Embed Size (px)
Citation preview

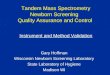
PPV (%): 70.4 75.2 82.2 73.8 85.4 77.3
Traditional and Instrument-Based Vision Screening in Third-Grade Students
Evan Silverstein, MD; Elaine R. McElhinny, MD Department of Ophthalmology Virginia Commonwealth University, Richmond, VA
References: 1 Sean P. Donahue, Brian Arthur, Daniel E. Neely, Robert W. Arnold, David Silbert, James B. Ruben, Guidelines for automated preschool vision screening: A 10-year, evidence-based update. JAAPOS 2013;17:4-8.2 April A. Salcido, Joel Bradley, Sean P. Donahue. Predictive Value of Photoscreening and Traditional Screening of Preschool Children. JAAPOS;9:114-120.
Introduction: AAPOS recommends optotype-based vision screening for children>5 years old.1 Instrument-based screening for 3-4 year olds are more time-efficientand have higher positive predictive value than traditional optotype screening.2 Thisstudy evaluates instrument-based vision screening and traditional screening forthird-grade students.
Methods: Third-graders from 16 schools in a single county in Virginia werescreened by traditional methods (optotypes and stereoacuity) and Plusoptix S12.Children referred from either method received a comprehensive eye examinationwith cycloplegic refraction in the schools (MD/OD). Time to screen was recorded.
Conclusion: Instrument-based vision screening is more time efficient thantraditional screening and has a similar PPV in third-grade students. Input fromteachers to identify struggling students may be helpful if students are screenedsolely with autorefractors or photoscreeners.
169 169
229118
0
100
200
300
400
500
600
Total Referred
87 87
9854
0
20
40
60
80
100
120
140
160
180
200
Examinations
74 74
5732
< 20/30 VA
80 80
7224
Glasses Prescribed
82 82
7627
Intervention*
22 2220 4
Amblyopia
*glasses or referral for more in-depth exam
Results: Screened: 1593 children. Referred: 516(32.4%). Examined: 247(47.9%).
Discussion: The Plusoptix has similar PPV to traditional vision screening anddetects children with acceptable visual acuity but may have a need for glasses.Children with non-refractive decreased visual acuity may be missed by instrument-based screens.
Time to screen (average)
Plusoptix 30 seconds
Traditional 120 seconds Traditional Only Plusoptix Only
Total 54 98
Intervention* 27 (50%) 75 (76.5%)
Non-refractive 8+ 2
Prescribed Rx 4 16
Characteristics of children with examinations that are referred by only one method.
+ visual acuity ranged 20/50 – 20/100 after manifest refraction
No statistical significance between PPVs.
P < 0.01