Embed Size (px)
Citation preview
Thorax 1987;42:296-301
Transmission electron microscopy of percutaneousfine needle aspirates from lung: a study of 70 casesD C DAVIES, A J RUSSELL, R TAYAR, N T COOKE, M M LEVENE
From the Regional Cell Pathology Service, Wandle Valley Hospital, Mitcham Junction, Surrey, and DepartmentsofRadiology and Medicine, St Helier Hospital, Carshalton, Surrey
ABSTRACT Seventy consecutive lung fine needle aspirates (FNA) from 69 patients were examined bycytology/cell block histology, by transmission electron microscopy (TEM), and, where available, athistological follow up to determine the value of TEM in interpreting lung FNAs. Of 70 FNAs, 50were suitable for TEM. Transmission electron microscopy was helpful in classifying seven of 10poorly differentiated tumours, and two case histories are reported. In 26 of 30 well differentiatedtumours TEM confirmed diagnosis by light microscopy. Two TEM false negatives, but no TEMfalse positives, were recorded. It is concluded that transmission electron microscopy of cells aspi-rated from lung can be helpful when unequivocal diagnosis has not been achieved.
Percutaneous fine needle aspiration (FNA) biopsymethods are widely used in the investigation of lungdisease.' 2 Aspirated specimens are examined cyto-logically or, less commonly, embedded for cell blockhistology.3`6 Methods for processing FNAs fortransmission electron microscopy (TEM) have alsobeen reported with good results,7-12 but TEM is notwidely used, despite its apparent value in the diagno-sis of lung disease. 3 -16
Specific diagnosis of cells aspirated from lung isvital as it largely determines treatment,'7-21 but toour knowledge there has been only one publicationthat offers a detailed examination of the potential ofTEM in interpreting lung FNAs." We report theresults of 70 consecutive FNAs of lung examined bycytology and cell block histology, by TEM, and atfollow up and assess the role of TEM in evaluatinglung FNAs with particular reference to two casehistories.
Patients and methods
From September 1983 to November 1985, 70consecutive FNAs were performed on 69 patients.Patients were selected who had a lesion demonstrableby conventional radiography and computed tomo-graphy (CT) but normal or equivocal findings on
Address for reprint requests: Dr A J Russell, Regional Cell Pathol-ogy Service, Wandle Valley Hospital, Mitcham Junction, Surrey CR44XL.
Accepted 28 November 1986
sputum cytology and negative results from bron-choscopy and lavage.Most biopsy examinations were carried out under
dual image intensification, but for small lesions,where lateral visualisation proved difficult, materialwas best obtained under CT control. A range ofneedles was used, the best results being obtained withthe 22 gauge Franseen type. Pneumothorax occurredin about 10% of patients, and on two occasions achest drain was necessary. No important haemoptysisoccurred.
Aspirated material was expressed onto clean glassslides and tissue fragments removed and fixed for cellblock histology and TEM. Smears made from thematerial that remained on the slides were either wetfixed in 99% alcohol for Papanicolaou orhaematoxylin and eosin staining or air dried and fixedin methanol for Romanowsky or periodic acid-Schiffstaining. For cell block histology, tissue fragmentswere fixed in 10% buffered formal saline, embeddedin agar, wax processed, sectioned at 5 gm, and stainedwith haematoxylin and eosin.
Tissue fragments were fixed for TEM in 1-2%phosphate buffered glutaraldehyde for 30-60minutes, post-fixed in 1% phosphate bufferedosmium tetroxide, and embedded in epoxy resin.Smears from seven cases were fixed and processed bythe "pop-off" technique.1022 One micron sectionswere stained with toluidine blue to locate areas forstudy. Ultrathin sections of these areas were stainedwith 3% alcoholic uranyl acetate and Reynolds' leadcitrate and examined with an AEI EM6B trans-
296
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.4.296 on 1 April 1987. D
ownloaded from
Transmission electron microscopy ofpercutaneous fine needle aspirates from lungmission electron microscope at 80 kV.
Smears and cell block preparations were examinedto give an overall cytology/cell block histology assess-ment. TEM assessment was made without referenceto cytology and cell block histology preparations orto follow up histology. The ultrastructural features oflung tumours used in diagnosis are defined else-where.' 11 23-25 Follow up information wasobtained in 42 cases from lung resection, necropsy, orobservation of the natural history of the disease, andtumours were classified according to the 1981classification of the World Health Organisation.26
Results
Table I shows the results of cytology/cell block histol-ogy and TEM. Of the 70 aspirates, 43 yielded positiveresults on cytology/cell block histology (tumour cellsidentified), five showed atypical features (suspiciousbut not obviously malignant cells present), 11 gavenegative results (good sample, but no tumour orsuspicious cells identified), and a further 11 aspirateswere inadequate (poor sample with only blood,macrophages, or necrotic material present). Fiftyspecimens could be classified as positive, atypical, ornegative by TEM. The remaining 20 were inadequate.
Table 2 compares diagnoses obtained by TEM,cytology/cell block histology, and follow up histol-ogy. Cytologically, the 50 cases suitable for TEMcomprised 30 well differentiated tumours, 10 poorlydifferentiated tumours, three atypical cases, and seven
Table 1 Broad classification of 70 consecutivefine needleaspirates examined by cytology/cell block histology and bytransmission electron microscopy
Classificationfrom No Classificationfrom Nocytology/cell block of transmission electron ofhistology cases microscopy cases
Positive 43 Positive 36Atypical 4Negative 0Inadequate 3
Atypical 5 Positive IAtypical 0Negative 2Inadequate 2
Negative II Positive 0Atypical 2Negative 5Inadequate 4
Inadequate I I Positive 0Atypical 0Negative 0Inadequate 11
Total 70 70
negative cases. The seven "pop-off' specimens wereall well differentiated tumours (six epidermoid andone small cell), and this diagnosis agreed with TEMdiagnosis from tissue fragments.
There was good agreement between cytology/cellblock histology, TEM, and follow up information inthe 21 well differentiated epidermoid tumours, thediagnosis being confirmed in 19 by TEM and in 13 atfollow up. Two cases were judged to be epidermoid byTEM but at follow up were considered to be
Table 2 Diagnosis in 50fine needle aspirates in which material was adequatefor transmission electron microscopy
Cytology/cell block Transmission electron Follow up Nofollow updiagnosis microscopy diagnosis diagnosis available
Epidermoid carcinoma 21 Epidermoid carcinoma 19 Epidermoid carcinoma 13 4Adenosquamous carcinoma IUndifferentiated carcinoma I
Adenosquamous carcinoma I Adenocarcinoma IAtypical I Large cell carcinoma I
Adenosquamous carcinoma I Adenosquamous carcinoma I Adenocarcinoma IAdenocarcinoma 3 Adenocarcinoma 2
Atypical I AdenocarcinomaSmall cell carcinoma 4 Small cell carcinoma 3 Small cell carcinoma 2
Large cell carcinoma IAtypical I Small cell carcinoma I
Chondrosarcoma I Chondrosarcoma I Chondrosarcoma IUndifferentiated carcinoma 10 Epidermoid carcinoma 3 Epidermoid carcinoma 1 2
Adenosquamous carcinoma I IAdenocarcinoma I Adenocarcinoma ISmall cell carcinoma 2 Small cell carcinoma 2Undifferentiated carcinoma 2 Metastatic carcinoma 2Atypical I Small cell carcinoma I
Atypical 3 Adenosquamous carcinoma I INegative 2 Negative 2
Negative 7 Atypical 2 Epidermoid carcinoma 2Negative 5 Negative 3
Large cell carcinoma 2Total 50 50 42 8
297
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.4.296 on 1 April 1987. D
ownloaded from
follow up.Of three cases reported as atypical at cytology/cell
4 block histology, one, without follow up, wasadenosquamous carcinoma at TEM and two werenegative at TEM and at follow up. Of the seven cases
tw 7 X __ 9jwhereresults of cytology/cell block histology werenegative, two were considered to be atypical at TEMand epidermoid at follow up and two negative atTEM but large cell at follow up (TEM false nega-tives). No TEM false positives were encountered.
Case reports
|-_| - X _Xa,_ b~~~~~ase I
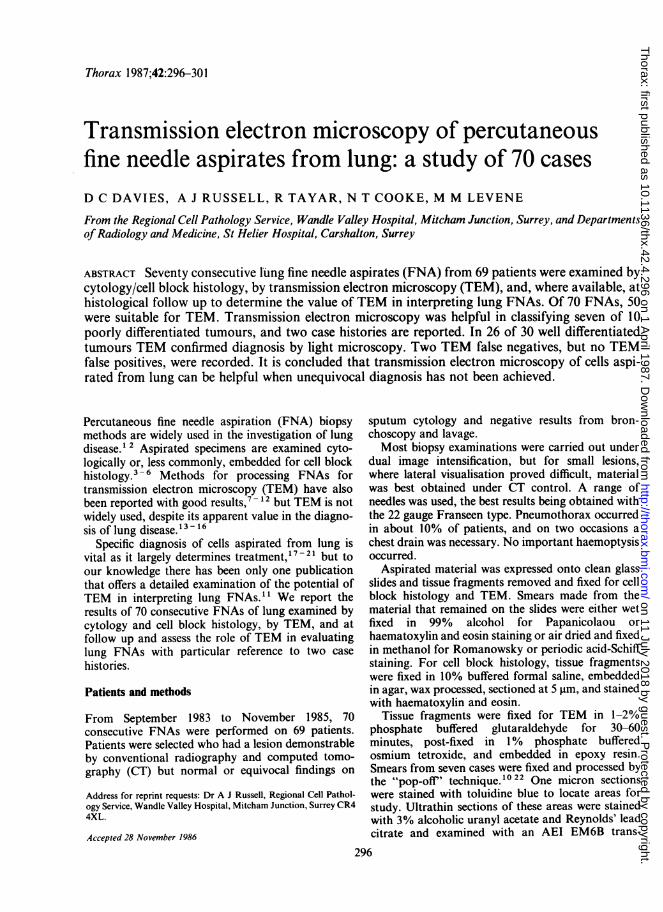
01 ? * wA 65 year old woman presented with persistent coughand shortness of breath. She was a smoker and haddiabetes and a history of bronchitis. A chest radio-graph showed shadowing in the left lower lobe.Cytology/cell block histology revealed pleomorphic,undifferentiated tumour cells with a homogenouscytoplasm, lying singly or in groups (Fig. 1). Nuclearvariation was present, chromatin was coarse, andoccasional nucleoli were seen. At TEM tumour cells
~~~~~~;.es. . | .4 :~#Y ow*N....Av *i
Fig I Cytological smear from case 1, with cells showingnuclear variation, coarse chromatin, and occasional nucleoli.(Haematoxylin and eosin.)
adenosquamous and undifferentiated carcinomas. Nofollow up material was available from four cases. Onetumour, found to have an adenocarcinomatouselement at TEM. was subsequently classified asadenocarcinoma. A further case was judged as atypi-cal at TEM and as large cell carcinoma at follow up.Agreement was fairly good in eight cases of well
differentiated adenosquamous carcinoma, adeno-carcinoma, and small cell carcinoma, although in twothe TEM appearances were considered to be atypicalrather than positive and one tumour initiallyclassified as small cell later proved to be a large cell ~carcinoma. In the patient with chondrosarcomacytology/cell block histology, TEM, and informationobtained at follow up were in complete agreement.TEM was helpful in the diagnosis of seven of the 10
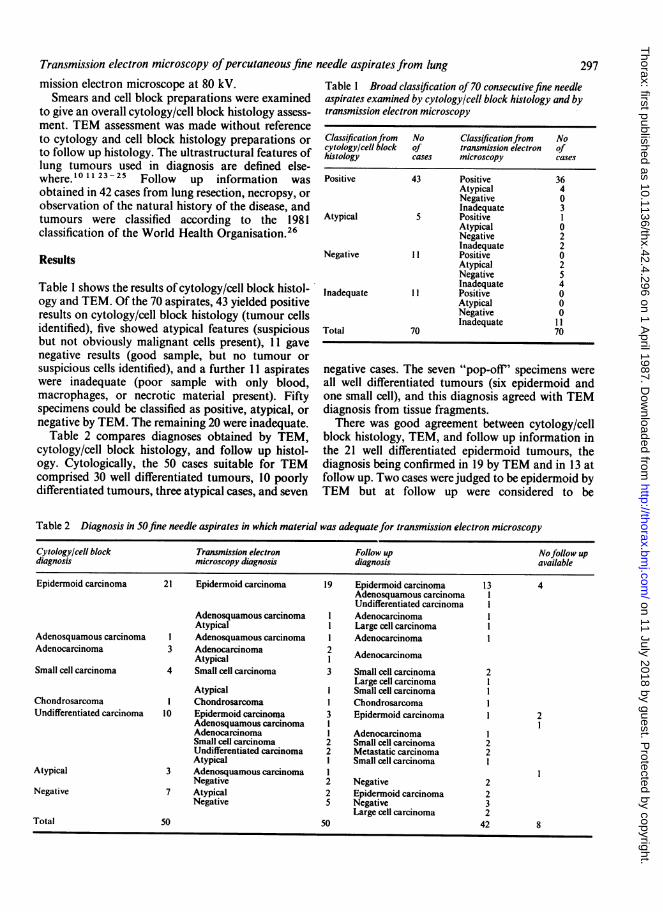
undifferentiated tumours, and in four instances it waspossible to confirm the diagnosis at follow-up. Thevalue ofTEM is illustrated further by reference to twoof these examples as case reports (below). Of the threeremaining undifferentiated tumours, two were Fig 2 Transmission ekctron micrograph from case 1classified as undifferentiated at TEM and untyped Cells with apical microvilli, abundant cytoplasm withmetastatic carcinomas at follow up and one was ribosomes and mitochondria, and large irregular nuclei withconsidered to be atypical at TEM and small cell at prominent nucleoli.
298 Davies, Russell.- Tayar, Cooke, Levene
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.4.296 on 1 April 1987. D
ownloaded from
Transmission electron microscopy ofpercutaneous fine needle aspirates from lung
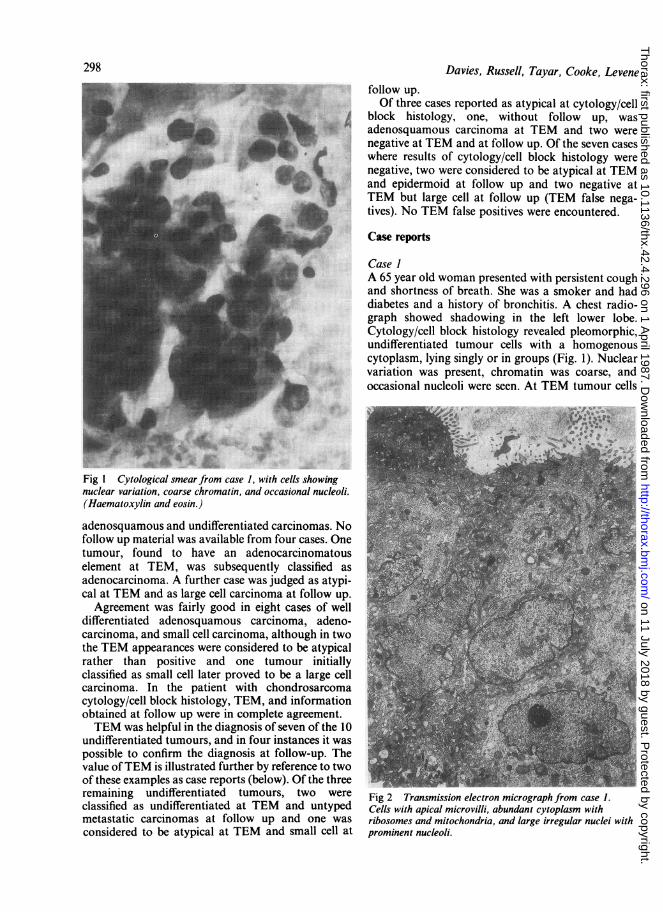
Fig 3 Cytological smear from case 2. Cells with little or
no cytoplasm, showing nuclear variation, coarse chromatin,and occasional nucleoli. (Haematoxylin and eosin.)
showed features of adenocarcinoma, with apicalmicrovilli, abundant ribosomes, mitochondria,Golgi's corpuscles, accumulations of glycogen, andtight junctional complexes (Fig. 2). Nuclei were large,often with indented membranes, and nucleoli wereprominent. Wedge resection of the apex of the leftlower lobe revealed an adenocarcinoma 2 cm indiameter, with central necrosis and some papillarydifferentiation. The patient has since died.
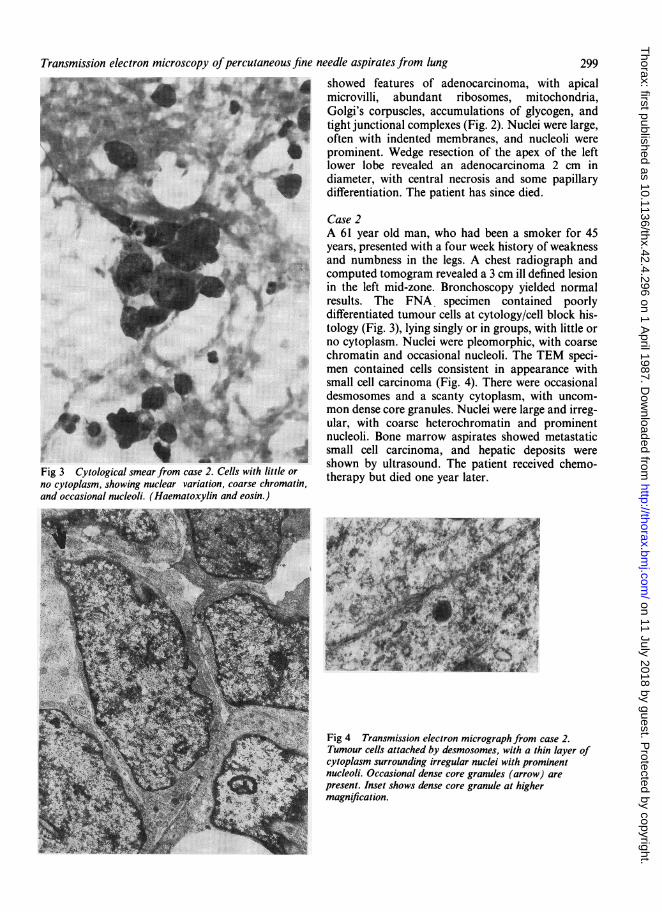
Case 2A 61 year old man, who had been a smoker for 45years, presented with a four week history of weaknessand numbness in the legs. A chest radiograph andcomputed tomogram revealed a 3 cm ill defined lesionin the left mid-zone. Bronchoscopy yielded normalresults. The FNA, specimen contained poorlydifferentiated tumour cells at cytology/cell block his-tology (Fig. 3), lying singly or in groups, with little orno cytoplasm. Nuclei were pleomorphic, with coarsechromatin and occasional nucleoli. The TEM speci-men contained cells consistent in appearance withsmall cell carcinoma (Fig. 4). There were occasionaldesmosomes and a scanty cytoplasm, with uncom-mon dense core granules. Nuclei were large and irreg-ular, with coarse heterochromatin and prominentnucleoli. Bone marrow aspirates showed metastaticsmall cell carcinoma, and hepatic deposits wereshown by ultrasound. The patient received chemo-therapy but died one year later.
Fig 4 Transmission electron micrograph from case 2.Tumour cells attached by desmosomes, with a thin layer ofcytoplasm surrounding irregular nuclei with prominentnucleoli. Occasional dense core granules (arrow) arepresent. Inset shows dense core granule at highermagnification.
299
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.4.296 on 1 April 1987. D
ownloaded from

300Discussion
There are few published ultrastructural studies ofFNA derived lung material and there is little withwhich to compare our results. Two useful con-tributions are from Sehested and his coworkers, usingpelleted aspirates,' 1 and from di Sant' Agnese, basedon a modified "pop-off' technique.'0
Like us, Sehested et al recorded one third of theirconsecutive aspirates unsuitable for TEM," despiteour using tissue fragments and, in a few cases, "pop-off' specimens. Others have noted a greater propor-tion of aspirates suitable for TEM using a pelletingtechnique,'4 although not all the material was derivedfrom lung. The "pop-off' technique apparentlyincreases the chances of locating suspicious cells.'0 22We have not compared this technique critically withmore traditional methods, but our limited obser-vations suggest that preparation time is similar to thatfor tissue fragments, although embedding and cuttingcan be more demanding. In the few comparable caseswe found tumour cells as quickly in tissue fragmentblocks, but the "pop-off' method may be beneficialwhen such cells are scarce.
Sehested et al recorded full agreement between theresults of cytology and TEM in all cases of welldifferentiated squamous cell carcinoma, small cellcarcinoma and adenocarcinoma." We did notachieve such agreement, but our results were broadlysimilar. We agree with others that in cases whereTEM does not significantly contribute to diagnosis itsuse may be unjustified. 14 - 16 Specimens can, however,be held in glutaraldehyde as Berkman et al have advo-cated, 14 so that TEM material can be prepared later ifcytohistological diagnosis is not specific.
Although poor light microscopic differentiation isoften paralleled at TEM, paradoxically it is in theclassification of poorly differentiated tumours thatTEM is most useful." 16 Poorly differentiatedtumours may show features that aid diagnosis, suchas tonofilaments, microvilli, dense core gran-ules, 10 11 15 16 23 - 25 although these structures mustbe interpreted with caution as some are shared byseveral cell types.'6 27-29 We found TEM helpful inseven of 10 poorly differentiated cases, four of whichwere confirmed at follow up. This figure is differentfrom that of Sehested et al (seven of eight with threeconfirmed at follow up)," but their results, togetherwith our two case reports, indicate the value ofTEMdiagnosis for poorly differentiated lung tumours.Some workers have reported the value of TEM indiagnosis of metastatic lesions, '4 whereas others havefound it of limited usefulness.'8 In two cases of meta-static carcinoma in our study TEM was unhelpful indetermining cell type or origin.The major disadvantages of FNAs at light micro-
Davies, Russell, Tayar, Cooke, Levene
scopy are sample size, sampling error, and vari-ation,' - 3 30 31 and these also apply to TEM of FNAderived material. Large resected lung specimens, forexample, may reveal a heterogeneity not apparent insmall FNA specimens.29 For this reason we havetried to compare, where possible, the results of cytol-ogy and TEM with those of follow up histology. Oneof our cases was diagnosed as epidermoid carcinomaby cytology/cell block histology and adenosquamouscarcinoma by TEM but as adenocarcinoma at followup. Such inconsistencies are inevitable where mixedlung tumours occur. A further example, classified assmall cell carcincma at light microscopy and TEM,eventually proved to be large cell carcinoma. We can-not explain this discrepancy but note that tumoursclassified histologically as large cell mostly exhibitfeatures of small cell carcinoma or adenocarcinoma atTEM.13
In conclusion, we agree with others"14 16 that thegreatest value of transmission electron microscopyfor lung FNAs is in the typing of poorly differentiatedtumours. It may also be of value in supporting orconfirming the light microscopy diagnosis for welldifferentiated tumours, but its use in the diagnosis ofmetastatic tumours may be limited.
Thanks are due to Mrs J Ardley for technical help, DrW Landells for allowing us access to histologicalreports, and Mrs B Blackmore for typing the manu-script.
References
I Linsk JA, Franzen S. Clinical aspiration cytology. Phila-delphia: J B Lippincott, 1983.
2 Koss LG, Woyke S, Olszewski W. Aspiration biopsy:cytologic interpretation and histological bases. NewYork: Igaku-Shoin, 1984.
3 Kline TS, Neal HS. Needle aspiration biopsy - a criticalappraisal. Eight years and 3267 specimens later.JAMA 1978;239:36-9.
4 Pilotti S, Rilke F, Gribandi G, Damascelli B. Fine needleaspiration biopsy cytology of primary and metastaticpulmonary tumours. Acta Cytol (Baltimore)1982;26:661-6.
5 Pilotti S, Rilke F, Gribandi G, Damascelli B, Ravasi G.Transthoracic fine needle aspiration biopsy in pul-monary lesions. Updated results. Acta Cytol (Bal-timore) 1984;28:225-32.
6 Stevens GM, Jackman RJ. Outpatient needle biopsy ofthe lung: its safety and utility. Radiology 1984;151:301-4.
7 Hagelqvist E. Light and electron microscopic studies onmaterial obtained by fine needle biopsy. Acta Oto-laryngol [Suppli (Stockh) 1978;354:1-75.
8 Akhtar M, Ali MA, Owen EW, Bakry M. A simplemethod for processing fine needle aspiration biopsyspecimens for electron microscopy. J Clin Pathol1980;33:1214-6.
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.4.296 on 1 April 1987. D
ownloaded from
Transmission electron microscopy ofpercutaneous fine needle aspirates from lung9 Akhtar M, Ali MA, Owen EW. Application of electron
microscopy in the interpretation of fine needle aspi-ration biopsies. Cancer 1981;48:2458-63.
10 di Sant' Agnese PA. Diagnostic electron microscopic andtransthoracic fine needle biopsy. In: Bonfiglio TA, ed.Cytopathologic interpretation of transthoracic fineneedle biopsies. New York: Masson Publishing,1983:175-85.
11 Sehested M, Francis D, Hainan B. Electron microscopyof transthoracic fine needle aspiration biopsies. ActaPathol Microbiol Immunol Scand [A] 1983; 91:457-61.
12 di'Sant Agnese PA, de Mesy Jensen KL, Bonfiglio TA,King DE, Patten SF. Plastic-embedded semi-thin sec-tions of fine needle aspiration biopsies with dibasicstaining. Acta Cytol (Baltimore) 1985;29:475-83.
13 Leong ASY. The relevance of ultrastructural exam-
ination in the classification of primary lung tumours.Pathology 1982;14:37-46.
14 Berkman WA, Chowdhury L, Brown NL, Padleckas R.Value of electron microscopy in cytologic diagnosis offine needle biopsy. AJR 1983;140:1253-8.
15 Wang NS. Application of electron microscopy todiagnostic pulmonary pathology. Hum Pathol1983;14:888-900.
16 Fisher C, Ramsay AD, Griffiths M, McDougall J. Anassessment of the value of electron microscopy intumour diagnosis. J Clin Pathol 1985;38:403-8.
17 Dahlgren S, Nordenstrom B. Transthoracic needlebiopsy. Stockholm: Almqvist and Wiksell, 1966.
18 Payne CR, Stovin PGI, Barker V, McVittie S, Stark JE.Diagnostic accuracy of cytology and biopsy in pri-mary bronchial carcinoma. Thorax 1979;34:294-9.
19 Thornbury JR, Burke DP, Naylor B. Transthoracicneedle aspiration; accuracy of cytological typing ofmalignant neoplasm. AJR 1981;136:719-27.
20 Dick R, Timmis B. Percutaneous needle biopsy ofpulmonary tumours. In: Bates M, ed. Bronchialcarcinoma. An integrated approach to diagnosis and
management. Berlin: Springer-Verlag, 1984:77-85.21 Sheppard MN, Corrin B, Bloom SR, Polak JM. Lung
endocrine tumours. In: Polak JM, Bloom SR, eds.Endocrine tumours. The pathology of regulatorypeptide-producing tumours. Edinburgh: ChurchillLivingstone, 1985:209-28.
22 Coleman DV, Russell WJI, Hodgson J, Tun PE, Mow-bray JF. Human papovavirus in Papanicolaou smearsof urinary sediment detected by transmission electronmicroscopy. J Clin Pathol 1977;30:1015-20.
23 Mennemeyer R, Hammar SP, Bauermeister DE, WhellisRF, Jones HW, Bartha M. Cytologic, histologic andelectron microscopic correlations in poorlydifferentiated primary lung carcinoma. Acta Cytol(Baltimore) 1979;23:297-302.
24 Ghadially FN. Diagnostic electron microscopy oftumours. London: Butterworths, 1980.
25 Mackay B. Introduction to diagnostic electron micro-scopy. New York: Appleton-Century-Crofts, 1981.
26 World Health Organisation. Histological typing of lungtumours. 2nd ed. Geneva: WHO, 1981. (InternationalHistological Classification of Tumours No 1.)
27 Wilson TS, McDowell EM, Marangos PJ, Trump BF.Histochemical studies of dense-core granulatedtumours of the lung. Arch Pathol Lab Med1985;109:613-20.
28 Wilson TS, McDowell EM, Trump BF. Immuno-histochemical studies of keratin in human bronchusand lung tumours. Arch Pathol Lab Med 1985;109:621-8.
29 Dunnill MS, Gatter KC. Cellular heterogeneity in lungcancer. Histopathology 1986;10:461-75.
30 Kline TS. Handbook of fine needle aspiration biopsycytology. St Louis: C V Mosby, 1981.
31 Hajdu SI, Melamed MR. Limitations of aspirationcytology in the diagnosis of primary neoplasms. ActaCytol (Baltimore) 1984;28:337-45.
301
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.4.296 on 1 April 1987. D
ownloaded from





























