Embed Size (px)
Citation preview

Transformation of NSTEMI Care at the Golden
Jubilee National Hospital
Dr M Mitchell Lindsay. MD. FRCP
Acting Associate Medical Director
Consultant Cardiologist
Golden Jubilee National Hospital
Glasgow

Background
i) Coronary angiography and consequent revascularisation in NSTEMI reduces major adverse cardiovascular events (MACE).
ii) The reduction in MACE is most dramatic amongst high risk patients defined by high Grace Score (Grace Score is a clinical risk score which predicts in-patient and 6 month mortality).
iii) Patients presenting with a high risk NSTEMI should undergo angiography and revascularisation within 24hrs of admission to maximise this clinical benefit.
iv) Those presenting with intermediate risk should be treated within 72 hours of admission to maximise clinical benefit.
v) The admission to a hospital with no cardiac cath lab facilities versus a PCI capable hospital results in an average 20hr delay to coronary angiography and subsequent intervention (BCIS audit 2014).

Selection of non-ST-elevation acute coronary syndrome (NSTE-ACS)
treatment strategy and timing according to initial risk stratification.
Marco Roffi et al. Eur Heart J 2016;37:267-
315
© The European Society of Cardiology 2016. All rights reserved. For
permissions please email: [email protected]

TIMACS (Death/MI/Stroke)
N Engl J Med 2009;360:2165-75

Lancet 2017; 390: 737–46

All Cause Mortality
Jobs, Mehta, Montalescot Lancet 2017; 390: 737–46

All Cause Mortality
Jobs, Mehta, Montalescot Lancet 2017; 390: 737–46

BCSI audit 2014

BCSI audit 2014

Dept of Health NHS England10
Best practice tariffs for PCI & Catheterisation in 2017/18
HRG code HRG name
Non-best
practice
tariff (£)
Best
practice
tariff (£)
Difference
(£)% Difference
EY40A Complex Percutaneous Transluminal Coronary Angioplasty with CC Score 12+ 6,719 7,437 718 11%EY40B Complex Percutaneous Transluminal Coronary Angioplasty with CC Score 8-11 4,790 5,303 513 11%EY40C Complex Percutaneous Transluminal Coronary Angioplasty with CC Score 4-7 3,286 3,637 351 11%EY40D Complex Percutaneous Transluminal Coronary Angioplasty with CC Score 0-3 2,580 2,856 276 11%EY41A Standard Percutaneous Transluminal Coronary Angioplasty with CC Score 12+ 6,639 7,349 710 11%EY41B Standard Percutaneous Transluminal Coronary Angioplasty with CC Score 8-11 3,999 4,426 427 11%EY41C Standard Percutaneous Transluminal Coronary Angioplasty with CC Score 4-7 2,857 3,162 305 11%EY41D Standard Percutaneous Transluminal Coronary Angioplasty with CC Score 0-3 2,247 2,487 240 11%EY42A Complex Cardiac Catheterisation with CC Score 7+ 4,490 4,970 480 11%EY42B Complex Cardiac Catheterisation with CC Score 4-6 2,788 3,086 298 11%EY42C Complex Cardiac Catheterisation with CC Score 2-3 2,144 2,373 229 11%EY42D Complex Cardiac Catheterisation with CC Score 0-1 1,732 1,917 185 11%EY43A Standard Cardiac Catheterisation with CC Score 13+ 7,464 8,262 798 11%EY43B Standard Cardiac Catheterisation with CC Score 10-12 5,092 5,637 545 11%EY43C Standard Cardiac Catheterisation with CC Score 7-9 3,838 4,249 411 11%EY43D Standard Cardiac Catheterisation with CC Score 4-6 2,788 3,086 298 11%EY43E Standard Cardiac Catheterisation with CC Score 2-3 2,131 2,359 228 11%EY43F Standard Cardiac Catheterisation with CC Score 0-1 1,648 1,824 176 11%

Timely and evidence based care of
NSTEMI patients cannot be
provided via traditional hub and
spoke model.

Analysis performed by AstraZeneca as part of the Joint Working project between NHS Greater Glasgow and Clyde (GGC), Golden Jubilee National Hospital
(GJNH), GGC Managed Clinical Network and AstraZeneca UK Ltd.
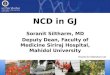
NSTEMI mean time to referral and angiography for spells
transferred directly to the intervention centre
Hospitals with a small number of NSTEMI referrals are not included in this analysis

Cardiovascular Registry Project
99.1% 100.0% 100.0% 100.0% 100.0%
87.0%
49.8%
60.0%
83.3%
54.5%
36.0%
56.5%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Any Pathway
(n=697)
1Direct to GJNH
(n=30)
2Local A&E to GJNH
(n=6)
3Direct Transfer
(n=415)
4Discharged Home
with Referral
(n=200)
6Elective GJNH Only
(n=46)
Pe
rce
nt o
f S
pe
lls i
n t
he
Pa
th
wa
y
Care Pathway
NSTEMI Patients: Percentage of Spells Receiving Angiography and Percentage Receiving PCI By Pathway
Angiography
PCI
N=697
11.2(median=6)
0.6(median=0)
0.3(median=0)
5.0(median=4)
26.0(median=23)
-5.0
0.0
5.0
10.0
15.0
20.0
25.0
30.0
Any Pathway
(n=651)
1Direct to GJNH
(n=30)
2Local A&E to GJNH
(n=6)
3Direct Transfer
(n=415)
4Discharged Home
with Referral
(n=200)
Me
an
Da
ys in
to
An
gio
gra
ph
y
Care Pathway
NSTEMI Patients: Mean Days from Acute Admission to Angiography
(Pathways 1-4)N=651
Analysis performed by AstraZeneca as part of the Joint Working project between NHS Greater Glasgow and Clyde (GGC), Golden Jubilee National
Hospital (GJNH), GGC Managed Clinical Network and AstraZeneca UK Ltd.
http://www.nhsresearchscotland.org. uk/uploads/tinymce/Acute%20Myoca rdial.pdf

NSTEMI Service Re-design
Two stages.
Optimisation of hub and spoke model
Introduction of Direct Admission model for high risk
NSTEMI ( Direct NSTEMI)

Service Re-design( Hub and spoke)
Medical Workforce Model
Consultant of the week
Capacity
Extra beds
Cath Lab Scheduling
Dedicated “hot” cath lab sessions and extended day
working.
Electronic referral.

GJNH experience.

Service pre-August 2016
Traditional hub and spoke. Catchment of 2.2 million.
7 referring hospitals generating circa 3000 NSTEMI angio referrals p.a
Patients presenting to the Emergency Department or the Scottish Ambulance Service with the clinical syndrome of NSTEMI are admitted to their local hospital.
Medical Rx and risk stratification -3 potential treatment paths:
Refer for in patient (IP) coronary Angiography
Refer for urgent OP angiography (patient is discharged and request made for urgent appointment at GJNH)
Medical management, where the patient is discharged when clinically stable.
Dept of National and Regional Medicine GJNH

Direct NSTEMI
Direct referral of high risk NSTEMI;
1. Scottish Ambulance Service.
2. A+E departments.
All patients will have coronary angiography within
24 hours.
Phased introduction.
Early direct discharge or repatriation if required.

Definition- High Risk NSTEMI
Cardiac chest Pain
ECG changes- ST depression or deep symmetrical T
wave inversion.
HEART score greater than 5
1. Backus BE, Six AJ, Kelder JC et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int
J Cardiol 2013;168(3):2153-8

Preparation and planning

Preparation and planning.
Dept of National and Regional Medicine GJNH

Dept of National and Regional Medicine GJNH

Dept of National and Regional Medicine GJNH

Assessment by the SAS
HEART Score: Risk scoring system developed for use
in unselected emergency presentations with chest
pain.
History
ECG
Age
Risk Factors
Troponin
Dept of National and Regional Medicine GJNH

Backus BE, Six AJ, Kelder JC, Mast TP, van den Akker F, Mast EG, Monnink SH, van Tooren RM,
Doevendans PA. Chest pain in the emergency room: a multicenter validation of the HEART Score. Crit Pathw
Cardiol. 2010 Sep: 9(3): 164-169

Outcome
Score > 5 – telemeter 12 lead ECG
contact CCU GJNH
agree care pathway – consider Aspirin, GTN,
Morphine, Metoclopramide.
Dept of National and Regional Medicine GJNH

A+E Referrals/M.A.U
Clinical Assessment
ECG.
Admission HsTn
CXR
Routine bloods.
HEART score.
Re-design of Chest Pain Protocol.
Dept of National and Regional Medicine GJNH

Adapted from GGC Acute Cardiac Pain Pathway
High risk chest pain
Ischaemic ECG changes
(for example 2mm ST depression in 2 adjacent
leads of deep symmetrical T wave inversion)
or ongoing typical cardiac pain
and HEART score >5
REFER GJNH FOR CONSIDERATION OF
DIRECT TRANSFER OF HIGH RISK NSTEMI.
07976 986058
STEMI
(for example ≥2mm ST elevation in 2 consecutive
chest leads
or >1mm in 2 adjacent limb leads
or new LBBB
or >2mm ST depression V1-V3 suggestive of
posterior infarct)
Treat as presumed ACS
Refer to cardiology
Give aspirin 300mg stat
Arrange CXR
Clerk in and write kardex
DO NOT GIVE Ticagrelor or Fondaparinux
unless discussed with cardiology
Treat as STEMI
Call 999 for emergency PCI transfer
Refer GJNH 0141 951 5299
Fax ECG to 0141 951 5867
Aspirin 300mg stat
Ticagrelor 180mg stat
IV Heparin 5000u (if not anticoagulated)
HEART SCORE < 5
History suggests possible cardiac pain
and non-diagnostic ECG
Consider aspirin 300mg stat
Arrange CXR
No other unrelated complaints
and no other acute comorbidities
and pain not pleuritic
and not mainly epigastric or posterior
ECG and troponin within 15 minutes
Patient presents with chest pain to ED/AAU
Nursing assessment in triage
Multiple other complaints
or multiple comorbidities
or pleuritic pain
or pain mainly epigastric or posterior
Chest pain assessment form completed by
medical staff (HEART score)Usual medical management pathways
Troponin 6 hours post-admission (PEAK)
Review baseline troponinConsider aspirin 300mg stat
Arrange CXR

London Experience
BMJ Open 2014;4:e005525doi:10.1136

Reproduced with consent of Dr N Swanson

Fast track NSTEACS toolInclusion. Patients must have:
Symptoms strongly suggesting an acute coronary syndrome – typically chest pain at rest.
High sensitivity troponin result above the 99th percentile upper reference limit
And/or ECG abnormalities suggesting NSTEACS*
And/or conscious post cardiac arrest.
*ECG changes suggestive of an NSTEACS:
ST depression in any leads
T wave inversion in leads V1-V4
Dynamic T wave changes in more than one lead.
Exclusion. Patients should not be considered for Fast Track Pathway with ANY of the following:
ST elevation MI – treat according to existing PPCI pathways
Overt sepsis
Major trauma/surgery within one month.
Acute renal failure eGFR<60.
Hb<100 or recent active bleeding.
O2 saturation <90% on air.
Severe comorbidity – e.g. metastatic cancer, moderate/severe dementia or delirium, exercise
tolerance<100yds normally, frailty of old age, post-arrest ventilated patients. This list is not
exhaustive.
following.
NECVN- Fast track tool
Reproduced with consent of Dr N Swanson

Economic Benefits to the Region
Dept of National and Regional Medicine GJNH

Direct NSTEMI-13 Month Results

Our Commitments
We could identify high risk NSTEMI patients at their
presentation ( A+E or S.A.S)
We could admit this patient directly 24/7
We would undertake Angiography within 24 hrs of
admission
This high risk group would benefit from high rates of
revascularisation.
We would aim for direct discharge/ early
repatriation.
Dept of National and Regional Medicine GJNH

Detractors- numerous
“You can’t expect paramedics or A+E staff to
identify high risk group”
“Your wards will be full of acute abdomens and
broken hips...”
“ They will too sick to cath and have too much co-
rmobidity”
“You won’t be able to get any of them home”

Direct NSTEMI referrals
Dept of National and Regional
Medicine GJNH

DIRECT NSTEMI Patients
715 Patients Referred.
249 Patients accepted for direct admission (35% of
referrals)
Median Age 63 ( range 24-95)
Median HEART Score 7 ( Range 5-10)

Performance indicators.
Angiography 99%
Within 24hr Guarantee 98%
Median Time from Admission to angiography 3
hours 49 mins.

Management
75% revascularisation Rate ( 70% PCI. 5% CABG)
25% Intensive Medical management.

Discharge
26% Discharged directly from GJNH
Median stay 1 day.
Median stay of whole cohort 1 day ( Mean 1.86
days)

Patients Not Accepted
Aug-Nov analysed
93 Patients
Median Age 69 ( range 28-86)
Median Heart Score 6 (range 3-9)
51% subsequently underwent angiography
52 % PCI
35% Medical Rx
12% CABG
Dept of National and Regional Medicine GJNH

Our Commitments
We could identify high risk NSTEMI patients at their
presentation ( A+E or S.A.S)
We could admit this patient directly 24/7
We would undertake Angiography within 24 hrs of
admission
This high risk group would benefit from high rates of
revascularisation.
We would aim for direct discharge/ early
repatriation.
Dept of National and Regional Medicine GJNH

Data collection
Dept of National and Regional Medicine GJNH

Meeting the Challenges of
Current Practice
Benefits of direct NSTEMI service
Clinical
Economic
Widely applicable
Sustainable
#bacpr2017