcome measures in practice.
Outline of the thesis First, in Chapter 2, a systematic review was performed to establish the value of the evidence of physiotherapy interventions related to improving functional outcomes after stroke and to convert this evidence in an overview of the efficacy of physiotherapy interventions in patients with stroke.
In Chapter 3, the effects of augmented exercise time were examined by systematically reviewing studies evaluating the effects of intensity of practice, expressed as time dedicated to practice, in patients with stroke on ADL, walking and dexterity. A secondary goal of this systematic review was to investigate the dose‐response relationship of augmented exercise training to outcome of ADL.
In Chapter 4, the evidence for applying ‘visual feedback therapy’ (VFT) on postural control in bilateral standing was systematically studied in patients with stroke.
In Chapter 5 the available evidence was collected and described to guide the clinical decision‐making process of physiotherapists dealing with the rehabilitation of patients with stroke especially with respect to the selection of prognostic factors, the appropriate physiotherapy interventions, and the outcome measures of choice to assess patients’ progress in functional health. This evidence is presented as a Clinical practice guideline on Physiotherapy management of patients with Stroke (CPGPS) in the Netherlands.
Assessing and monitoring the health status of patients is considered an aspect of good clinical practice in physiotherapy. Therefore, after disseminating the clinical practice guideline, physiotherapists’ self‐reported use of outcome measures as recommended in the CPGPS was investigated, and perceived barriers to and facilitators for the use of outcome measures in everyday practice were assessed in Chapter 6.
To enhance self‐reported use and actual use of the recommended outcome measures by physiotherapists in stroke management a new educational programme was developed, the Physiotherapists Educational Programme on Clinimetrics in Stroke (PEPCiS). In Chapter 7 feasibility and

Chapter 1
18
effectiveness were determined in a randomised controlled trial with thirty volunteering physiotherapists involved in stroke management who were randomised into two numeric equal groups, an expert tutor group and a non‐expert tutor group. Secondary to this aim, the influence of tutor style will be explored.
In the general discussion (Chapter 8) the pro’s and con’s of the research are discussed. Besides the possibilities and limitations of the applied methods and the implications and directions for further research and education are discussed concerning physiotherapy stroke management.
References
1. WHO. Stroke‐‐1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 1989; 20:1407‐1431.
2. Struijs JN, van Genugten ML, Evers SM et al. Modeling the future burden of stroke in The Netherlands: impact of aging, smoking, and hypertension. Stroke 2005; 36:1648‐1655.
3. Koek HL, Van Dis SJ, Peters RJG et al. Hart‐en vaatziekten in Nederland. In: Van Leest LATM, Koek HL, Van Trijp MJCA et al, editors. Hart‐en vaatziekten in Nederland 2005, cijfers over risicofactoren, ziekte, behandeling en sterfte [dutch]. Den Haag: Nederlandse Hartstichting, 2005: 6‐12.
4. Kwakkel G, Kollen B, Lindeman E. Understanding the pattern of functional recovery after stroke: facts and theories. Restor Neurol Neurosci 2004; 22:281‐299.
5. Stucki G, Cieza A, Melvin J. The international classification of functioning, disability and health (ICF): A unifying model for the conceptual description of the rehabilitation strategy. J Rehabil Med 2007; 39:279‐285.
6. Commissie CVA‐Revalidatie. Rehabilitation after a stroke, guidelines and recommendations for health care professionals (in Dutch: Revalidatie na een beroerte: richtlijnen en aanbevelingen voor zorgverleners). Franke EAM, editor. 2001. Den Haag, Dutch Heart Foundation (in Dutch: Nederlandse Hartstichting).
7. Bots ML, Looman SJ, Koudstaal PJ et al. Prevalence of stroke in the general population. The Rotterdam Study. Stroke 1996; 27:1499‐1501.
8. Koek HL, Grobbee DE, Bots ML. [Trends in cardiovascular morbidity and mortality in the Netherlands, 1980‐2000]. Ned Tijdschr Geneeskd 2004; 148:27‐32.
9. Van Exel J, Koopmanschap MA, Van Wijngaarden JD et al. Costs of stroke and stroke services: Determinants of patient costs and a comparison of costs of regular care and care organised in stroke services. Cost Eff Resour Alloc 2003; 1:2‐13.
10. Langhorne P, Legg L, Pollock A et al. Evidence‐based stroke rehabilitation. Age Ageing 2002; 31 Suppl 3:17‐20.

Introduction
19
11. Jette AM. Outcomes research: shifting the dominant research paradigm in physical therapy. Phys Ther 1995; 75:965‐970.
12. Kollen B, Van de Port I, Lindeman E et al. Predicting improvement in gait after stroke: a longitudinal prospective study. Stroke 2005; 36:2676‐2680.
13. Schenkman M, Deutsch JE, Gill‐Body KM. An integrated framework for decision making in neurologic physical therapist practice. Phys Ther 2006; 86:1681‐1702.
14. Jette DU, Latham NK, Smout RJ et al. Physical therapy interventions for patients with stroke in inpatient rehabilitation facilities. Phys Ther 2005; 85:238‐248.
15. Pomeroy VM, Tallis RC. Physical therapy to improve movement performance and functional ability poststroke. Part 1. Existing evidence. Reviews of Clinical Gerontology 2000; 10:261‐290.
16. Glasziou P, Irwig L, Mant D. Monitoring in chronic disease: a rational approach. BMJ 2005; 330:644‐648.
17. Jette AM. Assessing disability in studies on physical activity. Am J Prev Med 2003; 25 Suppl 2:122‐128.
18. WHO. ICF‐introduction, the International Classification of Functioning Disability and Health. 2001. Geneve. http://www.who.int/classification/icf/intros/ICF‐Eng‐Intro.pdf
19. Cieza A, Geyh S, Chatterji S et al. ICF linking rules: an update based on lessons learned. J Rehabil Med 2005; 37:212‐218.
20. Salter K, Jutai JW, Teasell R et al. Issues for selection of outcome measures in stroke rehabilitation: ICF Participation. Disabil Rehabil 2005; 27:507‐528.
21. Salter K, Jutai JW, Teasell R et al. Issues for selection of outcome measures in stroke rehabilitation: ICF Activity. Disabil Rehabil 2005; 27:315‐340.
22. Salter K, Jutai JW, Teasell R, et al. Issues for selection of outcome measures in stroke rehabilitation: ICF Body Functions. Disabil Rehabil 2005; 27:191‐207.
23. Jette AM. Physical disablement concepts for physical therapy research and practice. Phys Ther 1994; 74:380‐386.
24. Jette AM. Toward a common language for function, disability, and health. Phys Ther 2006; 86:726‐734.
25. Haynes RB. What kind of evidence is it that Evidence‐Based Medicine advocates want health care providers and consumers to pay attention to? BMC Health Serv Res 2002; 2:3‐10.
26. Guyatt G. Evidence‐Based Medicine. ACP J Club 1991;A‐16:114.
27. Dawes M, Summerskill W, Glasziou P et al. Sicily statement on evidence‐based practice. BMC Med Educ 2005; 5:1‐7.
28. Haynes RB, Devereaux PJ, Guyatt GH. Clinical expertise in the era of evidence‐based medicine and patient choice. Vox Sang 2002; 83 Suppl 1:383‐386.
29. Holm M. Our mandate for the new millennium: evidence based practice. Am J Occup Ther 2000; 54:575‐585.

Chapter 1
20
30. Parker‐Taillon D. CPA initiatives put the spotlight on evidence‐based practice in physiotherapy. Physiother Can 2002; 24:12‐15.
31. Lennon S, Ashburn A, Baxter D. Gait outcome following outpatient physiotherapy based on the Bobath concept in people post stroke. Disabil Rehabil 2006; 28:873‐881.
32. Pollock A, Baer G, Langhorne P et al. Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke: a systematic review. Clin Rehabil 2007; 21:395‐410.
33. Lennon S, Ashburn A. The Bobath concept in stroke rehabilitation: a focus group study of the experienced physiotherapistsʹ perspective. Disabil Rehabil 2000; 22:665‐674.
34. Luke C, Dodd KJ, Brock K. Outcomes of the Bobath concept on upper limb recovery following stroke. Clin Rehabil 2004; 18:888‐898.
35. Paci M. Physiotherapy based on the Bobath concept for adults with post‐stroke hemiplegia: a review of effectiveness studies. J Rehabil Med 2003; 35:2‐7.
36. Hafsteinsdottir TB, Algra A, Kappelle LJ et al. Neurodevelopmental treatment after stroke: a comparative study. J Neurol Neurosurg Psychiatry 2005; 76:788‐792.
37. Nilsson LM, Nordholm LA. Physical therapy in stroke rehabilitation: basis for Swedish physiotherapistsʹ choice of treatment. Physiotherapy Theory and Practice 1992; 8:49‐55.
38. Carr JH, Mungovan SF, Shepherd RB et al. Physiotherapy in stroke rehabilitation: a basis for Australian physiotherapistsʹ choice of treatment. Physiotherapy Theory and Practice 1994; 10:201‐209.
39. Davidson I, Waters K. Physiotherapists working with stroke patients: a national survey. Physiotherapy 2000; 86:69‐80.
40. Lennon S, Baxter D, Ashburn A. Physiotherapy based on the Bobath concept in stroke rehabilitation: a survey within the UK. Disabil Rehabil 2001; 23:254‐262.
41. Dutch Institute for Quality in Health Care (in Dutch: Kwaliteitsinstituut voor de gezondheidszorg Utrecht‐CBO‐). CBO Richtlijn Beroerte (Stroke Guidelines 2000, in Dutch). 2000. Den Haag, Nederlandse Hartstichting.
42. Scottish Intercollegiate Guidelines Network. Management of patients with stroke, rehabilitation, prevention and management of complications and discharge planning ‐ a national clinical guideline (no: 64). 2002. Edinburgh, SIGN.
43. Agency for Health Care Policy and Research. Post‐Stroke Rehabilitation: clinical practice guideline. No.16. 1995. Rockville, AHCPR Publication 95‐0662.
44. Royal College of Physicians ‐ the intercollegiate working party for stroke. National Clinical Guidelines for Stroke. 1999. London.
45. Hanger HC, Wilkinson T, Keeling S, Sainbury R. New Zealand guideline for management of stroke. N Z Med J 2004; 117:U863.
46. National Stroke Foundation. Clinical Guidelines for Stroke Rehabilitation and Recovery (Australian Government). 2005.
47. Khadilkar A, Phillips K, Jean N et al. Ottawa panel evidence‐based clinical practice guidelines for post‐stroke rehabilitation. Top Stroke Rehabil 2006; 13:1‐269.

Introduction
21
48. Field MJ, Lohr KN. Guidelines for clinical practice. From development to use. Washington DC: National Academy Press, 1992.
49. American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. Phys Ther 2001; 81(1):9‐746.
50. Australian Physiotherapy Association. APA Position Statement ‐ Clinical justification and outcome measures 2003: https://apa.advsol.com.au/staticcontent/staticpages/position_statements/public/ClinicalJustification&Outcome%20Measures.pdf
51. De Wit L, Putman K, Dejaeger E et al. Use of time by stroke patients: a comparison of four European rehabilitation centers. Stroke 2005; 36:1977‐1983.
52. Davidoff F. In the teeth of the evidence: the curious case of evidence based medicine. Mt Sinai J Med 1999; 66:75‐83.
53. Mulrow CD, Cook DJ, Davidoff F. Systematic reviews: critical links in the great chain of evidence. Ann Intern Med 1997; 126:389‐391.
54. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patientsʹ care. Lancet 2003; 362:1225‐1230.
55. Grol R, Wensing M, Eccles M. Improving patient care. The implementation of change in clinical practice. London: Elsevier Butterworth Heinemann, 2005.
56. Hendriks HJM, Bekkering GE, van Ettekoven H et al. Development and implementation of national practice guidelines: a prospect for continuous quality improvement in physiotherapy. Physiotherapy 2000; 86:535‐547.
57. Bekkering GE, Engers AJ, Wensing M et al. Development of an implementation strategy for physiotherapy guidelines on low back pain. Aust J Physiother 2003; 49:208‐214.
58. Greenhalgh T, Robert G, Macfarlane F et al. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q 2004; 82:581‐629.
59. Grimshaw JM, Thomas RE, MacLennan G et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess 2004; 8:iii‐72.
60. Lomas J. Teaching old (and not so old) does new tricks: effective ways to implement research findings. In: Dunn EV, Norton PG, Steward M, Tudiver F, Bass MJ, editors. Volume 6: Disseminating research / changing practice. London: Sage, 1993.
61. Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care 1998; 7:149‐158.
62. Davis WK, Nairn R, Paine ME et al. Effects of expert and non‐expert facilitators on the small‐group process and on student performance. Acad Med 1992; 67:470‐474.

Chapter 1
22

CHAPTER
The impact of physiotherapy on functional outcome after stroke: What’s the evidence?
Roland PS Van Peppen
Gert Kwakkel
Sharon Wood‐Dauphinee
Erik JM Hendriks
Philip J Van der Wees
Joost Dekker
Clinical Rehabilitation 2004; 18(8): 833‐862

Chapter 2
24
Abstract Objective: To determine the evidence for physiotherapy interventions aimed at improving functional outcome after stroke. Methods: MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, DARE, PEDro, EMBASE and DocOnline were searched for controlled studies. Physiotherapy was divided into 10 intervention categories, which were analysed separately. If statistical pooling (weighted summary effect sizes) was not possible due to lack of comparability between interventions, patient characteristics and measures of outcome, a best‐research synthesis was performed. This best‐research synthesis was based on methodological quality (PEDro score). Results: In total, 151 studies were included in this systematic review; 123 were randomised controlled trials (RCTs) and 28 controlled clinical trials (CCTs). Methodological quality of all RCTs had a median of 5 points on the 10‐point PEDro scale (range 2‐8 points). Based on high‐quality RCTs strong evidence was found in favour of task‐oriented exercise training to restore balance and gait, and for strengthening the lower paretic limb. Summary effect sizes (SES) for functional outcomes ranged from 0.13 (95% CI: 0.03 –0.23) for effects of high intensity of exercise training to 0.92 (95% CI: 0.54 –1.29) for improving symmetry when moving from sitting to standing. Strong evidence was also found for therapies that were focused on functional training of the upper limb such as constraint‐induced movement therapy (SES 0.46; 95% CI: 0.07 – 0.91), treadmill training with or without body weight support, respectively 0.70 (95% CI: 0.29 – 1.10) and 1.09 (95% CI: 0.56 – 1.61), aerobics (SES 0.39; 95% CI: 0.05 – 0.74), external auditory rhythms during gait (SES 0.91; 95% CI: 0.40 – 1.42) and neuromuscular stimulation for glenohumeral subluxation (SES 1.41; 95% CI: 0.76 – 2.06). No or insufficient evidence in terms of functional outcome was found for: traditional neurological treatment approaches; exercises for the upper limb; biofeedback; functional and neuromuscular electrical stimulation aimed at improving dexterity or gait performance; orthotics and assistive devices; and physiotherapy interventions for reducing hemiplegic shoulder pain and hand oedema. Conclusions: This review showed small to large effect sizes for task‐oriented exercise training, in particular when applied intensively and early after stroke onset. In almost all high‐quality RCTs, effects were mainly restricted to tasks directly trained in the exercise program.

Impact of physiotherapy on functional outcome
25
Introduction Systematic research has shown that organised multidisciplinary care and rehabilitation after stroke enhance patient survival and independence, as well as reducing the length of inpatient stay.1‐3 It remains unclear, however, why specialised stroke units are more effective than usual care. A number of components have been identified as contributing to the efficacious care delivered in such units. These include the comprehensive assessment of medical problems, impairments and disabilities; active physiological management; early mobilisation and avoidance of bedrest; skilled nursing care; early setting of rehabilitation plans involving carers; and early assessment and planning for discharge needs.1,4 Several of these factors are closely related to physiotherapy which is often perceived as one of the key disciplines in organised stroke care.5 In addition, a recent Cochrane review of 14 trials (N=1617) showed that outpatient services, including physiotherapy, may prevent deterioration in seven of 100 stroke patients residing in the community.6 The main foci of physiotherapy after stroke are to restore motor control in gait and gait‐related activities and to improve upper limb function, as well as to learn to cope with existing deficits in activities of daily living (ADL) and to enhance participation in general. Besides using physical exercises, physiotherapists often apply assistive devices for gait, and employ other equipment such as treadmills and electronic devices to support their treatments. In addition, advice and instructions are provided to the patient, family and other members of the stroke team regarding prevention of complications such as falls and shoulder pain. Today, the importance of evidence based medicine, as a guide for the clinical decision making process, is increasingly being recognised by physiotherapists.7,8 However, the efficacy of physiotherapy interventions for stroke has not been summarised in a systematic review. The objective of the present systematic review was to establish the evidence of physiotherapy interventions related to improving functional outcomes after stroke. Material and Methods Literature search A computerised literature search was conducted in MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, DARE, PEDro, EMBASE and DocOnline (Database of

Chapter 2
26
the Dutch Institute of Allied Health Care). Two researchers (RPSvP and JCFK) independently searched these electronic databases for relevant articles. The search strategy was built on cerebrovascular disease (patient type) and physiotherapy interventions (treatment type). Randomised controlled trials (RCTs) as well as controlled clinical trials (CCTs) were included for review. Excluded were noncontrolled pre‐experimental studies and controlled studies that investigated robotics or the effects of physiotherapy in combination with acupuncture or drug therapies. Studies were collected up to January 2004. The following MeSH and keywords were used for the electronic databases: cerebrovascular disorders, cerebrovascular accident, stroke, hemiplegia, physiotherapy, occupational therapy, exercise therapy, and rehabilitation. Bibliographies of review articles, narrative reviews and abstracts published in conference proceedings were also evaluated for relevant publications. In addition, citation tracking of all article references was conducted. Only articles written in English, German or Dutch were included for review. Inclusion of articles was based on agreement between the two independent reviewers. The full search strategy is available on request from the corresponding author. Subsequently, the two reviewers independently determined from the title and the abstract if the papers satisfied the following criteria: population of adults (18 years or older) diagnosed with stroke and studies evaluating effectiveness of physiotherapy interventions.
Intervention categories For the present review, physiotherapy was classified into 10 intervention categories to evaluate the effectiveness of: 1) traditional neurological treatment approaches; 2) programs for training sensorimotor function or influencing muscle tone; 3) cardiovascular fitness and aerobic programs; 4) methods for training mobility and mobility‐related activities; 5) exercises for the upper limb; 6) biofeedback therapy for the upper and lower limb; 7) functional and neuromuscular electrical stimulation for both limbs; 8) orthotics and assistive devices for both limbs; 9) treatments for hemiplegic shoulder pain and hand oedema; and 10) intensity of exercise therapy. This classification was based on the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization9 and the American Physical Therapy Association guide to physical therapist practice (2nd edition)10. A group of eight physiotherapists and two reviewers (GK and RPSvP) reached consensus about the categories.

Impact of physiotherapy on functional outcome
27
Methodological quality The methodological quality of the RCTs was rated with the PEDro scale.11 RCTs were scored by two independent reviewers (RPSvP and GK). Inter‐rater reliabilities of individual items of the PEDro scale were calculated by Cohen’s kappa. In case of disagreement, consensus was sought, but when disagreement persisted, a third independent reviewer (SWD) made the final decision. PEDro scores of 4 points or higher were classified as ‘high‐quality’, whereas studies with 3 points or lower were ‘low‐quality’. PEDro scores were not used as inclusion/exclusion criteria, but rather as a basis for best‐evidence synthesis and to discuss the strengths and weaknesses of studies.
Quantitative analysis Analysis of the results was performed separately for each intervention and restricted to RCTs. When they were comparable in terms of interventions, patient characteristics and outcome measures, statistical pooling was performed. Randomised studies using a cross‐over design were judged as an RCT by calculating effects before the point of cross‐over. The data were reanalysed by pooling the individual effect sizes using fixed effect sizes.12,13 Fixed effect sizes gu (Hedges’ g), were calculated for each study by finding the difference between mean changes in the experimental group and in the control group and dividing by the average population standard deviation (SDi). To estimate SDi for gu, baseline estimates and standard deviations of the control and experimental groups were pooled. The impact of sample size was addressed by estimating a weighting factor (wi) for each study, and assigning larger effect‐weights in studies with bigger samples. Subsequently, gu of individual studies were averaged, resulting in a weighted SES, whereas the weights of each study were combined to estimate the variance of the SES.14 If significant between‐study variation existed (statistical heterogeneity) a random effects model was applied.15 Based on the classification of Cohen, effect sizes below 0.2 were classified as small, from 0.2 to 0.5 as medium and above 0.5 as large.16
Best‐evidence synthesis If pooling of studies was not possible due to differences in outcomes, intervention types, patient characteristics or lack of point estimates (means and medians) and/or measures of variability (e.g. standard deviations and confidence intervals) a best research synthesis was applied. For this purpose we used the criteria set out by Van Tulder et al17 based on the methodological quality score of the PEDro scale. Subsequently, studies were categorised into five levels of evidence: 1) strong evidence, 2) moderate

Chapter 2
28
evidence, 3) limited evidence, 4) indicative findings, 5) no or insufficient evidence (Table 1).37
Table 1 – Best-evidence synthesis
Strong evidence
provided by statistically significant findings in outcome measures in • at least 2 high-quality RCTs, with PEDro scores of at least 4 pointsa
Moderate evidence
provided by statistically significant findings in outcome measures in • at least one high-quality RCT and • at least one low-quality RCT (< 3 points on PEDro) or one high-quality CCTa
Limited evidence
provided by statistically significant findings in outcome measures in • at least one high-quality RCT or • at least two high-quality CCTsa (in the absence of high-quality RCTs)
Indicative findings
provided by statistically significant findings in outcome measures in at least • one high-quality CCT or low-quality RCTs* (in the absence of high-quality
RCTs), or • two studies of a non-experimental nature with sufficient quality (in absence of
RCTs and CCTs)a
No or insufficient evidence
• in the case that results of eligible studies do not meet the criteria for one of the
above stated levels of evidence, or • in the case of conflicting (statistically significant positive and statistically
significant negative) results among RCTs and CCTs, or • in the case of no eligible studies
a If the number of studies that show evidence is < 50% of the total number of studies found within the same category of methodological quality and study design (RCT, CCT or non-experimental studies), no evidence will be classified.

Impact of physiotherapy on functional outcome
29
Results Literature search using multiple databases yielded 8024 citations on 29 January, 2004. After restricting these to the publication type ʹclinical trialʹ, 735 remained. Following the exclusion of: 1) pre‐experimental studies and 2) controlled studies investigating the effects of physiotherapy interventions that included people with nonstroke as a diagnosis or interventions with acupuncture, drugs or robotics, 204 relevant studies were selected by title and abstract. Twenty‐two of these articles were systematic reviews,13,18‐38 and 20 were critical or narrative reviews.39‐58 Eleven of the remaining 162 studies had been published in more than one article.59‐80 A total of 151 publications (123 RCTs and 28 CCTs) that focused on the effectiveness of physiotherapy interventions in people with stroke were included for further analysis. Cohen’s κ, as an estimate of agreement between the two raters for methodological quality of the 123 RCTs, was 0.81. For each intervention category the results of the studies that contributed to the meta‐analysis or best‐evidence synthesis are presented in Tables 2 and 3. The methodological quality of the RCTs is reported in Table 4.
1. Evidence related to the effects of the traditional neurological treatment approaches
Eight RCTs67,81‐87 and 2 CCTs88,89 investigated the effects of using a specific neurological treatment approach. Numbers of patients, characteristics of the interventions, measures of outcome and observed effects are shown in Table 2. Different neurological treatment approaches including Bobath,67,81‐83,86,88 Brunnstrom,85,87,89 Rood,82,83 Johnstone,84 Proprioceptive Neuromuscular Facilitation (PNF),85,88 Motor Relearning Programme (MRP),67 Ayres82 or combinations of the above89 were investigated. With exception of 2 RCTs84,85 all studies evaluated the effects of Bobath in one of the treatment arms, whereas one study used two experimental groups.86 Eight studies measured ADL with the Barthel Index (BI),67,82,83,86,88 the Functional Independence Measure (FIM)87 or other ADL scales85,89 as an outcome, and four studies evaluated strength,83,85 synergism84 or muscle tone88. Three studies assessed the effects of a neurological approach on length of stay (LOS)67,85,89 and compared the effects of MRP and Bobath,67 PNF and Brunnstrom85 or neuromuscular retraining techniques,89 whereas one CCT compared an impairment orientated with a disability focused approach.90 The quality score of the RCTs ranged from 382,83 to 667. Due to differences in both aims and outcomes, pooling of the studies was not possible. Best‐

Chapter 2
30
Ref
eren
ces
8 R
CTs
: 67,
81-8
7 2
CC
Ts: 8
8,89
6 R
CTs
: 91-
96
2 C
CTs
: 97,
98
1 C
CT:
99
9 R
CTs
: 71,
84,1
00-
106
1 C
CT:
107
3 R
CTs
: 109
-111
1
CC
T: 1
12
M.Q
. (P
ED
ro)
rang
e
3 –
6 p.
4 –
7 p.
4 p.
2 –
7 p.
4 –
7 p.
Res
ults
Mod
erat
e ev
iden
ce fo
und
for
redu
cing
LO
S in
favo
ur o
f con
trol
grou
ps. N
o ev
iden
ce fo
und
for
impr
ovin
g m
uscl
e st
reng
th,
syne
rgis
m, m
uscl
e to
ne, w
alki
ng
abili
ty, d
exte
rity
or A
DL.
Stro
ng e
vide
nce
foun
d fo
r im
prov
ing
mus
cle
stre
ngth
of
low
er e
xtre
mity
in fa
vour
of
expe
rimen
tal g
roup
s.
Lim
ited
evid
ence
foun
d fo
r im
prov
ing
gait
perfo
rman
ce o
r w
alki
ng e
ndur
ance
. No
evid
ence
fo
und
for i
mpr
ovin
g ha
ndgr
ip
forc
e, d
exte
rity,
sym
met
ry o
f w
eigh
t dis
tribu
tion,
tran
sfer
ring,
ga
it sp
eed,
sta
ir-w
alki
ng o
r ph
ysic
al a
nd m
enta
l hea
lth.
Indi
cativ
e fin
ding
s fo
und
for
impr
ovin
g so
mat
osen
sory
pe
rcep
tion.
Stro
ng e
vide
nce
foun
d fo
r re
duci
ng m
uscl
e to
ne in
favo
ur
of T
EN
S. L
imite
d ev
iden
ce fo
und
for A
RO
M in
favo
ur o
f slo
w
stre
tch
tech
niqu
es.
Insu
ffici
ent e
vide
nce
foun
d fo
r im
prov
ing
PR
OM
in fa
vour
of
TEN
S a
nd c
asts
or s
plin
ts.
Stro
ng e
vide
nce
foun
d fo
r m
axim
al w
orkl
oad,
gai
t spe
ed o
r w
alki
ng d
ista
nce
in fa
vour
of
expe
rimen
tal g
roup
s. L
imite
d ev
iden
ce fo
und
for a
erob
ic
capa
city
. No
evid
ence
foun
d fo
r sy
nerg
ism
, bas
ic A
DL
or
inst
rum
enta
l AD
L.
Inte
nsity
of
inte
rven
tion
mea
n (r
ange
)
30 –
90
min
/d
3 –
5 x
p/w
du
ring
2 –
8 w
30 –
90
min
/d
2 –
5 x
p/w
du
ring
2 –
6 w
20 –
45
min
/d
3 –
5 x
p/w
, du
ring
4 –
6 w
5 –
60
min
/d
2 –
5 x
p/w
du
ring
3 –
12 w
30 –
90
min
/d
3 –
5 x
p/w
du
ring
8 –
10 w
Mea
n tim
e po
st-s
troke
(r
ange
)
~ 1
w –
4.8
y
~ 3
mo
– 4
y
6.2
y
< 11
w –
6.7
y
> 30
d - >
6 m
o
N
RC
Ts:3
69
CC
Ts:1
70
RC
Ts:2
94
CC
Ts:4
7 C
CT:
39
RC
Ts: 2
45
CC
T: 8
R
CTs
:154
C
CT:
9
Type
of
inte
rven
tion
Trad
ition
al
neur
olog
ical
tre
atm
ent
appr
oach
es
Stre
ngth
enin
g pa
retic
mus
cles
Trai
ning
sen
sory
in
tegr
ity
Influ
enci
ng
mus
cle
tone
and
st
iffne
ss
Trai
ning
en
dura
nce
Tabl
e 2
P
hysi
othe
rapy
inte
rven
tion
cate
gorie
s In
terv
entio
n ca
tego
ries
1. N
euro
logi
cal
trea
tmen
t ap
proa
ches
2. P
rogr
ams
for
trai
ning
sen
sory
-m
otor
func
tion
or
influ
enci
ng m
uscl
e to
ne
3.C
ardi
ovas
cula
r fit
ness
and
aer
obic
pr
ogra
ms

Impact of physiotherapy on functional outcome
31
Ref
eren
ces
5 R
CTs
: 80,
113-
116
4 R
CTs
: 86,
117-
119
5 R
CTs
: 61
,113
,117
,119
,120
8 R
CTs
: 121
-127
, 12
9 1
CC
T: 1
28
5 R
CTs
: 77,
130-
133
2 C
CT:
134
,135
M.Q
. (P
ED
ro)
rang
e
3 –
7 p.
5 –
7 p.
5 –
7 p.
4 –
6 p.
4 –
7 p.
Res
ults
Stro
ng e
vide
nce
foun
d fo
r aer
obic
ca
paci
ty a
nd m
uscl
e st
reng
th o
f the
lo
wer
ext
rem
ity in
favo
ur o
f the
ex
perim
enta
l gro
ups.
No
evid
ence
fo
und
for s
yner
gism
, wal
king
en
dura
nce
and
gait
spee
d.
Stro
ng e
vide
nce
foun
d fo
r wei
ght
dist
ribut
ion
betw
een
pare
tic a
nd
nonp
aret
ic s
ide
in fa
vour
of
expe
rimen
tal g
roup
s.
Stro
ng e
vide
nce
foun
d fo
r sy
mm
etry
bet
wee
n bo
th le
gs d
urin
g si
t-to-
stan
d an
d st
and-
to-s
it or
tim
e ne
eded
to s
tand
up
or s
it-do
wn
in
favo
ur o
f exp
erim
enta
l gro
up.
Lim
ited
evid
ence
foun
d fo
r red
ucin
g th
e oc
curr
ence
of f
alls
.
Stro
ng e
vide
nce
foun
d fo
r red
ucin
g po
stur
al s
way
or i
ncre
asin
g sy
mm
etry
of w
eigh
t dis
tribu
tion
durin
g st
ance
in fa
vour
of
expe
rimen
tal g
roup
s.
No
evid
ence
foun
d fo
r bal
ance
m
easu
red
with
the
Ber
g B
alan
ce
Sca
le, w
here
as n
egat
ive
effe
cts
foun
d fo
r tim
ed u
p-an
d-go
.
Stro
ng e
vide
nce
foun
d fo
r im
prov
ing
wal
king
end
uran
ce in
fa
vour
of B
WS
TT. N
o ev
iden
ce
foun
d fo
r im
prov
ing
post
ural
co
ntro
l, w
alki
ng a
bilit
y or
co
mfo
rtabl
e ga
it sp
eed.
Inte
nsity
of
inte
rven
tion
mea
n (r
ange
)
60 –
90
min
/d
3 –
10 x
p/w
du
ring
4 –
12 w
30 –
120
min
/d
5 x
p/w
, du
ring
2 –
4 w
15 –
30
min
/d
5 –
15 x
p/w
du
ring
2-6
w
15 –
60
min
/d
3 –
10 x
p/w
du
ring
2 –
8 w
20 –
45
min
/d
3 –
5 x
p/w
du
ring
2 –
11 w
Mea
n tim
e po
st-s
troke
(r
ange
)
10 d
– 8
y
2 w
– 6
.3 y
38 d
– 6
.3 y
33 d
– 1
8 m
o
17 d
– 2
6 m
o
N
RC
Ts: 1
97
RC
Ts: 1
08
RC
Ts: 1
56
RC
Ts: 2
12
CC
T: 4
2 R
CTs
: 268
C
CT:
43
Type
of
inte
rven
tion
Trai
ning
ae
robi
cs
Trai
ning
sitt
ing
bala
nce
Trai
ning
tra
nsfe
rs fr
om
sit-t
o-st
and
and
visa
ver
sa
Trai
ning
st
andi
ng b
alan
ce
Body
-wei
ght
supp
orte
d tre
adm
ill tra
inin
g
Tabl
e 2
- Con
tinue
d -
Inte
rven
tion
cate
gorie
s
4. M
etho
ds fo
r tr
aini
ng m
obili
ty
and
mob
ility
re
late
d ac
tiviti
es

Chapter 2
32
Ref
eren
ces
5 R
CTs
: 80,
136-
139
3 R
CTs
: 140
-142
1 R
CT:
143
1 R
CT:
144
1
CC
T: 1
45
11 R
CTs
: 65
,69,
73,8
2,83
,87,
11
0,14
6-14
9
6 R
CTs
: 150
-155
1 R
CT:
156
1
CC
T: 9
7 2
RC
Ts: 1
46,1
57
M.Q
. (P
ED
ro)
rang
e
4 –
7 p.
3 –
6 p.
7 p.
7 p
.
3 –
7 p.
4 –
7 p.
3 p
.
4 –
5 p.
Res
ults
Stro
ng e
vide
nce
foun
d fo
r im
prov
ing
wal
king
abi
lity
in
favo
ur o
f tre
adm
ill tra
inin
g w
ithou
t bod
y w
eigh
t sup
port.
No
evid
ence
foun
d fo
r inc
reas
ing
com
forta
ble
gait
spee
d.
Stro
ng e
vide
nce
foun
d fo
r im
prov
ing
strid
e le
ngth
and
co
mfo
rtabl
e ga
it sp
eed
in fa
vour
of
ext
erna
l aud
itory
rhyt
hms.
No
evid
ence
foun
d in
favo
ur o
f lim
b lo
adin
g fo
r im
prov
ing
lanc
e co
ntro
l or g
ait s
peed
.
No
evid
ence
foun
d fo
r in
fluen
cing
mus
cle
tone
or
impr
ovin
g A
DL.
Insu
ffici
ent e
vide
nce
foun
d fo
r im
prov
ing
dext
erity
or A
DL
in
favo
ur o
f the
exp
erim
enta
l gr
oups
. No
evid
ence
foun
d fo
r m
uscl
e st
reng
th a
nd s
yner
gism
.
Stro
ng e
vide
nce
foun
d fo
r de
xter
ity o
f the
par
etic
arm
in
favo
ur o
f CIM
T. N
o ev
iden
ce
foun
d fo
r the
am
ount
of (
pare
tic)
arm
use
or A
DL.
Indi
cativ
e fin
ding
s fo
und
for
impr
ovin
g gr
ip s
treng
th o
r de
xter
ity o
f the
par
etic
arm
in
favo
ur o
f bila
tera
l arm
trai
ning
-pr
ogra
ms.
Lim
ited
evid
ence
foun
d fo
r im
prov
ing
dext
erity
of t
he p
aret
ic
arm
in fa
vour
of m
irror
ther
apy.
Inte
nsity
of
inte
rven
tion
mea
n (r
ange
)
5 –
60 m
in/d
3
– 5
x p/
w
durin
g 3
– 6
w
20 –
30
min
/d
2 –
10 x
p/w
du
ring
3 –
12 w
10 m
in/d
7
d/w
, du
ring
6 w
RC
T: d
urin
g 8
w
CC
T: ?
30 –
90
min
/d
3 –
5 x
p/w
du
ring
5 –
20 w
2 –
10 h
rs
imm
obilis
atio
n p/
d;
1-6
hrs
train
ing/
day
3 –
7 x
p/w
du
ring
2 –
10 w
15 –
20
min
/d
3 –
10 x
p/w
du
ring
2 –
6 w
15 –
30
min
/d
2 –
6 x
p/w
du
ring
5 –
8 w
Mea
n tim
e po
st-s
troke
(r
ange
)
10 d
– (>
6 m
o)
16 d
– 3
2 m
o
> 6
mo
RC
T: 1
6 d
CC
T: ?
7 d
– 4.
8 y
6 d
– 4.
8 y
8.4
w –
6.5
y
10 m
o –
4.8
y
N
RC
Ts: 1
63
RC
Ts: 8
0
RC
T: 2
4
RC
T: 1
6 d
CC
T: ?
RC
Ts: 9
71
RC
Ts: 1
34
RC
T: 7
C
CT:
27
RC
Ts: 2
5
Type
of
inte
rven
tion
Trea
dmill
train
ing
with
out
body
wei
ght
supp
ort
Ext
erna
l aud
itory
rh
ythm
s
Lim
b lo
adin
g
Whe
elch
air s
elf-
prop
ellin
g
Exe
rcis
ing
the
pare
tic a
rm
Con
stra
int-
indu
ced
mov
emen
t th
erap
y
Bila
tera
l arm
tra
inin
g
Mirr
or th
erap
y
Tabl
e 2
- Con
tinue
d -
Inte
rven
tion
cate
gorie
s
5.Ex
erci
ses
for
the
uppe
r lim
b

Impact of physiotherapy on functional outcome
33
Ref
eren
ces
12 R
CTs
: 140
,158
-16
8 4
CC
Ts: 1
69-1
72
10 R
CTs
: 81
,163
,173
-180
3
CC
Ts: 1
81-1
83
5 R
CTs
: 162
,184
-18
7
4 R
CTs
: 188
-191
4 R
CTs
: 192
-195
1
CC
T: 1
96
M.Q
. (P
ED
ro)
rang
e
2 –
6 p.
2 –
7 p.
4 –
6 p.
3 –
7 p.
3 –
5 p.
Res
ults
No
evid
ence
foun
d fo
r im
prov
ing
activ
e R
OM
ank
le o
r com
forta
ble
gait
spee
d in
favo
ur o
f bi
ofee
dbac
k th
erap
y.
Insu
ffici
ent e
vide
nce
foun
d fo
r im
prov
ing
dext
erity
in fa
vour
of
biof
eedb
ack
ther
apy.
No
evid
en-
ce fo
und
for i
mpr
ovin
g m
uscl
e st
reng
th a
nd a
ctiv
e R
OM
.
Lim
ited
evid
ence
foun
d fo
r im
prov
ing
mus
cle
stre
ngth
, ph
ysio
logi
cal c
ost i
ndex
or
wal
king
abi
lity
in fa
vour
of F
ES
. N
o ev
iden
ce fo
und
for i
mpr
ovin
g sy
nerg
ism
of l
ower
ext
rem
ity,
gait
spee
d or
AD
L.
Lim
ited
evid
ence
foun
d fo
r im
prov
ing
mus
cle
stre
ngth
of t
he
exte
nsor
s of
the
pare
tic fo
rear
m
or d
exte
rity.
The
evi
denc
e fo
r de
xter
ity w
as re
stric
ted
only
for
patie
nts
with
vol
unta
ry m
ove-
men
t con
trol o
f ext
ensi
on o
f wris
t an
d fin
gers
. No
evid
ence
foun
d fo
r dex
terit
y in
pat
ient
with
out
volu
ntar
y m
ovem
ent c
ontro
l. In
dica
tive
findi
ngs
foun
d fo
r im
prov
ing
activ
e R
OM
in fa
vour
of
the
expe
rimen
tal g
roup
s.
Insu
ffici
ent e
vide
nce
foun
d fo
r im
prov
ing
mus
cle
stre
ngth
or
dext
erity
of t
he p
aret
ic a
rm. N
o ev
iden
ce fo
und
for i
mpr
ovin
g sy
nerg
ism
in fa
vour
of t
he
expe
rimen
tal g
roup
s.
Inte
nsity
of
inte
rven
tion
mea
n (r
ange
)
20 –
60
min
/d
2 –
5 x
p/w
du
ring
2 –
12 w
2 0
– 60
min
/d
2 –
5 x
p/w
du
ring
1 –
10 w
20 –
60
min
/d
3 –
5 x
p/w
du
ring
4 –
6 w
30 –
90
min
/d
1 –
3 x
p/d
durin
g 3
– 8
w
30 –
90
min
/d
3 –
5 x
p/w
du
ring
2 –
12 w
Mea
n tim
e po
st-s
troke
(r
ange
)
36 d
– 3
3.6
mo
7 w
– 3
.1 y
26 d
– 4
.5 y
16 d
– 3
mo
18 d
– 3
.5 y
N
RC
Ts: 2
62
CC
Ts: 9
2
RC
Ts: 2
47
CC
Ts: 6
0
RC
Ts: 1
76
RC
Ts: 1
54
RC
Ts: 8
1 C
CT:
22
Type
of
inte
rven
tion
Bio
feed
back
to
the
pare
tic lo
wer
lim
b
Bio
feed
back
to
the
pare
tic u
pper
lim
b
Effe
cts
of F
ES
on
the
low
er li
mb
NM
S o
f the
pa
retic
fore
arm
w
ithou
t EM
G-
trigg
erin
g
NM
S o
f the
pa
retic
fore
arm
w
ith E
MG
-tri
gger
ing
Tabl
e 2
- Con
tinue
d -
Inte
rven
tion
cate
gorie
s
6.B
iofe
edba
ck
ther
apy
7.Fu
nctio
nal
Elec
tric
al
Stim
ulat
ion
and
N
euro
mus
cula
r st
imul
atio
n

Chapter 2
34
Ref
eren
ces
4 R
CTs
: 63
,75,
197,
198
2 C
CTs
: 199
,200
1 R
CT:
59
1 R
CT:
202
2
CC
Ts: 2
01,2
03
2 R
CTs
: 204
,205
2
CC
Ts: 2
06,2
07
1 R
CT:
208
20 R
CTs
: 65
,69,
73,8
0,85
,147
-14
9,20
9-22
0
3 C
CTs
: 221
-223
M.Q
. (P
ED
ro)
rang
e
4 –
7 p.
7 p.
7 p.
4 –
5 p.
7 p.
4 –
8 p.
Res
ults
Stro
ng e
vide
nce
foun
d fo
r in
crea
sing
pas
sive
RO
M (l
ater
al
rota
tion
of p
aret
ic s
houl
der)
and
educ
atio
n of
cau
dal s
ublu
xatio
n in
favo
ur o
f NM
S.
Insu
ffici
ent
evid
ence
foun
d fo
r red
ucin
g he
mip
legi
c sh
ould
er p
ain.
No
evid
ence
foun
d fo
r im
prov
ing
gait
spee
d in
favo
ur o
f app
lyin
g an
AFO
.
No
evid
ence
foun
d fo
r red
ucin
g gl
enoh
umer
al s
ublu
xatio
n or
de
crea
sing
hem
iple
gic
shou
lder
pa
in to
sup
port
the
effe
ctiv
enes
s of
hem
i- sl
ings
or s
trapp
ing
tech
niqu
es.
No
evid
ence
foun
d fo
r de
crea
sing
hem
iple
gic
shou
lder
pa
in o
r im
prov
ing
activ
e R
OM
.
No
evid
ence
foun
d fo
r in
term
itten
t pne
umat
ic
com
pres
sion
for r
educ
ing
hand
vo
lum
e.
Stro
ng e
vide
nce
foun
d fo
r im
prov
ing
com
forta
ble
gait
spee
d, b
asic
AD
L an
d in
stru
men
tal A
DL
in fa
vour
of
augm
ente
d ex
erci
se th
erap
y.
No
evid
ence
foun
d fo
r im
prov
ing
dext
erity
of t
he p
aret
ic a
rm.
Inte
nsity
of
inte
rven
tion
mea
n (r
ange
)
30 m
in/d
ay to
6-7
ho
urs/
day;
re
sp. 4
to 1
x p
/d
durin
g 4
– 8
w
1 da
y– 3
mo
daily
dur
ing
6 –
12 w
15–
30 m
in/d
3
– 5
x p/
w
durin
g 4
w –
3m
o
2 x
2 ho
urs/
d du
ring
4 w
132
– 68
16 m
in
Mea
n tim
e po
st-
stro
ke
()
2 d
– 43
0 d
3 m
o –
3 y
15 d
– 8
mo
15 d
– 8
.2m
o
RC
T: 3
.7 w
7d –
4.7
y
N
RC
Ts: 1
61
CC
Ts: 1
44
RC
T: 6
0
RC
T: 9
8 C
CTs
: 22
RC
Ts: 9
8 C
CTs
: 76
RC
T: 3
7
RC
Ts:2
686
CC
Ts :
813
Type
of
inte
rven
tion
NM
S fo
r gl
enoh
umer
al
subl
uxat
ion
and
hem
iple
gic
shou
lder
pai
n
App
lyin
g A
nkle
-Fo
ot-O
rthos
is
Slin
gs, s
uppo
rtive
de
vice
s an
d st
rap-
ping
tech
niqu
es fo
r re
duci
ng G
HS
and
H
SP
Exe
rcis
es fo
r the
he
mip
legi
c sh
ould
er
Trea
tmen
t of h
and
oede
ma
Inte
nsity
of
exer
cise
ther
apy
Tabl
e 2
- Con
tinue
d -
Inte
rven
tion
cate
gorie
s
8.A
pply
ing
orth
otic
s an
d as
sist
ive
devi
ces
for t
he lo
wer
and
upp
er
extr
emiti
es
9.Tr
eatm
ent o
f he
mip
legi
c sh
ould
er
pain
and
han
d oe
dem
a
10.In
tens
ity o
f ex
erci
se
ther
apy
AD
L in
dica
tes
activ
ities
of d
aily
livi
ng; A
FO, a
nkle
foot
orth
osis
; AR
OM
, act
ive
rang
e of
mot
ion;
BW
STT
, bod
y w
eigh
t sup
porte
d tre
adm
ill tra
inin
g; C
CT,
con
trolle
d cl
inic
al tr
ial;
C
IMT,
con
stra
int-i
nduc
ed m
ovem
ent t
hera
py; d
, day
(s);
EM
G, e
lect
rom
yogr
aphy
; FE
S, f
unct
iona
l ele
ctric
al s
timul
atio
n; G
HS
, gle
nohu
mer
al s
ublu
xatio
n; H
SP
, hem
iple
gic
shou
lder
pai
n;
LOS
, len
gth
of s
tay;
min
, min
ute(
s); m
o, m
onth
(s);
M.Q
., m
etho
dolo
gica
l qua
lity
(poi
nts
on P
ED
ro s
cale
); N
, num
ber o
f pat
ient
s in
volv
ed; N
MS
, neu
ro m
uscu
lar s
timul
atio
n;
PE
Dro
, phy
siot
hera
py e
vide
nce
data
base
; RC
T, ra
ndom
ised
con
trolle
d tri
al; P
RO
M, p
assi
ve ra
nge
of m
otio
n; R
OM
, ran
ge o
f mot
ion;
TE
NS
, tra
nscu
tane
ous
elec
trica
l ner
ve s
timul
atio
n;
w, w
eek(
s); y
, yea
r(s)

Impact of physiotherapy on functional outcome
35
evidence synthesis showed moderate evidence for a reduced LOS in favour of MRP or traditional care compared to an impairment‐focused neuromuscular treatment approach such as Bobath.67,89,90 No evidence was found for applying a specific neurological treatment programs in terms of muscle strength,83,85 synergism,84 muscle tone,88 walking ability,88 dexterity67,81,87 or ADL67,82,83,85‐89.
2. Programs for training sensory‐motor function or influencing muscle tone
‘Sensory motor training’ was defined as exercises for improving motor performance, strength, power, and endurance,10(S72) as well as sensory integrity (proprioception, pallaesthesia, stereognosis and topognosis)10(S90).
Strengthening paretic muscles Six RCTs91‐96 and two CCTs97,98 investigated eccentric98 and concentric strengthening exercises for the lower91‐94,96‐98 and upper limbs92,97. Treatment sessions ranged from 3096 to 9095 min per day, and were applied 291 to 595 times a week for 295 to 693,94 weeks (Table 2). Methodological quality ranged from 491,93 to 794. A meta‐analysis was possible for 3 RCTs91,92,94 that assessed self‐selected comfortable walking speed. A homogeneous nonsignificant SES was found in favour of strengthening muscles of the paretic lower limb on gait speed (Table 3). By weighting the quality of the studies, a best‐evidence synthesis showed strong evidence for the value of increasing the muscle strength of the lower limb in terms of maximal voluntary efforts,92 mass motion (on an Elgin‐table)93 or maximal isokinetic strength (on a Kin‐Com)94. Limited evidence was found for increasing walking endurance91,92 and gait performance (average torque of muscle groups of paretic and nonparetic leg)94,98. No evidence was found for strengthening exercises to improve handgrip force,92,97 to support strengthening muscles for climbing stairs,94 transferring,92 establishing symmetry of weight distribution between hemiplegic and nonhemiplegic sides,98 dexterity92,97 or for physical and mental health94.
Training sensory integrity In one CCT99 the effectiveness of sensory re‐education of arm and hand was investigated of the paretic limb. Training was provided 45 min, three times a week for six weeks (Table 2). Cutaneous stimulation contained tasks such as identificating letters, discriminating objects and localising body parts on the hemiplegic side. While significant effects were reported for somatosensory perception, evaluation of treatment effects for functional outcomes was

Chapter 2
36
lacking. Based on one CCT,99 there were indicative findings that sensory training may improve somatosensory perception. Influencing muscle tone and stiffness In nine RCTs71,84,100‐106 and one CCT107 the effects of different interventions for the treatment of spasticity of the paretic limbs were investigated by applying: an inflatable pressure splint84; reflex inhibiting positioning100,108; spastic muscle stretchings101; inhibitory casts or thermoplastic splints to the upper limbs102,103,107; and transcutaneous electrical nerve stimulation (TENS)71,104‐106 (Table 2). The quality scores of these RCTs ranged from 2103 to 7100. Due to differences in outcomes and treatment modalities, pooling of the studies was only possible for TENS, and showed a significant homogeneous SES for reducing muscle tone according to a (modified) Ashworth scale71,105 (Table 3). In addition, best‐evidence synthesis showed limited evidence for slow stretch techniques in improving active ROM.101 Insufficient evidence was found for TENS71,104 and inhibitory casts or thermoplastic splints102,103,107 in improving passive ROM. No evidence was found that stretching techniques, splinting or TENS improved functional outcome.
3. Cardiovascular fitness and aerobic programs Aerobic capacity and physical endurance were defined as the ability to perform work or participate in activity over time using body’s oxygen uptake, delivery and energy release mechanisms.10(S48) Three RCTs109‐111 and one CCT112 investigated the effects of cardiovascular fitness training after stroke. They studied the use of a home based exercise program110 incorporating a leg cycle ergometer109,111 or muscle strengthening110, in terms of synergism109,110, aerobic capacity109, gait speed110,111, walking endurance110,111 and instrumental ADL110,111. Treatment sessions ranged from 30109 to 90110 min and were applied 3109,110 to 5111 times a week for 8110,111 to 10109 weeks (Table 2). The quality of the RCTs ranged from 4109 to 7110,111. Due to differences in measurements, pooling was only possible for the Fugl‐Meyer (FM) motor scores and gait speed. It showed a statistically significant homogeneous SES for gait speed110,111 and a nonsignificant heterogeneous SES for FM‐motor score109,110 (Table 3). Best‐evidence synthesis demonstrated strong evidence for maximal workload109,111 and walking distance110,111, whereas limited evidence was found for aerobic capacity (VO2, Ve and VCO2)109. No evidence was found for basic110 or instrumental110,111 ADL.

Impact of physiotherapy on functional outcome
37
Five RCTs80,113‐116 investigated the effects of interventions combining muscle strengthening and endurance training. Outcomes were reported for lower limb strength114‐116, synergism of the lower extremity80,114, balance80,114, aerobic capacity114,115, endurance113,114, rising from sitting to standing113, gait speed80,113,114,116, dexterity114 and ADL80. Training sessions ranged from 60113,115 to 90114,116 min per day, and were applied 3113‐116 to 10 times a week for 4113 to 12114,115 weeks (Table 2). Methodological quality ranged from 3113,115,116 to 7114 points. Pooling was possible for muscle strength, synergism, aerobic capacity, walking endurance and gait speed. A homogeneous statistically significant SES was calculated for aerobic capacity114,115 and a heterogeneous statistically significant SES for muscle strength of the lower extremity114‐116. No statistically significant homogeneous SESs were found for synergism in the lower extremity80,114, walking endurance113,114 or gait speed80,113,114,116 (Table 3).
4. Methods for training mobility and mobility related activities Training mobility and mobility‐related activities was divided into three subcategories: balance, gait, and wheelchair propulsion.
Training balance and postural control Fourteen RCTs and one CCT studied the effects of balance training on improving sitting balance (four RCTs86,117‐119), rising from sitting to standing (five RCTs61,113,117,119,120), and standing balance with visual feedback (seven RCTs121‐127 and one CCT128) or perceptual feedback (1 RCT)129. Treatment sessions ranged from 1561 to 120118 min per day, 3123,127 to 15 times a week61 for 286,117,121,129 to 8124,126 weeks (Table 2). The goals of these interventions were to reduce postural sway121‐127,129, to increase the symmetry of weight distribution between paretic and nonparetic sides61,86,113,117‐120,122‐124 and to reduce number of falls120. Outcomes of these studies were evaluated in terms of weight distribution between paretic and nonparetic side, while sitting86,117‐
119 or standing up61,113,117,120, the time to rise from the sitting to standing position61,120 the Timed Up&Go124,126,127, postural sway/symmetry121‐125,129 and gait speed128. The methodological quality ranged from 4121,126 to 7117 points. Pooling was possible for those studies that aimed to improve transfers and standing balance. Statistically significant homogeneous SESs were found for postural symmetry of rising from sitting to standing61,113,117,120, sitting down from standing61,120, and time needed to rise61,120, whereas training standing balance resulted in a significant reduction in postural sway and an increase in the symmetry of weight distribution between paretic and non paretic sides121‐125 (Table 3). A significant heterogeneous SES was found for time

Chapter 2
38
needed to sit in making transfers61,120, whereas the Timed Up&Go test showed a heterogeneous significant negative SES for those patients who had received training for standing balance124,126,127. Moreover no significant effects were found in those studies124,126,127 that measured control of balance by the Berg Balance Scale (Table 3). The best‐evidence synthesis for evaluating effects of training sitting balance showed strong evidence that this intervention improves the ability to reach forward with the arm when in a seated position86,117‐119; limited evidence was observed for reducing the occurrence of falls in programs aimed at improving transfers.
Treadmill training Treadmill training was applied 1) with body weight support and 2) without body weight support. Five RCTs77,130‐133 and two CCTs134,135 investigated the effects of body weighted supported treadmill training (BWSTT) on recovery of balance77,131,134, gait77,130‐134, and walking endurance77,130,133. Amount of body weight support ranged from 0%77 to more than 40%134 and was applied 3132,134 to 5130,131,133 times a week for 2077,132,133 to 45130 min per day for 2134 to 11131 weeks (Table 2). The methodological quality ranged from 4130,133 to 7131 points. Meta‐analysis demonstrated large effect sizes for walking endurance77,130,133, whereas no significant effect sizes were found for postural control as measured by the Berg Balance Scale77,131, walking ability131,133 or gait speed77,130‐133 (Table 3). Five RCTs80,80,136‐139, with methodological quality ranging from 580 to 8139 points, investigated the effects of treadmill training without body weighted support. Treatment sessions lasted from 5 min136 to 1 h137 per day, and were applied 3137‐139 to 580,80 times a week for 380 to 680 weeks (Table 2). The RCTs showed significant homogeneous SES for walking ability136,138, whereas a heterogeneous nonsignificant SES was found for gait speed80,136‐138 (Table 3).
External auditory rhythms (EAR) Three RCTs140‐142 investigated the effects of EAR on tempero‐spatial parameters of gait including stride length, cadence, symmetry of gait and gait speed140‐142. Training sessions ranged from 20142 to 30141 min per day, occurred 2140 to 10141 times a week for 3142 to 12140 weeks (Table 2). The methodological quality varied from 3140,141 to 6142 points on the PEDro scale. Pooling these studies showed a homogeneous significant SES for stride length140,142 and gait speed140‐142 (Table 3).

Impact of physiotherapy on functional outcome
39
Limb loading One RCT143 investigated the effects of exercise training with weighted garments to improve balance and gait (Table 2). Home training with weighted garments was compared to a training program without garments. The study showed no statistically significant effects, and thus, no evidence to support limb loading in terms of balance or gait speed.
Wheelchair propulsion One RCT144 and one CCT145 investigated the effects of self‐propelling a wheelchair on muscle tone144, control in accuracy of wheelchair driving145 and ADL144. Best‐evidence synthesis of the studies showed no evidence that wheelchair propulsion with only the nonhemiplegic hand and foot resulted in better ADL, or that it influenced spasticity (Table 2).
5. Exercises for the upper limb Effectiveness of exercising the paretic arm Eleven RCTs65,69,73,82,83,87,110,146‐149 studied the effects of exercise therapy aimed at improving function of the paretic arm. Exercise training included the use of specific neurological treatment approaches or task‐oriented training programs. Therapy time ranged from 30147 to 90110,149 min per day, 3110 to 565,82,147,149 days a week for 569 to 2065 weeks (Table 2). Outcomes were evaluated in terms of muscle strength73,83,149, synergism110,147, dexterity65,69,73,87,147,149 or ADL65,69,73,82,83,87,110,147‐149. In some studies the specific exercise program was added to a conventional treatment program.65,69,73,147‐149 Methodological quality ranged from 382,83 to 765,110 points. Due to differences in outcomes, study pooling was not possible. Further, best‐evidence synthesis showed insufficient evidence for the use of exercise programs aimed at enhancing dexterity of the paretic arm or improving ADL. No evidence was found for improving muscle strength or synergism from exercise programs for the paretic arm.
Constraint‐ induced movement therapy (CIMT) Six RCTs150‐155 investigated the effects of CIMT on motor performance151,152,155, dexterity of the paretic arm150‐155 and ADL150,155. The nonparetic arm was constrained for 5151,152 to 10153 h per day over a 2150,154,155 to 10151,152 week period. In addition, exercise training was provided for 1151,152 to 6153‐155 h a day for 3 times a week151,152 to every weekday153 (Table 2). Quality of the RCTs ranged from 4153 to 7155 points on the PEDro scale. The meta‐analysis using dexterity measured with the Arm Motor Activity Test (AMAT) or Action Research Arm Test (ARAT) as an outcome showed a

Chapter 2
40
statistically significant SES150‐152,154,155 in support of CIMT. No significant effects were found for the Motor Activity Log that evaluates the amount of use in daily living 154,155 (Table 3). Best‐evidence synthesis showed no differential effects due to CIMT for ADL as measured by Barthel Index150, Rehabilitation Activities Profile (RAP)155 or the Functional Independence Measure150.
Bilateral arm training One RCT156 and one CCT97 investigated the effects of high repetitive bilateral cyclic training of the upper limb. Outcomes were muscle strength and dexterity97,156 (Table 2). Due to relatively poor methodological quality as well as differences in outcomes, pooling was not possible. Best‐evidence synthesis showed indicative findings in favour of bilateral arm training on grip strength97 and dexterity of the paretic arm97.
Mirror Therapy Using subjects with stroke, two RCTs146,157 investigated the effects of mirror therapy on active ROM146, muscle tone157 and dexterity as assessed with the ARAT157. Patients were asked to move the nonparetic arm while looking in a mirror that gave the impression that the paretic limb was moving. Therapy sessions ranged from 15146 to 30157 min per day, 2157 to 6146 times a week for 5157 to 8146 weeks (Table 2). Based on studies of moderate quality (scores of 4146 to 5157 points), a best‐evidence synthesis suggested limited support for improving dexterity through the use of mirror therapy.
6. Biofeedback therapy Biofeedback to the paretic lower limb Twelve RCTs140,158‐168 and four CCTs169‐172 investigated the effects of biofeedback including EMG feedback158‐160,162‐167 and positional feedback140,161. Biofeedback was aimed at improving knee flexion165, knee extension167, ankle dorsiflexion158,159,162,163,166 or ankle plantar flexion140 or reducing hyperextension of the knee168 of the paretic leg during gait. In six RCTs158,159,161,164,165,167,168 biofeedback was applied in adjunct to basic exercises, whereas in five studies the control group received a specific neurological treatment approach159,161,164,166,167, gait training158, placebo biofeedback160 or no treatment at all140. The intensity of biofeedback training ranged from 20163 to 60164 min per day, 2140,161 to 5 times a week163,164,167,168 for 2163 to 12140 weeks (Table 2). The quality of the RCTs ranged from 2165 to 6162‐164,168 points. Pooling of studies was only possible for two outcomes. Homogeneous non

Impact of physiotherapy on functional outcome
41
significant SESs were found for active ROM of the paretic ankle140,158,159,166 and gait speed140,159,161,162,164‐166 (Table 3).
Biofeedback to the paretic upper limb Ten RCTs81,163,173‐180 and three CCTs181‐183 studied the effects of EMG feedback on motor control and dexterity of the paretic upper limb. In 3 of 10 studies EMG feedback was applied as an adjunct to a basic exercise program173,175,177 and compared to a neurological treatment approach81,173,176‐178,181, placebo EMG163,175,180 or no treatment182. In terms of intensity, biofeedback was given for 30179 to 60177,178,181 min per day, 2176,178 to 5 times a week163,179 for between one week179 and six months182 (Table 2). Study quality ranged from 2174 to 7 points175. Due to different aims and outcomes across the studies, pooling of data was not possible. Most of the RCTs showed no statistically significant effects. Best‐evidence synthesis showed no evidence to support the use of biofeedback for improving strength177 or increasing active ROM163,176,177,179, whereas there was insufficient evidence to determine its effect on dexterity of the paretic upper limb173,175.
7. Functional Electrical Stimulation (FES) and Neuromuscular Stimulation (NMS)
Effects of FES on the lower limb Five RCTs162,184‐187 investigated the effects of FES on muscle strength187, synergism184,186, Physiological Cost Index (PCI)185, walking ability186, gait speed162,184,185 and ADL186 in stroke patients. A nonsignificant homogeneous SES was found for studies investigating synergism of the lower limb measured with the Fugl Meyer motor assesment184,186, whereas a non significant heterogeneous SES was observed for gait speed184,185 (Table 3). Based on best‐evidence syntheses, limited evidence was found in support of FES for muscle strengthening187, PCI185 and walking ability186. No evidence was found for ADL as measured with the Barthel Index.
Neuromuscular stimulation of the paretic forearm, with and without EMG triggering Four RCTs188‐191 investigated the effects of NMS without EMG triggering on active ROM of the wrist and dexterity in stroke patients. NMS of the extensors of the wrist and fingers of the paretic forearm was applied 30188 to 90191 min per day during 3189 to 8191 weeks. Outcome was evaluated in terms of muscle strength of the wrist extensors188,191, synergism189, active ROM188, dexterity191 or ADL189,191 (Table 2). Methodological quality ranged from 3188 to 7191. Pooling was not possible due to differences in outcomes and in the

Chapter 2
42
parameters of NMS that were used. Best‐evidence synthesis showed indicative findings in favour of NMS for active ROM188 and limited evidence for muscle strength188,191 and dexterity191. However, the evidence for dexterity was restricted to only those patients with some voluntary control of wrist and finger extension at baseline of the study191. Four RCTs192‐195 and one CCT196 studied the effects of NMS with EMG triggering for improvement of finger and hand‐extension in stroke patients. In two trials only patients with some voluntary wrist extension192 or strength in the forearm extensors193 were included. Stimulation ranged from 30193,194 to 90195 min per day, 2195 to 5193,194,196 times a week for 2192,195 to 12194,196 weeks (Table 2). Outcome was evaluated on the basis of strength of forearm extensors192 and flexors196, synergism192‐194,196, dexterity192,194,195 and ADL193. Methodological quality of the studies ranged from 3192 to 5193‐195 PEDro points. Pooling individual RCTs for synergism showed a non significant homogenous SES193,194 (Table 3). Insufficient evidence was found for EMG‐triggered NMS for muscle strength192,196 and dexterity192,194.
Neuromuscular stimulation for glenohumeral subluxation (GHS) and hemiplegic shoulder pain (HSP) Four RCTs63,75,197,198 and two CCTs199,200 investigated the effects of NMS on the subluxated hemiplegic shoulder. NMS was restricted to the supraspinatus and dorsal deltoid muscles of the paretic shoulder. Treatment sessions ranged from 30 min198,200to 6 hours a day63,75,197, 575,197,200 to 763,198 days a week for 4198 to 663,75,197,200 weeks (Table 2). Study quality ranged from 463,75,197 to 7198 points. Meta‐analysis of the RCTs showed a heterogeneous, statistically significant SES for reduction in caudal subluxation63,75,197,198, and a homogeneous statistically significant SES for the increase in lateral passive ROM63,198 (Table 3). The best‐evidence synthesis showed insufficient evidence for effects of NMS on reducing HSP.
8. Applying orthotics and assistive devices for the lower and upper Extremities
Assistive, supportive and adaptive devices for the lower limb were defined as equipment used to aid patients in ambulation. Assistive and supportive devices included crutches, canes, walkers, electric neuromuscular devices, static and dynamic (knee) ankle‐foot orthosis (AFO), whereas adaptive devices included environmental controls and seating systems.10(S54) Orthotic, assistive and supportive devices for the upper limb included braces, casts,

Impact of physiotherapy on functional outcome
43
slings, splints and supportive taping, neuromuscular stimulation and kinetic and EMG feedback equipment.10(S76)
Applying ankle‐foot orthosis (AFOs) One RCT59 investigated the effects of an AFO on walking ability and gait speed59. Best‐evidence synthesis based on one high‐quality RCT59 showed no evidence for increased gait speed when an AFO was provided after stroke (Table 2).
Slings, supportive devices and strapping for reducing glenohumeral subluxation (GHS) Several techniques, aimed at reducing GHS, and thereby, decreasing hemiplegic shoulder pain, have been studied. One CCT201 investigated the effectiveness of using a hemi‐sling. In addition, one RCT202 and one CCT203 investigated the impact of supportive taping for the hemiplegic shoulder (strapping). The quality of the RCT202 was 7 points (Table 2). Undertaken because of lack of comparability between studies, a best‐evidence synthesis revealed no evidence for reducing a glenohumeral subluxation or decreasing hemiplegic shoulder pain to support the effectiveness of hemi‐slings and strapping techniques.
9. Treatment of hemiplegic shoulder pain and hand oedema Effectiveness of exercises for the hemiplegic shoulder Two RCTs204,205 and two CCTs206,207 studied the effects of an exercise program for a painful hemiplegic shoulder. Comparisons were made with ultrasound204, cryotherapy205, nonsteroid anti‐inflammatory drugs207 or pulley exercises for the paretic shoulder206. The exercise programs were given for 15‐30 min per day, 3204,207 to 5206 times a week for four weeks204,205 to 3 months207 (Table 2)206. The quality of the studies ranged from 4206 to 5204 points205. Best‐evidence synthesis showed no positive effects of exercising the hemiplegic shoulder in terms of decreasing shoulder pain204‐207 or improving active ROM204‐207.
Treatment of hand oedema One RCT208 studied the effects of Intermittent Pneumatic Compression (IPC)208 on oedema of the paretic hand. IPC was offered for 2 h two times per workday for four weeks208. Best‐evidence synthesis showed no evidence for IPC in terms of reduction of oedema of the paretic hand (Table 2).
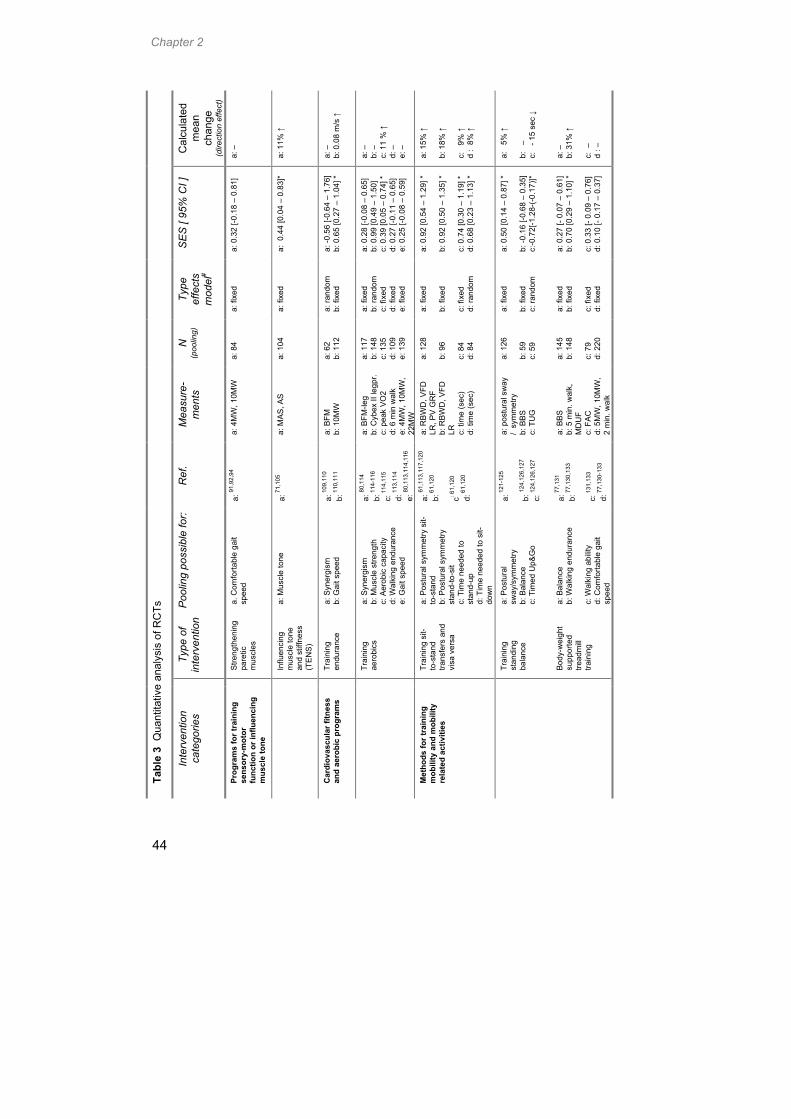
Chapter 2
44
Cal
cula
ted
mea
n ch
ange
(d
irect
ion
effe
ct)
a: –
a: 1
1% ↑
a: –
b:
0.0
8 m
/s ↑
a: –
b:
–
c: 1
1 %
↑
d: –
e:
–
a: 1
5% ↑
b:
18%
↑
c:
9% ↑
d
: 8%
↑
a:
5% ↑
b:
–
c:
- 1
5 se
c ↓
a:
–
b: 3
1% ↑
c:
–
d : –
SE
S [
95%
CI ]
a: 0
.32
[-0.1
8 –
0.81
]
a: 0
.44
[0.0
4 –
0.83
]*
a: -0
.56
[-0.6
4 –
1.76
] b:
0.6
5 [0
.27
– 1.
04] *
a: 0
.28
[-0.0
8 –
0.65
] b:
0.9
9 [0
.49
– 1.
50]
c: 0
.39
[0.0
5 –
0.74
] *
d: 0
.27
[-0.1
1 –
0.65
] e:
0.2
5 [-0
.08
– 0.
59]
a: 0
.92
[0.5
4 –
1.29
] *
b: 0
.92
[0.5
0 –
1.35
] *
c: 0
.74
[0.3
0 –
1.19
] *
d: 0
.68
[0.2
3 –
1.13
] *
a: 0
.50
[0.1
4 –
0.87
] *
b: -0
.16
[-0.6
8 –
0.35
] c:
-0.7
2[-1
.28-
(-0.
17)]*
a: 0
.27
[- 0.
07 –
0.6
1]
b: 0
.70
[0.2
9 –
1.10
] *
c: 0
.33
[- 0.
09 –
0.7
6]
d: 0
.10
[- 0.
17 –
0.3
7]
Type
ef
fect
s m
odel
#
a: fi
xed
a: fi
xed
a: ra
ndom
b:
fixe
d
a: fi
xed
b: ra
ndom
c:
fixe
d d:
fixe
d e:
fixe
d
a: fi
xed
b: fi
xed
c: fi
xed
d: ra
ndom
a: fi
xed
b: fi
xed
c: ra
ndom
a: fi
xed
b: fi
xed
c: fi
xed
d: fi
xed
N
(poo
ling)
a: 8
4
a: 1
04
a: 6
2 b:
112
a: 1
17
b: 1
48
c: 1
35
d: 1
09
e: 1
39
a: 1
28
b: 9
6 c:
84
d: 8
4
a: 1
26
b: 5
9 c:
59
a: 1
45
b: 1
48
c: 7
9 d:
220
Mea
sure
-m
ents
a: 4
MW
, 10M
W
a: M
AS
, AS
a: B
FM
b: 1
0MW
a: B
FM-le
g b:
Cyb
ex II
legp
r. c:
pea
k V
O2
d: 6
min
wal
k e:
4M
W, 1
0MW
, 22
MW
a: R
BW
D, V
FD
LR, P
V G
RF
b: R
BW
D, V
FD
LR
c: ti
me
(sec
) d:
tim
e (s
ec)
a: p
ostu
ral s
way
/
sym
met
ry
b: B
BS
c:
TU
G
a: B
BS
b:
5 m
in. w
alk,
M
DU
F c:
FA
C
d: 5
MW
, 10M
W,
2 m
in. w
alk
Ref
.
a: 91
,92,
94
a: 7
1,10
5
a: 1
09,1
10
b: 1
10,1
11
a: 80
,114
b:
114
-116
c:
114
,115
d:
113
,114
e:
80,1
13,1
14,1
16
a: 61
,113
,117
,120
b:
61,
120
c: 61,
120
d: 6
1,12
0
a: 1
21-1
25
b: 12
4,12
6,12
7 c:
124,
126,
127
a: 7
7,13
1 b:
77,
130,
133
c: 1
31,1
33
d: 7
7,13
0-13
3
Poo
ling
poss
ible
for:
a. C
omfo
rtabl
e ga
it sp
eed
a: M
uscl
e to
ne
a: S
yner
gism
b:
Gai
t spe
ed
a: S
yner
gism
b:
Mus
cle
stre
ngth
c:
Aer
obic
cap
acity
d:
Wal
king
end
uran
ce
e: G
ait s
peed
a: P
ostu
ral s
ymm
etry
sit-
to-s
tand
b:
Pos
tura
l sym
met
ry
stan
d-to
-sit
c:
Tim
e ne
eded
to
stan
d-up
d:
Tim
e ne
eded
to s
it-do
wn
a: P
ostu
ral
sway
/sym
met
ry
b: B
alan
ce
c: T
imed
Up&
Go
a: B
alan
ce
b: W
alki
ng e
ndur
ance
c:
Wal
king
abi
lity
d:
Com
forta
ble
gait
spee
d
Type
of
inte
rven
tion
Stre
ngth
enin
g pa
retic
m
uscl
es
Influ
enci
ng
mus
cle
tone
an
d st
iffne
ss
(TE
NS
)
Trai
ning
en
dura
nce
Trai
ning
ae
robi
cs
Trai
ning
sit-
to-s
tand
tra
nsfe
rs a
nd
visa
ver
sa
Trai
ning
st
andi
ng
bala
nce
Body
-wei
ght
supp
orte
d tre
adm
ill tra
inin
g
Tabl
e 3
Qua
ntita
tive
anal
ysis
of R
CTs
In
terv
entio
n ca
tego
ries
Prog
ram
s fo
r tra
inin
g se
nsor
y-m
otor
fu
nctio
n or
influ
enci
ng
mus
cle
tone
Car
diov
ascu
lar f
itnes
s an
d ae
robi
c pr
ogra
ms
Met
hods
for t
rain
ing
mob
ility
and
mob
ility
re
late
d ac
tiviti
es

Impact of physiotherapy on functional outcome
45
Cal
cula
ted
mea
n ch
ange
(d
irect
ion
effe
ct)
a: 1
7% ↑
b:
–
a: 0
.18
m ↑
b:
0.2
2m/s
↑
a: 1
3.5%
↑
b: –
a: –
b:
–
a: –
b:
–
a: –
a: 5
mm
↑
b: 1
3º la
t.rot
. ↑
SE
S [
95%
CI ]
a: 1
.09
[ 0.5
6 –
1.61
]* b:
0.5
8 [-
0.45
– 1
.62]
a: 0
.68
[0.0
6 –
1.30
] b:
0.9
1 [0
.40
– 1.
42]
a: 0
.46
[0.0
7 –
0.85
] *
b: 0
.23
[- 0.
24 –
0.7
0]
a: 0
.41
[- 0.
10 –
0.9
1]
b: 0
.35
[- 0.
04 –
0.7
3]
a: 0
.01
[- 0.
51 –
0.5
3]
b: 0
.73
[- 0.
93 –
2.4
0]
a: -0
.06
[-0.7
6 –
0.63
]
a: 1
.41
[0.7
6 –
2.06
] *
b: 0
.55
[0.0
5 –
1.04
] *
Type
ef
fect
s m
odel
#
a: fi
xed
b: ra
ndom
a: fi
xed
b: fi
xed
a: fi
xed
b: fi
xed
a: fi
xed
b: fi
xed
a: fi
xed
b: ra
ndom
a: fi
xed
a: ra
ndom
b:
fixe
d
N
(poo
ling)
a: 6
5 b:
102
a: 4
3
b: 6
7
a: 1
04
b: 7
1
a: 6
6 b:
98
a: 5
8 b:
52
a: 4
4
a: 1
61
b: 6
6
Mea
sure
-m
ents
a: F
AC
b:
10M
W
a: g
ait
anal
ysis
b:
10M
W, 3
0 se
c w
alk
a: A
RA
T,
AM
AT
b:
MA
L
a: R
OM
, A
RO
M
b: G
ait
anal
ysis
, 6M
W, 1
5MW
a: B
FM
b: 1
0MW
, 20
MW
a: B
FM
a: X
-ray
s
b: P
RO
M
Ref
.
a: 13
6,13
8 b:
80,1
36-1
38
a: 1
40,1
42
b: 1
40-1
42
a: 1
50-5
2,15
4,15
5 b:
154
,155
a:14
0,15
8,15
9,16
6 b:
140,
159,
161,
162,
164-
166
a: 1
84,1
86
b: 1
84,1
85
a: 1
93,1
94
a: 63
,75,
197,
198
b: 6
3,19
8
Poo
ling
poss
ible
for:
a: W
alki
ng a
bilit
y
b: G
ait s
peed
a: S
tride
leng
th
b: G
ait s
peed
a: D
exte
rity
b: A
mou
nt o
f use
(p
aret
ic a
rm)
a: A
ctiv
e R
OM
b:
Com
forta
ble
gait
spee
d
a: S
yner
gism
b:
Gai
t spe
ed
a: S
yner
gism
a: R
educ
tion
subl
uxat
ion
b:
Pas
sive
RO
M (l
ater
al
rota
tion)
Type
of
inte
rven
tion
Trea
dmill
train
ing
w
ithou
t BW
S
Ext
erna
l au
dito
ry
rhyt
hms
CIM
T
Bio
feed
back
to
the
low
er
limb
FES
for l
ower
lim
b
NM
S w
ith
EM
G-
trigg
erin
g
NM
S fo
r GH
S
and
HS
P
Tabl
e 3
- Con
tinue
d -
Inte
rven
tion
cate
gorie
s
Exer
cise
s fo
r the
upp
er
limb
Bio
feed
back
ther
apy
Func
tiona
l ele
ctric
al
stim
ulat
ion
(FES
) and
N
euro
mus
cula
r st
imul
atio
n (N
MS)

Chapter 2
46
Cal
cula
ted
mea
n ch
ange
(d
irect
ion
effe
ct)
a: 4
.5%
↑
b: 0
.07
m/s
↑
c: –
d:
5%
↑
SE
S [
95%
CI ]
a: 0
.13
[0.0
3 –
0.23
] *
b: 0
.19
[0.0
1 –
0.36
] *
c: 0
.03
[-0.1
3 –
0.19
] d:
0.2
3 [0
.13
– 0.
33] *
Type
ef
fect
s m
odel
#
a: ra
ndom
b:
fixe
d c:
fixe
d d:
fixe
d
N
(poo
ling)
a: 2
686
b:
576
c:
676
d:
157
0
Mea
sure
-m
ents
a: B
I, FI
M
b: 1
0MW
c:
AR
AT
d: N
EA
DL
Ref
.
a:65
,69,
73,8
0,85
,147
-
149,
209-
220
b:65
,80,
210,
214,
215,
218
c:65
,69,
147,
149,
218
d:65
,69,
149,
210,
212,
213,
216,
218,
219
Poo
ling
poss
ible
for:
a: A
DL
b:
Gai
t spe
ed
c: D
exte
rity
d: In
stru
men
tal A
DL
Type
of
inte
rven
tion
Tabl
e 3
- Con
tinue
d -
Inte
rven
tion
cate
gorie
s
Inte
nsity
of e
xerc
ise
ther
apy
* st
atis
tical
sig
nific
ant s
umm
ary
effe
ct s
ize
(SE
S):p
< 0
.05
; #
in c
ase
of a
rand
om e
ffect
s m
odel
, no
sens
itivi
ty a
naly
sis
took
pla
ce
AM
AT
indi
cate
s ar
m m
otor
act
ivity
test
; AR
AT,
act
ion
rese
arch
arm
test
; AR
OM
, act
ive
rang
e of
mot
ion;
AS
, ash
wor
th s
cale
; BB
S, b
erg
bala
nce
scal
e;
BFM
, bru
nnst
rom
fugl
-mey
er a
sses
smen
t; BI
, bar
thel
inde
x; B
WS
, bod
y-w
eigh
t sup
port;
CIM
T, c
onst
rain
t-ind
uced
mov
emen
t the
rapy
; FA
C, f
unct
iona
l am
bula
tion
cate
gorie
s;
FIM
, fun
ctio
nal i
ndep
ende
nce
mea
sure
; GH
S, g
leno
hum
eral
sub
luxa
tion;
HS
P, h
emip
legi
c sh
ould
er p
ain;
MA
L, m
otor
act
ivity
log;
MAS
, mod
ified
ash
wor
th s
cale
; M
DU
F, m
axim
al d
ista
nce
until
fatig
ue; M
W, m
etre
wal
k; N
, num
ber o
f pat
ient
s; N
EA
DL,
not
tingh
am e
xten
ded
AD
L; P
RO
M, p
assi
ve ra
nge
of m
otio
n;
PV
GR
F, p
eak
verti
cal g
roun
d re
actio
n fo
rce
thro
ugh
affe
cted
foot
; RB
WD
, rat
io b
ody
wei
ght d
istri
butio
n; R
CT,
rand
omis
ed c
ontro
lled
trial
; RO
M, r
ange
of m
otio
n;
TUG
, tim
ed u
p&go
-test
; VFD
LR
, ver
tical
forc
e di
ffere
nce
betw
een
left
+ rig
ht

Impact of physiotherapy on functional outcome
47
Med
ian/
M
ean
(ran
ge)
4 / 3
.8
(3 –
6)
4 / 4
.7
(2 –
7)
5 / 5
.3
(3 –
7)
5 / 5
.3
(3 –
8)
5 / 5
.0
(3 –
7)
4 / 4
.2
(2 –
7)
11
PM
an
d M
V
67,8
1,83
-85,
87
71,8
4,91
,
92,9
4,96
,
100,
101,
104-
106
80,1
09-1
11,
113,
115,
116
61,7
7,80
,113
,
117-
124,
126,
127,
131,
133,
136-
139,
142-
144
65,6
9,73
,83,
87,
110,
146,
147,
149,
155
81,1
58,1
59,
161-
164,
166-
168,
173,
175,
176,
179,
180
10
Bet
wee
n gr
oup
com
pa-
rison
s
67,8
1-87
71,8
4,91
-
94,1
00,1
01,
103,
105
80,1
09-1
11,
113-
116
61,7
7,80
,86,
113,
117-
124,
126,
127,
129-
133,
136-
143
65,6
9,73
,82,
83,8
7,
110,
147-
150,
154,
155,
157
81,1
40,1
59-
164,
166-
168,
173-
177,
179,
180
9
Inte
n-tio
n-to
-tre
at
-
100,
102,
106
110,
114
137,
139,
144
110,
151,
152,
155
-
8
Out
com
e >
85%
pa
tient
s
67,8
4,87
84,9
2,94
-
96,1
01,1
05,1
06
110,
111,
114,
115
61,1
17,1
18,
120-
123,
127,
129-
131,
136-
139,
142-
144
65,7
3,87
,110
,
147,
149-
157
158-
160,
163,
164,
173,
175,
176,
178,
179
7
Blin
ding
as
ses-
sors
67,8
1,82
,86
94-9
6,10
0,10
4-
106
80,1
14
77,8
0,86
,117
-
120,
123,
129,
131-
133,
136-
140,
143,
144
65,6
9,73
,82,
146-
148,
150-
155,
157
81,1
40,1
59,
160,
163-
165,
173,
175,
178,
179
6
Blin
ding
th
era-
pi
sts - - - - - -
5
Blin
ding
pa
tient
s
- - - - - -
4
Sim
ilarit
y ba
selin
e
67,8
1,84
-86
71,8
4,91
-
94,9
6,10
0,10
1,10
4
80,1
09-1
11,
113-
115
61,7
7,80
,86,
113,
117-
120,
122-
124,
126,
127,
129-
133,
136-
139,
141-
144
65,6
9,73
,110
,
146-
154,
156,
157
81,1
62-1
64,
167,
168,
173,
175-
177
3 C
once
aled
al
loca
tion
- 92-
94,9
6,10
0,10
2
110,
111,
113,
114
113,
117,
124,
129,
131,
139,
142,
143
65,6
9,11
0,
149,
155
162,
168,
175
2 R
ando
m
allo
ca-
tion
67,8
1-87
71,8
4,91
-
96,1
00-1
06
80,1
09-
111,
113-
116
61,7
7,80
,86,
113,
117-
124,
126,
127,
129-
133,
136-
144
65,6
9,73
,82,
83,8
7,11
0,
146-
157
81,1
40,
158-
168,
173-
180
Item
on
PE
Dro
sca
le
1*
Elig
ibi-
lity
crite
ria
67,8
1-
83,8
6,87
92-9
4,96
,100
-
102,
104-
106
80,1
10,
111,
113-
116
61,7
7,80
,86,
1
13,1
17-
121,
123,
124,
126,
127,
129-
65,6
9,7
3,
82,8
3,8
7,
110,
147
81,1
60-
165,
167,
168,
173-
175,
179
N
8 15
8 29
19
21
Tabl
e 4
Met
hodo
logi
cal q
ualit
y an
alys
is o
f the
RC
Ts b
ased
on
the
PE
Dro
sca
le
Inte
rven
tion
cate
gorie
s
1.
(Tra
ditio
nal)
neur
olog
ical
tr
eatm
ent
appr
oach
es
2.
Prog
ram
s fo
r tr
aini
ng s
enso
ry-
mot
or fu
nctio
n or
in
fluen
cing
mus
cle
tone
3.C
ardi
ovas
cula
r fit
ness
and
aer
obic
pr
ogra
ms
4.M
etho
ds fo
r tr
aini
ng m
obili
ty a
nd
mob
ility
rela
ted
activ
ities
5.Ex
erci
ses
for t
he
up
per l
imb
6.B
iofe
edba
ck
ther
apy
for t
he lo
wer
an
d up
per l
imb

Chapter 2
48
Med
ian/
M
ean
(ran
ge)
5 / 4
.9
(3 –
7)
7 / 7
(7
– 7
)
5 / 5
.6
(5 –
7)
6 / 5
.9
(4 –
8)
-
5 /
5.1
(2 –
8)
11
PM
an
d M
V
63,7
5,16
2,18
4-
191,
193-
195,
197,
198
59,2
02
204,
205,
208
65,6
9,73
,80,
85,
147,
149,
209-
219
111
97
10
Bet
wee
n gr
oup
com
pa-
rison
s
63,7
5,16
2,18
4-
187,
189-
195,
197,
198
59,2
02
204,
205,
208
65,6
9,73
,80,
85,
147-
149,
209-
220
127
109
9
Inte
n-tio
n-to
-tre
at
185,
198
202
-
212,
215-
219
21
19
8
Out
com
e >
85%
pa
tient
s
184,
185,
189-
192,
194,
195,
198
59
208
65,7
3,14
7,14
9,
210,
211,
213-
215,
217-
219
81
74
7
Blin
ding
as
ses-
sors
75,1
86,1
88,1
89,
191,
193,
198
59,2
02
204,
205,
208
65,6
9,73
,80,
147,
148,
210,
212-
216,
218,
219
83
72
6
Blin
ding
th
era-
pi
sts - - - - 0 0
5
Blin
ding
pa
tient
s
- - - - 0 0
4
Sim
ilarit
y ba
selin
e
63,1
62,1
84,1
86,
187,
189,
191,
193,
194,
197,
198
59,2
02
204,
205
,208
65,6
9,73
,80,
85,
147-
149,
209,
210,
212-
217,
219,
220
108
93
3 C
once
aled
al
loca
tion
162,
184,
185,
191,
195
59,2
02
208
65,6
9,14
9,20
9,
211-
216,
219,
220
46
39
2 R
ando
m
allo
ca-
tion
63,7
5,16
2,
184-
195,
197,
198
59,2
02
204,
205,
208
65,6
9,73
,80,
85,1
47-
149,
209-
220
142
123
Item
on
PE
Dro
sca
le
1*
Elig
ibi-
lity
crite
ria
75,1
62,1
84-
187,
189,
191-
194,
197,
198
59,2
02
204,
205,
208
65,6
9,73
,80,
147-
149,
210-
220
116
100
N
17
2 3 20
142
123
Tabl
e 4
- C
ontin
ued
-
Inte
rven
tion
cate
gorie
s
7.Fu
nctio
nal
elec
tric
al a
nd
neur
omus
cula
r st
imul
atio
n
8.A
pply
ing
orth
otic
s an
d as
sist
ive
devi
ces
for t
he lo
wer
and
up
pere
xtre
mity
9.Tr
eatm
ent o
f he
mip
legi
c sh
ould
er p
ain
and
hand
oed
ema
10.In
tens
ity o
f ex
erci
se th
erap
y
TOTA
L (R
CTs
)
TOTA
L w
ithou
t do
uble
s of
RC
Ts
* P
ED
ro-it
em 1
eva
luat
es th
e ex
tern
al v
alid
ity a
nd is
not
incl
uded
in th
e su
msc
ore
of th
e P
edro
. Sum
scor
e of
the
PE
Dro
is b
ased
on
the
item
s 2
- 11.
N
indi
cate
s nu
mbe
r of R
CTs
; PE
Dro
, phy
siot
hera
py e
vide
nce
data
base
; PM
and
MV
, poi
nt m
easu
res
and
mea
sure
s of
var
iabi
lity;
RC
Ts, r
ando
mis
ed c
ontro
lled
trial
s

Impact of physiotherapy on functional outcome
49
10. Intensity of exercise therapy Intensity of exercise therapy was defined as the additional time spent (in minutes) in exercise training when the experimental group was compared to the control group. Twenty RCTs65,69,73,80,85,147‐149,209‐220 and three CCTs221‐223 investigated the effect of augmented exercise therapy on functional outcomes (Table 2). In RCTs, the contrast in therapy time spent between the intervention and control groups ranged from 132215 to 6816 min209. Outcomes were evaluated in terms of comfortable walking speed65,80,210,214,215,218, dexterity65,69,147,149,218, ADL65,69,73,80,85,147‐149,209‐220 and instrumental ADL69,149,210,212,213,216,218,219. The quality of the RCTs ranged from 485,148 to 8215,219. Pooling the RCTs for differences in treatment contrast showed statistical significant SESs for ADL65,69,73,80,85,147‐149,209‐220, comfortable walking speed65,80,210,214,215,218 and instrumental ADL65,69,149,210,212,213,216,218,219. A homogeneous non‐significant SES was found for dexterity65,69,147,149,218 (Table 3).(See ref. 224 for an up‐to‐date review).
The methodological quality for all 123 RCTs is presented in Table 4. The median score of these studies was 5 points (mean 5.1; range 2‐8 points on a scale from 0 – 10 points). Only 39 RCTs mentioned a concealed allocation, whereas just 19 RCTs described an intention‐to‐treat analysis. In none of the studies was blinding possible for patient or therapist, and only 72 of the 123 RCTs had blinded the observer (Table 4).
Discussion
Evidence for physiotherapy interventions The present review showed small but statistically significant SESs supporting the intensity of exercise training. This represented a mean improvement of 5% on ADL. Significant medium‐sized SESs were found for aerobic training, TENS and constraint‐induced movement therapy. Large SESs were found for training sit‐to‐stand transfers, applying neuromuscular stimulation for glenohumeral subluxation, external auditory rhythms during gait and treadmill training with and without body weight support. The small to large effect sizes in high‐quality RCTs represent a mean improvement favouring the experimental group ranging from 5% for intensity of exercise therapy to 31% for BWSTT on walking endurance. The clinical meaning of effects in favour of physiotherapy is difficult to judge. The present findings however, support the use of physiotherapy to improve performance as well as the capacity to perform regular daily activities after

Chapter 2
50
stroke, in particular when studies started early after stroke.224 It should be noted that all the effective studies were characterised by focused exercise programs within which the functional tasks were directly trained. In several studies task‐oriented exercise training was intensified by offering a gait program on a treadmill30, by constraining the nonparetic arm for several hours per day225 or by offering patients a progressive series of different workstations aimed at improving strength and endurance in a functional way114. In contrast, impairment focused programs such as muscle strengthening, muscular re‐education with support of biofeedback21, neuromuscular22 or transcutaneous105 nerve stimulation showed significant improvement in range of motion, muscle power and reduction in muscle tone, however these changes failed to generalise to the activities themselves. Interestingly, a similar trend was found for studies designed to improve cardiovascular fitness by a cycle ergometer.27 Despite significant improvements in workload in the high‐quality RCTs27, general fitness failed to change. Strong evidence was found that neuromuscular stimulation aimed at reducing the amount of glenohumeral subluxation, had no positive impact on hemiplegic shoulder pain.
It was also noted that significant outcomes were most frequently found for those variables measured by continuous parameters defined at interval or ratio levels, such as gait speed77, walking distance110, postural sway and symmetry in weight bearing between hemiplegic and nonhemiplegic side61. Although these findings are perceived as important for functional avtivities226, their real impact on performance of gait‐related activities needs further clarification in future research.
The present review revealed no evidence in terms of functional outcomes to support the use of neurological treatment approaches, compared to usual care regimes. To the contrary, there was moderate evidence that patients receiving conventional functional treatment regimens needed less time to achieve their functional goals88 or had a shorter length of stay compared to those provided with specific neurological treatment approaches, such as Bobath.67,85,89 This discovery is in agreement with the criticism that these traditional approaches are too impairment focused.33,47,49 In addition, several treatment approaches have been criticised for having a weak theoretical framework49,227,228 that is in conflict with recent theories of motor control229,230. For the development of more effective exercise strategies, a better theoretical understanding of the underlying mechanisms of disordered movement co‐ordination in terms of perception and action is needed.49 Moreover, best‐evidence synthesis showed no support for providing orthotics, such as AFOs to the lower limb,59 or for decreasing hand oedema208. Neither was evidence

Impact of physiotherapy on functional outcome
51
found for providing walking aids perhaps due to the lack of controlled studies. Insufficient evidence was found for interventions designed to reduce hemiplegic shoulder pain204,205 or to correct the spastic hand24.
Limitations of this study The present review has a number of shortcomings in terms of the studies investigating the diversity of treatments used in physiotherapy. First, most studies exhibited methodological flaws such as lack of randomisation, or intention‐to‐treat analyses and the use of unblinded observers. A negative trend was found between the unbiased effect sizes of the selected RCTs and the methodological quality based on the PEDro scale (r = ‐0.19; p = 0.08). This finding suggests that bias due to the previously mentioned problems as well as the disregard for systematic dropouts tends to overestimate observed effects. On a more positive note, there was a significant association between year of publication and PEDro score (r = 0.42; p < 0.01) suggesting an increased awareness by researchers to aim for high‐quality studies that will provide an unbiased assessment of the effectiveness of physiotherapy. Another major problem in most RCTs was the small numbers of patients involved, and with that, the low statistical power to reveal statistically significant effects. Due to the diversity of selected outcomes and interventions, pooling of RCTs was limited in the present review. In contrast, there are few RCTs aimed at investigating the effects of physiotherapy interventions on stair climbing, use of walking aids or instructions for fall prevention in the literature. These shortcomings emphasises both the need for more high‐quality RCTs and for a consensus about using the same core set of measures in stroke rehabilitation studies in the future.
Due to lack of comparability of many interventions, and the small number of high‐quality RCTs, a qualitative best‐evidence synthesis was often used in the present study to analyse the results. Although this approach may be criticised as being based on arbitrary criteria, it seems justified when pooling is not appropriate or severely hampered.37
Finally, in the present review only studies written in English, Dutch or German were included. The classification of ‘physiotherapy’ into 10 different intervention categories was an arbitrary choice to deal with the heterogeneity of study objectives in the field.

Chapter 2
52
Clinical messages • There is strong evidence that patients benefit from exercise programs in
which functional tasks are directly and intensively trained. • Impairment‐focused programs such as biofeedback, neuromuscular or
transcutaneous nerve stimulation, cardiovascular fitness training and muscle strengthening, fail to generalise to functional improvements.
• The rational for different treatment approaches is still weak and needs a
better understanding of the ‘nature’ of coordination deficits in functional tasks after stroke.
Acknowledgments and Funding This part is a research project supported by a grant from the Royal Dutch Society of Physical Therapy (KNGF), grant reference number: IKPZ/KNGF/05/2000. We would like to thank M Heldoorn (KNGF), JCF Ket (VU Medical Library) and the physiotherapy members of the working group: BC Harmeling‐van der Wel, BJ Kollen, JSM Hobbelen, JH Buurke, J Halfens, L Wagenborg, MJ Vogel and M Berns.

Impact of physiotherapy on functional outcome
53
Referenties
1. Stroke Unit Trialists Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev 2002; 1: CD000197.
2. Hankey GJ, Warlow CP. Treatment and secondary prevention of stroke: evidence, costs, and effects on individuals and populations. Lancet 1999; 354: 457‐1463.
3. Langhorne P, Duncan P. Does the organization of postacute stroke care really matter? Stroke 2001; 32: 268‐274.
4. Langhorne P, Pollock A. What are the components of effective stroke unit care? Age Ageing 2002; 31: 365‐371.
5. Langhorne P, Legg L, Pollock A et al. Evidence‐based stroke rehabilitation. Age Ageing 2002; 31 (Suppl 3):17‐20.
6. Outpatient Service Trialists. Therapy‐based rehabilitation services for stroke patients at home. Cochrane Database Syst Rev 2003; 1: CD002925.
7. Holm M. Our mandate for the new millennium: evidence based practice. Am J Occup Ther 2000; 54: 575‐585.
8. Parker‐Taillon D. CPA initiatives put the spotlight on evidence‐based practice in physiotherapy. Physiother Can 2002; 24:12‐15.
9. WHO. ICF‐introduction, the International Classification of Functioning Disability and Health. 2002. Assessed 15 January 2004 from http://www.who.int/classification/icf/intros/ICF‐Eng‐Intro.pdf
10. American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. Phys Ther 2001; 81: 9‐746.
11. Sherrington C, Herbert RD, Maher CG, Moseley AM. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther 2000; 5: 223‐226
12. Hedges LV. Fixed effects models. In: Cooper LV, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation, 1994: 285‐300.
13. Kwakkel G, Wagenaar RC, Koelman TW et al. Effects of intensity of rehabilitation after stroke. A research synthesis. Stroke 1997; 28: 1550‐1556.
14. Shadish WR, Haddock CK. Combining estimates of effect size. In: Cooper HM, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation, 1994: 261‐282.
15. DerSimonian R, Laird N. Meta‐analysis in clinical trials. Control Clin Trials 1986; 7: 177‐188.
16. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Earlbaum Associates, 1988.
17. Van Tulder MW, Cherkin DC, Berman B et al. The effectiveness of acupuncture in the management of acute and chronic low back pain. A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 1999; 24: 1113‐1123.

Chapter 2
54
18. Ada L, Foongchomcheay A. Efficacy of electrical stimulation in preventing or reducing subluxation of the shoulder after stroke: a meta‐analysis. Aust J Physiother 2002; 48: 257‐267.
19. De Kroon JR, van der Lee JH, IJzerman MJ et al. Therapeutic electrical stimulation to improve motor control and functional abilities of the upper extremity after stroke: a systematic review. Clin Rehabil 2002; 16: 350‐360.
20. Geurts AC, Visschers BA, van Limbeek J et al. Systematic review of aetiology and treatment of post‐stroke hand oedema and shoulder‐hand syndrome. Scand J Rehabil Med 2000; 32: 4‐10.
21. Glanz M, Klawansky S, Stason W et al. Biofeedback therapy in poststroke rehabilitation: a meta‐analysis of the randomized controlled trials. Arch Phys Med Rehabil 1995; 76: 508‐515.
22. Glanz M, Klawansky S, Stason W et al. Functional electrostimulation in poststroke rehabilitation: a meta‐analysis of the randomized controlled trials. Arch Phys Med Rehabil 1996; 77: 549‐553.
23. Langhorne P, Wagenaar R, Partridge C. Physiotherapy after stroke: more is better? Physiother Res Int 1996; 1: 75‐88.
24. Lannin NA, Herbert RD. Is hand splinting effective for adults following stroke? A systematic review and methodological critique of published research. Clin Rehabil 2003; 17:807‐816.
25. Leung J, Moseley A. Impact of Ankle‐Foot‐Orthoses on gait and leg muscle activity in adults with hemiplegia ‐ systematic literature review. Physiotherapy 2003; 89: 39‐55.
26. Manning CD, Pomeroy VM. Effectiveness of treadmill retraining on gait of hemiparetic stroke patients; systematic review of current literature. Physiotherapy 2003; 89: 337‐349.
27. Meek C, Pollock A, Potter J et al. A systematic review of exercise trials post stroke. Clin Rehabil 2003; 17: 6‐13.
28. Moreland J, Thomson MA. Efficacy of electromyographic biofeedback compared with conventional physical therapy for upper‐extremity function in patients following stroke: a research overview and meta‐analysis. Phys Ther 1994; 74: 534‐543.
29. Moreland JD, Thomson MA, Fuoco AR. Electromyographic biofeedback to improve lower extremity function after stroke: a meta‐analysis. Arch Phys Med Rehabil 1998; 79: 134‐140.
30. Moseley AM, Stark A, Cameron ID, Pollock A. Treadmill training and body weight support for walking after stroke. Cochrane Database Syst Rev 2003; 3: CD002840.
31. Paci M. Physiotherapy based on the Bobath concept for adults with post‐stroke hemiplegia: a review of effectiveness studies. J Rehabil Med 2003; 35: 2‐7.
32. Pollock A, Baer G, Pomeroy V et al. Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke. Cochrane Database Syst Rev 2003; 2: CD001920.
33. Pomeroy VM, Tallis RC. Physical therapy to improve movement performance and functional ability poststroke. Part 1. Existing evidence. Reviews of Clinical Gerontology 2000; 10: 261‐290.

Impact of physiotherapy on functional outcome
55
34. Price CI, Pandyan AD. Electrical stimulation for preventing and treating post‐stroke shoulder pain: a systematic Cochrane review. Clin Rehabil 2001; 15: 5‐19.
35. Schleenbaker RE, Mainous AG, III. Electromyographic biofeedback for neuromuscular reeducation in the hemiplegic stroke patient: a meta‐analysis. Arch Phys Med Rehabil 1993; 74: 1301‐1304.
36. Snels IA, Dekker JH, van der Lee JH et al. Treating patients with hemiplegic shoulder pain. Am J Phys Med Rehabil 2002; 81: 150‐160.
37. Steultjens EM, Dekker J, Bouter LM et al. Occupational therapy for stroke patients: a systematic review. Stroke 2003; 34: 676‐687.
38. Van der Lee JH, Snels IA, Beckerman H et al. Exercise therapy for arm function in stroke patients: a systematic review of randomized controlled trials. Clin Rehabil 2001; 15: 20‐31.
39. Barbeau H. Locomotor training in neurorehabilitation: emerging rehabilitation concepts. Neurorehabilitation and Neural Repair 2003; 17: 3‐11.
40. Burridge JH, Swain ID, Taylor PN. Functional electrical stimulation: a review of the literature published on common peoneal vnerve stimulation for the correction of dropped foot. Reviews of Clinical Gerontology 1998; 8: 155‐161.
41. Carr EK, Kenney FD. Positioning of the stroke patient: a review of the literature. Int J Nurs Stud 1992; 29: 355‐369.
42. Chae J, Yu B. Neuromuscular stimulation for motor relearning in hemiplegia. Critical Reviews in Physical and Rehabilitation Medicine 1999; 11: 279‐297.
43. Cifu DX, Stewart DG. Factors affecting functional outcome after stroke: a critical review of rehabilitation interventions. Arch Phys Med Rehabil 1999; 80(5 Suppl 1): S35‐S39.
44. De Weerdt W, Harrison MA. The efficacy of electromyographic feedback for stroke patients: a critical review of the main literature. Physiotherapy 1986; 72: 108‐118.
45. Dombovy ML, Sandok BA, Basford JR. Rehabilitation for stroke: a review. Stroke 1986; 17: 363‐369.
46. Duncan PW. Synthesis of intervention trials to improve motor recovery following stroke. Topics in Stroke Rehabilitation 1997; 3: 1‐20.
47. Ernst E. A review of stroke rehabilitation and physiotherapy. Stroke 1990; 21(7):1081‐1085.
48. Gowland CA, Basmajian JV. In Clinical Decision Making in Rehabilitation. In: Basmajian JV, Banerjee SN, editors. New York: Churchill Livingstone, 1996: 5‐17.
49. Kwakkel G, Kollen BJ, Wagenaar R. Therapy impact on functional recovery in stroke rehabilitation: a critical review of literature. Physiotherapy 1999; 85: 377‐391.
50. Ottenbacher KJ, Jannell S. The results of clinical trials in stroke rehabilitation research. Arch Neurol 1993; 50: 37‐44.
51. Reding MJ, McDowell FH. Focused stroke rehabilitation programs improve outcome. Arch Neurol 1989; 46: 700‐701.
52. Turner‐Stokes L, Jackson D. Shoulder pain after stroke: a review of the evidence base to inform the development of an integrated care pathway. Clin Rehabil 2002; 16: 276‐298.

Chapter 2
56
53. Van der Lee JH. Constraint‐induced therapy for stroke: more of the same or something completely different? Curr Opin Neurol 2001; 14: 741‐744.
54. Wagenaar RC. Functional recovery after stroke. J Rehabil Sci 1991; 4: 13‐17.
55. Wagenaar RC, Meijer OG. Effects of stroke rehabilitation (2) ‐ a critical review of the literature. J Rehabil Sci 1991; 4: 97‐109.
56. Wagenaar RC, Meijer OG. Effects of stroke rehabilitation (1). J Rehabil Sci 1991; 4: 61‐73.
57. Barreca S, Wolf SL, Fasoli S et al. Treatment interventions for the paretic upper limb of stroke survivors: a critical review. Neurorehabil Neural Repair 2003; 17: 220‐226.
58. Ince LP, Leon MS, Christidis D. EMG biofeedback with upper extremity musculature for relaxation training: a critical review of the literature. J Behav Ther Exp Psychiatry 1985; 16: 133‐137.
59. Beckerman H, Becher J, Lankhorst GJ et al. Walking ability of stroke patients: efficacy of tibial nerve blocking and a polypropylene ankle‐foot orthosis. Arch Phys Med Rehabil 1996; 77(11):1144‐1151.
60. Beckerman H, Becher J, Lankhorst GJ et al. The efficacy of thermocoagulation of the tibial nerve and a polypropylene ankle‐foot‐orthosis on spasticity of the leg in stroke patients: results of a randomized clinical trial. Clin Rehabil 1996; 10: 112‐120.
61. Engardt M, Ribbe T, Olsson E. Vertical ground reaction force feedback to enhance stroke patientsʹ symmetrical body‐weight distribution while rising/sitting down. Scand J Rehabil Med 1993; 25: 41‐48.
62. Engardt M. Long‐term effects of auditory feedback training on relearned symmetrical body weight distribution in stroke patients. A follow‐up study. Scand J Rehabil Med 1994; 26: 65‐69.
63. Faghri PD, Rodgers MM, Glaser RM et al. The effects of functional electrical stimulation on shoulder subluxation, arm function recovery, and shoulder pain in hemiplegic stroke patients. Arch Phys Med Rehabil 1994; 75: 73‐79.
64. Faghri PD, Rodgers MM. The effects of functional neuromuscular stimulation‐augmented physical therapy program in the functional recovery of hemiplegic arm in stroke patients. Clinical Kinesiology: Journal of the American Kinesiotherapy Association 1997; 51: 9‐15.
65. Kwakkel G, Wagenaar RC, Twisk JW et al. Intensity of leg and arm training after primary middle‐cerebral‐artery stroke: a randomised trial. Lancet 1999; 354: 191‐196.
66. Kwakkel G, Kollen BJ, Wagenaar RC. Long term effects of intensity of upper and lower limb training after stroke: a randomised trial. J Neurol Neurosurg Psychiatry 2002; 72: 473‐479.
67. Langhammer B, Stanghelle JK. Bobath or motor relearning programme? A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomized controlled study. Clin Rehabil 2000; 14: 361‐369.
68. Langhammer B, Stanghelle JK. Bobath or motor relearning programme? A follow‐up one and four years post stroke. Clin Rehabil 2003; 17: 731‐734.
69. Lincoln NB, Parry RH, Vass CD. Randomized, controlled trial to evaluate increased intensity of physiotherapy treatment of arm function after stroke. Stroke 1999; 30: 573‐579.

Impact of physiotherapy on functional outcome
57
70. Parry RH, Lincoln NB, Vass CD. Effect of severity of arm impairment on response to additional physiotherapy early after stroke. Clin Rehabil 1999; 13: 187‐198.
71. Sonde L, Gip C, Fernaeus SE et al. Stimulation with low frequency (1.7 Hz) transcutaneous electric nerve stimulation (low‐tens) increases motor function of the post‐stroke paretic arm. Scand J Rehabil Med 1998; 30: 95‐99.
72. Sonde L, Kalimo H, Fernaeus SE et al. Low TENS treatment on post‐stroke paretic arm: a three‐year follow‐up. Clin Rehabil 2000; 14: 14‐19.
73. Sunderland A, Tinson DJ, Bradley EL et al. Enhanced physical therapy improves recovery of arm function after stroke. A randomised controlled trial. J Neurol Neurosurg Psychiatry 1992; 55: 530‐535.
74. Sunderland A, Fletcher D, Bradley L et al. Enhanced physical therapy for arm function after stroke: a one year follow up study. J Neurol Neurosurg Psychiatry 1994; 57: 856‐858.
75. Wang RY, Chan RC, Tsai MW. Functional electrical stimulation on chronic and acute hemiplegic shoulder subluxation. Am J Phys Med Rehabil 2000; 79: 385‐390.
76. Wang RY, Yang YR, Tsai MW et al. Effects of functional electric stimulation on upper limb motor function and shoulder range of motion in hemiplegic patients. Am J Phys Med Rehabil 2002; 81: 283‐290.
77. Visintin M, Barbeau H, Korner‐Bitensky N et al. A new approach to retrain gait in stroke patients through body weight support and treadmill stimulation. Stroke 1998; 29: 1122‐1128.
78. Barbeau H, Visintin M. Optimal outcomes obtained with body‐weight support combined with treadmill training in stroke subjects. Arch Phys Med Rehabil 2003; 84: 1458‐1465.
79. Malouin F, Potvin M, Prevost J et al. Use of an intensive task‐oriented gait training program in a series of patients with acute cerebrovascular accidents. Phys Ther 1992; 72: 781‐789.
80. Richards CL, Malouin F, Wood‐Dauphinee S et al. Task‐specific physical therapy for optimization of gait recovery in acute stroke patients. Arch Phys Med Rehabil 1993; 74: 612‐620.
81. Basmajian JV, Gowland CA, Finlayson MA et al. Stroke treatment: comparison of integrated behavioral‐physical therapy vs traditional physical therapy programs. Arch Phys Med Rehabil 1987; 68: 267‐272.
82. Jongbloed L, Stacey S, Brighton C. Stroke rehabilitation: sensorimotor integrative treatment versus functional treatment. Am J Occup Ther 1989; 43: 391‐397.
83. Logigian MK, Samuels MA, Falconer J et al. Clinical exercise trial for stroke patients. Arch Phys Med Rehabil 1983; 64: 364‐367.
84. Poole JL, Whitney SL, Hangeland N et al. The effectiveness of inflatable pressure splints on motor function in stroke patients. Occupational Therapy Journal of Research 1990; 10: 360‐366.
85. Stern PH, McDowell F, Miller JM et al. Effects of facilitation exercise techniques in stroke rehabilitation. Arch Phys Med Rehabil 1970; 51: 526‐531.

Chapter 2
58
86. Mudie MH, Winzeler‐Mercay U, Radwan S et al. Training symmetry of weight distribution after stroke: a randomized controlled pilot study comparing task‐related reach, Bobath and feedback training approaches. Clin Rehabil 2002; 16: 582‐592.
87. Gelber DA, Josefczyk PB, Herrman D et al. Comparison of two therapy approaches in the rehabilitation of the pure motor hemiparetic stroke patients. J Neuro Rehab 1995; 9: 191‐196.
88. Dickstein R, Hocherman S, Pillar T et al. Stroke rehabilitation. Three exercise therapy approaches. Phys Ther 1986; 66: 1233‐1238.
89. Lord JP, Hall K. Neuromuscular reeducation versus traditional programs for stroke rehabilitation. Arch Phys Med Rehabil 1986; 67: 88‐91.
90. Patel M, Potter J, Perez I et al. The process of rehabilitation and discharge planning in stroke: a controlled comparison between stroke units. Stroke 1998; 29: 2484‐2487.
91. Glasser L. Effects of isokinetic training on the rate of movement during ambulation in hemiparetic patients. Phys Ther 1986; 66: 673‐676.
92. Bourbonnais D, Bilodeau S, Lepage Y et al. Effect of force‐feedback treatments in patients with chronic motor deficits after a stroke. Am J Phys Med Rehabil 2002; 81: 890‐897.
93. Inaba M, Edberg E, Montgomery J et al. Effectiveness of functional training, active exercise, and resistive exercise for patients with hemiplegia. Phys Ther 1973; 53: 28‐35.
94. Kim CM, Eng JJ, MacIntyre DL et al. Effects of isokinetic strength training on walking in persons with stroke: a double‐blind controlled pilot study. Journal of Stroke & Cerebrovascular Diseases 2001; 10: 265‐273.
95. Lindsley HG, Musser L, Steward MR et al. The effects of Kinetron training on gait patterns with strokes. Neurology Report 1994; 19: 29‐34. (Abstract)
96. Moreland JD, Goldsmith CH, Huijbregts MP et al. Progressive resistance strengthening exercises after stroke: a single‐blind randomized controlled trial. Arch Phys Med Rehabil 2003; 84: 1433‐1440.
97. Butefisch C, Hummelsheim H, Denzler P et al. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J Neurol Sci 1995; 130: 59‐68.
98. Engardt M, Knutsson E, Jonsson M et al. Dynamic muscle strength training in stroke patients: effects on knee extension torque, electromyographic activity, and motor function. Arch Phys Med Rehabil 1995; 76: 419‐425.
99. Yekutiel M, Guttman E. A controlled trial of the retraining of the sensory function of the hand in stroke patients. J Neurol Neurosurg Psychiatry 1993; 56: 241‐244.
100. Dean CM, Mackey FH, Katrak P. Examination of shoulder positioning after stroke: A randomised controlled pilot trial. Aust J Physiother 2000; 46: 35‐40.
101. Carey JR. Manual stretch: effect on finger movement control and force control in stroke subjects with spastic extrinsic finger flexor muscles. Arch Phys Med Rehabil 1990; 71: 888‐894.
102. Langlois S, Pederson L, MacKinnon JR. The effects of splinting on the spastic hemiplegic hand: report of a feasible study. Can J Occup Ther 1991; 58: 17‐25.

Impact of physiotherapy on functional outcome
59
103. Rose V, Shah S. A comparitive study on the immediate effects of hand orthosis on reduction of hypertonus. Aust Occup Ther J 1980; 34: 59‐64.
104. Leandri M, Parodi CI, Corrieri N et al. Comparison of TENS treatments in hemiplegic shoulder pain. Scand J Rehabil Med 1990; 22: 69‐71.
105. Tekeoglu Y, Adak B, Goksoy T. Effect of transcutaneous electrical nerve stimulation (TENS) on Barthel Activities of Daily Living (ADL) index score following stroke. Clin Rehabil 1998; 12: 277‐280.
106. Conforto AB, Kaelin‐Lang A, Cohen LG. Increase in hand muscle strength of stroke patients after somatosensory stimulation. Ann Neurol 2002; 51: 122‐125.
107. McPherson JJ, Becker AH, Franszczak N. Dynamic splint to reduce the passive component of hypertonicity. Arch Phys Med Rehabil 1985; 66: 249‐252.
108. Dickstein R, Pillar T. Evaluating the effects of reflex‐inhibiting patterns among hemiplegic patients using EMG biofeedback. Physiother Can 1983; 35: 141‐143.
109. Potempa K, Braun LT, Tinknell T et al. Benefits of aerobic exercise after stroke. Sports Med 1996; 21: 337‐346.
110. Duncan P, Richards L, Wallace D et al. A randomized, controlled pilot study of a home‐based exercise program for individuals with mild and moderate stroke. Stroke 1998; 29: 2055‐2060.
111. Katz‐Leurer M, Shochina M, Carmeli E et al. The influence of early aerobic training on the functional capacity in patients with cerebrovascular accident at the subacute stage. Arch Phys Med Rehabil 2003; 84: 1609‐1614.
112. Kelly JO, Davis GM, Kilbreath SL et al. Exercise training improves walking endurance in chronic stroke patients: a pilot study. Research conference ‐ From cell to society 2002; (Abstract)
113. Dean CM, Richards CL, Malouin F. Task‐related circuit training improves performance of locomotor tasks in chronic stroke: a randomized, controlled pilot trial. Arch Phys Med Rehabil 2000; 81: 409‐417.
114. Duncan P, Studenski S, Richards L et al. Randomized clinical trial of therapeutic exercise in subacute stroke. Stroke 2003; 34: 2173‐2180.
115. Rimmer JH, Riley B, Creviston T et al. Exercise training in a predominantly African‐American group of stroke survivors. Med Sci Sports Exerc 2000; 32: 1990‐1996.
116. Teixeira‐Salmela LF, Olney SJ, Nadeau S et al. Muscle strengthening and physical conditioning to reduce impairment and disability in chronic stroke survivors. Arch Phys Med Rehabil 1999; 80: 1211‐1218.
117. Dean CM, Shepherd RB. Task‐related training improves performance of seated reaching tasks after stroke. A randomized controlled trial. Stroke 1997; 28: 722‐728.
118. De Seze M, Wiart L, Bon‐Saint‐Come A et al. Rehabilitation of postural disturbances of hemiplegic patients by using trunk control retraining during exploratory exercises. Arch Phys Med Rehabil 2001; 82: 793‐800.
119. Pollock AS, Durward BR, Rowe PJ et al. The effect of independent practice of motor tasks by stroke patients: a pilot randomized controlled trial. Clin Rehabil 2002; 16: 473‐480.

Chapter 2
60
120. Cheng PT, Wu SH, Liaw MY et al. Symmetrical body‐weight distribution training in stroke patients and its effect on fall prevention. Arch Phys Med Rehabil 2001; 82: 1650‐1654.
121. Shumway‐Cook A, Anson D, Haller S. Postural sway biofeedback: its effect on reestablishing stance stability in hemiplegic patients. Arch Phys Med Rehabil 1988; 69: 395‐400.
122. Wong AM, Lee MY, Kuo JK et al. The development and clinical evaluation of a standing biofeedback trainer. J Rehabil Res Dev 1997; 34: 322‐327.
123. Sackley CM, Lincoln NB. Single blind randomized controlled trial of visual feedback after stroke: effects on stance symmetry and function. Disabil Rehabil 1997; 19: 536‐546.
124. Grant T, Brouwer BJ, Culham EG et al. Balance retraining following acute stroke: a comparison of two methods. Canadian Journal of Rehabilitation 1997; 11: 69‐73.
125. Lin JJ, Chung KC. Evaluate a biofeedback training on the dynamic and static balance for preambulation in hemiplegic patients. Chinese Journal of Medical and Biological Engineering 1998; 18: 59‐65.
126. Walker C, Brouwer BJ, Culham EG. Use of visual feedback in retraining balance following acute stroke. Phys Ther 2000; 80: 886‐895.
127. Geiger RA, Allen JB, OʹKeefe J et al. Balance and mobility following stroke: effects of physical therapy interventions with and without biofeedback/forceplate training. Phys Ther 2001; 81: 995‐1005.
128. Winstein CJ, Gardner ER, McNeal DR et al. Standing balance training: effect on balance and locomotion in hemiparetic adults. Arch Phys Med Rehabil 1989; 70: 755‐762.
129. Morioka S, Yagi F. Effects of perceptual learning exercises on standing balance using a hardness discrimination task in hemiplegic patients following stroke: a randomized controlled pilot trial. Clin Rehabil 2003; 17: 600‐607.
130. Kosak MC, Reding MJ. Comparison of partial body weight‐supported treadmill gait training versus aggressive bracing assisted walking post stroke. Neurorehabil Neural Repair 2000; 14: 13‐19.
131. Nilsson L, Carlsson J, Danielsson A et al. Walking training of patients with hemiparesis at an early stage after stroke: a comparison of walking training on a treadmill with body weight support and walking training on the ground. Clin Rehabil 2001; 15: 515‐527.
132. Sullivan KJ, Knowlton BJ, Dobkin BH. Step training with body weight support: Effect of treadmill speed and practice paradigms on poststroke locomotor recovery. Arch Phys Med Rehabil 2002; 83: 683‐691.
133. Da Cunha IT Jr, Lim PA, Qureshy H et al. Gait outcomes after acute stroke rehabilitation with supported treadmill ambulation training: a randomized controlled pilot study. Arch Phys Med Rehabil 2002; 83: 1258‐1265.
134. Trueblood PR. Partial body weight treadmill training in persons with chronic stroke. NeuroRehabilitation 2001; 16: 141‐153.
135. Scheidtmann K, Brunner H, Muller F et al. ʹSequenzeffekte in der laufbandtherapieʹ. Neurologie und Rehabilitation 1999; 5: 198‐202.

Impact of physiotherapy on functional outcome
61
136. Laufer Y, Dickstein R, Chefez Y et al. The effect of treadmill training on the ambulation of stroke survivors in the early stages of rehabilitation: a randomized study. J Rehabil Res Dev 2001; 38: 69‐78.
137. Liston R, Mickelborough J, Harris B et al. Conventional physiotherapy and treadmill re‐training for higher‐level gait disorders in cerebrovascular disease. Age Ageing 2000; 29: 311‐318.
138. Pohl M, Mehrholz J, Ritschel C et al. Speed‐dependent treadmill training in ambulatory hemiparetic stroke patients: a randomized controlled trial. Stroke 2002; 33: 553‐558.
139. Ada L, Dean CM, Hall JM et al. A treadmill and overground walking program improves walking in persons residing in the community after stroke: a placebo‐controlled, randomized trial. Arch Phys Med Rehabil 2003; 84: 1486‐1491.
140. Mandel AR, Nymark JR, Balmer SJ et al. Electromyographic versus rhythmic positional biofeedback in computerized gait retraining with stroke patients. Arch Phys Med Rehabil 1990; 71: 649‐654.
141. Thaut MH, McIntosh GC, Rice RR. Rhythmic facilitation of gait training in hemiparetic stroke rehabilitation. J Neurol Sci 1997; 151: 207‐212.
142. Schauer M, Mauritz KH. Musical motor feedback (MMF) in walking hemiparetic stroke patients: randomized trials of gait improvement. Clin Rehabil 2003; 17: 713‐722.
143. Pomeroy VM, Evans B, Falconer M et al. An exploration of the effects of weighted garments on balance and gait of stroke patients with residual disability. Clin Rehabil 2001; 15: 390‐397.
144. Barrett JA, Watkins C, Plant R et al. The COSTAR wheelchair study: a two‐centre pilot study of self‐propulsion in a wheelchair in early stroke rehabilitation. Collaborative Stroke Audit and Research. Clin Rehabil 2001; 15: 32‐41.
145. Kirby RL, Ethans KD, Duggan RE et al. Wheelchair propulsion: descriptive comparison of hemiplegic and two‐hand patterns during selected activities. Am J Phys Med Rehabil 1999; 78: 131‐135.
146. Altschuler EL, Wisdom SB, Stone L et al. Rehabilitation of hemiparesis after stroke with a mirror. Lancet 1999; 353: 2035‐2036.
147. Feys HM, De Weerdt WJ, Selz BE et al. Effect of a therapeutic intervention for the hemiplegic upper limb in the acute phase after stroke: a single‐blind, randomized, controlled multicenter trial. Stroke 1998; 29: 785‐792.
148. Werner RA, Kessler S. Effectiveness of an intensive outpatient rehabilitation program for postacute stroke patients. Am J Phys Med Rehabil 1996; 75: 114‐120.
149. Rodgers H, Mackintosh J, Price C et al. Does an early increased‐intensity interdisciplinary upper limb therapy programme following acute stroke improve outcome? Clin Rehabil 2003; 17: 579‐589.
150. Dromerick AW, Edwards DF, Hahn M. Does the application of constraint‐induced movement therapy during acute rehabilitation reduce arm impairment after ischemic stroke? Stroke 2000; 31: 2984‐2988.
151. Page SJ, Sisto SA, Levine P et al. Modified constraint induced therapy: a randomized feasibility and efficacy study. J Rehabil Res Dev 2001; 38: 583‐590.

Chapter 2
62
152. Page SJ, Sisto S, Johnston MV et al. Modified constraint‐induced therapy after subacute stroke: a preliminary study. Neurorehabil Neural Repair 2002; 16: 290‐295.
153. Sterr A, Elbert T, Berthold I et al. Longer versus shorter daily constraint‐induced movement therapy of chronic hemiparesis: an exploratory study. Arch Phys Med Rehabil 2002; 83: 1374‐1377.
154. Taub E, Miller NE, Novack TA et al. Technique to improve chronic motor deficit after stroke. Arch Phys Med Rehabil 1993; 74: 347‐354.
155. Van der Lee JH, Wagenaar RC, Lankhorst GJ et al. Forced use of the upper extremity in chronic stroke patients: results from a single‐blind randomized clinical trial. Stroke 1999; 30: 2369‐2375.
156. Luft AR, McCombe Waller S, Whitall J et al. Repetitive bilateral arm training in long‐term stroke survivors induces cortical reorganisation. Stroke 2002; 33: 416‐417. (Abstract)
157. Rothgangel AS, Morton A, Van de Hout JWE, Beurskens AJHM. Phantoms in the brain: spiegeltherapie bij chronische CVA‐patiënten; een pilot‐study. Ned Tijdschr v Fysioth 2004; 114: 36‐40.
158. Basmajian JV, Kukulka CG, Narayan MG et al. Biofeedback treatment of foot‐drop after stroke compared with standard rehabilitation technique: effects on voluntary control and strength. Arch Phys Med Rehabil 1975; 56: 231‐236.
159. Binder SA, Moll CB, Wolf SL. Evaluation of electromyographic biofeedback as an adjunct to therapeutic exercise in treating the lower extremities of hemiplegic patients. Phys Ther 1981; 61: 886‐893.
160. Bradley L, Hart BB, Mandana S et al. Electromyographic biofeedback for gait training after stroke. Clin Rehabil 1998; 12: 11‐22.
161. Colborne GR, Olney SJ, Griffin MP. Feedback of ankle joint angle and soleus electromyography in the rehabilitation of hemiplegic gait. Arch Phys Med Rehabil 1993; 74: 1100‐1106.
162. Cozean CD, Pease WS, Hubbell SL. Biofeedback and functional electric stimulation in stroke rehabilitation. Arch Phys Med Rehabil 1988; 69: 401‐405.
163. Hurd WW, Pegram V, Nepomuceno C. Comparison of actual and simulated EMG biofeedback in the treatment of hemiplegic patients. Am J Phys Med 1980; 59: 73‐82.
164. Intiso D, Santilli V, Grasso MG et al. Rehabilitation of walking with electromyographic biofeedback in foot‐drop after stroke. Stroke 1994; 25: 1189‐1192.
165. John J. Failure of electrical myofeedback to augment the effects of physiotherapy in stroke. Int J Rehabil Res 1986; 9: 35‐45.
166. Mulder T, Hulstijn W, van der Meer J. EMG feedback and the restoration of motor control. A controlled group study of 12 hemiparetic patients. Am J Phys Med 1986; 65: 173‐188.
167. Winchester P, Montgomery J, Bowman B et al. Effects of feedback stimulation training and cyclical electrical stimulation on knee extension in hemiparetic patients. Phys Ther 1983; 63: 1096‐1103.
168. Morris ME, Matyas TA, Bach TM et al. Electrogoniometric feedback: its effect on genu recurvatum in stroke. Arch Phys Med Rehabil 1992; 73: 1147‐1154.

Impact of physiotherapy on functional outcome
63
169. Burnside IG, Tobias HS, Bursill D. Electromyographic feedback in the remobilization of stroke patients: a controlled trial. Arch Phys Med Rehabil 1982; 63: 217‐222.
170. Dursun E, Hamamci N, Donmez S et al. Angular biofeedback device for sitting balance of stroke patients. Stroke 1996; 27: 1354‐1357.
171. Montoya R, Dupui P, Pages B et al. Step‐length biofeedback device for walk rehabilitation. Med Biol Eng Comput 1994; 32: 416‐420.
172. Wolf SL, Binder‐MacLeod SA. Electromyographic biofeedback applications to the hemiplegic patient. Changes in lower extremity neuromuscular and functional status. Phys Ther 1983; 63: 1404‐1413.
173. Basmajian JV, Gowland C, Brandstater ME et al. EMG feedback treatment of upper limb in hemiplegic stroke patients: a pilot study. Arch Phys Med Rehabil 1982; 63: 613‐616.
174. Bate PJ, Matyas TA. Negative transfer of training following brief practice of elbow tracking movements with electromyographic feedback from spastic antagonists. Arch Phys Med Rehabil 1992; 73: 1050‐1058.
175. Crow JL, Lincoln NB, Nouri FM et al. The effectiveness of EMG biofeedback in the treatment of arm function after stroke. Int Disabil Stud 1989; 11: 155‐160.
176. Greenberg S, Fowler RS, Jr. Kinesthetic biofeedback: a treatment modality for elbow range of motion in hemiplegia. Am J Occup Ther 1980; 34: 738‐743.
177. Inglis J, Donald MW, Monga TN et al. Electromyographic biofeedback and physical therapy of the hemiplegic upper limb. Arch Phys Med Rehabil 1984; 65: 755‐759.
178. Smith KN. Biofeedback in strokes. Aust J Physiother 1979; 25: 155‐161.
179. Williams JM. Use of electromyographic biofeedback for pain reduction in the spastic hemiplegic shoulder: a pilot study. Physiotherapy Canada 1982; 34: 327‐333.
180. Lee KH, Hill E, Johnston R et al. Myofeedback for muscle retraining in hemiplegic patients. Arch Phys Med Rehabil 1976; 57: 588‐591.
181. Prevo AJ, Visser SL, Vogelaar TW. Effect of EMG feedback on paretic muscles and abnormal co‐contraction in the hemiplegic arm, compared with conventional physical therapy. Scand J Rehabil Med 1982; 14: 121‐131.
182. Wolf SL, Binder‐MacLeod SA. Electromyographic biofeedback applications to the hemiplegic patient. Changes in upper extremity neuromuscular and functional status. Phys Ther 1983; 63: 1393‐1403.
183. Skelly AM, Kenedi RM. EMG biofeedback therapy in the re‐education of the hemiplegic shoulder in patients with sensory loss. Physiotherapy 1982; 68: 34‐38.
184. Bogataj U, Gros N, Kljajic M et al. The rehabilitation of gait in patients with hemiplegia: a comparison between conventional therapy and multichannel functional electrical stimulation therapy. Phys Ther 1995; 75: 490‐502.
185. Burridge JH, Taylor PN, Hagan SA et al. The effects of common peroneal stimulation on the effort and speed of walking: a randomized controlled trial with chronic hemiplegic patients. Clin Rehabil 1997; 11: 201‐210.

Chapter 2
64
186. Macdonell RAL, Triggs WJ, Leikauskas J et al. Functional electrical stimulation to the affected lower limb and recovery after cerebral infarction. Journal of Stroke & Cerebrovascular Diseases 1994; 4: 155‐160.
187. Merletti R, Zelaschi F, Latella D et al. A control study of muscle force recovery in hemiparetic patients during treatment with functional electrical stimulation. Scand J Rehabil Med 1978; 10: 147‐154.
188. Bowman BR, Baker LL, Waters RL. Positional feedback and electrical stimulation: an automated treatment for the hemiplegic wrist. Arch Phys Med Rehabil 1979; 60: 497‐502.
189. Chae J, Bethoux F, Bohine T et al. Neuromuscular stimulation for upper extremity motor and functional recovery in acute hemiplegia. Stroke 1998; 29: 975‐979.
190. Packman‐Braun R. Relationship between functional electrical stimulation duty cycle and fatigue in wrist extensor muscles of patients with hemiparesis. Phys Ther 1988; 68: 51‐56.
191. Powell J, Pandyan AD, Granat M et al. Electrical stimulation of wrist extensors in poststroke hemiplegia. Stroke 1999; 30: 1384‐1389.
192. Cauraugh J, Light K, Kim S et al. Chronic motor dysfunction after stroke: recovering wrist and finger extension by electromyography‐triggered neuromuscular stimulation. Stroke 2000; 31: 1360‐1364.
193. Francisco G, Chae J, Chawla H et al. Electromyogram‐triggered neuromuscular stimulation for improving the arm function of acute stroke survivors: a randomized pilot study. Arch Phys Med Rehabil 1998; 79: 570‐575.
194. Hemmen B, Seelen H, Moennekens M et al. Effect van EMG‐triggered feedback op arm‐handfunctie bij CVA‐patiënten. Revalidatie na een beroerte‐Congres Zwolle 2002; (Abstract)
195. Cauraugh JH, Kim SB. Stroke motor recovery: active neuromuscular stimulation and repetitive practice schedules. J Neurol Neurosurg Psychiatry 2003; 74: 1562‐1566.
196. Kraft GH, Fitts SS, Hammond MC. Techniques to improve function of the arm and hand in chronic hemiplegia. Arch Phys Med Rehabil 1992; 73(3):220‐227.
197. Baker LL, Parker K. Neuromuscular electrical stimulation of the muscles surrounding the shoulder. Phys Ther 1986; 66(12):1930‐1937.
198. Linn SL, Granat MH, Lees KR. Prevention of shoulder subluxation after stroke with electrical stimulation. Stroke 1999; 30: 963‐968.
199. Chantraine A, Baribeault A, Uebelhart D et al. Shoulder pain and dysfunction in hemiplegia: effects of functional electrical stimulation. Arch Phys Med Rehabil 1999; 80: 328‐331.
200. Kobayashi H, Onishi H, Ihashi K et al. Reduction in subluxation and improved muscle function of the hemiplegic shoulder joint after therapeutic electrical stimulation. J Electromyogr Kinesiol 1999; 9: 327‐336.
201. Hurd MM, Farrell KH, Waylonis GW. Shoulder sling for hemiplegia: friend or foe? Arch Phys Med Rehabil 1974; 55: 519‐522.
202. Hanger HC, Whitewood P, Brown G et al. A randomized controlled trial of strapping to prevent post‐stroke shoulder pain. Clin Rehabil 2000; 14: 370‐380.

Impact of physiotherapy on functional outcome
65
203. Ancliffe J. Strapping the shoulder in patients following a cerebrovascular accident (CVA): a pilot study. Aust J Physiother 1992; 38: 37‐41.
204. Inaba MK, Piorkowski M. Ultrasound in treatment of painful shoulders in patients with hemiplegia. Phys Ther 1972; 52: 737‐742.
205. Partridge CJ, Edwards SM, Mee R et al. Hemiplegic shoulder pain: a study of two methods of physiotherapy treatment. Clin Rehabil 1990; 4: 43‐49.
206. Kumar R, Metter EJ, Mehta AJ et al. Shoulder pain in hemiplegia. The role of exercise. Am J Phys Med Rehabil 1990; 69: 205‐208.
207. Poduri KR. Shoulder pain in stroke patients and its effects on rehabilitation. J Stroke Cerebrovasc Dis 1993; 3: 261‐266.
208. Roper TA, Redford S, Tallis RC. Intermittent compression for the treatment of the oedematous hand in hemiplegic stroke: a randomized controlled trial. Age Ageing 1999; 28: 9‐13.
209. Smith DS, Goldenberg E, Ashburn A et al. Remedial therapy after stroke: a randomised controlled trial. Br Med J (Clin Res Ed) 1981; 282: 517‐520.
210. Wade DT, Collen FM, Robb GF et al. Physiotherapy intervention late after stroke and mobility. BMJ 1992; 304: 609‐613.
211. Sivenius J, Pyorala K, Heinonen OP et al. The significance of intensity of rehabilitation of stroke‐‐a controlled trial. Stroke 1985; 16: 928‐931.
212. Logan PA, Ahern J, Gladman JR et al. A randomized controlled trial of enhanced Social Service occupational therapy for stroke patients. Clin Rehabil 1997; 11: 107‐113.
213. Walker MF, Gladman JR, Lincoln NB et al. Occupational therapy for stroke patients not admitted to hospital: a randomised controlled trial. Lancet 1999; 354: 278‐280.
214. Partridge C, Mackenzie M, Edwards S et al. Is dosage of physiotherapy a critical factor in deciding patterns of recovery from stroke: a pragmatic randomized controlled trial. Physiother Res Int 2000; 5: 230‐240.
215. Green J, Forster A, Bogle S et al. Physiotherapy for patients with mobility problems more than 1 year after stroke: a randomised controlled trial. Lancet 2002; 359: 199‐203.
216. Parker CJ, Gladman JR, Drummond AE et al. A multicentre randomized controlled trial of leisure therapy and conventional occupational therapy after stroke. TOTAL Study Group. Trial of Occupational Therapy and Leisure. Clin Rehabil 2001; 15: 42‐52.
217. Slade A, Tennant A, Chamberlain MA. A randomised controlled trial to determine the effect of intensity of therapy upon length of stay in a neurological rehabilitation setting. J Rehabil Med 2002; 34: 260‐266.
218. The Glasgow Augmented Physiotherapy Stroke Group. Can augmented physiotherapy input enhance recovery of mobility after stroke? A randomized controlled trial. Clin Rehabil 2004; 18: 529‐537.
219. Gilbertson L, Langhorne P, Walker A et al. Domiciliary occupational therapy for patients with stroke discharged from hospital: randomised controlled trial. BMJ 2000; 320: 603‐606.
220. Fang Y, Chen X, Li H et al. A study on additional early physiotherapy after stroke and factors affecting functional recovery. Clin Rehabil 2003; 17: 608‐617.

Chapter 2
66
221. Keith RA, Wilson DB, Gutierrez P. Acute and subacute rehabilitation for stroke: a comparison. Arch Phys Med Rehabil 1995; 76: 495‐500.
222. Rapoport J, Judd‐Van Eerd M. Impact of physical therapy weekend coverage on length of stay in an acute care community hospital. Phys Ther 1989; 69: 32‐37.
223. Ruff RM, Yarnell S, Marinos JM. Are stroke patients discharged sooner if in‐patient rehabilitation services are provided seven v six days per week? Am J Phys Med Rehabil 1999; 78(2):143‐146.
224. Kwakkel G, Van Peppen RPS, Wagenaar RC et al. Effects of augmented exercise time after stroke: A meta‐analysis. Stroke 2004; 35: 2529‐2536
225. Van der Lee JH, Kwakkel G, Lankhorst GJ et al: ‘Woldag H, Hummelsheim H: evidence‐based physiotherapeutic concepts for improving arm and hand function in stroke patients: a review J Neurol (2002) 249:518‐528. J Neurol 2003; 250: 119.
226. Salbach NM, Mayo NE, Higgins J et al. Responsiveness and predictability of gait speed and other disability measures in acute stroke. Arch Phys Med Rehabil 2001; 82: 1204‐1212.
227. Lennon S. The Bobath concept: a critical review of the theoretical assumptions that guide physiotherapy practice in stroke rehabilitation. Phys Ther Review 1996; 1: 35‐45.
228. Wagenaar RC, Meijer OG, van Wieringen PC et al. The functional recovery of stroke: a comparison between neuro‐developmental treatment and the Brunnstrom method. Scand J Rehabil Med 1990; 22: 1‐8.
229. Latash ML, Anson JG. What are ʹnormal movementsʹ in atypical populations? Behavioral and Brain Science 1996; 19: 55‐106.
230. Kwakkel G, Wagenaar RC. Effect of duration of upper‐ and lower‐extremity rehabilitation sessions and walking speed on recovery of interlimb coordination in hemiplegic gait. Phys Ther 2002; 82: 432‐448.

CHAPTER
Effects of augmented exercise therapy time after stroke: A meta‐analysis
Gert Kwakkel
Roland PS Van Peppen
Robert C Wagenaar
Sharon Wood‐Dauphinee
Carol Richards
Ann Ashburn
Kimberly Miller
Nadina B Lincoln
Cecily Partridge
Ian Wellwood
Peter Langhorne
Stroke 2004; 35(11): 2529‐2536

Chapter 3
68
Abstract Background: To present a systematic review of studies that addresses the effects of intensity of augmented exercise therapy time (AETT) on activities of daily living (ADL), walking and dexterity in patients with stroke. Summary of review: A database of articles published from 1966 to May 2003 was compiled from MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, PEDro, DARE and PiCarta using combinations of the relevant keywords. References presented in relevant publications were examined as well as abstracts in proceedings. Studies that satisfied the following selection criteria were included: 1) patients had a diagnosis of stroke; 2) effects of intensity of exercise training were investigated; and 3) design of the study was a randomised controlled trial (RCT). For each outcome measure the estimated effect size (ES) and the summary effect size (SES) expressed in standard deviation units (SDU) were calculated for ADL, walking speed and dexterity, using fixed and random effect models. Correlation coefficients were calculated between, observed individual effect sizes on ADL of each study, additional time spent on exercise training and methodological quality. Cumulative meta‐analyses (random effects model) adjusted for the difference in treatment intensity in each study was used for the trials evaluating the effects of AETT provided. Twenty of the 31 candidate studies, involving 2686 stroke patients, were included in the synthesis. The methodological quality ranged from 2 to 11 out of the maximum score of 14 points. The meta‐analysis resulted in a small, but statistically significant SES with regard to ADL measured at the end of the intervention phase. Further analysis showed a significant homogeneous SES for 17 studies that investigated effects of increased exercise intensity within the first 6 months post stroke. No significant homogeneous SES was observed for the 3 studies conducted in the chronic phase. Cumulative meta‐analysis strongly suggests that at least a 16 hour difference in treatment time between experimental and control groups provided in the first 6 months after stroke is needed to obtain significant differences in ADL. A significant SES supporting a higher intensity was also observed for instrumental ADL and walking speed, whereas no significant SES was found for dexterity. Conclusions: The results of the present research synthesis support the hypothesis that augmented exercise therapy has a small, but favourable effect on ADL, particularly if therapy input is augmented at least 16 hours within the first 6 months post stroke. This meta‐analysis also suggests that clinically relevant treatment effects may be achieved on instrumental ADL and gait speed.
Effects of augmented exercise therapy time
69
Introduction Stroke is a leading cause of disability among adults in developed countries. Any treatment that improves functional outcome can significantly reduce suffering and the financial burden of this illness on the individual, the family and society. Rehabilitation is recognized as a corner stone of multidisciplinary stroke care.1 Two systematic reviews2,3 suggested that early implementation of intensive stroke rehabilitation is associated with enhanced and faster improvement of the performance of activities after stroke. Both groups found small but statistically significant summary effect sizes (SES) in favour of the group that spent more treatment time focused on activities of daily living (ADL). In a sensitivity analysis, larger overall effect sizes were found in studies that weighted individual effect sizes for the differences in amount of rehabilitation between experimental and control groups.3 In these 2 systematic reviews, however, methodological limitations of the primary studies, differences in organisational settings as well as marked heterogeneity of patient characteristics proved to be major confounding factors.
In the last few years, new trials that provided augmented exercise training by physiotherapists and occupational therapists have been conducted. The results of these trials show results that range from no measurable benefits4‐7 to significant effects on ADL.8‐11 This discrepancy can be related to differences in: 1) methodological quality of the trials, 2) patient selection, 3) amount of contrast between the intensity of treatment in experimental and control groups, 4) differences in type, focus and timing of intervention post stroke, 5) differences in outcome measures and 6) statistical power to show true effects. In particular, there is much debate about the amount of therapy that is needed and whether or not there is a minimum threshold below which there is no benefit.
The purpose of the present research synthesis was to examine the effects of treatment time by reviewing studies evaluating the effects of intensity of exercise therapy in patients with stroke on ADL, gait and dexterity. The hypothesis was that the extra treatment time provided to the augmented therapy group would result in clinically relevant improvements in ADL, walking speed and dexterity. A secondary goal was to determine whether or not there is a minimum threshold of additional time provided to the experimental group below which no clinically relevant benefit might be expected.

Chapter 3
70
Material and Methods Definitions Stroke has been defined by the World Health Organization (WHO) as ‘a clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hours or leading to death, with no apparent causes other than of vascular origin’.(12, page 1407)
Exercise therapy was defined as ‘physical activity that is usually regular and done with the intention of improving or maintaining physical fitness or health’ (Pubmed [Medline], MeSH database, 2003) and included both physiotherapy and occupational therapy. ADL was defined as performance of the basic activities of self care, such as dressing, ambulation and eating)in rehabilitation, and instrumental ADL (IADL), such as shopping, preparing meals, washing clothes and pursuing hobbies. Both outcomes were included in the present analysis. Finally, treatment contrast was defined as the amount of time spent on exercise training for the experimental group minus that for the control group.3 Studies that investigated the effectiveness of constraint induced movement therapy or application of special equipment to augment exercise therapy such as balance platforms, treadmills, biofeedback equipment or robotics, were excluded from the present study. Two independent reviewers (GK and RPSvP) selected articles based on the title and abstract. Study identification Potentially relevant literature was identified through computerised and manual searches. Two independent literature searches (RPSvP and JCFK) were conducted in the following data bases: MEDLINE (1966 through November 2003), CINAHL (1982 through November 2003), Cochrane Central Register of Controlled Trials, EMBASE (1988 through November 2003), PEDro, DARE, SCISEARCH (1974 through November 2003) and Picarta. The search was performed for the period 1966 to November 2003 using the following keywords (MesH): cerebrovascular disorders, stroke, physical therapy, physiotherapy, occupational therapy, exercise therapy, rehabilitation, intensity, dose‐response relationship, effectiveness, randomised controlled trial. Bibliographies of review articles, empirical articles and abstracts published in proceedings of conferences were also evaluated. Only articles written in English, German or Dutch were included. Studies were included when: 1) patients had a diagnosis of stroke, 2) effects of the intensity of physiotherapy and/or occupational therapy were

Effects of augmented exercise therapy time
71
presented in the article, 3) the outcome was measured in terms of ADL (including walking ability, dexterity or IADL such as leisure therapy), and 4) the study was a randomised controlled trial. Table 1 – Operationalisation of validity criteria (modification of list Kwakkel et al 3) Methodological aspect:
Criteria for operationalisation:
Operationalisation: (yes = 1 / no = 0)
A. Randomisation procedure is adequate if:
1. concealed allocation is applied (i.e. sealed envelopes)
1. yes / no
B. Blinding procedure is adequate if:
2. observer(s) are kept unaware of the groups to which patients have been assigned:
2. yes / no
3. those performing statistical analysis are kept unaware of the groups to which patients have been assigned:
3. yes / no
4. patients are kept unaware with respect to the condition to which they have been assigned:
4. yes / no
C: Drop-outs and intention-to-treat analysis are adequate if:
5. the number of drop-outs are described for each group separately:
5. yes / no
6. the number of intercurrent drop-outs are described for each group separately:
6. yes / no
7. intention-to-treat analysis has been applied:
7. yes / no
D. Measurement instruments are adequate if:
8. statistically significant test-retest correlation coefficient(s) and/or intra-, inter-observer reliability of relevant measurement instruments have been reported by the authors or have been established in studies which are cited by the authors:
8. yes / no
9. the relevant measurement instruments are compared statistically with other instrument(s) measuring the same modality by the authors or in studies reported by the authors:
9. yes / no
E. Control for co-intervention(s) is adequate if:
10. other co-interventions leading to systematic differences between groups are avoided:
10. yes / no
11. adjunctive (medical) interventions are reported for each group separately:
11. yes / no
F. Comparability of patient characteristics is adequate if:
12. relevant patient characteristics (i.e. initial ADL-score, type of stroke, age and time since stroke onset) are not statistically significant different between experimental and control group(s):
12. yes / no
G. Control for dose of therapy is adequate if:
13. predetermined rehabilitation time (in minutes or hours) and/or number of exercises and/or dosage of applied exercises have been reported in experimental and control group(s):
13. yes / no
14. predetermined rehabilitation time (in minutes or hours) and/or number of exercises and/or dosage of applied exercises have been reported in experimental and control group(s):
14. yes / no

Chapter 3
72
Methodological quality The methodological quality of each study was assessed by 2 independent reviewers (RPSvP and GK) by applying an adapted methodological scoring list derived from a list developed by Kwakkel et al3 and Cambach.13 The original list contained 16 items, with each scored on a binary scale. Because the present review was focused only on RCTs, items 2 and 3 were deleted so that 14 questions remained to be addressed. (Table 1). The revised tool showed good inter‐rater reliability according to Cohenʹs kappa (κ=0.85). When disagreement between the 2 reviewers persisted, a third reviewer made the final decision. Reviewers were not blind to author(s), institution(s) or journal. One reviewer (RvP) extracted all relevant data. The following items were evaluated: 1) randomisation and blinding procedures; 2) descriptions of drop‐outs and intention‐to‐treat analysis; 3) reliability and validity of assessment instruments; 4) control for co‐intervention(s); 5) comparability of baseline patient characteristics; and 6) presentation of amount of therapy provided.
Quantitative analysis The abstracted data (mean age, type of stroke, numbers of patients in experimental and control group, days of treatment, average length of daily treatment in minutes, mean difference in change scores in ADL and standard deviation [SD] of ADL scores in experimental and control groups at baseline) were entered into Excel for Windows. The formal statistical methods used to test the results of different trials have been described elsewhere.3 The effect size gi (Hedgesʹ g) for individual studies was established by calculating the difference between means of the experimental and control groups divided by the average population SDi.14 If necessary, means and SDi were requested from the respective authors. Otherwise point estimates were obtained from the graphs of included articles by recording the bitmap coordinates after scanning the graphs into Microsoft Paint.
To estimate SDi for gi, baseline SDs of control and experimental groups were pooled (eg, Hedges, 1985). As the gi tend to overestimate the population effect size in studies with a small number of patients, a correction was implemented to obtain an unbiased estimation gu. The impact of sample size was addressed by estimating a weighting factor wi for each study and applying more weight to effect sizes from studies with larger samples that resulted in smaller variances. Subsequently, gu of individual studies were averaged to obtain a weighted SES (Ť). Finally, the wi of each study were combined to estimate the variance of the SES.15 When information about point estimates and standard errors was lacking the

Effects of augmented exercise therapy time
73
original authors were consulted. The effect size gu for individual studies was computed for degree of disability in day‐to‐day activities, walking speed and dexterity. In addition, SESs expressed as number of standard deviation units (SDUs) were calculated for studies comparing effects of different intensities in rehabilitation in the chronic stage of stroke (>6 months after onset), and those initiated within 6 months of stroke. The fixed effects model was used to decide whether or not a SES was statistically significant. The homogeneity (or heterogeneity) test statistic (Q‐statistic) of each set of effect sizes was examined to determine whether or not studies shared a common effect size from which the variance could be explained by sampling error alone.14,16 Although the Q‐statistic underestimate the existing heterogeneity in meta‐analysis, the percentage of total variation across studies was used by calculating I2 which reveals a better measure of the consistency between trials.17 When significant heterogeneity was found on the Q‐statistic (or I2 values >50%),17 a random effects model was applied.18,19 Pearson correlation coefficients were calculated between, individual effect sizes, and additional time exercising in the experimental groups, as well as the methodological quality of the studies. To investigate the effects of differences in treatment contrast in selected studies a cumulative meta‐analysis adjusted for treatment contrast was applied for the ADL outcome, using a random effects model. Finally, a sensitivity analysis was performed for studies with high and low treatment contrasts. Effect sizes were calculated in Excel for Windows XP, whereas SPSS 11.5 for Windows was used for statistical analysis. For all outcome variables, the critical value for rejecting H0 (ie, there is no evidence for augmented therapy time) was set at 0.05. Results The search strategy resulted in a list of 7483 citations. After selection, based on title and abstract, 507 full articles were obtained. Thirty‐two studies were identified as being relevant. Five studies used a pretest – posttest assessment design;20‐24 3 studies included a control condition but no randomisation;25‐27 and 24 studies were RCTs.4‐11,28‐44 Despite being a RCT the article by Peacock et al29 was also excluded due to lack of information about treatment contrast as well as missing point measures and estimates of variability. Four studies referred to the same patients, who had been reported in 3 RCTs which had already been included in this meta‐analysis.35,38,39,40 One study included patients with traumatic brain injury;41 only the patients with stroke were included in the present analysis.

Chapter 3
74
Con
trast
(m
in)
(E/C
)
2100
E1:
681
6 E
2: 3
324
657
1185
496
1933
4608
167
900
PT:
262
0 O
T: 2
460
QP
T: 5
75
AP
T: 4
30
302
900
Dai
ly (m
in)
OT†
- E1:
41/
14
E2:
25/
14
0.06
/0.0
6
- - - 48/0
22/3
7
- 69/4
4
- 3/0
-
Dai
ly (m
in)
PT†
100/
60
E1:
73/
14
E2:
36/
14
40/2
4
45/2
8║
8/0
53/2
2
48/0
- 48/1
8
70/4
4
QP
T:65
/42
AP
T:59
/42
- 60/3
0
Dur
atio
n of
re
habi
litat
ion
(E/C
)
63/5
6 d
3 m
o
46/3
7 d
18/1
0 w
k*
3 m
o
5 w
k
12 w
k
<3 m
o
6 w
k
20 w
k
5 w
k
5 m
o
6 w
k
Mea
n ag
e,
y (E
/C)
64/6
4
63/6
6/65
72/7
0
66/6
9*
72/7
2
69/7
0
59/6
6
71/7
4
66/6
3
67/6
5
73/7
3*
74/7
5
77§
Type
of i
nter
vent
ion
(E/C
)
PN
F vs
co
nven
tiona
l
Inte
nsiv
e co
nven
tiona
l ca
re v
s se
lf-ca
re
Inte
nsiv
e vs
no
rmal
Enh
ance
d vs
co
nven
tiona
l
Trea
tmen
t vs
no
trea
tmen
t¶
Inte
nsiv
e vs
co
nven
tiona
l
Trea
tmen
t vs
no
trea
tmen
t
Enh
ance
d vs
us
ual s
ervi
ce
Enh
ance
d vs
se
nsor
imot
or s
timul
atio
n
Inte
nsiv
e vs
im
mob
ilisat
ion
Inte
nsiv
e vs
ro
utin
e
Trea
tmen
t (O
T) v
s
no tr
eatm
ent
Inte
nsiv
e vs
st
anda
rd
Sta
rt of
re
habi
litat
ion
(E
/C)
29/3
3 d
31/4
1/37
d
<1/<
1 w
k
9/9
d*
4.4/
5.0
y
8.5/
13 d
2.9/
3.3
y
39/4
5 d
21/2
4 d
7/7
d
12/1
2 d*
<1/<
1 m
o
?/?
Stro
ke ty
pe
TEI
? TEI (
89%
),
ICH
, (11
%)
SA
H a
nd b
rain
st
em e
xclu
ded
All
type
s
Mid
dle
band
st
roke
s
MC
A s
troke
s
All
type
s (fi
rst
stro
kes)
TEI o
r IC
H
(SA
H e
xclu
ded)
MC
A (f
irst e
ver
stro
ke)
All
type
s
All
type
s
All
type
s
N (E
/C)
62 (3
1/31
)
133
(46/
43/4
4)
95 (5
0/45
)
132
(65/
67)
94 (4
9/45
)
27 (1
8/9)
40 (2
8/12
)
111
(53/
58)
100
(50/
50)
101
(33/
31/3
7)
282
(94/
93/9
5)
185
(94/
91)
114
(54/
60)
Tabl
e 2
S
tudy
cha
ract
eris
tics
of tr
ials
on
inte
nsity
of s
troke
reha
bilit
atio
n R
efer
ence
Ste
rn, 1
970
Sm
ith, 1
981
Siv
eniu
s, 1
985
Sun
derla
nd, 1
992
Wad
e, 1
992
Ric
hard
s, 1
993‡
Wer
ner,
1996
Loga
n, 1
997
Feys
, 199
8
Kw
akke
l, 19
99
Linc
oln,
199
9
Wal
ker,
1999
Par
tridg
e, 2
000

Effects of augmented exercise therapy time
75
Con
trast
(m
in)
(E/C
)
380
442
502
132
614
420
900
720
Wei
ghte
d m
ean:
95
6
Dai
ly
(min
) O
T†
13/0
AD
L: 4
/0
Leis
ure:
4/
0- - - - 22
.9/
10.9
min
Dai
ly
(min
) P
T†
- - 2/0
30/1
9║
Mea
n: 5
2 vs
38
45
40/2
5
48.6
/ 23
.3 m
in
Dur
atio
n of
re
habi
litat
ion
(E/C
)
6 w
k
6 m
o
13 w
k
~12
wk
6 w
k
4 w
k
~10
wk
Mea
n ag
e,
y (E
/C)
71/7
1
72/7
2
72/7
4
52/5
4
74/7
5
65/6
2
68/6
7
Type
of i
nter
vent
ion
(E/C
)
Dom
icili
ary
prog
ram
vs
rout
ine
serv
ice
Leis
ure/
AD
L tre
atm
ent
vs n
o tre
atm
ent
Rou
tine
treat
men
t vs
no
treat
men
t
Inte
nsiv
e (O
T+P
T) v
s no
rmal
ther
apy
Enh
ance
upp
er li
mb
ther
apy
time
vs
inte
rdis
cipl
inar
y tre
atm
ent p
rogr
am
Ear
ly in
tens
ive
PT
vs
rout
ine
ther
apy
with
out
early
PT
Aug
men
ted
vs s
tand
ard
PT
to im
prov
e m
obilit
y
Sta
rt of
re
habi
litat
ion
(E
/C)
31/2
3 d
<6/<
6 m
o
>1/>
1 y
47/4
5 d
<10/
<10
d
<7 d
22/2
5 d
Stro
ke ty
pe
SA
H e
xclu
ded
All
type
s
All
type
s
All
type
s
All
type
s
All
type
s
All
type
s
N (E
/C)
138
(67/
71)
466
(153
/156
/157
)
170
(85/
85)
87 (4
7/40
)
123
(62/
61)
156
(78/
78)
70 (3
5/35
)
2686
(151
5/11
71)
Tabl
e 2
- C
ontin
ued
-
Ref
eren
ce
Gilb
erts
on, 2
000
Par
ker,
2001
Gre
en, 2
002
Sla
de, 2
002
Rod
gers
, 200
3
Fang
, 200
3
GA
PS
, 200
4
Tota
l
AD
L in
dica
tes
activ
ities
of d
aily
livi
ng; A
PT,
ass
ista
nt-p
hysi
othe
rapi
st; d
, day
(s);
wk,
wee
ks; y
, yea
r(s)
; ?, u
nkno
wn;
E/C
, exp
erim
enta
l vs
cont
rol g
roup
; IC
H, i
ntra
cere
bral
hem
orrh
age;
M
CA
, mid
dle
cere
bral
arte
ry; m
in, m
inut
es; m
o, m
onth
(s);
N, n
umbe
r of p
atie
nts
in e
ach
grou
p; O
T, o
ccup
atio
nal t
hera
pist
; PN
F, p
ropr
ioce
ptiv
e ne
urom
uscu
lar f
acilit
atio
n;
PT,
phy
siot
hera
pist
; QP
T, q
ualif
ied-
phys
ioth
erap
ist;
SA
H, s
ubdu
ral a
rach
noid
hem
orrh
age;
TE
I, th
rom
boem
bolic
infa
rctio
ns.
*, O
nly
med
ian
figur
es g
iven
; †,
Onl
y pe
riod
of d
iffer
ent r
ehab
ilitat
ion
inte
nsiti
es re
cord
ed; a
vera
ge o
f cal
cula
ted
min
utes
for e
very
wor
king
day
dur
ing
inte
rven
tion;
§,
Ave
rage
age
of e
xper
imen
tal a
nd c
ontro
l gro
up to
geth
er
‡, F
indi
ngs
of th
e ex
perim
enta
l (N
=10)
and
ear
ly c
onve
ntio
nal (
N=8
) are
com
bine
d an
d co
mpa
red
with
the
cont
rol g
roup
(N=9
);
¶, R
ando
mis
ed c
ross
over
des
ign
(onl
y fir
st p
hase
of t
he tr
ial i
s co
nsid
ered
);
║, O
T in
corp
orat
ed.

Chapter 3
76
Table 2 shows the main characteristics of the 20 eligible studies included in the meta‐analysis. Fourteen of these reported statistically significant effects for functional outcomes in favour of the group with augmented therapy time. In 6 studies, additional exercise therapy did not result in a significant difference in efficacy. In total, 2686 patients with stroke were involved. The start of therapy ranged from within the first week post stroke9,31,42 to >1 year after stroke onset.11,33,36 Seventeen of the 20 studies investigated the effects of intensity within the first 6 months following stroke, whereas in 3 studies the research protocol was initiated >6 months post stroke.11,33,36
On average the experimental group received twice as much physiotherapy (48.6 minutes; SD, 30.8) and occupational therapy (22.9 minutes; SD, 23.6) daily as the control group (23.3 minutes; SD, 18.0 and 10.9 minutes; SD, 16.8, respectively; Table 2). The additional time that exercise therapy was provided to the experimental group ranged from 132 minutes11 to 6816 minutes,30 with a weighted average of 956 minutes or about 16 hours additional therapy time per patient. Methodological quality
The results of the methodological quality scoring of the 20 RCTs are presented in Table 3. Initially there was disagreement between the 2 independent reviewers on 21 of the 266 criteria scored. Cohen kappa for agreement was 0.84. The methodological quality score ranged from 228,31 to 11 points.43
Ten studies used a randomisation procedure with concealed allocation.4,5,7,9‐11,31,37,40,43 In 16 studies, the observers were blinded to treatment allocation.4‐11,32‐34,36,37,41,43,44 However, none of the RCTs reported blinded statistical analysis or adjunct (medical) interventions for each group, separately. With the exception of Stern et al,28 all studies described drop‐outs for the experimental and control groups, separately. In 14 studies, the patients in the 2 groups had had a first stroke and were comparable for age, ADL index, and type of stroke.4‐7,9‐11,32‐34,36,41,43,44 In 12 studies the originally scheduled exercise therapy time was reported,4‐10,28,34,36,41,43, and in 11 trials the actual exercise therapy time was provided.5‐7,9,11,30,32,34,41,43,44

Effects of augmented exercise therapy time
77
Rep
orte
d ou
tcom
e N
o ef
fect
Pos
itive
Pos
itive
Pos
itive
Pos
itive
Pos
itive
Pos
itive
Pos
itive
Pos
itive
Pos
itive
No
effe
ct
Pos
itive
No
effe
ct
Pos
itive
No
effe
ct
Pos
itive
Pos
itive
No
effe
ct
Pos
itive
No
effe
ct
Co-
inte
rven
tion
No
No
Yes
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
Tota
l sc
ore
2 6 2 6 5 7 6 7 6 10
9 7 6 8 9 9 9 9 4 11
14
0 1 0 1 0 1 0 0 0 1 1 1 0 0 1 1 1 1 0 1 11
13
1 0 0 0 0 1 1 0 1 1 1 0 1 1 1 0 1 1 1 1 13
12
0 0 0 1 1 1 0 1 0 1 1 1 1 1 1 1 1 1 0 1 14
11
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
10
0 0 0 0 0 0 1 0 1 1 1 0 1 0 1 1 0 0 1 1 9
9 0 1 0 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 1 16
8 1 1 0 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 1 17
7 0 0 0 0 0 0 0 1 0 1 0 0 0 1 1 1 1 1 0 1 8
6 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1
5 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 18
4 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 1
3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
2 0 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 18
Item
of m
etho
dolo
gica
l sco
re
1 0 1 1 0 0 0 0 1 0 1 1 1 1 1 0 1 0 1 1 1 12
Tabl
e 3
A
pplic
atio
n of
met
hodo
logi
cal c
riter
ia to
stu
dies
inve
stig
atin
g th
e ef
fect
s of
inte
nsity
of e
xerc
ise
ther
apy
Aut
hor,
y
Ste
rn, 1
970
Sm
ith, 1
981
Siv
eniu
s, 1
985
Sun
derla
nd, 1
992
Wad
e, 1
992
Ric
hard
s, 1
993
Wer
ner,
1996
Loga
n, 1
997
Feys
, 199
8
Kw
akke
l, 19
99
Linc
oln,
199
9
Wal
ker,
1999
Par
tridg
e, 2
000
Gilb
erts
on, 2
000
Par
ker,
2001
Gre
en, 2
002
Sla
de, 2
002
Rod
gers
, 200
3
Fang
, 200
3
GA
PS
, 200
4
Sum
sco
re

Chapter 3
78
Meta‐analysis: ADL Pooling the effects was only possible for those studies assessing ADL as an outcome. Fifteen studies evaluated outcome with the Barthel Index (BI), 1 study used the Functional Independence Measure motor (FIM)35, and 4 studies used other measures that assess ADL.4,28,30,31
After intervention a small but statistically significant heterogeneous SES (χ2 =37.65, p<0.05) was found in favour of augmented exercise therapy (SES [random] 0.13 SDU; CI, 0.03 to 0.23; Z=2.49, p<0.007) (Figure 1 and Table 4). The SES obtained was almost the same for the 9 studies (N=1570) that also measured IADL (0.23 SDU [fixed]; CI, 0.13 to 0.33; Z=4.40, p<0.001) (Figure 2).5‐7,9,10,33,37,43,44
Figure 1. Meta‐analysis for trials on outcome of ADL at the end of the intervention
-1 0
S.E.S. N=2686 0.13 [0.03 - 0.23](random effects model)
Smith (2) N=65 0.35 [-0.16 - 0.87]
1 2
Intensive therapy worse Intensive therapy better
ADL (mean and 95% CI)
Sivenius N=95 0.75 [0.33 - 1.16]
Stern N=62 0.14 [-0.36 - 0.64]
Smith (1) N=68 0.49 [-0.02 - 1.01]
-2
Sunderland N=132 0.10 [-0.25 - 0.44]
Wade N=94 0.07 [-0.33 - 0.47]
Richards N=27 -0.38 [-1.18 - 0.44]
Werner N=40 0.32 [-0.36 - 1.00]
Logan N=111 0.00 [-0.37 - 0.37]
Feys N=100 - 0.03 [-0.42 - 0.36]
Kwakkel (1) N=49 0.42 [-0.17 - 1.01]
Kwakkel (2) N=52 0.44 [- 0.13 -1.09]
Lincoln (1) N=140 0.00 [-0.35 - 0.35]
Lincoln (2) N=142 0.00 [-0.35 - 0.35]
Walker N=185 0.33 [0.04 - 0.63]
Partridge N=114 0.17 [-0.20 - 0.54]
Parker (1) N=235 0.00 [- 0.27 - 0.27]
Parker (2) N=231 0.00 [-0.27 - 0.27]
Green N=170 0.00 [-0.30 - 0.30]
GAPS N=70 -0.31 [-0.78 - 0.16]
Slade N=87 -0.07 [-0.43 - 0.41]
Gilbertson N=138 0.50 [ 0.16 - 0.84]
Rodgers N=123 -0.33 [-0.69 - 0.02]
Fang N=156 0.32 [0.16 - 0.64]

Effects of augmented exercise therapy time
79
Figure 2. Meta‐analysis of intensity trials measuring outcome of instrumental ADLs
-1 0
S.E.S. N=1570 0.23 [0.13 - 0.33](fixed effects model)
Lincoln (2) N=142 0.34 [-0.01 - 0.69]
1 2
Logan N=111 0.33 [-0.05 - 0.71]
Intensive therapy worse Intensive therapy better
IADL (mean and 95% CI)
Walker N=185 0.50 [0.21 - 0.79]
Lincoln (1) N=140 0.61 [0.25 - 0.97]
-2
Parker (1) N=235 0.10 [-0.17 - 0.38]
Parker (2) N=231 0.01 [-0.26 - 0.29]
Wade N=94 0.06 [-0.35 - 0.46]
GAPS N=70 -0.21 [-0.68 - 0.26]
Kwakkel (1) N=49 0.46 [-0.13 - 1.04]
Kwakkel (2) N=52 0.13 [-0.43 - 0.70]
Rodgers N=123 0.00 [-0.35 - 0.35]
Gilbertson N=138 0.49 [0.15 - 0.83]
A homogeneous non‐significant SES were found (χ2 =0.72, p=0.70) for studies in which therapeutic intervention was initiated after 6 months post stroke (0.07 SDU [fixed]; CI, ‐0.17 to 0.28; Z=0.49), whereas the homogeneous (χ2 =28.61, p=0.10; I2 =33.6%) SES was significant (0.15 SDU [fixed]; CI, 0.06 to 0.23; Z=3.24, p<0.001) in which therapy when applied within the first 6 months.
A positive association was found between the additional number of minutes of therapy provided in the experimental group as compared with the control group with an unbiased effect size (r=0.393; p<0.058). Methodological quality, however, was negatively associated with effect size (rs= ‐ 0.438; p<0.053). A cumulative meta‐analysis, adjusted for differences in treatment contrast across all 20 studies, showed a gradual shift from no significant effect in studies with a low treatment contrast (0 SDU: CI, 0.30 to 0.30; Z=0.0 p=1.0) to statistically significant overall effect sizes when studies with a high treatment contrast were added (0.13 SDU; CI, 0.03 to 0.23; Z=2.49; p=0.007). (Figure 3). Sensitivity analysis revealed significant homogeneous (χ2 =7.07,

Chapter 3
80
p=0.60) SES for those studies that applied 15 hours or more (0.22 SDU; CI, 0.07 to 0.37; Z=2.95; p=0.005) when compared to studies with a lower treatment contrast (0.08 SDU; CI, 0.06 to 0.22; Z=1.10; p=0.136).
Figure 3. Cumulative meta‐analysis of intensity trials measuring outcome of ADL adjusted for treatment contrast
-0.5 0
N=466 Walker 0.12 [-0.10 - 0.35]
0.5 1Intensive therapy worse Intensive therapy better
INTENSITY: ADL (mean and 95% CI)
N=869 Lincoln (2) 0.09 [-0.14 - 0.32]
N=170 Green 0.00 [-0.44 - 0.44]
N=281 Logan 0.00 [-0.23 - 0.23]
-1
N=1104 Parker (1) 0.08 [-0.12 - 0.27]
N=1198 Wade 0.08 [ -0.09 - 0.25]
N=1429 Parker (2) 0.07 [ -0.08 - 0.21]
N=1569 Lincoln (1) 0.06 [-0.07 - 0.19]
N=1656 Slade 0.06 [-0.07 - 0.18]
N=1751 Sivenius 0.10 [-0.02 - 0.23]
N=1821 GAPS 0.08 [-0.07 - 0.23]
N=1935 Partridge 0.17 [-0.20 - 0.54]
N=2191 Feys 0.10 [-0.02 - 0.21]
N=2323 Sunderland 0.10 [-0.02 - 0.21]
N=2350 Richards 0.09 [-0.03 - 0.20]
N=2412 Stern 0.07 [-0.04 - 0.19]
N=2464 Kwakkel (2) 0.09 [-0.02 - 0.20]
N=2513 Kwakkel (1) 0.10 [-0.00 - 0.20]
N=2578 Smith (2) 0.10 [0.00 - 0.21]
N=2686 Smith (1) 0.13 [0.03 - 0.23]
N=2618 Werner 0.12 [0.00 - 0.21]
cumulative contrast
S.E.S. N = 2686 0.13 [0.03 - 0.23](random effects model)
132 min
146 min
Cumulativenumber ofpatients
208 min
276 min
301 min
331 min
344 min
370 min
388 min
400 min
413 min
425 min
453 min
508 min
544 min
560 min
600 min
639 min
678 min
744 min
804 min
Cumulativeeffect size
[mean 956 min]
N=604 Gilbertson 0.21 [-0.03 - 0.45] 247 min
N=727 Rodgers 0.11 [-0.17 - 0.38]
956 min
N=2091 Fang 0.12 [0.00 - 0.24] 487 min
Comfortable walking speed and dexterity
Six (N=524) of 20 studies measured the effects of augmented therapy on walking speed.4,9,11,33,34,43 Pooling individual effect sizes revealed a significant homogeneous SES of 0.19 (SDU); CI, 0.01 to 0.36; Z=2.12; p=0.017) (Table 4).

Effects of augmented exercise therapy time
81
Another 5 studies (N=420) measured the effects of augmented therapy for upper extremity function using the Action Research Arm test (ARAT).5,7‐9,43 Pooling these studies using this outcome showed no significant SES in favour of augmented exercise therapy (0.03 SDU; CI, ‐0.13 to 0.19; Z=0.352, p=0.637) (Table 5). Table 4 – Summary effect sizes for comfortable walking speed at the end of the intervention (N=524) Trial
Outcome
Duration of intervention
NE /NC
SDE /SDC
∆E - ∆C
ES gU
95% CI
Wade, 1992 10 m walk 3 months 49 / 45 0.36 / 0.27 0.03 –(–0.03) = 0.06 0.12 –0.28 – 0.53
Richards, 1993 4 m walk 6 weeks 18 / 9 19.8 / 18.7 0.31 –0.30 = 0.01 0.07 –0.74 – 0.87
Kwakkel,1999 D
10 m walk 20 weeks 31 / 18 0.45/0.37B 0.65 – 0.37 = 0.28 A 0.65 0.06 – 1.25
Partridge, 2000 5 m walk 6 weeks 54 / 60 0.15 / 0.16 0.10 – 0.12 = –0.02 –0.13 –0.50 – 0.24
Green, 2002 10 m walk 13 weeks 85 / 85 0.17 / 0.21 0.05 – 0.01 = 0.04 0.16 –0.14 – 0.46
GAPS, 2004 10 m walk ~10 weeks 35 / 35 0.12 / 0.12 0.05 C 0.41 –0.06 – 0.89
SES (fixed model)
272 / 252
Weighted mean (m/s) ~0.06
0.19
0.01– 0.36
Table 5 – Summary effect sizes for dexterity at the end of the intervention (N=627) Trial
Outcome
Duration of intervention
NE /NC
SDE /SDC
∆E - ∆C
ES gU
95% CI
Feys, 1998 ARAT 6 weeks 50 / 50 7.86/7.98A 9.28 – 8.06 = 1.22A 0.15 –0.24 – 0.54
Kwakkel, 1999 D
ARAT 20 weeks 33 / 19 16.4/15.4B 10.40 – 2.39 = 8.01C 0.49 –0.08 – 1.07
Lincoln, 1999 G
ARAT 5 weeks 93 / 47 9 / 9 –1 C –0.11 –0.46 – 0.24
Lincoln, 1999 H
ARAT 5 weeks 94 / 48 9 / 9 -1 C –0.11 –0.46 – 0.23
Rodgers, 2003 ARAT 6 weeks 62 / 61 14 / 15 11.5 – 11.0 = 0.5 0.04 –0.32 – 0.39
GAPS, 2004 ARAT ~10 weeks 35 / 35 6 / 6 D 0.35 F 0.06 –0.41 – 0.53
SES (fixed model)
367/260 Weighted mean (pnts)
~0.55
0.03
–0.13 – 0.19
A Data from correspondence with author B Standard deviations at 6 weeks in stead of baseline C Calculated from p‐value (Table 3, in GAPS, 2004) D Leg training group vs control group (immobilisation of paretic arm and leg by means of an inflatable pressure splint) E Arm training group vs control group (immobilisation of paretic arm and leg by means of an inflatable pressure splint) F Calculated from p‐value (data from correspondence with author) G Assistant‐physiotherapist group vs routine physiotherapy group H Qualified‐physiotherapist group vs routine physiotherapy group ARAT indicates Action Research Arm Test; C, control group; CI, confidence interval; E, experimental group; ES gu, effect size (Hedges’g); m, metre; N, number of patients; pnts, number of points on ARAT (range 0‐57); SD, standard deviation; SES, summary effect size.

Chapter 3
82
Table 6 – Summary effect sizes for ADL at the end of the intervention (N=2686) Trial
ADL outcome
Duration of intervention
NE /NC
SDE /SDC
∆E - ∆C
ES gU
95% CI
Stern, 1970 KIR scale Until dischar-ge 92 / 88.7d
31 / 31 10 / 10 9.7 – 8.3 = 1.4 0.14 -0.36 – 0.64
Smith, 1981 F
Mod ADL P 3 mo 46 / 22 14.1 / 13.7 6.99 0.49 -0.02 – 1.01
Smith, 1981 G
Mod ADL P 3 mo 43 / 22 14.1 / 13.8 5.02 0.35 –0.16 – 0.87
Sivenius, 1985
Lehman ADL 3 mo 50 / 45 9.4 / 11.3 10.5 – 2.7 = 7.8 0.75 0.33 – 1.16
●Sunderland, 1992
BI 6 mo 65 / 67 6.0 / 5.19 0.54 B 0.10 –0.25 – 0.44
Wade, 1992
BI 3 mo 49 / 45 3 / 2.8 –0.1–(–0.3) = 0.2 0.07 –0.33 – 0.47
Richards, 1993
BI ambulation
6 wk 18 / 9 4.2 / 4.2 22.5 – 24.1 = –1.6D – 0.38 –1.18 – 0.44
Werner, 1996
FIM-MM 12 wk 28 / 12 14 / 19 6.6 – 1.5 = 5.1 0.32 –0.36 – 1.00
Logan, 1997
BI 6 mo 53 / 58 6 / 6 16 – 16 = 0 0.00 –0.37 – 0.37
●Feys, 1998
BI 6 wk 50 / 50 19.8 / 18 A 22.8 – 23.4 = –0.6A – 0.03 –0.42 – 0.36
Kwakkel, 1999 H
BI 20 wk 31 / 18 3.49/3.88A 10.3 – 8.75 = 1.55A 0.42 –0.17 – 1.01
●Kwakkel, 1999 J
BI 20 wk 33 / 19 3.86/3.88A 10.43 – 8.75 = 1.68A 0.44 –0.13 – 1.09
●Lincoln, 1999 K
BI 5 wk 93 / 47 5 / 6 6 – 6 = 0 0.00 –0.35 – 0.35
●Lincoln, 1999 L
BI 5 wk 94 / 48 4 / 6 6 – 6 = 0 0.00 –0.35 – 0.35
Walker, 1999
BI 6 mo 94 / 91 3 / 3 1 R 0.33 0.04 – 0.63
Partridge, 2000
RLOC 6 wk 54 / 60 4.8 / 4.6 0.7 – (–0.1) = 0.8 0.17 –0.20 – 0.54
Gilbertson, 2000
BI 6 wk 67 / 71 2 / 2 1 – 0 = 1 0.50 0.16– 0.84
Parker, 2001 M
BI 6 mo 156 / 79 4 / 3 0 – 0 = 0 0.00 –0.27 – 0.27
Parker, 2001 N
BI 6 mo 153 / 78 4 / 3 0 – 0 = 0 0.00 –0.27 – 0.27
Green, 2002
BI 13 wk 85 / 85 1.5 / 1.5 0 – 0 = 0 0.00 –0.30 – 0.30
Slade, 2002 BI ~84.6 dQ 47 / 40 23.5/26.3A 15.53 – 15.6= –0.07A
0.00 –0.42 – 0.42
●Rodgers, 2003 BI 6 wk 62 / 61 3 / 3 4 – 5 = –1 – 0.33 –0.69– 0.02
Fang, 2003
MBI 4 wk 65 / 62 19.56 / 31.04 21.97 – 13.63 = 8.34 0.32 0.16 – 0.64
GAPS, 2004
BI ~10 wk 35 / 35 3.3 / 3.1 4.8 – 5.8 = –1.0 – 0.31 –0.78 – 0.16
SES (random model)
1515 / 1171
0.13
0.03 – 0.23
A Data from correspondence with author; BMean of severe and mild groups; DE indicates mean of experimental and early conventional group and C mean of conventional group (Table 4, in Richards et al,1993); F Intensive therapy vs no routine rehabilitation; G Conventional therapy vs no routine rehabilitation; HLeg training group vs control group (immobilisation of paretic arm and leg by means of an inflatable pressure splint); JArm training group vs control group (immobilisation of paretic arm and leg by means of an inflatable pressure splint); KAssistant‐physiotherapist group vs routine physiotherapy group; LQualified‐physiotherapist group vs routine physiotherapy group; MADL‐therapy group vs control group; NLeisure‐therapy group vs control group; PModification of the ADL index: 17 items on a 3‐point scale; a person with a score of 17 points requiring no help; 51 points means inability to make any contribution on any item; QUntil discharge; RMean difference is given in Table 2, in Walker et al, 1999. BI indicates Barthel Index; C, control group; ●, exercise therapy time focused on upper limb only; CI, confidence interval; d, day; E, experimental group; ES gu, effect size (Hedges’g); FIM‐MM, functional independence measure – motor measure; KIR, Kenny Institute of Rehabilitation; mo, month(s); N, number of patients; RLOC, recovery locus of control scale; SD, standard deviation; SES, summary effect size; wk, week

Effects of augmented exercise therapy time
83
Discussion:
From the present systematic review, it may be concluded that augmented exercise therapy time spent in exercise training in the first 6 months after stroke results in small improvements in ADL. Pooling reported differences in ADL, by applying a fixed and random effects model showed small, but significant SES. The effects were mainly restricted to therapies focused on the lower limb and ADL in general, as well as to those studies conducted within the first 6 months of stroke.
The SES in the cumulative meta‐analysis denotes an overall change of about 4% to 5% in favour of more therapy time when a minimum of at least about 16 hours additional exercise therapy time is provided. We must acknowledge, however, that the findings do not allow us to be precise about optimal treatment contrast. Another important point of discussion is the clinical significance of such a small finding reflecting only a 1‐point change (5%) in outcome for the Barthel Index in favour of augmented therapy. Acknowledging that >80% receive exercise therapy, one may argue from an epidemiological perspective that even this small change in ADL score is likely to have a disproportionately large impact for health care polices.1
The benefits of augmented therapy time were mainly related to studies that focused the extra time on the lower limb or general ADL and not to the 5 RCTs that provided additional therapy time to the upper limb. It is important to note, however, that an ADL outcome, such as the Barthel Index, is more sensitive to lower limb improvement than to that in the upper limb.9 Moreover, improvements in mobility are more easily obtained than improvements in dexterity. We also know that functional outcome of the upper limb at 6 months after stroke is closely related to the level of recovery achieved in the first month, at least in patients with a primary middle cerebral artery stroke.45 In addition, there are indications that gains in the upper limb may require more intense repetitive practice and may be limited to those with less severe upper extremity deficits.32,45,46 This finding also suggests that for patients who are expected to achieve at least some dexterity, every opportunity should be given to regain function in the affected upper limb. In contrast, those patients for whom a poor motor recovery without return of dexterity is anticipated should have treatment focused on achieving and maintaining a comfortable mobile arm and hand. Compensation strategies with the nonparetic arm should be fostered.47
Lastly, the findings of our meta‐analysis showed that augmented therapy also may lead to improvements of about 5% in IADL such as household and

Chapter 3
84
leisure activities. It should be noted, however, that the number of such studies (n=9) is limited.
Although, in the present study, the intensive rehabilitation groups received about 16 hours more exercise therapy than the control group, considerable differences in the total amount of additional therapy provided, as well as in the timing and the focus of interventions, were observed. The augmented time of exercise therapy ranged from a minimum of 13211 to a maximum of 6816 minutes.30 Cumulative meta‐analysis of studies showed a positive trend in favour of those studies that applied a larger treatment contrast between experimental and control therapies. This suggests that the treatment contrast should exceed 16 hours to promote significant differences in ADL and that this more intensive therapy should be provided in the first 6 months post stroke. Interestingly, no ceiling effect for therapeutic intensity, beyond which no further response is observed, was found in the present study. This finding is consistent with a recent RCT on the effects of additional rehabilitation intensity after brain injury.48 Increasing the number of hours of therapy per week given to adults recovering from brain injury accelerated the rate of recovery of personal independence. In agreement with this finding, Chen et al24 found in a retrospective analysis of 554 records of patients with stroke that gains on Functional Independence Measure were weakly, but significantly, related to therapy intensity and rehabilitation duration after controlling for other variables. Future studies should focus on the effects of larger treatment contrasts in stroke, either by increasing the intensity of exercise time in the experimental group and/or by restricting the therapy in the control group. However, this latter suggestion may cause ethical concerns about depriving control subjects of the usual and expected amount of treatment.9
The present meta‐analysis has several limitations. First, we defined intensity and treatment contrast on the basis of differences in time that therapy was provided to the experimental and control groups. This is, of course, a crude estimate of the actual effort and energy that is spent in performing exercises.2,3 Other aspects, such as patients’ motivation, attention paid by the therapist and time spent on home exercises, may have confounded the reported outcomes. Second, although all included studies investigated the effects of additional exercise therapy, the content of therapy differed between studies, with regard to goals set and the type of reference treatment (or condition) applied. Finally, we may have missed relevant studies not published in scientific journals or published in languages other than English, German, or Dutch.

Effects of augmented exercise therapy time
85
It should also be noted that a number of other factors may have influenced the present findings, including different intervention goals, treatment content in the experimental group and control groups, patient selection criteria and outcome measures. For example, most studies investigated the additional effects of a particular method of treatment such as the neurodevelopmental approach,4‐6 facilitation exercise techniques,28 or task‐specific exercise programs.9,34 In all but 1 study, the control group received some form of therapeutic intervention. In the RCT by Kwakkel et al,9 the affected limbs were immobilised applying an inflatable pressure splint. The increased treatment contrast between the intervention and control groups obtained by preventing these patients from an active motor learning process may have contributed to a relatively larger effect size for leg training compared to other studies. Finally, when considering the impact of intensity of rehabilitation on stroke outcome, it should be realised that the intensity of rehabilitation programs is often limited.49,50 For example, in stroke units the usual direct contact time may be as little as 4% of the total waking time. Ten hours of therapy per week (2 h daily) represents only 9% of the waking time.51 It should also be acknowledged that >2 hours of therapy each day is not feasible for every patient or clinical setting due to inability to tolerate the extra therapy sessions or to limited personnel. Several studies have shown, however, that augmentation of functional oriented therapy may be achieved by applying ‘constraints’ to the less affected arm forcing the affected limb to be used during ADL for 6 hours a day during 2 weeks (ie, augmentation of 60 hours).52 From these studies, it may be hypothesised that high dose of task‐specific exercise training should be applied over a shorter period of time. Recent studies have also shown that the efficiency of limited therapeutic resources can be increased by using circuit training programs in which a group of patients is allowed to practice at different workstations simultaneously under the supervision of a therapist.46,53
Future studies should focus on the most cost‐effective intensity of therapy in stroke rehabilitation and the identification of patients who should benefit most from early and intensive exercise therapy. Differences were found between studies comparing the effects of intensity in the chronic stage of stroke to those comparing effects within 6 months of stroke onset. It should be noted, however, that the absence of SESs for the 3 studies that started augmented exercise therapy time in the chronic phase may be caused by insufficient statistical power. Future studies should indicate if the effects of enhanced exercise programs are transient, suggesting an increased speed of functional recovery or sustained in the chronic phase if therapy is

Chapter 3
86
continued.39,51 Thus far, findings from trials using constraint‐induced movement therapy in patients with an incomplete upper limb deficit suggest that intensive, task‐specific exercising in the chronic stage after stroke may result in improved dexterity.52 Therefore, research on subjects likely to benefit from higher intensities of stroke rehabilitation should be part of the future research agenda. This review has demonstrated the lack of data to define the treatment contrast needed to optimise effects of rehabilitation. At least it suggests that treatment contrasts between control and experimental groups should be extended in future high‐quality RCTs. Acknowledgments and Funding This part is a research project supported by a grant from the Royal Dutch Society of Physical Therapy (KNGF; grant reference number IKPZ/KNGF/05/2000). Chest, Heart & Stroke Scotland provided funding for Ian Wellwood and the PINTAS study. In addition, it is supported by a grant of ZonMw in the Netherlands (1435.0017). We like to thank JCK (Hans) Ket from the VU Medical Library for his independent literature search. Referenties
1. Langhorne P, Duncan P. Does the organization of postacute stroke care really matter?
Stroke 2001; 32: 268‐274.
2. Langhorne P, Wagenaar R, Partridge C. Physiotherapy after stroke: more is better? Physiotherapy Research International 1996; 1: 75‐88.
3. Kwakkel G, Wagenaar R, Koelman T et al. Effects of intensity of stroke rehabilitation: a research synthesis. Stroke 1997; 28: 1550‐1556.
4. Partridge C, Mackenzie M, Edwards S et al. Is dosage of physiotherapy a critical factor in deciding patterns of recovery from stroke: a pragmatic randomized controlled trial. Physiother Res Int 2000; 5: 230‐240.
5. Lincoln N, Parry R, Vass C. Randomized, controlled trial to evaluate increased intensity of physiotherapy treatment of arm function after stroke. Stroke 1999; 30: 573‐579.
6. Parker C, Gladman J, Drummond A et al. A multicentre randomized controlled trial of leisure therapy and conventional occupational therapy after stroke. TOTAL Study Group. Trial of Occupational Therapy and Leisure. Clin Rehabil 2001; 15: 42‐52.
7. Rodgers H, Mackintosh J, Price C et al. Does an early increased‐intensity interdisciplinary upper limb therapy programme following acute stroke improve outcome? Clin Rehabil 2003; 17: 579‐589.

Effects of augmented exercise therapy time
87
8. Feys H, deWeerdt W, Selz B et al. Effect of a therapeutic intervention for the hemiplegic upper limb in the acute phase after stroke: a single‐blind, randomized, controlled multicenter trial. Stroke 1998; 29: 785‐792.
9. Kwakkel G, Wagenaar R, Twisk J et al. Intensity of leg and arm training after primary middle‐cerebral‐artery stroke: a randomised trial. Lancet 1999; 354: 191‐96.
10. Gilbertson L, Langhorne P, Walker A et al. Domiciliary occupational therapy for patients with stroke discharged from hospital: randomised controlled trial. BMJ 2000; 320: 603‐606.
11. Green J, Forster A, Bogle S et al. Physiotherapy for patients with mobility problems more than 1 year after stroke: a randomized controlled trial. Lancet 2002; 359: 199‐203.
12. Stroke‐1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 1989; 20: 1407‐31.
13. Cambach W, Wagenaar RC, Koelman TW et al. The long‐term effects of pulmonary rehabilitation in patients with asthma and chronic obstructive pulmonary disease: a research synthesis. Arch Phys Med Rehabil 1999; 80: 103‐111.
14. Hedges L, Olkin I. Statistical methods for meta‐analysis. Orlanda FL: Academic Press, 1985.
15. Shadish W Haddock K. Combining estimates of effect size. In: Cooper H. and Hedges LV (eds.): The handbook of research synthesis. Russell Sage Foundation, New York, 1994; 18: 261‐282.
16. Hedges L. Fixed effects models. in Cooper H. and Hedges LV (eds.): The handbook of research synthesis. Russell Sage Foundation, New York, 1994; 19: 285‐300.
17. Higgins JPT, Thomposon SG, Deeks JJ et al. Measuring inconsistency in meta‐analyses. BMJ 2003; 327: 557‐560.
18. DerSimonian R. and Laird N. Meta‐analysis in clinical trials. (1986). Controlled Clinical Trials 1986; 7: 177‐188.
19. Raudenbush S. Random Effects model. In: Cooper H. and Hedges LV (eds.): The handbook of research synthesis. Russell Sage Foundation, New York, 1994; 20: 301‐323.
20. Brocklehurst J, Andrews K, Richards B et al. How much physical therapy for patients with stroke? BMJ 1978; 1: 1307‐1310.
21. Wade D, Skilbeck C, Hewer R et al. Therapy after stroke: amounts, determinants and effects. Int Rehabil Med 1984; 6: 105‐10.
22. Nugent J, Schurr K, Adams R. A dose‐response relationship between amount of weight‐bearing exercise and walking outcome following cerebrovascular accident. Arch Phys Med Rehabil 1994; 75: 399‐402.
23. Ballinger C, Ashburn A, Low J et al. Unpacking the black box of therapy ‐ a pilot study to describe occupational therapy and physiotherapy interventions for people with stroke. Clin Rehabil. 1999; 13: 301‐309.
24. Chen C, Heinemann A, Granger C et al. Functional gains and therapy intensity during subacute rehabilitation: a study of 20 facilities. Arch Phys Med Rehabil 2002; 83: 1514‐23.
25. Keith R, Wilson DB, Gutierrez P. Acute and subacute rehabilitation for stroke: a comparison. Arch Phys Med Rehabil 1995; 76: 495‐500.

Chapter 3
88
26. Rapoport J, Judd‐Van Eerd M. Impact of physical therapy weekend coverage on length of stay in an acute care community hospital. Phys Ther 1989; 69: 32‐37.
27. Ruff R, Yarnell S, Marinos J. Are stroke patients discharged sooner if in‐patient rehabilitation services are provided seven v six days per week? Am J Phys Med Rehabil 1999; 78: 143‐146.
28. Stern P, McDowell F, Miller J et al. Effects of facilitation exercise techniques in stroke rehabilitation. Arch Phys Med Rehabil 1970; 51: 526‐531.
29. Peacock P, Riley C, Lampton T et al. The Birmingham Stroke Epidemiology and Rehabilitation Study. In: Steward GT, editor. Trends in Epidemiology. Springfield, I 11: Charles C Thomas. 1972: 231‐345.
30. Smith, D, Goldenberg E, Ashburn, A et al. Remedial therapy after stroke: a randomised controlled trial. BMJ 1981; 282: 517‐520.
31. Sivenius J, Pyorala K, Heinonen O et al. The significance of intensity of rehabilitation of stroke. A controlled trial. Stroke 1985; 16: 928‐931.
32. Sunderland A, Tinson D, Bradley L et al. Enhanced physical therapy improves recovery of arm function after stroke. A randomised controlled trial. J Neurol Neurosurg Psychiat 1992; 55: 530‐535.
33. Wade T, Collen M, Robb F, Warlow P. Physiotherapy intervention late after stroke and mobility. BMJ 1992; 304: 609‐613.
34. Richards C., Malouin F, Wood‐Dauphinee S et al. Task‐specific physical therapy for optimization of gait recovery in acute stroke patients. Arch Phys Med Rehabil 1993; 74: 612‐620.
35. Sunderland A, Fletcher D, Bradley L et al. Enhanced physical therapy for arm function after stroke: A one year following up study. J Neurol Neurosurg Psychiat 1994; 57: 856‐858.
36. Werner R, Kessler S. Effectiveness of an intensive outpatient rehabilitation program for postacute stroke patients. Am J Phys Med Rehabil 1996; 75: 114‐120.
37. Logan P, Ahern J, Gladman J et al. A randomized controlled trial of enhanced Social Service occupational therapy for stroke patients. Clin Rehabil 1997; 11: 107‐113.
38. Kwakkel G, Kollen B, Wagenaar R. Long term effects of intensity of upper and lower limb training after stroke: a randomised trial. J Neurol Neurosurg Psychiat 2002; 72: 473‐79.
39. Kwakkel G, Wagenaar R. Effect of duration of upper‐ and lower‐extremity rehabilitation sessions and walking speed on recovery of interlimb coordination in hemiplegic gait. Phys Ther 2002; 82: 432‐448.
40. Parry R, Lincoln N, Vass C. Effect of severity of arm impairment on the response to additional physiotherapy early after stroke. Clin Rehabil 1999; 13: 187‐198.
41. Slade A, Tennant A, Chamberlain M. A randomised controlled trial to determine the effect of intensity of therapy upon length of stay in a neurological rehabilitation setting. J Rehabil Med 2002; 34: 260‐266.
42. Fang Y, Chen X, Lin J et al. A study on additonal early physiotherapy after stroke and factors affecting functional recovery. Clin Rehabil 2003; 17: 608‐617.

Effects of augmented exercise therapy time
89
43. Wellwood I, Langhorne P. Glasgow Augmented Physiotherapy after Stroke (GAPS) study. Can augmented physiotherapy input enhance recovery of mobility after stroke? Clinical Rehabilitation 2004; 18: 1‐9.
44. Walker M, Gladman J, Lincoln N et al. Occupational therapy for stroke patients not admitted to hospital: a randomised controlled trial. Lancet 1999; 354: 278‐280.
45. Kwakkel G, Kollen B, van der Grond J et al. Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke 2003; 34: 2181‐2186.
46. Duncan PM, Studenski S, Richards L et al. Randomized clinical trial of therapeutic exercise in subacute stroke. Stroke 2003; 34: 2173‐2180.
47. Barreca S, Wolf SL, Fasoli S et al. Treatment interventions for the paretic upper limb of stroke survivors: a critical review. Neurorehabil Neural Repair 2003; 17: 220‐226.
48. Shiel A, Burn J, Clark D et al. The effects of increased rehabilitation therapy after brain injury: results of a prospective controlled trial. Clin Rehabil 2001; 15: 501‐514.
49. Tinson D. How stroke patients spend their days. International Disabilities Studies 1989; 11: 45‐49.
50. De Weerdt, W, Nuyens G, Feys H et al. Group physiotherapy improves time use by patients with stroke in rehabilitation. Australian Journal of Physiotherapy 2001; 47: 53‐61.
51. Wade D. Rehabilitation research – time for a change of focus. The Lancet (Neurology) 2002; 1: 209.
52. Van der Lee J, Constraint‐induced therapy for stroke: more of the same or something completely different? Curr Opin Neurol 2001; 14: 741‐744.
53. Dean C, Richards C, Malouin F. Task related circuit training improves performance of locomotor tasks in chronic stroke: a randomized controlled pilot trial. Arch Phys Med Rehabil 2000; 81: 409‐17.

Chapter 3
90

CHAPTER
Effects of visual feedback therapy on postural control in bilateral standing after stroke:
A systematic review
Roland PS Van Peppen
Michiel Kortsmit
Eline Lindeman
Gert Kwakkel
Journal of Rehabilitation Medicine 2006; 38(1): 3‐9

Chapter 4
92
Abstract
Objective: To establish whether bilateral standing after stroke with visual feedback therapy improves postural control compared with conventional therapy and to evaluate the generalisation of the effects of visual feedback therapy on gait and gait‐related activities. Design: A systematic review Methods: A computer‐aided literature search was performed. Randomised controlled trials and controlled clinical trials, comparing visual feedback therapy with conventional balance treatments were included up to April 2005. The methodological quality of each study was assessed with the Physiotherapy Evidence Database scale. Depending on existing heterogeneity, studies with a common variable of outcome were pooled by calculating the summary effect sizes using fixed or random effects models. Results: Eight out of 78 studies, presenting 214 subjects, were included for qualitative and quantitative analysis. The methodological quality ranged from 3 to 6 points. The meta‐analysis demonstrated non‐significant summary effect sizes in favour of visual feedback therapy for weight distribution and postural sway, as well as balance and gait performance, and gait speed. Conclusions: The additional value of visual feedback therapy in bilateral standing compared with conventional therapy shows no statistically significant effects on symmetry of weight distribution between paretic and non paretic leg, postural sway in bilateral standing, gait and gait‐related activities. Visual feedback therapy should not be favoured over conventional therapy. The question remains as to exactly how asymmetry in weight distribution while standing is related to balance control in patients with stroke. Key words: cerebrovascular disorders, visual feedback, force plate, postural control, rehabilitation, meta‐analysis

Effects of VFT on postural control in bilateral standing
93
Introduction The rate in which stroke occurs in developed countries is approximately 2400 per 1 million persons per year.1 Stroke is one of the leading causes of impairment and disability in the Western world.2 Many patients with stroke suffer from significant motor and cognitive impairments, such as visual spatial impairments, aphasia, hemi‐neglect, dyspraxia, gait disorders and poor sitting and standing balance control.3,4 In particular, recovery of postural control is found to be a prerequisite for regaining independence in activities of daily living (ADL).5
Unfortunately, there is no generally accepted definition of the term ‘postural control’; however, the definition of Pollock and colleagues6 is frequently used. They described postural control as ‘the act of maintaining, achieving or restoring a state of balance during any posture or activity’. In hemiplegic patients the postural control is characterised by an increased postural sway,7,8 and asymmetrical weight distribution with a shift in the average position of the body’s centre of pressure towards the unaffected side.9,10 Current research concerning balance deficits in hemiplegic patients focuses on differential components such as postural sway and symmetry of weight distribution. The use of force plate feedback in stroke rehabilitation has been examined in a number of these studies. This type of therapy provides visual or auditory feedback of patient’s postural sway or weight distribution between the paretic and non paretic lower limb.11,12 The interest in force plate feedback as a rehabilitation instrument was positively influenced by the development of the Balance Master™ (NeuroCom International). This computerised force plate provides continuous visual feedback on the position of the centre of gravity (COG), giving a new tool for training: the visual feedback therapy (VFT). Despite the number of publications dedicated to feedback therapy, only one recent review has systematically evaluated the effectiveness of this therapy on promoting the recovery of postural control after stroke.13 Barclay‐Goddard et al13 concluded after systematic reviewing 7 randomised controlled trials (RCT), that force plate feedback (visual or auditory) improved stance symmetry after stroke, but they could not establish effects on postural sway or measures related to gait and independency in ADLs.
The purpose of the present systematic review was to examine the effects of the additional VFT on postural control in bilateral standing in subjects suffering from stroke. The primary aim of this review was to establish whether VFT reduces postural sway and improves symmetry of weight distribution in bilateral standing after stroke compared with

Chapter 4
94
conventional treatment. In addition, the effects of VFT on parameters of gait and gait‐related activities including ADL were evaluated. Methods Search strategy for study identification A computer‐aided literature search was performed in the following electronic databases; PubMed (MEDLINE), Cochrane Central register of Controlled Trials, CINAHL, Physiotherapy Evidence Database (PEDro) and DOC‐online. Only articles published in the period up to April 2005 and written in English, German or Dutch were included. All references presented in relevant studies were also examined. The following MeSH and keywords were used: cerebrovascular accident, cerebrovascular disorders, hemiplegia, paresis or stroke (patient type), rehabilitation, posture, symmetry, balance, postural control, musculoskeletal equilibrium or weight‐bearing (intervention type), force plates, force platforms or feedback (device type) and randomised controlled trial, controlled clinical trial, comparative study or trial (publication type). The complete study identification was performed by 2 independent reviewers (RPSvP, MK). The databases were searched using a study identification strategy that was formulated in PubMed and adapted to the other databases. The full search strategy is available on request from the first author. The abstracts of the publications, retrieved from the computer‐aided literature search, were selected on basis of the following 3 inclusion criteria: • The studies involved adult subjects suffering from stroke. The
participants were diagnosed as patients with stroke following the definition of the World Health Organization. Stroke is defined as ‘a focal (at times global) neurological impairment of sudden onset, and lasting more than 24 hours (or leading to dead) and of presumed vascular origin’.14
• Effects of VFT on postural control in bilateral standing were evaluated. The feedback had to provide visual representations of the individual’s centre of gravity or weight distribution between the paretic and non paretic leg. In the present review feedback is defined as a ‘process by which a person uses biofeedback information to gain voluntary control over processes or functions that are primarily under autonomic control’.15
• The studies were RCTs or controlled clinical trials (CCT).16

Effects of VFT on postural control in bilateral standing
95
Methodological quality assessment The methodological quality of the selected RCTs and CCTs was rated using the PEDro scale17,18 by 2 independent reviewers (RPSvP, MK). Reviewers were not blinded to author(s), institution(s) or journal. The PEDro scale contains 11 items. The first item assesses external validity and the other 10 items assess the internal and statistical validity of the studies.17,18 These 10 items were used to calculate the PEDro score. All items were scored binary (i.e., yes=1/no=0), which could result in a maximum score of 10 points. Agreement regarding each item was evaluated by calculating a Kappa statistic. Disagreements regarding items were solved by discussion between the reviewers. If disagreement persisted, a third reviewer (GK) made the final decision. Quantitative analysis Analysis of the results was performed separately for each study. When the interventions, patient characteristics and outcome measures were comparable, statistical pooling was performed. The data were re‐analysed by pooling the individual effect sizes (gi) using Hedges’ g model.19,20 In this model the difference between mean changes in the experimental group and in the control group during the therapy period were calculated and divided by the average population standard deviation (SDi).
Subsequently, unbiased effect sizes (gu) were calculated for each study after adjusting for the number of degrees of freedom. The impact of sample size was addressed by calculating a weighting factor (wi) for each study, and assigning larger effect‐weights to studies with larger samples.
Subsequently, gu’s of individual studies were averaged, resulting in a weighted summary effect size (SES), whereas the weights of each study were combined to estimate the variance of the SES.21 The fixed effects model was used to decide whether a SES was statistically significant (SES [fixed]). If significant between‐study variation existed a random effects model was applied (SES [random]).22 Post hoc sensitivity analysis for study design was performed if significant heterogeneity was found between individual effect sizes. For all outcome variables, the critical value for rejecting H0 (i.e., there is no evidence for VFT) was set two‐tailed at 0.05.

Chapter 4
96
Met
hodo
- lo
gica
l qu
ality
**
Ext
. val
# : ye
s 4
poin
ts**
Fa
ilure
at
ques
tions
3,
4,5,
6,7,
9 Ext
. val
# : ye
s 3
poin
ts**
Fa
ilure
at
ques
tions
2,
3,5,
6,7,
8,9
Ext
. val
# : ye
s 6
poin
ts**
Fa
ilure
at
ques
tions
3,
5,6,
9
Ext
. val
# : ye
s 4
poin
ts**
Fa
ilure
at
ques
tions
3,
5,6,
7,8,
9 Ext
. val
# : ye
s 5
poin
ts**
Fa
ilure
at
ques
tions
3,
5,6,
7,9
Con
clus
ions
(a
utho
r)
VFT
is m
ore
effe
ctiv
e th
an C
T in
redu
cing
la
tera
l sw
ay a
nd in
crea
-si
ng lo
ad o
n th
e af
fect
ed
leg,
how
ever
, no
sign
ify-
cant
pos
t-tre
atm
ent
effe
cts
wer
e fo
und.
Sig
nific
ant i
mpr
ovem
ent
of s
tatic
sta
ndin
g sy
m-
met
ry w
as fo
und
in V
FT-
grou
p. N
o ad
ditio
nal
effe
cts
of V
FT o
n ga
it sp
eed,
cad
ence
, stri
de
leng
th a
nd c
ycle
tim
e w
ere
obse
rved
.
Sig
nific
ant b
ette
r pe
rform
ance
VFT
on
stan
ce s
ymm
etry
and
sw
ay a
nd m
otor
and
A
DL
func
tion.
Bet
wee
n gr
oup
diffe
renc
es
disa
ppea
red
at 3
m
onth
s po
st s
troke
.
No
betw
een-
grou
p di
ffere
nces
in a
ny o
f the
ou
tcom
e m
easu
res
wer
e fo
und
No
betw
een-
grou
p di
ffe-
renc
es o
n an
y ou
tcom
e m
easu
re w
ere
foun
d,
alth
ough
the
CT
grou
p te
nded
to p
erfo
rm b
ette
r on
task
s in
volv
ing
gait.
Out
com
e
(Gai
t & g
ait-
rela
ted
activ
ities
)¹
–
Gai
t spe
ed
Not
tingh
am
10 P
oint
s A
DL
Sca
le,
Riv
erm
ead
Mot
or
Func
tion
Ass
ess-
men
t
BB
S,
TUG
, G
ait s
peed
B
BS
, TU
G,
Gai
t spe
ed
Out
com
e
(B
ilate
ral
stan
ding
)¹
Tota
l Sw
ay
area
(EO
),
Late
ral
Sw
ay (E
O)
Sw
ay (E
O),
W
eigh
t D
istri
butio
n S
way
(EO
),
Wei
ght
Dis
tribu
tion
Sw
ay (E
O)
Sw
ay (E
C)
Sw
ay (E
O),
S
way
(EC
), W
eigh
t D
istri
butio
n
Trai
ning
pe
riod
(w
eeks
)
2 3-4
4 3-8
3-8
Equ
ipm
ent
Sta
ndin
g Fe
edba
ck
Trai
ner
Sta
ndin
g Fe
edba
ck
Trai
ner,
S
tride
an
alys
er
syst
em
Not
tingh
am
Bal
ance
P
latfo
rm
Bal
ance
M
aste
rTM
Bal
ance
M
aste
rTM
Tim
e (d
) si
nce
st
roke
(E
/C)
36/3
7
54/4
4
141/
13
2
41/3
5
33*
Mea
n ag
e
(E/C
)
66/6
4 52
/54
61/6
8
65/6
2
65/6
5
N
(E/C
)
16
(8/8
)
42
(21/
21)
26
(13/
13)
32##
(1
6/16
) 16
(8
/8)
Des
ign
RC
T
CC
T
RC
T
RC
T
RC
T
Obj
ectiv
e st
udy
To
inve
stig
ate:
the
effe
ct o
f ad
ditio
nal V
FT
com
pare
d w
ith C
T in
re-e
stab
lishi
ng
stan
ce s
tabi
lity
in
post
-acu
te s
troke
pa
tient
s
the
effe
ct o
f ad
ditio
nal V
FT
com
pare
d w
ith C
T fo
r bal
ance
re-
train
ing
in p
ost-
acut
e st
roke
pa
tient
s w
ith a
st
andi
ng fe
edba
ck
train
er
the
effe
ctiv
enes
s of
add
ition
al V
FT
vs p
lace
bo V
FT in
im
prov
ing
stan
ce
sym
met
ry a
nd
func
tiona
l abi
lity
in
post
-acu
te s
troke
pa
tient
s
the
effe
ct o
f ad
ditio
nal V
FT
com
pare
d w
ith
bala
nce
train
ing
on
CoG
pos
ition
in
post
-acu
te s
troke
pa
tient
s
the
bene
ficia
l ef
fect
of V
FT c
om-
pare
d w
ith C
T fo
r ba
lanc
e re
-trai
ning
in
pos
t-acu
te
stro
ke p
atie
nts
Tabl
e 1
C
hara
cter
istic
s of
the
incl
uded
stu
dies
Ref
eren
ce
(yea
r )
Shu
mw
ay-C
ook
et
al.
(198
8)
Win
stei
n et
al.
(198
9)
Sac
kley
et a
l.
(199
7)
Wal
ker e
t al.
(200
0)
Gra
nt e
t al.
(1
997)

Effects of VFT on postural control in bilateral standing
97
Met
hodo
- lo
gica
l qu
ality
**
Ext
.val
# : ye
s 5
poin
ts**
Fa
ilure
at
ques
tions
3,
5,6,
7,9
Ext
. val
# : ye
s 5
poin
ts**
Fa
ilure
at
ques
tions
3,
5,6,
7,9
Ext
. val
# : ye
s 4
poin
ts**
Fa
ilure
at
ques
tions
3,
5,6,
7,8,
9
Con
clus
ions
(a
utho
r)
No
addi
tiona
l effe
cts
of
VFT
was
foun
d co
mpa
red
with
the
CT
grou
p
No
sign
ifica
nt b
etw
een-
grou
p di
ffere
nces
wer
e fo
und
with
resp
ect t
o st
atic
bal
ance
and
loco
-m
otio
n an
d m
obilit
y sc
orin
g of
FIM
. Sig
nifi-
cant
impr
ovem
ents
wer
e ob
serv
ed fo
r dyn
amic
ba
lanc
e fu
nctio
n an
d ou
tcom
e of
AD
L in
fa
vour
of V
FT.
No
betw
een-
grou
p di
ffere
nce
for a
ny s
tatic
st
abilit
y ou
tcom
e w
as
foun
d. T
he p
ost-t
rain
ing
test
sho
wed
sig
nific
antly
be
tter d
ynam
ic b
alan
ce
perfo
rman
ce in
favo
ur o
f V
FT. T
he o
ccur
renc
e of
fa
lls d
ecre
ased
, al
thou
gh n
ot s
tatis
tical
si
gnifi
cant
in fa
vour
of
the
VFT
gro
up.
Out
com
e
(Gai
t & g
ait-
rela
ted
activ
ities
)¹
BB
S,
TUG
Bru
nnst
rom
st
ages
; FI
M
Fall
occu
rrenc
e
Out
com
e
(B
ilate
ral
stan
ding
)¹
– Sw
ay (E
O),
Sw
ay (E
C),
S
tatic
S
tabi
lity,
D
ynam
ic
Sta
bilit
y
Sta
tic
Sta
bilit
y,
Dyn
amic
S
tabi
lity
Trai
ning
pe
riod
(w
eeks
)
4 2 3
Equ
ipm
ent
Bal
ance
M
aste
rTM
Bal
ance
M
aste
rTM
Bal
ance
M
aste
rTM
Tim
e (d
) si
nce
st
roke
(E
/C)
100/
13
4 90
/ 11
3
96/9
9
Mea
n ag
e
(E/C
)
62/5
9
59/5
5
61/6
1
N
(E/C
)
13
(7/6
)
41
(23/
18)
52
(28/
24)
Des
ign
RC
T
RC
T
CC
T
Obj
ectiv
e st
udy
To
inve
stig
ate:
the
effe
cts
of
addi
tiona
l VFT
co
mpa
red
with
CT
on b
alan
ce a
nd
mob
ility
in p
ost-
acut
e st
roke
pa
tient
s
the
dela
yed
effe
cts
of a
dditi
onal
VFT
co
mpa
red
with
CT
on b
alan
ce
retra
inin
g in
pos
t-ac
ute
hem
iple
gic
patie
nts
the
effe
cts
of
addi
tiona
l VFT
co
mpa
red
with
CT
on th
e oc
curre
nce
of
falls
in p
ost-
acut
e he
mip
legi
c pa
tient
s
Tabl
e 1
- C
ontin
ued
-
Ref
eren
ce
(yea
r)
Gei
ger e
t al.
(200
1)
Che
n et
al.
(2
002)
Che
ng e
t al.
(2
004)
¹ Onl
y ou
tcom
es re
leva
nt fo
r thi
s sy
stem
atic
ana
lysi
s ar
e pr
esen
ted;
* A
vera
ge ti
me
sinc
e st
roke
of b
oth
grou
ps;
**Q
ualit
y as
sess
men
t of R
CT’
s is
mea
sure
d by
cou
ntin
g th
e nu
mbe
r of c
heck
list c
riter
ia (2
-11)
of t
he P
ED
ro-s
cale
tha
t are
sat
isfie
d in
the
trial
repo
rt (s
umsc
ore
0-10
) of t
he it
ems
2-11
).
# Th
e fir
st it
em o
f the
PE
Dro
-sca
le h
as a
yes
/no-
scor
e. Y
es m
eans
that
the
exte
rnal
val
idity
is s
atis
fied.
##
The
VFT
gro
up is
com
pare
d to
the
conv
entio
nal g
roup
(the
dat
a of
the
3th
grou
p –c
ontro
l gro
up- a
re n
ot u
sed
in th
is m
eta-
anal
ysis
B
BS
indi
cate
s B
erg
Bal
ance
Sca
le; C
, con
trol g
roup
; CC
T, c
ontro
lled
clin
ical
tria
l; C
oG, c
ente
r-of
-gra
vity
; CT,
con
vent
iona
l bal
ance
ther
apy;
E, e
xper
imen
tal g
roup
; EC
, eye
s cl
osed
; E
O. e
yes
open
; FIM
, fun
ctio
nal i
ndep
ende
nce
mea
sure
; N, n
umbe
r of p
atie
nts;
PE
Dro
, phy
siot
hera
py e
vide
nce
data
base
; RC
T, ra
ndom
ised
con
trolle
d tri
al; T
UG
, tim
ed u
p &
go
test
; V
FT, v
isua
l fee
dbac
k th
erap
y

Chapter 4
98
Results Study identification After screening 78 identified studies, 9 studies were found to be relevant for further analysis.8,11,12,23‐28 The study of Engardt et al25 was excluded, because the patients in this study received postural control therapy with auditory instead of visual feedback. A total of 8 studies, involving 214 patients, met all the inclusion criteria.8,11,12,23,24,26‐28 The patients included in the study of Grant et al (N=16),26 however, showed to be a subset of the study of Walker and colleagues.12 Therefore the study of Grant was only used for outcomes not investigated by the study of Walker and colleagues.12 Six studies (N=128) were classified as RCTs8,11,12,23,26,27 and 2 as CCTs (N=86)24,28 Table I shows the main characteristics of the 8 eligible studies included in the systematic review. All studies were performed within the first 6 months post stroke, ranging from 5 weeks8,26 to 20 weeks7 after stroke onset. Methodological quality assessment The methodological quality of the 8 included studies is presented in Table I.8,11,12,23,24,26‐28 Therefore 80 quality items (10 per study) were scored. Initially, the 2 reviewers disagreed on 5 of the 80 (6.3%) quality items. This resulted in an average Cohenʹs Kappa score for all items of 0.88. The median PEDro score was 4, ranging from 3 to 6 points.
Eight studies did not use a randomisation procedure with concealed allocation and did not describe an intention‐to‐treat analysis.8,11,12,23,24,26‐28 In one study the observers were blinded to treatment allocation.27 Quantitative analysis Pooling of outcomes was possible for (a) weight distribution and postural sway while bilateral standing; (b) Berg Balance Scale (BBS)29,30; (c) Timed Up & Go test (TUG)31 and (d) gait speed. Weight distribution while bilateral standing For purpose of the present meta‐analysis all weight distribution data were put in comparable datasets. A homogeneous non‐significant SES was found for 3 studies (N=75), 2 RCTs26,27 and 1 CCT28 evaluating weight distribution with VFT in bilateral standing compared with conventional treatment (SES [fixed] 0.40; CI ‐0.06 to 0.86) (26‐28) (Figure 1). Winstein et al28 presented the weight distribution in percentage body weight on the paretic side. Grant et al26 and Sackley et al27 depicted the weight distribution data as a ratio of the paretic vs the non paretic limb. A post hoc sensitivity analysis for study

Effects of VFT on postural control in bilateral standing
99
design was performed. Subsequently, when the CCT of Winstein et al28 was excluded from the analysis the post hoc analysis resulted in a non‐significant SES between VFT in bilateral standing and conventional therapy (SES [fixed] 0.51; CI: ‐0.11 to 1.14).26,27 Figure 1. Meta‐analysis of visual feedback therapy (VFT) trials measuring outcomes of weight distribution and postural sway performance while bilateral standing
SES weight distribution N=75 (fixed effects model)
Winstein 1989 N=34 Grant 1997 N=16 Sackley 1997 N=25
0.26 [ 0.03 - 0.49] 0.24 [-0.24 - 0.74] 0.70 [ 0.37 - 1.02]
0.40 [-0.06 - 0.86]
Weight Distribution
SES postural sway (EO) N=148 (fixed effects model)
0.20 [-0.12 - 0.53]
0.47 [-0.03 - 0.97] 0.50 [ 0.27 - 0.74]-0.33 [-0.64 -(-0.01)]-0.05 [-0.29 - 0.20] 0.38 [ 0.19 - 0.58]
0 1
SES postural sway (EC) N=73(fixed effects model)
Walker 2000 N=32Chen 2002 N=41
-1 2-2Favours conventional therapy Favours VF therapy
0.36 [ 0.11 - 0.61] 0.22 [ 0.03 - 0.42]
0.28 [-0.18 - 0.75]
Postural Sway with eyes open (EO)
Postural Sway with eyes closed (EC)
Shumway-Cook 1988 N=16 Winstein 1989 N=34 Sackley 1997 N=25 Walker 2000 N=32 Chen 2002 N=41
Meta‐analysis of weight distribution between paretic and non paretic lower limb, postural sway with eyes open (EO) and postural sway with eyes closed (EC) in VFT vs conventional therapy. Effect sizes are based on Hedges’ g (and 95% confidence intervals). The middle of each bar represents the mean effect size, whereas the length of the bar reflects the 95% confidence interval. Bars to the right of the vertical line denote a positive effect for the VFT and vice versa. When the bar of an individual study crosses the vertical line at zero, no definite conclusions can be drawn in favour of the VF or conventional group. The summary effect sizes (SES) value represents the summarised effect size of all included studies.

Chapter 4
100
Postural sway while bilateral standing Postural sway was measured in two conditions: with eyes open and with eyes closed. Five studies (N=148), 4 RCTs8,12,23,27 and 1 CCT28, investigated the effects of VFT on postural sway in bilateral standing with eyes open. Two of these studies12,23 presented the postural sway (eyes open) in percentage (%) of the theoretic limits of stability and 2 studies27,28 presented this outcome in displacement values. Despite the differences regarding postural sway measurement, all data were included in the present meta‐analysis. After intervention a non‐significant heterogeneous SES was found for postural sway (eyes open) (SES [random] 0.20; CI: ‐0.12 to 0.53)8,12,23,27,28 (Figure 1). The data in the RCT of Shumway‐Cook and colleagues were presented in interquartile ranges and standard error measurements (SEM).8 The means of the pre‐ and post‐treatment data were analysed and SEM was converted to standard deviations (SD).16 Excluding the CCT of Winstein et al28 a post hoc sensitivity analysis for study design resulted in a non‐significant SES between VFT and conventional therapy (SES [fixed] 0.26; CI: ‐0.11 to 0.63).8,12,23,27
Two RCTs (N=73) measured the effects of VFT on postural sway with eyes closed in bilateral standing.12,23 In both studies the postural sway data were presented in percentage limits of stability. The meta‐analysis resulted in a non‐significant homogeneous SES for postural sway (eyes closed) in bilateral standing comparing VFT and conventional therapy (SES [fixed] 0.28; CI: ‐0.18 to 0.75)12,23 (Figure 1). Berg Balance Scale Two RCTs (N=45) evaluated the effects of VFT while bilateral standing on balance, measured with the BBS.11,12 A non‐significant homogeneous SES was found for BBS (SES [fixed] ‐0.20; CI: ‐0.79 to 0.39)11,12 (Figure 2). Timed Up & Go test The TUG is evaluated in 2 RCTs (N=44).11,12 The effects of VFT in bilateral standing on the outcome measure TUG are presented in Figure 2. A non‐significant homogeneous SES was found for TUG, when comparing VFT with conventional therapy (SES [fixed] ‐0.14; CI: ‐0.73 to 0.45).11,12 Gait speed Two studies (N=44), 1 RCT12 and 1 CCT28, evaluated the effects of VFT while bilateral standing on gait speed. A non‐significant heterogeneous SES was found for gait speed when comparing VFT with conventional therapy (SES [random] 0.08; CI: ‐0.97 to 1.14)12,28 (Figure 2).

Effects of VFT on postural control in bilateral standing
101
The balance and gait performance tests (BBS, TUG and gait speed) tended to favour the conventional treatment instead of the VFT, but without statistical significance. Figure 2. Meta‐analysis of visual feedback therapy (VFT) trials measuring outcomes of gait and gait‐related activities
SES berg balance scale N=45 (fixed effects model)
Walker 2000 N=32 Geiger 2001 N=13
-0.12 [-0.37 - 0.12] -0.39 [-1.01 - 0.22]
-0.20 [-0.79 - 0.39]
Berg Balance Scale
SES timed up & go test N=44 (fixed effects model)
-0.14 [-0.73- 0.45]
-0.12 [-0.36 - 0.13]-0.19 [-0.85 - 0.46]
0 1
SES gait speed N=72(random effects model)
Winstein 1989 N=40 Walker 2000 N=32
-1 2-2Favours conventional therapy Favours VF therapy
0.61 [ 0.41 - 0.81] -0.46 [-0.71 -(-0.22)]
0.08 [-0.97 - 1.14]
Timed Up & Go test
Gait Speed
Walker 2000 N=32 Geiger 2001 N=12
Meta‐analysis of the Berg Balance Scale, the Timed Up & Go test and gait speed in VFT vs conventional therapy. Effect sizes are based on Hedges’ g (and 95% confidence intervals(CI)). The middle of each bar represents the mean effect size, whereas the length of the bar reflects the 95% CI. Bars to the right of the vertical line denote a positive effect for the VFT and vice versa. When the bar of an individual study crosses the vertical line at zero, no definite conclusions can be drawn in favour of the VF or conventional group. The summary effect sizes (SES) value represents the summarised effect size of all included studies.

Chapter 4
102
Discussion: The present systematic review aims to estimate the effects of the additional value of VFT while bilateral standing on postural control, gait performance and gait‐related activities after stroke. This review shows, however, no significant effects in favour of VFT for (left‐right) symmetry of weight distribution in bilateral standing, postural sway, balance control measured with BBS, transfers and walking ability measured with TUG or gait speed. Despite differences between inclusion criteria and number of included studies, the findings presented in this systematic review correspond to a large extent with those of Barclay‐Goddard et al13 who reviewed studies that also included non‐stroke victims.
Improving symmetry of weight distribution while bilateral standing, is one of the main treatment goals in the rehabilitation of patients with stroke, acknowledging that the degree of asymmetric weight distribution during quiet standing is negatively associated with motor function and independence.7 Furthermore, the transfer of weight distribution is seen as an indicator for walking performance.9,32 It has been documented that patients with stroke shift 60% to 90% of the body weight to the non paretic limb.27,33,34 However, the question is how this asymmetry in weight distribution while standing is related to balance control and with that to the safety not to fall. For example, Kirker et al35 found that patients with stroke are more stable, while standing when they keep their postural control, as soon as the center of pressure is successfully shifted above the unaffected limb.35 This finding suggests that the asymmetrical stance of people with hemiparesis may be a compensatory strategy to overcome muscle weakness,36,37 delayed muscle activation,35,38 synergistic‐dependent activation patterns of muscles39 and existing perceptual deficits.40‐42 This assumption is also supported by Sackley,7 who noted that asymmetrical weight transfer does not necessarily imply that the subjects are more unstable and less able to control their balance in order to prevent falling. In other words, asymmetry does not necessarily imply a decreased postural control and higher risks for falling.43,44 Unfortunately, almost none of the studies, except Cheng et al, did measure the impact of VFT on the incidence of falling or near falling after stroke.24
The lack of evidence on postural control may also reflect the absence of valid outcome measures that represents more appropriate the strategy to obtain postural control while bilateral standing on two force plates. For example, De Haart et al45 stated that the speed (i.e., number of weight shifts) and imprecision (normalised average lateral displacement) by asking

Effects of VFT on postural control in bilateral standing
103
patients well‐controlled weight shifts in the frontal plane, could provide additional information about their improvement in balance control after stroke compared with the traditional measures of outcome. In addition, it might be hypothesised that in stroke patients different strategies are used for maintaining upright position during quiet bilateral standing.46 For example, stabilogram analysis revealed that delaying time intervals of open‐loop control mechanisms as well as inappropriate timing of descending commands to postural muscles, may be important factors that contribute to inappropriate displacements of the centre of pressure beyond the limits of safety.47 A further understanding of these changes, as well as the adaptive mechanisms underlying the functional (re)organisation of postural control is needed to conceptualise the effects of hemiplegia on postural instability in patients with stroke. Subsequently, new treatment programs need to be developed aiming to improve postural control in stroke in stead of restoring symmetry alone.
The present review also suggests that VFT failed to generalise to a better balance control while performing gait and gait‐related activities. These results are of great clinical value indicating that training of postural control should preferably be applied while performing the gait‐related tasks itself. It should be noted, however, that the Berg Balance Scale is sensitive to ceilings effects48 and may have prevented to find significant effects, for example in the study of Walker et al.12 Future studies are needed to investigate the relationship of patients preferred asymmetrical standing position on performance of gait and to establish how recovery of (left‐right) symmetry in standing balance is related to improvements of gait and gait‐related activities.
Unfortunately, in the present review not all outcomes could be pooled. For example, the ADL outcomes of Sackley & Lincoln27 and Chen et al (23) were too diverse to be pooled. The studies reported significant effects on the Nottingham 10 points ADL scale27 and FIMTM 23 that favoured VFT. One should notice that these positive effects are in contrast to the findings of the present meta‐analysis. However, only limited evidence could be attributed to the individual results of these studies. Additionally, the data of the Balance Master™ outcome ‘dynamic stability’ were not defined in the individual studies.23,24 As a consequence, it was unclear how to interpret these outcomes in terms of improvement in postural control.
The present review has a number of shortcomings. We may have missed relevant studies not published in scientific journals or published in other languages than English, German or Dutch. These shortcomings

Chapter 4
104
emphasise the need for more high‐quality and larger RCTs in stroke rehabilitation studies in the future. Acknowledgments and Funding We thank Hans (J.C.F.) Ket from the VU Medical Library for providing support for the literature search. Referenties 1. Hankey GJ, Warlow CP. Treatment and secondary prevention of stroke: evidence, costs,
and effects on individuals and populations. Lancet 1999; 354:1457‐1463.
2. Rijken PM, Dekker J. Clinical experience of rehabilitation therapists with chronic disease: a quantitative approach. Clin Rehabil 1998; 12:143‐150.
3. Tatemichi TK, Desmond DW, Stern Y et al. Cognitive impairment after stroke: frequency, patterns, and relationship to functional abilities. J Neurol Neurosurg Psychiatry 1994; 57:202‐207.
4. Yamamoto L, Magalong E. Outcome measures in stroke. Crit Care Nurs Q 2003; 26:283‐293.
5. Fong KN, Chan CC, Au DK. Relationship of motor and cognitive abilities to functional performance in stroke rehabilitation. Brain Inj 2001; 15:443‐453.
6. Pollock AS, Durward BR, Rowe PJ et al. What is balance? Clin Rehabil 2000; 14:402‐406.
7. Sackley CM. Falls, sway, and symmetry of weight‐bearing after stroke. Int Disabil Stud 1991; 13:1‐4.
8. Shumway‐Cook A, Anson D, Haller S. Postural sway biofeedback: its effect on reestablishing stance stability in hemiplegic patients. Arch Phys Med Rehabil 1988; 69:395‐400.
9. Goldie PA, Matyas TA, Evans OM et al. Maximum voluntary weight‐bearing by the affected and unaffected legs in standing following stroke. Clin Biomech (Bristol , Avon ) 1996; 11:333‐342.
10. Nichols DS. Balance retraining after stroke using force platform biofeedback. Phys Ther 1997; 77:553‐558.
11. Geiger RA, Allen JB, OʹKeefe J et al. Balance and mobility following stroke: effects of physical therapy interventions with and without biofeedback/forceplate training. Phys Ther 2001; 81:995‐1005.
12. Walker C, Brouwer BJ, Culham EG. Use of visual feedback in retraining balance following acute stroke. Phys Ther 2000; 80:886‐895.
13. Barclay‐Goddard R, Stevenson T, Poluha W et al. Force platform feedback for standing balance training after stroke. Cochrane Database Syst Rev 2004:CD004129.

Effects of VFT on postural control in bilateral standing
105
14. WHO. Stroke‐‐1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 1989; 20:1407‐1431.
15. Walker A. Thesaurus of Psychological Index Terms. 8th ed. American Psychological Association, 1997.
16. Alderson P, Green S, Higgins JPT. Cochrane Reviewersʹ Handbook 4.2.2. Available from: http://www.cochrane.org/resources/handbook/hbook.htm. [Cited 2004 18th of November].
17. PEDro. The Physiotherapy Evidence Database (PEDro). Available from: http://www.pedro.fhs.usyd.edu.au/ . [Cited 2004 18th of November].
18. Sherrington C, Herbert RD, Maher CG et al. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther 2000; 5:223‐226.
19. Hedges LV, Olkin I. Statistical methods for research synthesis. Orlando, Fla: Academic Press, Inc, 1985.
20. Hedges LV. Fixed effects models. In: Cooper LV, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation, 1994: 285‐300.
21. Shadish WR, Haddock CK. Combining estimates of effect size. In: Cooper HM, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation, 1994: 261‐282.
22. DerSimonian R, Laird N. Meta‐analysis in clinical trials. Control Clin Trials 1986; 7:177‐188.
23. Chen IC, Cheng PT, Chen CL et al. Effects of balance training on hemiplegic stroke patients. Chang Gung Med J 2002; 25:583‐590.
24. Cheng PT, Wang CM, Chung CY et al. Effects of visual feedback rhythmic weight‐shift training on hemiplegic stroke patients. Clin Rehabil 2004; 18:747‐753.
25. Engardt M, Ribbe T, Olsson E. Vertical ground reaction force feedback to enhance stroke patientsʹ symmetrical body‐weight distribution while rising/sitting down. Scand J Rehabil Med 1993; 25:41‐48.
26. Grant T, Brouwer BJ, Culham EG et al. Balance retraining following acute stroke: a comparison of two methods. Canadian Journal of Rehabilitation 1997; 11:69‐73.
27. Sackley CM, Lincoln NB. Single blind randomized controlled trial of visual feedback after stroke: effects on stance symmetry and function. Disabil Rehabil 1997; 19:536‐546.
28. Winstein CJ, Gardner ER, McNeal DR et al. Standing balance training: effect on balance and locomotion in hemiparetic adults. Arch Phys Med Rehabil 1989; 70:755‐762.
29. Berg K, Wood‐Dauphinee S, Williams JI et al. Measuring balance in the elderly: preliminary development of an instrument. Physiother Can 1989; 41:304‐311.
30. Berg K, Wood‐Dauphinee S, Williams JI. The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med 1995; 27:27‐36.
31. Podsiadlo D, Richardson S. The timed ʺUp & Goʺ: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39:142‐148.
32. Cheng PT, Liaw MY, Wong MK et al. The sit‐to‐stand movement in stroke patients and its correlation with falling. Arch Phys Med Rehabil 1998; 79:1043‐1046.

Chapter 4
106
33. Dickstein R, Nissan M, Pillar T et al. Foot‐ground pressure pattern of standing hemiplegic patients. Major characteristics and patterns of improvement. Phys Ther 1984; 64:19‐23.
34. Laufer Y, Dickstein R, Resnik S et al. Weight‐bearing shifts of hemiparetic and healthy adults upon stepping on stairs of various heights. Clin Rehabil 2000; 14:125‐129.
35. Kirker SG, Jenner JR, Simpson DS et al. Changing patterns of postural hip muscle activity during recovery from stroke. Clin Rehabil 2000; 14:618‐626.
36. Dickstein R, Shefi S, Marcovitz E et al. Anticipatory postural adjustment in selected trunk muscles in post stroke hemiparetic patients. Arch Phys Med Rehabil 2004; 85:261‐267.
37. Hamrin E. II. Early activation in stroke: does it make a difference? Scand J Rehabil Med 1982; 14:101‐109.
38. Diener HC, Bacher M, Guschlbauer B et al. The coordination of posture and voluntary movement in patients with hemiparesis. J Neurol 1993; 240:161‐167.
39. Di Fabio RP, Badke MB, Duncan PW. Adapting human postural reflexes following localized cerebrovascular lesion: analysis of bilateral long latency responses. Brain Res 1986; 363:257‐264.
40. Eng JJ, Chu KS. Reliability and comparison of weight‐bearing ability during standing tasks for individuals with chronic stroke. Arch Phys Med Rehabil 2002; 83:1138‐1144.
41. Garland SJ, Willems DA, Ivanova TD et al. Recovery of standing balance and functional mobility after stroke. Arch Phys Med Rehabil 2003; 84:1753‐1759.
42. Yelnik AP, Lebreton FO, Bonan IV et al. Perception of verticality after recent cerebral hemispheric stroke. Stroke 2002; 33:2247‐2253.
43. Geurts AC, Nienhuis B, Mulder TW. Intrasubject variability of selected force‐platform parameters in the quantification of postural control. Arch Phys Med Rehabil 1993; 74:1144‐1150.
44. Panzer VP, Bandinelli S, Hallett M. Biomechanical assessment of quiet standing and changes associated with aging. Arch Phys Med Rehabil 1995; 76:151‐157.
45. de Haart M, Geurts AC, Dault MC et al. Restoration of weight‐shifting capacity in patients with postacute stroke: a rehabilitation cohort study. Arch Phys Med Rehabil 2005; 86:755‐762.
46. Collins JJ, De Luca CJ. Open‐loop and closed‐loop control of posture: a random‐walk analysis of center‐of‐pressure trajectories. Exp Brain Res 1993; 95:308‐318.
47. Collins JJ, De Luca CJ, Pavlik AE et al. The effects of spaceflight on open‐loop and closed‐loop postural control mechanisms: human neurovestibular studies on SLS‐2. Exp Brain Res 1995; 107:145‐150.
48. Mao HF, Hsueh IP, Tang PF et al. Analysis and comparison of the psychometric properties of three balance measures for stroke patients. Stroke 2002; 33:1022‐1027

CHAPTER
The development of a clinical practice stroke
guideline for physiotherapists in The Netherlands:
A systematic review of available evidence
Roland PS Van Peppen
Erik JM Hendriks
Nico LU Van Meeteren
Paul JM Helders
Gert Kwakkel
Disability and Rehabilitation 2007; 29(10): 767‐783

Chapter 5
108
Abstract Purpose: To develop a clinical practice guideline for the physiotherapy management of patients with stroke, as support for the clinical decision‐making process, especially with respect to the selection of appropriate interventions, prognostic factors and outcome measures. Introduction: Physiotherapists have a high caseload of patients with stroke, so there is a need to identify effective evidence‐based physiotherapy procedures. The availability of a guideline that includes information about prognostic factors, interventions, and outcome measures would facilitate clinical decision‐making. Method: A systematic computerised literature search was performed to identify evidence concerning the use of: 1) prognostic factors related to functional recovery; 2) physiotherapy interventions in patients with stroke; and 3) outcome measures to assess patients’ progress in functional health. Experts, physiotherapists working in the field of stroke rehabilitation, and a multidisciplinary group of health professionals reviewed the clinical applicability and feasibility of the recommendations for clinical practice and their comments were used to compose the definitive guideline. Results: Of 9482 relevant articles, 322 were selected. These were screened for methodological quality. Seventy‐two recommendations for clinical practice were retrieved from these articles and included in the guideline: 6 recommendations concerned the prediction of functional recovery of activities of daily living (ADL), including walking ability and hand/arm use; 65 recommendations concerned the choice of physiotherapy interventions; and 1 recommendation concerned the choice of outcome instruments to use. A core set of seven reliable, responsive, and valid outcome measures was established, to determine impairments and activity limitations in patients with stroke. Conclusions: The guideline provides physiotherapists with an evidence‐based instrument to assist them in their clinical decision making regarding patients with stroke. As most of the recommendations included in the guideline came from studies of patients in the post acute and chronic phase of stroke, and in general involved patients with less severe and uncomplicated stroke, more needs to be learned about the more complex cases. Key Words: clinical practice guideline, physiotherapy, rehabilitation, stroke, prognostic factors, interventions, outcome measures

Clinical practice stroke guideline for physiotherapists
109
Introduction Stroke is a major health problem with high societal costs due to its increasing prevalence and the long‐term disability it causes. In the Netherlands, the incidence of cerebrovascular disorders is estimated at 34,500 (~2.2/1000/year) and the prevalence at 190,000 (~1.2% of Dutch population), and nowadays more patients are admitted to hospital (admission for stroke has increased from 22,717 in 1980 to 32,623 in 2003).1 It is intrinsic to health care to continuously look for evidence‐based rehabilitation services. Recently, the ‘best evidence’ for stroke management, derived from methodologically sound clinical research, has been collected in systematic reviews and converted into several multidisciplinary stroke guidelines.2‐6 However, physiotherapists would probably prefer to have more detailed information about making a valid functional prognosis, designing the most effective intervention program, and selecting the most appropriate measures to evaluate outcome, to facilitate clinical decision making in each individual patient in line with his or her specific functional health status.7 As yet, there are no specific guidelines for physiotherapy in the management of stroke, even though physiotherapy accounts for a substantial proportion of the total therapy time provided by stroke rehabilitation services.8,9
The aim of the present article was to describe the available evidence to guide the clinical decision‐making process of physiotherapists dealing with the rehabilitation of patients with stroke regarding: 1) the best determinants of the ultimate functional recovery of patients diagnosed with stroke; b) the effectiveness of applicable physiotherapy interventions; and c) a core set of reliable, valid, and responsive outcome measures to assess patients’ progress in functional health at fixed moments after stroke. This evidence is presented as the Clinical Practice Guideline on Physiotherapy management of patients with Stroke (CPGPS) in the Netherlands.10 Method Development of guideline A systematic literature search was conducted to determine evidence (i.e., the ‘state of the art’) for three aspects of the physiotherapy management of patients with stroke: 1) prognostics; 2) interventions; and 3) outcomes. Subsequently, the methodological quality of the included studies was investigated. Levels of evidence were determined on the basis of the ‘best evidence’ from systematic reviews, randomised controlled trials (RCTs), controlled clinical trials (CCTs), and pre‐experimental studies. The best

Chapter 5
110
evidence was then converted into graded recommendations for clinical practice. Figure 1 Flow chart concerning the selection and grading of the available evidence of each therapeutic intervention in the CPGPS
Clinical PracticeGuideline
Physiotherapy Stroke(CPGPS)
Systematicreviews or> 2 RCTs
1 RCT or> 2 controlled
clinical trials (CCTs)
Pre-experimental
studies
Description ofphysiotherapy
-relatedintervention
Systematicliterature-
search
Quantitativeanalysis of
effect
Analysis ofmethodological
quality
Levelsof
evidence
Advice to evaluate the applied intervention withspecific outcome measures
Recommendations for everyday clinical practice
Summarisedeffect sizes-Hedges' g-
PhysiotherapyEvidence Database
-PEDro-
Level CLevel A1+A2 Level B
Grade 3Grade 1 Grade 2
1-generic priciples of rehabilitation2-walking & mobility-realed activities3-hand and arm use4-generic Activities of Daily Living
Figure 1 shows how the recommendations for physiotherapy‐related interventions were developed. Recommendations for each intervention were based on: 1) description of the intervention; 2) systematic literature search; 3) analysis of methodological quality of the studies, according to the PEDro scale11; 4) quantitative analysis of the effects of the individual studies, and, if the studies were comparable with respect to type of intervention and measurement of outcome (for methods see Chapter 2)12; 5) levels of evidence based on evidence from the literature; 6) formulation of recommendations for using the described intervention in clinical practice; and 7) advice regarding the use of valid, reliable, and responsive outcome measures to

Clinical practice stroke guideline for physiotherapists
111
describe the functional health status of patients with stroke and to evaluate the effects of a physiotherapy intervention. The interventions are described in terms of general principles of rehabilitation, walking and mobility‐related activities, hand and arm use, and activities of daily living (ADL). Participants in development process of CPGPS Seven groups of participants contributed to the development of the guidelines during the development period March 2002 to March 2004: 1) The board of the Royal Dutch Society for Physical Therapy (Koninklijk Nederlands Genootschap voor Fysiotherapie: KNGF), which initiated the development of the guideline and approved the definitive version. 2) The Department of Physical Therapy of the VU University Medical Center (VUmc) in Amsterdam, the Netherlands, which developed the guideline and formed a steering committee and task group. 3) A steering committee (N=5), which planned and coordinated the activities of the task group. 4) A task group (GK and RPSvP), which developed the format of the guideline; wrote the draft versions; invited the expert group, multiprofessional group, and pilot group to comment on these draft versions of the guideline; and wrote the definitive version of the CPGPS. 5) An expert group (N=8), consisting of clinical experts, especially on stroke, who commented on the guideline or parts of it during its development, assessed the draft versions of the guideline and its applicability in daily physiotherapy practice. The experts were all physiotherapists experienced in stroke rehabilitation, representative for Dutch institutions treating stroke patients. 6) A pilot group, consisting of randomly selected physiotherapists (N=169), who tested and commented on the draft version of the outcome measures and their applicability. Their comments, together with information on the clinical utility and overlap of the outcome measures, were used to develop the final version of the outcome measures. 7) A multiprofessional group (N=9), consisting of clinicians from various specialties providing care in this setting (neurologist, rehabilitation physician, general practitioner, nursing home doctor, geriatrician, psychologist, (district) nurse, occupational therapist, and speech therapist) and a patient representative of the Dutch Stroke Association, assessed the quality of the final draft version, and its applicability to everyday clinical practice. They also determined whether the physiotherapy guideline conflicted with the recommendations of their own disciplinary guidelines.2,3

Chapter 5
112
Definitions Stroke was defined according to the World Health Organization as ‘a clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hours or leading to death, with no apparent causes other than of vascular origin’.13 Three phases of stroke were identified, namely, acute/sub‐acute, post acute, and chronic phase. The acute phase of stroke was considered to be the first week after stroke onset, the sub‐acute phase from the 2nd to the 4th week after stroke, and the post acute phase from the 2nd to 6th month after stroke. The chronic phase started 6 months after stroke.12 Physiotherapy was defined as the skilled use of physical interventions (in contrast to medical or surgical treatments) to restore physical functioning and to improve activity and participation in daily‐life situations after injury or disease.4 Physiotherapy interventions for patients with stroke commonly include exercise therapy, neuromuscular electrical stimulation, mechanical devices, such as balance trainers and treadmills, as well as assistive devices (canes and walkers) along with instructions for their proper use. Literature Search An extensive computerised search of the Dutch, English, or German literature included in the MEDLINE (1966 through January 2004), CINAHL (1982 through January 2004), and EMBASE databases (1988 through January 2004), Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews (The Cochrane Library, Issue 4, 2003), DocOnline (Database of the Dutch Institute of Allied Health Care) (1987 through January 2004) and PEDro (January 2004) was conducted, using the keywords ‘cerebrovascular disorders’, ‘cerebrovascular accident’, ‘stroke’, ‘hemiplegia’, and ‘rehabilitation’. Two researchers (GK and RPSvP) independently searched these electronic databases for relevant articles. The bibliographies of review articles and narrative reviews, and the abstracts of conferences were also screened. In addition, the references of the retrieved studies were reviewed. Inclusion of articles was based on agreement between the two independent reviewers. This search strategy was the core search which served as the basis for further refinement according to the three topics: prognostic factors, physiotherapy‐related interventions and outcome measures. Prognostic factors To determine prognostic factors, the following keywords were used: ’prognostic factors’, ‘prognosis’, ‘prediction’, ‘functional outcome’, ‘outcome

Clinical practice stroke guideline for physiotherapists
113
assessment’, and ‘follow‐up’. Factors were included if they fulfilled the following three selection criteria: (1) the prognostic factors were described to affect the functional outcome of patients with stroke; (2) the prognostic factors were correlated with walking ability, hand and arm use, or ADL; and (3) the study was a systematic review or meta‐analysis. Quality assessment of studies of prognostic factors was based on 11 criteria for methodological quality for prognostic research.14,15 (Table 1) Table 1 – Criteria used to assign levels of evidence to studies on prognostic factors.14,15 Level of scientific evidence for studies on prognostic factors
I Studies that satisfy all items for internal and statistical validity (> 8 points)
II Studies that satisfy all items for internal validity (> 5 points)
III Studies that do not satisfy all items for internal validity Level of scientific evidence of the systematic reviews on prognostic factors
A Systematic reviews (meta-analyses) that include at least 5 studies at quality level I, which investigate the same prognostic factor
B Systematic reviews (meta-analyses) that include at least 3 studies at quality level I, which investigate the same prognostic factor
C Systematic reviews (meta-analyses) that include at least 2 studies at quality level I, II, or III, which investigate the same prognostic factor
Grades of recommendation of the studies on prognostic factors
1 Supported by research at level A
2 Supported by research at level B
3 Supported by research at level C
Physiotherapy‐related interventions The following keywords and MeSH were used to identify the interventions: ‘physiotherapy’, ‘physical therapy’, ‘exercise therapy’, ‘electrotherapy’, and ‘occupational therapy’. Systematic reviews (SR), randomised and controlled clinical trials (RCTs and CCTs), and (non‐controlled) pre‐experimental studies were included for review. Studies that investigated robotics or the effects of physiotherapy in combination with acupuncture or drug therapies were excluded.
Articles were considered relevant and selected if the study population included adults of 18 years or older, diagnosed with stroke, and

Chapter 5
114
the study evaluated the effectiveness of physiotherapy‐related interventions. The quality of the studies was assessed with the PEDro criteria11 for methodological quality and the levels of evidence were based on the criteria of Sackett et al.7 (Table 2) Table 2 – Criteria used to assign levels of evidence to intervention studies.7 Level of scientific evidence to intervention studies
A1 Systematic reviews (meta-analyses) that include at least 2 or more RCTs at quality level A2, which show consistent results between studies
A2 At least 2 RCTs of a good methodological quality (PEDro-score > 4 points) with sufficient power and consistency
B At least 2 RCTs of a moderate methodological quality (PEDro-score < 3 points) or with insufficient power, or at least 2 CCTs, or one RCT with PEDro-score > 4 points
C Pre-experimental studies
D Expert opinion*
Grades of recommendation to intervention studies
1 Supported by one systematic review al level A1 or at least 2 independent trials at level A2
2 Supported by research at level B
3 Supported by research at level C
4 Not supported by research; based on expert opinion*
CCT indicates controlled clinical trial; PEDro, physiotherapy evidence database; RCT, randomised controlled trial * In contrast to other guidelines, no recommendations of grade 4 were entered in the CPGPS. The grade 4 recommendations were recently established in the Dutch multidisciplinary guidelines for stroke rehabilitation.3
Outcome measures The following keywords were used to identify outcome measures: ’measurement’, ‘measure’, ‘assessment’, ‘instrument’, ‘scale’, ‘test’, ‘questionnaire’, ‘classification’, ‘evaluation’, and ‘outcome’. The following keywords were used to determine the quality of the outcome measures: ‘reliability’, ‘validity’, and ‘responsiveness’.
For inclusion in the analysis, the outcome measures needed to be consistent with the International Classification of Functioning, Disability and Health (ICF)16; to show high‐level psychometric properties, i.e., reliability (inter‐ and intra rater), validity and responsiveness17 in studies with adult

Clinical practice stroke guideline for physiotherapists
115
stroke patients, and to have good clinical utility (easy and quick to administer) (Table 3); to minimally overlap each other; and to be consistent with current physiotherapy practice. Excluded were outcome measures that evaluated the cognitive impairments of stroke patients. Quality assessment of outcome measures was based on the criteria for outcome measures formulated by Bot et al.18 (Table 3) Table 3 – Criteria used to assign levels of evidence to outcome measures.18 Level of scientific evidence for outcome measures
A
6 criteria: - Validated in a stroke patient population:
0 = no; 1 = yes - Test-retest reliability:
0 = ICC < 0.69; 1 = ICC > 0.70 - Concurrent validity, Spearman rho (rs) or Pearson correlationcoefficient:
0 = r < 0.69; 1 = r > 0.70 - Responsiveness:
0 = low; 1 = high - Clinical use:
0 = time to administer > 16 minutes, and 1 = time to administer < 15 minutes
- Test-protocol: 0 = test-protocol not available; 1 = test-protocol available
B Meets 5 of the level A criteria
C Meets 3 or 4 of the level A criteria
D Meets 1 or 2 of the level A criteria
Grades of recommendation for outcome measures
1 Supported by research at level A
2 Supported by research at level B
3 Supported by research at level C
4 Supported by research at level D
ICC indicates intra class correlation coefficient; SDD, smallest detectable difference

Chapter 5
116
Results Evidence to be included in the guideline In total 322 articles (out of 9482 citations) were used to establish the content of the guideline: Six studies14,15,19‐22 to establish prognostic factors to predict functional recovery in patients with stroke; 284 studies to establish physiotherapy interventions for stroke rehabilitation (for references: see10); and 32 studies23‐54 to establish outcome measures to assess patient progress. In total, 72 possible guideline elements were identified: 6 relevant to prognostic factors, 65 relevant to physiotherapy interventions, and 1 relevant to outcome measures (Table 4). Table 4 Summary of 72 recommendations of the CPGPS: Type of intervention and corresponding grade of recommendation
nr. Type of intervention Grade# nr. Type of intervention Grade#
Prognostic factors (grades of recommendation refer to criteria in Table 1)
36 Functional electro stimulation (paretic leg)
1*
1 Prognosis walking ability 3 37 Biofeedback to the paretic lower limb
1*
2 Prognosis dexterity paretic arm in first 4 weeks after onset stroke
3 38 Applying Ankle-Foot-Orthosis 2
3 Prognostic factor arm: paretic leg 3 39 Using walking aids 3*
4 Prognostic factor arm: Barthel index 3* 40 Limb loading 2*
5 Prognosis ADL 3 41 External auditory rhythms 2
6 Prognosis recovery of sequence in ADL
3 42 Therapeutic positioning paretic arm
2
Physiotherapy-related interventions (grades of recommendation refer to criteria in Table 2)
43 Stretching paretic wrist and fingers
2
7 Treatment in stroke teams (stroke unit)
1 44 Immobilisation techniques (arm/hand)
2
8 Incorporating stroke unit in stroke service
3 45 Sensory training paretic arm and hand
3
9 Adherence to evidence-based guidelines
3 46 Using air-splints 2
10 Intensity of exercise therapy 1 47 Wrapping paretic arm 3
11 Task-specific training 1 48 Exercise training the paretic arm 1*
12 Context-specific training 1 49 Bilateral training cyclic arm movements
3
13 Neurological treatment approaches 1* 50 Constraint-induced movement therapy: dexterity
1
14 Treating with basic principles of the NDT-concept
3** 51 Constraint-induced movement therapy: somatosensory deficits
1
15 Motor learning (variation and repetition-without-repetition)
3 52NMS of the paretic forearm without EMG-triggering: muscle strength and ROM
3

Clinical practice stroke guideline for physiotherapists
117
Table 4 - Continued -
nr. Type of intervention Grade# nr. Type of intervention Grade#
16 Early start of rehabilitation (within 72 hours after onset stroke)
3 53NMS of the paretic forearm: dexterity (absence of active wrist and finger extension)
2*
17 Positioning paretic site in bed 3* 54NMS of the paretic forearm: dexterity (with active wrist and finger extension)
2
18 Prevention decubitus 3 55 NMS of the paretic forearm with EMG-triggering
2
19 Prevention of broncho-pneumonia 3 56 Biofeedback to the paretic upper limb
1*
20 Pulmonal ventilation 3 57 TENS paretic arm 1
21 (Assistive) active movements 3 58 NMS for GHS and HSP 1
22 Prevention deep venous thrombosis 3 59 Exercises for reducing HSP 1*
23 Informing partner of patient 3 60 Shoulder exercises with pulleys in HSP
3**
24 Training sitting balance 1 61Treatment of hand oedema: intermittent pneumatic compression
2*
25 Asymmetric wheelchair self-propelling
2* 62 Treatment of hand oedema: other treatments
3*
26 Using paretic hand during wheelchair propelling
3 63 Mirror therapy paretic arm 2
27 Training transfers from sit-to-stand and visa versa
1 64 Slings and supportive devices for reducing GHS and HSP
3
28 Preventing falls during standing up and sitting down
2 65 Strapping techniques for reducing GHS and HSP
3
29 Training standing balance on force plates
1 66 Strategy training for apraxia 2
30 (Functional) strengthening paretic muscles
1 67 Training leisure activities 1*
31 Strengthening paretic leg and spasticity
2* 68 Training attention deficits 1
32 Aerobics (combination of strength- and endurance training)
3 69 Training memory deficits 1*
33 Body-weight supported treadmill training
1 70 Neglect: visual scanning training 1
34 Treadmill training without body weight support and walking ability
1 71 Visual scanning training: prism glasses
2
35 Treadmill training without body weight support and gait speed
2 Outcome measures (grades of recommendation refer to criteria in Table 3)
72 Monitoring outcomes (systematically)
3
* No or insufficient evidence was found for this intervention; ** Negative effect was found for this intervention ADL indicates activities of daily living; CPGPS, clinical practice guideline on physiotherapy management of patients with stroke; EMG, electromyogram; HSP, hemiplegic shoulder pain; GHS, glenohumeral subluxation; Grade#, grade of recommendation; NDT, neurodevelopmental treatment; NMS, neuromuscular stimulation; nr., number of recommendation of CPGPS; ROM, range of motion; TENS, transcutaneous electrical nerve stimulation.

Chapter 5
118
Prognostic factors of functional recovery The identification of prognostic factors was based on six systematic reviews.14,15,19‐22 Walking ability A number of factors to predict walking ability (defined in the guideline as regaining a Functional Ambulation Categories score > 4) at 6 months after stroke were identified. The best explanatory factors were initial walking ability in the first 2 weeks after stroke, degree of motor paresis of the paretic leg, homonymous hemianopia, sitting balance, urinary incontinence, high age, initial functioning (activities of daily living; ADL) in first 2 weeks after stroke14 (Grade 3 evidence). These factors were generally similar to those predicting ADL 6 months after stroke. Activities of Daily Living (ADL) The best predictor of recovery of independence in ADL at 6 months after stroke was the Barthel Index score in the first 2 weeks after stroke. Other predictors were urine incontinence in the first 2 weeks after stroke, level of consciousness in the first 48 hours after stroke, high age, status following recurrent stroke, degree of motor paresis, sitting balance in the first 2 weeks after stroke, orientation in time and place, and level of perceived social support14,15 (Grade 3 evidence). Hand and arm use The dexterity of the hemiplegic arm can best be predicted within 4 weeks after stroke.55 The best clinical predictor of recovery of dexterity of the paretic arm 6 months after stroke was severity of arm paresis at 4 weeks after stroke, as assessed with the Fugl‐Meyer Assessment.55 Other strong predictors of recovery of dexterity after stroke were severity of the upper extremity paresis, voluntary grip function of the hemiplegic arm37,56 or voluntary extension movements of the hemiplegic’s wrist and fingers57 within the first 4 weeks after stroke, and muscle strength of the paretic leg55 (Grade 3 evidence). By using these prognostic factors in an early stage of rehabilitation, physiotherapists should be able to predict the functional outcome of their patients 6 months after stroke58 (Grade 3 evidence). An example of a model to predict the recovery of walking ability after stroke is given in Box 1.

Clinical practice stroke guideline for physiotherapists
119
Box 1. An example of using outcome measures to predict functional recovery after stroke Kwakkel93 developed a model to predict the degree of walking ability, as measured with the Functional Ambulation Categories (FAC), 6 months after stroke, using the initial Barthel Index (BI) score at 2 weeks after stroke in a linear regression model: FAC = 1.860 + (0.03*(BI*5)) + (1.236*SB), where sitting balance (SB) is defined as ability to maintain sitting balance for minimally 30 seconds without support (score = 1 indicates maintaining SB is possible; score = 0, maintaining SB is not possible). As an example, a stroke patient has a BI score of 5 points 2 weeks after stroke, then the FAC score at 6 months would be calculated as follows: FAC = 1.860 + (0.03*25) + (1.236*1) = 3.846
Physiotherapy interventions The choice of physiotherapy interventions to include in the guideline was in part based on a recent review of the efficacy of physiotherapy interventions on functional outcome in stroke patients (see Chapter 2).10,12 The literature search identified 284 relevant studies (25 SR, 16 critical reviews, 153 RCTs, 49 CCTs, and 41 pre‐experimental studies).10 We used PICO search questions (Patient, Intervention, Comparison, and Outcome)7 to identify 46 relevant physiotherapy interventions, as outlined in Figure 1.10 An example of a PICO question is: “What is the evidence for constraint‐induced movement therapy compared to regular arm/hand therapy on dexterity of the paretic arm in patients with stroke?” (Table 5). We grouped these interventions as being consistent with the general principles of rehabilitation, or as influencing walking and mobility‐related activities, hand and arm use, and generic ADL.
We included 65 recommendations/interventions in the guideline, 24 of grade 1 evidence (Table 5); 18 of grade 2 evidence10, and 23 of grade 3 evidence10. In this way, the guideline recommends task‐oriented and context‐specific exercise training, in particular when applied intensively and early after stroke onset (Grade 1 evidence). The interventions/recommendations (together with the level of evidence) are given in Table 4.12

Chapter 5
120
Out
com
e
…is
effe
ctiv
e fo
r…
...in
crea
sing
sur
viva
l, de
crea
sing
leng
th o
f sta
y an
d in
crea
sing
AD
L-in
depe
nden
cy in
the
(sub
)acu
te
phas
e af
ter s
troke
.
…in
crea
sing
the
rate
of r
ecov
ery
of A
DL
in th
e (s
ub)a
cute
and
pos
tacu
te p
hase
afte
r stro
ke.
…in
crea
sing
the
train
ed ta
sk in
the
(sub
)acu
te,
post
acut
e an
d ch
roni
c ph
ase
afte
r stro
ke;
gene
ralis
abili
ty to
oth
er tr
aine
d ta
sks
is h
ardl
y fo
und.
…in
crea
sing
the
effe
ctiv
enes
s of
task
-lear
ning
in th
e (s
ub)a
cute
, pos
tacu
te a
nd c
hron
ic p
hase
afte
r st
roke
.
…is
not
effe
ctiv
e on
out
com
es a
t act
ivity
-leve
l.
…in
crea
sing
the
sitti
ng b
alan
ce.
…in
crea
sing
the
sym
met
ric w
eigh
t-bea
ring
durin
g st
andi
ng-u
p an
d si
tting
-dow
n be
twee
n th
e 2
legs
, an
d th
e sp
eed
of th
ese
trans
fers
in th
e po
stac
ute
and
chro
nic
phas
e af
ter s
troke
.
…in
crea
sing
sym
met
rical
wei
ght-b
earin
g be
twee
n bo
th le
gs w
hile
bila
tera
l sta
ndin
g in
the
post
acut
e ph
ase
afte
r stro
ke. U
ncle
ar if
effe
cts
will
gene
ralis
e to
bet
ter w
alki
ng a
bilit
y.
Com
paris
on
…co
mpa
red
to…
…co
nven
tiona
l
reha
bilit
atio
n se
tting
s…
…re
gula
r tim
e sp
ent i
n re
habi
litat
ion…
…th
e no
t-tra
ined
ta
sks…
…tra
inin
g in
a n
ot-w
ell
know
n co
ntex
t…
…an
othe
r spe
cific
ne
urol
ogic
al tr
eatm
ent
appr
oach
(suc
h as
ND
T,
PN
F, M
RP
, Bru
nnst
rom
et
cete
ra)…
–
– …co
nven
tiona
l sta
ndin
g ba
lanc
e tra
inin
g…
Inte
rven
tion
…th
e ef
fect
iven
ess
of…
…m
ultid
isci
plin
ary
inte
rven
tions
in s
troke
-un
its…
…au
gmen
ted
exer
cise
th
erap
y tim
e sp
ent i
n th
e fir
st 6
mon
ths
afte
r stro
ke…
…ta
sks
dire
ctly
trai
ned
(suc
h as
trai
ning
bal
ance
in
stan
ding
pos
ition
)…
…tra
inin
g in
a w
ell-k
now
n co
ntex
t…
…on
e sp
ecifi
c ne
urol
ogic
al
treat
men
t app
roac
h (s
uch
as N
DT,
PN
F, M
RP
, B
runn
stro
m e
tcet
era)
…
…re
achi
ng w
ith th
e pa
retic
ar
m, w
hile
sitt
ing,
with
the
arm
reac
hing
out
side
the
bear
ing
surfa
ce…
…tra
inin
g sy
mm
etric
ally
st
andi
ng u
p an
d si
tting
do
wn…
…ad
ditio
nal t
rain
ing
of
stan
ding
bal
ance
on
forc
e pl
ates
with
vis
ual f
eedb
ack
whi
le b
ilate
ral s
tand
ing…
Patie
nts
In p
atie
nts
w
ith s
trok
e…
Tab
le 5
T
he 2
4 ‘G
rade
1’-r
ecom
men
datio
ns o
f int
erve
ntio
n st
udie
s (le
vel A
evi
denc
e), i
n de
tail
desc
ribed
in th
e C
PG
PS10
PI
CO
1.
Gen
eric
prin
cipl
es:
Wor
king
in s
troke
team
s
2.
Gen
eric
prin
cipl
es:
Inte
nsity
of e
xerc
ise
train
ing
3.
Gen
eric
prin
cipl
es:
Task
- spe
cific
trai
ning
4.
Gen
eric
prin
cipl
es:
Con
text
- spe
cific
trai
ning
5.
Gen
eric
prin
cipl
es:
Neu
rolo
gica
l tre
atm
ent a
ppro
ache
s
6.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: S
ittin
g ba
lanc
e
7.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: S
tand
ing
up a
nd s
ittin
g do
wn
8.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: S
tand
ing
bala
nce
on fo
rce
plat
es

Clinical practice stroke guideline for physiotherapists
121
Out
com
e
…is
effe
ctiv
e fo
r…
…in
crea
sing
mus
cle
stre
ngth
of t
he p
aret
ic le
g an
d in
crea
sing
gai
t spe
ed in
the
post
acut
e an
d ch
roni
c ph
ase
afte
r stro
ke.
…in
crea
sing
end
uran
ce.
…in
crea
sing
wal
king
abi
lity
in th
e po
stac
ute
phas
e af
ter s
troke
.
…is
not
effe
ctiv
e in
on
gait
spee
d an
d w
alki
ng
abili
ty.
…is
not
effe
ctiv
e on
RO
M o
f the
dor
sifle
xion
of t
he
pare
tic a
nkle
and
gai
t spe
ed.
…is
not
effe
ctiv
e fo
r fas
ter r
ecov
ery
of th
e de
xter
ity
the
pare
tic a
rm.
…in
crea
sing
dex
terit
y of
the
pare
tic a
rm. T
he e
ffect
ca
n be
incr
ease
d on
beh
alf o
f the
incr
easi
ng
train
ings
inte
nsity
of C
IMT.
Com
paris
on
…co
mpa
red
to…
– – – – – … a
noth
er s
peci
fic
neur
olog
ical
trea
tmen
t ap
proa
ch…
–
Inte
rven
tion
…th
e ef
fect
iven
ess
of…
…(fu
nctio
nal)
stre
ngth
tra
inin
g of
the
pare
tic le
g (u
sing
fitn
ess-
appa
ratu
s of
fu
nctio
nal t
rain
ing)
, 2 to
3
times
a w
eek…
…B
WS
TT (<
40%
bod
y-w
eigh
t sup
port)
in s
troke
pa
tient
s w
ho c
anno
t wal
k in
th
e fir
st 6
wee
ks a
fter
stro
ke a
nd d
ecre
ased
ph
ysic
al c
ondi
tion…
…in
tens
ive
tread
mill
train
ing
with
out b
ody-
wei
ght
supp
ort i
n pa
tient
s w
ith a
de
crea
sed
wal
king
abi
lity…
…FE
S o
n th
e pa
retic
leg…
.
…bi
ofee
dbac
k to
the
dors
iflex
ion
mus
cles
of t
he
pare
tic lo
wer
lim
b du
ring
gait…
…ex
erci
se tr
aini
ng o
f the
pa
retic
upp
er li
mb
base
d on
a
spec
ific
neur
olog
ical
tre
atm
ent a
ppro
ach…
…co
nstra
int-i
nduc
ed
mov
emen
t the
rapy
(=
forc
ed u
se) i
n co
mbi
natio
n w
ith a
n in
tens
ive
func
tiona
l tra
inin
g pr
ogra
m in
pat
ient
s w
ith a
ctiv
e w
rist e
xten
sion
(2
0 de
gree
s) a
nd fi
nger
ex
tens
ion
(10
degr
ees)
…
Patie
nts
In p
atie
nts
w
ith s
trok
e…
Tab
le 5
-
Con
tinue
d -
PIC
O
9.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: S
treng
th tr
aini
ng p
aret
ic le
g
10.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: B
WS
TT
11.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: Tr
eadm
ill tra
inin
g w
ithou
t bod
y-w
eigh
t su
ppor
t
12.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: FE
S (p
aret
ic le
g)
13.
Wal
king
and
mob
ility-
rela
ted
activ
ities
: B
iofe
edba
ck to
the
pare
tic lo
wer
lim
b
14.
Han
d an
d ar
m u
se:
Exe
rcis
e tra
inin
g th
e pa
retic
arm
15.
Han
d an
d ar
m u
se:
CIM
T

Chapter 5
122
Out
com
e
…is
effe
ctiv
e fo
r…
…is
mor
e ef
fect
ive
in p
atie
nts
with
som
atos
enso
ry
defic
its.
…is
not
effe
ctiv
e on
act
ive
RO
M a
nd m
uscl
e st
reng
th o
f the
par
etic
arm
.
…de
crea
sing
spa
stic
ity in
the
post
acut
e ph
ase
afte
r st
roke
, but
the
effe
cts
will
not
gen
eral
ise
to b
ette
r de
xter
ity.
…in
crea
sing
pas
sive
RO
M o
f lat
eral
rota
tion
of th
e pa
retic
sho
ulde
r (13
deg
rees
) and
redu
cing
the
glen
ohum
eral
sub
luxa
tion
(5 m
m) i
n th
e (s
ub)a
cute
an
d po
stac
ute
phas
e af
ter s
troke
. How
ever
thes
e ef
fect
s ar
e te
mpo
rary
. NM
S d
oesn
’t re
sult
in a
re
duct
ion
of th
e he
mip
legi
c sh
ould
er p
ain.
…is
not
mor
e ef
fect
ive
to o
ther
phy
siot
hera
py
inte
rven
tions
aim
ed a
t red
ucin
g he
mip
legi
c sh
ould
er
pain
.
…in
crea
sing
AD
L-in
depe
nden
cy, p
artic
ipat
ion
in
leis
ure
activ
ities
, and
moo
d of
the
patie
nt.
…in
crea
sing
ale
rtnes
s an
d su
stai
ned
atte
ntio
n in
the
post
acut
e ph
ase
afte
r stro
ke. T
he e
ffect
s w
ill no
t re
sult
in im
prov
ing
AD
L.
…is
not
effe
ctiv
e to
redu
ce m
emor
y pr
oble
ms
in th
e po
stac
ute
phas
e af
ter s
troke
.
…in
crea
sing
the
negl
igib
le b
ody
side
, mea
sure
d w
ith v
isua
l sca
nnin
g te
sts.
The
effe
cts
will
not r
esul
t in
impr
ovem
ent o
f sca
nnin
g in
dai
ly li
ve.
Com
paris
on
…co
mpa
red
to…
– – – – – – – – –
Inte
rven
tion
…th
e ef
fect
iven
ess
of…
…co
nstra
int-i
nduc
ed
mov
emen
t the
rapy
(=
forc
ed u
se)…
…bi
ofee
dbac
k to
the
mus
cles
of p
aret
ic a
rm…
…tra
nscu
tane
ous
nerv
e st
imul
atio
n of
the
pare
tic
arm
…
… n
euro
mus
cula
r st
imul
atio
n in
pat
ient
s w
ith
glen
ohum
eral
sub
luxa
tion
of th
e pa
retic
sho
ulde
r and
he
mip
legi
c sh
ould
er p
ain…
…pa
ssiv
e of
ass
iste
d ac
tive
shou
lder
exe
rcis
es w
ith th
e pa
retic
arm
…
…ho
me-
base
d th
erap
y ai
med
at i
ncre
asin
g le
isur
e ac
tiviti
es (s
uch
as re
gain
ing
gard
enin
g or
pai
ntin
g)…
…at
tent
ion
train
ing…
…m
emor
y tra
inin
g…
…tre
atin
g ne
glec
t, da
ily 3
0 to
60
min
utes
dur
ing
a fe
w
wee
ks in
pat
ient
s w
ith ri
ght
hem
isph
eric
al s
troke
…
Patie
nts
In p
atie
nts
w
ith s
trok
e…
Tab
le 5
-
Con
tinue
d -
PIC
O
16.
Han
d an
d ar
m u
se:
CIM
T
17.
Han
d an
d ar
m u
se:
Bio
feed
back
to th
e pa
retic
upp
er li
mb
18.
Han
d an
d ar
m u
se:
TEN
S
19.
Han
d an
d ar
m u
se:
NM
S w
ith G
HS
and
HS
P
20.
Han
d an
d ar
m u
se:
NM
S w
ith G
HS
and
HS
P
21.
AD
L:
Trai
ning
leis
ure
activ
ities
22.
AD
L:
Trai
ning
atte
ntio
n de
ficits
23.
AD
L:
Trai
ning
mem
ory
defic
its
24.
AD
L:
Neg
lect
: vis
ual s
cann
ing
train
ing
AD
L in
dica
tes
activ
ities
of d
aily
livi
ng; B
WS
TT, b
ody-
wei
ght s
uppo
rted
tread
mill
train
ing;
CIM
T, c
onst
rain
t-ind
uced
mov
emen
t the
rapy
; FE
S, f
unct
iona
l ele
ctric
al s
timul
atio
n;
GH
S, g
leno
hum
eral
sub
luxa
tion;
HS
P, h
emip
legi
c sh
ould
er p
ain;
MR
P, m
otor
rele
arni
ng p
rogr
amm
e; N
DT,
neu
rode
velo
pmen
t tre
atm
ent;
NM
S, n
euro
mus
cula
r stim
ulat
ion;
P
NF,
pro
prio
cept
ive
neur
omus
cula
r fac
ilitat
ion;
RO
M, r
ange
of m
otio
n; T
EN
S, t
rans
cuta
neou
s el
ectri
cal n
erve
stim
ulat
ion

Clinical practice stroke guideline for physiotherapists
123
Outcome measures The recent emphasis on ‘evidence‐based practice’ means that extra attention should be paid to the validity of outcome measures.59 Thirty‐three studies23‐54 of outcome measures were identified, yielding 32 potential outcome measures. An independent sample of 169 physiotherapists not involved in guideline development were asked to measure outcome according to the three ICF domains (functions, activities, and participation)16, and to indicate which of the33 outcome measures they would prefer to use to assess treatment outcome in patients who had had a stroke. The definitive test battery (25 outcome measures) was established in consensus meetings with the experts and task group. These outcome measures were considered to reflect the three ICF activity categories, namely, walking and mobility‐related activities; hand and arm use; and ADL. The outcome measures were divided into two sections. The first section, consisting of the core set of outcome measures, should be applied to all stroke patients, since these measures were considered to evaluate whether physiotherapy care was adequate in all phases after stroke. These core outcome measures had minimal overlap and were 1) the Motricity Index (MI)29,33 (Grade 2 evidence), 2) Trunk Control Test (TCT)29,35 (Grade 2 evidence), 3) Berg Balance Scale (BBS)23 (Grade 1 evidence), 4) Functional Ambulation Categories (FAC)40,41 (Grade 2 evidence), 5) comfortable Ten Metre Walk (TMW)54 (Grade 1 evidence), 6) Frenchay Arm Test (FAT)34,37,54 (Grade 2 evidence), and 7) Barthel Index (BI)28 (Grade 2 evidence). The psychometric properties and level of evidence of these selected measures of outcome are summarised in Table 6. Optional outcome measures The second section consisted of 18 optional outcome measures, to be used to evaluate a specific function or activity in individual patients with stroke. For instance, if the hand of the paretic arm becomes edematous, it would be desirable to measure the volume of the hand. This is not necessary if the hand is not edematous. The optional outcome measures are: Modified Rankin Scale52, Neutral‐0‐Method (Range of Motion)49, Numeric Pain Rating Scale42, Nottingham Sensory Assessment30,44, Modified Ashworth Scale24,60, testing the cranial nerves32, Brunnstrom Fugl‐Meyer assessment36, Hand volumeter47, Trunk Impairment Scale53, Action Research Arm Test45, Nine Hole Peg Test37, Timed Balance Test25,43, Rivermead Mobility Index27, Falls Efficacy Scale for Stroke38,39, Timed Up&Go Test48, Six Minutes Walk26, Nottingham Extended ADL‐index46,54, and Frenchay Activities Index31,50.

Chapter 5
124
Leve
l of
evid
ence
2 2 1 2
Num
ber
of c
riter
ia
max
6
crite
ria,
see
Tabl
e 2
5 5 6 5
Clin
ical
U
se
TPA
: yes
TT
A: 1
0-15
m
in.
TPA
: yes
TT
A: 5
-10
min
.
TPA
: yes
TT
A: 1
5 m
in.
TPA
: yes
TT
A: 1
m
in.
Res
pon-
sive
ness
:
Low
S
DD
(MI-a
rm) =
12
poi
nts
SD
D (M
I-leg
) =
13 p
oint
s (K
ools
tra 2
004)
Low
S
DD
= 2
5 po
ints
(K
ools
tra 2
004)
Hig
h
SD
D =
6 p
oint
s (S
teve
nson
et a
l ‘0
1)
Low
S
DD
= 1
poi
nt
(Koo
lstra
200
4)
Test
-Ret
est
Rel
iabi
lity:
r s (i
nter
) = 0
.91*
* r s
(int
ra) =
0.9
8**
(Koo
lstra
200
4)
r s (i
nter
) = 0
.96*
* r (
intra
) = 0
.87*
* (K
ools
tra 2
004)
ICC
(int
er) =
0.
96**
IC
C (i
ntra
) =
0.98
**
(Koo
lstra
200
4)
r s (i
nter
) = 0
.79*
* IC
C (i
ntra
) =
0.96
**
(Koo
lstra
200
4)
Con
curre
nt
valid
ity:
MI-l
eg v
s FM
-le
g:
r s =
0.6
9**
MI-a
rm v
s FM
-ar
m:
r s =
0.7
1**
(Koo
lstra
200
4)
TCT
vs M
I-leg
: r s
= 0
.71*
* TC
T vs
FA
C:
r s =
0.6
9**
(Koo
lstra
200
4)
BB
S v
s TU
G:
r s =
-0.7
0**
BB
S v
s FR
T:
r s =
0.8
8**
(Koo
lstra
200
4)
FAC
vs
TMW
com
f.:
r s =
0.7
9**
FAC
vs
BI:
r =
0.8
9**
(Koo
lstra
200
4)
Val
idat
ed
in s
troke
pa
tient
po
pula
tion
Dem
euris
se
1980
C
ollin
& W
ade
1990
Col
lin &
Wad
e 19
90
Fran
chig
noni
19
97
Ber
g 19
95
Hol
den
1984
H
olde
n 19
86
Brie
f des
crip
tion
Eva
luat
es v
olun
tary
mot
or a
ctiv
ity o
r m
axim
al is
omet
ric m
uscl
e st
reng
th o
f (p
aret
ic) a
rm a
s w
ell a
s (p
aret
ic) l
eg
mus
cles
. Rel
iabl
e, v
alid
, and
qui
ck to
pe
rform
, and
poo
r res
pons
iven
ess.
S
ix it
ems
scor
ed o
n an
ord
inal
ratin
g sc
ale
(sum
sco
re 0
-200
poi
nts)
Eva
luat
es th
e st
abilit
y of
the
trunk
. R
elia
ble,
val
id, s
impl
e to
adm
inis
ter,
and
poor
resp
onsi
vene
ss.
A 3
-poi
nt o
rdin
al ra
ting
scal
e (0
, 12,
or
25
poin
ts fo
r eac
h ite
m) i
s us
ed to
sc
ore
four
axi
al m
ovem
ents
(sum
sc
ore:
0-1
00 p
oint
s)
Eva
luat
es s
tatic
and
dyn
amic
ba
lanc
e in
a fu
nctio
nal w
ay. T
he
scal
e is
val
id, r
elia
ble,
and
re
spon
sive
, and
take
s ab
out 1
5 m
inut
es to
adm
inis
ter.
The
BB
S
cons
ists
of 1
4 ite
ms,
sco
red
on 5
-po
int o
rdin
al ra
ting
scal
e (0
-4 p
oint
s).
The
sum
sco
re v
arie
s be
twee
n 0
and
56 p
oint
s
Eva
luat
es th
e de
gree
of d
epen
denc
e in
wal
king
abi
lity.
The
FA
C is
a v
alid
, re
liabl
e as
sess
men
t too
l, ea
sy to
ad
min
iste
r, an
d po
or re
spon
sive
ness
. It
cont
ains
6 it
ems,
sco
red
on a
2-
poin
t ord
inal
sca
le (s
um s
core
, 0-5
po
ints
)
Tabl
e 6
C
hara
cter
istic
s of
the
prim
ary
set o
f out
com
e m
easu
res
incl
uded
in th
e C
PG
PS
(for
exp
lana
tion
of th
e us
ed c
riter
ia s
ee T
able
3)
Out
com
e m
easu
re
Mot
ricity
Inde
x
Trun
k C
ontro
l Te
st
Ber
g B
alan
ce
Sca
le
Func
tiona
l A
mbu
latio
n
Cat
egor
ies

Clinical practice stroke guideline for physiotherapists
125
Leve
l of
evid
ence
1 2 2
Num
ber
of c
riter
ia
max
6
crite
ria,
see
Tabl
e 2
6 5 5
Clin
ical
U
se
TPA
: yes
TT
A: 5
-10
min
.
TPA
: yes
TT
A: 5
-10
min
.
TPA
: yes
TT
A: 3
-5m
in.
Res
pon-
sive
ness
:
Hig
h
SD
D =
0.1
6 m
/s
(Koo
lstra
200
4)
Low
S
DD
= 1
.3 p
oint
s (H
oogs
traat
un
publ
.)
Low
S
DD
= 4
poi
nts
(Koo
lstra
200
4)
Test
-Ret
est
Rel
iabi
lity:
r p (i
nter
) = 0
.97*
* IC
C (i
ntra
) =
0.97
**
ICC
= 0
.90*
* (H
oogs
traat
un
publ
.)
r s (i
nter
) = 0
.95*
* r s
(int
ra) =
0.9
5**
(Koo
lstra
200
4)
Con
curre
nt
valid
ity:
TMW
com
f. vs
FA
C :
r s
=0.
79**
(K
ools
tra 2
004)
FAT
vs U
AT.
: r p
= 0
.93*
* (K
ools
tra 2
004)
BI v
s FA
C:
r s =
0.8
9**
BI v
s A
RA
T:
r s =
0.4
6*
(Koo
lstra
200
4)
Val
idat
ed
in s
troke
pa
tient
po
pula
tion
Wad
e 19
92
Wad
e 19
92
DeS
ouza
19
80
Col
lin 1
988
Brie
f des
crip
tion
Giv
es a
val
id a
nd re
liabl
e in
dica
tion
of th
e co
mfo
rtabl
e w
alki
ng s
peed
. It
is re
spon
sive
and
sim
ple
to
adm
inis
ter,
and
can
be te
sted
in
patie
nts
with
a F
AC
sco
re o
f 3 o
r m
ore
poin
ts. T
he m
ean
of 3
wal
king
tri
als
is re
cord
ed. P
atie
nts
can
be
test
ed w
earin
g or
thot
ics
or u
sing
w
alki
ng a
ids
Eva
luat
es th
e us
e of
par
etic
han
d an
d ar
m. T
he F
AT
is a
relia
ble
and
valid
tool
with
poo
r res
pons
iven
ess.
Ite
ms
scor
ed o
n a
2-po
int o
rdin
al
ratin
g sc
ale
(0-1
poi
nt),
with
a to
tal
scor
e of
0 to
5 p
oint
s
Eva
luat
es th
e de
gree
of d
epen
denc
e in
AD
L. T
he B
I is
a va
lid, r
elia
ble
asse
ssm
ent t
ool,
and
is e
asy
to
adm
inis
ter w
ith p
oor r
espo
nsiv
enes
s.
Ther
e ar
e se
vera
l diff
eren
t ver
sion
s of
the
test
; we
chos
e th
e 20
-poi
nt
Col
lin v
ersi
on.28
Thi
s ve
rsio
n co
ntai
ns 1
0 ite
ms,
som
e of
whi
ch a
re
scor
ed o
n a
2-po
int (
0-1
poin
t) an
d ot
hers
on
a 4-
poin
t ord
inal
ratin
g sc
ale
(0-3
poi
nts)
Tabl
e 6
- C
ontin
ued
-
Out
com
e m
easu
re
Ten
Met
re W
alk
Fren
chay
Arm
Te
st
Bar
thel
Inde
x
** p
<0.0
01
* p<
0.01
A
RA
T in
dica
tes
actio
n re
sear
ch a
rm te
st; B
BS, b
erg
bala
nce
scal
e; B
I, ba
rthel
inde
x; F
AC, f
unct
iona
l am
bula
tion
cate
gorie
s; F
AT,
fren
chay
arm
test
; FM
, fug
l-mey
er a
sses
smen
t;
FRT,
func
tiona
l rea
ch te
st; I
CC
, int
racl
ass
corr
elat
ion
coef
ficie
nt; M
I, m
otric
ity in
dex;
r p ,
pear
sons
cor
rela
tion
coef
ficie
nt; r
s ,sp
earm
an c
orre
latio
n co
effic
ient
; SD
D, s
mal
lest
det
ecta
ble
diffe
renc
e;
TCT,
trun
k co
ntro
l tes
t; TM
W, t
en m
etre
wal
k; T
PA
, tes
t pro
toco
l ava
ilabl
e; T
TA, t
ime
to a
dmin
iste
r; TU
G, t
imed
up&
go te
st; U
AT,
utre
cht a
rm te
st; v
s =
vers
us

Chapter 5
126
Moments of assessment after stroke The task group and expert group reached agreement on when the core outcome variables should be measured. Since the information acquired can assist physiotherapists in their clinical reasoning and decision making, it is important to measure these variables at the start and end of a course of treatment, before each (multidisciplinary) stroke team meeting (actual information about patients’ status and progress), and at 3 and 6 months after stroke (to use in future prognostic research). Discussion In general, the use of evidence‐based guidelines improves patient care.7,61 The same is true regarding clinical decision‐making in physiotherapy.9,62 To improve physiotherapy care for patients with stroke in the Netherlands, we developed a clinical practice guideline on physiotherapy for patients with stroke (CPGPS). We first performed a literature review, identifying 322 relevant articles that covered three aspects of the physiotherapy management of stroke patients, namely, prognostics, interventions, and outcomes. The methodological quality of these studies was assessed, as was the content of the interventions used. Seventy‐two recommendations for clinical practice for physiotherapists were distilled from these articles: Six recommendations concerned the prediction of functional recovery of generic ADL, including specific ADLs such as walking ability and hand/arm use (grade 3 evidence); 65 recommendations concerned physiotherapy interventions (24 of grade 1 evidence; 18 of grade 2 evidence; and 23 of grade 3 evidence); and 1 recommendation concerned when to assess functional outcome, using reliable, responsive, and valid outcome measures. According to the guideline, physiotherapists should assess each stroke patient with the core set of 7 high‐quality outcome measures (grade 1 or 2). Most (6 of 7) of these outcome measures assessed activities of the ICF framework.59,63,64 As such, the guideline should be used by physiotherapists in clinical decision‐making.65
The guideline was constructed according to international standards.66‐68 The main electronic databases were searched and the methodological quality of the included studies was analysed.7,11,14,15,18 Although sometimes arbitrary choices were made when scoring the methodological quality of the studies,69 our choices seem to have been justified, according to recent stroke rehabilitation literature.70 Furthermore, where possible, we analysed the effects of the interventions (and if possible

Clinical practice stroke guideline for physiotherapists
127
statistical pooling of comparable interventions).10,12 Most of the intervention studies included were small and hence had a low statistical power to reveal statistically significant effects.12 The differences in methodological quality resulted in an almost significant negative trend between the calculated effect sizes in 123 of the included RCTs and the quality rating according to the PEDro scale.12 In addition, the generalisability of the results of studies of prognostic factors is often limited due to methodological flaws and the often arbitrary timing of predicting outcome after stroke.14 Recently, a new longitudinal regression model was developed in which the longitudinal relationship of observed changes in body functions, such as strength and synergism, is related with observed improvements in activities such as gait.71 The advantage of such longitudinal regression models is that time is used as a covariate that independently determines the accuracy of outcome.71 In addition, most regression models have not been cross‐validated in an independent group of stroke patients, which makes the generalisability of the derived model questionable. There is a need for long‐term studies of the chronic phase in order to identify those patients who are susceptible for functional decline, for example in gait performance.72 Each step in the clinical decision‐making process should incorporate the patient’s wishes and be based on the patient’s functional prognosis. However, physiotherapists should use their clinical experience to critically appraise treatment goals and evaluative measurements in term of activities and participation.65,73,74 In other words, when treating patients, there is always a compromise between existing evidence on the one hand, and the patients’ clinical state and circumstances, the patients’ preferences, including cultural and ethical factors, and constraints, such as time available to apply the guideline and available equipment and expertise,65,73 on the other. Consequently, clinical practice guidelines cannot be seen as a simple cookbook in which steps are taken automatically. Moreover, such guidelines do not always cover all the aspect or events that occur in “real life”. While many of the physiotherapy interventions included in the guideline were restricted to exercises,10 in practice physiotherapists often use combined interventions or interventions which, to our knowledge, have never been investigated in well‐designed studies.10,12 For example, there are few RCTs of the effect of physiotherapy on stair climbing, of the use of walking aids, of training transfers (bed to chair), or of instructions for fall prevention.10,12 In addition, a discussion is warranted on which research design is most appropriate for generating evidence to improve everyday physiotherapy practice.75‐77 It might be useful to consider non‐linear

Chapter 5
128
dynamics,78,79 and psychological constructs in physiotherapy research and stroke rehabilitation, such as control perceptions.80
Recently, a number of multidisciplinary stroke guidelines have been developed in the UK6, Scotland4, USA81, Canada82, New Zealand83, and the Netherlands2,3. To date, to our knowledge, beside our guideline10, no physiotherapy‐specific stroke guideline has been published, except extracts of the physiotherapy elements of the UK stroke guideline.84 However, the development of a monodisciplinary stroke guideline has been criticised recently,85 because stroke rehabilitation is a team activity and therefore cannot be split up into the effects of specific professional therapies.85 We consider monodisciplinary guidelines an extension of existing multidisciplinary guidelines, offering more detailed information related to a certain discipline.86
We are aware, however, that the applications of CPGPS are not restricted to the discipline ‘physiotherapy’ alone. Moreover, it should be emphasised that the content of physiotherapy differs in each institutional setting and heavily depends on the available expertise in each multidisciplinary team as well as the context of health care system in general. Therefore, the present CPGPS should not be seen as an attribution of certain interventions to a certain discipline but rather as a collection of available knowledge about the effectiveness of interventions applicable by physiotherapists working in the Dutch health care system.
Posthoc analyses of the content of the guideline demonstrated that almost 90% of the recommendations were based on the results of intervention studies involving patients in the post acute and chronic phase of stroke, and patients who had experienced a less severe or uncomplicated stroke. We have to conclude that evidence‐based interventions are based on only a minority of patients, given the complexity of stroke. In fact, it could be queried whether individual stroke patients will benefit from this guideline and evidence‐based interventions in everyday physiotherapy practice. To our knowledge, this gap between evidence‐based knowledge and the real world has not been investigated.
We are also aware that developing CPGPS does not automatically result into a changed behaviour of physiotherapists in their daily practice by lack of knowledge about the factors impeding successful implementation. For example, the present CPGPS showed moderate evidence for a reduced length of stay in favour of Motor Relearning Programme (MRP) or traditional care, compared to a rather impairment focused neuromuscular treatment approach such as neurodevelopmental treatment (NDT). No evidence was found for applying a specific neurological treatment program

Clinical practice stroke guideline for physiotherapists
129
in terms of muscle strength, synergism, muscle tone, walking ability, dexterity or ADL.12 Achieved consensus of the dubious role of strictly applying NDT concept after stroke has resulted in an implementation research program for 2 years paid by the Dutch Government.87 In this implementation project NDT teachers are educated how to apply the evidence‐based guidelines into practice, how to measure change and how to estimate prognosis in patients with stroke. Since recently, all NDT teachers in the Netherlands accepted to participate in this implementation project of the CPGPS and endorsed to change their name into ‘Neurorehabilitation‐CVA’.
The conceptual evidence‐based model for clinical decision‐making composed by Haynes et al.65 emphasises the central role of clinical expertise in this process. Clinical expertise has three components, namely, research evidence, patients’ clinical state and circumstances, and patients’ preferences and actions. In developing the guideline, we concentrated on one component, research evidence, and paid less attention to the other two components.65 To improve the guidelines, we suggest that in the future a) patients with stroke should be stratified into different functional profiles according to their prognosis in their recovery of functional health status71,88,89; b) clinical decision rules for each stratum or group should be developed90; and c) concepts concerning clinimetric monitoring of functional health status of patients with stroke should be developed.91 In addition, we need to know more about the time dependence of functional recovery after stroke,71,88 about the mechanisms underlying therapy‐induced functional improvement, and the time dependence of predictors of functional outcome.71,88,89 The recent shift in physiotherapy toward task‐oriented and context‐specific training means that outcome measures may need to be developed in order to evaluate patients with stroke in their real‐life activities.64,92 These improvements can be integrated in an update of the CPGPS. The board of the Royal Dutch Society for Physical Therapy stipulated that the guideline should be revised every 5 years. As one of the aims of developing this guideline was to improve everyday physiotherapy practice, in the future attention should be paid to factors that hinder the implementation of the guideline. Acknowledgement We would like to thank the members of the expert group: BC Harmeling‐van der Wel; BJ Kollen; JSM Hobbelen; JH Buurke; J Halfens; L Wagenborg; MJ

Chapter 5
130
Vogel; and M Berns and the steering committee: J Dekker; PhJ Van der Wees; M Heldoorn; and R Van Klaveren, and also JCF Ket (VU Medical Library) and the representatives of the multi‐professional groups. This project is supported by a grant from the KNGF, grant reference number: IKPZ/KNGF/05/2000. References
1. Koek HL, Van Dis SJ, Peters RJG et al. Hart‐en vaatziekten in Nederland. In: Van Leest LATM, Koek HL, Van Trijp MJCA, Van Dis SJ, Peters RJG, Bots ML et al., editors. Hart‐en vaatziekten in Nederland 2005, cijfers over risicofactoren, ziekte, behandeling en sterfte [dutch]. Den Haag: Nederlandse Hartstichting, 2005: 6‐12.
2. Dutch Institute for Quality in Health Care (in Dutch: Kwaliteitsinstituut voor de gezondheidszorg Utrecht‐CBO‐). CBO Richtlijn Beroerte (Stroke Guidelines 2000, in Dutch). 2000. Den Haag, Nederlandse Hartstichting.
3. Commissie CVA‐Revalidatie. Rehabilitation after a stroke, guidelines and recommendations for health care professionals (in Dutch: Revalidatie na een beroerte: richtlijnen en aanbevelingen voor zorgverleners). Franke EAM, editor. 2001. Den Haag, Dutch Heart Foundation (in Dutch: Nederlandse Hartstichting).
4. Scottish Intercollegiate Guidelines Network. Management of patients with stroke, rehabilitation, prevention and management of complications and discharge planning ‐ a national clinical guideline (no: 64). 64. 2002. Edinburgh, SIGN.
5. Agency for Health Care Policy and Research. Post‐Stroke Rehabilitation: clinical practice guideline. No.16. 1995. Rockville, AHCPR Publication 95‐0662.
6. Royal College of Physicians ‐ the intercollegiate working party for stroke. National Clinical Guidelines for Stroke. 1999. London.
7. Sackett DL, Straus SE, Richardson WS et al. Evidence‐Based Medicine. How to practice and teach EBM. 2nd ed. Edinburgh: Churchill Livingstone, 2000.
8. De Wit L, Putman K, Dejaeger E al. Use of time by stroke patients: a comparison of four European rehabilitation centers. Stroke 2005; 36:1977‐1983.
9. Jette DU, Latham NK, Smout RJ et al. Physical therapy interventions for patients with stroke in inpatient rehabilitation facilities. Phys Ther 2005; 85:238‐248.
10. Van Peppen RPS, Kwakkel G, Harmeling BC et al. Clinical practice guideline on Physiotherapy‐management of patients with Stroke [in dutch: KNGF‐richtlijn Beroerte]. Ned Tijdschr v Fysioth 2004; 114 (5:supplement):1‐78.
11. PEDro. The Physiotherapy Evidence Database (PEDro). 2004. http://www.pedro.fhs.usyd.edu.au/
12. Van Peppen RP, Kwakkel G, Wood‐Dauphinee S et al. The impact of physical therapy on functional outcomes after stroke: whatʹs the evidence? Clin Rehabil 2004; 18:833‐862.

Clinical practice stroke guideline for physiotherapists
131
13. WHO. Stroke‐‐1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 1989; 20:1407‐1431.
14. Kwakkel G, Wagenaar RC, Kollen BJ et al. Predicting disability in stroke‐‐a critical review of the literature. Age Ageing 1996; 25:479‐489.
15. Meijer R, Ihnenfeldt DS, de Groot IJ et al. Prognostic factors for ambulation and activities of daily living in the subacute phase after stroke. A systematic review of the literature. Clin Rehabil 2003; 17:119‐129.
16. WHO. ICF‐introduction, the International Classification of Functioning Disability and Health. http://www.who.int/classification/icf/intros/ICF‐Eng‐Intro.pdf . 2001. Geneve.
17. Streiner DL, Norman GR. Health measurement scales, a practical guide to their development and use. second ed. New York: Oxford University Press, 2003.
18. Bot SD, Terwee CB, van der Windt DA et al. Clinimetric evaluation of shoulder disability questionnaires: a systematic review of the literature. Ann Rheum Dis 2004; 63:335‐341.
19. Counsell C, Dennis M. Systematic review of prognostic models in patients with acute stroke. Cerebrovasc Dis 2001; 12:159‐170.
20. Dombovy ML, Sandok BA, Basford JR. Rehabilitation for stroke: a review. Stroke 1986; 17:363‐369.
21. Jongbloed L. Prediction of function after stroke: a critical review. Stroke 1986; 17(4):765‐776.
22. Meijer R, Ihnenfeldt DS, van Limbeek J, Vermeulen M, de Haan RJ. Prognostic factors in the subacute phase after stroke for the future residence after six months to one year. A systematic review of the literature. Clin Rehabil 2003; 17:512‐520.
23. Berg K, Wood‐Dauphinee S, Williams JI. The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med 1995; 27:27‐36.
24. Blackburn M, van Vliet P, Mockett SP. Reliability of measurements obtained with the modified Ashworth scale in the lower extremities of people with stroke. Phys Ther 2002; 82:25‐34.
25. Bohannon RW, Larkin PA, Cook AC, Gear J, Singer J. Decrease in timed balance test scores with aging. Phys Ther 1984; 64(7):1067‐1070.
26. Butland RJ, Pang J, Gross ER et al. Two‐, six‐, and 12‐minute walking tests in respiratory disease. Br Med J (Clin Res Ed) 1982; 284:1607‐1608.
27. Collen FM, Wade DT, Robb GF et al. The Rivermead Mobility Index: a further development of the Rivermead Motor Assessment. Int Disabil Stud 1991; 13:50‐54.
28. Collin C, Wade DT, Davies S et al. The Barthel ADL Index: a reliability study. Int Disabil Stud 1988; 10:61‐63.
29. Collin C, Wade D. Assessing motor impairment after stroke: a pilot reliability study. J Neurol Neurosurg Psychiatry 1990; 53:576‐579.
30. Crow JL, Harmeling BC. Development of a consensus and evidence‐based standardised clinical assessment and record form for neurological inpatients: the Neuro Dataset. Physiotherapy 2002; 88:33‐46.

Chapter 5
132
31. De Haan RJ. Clinimetrics in stroke. Dept. Clin. Epidemiology & Biostatistics, Academic Medical Centre, Amsterdam, 1994.
32. De Weerdt W. Patiënten met neurologische aandoeningen. Deel 1: handleiding voor het functioneel onderzoek. Leuven (België): Acco, 2001.
33. Demeurisse G, Demol O, Robaye E. Motor evaluation in vascular hemiplegia. Eur Neurol 1980; 19:382‐389.
34. DeSouza LH, Langton‐Hewer R, Miller S. Assessment of recovery of arm control in hemiplegic stroke patients. Arm function test. Int Rehabil Med 1980; 2:3‐9.
35. Franchignoni FP, Tesio L, Ricupero C et al. Trunk control test as an early predictor of stroke rehabilitation outcome. Stroke 1997; 28:1382‐1385.
36. Fugl‐Meyer AR, Jaasko L, Leyman I et al. The post‐stroke hemiplegic patient. 1: a method for evaluation of physical performance. Scand J Rehabil Med 1975; 7:13‐31.
37. Heller A, Wade DT, Wood VA et al. Arm function after stroke: measurement and recovery over the first three months. J Neurol Neurosurg Psychiatry 1987; 50:714‐719.
38. Hellstrom K, Lindmark B. Fear of falling in patients with stroke: a reliability study. Clin Rehabil 1999; 13:509‐517.
39. Hellstrom K, Lindmark B, Fugl‐Meyer A. The Falls‐Efficacy Scale, Swedish version: does it reflect clinically meaningful changes after stroke? Disabil Rehabil 2002; 24:471‐481.
40. Holden MK, Gill KM, Magliozzi MR et al. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys Ther 1984; 64:35‐40.
41. Holden MK, Gill KM, Magliozzi MR. Gait assessment for neurologically impaired patints. Sandards for outcome assessment. Phys Ther 1986; 66:1530‐1539.
42. Joos E, Peretz A, Beguin S et al. Reliability and reproducibility of visual analogue scale and numeric rating scale for therapeutic evaluation of pain in rheumatic patients. J Rheumatol 1991; 18:1269‐1270.
43. Kwakkel G, Wagenaar RC, Twisk JW et al. Intensity of leg and arm training after primary middle‐cerebral‐artery stroke: a randomised trial. Lancet 1999; 354:191‐196.
44. Lincoln NB, Jackson JM, Adams SA. Reliability and revision of the Nottingham sensory assessment for stroke patients. Physiotherapy 1998; 84:358‐365.
45. Lyle RC. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int J Rehabil Res 1981; 4:483‐492.
46. Nouri FM, Lincoln NB. An extended activities of daily living scale for stroke patients. Clin Rehabil 1987; 1:301‐305.
47. Oerlemans HM, Goris RJ, Oostendorp RA. Impairment level sumscore in reflex sympathetic dystrophy of one upper extremity. Arch Phys Med Rehabil 1998; 79:979‐990.
48. Podsiadlo D, Richardson S. The timed ʺUp & Goʺ: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39:142‐148.
49. Ryf C, Weymann A. Range of Motion ‐ AO Neutral‐0‐Method; measurement and documentation. Stutgart: Thieme, 1999.

Clinical practice stroke guideline for physiotherapists
133
50. Schuling J, de Haan R, Limburg M et al. The Frenchay Activities Index. Assessment of functional status in stroke patients. Stroke 1993; 24:1173‐1177.
51. Stevenson TJ. Detecting change in patients with stroke using the Berg Balance Scale. Aust J Physiother 2001; 47:29‐38.
52. Van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, Van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988; 19:604‐607.
53. Verheyden G, Nieuwboer A, Mertin J et al. The Trunk Impairment Scale: a new tool to measure motor impairment of the trunk after stroke. Clin Rehabil 2004; 18:326‐334.
54. Wade DT. Measurements in neurological rehabilitation. Oxford: Oxford University Press, 1992.
55. Kwakkel G, Kollen BJ, Van der Grond J, et al. Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke 2003; 34:2181‐2186.
56. Sunderland A, Tinson D, Bradley L et al. Arm function after stroke. An evaluation of grip strength as a measure of recovery and a prognostic indicator. J Neurol Neurosurg Psychiatry 1989; 52:1267‐1272.
57. Wade DT, Langton‐Hewer R, Wood VA et al. The hemiplegic arm after stroke: measurement and recovery. J Neurol Neurosurg Psychiatry 1983; 46:521‐524.
58. Kwakkel G, van Dijk GM, Wagenaar RC. Accuracy of physical and occupational therapistsʹ early predictions of recovery after severe middle cerebral artery stroke. Clin Rehabil 2000; 14:28‐41.
59. Salter K, Jutai JW, Teasell R et al. Issues for selection of outcome measures in stroke rehabilitation: ICF activity. Disabil Rehabil 2005; 27:315‐340.
60. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987; 67:206‐207.
61. Duncan PW, Zorowitz R, Bates B et al. Management of Adult Stroke Rehabilitation Care: a clinical practice guideline. Stroke 2005; 36:e100‐e143.
62. Jette DU, Bacon K, Batty C et al. Evidence‐based practice: beliefs, attitudes, knowledge, and behaviors of physical therapists. Phys Ther 2003; 83:786‐805.
63. Australian Physiotherapy Association. APA Position Statement ‐ Clinical justification and outcome measures. 2003: https://apa.advsol.com.au/staticcontent/staticpages/position_statements/public/ClinicalJustification&Outcome%20Measures.pdf
64. Jette AM. Assessing disability in studies on physical activity. Am J Prev Med 2003; 25 (3 Suppl 2):122‐128.
65. Haynes RB, Devereaux PJ, Guyatt GH. Clinical expertise in the era of evidence‐based medicine and patient choice. Vox Sang 2002; 83 Suppl 1:383‐386.
66. Hendriks HJM, Bekkering GE, van Ettekoven H et al. Development and implementation of national practice guidelines: a prospect for continuous quality improvement in physiotherapy. Physiotherapy 2000; 86:535‐547.

Chapter 5
134
67. Shaneyfelt TM, Mayo‐Smith MF, Rothwangl J. Are guidelines following guidelines? The methodological quality of clinical practice guidelines in the peer‐reviewed medical literature. JAMA 1999; 281:1900‐1905.
68. The AGREE Collaboration. Appraisal of Guidelines Research & Evaluation (AGREE); Instrument voor beoordeling van richtlijnen. 2001.
69. Juni P, Witschi A, Bloch R et al. The hazards of scoring the quality of clinical trials for meta‐analysis. JAMA 1999; 282:1054‐1060.
70. Bhogal SK, Teasell RW, Foley NC et al. The PEDro scale provides a more comprehensive measure of methodological quality than the Jadad scale in stroke rehabilitation literature. J Clin Epidemiol 2005; 58:668‐673.
71. Kollen B, Van de Port I, Lindeman E et al. Predicting improvement in gait after stroke: a longitudinal prospective study. Stroke 2005; 36:2676‐2680.
72. Van de Port I, Kwakkel G, van Wijk I et al. Susceptibility to deterioration of mobility long‐term after stroke: a prospective cohort study. Stroke 2006; 37:167‐171.
73. Davidoff F. In the teeth of the evidence: the curious case of evidence based medicine. Mt Sinai J Med 1999; 66:75‐83.
74. Grol R, Wensing M, Eccles M. Improvement patient care. The implementation of change in clinical practice. London: Elsevier Butterworth Heinemann, 2005.
75. Devereaux PJ, Bhandari M, Clarke M et al. Need for expertise based randomised controlled trials. BMJ 2005; 330:88.
76. Hotopf M. The pragmatic randomised controlled trial. Advances in Psychiatric Treatment 2002; 8:326‐333.
77. Tunis SR, Stryer DB, Clancy CM. Practical clinical trials: increasing the value of clinical research for decision making in clinical and health policy. JAMA 2003; 290:1624‐1632.
78. Kwakkel G, Wagenaar RC. Effect of duration of upper‐ and lower‐extremity rehabilitation sessions and walking speed on recovery of interlimb coordination in hemiplegic gait. Phys Ther 2002; 82:432‐448.
79. Scholz JP. Dynamic pattern theory‐‐some implications for therapeutics. Phys Ther 1990; 70:827‐843.
80. Johnston M, Pollard B, Morrison V et al. Functional limitations and survival following stroke: psychological and clinical predictors of 3‐year outcome. Int J Behav Med 2004; 11:187‐196.
81. Gresham GE, Duncan PW, Statson WB. Priorities for future research: clinical practice guidelines, number 16. US Dept Health and Human Services ‐ Agency for Health Care Policy and Research, editor. AHCPR publication no. 95‐0662. 1995. Rockville.
82. Teasell RW, Foley NC, Bhogal SK et al. An evidence‐based review of stroke rehabilitation. Top Stroke Rehabil 2003; 10:29‐58.
83. Hanger HC, Wilkinson T, Keeling S et al. New Zealand guideline for management of stroke. N Z Med J 2004; 117:U863.

Clinical practice stroke guideline for physiotherapists
135
84. Hammond R, Lennon S, Walker MF et al. Changing occupational therapy and physiotherapy practice through guidelines and audit in the United Kingdom. Clin Rehabil 2005; 19:365‐371.
85. Wade D. Investigating the effectiveness of rehabilitation professions‐‐a misguided enterprise? Clin Rehabil 2005; 19:1‐3.
86. Michie S, Johnston M. Changing clinical behaviour by making guidelines specific. BMJ 2004; 328:343‐345.
87. Geurts AC, Halfens JHC, Buurke JH et al. Implementatie van nieuwe klinische inzichten in studies over herstel van loopvaardigheid na een CVA. Grant ZonMW, projectnr: 1435.0047. 2006.
88. Kwakkel G, Kollen B, Lindeman E. Understanding the pattern of functional recovery after stroke: facts and theories. Restor Neurol Neurosci 2004; 22:281‐299.
89. Vlaeyen JW, Morley S. Cognitive‐behavioral treatments for chronic pain: what works for whom? Clin J Pain 2005; 21:1‐8.
90. Craik RL. Thirty‐Sixth Mary McMillan Lecture: Never satisfied. Phys Ther 2005; 85:1224‐1237.
91. Glasziou P, Irwig L, Mant D. Monitoring in chronic disease: a rational approach. BMJ 2005; 330:644‐648.
92. Jette AM. Outcomes research: shifting the dominant research paradigm in physical therapy. Phys Ther 1995; 75:965‐970.
93. Kwakkel G. Dynamics in functional recovery after stroke. Wageningen, The Netherlands, 1998.

Chapter 5
136

CHAPTER
Outcome measures in physiotherapy management of
patients with stroke: a survey into self‐reported use,
and barriers to and facilitators for use
Roland PS Van Peppen
Francois JF Maissan
Frank R Van Genderen
Rob van Dolder
Nico LU Van Meeteren
Submitted

Chapter 6
138
Abstract Objective: To investigate physiotherapists’ self‐reported use of outcome measures as recommended in the Dutch clinical practice guideline for the management of patients with stroke (CPGPS), and to assess perceived barriers to and facilitators for the use of outcome measures in everyday practice. Method: A 41‐item survey, including the Barriers and Facilitators Questionnaire (BFQ), was sent by post to 400 physiotherapists in each of the following settings in the Netherlands: acute care hospitals (ACH; N=100), rehabilitation centres (RC; N=100), nursing homes (NH; N=100) and private physiotherapy practices (PPP; N=100). Results: One hundred and eighty‐nine physiotherapists returned the survey (47%; ACH, N=57; RC, N=67; NH, N=26 and PPP, N=39); the surveys of 167 physiotherapists involved in stroke settings were analysed. These physiotherapists reported regularly using three (median; range 0‐7) of the seven recommended measurement instruments, with those working in RC or ACH reporting a significantly higher use than their colleagues in PPP (4 vs. 0 and 3 vs. 0; p<0.001 and p=0.02 respectively). The BFQ revealed that there were setting‐specific facilitators, such as ‘a positive attitude towards outcome measures’ (as mentioned by 93% of the physiotherapists) and ‘acquaintance with outcome measures’ (90%), and barriers such as ‘changing routines’ (32%), ‘time investment’ (29%), and ‘financial compensation’ (21%). Conclusion: Despite an almost uniformly positive attitude, physiotherapists infrequently use the outcome measures recommended in the CPGPS. Robust setting‐specific tailored implementation strategies based on the reported barriers and facilitators are needed. Key Words: physiotherapy, cerebrovascular disorders, outcome measures, guideline, implementation, survey

Outcome measures in physiotherapy stroke management
139
Introduction The judicious use of outcome measures to monitor the health status of patients is considered an aspect of good clinical practice in physiotherapy.1‐4 Their use leads to improved patient care, because professionals have feedback on the effect of an intervention, and to improved communication, both with patients and members of an interdisciplinary team.5 While physiotherapists are encouraged to use outcome measures as a part of their daily practice,6,7 recent surveys indicate they do not regularly do so.2,4,8‐12
In September 2004 a Clinical Practice Guideline on the Physiotherapy management of patients with Stroke (CPGPS) was published in the Netherlands.7,13 One part of the CPGPS recommends the use of a core set of seven valid, reliable and responsive measurement instruments to assess the functional health status of patients who have had a stroke.7 This evidence‐based core set aims to monitor specific aspects in the ‘Activities’ domain of the International Classification of Functioning, Disability and Health (ICF)14‐16, as advocated by Geyh and colleagues.17
It will be difficult to study the adherence of physiotherapists to the entire CPGPS at once. The use of outcome measures by professionals can be seen as a useful indicator of guideline adherence.4 Consequently, in the present survey we focused on the CPGPS recommendations concerning the use of a core set of outcome measures. A crucial element for the successful implementation of evidence‐based therapy in daily practice is an initial analysis of the patients and professionals involved and their institutional context.18 This study analysed the current use of outcome measures by physiotherapists involved in the care of patients with stroke. Such knowledge makes it possible to tailor future implementation strategies. To date, little is known about the use of outcome measures by physiotherapists who provide care for patients with stroke in the Netherlands.
We therefore carried out a survey among physiotherapists in different Dutch stroke settings, to investigate the self‐reported use of outcome measures as recommended in the CPGPS, 2 months after publication of the CPGPS, and to identify perceived barriers to and facilitators for the use of these outcome measures (Barriers and Facilitators Questionnaire). This information may prove helpful in tailoring strategies to promote the implementation of the CPGPS recommendations.

Chapter 6
140
Methods A questionnaire was sent to a proportionally stratified sample19 of physiotherapists in the Netherlands to assess the self‐reported use of measurement instruments as recommended in the CPGPS. Physiotherapists were also asked to provide information about apparent barriers to and facilitators for the use of the recommended outcome measures. In this survey, outcome measures included the objectification, quantification, interpretation and registration of patients’ outcomes and were based on the ‘clinimetrics’ definition by Feinstein “the domain concerned with indexes, rating scales, and other expressions that are used to describe or measure symptoms, physical signs, and other distinctly clinical phenomena in clinical medicine”.20
CPGPS The seven measurement instruments recommended in the CPGPS are the Motricity Index (MI)21, Trunk Control Test (TCT)22, Berg Balance Scale (BBS)23, Functional Ambulation Categories (FAC)24, Ten Metre Walk (TMW)25, Frenchay Arm Test (FAT)26 and Barthel Index (BI)27. The guideline recommends that physiotherapists assess patients’ functional status at least five times at fixed time points during treatment, namely, (a) at the start, (b) at the end of a course of treatment in any location; (c) before each multidisciplinary stroke team meeting (information about patients’ current status and progress); (d) at 3 months, and (e) at 6 months after the stroke.7 The CPGPS also recommends that appropriate outcome data are sent to colleagues if patients are transferred from one clinical setting to another,7 to safeguard the continuity of physiotherapy care during rehabilitation, which is usually started in an acute care hospital (e.g. stroke‐unit of a local or university hospital) and continued in a rehabilitation centre, a nursing home or the community (private physiotherapy practice).28
Questionnaire design A 41‐item questionnaire on the self‐reported use of outcome measures in the physiotherapy management of patients with stroke was used. This questionnaire comprised three sections: Section I consisted of seven multiple choice questions about relevant
personal, demographic and professional characteristics of the physiotherapists, such as age, professional experience and number of stroke patients treated weekly. Section II included 14 questions concerning (a) the routine use of
measurement instruments on a nominal scale (yes / no), (b) the self‐reported

Outcome measures in physiotherapy stroke management
141
use of the recommended core measurement instruments (e.g. Berg Balance Scale), and (c) time points of assessment (e.g. at admission and discharge) and registration (e.g. sending discharge letters). Section III contained 20 statements concerning potential barriers to and
facilitators for the use of outcome measures in everyday practice in physiotherapy stroke management, such as ‘Reluctance to adhere to guidelines’ or ‘Experience with outcome measures’, etc. This ‘Barriers and Facilitators Questionnaire’ (BFQ) was based on a validated questionnaire for perceived barriers to professional change.29,30 The original 27 statement questionnaire was adapted for the purpose of this study. Eleven statements concerning ‘prevention’ were not applicable and therefore removed. Four statements with regard to patients’ view about outcomes and physiotherapists’ training and experience with outcome measures were added. The final 20 statements were tested for content‐validity by five experts. Physiotherapists rated each statement on a 5‐point Likert scale, ranging from ‘fully disagree’ (1 point) to ‘fully agree’ (5 points).
Sample The survey was performed in November 2004, 2 months after the publication of the CPGPS in the Netherlands. The survey was sent by post to a proportionally stratified sample of physiotherapists (N=4x100), randomly selected from the database of the Royal Dutch Society for Physical Therapy and equally distributed over the four main settings of physiotherapy stroke management: acute care hospitals (ACH), rehabilitation centres (RC), nursing homes (NH), and private physiotherapy practices (PPP).28 Non‐responders were sent a reminder in February 2005. The data supplied by physiotherapists who reported treating patients with stroke were analysed.
Data analysis SPSS 12.0 statistical software was used for data analysis (SPSS Inc, Chicago, Illinois, USA), using a significance level of p<0.05. Descriptive statistics were used to describe the physiotherapists and their responses, and to examine the frequency of the self‐reported use of the recommended measurement instruments.31 Sum scores were calculated for all self‐reported outcome measures, ranging from 0 (no use of any of the outcome measures) to 7 (regular use of all recommended outcome measures). The association between sum scores of self‐reported use of recommended core instruments and the number of stroke patients treated weekly and the age of the physiotherapists was assessed using Spearmans rho. The strength of the associations was worded as recommended by Learner and Goodman, who

Chapter 6
142
suggested that a correlation coefficient ≥ 0.7 is indicative of a strong association.32 To assess perceived barriers to and facilitators for the use of outcome measures in the four settings, cross tables and (cumulative) frequencies were used: the 5‐point Likert scale was recoded into a 3‐point scale (fully disagree/disagree, do not agree nor disagree, and agree/fully agree) to simplify data interpretation. Rank scores were used to determine the barriers and facilitators most frequently mentioned.
A principal component analysis (PCA) with Varimax rotation was used to uncover underlying dimensions of the BFQ in this specific professional area.31,33 Subsequently, the internal consistency of the total BFQ and of each of the identified factors was assessed using Cronbachʹs α. Finally, sum scores were calculated for each identified factor by adding up the individual item scores assigned to that specific factor. To assess differences between statements regarding perceived barriers and facilitators in the four settings, a one‐way analysis of variance (ANOVA) was performed with post hoc multiple setting comparison using Bonferroni post‐hoc test.31 All analyses were assessed at a significance level of p< 0.05. Figure 1. Physiotherapists (N) per setting
ACH100
Questionnaires
PPP100
RC100
NH100Sent
Reminder
23 1837 10
57 3967 26
57 2263 25
Total Response 122% (N=88)
Total Response 1+247% (N=189)
Total Included42% (N=167)
DataAnalysis
Response 1
Response 1+2
Results Of the 400 questionnaires sent, 2 were undeliverable and 189 were returned (of which 88 within 2 months; the remainder were returned after a reminder was sent), representing an overall response rate of 47%. Twenty‐two
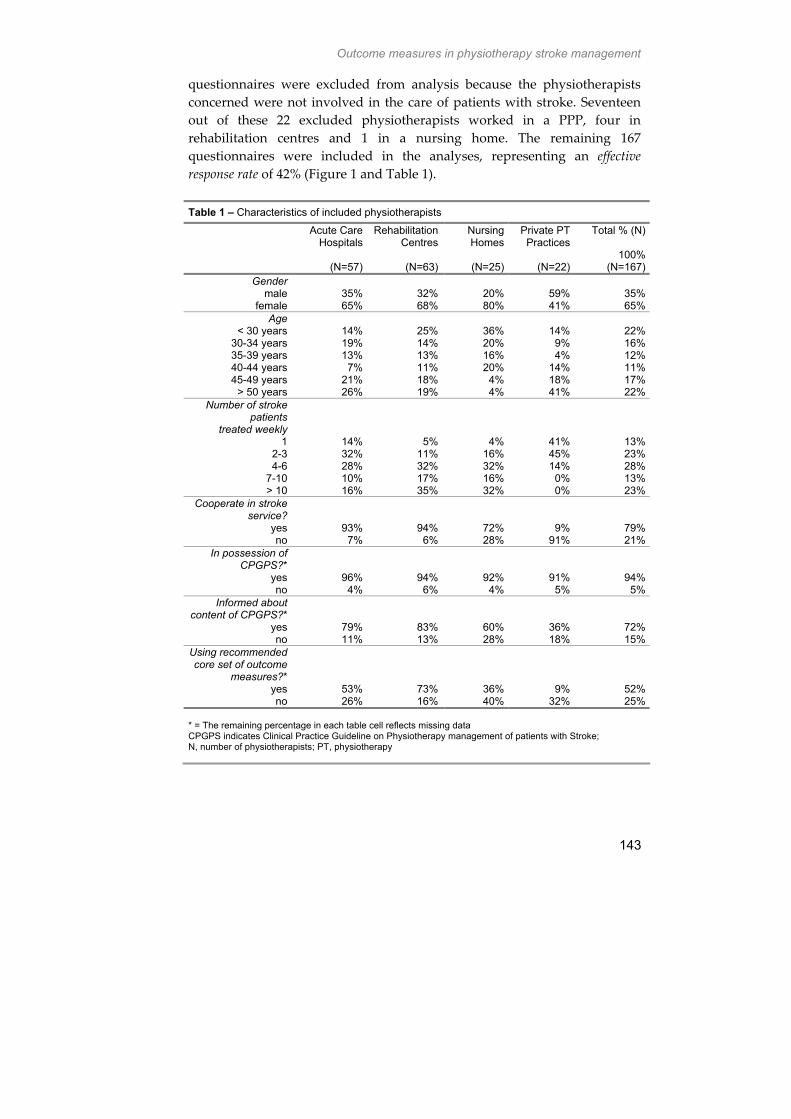
Outcome measures in physiotherapy stroke management
143
questionnaires were excluded from analysis because the physiotherapists concerned were not involved in the care of patients with stroke. Seventeen out of these 22 excluded physiotherapists worked in a PPP, four in rehabilitation centres and 1 in a nursing home. The remaining 167 questionnaires were included in the analyses, representing an effective response rate of 42% (Figure 1 and Table 1).
Table 1 – Characteristics of included physiotherapists
Acute Care Hospitals
(N=57)
Rehabilitation Centres
(N=63)
Nursing Homes
(N=25)
Private PT Practices
(N=22)
Total % (N)
100% (N=167)
Gender male
female 35%65%
32% 68%
20% 80%
59% 41%
35% 65%
Age < 30 years
30-34 years 35-39 years 40-44 years 45-49 years
> 50 years
14%19%13% 7% 21%26%
25%14%13%11%18%19%
36%20%16%20% 4% 4%
14% 9% 4% 14% 18% 41%
22% 16% 12% 11% 17% 22%
Number of stroke patients
treated weekly 1
2-3 4-6
7-10 > 10
14%32%28%10%16%
5%11%32%17%35%
4% 16% 32% 16% 32%
41% 45% 14% 0% 0%
13% 23% 28% 13% 23%
Cooperate in stroke service?
yes no
93% 7%
94% 6%
72%28%
9% 91%
79% 21%
In possession of CPGPS?*
yes no
96% 4%
94% 6%
92% 4%
91% 5%
94% 5%
Informed about content of CPGPS?*
yes no
79%11%
83%13%
60% 28%
36% 18%
72% 15%
Using recommended core set of outcome
measures?* yes no
53%26%
73%16%
36% 40%
9% 32%
52% 25%
* = The remaining percentage in each table cell reflects missing data CPGPS indicates Clinical Practice Guideline on Physiotherapy management of patients with Stroke; N, number of physiotherapists; PT, physiotherapy

Chapter 6
144
Section I: characteristics of the effective response Of the 167 physiotherapists whose information was analysed, 63 worked in RC, 57 in ACH, 25 in NH, and 22 in PPP. Most of these physiotherapists worked in an institutional or interinstitutional stroke service (N=132; 79%), had a copy of the CPGPS (94%), were knowledgeable about the content of the CPGPS (72%) and reported using at least some of the recommended measurement instruments of the CPGPS (52%). Most of the physiotherapists who worked in PPP had a copy of the CPGPS (N=20; 91%) and did not work in a stroke service (91%). Of these physiotherapists in PPP, 46% and 69% did not provide information about the content of the CPGPS and their use of the core set of recommended outcome measures.
Section 2: self‐reported use of recommended outcome measures The 167 physiotherapists reported using three of the seven recommended outcome measures. The most widely used measurement instrument was the FAC (N=82; 49%); the least used was the FAT (N=11; 7%). Specified per setting, the highest reported use of the seven measurement instruments was among physiotherapists working in RC (median=4 / modus=4), followed by physiotherapists working in ACH (3 / 3), in NH (2 / 0) and in PPP (0 / 0). Physiotherapists working in RC or ACH made significantly greater use of outcome measures than their colleagues working in PPP (4 versus 0 and 3 versus 0; p<0.001 and p=0.02 respectively).
Physiotherapists working in PPP reported the most infrequent use of the recommended measurement instruments: reported use was lower than 10% for six of the seven measures. The highest reported use of outcome measures was by physiotherapists working in RC, ranging from 79% for the BBS (N=50) to 11% for the FAT; and the lowest was by physiotherapists working in PPP, ranging from 23% for the TMW (N=5) to 5% for the BI (Table 2).
Overall, outcome monitoring of the patient’s health status at fixed time points as recommended by the CPGPS varied from 69% (N=115) in the week of admission to 16% at 6 months after stroke (Table 3). Compared to physiotherapists working in the other settings, physiotherapists working in PPP followed the guideline recommendations the least in this respect, ranging from 18% (N=4) at 6 months after stroke to 5% at discharge or at the end of a treatment period. The number of missing values for these physiotherapists was relatively high (≥ 45%).
Most physiotherapists (93%) reported sending a discharge letter to the professional responsible for the further treatment of the patient (proportion of physiotherapists by setting: ACH=96%; RC=93%; NH=83% and

Outcome measures in physiotherapy stroke management
145
PPP=100%), whereas only 42% of them stated receiving such discharges letter (RC=60% NH=54%; PPP=42%; and ACH=12%).
The association between the sum scores of self‐reported use of core outcome measures and the number of stroke patients treated weekly was only significant (though weak) for physiotherapists working in ACH (rho=0.35; p=0.009). For the other settings, no significant relation was found (RC, rho=0.18, p=0.17; NH, rho=‐0.16, p=0.46; and PPP, rho=0.15, p=0.64). Physiotherapists’ age was negatively, but not significantly, associated with their compliance with the core set of measurements (ACH, rho=‐0.13, p=0.97; RC, rho=‐0.25, p=0.07; NH, rho=‐0.08, p=0.70; and PPP, rho=‐0.14, p=0.27).
Table 2 – Self-reported use of recommended core outcome measures by physiotherapists
Acute Care Hospitals
(N=57)
Rehabilitation Centres
(N=63)
Nursing Homes
(N=25)
Private PT Practices
(N=22)
Total % (N)
100% (N=167)
Motricity Index* yes no
47% 42%
49%44%
28%64%
5% 55%
40% 48%
Trunk Control Test* yes no
60%32%
40%52%
40%52%
9% 50%
43% 45%
Berg Balance Scale* yes no
33%49%
79%17%
40%52%
5% 55%
48% 38%
Functional Ambulation Categories*
yes no
49%39%
67%24%
44%48%
5% 55%
49% 37%
Ten Metre Walk* yes no
19%65%
73%22%
40%52%
23% 36%
44% 44%
Frenchay Arm Test* yes no
4%79%
11%79%
4%88%
5% 55%
7% 79%
Barthel Index* yes no
39%47%
19%76%
36%60%
5% 50%
26% 62%
* = The remaining percentage in each table cell reflects missing data N indicates number of physiotherapists; PT, physiotherapy
Section 3: Barriers and facilitators questionnaire (BFQ) A: Psychometrics of BFQ All data of the BFQ were normally distributed. The internal consistency of the complete BFQ was good (Cronbachʹs α=0.86). Factor analysis identified six factors that together explained 65% of the variance in the use of outcome

Chapter 6
146
measures (Table 4). These were: (1) ‘personal environment’ (explained 15.4% of variance, Cronbach’s α=0.86); (2) ‘practitioner’ (12.1%, α=0.77); (3) ‘patient’ (10.5%, α=0.61); (4) ‘professional attitude’ (9.6%, α=0.58); (5) ‘economic environment’ (9.5%, α=0.62); and (6) ‘administrative environment’ (7.0%, α=0.34).
Table 3 – Self-reported use of assessment time points by physiotherapists
According to
recommendations in CPGPS:7
Acute Care Hospitals
(N=57)
Rehabilitation Centres
(N=63)
Nursing Homes
(N=25)
Private PT Practices
(N=22)
Total % (N)
100% (N=167)
In week of admission* yes no
84%11%
81%14%
56%40%
9%32%
69% 19%
In week of discharge* yes no
77%16%
60%29%
48%40%
5%41%
57% 28%
In week of multidisciplinary
meeting* yes no
33%49%
67%22%
36%52%
5%36%
43% 38%
3 months after onset of stroke*
yes no
4%70%
21%65%
44%48%
14%41%
17% 61%
6 months after onset of stroke*
yes no
4%70%
14%70%
44%48%
18%32%
16% 62%
* = The remaining percentage in each table cell reflects missing data N indicates number of physiotherapists; PT, physiotherapy
B: Outcomes of BFQ Four major facilitators and three barriers to the use of outcome measures were identified (Table 4). Facilitators were ‘a positive attitude towards outcome measures’ (mentioned by 156 physiotherapists = 93%), ‘familiarity with outcome measures’ (90%), ‘ability to make a comparative clinical assessment’ (90%), and ‘cooperation of colleagues in applying outcome measures’ (83%). The barriers that were mentioned the most were ‘changing routines’ (N=52; 32%), ‘time investment’ (29%), and ‘financial compensation’ (21%). Physiotherapists working in different settings mentioned different barriers and facilitators (see Table 4). The most marked differences concerned the factors ‘personal environment’ (PPP‐RC (p=0.02) and PPP‐ACH (p=0.02)), ‘practitioner’ (PPP‐RC (p<0.001); PPP‐ACH (p<0.001); PPP‐NH (p=0.014) and RC‐NH (p=0.02)) and ‘economic environment’ (PPP‐RC (p=0.03)). The other three factors were not significantly different between settings.

Outcome measures in physiotherapy stroke management
147
Table 4 – Barriers to and facilitators for the use of the recommended outcome measures, as reported by physiotherapists Factor:
% Fully disagree or disagree* % Agree or fully agree*
‘Personal environment’ ACH RC NH PPP Tot ACH RC NH PPP Tot
1. Familiarity with outcome measures 0.0 1.9 7.1 16.7 2.5 88.9 92.4 85.8 83.3 89.8
2. Experience with outcome measures 11.1 5.7 28.6 66.7 13.5 77.8 88.6 57.1 16.7 77.1
3. Knowing much about outcome measures 6.7 7.5 14.3 14.3 8.4 73.3 75.5 64.3 57.1 72.2
4. Trained to use outcome measures correctly 4.4 5.8 7.1 14.3 5.9 64.5 75.0 64.3 57.1 68.7
‘Practitioner’ ACH RC NH PPP Tot ACH RC NH PPP Tot
5. Cooperation of fellow physiotherapists in applying outcome measures
0.0 1.9 7.1 33.3 3.4 88.9 92.4 64.3 33.4 83.1
6. Cooperation of managers in applying outcome measures
11.6 5.7 7.7 50.0 9.0 57.5 81.1 53.8 0.0 71.2
7. No need for extra accommodation to apply outcome measures**
6.8 2.0 7.1 0.0 4.3 65.9 92.1 64.3 50.0 76.6
8. Outcome measures fit in with my daily practice routine
8.8 3.8 7.1 14.3 6.7 73.3 83.0 64.3 57.1 75.6
‘Patient’ ACH RC NH PPP Tot ACH RC NH PPP Tot
9. Outcome measures give patients insight into their physical functioning
20.0 5.7 0.0 14.3 10.9 37.8 66.0 78.6 28.6 54.6
10. Outcome measures leave enough room for individual patients’ preferences
6.7 7.7 7.1 16.7 7.7 53.3 63.5 50.0 83.3 59.9
11. Lay-out of measurement part of CPGPS makes it easy to use
13.3 11.5 0.0 0.0 10.2 35.6 61.6 66.7 16.7 50.0
‘Professional attitude’ ACH RC NH PPP Tot ACH RC NH PPP Tot
12. No general reluctance to adhere to guidelines**
4.4 7.5 0.0 0.0 5.1 82.2 73.6 92.9 42.9 77.3
13. Positive attitude towards the use of outcome measures
0.0 0.0 0.0 0.0 0.0 95.5 94.3 92.9 71.4 93.3
14. Outcome measures allow me to make a balanced clinical assessment
0.0 2.0 6.7 0.0 1.7 88.6 90.2 86.7 100 89.7
15. No problems with changing routines** 22.2 37.7 50.0 14.3 31.8 51.1 34.0 35.7 57.1 42.1
‘Economic environment’ ACH RC NH PPP Tot ACH RC NH PPP Tot
16. Use of outcome measures does not require financial compensation**
31.8 7.5 20.0 66.7 21.1 27.3 66.1 66.6 0.0 48.3
17. Patients do not find the use of outcome measures too time-consuming**
6.6 5.7 0.0 0.0 5.1 62.2 60.3 35.7 33.3 56.8
18. Use of outcome measures is not too time-consuming**
26.6 26.4 28.5 57.1 28.6 31.1 56.6 42.8 28.6 43.7
‘Administrative environment’ ACH RC NH PPP Tot ACH RC NH PPP Tot
19. No risk that use of outcome measures will be abused for disciplinary action against physiotherapists**
6.8 4.1 0.0 16.7 5.3 38.6 38.8 40.0 33.3 38.6
20. Description of outcome measures is mainly correct
15.9 17.7 20.0 33.3 18.1 47.7 35.3 40.0 16.7 39.7
ACH indicates acute care hospitals; NH, nursing homes; RC, rehabilitation centres; PPP, private physiotherapy practices; CPGPS, Clinical Practice Guideline on the Physiotherapy management of patients with Stroke. *The remaining percentages correspondent to ‘do not agree nor disagree’ answers. ** The original statements of the BFQ were reformulated for the purpose of data analysis

Chapter 6
148
Discussion The outcome measures recommended by the CPGPS appear to be used modestly in physiotherapy practice (Table 2 and 3) leaving ample room for improvement in this respect among physiotherapists working in stroke management in the Netherlands. While most physiotherapists were positive about using such clinical outcome measures (Table 4, item 13), only half of them actually claimed to use these instruments (Table 2), with the highest use being reported by physiotherapists who either reported to be familiar with the content of the guideline or were involved in institutional stroke management with a relatively high case load or both (Table 1). Almost half of the therapists reported using measurement instruments for mobility‐related activities (40% MI, 43% TCT and 48% BBS) and walking (44% TMW and 49% FAC). Instruments broadly quantifying ADL (BI) and hand and arm use (FAT) were reported to be used far less, by 26% and 7% of the physiotherapists, respectively (see Table 2). The frequency with which therapists claim to assess patients decreased if patients were situated in (or perhaps transferred to) the acute care setting (ACH), the long stay in RC and NH, or were treated in PPP (Table 3). Physiotherapists working in PPP in particular reported poor adherence to the CPGPS recommendations (Table 2 and 3). This might be attributable more to the phase of rehabilitation of the patients than to the setting per se, as these data are in line with those of Lennon (2% of senior physiotherapists in UK stroke care reassess patients at 6 months after stroke).34 Alternatively, this might be a consequence of the relatively low case load (Table 1) and barriers, such as physiotherapists’ opinions about financial compensations and competencies, in PPP (Table 4). While we expected that physiotherapists who regularly treated stroke patients would make most use of outcome measures, there was only a weak correlation between the number of patients treated and guideline adherence, and only for physiotherapists working in ACH (rho=0.35; p<0.01). This weak correlation also means that physiotherapists who saw few patients (i.e., those working in PPP) did not use the guideline to monitor patients’ functional status either.
An adequate sample of physiotherapists according to Field completed the questionnaire,31 leading to an acceptable response rate,3 comparable to that in other similar studies.2,8,34 Those physiotherapists who have a special interest in guidelines were more likely to respond in the present survey, resulting in selection bias, and in combination with socially preferable answers this may mean that the use of outcome measures was overestimated. The use of outcome measures appears to be governed by the

Outcome measures in physiotherapy stroke management
149
physiotherapists’ personal environment, the role of practitioner and the economic environment (Table 4). Almost a third of the physiotherapists reported reluctance to change routines as a barrier to the use of outcome measures (item 15), in parallel with some of the economic environment (item 16 and 18). These distinct barriers have been mentioned by other authors.35,36 In this respect, one should bear in mind the differences in the responses between settings, which may at the same time reflect the progress of rehabilitation in consecutive settings. This especially holds true for physiotherapists working in a PPP. The therapists in PPP differed significantly more than their colleagues (p<0.05) on items such as reported experience with outcome measures, cooperation of managers in applying outcome measures, financial compensation, and time investment (see Table 4, items 2, 6, 16 and 18, respectively). The present response supports the tailoring of implementation strategies to physiotherapists in general to the different Dutch stroke settings they are working in. Although Cronbach’s alpha for the overall BFQ was adequate, not all factors reached the generally accepted standard of 0.7. Three factors have a moderate internal consistency, varying from 0.58 to 0.62, and only the ‘administrative environment’ factor did not reach an acceptable level. All in all, Dutch physiotherapists reported a positive attitude and a moderate use of outcome measures, with those working in PPP adhering poorly to the CPGPS recommendations related to outcomes.
We sampled 100 physiotherapists per setting, whose age and sex were comparable to those of the general Dutch physiotherapist population.37 Although physiotherapists working in PPP were probably underrepresented because two‐thirds of practicing physiotherapists in the Netherlands (about 12,000 of 18,650) work in a PPP,37,38 it should be remembered that few patients with stroke consult such physiotherapists38 (see Table 1). However, a larger study should investigate not only the reported use but also the actual use and performance of outcome measures. Such an investigation should be combined with a study of the origin of explicit barriers to and facilitators for guideline implementation. Physiotherapists tend to overestimate their use of such instruments, as can be seen in comparisons of actual use and self‐reported use (Chapter 7), possibly because of their tendency to give socially desirable answers. This was probably also the case in the present study, which all the more suggests that the use of outcome measures could be improved. Nevertheless, physiotherapists claimed to use the recommended measurement instruments, with the exception of the FAT, which was introduced only recently with the publication of the CPGPS in the Netherlands, and was thus relatively unknown at the time of the survey.

Chapter 6
150
Alternatively, the FAT39 might be used less because physiotherapists do not expect functional recovery of the paretic arm, and occupational therapists take over the assessment of the paretic arm. The low reported use of the BI can be explained, in agreement with the data by Lennon,34 from the fact that in intramural settings (ACH, RC, and NH), it is usually other members of a multidisciplinary team (e.g. occupational therapists) who monitor patients’ arm and hand use with the help of this ADL outcome measure. Future research therefore needs to ask for both the use of the measure itself and the use of the data produced by an instrument.
With the exception of the FAT the self‐reported use of the other outcome measures by the Dutch physiotherapists in our sample was between 26% and 49%, which is comparable with the baseline measures in other studies investigating the (self‐reported) use of measurement instruments.8,9,12
The decreasing frequency of outcome assessment throughout the rehabilitation process (Table 3) seems to be associated with the fixed time points of assessment recommended in the guideline.7 This ‘fixed‐time‐point strategy’ for the use of outcome measures contrasts with the ‘success‐of‐treatment‐related strategy’ advocated by Glasziou et al.4 Glasziou recognized the need for different monitoring intervals for different phases, such as the phases of a disease for diagnosis, prognosis and therapy evaluation4 In practice, however, the physiotherapists surveyed may have used the measurement instruments to monitor the success of treatment rather than to monitor patient functional recovery per se. The fact remains that the assessment frequency was low, lower than that reported by others.15,40 Another explanation for the decreasing frequency of use of outcome measures throughout the rehabilitation process is that physiotherapists in ACH were unable to use measurement instruments at for instance 6 months after stroke, because their patients had moved on from the ACH by then.
As yet physiotherapists do not routinely use clinical assessment instruments in the management of patients with stroke. The use of clinical outcome measures in different phases of a disease for diagnosis, prognosis and therapy evaluation to monitor the health status of patients can help physiotherapists to specify relevant and attainable treatment goals, to get feedback on the success during the intervention and to optimise the communication with patients and/or members of an interdisciplinary team.1‐3 However, physiotherapists seem unable to educate themselves in the use of clinical measurement tools. If this is indeed so, teaching physiotherapists to enhance the use of outcome measures has to be integrated in a clinical reasoning process in the management of patients with stroke. Setting‐specific strategies are needed to promote the implementation of clinical

Outcome measures in physiotherapy stroke management
151
outcome measures in the physiotherapy management of patients with stroke,18 based on the barriers and facilitators found in this study. Such strategies could be based on the implementation model by Lomas et al,41,42 with a focus on education in stroke management. In future guideline development and dissemination, these tailored implementation strategies will have to be based on an initial analysis of the patients and professionals involved and their specific institutional context.
Acknowledgements We would like to thank the students of the Graduate Programme of Physiotherapy Science at the University of Utrecht (Ivo Daanen, Hans Herik, Erwin Huiszoon, Han Kingma, Leny de Ligny, Koert Nederbragt, Eric Passchier, Peter Viehoff, Judith Weijman, and Elles Zock) for contributing to this project, and Dr Paul Westers of the Centre for Biostatistics (Utrecht University) for his valuable suggestions for improving the statistical analysis. We are grateful to all the physiotherapists who responded to this survey.
References 1. Parker‐Taillon D. CPA initiatives put the spotlight on evidence‐based practice in
physiotherapy. Physiother Can 2002; 24:12‐15.
2. Haigh R, Tennant A, Biering‐Sorensen F et al. The use of outcome measures in physical medicine and rehabilitation within Europe. J Rehabil Med 2001; 33:273‐278.
3. Jette DU, Bacon K, Batty C et al. Evidence‐based practice: beliefs, attitudes, knowledge, and behaviors of physical therapists. Phys Ther 2003; 83:786‐805.
4. Glasziou P, Irwig L, Mant D. Monitoring in chronic disease: a rational approach. BMJ 2005; 330:644‐648.
5. Hammond R. Evaluation of physiotherapy by measuring outcome. Physiotherapy 2000; 86:170‐172.
6. Partridge CJ. The outcome of physiotherapy and its measurement. Physiotherapy 1982; 68:362‐363.
7. Van Peppen RPS, Hendriks HJM, Van Meeteren NLU et al. The development of a clinical practice stroke guideline for physiotherapists in The Netherlands: A systematic review of available evidence. Disabil Rehabil 2007; 29:767‐783.
8. Abrams D, Davidson M, Harrick J et al. Monitoring the change: current trends in outcome measure usage in physiotherapy. Man Ther 2006; 11:46‐53.

Chapter 6
152
9. Akinpelu AO, Eluchie NC. Familiarity with, knowledge, and utilization of standardized outcome measures among physiotherapists in Nigeria. Physiother Theory Pract 2006; 22:61‐72.
10. Chesson R, Macleod M, Massie S. Outcome measures used in therapy departments in Scotland. Physiotherapy 1996; 82:673‐679.
11. Duckworth M. Outcome measurement selection and typology. Physiotherapy 1999; 85:21‐27.
12. Maher C, Williams M. Factors influencing the use of outcome measures in physiotherapy management of lung transplant patients in Australia and New Zealand. Physiother Theory Pract 2005; 21:201‐217.
13. Van Peppen RPS, Kwakkel G, Harmeling BC et al. Clinical practice guideline on Physiotherapy‐management of patients with Stroke [in dutch: KNGF‐richtlijn Beroerte]. Ned Tijdschr v Fysioth 2004; 114 (5:supplement):1‐78.
14. WHO. ICF‐introduction, the International Classification of Functioning Disability and Health. 2001. Geneve. http://www.who.int/classification/icf/intros/ICF‐Eng‐Intro.pdf .
15. Australian Physiotherapy Association. APA Position Statement ‐ Clinical justification and outcome measures. 2003: https://apa.advsol.com.au/staticcontent/staticpages/position_statements/public/ClinicalJustification&Outcome%20Measures.pdf
16. Jette AM. Assessing disability in studies on physical activity. Am J Prev Med 2003; 25(3 Suppl 2):122‐128.
17. Geyh S, Cieza A, Schouten J et al. ICF Core Sets for stroke. J Rehabil Med 2004;(44 Suppl):135‐141.
18. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patientsʹ care. Lancet 2003; 362:1225‐1230.
19. Portney LG, Watkins MP. Foundations of clinical research, applications to practice. 2nd edition ed. New Jersey: Prentice‐Hall, 2000.
20. Feinstein JL. Clinimetrics. New Haven ‐ London: Yale University Press, 1987.
21. Demeurisse G, Demol O, Robaye E. Motor evaluation in vascular hemiplegia. Eur Neurol 1980; 19:382‐389.
22. Franchignoni FP, Tesio L, Ricupero C et al. Trunk control test as an early predictor of stroke rehabilitation outcome. Stroke 1997; 28:1382‐1385.
23. Berg K, Wood‐Dauphinee S, Williams JI. The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med 1995; 27:27‐36.
24. Holden MK, Gill KM, Magliozzi MR. Gait assessment for neurologically impaired patients. Standards for outcome assessment. Phys Ther 1986; 66:1530‐1539.
25. Wade DT. Measurements in neurological rehabilitation. Oxford: Oxford University Press, 1992.
26. Heller A, Wade DT, Wood VA et al. Ward E. Arm function after stroke: measurement and recovery over the first three months. J Neurol Neurosurg Psychiatry 1987; 50:714‐719.

Outcome measures in physiotherapy stroke management
153
27. Collin C, Wade DT, Davies S et al. The Barthel ADL Index: a reliability study. Int Disabil Stud 1988; 10:61‐63.
28. Commissie CVA‐Revalidatie. Rehabilitation after a stroke, guidelines and recommendations for health care professionals (in Dutch: Revalidatie na een beroerte: richtlijnen en aanbevelingen voor zorgverleners). Franke EAM, editor. 2001. Den Haag, Dutch Heart Foundation (in Dutch: Nederlandse Hartstichting).
29. Grol R, Wensing M, Eccles M. Improving patient care. The implementation of change in clinical practice. London: Elsevier Butterworth Heinemann, 2005.
30. Peters MAJ, Harmsen M, Laurant MGH et al. Room for improvement? Barriers to and opportunities for improvement of patient care [dutch: Ruimte voor verandering? Knelpunten en mogelijkheden voor verbeteringen in de patientenzorg]. Centre for Quality of Care Research (WOK), editor. 2003. Nijmegen, The Netherlands, Radbout University Medical Centre.
31. Field AP. Discovering Statistics using SPSS. second ed. London: SAGE Publications Ltd, 2005.
32. Learner J, Goodman NW. Descriptions of correlation. Lancet 1996; 348:199‐200.
33. Streiner DL, Norman GR. Health measurement scales, a practical guide to their development and use. second ed. New York: Oxford University Press, 2003.
34. Lennon S. Physiotherapy practice in stroke rehabilitation: a survey. Disabil Rehabil 2003; 25:455‐461.
35. Pollock AS, Legg L, Langhorne P et al. Barriers to achieving evidence‐based stroke rehabilitation. Clin Rehabil 2000; 14:611‐617.
36. Turner‐Stokes L, Turner‐Stokes T. The use of standardized outcome measures in rehabilitation centres in the UK. Clin Rehabil 1997; 11:306‐313.
37. Kenens RJ, Hingstman L. Cijfers uit de registratie van fysiotherapeuten, peiling 1 januari 2005. 2006. Utrecht, NIVEL.
38. Vugts CJ, Van der Velden LFJ, Hingstman L et al. Behoefteraming Fysiotherapeuten 2002‐2015. 2003. Utrecht, NIVEL/Prismant.
39. Nakayama H, Jorgensen HS, Raaschou HO et al. Recovery of upper extremity function in stroke patients: the Copenhagen Stroke Study. Arch Phys Med Rehabil 1994; 75:394‐398.
40. Rothstein JM, Echternach JL, Riddle DL. The Hypothesis‐Oriented Algorithm for Clinicians II (HOAC II): a guide for patient management. Phys Ther 2003; 83:455‐470.
41. Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care 1998; 7:149‐158.
42. Lomas J. Teaching old (and not so old) does new tricks: effective ways to implement research findings. In: Dunn EV, Norton PG, Steward M, Tudiver F, Bass MJ, editors. Volume 6: Disseminating research / changing practice. London: Sage, 1993.

Chapter 6
154

CHAPTER
Feasibility and effectiveness of an educational
program to promote the use of outcome measures by
physiotherapists involved in stroke rehabilitation:
An RCT on tutor expertise
Roland PS Van Peppen
Marieke J Schuurmans
Eric C Stutterheim
Eline Lindeman
Nico LU Van Meeteren
Submitted

Chapter 7
156
Abstract Objective: To determine the feasibility and effectiveness of a tutor‐guided educational programme for physiotherapists, the Physiotherapists‘ Educational Programme on Clinimetrics in Stroke (PEPCiS), intended to promote the use of outcome measures in the management of patients with stroke. Design: Randomized controlled feasibility trial. Methods: Thirty voluntarily participating physiotherapists involved in stroke management were randomized into two groups and participated in 5 tutor‐guided training sessions for physiotherapists (i.e., PEPCiS). Tutors differed in their clinical experience with outcome measures in stroke. Feasibility was estimated by physiotherapists’ adherence to PEPCiS, satisfaction with PEPCiS and their appreciation of the tutoring style of the allocated tutor; effectiveness was estimated by counting the frequencies with which outcome measures were mentioned in the records of patients entrusted to the participating therapists. Results: The participants’ attendance record was generally good (a median of 5 of the 5 sessions; range 4‐5) and they were satisfied with PEPCiS (mean: 7.5 on a 0‐10 scale). In the entire group (N=30) the use of outcome measures increased from 3 per patient before PEPCiS to 5 thereafter (p=0.001). Between‐group differences were non‐significant for the totals of the instruments used (median 3 to 6 in the expert tutor group [ETG] vs. 3 to 4 in the non‐expert tutor group [NETG]; p=0.07). Physiotherapists in the ETG appreciated the PEPCiS content, their knowledge gain and all tutor style aspects significantly more than those in the NETG (p<0.05). Conclusion: The present pilot study suggests that education by PEPCiS enhances the use of clinical outcome measures by physiotherapists in the management of patients with stroke. A future study with sufficient power will investigate the influence of PEPCiS as well as interfering factors, e.g. tutor expertise and performance, in order to establish and improve the effectiveness of educational interventions as a part of implementation strategies for the regular use of outcome measures by physiotherapists. Key Words: physiotherapy, cerebrovascular disorders, outcome measures, implementation, educational programme

Feasibility and effectiveness of PEPCiS
157
Introduction Like their colleagues in other countries1‐6 physiotherapists in the Netherlands7 fail to regularly use outcome measures. This was demonstrated again recently for Dutch physiotherapists involved in stroke management (Chapter 6), despite the recommendation for regular use of outcome measures in the relevant professional physiotherapy guideline of the Royal Dutch Society for Physical Therapy, the Clinical Practice Guideline for Physiotherapy management of patients with Stroke (CPGPS).8,9 Common barriers to the proper use of outcome measures include lack of experience and uncertainty about the use of the instruments.1,5,10‐12 Despite these barriers, physiotherapists have reported an overall positive attitude towards the use of outcome measures.1,12 In line with the opinion of several experts in the field, physiotherapists are aware of the importance of a considered use of outcome measures to monitor the health status of patients as an essential aspect of good clinical practice.13,14
In an attempt to facilitate the practical use of outcome measures and hence to improve the transparency of the clinical decision making process according to the recommendations in the CPGPS,15 a ‘Physiotherapists’ Educational Programme on Clinimetrics in Stroke’ (PEPCiS) has been developed. This educational programme was designed to train Dutch physiotherapists involved in stroke management to use outcome measures and thereby to increase the use of these measures in their daily practice routine.
Training is often a precondition for successful behavioural changes of professionals like using outcome measures on a regular basis.16 In such contexts, interactive and personal training in small groups has shown to be more effective than more traditional lectures in large groups.17,18 We tried to gain further insights into the necessary behavioural change in physiotherapists and to identify the perceived motivational, organizational and institutional barriers to and facilitators for this change, using the theories by Ajzen19 and Grol20 respectively.
Consequently, this pilot study aimed to investigate the feasibility (in terms of adherence and satisfaction) and effectiveness (in terms of frequency with which outcome measures were mentioned) of the PEPCiS programme as regards increasing physiotherapists’ use of outcome measures in stroke care. Secondary to this aim, the influence of tutor style will be explored.

Chapter 7
158
Method Design In this pilot study, 30 voluntarily participating physiotherapists involved in the management of patients with stroke were stratified based on the setting in which they work (i.e., acute care hospital, rehabilitation centre, nursing home or private physiotherapy practice). Within each stratum, physiotherapists were randomly assigned to group taught by an expert tutor (expert tutor group: ETG, N=15) or a group taught by a non‐expert tutor (NETG, N=15). The ETG was taught by a tutor who had extensive experience with outcome measures in stroke (RvP; > 10 years), whereas the NETG was taught by a tutor with little experience in this respect (MW; < 1 year). Both tutors had comparable experience with teaching the programme, which they had gained in a prior pilot project,21 as well as with process‐oriented tutoring (> 3 years) from their regular job as lecturers at the University of Applied Sciences Utrecht. The participating physiotherapists were unaware of the differences in expertise between the allocated tutors. Physiotherapists in the ETG and NETG groups received the same educational programme aimed to implementing and enhancing the use of outcome measures in clinical practice. The programme is based on several learning strategies and focusing on the evidence‐based practice, clinical reasoning and outcome measures recommended in the CPGPS. The educational programme was presented from March to June 2006.
Subjects For logistical reasons, a maximum of 30 physiotherapists were recruited from responders to a ‘call for participation’ in the newsletter of the Utrecht regional section of the Royal Dutch Society for Physical Therapy. Six weeks prior to the study, all responders received a hard‐copy of the clinical practice guideline (CPGPS) and were instructed to read the whole document thoroughly. In a preparatory meeting, 4 weeks before the start of the educational programme, all responders were informed about the study. We tried to blind the participants by deliberately leaving them unaware of the precise aims of the study, namely the planned patient record analyses and the contrast between the two tutors. To be included participants had to treat at least 1 patient with stroke per week on a regular basis.
Intervention Physiotherapists in both groups attended the same interactive evidence‐based training course, the Physiotherapists’ Educational Programme on

Feasibility and effectiveness of PEPCiS
159
Clinimetrics in Stroke (PEPCiS, see Appendix).15 The two groups of physiotherapists were taught on different evenings (Tuesdays and Thursdays respectively) in a fully‐equipped ‘clinimetrics‐classroom’ at the Institute for Human Movement Studies, Department of Physiotherapy of the University of Applied Sciences Utrecht, the Netherlands. The classroom setting included physiotherapy equipment, all materials and forms to record the outcome measures, and ‘on‐line’ computers for patient data recording. Both groups were taught in five 2‐hour evening sessions over a 14‐week period. The 5 training sessions started in week 11 of 2006 (March), and continued in weeks 13, 15, 20 and 25 (June 2006).
Measurements The intervention was assessed on variables of feasibility and effectiveness of the educational programme. Variables of feasibility were (1) the participants’ compliance with study procedures, (2) the participants’ satisfaction with PEPCiS and (3) the participants’ appreciation of the tutoring style of their allocated tutor. The variables of effectiveness were the actual use and self‐reported use of outcome measures by participants in their own practice routine. The characteristics of the participants, including the psychological predictors of behaviour, e.g. motivation according to the theory of planned behaviour,19 and the barriers to and facilitators for the use of outcome measures, were assessed at baseline (T0), while the feasibility variables were assessed after the end of the 14‐week intervention (T1). Actual use and self‐reported use were assessed at T0 and T1. Compliance with study procedures was assessed as attendance at the
training sessions and drop‐outs rates from the study. Attendance was recorded by the tutors at each session (ranging from 0 to 5 sessions) in programme diaries. Participants had to attend at least 4 of the 5 PEPCiS sessions to get credits for the quality register of the Royal Dutch Society for Physical Therapy. Drop‐outs were defined as participants who quit the study and were lost to follow‐up. Compliance with measurement procedures was assessed measured by counting the number of participants who (a) delivered their patients’ records (to assess actual use), and (b) completed the on‐line self‐report questionnaires (to assess self‐reported use), while recording those who were lost to analysis. Participant satisfaction was determined after the end of the intervention
(T1) using a 4‐item questionnaire. Each item was given a mark between 0 and 10. Information was obtained on satisfaction with PEPCiS, in terms of

Chapter 7
160
(1) ‘organization’, (2) ‘content’, (3) ‘knowledge gain’, and 4) ‘level of participation’. Participants’ appreciation of tutoring style was evaluated after the end
of the PEPCiS programme, using the Tutor Behaviour Questionnaire (TBQ).22,23 The TBQ consists of 39 items which explore tutoring style in terms of ‘knowledge of subject matter’ (19 items) and ‘skill in process facilitation’ (19 items), using 5‐point Likert‐scale (range 1 to 5), and ‘overall effectiveness’, defined as the participants’ perception of how well the tutor performed in his/her role (1 item; 1‐10 scale).22 Knowledge of subject matter was assessed using three scales assessing the corresponding sub‐categories of behaviour: A1) use of expertise (UE), i.e. the degree to which the tutor used his/her knowledge of the subject matter to help the participants; A2) cognitive congruence (CC), i.e. the degree to which the tutor understood the participants’ existing level of knowledge and A3) test orientation (TO), i.e. the degree to which the tutor focused on summative assessment to direct the physiotherapists’ learning. The ‘skill in process facilitation’ was assessed by three subscales: B1) authority (AU), i.e. the degree to which the tutor used authority to direct participants’ activities within the group; B2) role congruence (RC), i.e. the degree to which the tutor was able to empathize with, and relate to, participants’ lives; and B3) cooperation orientation (CO), i.e. the degree to which the tutor was interested in encouraging cooperation among members of the group.22 Psychological predictors of behaviour in terms of using the
recommended outcome measures were assessed at baseline (T0) using a questionnaire based on the Theory of Planned Behaviour (TPB).19 This questionnaire was developed using operationalisation instructions from the manual for health service researchers.24 The TPB is a model which is widely used to predict a wide range of behaviour25 and can also be applied to the behaviour of health professionals.26 The TPB proposes that ‘intention to engage in the behaviour’ (INT) and ‘perceived control over the behaviour’ (PBC) are the proximal predictors of (professional) behaviour. We hypothesized that participants with high INT and high levels of PBC would be more likely to change their professional behaviour and will use outcome measures more regularly. INT is defined as the motivation to engage in a particular behaviour (in this case: using outcome measures) and indicates the extent to which people are willing to try or how much effort they would invest to perform the behaviour.19 PBC is defined as ‘a person’s perception of the ease or difficulty of performing a behaviour’.19 The INT and PBC items

Feasibility and effectiveness of PEPCiS
161
were rated on 5‐point Likert scales. Mean scores were calculated for the items of INT and PBC, with a mean score of 5 meaning very high intention and perceived behaviour control, respectively. Perceived barriers and facilitators. The validated Barriers and
Facilitators Questionnaire (BFQ),12 which includes 20 statements (1‐5 scale), was used at baseline (T0) to identify perceived barriers to and facilitators for the use of outcome measures in everyday practice in physiotherapy stroke management. An initial analysis of perceived barriers to and facilitators for using outcome measures by professionals involved is a crucial condition for successful implementation20 of the outcome measures recommended in the CPGPS in daily physiotherapy practice. Actual use of outcome measures, defined as the number of times their use
was recorded in patient records by physiotherapists involved in stroke management, was assessed by analyzing patient records (maximum 5 per physiotherapist) for the frequency with which the participants used the core outcome measures recommended in the CPGPS (0 to 7). Before the start of the educational programme, participants had to bring an anonymous copy of their 5 most recent (stroke) patient records. The actual use of outcome measures was analysed again at T1 by assessing new patient records (maximum 5). Self‐reported use of outcome measures was assessed with a 7‐item
questionnaire relating to the 7 recommended outcome measures. The questions invited the participants to report their own use of the 7 recommended outcome measures for the 5 most recently treated patients on a 6‐point Likert scale, e.g., ‘I used the Berg Balance Scale in [1,2,3,4 or 5 patients: select one option] for the 5 patients with stroke I most recently treated’.
Statistical analysis Data were analysed by an independent researcher (ES) with SPSS 12.0 statistical software (SPSS Inc, Chicago, Illinois, USA), using a significance level of p<0.05. Summary descriptive statistics, i.e. central tendencies were computed for the actual and self‐reported use of recommended outcome measures.27 Differences in numbers of patient records at T0 and T1 and actual and self‐reported frequencies of use were converted to percentage scores to compare physiotherapists’ actual use and self‐reported use of

Chapter 7
162
outcome measures. The BFQ statements (1‐5 points on each statement) were converted to a sum score (max 100 points).
Baseline differences in group characteristics, adherence, satisfaction and tutor behaviour were analysed by either independent samples T‐test or Chi‐square test where appropriate.27,28 Non‐parametric statistical tests were used to analyze the change scores for the use of outcome measures by the total group (Wilcoxon). Between‐group comparisons for feasibility variables were made using the independent T‐test, while comparisons of the effectiveness variable (effect of training), i.e. the median of change scores for actual use between T0 and T1, were done with the Mann‐Whitney U‐test.27,28
Results
Physiotherapists Of the 41 physiotherapists who responded to the original invitation, 35 were involved in stroke management and were considered eligible after screening by telephone (Figure 1). However, 5 candidates were unable to fit the training sessions into their schedule leaving 30 participants. Figure 1. Flow of participants through the trial
ExpertTutor Group
(n=15)
41 responded to newsletter
30 physiotherapists randomized
6 excluded by criteria
35 screened by telephone
5 excluded
Non-ExpertTutor Group
(n=15)
0 withdrew at T1 -immediately after
intervention
0 withdrew at T1 -immediately after
intervention
15 physiotherapists15 physiotherapists

Feasibility and effectiveness of PEPCiS
163
Table 1 – Baseline characteristics of participating physiotherapists
Characteristics ETG (N=15)
NETG (N=15)
Total (N=30)
Statistics
Sig.*
Gender, female
12
13
25
0.24C
0.62
Setting of practice:ACH
RCNH
PPP
2 0 10 3
3 1 9 2
5 1 19 5
1.45C
0.69
Age, mean (SD), y
range, y
36.5 (9.8)
25-53
39.0
(10.2) 22-53
37.7 (9.9)
22-53
-0.64T
0.53
Experience in stroke management, mean (SD), y
range, y
9.5 (8.1) 2-27
11.0 (5.6)2-20
10.2 (6.9)2-27
-0.60T
0.55
Number of patients with stroke treated/ wk, median (mode), n
range
4 (3) 2-12
4 (3) 3-15
4 (3) 2-15
-0.54T
0.59
Psychological predictors of behaviour:- Intention, mean (SD)
- PBC, mean (SD)
4.2 (0.4) 3.7 (0.7)
4.1 (0.6) 3.9 (0.6)
4.2 (0.5) 3.8 (0.6)
0.34T
-1.05T
0.74 0.30
Barriers and facilitators to use outcome measures:
BFQ total scoremean (SD)
60.7 (5.2)
62.0 (4.9)
61.4 (5.0)
-0.68T
0.50
ACH indicates acute care hospitals; BFQ, barriers and facilitators questionnaire; N, number of physiotherapists; NH, nursing homes; RC, rehabilitation centres; PBC, perceived behavioural control; PPP, private physiotherapy practices; SD, standard deviation; sig., significance (p value); wk, weekly; and y, years. C=Chi‐square test; T=T‐test; * sig. at p<0.05
Table 1 shows the baseline characteristics of these 30 participating physiotherapists. The mean age of the participants was 38 years (SD: 10y). They had a mean of 10 years experience in stroke rehabilitation (SD: 7y) and treated about 4 patients with stroke per week. The majority of the participants in both experimental arms were female (N=25) and worked in nursing homes (N=19). No statistically significant baseline differences between the groups were found (p>0.05) in terms of age, median number of patients treated, experience, intention and perceived behavioural control or perceived barriers and facilitators (Table 1).

Chapter 7
164
Outcomes Feasibility (Table 2): Adherence to study procedures. There were no drop‐outs, and the
participants in both groups attended at a median of 5 of the 5 PEPCiS sessions. Twelve participants in each group were present at all 5 sessions. The remaining participants in the ETG (N=3) as well as in the NETG (N=3) attended 4 sessions. After the end of the PEPCiS programme, no significant differences were found between the two arms in terms of the number of anonymous copies of their most recent (stroke) patient records presented by the participants and completion of the on‐line self‐report questionnaires. Participants’ satisfaction. All participants in both groups (N=30) answered
the 4 questions about satisfaction with PEPCiS and rated the 4 items at 6.9 to 8.9 points. The mean score for satisfaction with PEPCiS as a whole was 7.5 points, ranging from 8.0 (ETG) to 6.9 (NETG). Physiotherapists in the ETG rated 2 items significantly higher than those in the NETG, i.e., ‘content’ (8.9 vs 7.8; p=0.02) and ‘ knowledge gain’ (8.6 vs 6.5; p=0.03). Participants’ appreciation of tutoring style. Compared to participants in the
NETG, those in the ETG reported a significantly higher degree of ‘knowledge of subject matter’ (73 vs 56 points; p<0.001) and ‘skill in process facilitation’ (71 vs 60; p<0.001) for their tutor. Participants in the ETG also rated the overall effectiveness of their tutor significantly higher (8.3 vs 6.2; p<0.001).
Effectiveness (Table 3): Use of outcome measures. For the entire group, the median actual use of the
7 recommended outcome measures, as recorded in the 5 patient records, increased significantly from 3 to 5, while the self‐reported use increased from 4 to 6 per patient (p<0.001) (Figure 2).
Except for the FAT and BI, the group as a whole showed a statistically significant change in the actual use of the recommended outcome measures (p<0.05) during the intervention, with increases for the other 5 measures ranging from 37% (for FAC) to 17% (for TMW). Self‐report use of all outcome measures showed a statistically significant increase between the baseline and post‐intervention assessments (p<0.05), varying from 43% (for FAC) to 21% (for FAT) (Figure 3).
Summarizing the use of all 7 recommended outcome measures (by calculating the sum score of percentages of means divided by the 7 outcome measures) shows that the actual use increased from 25% to 49%, and the self‐

Feasibility and effectiveness of PEPCiS
165
reported use from 30% to 61%, respectively, between the baseline and post‐ intervention assessments (Table 3).
Table 2 – Feasibility of PEPCiS
ETG
NETG
Outcome variables
Post intervention
(T1) (N=15)
Post intervention
(T1) (N=15)
T-statistics (T1)-between groups- (sign.)
1. Compliance with study procedures - Attendance / Drop-out
number of PTs (N):number of sessions: median, range 0-5
15 / 0 5 (4-5)
15 / 0 5 (4-5)
0.26
p = 0.80 - Delivered patient records:
PTs lost to analysis in (N)13 2
14 1
0.59 p = 0.56
- Completed self-report questionnaires:PTs lost to analysis in (N)
13 2
14 1
0.59 p = 0.56
2. Participants’ satisfaction (range 0-10) about:
- Organization of PEPCiS: mean (SD)
7.7 (0.8)
6.9 (1.9) 1.34
p=0.19
- Content of PEPCiS: mean (SD)
8.9 (1.0)
7.8 (1.9) 3.56
p = 0.02#
- Knowledge gain by PEPCiS: mean (SD)
8.6 (1.0)
6.5 (2.2) 3.26
p=0.03#
- Own participation in PEPCiS: mean (SD)
6.9 (0.8)
7.1 (1.3)
-0.36 p = 0.72
Overall score of the 4 PEPCIS items: 8.0 6.9
3. Participants’ appreciation of tutoring style (TBQ)
A. TBQ-subject-matter expertise (total of 3 scales): mean (SD)
72.7 (5.0)
56.1 (11.9)
4.63 p< 0.001#
B. TBQ-process facilitation skill (total of 3 scales) (mean (SD)
71.1 (4.5)
59.7 (6.8)
5.10 p< 0.001#
C. TBQ-Overall effectiveness (appreciation, 1-10 scale): mean (SD)
8.3 (0.5)
6.2 (1.5)
4.87 p< 0.001#
ETG indicates expert tutor group; NETG, non‐expert tutor group; N, number of physiotherapists; PT, physiotherapist; SD, standard deviation; TBQ, tutor behaviour questionnaire; and T1, post intervention; * Self‐reported use of outcome measures is based on a questionnaire about 5 most recently treated patients (converted to 0‐100% scores) ** Actual use of outcome measures, based on records of 5 most recently treated patients (converted to 0‐100% scores) # significance at p<0.05

Chapter 7
166
Cha
nge
in
tota
l gro
up,
T0 t
o T
1#
Wilc
oxon
(sig
)
3.4
(p=0
.001
# )
3.7
(p<0
.001
# )
3.0
(p=0
.003
# )
3.0
(p=0
.003
# )
3.4
(p=0
.001
# )
2.4
(p=0
.015
# )
0.9
(p=0
.35)
1.6
(p=0
.11)
Post
in
terv
entio
n (T
1)
27
5 (6
) [0
-7]
63 (3
8)
66 (3
7)
68 (3
7)
77 (3
4)
27 (3
2)
9 (2
5)
34 (3
6)
49
Tota
l gro
up
Bas
elin
e (T
0)
30
3 (2
) [0
-6]
28 (3
4)
39 (3
7)
38 (3
1)
40 (3
8)
10 (2
0)
4 (1
9)
18 (3
2)
25
Post
in
terv
entio
n (T
1)
14
4 (4
) [0
-6]
51 (4
1)
59 (3
7)
65 (3
8)
66 (3
6)
16 (2
8)
1 (2
9)
16 (2
0)
39
NET
G
Bas
elin
e (T
0)
15
3 (2
) [0
-6]
31 (3
6)
44 (3
9)
39 (2
8)
43 (3
9)
11 (1
8)
8 (2
6)
9 (2
1)
26
Post
in
terv
entio
n (T
1)
13
6 (6
) [0
-7]
76 (3
1)
74 (3
6)
72 (3
7)
89 (2
8)
40 (3
3)
17 (3
4)
53 (4
0)
60
ETG
Bas
elin
e (T
0)
15
3 (2
) [0
-6]
26 (3
4)
33 (3
4)
37 (3
6)
37 (3
8)
8 (2
1)
0 (-
)
26 (3
9)
24
Tab
le 3
E
ffect
iven
ess
of P
EP
CiS
Out
com
e va
riabl
es
1.
Act
ual u
se*:
(
N)
Med
ian
(mod
e) –
num
ber o
ut o
f 7R
CO
Ms:
[ran
ge]
Mea
n us
e %
(SD
)
-Mot
ricity
Inde
x
-Tru
nk C
ontro
l Tes
t
-Ber
g B
alan
ce S
cale
-Fun
ctio
nal A
mbu
latio
n C
ateg
orie
s
-Ten
Met
re W
alk
-Fre
ncha
y A
rm T
est
-Bar
thel
Inde
x
Sum
mar
izin
g th
e us
e of
all
7 R
CO
Ms
(%)

Feasibility and effectiveness of PEPCiS
167
Cha
nge
in
tota
l gro
up,
T0 t
o T
1#
Wilc
oxon
(sig
)
4.2
(p<0
.001
# )
4.0
(p<0
.001
# )
2.7
(p=0
.007
# )
4.0
(p<0
.001
# )
3.6
(p<0
.001
# )
3.0
(p=0
.003
# )
3.0
(p=0
.003
# )
2.3
(p=0
.019
# )
Post
in
terv
entio
n (T
1)
27
6 (5
) [4
-7]
70 (2
9)
73 (2
7)
77 (2
6)
91 (1
9)
39 (3
0)
22 (3
2)
53 (4
6)
61
Tota
l gro
up
Bas
elin
e (T
0)
30
4 (4
) [0
-6]
29 (3
6)
50 (3
9)
41 (3
4)
48 (4
3)
16 (2
3)
1 (7
)
25 (4
3)
30
Post
in
terv
entio
n (T
1)
14
5 (5
) [4
-7]
61 (3
2)
69 (2
5)
70 (2
7)
90 (2
2)
29 (2
7)
7 (1
3)
33 (4
5)
51
NET
G
Bas
elin
e (T
0)
15
4 (4
) [0
-6]
28 (3
6)
53 (3
8)
40 (3
3)
47 (4
3)
13 (2
2)
3 (1
0)
20 (4
1)
29
Post
in
terv
entio
n (T
1)
13
6 (7
) [5
-7]
80 (2
2)
79 (3
0)
85 (2
3)
92 (1
5)
49 (3
1)
39 (3
8)
74 (3
7)
71
ETG
Bas
elin
e (T
0)
15
4 (5
) [0
-6]
31 (3
6)
47 (4
2)
41 (3
6)
49 (4
4)
19 (2
3)
0 (-
)
31 (4
6)
31
Tabl
e 3
-
Con
tinue
d -
Out
com
e va
riabl
es
2.
Self-
repo
rted
use
**:
(
N)
Med
ian
(mod
e) –
num
ber o
ut o
f 7R
CO
Ms:
[ran
ge]
Mea
n us
e %
(SD
)
-Mot
ricity
Inde
x
-Tru
nk C
ontro
l Tes
t
-Ber
g B
alan
ce S
cale
-Fun
ctio
nal A
mbu
latio
n C
ateg
orie
s
-Ten
Met
re W
alk
-Fre
ncha
y A
rm T
est
-Bar
thel
Inde
x
Sum
mar
izin
g th
e us
e of
all
7 R
CO
Ms
(%)
ETG
indi
cate
s ex
pert
tuto
r gro
up; N
ETG
, non
-exp
ert t
utor
gro
up; N
, num
ber o
f phy
siot
hera
pist
s; R
CO
Ms,
reco
mm
ende
d co
re o
utco
me
mea
sure
s;
SD
, sta
ndar
d de
viat
ion;
T0,
bas
elin
e an
d T1
, pos
t int
erve
ntio
n
# Sig
nific
ance
at p
<0.0
5;
* A
ctua
l use
of o
utco
me
mea
sure
s, b
ased
on
reco
rds
of 5
mos
t rec
ently
trea
ted
patie
nts
(con
verte
d to
0-1
00%
sco
res)
*
* S
elf-r
epor
ted
use
of o
utco
me
mea
sure
s ba
sed
on a
que
stio
nnai
re a
bout
5 m
ost r
ecen
tly tr
eate
d pa
tient
s (c
onve
rted
to 0
-100
% s
core
s)

Chapter 7
168
Figure 2. Median actual and self‐reported use of recommended outcome measures
Median Use of recommended outcome measures
01234567
ETG (n=15) NETG (n=15)
Med
ian
Actual use T0 Self-reported use T0Actual use T1 Selfreported use T1
ETG indicates expert tutor group; NETG, non‐expert tutor group; T0, baseline; and T1, post intervention
Figure 3. Actual and self‐reported use of outcome measures
T0 indicates baseline and T1, post intervention
Expert Tutor Group (Actual and Self-reported Use)
0
20
40
60
80
100
MI TCT BBS FAC TMW FAT BI
Outcome measures
Perc
enta
ge o
f use
Non-Expert Tutor Group (Actual and Self-reported Use)
0
20
40
60
80
100
MI TCT BBS FAC TMW FAT BI
Outcome measures
Perc
enta
ge o
f use
Actual Use T0 Self-reported T0Actual Use T1 Self-reported Use T1

Feasibility and effectiveness of PEPCiS
169
Discussion The newly developed PEPCiS educational programme was well appreciated by physiotherapists participating in this pilot study. The absence of drop‐outs, the high attendance rate and the participants’ satisfaction with the programme substantiate its feasibility (Table 2). Moreover, after the 30 participants had attended PEPCiS, their average actual use and self‐reported use of the recommended CPGPS outcome measures almost doubled. A secondary objective in this feasibility study was to detect differences between participants trained by a tutor who had extensive experience with outcome measures in stroke versus those trained by a tutor with less experience. Both groups increased their use of outcome measures, going from a median of 3 to 6 different outcome measures for those trained by the expert‐tutor and from 3 to 4 for the non‐expert group, these between‐group differences were statistically non‐significant (p=0.07). Physiotherapists in both groups appreciated the PEPCiS content, their knowledge gain and all tutor style aspects, but those in the ETG did so significantly more than those in the NETG.
The use of clinical assessment instruments in different phases of a disorder to assess or monitor the health status of patients for the purpose of diagnosis, prognosis and therapy evaluation is considered an aspect of good clinical practice in physiotherapy.13,14,29 Outcome measures assist physiotherapists to in specifying relevant and attainable treatment goals, getting feedback on the effect of interventions and optimizing communication with patients and other professionals in an interdisciplinary team.30 There is an increasing need to prove the effectiveness of therapeutic interventions and to improve the transparency of the clinical decision‐making process by health care professionals such as physiotherapists. However, physiotherapists often wonder when they need to monitor patients, and what functional impairments or limitations in terms of activities or participation should be assessed.31 Our attempt to teach physiotherapists to integrate the use of outcome measures in the clinical reasoning process in the management of patients with stroke (by means of the PEPCiS programme) led to a significant increase in the use of the recommended clinical assessment instruments of the Dutch guidelines (CPGPS), and hence to greater transparency of physiotherapy stroke care. The relationship between patients’ preferences, therapeutic goals and chosen outcome measures remains to be studied in future research.
Unlike their colleagues in e.g. Australia, where the Australian Physiotherapy Association recommends that ‘a clinical justification for

Chapter 7
170
physiotherapy services would routinely include the use of outcome measures’,32, Dutch physiotherapists are not yet obliged to use outcome measures as an integral part of daily professional practice. We hypothesized that the use of outcome measures would increase when physiotherapists were educated about the integrated use of these outcome measures in their daily clinical practice and decision‐making during the rehabilitation of patients with stroke.12
The increased use of recommended outcome measures by the participating physiotherapists in this brief study is in line with the findings of comparable studies in which the behaviour of health care providers was observed over periods of 6 months1 to 5 years6,33. However, physiotherapists tended to overestimate their use of outcome measures. This overestimation may have been caused by their tendency to give socially desirable answers, because recommendations in clinical practice guidelines and ethical professional requirements imply that they are expected to use outcome measures. The post‐hoc analysis at the baseline of the present study showed that the self‐reported use of outcome measures among participants was non‐significantly higher (median=4) than actual use (median=3). After the intervention, the participants reported a median use of 6 recommended outcome measures, whereas our analysis found an actual use of 5 measures.
The physiotherapists participating in this study were self‐selected and the majority worked in nursing homes. They probably volunteered because they had a more than average interest in caring for patients with stroke and hence a greater intention to use the CPGPS and its recommended outcome measures (Table 1), so they can be regarded as a preferred group of interest. Moreover, they might represent a specific subgroup of ‘innovators’ or ‘early adopters’.34 Overall the physiotherapists in this study claimed a more frequent use of outcome measures before PEPCiS than those who responded to a recent survey in the Netherlands (N=167).12 In line with this survey, a notable finding of the present study is the extremely infrequent use of the FAT. Since the FAT was only introduced among Dutch physiotherapists in 2002, it is still a relatively unknown outcome measure for classifying arm and hand use of patients with stroke.12
The present study had certain methodological limitations, in that tutors were not blinded and the physiotherapists, who were unaware of the precise objectives of the study, were semi‐blinded.
Although several authors35,36 have advised against using statistical analysis in feasibility studies, our analysis demonstrated a potential effect of the level of tutor expertise in the educational programme investigated in the present study (p=0.07).

Feasibility and effectiveness of PEPCiS
171
A power analysis on the basis of the results presented here demonstrates that an adequate sample size in an RCT to test the hypothesis ‘PEPCiS results in an enhanced use of 2 or more outcome measures by physiotherapists’ would be 140 physiotherapists in each of the experimental arms. A post hoc univariate logistic regression analysis (significance set at p<0.2) on the entire set of data from the present study revealed the following factors that were associated with a change score of 2 or more outcome measures before and after PEPCiS: (1) initial use of outcome measures, that is, before the start of PEPCiS (≤ 2 outcome measures; p<0.01), (2) experience with patients with stroke (≤ 9 years; p<0.01), (3) age of physiotherapist (≤ 34 years; p=0.02), (4) number of patients with stroke treated per week (p=0.10), (5) physiotherapists’ intention to use outcome measures at baseline (TPB; p=0.11), (6) gender (female; p=0.14) and (7) appreciation of the tutor (≥ 7 on 1‐10 scale; p=0.16). Since the tutors’ performance was one of the predicting factors this might be investigated in future multilevel analysis in a larger trial.
The present feasibility trial was designed with two tutors. Because of the cross‐level interaction between the participants and their allocated tutor, a multilevel analysis randomized at tutor level would be necessary to detect effects at the level of the participants. Using these techniques, in more robust future trials (N=280) would allow corrections for the effects of other factors, such as ‘intention’ on the numbers of outcome measures recorded in electronic patient records. In addition, we need to examine the impact of improved use of outcome measures by therapists on the outcome and quality of care at the level of the patients, nested within therapists. A more powerful trial comparing more expert and non‐expert tutors could preclude bias by aspects of tutors not related to their content expertise. This is in line with what has been found in tutor studies in university education.23,37,38
To our knowledge, this is the first study to examine the effects of differences in content expertise between tutors in physiotherapy education. In the present study, the tutors differed in content expertise as regards clinical experience with using clinical assessments in stroke. Although the study participants evaluated several important aspects of tutoring style (knowledge of subject matter, skill in process facilitation and overall effectiveness of the tutor), other aspects, such as personality and seniority, were disregarded. In a future study with sufficient power, we intend to investigate the influence of PEPCiS as well as interfering factors, such as expertise and performance of tutors, in order to establish and improve the effectiveness of educational interventions as a part of implementation strategies for the regular use of outcome measures by physiotherapists.

Chapter 7
172
Acknowledgement We would like to thank the physiotherapists who participated in this study, as well as Meta Wildenbeest (MW) for her tutorship and Dr Gert Kwakkel for his constructive comments. Appendix Physiotherapists’ Educational Programme on Clinimetrics in Stroke (PEPCiS) The PEPCiS course book is based on the recommendations for the use of clinical assessments in the Dutch Clinical Practice Guideline on Physiotherapy management of patients with Stroke (CPGPS)9 and consists of 89 pages of text, including detailed explanations on the 25 unique outcome measures, including the 7 outcome measures recommended in the CPGPS. PEPCiS supports physiotherapists to enhance the use of the recommended outcome measures by integrating the triad of clinical reasoning in physiotherapeutic stroke management,39 objectifying patients’ functional recovery with the help of outcome measures,31 and recording these outcomes.40 The physiotherapists participating in PEPCiS use the data of their own patients. The content of the programme, summarized in Box 1, is based on (1) evidence‐based practice (EBP) principles, as described by Haynes et a,41; (2) learning strategies, such as interactive teaching, measurement skills training, peer learning, discussions and reflective thinking, and (3) professional education tools such as: (a) the Rehabilitation Problem Solving Form (RPS),42 based on the International Classification of Functioning, Disability and Health (ICF)43 and (b) the Hypothesis‐Oriented Algorithm for Clinicians II (HOAC II)39 for neurological physiotherapy practice.44 The core set of 7 recommended outcome measures of the CPGPS included in the present study consisted of the Motricity Index (MI), Trunk Control Test (TCT), Berg Balance Scale (BBS), Functional Ambulation Categories (FAC), Ten Metre Walk (TMW), Frenchay Arm Test (FAT) and Barthel Index (BI).9 This core set should be applied to all patients with stroke in all phases after stroke, in each setting where physiotherapists work.9 The time required to administer all 7 recommended outcome measures is about 45 to 60 minutes.9 The programme is offered in a fully‐equipped ‘clinimetrics‐classroom’, with software available for the recording of patient data.

Feasibility and effectiveness of PEPCiS
173
Box 1 – Content of PEPCiS Session 1
- Introduction to EBP, ICF and RPS as educational tools - Peer learning and reflective thinking about outcome measures used by
participating physiotherapists - Discussions about the use of outcome measures in clinical reasoning and clinical
decision making - General introduction to physiotherapeutic stroke management - Participants’ own patient records guiding participants in PEPCiS
Session 2
Theme: Walking and mobility-related activities - Introduction of software for recording patients’ data - Introduction of 3 recommended outcome measures: interactive teaching on FAC,
TMW and BBS - Training measurement skills and peer learning - Discussions about prediction models (walking)
Session 3
Theme: Hand and arm use - Introduction of HOAC II - Introduction of 2 recommended outcome measures: interactive teaching on MI and
FAT - Discussions about prediction models (hand and arm use)
Session 4
Theme: Integration of outcome measures, therapeutic (SMART) goals and evaluations - Introduction of 2 recommended outcome measures: interactive teaching the TCT
and BI - Peer learning with RPS and patients’ data (platform presentations by participating
physiotherapists) Session 5
Theme: How to communicate outcome measure data - Peer learning, using HOAC II and RPS in physiotherapeutic stroke management
during everyday practice
SMART = specific, measurable, attainable, realistic and timely

Chapter 7
174
References
1. Abrams D, Davidson M, Harrick J et al. Monitoring the change: current trends in outcome measure usage in physiotherapy. Man Ther 2006; 11(1):46‐53.
2. Akinpelu AO, Eluchie NC. Familiarity with, knowledge, and utilization of standardized outcome measures among physiotherapists in Nigeria. Physiother Theory Pract 2006; 22(2):61‐72.
3. Chesson R, Macleod M, Massie S. Outcome measures used in therapy departments in Scotland. Physiotherapy 1996; 82(12):673‐679.
4. Lennon S. Physiotherapy practice in stroke rehabilitation: a survey. Disabil Rehabil 2003; 25(9):455‐461.
5. Maher C, Williams M. Factors influencing the use of outcome measures in physiotherapy management of lung transplant patients in Australia and New Zealand. Physiother Theory Pract 2005; 21(4):201‐217.
6. Mayo N, Cole B., Dowler J., Gowland C, Finch E. Use of outcome measures in physiotherapy: survey of current practice. Canadian Journal of Rehabilitation 1994; 7:81‐82.
7. Oostendorp RAB, Pluimers DJ, Nijhuis‐van der Sanden MWG et al. Physiotherapy patient documentation: the Achilles heel of evidence‐based practice? [In Dutch: Fysiotherapeutische verslaglegging: de Achilleshiel voor Evidence‐based Practice (EBP)?]. Ned Tijdschr v Fysioth 2006; 116(3):56‐61.
8. Van Peppen RPS, Kwakkel G, Harmeling BC et al. Clinical Practice Guideline on Physiotherapy‐management of patients with Stroke [in dutch: KNGF‐richtlijn Beroerte]. Ned Tijdschr v Fysioth 2004; 114 (5:supplement):1‐78.
9. Van Peppen RPS, Hendriks HJM, Van Meeteren NLU et al. The development of a clinical practice stroke guideline for physiotherapists in The Netherlands: A systematic review of available evidence. Disabil Rehabil 2007; 29(10):767‐783.
10. Turner‐Stokes L, Turner‐Stokes T. The use of standardized outcome measures in rehabilitation centres in the UK. Clin Rehabil 1997; 11(4):306‐313.
11. Pollock AS, Legg L, Langhorne P et al. Barriers to achieving evidence‐based stroke rehabilitation. Clin Rehabil 2000; 14(6):611‐617.
12. Van Peppen RPS, Maissan JF, Van Genderen FR et al. Outcome measures in physiotherapy management of patients with stroke: a survey into self‐reported use, and barriers to and facilitators for use. Disabil Rehabil. (Submitted)
13. Jette DU, Bacon K, Batty C et al. Evidence‐based practice: beliefs, attitudes, knowledge, and behaviors of physical therapists. Phys Ther 2003; 83(9):786‐805.
14. Parker‐Taillon D. CPA initiatives put the spotlight on evidence‐based practice in physiotherapy. Physiother Can 2002; 24:12‐15.
15. Van Peppen RPS, Stutterheim EC, Wildenbeest M., Wittink H. Physiotherapists Educational Programme on Clinimetrics in Stroke (PEPCiS) [in Dutch: KNGF IOF Jaarprogramma: Klinimetrie CVA]. 2006. Amersfoort, KNGF.

Feasibility and effectiveness of PEPCiS
175
16. Lomas J. Teaching old (and not so old) does new tricks: effective ways to implement research findings. In: Dunn EV, Norton PG, Steward M, Tudiver F, Bass MJ, editors. Volume 6: Disseminating research / changing practice. London: Sage, 1993.
17. Davis D, OʹBrien MA, Freemantle N et al. Impact of formal continuing medical education: do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes? JAMA 1999; 282(9):867‐874.
18. Powell CV. How to implement change in clinical practice. Paediatr Respir Rev 2003; 4(4):340‐346.
19. Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes 1991; 50:179‐211.
20. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patientsʹ care. Lancet 2003; 362(9391):1225‐1230.
21. Wittink H, Van Peppen RPS, Stutterheim EC et al. Physiotherapists Educational Programme on Clinimetrics (PEPC) [in Dutch: KNGF IOF Jaarprogramma: Klinimetrie]. 2005. Amersfoort, KNGF.
22. Groves M, Rego P, OʹRourke P. Tutoring in problem‐based learning medical curricula: the influence of tutor background and style on effectiveness. BMC Med Educ 2005; 5(1):20.
23. Schmidt HG, van der Arend A., Moust JH, Kokx I, Boon L. Influence of tutorsʹ subject‐matter expertise on student effort and achievement in problem‐based learning. Acad Med 1993; 68(10):784‐791.
24. Francis JJ, Eccles MP, Johnston M et al. Constructing questionnaires based on the theory of planned behaviour, a manual for health services researchers. 2004. Newcastle upon Tyne, Centre for Health Services Research, University of Newcastle.
25. Armitage CJ, Conner M. Efficacy of the Theory of Planned Behaviour: a meta‐analytic review. Br J Soc Psychol 2001; 40(Pt 4):471‐499.
26. Eccles M, Grimshaw J, Walker A et al. Changing the behavior of healthcare professionals: the use of theory in promoting the uptake of research findings. J Clin Epidemiol 2005; 58(2):107‐112.
27. Portney LG, Watkins MP. Foundations of clinical research, applications to practice. 2nd edition ed. New Jersey: Prentice‐Hall, 2000.
28. Field AP. Discovering Statistics using SPSS. second ed. London: SAGE Publications Ltd, 2005.
29. Haigh R, Tennant A, Biering‐Sorensen F et al. The use of outcome measures in physical medicine and rehabilitation within Europe. J Rehabil Med 2001; 33(6):273‐278.
30. Hammond R. Evaluation of physiotherapy by measuring outcome. Physiotherapy 2000; 86(4):170‐172.
31. Glasziou P, Irwig L, Mant D. Monitoring in chronic disease: a rational approach. BMJ 2005; 330(7492):644‐648.
32. Australian Physiotherapy Association. APA Position Statement ‐ Clinical justification and outcome measures. 2003: https://apa.advsol.com.au/staticcontent/staticpages/position_statements/public/ClinicalJustification&Outcome%20Measures.pdf

Chapter 7
176
33. Kay TM, Myers AM, Huijbregts MP. How far have we come since 1992? A comparative survey of physiotherapistsʹ use of outcome measures. Physiother Can 2001;(Fall):268‐275.
34. Rogers EM. Diffusion of innovations. New York: The Free Press, 1983.
35. Beurskens AJ, de Vet HC, Kant I. [Roaming through the methodology. VIII. Pilot studies: sense and nonsense]. Ned Tijdschr Geneeskd 1998; 142(39):2142‐2145.
36. Lancaster GA, Dodd S, Williamson PR. Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract 2004; 10(2):307‐312.
37. Davis WK, Nairn R, Paine ME et al. Effects of expert and non‐expert facilitators on the small‐group process and on student performance. Acad Med 1992; 67(7):470‐474.
38. Dolmans DH, Gijselaers WH, Moust JH et al. Trends in research on the tutor in problem‐based learning: conclusions and implications for educational practice and research. Med Teach 2002; 24(2):173‐180.
39. Rothstein JM, Echternach JL, Riddle DL. The Hypothesis‐Oriented Algorithm for Clinicians II (HOAC II): a guide for patient management. Phys Ther 2003; 83(5):455‐470.
40. Vreeman DJ, Taggard SL, Rhine MD et al. Evidence for electronic health record systems in physical therapy. Phys Ther 2006; 86(3):434‐446.
41. Haynes RB, Devereaux PJ, Guyatt GH. Clinical expertise in the era of evidence‐based medicine and patient choice. Vox Sang 2002; 83 Suppl 1:383‐386.
42. Steiner WA, Ryser L, Huber E et al. Use of the ICF model as a clinical problem‐solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002; 82(11):1098‐1107.
43. WHO. ICF‐introduction, the International Classification of Functioning Disability and Health. 2001. Geneve.http://www.who.int/classification/icf/intros/ICF‐Eng‐Intro.pdf
44. Schenkman M, Deutsch JE, Gill‐Body KM. An integrated framework for decision making in neurologic physical therapist practice. Phys Ther 2006; 86(12):1681‐1702.
CHAPTER
General discussion

Chapter 8
178
Introduction In this chapter the main conclusions of this thesis in combination with the applied methods will be discussed. Furthermore, essentials for further research in the field of physiotherapy practice and education will be considered in the light of the findings and experiences in developing and implementing evidence‐based guidelines for patients with stroke. Finally, I elaborate on implications for future management by rehabilitation specialists of patients with stroke, including the professional role of disciplines involved such as physiotherapy. In the present thesis the steps of the Lomas model1 were followed (Figure 1). This implementation model is defined by Kitson et al2 as an acceptable representation of issues, contexts and processes suggesting that implementation occurs when evidence meets everyday practice. The aim of the work described in this thesis was: 1) to collect and review systematically, and appraise critically the evidence, based on research in physiotherapy and physiotherapy‐related studies in patients with stroke (research findings and credible dissemination, see Figure 1), and 2) to integrate the recommendations that emerged from the aforementioned review activities concerning the use of outcome measures into the daily practice of the physiotherapists involved in the management of patients with stroke (educational environment and implementation into daily practice of practitioner and patient, Figure 1).
Figure 1. Steps in present thesis based on implementation model by Lomas.2
Implementation model described byLomas
Research findings
Credible dissemination
Educational environment
Practioner&
Patient
Steps of Lomas in the present thesis
Systematic reviews(chapters 2, 3 and 4)
Clinical practice guideline(chapter 5)
and survey (chapters 6)
Educational programmePEPCiS
(chapter 7)
Implementation PEPCiS(chapter 7)

General Discussion
179
Main conclusions
Collecting, reviewing and appraising the evidence With regard to the first aim, I concluded that the application of physiotherapy improves performance to execute regular daily activities by patients with stroke. In particular, strong evidence was found that patients benefit from therapeutic exercise programmes, when the exercise training was applied intensively and started as soon as possible after stroke occurred (Chapter 3). In about 90% of the 151 reviewed studies, therapy effects were mainly restricted to tasks directly trained in the exercise programme (Chapters 2, 3 and 4; idem), thereby underscoring the principle of specificity of training.3 As our systematic reviews demonstrate, walking ability in patients with stroke can best be improved by interventions to train specific functional gait and gait related tasks, e.g., gait training added by external auditory rhythms during gait, over ground or on a treadmill, with and without body weight support (Chapter 2). Functional use of the paretic arm and hand can best be improved by for instance constraint‐induced movement therapy (CIMT), and activities of daily living (ADL), for instance sit‐to‐stand transfers by frequent training of taking a seat and standing up (Chapter 2). Based on the review results the small to large effect‐sizes and the results of the best‐evidence syntheses, physiotherapists involved in stroke management were recommended to train their patients intensively and in a task‐ and context specific manner.
The results of our review‐activities (Chapters 2, 3 and 4) formed the fundament of the Clinical Practice Guideline on Physiotherapy management of patients with Stroke (CPGPS), a guideline initiated, developed and approved by the Royal Dutch Society for Physical Therapy (Koninklijk Nederlands Genootschap voor Fysiotherapie: KNGF). The CPGPS is the first physiotherapy specific stroke guideline worldwide (Chapter 5), and was recently translated in English4 and German5 Besides these, the Royal College of Physicians came with a compilation of the physiotherapy elements of the UK multidisciplinary stroke guideline.6
The CPGPS aims to give decision support for physiotherapists involved in stroke management, and thus has to be a helpful assistant in applying evidence‐based practice by physiotherapists.7,8 The CPGPS states 72 recommendations which concern three important aspects of physiotherapy: 1) prediction of functional recovery of activities of daily living (ADL), including walking ability and hand/arm use, 2) selection of cost‐effective physiotherapy interventions, and 3) selection of relevant outcome measures, of which seven are to be seen as a minimal optional base, to determine

Chapter 8
180
impairments and activity limitations. Each recommendation is based on systematic literature search, analysis of methodological quality of the included studies, and quantitative analysis of the effectiveness (Chapter 2). Furthermore each recommendation is provided with a level of evidence and connected to a recommended set of outcome measurements to monitor the patients with stroke. As such, these recommendations combine quantity and quality of evidence with practically, in my opinion useful tools for physiotherapists in the management of patients with stroke.
Implementing the evidence The second aim of this thesis addressed the integration of the recommended outcome measures into the daily practice of the physiotherapists involved in the management of patients with stroke. Two months after disseminating the CPGPS by the KNGF (see Figure 1) we carried out a survey on Dutch physiotherapists involved in stroke management (N=400; effective response: 43%). On the base of this survey we concluded that in general responders demonstrate a positive attitude for the use of outcome measures but still claim to use only three out of the seven recommended instruments. The survey also indicated several barriers to and facilitators for the use of these instruments, such as problems with changing routines’, ‘too much time investment’, and ‘lack of financial compensation’ (Chapter 6). In order to enhance the use of the recommended outcome measurements an educational programme was developed (see Figure 1), the Physiotherapists’ Educational Programme on Clinimetrics in Stroke (PEPCiS) (Chapter 7) and tested for its feasibility in thirty volunteering physiotherapists. During the PEPCiS, which was well appreciated by the highly compliant therapists, the use of clinical measurements increased from a median of three per patient to five. A secondary objective in this feasibility study was to detect differences between a group of physiotherapists trained by either a tutor with high‐experience with outcome measures in stroke versus a group trained by a tutor with low‐experience (tutor allocation was random). Both groups reported the use of outcome measures more often in their patient records, from a median of 3 to 6 for those trained by the expert‐tutor and from 3 to 4 for the non‐expert trained group. However the between‐group differences were not statistically significant (p=0.07). Physiotherapists in the expert tutor group (ETG) appreciated the PEPCiS‐content, gain in knowledge, and the education style of tutor, more than those in the non‐expert tutor group (NETG). These findings are in line with other non‐physiotherapy education studies.9‐11 On the base of this feasibility study we thus hypothesised that tutor content expertise shows the promise of being more effective in the

General Discussion
181
education of physiotherapy groups than non‐content tutors, a proposition worth further experimentation in a fully powered trial, preferably an RCT. Strengths and considerations Elaborating on the first aim of this thesis and the systematically collected, reviewed and appraised evidence, I want to address the following issues: a) understanding of recovery after stroke (Chapters 2, 3, and 4; idem), an
important question in our search to the most effective treatment approaches.
b) process of development of the CPGPS (Chapter 5), c) methodology of the research, that aims to select prognostics (Chapter 5),
interventions (Chapters 2 tot 5) and outcome measures (Chapters 5 and 6).
Dwelling on the second aim of the thesis, to integrate the clinical guideline where it concerns its recommendations, I would like to discuss: a) process of implementation of evidence into the daily practice of
physiotherapists (Chapters 5, 6 and 7; idem), and b) optimising physiotherapy‐services in rehabilitation management of
patients with stroke (Chapters 5 and 7; idem).
1a. Understanding recovery after stroke The clinically relevant outcomes (Chapters 2, 3, and 4; idem) are beneficial for the profession of physiotherapists and address the demand for more understanding of the underlying mechanisms of recovery after stroke. We also need to gain more insight into how exactly a patient with stroke learns when showing improvement in motor performance. An example of this based on recent studies, relates to a change in the assumption of ‘normal motor behaviour’ as a common reference to describe the ‘abnormal’ asymmetric motor behaviour of people with stroke.12‐14 Asymmetrical weight transfer in patients with stroke does not necessarily imply that these patients are more unstable and less able to control their balance in order to prevent falling.15,16
In Chapter 4 we systematically studied the effects of ‘visual feedback therapy’ (VFT) on postural control in bilateral standing in patients with stroke. We can conclude, in agreement with Barclay‐Goddard,17 that training symmetry in weight distribution while standing on balance equipment tools

Chapter 8
182
fails to generalise to more effective control when walking. For example, improvement in control of standing balance occurs without significant changes in EMG activation on the paretic side18 or weight bearing on the paretic leg.15 Also for regaining gait control Kautz et al.19 as well as Buurke12 found that therapy‐induced improvements in gait speed and walking ability occur without significant changes in EMG timing of the paretic leg while walking. In addition, longitudinal research shows that improvement of walking ability is only weakly associated with observed changes in strength and synergism of the paretic leg20 and that recovery of hand orientation for grasping with the paretic upper limb strongly depends on adaptive trunk movements in the event of distal deficits.21 On the basis of this clinically relevant evidence it now seems invalid for physiotherapists to continue to strive for ‘normal motor behaviour’ during the treatment of patients with stroke.
Manufacturers, who produce rehabilitation tools, such as balance masters, seem to promote these tools for improving stance symmetry without obeying the longitudinal changes needed to restore control in standing balance after stroke.13
In other words, normal movement characterised by symmetry in weight bearing13 and arm and leg swing while walking22, may not serve as an appropriate reference for the treatment of hemiplegic patients with stroke if incomplete recovery is expected. In contrast, it suggests that patients can continue to adapt to their existing deficits while showing functional improvement in gait or upper limb performance. Unfortunately, previous neurological approaches such as Bobath, Johnstone and Affolter have characterised these behavioural movement strategies as pathologic, and recent research now suggests that these adaptations may in fact be optimal for the state of independent movement control.23
1b. Developing clinical practice guidelines There is strong evidence that stroke rehabilitation is effective when delivered by an expert team that is well coordinated.24 Teamwork and goal setting are considered to be the core skills associated with multidisciplinary rehabilitation.25 Stroke patients who receive organised inpatient multidisciplinary rehabilitation in a stroke unit are more likely to survive and participate independent and to live in their own home setting one year after stroke.24 For every 100 patients receiving organised inpatient multidisciplinary rehabilitation in a stroke unit, an extra five return home in an independent state.26 Based on these findings several multidisciplinary stroke guidelines were developed.27‐34 However, it is uncertain which

General Discussion
183
particular parts of multidisciplinary rehabilitation are specifically effective and which are not. The need for more applicable and more specific, detailed information35 was a part of the first aim of this thesis, resulting in the development of the CPGPS. This guideline (Chapter 5) was derived from systematically research (Chapters 2, 3 and 4; idem) and mainly constructed according to internationally accepted standards.36‐38 The CPGPS complied 19 out of 23 AGREE‐criteria. The four missing criteria are concerned about considering of health benefits, side effects and risks or potential cost implications of applying the recommendations. However, the CPGPS offers physiotherapists detailed information to foster and enrich their clinical decisions where it concerns functional prognosis, design of an intervention programme, and selecting of the measures to monitor and evaluate functional outcome pending time. Furthermore, the development process of the CPGPS was considered as a blueprint for other professional groups in stroke rehabilitation, which planned to develop their own specific and detailed monodisciplinary guideline, e.g. occupational therapy39 and nursing care40.
1c. Methodological considerations Best‐evidence interventions are just one aspect of EBP. At the least knowledge about (and adequate use of) prognostic factors and methods of evaluating patients recovery are as important. Physiotherapists are in need of more sophisticated prognostic tools in order to formulate more specific and realistic intervention goals. Considerations about these aspects, i.e., prognostics, interventions and outcome measures used in our systematic reviews and CPGPS are described below. With reference to prognostics The generalisability of the results of studies of prognostic factors is often
limited due to methodological flaws and the often arbitrary timing of predicting outcome after stroke.41 The linear regression model used in Chapter 5 is instructive and illustrative for physiotherapists to use the initial Barthel Index score to predict ADL‐outcomes at six months after stroke.42 However, recently, new logistic regression models were developed in which the longitudinal relationship of observed changes in body functions, such as strength and synergism, is related to improvements in activities such as gait.20 The advantage of such longitudinal regression models is that time is used as a covariate that independently determines the accuracy of outcome.20 In addition, most regression models have not been cross‐validated in an independent group of stroke patients, which makes the

Chapter 8
184
validity of the derived model questionable. There is a need for long‐term studies to validate these models with patients from the acute till chronic phase in order to identify those patients who are susceptible for functional decline, for instance in gait performance43 or dexterity of the paretic arm44. In line with McGinn et al we could conclude that there is a need to develop and validate clinical decision rules and more valid and trustworthy outcome measures to increase the accuracy of physiotherapists’ diagnostic and prognostic assessments.45 With reference to interventions The interventions described in this thesis were classified as
‘physiotherapy‐related’ interventions. Some of these interventions are also applicable for related disciplines, such as occupational therapy. However, the primary aim of this thesis was dedicated to the professional domain of physiotherapy. This latter does not preclude that other professions in stroke care management can underpin their own professional activities with found evidence from the present thesis.
The CPGPS provides detailed descriptions of numeric variables of therapy in order to facilitate replication of interventions in daily practice (Chapter 5). Uncertainty however remains about the identification of which interventions might be most beneficial for patients with stroke.46 It would be helpful to accompany guideline recommendations with advices concerning ‘what’, ‘who’, ‘when’, ‘where’ and ‘how’ to treat and monitor patients.
Considering the methodological choices made in the present thesis, three aspects have to be discussed, namely 1) methodological quality, 2) statistical power and 3) best‐evidence synthesis. First, after a comprehensive search strategy, identifying 322 relevant articles, the methodological quality of the individual studies was assessed with the reliable PEDro scale.47 In line with other scales, such as the Cochrane collaboration scale,48 Delphi scale,49 Jadad scale,50 nonpharmacological trials scale (Clear NPT),51 the PEDro scale52 as well provides a comprehensive measure of methodological quality of stroke studies.53 Most of the included studies exhibited one or more methodological flaws such as lack of randomisation, or omitted intention‐to‐treat analyses and the use of un‐blinded assessors. In agreement with Foley et al. studies with a PEDro score below four points were felt to be ‘low‐quality’ studies, and studies scoring four or more points as ‘high‐quality’ studies.54 Each cut‐off point for the methodological quality of studies measured with one of many quality lists can be denoted as an arbitrary choice.55‐57 We need to reach consensus about the most appropriate, probably higher cut‐off point to indicate studies as ‘high‐quality studies’. Besides methodological quality,

General Discussion
185
individual studies have to be rated on aspects of relevance. However, high‐methodological studies, measured with any of the accepted scoring scales, might provide little information about the clinical relevance for the profession.58 So in future, researchers need to describe patients, interventions and treatment settings in more detail and to report on experiments using clinically relevant outcomes and comparisons between treatment benefits and potential harms.58 In the present thesis a significant association was detected between year of publication and PEDro‐score (r = 0.42; p < 0.01). The quality improvement probably suggests an increased awareness by researchers to aim for studies with higher quality and involvement of epidemiology, leading to maturation of research‐qualities in the profession of physiotherapy. Based on the scores in our reviews (explained variance ~17%), we would like to urge researchers to comply to the rules more intentionally, for instance by using the PEDro scale52 for the methodological quality and the CONSORT statement59 for the report. This statement consists of a list of 21 recommended items which should be included in a trial report.
Besides methodological quality of individual studies, a second aspect to be considered, concerns statistical power (Chapters 2, 3 and 4; idem). Due to the relatively small numbers of patients (mean 49, range from 6 to 466 patients) involved in the 123 included RCTs (Chapter 2) and the low amount of measurement‐points in time (2 on average, which might be proper in the light of research questions; the CPGPS recommended for clinicians at least five times at fixed time points), there was a low statistical power to reveal true or false statistically significant effects. Caused by the diversity of selected outcomes and intervention strategies of included RCTs, pooling of the data in those studies was in most cases impossible. In this thesis individual effect sizes, if possible, were pooled, resulting in weighted summary effect sizes (SESs).60,61 Recently, a study reported a diversity of used statistical methods in meta‐analyses to calculate standardised mean differences (SMDs).62 Even when researchers use the meanwhile widely accepted Cochrane method to calculate SMDs still errors were found, for instance using wrong standard deviations or wrong time points.62,63 Consensus about a scheme for unambiguous data extraction is necessary.
The third aspect considers the qualitative best‐evidence synthesis (BES). If pooling was not possible due to a lack of comparability of intervention types, outcomes, patient characteristics and lack of point estimates and/or measures of variability, a BES was used to analyse the results. In this thesis the criteria used by Steultjens et al.56 were modified by integrating the PEDro scores. Further improvement of defining the levels of evidence of BES and their subsequent validation is desirable because there are variable

Chapter 8
186
interpretations and claims of strength of evidence. BES will conclude inconsistent levels of evidence, using different BES.55‐57,64 For example, analysis of five comparable, low‐quality studies with insignificant results (i.e., two RCTs, two controlled clinical trials and one pre‐experimental study), BES lead to conclusions such as ‘insufficient evidence’56, ‘limited evidence’57, ‘no evidence’64 or ‘moderate evidence’.55 To minimise bias in BES conclusions a rating system based on consensus is necessary to assess the strength of evidence, and of course such a system has to be validated before further use. With reference to outcome measures The CPGPS recommends a core set of seven outcome measures that was
compiled in consensus meetings with eight experienced physiotherapists in stroke research and daily practice as well. The core set was tested on its applicability by a randomly selected group of physiotherapists (N=169) (Chapter 6). For the final inclusion in the core set, the outcome measures needed a) to be classified into the International Classification of Functioning, Disability and Health (ICF)65; b) to show adequate psychometric properties66, i.e. reliability (inter‐ and intrarater), validity and responsiveness in studies with adult stroke patients; and good clinical utility (easy and quick to administer); c) to minimally overlap each other; and d) to be consistent with current physiotherapy practice. Choices that were made are in essence arbitrary. In international stroke research we have to strive for a compilation of a feasible multidisciplinary core set of outcome measures. Recently in 491 RCTs, examining stroke rehabilitation therapies, 489 assessment tools were identified, resulting in an attempt to compile a core set of 30 cited tools.67 Five out of the seven recommended instruments in the CPGPS, i.e. Motricity Index, Berg Balance Scale, Ten Metre Walk, Functional Ambulation Categories, and Barthel Index, are reported in the list of Salter et al.67 The CPGPS core set is considered to evaluate walking and mobility‐
related activities, hand and arm use, and ADL, and should be applied to all stroke patients in all phases after stroke. The use of a core set of outcome measures is needed to objectify changes in body functions and activities of the patient and to improve communication between physiotherapists and their patients and between professionals of the multidisciplinary team together, such as neurologists, rehabilitation physicians, general practitioners, nursing home doctors, geriatricians, psychologists, (district) nurses, occupational therapists, speech therapists.28

General Discussion
187
2a. Implementing evidence into daily practice “Evidence‐based practice is the integration of best research evidence with clinical expertise and patient values”. In this concept it is accepted that new evidence invalidates previously validated treatments and replaces them with new ones that are more powerful, more accurate and more efficacious and safer to apply. Evidence, as only one element in the clinical decision making process, can inform, refine, and enrich clinical expertise of the professionals. In this way it might be better to use the term “evidence in support of practice”,68 or “evidence in support of a patient’s decision” after publication of the Sicily‐statement.69 Furthermore, EBP demands that the decisions in physiotherapy are made ‐and this is essential‐ by informed patients, based on the best available, current, valid and relevant evidence, combined with optimal clinical experience of the professionals.69 Consequently, physiotherapists have to formulate and thereafter suggest to the patient treatment plans based on patients’ preferences, prognostic determinants, available best‐evidence interventions and knowledge about using outcome measures. In my opinion future guideline developers have to involve patients in decision making by communicating evidence, leading to guidelines that are accessible, readable, and understandable for patients.69,70 However, to optimise the integration of all aspects of EBP in daily practice, we need to detect potentially constraints or barriers, such as time available to apply a guideline or a core set of outcome measures. We also need to identify facilitators which might enhance a successful implementation of evidence or guideline recommendations into daily practice. In this line, guidelines have to be updated when necessary, e.g., as new or conflicting evidence comes up, or when politics drastically changes and the construct of the guideline should be prepared for this, or in case of a paradigm shift as might the result from the Sicily‐statement.
Guideline development is approved, but without an implementation quite meaningless. The CPGPS is a huge document of 317 pages including 72 recommendations for clinical practice (Chapter 5). It will be difficult to implement such a complex guideline. Consequently, with regard to the second aim of the thesis, one part of the CPGPS, the core set of outcome measures, was implemented into daily practice of a select group of physiotherapists involved in the management of patients with stroke. The use of outcome measures by professionals can be seen as a useful indicator of guideline adherence.71
First, an analysis under representatives of the involved professionals (N=167 physiotherapists) was performed to detect perceived barriers and facilitators, regarding to Dutch physiotherapists’ attitude and opinion

Chapter 8
188
towards using outcome measures (Chapter 6). The analysis was performed with the Barriers and Facilitators Questionnaire (BFQ), modified for the purpose of this population. The BFQ might in time be used as a diagnostic tool to select implementation strategies for instance to promote the use of outcome measures by physiotherapists involved in stroke management.
Second, in a feasibility study a select group of Dutch physiotherapists were educated (PEPCiS) to enhance their use of recommended outcome measures (Chapter 7). Pilot studies are primary designed to analyse feasibility.72,73 The survey study (Chapter 6) as well as the PEPCiS study (Chapter 7) were shown to be feasible. We recommend a full trial in order to investigate the dependency of the physiotherapists to their allocated tutor in an appropriate multilevel analysis method to detect differences between groups with different tutors. To preclude bias by non‐content expertise dependent aspects of each tutor, a larger cluster randomised study is necessary with, based on power calculation consisted of 280 physiotherapists, a comparison of 10 expert and 10 non‐expert tutors, each of them educating a group of 14 physiotherapists will be adequate. Such a trial is needed in which the effects of implementation of CPGPS in different stroke settings are evaluated. In particular acknowledging that greater levels of adherence to multidisciplinary stroke guidelines74 are associated with improved outcomes in terms of ADLs and health‐related quality of life.75 With that, compliance with guidelines may be viewed as a quality‐of‐care indicator with which to evaluate new organisational and funding changes involving stroke rehabilitation.75
Not only guideline implementation studies are important, also the education of future physiotherapists, the present students, needs attention. In my opinion CPGs have to be an integrated part in the education of physiotherapists in programmes at the universities or polytechnics, and in the postgraduate courses, and can be used as a knowledge transfer tool to educate physiotherapists to use scientific research findings in their daily practice. At the same time one might test whether the guidelines can be understood and the recommendations been followed up by the students.
We based or investigations concerning implementation on a model described by Lomas1,2 in which education plays an important role. Prior to the education of the professionals we detected potentially barriers and facilitators76, and integrated solutions for the barriers and facilitators in our educational programme. With these, we performed a diagnostic analysis of our target group, the physiotherapists, with the modified BFQ (Chapter 6). The BFQ, coming from a validated questionnaire,77 includes statements about a four domains‐model, i.e., characteristics of the innovation, the care

General Discussion
189
provider, the patient and the context. Both the model by Lomas and that by Peters seemed valuable and complemented each other for the aims of this thesis, based on integrating detailed information to specific target groups in daily practice.
The newly developed, well appreciated and feasible PEPCiS aims to enhance the infrequent use of outcome measures in the management of patients with stroke (Chapter 6). PEPCiS might be used to assist tutors in the education of physiotherapists and students in linking interventions to outcome measures. The late Rothstein already stated that “measurement is the sine qua non for effective practice in physiotherapy. Without measurement, there can be no effective practice”.78 In Chapter 6 we detected why the physiotherapists included in the survey did not regularly use measurement instruments. In line with findings from other studies,79,80 main barriers why physiotherapists do not use these instruments on a regular basis are lack of time and lack of knowledge about outcome measures. By integrating outcome results in discharge letters to colleagues in a further stroke service setting and by visualising patients’ outcome data in web‐based electronic patient records81 physiotherapists and their patients will appreciate the added value of monitoring change in body functions and activities by using valid measurement instruments. As a result, I expect that the continuity, transparency, and accuracy of physiotherapy stroke management will be improved, an expectation that remains to be underscored by further investigations.
2b. Optimising of physiotherapy stroke management Based on the findings of the present thesis, I infer that the management by physiotherapists of patients with stroke can be optimised. For instance to formulate SMART designed clinical questions (specific, measurable, attainable, realistic and timely) based on patients’ preferences before starting a (multidisciplinary) treatment. In order to do so, physiotherapists have to gain explicit knowledge of the recommendations in the CPGPS and use their clinical expertise to critically appraise 1) patient’s functional prognosis, 2) treatment goals, and 3) evaluative measurements in (ICF) terms of functions and structures, activities and participation. Therapists then ought to treat patients with stroke on an intensive, task‐specific way and monitor and communicate clinical changes explicitly, both in the multidisciplinary team as well with the patient. However, the evidence that more intensive rehabilitation improves outcome after stroke has to be reflected in today’s rehabilitation practice.82 The intensity of rehabilitation programmes is often limited.83‐85 For example, in stroke units or other inpatient rehabilitation

Chapter 8
190
settings the usual direct contact therapy practice time of all stroke team members is about two hours per working day.83‐85 It should also be acknowledged that more than 2 hours of therapy each day is not feasible for every patient or clinical setting. The most pragmatic way to create more therapy practice time is by adding on (task‐specific) group training programmes.86 For example, constraining the non‐paretic arm for several hours per day,87 or offering patients circuit training in groups in a progressive functional way.88 Moreover, impairment‐focused programmes such as biofeedback, neuromuscular or transcutaneous nerve stimulation fail to generalise to functional improvements. Therapists have to be aware that a mix of components from different treatment approaches89, an eclectic approach, integrated in a multidisciplinary stroke team26,90 is more effective in attaining functional independence, and that impairment‐focused neuromuscular treatment approaches lead to longer lengths of stay compared to activity‐focused therapy.91 With the sharp rise in the ageing population and the increasing prevalence of the number of patients with stroke, it is necessary that the treatment approaches in rehabilitation be optimised and that the professionals become specialists with knowledge about prognostics, interventions and outcomes.
Recommendations in future research Addressing fundamental key questions Longitudinal kinetic and neurophysiological studies are needed to explain, or to improve the understanding of the underlying mechanisms of functional recovery as a function of time.20,23 For this purpose, more knowledge is needed about the ‘nature’ of movement coordination deficits as well as their adaptation strategies to accomplish functional tasks such as reaching activities with the paretic arm or gait.23 New clarifying models are needed to explain why recovery after stroke occurs to a large extent through behavioural compensation rather than through recovery of for instance cerebral tissues and neural plasticity.23 With a better understanding of these recovery strategies, we may find relationships between behavioural adaptations and improved skills and activities after stroke. Clear relationships will change our future therapeutic approaches of patients with stroke. At the moment, in our research to the most effective rehabilitation interventions we have to focus on intensive, task‐specific approaches which are more effective than traditional approaches focusing on impairments.92

General Discussion
191
Innovating interventions with help of fundamental research findings Research is also needed to address specific questions about for instance the type of functional electro stimulation (FES) that might be most effective, in what dose and at what time after stroke,93 or to study the additional value of new treatment interventions such as ‘upper limb robotics’,94 ‘virtual reality’,95 mirror therapy’,96 or bilateral movement training,97 e.g., ‘BATRAC’.98
To find answers to these questions we have to join forces with other research fields, i.e., human movement sciences, biomechanics, biology, ecological psychology and neuroradiology to connect fundamental and clinical research into transversal lines of research.
Selecting patients and clinical decision rules In the CPGPS almost 90% of the recommendations were based on the results of intervention studies, involving patients in the post acute and chronic phase of stroke, and patients who had experienced a less severe or uncomplicated stroke. Further specification of patients’ characteristics (e.g. stroke severity) and the content of interventions in individual studies is needed to select the appropriate patients for specific therapeutic interventions.99 However, future research has to be better attuned to patients with co‐morbidities, acknowledging that these patients are often not selected for controlled trials. As long as patients with stroke are recruited in RCTs without stratification for their prognosis of functional recovery any effort to find cost‐effectiveness will be in vain. Consequently, future research should focus on a) stratifying patients with stroke into different functional profiles, according to their prognosis in their recovery of functional health status;20,23 b) obtaining clinical decision rules for professionals, available for each stratum;100 c) implementing these rules and changing clinical behaviour of professionals45 and d) developing concepts concerning longitudinal monitoring (with high‐quality outcome measures) of functional health status of patients with stroke,71 and observational studies on single subjects or small cohorts with high frequency sampling of data (for instance daily) in order to detect day‐to‐day dynamics of functioning of these patients.
Monitoring changes of functional health In future research we also have to emphasise on longitudinal monitoring processes of patients with stroke during their rehabilitation.71 Using change scores in studies gives the opportunity to explore the longitudinal relationship between time‐independent changes of functional recovery profiles after stroke, for instance in functions as walking speed and

Chapter 8
192
endurance, and observed changes in extended daily activities such as community walking.20,23 Besides we have to learn physiotherapists and other health care providers to interpret the monitored data coming from outcome measurements and to communicate these data to their patients. Involving patients and caregivers Based on new insights, an important aspect of improving stroke care is to enhance the involvement of patients and care givers in the rehabilitation process. In my opinion a freely and easily accessible website might be a useful tool to stimulate the involvement of patients and caregivers as well. According to the Canadian Stroke Network (CSN) an evidence‐based stroke rehabilitation intervention website for patients, caregivers and professionals (StrokEngine: http://www.medicine.mcgill.ca/strokengine) can be developed in the Netherlands. The CSN took an effort to bridge this gap between research findings and current clinical practice. The StrokEngine targeted three groups: 1) individuals who have had a stroke, their families, friends or care partners; 2) clinicians with varying stroke expertise; and 3) administrators and policy makers who need quick accurate information about interventions and their effectiveness.
Improving clinical practice guidelines Stroke research needs a more structured and detailed way of reporting study results. With that, guideline recommendations can be more specific about the content, selected patients, intensity and duration of the interventions.101 International and multidisciplinary collaboration in guideline development is advisable, because many countries and professions pass through the same processes and debates during their development but at different phases.102 In fact, the aim to improve healthcare decision‐making process globally has been started already by the Cochrane Collaboration. They combined forces in systematic literature searches, methodological quality ratings and grading levels of evidence. However, cultural and national care specific differences between countries in the formulations of recommendations for clinical practice will always remain.103 Therefore the foundation of a global network for stroke‐neurorehabilitation is crucial for an efficient worldwide cooperation, aiming to enable and advance national organisations within neuroscience physiotherapy and their individual members by supporting and facilitating research, sharing clinical specialisation, selecting multidisciplinary core sets of measurements instruments, sharing good practice with developing countries and enhancing the transferability of physiotherapy guidelines. Recently, the initiative was taken by an

General Discussion
193
international group of physiotherapists to create a new association that should facilitate communication and collaboration among neuroscience physiotherapists throughout the world and to promote the physiotherapy perspective within the sphere of neuroscience. The current working title for this new association is the International Neuroscience Physiotherapy Association. Improving implementation of research findings Taskforces have to be set up to promote collaboration between stroke rehabilitation research and implementation research. These research domains are in line with each other, but nowadays unsatisfactory linked and ad hoc combined. Those who found evidence in fundamental and clinical research have to cooperate with those who implement these findings in daily practice of the health care professionals. Taskforces have to create objective methods to define when an implementation of a CPG is successful. In that process taskforces have to develop outcome measures to evaluate a) compliance to guidelines by professionals and patients; b) ‘successful’ implementation of guidelines; and c) ‘successful’ knowledge exchange from guidelines to daily practice.
Implementation research in the field of physiotherapy science is relatively new and mainly focused on current models in general health care. Developing physiotherapy specific implementation models is necessary to create tailored implementation strategies. Parallels can be drawn between the implementation models and physiotherapy treatment models. Both need a well performed diagnostic analysis (target group versus patient), a plan (implementation versus treatment), and an evaluation (process indicators versus outcome indicators). Furthermore, in future guideline implementation research not only effects have to be investigated at the level of physiotherapists (do they act according to the guideline), but also at the level of patients (does guideline‐driven therapy result in better patient outcomes?).
Physiotherapy students in graduate programmes, and practicing colleagues in post‐graduate education programmes need to gain explicit knowledge and skills about the ‘state of the art’ in stroke rehabilitation. After graduating physiotherapists have to adopt the principles of lifelong learning (i.e., continuous physiotherapy education and professional development to enhance a professional attitude and opinion about physiotherapy stroke management). In my opinion, physiotherapy as a crucial part of stroke management is a profession with a relatively young history and with many challenges for further growth in the future.

Chapter 8
194
References
1. Lomas J. Teaching old (and not so old) does new tricks: effective ways to implement research findings. In: Dunn EV, Norton PG, Steward M, Tudiver F, Bass MJ, editors. Volume 6: Disseminating research / changing practice. London: Sage, 1993.
2. Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care 1998; 7:149‐158.
3. McDonnell MN, Hillier SL, Miles TS et al. Influence of combined afferent stimulation and task‐specific training following stroke: a pilot randomized controlled trial. Neurorehabil Neural Repair 2007; 21:435‐443.
4. Van Peppen RPS, Hendriks HJM, Van Meeteren NLU et al. The development of a clinical practice stroke guideline for physiotherapists in The Netherlands: A systematic review of available evidence. Disabil Rehabil 2007; 29:767‐783.
5. Van Peppen RPS, Kwakkel G, Wood‐Dauphinee S et al. Einfluss der Physiotherapie auf das funktionelle Outcome nach Schaganfall: Evidenzen. In: Dettmers C, Bülau P, Weiller CH, editors. Schlaganfall Rehabilitation. Bad Honnef: Hippocampus Verlag, 2007: 137‐174.
6. Hammond R, Lennon S, Walker MF et al. Changing occupational therapy and physiotherapy practice through guidelines and audit in the United Kingdom. Clin Rehabil 2005; 19:365‐371.
7. Miller M, Kearney N. Guidelines for clinical practice: development, dissemination and implementation. Int J Nurs Stud 2004; 41:813‐821.
8. Field MJ, Lohr KN. Guidelines for clinical practice. From development to use. Washington DC: National Academy Press, 1992.
9. Schmidt HG, van der Arend A., Moust JH et al. Influence of tutorsʹ subject‐matter expertise on student effort and achievement in problem‐based learning. Acad Med 1993; 68:784‐791.
10. Davis WK, Nairn R, Paine ME et al. Effects of expert and non‐expert facilitators on the small‐group process and on student performance. Acad Med 1992; 67:470‐474.
11. Dolmans DH, Gijselaers WH, Moust JH et al. Trends in research on the tutor in problem‐based learning: conclusions and implications for educational practice and research. Med Teach 2002; 24:173‐180.
12. Buurke JH. Walking after stroke, co‐ordination patterns and functional recovery. Universiteit Twente, 2005.
13. De Haart M. Recovery of standing balance in patients with a supratentorial stroke. Radboud Universiteit Nijmegen, 2005.
14. Latash ML, Anson JG. What are ʹnormal movementsʹ in atypical populations? Behavioral and Brain Science 1996; 19:55‐106.
15. De Haart M, Geurts AC, Huidekoper SC et al. Recovery of standing balance in postacute stroke patients: a rehabilitation cohort study. Arch Phys Med Rehabil 2004; 85:886‐895.
16. Sackley CM. Falls, sway, and symmetry of weight‐bearing after stroke. Int Disabil Stud 1991; 13:1‐4.

General Discussion
195
17. Barclay‐Goddard R, Stevenson T, Poluha W et al. Force platform feedback for standing balance training after stroke. Cochrane Database Syst Rev 2004;(4):CD004129.
18. Garland SJ, Willems DA, Ivanova TD et al. Recovery of standing balance and functional mobility after stroke. Arch Phys Med Rehabil 2003; 84:1753‐1759.
19. Kautz SA, Duncan PW, Perera S et al. Coordination of hemiparetic locomotion after stroke rehabilitation. Neurorehabil Neural Repair 2005; 19:250‐258.
20. Kollen B, Van de Port I, Lindeman E et al. Predicting improvement in gait after stroke: a longitudinal prospective study. Stroke 2005; 36:2676‐2680.
21. Cirstea MC, Levin MF. Compensatory strategies for reaching in stroke. Brain 2000; 123 ( Pt 5):940‐953.
22. Kwakkel G, Kollen BJ, Wagenaar RC. Long term effects of intensity of upper and lower limb training after stroke: a randomised trial. J Neurol Neurosurg Psychiatry 2002; 72:473‐479.
23. Kwakkel G, Kollen B, Lindeman E. Understanding the pattern of functional recovery after stroke: facts and theories. Restor Neurol Neurosci 2004; 22:281‐299.
24. Stroke Unit Trialists Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev 2002;(1):CD000197.
25. Wade DT, de Jong BA. Recent advances in rehabilitation. BMJ 2000; 320:1385‐1388.
26. Langhorne P, Duncan P. Does the organization of postacute stroke care really matter? Stroke 2001; 32:268‐274.
27. Dutch Institute for Quality in Health Care (in Dutch: Kwaliteitsinstituut voor de gezondheidszorg Utrecht‐CBO‐). CBO Richtlijn Beroerte (Stroke Guidelines 2000, in Dutch). 2000. Den Haag, Nederlandse Hartstichting.
28. Commissie CVA‐Revalidatie. Rehabilitation after a stroke, guidelines and recommendations for health care professionals (in Dutch: Revalidatie na een beroerte: richtlijnen en aanbevelingen voor zorgverleners). Franke EAM, editor. 2001. Den Haag, Dutch Heart Foundation (in Dutch: Nederlandse Hartstichting).
29. Scottish Intercollegiate Guidelines Network. Management of patients with stroke, rehabilitation, prevention and management of complications and discharge planning ‐ a national clinical guideline (no: 64). 64. 2002. Edinburgh, SIGN.
30. Agency for Health Care Policy and Research. Post‐Stroke Rehabilitation: clinical practice guideline. No.16. 1995. Rockville, AHCPR Publication 95‐0662.
31. Royal College of Physicians ‐ the intercollegiate working party for stroke. National Clinical Guidelines for Stroke. 1999. London.
32. Hanger HC, Wilkinson T, Keeling S et al. New Zealand guideline for management of stroke. N Z Med J 2004; 117(1192):U863.
33. National Stroke Foundation. Clinical Guidelines for Stroke Rehabilitation and Recovery (Australian Government). 2005.
34. Khadilkar A, Phillips K, Jean N et al. Ottawa panel evidence‐based clinical practice guidelines for post‐stroke rehabilitation. Top Stroke Rehabil 2006; 13:1‐269.
Chapter 8
196
35. Michie S, Johnston M. Changing clinical behaviour by making guidelines specific. BMJ 2004; 328:343‐345.
36. AGREE Collaboration. Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project. Qual Saf Health Care 2003; 12:18‐23.
37. Shaneyfelt TM, Mayo‐Smith MF, Rothwangl J. Are guidelines following guidelines? The methodological quality of clinical practice guidelines in the peer‐reviewed medical literature. JAMA 1999; 281:1900‐1905.
38. Hendriks HJM, Bekkering GE, van Ettekoven H et al. Development and implementation of national practice guidelines: a prospect for continuous quality improvement in physiotherapy. Physiotherapy 2000; 86:535‐547.
39. Cup EHC, Steultjens EMJ. Occupational Therapy Guideline Stroke [in dutch: Ergotherapierichtlijn Beroerte]. 2005. Utrecht, Nederlandse Vereniging voor Ergotherapie (NVE).
40. Hafsteinsdottir TB, Schuurmans MJ. Clinical Nursing Rehabilitation Guideline Stroke [in Dutch: Verpleegkundige Revalidatierichtlijn Beroerte]: in preparation. 2008.
41. Kwakkel G, Wagenaar RC, Kollen BJ, Lankhorst GJ. Predicting disability in stroke ‐ a critical review of the literature. Age Ageing 1996; 25:479‐489.
42. Kwakkel G, van Dijk GM, Wagenaar RC. Accuracy of physical and occupational therapistsʹ early predictions of recovery after severe middle cerebral artery stroke. Clin Rehabil 2000; 14:28‐41.
43. Van de Port I, Kwakkel G, van Wijk I et al. Susceptibility to deterioration of mobility long‐term after stroke: a prospective cohort study. Stroke 2006; 37:167‐171.
44. Kwakkel G, Kollen BJ, Van der Grond J et al. Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke 2003; 34:2181‐2186.
45. McGinn TG, Guyatt GH, Wyer PC et al. Usersʹ guides to the medical literature: XXII: how to use articles about clinical decision rules. Evidence‐Based Medicine Working Group. JAMA 2000; 284:79‐84.
46. Pomeroy VM. Stroke rehabilitation. Disabil Rehabil 2006; 28:813‐814.
47. Foley NC, Bhogal SK, Teasell RW et al. Estimates of quality and reliability with the physiotherapy evidence‐based database scale to assess the methodology of randomized controlled trials of pharmacological and nonpharmacological interventions. Phys Ther 2006; 86:817‐824.
48. Van Tulder MW, Assendelft WJ, Koes BW et al. Method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group for Spinal Disorders. Spine 1997; 22:2323‐2330.
49. Verhagen AP, de Vet HC, de Bie RA et al. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol 1998; 51:1235‐1241.
50. Jadad AR, Moore RA, Carroll D et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996; 17:1‐12.

General Discussion
197
51. Boutron I, Moher D, Tugwell P et al. A checklist to evaluate a report of a nonpharmacological trial (CLEAR NPT) was developed using consensus. J Clin Epidemiol 2005; 58:1233‐1240.
52. Sherrington C, Herbert RD, Maher CG et al. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther 2000; 5:223‐226.
53. Bhogal SK, Teasell RW, Foley NC et al. The PEDro scale provides a more comprehensive measure of methodological quality than the Jadad scale in stroke rehabilitation literature. J Clin Epidemiol 2005; 58:668‐673.
54. Foley NC, Teasell RW, Bhogal SK et al. Stroke Rehabilitation Evidence‐Based Review: methodology. Top Stroke Rehabil 2003; 10:1‐7.
55. Lenssen AF, Köke AJA, de Bie RA et al. Continuous passive motion following primary total knee arthroplasty: short‐ and long‐term effects on range of motion. A systematic review. Phys Ther Review 2003;:113‐121.
56. Steultjens EM, Dekker J, Bouter LM et al. Occupational therapy for stroke patients: a systematic review. Stroke 2003; 34:676‐687.
57. Van Tulder MW, Cherkin DC, Berman B et al. The effectiveness of acupuncture in the management of acute and chronic low back pain. A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 1999; 24:1113‐1123.
58. Heymans MW, van Tulder MW, Esmail R et al. Back schools for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 2005; 30:2153‐2163.
59. Altman DG. Better reporting of randomised controlled trials: the CONSORT statement. BMJ 1996; 313:570‐571.
60. DerSimonian R, Laird N. Meta‐analysis in clinical trials. Control Clin Trials 1986; 7:177‐188.
61. Shadish WR, Haddock CK. Combining estimates of effect size. In: Cooper HM, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation, 1994: 261‐282.
62. Gotzsche PC, Hrobjartsson A, Maric K et al. Data extraction errors in meta‐analyses that use standardized mean differences. JAMA 2007; 298:430‐437.
63. Jones AP, Remmington T, Williamson PR et al. High prevalence but low impact of data extraction and reporting errors were found in Cochrane systematic reviews. J Clin Epidemiol 2005; 58:741‐742.
64. Van Peppen RP, Kwakkel G, Wood‐Dauphinee S et al. The impact of physical therapy on functional outcomes after stroke: whatʹs the evidence? Clin Rehabil 2004; 18:833‐862.
65. Geyh S, Cieza A, Schouten J et al. ICF Core Sets for stroke. J Rehabil Med 2004;(44 Suppl):135‐141.
66. Bot SD, Terwee CB, van der Windt DA et al. Clinimetric evaluation of shoulder disability questionnaires: a systematic review of the literature. Ann Rheum Dis 2004; 63:335‐341.
67. Salter KL, Teasell RW, Foley NC et al. Outcome Assessment in Randomized Controlled Trials of Stroke Rehabilitation. Am J Phys Med Rehabil 2007; 86:1007‐1012.

Chapter 8
198
68. Davidoff F. In the teeth of the evidence: the curious case of evidence based medicine. Mt Sinai J Med 1999; 66:75‐83.
69. Dawes M, Summerskill W, Glasziou P et al. Sicily statement on evidence‐based practice. BMC Med Educ 2005; 5:1‐7.
70. Epstein RM, Alper BS, Quill TE. Communicating evidence for participatory decision making. JAMA 2004; 291:2359‐2366.
71. Glasziou P, Irwig L, Mant D. Monitoring in chronic disease: a rational approach. BMJ 2005; 330:644‐648.
72. Beurskens AJ, de Vet HC, Kant I. [Roaming through the methodology. VIII. Pilot studies: sense and nonsense]. Ned Tijdschr Geneeskd 1998; 142:2142‐2145.
73. Lancaster GA, Dodd S, Williamson PR. Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract 2004; 10:307‐312.
74. Gresham GE, Duncan PW, Statson WB. Priorities for future research: clinical practice guidelines, number 16. US Dept Health and Human Services ‐ Agency for Health Care Policy and Research, editor. AHCPR publication no. 95‐0662. 1995. Rockville.
75. Duncan PW, Horner RD, Reker DM et al. Adherence to postacute rehabilitation guidelines is associated with functional recovery in stroke. Stroke 2002; 33:167‐177.
76. Grol R, Wensing M, Eccles M. Improving patient care. The implementation of change in clinical practice. London: Elsevier Butterworth Heinemann, 2005.
77. Peters MAJ, Harmsen M, Laurant MGH et al. Room for improvement? Barriers to and opportunities for improvement of patient care [dutch: Ruimte voor verandering? Knelpunten en mogelijkheden voor verbeteringen in de patientenzorg]. Centre for Quality of Care Research (WOK), editor. 2003. Nijmegen, The Netherlands, Radbout University Medical Centre.
78. Rothstein JM. Measurement and clinical practice: Theory and application. In: Rothstein JM, editor. Measurement in Physical Therapy: Clinics in Physical Therapy. New York: Churchill Livingstone, 1985: 1‐46.
79. Abrams D, Davidson M, Harrick J et al. Monitoring the change: current trends in outcome measure usage in physiotherapy. Man Ther 2006; 11:46‐53.
80. Pollock AS, Legg L, Langhorne P et al. Barriers to achieving evidence‐based stroke rehabilitation. Clin Rehabil 2000; 14:611‐617.
81. Swinkels IC, van den Ende CH, de Bakker D et al. Clinical databases in physical therapy. Physiother Theory Pract 2007; 23:153‐167.
82. De Wit L, Putman K, Dejaeger E et al. Use of time by stroke patients: a comparison of four European rehabilitation centers. Stroke 2005; 36:1977‐1983.
83. Bernhardt J, Chan J, Nicola I et al. Little therapy, little physical activity: rehabilitation within the first 14 days of organized stroke unit care. J Rehabil Med 2007; 39:43‐48.
84. De Weerdt W, Selz B, Nuyens G et al. Time use of stroke patients in an intensive rehabilitation unit: a comparison between a Belgian and a Swiss setting. Disabil Rehabil 2000; 22:181‐186.

General Discussion
199
85. Tinson DJ. How stroke patients spend their days. An observational study of the treatment regime offered to patients in hospital with movement disorders following stroke. Int Disabil Stud 1989; 11:45‐49.
86. Kwakkel G. Impact of intensity of practice after stroke: issues for consideration. Disabil Rehabil 2006; 28:823‐830.
87. Hakkennes S, Keating JL. Constraint‐induced movement therapy following stroke: a systematic review of randomised controlled trials. Aust J Physiother 2005; 51:221‐231.
88. Van de Port I, Wood‐Dauphinee S, Lindeman E et al. Effects of Exercise Training Programs on Walking Competency After Stroke: A Systematic Review. Am J Phys Med Rehabil 2007; 86:935‐951.
89. Pollock A, Baer G, Langhorne P, Pomeroy V. Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke: a systematic review. Clin Rehabil 2007; 21:395‐410.
90. Wade D. Investigating the effectiveness of rehabilitation professions‐‐a misguided enterprise? Clin Rehabil 2005; 19:1‐3.
91. Patel M, Potter J, Perez I et al. The process of rehabilitation and discharge planning in stroke: a controlled comparison between stroke units. Stroke 1998; 29:2484‐2487.
92. Teasell RW, Kalra L. Whatʹs new in stroke rehabilitation: back to basics. Stroke 2005; 36:215‐217.
93. Pomeroy VM, King LM, Pollock A et al. Electrostimulation for Promoting Recovery of Movement or Functional Ability After Stroke. Systematic Review and Meta‐Analysis. Stroke 2006; 37:2441‐2442.
94. Kwakkel G, Kollen BJ, Krebs HI. Effects of Robot‐Assisted Therapy on Upper Limb Recovery After Stroke: A Systematic Review. Neurorehabil Neural Repair 2007.
95. Crosbie JH, Lennon S, Basford JR et al. Virtual reality in stroke rehabilitation: still more virtual than real. Disabil Rehabil 2007; 29:1139‐1146.
96. Sutbeyaz S, Yavuzer G, Sezer N et al. Mirror therapy enhances lower‐extremity motor recovery and motor functioning after stroke: a randomized controlled trial. Arch Phys Med Rehabil 2007; 88:555‐559.
97. Stewart KC, Cauraugh JH, Summers JJ. Bilateral movement training and stroke rehabilitation: a systematic review and meta‐analysis. J Neurol Sci 2006; 244:89‐95.
98. Richards LG, Senesac CR, Davis SB et al. Bilateral Arm Training With Rhythmic Auditory Cueing in Chronic Stroke: Not Always Efficacious. Neurorehabil Neural Repair 2007.
99. Bode RK, Heinemann AW, Semik P et al. Relative importance of rehabilitation therapy characteristics on functional outcomes for persons with stroke. Stroke 2004; 35:2537‐2542.
100. Craik RL. Thirty‐Sixth Mary McMillan Lecture: Never satisfied. Phys Ther 2005; 85:1224‐1237.
101. Hurdowar A, Graham ID, Bayley M et al. Quality of stroke rehabilitation clinical practice guidelines. J Eval Clin Pract 2007; 13:657‐664.

Chapter 8
200
102. Van der Wees PJ, Hendriks EJ, Custers JW, Burgers JS, Dekker J, de Bie RA. Comparison of international guideline programs to evaluate and update the Dutch program for clinical guideline development in physical therapy. BMC Health Serv Res 2007; 7:191.
103. South African Medical Association (Neurological Association of South Africa Stroke Working Group). Stroke therapy clinical guideline. S Afr Med J 2000; 90(3 Pt 2):276‐9, 292.

Summary

Summary
202
Summary In Chapter 1 several aspects of evidence‐based physiotherapy in patients with stroke are introduced. Stroke is the leading cause of severe long term disability in adults in the Western World. Every year, an estimated 34,500 people a have a stroke in the Netherlands.1 Approximately 70% of the stroke surviving patients experience long term problems in their activities of daily living (ADL) and social participation.2 In the absence of any cure for the initial pathology, rehabilitation is the most universally adopted treatment strategy to improve quality of life in patients with stroke. In the Netherlands patients with stroke generally rehabilitate in different settings, usually started in an acute stroke‐unit care and continued in a rehabilitation centre, a nursing home, or in the community by physiotherapists employed in health centres or private practices. Physiotherapy is perceived as one of the key disciplines in providing organised‐stroke care. In stroke care several multidisciplinary guidelines are available; however these guidelines do not review in depth all available evidence with regard to physiotherapy practice. Physiotherapists need to have more detailed information to foster and enrich their clinical decision making process. This includes making a valid functional prognosis of outcome, selecting the most effective intervention and the most appropriate measures to evaluate functional change. These aspects have to be an integrated part of everyday practice. Accordingly, in the present thesis two main aims were studied.
The first aim was to collect and review systematically, and to appraise critically the available evidence stemming from physiotherapy and physiotherapy related studies in patients with stroke. On the basis of these findings, recommendations were made that permitted guidance in the process of clinical decision‐making. The results of these review‐activities will be presented as a Clinical Practice Guideline on Physiotherapy management of patients with Stroke (CPGPS).
The second aim was to integrate the recommendations of the guideline into daily physiotherapists’ practice. Subsequently, one part of the clinical practice guideline related with using the core set of outcome measures was implemented. Based on an analysis of barriers and facilitators of implementation, an educational program was performed to implement the recommendations into daily practice in a selected group of physiotherapists who were dedicated to management of patients with stroke.

Summary
203
In Chapter 2 a systematic review was performed to establish the scientific value of the evidence of physiotherapy interventions related to improving functional outcomes after stroke and to convert this evidence in an overview of the efficacy of physiotherapy interventions in patients with stroke. Databases (MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, DARE, PEDro, EMBASE and DocOnline) were systematically searched for randomised controlled trials (RCTs) or controlled clinical trials (CCTs) by two independent researchers. For this systematic review, physiotherapy was classified into 10 intervention categories to evaluate the effectiveness of: 1) traditional neurological treatment approaches; 2) programs for training sensory‐motor function or influencing muscle tone; 3) cardiovascular fitness and aerobic programs; 4) methods for training mobility and mobility related activities; 5) exercises for the upper limb; 6) biofeedback therapy for the upper and lower limb; 7) functional and neuromuscular electrical stimulation for both limbs; 8) orthotics and assistive devices for both limbs; 9) treatments for hemiplegic shoulder pain and hand oedema; and 10) intensity of exercise therapy. The following inclusion criteria were applied: 1) participants had be diagnosed with stroke and older than 18 years; 2) studies had to evaluate the effectiveness of physiotherapy interventions in one of the intervention categories; and 3) the publication had to be in English, German or Dutch. Studies were collected up to January 2004 and their methodological quality was assessed using the 10‐point PEDro scale. One hundred and fifty one studies were included: 123 RCTs and 28 CCTs. All included RCTs had a median of 5 points on the PEDro scale (range 2‐8 points). Meta‐analysis showed significant summary effect sizes (SES; p<0.05) for therapies that were focused on functional training of the upper limb such as constraint‐induced movement therapy (SES 0.46; 95% CI: 0.07 – 0.91), treadmill training with or without body weight support (respectively SES 0.70; 95% CI: 0.29 – 1.10 and SES 1.09; 95% CI: 0.56 – 1.61), aerobics (SES 0.39; 95% CI: 0.05 – 0.74), external auditory rhythms during gait (SES 0.91; 95% CI: 0.40 – 1.42), improving symmetry when moving from sitting to standing (SES 0.92; 95% CI: 0.54 –1.29), and effects of high intensity of exercise training on ADL (SES 0.13; 95% CI: 0.03 –0.23) and neuromuscular stimulation for glenohumeral subluxation (SES 1.41; 95% CI: 0.76 – 2.06). No or insufficient evidence in terms of functional outcome was found for: traditional neurological treatment approaches; exercises for the upper limb; biofeedback; functional and neuromuscular electrical stimulation aimed at improving dexterity or gait performance; orthotics and assistive devices; and physiotherapy interventions for reducing hemiplegic shoulder pain and hand oedema. We

Summary
204
concluded that this review showed small to large effects for task‐oriented exercise training, in particular when applied intensively and early after stroke onset. In almost all studies the effects were mainly restricted to tasks directly trained in the exercise program. The overall review in Chapter 2 suggested that early provision of
intensive stroke rehabilitation is associated with enhanced and faster improvement of the performance of activities in patients after stroke. Consequently, in Chapter 3 a research synthesis was performed to examine the effects of augmented exercise therapy time in patients with stroke. Therefore studies were systematically reviewed by evaluating the effects of intensity of practice, expressed as time dedicated to practice, on ADL, gait and dexterity. The hypothesis was that the extra treatment time provided to the augmented therapy group would result in clinically relevant improvements. SES were calculated for ADL, walking speed and dexterity, using fixed and random effect models. Twenty RCTs, involving 2686 stroke patients, were included in the synthesis. The methodological quality ranged from 2 to 11 out of the maximum score of 14 points on an adapted methodological scoring list. Pooling reported differences resulted in a small, but statistically significant random SES with regard to ADL measured at the end of the intervention phase (SES 0.13; 95% CI, 0.03 to 0.23). Further analysis showed a significant homogeneous SES for 17 studies that investigated effects of increased exercise intensity within the first 6 months post stroke. No significant homogeneous SES was observed for the 3 studies conducted in the chronic phase. On average the experimental groups daily received twice as much physiotherapy (49 min) and occupational therapy (23 min) as the control groups (23 and 11 min. respectively). Cumulative meta‐analysis, adjusted for the difference in treatment intensity in each study, strongly suggests that at least a 16 hour difference in treatment time between experimental and control groups provided in the first 6 months after stroke is needed to obtain significant differences in ADL. A significant SES supporting a higher intensity was also observed for instrumental ADL (SES 0.23; 95% CI: 0.13 – 0.33) and walking speed (SES 0.19; 95% CI: 0.01 – 0.36), whereas no significant SES was found for dexterity (SES 0.03; 95% CI: ‐0.13 – 0.19). Improving symmetry of weight distribution while bilateral standing, is
one of the main treatment goals in the rehabilitation of patients with stroke. In Chapter 4, the evidence for applying additional ‘visual feedback therapy’ (VFT) on postural control in bilateral standing was systematically studied in

Summary
205
patients with stroke. The primary aim was to establish whether VFT reduces postural sway and improves left‐right symmetry of weight distribution in bilateral standing after stroke compared with conventional treatment. In addition, the effects of VFT on parameters of gait and gait‐related activities including ADL were evaluated. Eight out of 78 studies (6 RCTs and 2 CCTs), presenting 214 subjects, were included for qualitative and quantitative analysis. The methodological quality ranged on the PEDro scale ranged from 3 to 6 points. The additional value of visual feedback therapy in bilateral standing compared with conventional therapy shows no statistically significant effects on symmetry of weight distribution between paretic and non paretic leg, postural sway in bilateral standing, gait and gait‐related activities. Visual feedback therapy should not be favoured over conventional therapy. These results are of great clinical value indicating that training of postural control should preferably be applied while performing the gait‐related tasks itself. The question remains as to exactly how asymmetry in weight distribution while standing is related to balance control in patients with stroke. In Chapter 5 the available evidence was collected and described to guide
the clinical decision‐making process of physiotherapists dealing with the rehabilitation of patients with stroke especially with respect to the selection of prognostic factors, physiotherapy interventions, and outcome measures. This evidence is presented as a Clinical practice guideline on Physiotherapy management of patients with Stroke (CPGPS) in the Netherlands. A systematic computerised literature search was performed to identify evidence concerning the use of: 1) prognostic factors related to functional recovery; 2) physiotherapy interventions in patients with stroke; and 3) outcome measures to assess patients’ progress in functional health. Physiotherapists working in the field of stroke rehabilitation and a multidisciplinary group of health professionals reviewed the clinical applicability and feasibility of the recommendations for clinical practice and their comments were used to compose the definitive guideline. Of 9482 relevant articles, 322 were selected and screened for methodological quality. Seventy‐two recommendations for clinical practice were retrieved from these articles and included in the guideline: 6 recommendations concerned the prediction of functional recovery of activities of daily living (ADL), including walking ability and hand/arm use; 65 recommendations concerned the choice of physiotherapy interventions; and 1 recommendation concerned the choice of outcome instrument to use. A core set of seven reliable, responsive, and valid outcome measures was established, to

Summary
206
determine impairments and activity limitations in patients with stroke. The guideline provides physiotherapists evidence‐based recommendations to assist them in their clinical decision making regarding patients with stroke. As most of the recommendations included in the guideline came from studies of patients in the post acute and chronic phase of stroke, and in general involved patients with less severe and uncomplicated stroke, more needs to be learned about the more complex cases. The core set of measurement instruments in the CPGPS includes the
Motricity Index (MI), Trunk Control Test (TCT), Berg Balance Scale (BBS), Functional Ambulation Categories (FAC), Ten Metre Walk (TMW), Frenchay Arm Test (FAT) and Barthel Index (BI). Assessing and monitoring the health status of patients is considered an aspect of good clinical practice in physiotherapy. Consequently, in Chapter 6, after disseminating the CPGPS, physiotherapists’ self‐reported use of outcome measures as recommended in the CPGPS was investigated, and the perceived barriers to and facilitators for the use of outcome measures in everyday practice were assessed. A 41‐item survey, including the Barriers and Facilitators Questionnaire (BFQ), was sent by post to 400 physiotherapists in acute care hospitals (ACH; N=100), rehabilitation centres (RC; N=100), nursing homes (NH; N=100) and private physiotherapy practices (PPP; N=100). One hundred and eighty‐nine physiotherapists returned the survey (47%; ACH, N=57; RC, N=67; NH, N=26 and PPP, N=39); the surveys of 167 physiotherapists involved in stroke settings were analysed. These physiotherapists reported regularly using three (median; range 0‐7) of the seven recommended measurement instruments, with those working in ACH or RC reporting a significantly higher use than their colleagues in PPP (4 vs. 0 and 3 vs. 0; p<0.001 and p=0.02 respectively). The BFQ revealed that there were specific facilitators, such as ‘a positive attitude towards outcome measures’ (as mentioned by 93% of the physiotherapists) and ‘familiarity with outcome measures’ (90%), and barriers such as ‘changing routines’ (32%), ‘time investment’ (29%), and ‘financial compensation’ (21%). Despite an almost uniformly positive attitude, Dutch physiotherapists infrequently use the outcome measures recommended in the CPGPS. Robust setting‐specific and tailored implementation strategies based on the reported barriers and facilitators are recommended. To promote self‐reported use and actual use of the recommended
outcome measures by physiotherapists in stroke management a new educational programme was developed, the Physiotherapists’ Educational

Summary
207
Programme on Clinimetrics in Stroke (PEPCiS). In Chapter 7 feasibility and effectiveness were determined in an RCT with thirty voluntarily participating physiotherapists involved in stroke management who were randomised into two numeric equal groups, an expert tutor group (ETG) and a non‐expert tutor group (NETG). The two tutors differed in their clinical experience with outcome measures in stroke. Feasibility was estimated by physiotherapists’ adherence to PEPCiS, satisfaction with PEPCiS and appreciation of tutoring style of their allocated tutor; effectiveness was estimated by counting the frequencies with which outcome measures were mentioned in the records of patients entrusted to the participating therapists. Secondary to this aim, the influence of tutor style will be explored. The participants’ attendance record was generally good (a median of 5 of the 5 sessions; range 4‐5) and they were satisfied with PEPCiS (mean: 7.5 on a 0‐10 scale). In the entire group (N=30) the use of outcome measures increased from 3 per patient before PEPCiS to 5 thereafter (p=0.001). Between‐group differences were non‐significant for the totals of the instruments used (median 3 to 6 in the ETG vs. 3 to 4 in the NETG; p=0.07). Physiotherapists in the ETG appreciated the PEPCiS content, their knowledge gain and all tutor style aspects, significantly more than those in the NETG (p<0.05). The present pilot study suggests that education by PEPCiS enhanced the use of clinical outcome measures by physiotherapists in the management of patients with stroke. A future study with sufficient power will investigate the influence of PEPCiS as well as the interfering factors, e.g. tutor expertise and performance, in order to establish and improve the effectiveness of educational interventions as a part of implementation strategies for the regular use of outcome measures by physiotherapists. Chapter 8 presents a general discussion reflecting on the main
conclusions of this thesis and discusses the strengths and limitations of the applied methods. In addition, chapter 8 offers clinical implications concerning physiotherapy stroke management, recommendations for future research on patients with stroke and suggestions for education and implementation of research findings into everyday practice of professionals in stroke care.

Summary
208
References
1. Struijs JN, van Genugten ML, Evers SM et al. Modeling the future burden of stroke in The Netherlands: impact of aging, smoking, and hypertension. Stroke 2005; 36:1648‐1655.
2. Koek HL, Van Dis SJ, Peters RJG et al. Hart‐en vaatziekten in Nederland. In: Van Leest LATM, Koek HL, Van Trijp MJCA et al., editors. Hart‐en vaatziekten in Nederland 2005, cijfers over risicofactoren, ziekte, behandeling en sterfte [dutch]. Den Haag: Nederlandse Hartstichting, 2005: 6‐12.

Nederlandse samenvatting

Nederlandse samenvatting
210
Samenvatting In Hoofdstuk 1, de inleiding, worden verschillende aspecten van evidence‐based fysiotherapie bij patiënten met een beroerte (cerebrovasculair accident; CVA) geïntroduceerd. Beroerte (in het Engels ‘stroke’) is een verzameling ziektebeelden waarbij sprake is van een stoornis in de bloedvoorziening van de hersenen. In Westerse landen is CVA bij volwassenen de meest belangrijke reden voor het ontstaan van een ernstige chronische beperking. Elk jaar worden ongeveer 34.500 mensen in Nederland getroffen door een CVA.{Struijs, 2005 1171 /id} Ongeveer 70% van de patiënten die het CVA overleven ondervinden onomkeerbare problemen in de activiteiten van hun dagelijks leven (ADL) en sociale participatie.{Koek, 2005 990 /id} De initiële pathologie waardoor een CVA ontstaat is niet te genezen, waardoor revalidatie internationaal gezien de meest geaccepteerde behandelstrategie blijkt om het fysiek functioneren en de kwaliteit van leven voor patiënten met een CVA te verbeteren. In Nederland revalideren patiënten met een CVA in verschillende settings, doorgaans startend in een stroke‐unit voor acute zorg en vervolgend in een revalidatiecentrum, verpleeghuis of in de eerste lijn in een fysiotherapiemaatschap of gezondheidscentrum. Fysiotherapie wordt beschouwd als een van de kerndisciplines in het verstrekken van georganiseerde CVA‐zorg, waarvoor de laatste jaren verschillende multidisciplinaire richtlijnen zijn gepubliceerd. Deze richtlijnen beschouwen echter niet gedetailleerd alle beschikbare bewijs met betrekking tot de fysiotherapeutische handelingspraktijk. Fysiotherapeuten hebben de gedetailleerde informatie juist nodig om hun klinisch besluitvormingsproces te voeden en te verrijken. De fysiotherapeuten moeten bij deze besluitvorming in staat zijn een valide functionele prognose te stellen, de meest effectieve interventie te kiezen en de meest geschikte meetinstrumenten te selecteren om functionele verandering bij patiënten met een CVA te meten. Deze aspecten moeten een geïntegreerd onderdeel zijn van het dagelijks handelen. Derhalve worden in dit proefschrift twee hoofddoelstellingen bestudeerd. De eerste doelstelling betreft het systematisch verzamelen, analyseren en kritisch beoordelen van beschikbaar bewijs uit wetenschappelijke literatuur afkomstig van fysiotherapie gerelateerde studies bij patiënten met een CVA. Gebaseerd op deze bevindingen zijn richtinggevende aanbevelingen geformuleerd die medebepalend zijn in het klinisch besluitvormingsproces van fysiotherapeuten. De resultaten van de systematische werkwijze zijn gepresenteerd als de Richtlijn‐Beroerte van het

Nederlandse samenvatting
211
Koninklijk Nederlands Genootschap voor Fysiotherapie. Deze KNGF‐Richtlijn Beroerte heeft als Engelse naamgeving meegekregen: ‘Clinical practice guideline on Physiotherapy management of patients with Stroke’ (CPGPS). De tweede doelstelling is gericht op het integreren van de aanbevelingen uit de richtlijn in de dagelijkse handelingspraktijk van fysiotherapeuten die betrokken zijn bij het revalideren van patiënten met een CVA. Hierbij is het deel van de KNGF Richtlijn Beroerte geïmplementeerd dat gerelateerd is aan het ‘meten van patiëntenuitkomsten’ met de geadviseerde basisset meetinstrumenten. Gebaseerd op een analyse van belemmerende en bevorderende factoren voor het gebruik van meetinstrumenten door fysiotherapeuten is een educatieve scholingsmodule ontwikkeld (Physiotherapists’ Educational Programme on Clinimetrics in Stroke: PEPCiS). PEPCiS is in een later stadium geïmplementeerd bij een geselecteerde groep fysiotherapeuten die betrokken zijn bij de zorg van patiënten met een CVA. Hoofdstuk 2 beschrijft de resultaten van een systematische review over het effect van fysiotherapeutische interventies gericht op het verbeteren van het functioneren van patiënten met een CVA. Om de effectiviteit van fysiotherapeutische interventies te beoordelen werden tien verschillende interventiecategorieën bepaald, namelijk 1) traditionele neurologische oefenmethoden c.q. behandelconcepten; 2) programma’s voor het trainen van sensomotoriek en/of het beïnvloeden van spiertonus en stijfheid; 3) cardiovasculaire fitness‐ en aerobicprogramma’s; 4) methoden voor het trainen van loopvaardigheid en mobiliteitsgerelateerde vaardigheden; 5) oefeningen voor de bovenste extremiteit; 6) biofeedback‐therapie voor de onderste en bovenste extremiteit; 7) functionele elektrostimulatie en neuromusculaire stimulatie voor beide extremiteiten; 8) het gebruik van orthesen, slings en/of hulpmiddelen; 9) behandelingen van hemiplegische schouderpijn of handoedeem; en 10) intensiteit van oefentherapie. In de databestanden MEDLINE, CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, DARE, PEDro, EMBASE en DocOnline werd systematisch gezocht door twee onderzoekers naar gerandomiseerde studies (randomised controlled trials: RCT’s) of quasi‐experimentele studies (controlled clinical trials: CCT’s). Deze studies moesten gepubliceerd zijn voor 1 januari 2004. De gehanteerde inclusiecriteria waren: 1) participerende patiënten moesten gediagnosticeerd zijn met CVA en 18 jaar en ouder zijn; 2) studies moesten de effectiviteit van fysiotherapie evalueren in een van de tien interventiecategorieën; en 3)

Nederlandse samenvatting
212
studie waren gepubliceerd in Engels, Duits of Nederlands. De methodologische kwaliteit van de geïncludeerde studies werd beoordeeld met de 10‐punts PEDro‐schaal. Honderdeenenvijftig studies zijn geïncludeerd: 123 RCT’s en 28 CCT’s. De geïncludeerde studies hadden een mediaanscore van 5 punten op de PEDro‐schaal (range: 2‐8 punten). Meta‐analyses lieten significante ‘Summary Effect Sizes’ (SES; p<0.05) zien voor therapie gericht op functionele training van de bovenste extremiteit, zoals ‘constraint‐induced movement therapy’ (SES 0.46; 95% BI: 0.07 – 0.91), loopbandtraining met en zonder gewichtsondersteuning (respectievelijk SES 0.70; 95% BI: 0.29 – 1.10 en SES 1.09; 95% BI: 0.56 – 1.61), aerobics (SES 0.39; 95% BI: 0.05 – 0.74), het aanbieden van externe auditieve ritmen tijdens het lopen (SES 0.91; 95% BI: 0.40 – 1.42), het verbeteren van de symmetrie tijdens het opstaan vanuit een zittende positie (SES 0.92; 95% BI: 0.54 –1.29), effecten van een hogere intensiteit van oefentherapie (SES 0.13; 95% BI: 0.03 –0.23) en neuromusculaire elektrostimulatie in geval van glenohumerale subluxatie (SES 1.41; 95% BI: 0.76 – 2.06). Onvoldoende evidentie werd gevonden voor het geven van oefentherapie volgens traditionele neurologische behandelconcepten; oefentherapie voor de bovenste extremiteit; biofeedback‐therapie; neuromusculaire en functionele elektrostimulatie gericht op het verbeteren van armhand‐ of loopvaardigheid; het geven van orthesen voor de onderste extremiteit, loophulpmiddelen en/of slings. Evenmin werd evidentie gevonden voor interventies die gericht waren op het verminderen van hemiplegische schouderpijn of handoedeem. Geconcludeerd kan worden dat in deze systematische review kleine tot grote effect sizes zijn gevonden voor functionele taakgeoriënteerde oefentherapie, vooral wanneer deze intensief in de eerste maanden na het ontstaan van het CVA werd gegeven. In bijna alle geïncludeerde studies beperkten de effecten zich voornamelijk tot de activiteiten die direct in het oefenprogramma waren getraind. De allesomvattende review (Hoofdstuk 2) suggereert dat intensieve oefentherapie, gestart in de eerste 6 maanden na het ontstaan van het CVA, geassocieerd is met een sneller herstel van de uitvoering van activiteiten door patiënten met een CVA. Hierop gebaseerd is in Hoofdstuk 3 een studie uitgevoerd om ten aanzien van oefentherapie het effect van intensiteit van therapie te onderzoeken bij patiënten met een CVA. Intensiteit werd hierbij uitgedrukt in de tijd (aantal minuten) die praktisch werd besteed aan het behandelen van patiënten met een CVA. Hiertoe zijn gerandomiseerde studies systematisch beoordeeld door middel van het evalueren van de effecten van intensiteit van therapie op ADL, loopvaardigheid en

Nederlandse samenvatting
213
armhandvaardigheid. De hypothese hierbij was dat de extra therapietijd die de experimentele groepen werd toebedeeld, zou resulteren in klinisch relevante verbeteringen. Door middel van het gebruik van ‘fixed’ en ‘random’ effect modellen werden voor ADL, loopsnelheid en armhandvaardigheid SES’s berekend. Twintig RCT’s, waarin 2686 patiënten met een CVA participeerden, werden geïncludeerd in deze studie. De methodologische kwaliteit varieerde van 2 tot 11 punten (max. score 14 punten) op een aangepaste methodologische scorelijst. Statistische pooling van data die bij beëindiging van de interventieperiodes werden verzameld, resulteerde in een kleine maar statistisch significante random SES voor ADL (SES 0.13; 95% BI, 0.03 ‐ 0.23). Verdere analyses lieten een significante homogene SES zien voor 17 studies die de effecten van een toegenomen intensiteit van oefentherapie onderzochten in de eerste 6 maanden na ontstaan van het CVA. Geen significante homogene SES werd gevonden voor de 3 studies die plaats vonden in de chronische fase na het CVA. Gemiddeld ontvingen de experimentele groepen twee keer zoveel fysiotherapie (49 min.) en ergotherapie (23 min.) dan de controlegroepen (resp. 23 en 11 min.). Een cumulatieve meta‐analyse voor het verschil in behandelintensiteit van elke individuele studie suggereert in sterke mate dat tenminste 16 uur verschil in behandeltijd, aangeboden in de eerste 6 maanden na het ontstaan van een CVA, nodig is om een significant verschil in ADL te verkrijgen. Een significante SES, in het voordeel van een hogere behandelintensiteit, werd ook aangetoond voor instrumentele ADL (SES 0.23; 95% BI: 0.13 – 0.33) en loopsnelheid (SES 0.19; 95% BI: 0.01 – 0.36), terwijl geen significante SES werd gevonden voor armhandvaardigheid (SES 0.03; 95% BI: ‐0.13 – 0.19). Verbetering van een symmetrische gewichtverdeling over beide benen tijdens het rechtop staan is een van de belangrijkste behandeldoelen gebleken bij het revalideren van patiënten met een CVA. In Hoofdstuk 4, is systematisch de evidentie bestudeerd voor het effect van de toepassing van additionele ‘visuele feedback therapie’ (VFT) op het evenwicht tijdens het rechtop staan bij patiënten met een CVA. Het hoofddoel was te onderzoeken of VFT bij patiënten met een CVA de houdingszwaai kan reduceren en de links‐rechts symmetrie tijdens bilateraal staan kan verbeteren, vergeleken met patiënten die conventionele therapie ondergingen. Tevens werden de effecten van VFT bestudeerd op parameters zoals evenwicht, lopen en ADL. Acht van de 78 verzamelde studies (6 RCT’s en 2 CCT’s), waarin 214 patiënten participeerden, werden geïncludeerd voor een kwalitatieve en kwantitatieve analyse. De methodologische kwaliteit op de PEDro‐schaal

Nederlandse samenvatting
214
varieerde van 3 tot 6 punten. De toegevoegde (additionele) waarde van VFT tijdens bilateraal staan vergeleken met conventionele therapie liet geen statistisch significant effect zien op symmetrie van gewichtsverdeling tussen het paretische en niet‐paretische been, houdingszwaai, evenwicht, lopen en ADL. Visuele feedback therapie moet derhalve niet de voorkeur krijgen boven conventionele therapie. Deze resultaten van hoogklinische waarde geven aan dat het trainen van evenwicht bij voorkeur plaats moet vinden tijdens de te trainen loopgerelateerde activiteiten zelf. De vraag blijft bestaan hoe asymmetrie in gewichtverdeling zich verhoudt tot controle van het evenwicht bij patiënten met een CVA. In Hoofdstuk 5 is de beschikbare evidentie verzameld en beschreven om fysiotherapeuten te assisteren in hun klinisch besluitvormingsproces tijdens het revalideren van patiënten met een CVA. Dit is vooral toegespitsts op het selecteren van 1) geschikte prognostische factoren, 2) fysiotherapeutische interventies en 3) meetinstrumenten die in staat zijn functionele vooruitgang van patiënten met een CVA te evalueren. Deze evidentie is in Nederland gepresenteerd als de KNGF‐Richtlijn Beroerte (Clinical Practice Guideline on Physiotherapy management of patients with Stroke: CPGPS). In verschillende databestanden werd systematisch gezocht naar evidentie met betrekking tot prognostiek, interventies en meetinstrumenten. Fysiotherapeuten werkzaam in de CVA‐revalidatie en een multidisciplinaire groep professionals die ook betrokken zijn bij CVA‐zorg hebben de klinische bruikbaarheid van de richtlijn en de praktische toepassing van de aanbevelingen beoordeeld. Hun commentaar werd gebruikt om de definitieve richtlijn op te stellen. Van de 9482 relevante artikelen zijn er 322 geselecteerd en op methodologische kwaliteit beoordeeld. Uit de geselecteerde artikelen zijn 72 aanbevelingen voor de klinische praktijk opgesteld en opgenomen in de richtlijn: 6 aanbevelingen betreffen het voorspellen van functioneel herstel na CVA voor activiteiten van het dagelijks leven, loopvaardigheid en armhandvaardigheid; 65 aanbevelingen betreffen de keuzes voor fysiotherapeutische interventies; en 1 aanbeveling betreft de keuze voor het gebruik van meetinstrumenten. Een basisset van 7 betrouwbare, responsieve en valide meetinstrumenten is vastgesteld om stoornissen in functies en beperkingen in activiteiten en participatie te kunnen bepalen bij patiënten met een CVA. De richtlijn geeft fysiotherapeuten evidence‐based aanbevelingen die hen assisteren in de klinische besluitvorming ten aanzien van het behandelen en evalueren van patiënten met een CVA. De meeste aanbevelingen die in de richtlijn zijn opgenomen, zijn afkomstig van studies waarin patiënten participeerden die

Nederlandse samenvatting
215
zich in de postacute en chronische fase na een CVA bevonden. Tevens hebben de meeste studies die in de richtlijn zijn opgenomen minder ernstig aangedane patiënten en patiënten met weinig of geen co‐morbiditeit geïncludeerd, terwijl juist behoefte is aan meer kennis omtrent ernstige en gecompliceerde patiënten met een CVA. De basisset meetinstrumenten uit de KNGF‐Richtlijn Beroerte bestaat uit de Motricity Index (MI), Trunk Control Test (TCT), Berg Balance Scale (BBS), Functional Ambulation Categories (FAC), Ten Metre Walk (TMW), Frenchay Arm Test (FAT) en Barthel Index (BI). Het meten, evalueren en monitoren van de functionele status van patiënten wordt beschouwd als een aspect van goede klinische praktijkvoering door fysiotherapeuten. Zodoende is na disseminatie van de KNGF‐Richtlijn Beroerte in Hoofdstuk 6 onderzocht, in welke mate fysiotherapeuten aangeven de geadviseerde meetinstrumenten uit de KNGF‐Richtlijn Beroerte te gebruiken. Tevens is bestudeerd welke belemmerende en bevorderende factoren door hen worden ervaren om meetinstrumenten al dan niet in de dagelijkse handelingspraktijk te gebruiken. Een vragenlijst bestaande uit 41 items, waaronder de vragen naar belemmerende en bevorderende factoren (Barriers and Facilitators Questionnaire, BFQ), was per post verzonden naar 400 fysiotherapeuten, werkzaam in ziekenhuizen (acute care hospitals: ACH; N=100), revalidatiecentra (RC; N=100), verpleeghuizen (nursing homes: NH; N=100) en 1e lijnfysiotherapie praktijken (private physiotherapy practices: PPP; N=100). De vragenlijst werd door 198 fysiotherapeuten geretourneerd (47%; ACH, N=57; RC, N=67; NH, N=26 en PPP, N=39). De 167 vragenlijsten afkomstig van fysiotherapeuten betrokken bij CVA‐zorg konden worden geanalyseerd. Deze fysiotherapeuten rapporteerden een regulier gebruik van drie (mediaan; range 0‐7) van de zeven geadviseerde meetinstrumenten, waarbij de fysiotherapeuten werkzaam in ACH of RC een significant hoger gebruik rapporteerden dan hun collega’s in PPP (resp. 4 versus 0 en 3 versus 0; p<0.001 en p=0.02). De BFQ laat specifieke bevorderende factoren zien, zoals ‘positieve attitude ten aanzien van meetinstrumenten’ (genoemd door 93% van de fysiotherapeuten) en ‘bekendheid met meetinstrumenten’ (90%) en belemmerende factoren, zoals ‘veranderen van routines’ (32%), ‘tijdsinvestering’ (29%), en ‘financiële compensatie’ (21%). Ondanks een door vrijwel alle therapeuten geopperde positieve attitude, gebruiken Nederlandse fysiotherapeuten de geadviseerde meetinstrumenten niet in voldoende mate. Krachtige settingspecifieke en op maat gesneden implementatiestrategieën gebaseerd op de gerapporteerde bevorderende en belemmerende factoren worden aanbevolen.

Nederlandse samenvatting
216
Om het zelfgerapporteerde en actuele gebruik van meetinstrumenten door fysiotherapeuten in de CVA‐zorg te verhogen, is een nieuwe scholingsmodule ontwikkeld, het zogenoemde Physiotherapists Educational Program Clinimetrics in Stroke (PEPCiS). In Hoofdstuk 7 wordt de haalbaarheid en effectiviteit van deze scholingsmodule onderzocht in een gerandomiseerd onderzoek. In deze RCT werden 30 fysiotherapeuten, werkzaam in de CVA‐zorg, gerandomiseerd over twee numeriek gelijke groepen, een ‘expert tutor groep’ (ETG) en ‘non‐expert tutor groep’ (NETG). De twee tutoren verschilden in de mate van klinische ervaring met meetinstrumenten bij patiënten met CVA. Tevens werd de invloed van tutorstijl verkend in deze haalbaarheidsstudie. De haalbaarheid van de studie werd beoordeeld door middel van het evalueren van de betrokkenheid van de geïncludeerd fysiotherapeuten, de tevredenheid ten aanzien van PEPCiS, en de waardering van tutorstijl van de aan hen toegewezen tutor. Effectiviteit door het berekenen van het aantal keer genoteerd gebruik van meetinstrumenten in de patiëntenstatussen door de participerende fysiotherapeuten. Over het algemeen waren de fysiotherapeuten goed betrokken (mediaan van 5 scholingssessies; range 4‐5) en tevreden met PEPCiS (gemiddeld cijfer: 7.5 op een 0‐10 schaal). In de totale groep (N=30) steeg het gebruik van meetinstrumenten van 3 per patiënt voorafgaand aan PEPCiS tot 5 na afloop (p=0.001). De ‘tussen‐groep’ verschillen zijn niet significant voor het totaal aantal gebruikte meetinstrumenten (mediaan van 3 naar 6 in de ETG versus van 3 naar 4 in de NETG; p=0.07). Fysiotherapeuten in the ETG waarderen de inhoud van PEPCiS, hun kennistoename en alle tutorstijl aspecten significant beter dan hun collega’s in de NETG (p<0.05). Deze pilotstudie suggereert dat educatie door middel van PEPCiS het gebruik van klinische meetinstrumenten door fysiotherapeuten die betrokken zijn bij de zorg van patiënten met een CVA, doet toenemen. In een toekomstig onderzoek met voldoende statistische power zal de invloed van PEPCiS en interfererende factoren zoals ervaring en performance van de tutoren bestudeerd moeten worden om daarmee de effectiviteit van educatieve interventies, als onderdeel van een implementatiestrategie, te verbeteren, zoals bijvoorbeeld het reguliere gebruik van meetinstrumenten door fysiotherapeuten. Hoofdstuk 8 presenteert een algemene discussie waarin de hoofdconclusies van dit proefschrift besproken worden en de sterke en zwakkere punten van de gehanteerde methoden bediscussieerd worden. Tevens geeft Hoofdstuk 8 klinische implicaties betreffende fysiotherapie bij patiënten met een CVA, aanbevelingen voor toekomstig CVA‐onderzoek en suggesties voor educatie

Nederlandse samenvatting
217
en implementatie van onderzoeksresultaten in de dagelijkse handelingspraktijk van professionals in de CVA‐zorg. References
1. Struijs JN, van Genugten ML, Evers SM et al. Modeling the future burden of stroke in The Netherlands: impact of aging, smoking, and hypertension. Stroke 2005; 36:1648‐1655.
2. Koek HL, Van Dis SJ, Peters RJG et al. Hart‐en vaatziekten in Nederland. In: Van Leest LATM, Koek HL, Van Trijp MJCA et al., editors. Hart‐en vaatziekten in Nederland 2005, cijfers over risicofactoren, ziekte, behandeling en sterfte [dutch]. Den Haag: Nederlandse Hartstichting, 2005: 6‐12.

Nederlandse samenvatting
218

Dankwoord

Dankwoord
220
Dankwoord Tijdens de jaren die ik als fysiotherapeut werkzaam was in revalidatiecentra, stelde ik mij meer en meer de vraag of fysiotherapie bij patiënten met een CVA er wel toe doet. Is er bewijs voorhanden dat bepaalde behandelingen effectief zijn? Is het mogelijk om beter te voorspellen welke activiteiten een patiënt na een beroerte weer kan uitoefenen? Zijn veranderingen in het herstel van deze patiënten objectief te beschrijven? Dat deed mij besluiten om bewegingswetenschappen te gaan studeren. De antwoorden die ik tijdens die studie kreeg hebben mij geholpen om ‘fysiotherapie bij patiënten met een CVA’ kritischer te gaan bekijken. Maar niet alle vragen kregen een antwoord. Er lag nog een groot onderzoeksveld braak. Het was eigenlijk nooit mijn ambitie te gaan promoveren, ik rolde min of meer vanzelf in dit promotietraject. Ik kreeg de kans om mijn interessegebied verder te onderzoeken, waarbij ik zowel de ‘wetenschap’ als de ‘praktijk’ wilde voeden. Maar zoals, ‘towards’, het startwoord van mijn thesistitel al doet vermoeden, is nog niet alles bekend, onderbouwd of bewezen op het gebied van evidence‐based fysiotherapie bij patiënten met een beroerte. De jaren van mijn promotie vormde een prachtige leerzame periode waarin veel vragen zijn gesteld, veel antwoorden zijn gegeven, maar ook veel nieuwe vragen zijn ontstaan. Het interessante van een promotietraject is dat het je ook samen brengt met veel mensen die ieder op zijn of haar eigen wijze een bijdrage leveren aan de totstandkoming van het proefschrift. In het bijzonder wil ik dan ook de volgende personen bedanken: Professor dr. Eline Lindeman, beste Eline, je bent als mijn promotor op
een rijdende trein gesprongen. Ik was al deels op gang gekomen toen ik in Utrecht kwam werken. Jouw hoogleraarschap bij de Divisie Hersenen van het UMC Utrecht maakte het logisch dat ik, als medewerker van dezelfde divisie, bij jou ging promoveren. Mijn verzoek of je als mijn promotor wilde fungeren heb je direct en enthousiast opgepakt. Zelfs op de momenten dat je fysieke tegenslag kende, maakte je tijd vrij voor mij. Ons interessegebied qua onderzoek ligt bij het revalideren van patiënten met een CVA en dat was merkbaar in de discussies die we voerden. Bedankt voor de begeleiding en het vertrouwen dat ‘promoveren’ mij zou lukken. Dr. Gert Kwakkel, beste Gert, ik ben jou veel dank verschuldigd. Jij hebt
mij als onderzoeker een plek heeft gegeven in de wetenschappelijke wereld. In 2002 kreeg jij mijn scriptie over ‘het meten van evenwicht bij patiënten

Dankwoord
221
met een CVA’ onder ogen, waarmee ik de universitaire opleiding bewegingswetenschappen had afgerond. Deze scriptie hebben we samen omgevormd tot onze eerste gezamenlijke publicatie in het Jaarboek Fysiotherapie. Later hebben we ook andere hoofdstukken en artikelen samen geschreven. Ook bood je me de gelegenheid om als projectmedewerker in het VU medisch centrum te komen werken, waar onder jouw bezielende en vakkundige leiding de KNGF‐Richtlijn Beroerte tot stand is gekomen. Daar is ook het idee ontstaan om te gaan promoveren. Uiteraard werd jij mijn co‐promotor, voor een promotorschap was het nog net te vroeg, anders had ik het je zeker gevraagd. Je hebt me veel bijgebracht op zowel methodologisch als vakinhoudelijk gebied. Inmiddels heb je wereldwijd faam opgebouwd als vooraanstaand wetenschapper op het gebied van ‘stroke rehabilitation’. Bedankt voor jouw begeleiding. Ik ben er trost op dat je mijn opleider bent geweest en hoop de samenwerking nog lang met je voort te zetten . Dr. Nico van Meeteren, beste Nico, mijn tweede co‐promotor. In 2004
heb je mij aangenomen als stafmedewerker Onderwijs, Onderzoek & Ontwikkeling voor de opleiding Fysiotherapiewetenschap (FW). Een opleiding die jij ‘smoel’ hebt gegeven. Ik werd onderdeel van jouw docenten‐ en onderzoekersteam, een dedicated team. De drie FW‐jaren zal ik om meerdere redenen niet snel vergeten. Naast onze reguliere drukke onderwijswerkzaamheden heb je altijd tijd gevonden mij positiefkritisch bij te staan in het afronden van mijn proefschrift. In onze gesprekken heeft jouw passie voor wetenschap en fysiotherapie mij enorm geïnspireerd. Net als de andere pioniers van de opleiding Fysiotherapiewetenschap heb jij inmiddels een nieuwe uitdagende baan gevonden. Succes op jouw nieuwe stek. Ik kijk met een goed gevoel terug op onze samenwerking en wil je daar uiteraard voor bedanken. In de toekomst hoop ik dat we elkaar zullen blijven treffen en inspireren. Dr. Marieke Schuurmans, beste Marieke, mijn derde co‐promotor. Ik
werk pas een jaar in ‘jouw lectoraat’ op de Hogeschool Utrecht en heb daarin volop ruimte gekregen om mijn proefschrift af te ronden. Ook jij bent op de rijdende trein gesprongen, maar voordat je dat deed, heb je me duidelijk gemaakt dit alleen te doen als je een relevante bijdrage kon leveren aan mijn proefschrift. Inmiddels een jaar verder is dat duidelijk waarneembaar. Je hebt me ‘achter de oren laten krabbelen’ als ik in de conceptversies van mijn manuscript jouw potloodkanttekeningen las. Het proefschrift is er door jouw inbreng zeker beter van geworden. Bedankt, ik

Dankwoord
222
hoop in het Kenniscentrum ‘Innovatie van Zorgverlening’ nog veel projecten samen met je op te pakken. Het is prettig met je samenwerken.
Om alle schijn van voorkeur te voorkomen pak ik de ‘bedankdraad’ chronologisch en alfabetisch op.
Als fysiotherapeut‐in‐opleiding ben ik door docenten en studenten gevormd op de Haagse Academie voor Lichamelijke Opvoeding & Fysiotherapie. Op mijn stageadres, het Nederlands Zeehospitium in Kijkduin, heb ik mijn eerste patiënt met een CVA behandeld. En bij mijn eerste werkgever, het revalidatiecentrum De Trappenberg in Huizen ben ik door het volgen van de cursus Neuro Developmental Treatment (NDT) begonnen met het specialiseren op het specifieke domein CVA. Daarna nog een uitstap gemaakt naar De Adriaanstichting in Schiebroek, waar ik met veel plezier en met een hoop toegewijde collega’s, kinderen met diverse aandoeningen heb gerevalideerd. Hoewel de aangereikte kennis met betrekking tot het behandelen van patiënten met een CVA uit deze jaren enigszins is veranderd, wellicht verouderd, heb ik in die tijd veel opgestoken. Een ieder die mij in die periode op weg heeft geholpen wil ik, zonder namen te noemen, bedanken. Vanaf 1995 ben ik gaan werken in het revalidatiecentrum Rijndam in
Rotterdam. Vanaf de bouw ben ik bij dit centrum betrokken geweest, en hoe kan het anders, de eerste patiënt die ik op de klinische behandelafdeling 2 (KBA‐2) ging behandelen was een patiënt met een CVA. Rijndam heeft mij de mogelijkheid gegeven om de deeltijdopleiding bewegingswetenschappen in Maastricht op te pakken. Ook heb ik op KBA‐2 mijn eerste pilotstudy uit kunnen voeren om de relatie tussen evenwicht en loopfunctie te onderzoeken bij patiënten met een CVA. Hier is ook het besef gekomen dat ‘klinimetrie’ (het in kaart brengen, meten, van mogelijkheden en onmogelijkheden van patiënten met meetinstrumenten) een belangrijk hulpmiddel is. Uit de ‘Rijndamtijd’ wil ik alle collega’s bedanken die het werken in dit centrum tot een plezier maakten. Een aantal Rijndam‐collega’s wil ik in het bijzonder bedanken, omdat zij samen met de eerste ‘klinimetrische stappen’ hebben gezet (Mariella Aarden, Irene de Bruijn, Arne Goedhart, Gerard Hommes, Leonie Oostveen, Karin Postma) of mij gestimuleerd hebben bij mijn eerste ‘wetenschappelijke stappen’ (Michael Bergen, Hans Bussman en Gerard Ribbers).

Dankwoord
223
Tijdens mijn opleiding Bewegingswetenschappen aan de Universiteit Maastricht ben ik in een enorme enthousiaste groep medestudenten terechtgekomen. Tijdens de studie zijn Jan Willem de Bruijn, Roland van Grinsven, Hans Hobbelen, Ton Lenssen, Karin Postma en Walter van der Weegen, vrienden geworden en hebben we met elkaar het Instituut voor Bewegingsvraagstukken (IBV) opgericht. Door onze drukke reguliere werkzaamheden is deze IBV‐denktank verworden tot een reünieclub die elkaar één à twee keer per jaar treft bij een sportieve activiteit, een biertje of een etentje. Maar ook Rob de Bie, Eric van Rossum en Henk Seelen wil ik bedanken voor het begeleiden van mijn afstudeerproducten in Maastricht. De twee jaar die ik op het Vrije Universiteit medisch centrum in
Amsterdam heb gewerkt bij de Dienst Fysiotherapie zullen me altijd bij blijven. Met Marc Rietberg en Benno van Tol als kamergenoten hebben we naast heel hard werken ook veel plezier kunnen hebben. Niet iedereen kon in Amsterdam mijn liefde voor Feijenoord begrijpen, helaas speelden Ajax (Marc) en AZ (Benno) in die tijd regelmatig beter voetbal dan Feijenoord, maar mijn pantser heeft altijd stand gehouden. Ook met Erwin van Wegen heb ik destijds een geweldige tijd beleefd in het VUmc en zeker onze gezamenlijke trip naar de World Confederation for Physical Therapy (WCPT) in Barcelona zal onuitwisbaar blijven. Ook alle andere collega’s van de Dienst Fysiotherapie van het VUmc wil ik bedanken voor de prettige samenwerking. En speciaal Rob van Klaveren voor zijn vertrouwen in mij en zijn inspanningen om mijn tijdelijke aanstelling telkens maar weer te verlengen, totdat de rek er uit was. Daarna zocht, en vond, ik mijn heil in Utrecht. Ik kwam in een enorm
inspirerend team te werken bij de opleiding Fysiotherapiewetenschap van de Universiteit Utrecht met collega’s die zowel gedreven docenten, onderzoekers als onderwijsontwikkelaars waren. Met alle collega’s uit die tijd was het fantastisch samenwerken. Rob van Dolder, Jaap Dronkers, Frank van Genderen (ook bedankt voor de waardevolle tips hoe je zelf de lay‐out van tekst en tabellen in het proefschrift kunt verzorgen), Janke de Groot, Nico van Meeteren, Jan Prins, Carin Schröder (ook bedankt voor de jouw suggesties met betrekking tot de Theory of Planned Behaviour), Miranda Velthuis en Harriet Wittink zijn inmiddels allemaal bij de opleiding Fysiotherapiewetenschap vertrokken. Onderling hebben, en houden, wij een sterke en vriendschappelijke band, dat weet ik zeker. Het waren drie inspirerende, leerzame jaren.

Dankwoord
224
Naast mijn deeltijdbaan bij de Universiteit Utrecht startte ik in die tijd ook als docent ‘centraal neurologische aandoeningen’ (CNA) bij de opleiding Fysiotherapie van de Hogeschool Utrecht. Ook daar trof ik het met Henk Dekkers, Joost Leonhard, Mient Riddersma, Mariska van Vugt en Els Veekens als naaste CNA collega‐docenten. Na een jaar heb ik de overstap gemaakt naar de Professional Masteropleiding Fysiotherapie (PMF) en heb me daar ingezet om de implementatie van ‘best‐practice ontwerpen’ door masterstudenten in het fysiotherapeutisch werkveld gestalte te geven. Het kernteam van de PMF is klein en ook weer gedreven. Het is prettig samenwerken in dit team met Ina Bettman, Rob van Dolder, Jaap Dronkers, Rutger IJntema, Han Kingma, Els de Lange, Jacqueline Nuijsink, Jorrit Rehorst en Dammis Vroegindeweij. Maar niet alleen mijn collega’s van het kernteam PMF wil ik bedanken, zeker ook de collega’s die als projectbegeleiders dagelijks met onze studenten optrekken in het BPO‐onderwijs. De laatste tijd heb ik veel drukte aan mijn hoofd gehad met het afronden van mijn thesis, maar met elkaar hebben we toch het BPO‐onderwijs op de kaart gezet en draaiende gehouden. Liesbeth Bosma, Mohamed Elhadouchi, Raoul Engelbert, Hans Heneweer, Hans Hobbelen, Erik Hulzebos, Jaap Jansen, Sandra Jorna, Barbara Kölzer, Francois Maissan, Jacqueline Outermans, Edwin de Raaij en Kitty Meijer, bedankt.
En mijn speciale dank gaat uit naar Mieke Klootwijk, Harm Drost, Harriët Wittink en Marieke Schuurmans die mogelijkheden wisten te creëren waarmee het promoveren via de Hogeschool Utrecht voor mij mogelijk werd. En ook de andere collega’s van de hogeschool zijn een factor waardoor ik toch telkens weer met een positieve insteek de reis van Delft naar Utrecht onderneem. En dat we deze zomer tijdens de Tour de France met veel hogeschoolcollega’s weer om de ‘wisselfiets’ kunnen strijden. Lars (van Rijswijk), ‘patron’ van ons tourspel, ik heb nu weer alle tijd om mij optimaal voor te bereiden op de editie 2008, alle uitslagen zal ik in het voorseizoen weer punctueel napluizen. Dat het wederom een mooi jaar mag worden. Bij de prijsuitreiking van de ‘wisselfiets’ op de Beaujolaisavond ben ik er zeker bij. De lectoren en mijn collega’s van het Lectoraat ‘Verpleegkundige en
paramedische zorg voor mensen met chronische aandoeningen’ van de Hogeschool Utrecht, Ilse Arts, Mia Duijnstee, Roelof Ettema, Thóra Hafsteinsdóttir, Jita Hoogerduijn, Michel Jansen, Anneke de Jong, Marijke Rensink, Maaike Smole, Marieke Schuurmans en Carolien Sino, wil ik bedanken dat ik mijn aandacht in het eerste jaar van mijn aanstelling volledig heb kunnen richten op het afronden van mijn proefschrift.

Dankwoord
225
Bij de verschillende werkgevers tijdens mijn promotietraject heb ik goede
en prettige secretariële ondersteuning gehad. Inge Kuurman (Fysiotherapiewetenschap), Sue McClelland (UMCU), Marjan van de Monde (VUmc) en Maaike Smole (HU), bedankt voor de werkzaamheden die jullie mij uit handen hebben genomen. Bij het tot stand komen van de KNGF‐Richtlijn Beroerte heb ik met een
achttal zeer bekwame en in CVA‐zorg gespecialiseerde fysiotherapeuten kunnen samen werken, die als klankbordgroep hebben gefungeerd. Ik wil Meike Berns, Jaap Buurke, Barbara Harmeling, Jos Halfens, Hans Hobbelen, Boudewijn Kollen, Matthijs Vogel en Lydia Wagenborg bedanken voor hun specialistische bijdrage en plezierige samenwerking. Ook veel dank aan de medeauteurs van de artikelen die de afgelopen
jaren zijn geschreven en zijn opgenomen in dit proefschrift: Ann Ashburn, Joost Dekker, Rob van Dolder, Frank van Genderen, Paul Helders, Erik Hendriks, Michiel Kortsmit, Gert Kwakkel, Peter Langhorne, Eline Lindeman, Nadina Lincoln, Francois Maissan, Nico van Meeteren, Kimberly Miller, Cecily Partridge, Carol Richards, Marieke Schuurmans, Eric Stutterheim, Robert Wagenaar, Philip van der Wees, Ian Welwood en Sharon Wood‐Dauphinee. Zonder jullie inbreng was de kwaliteit van de artikelen waarschijnlijk minder goed geweest. Meta Wildenbeest ben ik dank verschuldigd voor haar inzet als ‘tutor’ in
een van de studies van dit proefschrift. Tevens wil ik een aantal studenten van de opleiding Fysiotherapiewetenschap bedanken: Ivo Daanen, Hans Herik, Erwin Huiszoon, Han Kingma, Leny de Ligny, Koert Nederbragt, Eric Passchier, Peter Viehoff, Judith Weijman en Elles Zock. Zij hebben geholpen bij het uitvoeren van een deelproject dat nu deel uitmaakt van dit proefschrift. Boudewijn Kollen, Cas Kruitwagen en Paul Westers, bedankt voor jullie
suggesties met betrekking tot de statistische analyses die ik heb uitgevoerd. Statistiek blijft een vak apart. Verder ben ik dankbaar, dat ik in juni 2007 in Canada tijdens de World
Confedaration for Physical Therapy (WCPT) in Vancouver een zeer gemotiveerde internationale groep fysiotherapeuten heb ontmoet. Deze fysiotherapeuten en onderzoekers uit Amerika, Australië, Canada,

Dankwoord
226
Engeland, Zuid‐Afrika en Nederland zijn voornemens de International Neuroscience Physiotherapy Association op te richten. Louise Ada, Ralph Hammond, Fiona Jones, Cherry Kilbride, Mindy Levin and Mary Solomon thanks for inviting me. A collaboration to look forward to. Het manuscript ben ik vlak voor de kerstvakantie gaan afleveren bij alle
leden van de beoordelingscommissie. In plaats van vakantie vieren hebben ze tijd vrij gemaakt voor mijn proefschrift. Ik wil Prof. dr. R.A. De Bie, Prof. dr. G. Croiset, Prof. dr. J. Dekker, Prof. dr. L.J. Kappelle en Prof. dr. Th.J.M. Verheij, als voorzitter van deze commissie, hartelijk danken voor het kritisch beschouwen van het manuscript. Mijn paranimfen, Rob van Dolder en Frans van der Zon. Beste Rob, we zijn in 2004 ongeveer tegelijk gaan werken bij de opleiding
Fysiotherapiewetenschap en sindsdien zijn we onafscheidelijk gebleken. We hebben op diverse plekken intensief samen gewerkt en doen dat nog steeds op innige en humoristische wijze. Niet alleen als collega ook als vriend heb je een plek veroverd. Laten we nog veel mooie dingen samen gaan maken en doen. En laat de spreuk op jouw toilet, thuis in Zeist, altijd hangen: ‘No Brain, No Headache’. Ik weet namelijk nog steeds niet of je dan blij moet zijn met hoofdpijn of juist niet.
Beste Frans, wij kennen elkaar al een aanzienlijke tijd. Een vriendschap vanaf de 1e klas van de Cornelius Musiusschool, onze lagere school in Delft. In augustus 2007 vierden we onze veertigjarige vriendschap. Onze wegen liepen lang parallel, zelfde lagere en middelbare school, zelfde sportverenigingen, gezamenlijke vakanties. Dat we er nog minstens 40 jaar aan vast mogen knopen en nog lang samen kunnen biken, schaatsen, hardlopen (je weet het nooit), skeeleren, voetballen (nee, dat is echt voorbij, toch?) en korfballen (maar uitsluitend kijken hoor!).
Rob en Frans, vrienden hoef je eigenlijk niet op schrift te bedanken, dat blijkt uit andere dingen. Ik hoop nog veel plezier uit onze vriendschappen te halen. En het etentje bij de Heeren van Delft is voor herhaling vatbaar. Mijn fietsmaten, William Lustig, Edward Nijboer, Cinco Veldman,
Gerco Vredeveldt, Mario van der Wel en Frans van der Zon, zonder onze asfalt‐ of terreintochten op zondagochtend had ik nu stijf, dik en humorloos aan de kant gezeten. Ik kijk weer uit naar de stormachtige ritten door het Westland of het Groene Hart, de acrobatische hoogstandjes in Sweet Lake City of in Warempage, de verhalen die vaak nergens over gaan en natuurlijk naar het koffiedrinken bij de Klimwand of De Snor (hoewel die gevlogen

Dankwoord
227
lijkt). In plaats van de wekelijkse korte en krachtige fietsoproep per e‐mail, nu alvast (is weer eens wat anders) een oproep voor aanstaande zondag: “Bikers, zondag 1 juni 2008, 9.15 uur, V16, terrein, noppenbanden, akkoord?” Mijn andere vrienden en vriendinnen die ik ondanks de hectiek van
alledag die we allemaal ervaren, toch met regelmaat blijf zien. Door het schrijven van het proefschrift is bij sommige vrienden de regelmaat wel in een zeer lage frequentie terechtgekomen (maar dan zit er toch regelmaat in). De afronding van het proefschrift is een goede aanleiding om weer bij vrienden langs te gaan voor een kop koffie of gewoon een avondje de kroeg in te duiken. En niemand hoeft zich meer op voorhand bezwaard te voelen om spontaan bij ons aan te bellen. Ik dank mijn schoonouders, Krijna en Henny Kouwenhoven, mijn zus,
Angelique, maar bovenal mijn ouders, Coby en Martin van Peppen, die mij stimuleerden en ook altijd hun belangstelling toonden over de voortgang van mijn promotie. Ik draag het proefschrift op aan mijn ouders. Ook al was het voor jullie soms lastig om inhoudelijk te kunnen doorgronden waar ik mee bezig was. Jullie hebben mijn basis gelegd, me klaar gestoomd voor deze wereld en me in staat gesteld om mijn eigen keuzes te leren maken. Ik hoop voor jullie en mijn andere familieleden en vrienden de komende periode meer tijd vrij te kunnen maken om elkaar te zien. Mijn kinderen Tim & Lara zagen mij in de avonduren en weekenden vaak achter mijn laptop zitten. “Is dat nou promoveren?”, hoorde ik ze regelmatig mompelen. In de weekenden maakte ik gelukkig steeds tijd vrij om als supporter bij hun korfbalwedstrijden te zijn. Blijf lekker sporten, is beter dan achter de PC zitten. Ik ga, nu het leven (hopelijk) iets minder ‘vol’ zal worden, ook minder ‘computeren’ en meer sporten. Blijk ik toch opeens aan voornemens te doen!
Maar de meeste dank en waardering gaat natuurlijk uit naar Marianne. Ze heeft me, om in wielertermen te spreken, ‘uit de wind gehouden’. Ik heb de afgelopen jaren vrijwel niets meer in het huishouden gedaan, terwijl ik me daar voorheen toch wel hard voor maakte. Albert Heijn heb ik al lang niet meer van binnen gezien. Marianne, jouw schaarse vrije tijd ging op aan dingen waar ik niet aan toe kwam. Wat ik van jou vind, weet je al en zeg ik liever rechtsreeks tegen je dan dat ik het via dit proefschrift kenbaar maak. En mocht ik iemand vergeten zijn in dit dankwoord. Dat was niet mijn
bedoeling. Ook alle niet bij naam genoemden bedankt.

Dankwoord
228

Publications

Publications
230
International journals
Van Peppen RPS. Guest Editorial ‐ International collaboration in physiotherapy management of people with stroke. Physiotherapy Research International, 2008;13(1):3‐8
Van Peppen RPS; Hendriks HJM; Van Meeteren NLU; Helders PJM; Kwakkel G. The development of a clinical practice stroke guideline for physiotherapists in the Netherlands: a systematic review of available evidence. Disability and Rehabilitation, 2007;29(10):767‐783
Van Peppen RPS, Kortsmit M, Lindeman E, Kwakkel G. Effects of visual feedback therapy on postural control in bilateral standing after stroke: a systematic review. Journal of Rehabilitation Medicine, 2006;38 (1):3‐9
Hobbelen JS, Koopmans RT, Verhey FR, Van Peppen RP, de Bie RA. Paratonia: a delphi procedure for consensus definition. Journal of Geriaticr Physical Therapy, 2006;29(2):50‐56
Smidt N, De Vet HC, Bouter LM, Dekker J, Arendzen JH, De Bie RA, Bierma‐Zeinstra SM, Helders PJ, Keus SH, Kwakkel G, Lenssen T, Oostendorp RA, Ostelo RW, Reijman M, Terwee CB, Theunissen C, Thomas S, Van Baar ME, Van ʹt Hul A, Van Peppen RP, Verhagen A, Van der Windt DA; Exercise Therapy Group. Effectiveness of exercise therapy: a best‐evidence summary of systematic reviews. Australian Journal of Physiotherapy, 2005;51(2):71‐85
Van Peppen RPS; Kwakkel G; Wood‐Dauphinee S; Hendriks HJM, Van der Wees Ph; Dekker J. The impact of physical therapy on functional outcomes after stroke: whatʹs the evidence? Clinical Rehabilitation, 2004;18(8):833‐862
Kwakkel G; Van Peppen R; Wagenaar RC; Wood Dauphinee S; Richards C; Ashburn A; Miller K; Lincoln N; Partridge C; Wellwood I; Langhorne P. Effects of augmented exercise therapy time after stroke: A meta‐analysis. Stroke, 2004;35(11):2529‐2536

Publications
231
Dutch journals
Outermans J, Van Peppen RPS.Trainen na een beroerte: dat kan! Training van de fysieke fitheid bij CVA‐patiënten voor het verbeteren van de loopvaardigheid. Sportgericht, 2007;61(6):37‐40
Kleijn A, Schuurmans R, De Raaij E, Van de Hart M, Baijens H, Van Peppen RPS. Manuele Therapie bij heuparthrose: Een evidence‐based manueeltherapeutisch behandelprotocol met objectivering van behandelresultaten. MoveMens, 2007;8(5):44‐45
Vereijken A, Sijbers R, Outermans J, Meijer A, Portegies S, Stok K, Baijens H, Van Peppen RPS. Sporthervatting na voorste kruisband reconstructie. InFysio, 2007; 3(11):14‐15
Van Peppen RPS. ‘Uw Vraag, Ons Project’: Praktijkveld en masterstudenten fysiotherapie maken samen Best‐Practice Ontwerp. FysioPraxis, 2007; 16(11):18‐21
Outermans JC; Van Peppen RPS; Takken T. Fysieke Fitheidstraining na een CVA: een review. Nederlands Tijdschrift voor Fysiotherapie, 2007;117(4):135‐141
Prins JCM; Velthuis JM; Van Peppen RPS; Van Meeteren NLU. Peer support in de Utrechtse opleiding Fysiotherapiewetenschap. Tijdschrift voor Hoger Onderwijs & Management (TH&MA), 2007 (1):58‐63
Van Peppen RPS; Harmeling‐van der Wel BC; Kollen BJ; Hobbelen JSM; Buurke JH; Halfens J; Wagenborg L; Vogel MJ; Berns M, Van Klaveren R, Hendriks HJM, Heldoorn M; Van der Wees PhJ; Dekker J; Kwakkel G. Effecten van fysiotherapeutische interventies bij patiënten met een beroerte: een systematisch literatuuronderzoek. Nederlands Tijdschrift voor Fysiotherapie, 2004;114(5):126‐153. This article was awarded with the ‘KNGF Auteursprijs 2006’ for the best original paper of vol. 2005‐2006 in the Dutch Journal of Physical Therapy
Van Peppen RPS; De Bie R. Systematisch meten van evenwicht en loop‐vaardigheid bij patiënten met een CVA. Stimulus, 2003‐4: 300‐315

Publications
232
Bookchapters
Van Peppen RPS; Kwakkel G; Wood‐Dauphinee S; Hendriks HJM; Van der Wees Ph;Dekker J. Einfluss der Physiotherapie auf das funktionelle Outcome nach Schaganfall: Evidenzen. In: Ch. Dettmers,P. Bülau, C. Weiller (editors). Schlaganfall Rehabilitation. ISBN 978‐936817‐20‐1 Hippocampus Verlag. Bad Honnef 2007. Chapter 8, p137‐174
Kwakkel G, Van Peppen RPS, Cup EHC, Kalf JG, Fasotti L. Hoofdstuk 27 Revalidatie na een beroerte 3: Effectiviteit. In: CL Franke, M Limburg (editors). Handboek Cerebrovasculaire aandoeningen. Enschede: De Tijdstroom, 2006: 347‐368
Van Peppen R; Kwakkel G. Welke Klinimetrie is het meest geschikt voor het meten van evenwicht bij een CVA‐patiënt? In: Vaes P (editor). Jaarboek Fysiotherapie‐Kinesitherapie 2002. Houten: Bohn Stafleu Van Loghum, 2002: 59‐85
Kwakkel G; Van Peppen R. De CVA‐patiënt in evenwicht. In: Vaes P (editor). Jaarboek Fysiotherapie‐Kinesitherapie 2002. Houten: Bohn Stafleu Van Loghum, 2002: 45‐58
Books
Beurskens AJHM, Van Peppen RPS, Stutterheim EC, Swinkels RAHM en Wittink H (redactie). Meten in de Praktijk: Stappenplan voor gebruik van meetinstrumenten in de gezondheidszorg. Bohn Scheltema Lochem. Utrecht. In preparation, expected in Summer 2008
- Hoofdstuk 1. Meten met behulp van het stappenplan. Beurskens AJHM, Stutterheim EC, Swinkels RAHM, Van Peppen RPS.
- Hoofdstuk 4. Zoeken naar meetinstrumenten. Swinkels RAHM, Van Peppen RPS, Wolters P.
- Hoofdstuk 6. Klinimetrische eigenschappen van meetinstrumenten. De Vet HCW, Beurskens AJHM, Van Peppen RPS
- Hoofdstuk 8. Interpreteren en rapporteren van meetgegevens. Stutterheim EC, Swinkels RAHM, Van Peppen RPS

Publications
233
Clinical Practice Guidelines
Dutch version:
Van Peppen RPS, Kwakkel G, Harmeling‐van der Wel BC, Kollen BJ, Hobbelen JSM, Buurke JH, Halfens J, Wagenborg L, Vogel MJ, Berns M, Van Klaveren R, Hendriks HJM, Dekker J. KNGF‐richtlijn Beroerte (V‐12/2004), ISSN 1567‐6137. Amersfoort, September 2004
English version:
Van Peppen RPS, Kwakkel G, Harmeling‐van der Wel BC, Kollen BJ, Hobbelen JSM, Buurke JH, Halfens J, Wagenborg L, Vogel MJ, Berns M, Van Klaveren R, Hendriks HJM, Dekker J. KNGF Clinical Practice Guideline for Physical Therapy in Patients with Stroke. Supplement to the Dutch Journal of Physical Therapy. Volume 114 / Issue 5 / 2004. September 2004, English version: April 2008

Publications
234

About the author

About the author
236
About the author Roland (PS) van Peppen was born on March 15, 1961 in Delft, the Netherlands. After completing secondary school (Atheneum) at the ‘Sint Stanislascollege’ in Delft in 1979, he studied between 1979 and 1983 Physiotherapy at the ‘Haagse Academie voor Lichamelijke Opvoeding & Fysiotherapie’ in The Hague. After graduating he worked for 19 years as a physiotherapist in several Dutch rehabilitation centres. The last years he worked mainly patients with stroke, traumatic brain injuries and lower limb amputees. Roland studied Human Movement Sciences at the Maastricht University from 1998 until 2001. After his graduation he worked for two years as a research assistant at the Vrije University medical centre (VUmc) in Amsterdam. In that period he developed the Clinical Practice Guideline on Physiotherapy management in patients with Stroke (CPGPS). In 2004, he started as a lecturer/researcher at the Graduate Programme of Physiotherapy Science at the Utrecht University and also as a lecturer in the Institute for Human Movement Studies, Department of Physiotherapy of the University of Applied Sciences Utrecht. In 2004 he started his PhD‐project in Utrecht where he performed research to evidence‐based physiotherapy for patients with stroke. Currently he is working as senior lecturer, staff member and researcher at the University of Applied Sciences Utrecht. Roland is still living in Delft.


![Chest physiotherapy compared to no chest physiotherapy for ... · [Intervention Review] Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis Cees P van der](https://img.pdfslide.net/doc/110x75/5cc2dd0188c99389538bb642/chest-physiotherapy-compared-to-no-chest-physiotherapy-for-intervention.jpg)