Embed Size (px)
Citation preview

Transforming Complement TherapeuticsDecember 2019

2
This presentation contains "forward-looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995, including, but not limited to,
statements regarding the safety, efficacy, regulatory and clinical progress, and therapeutic potential of the product candidates of Ra Pharmaceuticals, Inc. (“Ra
Pharma” or “we”), including zilucoplan, the poly(D,L-lactic-co-glycolic acid) (PLGA) and FluidCrystal® (FC) extended release (XR) formulations of zilucoplan, and
an oral small molecule inhibitor of C5, plans and timing for the presentation of clinical data, expectations surrounding the trial design, timeline, and enrollment
of our ongoing and planned clinical programs, including a Phase 3 clinical program evaluating zilucoplan for the treatment of generalized myasthenia gravis
(gMG), a Phase 2 trial of zilucoplan for the treatment of immune-mediated necrotizing myopathy (IMNM), and the Healey Center-led ALS platform trial, our
market opportunities, the anticipated pricing of our product candidates, if approved, including zilucoplan, and management’s estimates about the potential size
and characteristics for the patient populations that our product candidates are targeting and statements regarding the completion and anticipated proceeds of
the proposed offering and the use of the net proceeds of the proposed offering. Zilucoplan is an investigational drug, and the claims, or indications, discussed
are not yet approved by the FDA. All such forward-looking statements are based on management's current expectations of future events and are subject to a
number of risks and uncertainties that could cause actual results to differ materially and adversely from those set forth in or implied by such forward-looking
statements. These risks and uncertainties include the risks that Ra Pharma’s product candidates, including zilucoplan, the PLGA and FC XR formulations of
zilucoplan, and an oral small molecule inhibitor of C5, will not successfully be developed or commercialized, risks related to fluctuations in our stock price, as
well as the other factors discussed in the “Risk Factors” section in Ra Pharma’s most recently filed Annual Report on Form 10-K, as well as other risks detailed in
Ra Pharma’s subsequent filings with the Securities and Exchange Commission. There can be no assurance that the actual results or developments anticipated by
Ra Pharma will be realized or, even if substantially realized, that they will have the expected consequences to, or effects on, Ra Pharma. Except as noted, all
information in this presentation is as of October 2, 2019, and Ra Pharma undertakes no duty to update this information unless required by law.
Forward-Looking Statements

� Focused on delivering innovative and accessible therapies to patients with rare, complement-mediated diseases
� Zilucoplan: A convenient, self-administered, subcutaneous complement C5 inhibitor
� Generalized myasthenia gravis (gMG): Successful Phase 2 study in a broad spectrum of patients with gMG ; Phase 3 clinical trial ongoing
� Immune-mediated necrotizing myopathy (IMNM): Phase 2 clinical trial ongoing
� Amyotrophic lateral sclerosis (ALS): Selected for HEALEY ALS Platform Trial by Sean M. Healey & AMG Center for ALS at Mass General
� Positive Phase 1b trials: Ethno-bridging (Japan) and in patients with renal impairment; Support further development with no need for dose modification
� Advancing a portfolio of investigational C5 inhibitors in pre-clinical development� XR: PLGA and FluidCrystal® (FC) XR formulations of zilucoplan achieved rapid and sustained pharmacodynamic inhibition of complement C5 in
non-human primates, supporting once weekly or less frequent dosing in clinical trials
� SMi: First-in-class oral small molecule C5 inhibitor
� Proprietary drug discovery engine
� Trillion member, highly diverse, synthetic macrocyclic peptide libraries; Diversity and specificity of mAbs with the pharmacologic advantages of small molecules
� Merck Collaboration: Oral peptide targeting a large CV market opportunity
Transforming Complement Therapeutics
3

4
Pipeline Programs
DISCOVERY/
Zilucoplan (gMG)
Oral Macrocyclic PeptideCardiovascular target with a large market opportunity
Orphan Renal Diseases (SC)
Phase 1 trial ongoing
Renal/Autoimmune/CNS Diseases
Phase 3 RAISE trial ongoing
PRE-CLINICAL PHASE 1 PHASE 2
C5 Inhibition
Oral Small Molecule Inhibitor
Zilucoplan Extended Release (XR)
Partnered Program(Non-Complement Target)
Factor D Inhibition
Other Complement Inhibitors
Zilucoplan (ALS)
Phase 2 trial ongoing
PHASE 3
Zilucoplan (renal disorders) Phase 1b trial complete
Zilucoplan (IMNM)
Phase 2/3 HEALEY ALS Platform Trial planned

Renal Disorders: Phase 1b positive
1
FactortargetedbyRaPharmaproductcandidates
Activatedbynon-selfcells Activatedbyantibody-antigencomplexes Activatedbypathogensurfaces
C5a
C3 C1q – C1r – C1s
C7,C8,C9
C5b6
MAC
BindsC5
FactorD,FactorB
eculizumab RA101495
Proinflammatorycytokine
BindsC5&C5b
LectinPathwayClassicalPathwayAlternativePathway
PNH:ruptureofRBC
gMG:destructionofneuromuscularjunction
LN:inflammationofkidneyglomerulus
C5
C2,C3,C4
C5b
C6
1
FactortargetedbyRaPharmaproductcandidates
Activatedbynon-selfcells Activatedbyantibody-antigencomplexes Activatedbypathogensurfaces
C5a
C3 C1q – C1r – C1s
C7,C8,C9
C5b6
MAC
BindsC5
FactorD,FactorB
eculizumab RA101495
Proinflammatorycytokine
BindsC5&C5b
LectinPathwayClassicalPathwayAlternativePathway
PNH:ruptureofRBC
gMG:destructionofneuromuscularjunction
LN:inflammationofkidneyglomerulus
C5
C2,C3,C4
C5b
C6
Activated by non-self cells Activated by antibody-antigen complexes Activated by pathogen surfaces
C5a
C3 C1q – C1r – C1s
C7, C8, C9
C5b6
Membrane attack complex (MAC)
Binds C5, blocks cleavageEculizumab (IV)
Zilucoplan (SC)Binds C5, blocks cleavage;
Blocks MAC assembly
Proinflammatory cytokine
Lectin PathwayClassical PathwayAlternative Pathway
C5
C5b
C6
Factor D, Factor B
5
Zilucoplan: A Self-Administered, Subcutaneous, Macrocyclic Peptide Inhibitor of Complement C5
PNH: Phase 2 positive
gMG: Phase 2 positivePhase 3 ongoing
IMNM: Phase 2 ongoing
Multiple Indications
15 amino-acid cyclic peptide inhibitor of C5
Multiple validated indications, pipeline-in-a-product potential
gMG – generalized myasthenia gravis; IMNM – immune-mediated necrotizing myopathy; ALS – amyotrophic lateral sclerosis; PNH – paroxysmal nocturnal hemoglobinuria
✅
✅
✅
1
FactortargetedbyRaPharmaproductcandidates
Activatedbynon-selfcells Activatedbyantibody-antigencomplexes Activatedbypathogensurfaces
C5a
C3 C1q – C1r – C1s
C7,C8,C9
C5b6
MAC
BindsC5
FactorD,FactorB
eculizumab RA101495
Proinflammatorycytokine
BindsC5&C5b
LectinPathwayClassicalPathwayAlternativePathway
PNH:ruptureofRBC
gMG:destructionofneuromuscularjunction
LN:inflammationofkidneyglomerulus
C5
C2,C3,C4
C5b
C6
ALS: Platform trial planned

Designed for Everyday Control with Easy-to-Use Prefilled Syringe
ü Short Injectionü UltraSafe™ PLUS
ü Everyday Control
ü ü ü üü
Dise
ase
man
agem
ent
ü Convenience & Privacy
Zilucoplan
~5 Seconds
ü Small Volume
Privacy of self administration at home and freedom to travel
Part of daily routine, like brushing your teeth or taking insulin injection
Easy-to-use self-injection (used in approved
products) ~1/4 of a thimble
~0.5 mL
6

7
Generalized Myasthenia Gravis (gMG) Is a Rare, Debilitating, C5-Mediated Disease1
References: 1. Howard JF. Lancet Neurol. 2017;16(12):976-986. 2. Gilhus N, N Engl J Med 2016;375:2570-812015 3. Conti-Fine BM. J Clin Invest. 2006; 116(11):2843-2855. 4. Wang et al. BMC Neurology. 2017;17:77-83. 5. Renton AE, et al. JAMA Neurol. 2015 Apr;72(4):396-404. 6. Heatwole C, et al. J Clin Neuromuscul Dis. 2011; 13(2): 85–94. 7. MG Cost Calculator, Data on File. 8. Soliris® [package insert]. Alexion Pharmaceuticals Inc; revised 1/2017. 9. Prime Therapeutics. AMCP 2018, April 23-26, Boston.
150-250/Million, ~60,000 (US), ~100,000 (EU), ~24,000 (JP)2
Autoantibodies block signals from nerves to muscles and complement activation destroys the neuromuscular junction3
Acetylcholine receptor antibody positive2
Serious and progressive§ Significantly impacts quality of life1,2
§~80% progress to generalized muscle weakness4
§ ~20% experience crisis5
Sporadic, expensive, and often non-specific§Cholinesterase inhibitors, corticosteroids, ISTs, thymectomy§ IVIG, PLEX total maintenance costs ~$150,0006,7 per year§Eculizumab (Soliris®; Alexion), bi-weekly IV therapy approved in
20178; ~$700,0009
Autoantibodies and complement-mediated destruction of the neuromuscular junction cause pathology in gMG1,2
Signal blocked
Signal proceeds
Myasthenia Gravis
Normal
Acetylcholine (ACh)
Acetylcholinereceptor (AChR)
Muscle cell
Autoantibody that binds to AChR
Complement-mediated MAC assembly
Muscle contracts
Destruction of membrane
FREQUENCY
CAUSE
DIAGNOSIS
TREATMENT
CONSEQUENCES

Significant Disease Burden for Most Patients with gMGDespite Ongoing Treatment
1. Kaminski HJ. MG Disease Burden study, under review. Accessed in Dr. Ikjae Lee 2019 MGFA National Conference presentation. 2. Schneider-Gold C, Hagenacker T, Melzer N, Ruck T. Understanding the burden of refractory myasthenia gravis. 2019 Mar 1. 3. MGFA. MG Activities of Daily Living (MG-ADL) profile. 4. Mindspot Research. Myasthenia Gravis Patient Needs Exploration (2018). 5. Lee I, Kaminski HJ, McPherson T, Feese M, Cutter G. Gender differences in prednisone adverse effects: Survey result from the MG registry. Neurol Neuroimmunol Neuroinflamm. 2018 Oct 15;5(6):e507. Accessed in Dr. Ikjae Lee 2019 MGFA National Conference presentation. 6. Mindspot Research. Myasthenia Gravis Patient Needs Exploration (2018).
Patients Dissatisfied with Current Treatments4
§ Prednisone adverse effects extremely common & intolerable (more than 90% of patients reported adverse events)5
§ Treatment dissatisfaction: 1) too much time to start working; 2) does not relieve symptoms; 3) inconvenient6
§ ~40% of patients do not feel in control of their condition, treatments do not target underlying disease6
~50% of Patients with Moderate to Severe Disease (ADL ≥6)1,2
§ Activities of Daily Living (ADL) - talking, chewing, swallowing, breathing, brush teeth, comb hair, arise from chair, double vision, eyelid droop3
§ ~70% of patients with ADL >6 feel their treatment goals are not being met4
MG-ADL score
Perc
ent
8

Treatment Paradigm: Target Complement-Mediated Damage Earlier
Data source: IQVIA market projections (93% retail, 1.5B LRx & Dx claims, CDM ~350 hospitals, PharMetrics health plan 150M pts)Jan 2016 – Dec 2017 selection period (patients with at least 1 MG diagnosis claim ICD-10 G70.00 or G70.01); 5 years history for treatment and procedures for pathway analyses (starting Jan 2013)Applied best practice eligibility controls and apply appropriate pre-screener/end-treater rulesUsed Rx/Dx intersection to project Rx and office-based treatments, and projected hospital utilization of relevant therapies (ie. IVIG, PLEX) using CDM Segment size projected with Pharmetrics Plus data, therapy usage does not use Pharmetrics Plus; therapy analysis on steroid dosage used to allocate patients on high dose steroid to uncontrolled
9
>90% of these patients chronic IVIG, PLEX
US Prevalence: ~200 per million (~60K pts)
Last Line<10K pts ~ 15%
Uncontrolled>20K pts ~ 35%
Acetylcholinesterase Inhibitor
Steroids Immunosuppressive Therapies
IVIG/PLEXMG Diagnosis
>70% of these patients>20mg/day steroids AND at least 1 IST
Zilucoplan Target Population
Opportunity to Treat ~30K Patients (U.S. Only) with AChR+ gMG
REGAIN Population (Eculizumab)

Randomized, Double-Blind, Placebo-Controlled Phase 2 Study of Zilucoplan in a Broad Generalized Myasthenia Gravis Population
Broad Patient Population:
� Generalized myasthenia gravis (MGFA class II-IVa)
� Acetylcholine receptor (AChR) antibody positive
� QMG score of ≥12
� Stable doses of corticosteroids and/or immunosuppressants
� No requirement to be “refractory” or to have failed multiple prior therapies
� Patients must be vaccinated against meningococcus
Endpoints:
� Primary: Change in QMG score from baseline to week 12
� Secondary: Change in MG-ADL, MG Composite, and MGQoL15r scores from baseline to week 12
� Pre-specified significance testing at a 1-sided alpha of 0.1
Enrollment: 44 patients (vs. target of 36)
QMG, Quantitative Myasthenia Gravis; MG-ADL, Myasthenia Gravis Activities of Daily Living; MGFA, Myasthenia Gravis Foundation of America; MGQoL15r, 15-item Myasthenia Gravis Quality-of-Life revised scale; SC, subcutaneous; SOC, standard of care.
10
Screening 1:1:1 Randomization 0.1 mg/kg SC + SOC (n=15) Open-Label Extension (n=42)
0.3 mg/kg SC + SOC (n=14)
Placebo + SOC (n=15)
Main Study Period (12 weeks) Long-Term Extension (12 weeks)
Placebo arm randomized 1:1 to receive0.3 mg/kg (n=7) or 0.1 mg/kg (n=7)

11
Baseline Characteristics Confirm Breadth of gMG Study PopulationVariable Placebo (n=15) Zilucoplan 0.1 mg/kg (n=15) Zilucoplan 0.3 mg/kg (n=14)
Age, mean years (± SD) 48 (15.7) 46 (15.7) 55 (15.5)
Male, n(%) 4 (27%) 7 (47%) 10 (71%)
Race, n(%)• White• Asian• Black or African American
12 (80%)1 (7%)
2 (13%)
13 (87%)0
2 (13%)
11 (79%)1 (7%)
2 (14%)
MGFA Class at Screening• II• III• IVa
7 (47%)8 (53%)
0
5 (33%)10 (67%)
0
5 (36%)5 (36%)4 (29%)
Duration of Disease, mean years (min, max) 8.0 (0.1, 20.9) 8.7 (1.6, 24.1) 8.3 (0.5, 26.0)
Baseline QMG Score, mean (± SD) 18.7 (4.0) 18.7 (4.0) 19.1 (5.1)
Baseline MG-ADL Score, mean (± SD) 8.8 (3.6) 6.9 (3.3) 7.6 (2.6)
Baseline MG Composite Score, mean (± SD) 18.7 (5.7) 14.5 (6.3) 14.6 (6.3)
Baseline MGQoL15r Score, mean (± SD) 15.9 (7.4) 19.1 (5.0) 16.5 (7.3)
Prior MG Therapies (Standard of Care)• Pyridostigmine, n(%)• Corticosteroids, n(%)• Immunosuppressants, n(%)
14 (93%)13 (87%)12 (80%)
15 (100%)13 (87%)12 (80%)
14 (100%)14 (100%)
9 (64%)
Prior IVIG, n(%) 9 (60%) 8 (53%) 10 (71%)
Prior Plasma Exchange, n(%) 7 (47%) 9 (60%) 7 (50%)
Prior Thymectomy, n(%) 5 (33%) 8 (53%) 7 (50%)
Prior MG Crisis Requiring Intubation, n(%) 3 (20%) 4 (27%) 2 (14%)
Non-RefractoryPatients Included9% no prior steroids
25% no prior ISTs39% no prior IVIG48% no prior PLEX
High Unmet Medical Need

12
Pharmacokinetic and Pharmacodynamic ResultsSupport Evaluation 0.3 mg/kg Dose of Zilucoplan
Placebo
50
100
Study Week
%H
emol
ysis
0 4 8 12LLOQ
Study Week
Zilu
copl
an(n
g/m
L)
0 4 8 12
25
75
1 2 1 2
0.1 mg/kg Zilucoplan 0.3 mg/kg Zilucoplan

Zilucoplan 0.3 mg/kg Achieved Rapid, Clinically Meaningful, Statistically Significant, and Sustained Reductions in QMG and MG-ADL
13
CFB
(SEM
) in
QM
G
0-2-4-6-8
-10
0 1 2 4 8 12 14 16 20 24
N = 15 15 7N = 14 14 13
Study Week Study Week
P=0.01†
CFB
(SEM
) in
MG
-AD
L
0
-2
-4
-6
0 1 2 4 8 12 14 16 20 24
N = 15 15 7N = 14 14 13
Study Week Study Week
P=0.05*
P=0.04*
P=0.0004†
Placebo 0.3 mg/kg Zilucoplan Placebo → 0.3 mg/kg Zilucoplan
P<0.0001‡
P<0.0001‡
/7/13
/13/7
*1-sided analysis of covariance for LS mean change from baseline for 0.3 mg/kg arm vs. placebo; placebo patients re-baselined to zero upon completion of 12-week main study.†2-sided t test for LS mean change from week 12 to week 24 for placebo patients crossing over to 0.3 mg/kg (n=7).‡2-sided t test for LS mean change from week 0 to week 24 for 0.3 mg/kg arm.CFB, change from baseline; LS, least squares; MG-ADL, Myasthenia Gravis Activities of Daily Living; QMG, Quantitative Myasthenia Gravis; SEM, standard error of the mean.

Zilucoplan 0.3 mg/kg Achieved Rapid, Clinically Meaningful, Statistically Significant, and Sustained Reductions in MG Composite and MGQoL15r
14
CFB
(SEM
)in
MG
Com
posi
te
0-2-4-6-8
-10
0 1 2 4 8 12 14 16 20 24
N = 15 15 7N = 14 14 13
Study Week Study Week
P=0.004†
CFB
(SEM
)in
MG
QoL
15r
0
-5
-100 1 2 4 8 12 14 16 20 24
N = 15 15 7N = 14 14 13
Study Week Study Week
P=0.04*
P=0.06*
Placebo 0.3 mg/kg Zilucoplan Placebo → 0.3 mg/kg Zilucoplan
P<0.0001‡
P=0.04†
P=0.0006‡
/7/13
/7/13
*1-sided analysis of covariance for LS mean change from baseline for 0.3 mg/kg arm vs. placebo; placebo patients re-baselined to zero upon completion of 12-week main study.†2-sided t test for LS mean change from week 12 to week 24 for placebo patients crossing over to 0.3 mg/kg (n=7).‡2-sided t test for LS mean change from week 0 to week 24 for 0.3 mg/kg arm.CFB, change from baseline; LS, least squares; MGQoL15r, 15-item Myasthenia Gravis Quality-of-Life revised scale; SEM, standard error of the mean.

15
Pre-Specified Pooled Analysis of MG-ADL at Week 12 Satisfied 2-Sided p<0.05
LOCF ANCOVA 2-sided p value shown; error bars denote standard errors of least squares mean; mITT* Placebo-corrected change in MG-ADL at 26 weeks in REGAIN study: -1.9 LOCF ANCOVA p=0.039; ref. Howard et al AANEM 2016; For Informational Purposes: Differences exist between trial designs and subject populations. Ra Pharma has not conducted any head-to-head trials comparing zilucoplan to eculizumab.
In Phase 2, zilucoplan met Phase 3 primary endpoint (MG-ADL at 12
weeks) with similar magnitude and statistical significance as eculizumab
in Phase 3 REGAIN study at 26 weeks*
Change from Baseline in MG-ADL
-3.3
-1.1
p=0.047
-4
-2
0
S tu d y W e e k
Ch
an
ge
fro
m B
ase
line
(S
EM
)
P la c e b o
P o o le d A c tiv e
0 1 2 4 8 12
-4
-2
0
S tu d y W e e k
Ch
an
ge
fro
m B
ase
line
(S
EM
)
P la c e b o
Z ilu c o p la n P o o le d
0 1 2 4 8 12

16
Minimal Symptom Expression Observed by Week 12
*Vissing J, Jacob S, Fujita K, et al. Minimal Symptom Expression with Eculizumab in Myasthenia Gravis. AANEM 2018
0 .1 m g /k g Zi lu c o p la n
W e e k 1 2
1 2 0 0 m gEc u l iz u m a b
W e e k 2 6
0 .3 m g /k g Zi lu c o p la n
W e e k 1 2
0
5
1 0
1 5
2 0
2 5
P la c e b o - C o r r e c t e d R a t e s
Pe
rce
nt
of
Pa
tie
nts
(%
)
23% of patients (placebo-corrected) achieved MSE in 12 weeks in
0.3 mg/kg zilucoplan arm
Minimal symptom expression (MSE) = Achieving MG-ADL score of 0 or 1

17
Phase 2 Safety and Tolerability Profile Support Continued Development
Placebo(n=15)
Zilucoplan 0.1 mg/kg (n=15)
Zilucoplan 0.3 mg/kg (n=14)
Patients Requiring Rescue with IVIG or PLEX 3 (20%) 1 (7%) 0 (0%)
Patients with adverse events (AEs) 12 15 12
Patients with related AEs 3 8 3
Patients with serious AEs 3 0 5
Patients with related serious AEs 0 0 0
Patients with most common related AEs:
Nausea 0 2 0
Injection site bruising 1 2 0
Injection site scab 0 3 0
Contusion 0 1 1
Headache 1 4 2
Patients with injection site reactions 2 4 3
• No meningococcal infections• Profile consistent with Ph1 and Ph2 PNH studies
MedDRA Version 20.0 Adverse Event Preferred Terms; injection site reactions defined as pain, tenderness, erythema, or induration
• All 44 subjects completed 12-week study; No early withdrawals• 42/44 subjects (95%) entered long-term extension
No patients required rescue
in 0.3 mg/kg zilucoplan arm

Zilucoplan: A Convenient Complement Inhibitor for a Broad gMG Population
Zilucoplan
1Soliris QMG, ADL at 12wk estimated (Ref. Howard et al. Lancet 2017)2Soliris QMG, ADL improvement at 26wks (Ref. Howard et al. Lancet 2017)3Soliris Highlights of Prescribing Information; http://alexion.com/Documents/Soliris_USPI.aspx; For Informational Purposes: Differences exist between trial designs and subject populations. Ra Pharma has not conducted any head-to-head trials comparing zilucoplan to eculizumab.
~0.5 mL (3 kDa)SC daily self-admin
120 mL (140 kDa) Intravenous infusion every 14 days ADL
QMG
~-1.7
≥7 34%
≥6 39%
ADL
QMG -2.8
@ 12wks
@ 12wks
@ 26wks
@ 24wks
(-3*)
≥7 62%
≥6 46%
18
QMG, ADLMean δ vs Placebo1 % Improvement2
*At 26wks
C5 mAb
C5 Cyclic
Peptide
(-1.9*)
Eculizumab3
UncontrolledMG
(~30k)
Refractory MG
(~3-5k)
5-8 sec.
45 min.
Administration Tx Time Population Mechanism
-2.3
~-2.5

� Inclusion Criteria:� Generalized myasthenia gravis (MGFA class II to IV)� Acetylcholine receptor antibody positive� MG ADL score ≥ 6 and QMG total score ≥ 12� Stable doses of corticosteroids and/or immunosuppressants� No requirement to be “refractory” or to have failed multiple
prior therapies� Patients must be vaccinated against meningococcus
Pivotal, 12-Week, Placebo-Controlled Phase 3 Clinical Trial in Generalized Myasthenia Gravis
� Primary Endpoint:� Change from baseline to week 12 in MG-ADL total
score, *p<0.05
� Enrollment: ~130 patients
19
Open-Label Long-Term Extension (Active Drug)1:1 Randomization n = 130Screening
Placebo + Standard of Care
Main Study Period (12 Weeks)
0.3 mg/kg SC + Standard of Care

20
Improved Biodistribution of Zilucoplan into Tissue vs. Typical mAb
Antibody Biodistribution1 (%)
ZilucoplanBiodistribution2 (%)
Lung 14.9 37.5
Heart 10.2 22.9
Muscle 3.97 7.0
Small Intestine 5.22 10.9
Large Intestine 5.03 21.7
Spleen 12.8 15.5
Liver 12.1 27.1
Bone 7.27 15.3
Stomach 4.98 8.5
Lymph nodes 8.46 12.8
Fat 4.78 16.2
Brain 0.35 0.9
Pancreas 6.4 15.8
Testes 5.88 15.5
Thymus 6.62 7.8 1. Shah DK, Betts AM. Antibody biodistribution coefficients: Inferring tissue concentrations of monoclonal antibodies based on the plasma concentrations in several preclinical species and human. mAbs 2013; 5:297-305
2. Ra Internal Data – Rat QWBA Study using radiolabeled zilucoplan; Data represent tissue AUC0-24 as a percentage of Plasma
Input
Rodent quantitative whole-body autoradiography (QWBA) studies

Modeling Permeability Across the Basal Lamina Zilucoplan Exhibited Improved Diffusion in Matrigel Model
21
Site of action
Passage of drug from interstitial fluid
* Composition and Function of the Extracellular Matrix in the Human Body: Biophysical Properties of the Basal Lamina: A Highly Selective Extracellular Matrix By Fabienna Arends and Oliver Lieleg. DOI: 10.5772/62519
Schematic of neuromuscular junction* Model of basal lamina diffusion using Matrigel membrane
Zilucoplan demonstrates a 4x improvement in permeability across Matrigel membrane at 24 hours compared with
eculizumab**
0 10 200
20
40
60
80
100
Hours
Lowe rt oUppe rChamber
Mate rialRatio%
Eculizumab
**Data on record at Ra Pharma
Zilucoplan

Immune-Mediated Necrotizing Myopathy (IMNM): A Distinct Idiopathic Inflammatory Myopathy
22
IMNM
Anti-SRP
Anti-HMGCR
Prevalence: ~21/Million2-10
US: ~6,300 casesEU: ~6,500 casesJapan: ~2,500 cases
Idiopathic InflammatoryMyopathies1
Ab negative
Anti-synthetase syndrome
Dermatomyositis
Inclusion body myositis
Epidemiology:Age of onset, typically 40 to 60 years, predominantly affects females5-7
1. Mariampillai K, et al. JAMA Neurol. 2018;75:1528-1537. 2. Smoyer-Tomic KE, et al. BMC Musculoskeletal Disorders.2012;13:10. 3. Dobloug C, et al. Ann Rheum Dis. 2017;74:1551-1556. 4. Svennson J, et al. Rheumatology;2017;56:802-810. 5. Pinal-Fernandez I, et al. Arthritis Care Res. 2017;69:263–270. 6. Mammen AL, et al. Arthritis Rheum. 2011;63:713–721. 7. Allenbach Y, et al. Medicine. 2014;93:150-157. 8. Hengstman GJD, et al. J Neurol. 2002;249:69–75. 9. Brouwer R, et al. Ann Rheum Dis. 2001;60:116–23. 10. Watanabe Y, et al. J Neurol Neurosurg Psychiatry. 2016;87:1038–1044.
Diagnosis:Anti-SRP and anti-HMGCR IMNMcan be diagnosed with commercially-available antibody tests
~70%
~30%

IMNM: A Severe and Debilitating Disease of Muscle Necrosis
1. Allenbach Y, et al. Neuromuscul Disord. 2018;28:87-99. 2. Pinal-Fernandez I, et al. Ann Rheum Dis. 2017;76:681–687. 3. Watanabe Y, et al. J Neurol Neurosurg Psychiatry. 2016;87:1038-1044. 4. Pinal-Fernandez I, et al. Arthritis Care Res; 2017;69:263–270 . 5. Allenbach Y, et al. Brain. 2016;39:2131-2135. 6. Mammen AL, et al. Arthritis Rheum. 2011;63:713-721.
Anti-SRP subtype3,4
Associated with extra-muscular manifestations in approximately 10-20% of patients
Anti-HMGCR subtype4,5,6
Associated with statin use in approximately 75% of patients
Muscle atrophy and fatty replacement2
Severe proximal muscle weakness, especially in lower limbs1
Dysphagia3
Neck weakness3
Myalgia3
Severe necrotizing myopathy with prominent complement deposition1
Markedly elevated serum CK1
23
Necrotic muscle fiber
Healthy Patient
Patient With
IMNM

Noris M, et al. Semin Nephrol. 2013;33:479-492. 24
Anti-SRP or Anti-HMGCR–Mediated Complement Activation
Necrotic Muscle Tissue
Formation of MAC on cells
Creatine kinasereleaseC5
Muscle Cell
Complement Cascade
Anti-SRP or Anti-HMGCR
binding
C5a
C5b
Healthy Muscle Tissue
Anti-SRP and Anti-HMGCR Antibodies Initiate Complement-Mediated Tissue Damage in IMNM

Complement Plays a Central Role in the Pathophysiology of IMNMStrong deposition of C5b-9 (MAC) in muscle fibers and blood vessels of patients with IMNM1
Muscle fibers Muscle fibers Capillaries Vascular endothelial and smooth muscle layers of the small artery wall
Small vein wall
1. Cong L, et al. Int J Clin Exp Pathol. 2014;7:4143-4149. 2. Bergua C, et al. Ann Rheum Dis. 2019;78:131-139.25
A B EC D
Anti-SRP IgG
20
40
60
Mus
cle
Stre
ngth
(g)
C3wt C3-/-
Anti-HMGCR IgG
60
80
100
120
40Mus
cle
Stre
ngth
(g)
C3wt C3-/-
Phenotypic rescue of IMNM-induced muscle weakness in complement-deficient mice2
Muscle weakness in mice can be induced with sera from patients with IMNM2
Pathogenicity of patient serum is dependent on the presence of complement2

Anti-SRP Myopathy
Anti-HMGCR Myopathy
aUsed in severe cases of IMNM.bAzathioprine/mycophenolate mofetil may be used in the case of methotrexate intolerance.cIn patients with anti-SRP myopathy, methotrexate and rituximab are generally considered before IVIg. In patients with anti-HMGCR myopathy, methotrexate and IVIg are generally considered before rituximab; IVIg may be used as maintenance treatment on a case-by-case basis. 1. Allenbach Y, et al. Neuromuscul Disord. 2018;28:87-99. 2. Day, J., et al. Seminars in Arthritis and Rheumatism. 2019;00:1-10.
Current Treatment Paradigm for IMNM Is Non-Specific and Inadequate
Rheumatologists Neurologists NeuromuscularSpecialists
CorticosteroidsPredinsone/prednisolone
(oral)
or
Methylprednisolone (IV)a
ImmunosuppressivesMethotrexateAzathioprine
Mycophenolate mofetilb
Rituximab (IV)c
IVIgc
Diagnose/Refer
Treat/Manage
Despite intense immunosuppression,~52 - 66% of patients show progression and incomplete recovery at two years2
Multiple specialties are involved in IMNM management
There are currently no approved treatments for IMNM1
26
1ST LINE 2ND/3RD LINE

Randomized, double-blind, placebo-controlled, multi-center study, followed by an open-label long-term extension
Phase 2 Clinical Trial Is Designed to Evaluate the Potential of Zilucoplan for the Treatment of IMNM
Broad Patient Population• Clinical diagnosis of IMNM• Autoantibody positive (HMGCR, SRP)• MRC weakness of ≤ 4/5 in at least 1 proximal
muscle group• CK >1000 IU/L• Stable doses of corticosteroids,
immunosuppressants, or IVIg• Vaccinated against meningococcus
Long-Term Extension (Active Drug)1:1 RandomizationScreening
Placebo + Standard of Care (n=12)
Main Study Period (8 Weeks) Long-Term Extension
0.3 mg/kg SC + Standard of Care (n=12)
Endpoints• Primary endpoint: Change from baseline to week 8 in CK• Secondary endpoints include functional assessments using validated
measures, such as:– Triple Timed Up and Go (3TUG) Test– Proximal Manual Muscle Testing (MMT)– Physician and Patient Global Activity Visual Analogue Scales (VAS)– Health Assessment Questionnaire (HAQ)– Myositis Disease Activity Assessment Tool (MDAAT)
27

28
Spinal67%
Bulbar33%
Onset of ALS1
eg, limbs affected
eg, dysarthria, dysphagia
80%mortality
within 5 years4
Fasciculations, cramps, spasticity5,6
Focal symptom onset:
Dysarthria, dysphagia5,6
Death by respiratory failure5
SymptomsPresentation and Prognosis Pathophysiology
Causes of ALS2
Sporadic90%–95%
Familial 5%-10%
ALS is a severe neurodegenerative disorder characterized by the loss of upper and lower motor neurons, resulting in progressive muscle weakness, atrophy, and eventually partial or total paralysis1
Upper or lower limb fatigable or persistent muscle weakness6
Progressive symptoms:
Global muscle weakness6
• Neurodegeneration: involvement of upper (cortico-spinal) and lower (bulbospinal) motor neurons5
• Gliosis: reactive inflammation of astrocyte and microglial cells5
Muscle atrophy, stiffness5,6
Paralysis5,6
Respiratory failure5,6
2–5 yearsaverage life expectancy3
Amyotrophic Lateral Sclerosis (ALS) Is a Rapidly Progressive and Fatal Neurodegenerative Disease
Spinal67%
Bulbar33%
Sporadic90%–95%
1. National Institute of Neurological Disorders and Stroke. Amyotrophic lateral sclerosis (ALS) fact sheet. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Amyotrophic-Lateral-Sclerosis-ALS-Fact-Sheet. Accessed July 8, 2019. 2. ALS Association. Causes/inheritance. https://www.mda.org/disease/amyotrophic-lateral-sclerosis/causes-inheritance. Accessed July 8, 2019. 3. Wijesekera LC and Leigh PN. Orphanet J Rare Dis. 2009;4:3. 4. Sorenson EJ, et al. Neurology. 2002;59:280-282. 5. Hardiman O, et al. Nat Rev Dis Primers. 2017;3:17071. 6. ALS Association. Symptoms and diagnosis. http://www.alsa.org/about-als/symptoms.html. Accessed August 8, 2019.

ALS Is a Rare Disease With Few Therapeutic Options
29aRepresented by Spain, France, Italy, Germany, and United Kingdom.1. ALS Association. Epidemiology of ALS and suspected clusters. http://www.alsa.org/als-care/resources/publications-videos/factsheets/epidemiology.html. Accessed July 8, 2019. 2. National Institute of Neurological Disorders and Stroke. Amyotrophic lateral sclerosis (ALS) fact sheet. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Amyotrophic-Lateral-Sclerosis-ALS-Fact-Sheet. Accessed July 8, 2019.
There is no cure
for ALS2
Only 2FDA-approved
drugs2
Riluzole
Edaravone>1.5 ×
Mean age at diagnosis1
55–65 yr more common1
PREVALENCE1
INCIDENCE1
JAPANUNITED STATES EUROPEa
~8,000
~2,400~6,000
~20,000
~6,500
~22,00050-70per 1 million people
~20per 1 million people

Complement MAC Proteins Are Associated With Neuroinflammation in Patients With ALS
30
Activation of the immune system, including a high expression of complement proteins, has been observed in the spinal cord and motor neurons of patients with ALS1,2
P value calculated using a nonparametric Wilcoxon rank-sum test. sC5b-9, serum complement components C5b through C9, also known as membrane attack complex (MAC).1. Sta M, et al. Neurobiol Dis. 2011;42:211–220. 2. Bahia El Idrissi N, et al. J Neuroinflammation. 2016;13:72. 3. Kjældgaard A, et al. Molecular Immunology. 2018;102:14-25.
30
Motor end plates
C5b-9 (MAC) detected in glial cells associated with the motor neurons of the spinal cord of patients with
ALS, which is absent in healthy controls
MAC
Complement activation and MAC deposition
Arrows indicate positive MAC staining on glial cells
Glial cells of ventral horn
White matter of spinothalamic tract Upper motor neurons
Medulla
Lower motor neurons
Cervical spinal cord
Thoracic spinal cord
Lumbar spinal cord
Bulbar motor neuron
Oropharyngeal muscles
Somatic motor neuron
Limb muscles
Arrow indicates positive MAC staining on motor end plates
MAC detected on the innervated motor end plates of intercostal muscle from patients with ALS,
which is absent in healthy controls
Bulbar region
Spinal cord
Motor cortex
Medulla
Log
sC5b
-9 [n
g/m
L]
sC5b-9 in serum samples
P<0.0001****
Healthy ALS

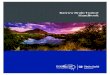
PLGA XR Formulation of Zilucoplan Designed to Have Uniform Microsphere Morphology with High Drug Loading and Homogeneous Distribution
Optimization of process has delivered a uniform particle with homogenous distribution of zilucoplan throughout microspheres
� Target drug load achieved: Morphology and size range enable good syringeability
� Homogeneous distribution of drug in particle designed to enable predictable drug release with minimal burst (<5%)
Zilucoplan PLGA microsphere (A) Surface morphology by scanning electron microscopy and(B) Drug distribution by Na+ Energy Dispersive X-Ray Spectroscopy*
A) B)
31*Data on record at Ra Pharma

Zilucoplan PK/PD Have Been Highly Comparable Across Non-Human Primate Pre-Clinical and Human Clinical Studies
Comparable concentration dependence of complement inhibition observed in pre-clinical NHP and Phase 1 and Phase 2 human clinical studies
*Data on record at Ra Pharma
0 5000 10000 15000 200000
50
100
8000Zilucoplan plasma concentration (ng/mL)
510
% H
emol
ysis
P2 PNH; 0.1 mg/kgPhase 1 HV
P2 PNH; 0.3 mg/kg
0 5000 10000 15000 200000
50
100
Zilucoplan plasma concentration (ng/mL)
% H
emol
ysis
0 5000 10000 15000 200000
50
100
Zilucoplan plasma concentration (ng/mL)
% H
emol
ysis
NHP PK/PD Zilucoplan Immediate Release (IR)* NHP PK/PD Zilucoplan XR* Human PK/PD Zilucoplan IR*
For reference across species, vertical dotted line represents clinical trough concentration for daily 0.3 mg/kg
32

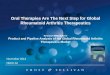
Once-Weekly Administration of PLGA XR Formulation of Zilucoplan Rapidly Achieved Target C5 Inhibition Equivalent to Daily Administration
Comparison of PLGA XR formulation of zilucoplan Q1W PD to zilucoplan IR daily in NHP and myasthenia gravis patients
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13 140
Time (Day)
510
% H
emol
ysis
Dose A 0.3x Dose AZilucoplan XR dose(NHP)
Zilucoplan XR (NHP)Zilucoplan IR (0.3 mg/kg), (NHP)
Zilucoplan IR dose(Phase 2 MG)
0.3 mg/kg
Zilucoplan IR (0.3 mg/kg), (MG patients)
Zilucoplan IR dose(NHP)
0.3 mg/kg
33
Inhibition of complementactivity following a singlesubcutaneous dose of PLGAXR formulation of zilucoplanin cynomolgus monkeys asmeasured by an ex-vivo sheepred blood cell assay.

FC XR Formulation of Zilucoplan Rapidly Achieved and Maintained Target Levels of Complement Inhibition for at Least Seven Days in NHPs
� Exclusive worldwide license agreement with Camurus AB for proprietary FluidCrystal® (FC)technology
� FC injection depot is a lipid-based liquid that absorbs interstitial aqueous body fluid and transforms to gel-like phases in situ, encapsulating the active substance
� FC technology designed to enable disease control with a simple presentation:
� Low volume, SC self-administration
� Room-temperature stable
� No need for IV loading
� FC XR formulation of zilucoplan achieved rapid and sustained pharmacodynamic inhibition of complement C5 in non-human primates, supporting the potential for at least once weekly dosing
34
Inhibition of complement activity following a singlesubcutaneous dose of FC XR formulation of zilucoplan incynomolgus monkeys as measured by an ex-vivo sheep redblood cell assay (Mean+SEM, n=4).

� Small molecule C5 inhibitors (SMi) do not bind to mouse complement C5� Immunodeficient mice transplanted with human hepatocytes provide circulating human complement
� Oral dosing of SMi resulted in full blockade of ex vivo zymosan-mediated C5 activation (incubation in whole blood)
Humanized Liver Mouse Model –Inhibition of Complement C5 Observed Following Oral Dosing
+ Zymosan
C5 SMi
Inhibition
35

Array of C5 Inhibitor Assets Provides an Opportunity to Build a Transformative Pipeline in Neurology
Zilucoplan QD Zilucoplan XROral Small Molecule
C5 Inhibitor
Neuromuscular NeurodegenerativeNeuropathies/Myopathies
Once daily SC small peptide inhibitor, designed to inhibit C5 systemically and locally
Added convenience of SC once weekly Highly potent, orally available
C5 Inhibitor Lifecycle
Neurology Disease Targets,Systemic & Local C5
Potential of a Peptide Inhibitor in Tissue-Based C5 Diseases and a First-in-Class Oral Small Molecule 36

� Focused on delivering innovative and accessible therapies to patients with rare, complement-mediated diseases
� Zilucoplan: A convenient, self-administered, subcutaneous complement C5 inhibitor
� Generalized myasthenia gravis (gMG): Successful Phase 2 study in a broad spectrum of patients with gMG ; Phase 3 clinical trial ongoing
� Immune-mediated necrotizing myopathy (IMNM): Phase 2 clinical trial ongoing
� Amyotrophic lateral sclerosis (ALS): Selected for HEALEY ALS Platform Trial by Sean M. Healey & AMG Center for ALS at Mass General
� Positive Phase 1b trials: Ethno-bridging (Japan) and in patients with renal impairment; Support further development with no need for dose modification
� Advancing a portfolio of investigational C5 inhibitors in pre-clinical development� XR: PLGA and FluidCrystal® (FC) XR formulations of zilucoplan achieved rapid and sustained pharmacodynamic inhibition of complement C5 in
non-human primates, supporting once weekly or less frequent dosing in clinical trials
� SMi: First-in-class oral small molecule C5 inhibitor
� Proprietary drug discovery engine
� Trillion member, highly diverse, synthetic macrocyclic peptide libraries; Diversity and specificity of mAbs with the pharmacologic advantages of small molecules
� Merck Collaboration: Oral peptide targeting a large CV market opportunity
Transforming Complement Therapeutics
37