Embed Size (px)
Citation preview
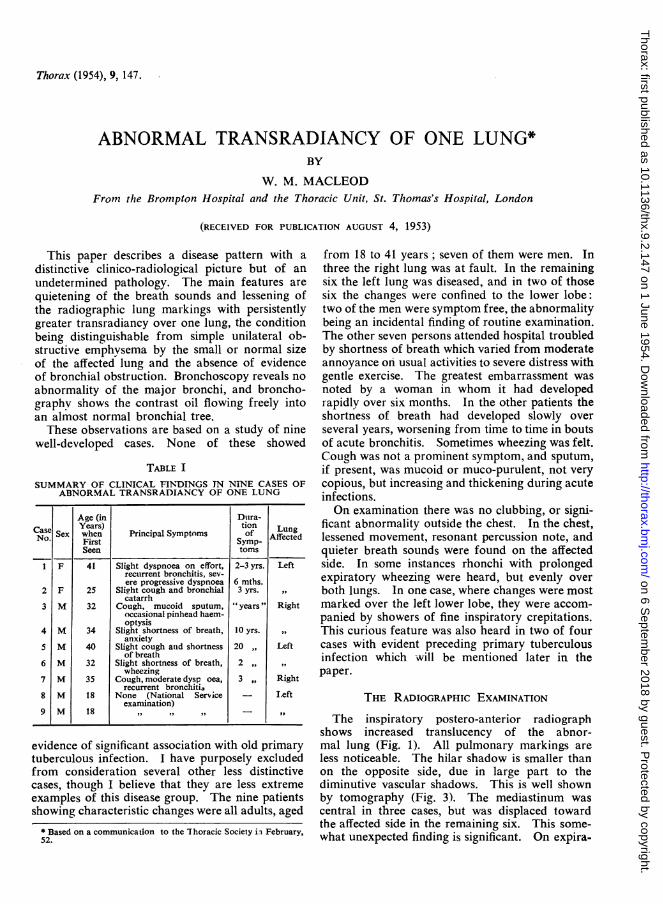
Thorax (1954), 9, 147.
ABNORMAL TRANSRADIANCY OF ONE LUNG*BY
W. M. MACLEODFronm the Brompton Hospital and the Thoracic Unit, St. Thomas's Hospital, London
(RECEIVED FOR PUBLICATION AUGUST 4, 1953)
This paper describes a disease pattern with adistinctive clinico-radiological picture but of anundetermined pathology. The main features arequietening of the breath sounds and lessening ofthe radiographic lung markings with persistentlygreater transradiancy over one lung, the conditionbeing distinguishable from simple unilateral ob-structive emphysema by the small or normal sizeof the affected lung and the absence of evidenceof bronchial obstruction. Bronchoscopy reveals noabnormality of the major bronchi, and broncho-graphy shows the contrast oil flowing freely intoan almost normal bronchial tree.These observations are based on a study of nine
well-developed cases. None of these showed
TABLE ISUMMARY OF CLINICAL FINIDINGS IN NINE CASES OF
ABNORMAL TRANSRADIANCY OF ONE LUNG
Age (in Doira-Case SxYears) tion LnNo. Sex when Principal Symptoms of AffectedFirst Affecte
Seen toms
1 F 41 Slight dyspnoea on effort, 2-3 yrs. Leftrecurrent bronchitis, sev-ere progressive dyspnoea 6 mths.
2 F 25 Slight cough and bronchial 3 yrs.catarrh
3 M 32 Cough, mucoid sputum, " years " Rightoccasional pinhead haem-optysis
4 M 34 Slight shortness of breath, 10 yrs.anxiety
5 M 40 Slight cough atid shortness 20 ,, Leftof breath
6 M 32 Slight shortness of breath, 2wheezing
7 M 35 Cough, moderate dysp oea, 3 ,, Rightrecurrent bronchitis
8 M 18 None (National Service Leftexaniination)
9 M 18 ,,
evidence of significant association with old primarytuberculous infection. I have purposely excludedfrom consideration several other less distinctivecases, though I believe that they are less extremeexamples of this disease group. The nine patientsshowing characteristic changes were all adults, aged
* Based on a communication to the Thoracic Society ii February,52.
from 18 to 41 years; seven of them were men. Inthree the right lung was at fault. In the remainingsix the left lung was diseased, and in two of thosesix the changes were confined to the lower lobe:two of the men were symptom free, the abnormalitybeing an incidental finding of routine examination.The other seven persons attended hospital troubledby shortness of breath which varied from moderateannoyance on usual activities to severe distress withgentle exercise. The greatest embarrassment wasnoted by a woman in whom it had developedrapidly over six months. In the other patients theshortness of breath had developed slowly overseveral years, worsening from time to time in boutsof acute bronchitis. Sometimes wheezing was felt.Cough was not a prominent symptom, and sputum,if present, was mucoid or muco-purulent, not verycopious, but increasing and thickening during acuteinfections.On examination there was no clubbing, or signi-
ficant abnormality outside the chest. In the chest,lessened movement, resonant percussion note, andquieter breath sounds were found on the affectedside. In some instances rhonchi with prolongedexpiratory wheezing were heard, but evenly overboth lungs. In one case, where changes were mostmarked over the left lower lobe, they were accom-panied by showers of fine inspiratory crepitations.This curious feature was also heard in two of fourcases with evident preceding primary tuberculousinfection which will be mentioned later in thepaper.
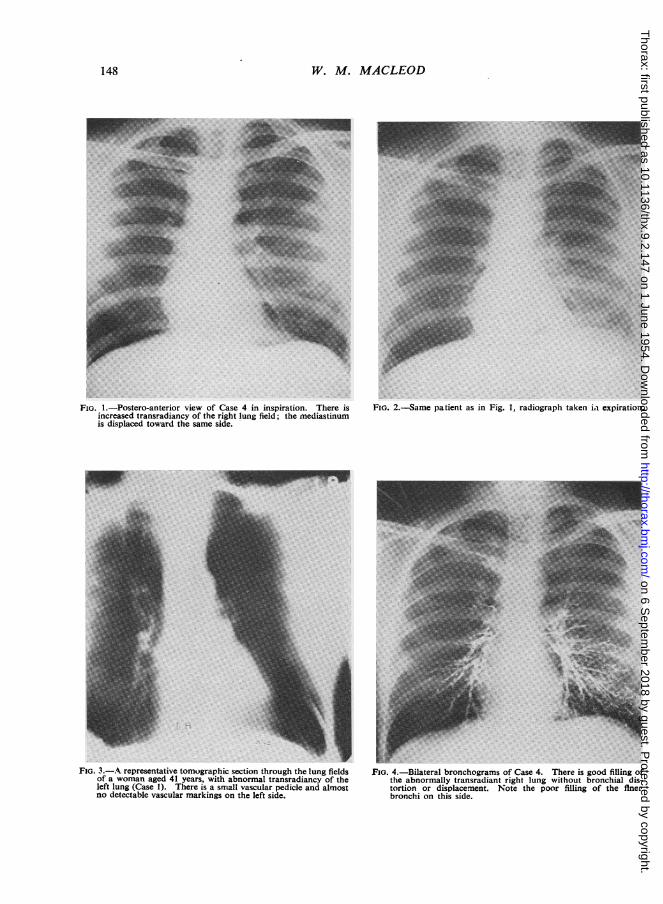
THE RADIOGRAPHIC EXAMINATIONThe inspiratory postero-anterior radiograph
shows increased translucency of the abnor-mal lung (Fig. 1). All pulmonary markings areless noticeable. The hilar shadow is smaller thanon the opposite side, due in large part to thediminutive vascular shadows. This is well shownby tomography (Fig. 3). The mediastinum wascentral in three cases, but was displaced towardthe affected side in the remaining six. This some-what unexpected finding is significant. On expira-
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from
W. M. MACLEOD
FIG. l.-Postero-anterior view of Case 4 in inspiration. There isincreased transradiancy of the right lung field; the mediastinumis displaced toward the same side.
.gSii-
.i__-....-_.w
FIs. 3.-A representative tomographic section through the lung fieldsof a woman aged 41 years, with abnormal transradiancy of theleft lung (Case 1). There is a small vascular pedicle and almostno detectable vascular markings on the left side.
FIG. 2.-Same patient as in Fig. 1, radiograph taken Li expiration.
FIG. 4.-Bilateral bronchograms of Case 4. There is good filling ofthe abnormally transradiant right lung without bronchial dis-tortion or displacement. Note the poor filling of the flnerbronchi on this side.
148
-"7"w
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from
ABNOR VIAL TRANSRADIANCY OF ONE LUNG
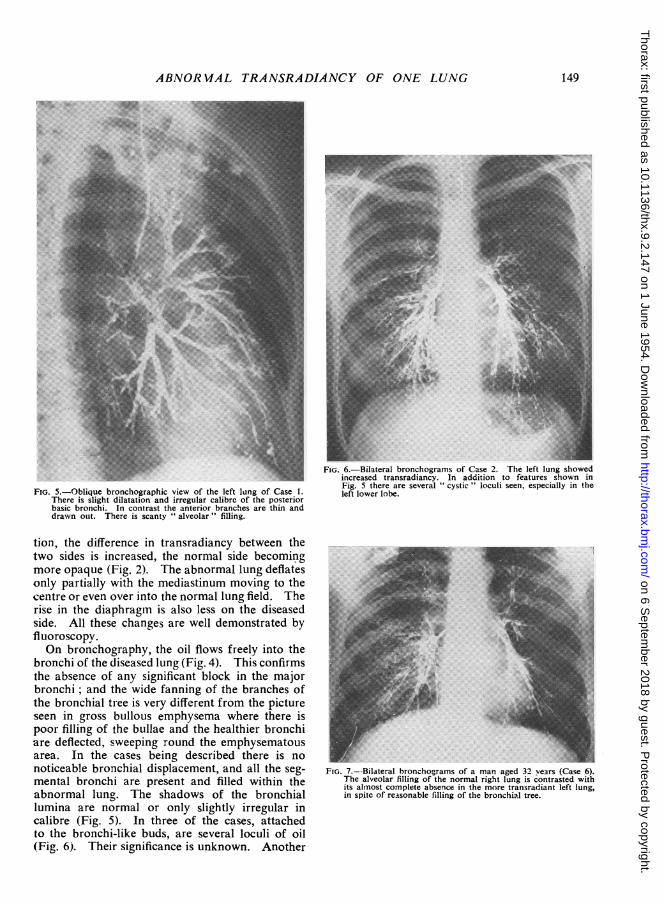
FIG. 5.-Oblique bronchographic view of the left lung of Case 1.There is slight dilatation and irregular calibre of the posteriorbasic bronchi. In contrast the anterior branches are thin anddrawn otut. There is scanty " alveolar " filling.
tion, the difference in transradiancy between thetwo sides is increased, the normal side becomingmore opaque (Fig. 2). The abnormal lung deflatesonly partially with the mediastinum moving to thecentre or even over into the normal lung field. Therise in the diaphragm is also less on the diseasedside. All these changes are well demonstrated byfluoroscopy.On bronchography, the oil flows freely into the
bronchi of the diseased lung (Fig. 4). This confirmsthe absence of any significant block in the majorbronchi; and the wide fanning of the branches ofthe bronchial tree is very different from the pictureseen in gross bullous emphysema where there ispoor filling of the bullae and the healthier bronchiare deflected, sweeping round the emphysematousarea. In the cases being described there is nonoticeable bronchial displacement, and all the seg-mental bronchi are present and filled within theabnormal lung. The shadows of the bronchiallumina are normal or only slightly irregular incalibre (Fig. 5). In three of the cases, attachedto the bronchi-like buds, are several loculi of oil(Fig. 6). Their significance is unknown. Another
FIG. 6.-Bilateral bronchograms of Case 2. The left lung showedincreased transradiancy. In addition to features shown inFig. 5 there are several " cystic " loculi seen, especially in theleft lower lobe.
FIG. 7.--Bilateral bronchogramns of a man aged 32 vears (Case 6).The alveolar filling of the normal right lung is contrasted withits almnost complete absence in the more transradiant left lung,in spite of reasonable filling of the bronchial tree.
149
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from
W. M. MACLEOD
interesting difference between the two lungs is thescanty or absent " alveolar filling " on the abnormalside. The bronchi of both lungs were outlined atone examination, and the poor filling of the finerbronchial radicles in the diseased lung was verynoticeable (Fig. 7).Bronchoscopy was performed in every case, and
was absoltutely normal. Several cases whichshowed narrowing of a major bronchus, thoughonly of slight degree, were excluded from thisseries. In other respects they were similar to thenine cases described, and I believe that the stenosiswas not a significant factor in the persistence of theabnormal changes.When these cases were first seen a presumptive
diagnosis of obstructive distension, secondary to apartial block of a major bronchus, was usuallymade. This was soon disproved by the investiga-tions described. Gross bullous emphysema, therare congenital cystic lung, and complete or partialpneumothorax were excluded by adequate radio-graphy. Distension or emphysema, compensatoryto a collapsed or diseased lobe, were excluded bybronchography. Elementary precautions and carewill avoid confusion with anomalies of the chestwall and differences in penetration due to technicalerrors and faulty positioning.
DISCUSSIONThe present series was studied only by clinical
and radiological methods. No material has beenavailable for morbid anatomical or histologicalexamination. It is unavoidable, therefore, that in-formation regarding the true nature of these casesmust for the present be incomplete. Nevertheless,various processes that might have led to thedevelopment of this distinctive picture may usefullybe reviewed. First let us consider the evidence infavour of a congenital developmental defect.Under the title of " Congenital Lobar Emphysema "
Robertson and Stewart James (1951) describe lungchanges in five young patients, aged from 2 weeksto 11 months. In each patient the disease was con-fined to one lobe, the right upper in three in-stances, and the left upper and the right middle inone each. The lobe was distended, compressingthe remaining healthy lobes of the lung and pushingthe mediastinum over to the other side with embar-rassment of the normal lung. All lobes showeddilated alveoli with thinning and rupture of thealveolar walls, but gross bullous formation was notpresent. In three of the cases no lesion of the mainbronchus was found, but in one case a large veinhooked round the right upper lobe bronchus andaccompanied a narrowing of the bronchial lumen.In the remaining case, valve-like mucosal flaps were
present in the right upper lobe bronchus and wereheld responsible for the obstructive distension ofthe lobe. A similar mucosal flap was reported byRoyes (1938) as an incidental necropsy finding inan adult with an emphysematous right middle lobe.Other cases of unilobar emphysema in infants andchildren have been reported by Leahy and Butsch(1949), Shaw (1952), Williams (1952), and Fischer,Potts, and Holinger (1952). Shaw noted that thebronchi of the affected lobes were abnormallyflaccid and suggested that a localized chondroma-lacia of the bronchus results in expiratory bronchialcollapse with obstructive emphysema distal to theblock. Ferguson and Neuhauser (1944) had pre-viously reported absent cartilaginous rings in theleft main bronchus of two cases with emphysema ofthe whole lung. Fischer and others (1952) con-sidered that the unusually low attachment to theleft pulmonary artery of a persistent ductus arteri-osus was the causative factor in two of their sixcases. Only two of my cases showed changespredominant in one lobe. In both instances theleft lower lobe was involved, and in neither wassuch gross distension as is reported in lobar emphy-sema of infants. It is probable that bronchoscopyand complete bronchography, with inspiratory,expiratory, and delaved contrast pictures, woulddetect the presence of a mucosal flap or significantweakness of the bronchial wall. These anomalieswere not found in this series.
Congenital cystic disease of the lung, especiallywhen it presents with multiple peripheral bronchialdilatations, would, if unilateral, show increasedtransradiancv of one lung. In adults this rareanomaly is difficult to distinguish from acquiredbronchial disease (Sellors, 1938).
I have already commented on the small vascularshadows seen by radiography in these lungs. Thepulmonaiy circulation adjusts itself to the oxygenuptake and in these examples the diminutive vesselsare probably secondary to the poorly functioninglung. There is no evidence to support the sug-gestion that the lung changes follow a congenitalhypoplasia or absence of one pulmonary artery ora developmental abnormality of the bronchialarteries (Madoff, Gaensler, and Strieder, 1952).An interesting case of unilateral emphysema in aboy of 6 is recorded by Swyer and James (1953).In their case radiographic studies, including angio-graphy, suggested a hypoplasia of the right pul-monary artery, but this was in fact not demon-strable in the resected lung. There was, however,a widespread obliteration of the peripheral lungcapillaries and the authors presumed a functionalinsufficiency of the right pulmonary artery second-ary to the lung disease.
150
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from
ABNORMAL TRANSRADIANCY OF ONE LUNG
If we now turn to acquired disease processesthere are several conditions which should be con-sidered. There is an obvious similarity betweenthis group and hypertrophic or vesicular emphy-sema. Laennec (1819, translated by Forbes, 1834)was fully aware that emphysema could developsolely or predominantly in one lung.
"Emphysema may affect both lungs at the sametime, one only, or part of one or both. In thelatter case, and indeed in any case, as long as theredo not exist vesicles of considerable size on thesurface of the lungs, it is easy to overlook thedisease in the dead subject.... Later he re-marks: "When a single lung is affected, it be-comes much more voluminous than the other-somuch so, indeed, as sometimes to pass aside theheart and mediastinum, and to cause an evidentenlargement of the bony walls of that side of thechest."
We may assume that Laennec found no majorbronchial stenosis, but whether the open bronchicommunicated freely with the emphysematous lungmust remain unknown. Three of the nine casesin my series might well have been instances ofunilateral vesicular emphysema, though the lungsare not so voluminous nor the changes so extremeas noted by Laennec at necropsy. For example,a woman of 41 years was admitted to St. Thomas'sHospital under the care of Dr. John Anderson.She gave a remarkably short history of only fourmonths' progressive shortness of breath. She thensuffered from an attack of acute bronchitis. Thisled to severe distress and she became bed-fast.She was admitted six months after the onset of hersymptoms. She showed the characteristic featuresdescribed above with evidence of bilateral bron-chitis. On inspiration the mediastinum was central,but swinging away from the transradiant lung onexpiration. Bronchography (Fig. 5) and broncho-scopy were characteristic of the group. Thepleural pressures at the start of an induced pneumo-thorax were - 12 cm. water on inspiration and+4 cm. water on expiration, being a clear indica-tion of the diminished elastic recoil of the lung.These features suggest that the disease in this
instance is similar in nature to that seen in general-ized emphysema, but that for obscure reasons ithas developed predominantly in one lung.Whether such one-sided changes, together with thebilateral bronchitis, are a prelude to generalizedlung disease with an equalizing increase in trans-radiancy of the more normal lung must be left tofurther observation.
Bilateral bronchial catarrh was found in five ofthe nine cases. Where a prolonged expiratorysound was present it appeared equally in the twolungs, though it was quieter and more difficult to
hear on the diseased side. However, the qualityof the breath sounds is a very rough guide to thedegree of bronchial obstruction. The poor " alve-olar filling" seen on the more transradiant side atbronchography is suggestive of a significant differ-ence in calibre of the terminal bronchi and bronchi-oles. It is well recognized that gross unilateralbronchial disease is commonly associated withemphysema. Such lungs, apart from the obviousdifferences in bronchial dilatation, may presentclinically and radiologically in a similar mannerto those under review.An account of advanced unilateral emphysema
in a man of 34 years is to be found in the caserecords of the Massachusetts General Hospital(1950). The patient was known to have had onlyone lung for over 19 years. He had a greatlydistended left lung with displacement of the medias-tinum to the right. The lung was examined aftersuccessful pneumonectomy and showed severeemphysema throughout. There were no giantbullae, the pulmonary artery and veins wererelatively small, while the bronchial arteries wereabout four times normal diameter. Scatteredthrough the lung were groups of epithelioid cells,and giant cells with tubercle formation. Thesechanges were interpreted as sarcoidosis. The hilarnodes were also affected. Many of the foci werecollagenous and in a healing phase. The relationbetween the two diseases is open to conjecture, butit is not impossible that the emphysema resultedfrom the extensive scarring of healed sarcoidosis.Little is known of the state of the lung years afterresolution of sarcoid infiltration. In this case theevidence is far from complete, and in a diseasewhich so frequently affects both sides knowledgeof the remaining lung would be necessary beforeany more definite conclusions could be drawn.
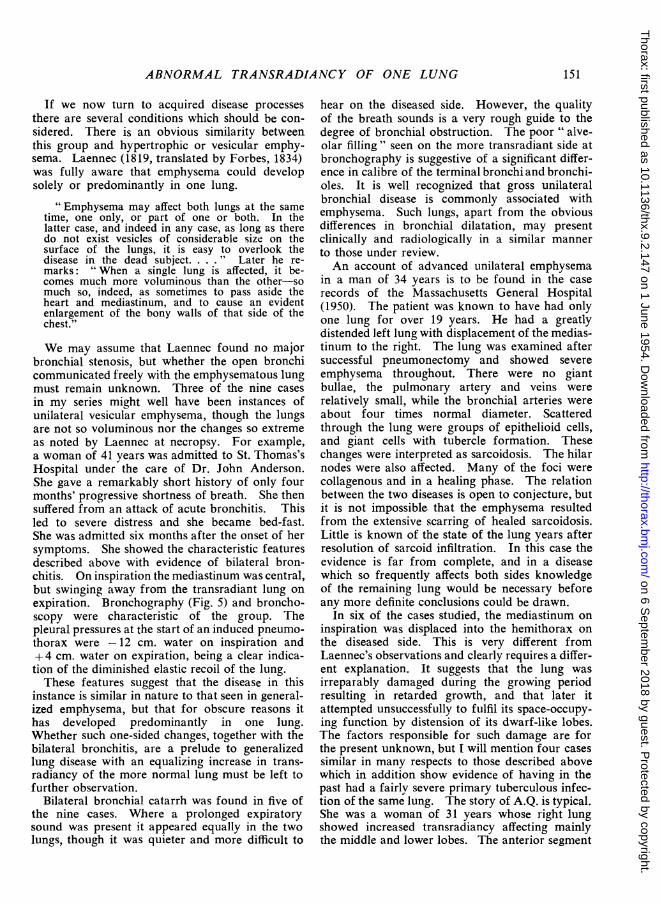
In six of the cases studied, the mediastinum oninspiration was displaced into the hemithorax onthe diseased side. This is very different fromLaennec's observations and clearly requires a differ-ent explanation. It suggests that the lung wasirreparably damaged during the growing periodresulting in retarded growth, and that later itattempted unsuccessfully to fulfil its space-occupy-ing function by distension of its dwarf-like lobes.The factors responsible for such damage are forthe present unknown, but I will mention four casessimilar in many respects to those described abovewhich in addition show evidence of having in thepast had a fairlv severe primary tuberculous infec-tion of the same lung. The story of A.Q. is typical.She was a woman of 31 years whose right lungshowed increased transradiancy affecting mainlythe middle and lower lobes. The anterior segment
151
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from
W. M. MACLEOD
A~~~~~~~
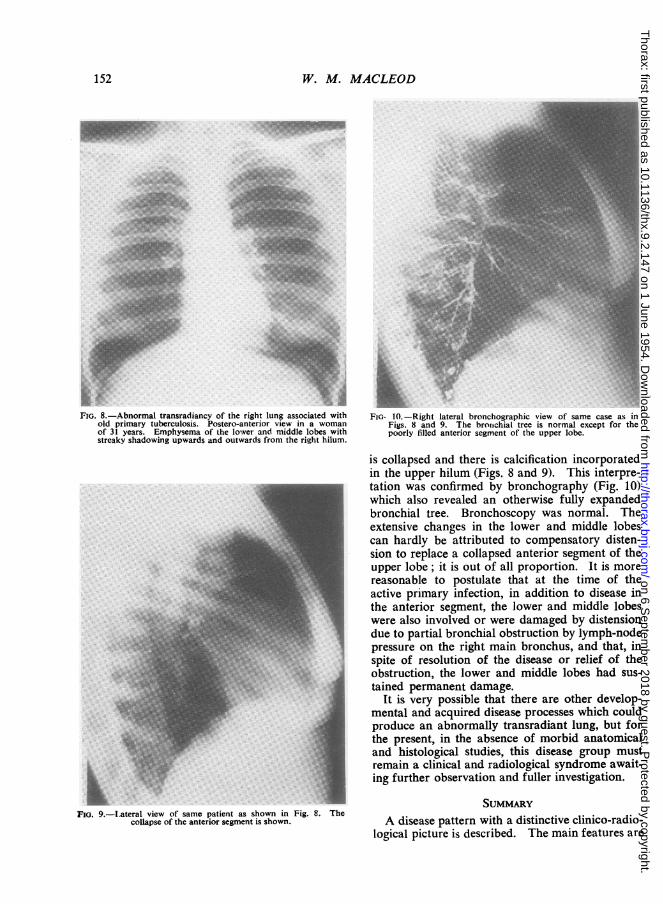
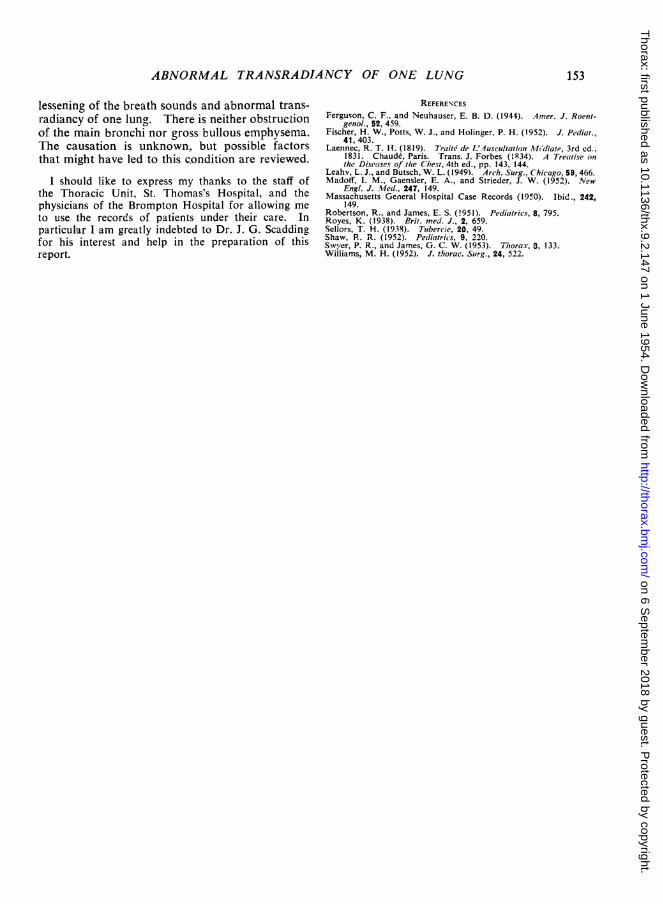
FIG. 8.-Abnormal transradiancy of the right lung associated with FIG. 10.-Right lateral bronchographic view of tame case as inold primary tuberculosis. Postero-anterior view in a woman Figs. 8 ansd 9. The bronichial tree is normal except for theof 31 years. Emphysema of the lower and middle lobes with poorly tilled anterior segment of the upper lobe.streaky shadowing upwards and outwards from the right hilum.
is collapsed and there is calcification incorporatedin the upper hilum (Figs 8 and 9). This interpretation was confirmed by bronchography (Fig. 10)which also revealed an otherwise fully expandedbronchial tree. Bronchoscopy was normal. Theextensive changes in the lower and middle lobescan hardly be attributed to compensatory disten-sion to replace a collapsed anterior segment of theupper lobe; it is out of all proportion. It is morereasonable to postulate that at the time of theactive primary infection, in addition to disease inthe anterior segment, the lower and middle lobes
A
Fi.'s ~~~~~~~were also involved or were damaged by distensiondue to partial bronchial obstruction by lymph-nodepressure on the right main bronchus, and that, inspite of resolution of the disease or relief of theobstruction, the lower and middle lobes had sus-tained permanent damage.
It is very possible that there are other develop-mental and acquired disease processes which couldproduce an abnormally transradiant lung, but forthe present, in the absence of morbid anatomicaland histological studies, this disease group mustremain a clinical and radiological syndrome await-ig further observation and fuller investigation.
FIG. 9.-Lateral view of same patient as shown in Fig 8. Thecoalapse of the anterior segment is shown A disease pattern with a distinctive clinico-radio-logical picture is described. The main features are
152
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from
ABNORMAL TRANSRADIANCY OF ONE LUNG
lessening of the breath sounds and abnormal trans-radiancy of one lung. There is neither obstructionof the main bronchi nor gross bullous emphysema.The causation is unknown, but possible factorsthat might have led to this condition are reviewed.
I should like to express my thanks to the staff ofthe Thoracic Unit, St. Thomas's Hospital, and thephysicians of the Brompton Hospital for allowing me
to use the records of patients under their care. Inparticular I am greatly indebted to Dr. J. G. Scaddingfor his interest and help in the preparation of thisreport.
REFERENCESFerguson, C. F., and Neuhauser, E. B. D. (1944). 4mer. J. Roent-
genol., 52, 459.Fischer, H. W., Potts, W. J., and Holinger, P. H. (1952). J. Pediat.,
41, 403.Laennec, R. T. 1H. (1819). 7raitd de JA'uscultation Atl-'diate, 3rd ed.,
1831. Chaude, Paris. rrans. J. Forbes (1834). A Treatise on
the Diseases of the Cihest, 4th ed., pp. 143, 144.Leahy, L. J., and Butsch, W. L. (1949). Arch. Surg., Chicago, 59, 466.Madoff, I. M., Gaensler, F. A., and Strieder, J. W. (1952). New
Engl. J. Med., 247, 149.Massachusetts General Hospital Case Records (1950). Ibid., 242,
149.Robertson, R., and James, E. S. (1951). Peliatrics, 8, 795.Royes, K. (1938). Prit. med. J., 2, 659.Sellors, T. H. (1938). Tubercie, 20, 49.Shaw, R. R. (1952). Pediatrics, 9, 220.Swyer, P. R., and James, G. C. W. (1953). T7horax, 3, 133.Williams, M. H. (1952). J. thorac. Surg., 24, 522.
153
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.9.2.147 on 1 June 1954. Dow
nloaded from