-
7/28/2019 Towner
1/36
Acinetobacteran old friend, but a new enemy
Kevin Towner
Nottingham University Hospitals NHS Trust
-
7/28/2019 Towner
2/36
-
7/28/2019 Towner
3/36
-
7/28/2019 Towner
4/36
-
7/28/2019 Towner
5/36
The genusAcinetobacter
Non-motile Gram-negative coccobacilli Catalase-positive
Oxidase-negative Non-fermentative
Non-fastidious strict aerobes
-
7/28/2019 Towner
6/36
Habitats
Environmentsoil, water, sewage
Foodstuffs (as spoilage organisms)milk products, meat, poultry,
fish
Human skin (25-70% of individuals) Infections in hospitalised
patients
-
7/28/2019 Towner
7/36
Members of the genusAcinetobacterare nowrecognised as
significant nosocomial
pathogens
Critically-ill patients, particularly those
requiring mechanical ventilation in ICUs
Wound infections (trauma patients)
Community-acquired infections (usually in
patients with co-morbidities, with most
reports from tropical or sub-tropical areas)
-
7/28/2019 Towner
8/36
WhichAcinetobacter?
Modern molecular-based taxonomyrecognises at least 33 different
genomic
groups
18 of these have species names
A further 28 groups have been identified
that contain multiple strains, and there are atleast 21
ungrouped single strains
-
7/28/2019 Towner
9/36
Three major overlapping populations
Hospitals and hospitalised patientsmultiresistant isolates
A. baumannii, sp.3, sp.13TU
(theA. baumannii complex)particularly adapted to this
environment?
Skin (humans and animals) / foodstuffs
sensitive isolatesA. johnsonii, A. lwoffii, A.
radioresistens
Soil / environment / wastewaters
sensitive isolatesA. calcoaceticus, A. johnsonii
Natural habitats of other species still poorly defined
-
7/28/2019 Towner
10/36
Acinetobacter baumannii common misconceptions
A. baumannii is an aerobic, Gram-negative coccobacillus that is
highly prevalent innature. These organisms are usually commensal,
but they are emerging as importantopportunistic pathogens. (Villers
et al., Ann Intern Med1998)
A. baumannii is a non-fermenting, Gram-negative, aerobic
coccobacillus foundextensively in natural environments that has
assumed an increasing importance innosocomial infections.
(Garnacho-Montero et al., Clin Infect Dis 2003)
A. baumannii, an aerobic Gram-negative coccobacillus, is
ubiquitous in fresh waterand soil. It is a frequent skin and
oropharyngeal commensal. (Chen et al., Chest
2005) A. baumannii is a species of non-fermentative
Gram-negative bacteria commonly
found in water and soil. This organism was susceptible to most
antibiotics in the1970s. (Fournieret al., PLoSGenetics 2006)
A. baumannii is ubiquitous in nature and has been recovered from
soil, water,animals, and humans.Acinetobacterspecies are normal
inhabitants of human skin.For this reason, it has been suggested
that human skin could be the source of severeinfections. (Fournier
and Richet, Clin Infect Dis 2006)
slide courtesy of H. Seifert
-
7/28/2019 Towner
11/36
Epidemiology ofAcinetobacter - the truth (?)
A. non-baumannii:
water, soil, plants, vegetables, human skin
A. baumannii is not a ubiquitous organism
Hospital environmental sources during outbreaks equipment,
beds, respiratory tubing, computer keyboards, cellphones
Patients
Natural habitat (if any) remains to be defined
slide courtesy of H. Seifert
-
7/28/2019 Towner
12/36
Problems in the hospital setting caused
byA. baumannii Persistence
resistant to drying and disinfectants Antibiotic resistance
increasing proportion of isolates aremultiresistant (including
carbapenems
24% in 2007 in the UK, compared
with
-
7/28/2019 Towner
13/36
0 5 10 15 20 25 30 35 40 45
A. baumani i
E. col i
Enterococcus
Acinetobacter spp.
A. baumannii
S. aureus
BSA
Water[days]
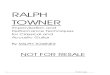
Survival strategies ofA. baumannii
long-term survival on dry surfaces
29 days
J awad et al. J CM 1996; 34:2881-87; J awad et al. J CM 1998;
36:1938-41
-
7/28/2019 Towner
14/36
Where is the reservoir for nosocomial
infection withAcinetobacter baumannii ?
Patients admitted from the community?
Patients admitted from other hospitals?
Within the hospital itself?
-
7/28/2019 Towner
15/36
Potential hospital sources
Hands of staff
Ventilators
Humidifiers
Oxygen analysers
Respirometers Bronchoscopes
Lotion dispensers
Bed frames
Rubbish bins
Sinks
Air supply
Jugs
Bowls
Soap
Hand cream Plastic screens
Bed linen
Service ducts /dust
Bedside charts
Patients
-
7/28/2019 Towner
16/36
Common source outbreaks of A. baumannii
examples
Patients mattresses (Sherertz et al., JID 1985)
Humidifiers (Gervich & Grout, AJIC 1985)
Resuscitation bags (Hartstein et. al., AJM 1988)
Ventilator tubing (Cefai et al., JHI 1990)
Gloves (Patterson et al., AJM 1991) Pillows (Weernink et al.,
JHI 1995)
Computer keyboards (Neely et al., CID 1999)
Blood pressure cuffs (Bureau-Chalot et al., JHI 2004) Cell
phones (Borer et al., EID 2005)
Parenteral nutrition solution (De Vegas et al., ICHE 2006)
-
7/28/2019 Towner
17/36
Epidemiology of A. baumannii
Transmission from a common source
Airborne transmission
Patient-to-patient transmission
Hands of hospital personnel
Contamination of environmental surfaces
Contamination of medical equipment
Colonised patient is the primary reservoir
-
7/28/2019 Towner
18/36
Normal infection control procedures
Identify whether cross-infection or common-source infection
Review policies and procedures related to patient care
Epidemiological survey and surveillance cultures; epi typing
Contact isolation, cohorting of patients (and nurses)
Enforce strict hand disinfection
Environmental disinfection of patient rooms and surfaces
Restrict antibiotic use
Conventional infection control measures are unable to halt
transmission ofA. baumannii
-
7/28/2019 Towner
19/36
Patients screened 3x/week 2x/week environmental screening
identified reservoirs such as phones and
computers
Full gown/gloves worn for all interaction with MRAB patients
Isolation/cohorting of MRAB patients
Repeated deep cleaning of whole ICU until environmental
clearance Deep/internal cleaning of all equipment (e.g.
ventilators, mattresses etc) Restricted access to ICU
Daily Infection Control ward round Register of cases kept
previous patients isolated on readmission
Enhanced measures to eliminateA. baumannii
from an ICU in London, UK (1)
-
7/28/2019 Towner
20/36
Major elective surgical cases delayed or transferred to other
hospitals
6 beds closed; 2 beds closed long term Gown/gloves adopted for
contact with any bed area or equipment
Clear distinction between clean and dirty areas
Results:No new case of MRAB in ICU since 6th June 2005.
The cost of the first six months of this episode: 1.1 million
Euro Conclusion: It is still possible to eradicate MRAB from an
ICU
when an uncompromising approach is taken to infection
control
Enhanced measures to eliminateA. baumannii
from an ICU in London, UK (2)
-
7/28/2019 Towner
21/36
Factors facilitating the spread of A.baumannii
Increased length of hospital stay
Prior antibiotics
Mechanical ventilation
Exposure to patients colonised withA.baumannii
Environmental contamination
Understaffing
Poor adherence of staff to hand hygiene
Once endemic,A. baumannii is
difficult to eradicate
-
7/28/2019 Towner
22/36
Ward closure to combatA. baumanniioutbreaks
Idzenga et al., J Hosp Infect 2006, NL
Kraniotaki et al, IJ AA 2006, GR, 2 weeks Longo et al., J Hosp
Infect 2006, IT, 3 weeks
Carbonneet al
., J Hosp Infect 2005, FR, 4 weeks Pimentel et al., J Hosp
Infect 2005, AUS 4 days
Bernards et al., ICHE 2004, NL
De J ong et al., J Hosp Infect 2004, SA
Denton et al. J Hosp Infect. 2004, UK, 8 days
Maragakis et al., J AMA 2004, USA, 4 weeks
-
7/28/2019 Towner
23/36
In a potential outbreak situation:-
Most important source is already colonisedor infected
patients
In a non-outbreak (sporadic) situation:-
Survives or is introduced?
-
7/28/2019 Towner
24/36
Global epidemiology of individualA. baumannii
strains Multiple hospital outbreak within a city
New York (Landmanet al
., ArchIM 2002)
London (Turton et al., J HI 2004)
J ohannesburg (Marais et al., AJ IC 2004)
Multiple city outbreaks within a country
Czech Republic (Nemec et al., J MM 2004)
Southeast England (Coelho et al., J CM 2004)
France (Naas et al., EID 2006)
Outbreaks from hospitals in several countries in Europe
van Dessel et al., Res Microbiol 2004
Seifert et al., J CM 2005
-
7/28/2019 Towner
25/36
Developing epidemiology ofA.
baumannii in the UK
A survey in 1999-2001 identified 34 different genotypes in46 UK
hospitals
These were shown to belong to 10 different clusters
In general, particular strains were characteristic of
particular hospitals
(J Clin Microbiol 42: 832-834)
-
7/28/2019 Towner
26/36
Between 2003 and 2006, two carbapenem-
resistantA. baumannii lineages (SE cloneand OXA-23 clone) became
prevalent inover 40 hospitals each; susceptible only tocolistin and
tigecycline (J Clin Microbiol44: 3623-3627)
More recently, a further lineage (theNorthwest strain) has
become prevalent inseveral hospitals in the northern/midlands ofthe
UK
-
7/28/2019 Towner
27/36
Are specific carbapenem-resistant clones
spreading in European hospitals?
As part of the EU ARPAC project, 169 hospitals
in 32 countries provided data concerning
multiresistant isolates ofAcinetobacterspp. 130 reported
encountering carbapenem-resistant
isolates ofAcinetobacter, ranging from rare
sporadic isolates to an endemic/epidemic situation(Clin
Microbiol Infect2008; 14: 161-167)
-
7/28/2019 Towner
28/36
Diverse clusters identified by RAPD,
PFGE and PCR-based sequence typing
in European hospitals
Three major European lineages
As in the UK, multiple isolates from asingle hospital generally
belong to the
same clone (some exceptions)
-
7/28/2019 Towner
29/36
Acinetobacter baumannii has become a major cause
of hospital-acquired infections because of itsremarkable ability
to survive and spread in the
hospital environment and to rapidly acquire
resistance determinants to a wide range ofantibacterial
agents
Are we seeing worldwide spread of multiresistantlineages
selected primarily on the basis of theresistance genes that they
carry?
Or is there something special about certainlineages that confers
epidemic potential?
Wh i i
-
7/28/2019 Towner
30/36
What treatment options remain
for multidrug-resistant strains? Polymyxin (colistin) (possibly
in combinations)
Sulbactam combinations
Rifampicin/amikacin combinations
Tigecycline (possibly in combinations)
New siderophore monobactam (BAL30072)
Synthetic peptides (in development)
Phage therapy
(may be useful in individual patients, but resistance has
already appeared tothese options)
-
7/28/2019 Towner
31/36
Whats the problem with
Acinetobacter?
Epidemic spread of multidrug-resistant strainsamong patients in
hospitals, particularly in ICUs
Patients disseminate large numbers of organisms
into their environment Survival on numerous surfaces and
inanimate
objects
Resistant to drying, disinfectants and antibiotics
Difficult to eradicate
-
7/28/2019 Towner
32/36
Control is still possible!
1. Do you have a problem ?
Determine the base line
Compare with other hospitals
2. If the answer is yes
Identify and type isolates
Trace and isolate patients
Re-emphasise andenhance hygieneand infection control
procedures
Review antibiotic policy
Clean the Unit
-
7/28/2019 Towner
33/36
More detailed guidance available on the HPA
website (www.hpa.org.uk)
Contact isolation precautions Risk factors for colonisation or
infection
Antibiotic prescribing policies
Patient transfer procedures (internal and external)
Use of dedicated equipment
Screening strategies Cleaning and decontamination procedures
-
7/28/2019 Towner
34/36
So what else is special about
Acinetobacter?
Perhaps by accident, it has evolved a range of its
own special resistance genes (particularly
carbapenemases) and the capacity to over-express
them in response to antibiotic challenge It has evolved
molecular mechanisms to capture
resistance genes from other organisms
A range of expression mechanisms (provision of
promoters on insertion sequences) enables
foreign resistance genes to be expressed
-
7/28/2019 Towner
35/36
Acinetobacter the Gram-negative MRSA?
it infects the ill it is multi-drug resistant
it prolongs hospitalisation it causes outbreaks
it persists
its an EXPENSIVE pathogen!
-
7/28/2019 Towner
36/36
Coming soon to a
hospital near you!