Embed Size (px)
Citation preview

The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1467–1472
Contents lists available at ScienceDirect
The Egyptian Journal of Radiology and Nuclear Medicine
journal homepage: www.sciencedirect .com/ locate /e j rnm
Transarterial chemoembolization using drug elutingmicrospheres in refractory colorectal liver metastases with18F-FDG PET/CT follow-up to assess therapeutic response
http://dx.doi.org/10.1016/j.ejrnm.2016.09.0140378-603X/� 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Peer review under responsibility of The Egyptian Society of Radiology andNuclear Medicine.⇑ Corresponding author.
E-mail addresses: [email protected] (M.G. Mansour),[email protected] (S.A. Ali).
Mohamed G. Mansour, MD ⇑, Susan A. Ali, MDRadiodiagnosis Department, Ain Shams University, Cairo, Egypt
a r t i c l e i n f o a b s t r a c t
Article history:Received 30 July 2016Accepted 25 September 2016Available online 29 September 2016
Keywords:Colorectal liver metastasesTransarterial chemoembolizationDrug-eluting microspheres
Purpose: The purpose of this study was to evaluate the efficiency of transarterialchemoembolization using drug eluting microspheres loaded with irinotecan in the treat-ment of the colorectal liver metastases after failure of chemotherapy.Patients and methods: This prospective study was conducted from March 2014 to June2016. The patients including 16 men and 6 women (mean age, 55 years) with metastaticcolorectal carcinoma to the liver underwent transarterial chemoembolization using drugeluting microspheres as a salvage therapy after failure of systemic chemotherapy. Eachpatient underwent 18F-FDG PET/CT study before the procedure as well as 2 and 4 monthsafter it to assess the response to therapy.Results: Favorable response was seen in 13 patients (59.1% of patients), progression of thedisease occurred in 3 patients (13.6% of patients) while stationary disease was seen in 5patients (22.7% of patients) and one patient died from brain metastases before the 2months follow-up.Conclusion: Transarterial chemoembolization using drug-eluting microspheres loadedwith irinotecan is a safe and effective salvage treatment of liver metastases from colorectalcarcinoma not responding to systemic chemotherapy.� 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting byElsevier. This is an open access article under the CC BY-NC-ND license (http://creativecom-
mons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Advanced colorectal carcinoma with development ofhepatic metastases leads to poor prognosis unless lesionresection is possible. Unfortunately, about 80% of patientswith hepatic metastases are unsuitable candidates for rad-ical resection and liver metastatic disease is considered aslife limiting for the majority of patients. Systemic
chemotherapy can cause regression of activity, size andnumber of hepatic metastases; yet, local therapy could beused in non responding cases and may be helpful forlong-term survival. Transarterial chemoembolization(TACE) was introduced several years ago (as a local ther-apy) in order to provide high concentration of thechemotherapeutic agent within the lesion. This techniqueleads to stable disease or partial response in 60–75% ofpatients with liver metastases [1–3].
Chemoembolization using drug eluting microspheres(DEM TACE) was developed to prolong the release ofchemotherapeutic agent within the tumor in a prolongedand slow manner. Microspheres (HepaSphereTM Micro-spheres) 30–60 lm are able to absorb chemotherapeutic

1468 M.G. Mansour, S.A. Ali / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1467–1472
agent (Irinotecan). After being mixed with contrast media,microspheres get larger size to 100–200 lm and slowlyrelease the cytotoxic drug. The advantage of DEM TACE isto increase the concentration of chemotherapeutic agentwithin the tumor, with decreased systemic side effectsand toxicity [4,5]. Additionally, the arterial supply of thetumor is embolized by the spheres inducing ischemiceffect [6,7].
PET/CT using 18F-FDG can reveal the metabolic infor-mation of tumor tissues at the molecular level and canbe used to diagnose malignancy with high sensitivity andspecificity. Because changes in tissue metabolism alwaysprecede changes in tissue structure, PET/CT can be usedto assess the early response after TACE treatment and toshow residual, recurring and metastasized lesions by quan-titatively analyzing the changes in the standardized uptakevalue (SUV) of the lesions before and after TACE treatment[8–13].
The aim of this study was to evaluate safety and efficacyof DEM TACE loaded with irinotecan in treatment ofpatients with unresectable colorectal liver metastases afterfailure of systemic chemotherapy, using 18F-FDG PET/CTstudy as a method to assess the therapeutic response.
2. Patients and methods
2.1. Patients
From March 2014 to June 2016, a total of 22 patients(16 males and 6 females) ranging in age from 43 to65 years (mean age, 55 years) with colorectal hepaticmetastases, after unfavorable response to systemicchemotherapy were subjected to transcatheter arterialchemoembolization (TACE) using drug-eluting micro-spheres with irinotecan. The number and size of lesionsare shown in Table 1. The exclusion criteria were as fol-lows: Child-Pugh class B and C patients, poor bleeding pro-
Table 1The number and size of the hepatic lesions in the study population.
Patient number Age Sex Other metastases
1 55 Male Yes2 47 Male No3 62 Male No4 52 Female No5 60 Male No6 57 Male Yes7 53 Female Yes8 43 Male No9 60 Male No10 64 Male No11 47 Female Yes12 50 Female No13 65 Male No14 60 Male Yes15 57 Male No16 52 Male No17 58 Female No18 60 Female Yes19 49 Male No20 53 Male No21 48 Male Yes22 59 Male No
file, main portal vein thrombosis and renal impairment.Each patient underwent 18F-FDG PET/CT study before theprocedure as well as 2 and 4 months after it, to assessthe response to therapy.
2.2. DEM TACE technique
Under strict sterile conditions, right femoral arteryapproach was used as an access for catheterization of thehepatic and superior mesenteric arteries as well as left gas-tric arteries to identify the tumor arterial blood supply. A 5or 4-French polyethylene catheter with a cobra head con-figuration was used. The DEM TACE procedure was per-formed using one vial of Hepasphere of size 30–60 lm(HepaSphere�, Merit medical, Utah, USA) loading 100 mgof irinotecan. The prepared syringes were left for aboutone hour to allow the microspheres to absorb the irinote-can. Before embolization excessive fluid was removed fromsyringes, the mixture was added to 10 cc of non ionic con-trast media (Omnipaque 350).
A lobar approach was used in most of the cases and in 9cases a microcatheter (Renegade Hi Flow, Boston Scientific,USA) for superselective catheterization of the feedingbranches. Fourteen patients were subjected to one sessionof chemoembolization and 8 patients with bilobar hepaticmetastasis had another session of intervention one monthlater. After the procedure, analgesics, antibiotics and antie-metic drugs were given.
2.3. PET/CT technique
All patients were examined using a hybrid PET/CT sys-tem (PHILIPS; Ingenuity TF 128 PET/CT scanner, USA), insupine position from base of skull to mid thigh. The tracerused was 18F-FDG which was injected intravenously witha dose of 0.1 mCi/kg adjusted according to patient’s weight.
Number of tumor nodules Size of the largest lesion (mm)
2 454 221 30Multiple (>5) 345 303 65Multiple (>5) 361 551 251 404 533 452 25Multiple (>5) 505 334 453 20Multiple (>5) 55Multiple (>5) 352 404 50Multiple (>5) 34

M.G. Mansour, S.A. Ali / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1467–1472 1469
The patients were asked to fast for 6–8 h before thestudy and their blood glucose value was kept less than160 mg/dl at the time of the tracer injection. The time ofuptake from 18F-FDG injection to onset of emission scanwas about 60 min.
A PET emission scan was performed over several bedpositions (5–7), each with an axial field of view of approxi-mately 15 cm per bed position with an in-plane spatial res-olution of 4 mm. The acquisition time of emission data was2 minperbedposition in timerangebetween13and17 min.
A 128 integrated multi-slice CT machine was used to dothe diagnostic contrast-enhanced CT images immediatelyafter PET scanning, covering the identical transverse fieldof view. Iodinated non ionic contrast agent (Omnipaque350) was administrated IV (100 ml) using an injector, withan injection flow of 5 ml/s just before the beginning of thescan. The parameters of the diagnostic CT scan were as fol-lows: 120 mA, 130 kV, 0.5 s tube rotation time, slice thick-ness 5 mm, 8-mm table feed and 3 mm incrementalreconstruction. All PET, CT and PET/CT images were recon-structed andviewedonPhilipsworkstation,whichprovidedmulti-planar reformatted PET, CT and fused PET/CT imageswith linked cursors as well as 3D maximum intensity pro-jection (MIP) images and PET images in video mode.
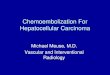
Fig. 1. (a) Axial fused PET/CT image of a 60 years old female patient with multipdigital subtraction angiogram shows faint tumoral blushes (arrows); The patien100 mg of irinotecan. (c) Follow-up axial fused PET/CT image after 4 monthsmetastatic deposits.
2.4. Image analysis
A combined team, including onenuclearmedicinephysi-cian and one radiologist, interpreted the PET, CT and fusedPET/CT images. They were aware of each patient’s historyand clinical data. They recorded the number, size and activ-ity of the hepatic metastatic lesions before and after DEMTACE. The activity of the lesions was detected qualitativelyas well as quantitatively using the Standardized UptakeValue to assess the response to therapy.
3. Results
DEMTACEof the hepatic colorectalmetastaseswas tech-nically successful in all cases with clinical success in about81.8% of patients. One patient died from brain metastasis 6weeks after the procedure. Favorable response (decreasein activity, size or number of the hepatic metastases) waspresent in 13 (59.1%) patients (Figs. 1–3), while stationarydisease was seen in 5 (22.7%) patients. However, progres-sion of the disease occurred in 3 (13.6%) patients.
There were no severe complications after the proce-dure. The main adverse effects were right hypochondrial
le right hepatic lobe metastases from colonic carcinoma. (b) Right hepatict underwent DEM TACE using Hepasphere of size 30–60 lm loaded withshowing favorable response with reduction of size and activity of the

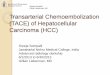
Fig. 2. (a) Axial fused PET/CT image for a 43 years old male patient with a large left lobe hepatic metastatic deposit from rectal carcinoma. (b) and (c)Hepatic angiograms show early and late tumoral stain (arrowed), the patient underwent DEM TACE using Hepasphere loaded with irinotecan. (d) Follow-upaxial fused PET/CT image after 4 months showing regression of the disease with decreased size and activity of the lesion.
1470 M.G. Mansour, S.A. Ali / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1467–1472
pain (96.6%), fever (46.6%), nausea (66.6%), vomiting (20%),minimal ascites (13%) and anorexia (60%). The developedpost procedural ascites was mild and cytological examina-tion of the ascitic fluid revealed absence of malignant cells.The mean time of the procedure was 70 min and allpatients were hospitalized for a day after the procedure.
Unfortunately one patient died before the first follow-up (not included in the post procedural response), andtwo patients died before the second follow-up (70 and133 days after TACE).
4. Discussion
Although the colorectal liver metastases appear hypo-vascular in the post contrast cross sectional examinations,that does not indicate that they are not vascularized. A rel-atively old post-mortem study suggests that liver metas-tases obtain the majority of their nutrition from thehepatic artery [14]. On the basis of the results of variousmulticenter trials, it is well known that the regionalchemotherapy of liver metastases of colon cancer is much

Fig. 3. (a) PET and (b) Fused PET/CT images of a 58 years old female patient with multiple right hepatic lobe and single left lobe active metastases fromcolonic carcinoma (arrows). (c) Right hepatic digital subtraction angiogram with no definite tumoral blush; DEM TACE for the right lobe was done usingHepasphere loaded with 100 mg of irinotecan. (d) Follow-up fused PET/CT image after 2 months showing complete resolution of right lobe lesions. The leftlobe lesion is still noted (arrowed) and the patient later on underwent radiofrequency ablation for that lesion.
M.G. Mansour, S.A. Ali / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1467–1472 1471
superior to the systemic chemotherapy and is accepted asan alternative strategy to control tumor progression [15].However, the proper method of chemotherapeutic drugdelivery is still under investigation [1].
Drug eluting microspheres are widely used for hepato-cellular carcinoma which usually has high vascularity fromthe hepatic arterial branches with significant enhancementin the arterial phase in the triphasic CT examination withsatisfactory results [16].
Jarzabek et al., conducted a study on 15 patients withliver metastases from different primaries (colorectal carci-noma, cholangiocarcinoma, gastrinoma, gallbladder andpancreatic carcinoma, GIST, lung, renal, breast and laryn-geal carcinoma) using HepaSphere 30–60 lm impregnatedwith 100 mg of Doxorubicin with follow-up by post con-trast MRI. Four patients (26.7%) had partial response, fivepatients (33.3%) had stable disease and four patients(26.7%) suffered from metastatic progression. Two patientsdid not report to the follow-up MRI examination. One ofthe tumors which is well responded to the treatment wascolorectal metastasis [1].
Martin RC et al., showed the results of treating unre-sectable colorectal liver metastases refractory to systemictherapy. This study had evaluated 55 patients with pre-DEBIRI (drug eluting beads loaded with irinotecan) andsystemic chemotherapy (FOLFOX + Avastin - 17 patients),(FOLFOX + Avastin and FOLFIRI + Erbitux - 14 patients)and (FOLFOX + Avastin and FOLFIRI + Erbitux and XELOX
+ Vectibex or other - 24 patients). The median treatmentdose of irinotecan was 100 mg (range 100–200 mg). Themedian number of DEBIRI treatment sessions was 2 (range1–5). Complete response was noted in 7 (12%), 7 (12%) and8 (15%) patients 3, 6 and 12 months respectively, partialresponse in 28 (53%), 21 (38%) and 14 (25%) patients 3, 6and 12 months respectively, stable disease in 15 (30%),19 (34%) and 23 (42%) patients 3, 6 and 12 months respec-tively, progression of disease in 3 (5%), 8 (15%) and 10(18%) patients 3, 6 and 12 months respectively, death ofdisease in 0, 5 and 9 patients 3, 6 and 12 months respec-tively and death of other causes in 2, 0 and 0 patients 3,6 and 12 months respectively. The authors found thattreatment using DEBIRI is safe and effective for patientswith metastatic colorectal cancer refractory to multiplelines of systemic therapy [17].
In this study we used the irinotecan, a topoisomeraseinhibitor, which is more specific to the colorectal hepaticmetastases; also the particles selected to be loaded withirinotecan were drug-eluting microspheres (HepaSphere)with good comparable results with the studies usingDEBIRI [18].
Moreover PET/CT, as a follow-up technique, is betterthan triphasic CT alone or MRI as it has both qualitativeand quantitative (SUV) criteria to assess the tumorresponse to therapy. PET/CT is a hybrid imaging technique,which introduces both anatomical and functional informa-tion. This characteristic makes PET/CT the best tool to

1472 M.G. Mansour, S.A. Ali / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1467–1472
assess the post therapy response. Some hepatic metastasesafter DEM TACE get larger in size yet appear totally necro-tic with diminished activity by PET/CT that may give a falseindication of progression (pseudoprogression) in triphasicCT or MRI alone [19].
The difference between HepaSphere and drug elutingbeads is that, the HepaSphere particles are present in adry form in which when hydrated (mixed with thechemotherapeutic agent or contrast media) they get largersize. However both can load the irinotecan and can be usedin TACE procedure for colorectal liver metastases [20].
The main limitations of this study are the small numberof patients and the relatively limited follow-up sessionswhich may be attributed to the high cost of PET/CT. How-ever, we demonstrated that DEM TACE is an effective pro-cedure after failure of systemic chemotherapy in patientswith hepatic colorectal metastases.
5. Conclusion
Transarterial chemoembolization using drug-elutingmicrospheres loaded with irinotecan is a safe and effectivesalvage treatment of liver metastases from colorectal carci-noma not responding to systemic chemotherapy.
Conflict of interest
The authors declared that there is no conflict of interest.
References
[1] Jarzabek M, Jargiełło T, Wolski A, Poluha P, Szczerbo-Trojanowska M.Drug-eluting microspheres transarterial chemoembolization (DEMTACE) in patients with liver metastases. Pol J Radiol 2011;76(3):26–32.
[2] Vogl TJ, Gruber T, Balzer JO, Eichler K, Hammerstingl R, Zangos S.Repeated transarterial chemoembolization in the treatment of livermetastases of colorectal cancer. Radiology 2009;250(1):281–9.
[3] Bower M, Metzger T, Robbins K, Tomalty D, Válek V, Boudny J, et al.Surgical downstaging and neo-adjuvant therapy in metastaticcolorectal carcinoma with irinotecan drug-eluting beads: a multi-institutional study. HPB (Oxford) 2010;12(1):31–6.
[4] Jordan O, Denys A, De Baere T, Boulens N, Doelker E. Comparativestudy of chemoembolization loadable beads: in vitro drug release andphysical properties of DC bead and hepasphere loaded withdoxorubicin and irinotecan. J Vasc Interv Radiol 2010;21(7):1084–90.
[5] Vogl TJ, Zangos S, Eichler K, Yakoub D, Nabil M. Colorectal livermetastases: regional chemotherapy via transarterial
chemoembolization (TACE) and hepatic chemoperfusion: anupdate. Eur Radiol 2007;17(4):1025–34.
[6] Lewis AL, Gonzalez MV, Lloyd AW, Hall B, Tang Y, Willis SL, et al. DCbead: in vitro characterization of a drug-delivery device fortransarterial chemoembolization. J Vasc Interv Radiol 2006;17(2 Pt1):335–42.
[7] Taylor RR, Tang Y, Gonzalez MV, Stratford PW, Lewis AL. Irinotecandrug eluting beads for use in chemoembolization: in vitro andin vivo evaluation of drug release properties. Eur J Pharm Sci 2007;30(1):7–14.
[8] Kim HO, Kim JS, Shin YM, Ryu JS, Lee YS, Lee SG. Evaluation ofmetabolic characteristics and viability of lipiodolized hepatocellularcarcinomas using 18F-FDG PET/CT. J Nucl Med 2010;51:1849–56.
[9] Mocherla B, Kim J, Roayaie S, Kim S, Machac J, Kostakoglu L. FDG PET/CT imaging to rule out extrahepatic metastases before livertransplantation. Clin Nucl Med 2007;32:947–8.
[10] Kim SH, Won KS, Choi BW, Jo I, Zeon SK, Chung WJ, et al. Usefulnessof F-18 FDG PET/CT in the evaluation of early treatment responseafter interventional therapy for hepatocellular carcinoma. Nucl MedMol Imag 2012;46:102–10.
[11] Zhao M, Wu PH, Zeng YX, Zhang FJ, Huang JH, Fan WJ, et al.Evaluating efficacy of transcatheter arterial chemo-embolizationcombined with radiofrequency ablation on patients withhepatocellular carcinoma by 18FDG-PET/CT. Ai Zheng2005;24:1118–23.
[12] Han AR, Gwak GY, Choi MS, Lee JH, Koh KC, Paik SW, et al. Theclinical value of 18F-FDG PET/CT for investigating unexplainedserum AFP elevation following interventional therapy forhepatocellular carcinoma. Hepatogastroenterology 2009;56:1111–6.
[13] Chen YK, Hsieh DS, Liao CS, Bai CH, Su CT, Shen YY, et al. Utility ofFDG-PET for investigating unexplained serum AFP elevation inpatients with suspected hepatocellular carcinoma recurrence.Anticancer Res 2005;25:4719–25.
[14] Taylor I, Bennett R, Sherriff S. The blood supply of colorectal livermetastases. Br J Cancer 1978;38(6):749–56.
[15] Daly JM, Kemeny NE. Chapter 50.2 Treatment of metastatic cancer.In: DeVita VT, Hellman S, Rosenberg SA, editors. Cancer, Principlesand Practice of Oncology, fifth ed., vol. 2. Philadelphia: Lippincott-Raven Publ. Co; 1997. p. 2551–70.
[16] Lencioni R. Loco-regional treatment of hepatocellular carcinoma.Hepatology 2010;52(2):762–73.
[17] Martin RC, Joshi J, Robbins K, Tomalty D, Bosnjakovik P, Derner M,et al. Hepatic intra-arterial injection of drug-eluting bead, irinotecan(DEBIRI) in unresectable colorectal liver metastases refractory tosystemic chemotherapy: results of multi-institutional study. AnnSurg Oncol 2011;18(1):192–8.
[18] Grosso M, Vignali C, Quaretti P, Nicolini A, Melchiorre F, Gallarato G,et al. Transarterial chemoembolization for hepatocellular carcinomawith drug-eluting microspheres: preliminary results from anItalian multicentre study. Cardiovasc Intervent Radiol 2008;31(6):1141–9.
[19] Zaniboni A, Savelli G, Pizzocaro C, Basile P, Massetti V. Positronemission tomography for the response evaluation followingtreatment with chemotherapy in patients affected by colorectalliver metastases. Gastroenterol Res Pract 2015:706808.
[20] Wáng XY, De Baere T, Idée JM, Ballet S. Transcatheter embolizationtherapy in liver cancer: an update of clinical evidences. Chin J CancerRes 2015;27(2):96–121.