-
Transfusion Medicine Quality Manual Standard Operating Procedure
for Rh Typing Tube
Method
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 2 of 12
Standard Operating Procedure for
Rh Typing Tube Method
1.0 Policy Statements
1.1 Each recipient blood sample for compatibility testing shall
be tested for Rh (D).
1.2 Rh (D) type shall be determined by phenotyping the
recipient’s red cells for the presence or absence of the D
antigen.
1.3 Red cells shall be tested with anti-D reagent. An Rh control
system, appropriate to the anti-D reagent in use must be
included.
1.4 The Transfusion Medicine Laboratory Technologist shall check
the prenatal status of the patient being tested.
1.5 Adult and pediatric specimens are tested with anti-D by
direct agglutination only. The test for weak D is not required.
1.6 Weak D testing shall be performed in the case of:
1.6.1 An Rh negative neonate of an Rh negative mother; and
1.6.2 To resolve discrepancies between current and previous
results.
1.7 All adult and pediatric samples that test Rh negative on
initial testing shall be confirmed Rh negative using a broad
reactivity anti-D reagent
(Novaclone anti-D, Bioclone anti-D).
1.8 Current and previous results should be compared to identify
any discrepancy. All discrepancies shall be resolved and the
resolution
documented before reporting.
1.9 If an Rh typing discrepancy is detected or in an emergency
situation:
1.9.1 Rh negative recipients should be transfused with Rh
negative red cells. Follow facility established policy for the
transfusion of Rh
positive red cells to an Rh negative recipient when Rh negative
red
cells are in diminished supply.
1.9.2 Rh negative women of child bearing age and children shall
receive Rh negative red cells, except for a life-threatening
situation and
when Rh negative red cells are not available.
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 3 of 12
Standard Operating Procedure for
Rh Typing Tube Method
1.9.3 Rh positive recipients may receive red blood cells that
are either Rh positive or Rh negative.
2.0 Linkages
Canadian Blood Services request for genotyping form. Available
at:
https://www.blood.ca/sites/default/files/requisition-for-blood-group-genotyping-
patient.pdf
Determining Specimen Suitability. Available at:
http://www.health.gov.nl.ca/health/bloodservices/pdf/determining_specimen_suitability.p
df
Patient History Check. Available at:
http://www.health.gov.nl.ca/health/bloodservices/pdf/patient_history_check.pdf
Patient Identification and Specimen Labeling. Available at:
http://www.health.gov.nl.ca/health/bloodservices/pdf/patient_id_and_specimen_labeling.
pdf
Preparation of Red Cell Suspensions. Available at:
http://www.health.gov.nl.ca/health/bloodservices/pdf/preparation_of_red_cell_suspensio
ns.pdf
Quality Control of Reagents and Antisera. Available at:
http://www.health.gov.nl.ca/health/bloodservices/pdf/quality_control_of_reagents_and_a
ntisera_ver1.pdf
Weak D Typing: Available at:
http://www.health.gov.nl.ca/health/bloodservices/pdf/sop_for_weak_d_typing.pdf
3.0 Scope 3.1 All Transfusion Medicine Laboratory
Technologists.
https://www.blood.ca/sites/default/files/requisition-for-blood-group-genotyping-patient.pdfhttps://www.blood.ca/sites/default/files/requisition-for-blood-group-genotyping-patient.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-determining-specimen-suitability.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-determining-specimen-suitability.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-patient-history-check.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-patient-id-and-specimen-labeling.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-patient-id-and-specimen-labeling.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-preparation-of-red-cell-suspensions.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-preparation-of-red-cell-suspensions.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-quality-control-of-reagents-and-antisera-ver1.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-quality-control-of-reagents-and-antisera-ver1.pdfhttps://www.gov.nl.ca/hcs/files/bloodservices-pdf-sop-for-weak-d-typing.pdf
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 4 of 12
Standard Operating Procedure for
Rh Typing Tube Method
4.0 General Information
4.1 Rh typing is a part of the forward blood group.
4.2 Pre-transfusion Rh testing is second only to ABO testing in
importance.
4.3 Due to changes in the Rh reporting process, there may be
occasions when patients were previously reported as Rh positive and
must now be reported
as Rh negative. A second sample may not be required to confirm
this change
because it is a result of an update in policy. The attached
physician memo
may be sent to the attending physician to assist in explaining
the change in
patients’ blood group.
4.4 Pre-washing the red cells is not necessary, however, if a
discrepancy is detected, the cells should be washed and the tests
repeated.
4.5 Agglutination less than grade 2 with anti-D requires further
investigation as the reactions may not be due to interaction
between reagents and test cells.
4.6 If two limited specificity anti-D reagents are used for
initial testing, (example Immucor series 4 and series 5), the
reaction strength should agree
within 2 grades or the patient should be investigated.
4.7 If indicated in the manufacturer’s insert, weak reactions
may be enhanced by incubating at room temperature for up to15
minutes.
4.8 False positive or negatives can be caused by variables such
as:
4.8.1 Improper technique;
4.8.2 Contaminated materials;
4.8.3 Omission of reagents or antisera;
4.8.4 Delays in reading tests;
4.8.5 Inadequate incubation time and temperature;
4.8.6 Inappropriate centrifugation;
4.8.7 Inappropriate or prolonged storage of red cells;
4.8.8 Rouleaux (may be eliminated by washing the red cells prior
to testing);
4.8.9 Polyagglutinable red cells; and
4.8.10 Autoantibodies.
4.9 Very weak reactions may indicate the presence of
quantitatively weak D or partial D antigen.
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 5 of 12
Standard Operating Procedure for
Rh Typing Tube Method
4.10 Anti-D reagents may not detect all examples of partial D.
Reagents may react with weak D cells and rare examples of partial D
cells that may have
previously been tested and interpreted as Rh negative using
other sources
of Anti-D.
4.11 It is recommended to note in the patients transfusion
history if testing using anti-D reagent is positive but
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 6 of 12
Standard Operating Procedure for
Rh Typing Tube Method
negative red cells. Positive control cells should be selected
to
represent weak expression of the specific antigen.
5.2 Procedure
5.2.1 Determine specimen suitability.
5.2.2 Centrifuge specimen.
5.2.3 Check specimen for abnormal appearance after centrifuging
(e.g. hemolysis).
5.2.4 Perform a patient history check.
5.2.5 Ensure patient information on the sample corresponds with
the patient information on the worksheet.
5.2.6 Label 2 tubes, one with the recipient’s identifier and
anti-sera reagent (A/D) and the other with the recipient’s
identifier and
control.
5.2.7 Add 1 drop of anti-D reagent and 1drop of control to the
appropriate labelled tubes.
5.2.8 Prepare a 3-5% recipient red cell suspension.
5.2.9 Add 1 drop of the recipient’s red cell suspension to each
tube.
5.2.10 Mix the contents of the tubes.
5.2.11 Centrifuge the tubes (speed and time as recommended by
manufacturer’s instructions).
5.2.12 Remove the tubes from the centrifuge. Verify that the
recipient’s identification on the tubes, specimens and worksheet
correspond.
If more than one recipient is being tested, read and record
results
on one recipient at a time.
5.2.13 Re-suspend the cell button.
5.2.14 Read macroscopically.
5.2.15 Grade and record results.
5.2.16 Reaction strength of 2+, 3+ and 4+ report as Rh
positive.
NOTE: If the result is negative or
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 7 of 12
Standard Operating Procedure for
Rh Typing Tube Method
5.2.17 Add 1 drop of Novaclone anti-D reagent and 1drop of
control to the appropriate labelled tubes.
5.2.18 Add 1 drop of the recipient’s red cell suspension to each
tube.
5.2.19 Mix the contents of the tubes.
5.2.20 Centrifuge the tubes (speed and time as recommended by
manufacturer’s instructions).
5.2.21 Remove the tubes from the centrifuge. Verify that the
recipient’s identification on the tubes, specimens and worksheet
correspond.
If more than one recipient is being tested, read and record
results
on one recipient at a time.
5.2.22 Re-suspend the cell button.
5.2.23 Read macroscopically.
5.2.24 Grade and record results. If positive 2+, 3+ or 4+ report
as Rh positive. If negative or < 2+ reaction:
5.2.24.1 Incubate tube at room temperature for 5 (five) minutes.
5.2.24.2 Centrifuge the tubes (speed and time as recommended
by manufacturer’s instructions).
5.2.24.3 Grade and record results. If positive 2+, 3+ or 4+
report as Rh positive. If negative report as Rh negative.
5.2.24.4 If the result is weak or 1+ refer to the table provided
in section 10 (ten) for Rh determination and reporting.
5.2.24.5 If the control tube is positive at any time during
testing, the results are invalid and must not be reported.
5.3 Guidelines (N/A)
5.4 Materials
5.4.1 Sample: 5.4.1.1 Blood sample collected in EDTA
anticoagulant. 5.4.1.2 Red cells from clotted sample. (SST tubes
with gel
separator should not be used).
5.4.1.3 Venous or capillary blood sample can be used for
neonates. Note: Cord blood must not be used for pre-transfusion
testing.
5.4.2 Reagents: 5.4.2.1 Anti-D reagent 5.4.2.2 Broad reactivity
Anti-D reagent (Novaclone D)
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 8 of 12
Standard Operating Procedure for
Rh Typing Tube Method
5.4.2.3 Diluent control or 6-8% bovine albumin 5.4.2.4 Isotonic
Saline
5.4.3 Supplies: 5.4.3.1 Test tubes (10x75mm)
5.4.3.2 Transfer pipettes
5.4.3.3 Test tube rack
5.4.4 Equipment:
5.4.4.1 Serological centrifuge
5.4.4.2 Timer
6.0 Acronyms
EDTA Ethylenediamine tetracetic acid anticoagulant
RBCs Red blood cells
SST Serum-separating tubes
RT Room temperature
7.0 Definitions
Rouleaux The stacking up of red blood cells caused by extra or
abnormal
proteins in the blood that decrease the normal distance red
cells
maintain between each other.
Compatibility testing Testing to determine if the donor's blood
is compatible with the
blood of an intended recipient.
8.0 Records Management
8.1 The recipient transfusion data file in the Transfusion
Medicine Laboratory shall be retained indefinitely.
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 9 of 12
Standard Operating Procedure for
Rh Typing Tube Method
8.2 All transfusion records in the recipient’s medical chart
shall be retained in accordance with health care facility
policy.
8.3 Quality control of blood components, blood products,
reagents and equipment shall be retained for 5 years.
8.4 Date and time of specimen collection and phlebotomist’s
identification shall be retained for 1 year.
8.5 Request form for serologic tests shall be retained for one
month or as per facility policy.
8.6 Documentation of staff training and competency must be kept
for a minimum of ten years.
9.0 Key Words
Forward blood group, Rh typing
10.0 Supporting Documents
10.1 Tables/Charts
Note: Neonate and cord samples require IAT weak D testing
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 10 of 12
Standard Operating Procedure for
Rh Typing Tube Method
10.1 Interpreting Rh Test Results: Rh control tube must be
negative for valid Rh type
LIMITED
SPECIFICITY
ANTI-D (routine
testing i.e. provue,
immucor series 4 and
series 5)
BROAD
REACTIVITY
ANTI-D
(NOVACLONE
D)
RESULT/INTERPRETATION
4+ Not required Rh positive
3+ Not required Rh positive
2+ Not required Rh positive
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 11 of 12
Standard Operating Procedure for
Rh Typing Tube Method
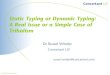
10.2 Process Flow/Algorithm
Process Flow for Rh Typing
Label Test Tubes
Add A/D reagent
to tube labeled
A/D
Prepare RBC
suspension
NL2012-033
Add RBC
suspension to
tubes
Mix contents of
tubes
Centrifuge tubes
Remove tubes
from centrfuge
Verify recipient’s
identification on
tubes, specimens
and worksheet match
Re-suspend cell
button
Read
Macroscopically
Grade and record
Interpret results
and compare to
previous reports
Rh
Discrepancy
Resolve
Discrepancy
before reporting
No
Yes
Yes
No
Add Rh control to
tube labeled
Control
Report Rh typing
as outlined in
table 10.1
If Rh neg or
-
Provincial Blood
Coordinating Program
_______________________________________________________________________
This document may be incorporated into each Regional
Policy/Procedure Manual.
NL2010.-009–TMQ
Version: 3.0
Effective Date: 2015-04-03
Page 12 of 12
Standard Operating Procedure for
Rh Typing Tube Method
References
American Association of Blood Banks, (2011). Standards for Blood
Banks and
Transfusion Services, (27th
ed.). Bethesda, MD: Author.
British Columbia Provincial Blood Coordinating Program. (2009,
January).ABO/D
Examination by tube Procedure. (Ver. 1.0). British Columbia:
Author.
Canadian Society for Transfusion Medicine, (2011). Standards for
Hospital
Transfusion Services, Version 3.0. Ottawa, ON: Author.
Canadian Standards Association, (2010). CAN/CSA-Z902-10, Blood
and Blood
Components. Mississauga, ON: Author.
Cooling L. ABO, H, and Lewis blood groups and structurally
related antigens. In: Fung
M, Grossman BJ, Hillyer CD, Westhoff CM, eds. Technical manual.
18th edition.
Bethesda, MD: AABB, 2014:291-315.
Immucor Gamma. (2012) Blood Grouping Reagent: Package
Insert.
Immucor Gamma. (2012) Reagent Red Cells; Package Insert.
Nova Scotia Provincial Blood Coordinating Program.Guidelines for
Rh Testing in Nova
Scotia (Ver. 1.0.DRAFT).). Halifax, NS: Author.