Embed Size (px)
Citation preview

http://cre.sagepub.com/Clinical Rehabilitation
http://cre.sagepub.com/content/early/2013/12/04/0269215513511342The online version of this article can be found at:
DOI: 10.1177/0269215513511342
published online 4 December 2013Clin RehabilJean-Sébastien Roy, Jean-Francois Esculier and Désirée B Maltais
Activities of Daily Living Scale−Outcome Survey Translation, cross-cultural adaptation and validation of the French version of the Knee
Published by:
http://www.sagepublications.com
can be found at:Clinical RehabilitationAdditional services and information for
http://cre.sagepub.com/cgi/alertsEmail Alerts:
http://cre.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Dec 4, 2013OnlineFirst Version of Record >>
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from
Clinical Rehabilitation0(0) 1 –10© The Author(s) 2013Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/0269215513511342cre.sagepub.com
CLINICALREHABILITATION
Translation, cross-cultural adaptation and validation of the French version of the Knee Outcome Survey–Activities of Daily Living Scale
Jean-Sébastien Roy1,2, Jean-Francois Esculier2 and Désirée B Maltais1,2
AbstractPurpose: The Activities of Daily Living Scale of the Knee Outcome Survey (KOS-ADLS) is a joint-specific questionnaire measuring functional limitation experienced by individuals with knee disorders. The original English version of the KOS-ADLS has been shown to be highly reliable and responsive to change. The purpose of this study was to perform a translation and cross-cultural adaptation of the original version of the KOS-ADLS questionnaire into French and to validate this French version of the questionnaire.Method: In accordance with standard procedure, the original version of the KOS-ADLS was translated and cross-culturally adapted into French. Once the final French version of the KOS-ADLS was developed, it was subjected to further psychometric evaluation with 76 individuals with knee disorders. Each participant completed the KOS-ADLS on three occasions: at baseline, two days later to evaluate test–retest reliability, and four weeks later to evaluate responsiveness. Symptoms and function-oriented construct questions were also completed to evaluate construct-convergent and known-group validity.Results: The cross-cultural adaptation procedure revealed no major problems with content or language. The French version of the KOS-ADLS showed excellent test–retest reliability with low measurement error (intraclass correlation coefficient = 0.92, minimal detectable change = 8.3), as well as high responsiveness (standardized response mean = 1.41; clinically important difference = 13.6). Further, it discriminates between different levels of self-rated or clinician-rated knee function.Conclusions: The French version of the KOS-ADLS is a reliable, valid and responsive questionnaire for the assessment of functional limitation in individuals with musculoskeletal knee disorders.
KeywordsKnee, outcome assessment, questionnaires, reliability and validity, responsiveness to change
Received: 7 July 2013; accepted: 12 October 2013
1 Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec City (QC), Canada
2 Centre for Interdisciplinary Research in Rehabilitation and Social Integration, Quebec Rehabilitation Institute, Quebec City (QC), Canada
511342 CRE0010.1177/0269215513511342Clinical RehabilitationRoy et al.research-article2013
Article
Corresponding author:Jean-Sébastien Roy, Centre for Interdisciplinary Research in Rehabilitation and Social Integration, Quebec Rehabilitation Institute, 525, Boulevard Wilfrid Hamel, Quebec City (QC), G3A 0B4, Canada. Email: [email protected]
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

2 Clinical Rehabilitation 0(0)
Introduction
A large number of joint- and disease-specific dis-ability scales have been developed for people with knee disorders.1,2 In a systematic review pertain-ing to the psychometric properties of self-adminis-tered questionnaires used to assess pain and disability in individuals with patellofemoral pain, the Activities of Daily Living Scale of the Knee Outcome Survey (KOS-ADLS) was recommended over other knee-specific scales based on its psy-chometric properties.1 The KOS-ADLS was devel-oped as a joint-specific self-reported questionnaire for the measurement of symptoms and functional limitations experienced during activities of daily living by individuals who have various pathologi-cal disorders of the knee.3 Since its development in 1998, the KOS-ADLS has been translated into various languages including Portuguese, Turkish, Greek, Japanese and German.4–7 Studies of its validity, reliability, and responsiveness have been published not only for the original version,3 but also for the translated versions.4–7 These differ-ence versions of the KOS-ADLS have been shown to be highly reliable with low measurement error. They are also highly responsive to change and they discriminate between knee conditions and levels of severity.1
To use a questionnaire with different language groups and in different cultural settings, the ques-tionnaire must not only be translated into the new language, but it must also be adapted to the local culture.8,9 The purpose of this study was to perform a translation and cross-cultural adaptation of the original version of the KOS-ADLS questionnaire into French and to evaluate validity, reliability and responsiveness to change of the new version of the questionnaire. A secondary objective was to com-pare reliability and responsiveness of the KOS-ADLS and the participant’s assessment of pain as measured with a 10-cm visual analogue scale (VAS).
Methods
The Activities of Daily Living Scale of the Knee Outcome Survey (KOS-ADLS)
The KOS-ADLS is a 14-item questionnaire that evaluates symptom-related and specific functional
limitations.3 Six items assess knee symptoms (pain, stiffness, swelling, instability, weakness, limping) and eight items assess functional limitations (walk-ing, stairs ascent/descent, standing, kneeling, squatting, sitting, rising from a sitting position) experienced within the last 1–2 days during the performance of daily activities. Each item is scored on a 6-point Likert scale (0–5 points). The KOS-ADLS score is transformed to a 0–100 point scale with 100 indicating the absence of symptoms and functional limitations.3
Translation and cross-cultural adaptation
In accordance with recommended standard proce-dures,8 the original version of the KOS-ADLS was translated and cross-culturally adapted into French following five steps:
•• Step I – Initial translation: two bilingual trans-lators (a physical therapist and a French lin-guist) whose first language was French performed the forward translation;
•• Step II – Synthesis of the translations;•• Step III – Back translation: two other bilingual
translators (a researcher and a computer spe-cialist) whose first language was English trans-lated the French version back into English;
•• Step IV – Expert committee: a pre-final version of the questionnaire with conceptual equiva-lence to the original was created;
•• Step V – Test of the pre-final version: the pre-final version was field-tested on individuals with knee disorders.
The expert committee then met to discuss and refine the French version of the KOS-ADLS (KOS-ADLS-F) based on the findings from the field-testing. The final French version was produced.
Psychometric evaluation of the final KOS-ADLS-F
Individuals, 18 years of age and older, who were undergoing evaluation and treatment for a muscu-loskeletal knee disorder at a physical therapy clinic located in Quebec City were invited to participate in this study. Individuals whose native language or
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

Roy et al. 3
principal spoken language was not French were excluded. The participants provided written informed consent before participation in this study. The Ethics Committee of the Quebec Rehabilitation Institute approved the study.
Each participant took part in one evaluation ses-sion. After recruitment, participants completed a questionnaire on sociodemographic data and symp-tomatology, and the KOS-ADLS-F. To assess the construct convergent and known-group validity of KOS-ADLS-F, each participant also rated: (1) the overall function of their knee during their usual daily activities;3 (2) their current level of daily activity with respect to the level before the knee injury;3 (3) their overall worst and usual pain over the previous week (using 10-cm VAS);10,11 and (4) their pain over the previous week during walking, stair ascent and descent, and squatting activities (using 10-cm VAS).10,12 A physical therapist then performed a clinical evaluation and rated their per-ception of the participants’ functional level based on this evaluation (normal, nearly normal, abnor-mal, and severely abnormal).
Finally, participants received two postage-paid envelopes that each contained a copy of the KOS-ADLS-F, the VAS questions and a question per-taining to global change since the initial session (Global Rating of Change). Using a 15-point Global Rating of Change scale, ranging from −7 (a very great deal worse) to 0 (about the same) to +7 (a very great deal better), participants were asked to answer the following question: ‘Overall, has there been any change in your condition since the evaluation session? Please indicate if there has been any change in your condition by choosing one of the following options’. Questionnaires in the first and second envelope had to be completed two days and four weeks after the evaluation session, respectively, and mailed back to the research team. Data from the first envelope were used to evaluate the test–retest reliability, while the data from the second envelope were used to determine respon-siveness. For the test–retest reliability calculation, only data from participants who stated they were stable on the Global Rating of Change question were used. As for responsiveness, only data from participants who stated they were improved were considered.
Statistical analysis
All analyses were conducted with the SPSS soft-ware (Version 21 for Mac; SPSS Inc, Chicago, IL, USA). The alpha level was set at 0.05.
Validity. Construct convergent validity was assessed with Pearson correlations by evaluating whether the KOS-ADLS-F correlated with each of the six VAS questions. Correlations were categorized as follows: high ≥0.7, moderate between 0.5 and 0.7, and low between 0.26 and 0.5. The a priori hypoth-esis was that low correlations would be observed between the KOS-ADLS-F and participant’s assessments of pain since these VAS questions evaluate specific aspects of lower limb pain while the KOS-ADLS-F assesses overall knee functional limitation and symptoms. Using independent t-tests, several comparisons were performed to evaluate the known-group validity of KOS-ADLS-F: (1) partici-pants who had normal or nearly normal overall function of their knee during usual daily activities were compared to those who had abnormal or severely abnormal overall function; (2) partici-pants who rated their current level of daily activity as normal or nearly normal were compared to those who rated abnormal or severely abnormal; and (3) participants for whom the physical therapist rated their level of function as normal or nearly normal were compared to those whose physical therapist rated abnormal or severely abnormal. The a priori hypothesis was that the KOS-ADLS-F would dis-criminate between participants classified into dif-ferent known-groups (P < 0.05). Factors analysis was performed using principal component analysis with varimax rotation (SPSS 21). Retained factors had eigenvalues >1. Finally, floor and ceiling effects were determined and considered if more than 15% of the participants achieved the highest or lowest possible scores.13
Reliability. To establish the test–retest reliability of KOS-ADLS-F, intraclass correlation coefficients (ICC) (model 2,1) and their associated 95% confi-dence intervals were calculated.14,15 The ICC value was considered to reflect: poor reliability <0.20; fair reliability between 0.21 and 0.40; moderate reliability between 0.41 and 0.60; good reliability between 0.61 and 0.80, and excellent reliability
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

4 Clinical Rehabilitation 0(0)
≥0.81.16 Absolute reliability was established with standard errors of measurement (SEM) and mini-mal detectable change (MDC).14,17 The MDC was calculated by multiplying the z-score correspond-ing to the level of significance (z-score of 1.65), the square root of 2, and the SEM.13 Test–retest relia-bility was also assessed using the Bland and Alt-man plotting method and the corresponding bar charts.18,19 The limits of agreement were estimated as the mean test–retest. Internal consistency was assessed with the Cronbach’s alpha coefficient. ICC, SEM and MDC of the six VAS questions were also calculated.
Responsiveness. Responsiveness to change was established using standardized response means (SRMs – mean change score divided by the stand-ard deviation of the change score) for participants who were better at the four-week evaluation. SRM were considered large if ≥0.8, moderate if between 0.5 and 0.8, and small if between 0.2 and 0.5.7 Again, SRMs of the six VAS questions were calcu-lated. A receiver operating characteristics (ROC) curve was plotted to determine the amount of change on KOS-ADLS-F that best differentiated those individuals who were moderately to greatly improved (5 to 7 on the Global Rating of Change) from those who were stable to slightly improved (0 to 2 on the Global Rating of Change). By examina-tion of the intersections of the sensitivity and 1–specificity plots nearest to the upper left hand corner of the graph, the optimal cut-off value for maximal average sensitivity and specificity for detecting change was identified.
Results
Cross-cultural adaptation and test of the pre-final version (step V)
Forward and back-translation of the KOS-ADLS revealed no major problems or language difficul-ties. Pretesting of the pre-final French version revealed no further difficulties and the question-naire was well accepted in the pilot test involving 30 subjects with knee pain (mean age: 35.7 ± 6.7 years; 19 women, 11 men). This version was used
in the subsequent validation study without any fur-ther adaptation.
Psychometric evaluation of the final version
Seventy-six participants with knee pain were enrolled (see Table 1 for participants’ characteris-tics). At the two-day evaluation, nine participants did not mail back the questionnaire and 26 were not stable, resulting in 41 participants for the eval-uation of test–retest reliability. At the four-week evaluation, 16 participants did not mail back the questionnaire and 10 were stable or deteriorated, resulting in 50 participants for the evaluation of responsiveness. No differences were found (P < 0.05) in baseline age, gender and KOS-ADLS-F scores between participants who did or did not dropout.
Validity. No floor/ceiling effects were observed for KOS-ADLS-F as no participant achieved the
Table 1. Baseline patients’ characteristics.
Characteristics (n = 76)
Age (years) 36.0 ± 11.4*Sex (% male/female) 46%/54%Height (cm) 170.3 ± 8.5*Weight (kg) 71.8 ± 19.0*Symptoms duration (weeks) 69.9 ± 143.1*KOS-ADLS-F (/100) 74.2 ± 14.2*Visual analogue scale (/10) Worst pain 6.1 ± 2.0 Usual pain 2.4 ± 1.6 Pain during walking 2.8 ± 2.5 Pain during stairs ascent 4.1 ± 2.6 Pain during stairs descent 4.4 ± 2.7 Pain during squatting 4.7 ± 2.8Clinical diagnosis Ligamentous or meniscal injury 14% Patellofemoral pain 51% Tendinopathy 21% Osteoarthritis 7% Others 7%
KOS-ADLS-F, French version of the Activities of Daily Living Scale of the Knee Outcome Survey.*Mean ± standard deviation.
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

Roy et al. 5
highest or lowest possible scores at baseline. Low to moderate significant correlations (–0.37 < r < –0.57) were observed between KOS-ADLS-F and VAS (Table 2). As for known-group validity, mean scores of KOS-ADLS-F at baseline significantly differentiated between different levels of self-rated or clinician-rated functional level (Table 3).
Principal component analysis (Kaiser–Meyer–Olkin value = 0.812) extracted four factors with eigenvalues >1 (Table 4). Varimax rotation showed that the first factor comprised six items related essentially to symptoms and activities that require knee flexion. The second factor comprised five items mainly related to mobility. Given that factors 3 and 4 have small eigenvalues and include one item each, a two-factor solution was chosen. The two items not included in the two-factor model are ‘Swelling’ (S3) and ‘Giving way, buckling or shift-ing of knee’ (S4). Two reasons might explain that these items are not included in the two first factors as in the development study by Irrgang et al.3 First, more than 50% of our population presented patel-lofemoral pain, for which symptoms like ‘Swelling’ (S3) and ‘Giving way, buckling or shifting of knee’ (S4) are less prevalent than in ligamentous or meniscal injuries (57% of the population in Irrgang et al.3). Second, symptom of ‘Giving way, buckling or shifting of knee’ might be a concept more diffi-cult to understand than the other symptoms.
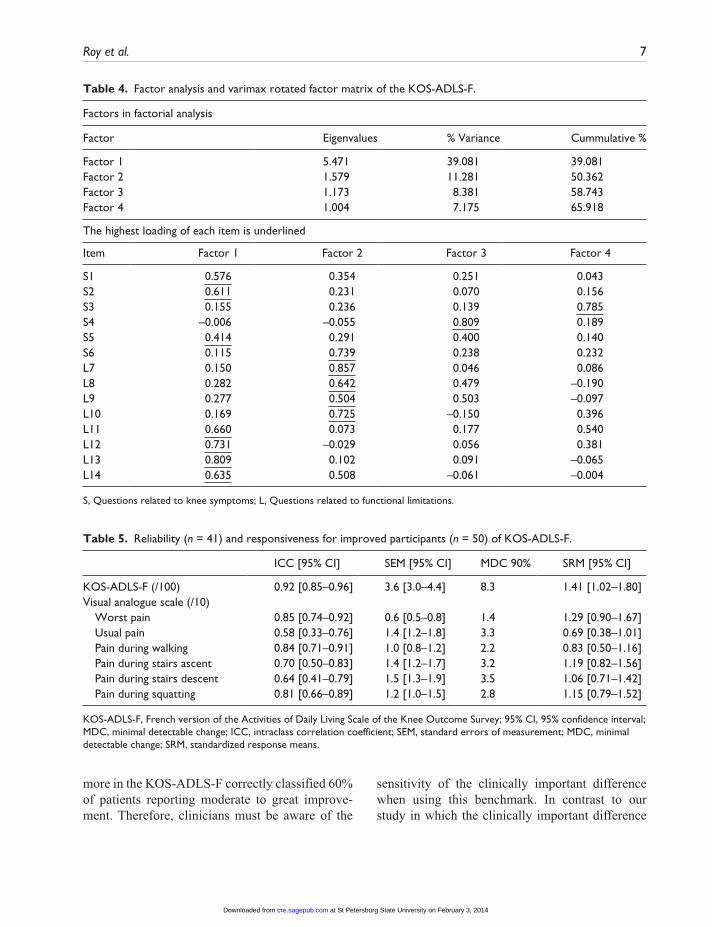
Reliability. Test–retest reliability of KOS-ADLS-F was excellent (Table 5). By comparison, it was moderate to excellent for VASs (Table 5). The Bland and Altman plots revealed that test–retest differences for the KOS-ADLS-F were centred around zero (i.e. no bias indicated – Figure 1). Internal consistency was high with a Cronbach’s alpha coefficient of 0.87.
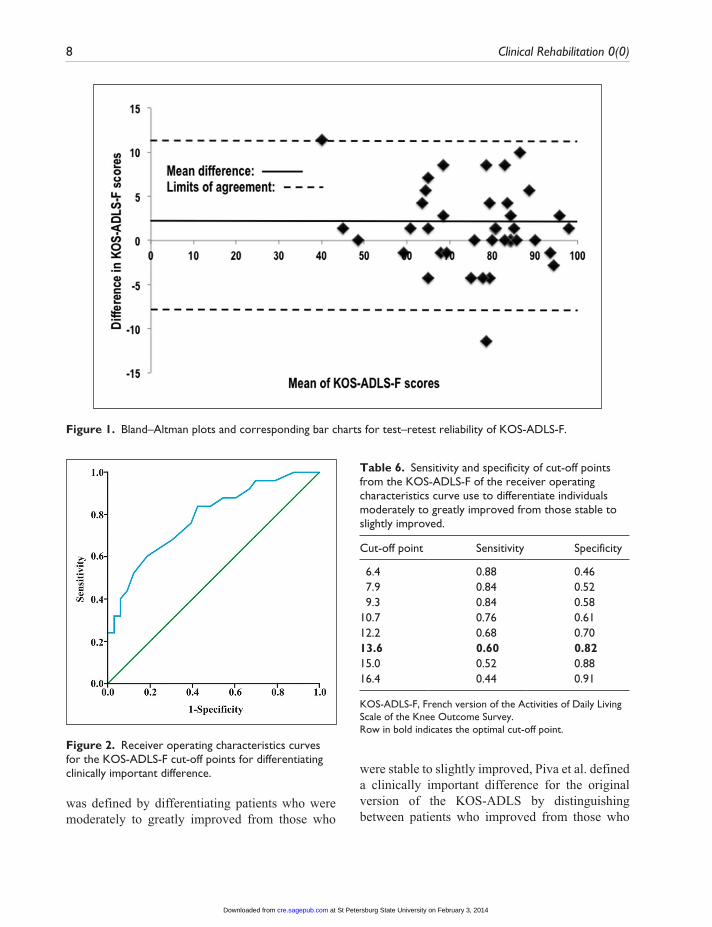
Responsiveness. High responsiveness values were observed for the KOS-ADLS-F for improved patients (Table 5). As for the VASs, moderate to large responsiveness values were obtained (Table 5). Using ROC curves (area under the curve: 0.78; fair discriminative abilities), the optimal cut-off point, which defined the clinically important dif-ference, was 13.6% on KOS-ADLS-F (Figure 2). Table 6 presents the sensitivity and specificity data of the cut-off points.
Discussion
In this study, evidence of the validity, test–retest reliability and responsiveness of the KOS-ADLS-F are provided. In summary, excellent test–retest reliability with low measurement error, as well as high responsiveness were obtained. Further, our results suggest that KOS-ADLS-F discriminates between different functional levels and has no floor or ceiling effect. The relationships between the KOS-ADLS-F and participants’ assessment of pain using VAS mostly followed expectations of low relationships (r < –0.57).
As in the other adaptation studies,4–7 no particu-lar difficulties arose during the cross-cultural adap-tation of the KOS-ADLS-F and the participants considered all questions and response options sat-isfactorily comprehensible. The questionnaire was validated in a population living in the French-speaking part of Canada. During the translation/adaptation process, special attention was paid to ensure that the terms and expressions used in the French version were applicable to any person residing in a francophone country. Therefore, this version of the KOS-ADLS has the potential to be used with any French-speaking patients with knee disorders. However, it should preferably be
Table 2. Convergent construct validity: Pearson correlations between the KOS-ADLS-F and participants’ assessments of pain.
Worst pain Usual pain Walking Stairs ascent Stairs descent Squatting
KOS-ADLS-F –0.40* –0.38* –0.41* –0.47* –0.42* –0.57*
KOS-ADLS-F, French version of the Activities of Daily Living Scale of the Knee Outcome Survey.Bold: Correlations above 0.50.*Significant at P < 0.001
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

6 Clinical Rehabilitation 0(0)T
able
3.
Kno
wn-
grou
p va
lidity
of t
he K
OS-
AD
LS-F
.
Self-
rate
d ov
eral
l fun
ctio
n of
the
kne
e du
ring
us
ual d
aily
act
iviti
esSe
lf-ra
ted
curr
ent
leve
l of d
aily
act
ivity
Pe
rcep
tion
of t
he p
artic
ipan
ts’ l
evel
of
func
tion
by t
he p
hysi
cal t
hera
pist
A
bnor
mal
or
sev
erel
y ab
norm
al
(n =
28)
*
Nor
mal
or
nea
rly
norm
al
(n =
48)
*
P-va
lue
Mea
n di
ffere
nce
[95%
CI]
Abn
orm
al
or s
ever
ely
abno
rmal
(n
= 2
9)*
Nor
mal
or
nea
rly
norm
al
(n =
47)
*
P-va
lue
Mea
n di
ffere
nce
[95%
CI]
Abn
orm
al
or
seve
rely
ab
norm
al
(n =
20)
*
Nor
mal
or
nea
rly
norm
al
(n =
56)
*
P-va
lue
Mea
n di
ffere
nce
[95%
CI]
KO
S-A
DLS
-F66
.1 (
15.7
)78
.9 (
10.9
)<0
.001
12.8
[6
.7, 1
8.9]
64.8
(14
.7)
79.9
(10
.4)
<0.0
0115
.1
[9.3
, 20.
8]65
.7 (
17.2
)77
.2 (
11.7
)<0
.001
11.5
[4
.5, 1
8.4]
KO
S-A
DLS
-F, F
renc
h ve
rsio
n of
the
Act
iviti
es o
f Dai
ly L
ivin
g Sc
ale
of t
he K
nee
Out
com
e Su
rvey
.*M
ean
KO
S-A
DLS
(st
anda
rd d
evia
tion)
.
validated in other French-speaking countries before being used there.
The psychometric properties of KOS-ADLS-F compare favourably with those obtained in the development study of the original version of the KOS-ADLS, and in subsequent studies that have evaluated its properties.4,5,20–23 In the development study,20 ICC of 0.97, MDC 90% of 7.5 and an effect size of 0.94 (effect size of 0.96 in the present study) were obtained in 397 patients with various knee disorders. Higher reliability indices in the development study might be explained by the fact that the retest was performed within the same day compared to the two-day interval in the present study. As for the other studies, according to a sys-tematic review,1 the weighted average ICC for the KOS-ADLS is 0.96 (five studies, 288 subjects), the weighted average MDC90% is 8.0 (three studies, 177 subjects) and the SRM for improved subjects is 1.10 (one study, 42 subjects).4,5,21–23
Based on psychometric evidence, KOS-ADLS should be favoured over participants’ assessment of pain using VAS in this population. VAS are often used in clinical and research setting following knee disorders to measure participants’ assessment of pain or functional level. The advantages of VAS assessment over self-reported questionnaires mainly include that they are quicker to complete and can be more easily interviewer-administered. However, our results suggest that the psychometric properties of VAS are less favourable than the ones of the KOS-ADLS. For example, the measurement error of VAS, defined by the MDC, represents a much larger proportion of the total score (from 14% to 35% of the total score for VAS) compared to the KOS-ADLS-F (8% of the total score). Still, VAS for worst pain and pain during stairs ascent were both highly reliable and responsive, and can be used in this population. In patients with patel-lofemoral pain, Crossley et al. had similar findings with the AKPS, a knee-specific self-reported ques-tionnaire, showing slightly better reliability and responsiveness indices than VAS for usual and worst pain.10
A limitation of the KOS-ADLS-F is that the sensitivity of the clinically important difference is low at 60%. This means that a change of 13.6% or
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from
Roy et al. 7
Table 4. Factor analysis and varimax rotated factor matrix of the KOS-ADLS-F.
Factors in factorial analysis
Factor Eigenvalues % Variance Cummulative %
Factor 1 5.471 39.081 39.081Factor 2 1.579 11.281 50.362Factor 3 1.173 8.381 58.743Factor 4 1.004 7.175 65.918
The highest loading of each item is underlined
Item Factor 1 Factor 2 Factor 3 Factor 4
S1 0.576 0.354 0.251 0.043S2 0.611 0.231 0.070 0.156S3 0.155 0.236 0.139 0.785S4 –0.006 –0.055 0.809 0.189S5 0.414 0.291 0.400 0.140S6 0.115 0.739 0.238 0.232L7 0.150 0.857 0.046 0.086L8 0.282 0.642 0.479 –0.190L9 0.277 0.504 0.503 –0.097L10 0.169 0.725 –0.150 0.396L11 0.660 0.073 0.177 0.540L12 0.731 –0.029 0.056 0.381L13 0.809 0.102 0.091 –0.065L14 0.635 0.508 –0.061 –0.004
S, Questions related to knee symptoms; L, Questions related to functional limitations.
Table 5. Reliability (n = 41) and responsiveness for improved participants (n = 50) of KOS-ADLS-F.
ICC [95% CI] SEM [95% CI] MDC 90% SRM [95% CI]
KOS-ADLS-F (/100) 0.92 [0.85–0.96] 3.6 [3.0–4.4] 8.3 1.41 [1.02–1.80]Visual analogue scale (/10) Worst pain 0.85 [0.74–0.92] 0.6 [0.5–0.8] 1.4 1.29 [0.90–1.67] Usual pain 0.58 [0.33–0.76] 1.4 [1.2–1.8] 3.3 0.69 [0.38–1.01] Pain during walking 0.84 [0.71–0.91] 1.0 [0.8–1.2] 2.2 0.83 [0.50–1.16] Pain during stairs ascent 0.70 [0.50–0.83] 1.4 [1.2–1.7] 3.2 1.19 [0.82–1.56] Pain during stairs descent 0.64 [0.41–0.79] 1.5 [1.3–1.9] 3.5 1.06 [0.71–1.42] Pain during squatting 0.81 [0.66–0.89] 1.2 [1.0–1.5] 2.8 1.15 [0.79–1.52]
KOS-ADLS-F, French version of the Activities of Daily Living Scale of the Knee Outcome Survey; 95% CI, 95% confidence interval; MDC, minimal detectable change; ICC, intraclass correlation coefficient; SEM, standard errors of measurement; MDC, minimal detectable change; SRM, standardized response means.
more in the KOS-ADLS-F correctly classified 60% of patients reporting moderate to great improve-ment. Therefore, clinicians must be aware of the
sensitivity of the clinically important difference when using this benchmark. In contrast to our study in which the clinically important difference
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from
8 Clinical Rehabilitation 0(0)
was defined by differentiating patients who were moderately to greatly improved from those who
were stable to slightly improved, Piva et al. defined a clinically important difference for the original version of the KOS-ADLS by distinguishing between patients who improved from those who
Table 6. Sensitivity and specificity of cut-off points from the KOS-ADLS-F of the receiver operating characteristics curve use to differentiate individuals moderately to greatly improved from those stable to slightly improved.
Cut-off point Sensitivity Specificity
6.4 0.88 0.46 7.9 0.84 0.52 9.3 0.84 0.5810.7 0.76 0.6112.2 0.68 0.7013.6 0.60 0.8215.0 0.52 0.8816.4 0.44 0.91
KOS-ADLS-F, French version of the Activities of Daily Living Scale of the Knee Outcome Survey.Row in bold indicates the optimal cut-off point.
Figure 1. Bland–Altman plots and corresponding bar charts for test–retest reliability of KOS-ADLS-F.
Figure 2. Receiver operating characteristics curves for the KOS-ADLS-F cut-off points for differentiating clinically important difference.
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

Roy et al. 9
did not.23 They obtained a clinically important dif-ference of 7.1% (area under the curve = 0.84).23 However, the sensibility and specificity associated with this clinically important difference was not published.
A limitation of this study is that a two-day retest interval was used for the evaluation of reliability. A retest interval of 1 or 2 weeks is often recom-mended to limit the carryover effects due to mem-ory.24 However, a longer retest interval was not possible given that the participants started their rehabilitation right after the baseline evaluation. In fact, 39% of the subjects were improved after two days according to the Global Rating of Change question. According to Marx et al., there are no sta-tistical differences in the test–retest reliability of the KOS-ADLS between a retest interval of two days or of two weeks (ICC of 0.93 on both occasions).22
Conclusions
The French version of the KOS-ADLS is valid, reli-able and responsive to change for the assessment of symptoms and functional limitation in patients with knee disorders. Psychometric properties similar to those of the original English version and other lan-guage versions of the KOS-ADLS were demon-strated. The French version of the KOS-ADLS can now be used in clinical settings and future outcome studies for patients with knee disorders.
Clinical messages
•• The French version of the KOS-ADLS is valid, reliable and responsive to change.
•• It discriminates between different levels of self-rated or clinician-rated functional level.
Conflict of interest
The author declares that there is no conflict of interest.
Funding
This study was supported by a grant from the Ordre pro-fessionnel de la physiothérapie du Québec. JF Esculier
was supported by a scholarship from the Fonds de recherche du Québec - Santé (FRQ-S). JS Roy was sup-ported by a salary award from the FRQ-S.
References
1. Esculier JF, Roy JS and Bouyer LJ. Psychometric evidence of self-reported questionnaires for patel-lofemoral pain syndrome: a systematic review. Disabil Rehabil. Epub ahead of print 29 April 2013. DOI: 10.3109/09638288.2013.774061.
2. Wang D, Jones MH, Khair MM and Miniaci A. Patient-reported outcome measures for the knee. J Knee Surg 2010; 23: 137–151.
3. Irrgang JJ, Snyder-Mackler L, Wainner RS, et al. Development of a patient-reported measure of function of the knee. J Bone Joint Surg Am 1998; 80: 1132–1145.
4. Bizzini M and Gorelick M. Development of a German version of the knee outcome survey for daily activities. Arch Orthop Trauma Surg 2007; 127: 781–789.
5. Evcik D, Ay S, Ege A, et al. Adaptation and validation of Turkish version of the Knee Outcome Survey-Activities for Daily Living Scale. Clin Orthop Relat Res 2009; 467: 2077–2082.
6. Goncalves RS, Cabri J and Pinheiro JP. Cross-cultural adaptation and validation of the Portuguese version of the Knee Outcome Survey-Activities of Daily Living Scale (KOS-ADLS). Clin Rheumatol 2008; 27: 1445–1449.
7. Kapreli E, Panelli G, Strimpakos N, et al. Cross-cultural adaptation of the Greek version of the Knee Outcome Survey—activities of Daily Living Scale (KOS-ADLS). Knee 2011; 18: 424–427.
8. Beaton DE, Bombardier C, Guillemin F and Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000; 25: 3186–3191.
9. Guillemin F, Bombardier C and Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 1993; 46: 1417–1432.
10. Crossley KM, Bennell KL, Cowan SM and Green S. Analysis of outcome measures for persons with patel-lofemoral pain: which are reliable and valid? Arch Phys Med Rehabil 2004; 85: 815–822.
11. Harrison E, Quinney H, Magee D, et al. Analysis of out-come measures used in the study of patellofemoral pain syndrome. Physiother Can 1995; 47: 264–272.
12. Eng JJ and Pierrynowski MR. Evaluation of soft foot orthotics in the treatment of patellofemoral pain syn-drome. Phys Ther 1993; 73: 62–70.
13. McHorney CA and Tarlov AR. Individual-patient monitor-ing in clinical practice: are available health status surveys adequate? Qual Life Res. 1995; 4: 293–307.
14. Finch E, Brooks D, Stratford PW and Mayo NE. Why Measurement properties Are Important. In: Physical reha-bilitation outcome measures: a guide to enhanced clini-cal decision making. Hamilton: Canadian Physiotherapy Association, 2002, pp. 26–41.
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from

10 Clinical Rehabilitation 0(0)
15. Shrout PE and Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull 1979; 86: 420–428.
16. Altman DG, Schulz KF, Moher D, et al. The revised CONSORT statement for reporting randomized trials: expla-nation and elaboration. Ann Intern Med 2001; 134: 663–694.
17. Stratford PW, Binkley J, Solomon P, et al. Defining the mini-mum level of detectable change for the Roland-Morris ques-tionnaire. Phys Ther 1996; 76: 359–368.
18. Bland JM and Altman DG. Statistical methods for assess-ing agreement between two methods of clinical measure-ment. Lancet 1986; 1(8476): 307–310.
19. Smith MW, Ma J and Stafford RS. Bar charts enhance Bland-Altman plots when value ranges are limited. J Clin Epidemiol 2010; 63: 180–184.
20. Irrgang JJ, Snyder-Mackler L, Wainner RS, et al. Development of a patient-reported measure of function of the knee. J Bone Joint Surg Am 1998; 80: 1132–1145.
21. Marx RG, Jones EC, Allen AA, et al. Reliability, valid-ity, and responsiveness of four knee outcome scales for athletic patients. J Bone Joint Surg Am 2001; 83-A: 1459–1469.
22. Marx RG, Menezes A, Horovitz L, et al. A compari-son of two time intervals for test-retest reliability of health status instruments. J Clin Epidemiol 2003; 56: 730–735.
23. Piva SR, Gil AB, Moore CG and Fitzgerald GK. Responsiveness of the activities of daily living scale of the knee outcome survey and numeric pain rating scale in patients with patellofemoral pain. J Rehabil Med 2009; 41: 129–135.
24. Portney LG and Watkins MP. Foundation of clini-cal research: applications to practice, third edi-tion. Upper Saddle River, NJ: Pearson Prentice Hall, 2009.
at St Petersburg State University on February 3, 2014cre.sagepub.comDownloaded from




























