Embed Size (px)
Citation preview

1
TRANSITIONS: Improving Care for High-Risk Medicaid Beneficiaries
in Tompkins County
Aging Concerns Unite Us ConferenceJune 7, 2016
Lisa Holmes, Tompkins County Office for the Aging
Sue Ellen Stuart, Visiting Nurse Services of Ithaca and Tompkins County

2
Why Care
Transitions?
3
National Data on Hospital Readmissions
New England Journal of Medicine (2009):
� Nationally, 1 in 5 Medicare beneficiaries are readmitted within 30 days following hospitalization
� Medicare cost of over $17 billion annually
� Heart failure, pneumonia, COPD were among most frequent medical diagnoses of patients readmitted
� Half of patients readmitted had no physician contact within 30 days post- discharge
4
National Data on Hospital Readmissions
� Medicaid patients have readmission rates as high or higher than Medicare patients
� 25% of Medicare patients with CHF returned to hospital in 30 days; 33% Medicaid patients.
� Medicaid readmission patterns: more behavioral health conditions, socio-economic factors affecting access, substance abuse.
Agency for Healthcare Research and Quality
5
Tompkins County’s Previous Care Transitions Experience
� CMS Community Based Care Transitions Program (CCTP) 2012-2014
� Goal: To reduce hospital readmissions among Medicare FFS beneficiaries by 20%
� Strategy: Collaboration of multiple community agencies facilitated and led by Tompkins County Office for the Aging: including VNS, Hospice, Cayuga Medical Center

6
CCTP Partners
� Tompkins County Office for the Aging: lead agency, coordination, reporting, billing
� Cayuga Medical Center– community hospital
� Visiting Nurse Services– coaching
� Hospicare– coaching
7
Care Transitions Intervention™
� Developed by Dr. Eric Coleman of the University of Colorado
� Designed to encourage older patients and their caregivers to assert a more active role during care transitions
Low cost ▪ Low intensity ▪ Easily adaptableShort – 30 days – with 1 home visit and 3 phone calls
8
The “Four Pillars” of CTI
� Transitions Coach is used to build skills, confidence and to provide tools to support self-management
� Model behavior for common problems
� Practice or role play for health care encounters
� Create an accurate medication list
� Transitions Coach is used to build skills, confidence and to provide tools to support self-management
� Model behavior for common problems
� Practice or role play for health care encounters
� Create an accurate medication list
1. Medication self-management
2. Follow-up with PCP/Specialist
3. Knowledge of “red flags” or warning signs/symptoms and how to respond
4. Patient-centered medical record
9
Tompkins CCTP: Challenges and Lessons Learned
� Challenge: Low patient volume� Smallest CCTP site in nation, small rural hospital
� Could only bill for Medicare FFS inservice patients
(no Medicare Advantage or observation stays)
� Restrictive eligibility based on patient diagnosis: originally CHF, COPD, Pneumonia; later CMS granted permission to broaden criteria to include additional diagnoses, age, polypharmacy and social factors
� Lesson Learned: Cast a wide net� Broaden targeting criteria to be all-inclusive
10
Tompkins CCTP: Challenges and Lessons Learned
� Challenge: Patient identification and referral� Few referrals among hospital discharge planners
� Turnover among key hospital staff and leadership
� No direct access to charts/ medical records
� Communication of protected health information between partners a challenge
� Lesson Learned: Embed transitions staff in hospital system
� Staff credentialing at hospital (this took a “champion”)
� Daily rounds
� Access to electronic medical records
11
Tompkins CCTP: Challenges and Lessons Learned
� Challenge: Too many cooks� Two agencies involved in hospital case finding and in-
home coaching
� Complex communication, information dropped
� Paid per coaching session: agencies losing money on staff time in rounds
� Lessons Learned: Streamline� Right-size program to one agency
12
Tompkins CCTP: Challenges and Lessons Learned
� Challenge: Patient acceptance of intervention
� Patients declining intervention in hospital
� Patients accepting in hospital, declining when home
� Lesson Learned: Present program as standard part of discharge
� Schedule home visit while in hospital if possible
� Utilize same person to introduce program to patient to conduct home visit when possible
13
Tompkins CCTP Results
� Goal: reduce hospital readmissions of Medicare patients by 20% in 2 years
� Program served 85 patients total
� Though good results for individual patients, not enough volume to create impact
� CCTP contract period ended 5/31/14
14
15
…From CCTP…to BIP
� BIP Innovations Fund: NYSDOH
� Target: Medicaid beneficiaries
� Goal: To increase access to community-based care options over institutional settings
� Tompkins submitted application: May, 2014
� Notification of grant award: July, 2014
� Start of service: Sept. 2014
16
Structure of BIP Transitions Program
� Tompkins County Office for the Aging: lead organization, coordination, reporting.
� Cayuga Medical Center– community hospital
� Visiting Nurse Service– coaching
� CAP CONNECT– clinical integration organization, marketing, outreach, data analytics
17
Structure of BIP Transitions Program
� Studied hospital data on Medicaid readmission patterns
� In addition to chronic diseases, behavioral health issues, substance abuse, health literacy issues, barriers in accessing community supports
� Modified model to suit needs of Medicaid patients
18
Structure of BIP Transitions Program
� Modified Coleman approach: 1 or more home visits by an RN with physician’s order
� Importance of medication reconciliation by RN
� Medicaid-reimbursable service: sustainable after grant period ends
� Available to ALL Medicaid patients who could benefit
� Including behavioral health patients
� Including patients discharged home from 2 large skilled nursing facilities
� Referrals accepted from community physicians
19
Goals of BIP Transitions Program
1) Raise awareness of Transitions Program among clinical partners/referral sources
� Outreach through CAP Connect
2) Foster case finding and patient introduction to Transitions Program
� Active involvement at daily rounds by VNS
20
Goals of BIP Transitions Program
3) Improve health outcomes and reduce avoidable 30 and 90 day ED visits and inpatient admissions� Serve Medicaid beneficiaries with 1+ home visits by
Transitions nurse, using modified Coleman approach
4) Ensure program stability beyond grant period� Establish referral patterns to ensure program is
regularly utilized beyond grant period

21
BIP Transitions Program Marketing
22
BIP Transitions Program Marketing

23
BIP Transitions Program Marketing

24
Patient Testimonials
�Vaness
�Joanne
�Andrew
�Martha
�Vaness
�Joanne
�Andrew
�Martha
25
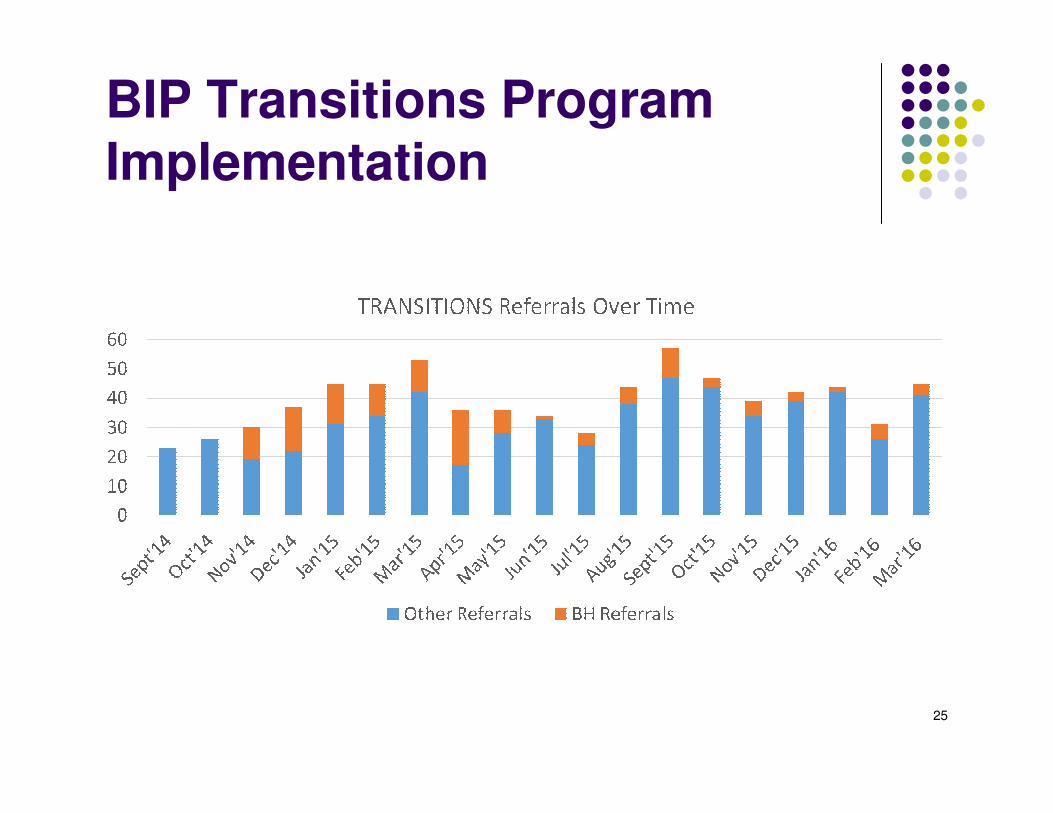
BIP Transitions Program Implementation
26
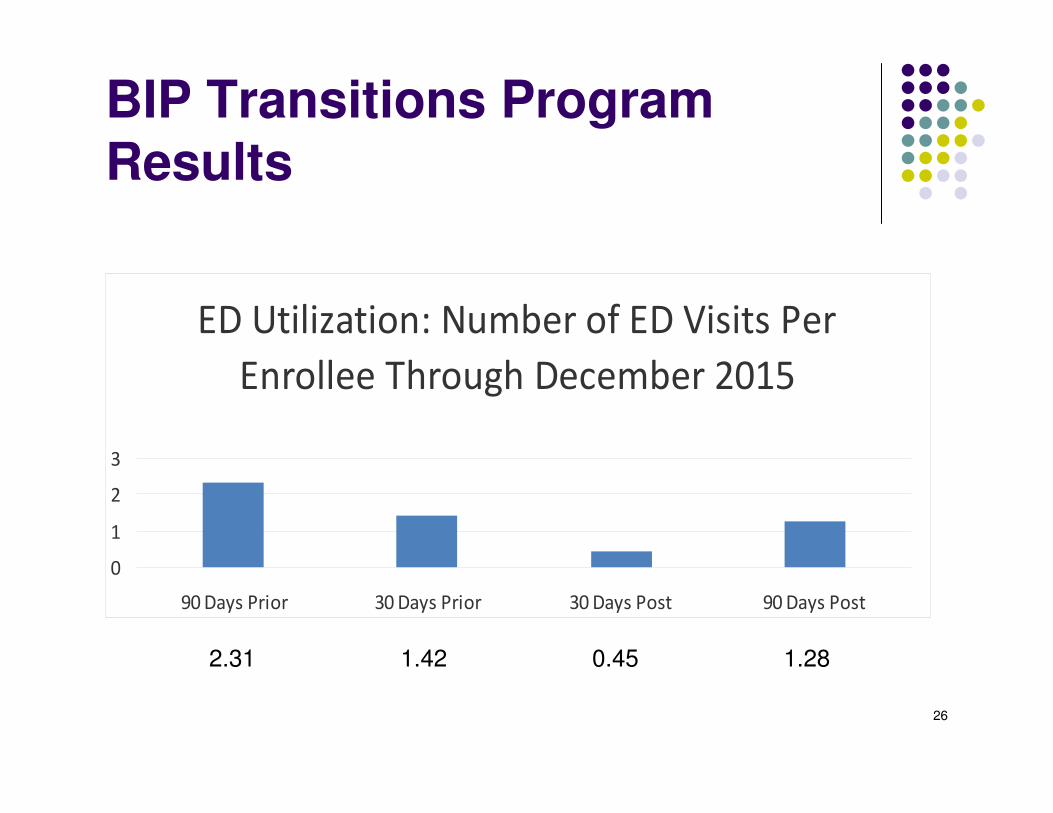
BIP Transitions Program Results
ED Utilization: Number of ED Visits Per
Enrollee Through December 2015
0
1
2
3
90 Days Prior 30 Days Prior 30 Days Post 90 Days Post
2.31 1.42 0.45 1.28
27
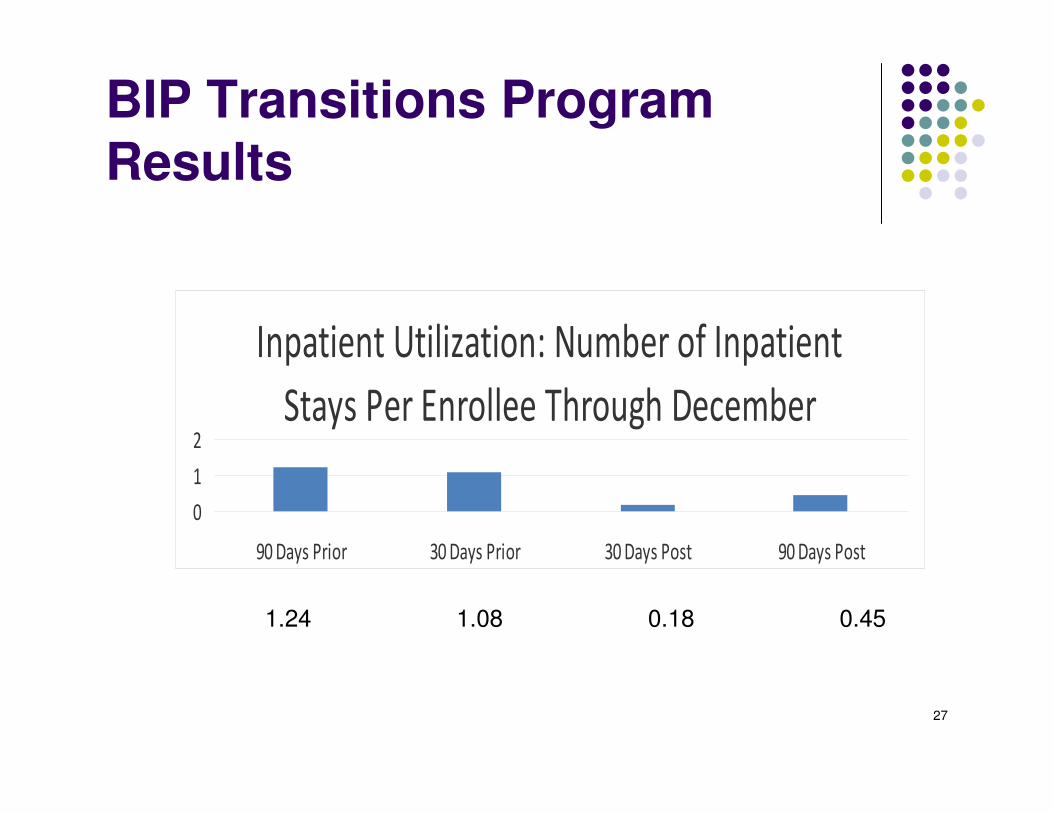
BIP Transitions Program Results
1.24 1.08 0.18 0.45
Inpatient Utilization: Number of Inpatient
Stays Per Enrollee Through December
0
1
2
90 Days Prior 30 Days Prior 30 Days Post 90 Days Post
28
BIP Transitions Program Results
Estimated program savings through December 31st, 2015
• ED visits per patient 90 days prior to enrollment = 2.31
• ED visits per patient 90 days post enrollment = 1.28
• Estimated ED visits prevented = 1.03 visits
• Number of patients enrolled = 137
• Average charges for a Medicaid ED visit* = $350.00
• Estimated program savings related to preventable ED visits =
$49,388.50
*This number based on the average charges for a Medicaid ED
visit based on the 2013 Medicaid fee schedule
29
BIP Transitions Program Results
Estimated program savings through December 31st, 2015
• Inpatient admissions per patient 90 days prior to enrollment =
1.24
• Inpatient admissions per patient 90 days post enrollment =
0.45
• Estimated Inpatient admissions prevented per patient = 0.79
• Number of patients enrolled = 137
• Average charges for a Medicaid inpatient visit* = $3,000.00
• Estimated program savings related to preventable inpatient
admissions = $324,690.00
*This number based on the average charges for a Medicaid
inpatient visit based on the 2013 Medicaid fee schedule
30
BIP Transitions Program Results
Estimated total cost savings from
September 2014 through
December 31st, 2015:
$374,078.50
31
The Future of the Transitions
Program
� Program infrastructure and procedures remain in place
� Transitions will be the model used for DSRIP Care Transitions project in Tompkins County
� Program details shared with Care Compass Network for consideration throughout DSRIP PPS.
32
VNS Role
1. Pt. Identification & Hospital Visit 2. Home Visits3. Follow up Phone Calls4. Referrals to other agencies5. Integrating techniques to enhance results such as motivational interviewing
33
Identification of Medicaid Recipients
� Access & Review Hospital Census each morning
� Identify all newly admitted Medicaid patients
� Review identified patients at hospital rounds and discuss with discharge planning team to identify patients appropriate for the program.
34
Approach Medicaid Patient in the hospital about the program
� It has been determined through the Coleman project that the program is more successful if the same person making the home visits also approaches the patient in the hospital.
� This begins to develop trust in the relationship and more success in ensuring the home visit.
� There is usually a 50% acceptance rate.
35
Transitions Nurse called discharged
patient and set up visit within 3 days of discharge
� This has been a challenge for the program!
� Medicaid recipients tend to be more mobile and not as likely to answer their phones or to be reached (or found) after discharge.
� Early in the program, Transitions RN would visit even if not reached on the phone first usually without success and this practice was stopped.
� Saw on average, 39% of patients that accepted the program in the hospital.
36
Home Visit
Based on Four Pillars of CTI
1. Medication self-management
2. Follow-up with PCP/Specialist
3. Knowledge of “red flags” or warning signs/symptoms and how to respond
4. Patient-centered medical record
37
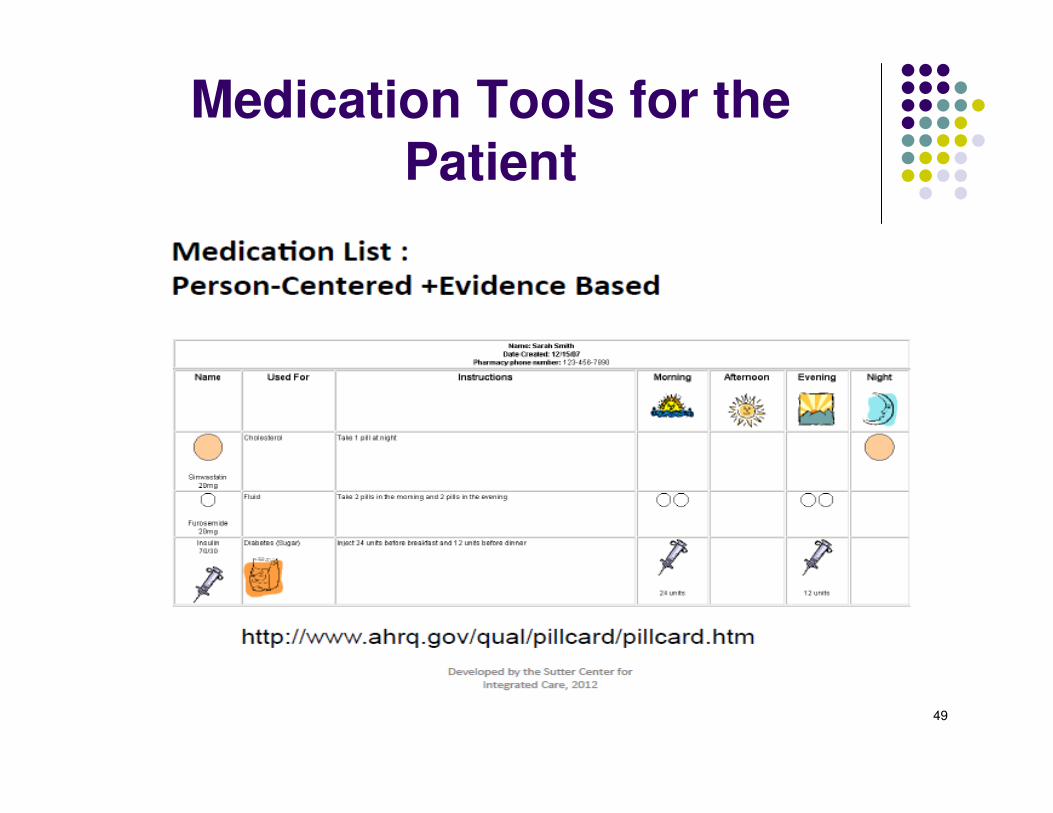
MEDICATION RECONCILIATION
The key for our project was medication reconciliation by an RN which differed from the Coleman Model which did not require an
RN for the coach.
38
39
40
41
42
43
used. It is the responsibility of the nurse to Call the physician to reconcile any discrepancies
44
45
46

47
48
49
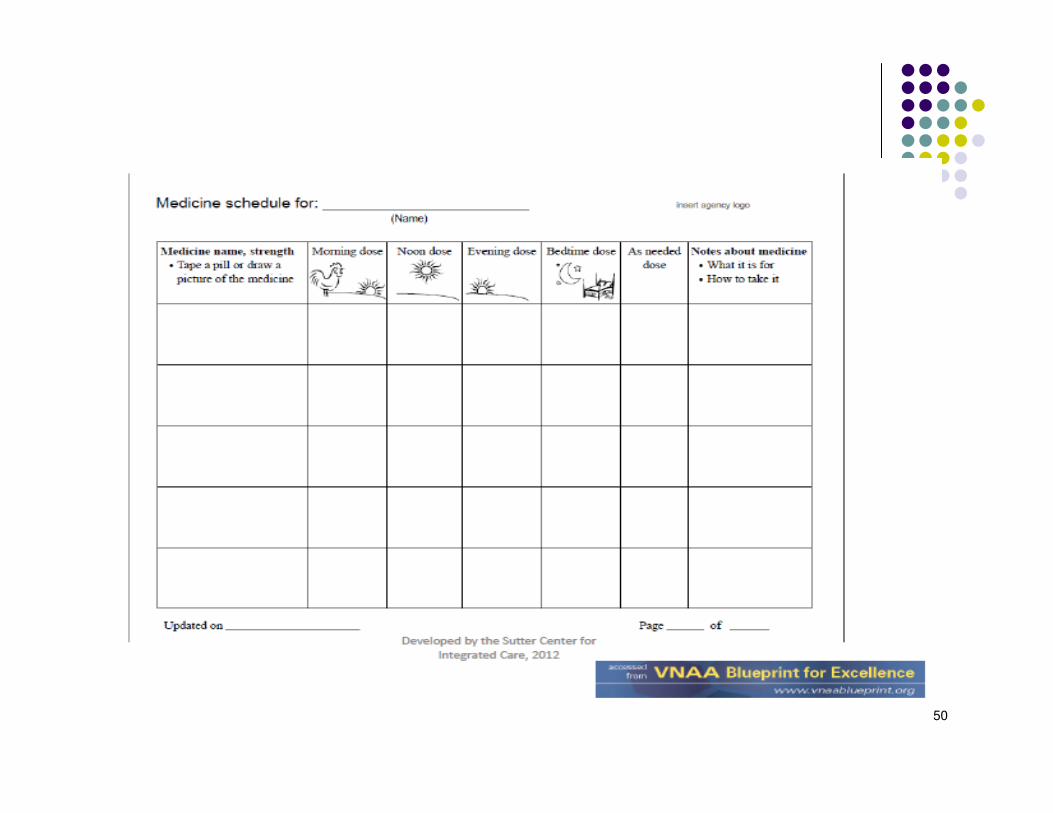
Medication Tools for the Patient
50

51
Steps to assure MD appointment
� Ascertain whether patient has a follow-up appointment with MD
� Confirm appropriate MD responsible managing patients
� Work with patient to schedule the appointment
� Discuss barriers to appointment including transportation and scheduling with family member, caregiver or friend
� Confirm/assist with transportation arrangements
� Provide appointment reminders and work with patient to put appointment information in a convenient place
� Confirm patient’s use of personal health record
� Use coaching to encourage patient/caregiver to understand importance of scheduling the appointment
� Confirm that patient understands to take medication list
52
Physician Visit
53
Knowledge of “red flags” or warning signs/symptoms and how to respond
Red Flags worksheets are disease specific
Many free resources to find Red Flags including :
54
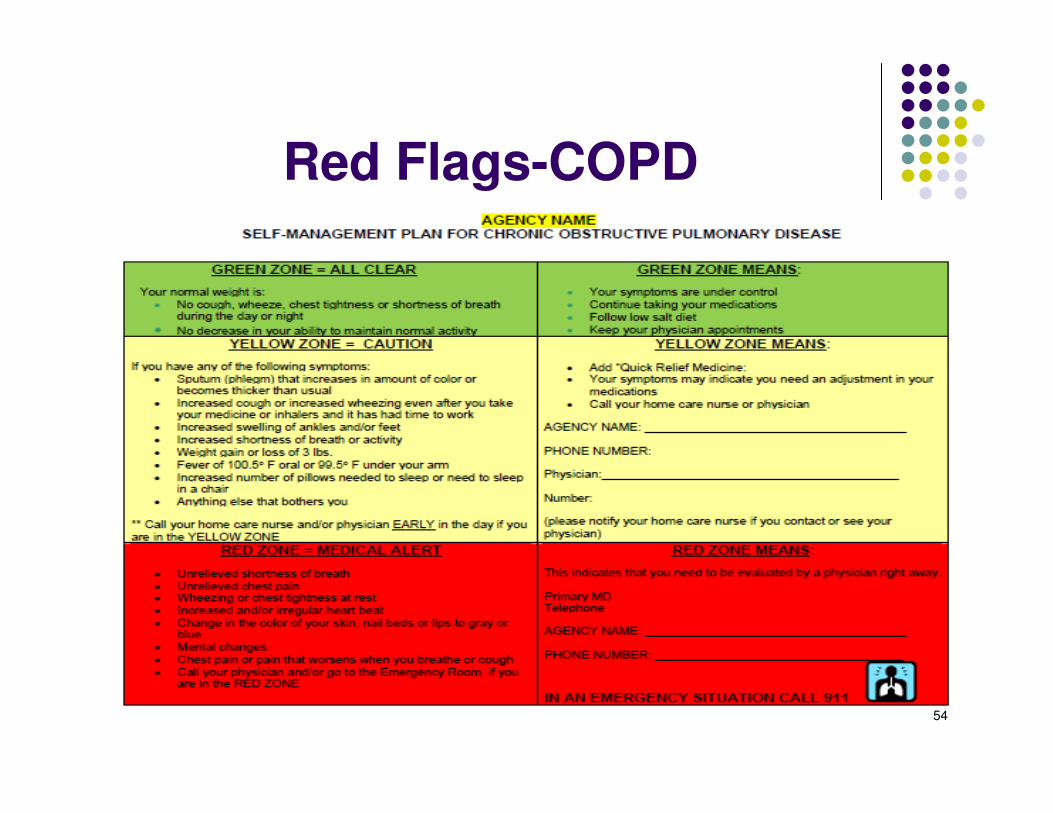
Red Flags-COPD
55
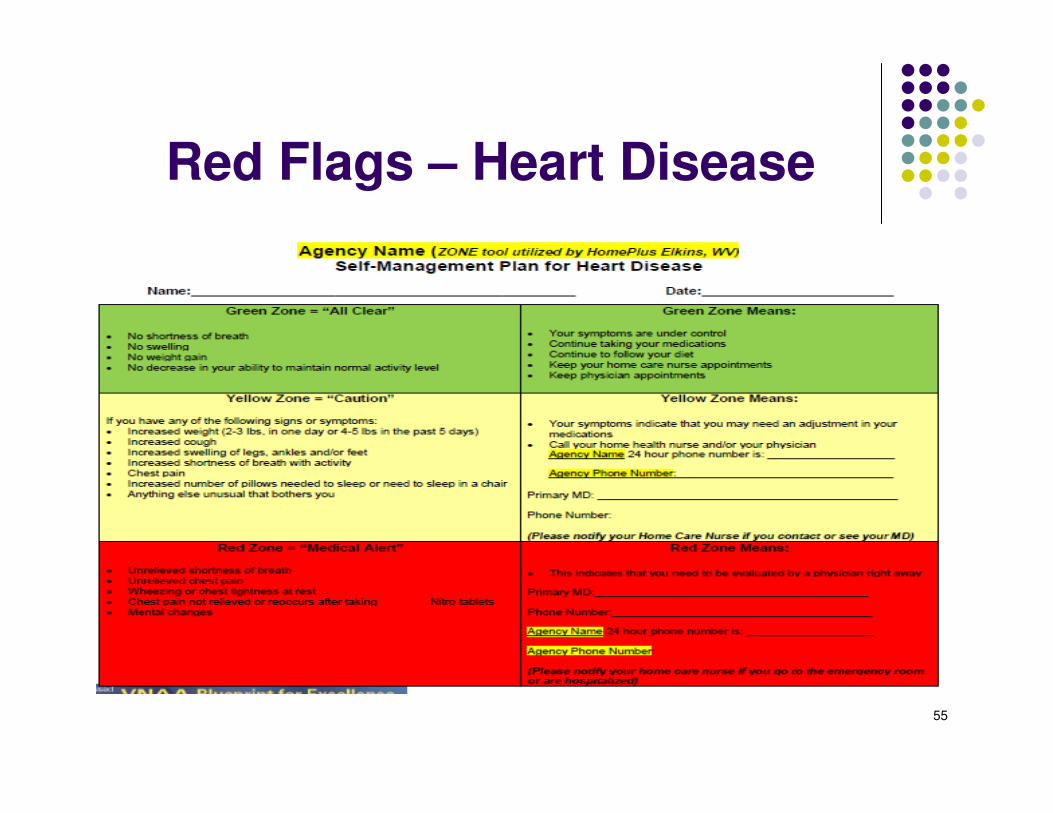
Red Flags – Heart Disease
56
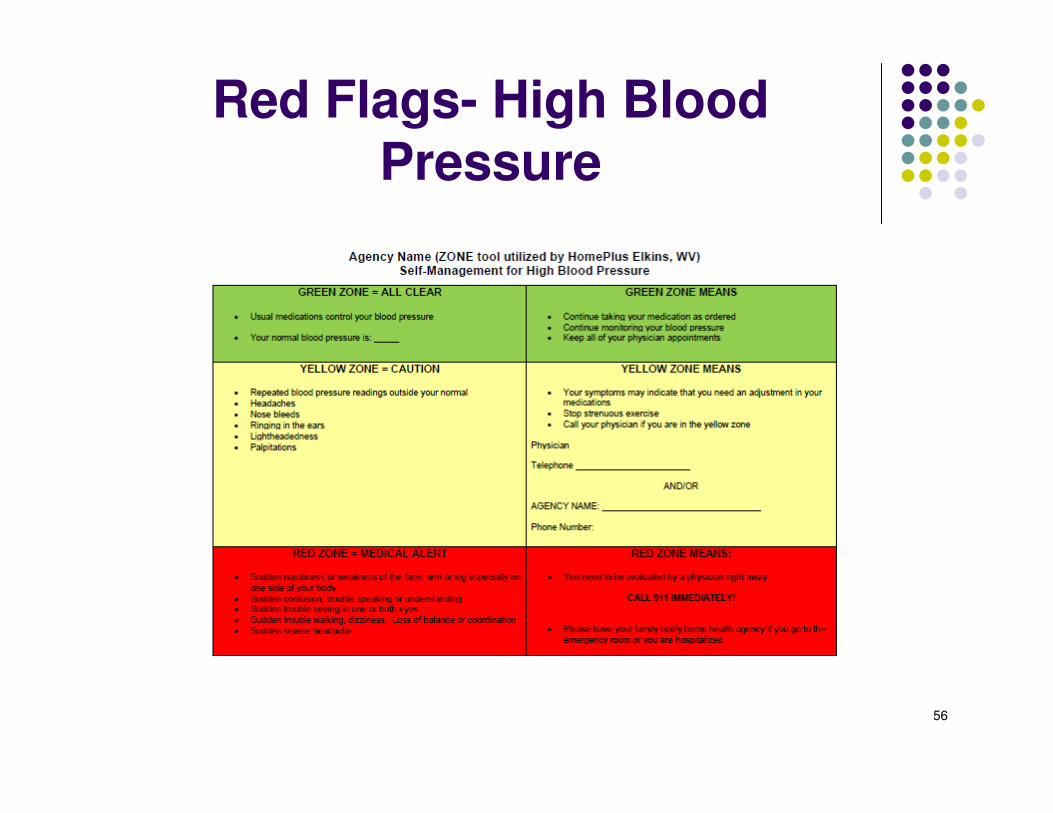
Red Flags- High Blood Pressure
57
Personal Health Record
Booklet given to Patient to take to
MD visits.
Coach Provides Assistant to
complete
58
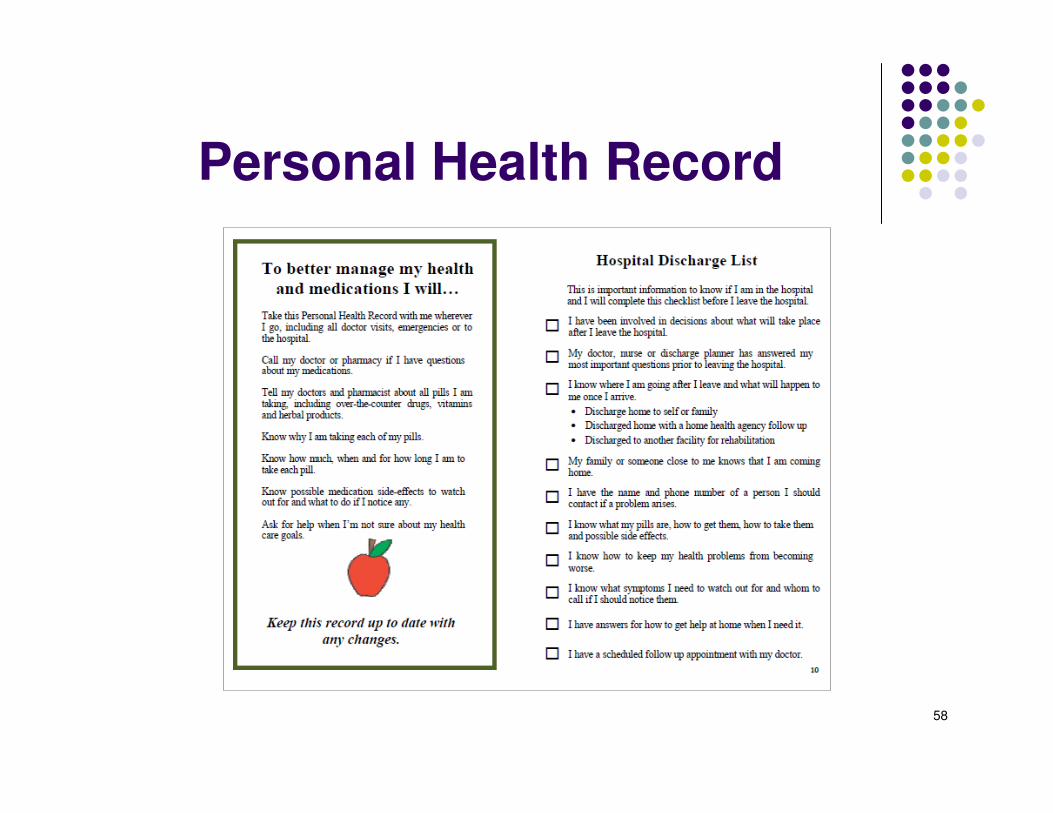
Personal Health Record
59
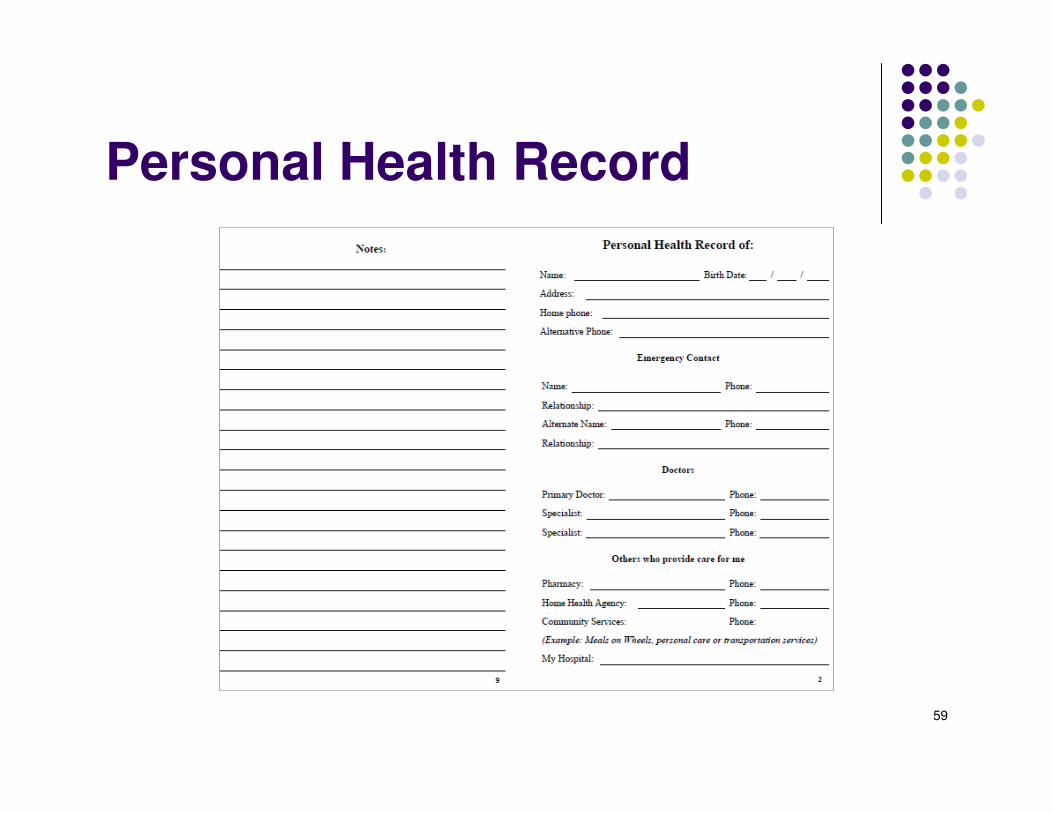
Personal Health Record
60
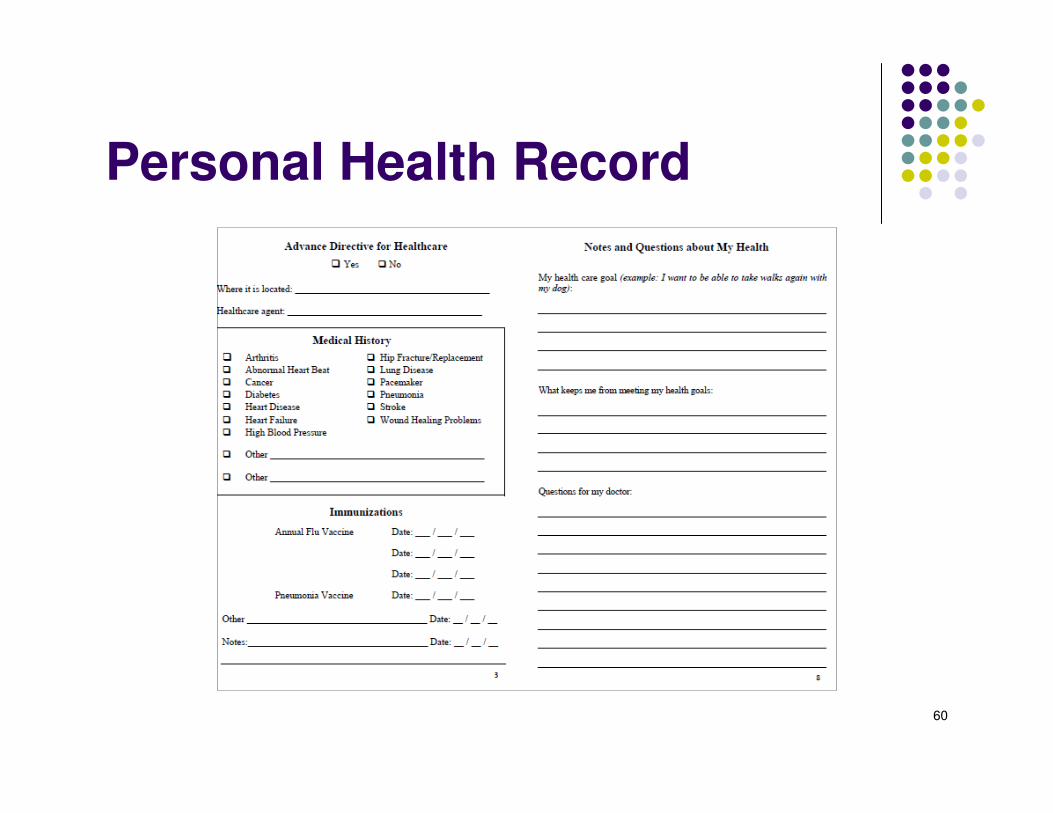
Personal Health Record
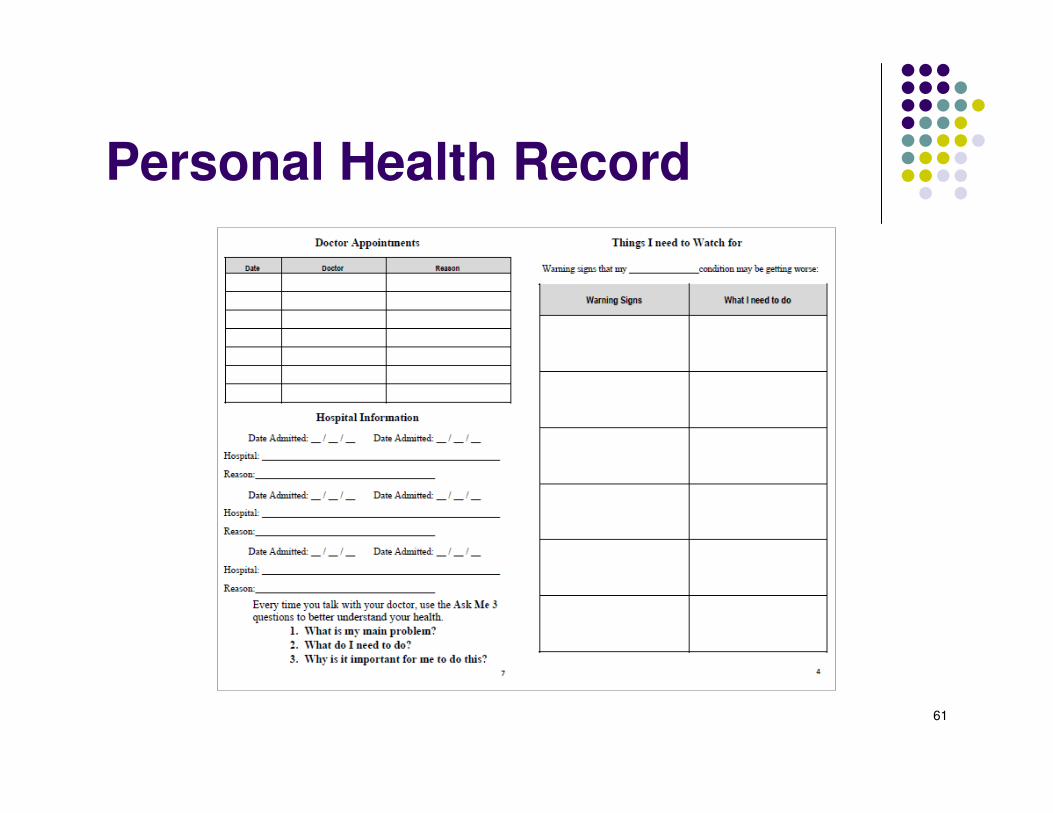
61
Personal Health Record
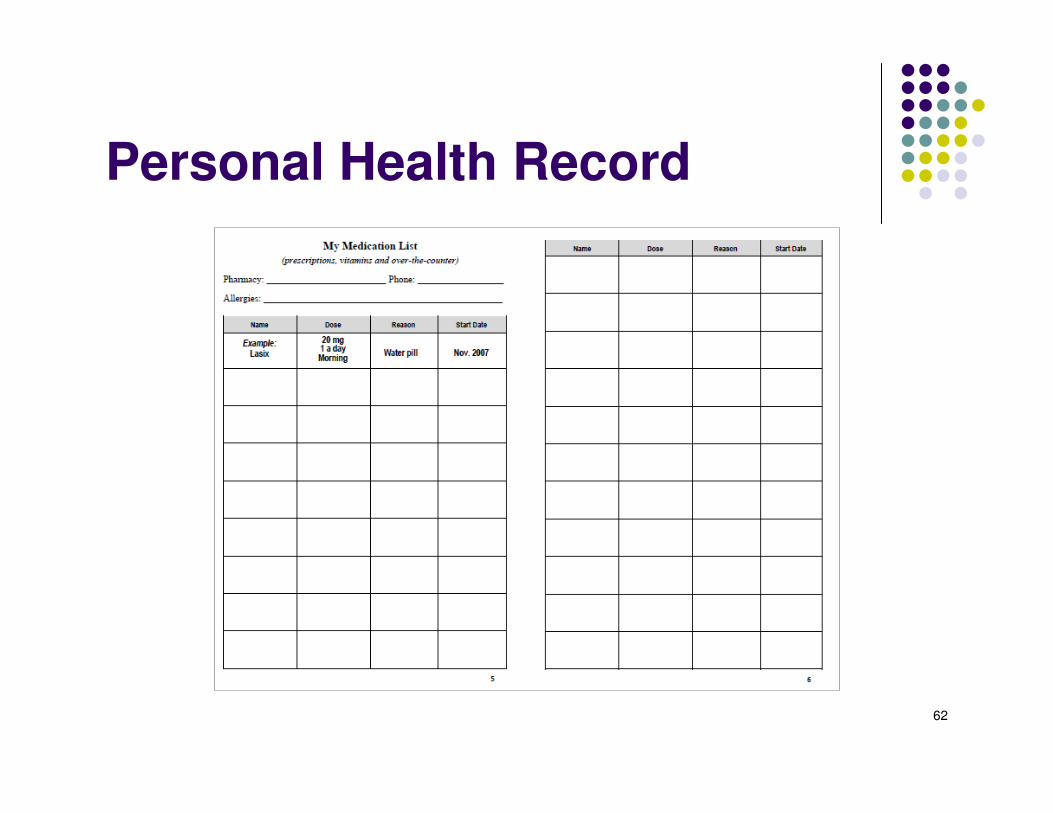
62
Personal Health Record
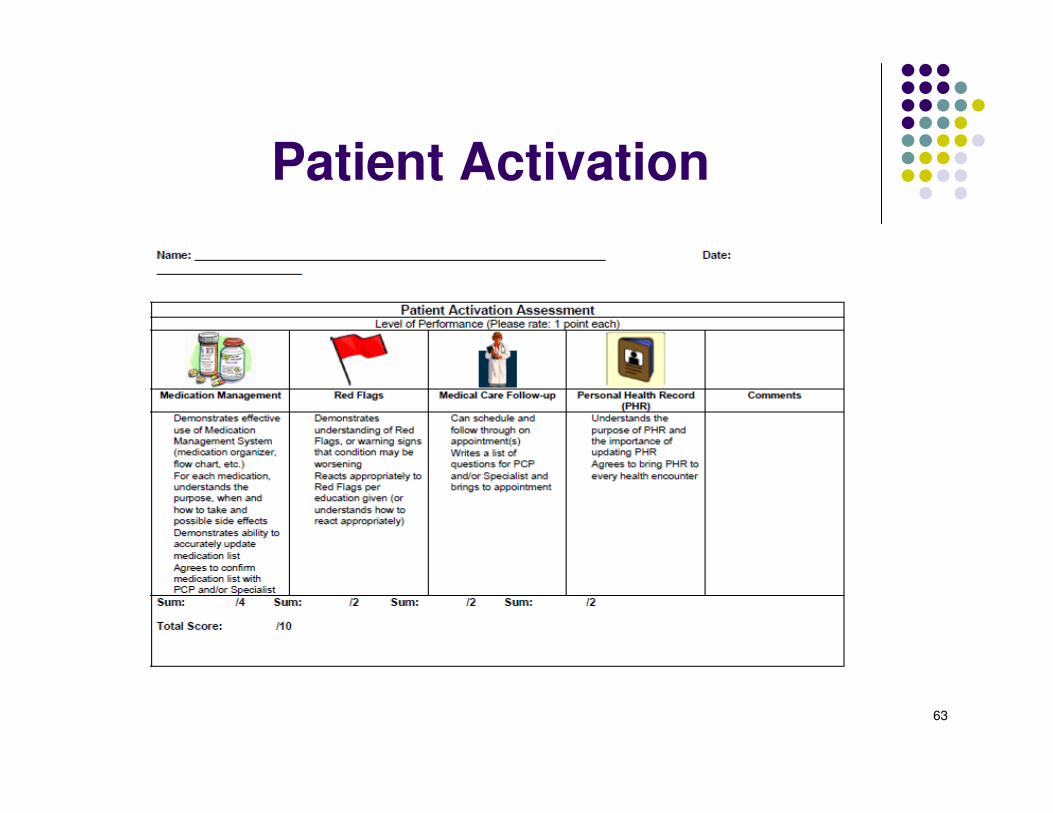
63
Patient Activation
64
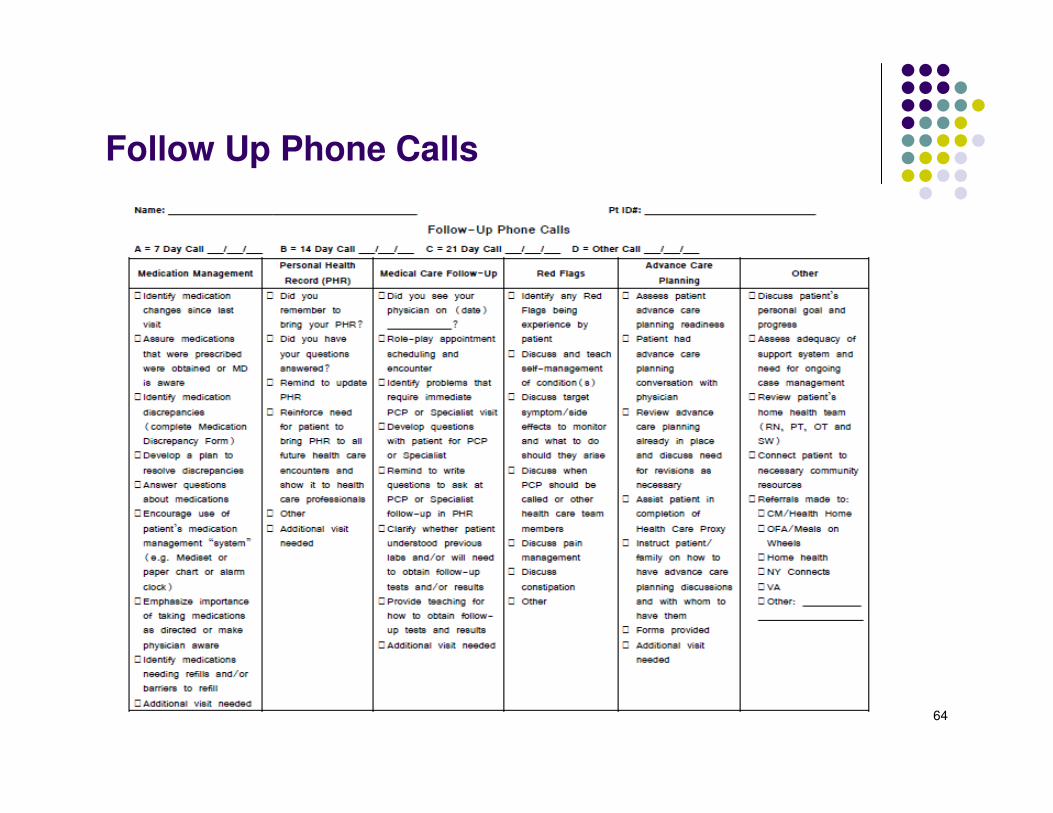
Follow Up Phone Calls
65
Important Components incorporated into the Program
�Teach Back
�Motivational Interviewing
�Health Literacy
66
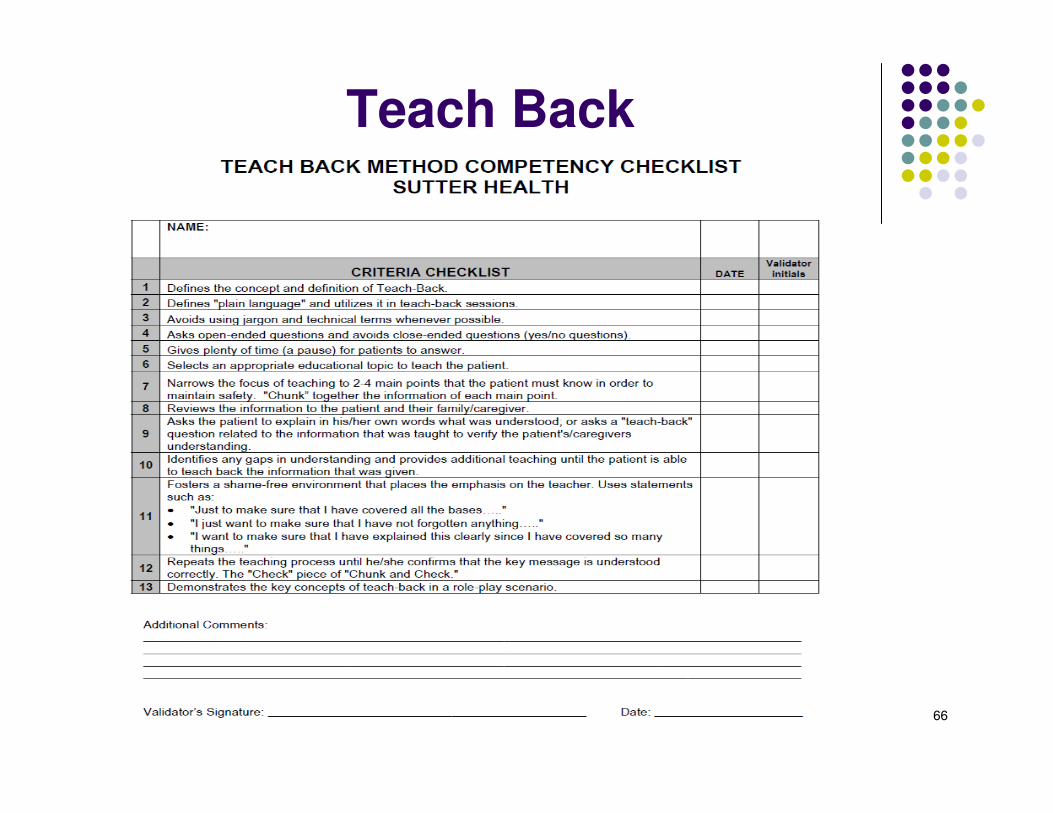
Teach Back
67
Motivational Interviewing
� Designed to enhance client motivation to change
� Especially effective for patients that are “stuck” –not making recommended health related behavior changes
� “MI is a directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence”
� MI helps activate the patient’s own motivations to change
� 6 Source: Rollnick, Miller, and ButlerInterview: Motivational ing in Healthcare. 2008
68
Motivational Interviewing
Collaboration through COACHING:
•“An approach of partnering with patients to enhance self-management strategies for the purpose of preventing exacerbations of chronic illness and supporting lifestyle change”
(Huffman, 2007, p. 271).
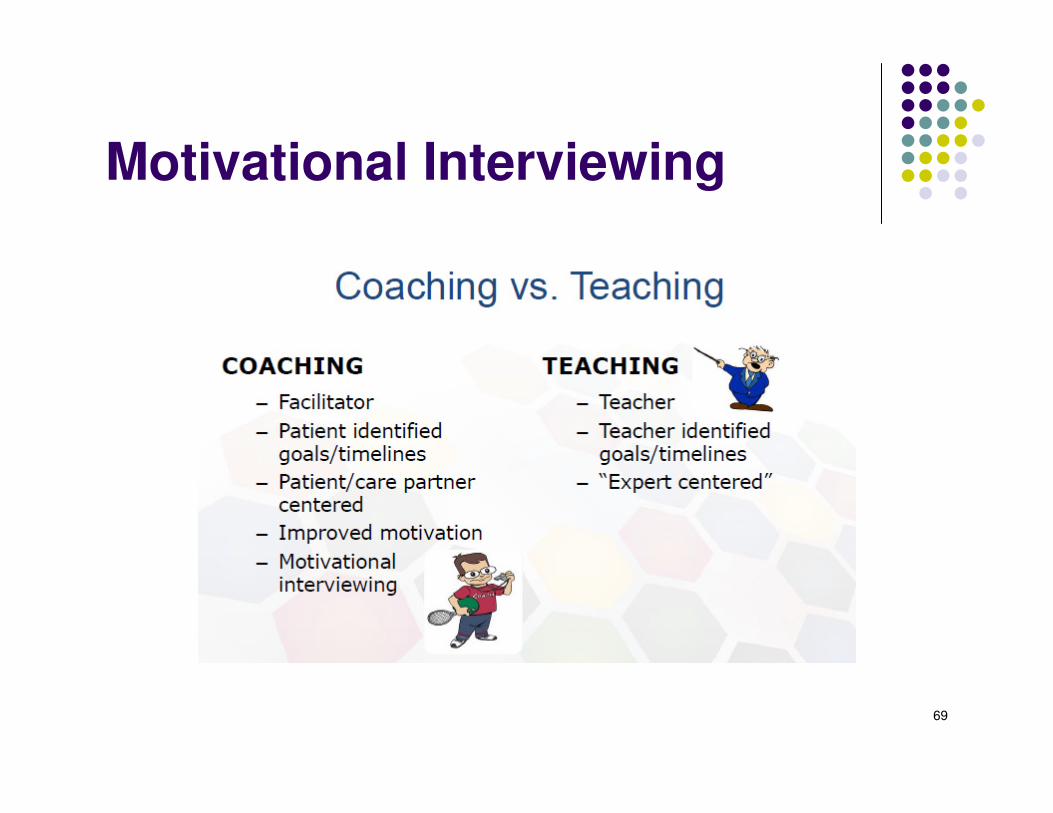
69
Motivational Interviewing
70
Motivational Interviewing
71
Motivational Interviewing
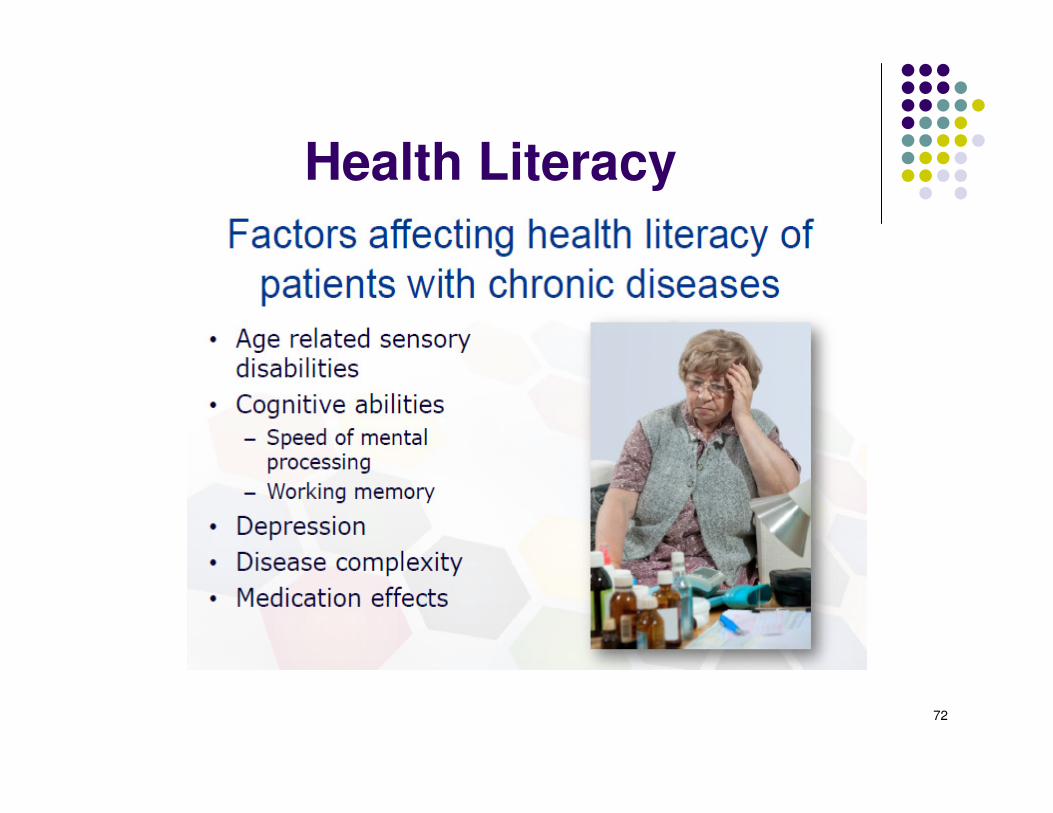
72
Health Literacy
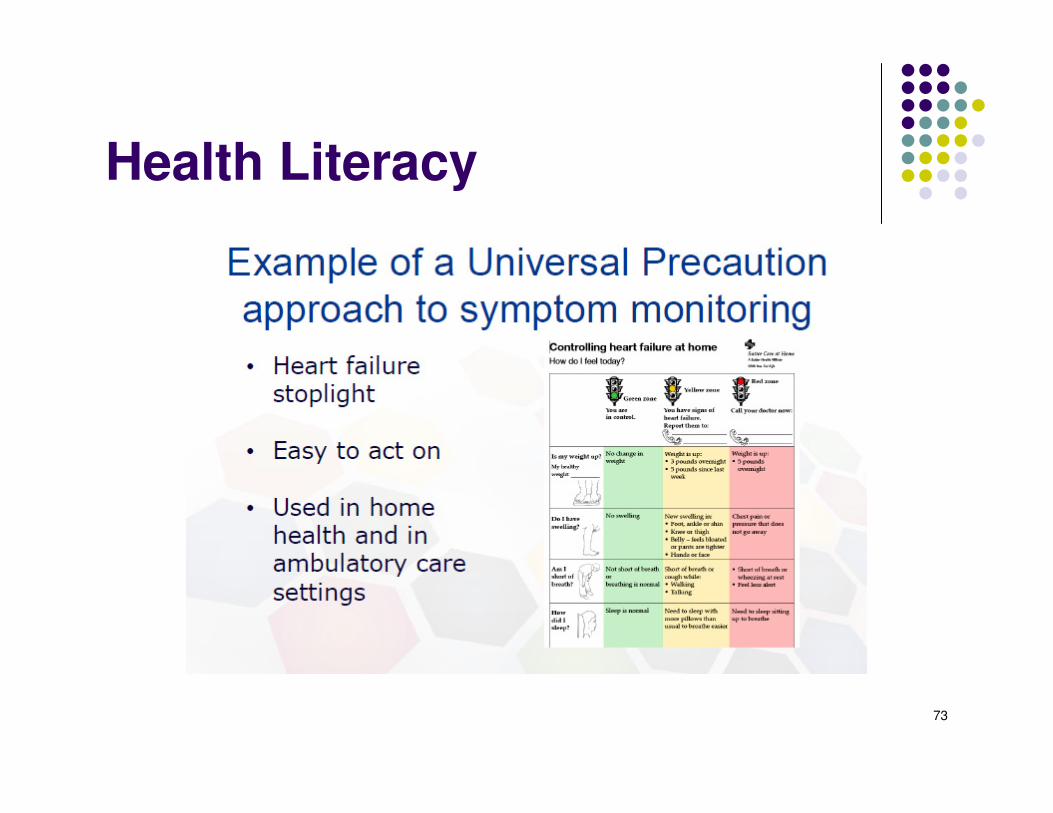
73
Health Literacy

74
Health Literacy
75
Resources
List of websites to access resources :� http://vnaablueprint.org/main-menu.html
� http://www.ihi.org/resources/Pages/Tools/AlwaysUseTeachBack!.aspx
� https://www.youtube.com/watch?v=IKxjmpD7vfY
� http://caretransitions.org/

76
Questions?





























