Embed Size (px)
Citation preview

Transforming growth factor-b1 hyperexpression in AfricanAmerican end-stage renal disease patientsRapid Communication
MANIKKAM SUTHANTHIRAN, ASHWANI KHANNA, DAVID CUKRAN, ROHINI ADHIKARLA, VIJAY K. SHARMA,TEJINDER SINGH, and PHYLLIS AUGUST
Department of Transplantation Medicine and Extracorporeal Therapy, and Divisions of Nephrology and Hypertension, Department ofMedicine; Office of AIDS Surveillance, New York City Department of Health; and The Rogosin Institute, The New York Hospital-Cornell Medical Center, New York, New York, USA
Transforming growth factor-b1 hyperexpression in African Americanend-stage renal disease patients. End-stage renal disease (ESRD) is morefrequent in African Americans (blacks) compared to Caucasian Ameri-cans (whites). Identification of remediable causes of the increased preva-lence has the potential to reduce the excess burden of ESRD. Becauserenal fibrosis is a correlate of progressive renal failure and a dominantfeature of ESRD, and because transforming growth factor-beta1 (TGF-b1)can induce fibrosis and renal insufficiency, we explored the hypothesis thatTGF-b1 hyperexpression is more frequent in black ESRD patients com-pared to white ESRD patients. Our postulate was tested by determiningcirculating levels of TGF-b1 protein in the sera of 56 black and 42 whiteESRD patients treated by chronic hemodialysis. A solid-phase sandwichenzyme-linked immunosorbent assay, specific for TGF-b1, was used toquantify TGF-b1 levels in the ESRD cohort. Additional cytokines impli-cated in tissue repair/remodeling, interleukin-6 (IL-6) and tumor necrosisfactor-alpha (TNF-a), were also measured. Our investigation demon-strated a significantly higher concentration of TGF-b1 protein but not thatof IL-6 or TNF-a in blacks compared to whites. Our observation thatTGF-b1 is hyperexpressed in black ESRD patients suggests a mechanismfor the increased prevalence of renal failure (since TGF-b1 hyperexpres-sion can result in renal insufficiency in experimental models) among theblack population.
Irreversible renal failure (that is, end-stage renal disease,ESRD), a debilitating and costly sequela of most forms of chronicrenal disease, is four times more frequent in African Americans(blacks) compared to Caucasian Americans (whites) [1]. Whereas12.5% of the U.S. population is black, more than 31% of patientsrequiring dialysis therapy for ESRD are blacks. The three mostcommon causes of ESRD in the U.S. are diabetes, hypertensionand glomerulonephritis, and all three are more prevalent in the
black population compared to whites. However, the increasedincidence of these diseases fails to fully explain the excess burdenof ESRD among blacks since the age- and gender-adjustedincidence of ESRD due to hypertension, diabetes or glomerulo-nephritis is 3- to 10-fold higher in blacks compared to whites [1].The heightened risk is perhaps best exemplified by the recent datafrom two major clinical trials, the Multiple Risk Factor Interven-tion Trial (MRFIT), and the Modification of Diet in RenalDisease (MDRD) study. In the MRFIT study, in which blackmales and white males with mild to moderate hypertension andnormal renal function were treated with anti-hypertensive medi-cation, the age-adjusted ESRD incidence was 42.22 per 100,000person-years in black men and 13.90 per 100,000 person-years inwhite men [2]. In the MDRD study, black race was a predictor ofprogression of nephropathy [3]. Although several hypotheses havebeen proposed to explain these observations, including geneticdifferences, increased prevalence of hypertension, and socioeco-nomic factors, to date these proposed genetic or environmentalfactors have not provided a satisfactory or unifying explanation forthe increased risk of ESRD in blacks.
Transforming growth factor-beta1 (TGF-b1), a multifunctionalcytokine with fibrogenic properties, has been implicated in thepathogenesis as well as the progression of a variety of chronicrenal diseases [4]. In addition to its fibrogenic properties, TGF-b1
has been shown to stimulate endothelin-1 production [5], and thusmay be involved in the pathogenesis of hypertension. In anattempt to explain the basis for the increased prevalence of ESRDin the black population, we explored the hypothesis that TGF-b1
hyperexpression is more frequent in black ESRD patients com-pared to white ESRD patients.
METHODS
End-stage renal disease patient population
Fifty-two black and 46 white patients with ESRD, treated withchronic hemodialysis therapy, were studied for level of expressionof TGF-b1 protein in their peripheral blood. In addition, circu-lating levels of interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-a) were also determined in the ESRD cohort.Interleukin-6 and TNF-a were selected for study because of their
1 See Editorial by Klahr, p 792.
Key words: African American ESRD, end-stage renal disease, transform-ing growth factor-b1, genetics and TGF-b1, race and ESRD, renal failurein blacks, hypertension, HIV and genetics.
Received for publication October 24, 1997and in revised form November 24, 1997Accepted for publication November 24, 1997
© 1998 by the International Society of Nephrology
Kidney International, Vol. 53 (1998), pp. 639–644
639

potent immunoregulatory and remodeling properties [6, 7] and inconsideration of earlier reports of their dysregulated expression inESRD patients [8]. All patients were clinically stable and werefree of any active infection. Blood was also drawn from 30 healthywhite and 32 healthy black individuals for cytokine analysis. Thesecontrol subjects did not have any history of hypertension, diabe-tes, renal, cardiovascular, peripheral vascular, or cerebrovasculardisease.
Quantification of cytokine concentration in the serum
Peripheral venous blood was obtained from the patients and thesera were isolated and stored at 270°C until assayed for cytokines.The blood samples were drawn prior to the dialysis procedure.Pre- and well as post-dialysis blood specimens were obtained onthe same day to calculate urea reduction ratio. The biologically-active TGF-b1 protein concentration was determined using a solidphase TGF-b1-specific sandwich ELISA (Promega, Madison, WI,USA), as described [9]. The sera were activated by acidificationand tested at 1:300 dilution, as recommended. A TGF-b1 standardcurve was constructed using 1000, 500, 250, 62.5, 31.25, and 15.6pg/ml of recombinant human TGF-b1 protein, and a curve-fittingsoftware program was used to quantify TGF-b1 protein concen-tration in the sera. The minimum level of detection of TGF-b1
with the sandwich ELISA was 25 pg/ml. ELISA kits (Cytoscreenimmunoassay kit), purchased from Biosource International (Cam-arillo, CA, USA), were used to measure the concentrations ofIL-6 and TNF-a. Sera were tested at 1:10 dilution and theminimum detectable concentration was 2 pg/ml for IL-6, and 1pg/ml for TNF-a.
Statistical analyses
The correlation analysis procedure of SAS (Statistical AnalysisSoftware Program) [10] was used to calculate Pearson’s correla-tion coefficients between the variables measured in the ESRDpopulation. The general linear model (GLM) procedure of SASwas used for the multivariate linear regression model in which theTGF-b1 level was considered as the dependent variable, andseveral variables such as sex, race, age, albumin, cholesterol andglucose that were not highly correlative among themselves (byPearson’s correlation analysis) were considered as independentvariables.
RESULTS
End-stage renal disease patient characteristics
Diabetes, hypertension and glomerulonephritis were the mostfrequent causes of ESRD in our study cohort, as it is in thegeneral U.S. dialysis population [1]. There were no significantdifferences between black and white patients with respect to thefrequencies of the different diseases responsible for their ESRD(P . 0.05 by Fisher’s exact test). As summarized in Table 1, therewere also no significant differences between black patients andwhite patients with respect to age, sex, years on dialysis, serumelectrolytes (Na, K, Cl, HCO3
2, Ca21, PO42), serum glutamic-
pyruvic transaminase (SGPT), alkaline phosphatase, albumin,cholesterol, glucose and hematocrit. Dialysis efficacy, as assessedby urea reduction ratio [11], was also similar in both groups (Table1). Plasma creatinine concentration and systolic, diastolic andmean arterial blood pressures were higher in the black cohortcompared to the white ESRD cohort.
Hyperexpression of transforming growth factor-b1 protein inthe black end-stage renal disease patients
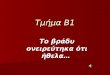
Transforming growth factor-b1 protein was detected in theperipheral blood of all 98 ESRD patients studied, and the mean 6SEM TGF-b1 concentration for the entire study group was 174 67 ng/ml (median value 5 169 ng/ml). The TGF-b1 protein levelwas higher in the black patients compared to their white counter-parts (Fig. 1). The mean 6 SEM TGF-b1 protein concentration was207 6 10 ng/ml in the 52 black ESRD patients (median value 5199 ng/ml); the concentration was 137 6 8 ng/ml in the 46 whiteESRD patients (median value 5 138 ng/ml). The race-dependentdifference in the circulating level of TGF-b1 protein in the ESRDgroup was significant at P 5 0.0001 by Student’s t-test.
We determined whether the race-dependent difference inTGF-b1 protein concentration was demonstrable in male as wellas female ESRD patients. Transforming growth factor-b1 proteinconcentrations in black male ESRD patients were significantlyhigher than that in white male ESRD patients (197 6 18 ng/ml,N 5 24 vs. 139 6 12 ng/ml, N 5 27, P 5 0.01). The TGF-b1
protein levels were also significantly higher in black female ESRDpatients compared to white female ESRD patients (215 6 12ng/ml, N 5 28 vs. 133 6 9 ng/ml, N 5 19, P 5 0.0000). The sex ofthe ESRD patients, independent of the race, did not affectcirculating TGF-b1 levels. The mean 6 SEM TGF-b1 protein levelin the males was 166 6 11 ng/ml (N 5 51) and was 182 6 10 ng/mlin females (N 5 47) (P 5 0.32 by Student’s t-test).
The hemodialysis membranes used in the hemodialyzers can becharacterized as “biocompatible” or “bioincompatible” mem-branes on the basis of their ability to activate diverse cell typesand/or complement components [12]. The bioincompatible mem-branes have been implicated in the increased expression ofproinflammatory cytokines such as IL-6 and TNF-a in ESRDpatients [8, 12]. Seventy (38 blacks and 32 whites) of the 98 ESRD
Table 1. Clinical and laboratory features of the end-stage renal disease(ESRD) patients
VariableBlack
(N 5 52)Whites
(N 5 46) P valuea
Age 56.9 6 2.1b 61 6 2.3 0.20Sex (M/F) 24/28 27/19 0.23Years on hemodialysis 6 6 0.9 4 6 0.7 0.15Sodium mmol/liter 138 6 0.5 139 6 0.4 0.70Potassium mmol/liter 4.9 6 0.1 5.0 6 0.09 0.59Chloride mmol/liter 99 6 0.5 99 6 0.5 0.65CO2 mmol/liter 23 6 0.5 23 6 0.5 0.86Glucose mg/dl 117 6 11 119 6 8 0.87Calcium mg/dl 9.3 6 0.1 9.5 6 0.1 0.76Phosphate, mgl/dl 6.2 6 0.3 5.7 6 0.3 0.23AST/SGPT units/liter 16 6 2 15 6 2 0.93Alk. phosphatase, units/liter 156 6 15 126 6 14 0.11Albumin g/dl 3.9 6 0.06 4.1 6 0.06 0.07Cholesterol, mg/dl 171 6 4 173 6 5 0.79Hematocrit 33.5 6 0.5 33.2 6 0.5 0.51Urea reduction ratio % 66 6 1 65 6 0.9 0.52Urea nitrogen mg/dl 66 6 2 74 6 3 0.06Creatinine mg/dl 11.0 6 0.4 9.2 6 0.4 0.004Systolic pressure mm Hg 152 6 3 141 6 3 0.03Diastolic pressure mm Hg 78 6 2 71 6 2 0.004Mean arterial pressure mm Hg 103 6 2 94 6 2 0.004
a P values based on Student’s t-test for continuous variables and onFisher’s exact test for categorical variables.
b mean 6 SEM.
Suthanthiran et al: TGF-b1 hyperexpression in ESRD patients640

patients were being dialyzed with the high-flux polysulfone mem-brane dialyzer (biocompatible dialyzer) and the remaining 28 (14blacks and 14 whites) were being dialyzed with the celluloseacetate membrane dialyzer (bioincompatible dialyzer).
We investigated (1) whether the race-dependent difference inTGF-b1 protein levels is demonstrable in ESRD patients dialyzedwith a biocompatible or a bioincompatible dialyzer, and (2)whether the type of dialysis membrane influenced TGF-b1 levels.This analysis demonstrated that black ESRD patients dialyzedwith either type of dialyzer had higher TGF-b1 levels compared towhite ESRD patients dialyzed with a similar dialyzer. BlackESRD patients dialyzed with a biocompatible dialyzer displayedsignificantly higher levels of TGF-b1 compared to white ESRDpatients dialyzed with the biocompatible dialyzer (202 6 13 ng/ml,N 5 38 vs. 147 6 9, N 5 32, P 5 0.001); black ESRD patientsdialyzed with a bioincompatible dialyzer also had higher levels ofTGF-b1 compared to white ESRD patients dialyzed with thebioincompatible dialyzer (217 6 17 ng/ml, N 5 14 vs. 111 6 12,N 5 14, P 5 0.0001). On the other hand, the type of dialyzer,independent of race, did not influence TGF-b1 protein concen-tration. The mean 6 SEM level of TGF-b1 protein in the group(black and white ESRD patients) dialyzed with the biocompatibledialyzer was 177 6 19 ng/ml (N 5 70) and the mean 6 SEM levelin those dialyzed with the bioincompatible dialyzer was 164 6 14ng/ml (N 5 28) (P 5 0.11 by Student’s t-test).
The association between TGF-b1 levels and race, and thecorrelation between TGF-b1 levels and other clinical and bio-chemical variables measured in the ESRD cohort were deter-mined using the correlation analysis procedure of SAS [10]. Theassociation between TGF-b1 levels and race was highly significant(correlation coefficient, r 5 0.460, P 5 0.0001); TGF-b1 levelswere also a significant correlate of mean arterial pressure (r 50.212, P 5 0.035). Race, in addition to TGF-b1 levels, was alsosignificantly associated with mean arterial pressure (r 5 0.282,P 5 0.004) and creatinine (r 5 0.288, P 5 0.004). In contrast,additional variables such as age, albumin, cholesterol, glucose,hematocrit, creatinine, blood urea nitrogen, urea reduction ratio,
and years of dialysis therapy were not significant correlates ofTGF-b1 levels.
Multivariate linear regression model of transforming growthfactor-b1 levels in end-stage renal disease patients
In a multivariate linear regression model, TGF-b1 was consid-ered as the dependent variable, and race and five other variables(sex, age, albumin, cholesterol, glucose) that did not correlatewith each other (by correlation analysis) were considered asindependent variables. The general linear model procedure ofSAS [10] was used, and Table 2 demonstrates that the race of theESRD patient is a significant (P 5 0.0001) determinant ofcirculating TGF-b1 protein level in this ESRD cohort.
The general linear model procedure also revealed that addi-tional renal related variables such as blood urea nitrogen, ureareduction ratio, serum creatinine, type of dialyzer, or years ondialysis are not significant determinants of circulating TGF-b1
levels in the ESRD cohort.
Hyperexpression of transforming growth factor-b1 in the blackend-stage renal disease patient is cytokine specific
Interleukin-6 is a multifunctional cytokine implicated in acuteand chronic inflammation [6]. Elevated levels of IL-6 have beenreported in patients with chronic renal failure and in ESRDpatients managed by chronic hemodialysis therapy [8]. Among the
Fig. 1. Differential level of expression oftransforming growth factor-b1 (TGF-b1)protein in black end-stage renal disease(ESRD) patients (u) and white ESRD patients(M). The mean 6 SEM TGF-b1 protein levelwas 207 6 10 ng/ml in black ESRD patients(N 5 52) and 137 6 8 ng/ml in white ESRDpatients (N 5 46) (A). The frequencydistribution of TGF-b1 levels in the ESRDpatients, distinguished by race, is shown in (B).A total of 96% of the TGF-b1 values fromblack ESRD patients were within 2 SD of themean value, and the coefficient of skewness andthe coefficient of kurtosis were 0.20 and 0.24,respectively; 93% of the TGF-b1 values fromwhite ESRD patients were within 2 SD of themean value, and the coefficient of skewness andthe coefficient of kurtosis were 0.38 and 0.78,respectively. In view of the normal distributionof TGF-b1 values in the black as well as whiteESRD patients, Student’s t-test was used toderive the P 5 0.0001 in (A).
Table 2. Multivariate linear regression model of transforming growthfactor-B1 levels in the ESRD cohort
Variable Beta SE 95% CI P value
Intercept 40.191 85.720 2127.81 to 208.202 0.6403Race 70.040 14.570 41.483 to 98.597 0.0001Sex 5.065 14.500 223.355 to 33.485 0.7278Age 0.134 0.460 20.768 to 1.035 0.7731Albumin 21.488 15.780 232.416 to 29.441 0.9251Cholesterol 0.050 0.190 20.323 to 0.422 0.8033Glucose 0.075 0.100 20.121 to 0.271 0.4600
Suthanthiran et al: TGF-b1 hyperexpression in ESRD patients 641

52 black ESRD patients studied, 7 patients had high levels of IL-6(32, 40, 102, 240, 307, 405, and . 500 pg/ml), and among the 42white ESRD patients, high IL-6 levels were detected in 7 patients(69, 164, 209, 237, 245, 269, and 296 pg/ml). In contrast to thesignificant difference between black and white ESRD patientswith respect to TGF-b1 protein levels, circulating IL-6 levels werenot significantly different between the black ESRD patients andthe white ESRD patients.
Tumor necrosis factor-a has been identified as both a circulat-ing factor as well as a cell-associated cytokine [7]. Implicated inendotoxic septic shock as well as in cachexia, TNF-a has beendetected in the sera of hemodialysis patients, and TNF-a over-production by peripheral blood mononuclear cells has beencorrelated with an immunocompromised state in ESRD patientstreated with hemodialysis [8, 13]. In the current study, high levelsof TNF-a protein were detected in 4 of 52 black ESRD patients(22, 25, 35, and . 1000 pg/ml) and in 4 of 46 white patients (53,53, 95, and 162 pg/ml).
DISCUSSION
The original observation that has emerged from this investiga-tion is that TGF-b1 is hyperexpressed in black ESRD patients.Our finding, in view of the multifunctional capabilities of TGF-b1,supports a new hypothesis for the excess burden of ESRD in theblack population.
Experimental data supporting a pathogenetic role fortransforming growth factor-b1 in progressive renal disease
A participatory role for the 25 kDa homodimeric polypeptideTGF-b1 in renal fibrosis has been demonstrated in a number ofelegant experimental models. Isaka and colleagues have demon-strated that in vivo transfection of the TGF-b1 gene (and not thatof the platelet-derived growth factor gene) results in glomerulo-sclerosis [14]. Akagi and colleagues have shown, in a rat experi-mental glomerulonephritis model, that a TGF-b1 antisense oli-gomer reduces the level of intrarenal expression of TGF-b1 andsuppresses extracellular matrix accumulation [15]. In mice withhigh levels of circulating TGF-b1 due to a TGF-b1 transgeneunder the control of an albumin promoter, mesangial expansion,glomerular immune deposits, extracellular matrix accumulation,interstitial fibrosis, and progressive renal disease have all beenobserved [16]. Moreover, fatal renal disease occurred in about25% of the TGF-b1 transgenic mice.
Renal implications of transforming growth factor-b1
hyperexpression in the black end-stage renal disease patients
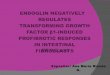
On the basis of the aforementioned compelling experimentaldata and on the basis of information that human renal diseaseincluding chronic renal allograft rejection is distinguished by highlevels of intrarenal expression of TGF-b1 [17–19], we offer thehypothesis that the heightened risk of progressive renal failure inthe black population is a consequence of increased TGF-b1
protein production (Fig. 2). In this conceptualization, hyperten-sion, diabetes or intrinsic renal diseases are envisioned as theinitial injury that elicits an exaggerated TGF-b1 response in thispatient population. This excessive reaction, then, results in theabnormal repair and remodeling that eventually lead to irrevers-ible renal failure. An exaggerated TGF-b1 response to an injuryrather than a pre-existing high TGF-b1 concentration in the blackpopulation is suggested here in view of our finding that TGF-b1
protein levels in normal blacks and normal whites are quite similar(68 6 6 ng/ml in 32 normal blacks vs. 64 6 5 ng/ml in 30 normalwhites), while being significantly (P , 0.001) less than that in theircounterparts with ESRD. That the level of expression of TGF-b1
protein distinguishes black ESRD patients from white ESRDpatients but not normal blacks from normal whites is reminiscentof an earlier observation that plasma endothelin-1 levels arehigher in the black hypertensives compared to white hyperten-sives, but not in the non-hypertensive blacks compared to whites[20].
An additional clinical setting in which TGF-b1 may play a rolein a progressive renal disease is human immunodeficiency virus(HIV) nephropathy, which is significantly more common in blacks[1]. In this regard, it is noteworthy that TGF-b1 can stimulate thereplication of HIV by several mechanisms [21]. Thus, the height-ened expression of TGF-b1 might be involved in initiating as wellas perpetuating injury.
Transforming growth factor-b1 hyperexpression: Implicationsfor hypertension and hypertensive renal disease
Hypertension is more prevalent in blacks compared to whites,and genetic as well as non-genetic hypotheses have been advancedto explain this observation [22, 23]. Polymorphisms in a number ofgenes related to blood pressure have been reported to be morecommon in blacks, including genes for mitochondrial proteins,angiotensinogen, angiotensin converting enzyme, and the a-2-adrenergic receptor [23]. In our investigation, TGF-b1 levelscorrelated with mean arterial blood pressure. Thus, our identifi-cation of heightened expression of TGF-b1 in blacks with ESRDsuggests a new mechanism for hypertension in blacks.
How might TGF-b1 contribute to the pathogenesis of hyper-tension? One potential pathway is via its ability to stimulate theexpression of endothelin-1, a potent vasoconstrictor and a smoothmuscle mitogen [24, 25]. Additional properties of TGF-b1 such asincreased biosynthesis of extracellular matrix components and
Fig. 2. Hypothetical model of transforming growth factor-b1 (TGF-b1)hyperexpression as a contributory factor for progressive renal insuffi-ciency. In this hypothesis for the pathogenesis of progressive renalinsufficiency, patients expressing high levels of TGF-b1 in response torenal injury are at an increased risk for progression. In this formulation,TGF-b1 expression is engendered by the primary insult (such as diabetes),and progressive renal insufficiency results from the heightened expressionof TGF-b1. Abbreviations are: DM, diabetes mellitus; GN, glomerulone-phritis; HT, hypertension; ESRD, end-stage renal disease.
Suthanthiran et al: TGF-b1 hyperexpression in ESRD patients642

induction of vascular smooth muscle hypertrophy and fibrocellu-lar hyperplasia [26, 27] might also contribute to abnormal remod-eling of the vasculature, narrowing of the vascular lumen andhypertensive vascular disease.
A perplexing clinical observation has been that aggressive bloodpressure control has not always led to similar renal benefits inblacks and in whites. Rostand et al have reported that renalfunction deteriorated more frequently in hypertensive black pa-tients compared to hypertensive whites despite similar levels ofblood pressure control [28]. Perry et al have noted a twofoldhigher risk of ESRD among black hypertensives compared totheir white counterparts [29]. Recent data from the MRFIT studyhave shown that for every level of blood pressure control, blacksare at an increased risk for the development of renal disease [2].Thus, the earlier observations [28, 29] and the recent supportingdata from the MRFIT study [2] suggest that there are factor(s) inaddition to hypertension that contribute to the association be-tween hypertension and ESRD in the black population. Based onour finding of increased TGF-b1 in blacks with ESRD, and ourobservation that TGF-b1 levels correlate with blood pressure, wesuggest that excess expression of TGF-b1 may explain the in-creased renal morbidity in hypertensive blacks compared withwhites. In this regard it is of interest that a high-salt diet results inincreased TGF-b1 expression and hypertensive renal injury in theDahl salt-sensitive rats [30], and that salt-sensitivity of bloodpressure is more frequent in the black hypertensives compared towhite hypertensives (75% vs. 55%) [31]. Also, renovascular resis-tance is reported to be higher in blacks with essential hypertensioncompared to their white counterparts [32], and arterial intimalfibroplasia is more accelerated in blacks compared to whites [33].Transforming growth factor-b1 can increase vascular resistancevia stimulation of endothelin-1 expression [5], and facilitatefibroplasia via its ability to increase extracellular matrix accumu-lation [3, 4].
Transforming growth factor-b1 hyperexpression: Implicationsfor end-stage renal disease patient outcome
Survival rates of black ESRD patients treated with chronicmaintenance hemodialysis are higher than that of their whitecounterparts [1]. This superior outcome is still apparent aftercorrection for a number of variables such as age, sex and cause ofrenal disease, which have all been shown to influence patientoutcome. The reason(s) for the better outcome is(are) not known.In view of the observation that TGF-b1 deficiency is associatedwith significant coronary artery disease [34], and in light of thedata that cardiovascular disease is a major reason for mortality inthe ESRD population [1], a provocative hypothesis is that thehigher TGF-b1 levels in the black ESRD patients protect, at leastpartially, from death due to coronary artery disease. In thisregard, it is noteworthy that the incidence of dialysis-acquiredischemic heart disease has been reported to be lower in blackESRD patients compared to white ESRD patients [35], and thatcoronary artery disease [36, 37] as well as mortality due tomyocardial infarction [38] are reported to be lower in black mencompared to white men.
Mechanisms for transforming growth factor-b1 hyperexpression
What might be the mechanism for differential levels of TGF-b1
expression? A genetic basis is a distinct possibility. Indeed,differential levels of expression of cytokines such as TNF-a and
IL-10 have been reported and have been linked to polymorphismsin the promoter regions of these genes [39–41]. With respect tothe TGF-b1 gene, at least seven polymorphisms have beenidentified [42]. However, none of these polymorphisms have yetbeen linked to the rate of transcription of TGF-b1 gene or to thelevel of expression of TGF-b1 protein.
Our hypothesis implicating TGF-b1 in the pathogenesis ofprogressive renal injury in patients with ESRD needs to beexplored with a larger patient base. Moreover, it would be ofinterest to correlate TGF-b1 levels and the rate of progression ofrenal disease, and test the postulate that high levels of TGF-b1 inpatients with diseases such as diabetes or hypertension, identifiesa priori, patients at risk for progression. The information regard-ing circulating levels of TGF-b1 might also help guide therapeuticdecisions. For example, blockade of the renin-angiotensin axismight be more efficacious in patients with high TGF-b1 protein,since angiotensin II is a potent stimulus for TGF-b1 expression[43]. Indeed, angiotensin II (Ang II) blockade with a convertingenzyme inhibitor or an Ang II receptor antagonist has beendemonstrated to reduce TGF-b1 mRNA expression as well astubulointerstitial fibrosis in a unilateral ureteral obstructionmodel [44]. In view of the data demonstrating the beneficialeffects of converting enzyme inhibitors in patients with diabeticnephropathy [45] as well as in patients with other primary renaldiseases [46], we speculate that therapy-associated decreasedlevels of TGF-b1 might be a contributory factor to the salutaryeffects of converting enzyme inhibitors in the clinic.
In conclusion, we have demonstrated in vivo hyperexpression ofTGF-b1 in the black ESRD population. In view of the potential ofthis multifunctional cytokine to induce renal fibrosis and progres-sive renal disease, as well as its association with peptides involvedin blood pressure regulation such as endothelin-1 and angiotensinII, we offer here the hypothesis that heightened TGF-b1 expres-sion is a mechanism for the increased prevalence of ESRD in theU.S. black population. Increased TGF-b1 may also contributeindependently to the pathogenesis of hypertension, or it maycontribute to the vascular complications of increased blood pres-sure. We also suggest that high levels of TGF-b1 in blacks may beassociated with certain beneficial clinical effects such as a lowerincidence of coronary heart disease, and that this may explain theobservations that survival of blacks is better than whites onhemodialysis. Future studies exploring polymorphisms in theTGF-b1 gene and their functional consequences might help toresolve the existing enigma of the increased risk of ESRD in theU.S. black population, as well as identify a risk factor forprogressive renal disease.
ACKNOWLEDGMENT
The authors are grateful to Ms. Linda Stackhouse for her meticuloushelp in the preparation of this manuscript.
Reprint requests to Manikkam Suthanthiran, M.D., The New York Hospi-tal-Cornell Medical Center, 525 East 68th Street, Box 3, New York, New York10021, USA.E-mail: [email protected]
REFERENCES
1. UNITED STATES RENAL DATA SYSTEM (USRDS): USRDS 1996 AnnualData Report. Bethesda, National Institutes of Health, NIDDK, 1996
2. KLAG MJ, WHELTON PK, RANDALL BL, NEATON JD, BRANCATI FL,STAMLER J: End-stage renal disease in African-American and whitemen. 16-year MRFIT findings. JAMA 277:1293–1298, 1997
Suthanthiran et al: TGF-b1 hyperexpression in ESRD patients 643

3. KLAHR S: Prevention of progression of nephropathy. Nephrol DialTransplant 12(Suppl 2):63–66, 1997
4. BORDER WA, NOBEL NA: Transforming growth factor-b in tissuefibrosis. N Engl J Med 331:1286–1292, 1994
5. KURIHARA H, YOSHIZUMI M, SUGIYAMA T, TAKAKU F, YANAGISAWAM, MASAKI T, HAMAOKI M, KATO H, YAZAKI Y: Transforming growthfactor b stimulates the expression of endothelin mRNA by vascularendothelial cells. Biochem Biophys Res Commun 159:1435–1440, 1989
6. VAN SNICK J: Interleukin-6: An overview. Annu Rev Immunol 8:253–278, 1990
7. TRACEY KJ, CERAMI A: Tumor necrosis factor: A pleiotropic cytokineand therapeutic target. Annu Rev Med 45:491–503, 1994
8. DESCAMPS-LATSCHA B, HERBELIN A: Long-term dialysis and cellularimmunity: A critical survey. Kidney Int 43(Suppl 41):S135–S142, 1993
9. KHANNA A, LI B, STENZEL KH, SUTHANTHIRAN M: Regulation of newDNA synthesis in mammalian cells by cyclosporine: Demonstration ofa transforming growth factor b dependent mechanism of inhibition ofcell growth. Transplantation 57:577–582, 1994
10. SAS INSTITUTE INC: SAS User’s Guide: Statistics (Version 5). Cary,SAS Institute, 1985, 956 pp
11. PARKER T: Hemodialysis adequacy, in Principles and Practice ofDialysis, edited by HENRICH WL, Baltimore, Williams & Wilkins,1994, pp. 63–75
12. HAKIM RM: Choice of the hemodialysis membrane, in Principles andPractice of Dialysis, edited by HENRICH WL, Baltimore, Williams &Wilkins, 1994, pp 1–7
13. GIRNDT M, KOHLER H, SCHIEDHELM-WEICK E, SHLAAK JF, MEYERZUM BUSCHENFELDE K-H, FLEISCHER B: Production of interleukin-6,tumor necrosis factor-a and interleukin-10 in vitro correlates with theclinical immune defect in chronic hemodialysis patients. Kidney Int47:559–565, 1995
14. ISAKA Y, FUJIWARA Y, UEDA N, KANEDA Y, KAMADAT, IMAI E:Glomerulosclerosis induced by in vivo transfection of transforminggrowth factor-b or platelet-derived growth factor gene into the ratkidney. J Clin Invest 92:2597–2601, 1993
15. AKAGI Y, ISAKAY, ARAI M, KANEKIT, TAKENAKA M, MORIYAMAT,KANEDA Y, ANDO A, ORITAY, KAMADA T, UEDA N, IMAI E: Inhibitionof TGF-beta 1 expression by antisense oligonucleotides suppressedextracellular matrix accumulation in experimental glomerulonephritis.Kidney Int 50:148–155, 1996
16. BOTTINGER EP, LETTERIO JJ, ROBERTS AB: Biology of TGF-b inknockout and transgenic mouse models. Kidney Int 51:1255–1360, 1997
17. YAMAMOTO T, NOBLE NA, COHEN AH, NAST CC, HISHIDA A, GOLDLI, BORDER WA: Expression of transforming growth factor-betaisoforms in human glomerular diseases. Kidney Int 49:461–469, 1996
18. IWANO M, KUBO A, NISHINO T, SATO H, NISHIOKA H, AKAI Y,KURIOKA H, FUJII Y, KANAUCHI M, SHIIKI H, DOHI K: Quantificationof glomerular TGF-beta 1 mRNA in patients with diabetes mellitus.Kidney Int 49:1120–1126, 1996
19. SHARMA VK, BOLOGA RM, XU G-P, LI B, MOURADIAN J, WANG J,SERUR D, RAO V, SUTHANTHIRAN M: Intragraft TGFb1 mRNA: Acorrelate of interstitial fibrosis and chronic allograft nephropathy.Kidney Int 49:1297–1303, 1996
20. ERGUL S, PARISH DC, PUETT D, ERGUL A: Racial differences inplasma endothelin-1 concentrations in individuals with essential hy-pertension. Hypertension 28:652–655, 1996
21. LOTZ M, SETH P: TGB-beta and HIV infection. Ann NY Acad Sci685:501–511, 1993
22. LACKLAND DT, KEIL JE: Epidemiology of hypertension in African-Americans. Semin Nephrol 16:63–70, 1996
23. GRIM CE, ROBINSON M: Blood pressure variation in blacks: Geneticfactors. Semin Nephrol 16:83–93, 1996
24. YANAGISAWA M, KURIHARA H, KIMURA S, TOMOBE Y, KOBAYASHI M,MITSUI Y, YAZAKI Y, GOTO K, MASAKI T: A novel potent vasocon-strictor peptide produced by vascular endothelial cells. Nature 332:411–415, 1988
25. BATTISTINI B, CHAILLER P, D’ORLEANS-JUSTE P, BRIERE N, SIROIS P:Growth regulatory properties of endothelins. Peptides 14:385–399, 1993
26. SALTIS J, AGROTIS A, BOBIL A: Regulation and interactions oftransforming growth factor-beta with cardiovascular cells: Implica-tions for development and disease. Clin Exp Pharmacol Physiol23:193–200, 1996
27. NABEL EG, SHUM L, POMPILI VJ, YANG ZY, SAN H, SHU HB, LIPTAY
S, GOLD L, GORDON D, DERYNCK R, NABEL GJ: Direct transfer oftransforming growth factor beta 1 gene into arteries stimulatesfibrocellular hyperplasia. Proc Natl Acad Sci USA 90:10759–10763,1993
28. ROSTAND SG, BROWN G, KIRK KA, RUTSKY EA, DUSTAN HP: Renalinsufficiency in treated essential hypertension. N Engl J Med 320:684–688, 1989
29. PERRY HM JR, MILLER JP, FORNOFF JR, BATY JD, SAMBHI MP,RUTAN G, MOSKOWITZ DW, CARMODY SE: Early predictors of15-year end-stage renal disease in hypertensive patients. Hypertension25:587–594, 1995
30. TAMAKI K, OKUDA S, NAKAYAMA M, YANAGIDA T, FUJISHIMA M:Transforming growth factor-beta 1 in hypertensive renal injury inDahl salt-sensitive rats. J Am Soc Nephrol 7:2578–2589, 1996
31. WEINBERGER MH: Hypertension in African Americans: The role ofsodium chloride and extracellular fluid volume. Semin Nephrol 16:110–116, 1996
32. BERGMAN SM, CURTIS JJ: Possible mediators in hypertension: Renalfactors. Semin Nephrol 16:134–139, 1996
33. TRACY RE: Renovasculopathies of hypertension and the rise of bloodpressure with age in blacks and whites. Semin Nephrol 16:126–133, 1996
34. GRAINGER DJ, KEMP PR, METCALFE JC, LIU AC, LAWN RM, WIL-LIAMS NR, GRACE AA, SCHOFIELD PM, CHAUHAN A: The serumconcentration of active transforming growth factor-beta is severelydepressed in advanced atherosclorisis. Nature Med 1:74–79, 1995
35. ROSTAND SG, KIRK KA, RUTSKY EA: Relationship of coronary riskfactors to hemodialysis-associated ischemic heart disease. Kidney Int22:304–308, 1982
36. KEIL JE, SUTHERLAND SE, HAMES CG, LACKLAND DT, GAZES PC,KNAPP RG, TYROLER HA: Coronary disease mortality and risk factorsin Black and White men. Arch Intern Med 155:1521–1527, 1995
37. PENISTON RL, ADAMS-CAMPBELL L, FLETCHER JW, WILLIAMS EC,MURIGANDE C, MENSAH E, CRITTENDEN MD DIGGS JA: Coronaryarteriographic findings in black patients and risk markers for coronaryartery disease. Am Heart J 127:552–559, 1994
38. OOI WL, BUDNER NS, COHEN H, MADHAVAN S, ALDERMAN MH:Impact of race on treatment response and cardiovascular diseaseamong hypertensives. Hypertension 14:227–234, 1989
39. WILSON AG, SYMONS JA, MCDOWELL TL, MCDEVITT HO, DUFF GW:Effects of a polymorphism in the human tumor necrosis factor alphapromoter on transcriptional activation. Proc Natl Acad Sci USA94:3195–3199, 1997
40. TURNER DM, WILLIAMS DM, SANKARAN D, LAZARUS M, SINNOTT PJ,HUTCHINSON IV: An investigation of polymorphism in the interleu-kin-10 gene promoter. Eur J Immunogenet 24:1–8, 1997
41. WESTENDORP RGJ, LANGERMANS JAM, HUIZINGATWJ, ELOUALI AH,VERWEIJ CL, BOOMSMA DI, VANDENBROUKE JP: Genetic influence oncytokine production and fatal meningococcal disease. Lancet 349:170–173, 1997
42. CAMBIEN F, RICARD S, TROESCH A, MALLET C, GENERENAZ L, EVANS A,ARVEILER D, LUC G, RUIDAVETS J-B, POIRIER O: Polymorphisms of thetransforming growth factor-beta 1 gene in relation to myocardial infarc-tion and blood pressure. The Etude Cas-Temoin de l’Infarctus duMyocarde (ECTIM) Study. Hypertension 28:881–887, 1996
43. KAGAMI S, BORDER WA, MILLER DE, NOBLE NA: Angiotensin IIstimulates extracellular matrix protein synthesis through induction oftransforming growth factor-beta expression in rat glomerular mesan-gial cells. J Clin Invest 93:2431–2437, 1994
44. ISHIDOYA S, MORRISSEY J, MCCRACKEN R, REYES A, KLAHR S:Angiotensin II receptor antagonist ameliorates renal tubulointerstitialfibrosis caused by unilateral ureteral obstruction. Kidney Int 47:1285–1294, 1995
45. LEWIS EJ, HUNSICKER LG, BAIN RP, ROHDE RD: The effect ofangiotensin-converting enzyme inhibition on diabetic nephropathy.The Collaborative Study Group. N Engl J Med 329:1456–1462, 1993
46. MASCHIO G, ALBERTI D, JANIN G, LOCATELLI F, MANN JFE, MO-TOLESE M, PONTICELLI C, RITZ E, ZUCCHELLI P: Effect of theangiotensin-converting enzyme inhibitor benazepril on the progres-sion of chronic renal insufficiency. N Engl J Med 334:939–945, 1996
Suthanthiran et al: TGF-b1 hyperexpression in ESRD patients644