Embed Size (px)
Citation preview

Journal of Clinical Neuroscience 18 (2011) 910–915
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
Transient, symptomatic, post-operative, non-infectious hypodensity aroundthe deep brain stimulation (DBS) electrode
Milind Deogaonkar a,⇑, Jules M. Nazzaro b, Andre Machado a, Ali Rezai c
a Center for Neurological Restoration, Department of Neurosurgery, Cleveland Clinic Foundation, 9500 Euclid Avenue, S31, Cleveland, Ohio 44195, USAb Department of Neurosurgery, The University of Kansas Medical Center, Kansas City, Kansas, USAc Department of Neurosurgery, The Ohio State University, Columbus, Ohio, USA
a r t i c l e i n f o a b s t r a c t
Article history:Received 7 October 2010Accepted 6 November 2010
Keywords:Brain edemaComplicationDeep brain stimulationDystoniaHemorrhageParkinson’s disease
0967-5868/$ - see front matter � 2011 Elsevier Ltd. Adoi:10.1016/j.jocn.2010.11.020
⇑ Corresponding author. Tel.: +1 216 444 5188; faxE-mail address: [email protected] (M. Deogaonkar
Post-operative edema around a deep brain stimulation (DBS) lead is a rare presentation. Post-operativeedema that is symptomatic, self-limiting and not due to infection, in particular, is rarely reported as aseparate entity. We aim to discuss the morphological characteristics of post-operative edema around aDBS lead with an insight into possible etiologies and management. We present eight patients with symp-tomatic, self-limiting peri-electrode edema post-DBS electrode implantation who presented post-opera-tively with distinct clinical presentations with imaging that revealed a hypodense area in the whitematter surrounding the DBS electrode. Local and systemic tests for infection were negative. The edemaresolved over time without surgical intervention. The etiology of the edema remains obscure. The tran-sient nature of the edema and benign course with rapid and full resolution in all our patients cautionsagainst any hasty decision to explant the electrode, in the absence of any obvious signs of infection.
� 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Since the placement of the first deep brain stimulation (DBS)electrode in the thalamus,1 DBS has become an increasingly com-mon treatment option for disorders such as movement disor-ders,2–6 chronic pain disorders,7 epilepsy,8 minimally consciousstates,9 psychiatric disorders10 and is used increasingly for neuro-psychiatric disorders such as Gilles de la Tourette’s syndrome.11 Anincreasing number of targets and indications, variations in surgicaltechniques and use of microelectrode recordings (MER) can resultin an increase in the number and types of potential complicationsthat can occur as a result of DBS placement. The most commoncomplications include device-related failures, infections, hemor-rhage and neuropsychologic/psychiatric manifestions.6,12–14 Thereare no published reports of transient non-infectious, but symptom-atic, brain edema surrounding the DBS electrode that resolvedwithout intervention other than an occasional reference to it asischemia in published complications.15,16 The authors discuss eightpatients with this edema and hypothesize possible etiologies.
2. Methods
After Institutional Review Board approval, a retrospective chartreview of the eight patients who presented with peri-electrode
ll rights reserved.
: +1 216 444 1015.).
edema was carried out. The patients presented between 2004and 2009. Seven patients were operated in Cleveland Clinic andone was operated by JMN at an outside institution. Medical recordsof these patients were reviewed, with particular emphasis on thedemographic data, diagnosis, procedural details, time between sur-gery and appearance of edema, symptoms, diagnostic tests, inter-vention and days needed for radiological resolution of edema andclinical resolution of symptoms. Statistical analysis was performedusing the Student’s t-test.
2.1. Surgical technique for DBS
Although one patient was operated at a different institution, thebasic operating technique was similar. The surgical technique in allpatients consisted of stereotactic frame placement, MRI and CTscan acquisition, use of a stereotactic navigation system for ana-tomic targeting and trajectory planning and micro-electroderecording (MER) for physiological targeting. The basic componentsof DBS implantation surgery in all patients remained the same as inthe last 1000 lead placements done at our center, including frameplacement, burr-hole placement, physiological mapping, place-ment of DBS electrode and in a second stage, placement of implant-able pulse generator (IPG). The pre-operative planning was doneusing pre-operative MRI loaded into a surgical navigation com-puter and fused with the CT scan done after frame placement.The target of DBS placement was either the subthalamic nucleus(STN) or the globus pallidus internus (GPi). After trajectory

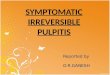
Fig. 1. Axial CT scan without contrast on post-operative day 4 at (a) the tip of the electrode, and (b) the subcortical level, showing a large hypodense area (edema) from theleft basal ganglia to the subcortical region around the left deep brain stimulation electrode.
M. Deogaonkar et al. / Journal of Clinical Neuroscience 18 (2011) 910–915 911
planning, the patient was placed supine on the operating table andthe frame attached to the table using an adaptor. Under local anes-thesia and intravenous sedation, a parasagittal linear incision wasmade and a burr-hole placed centered on the entry point. Once theburr hole was made, the intravenous sedation was stopped beforestarting the MER. Microelectrode mapping was then performedusing microelectrodes to accurately define the target structureand to allow for proper placement of the DBS lead. Finally acommercially available DBS electrode (either 3389 or 3387)(Medtronic, Minneapolis, MN, USA) was placed at the final target.Once in place, the distal end of the DBS lead was tunneled to theparietal region and placed in the subgaleal space. In the secondstage of the DBS procedure, the IPG was inserted under generalanesthesia either on the same day or in a staged fashion. A subcla-vicular pocket was used for the placement of the IPG, which wasthen connected to the DBS electrode using an extension wiretunneled from the parietal incision to the pocket.
2.2. Illustrative patients
2.2.1. Patient 1A 65-year-old right-handed woman with a history of idiopathic
Parkinson’s Disease (PD) was admitted for the placement of bilat-eral STN electrodes. She underwent the procedure using local anes-thesia and sedation. MER was performed using a micro-electrodeattached to the stereotactic frame and advanced through the brainwith a calibrated microdrive. Neuronal activity was recorded alongeach track. Single units were isolated and somatosensory re-sponses were determined. Three tracks of MER were performedon each side to map the anterior and lateral borders of the STN,starting 15 mm above the target, followed by placement of the per-manent electrode, model 3389 (Medtronic). The burr holes weresealed with fibrin glue between trajectories to minimize cerebro-spinal fluid (CSF) loss and subsequent pneumocephalus duringand after the procedure, respectively. An immediate post-operativeCT head scan revealed a small amount of pneumocephalus with noparenchymal hemorrhage. The patient was discharged on post-operative day 2 with a normal exam. Her second stage of surgeryfor IPG implantation was scheduled for a later date.
Four days after her surgical procedure, the patient presented toa local emergency room (ER) complaining of a new headache onthe top of her head that would not go away with prescribed pain
medications. Because the patient was confused, CT head scanwas obtained. This scan revealed a large hypodense area(4 cm � 4 cm � 6 cm) centered around the left DBS electrodeextending from the left basal ganglia to the subcortical region(Fig. 1). Upon admission to the hospital, a small subgaleal fluid col-lection over the left burr hole was noticed. The patient’s exam wasotherwise normal. No local or systemic signs or symptoms of infec-tion were present. The subgaleal fluid was aspirated and sent forgram stain, fungal (potassium hydroxide [KOH]) stain and bacterialcultures, all of which were negative. The clinical symptoms im-proved to baseline over the next 4 days and the patient was dis-charged home on a short course of oral steroids. Antibiotics werenot administered. A 1-week follow-up CT scan showed resolutionof the edema.
2.2.2. Patient 2A 69-year old left-handed male with a history of idiopathic PD
was admitted for placement of a right-sided STN electrode. Heunderwent the procedure using local anesthesia and sedation be-tween episodes of sensory and motor mapping. MER was per-formed using a platinum iridium micro-electrode attached to thestereotactic frame and advanced through the brain with a cali-brated microdrive. Neuronal activity was recorded along eachtract. Single units were isolated and somatosensory responseswere determined. Three tracks of MER were performed on eachside to map the anterior and lateral borders of STN, starting15 mm above the target, followed by placement of the permanentelectrode model 3389 (Medtronic). The burr holes were sealedwith fibrin glue between trajectories to minimize CSF loss and sub-sequent pneumocephalus. Immediate post-operative CT headscans revealed minimal pneumocephalus with no parenchymalhemorrhage. The patient was discharged on post-operative day 2with a normal examination. His second stage of surgery for implan-tation of the IPG was scheduled for a later date.
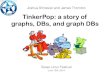
Two weeks after discharge, the patient presented to the emer-gency room with a history of a single generalized convulsion fol-lowed by a brief loss of consciousness. On examination he wasorientated and had no focal deficits. A CT brain scan revealed alarge hypodense area (3 cm � 4 cm � 3 cm) centered around theleft DBS electrode primarily in the subcortical region and centrumsemiovale that did not enhance on contrast administration (Fig. 2).No local or systemic signs or symptoms of infection were present.

Fig. 2. Axial CT scan without contrast on post-operative day 14 at the centrumsemiovale showing edema around the deep brain stimulation electrode at thesubcortical region.
912 M. Deogaonkar et al. / Journal of Clinical Neuroscience 18 (2011) 910–915
He did not have any further episodes of seizure and was dischargedhome on anti-convulsant medication and a short course of oral ste-roids. A follow-up CT scan after 1 week showed resolution of theedema. The patient was not given any antibiotics.
3. Results
Our eight patients did not differ in clinical profile, demograph-ics, procedure planning, procedure execution or post-operativecare from the rest of the patient cohort undergoing DBS (Table 1).The average age of these patients was 54 years (range: 21–73 years). Four patients were male and four were female. Five pa-tients underwent DBS for idiopathic PD and three for dystonia.Four patients underwent STN, and the remaining half, GPi im-plants. All patients underwent MER and an average of 3.75 tractsper implantation (range: 1–6 tracts). The clinical and radiologicalonset of edema was between 4 days and 120 days after surgery(average: 27 days). The location of edema was at the tip in threepatients, subcortical in two patients and at both locations in threepatients. The average maximum axial diameter of edema was 5 cm
Table 1Demographic, clinical, radiological and treatment details of all the eight patients with per
Patientno.
Age(years)
Sex Edema appearance(days after surgery)
Target No. MERtracts
Largest diameteedema (cm)
1 65 F 4 STN 3 62 69 M 21 STN 3 43 65 M 14 GPi 4 64 21 M 18 GPi 5 65 41 F 9 GPi 4 46 56 F 30 STN 6 67 73 F 7 STN 1 68 48 M 120 GPi 4 2
AED = anti-epileptic drugs, GPi = globus pallidus internus, MER = microelectrode recordi
(range: 2–6 cm). The edema resolved over an average of 33 days(range: 7–60 days). All patients were symptomatic with headaches(two patients), new neurological deficits (one patient), seizures(two patients) or worsening of pre-existing symptoms includingdyskinesia, gait and speech (three patients). All patients under-went systemic tests for infection including C-reactive protein,erythrocyte sedimentation rate and white blood cell counts, whichwere normal. In addition, two patients underwent tapping of fluidcollection at the burr hole sites that turned out to be CSF collec-tions without any evidence of infection. One patient underwent al-lergy testing to parts of the DBS lead, which was negative. Allpatients except one were treated with low-dose steroids for2 weeks to 3 weeks that resulted in complete resolution of the ede-ma. The patients presenting with seizures were started on anti-convulsant medication. The edema resolved over an average of33 days (range: 7–60 days). There was no correlation found be-tween the number of MER tracts to the size (p = 0.13, Student’s t-test) or timing (p = 0.11, Student’s t-test) of edema. However, thenumber of MER tracts was positively correlated with the durationof edema resolution (p = 0.004, Student’s t-test). There was no evi-dence of infection in any patient and no patient was treated withantibiotics.
4. Discussion
Although the presentation of all patients differed in some aspect(time of onset, clinical symptomatology), the CT scan appearance,transient nature and resolution with a short course of oral steroidswithout any further complications, point towards an identicalpathological process. Complications after DBS placement are com-mon and generally belong to distinct subgroups such as hemor-rhage, infection or hardware-related complication.12–14,17–20 Thecomplication we report does not belong to any of these groups.Although the clinical outcome in all these patients was satisfactory,the nature and etiology of this yet unreported phenomenon re-mains obscure.
The foremost possible etiology that was considered while treat-ing these patients was infection and cerebritis. Absence of any localor systemic pointers for infection, absence of fever, absence ofenhancement on the CT scan, normal acute phase reactants andwhite blood cell counts and resolution of the edema without anyspecific treatment ruled out infectious etiology. The fluid collec-tions around the burr hole site tapped in two patients yielded nor-mal CSF. Although infections are common after DBSimplantation,18,21 tracking of infection along the DBS lead in brainparenchyma is uncommon.22 The self-limiting of the edema andresolution without any antibiotics again suggests that it was notan infectious process. We use irrigating solutions that include di-lute Betadine (Purdue Products LP, Stamford, CT, USA) (povidoneiodine concentration about 1:10,000) and dilute bacitracin solution(about 25 IU/mL) at the end of the surgical procedure. Tracking of
i-electrode edema
r of Location Symptoms Intervention Days forresolution
Whole electrode Headache Steroids, tap 14Subcortical Seizure Steroids, AED 7Tip Headache Steroids 21Whole electrode Worsening of symptoms Steroids 30Tip Worsening of symptoms None 30Whole electrode Seizure Steroids, AED 42Subcortical Neurological deficits Steroids 60Tip Worsening of symptoms Steroids, tap 60
ng, STN = subthalamic nucleus

Fig. 3. Axial CT scan showing peri-electrode edema seen only near the tip of theelectrode used for deep brain stimulation.
M. Deogaonkar et al. / Journal of Clinical Neuroscience 18 (2011) 910–915 913
this solution along the lead resulting in chemical cerebritis andedema is a possibility, but we have used this procedure in morethan 1000 implantations without any increase in this complication.In addition, for the patient who underwent surgery at a differentinstitution (by JMN) sterile water without Betadine or bacitracinwas used for irrigation. Moreover, the time of onset, which variesfrom 4 days to 120 days, does not correlate with lead irrigationas a possible etiology.
Cortical venous infarction was considered as a second possibil-ity. Although cortical venous infarcts are known to occur afterDBS23, the clinical presentation is acute and radiological
Fig. 4. Axial T2-weighted brain MRI showing peri-electrode edema in
appearance is that of a cortical, subcortical typical wedge-shapedischemia.23 Isolated edema around the tip of the electrode seenin three patients (Fig. 3) is unlikely be due to a cortical venous in-farct. The cortical venous thrombosis on MRI always involves thecortical region and is wedge shaped,24,25 but MRI conducted onone of our patients at an outside hospital failed to show that distri-bution of edema (Fig. 4). The onset of symptoms, location and mor-phology of edema and absence of any neurological sequelae argueagainst the etiology to be cortical venous thrombosis.
Edema as a result of intra-operative micro-hemorrhages track-ing around the lead was also considered a possibility. The immedi-ate post-operative CT scan did not show any evidence of bleedingin any patient. Micro-hemorrhages and mechanical trauma due tomicro-electrodes and macro-electrodes leading to a blood–brainbarrier breakdown resulting in ‘‘luxury perfusion’’ remains a possi-bility. All patients had an MER-guided implantation with an aver-age of 3.75 tracks per implant. Using multiple, sequential MERtracks is routine at our centre and is part of our routine mappingprotocol to outline the anterior and lateral borders of the STNand the posterior and lateral borders of the GPi. An average of threeMER tracks per implant are used. Moreover, the numbers of MERtracks do not correlate with the onset or extent of edema in thisgroup of patients (p = 0.11 and p = 0.13 respectively, Student’s t-test). However, the time taken for resolution does correlate withthe number of MER tracks (p = 0.004, Student’s t-test) suggestinga mechanical reason for the appearance of edema. Time of onsetas delayed as 120 days and the varied morphology of edema cannot be explained based on this etiological hypothesis.
Another possible etiological consideration is an inappropriateimmune reaction, either in the form of a hypersensitivity or aller-genic response to the components of the DBS electrode. To addressthis issue, one patient underwent a comprehensive sensitivity testto the components of the DBS hardware, which did not result inany positive identification of allergy or inappropriate immune sen-sitivity to any lead component. Moreover in bilateral lead place-ment, only one side has resulted in edema, which counters anysuggestion of allergic origin of the edema.
Another possible etiological consideration is CSF tracking,which might create an intraparenchymal CSF collection. In one
the subcortical region sparing (a) the cortex and (b) near the tip.

Fig. 5. Morphological characteristics of the peri-electrode edema reconstructed on(a, b) sagittal CT brain scans and (c) sagittal MRI showing edema: (a) around the tip,(b) in the subcortical region and (c) sagittal around most of the electrode.
914 M. Deogaonkar et al. / Journal of Clinical Neuroscience 18 (2011) 910–915
patient, because the trajectory of the lead was through the ventri-cle, the possibility of a pressurized fluid collection tracking in thecerebral white matter or ‘‘intracerebral hygroma’’ was considered.Close proximity of the STN trajectory to the lateral ventricular wallcould result in an ependymal perforation and a resulting ball–valveaccumulation of CSF into the white matter.26 However, the trajec-tory was not near or traversed the ventricle in any other patient,thus refuting this etiological consideration.
The morphology of the edema was peculiar and could be classi-fied into: near the tip; in the subcortical region; or around the
whole electrode (Fig. 5). The edema was either oval or cylindricalin shape and was centered clearly around the electrode. The mor-phology did not correlate to the target, number of MER tracks, thetime of appearance or time taken for resolution, but it was corre-lated with clinical symptomatology. Edema around the tip primar-ily resulted in worsening of symptoms. Seizures or newneurodeficits were seen only if there was a subcortical component.
Treatment of the edema was conservative. A small dose of ste-roids (dexamethasone, 4 mg every 6 hours for 1 week) usuallyimproved the patients symptomatically and radiologically.Anti-epileptic drugs were given if there were seizures. No patientsneeded extraction of the hardware – this is an important point asany edema can look like an infection and lead to a hasty explanta-tion of the hardware.
In summary, this report aims to highlight this unusual phenom-enon of transient peri-electrode edema following DBS placement.The etiology of the edema remains obscure. The transient natureof the edema, and benign course with rapid and full resolution seenin all our patients, cautions against any hasty decision to explantthe electrode, in absence of any obvious signs of infection.
The exact mechanism of this phenomenon is not known, butwith the increasing number of DBS implants, we may learn moreabout this phenomenon.
References
1. Pool JL. Psychosurgery in older people. J Am Geriatr Soc 1954;2:456–66.2. Kupsch A, Benecke R, Muller J, et al. Pallidal deep-brain stimulation in primary
generalized or segmental dystonia. N Engl J Med 2006;355:1978–90.3. Benabid AL. Deep brain stimulation for Parkinson’s disease. Curr Opin Neurobiol
2003;13:696–706.4. Krause M, Fogel W, Kloss M, et al. Pallidal stimulation for dystonia.
Neurosurgery 2004;55:1361–8 [discussion 1368–1370].5. Deuschl G, Schade-Brittinger C, Krack P, et al. A randomized trial of deep-brain
stimulation for Parkinson’s disease. N Engl J Med 2006;355:896–908.6. Rezai AR, Machado AG, Deogaonkar M, et al. Surgery for movement disorders.
Neurosurgery 2008;62(Suppl 2):809–38.7. Bittar RG, Kar-Purkayastha I, Owen SL, et al. Deep brain stimulation for pain
relief: a meta-analysis. J Clin Neurosci 2005;12:515–9.8. Goodman JH. Brain stimulation as a therapy for epilepsy. Adv Exp Med Biol
2004;548:239–47.9. Schiff ND, Giacino JT, Kalmar K, et al. Behavioural improvements with thalamic
stimulation after severe traumatic brain injury. Nature 2007;448:600–3.10. Nuttin B, Gybels J, Cosyns P, et al. Deep brain stimulation for psychiatric
disorders. Neurosurg Clin N Am 2003;14:xv–xvi.11. Flaherty AW, Williams ZM, Amirnovin R, et al. Deep brain stimulation of the
anterior internal capsule for the treatment of Tourette syndrome: technicalcase report. Neurosurgery 2005;57(4 Suppl):E403 [discussion E403].
12. Beric A, Kelly PJ, Rezai A, et al. Complications of deep brain stimulation surgery.Stereotact Funct Neurosurg 2001;77:73–8.
13. Hariz MI. Complications of deep brain stimulation surgery. Mov Disord2002;17(Suppl 3):S162–6.
14. Deogaonkar M, Boulis N, Machado A, et al. Surgical complications in 800consecutive DBS implants. J Neurosurg 2007;106:A774.
15. Voges J, Waerzeggers Y, Maarouf M, et al. Deep-brain stimulation: long-termanalysis of complications caused by hardware and surgery–experiences from asingle centre. J Neurol Neurosurg Psychiatry 2006;77:868–72.
16. Novak KE, Nenonene EK, Bernstein LP, et al. Two cases of ischemia associatedwith subthalamic nucleus stimulator implantation for advanced Parkinson’sdisease. Mov Disord 2006;21:1477–83.
17. Spiotta AM, Bain MD, Deogaonkar M, et al. Methods of scalp revision for deepbrain stimulator hardware: case report. Neurosurgery 2008;62(3 Suppl):249–50 [discussion 250].
18. Sillay KA, Larson PS, Starr PA. Deep brain stimulator hardware-relatedinfections: incidence and management in a large series. Neurosurgery2008;62:360–6 [discussion 366–367].
19. Bhatia S, Oh M, Whiting T, et al. Surgical complications of deep brainstimulation. A longitudinal single surgeon, single institution study. StereotactFunct Neurosurg 2008;86:367–72.
20. Oh MY, Abosch A, Kim SH, et al. Long-term hardware-related complications ofdeep brain stimulation. Neurosurgery 2002;50:1268–74 [discussion 1274–1266].
21. Blomstedt P, Hariz MI. Hardware-related complications of deep brainstimulation: a ten year experience. Acta Neurochir (Wien) 2005;147:1061–4.
22. Merello M, Cammarota A, Leiguarda R, et al. Delayed intracerebral electrodeinfection after bilateral STN implantation for Parkinson’s disease. Case report.Mov Disord 2001;16:168–70.

M. Deogaonkar et al. / Journal of Clinical Neuroscience 18 (2011) 910–915 915
23. Umemura A, Jaggi JL, Hurtig HI, et al. Deep brain stimulation for movementdisorders: morbidity and mortality in 109 patients. J Neurosurg2003;98:779–84.
24. Kawaguchi T, Kawano T, Kaneko Y, et al. Classification of venous ischaemiawith MRI. J Clin Neurosci 2001;8(Suppl 1):82–8.
25. Nakase H, Shin Y, Nakagawa I, et al. Clinical features of postoperative cerebralvenous infarction. Acta Neurochir (Wien) 2005;147:621–6 [discussion 626].
26. Koizumi H, Fukamachi A, Nukui H. Postoperative subdural fluid collections inneurosurgery. Surg Neurol 1987;27:147–53.