Embed Size (px)
Citation preview

CASE REPORT
Translocation t(X;10)(p10;p10): a rare chromosomal abnormalityin a new born female with acute myeloid leukemia
Ayda Bennour • Halima Sennana • Monia Zaier •
Ines Ouahchi • Zannouba Mrad • Yosra Ben Youssef •
Abderrahim Khelif • Ali Saad
Received: 7 March 2011 / Accepted: 9 March 2011 / Published online: 26 March 2011
� Springer Science+Business Media, LLC 2011
Abstract Sex chromosomes are infrequently involved in
patients with hematologic malignancies. In most instances,
the abnormality is either duplication in the q arm or dele-
tion and translocation involving the q13 and q24 regions.
We report herein a rare translocation t(X;10)(p10;p10) in a
newborn with 2 months and 20 days with acute myeloid
leukemia (AML) (FAB, M4). Cytogenetic analysis detec-
ted a cell clone with t(X;10)(p10;p10). Thus was confirmed
by FISH analysis with whole chromosome painting (WCP)
specific for chromosomes X and 10. The patient was
treated with chemotherapy, and a complete morphologic
and cytogenetic remission was achieved. To our knowl-
edge, our case is the first report of a neonatal AML4 with
t(X; 10). The patient had an excellent early response to a
salvage AML-type therapy. The prognostic significance of
the t(X; 10) in this setting remains unclear. Due to the
rarity of this translocation, further cytogenetic and molec-
ular biologic studies are required to elucidate the clinical
and molecular significance of this unusual karyotypic
finding.
Keywords Acute myeloid leukemia � Sex chromosome
abnormality � t(X;10)(p10;p10) � Neonatal AML 4 �Fluorescence in situ hybridization �Whole chromosome painting
Introduction
Sex chromosomes are involved uncommonly in karyotypic
aberrations in patients with hematologic malignancies.
A loss of chromosome Y, monosomy or trisomy X is
occasionally found in these patients [1]. However, struc-
tural abnormalities involving chromosome X are unusual in
hematologic neoplasia. In the literature, chromosomal
aberrations involve deletion, duplication, or translocation
of the long arm of chromosome X.
Translocation t(X;10)(p10;p10) is a rare occurrence in
pediatric leukemia of unclear prognostic significance [2].
We report herein such a translocation in a patient with
acute myeloid leukemia (AML).
Case report
A newborn with 2 months and 20 days presented with
acute leucosis and fever 40�C.
After admission to the pediatric department, her clinical
examination revealed splenomegaly but no hepatomegaly.
Peripheral blood examination revealed hemoglobin 10 g/dl,
platelets 102 9 109/l, and leukocytes 207 9 109/l with 4%
neutrophils, 14% lymphocytes, 15% monocytes, and 60%
blast cells.
Bone marrow examination showed hypercellular mar-
row infiltrated with blast cells with 23% myeloblasts and
43% monoblasts.
The myeloblast cells were cytochemically positive for
myeloperoxidase and the monoblast cells were faintly
positive.
A diagnosis of acute myelomonocytic leukemia was
made (FAB type 4). The patient was treated with
A. Bennour (&) � H. Sennana � I. Ouahchi � Z. Mrad � A. Saad
Department of Cytogenetics, Molecular Genetics
and Reproductive Biology, Farhat Hached University
Teaching Hospital, Sousse, Tunisia
e-mail: [email protected]
M. Zaier � Y. Ben Youssef � A. Khelif
Department of Clinical Hematology, Farhat Hached University
Teaching Hospital, Sousse, Tunisia
123
Med Oncol (2012) 29:1134–1136
DOI 10.1007/s12032-011-9908-x

Aracytine-C (60 mg/day) for 7 days and with Fludarabine
(3.5 mg/day) for 3 days.
Five weeks later, bone marrow examination revealed
decreased cellularity with 6% of blast cells.
The patient was then treated with Aracytine-C
1,800 mg/day and Amsacrine 30 mg/day for 3 days, fol-
lowed by Aracytine-C (60 mg/day) and Rubidomycine
12.5 mg/day for 4 days and subsequently Aracytine-C
(1,800 mg/day) and Kidrolase 1,900 IU/day for two days.
A complete morphologic and cytogenetic remission was
achieved after these cycles of chemotherapy, which she
tolerated very well. Her latest peripheral blood examina-
tion revealed hemoglobin 4.8 g/dl, platelets 185 9 109/l,
and leukocytes 2.6 9 109/l with 51% neutrophils and 44%
lymphocytes.
Cytogenetic studies
Karyotypic analyses were performed by overnight cultures
of bone marrow samples. Metaphase chromosomes were
R-banded and karyotyped according to the recommenda-
tions of the International System for Human Cytogenetic
Nomenclature (ISCN) [3].
FISH studies
Fluorescence in situ hybridization (FISH) analysis with
whole chromosome painting (WCP) was performed for
chromosomes X and 10 (Vysis, IL, Downers Grove, USA).
Metaphases were viewed with a Zeiss epifluorescence
microscope and analyzed using Cytovision software 3.6
(Applied Imaging).
Results
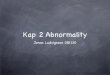
At diagnosis, the patient showed an abnormal cell clone
with a balanced translocation between X and 10 chromo-
somes with breakpoints, respectively, at Xp10 and 10p10:
46,X,t(X;10)(p10;p10) [17](Fig. 1), in addition to a normal
cell clone of 46,XX[10].
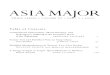
Fluorescence in situ hybridization analysis with WCP X
and WCP 10 disclosed an exchange between chromosomes
X and 10, and confirmed the reciprocal translocation
t(X;10) (Fig. 2).
After treatment, cytogenetic analysis, revealed a normal
female karyotype in 20 metaphases.
Discussion
Sex chromosomes are infrequently involved in chromo-
somal aberrations in patients with hematologic malignan-
cies [1]. Structural abnormalities of the chromosome X in
acute leukemia are described in very few reports [2] In
most instances, the abnormality is either duplication of the
Xq arm or deletion and translocation involving the Xq13
and Xq24 regions [2].
Translocation t(X;10)(pl0;pl0) has been rarely reported
in acute leukemia of myeloblastic or monoblastic lineage
Fig. 1 Karyotype of the
abnormal cell clone:
46,X,t(X;10)(p10;p10)
Med Oncol (2012) 29:1134–1136 1135
123

[4]. In the reported cases, it appears to coincide with the
emergence of the myeloid clone, and in some cases,
additional cytogenetic changes involving deletion (5q),
monosomy 7, or trisomy 8 tend to occur together with this
abnormality [4].
A review of the literature and the Mitelman Database of
Chromosome Aberrations in Cancer [5] showed four pre-
vious reports of a similar translocation t(X;10) in childhood
AML [6–9]. The first case was a 2-year-old girl with AML-
M1 and t(X;10)(p11;p11) who had a relapse-free survival
of 7 months until the time of report [6]. The second child
was a 14-year-old boy with a morphologically FAB-M1
peroxidase positive acute leukemia. The patient was treated
successfully with an acute lymphoblastic leukemia (ALL)-
type protocol and bone marrow transplant [7]. The third
patient had therapy-related AML after exposure to etopo-
side (cumulative dose, 9.9 grams/m2), which was previ-
ously given as part of ALL therapy [8], and the fourth
patient was a pediatric 15-year-old girl with a secondary
AML with t(X; 10) arising after chemotherapy for Ewing’s
sarcoma, the patient had an excellent early response to a
salvage AML-type therapy [9].
Translocation t(X;10)(p10;p10) has also been reported
in two adult patients with acute leukemia, one with acute
monocytic leukemia and the other with a myeloid relapse
of a bilineage leukemia [4]. Moreover, translocation
t(X;10)(p11;q11) has also been described in a case of
therapy-related AML-M5, [10] and in a premature girl with
congenital acute monocytic leukemia [11].
To our knowledge, translocation involving the whole p
arms of chromosomes X and 10, has only been reported in
6 cases [4, 6–9].
In our case, the karyotype disclosed clearly the break-
points implicated on Xp and 10p arms, concerned in
t(X;10). According to ISCN, the karyotype should be
assigned as t(X;10)(pl0;pl0). Furthermore, FISH experi-
ments with whole chromosome paintings were performed
for the first time to confirm this translocation.
This study, further confirms the observation that t(X;10)
is a recurrent chromosomal abnormality involving acute
leukemia of myeloid lineage. To the best of our knowledge,
our case is the first report of a neonatal AML4 with t(X;
10). Although the patient had an excellent early response to
a salvage AML-type therapy, the prognostic significance of
the t(X; 10) in this setting remains unclear. Due to the
rarity of this translocation, further cytogenetic and molec-
ular biologic studies are required to elucidate the clinical
and molecular significance of this unusual karyotypic
finding. Additional reports of similar cases or from larger
registries may help in understanding its association with
clinical presentation and outcome.
Acknowledgments This work was supported by the Ministry of
Health and the Ministry of Scientific Research and Biotechnology of
Tunisia.
References
1. Mitelman F, Kaneko Y, Trent J. Report of the committee on
chromosome changes in neoplasia. Cytogenet Cell Genet.
1991;58:1053–79.
2. Werner-Favre C, Beris P, Engel E. X chromosome rearrange-
ments and leukemia. Cytogenet Cell Genet. 1985;39:80.
3. ISCN An international system for human cytogenetic nomen-
clature. In: Shaffer LG, Tommerup N, editors. Karger.
4. Wong KF, Hayes KJ, Huh YO, et al. Translocation
(X;10)(p10;p10) a rare but nonrandom chromosomal abnormality
in acute leukemia of myeloid differentiation. Cancer Genet
Cytogenet. 1996;86:153–5.
5. Mitelman F, Johansson B, Mertens F (eds) Mitelman Database of
Chromosome Aberrations in Cancer (2007). Available at:
http://www. cgap.nci.nih.gov/Chromosomes/Mitelman. Accessed
on June 1 (2007).
6. Heim S, Bekassy AN, Garwicz S, et al. Bone marrow karyotypes
in 94 children with acute leukemia. Eur J Haematol.
1990;44:227–33.
7. Lelong F, Chretien P, Jouault H, et al. A case of peroxidase-
positive acute leukaemia expressing only T lineage lymphoid
markers. Br J Haematol. 1994;86:195–7.
8. Winick NJ, McKenna R, Shuster J, et al. Secondary acute mye-
loid leukemia in children with acute lymphoblastic leukemia
treated with etoposide. J Clin Oncol 1993;11: 209–17.
9. Abla O, Dror Y, Shago M. Translocation (X;10) in a child with
therapy-related acute myeloid leukemia following chemotherapy
for Ewing’s Sarcoma. Cancer Genet Cytogenet. 2007;178:168–9.
10. Ackland SP, Westbrook CA, Diaz MO, et al. Evidence favoring
lineage fidelity in acute nonlymphocytic leukemia: absence of
immunoglobulin gene rearrangements in FAB types M4 and M5.
Blood. 1987;69:87–91.
11. Weiss J, De Vito V, Allen L, et al. Translocation X;10 in a case of
congenital acute monocytic leukemia. Cancer Genet Cytogenet.
1985;16:357–64.
Fig. 2 Fluorescence in situ hybridization using whole chromosome
paint probes for chromosomes X (red) and 10 (green) disclosed a
reciprocal translocation between chromosomes X and 10
1136 Med Oncol (2012) 29:1134–1136
123