Embed Size (px)
Citation preview
Transmission of MDR-Mtb : Infection Control in Resource Limited Settings
Edward A. Nardell, MDDivision of Social Medicine & Health InequalitiesPulmonary Division, Brigham & Women’s Hospital
Associate Professor, HMS, HSPHPartners In Health
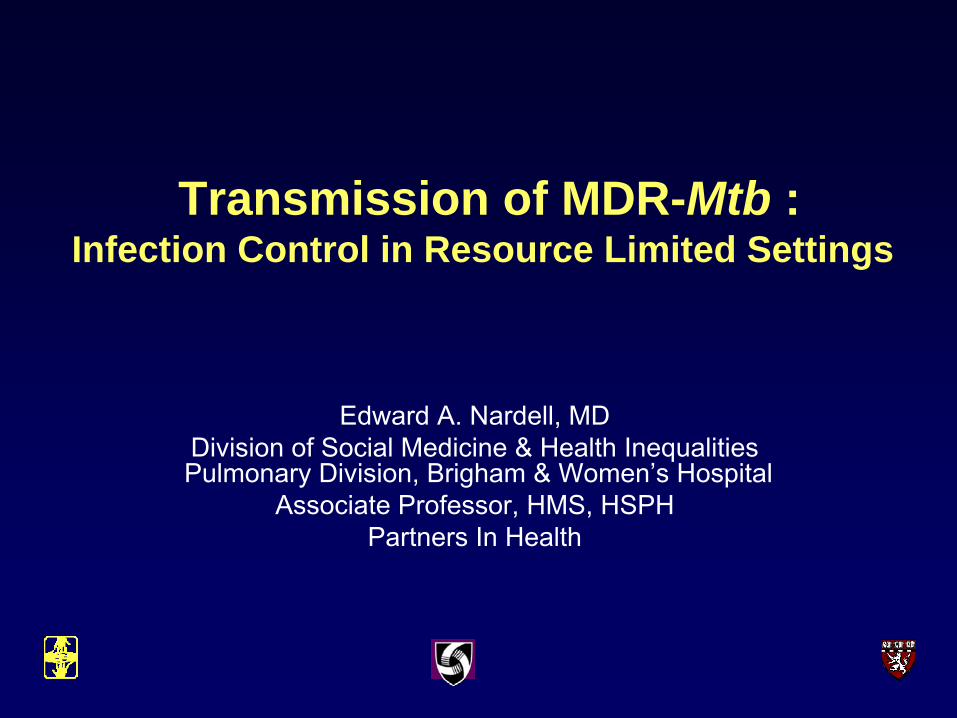
PIH Sites – Cange TB Triage
Community based TB treatment
Hospitalized patients
General ward
Sm -, HIV +/-
TB Pavilion
Sm+, HIV-
6 isolation rms
SM+ and HIV+
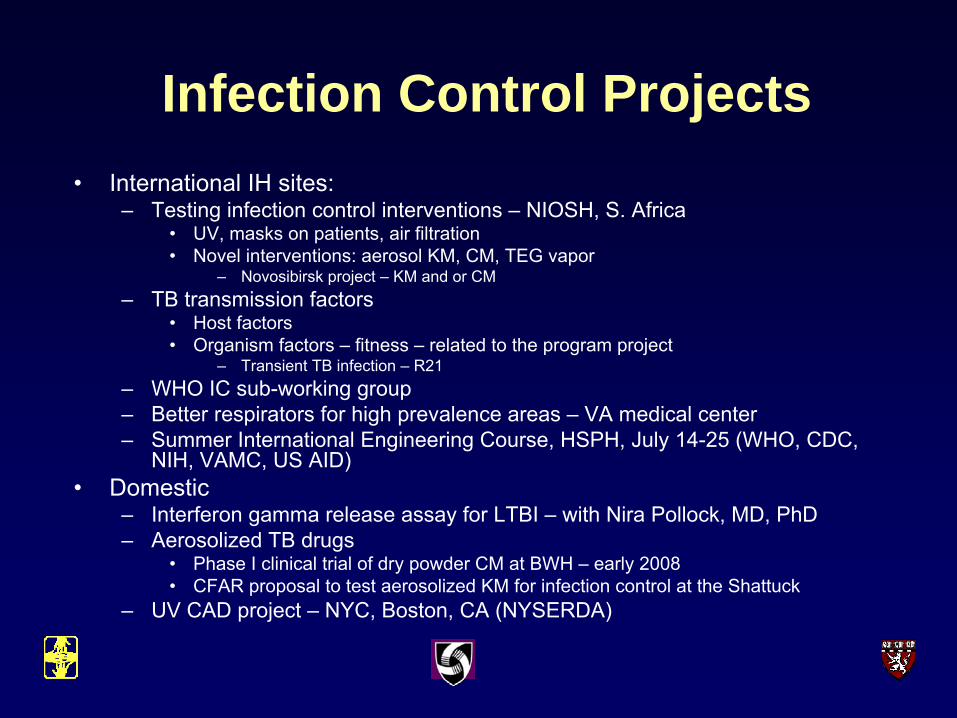
Infection Control Projects• International IH sites:
– Testing infection control interventions – NIOSH, S. Africa• UV, masks on patients, air filtration• Novel interventions: aerosol KM, CM, TEG vapor
– Novosibirsk project – KM and or CM– TB transmission factors
• Host factors • Organism factors – fitness – related to the program project
– Transient TB infection – R21– WHO IC sub-working group– Better respirators for high prevalence areas – VA medical center– Summer International Engineering Course, HSPH, July 14-25 (WHO, CDC,
NIH, VAMC, US AID)• Domestic
– Interferon gamma release assay for LTBI – with Nira Pollock, MD, PhD– Aerosolized TB drugs
• Phase I clinical trial of dry powder CM at BWH – early 2008• CFAR proposal to test aerosolized KM for infection control at the Shattuck
– UV CAD project – NYC, Boston, CA (NYSERDA)
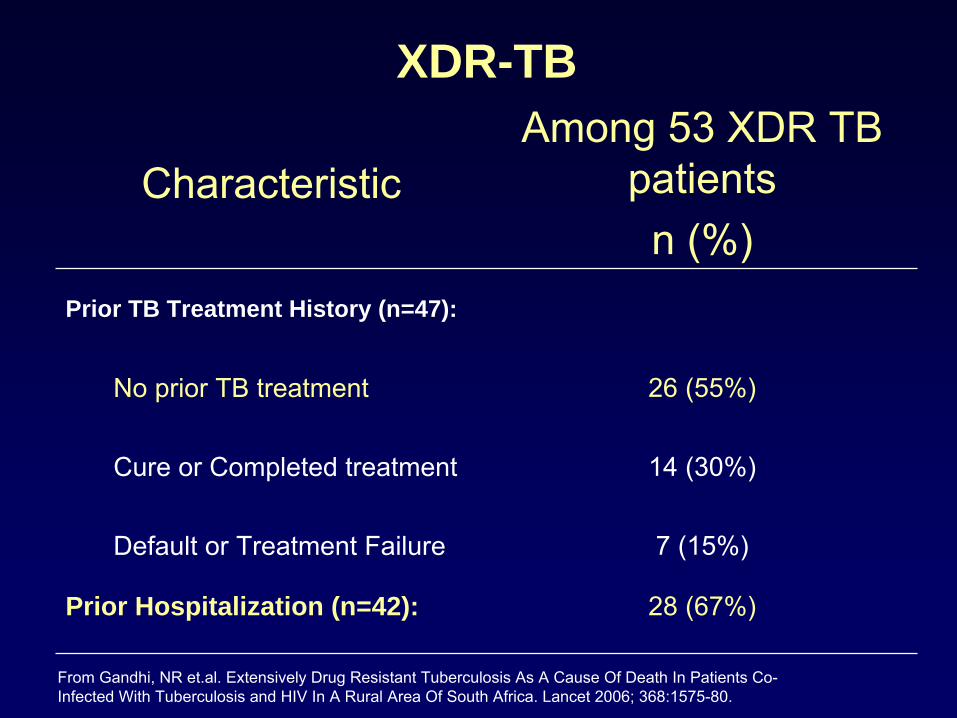
XDR-TB
28 (67%)Prior Hospitalization (n=42):
7 (15%)Default or Treatment Failure
14 (30%)Cure or Completed treatment
26 (55%)No prior TB treatment
Prior TB Treatment History (n=47):
Among 53 XDR TB patientsn (%)
Characteristic
From Gandhi, NR et.al. Extensively Drug Resistant Tuberculosis As A Cause Of Death In Patients Co-Infected With Tuberculosis and HIV In A Rural Area Of South Africa. Lancet 2006; 368:1575-80.
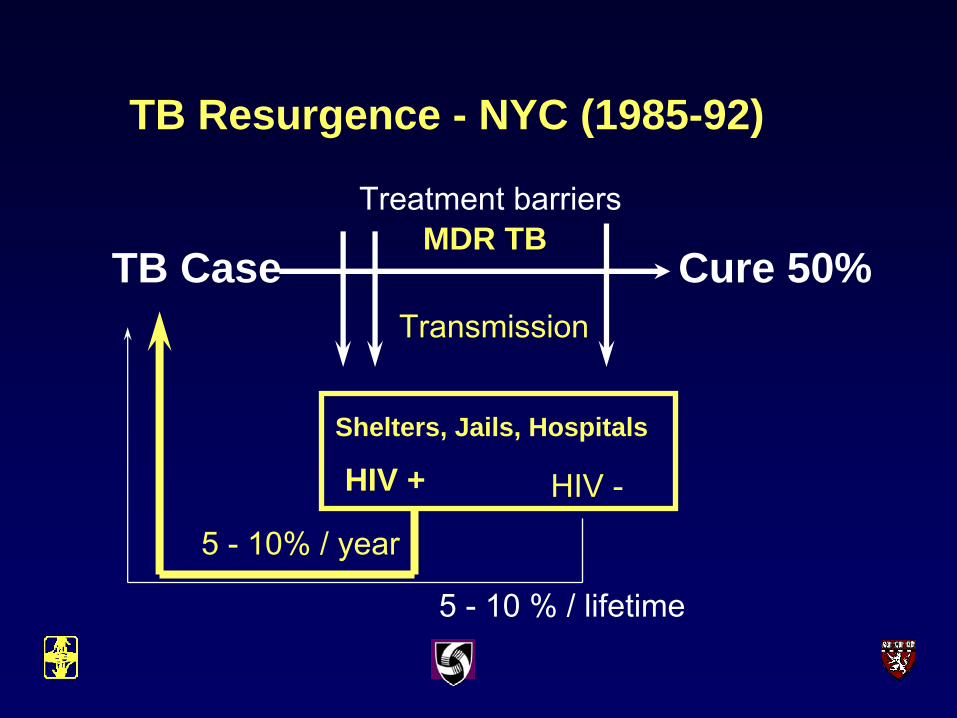
TB Resurgence - NYC (1985-92)
TB Case Cure 50%
Shelters, Jails, Hospitals
Treatment barriers
Transmission
MDR TB
HIV + HIV -
5 - 10 % / lifetime
5 - 10% / year
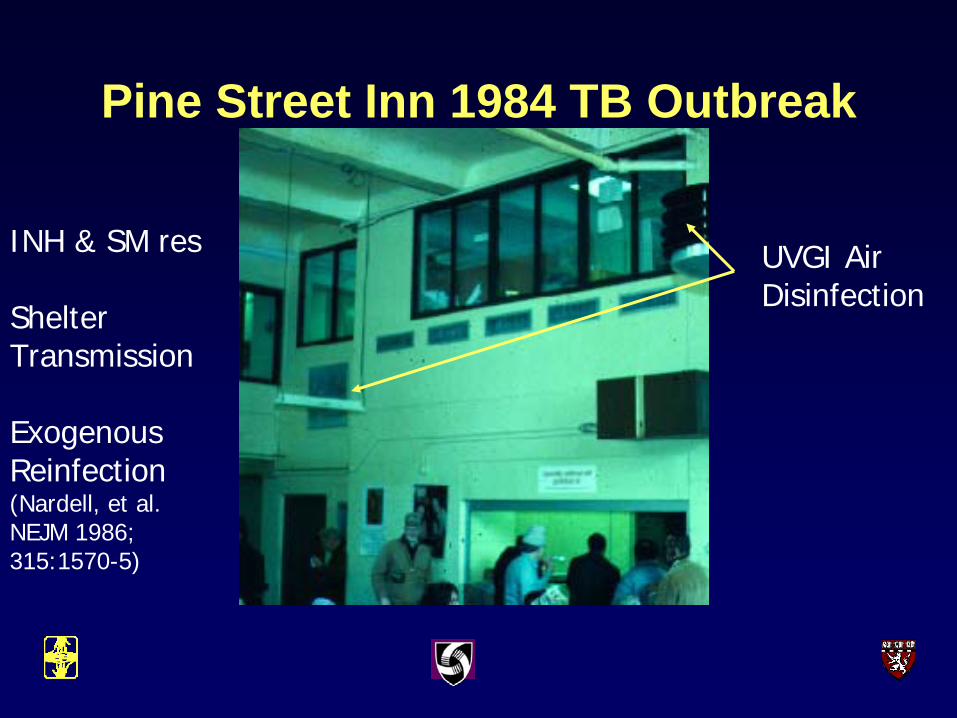
Pine Street Inn 1984 TB Outbreak
INH & SM res
ShelterTransmission
Exogenous Reinfection(Nardell, et al. NEJM 1986; 315:1570-5)
UVGI AirDisinfection
Shelter in Boston, Prison in S.A.
What do we know about M tbtransmission & aerobiology?
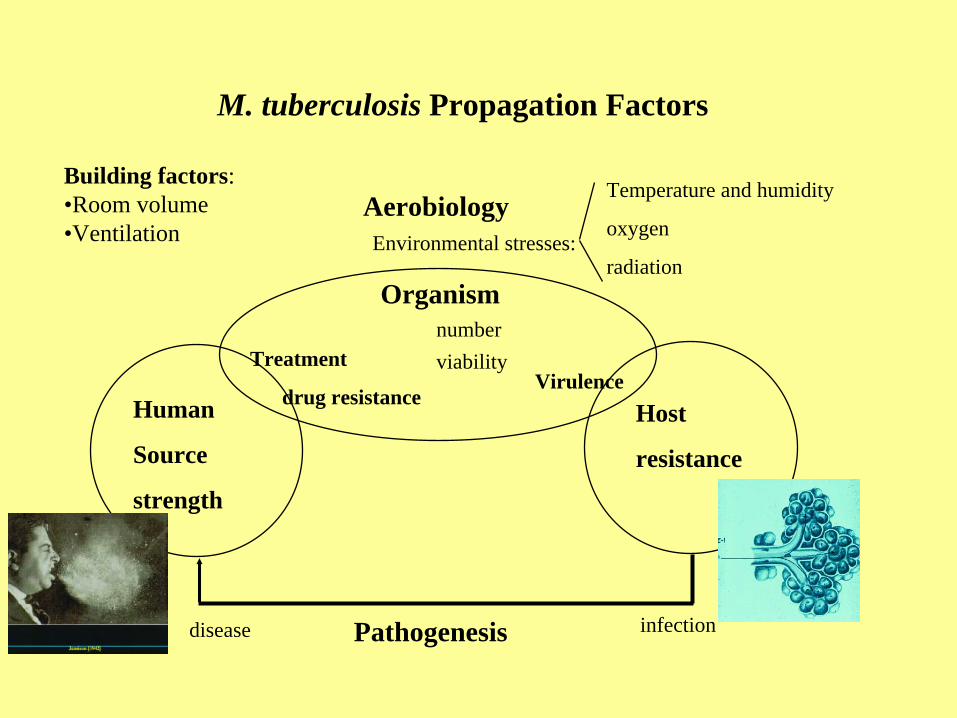
AerobiologyEnvironmental stresses:
Temperature and humidity
oxygen
radiation
Pathogenesis infectiondisease
Host
resistance
Human
Source
strength
Organism
Treatment
drug resistance
numberviability
Virulence
M. tuberculosis Propagation Factors
Building factors:•Room volume•Ventilation
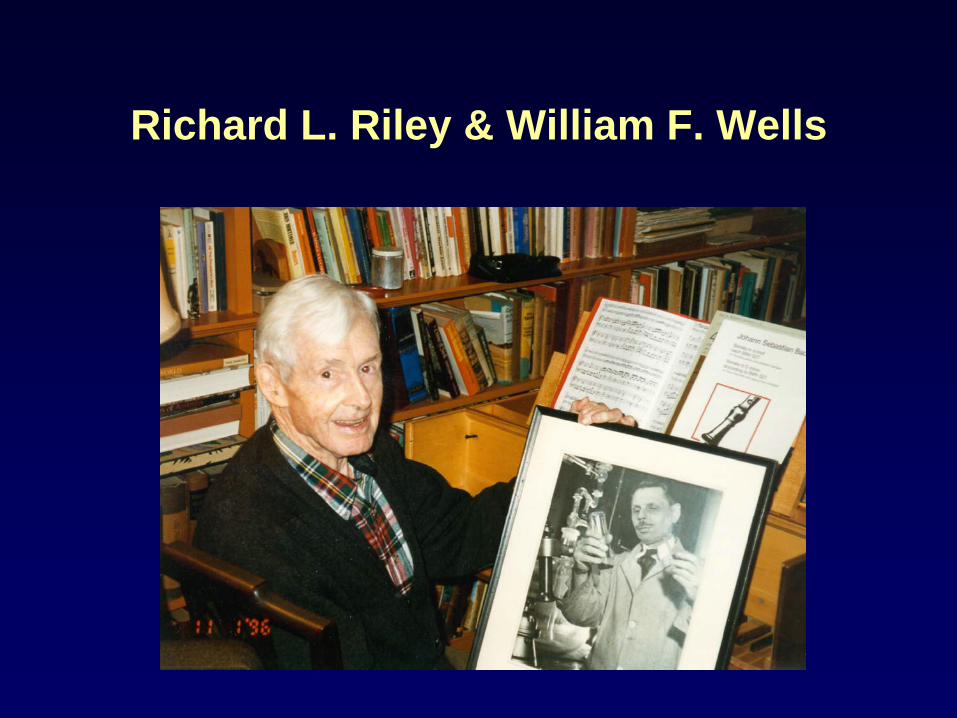
Richard L. Riley & William F. Wells
Wells/Riley Experimental TB Ward• Riley RL, Mills C, Nyka W.
Aerial dissemination of tuberculosis – a two year study of contagion on a tuberculosis ward. Am J Hyg1959; 70:185-196.(reprinted as “classic” Am J Epidemiol 1995; 142:3-14)
• Riley RL. What nobody needs to know about airborne infection. (How It Really Happened) AJRCCM 2001; 163:7-8.
Quantitative air sampling for TB
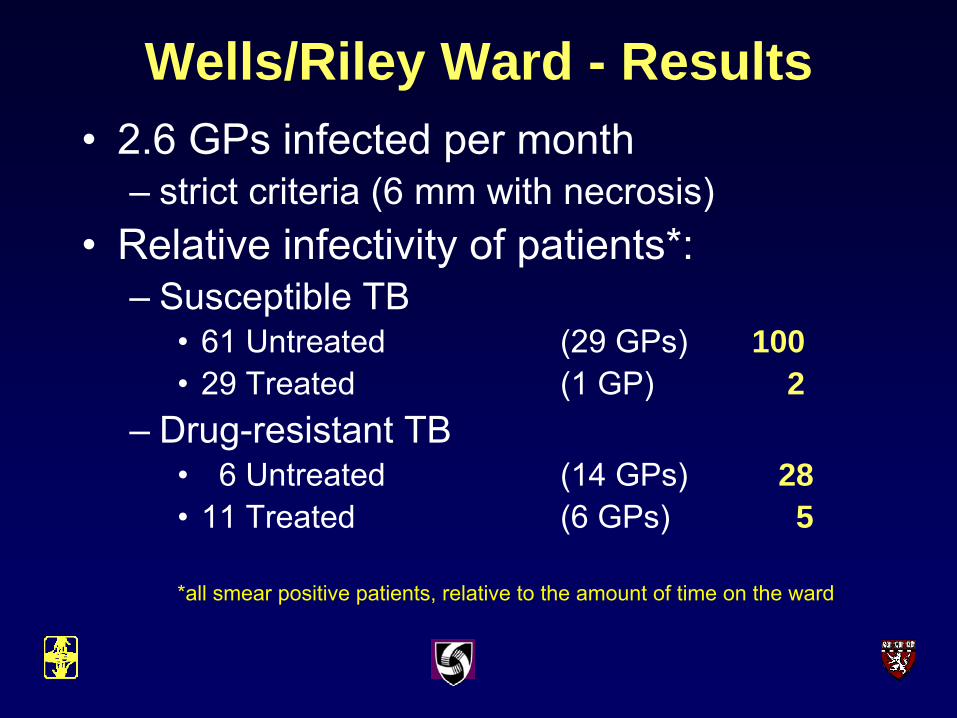
Wells/Riley Ward - Results• 2.6 GPs infected per month
– strict criteria (6 mm with necrosis)• Relative infectivity of patients*:
– Susceptible TB• 61 Untreated (29 GPs) 100• 29 Treated (1 GP) 2
– Drug-resistant TB• 6 Untreated (14 GPs) 28• 11 Treated (6 GPs) 5
*all smear positive patients, relative to the amount of time on the ward
Collaborators:• MRC
– Karin Weyer– Matsie Mphahlele– Kobus Venter– Bernard Fourie
• CSIR– Sidney Parsons
• CDC– Paul Jensen– Charles Wells– Paul Arguin
• Mpumalanga Province
• Harvard– Edward Nardell– Melvin First– Ashwin Dharmadhikari
• Other– Dave McMurray– Randall Basaraba– Paul Van Helden
• Funding– USAID/CDC– MRC– Harvard CFAR– Brigham & Women’s Hospital– NIOSH/NIH RO1
The AIR FacilityWhitbank, Mpumalanga Provence
First Experiment:• 4 months exposure of 360 GPs• 28 different patients in groups of 6• Approximately half HIV pos.• Patient selection
– clinical and lab features associated with infectivity • sm+, cavitary, coughing, recent treatment
• Purpose: Does the AIR facility function as designed?• All animals TST 1-5, and 20 had TST6
– Guinea pig health status monitored– Half ≥ 6 mm were immunosuppressed (dexamethasone)
• All animals sacrificed at month 5– Autopsied, and specimens fixed or frozen for pathology, culture, molecular
fingerprinting• Isolates from guinea pigs and human source patients
– DST, fingerprinted and will be matched

Using 6 mm as pos75% of GPs infected
0
20
40
60
80
100
TST1 2 3 4 5
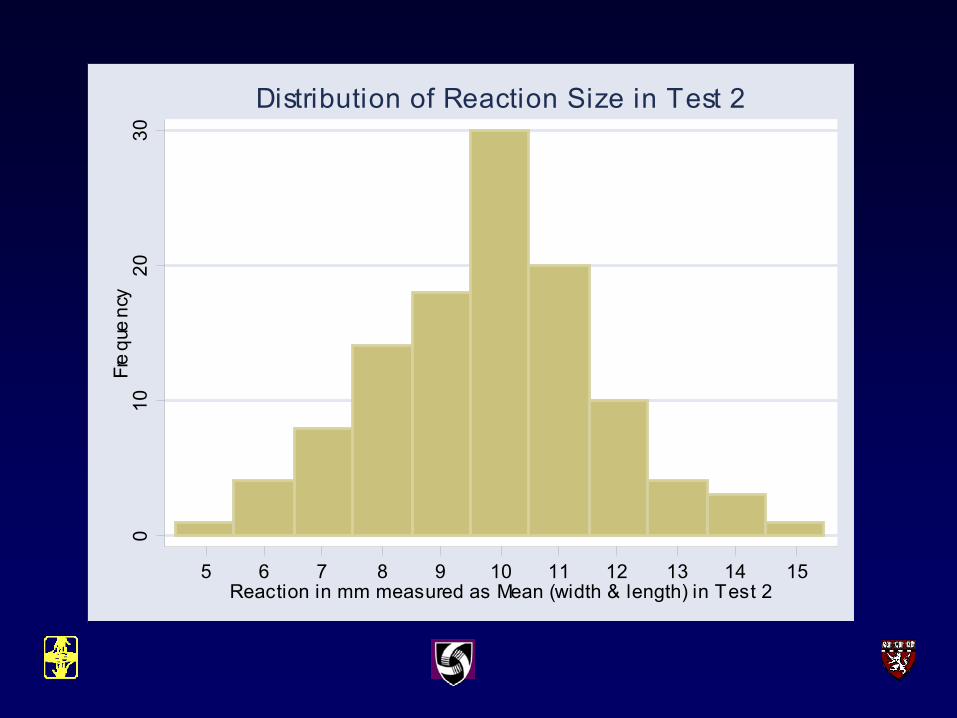
010
2030
Fre
que
ncy
5 6 7 8 9 10 11 12 13 14 15Reaction in mm measured as Mean (width & length) in Test 2
Distribution of Reaction Size in Test 2
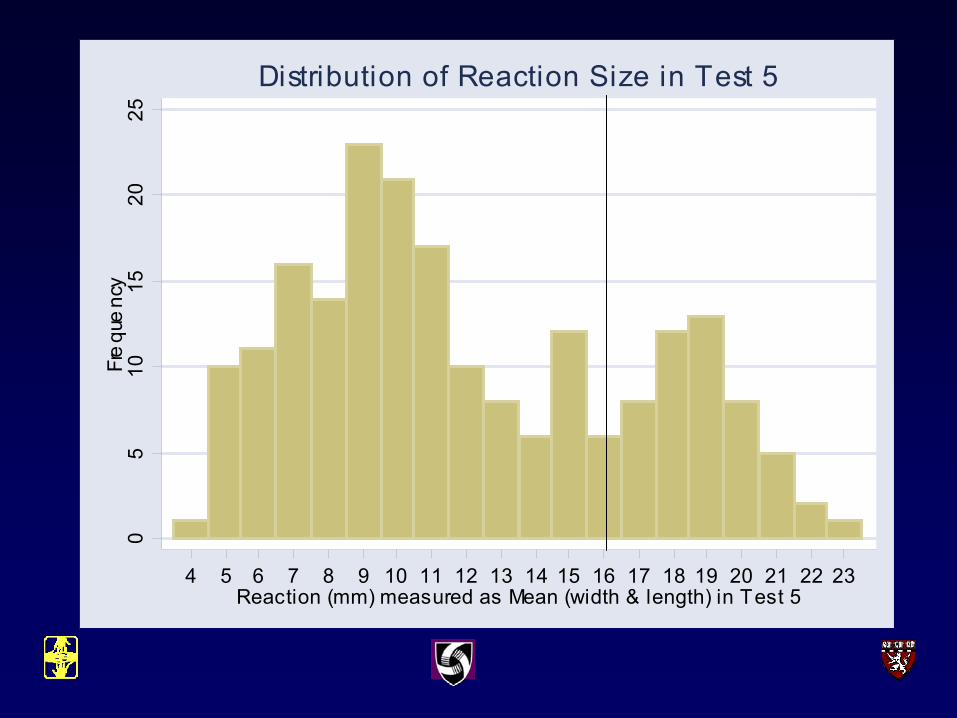
05
1015
2025
Fre
que
ncy
4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23Reaction (mm) measured as Mean (width & length) in Test 5
Distribution of Reaction Size in Test 5
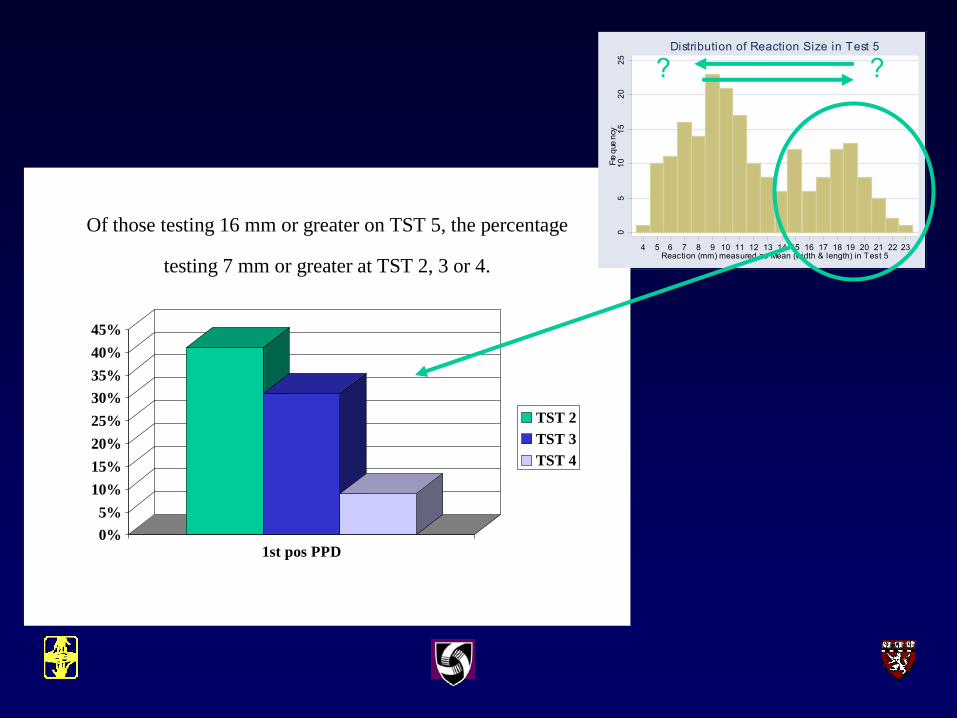
Of those testing 16 mm or greater on TST 5, the percentage
testing 7 mm or greater at TST 2, 3 or 4.
0%5%
10%15%20%25%30%35%40%45%
1st pos PPD
TST 2TST 3TST 4
05
1015
2025
Fre
que
ncy
4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23Reaction (mm) measured as Mean (width & length) in Test 5
Distribution of Reaction Size in Test 5
??
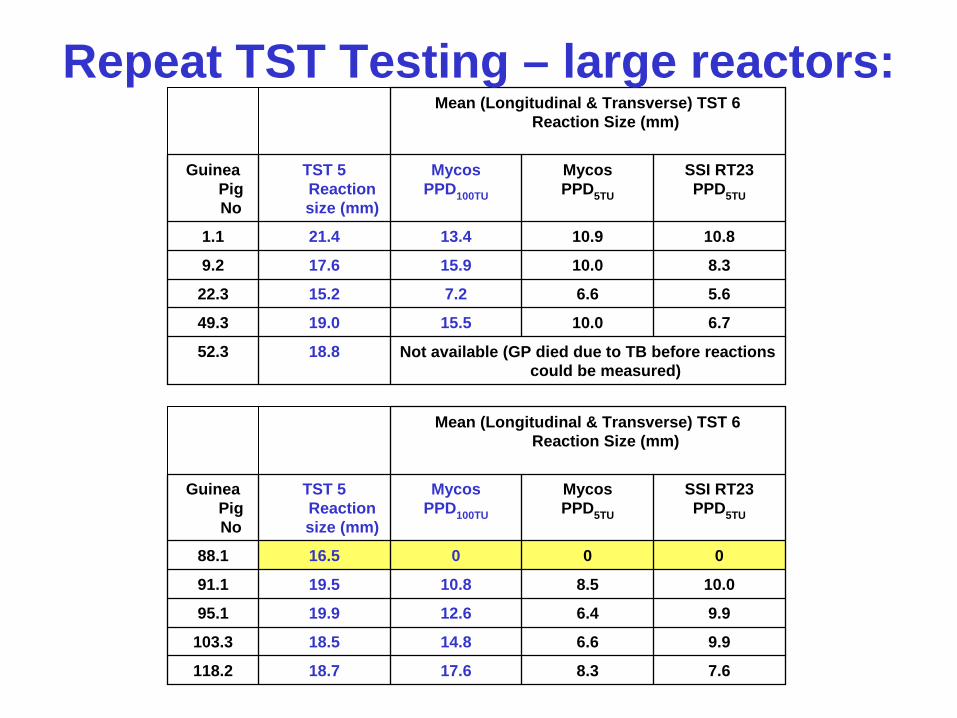
Not available (GP died due to TB before reactions could be measured)
18.852.3
6.710.015.519.049.3
5.66.67.215.222.3
8.310.015.917.69.2
10.810.913.421.41.1
SSI RT23 PPD5TU
MycosPPD5TU
MycosPPD100TU
TST 5 Reaction size (mm)
Guinea Pig No
Mean (Longitudinal & Transverse) TST 6 Reaction Size (mm)
7.68.317.618.7118.2
9.96.614.818.5103.3
9.96.412.619.995.1
10.08.510.819.591.1
00016.588.1
SSI RT23 PPD5TU
MycosPPD5TU
MycosPPD100TU
TST 5 Reaction size (mm)
Guinea Pig No
Mean (Longitudinal & Transverse) TST 6 Reaction Size (mm)
Repeat TST Testing – large reactors:
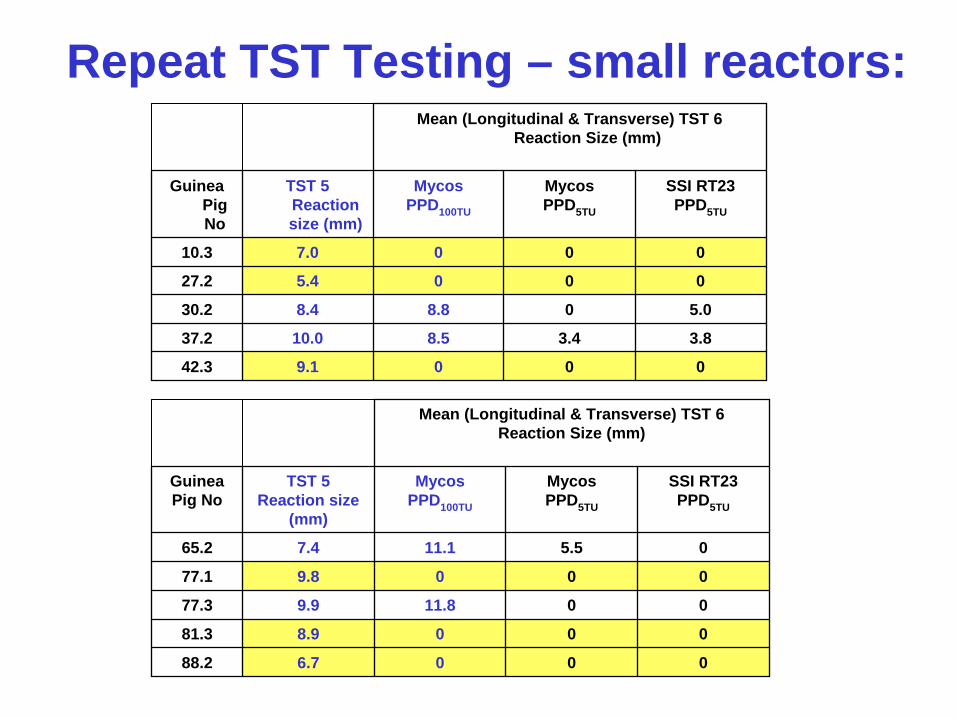
Repeat TST Testing – small reactors:
0009.142.3
3.83.48.510.037.2
5.008.88.430.2
0005.427.2
0007.010.3
SSI RT23 PPD5TU
MycosPPD5TU
MycosPPD100TU
TST 5 Reaction size (mm)
Guinea Pig No
Mean (Longitudinal & Transverse) TST 6 Reaction Size (mm)
0006.788.2
0008.981.3
0011.89.977.3
0009.877.1
05.511.17.465.2
SSI RT23 PPD5TU
MycosPPD5TU
MycosPPD100TU
TST 5 Reaction size
(mm)
Guinea Pig No
Mean (Longitudinal & Transverse) TST 6 Reaction Size (mm)
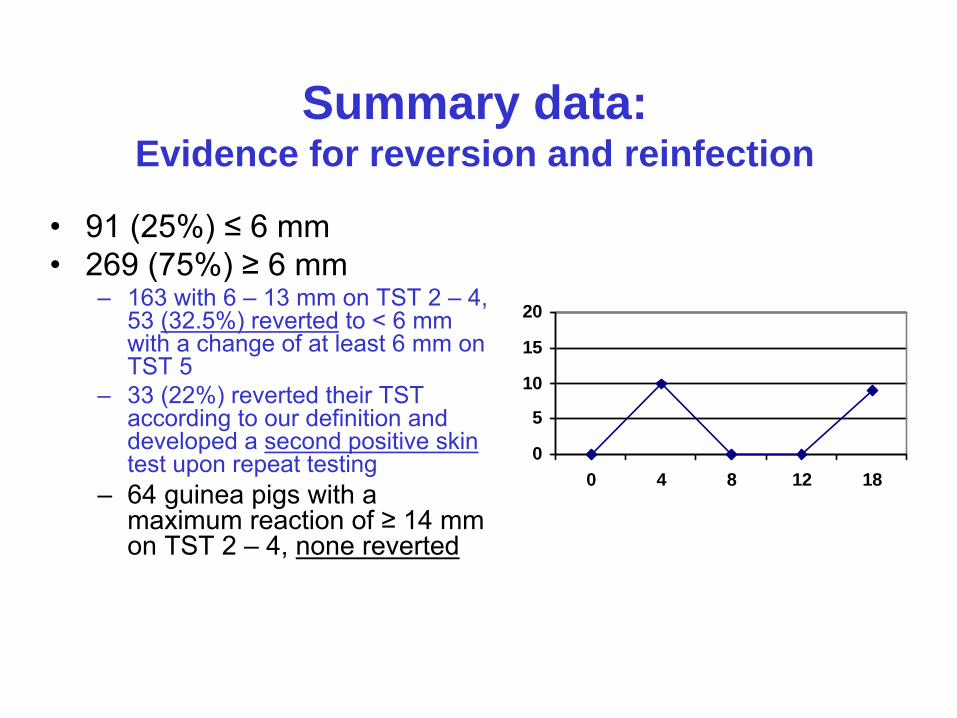
Summary data:Evidence for reversion and reinfection
• 91 (25%) ≤ 6 mm• 269 (75%) ≥ 6 mm
– 163 with 6 – 13 mm on TST 2 – 4, 53 (32.5%) reverted to < 6 mm with a change of at least 6 mm on TST 5
– 33 (22%) reverted their TST according to our definition and developed a second positive skintest upon repeat testing
– 64 guinea pigs with a maximum reaction of ≥ 14 mm on TST 2 – 4, none reverted
0
5
10
15
20
0 4 8 12 18
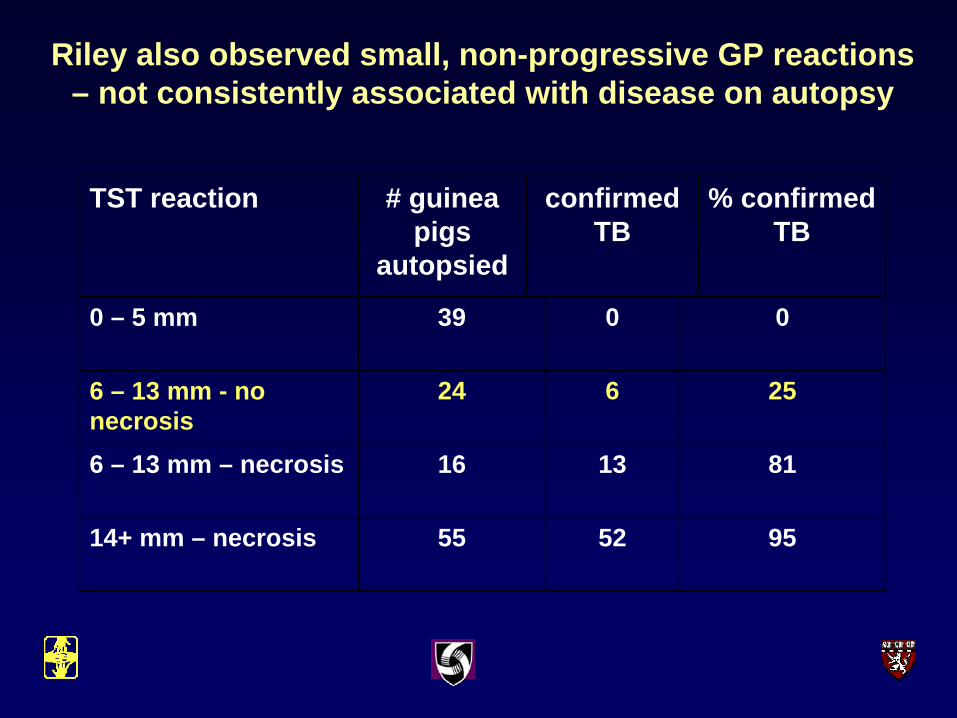
95525514+ mm – necrosis
8113166 – 13 mm – necrosis
256246 – 13 mm - no necrosis
00390 – 5 mm
% confirmed TB
confirmedTB
# guinea pigs
autopsied
TST reaction
Riley also observed small, non-progressive GP reactions – not consistently associated with disease on autopsy
TST & IGRA reversion:Self-limited infections?
• Reversion of TSTs known to occur in humans – after prompt treatment for LTBI– Spontaneously among non-anergic elderly– spontaneously in health workers
• BCG vaccination – another example of acute transient mycobacterial
infection • complete clearance and reversion in most cases
• Serial IGRAs– detecting reversions among Mtb contacts
• with and without treatment.
Future Experiments
• Factors associated with transient infection– Strain, drug resistance, dose, re-infection, host factors
• Mine existing experimental material– with and without immunosupression
• Culture, pathology• Immuno-histochemistry• Fingerprinting • katG mutations -
• Prospective experiments• Validate the pilot study observations
– Minimize reinfection • Lymphocyte stimulation
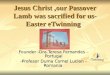
AIR facility capabilities:
1. Test conventional and new air disinfection interventions
• Masks on patients• Topic antibiotics for IC• Portable room air disinfection units (filtration, UV, other)• Upper room UVGI• Chemical air disinfectants
2. Study basic TB aerobiology• Human source factors• Organism factors – the fitness issue• Host responses (pathogenesis) – transient TB infection• Environmental factors
• air pollution – modeling – computational fluid dynamics
2. Mycobacterial strain differences:oCatalase Pos. vs. Neg. INH resistanceoBeijing vs. non-Beijing strainsoSpecific mutations associated with transmission
Parallel measurements: Cough Aerosol SamplingoResistance to environmental stress - close range culture rate vs. guinea pig infection rate
Infection rate of normal
Guinea Pigs
AirborneMDR-Mtb
1. Infectiousness of MDR-TB patients: HIV vs. Non-HIV
oAFB smear, 1-4+oLung cavitationoCough frequencyoHIV status indicators:
oCD4 oviral loadoARV treatment
Parallel measurements: Cough Aerosol SamplingoTotal particlesoTotal stainable Mtb & clumping estimateoCulturable Mtb
Mtb Source:MDR-TB
patients on therapy
3. Host response: oNatural, low-dose MDR-Mtb infection from patients on therapy vs. artificial aerosol infection with cultured isolates from the same patients.
oCompare pathologyoEstimate impact of reinfection
oDetermine fate of GPs with small skin test reactions or reversions

Germicidal UV fixtures (louvered)
AIR Facility, Experimental Plan
A B
Odd days Even days
Intervention on/off on alternative days
Guinea Pig Air Sampling
UVGI OR OTHER INTERVENTION
EXHAUST AIR
Infection rate withIntervention on
Control infection rate -Intervention off
Conclusions – so far:• MDR-TB is very transmissible to highly
susceptible guinea pigs – and probably to immunocompromised patients
• Only a portion of those infected guinea pigs remain infected– Probably primarily strain related– MDR-TB has variably reduced virulence
• Strain W, a member of Beijing family, KZN strain– Host factors also play a role