Embed Size (px)
Citation preview
Traditional mismanagement Traditional mismanagement of labour – of labour –
What can we do?What can we do?Dan Farine MD
Professor of Ob/Gyn & Medicine
Head of Maternal Fetal Medicine
University of Toronto
The issues in L&D
• Fetal distress - <2% of labours
• Non progressive labour and Oxytocin use – 40-50%
• Increased CS rate –mainly for failure to progress
Labor monitors
• Fetal distress (<2%)– Fetal heart rate (mid 20th century)– Scalp pH (mid 20th century)– Fetal ECG -STAN (late 20th century)– Pulse Oximetry (late 20th century)
• Labour progress (30-50%)– Fingers (17th century)
Current assessment of Current assessment of DilatationDilatation
Inter-observer variability
- Up to 6 cm (Bergsjo 1982)
- Average 1-2 cm (Phelps 1995)
Stretching during examination?
Contraction effect?
Current assessment of labor Current assessment of labor progress - Positionprogress - Position
Misdiagnosed position in 61% (defined as +
45 degrees) Sherer et al. 2001
Misdiagnosed 46% of occipito posterior/
transverse – Prior to forceps.
Potential misapplication in 25%
Akmal & Nicolaides 2003
Current assessment of labor Current assessment of labor progress - Stationprogress - Station
- Definition of station checked with 243 care givers
in 4 Denver Units
- Four different definitions were provided
- Care givers were not aware of other care givers
different definition
Carollo et al. 2004
Current assessment of labor Current assessment of labor progress - Stationprogress - Station
- Simulator used to assess station
- Wrong station:
Residents 50-88% Staff: 36-80%
- Wrong level (high, mid…) – 30% vs. 34%
Dupuis et al. 2004
Attempts to overcome these Attempts to overcome these limitationslimitations
• Cervicometry - Friedman, Zador,
Wladimirof etc.
• Data on contractions (Toko, pressure)
• Surrogate parameters (compliance,
distensibility etc.)
Results of the limitations of Results of the limitations of our fingersour fingers
• PTL - diagnosed (too) late• Latent phase - retrospective diagnosis• Active phase – Start? End?
– examinations q 1-4 hours (20-120 contractions)
– Dystocia is not suspected/diagnosed for this interval
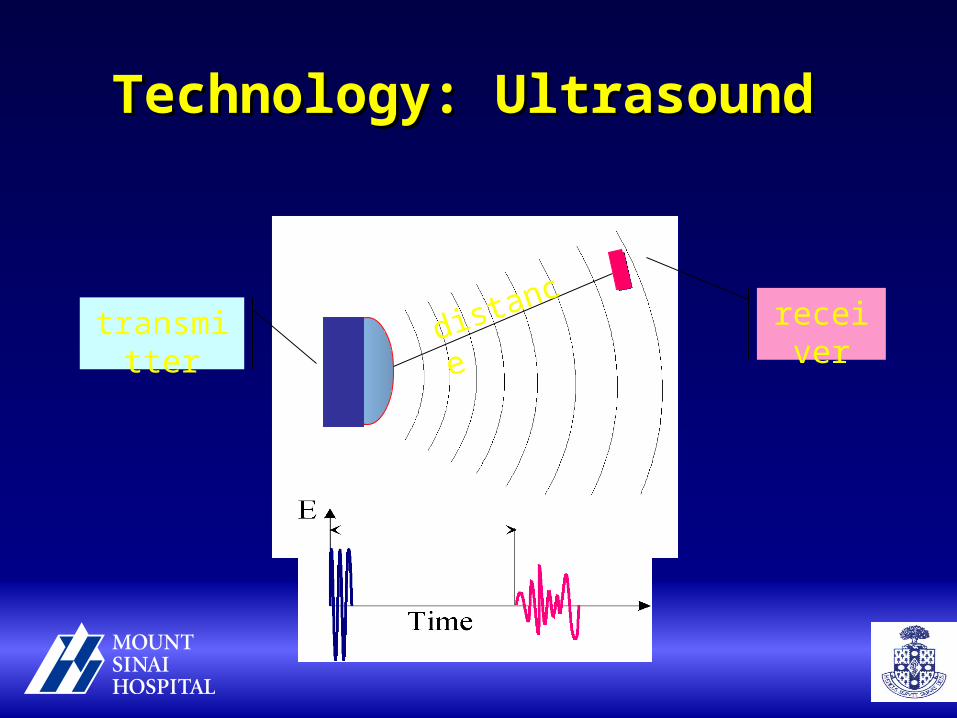
Technology: Ultrasound Technology: Ultrasound
transmitter receiverdistance
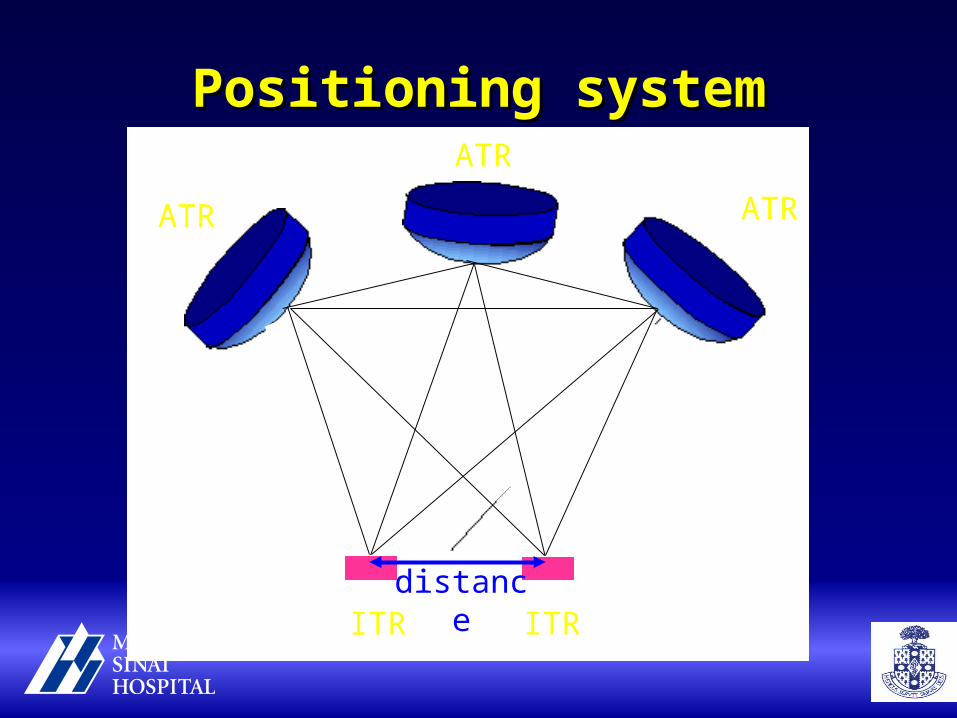
Positioning systemPositioning system
ATR ATR
ITR
ATR
ITRdistance
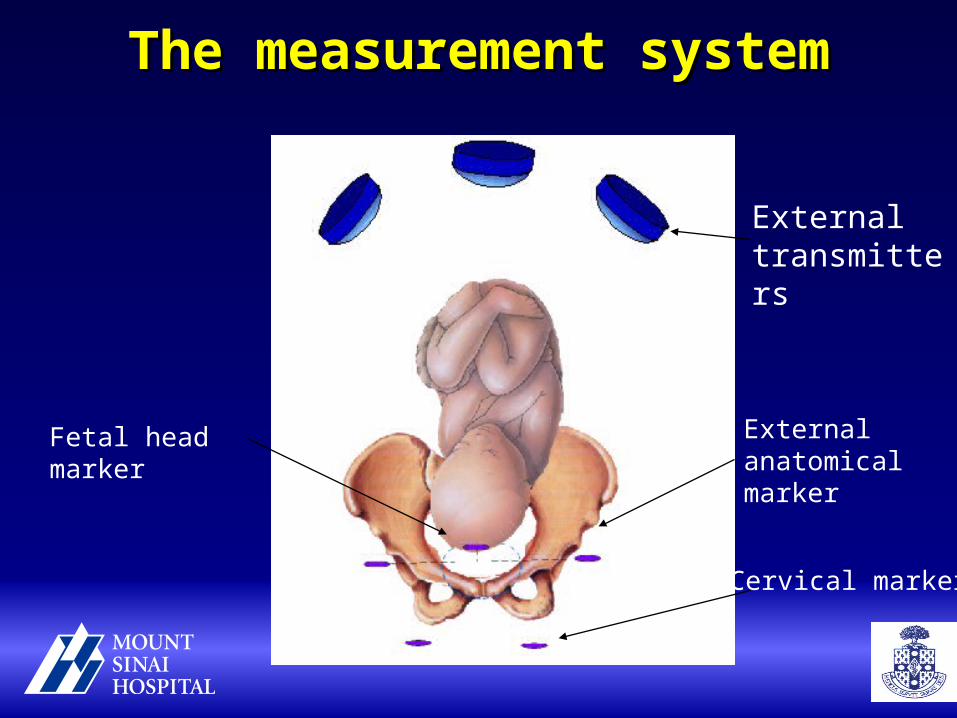
The measurement systemThe measurement system
External transmitters
External anatomical marker
Fetal head marker
Cervical markers
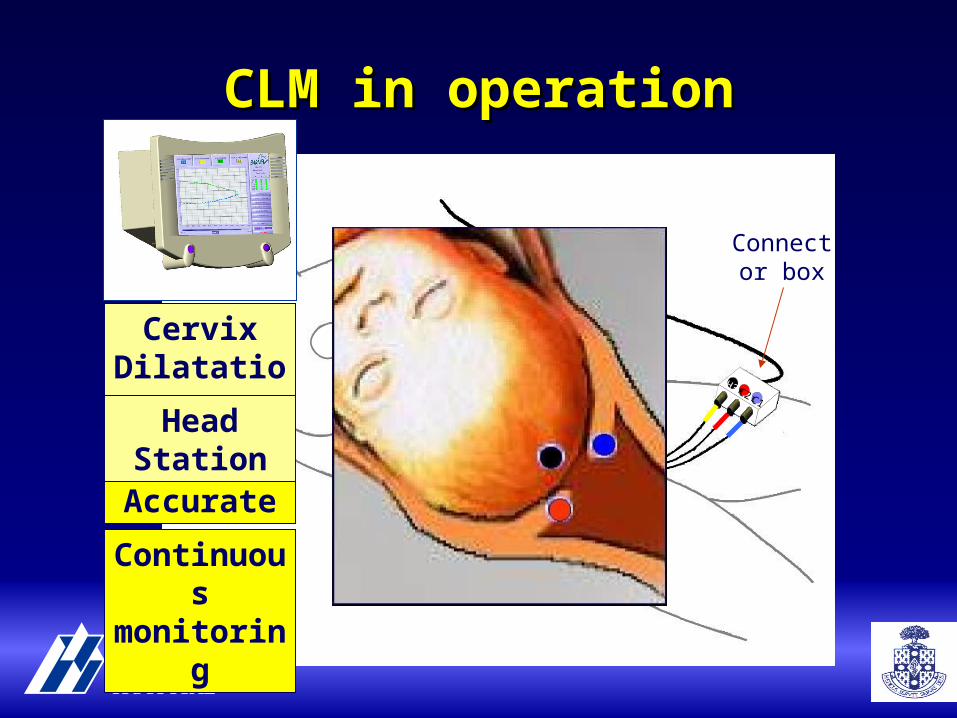
CLM in operationCLM in operation
LC1
H3 RC2
ATRs
Connector box
ITRs
Safe
Accurate
Continuousmonitoring
Cervix Dilatation
Head Station
System advantages
• Add-on system – (as opposed to stand alone)
• Compatible with GE and Phillips
• Data display and collections at all levels– Monitor, central system, internet
Results of clinical trialsResults of clinical trials
• Safety – >600 attachments– 1 laceration, 1 single stitch
• Accuracy – 1-3 mm
• Displacement – Rare (mainly exams)
• Satisfaction – Good (both patients and MDs)
Benefits of cervicometryBenefits of cervicometry• Accurate data
• eliminates inter and intra-observer variability
• Real time data - • Eliminates delays in diagnosis & therapy• Detection of precipitous labors
• Documentation• Reduces number of vaginal examinations
• Patient satisfaction/control• infections• Emergency effect
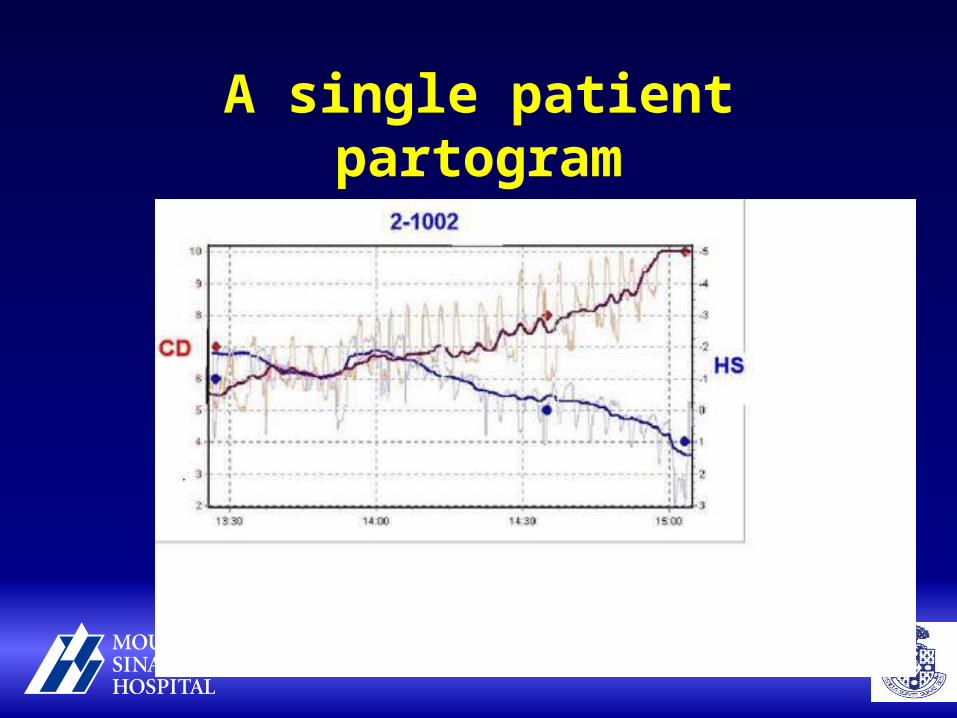
A single patient partogram
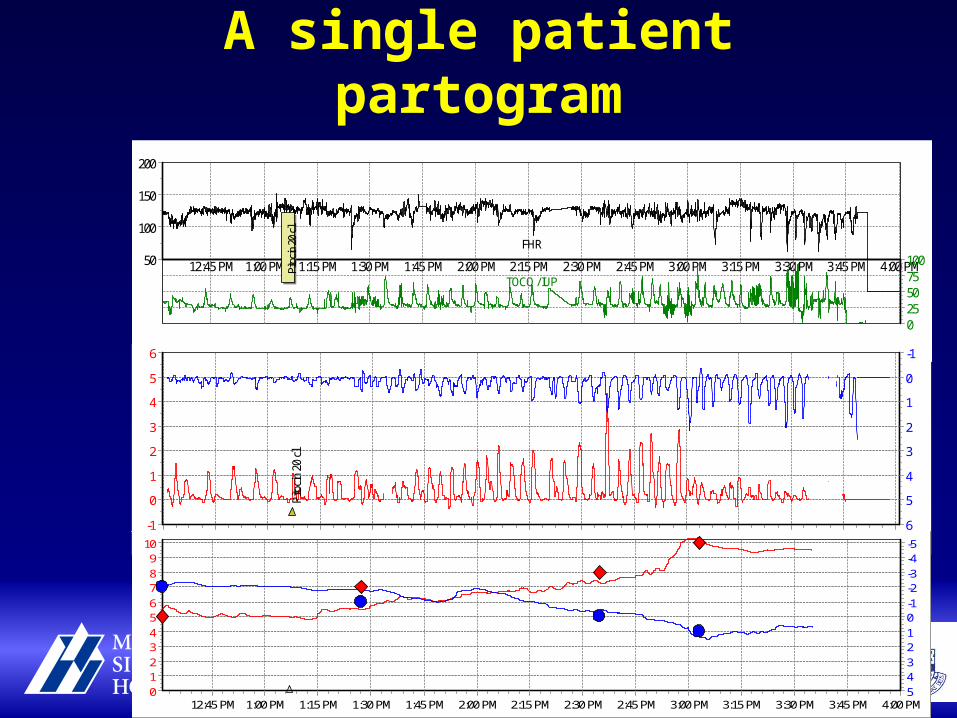
A single patient partogram
TOCO / IUP4:00 PM3:45 PM3:30 PM3:15 PM3:00 PM2:45 PM2:30 PM2:15 PM2:00 PM1:45 PM1:30 PM1:15 PM1:00 PM12:45 PM
FHR
200
150
100
50 1007550250
Pito
cin
20 c
l
4:00 PM3:45 PM3:30 PM3:15 PM3:00 PM2:45 PM2:30 PM2:15 PM2:00 PM1:45 PM1:30 PM1:15 PM1:00 PM12:45 PM12:30 PM
6
5
4
3
2
1
0
-1 6
5
4
3
2
1
0
-1
Pito
cin
20 c
l
4:00 PM3:45 PM3:30 PM3:15 PM3:00 PM2:45 PM2:30 PM2:15 PM2:00 PM1:45 PM1:30 PM1:15 PM1:00 PM12:45 PM
109876543210 5
43210-1-2-3-4-5
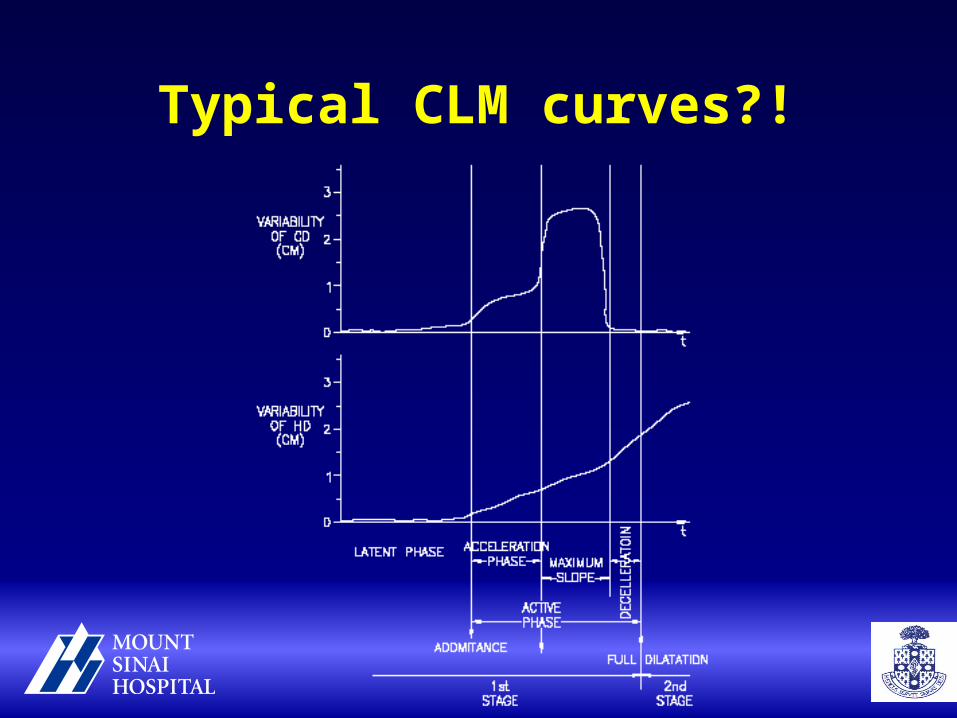
Typical CLM curves?!
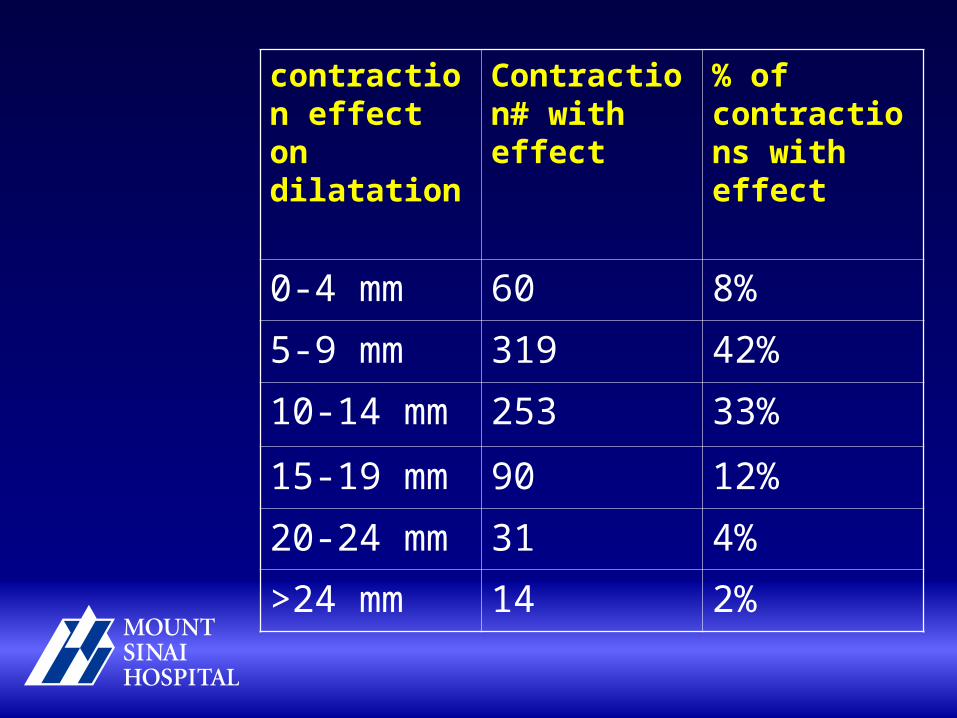
contraction effect on dilatation
Contraction# with effect
% of contractions with effect
0-4 mm 60 8%
5-9 mm 319 42%
10-14 mm 253 33%
15-19 mm 90 12%
20-24 mm 31 4%
>24 mm 14 2%
When does the active phase start?
• Van Dessel – “Reaction point”
The cervix started to oscillate around 4-5 cm
• Cervicometry?
Could we predict CPD?
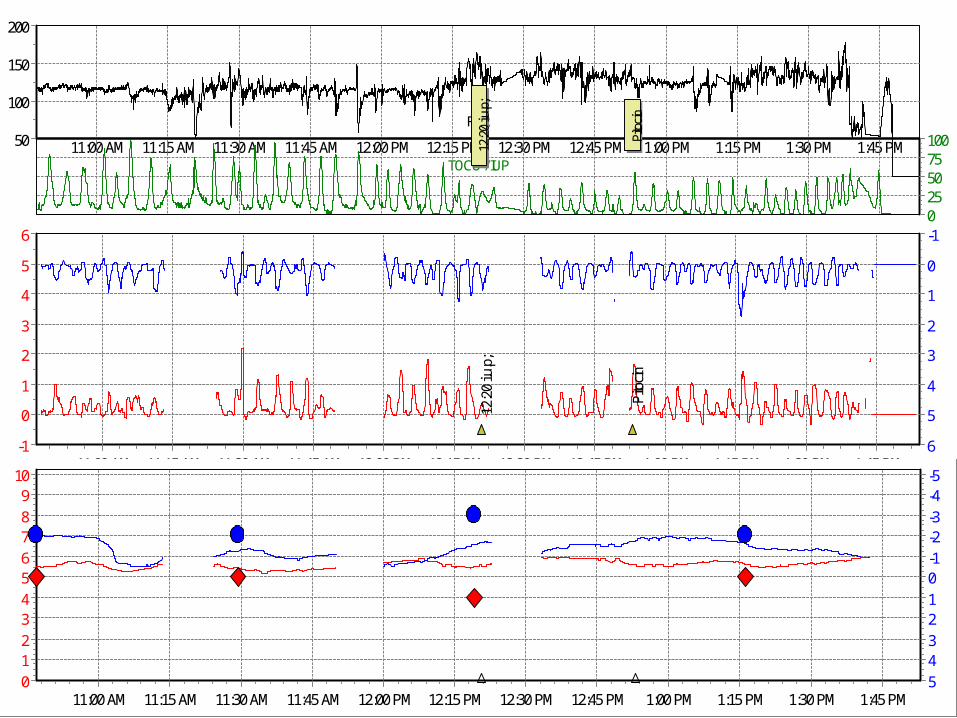
TOCO / IUP1:45 PM1:30 PM1:15 PM1:00 PM12:45 PM12:30 PM12:15 PM12:00 PM11:45 AM11:30 AM11:15 AM11:00 AM
FHR
200
150
100
50 1007550250
12:
20 i.
u.p;
Pito
cin
1:45 PM1:30 PM1:15 PM1:00 PM12:45 PM12:30 PM12:15 PM12:00 PM11:45 AM11:30 AM11:15 AM11:00 AM
6
5
4
3
2
1
0
-1 6
5
4
3
2
1
0
-1
12:
20 i.
u.p;
Pito
cin
1:45 PM1:30 PM1:15 PM1:00 PM12:45 PM12:30 PM12:15 PM12:00 PM11:45 AM11:30 AM11:15 AM11:00 AM
109876543210 5
43210-1-2-3-4-5
The future?
• Early detection of labor abnormalities
• Oxytocin administration based on “mini-partogram”
• Improved outcome (CS, infections, satisfaction)
• Costs (shorter labor, medico-legal)
CLM provides a systematic approach for individual care
Anything not covered?