Embed Size (px)
Citation preview

TRANSDERMAL PATCH GUIDANCE 3T’s Formulary Transdermal Patch Guidelines
General Guidance Transdermal administration is an alternative, (not necessarily better), method of drug administration. After the application of any patch there is a delay of many hours before therapeutic levels of a drug are reached. Also, after removal of a patch, there is a delay of many hours before circulating levels of a drug drop to a sub‐ therapeutic level, i.e. there is a SLOW ONSET and SLOW OFFSET of analgesia and of side effects. Transdermal patches are considerably more expensive than oral therapy.
Consider using patches only when:
• Difficulty/inability to swallow
• Intractable nausea and vomiting
• Poor absorption from GI tract, (short bowel/inflammatory bowel disease)
• Persistent excessive side effects from oral opiates due to peaks in plasma concentrations
• Compliance problems
• Pain is stable and therefore analgesic requirement is stable
Acute pain is an absolute contra‐indication for the use of the Transdermal Route.
Consider prescribing a course of anti‐emetic for first seven to ten days due to high incidence of nausea and vomiting.
Temperature increase, (fever, bath, shower, heat pad) may increase delivery rate of patches causing toxicity and shortening duration of action of patch.
Buprenorphine is a synthetic opioid agonist/antagonist for use in moderate to severe pain and transdermally is available as two different brands‐‐low strength BuTrans® and high strength Transtec®
Buprenorphine (BuTrans®) patches releasing 5µg/hr, 10µg/hr and 20µg/hr Indications for use: treatment of non‐malignant pain of moderate intensity when an opioid is necessary for obtaining adequate analgesia.
Criteria for use: patients with chronic pain, who have previously received weak opiates, (e.g. Codeine, Dihydrocodeine, Tramadol) and require a topical preparation but do not yet require the level of analgesia provided by morphine or Fentanyl patches.
Butrans® patches contain Buprenorphine in a continuous release formulation to be worn for seven consecutive days. Initiate treatment with the lowest strength patch. Patches must be worn for three days until maximal effect attained. After three days the dose may be increased depending on the patients’ response and the need for current ‘top up’ analgesia; however it is recommended that in most cases the patch be changed after seven days. This is to achieve pain control whilst at the same time minimising opioid side effects. The decision to increase the patch strength should be based on the patients’ need for supplemental pain relief and their analgesic response to patch. The dose should be titrated individually to a level that controls pain with no, or tolerable side effects. A larger patch should replace the current patch or a combination of patches may be worn.
No dose adjustment required for renal impairment or elderly patients but use with caution in patients with hepatic impairment.
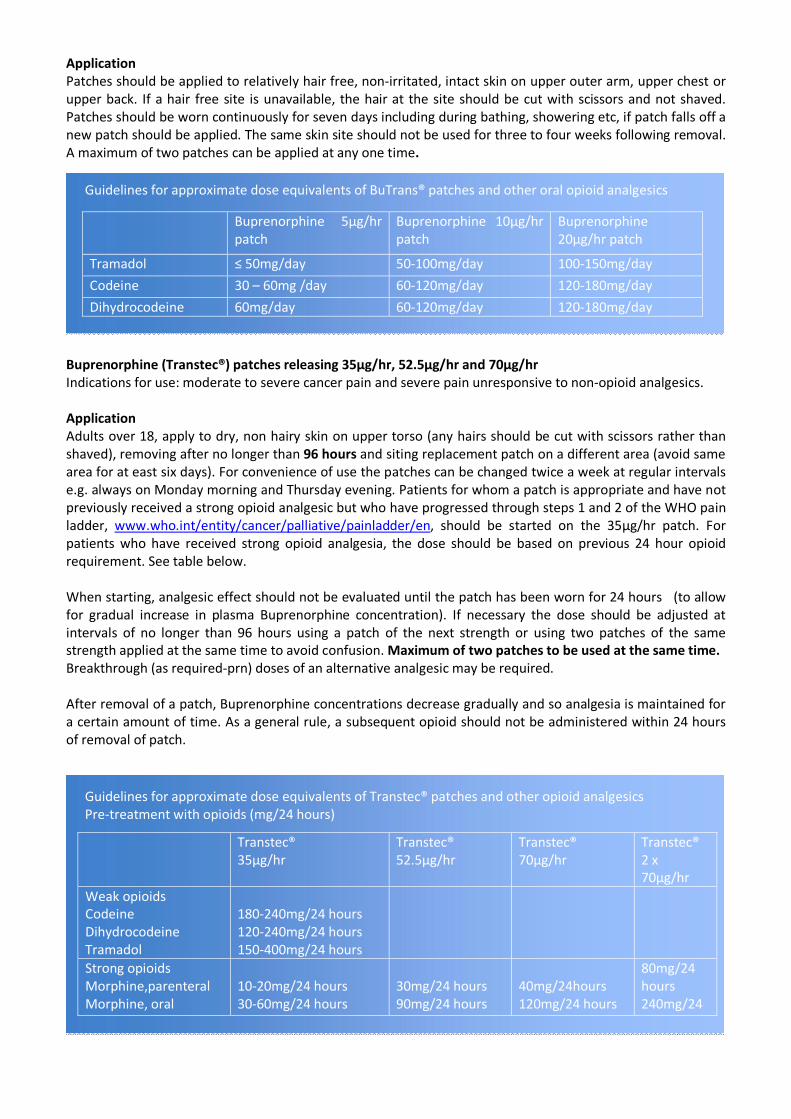
Application Patches should be applied to relatively hair free, non‐irritated, intact skin on upper outer arm, upper chest or upper back. If a hair free site is unavailable, the hair at the site should be cut with scissors and not shaved. Patches should be worn continuously for seven days including during bathing, showering etc, if patch falls off a new patch should be applied. The same skin site should not be used for three to four weeks following removal. A maximum of two patches can be applied at any one time.
Guidelines for approximate dose equivalents of BuTrans® patches and other oral opioid analgesics
Buprenorphine (Transtec®) patches releasing 35µg/hr, 52.5µg/hr and 70µg/hr Indications for use: moderate to severe cancer pain and severe pain unresponsive to non‐opioid analgesics.
Application Adults over 18, apply to dry, non hairy skin on upper torso (any hairs should be cut with scissors rather than shaved), removing after no longer than 96 hours and siting replacement patch on a different area (avoid same area for at east six days). For convenience of use the patches can be changed twice a week at regular intervals e.g. always on Monday morning and Thursday evening. Patients for whom a patch is appropriate and have not previously received a strong opioid analgesic but who have progressed through steps 1 and 2 of the WHO pain ladder, www.who.int/entity/cancer/palliative/painladder/en, should be started on the 35µg/hr patch. For patients who have received strong opioid analgesia, the dose should be based on previous 24 hour opioid requirement. See table below.
When starting, analgesic effect should not be evaluated until the patch has been worn for 24 hours (to allow for gradual increase in plasma Buprenorphine concentration). If necessary the dose should be adjusted at intervals of no longer than 96 hours using a patch of the next strength or using two patches of the same strength applied at the same time to avoid confusion.Maximum of two patches to be used at the same time. Breakthrough (as required‐prn) doses of an alternative analgesic may be required.
After removal of a patch, Buprenorphine concentrations decrease gradually and so analgesia is maintained for a certain amount of time. As a general rule, a subsequent opioid should not be administered within 24 hours of removal of patch.
Guidelines for approximate dose equivalents of Transtec® patches and other opioid analgesics Pre‐treatment with opioids (mg/24 hours)
Buprenorphine 5µg/hr patch
Buprenorphine 10µg/hr patch
Buprenorphine 20µg/hr patch
Tramadol ≤ 50mg/day 50‐100mg/day 100‐150mg/day
Codeine 30 – 60mg /day 60‐120mg/day 120‐180mg/day
Dihydrocodeine 60mg/day 60‐120mg/day 120‐180mg/day
Transtec® 35µg/hr
Transtec® 52.5µg/hr
Transtec® 70µg/hr
Transtec® 2 x 70µg/hr
Weak opioids Codeine Dihydrocodeine Tramadol
180‐240mg/24 hours 120‐240mg/24 hours 150‐400mg/24 hours
Strong opioids Morphine,parenteral Morphine, oral
10‐20mg/24 hours 30‐60mg/24 hours
30mg/24 hours 90mg/24 hours
40mg/24hours 120mg/24 hours
80mg/24 hours 240mg/24
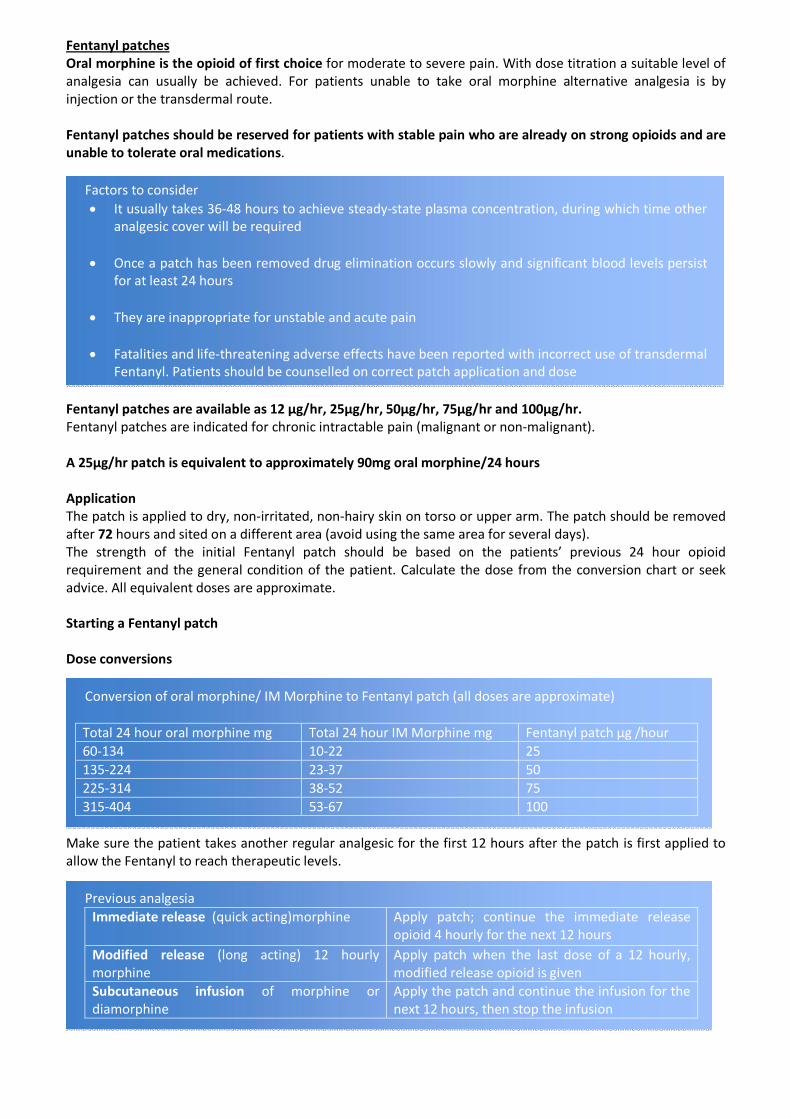
Fentanyl patches Oral morphine is the opioid of first choice for moderate to severe pain. With dose titration a suitable level of analgesia can usually be achieved. For patients unable to take oral morphine alternative analgesia is by injection or the transdermal route.
Fentanyl patches should be reserved for patients with stable pain who are already on strong opioids and are unable to tolerate oral medications.
Factors to consider • It usually takes 36‐48 hours to achieve steady‐state plasma concentration, during which time other
analgesic cover will be required
• Once a patch has been removed drug elimination occurs slowly and significant blood levels persist for at least 24 hours
• They are inappropriate for unstable and acute pain
• Fatalities and life‐threatening adverse effects have been reported with incorrect use of transdermal Fentanyl. Patients should be counselled on correct patch application and dose
Fentanyl patches are available as 12 µg/hr, 25µg/hr, 50µg/hr, 75µg/hr and 100µg/hr. Fentanyl patches are indicated for chronic intractable pain (malignant or non‐malignant).
A 25µg/hr patch is equivalent to approximately 90mg oral morphine/24 hours
Application The patch is applied to dry, non‐irritated, non‐hairy skin on torso or upper arm. The patch should be removed after 72 hours and sited on a different area (avoid using the same area for several days). The strength of the initial Fentanyl patch should be based on the patients’ previous 24 hour opioid requirement and the general condition of the patient. Calculate the dose from the conversion chart or seek advice. All equivalent doses are approximate.
Starting a Fentanyl patch
Dose conversions
Conversion of oral morphine/ IM Morphine to Fentanyl patch (all doses are approximate)
Total 24 hour oral morphine mg Total 24 hour IM Morphine mg Fentanyl patch µg /hour 60‐134 10‐22 25 135‐224 23‐37 50 225‐314 38‐52 75 315‐404 53‐67 100
Make sure the patient takes another regular analgesic for the first 12 hours after the patch is first applied to allow the Fentanyl to reach therapeutic levels.
Previous analgesia Immediate release (quick acting)morphine Apply patch; continue the immediate release
opioid 4 hourly for the next 12 hours Modified release (long acting) 12 hourly morphine
Apply patch when the last dose of a 12 hourly, modified release opioid is given
Subcutaneous infusion of morphine or diamorphine
Apply the patch and continue the infusion for the next 12 hours, then stop the infusion
An immediate release opioid (e.g. oral morphine or morphine SC) must be available as required for breakthrough pain.
Review the Fentanyl patch dose after 72 hours when drug levels should be at a steady state. If the patient shows signs of opioid toxicity (drowsiness, confusion) reduce the dose and reassess the pain. If the patient still has pain which is opioid responsive, titrate the Fentanyl dose in 12‐25µg/hr increments. It will take 12 ‐24 hours for the new dose to take effect so give breakthrough analgesia as required.
References 1. 7 day Buprenorphine patch for severe chronic pain,www.nelm.nhs.uk 2. Summary of product characteristics – Transtec patches. BuTrans patches. Napp Pharmaceuticals. 3. Accessed via http://emc.medicines.org.uk 4. Guidelines for the use of transdermal opioids, Cambridge and Huntingdon palliative care group,
www.arthurrankhouse.nhs.ukfact sheet 5. 5. Principles of pain control. Cambridge and Huntingdon palliative care group. 6. www.arthurrankhouse.nhs.uk fact sheet 6. 7. Recommendations for the appropriate use of opioids for persistent non‐cancer pain
http://www.britishpainsociety.org/opioids_doc_2004.pdf 8. Dorothy house/Wessex palliative care Handbook,www.dorothyhouse.co.uk 9. Pharmacologic approaches to pain management,www.endlink.lurie.northwestern.edu 10. Equianalgesic doses,www.elmmb.nhs.uk 11. Analgesics chapter 4.7 BNF 58,www.bnf.org
Approved by 3T’s Formulary Working Group: June 2011 Review Date: June 2014 Number of pages: 4
This Guideline has been adapted from the BCAP: Transdermal Patch Guidance, November 2009.





























