Embed Size (px)
Citation preview
TRANSVERSUS ABDOMINIS PLANE BLOCKPrepared By: Mohd Fadzli Zahari
Supervised By: Dr Muhammad Rozi Bin Mamat
Review Article
Clinical Implications of the Transversus AbdominisPlane Block in Adults
Mark J. Young,1 AndrewW. Gorlin,2 Vicki E. Modest,1, 3and Sadeq A. Quraishi1, 3
Hindawi Publishing CorporationAnesthesiology Research and PracticeVolume 2012, Article ID 731645, 11 pages
OUTLINE
Introduction History Anatomy Contraindication Technique Local anesthetic dosing Complications Conclusion
INTRODUCTION
Technique that provides analgesia to the parietal peritoneum as well as the skin and muscles of the anterior abdominal wall.
Relatively low risk of complications and a high success rate using modern techniques but remain overwhelmingly underutilized.
HISTORY
A.N. Rafi first described the TAP block in 2001. “Abdominal field block: a new approach via the lumbar triangle,” Anaesthesia,
vol. 56, no. 10, pp. 1024–1026, 2001.
He portrayed it as a refined abdominal field block, with a targeted single shot anesthetic delivery into the TAP.
Significant advance from earlier strategies that required multiple injections.
Lumbar triangle of Petit: enclosed medially by the external oblique, posteriorly by the latissimus dorsi, and inferiorly by the iliac crest.
Single confirmatory “pop” was appreciated.
HISTORY
In 2004, McDonnell et al. presented preliminary work on TAP blocks in cadavers and in healthy volunteers at the scientific meeting of the American Society of Anesthesiologists.
evidence to support the anatomical basis for TAP blocks and demonstrated sensory loss spanning the xiphoid to the pubic symphysis following delivery of local anesthetic to the TAP via the triangle of Petit.
McDonnell and his colleagues had already adopted the term TAP block and had demonstrated its analgesic utility in patients undergoing open retropubic prostatectomy.
ANATOMY
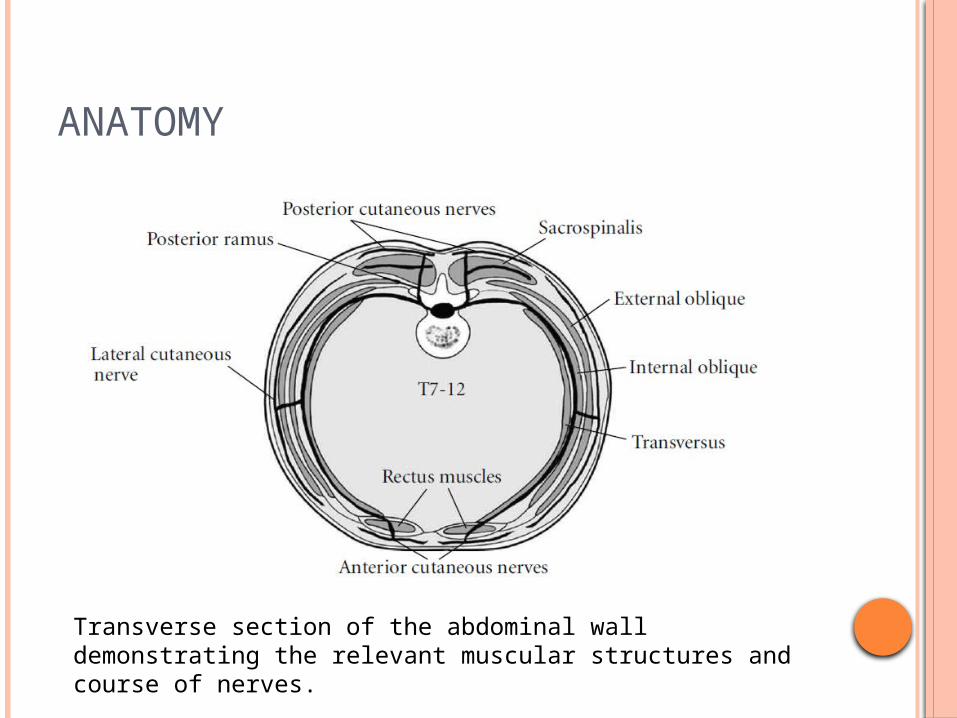
Transverse section of the abdominal wall demonstrating the relevant muscular structures and course of nerves.
ANATOMY
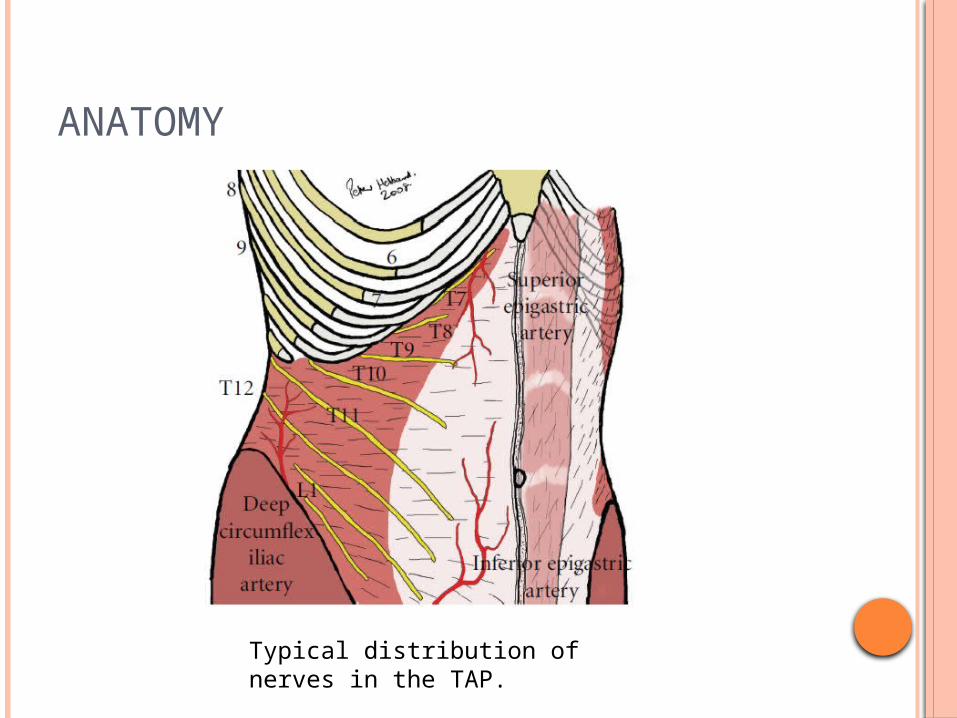
Typical distribution of nerves in the TAP.
ANATOMY
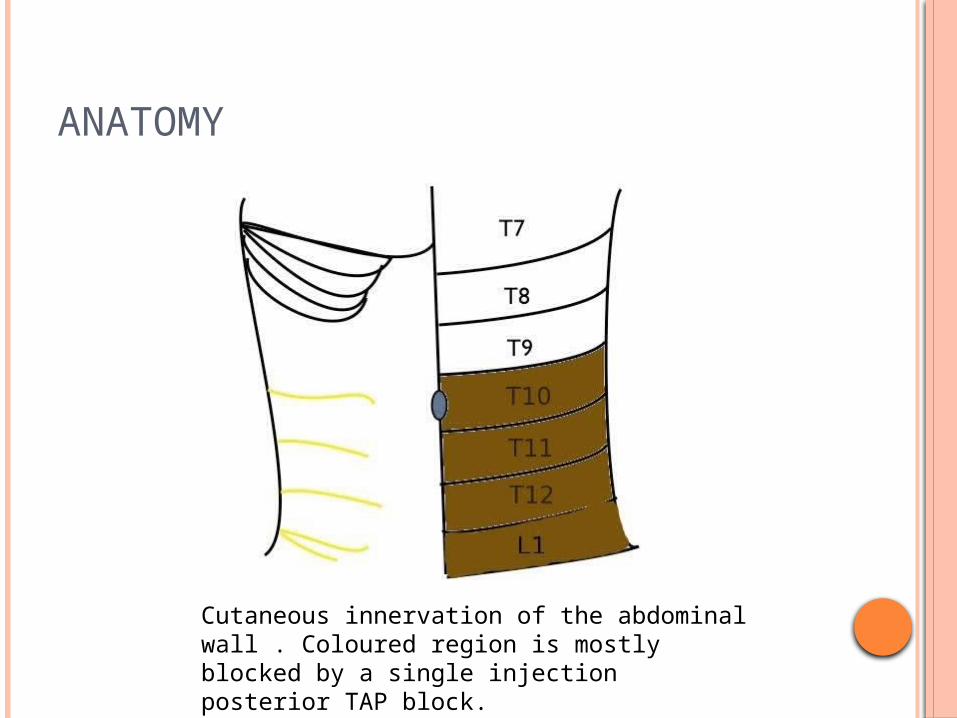
Cutaneous innervation of the abdominal wall . Coloured region is mostly blocked by a single injection posterior TAP block.
ANATOMY 3 Muscle layers. Transversus Abdominus Plane (TAP) located between
Internal Oblique and Transversus Abdominis Muscle. TAP boundaries:
Medial-Lateral border of Rectus Abdominis muscle. Superior- Costal margin Inferior- Iliac crest
Sensory innervation: Ventral Rami from T6-L1. The seventh to eleventh intercostals nerves, subcostal nerve, iliohypogastric and ilioinguinal nerves, all run a variable part of their courses between internal oblique and transversus abdominis muscles.
INDICATION
Lower abdominal surgery: Appendectomy Hernia repair Caesarean section
Abdominal hysterectomy Prostatectomy
CONTRAINDICATION
Patient refusal. Soft tissue infection. Abnormality at needle insertion area.
TECHNIQUE 1:ANATOMICAL LANDMARK-BASED APPROACHES
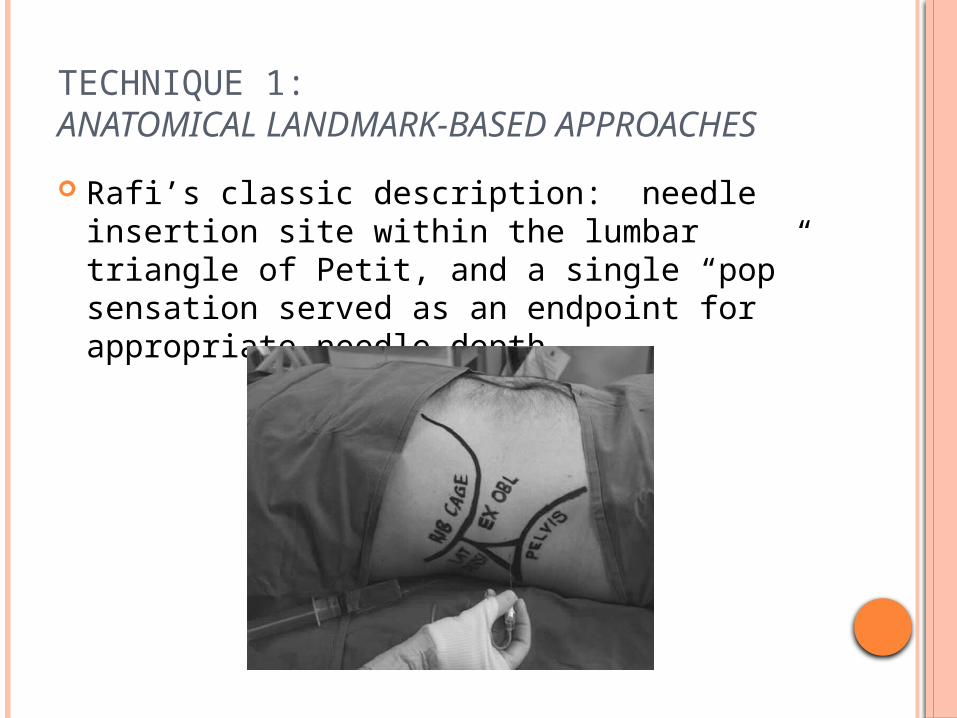
Rafi’s classic description: needle insertion site within the lumbar triangle of Petit, and a single “pop” sensation served as an endpoint for appropriate needle depth.
Methods: Pt place in supine position finger was walked from the anterior superior iliac
spine along the top of the iliac crest until it dipped slightly inward.
On further posterior movement, the finger tip was felt to slip over the lateral border of the latissimus dorsi ( attachement to the external lip of the iliac crest ).
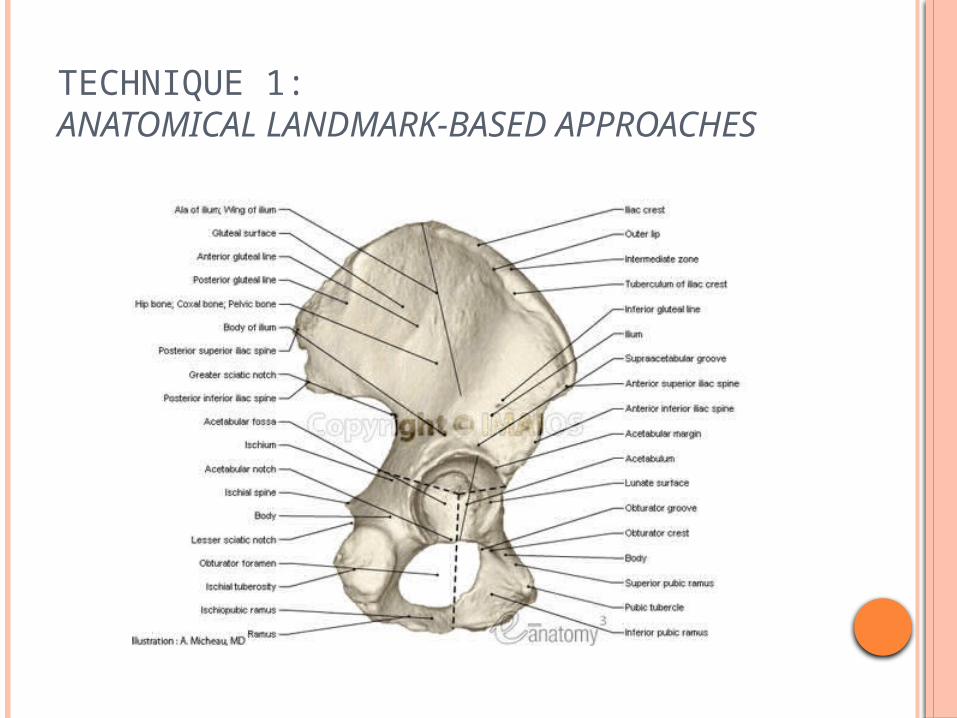
Skin nick with 18G cutting edge needle then followed by insertion 24G blunt tipped needle perpendicular to the skin until it touched the bone of the external lip.
The needle was then slowly advanced over the intermediate zone of the iliac crest until the definite “pop” was felt.
TECHNIQUE 1:ANATOMICAL LANDMARK-BASED APPROACHES
TECHNIQUE 1:ANATOMICAL LANDMARK-BASED APPROACHES
Single “pop” method differs from the “double pop” method described by O’Donnell et al. in which the needle was inserted cephalad to the iliac crest and advanced until two distinct “pops” were appreciated.
All anatomical landmark-based approaches to the TAP make use of blunt-tipped needles to improve tactile sensitivity and appreciation for distinct “pop” sensations.
TECHNIQUE 1:ANATOMICAL LANDMARK-BASED APPROACHES
First described in 2007 by Hebbard et al. Real-time ultrasonography facilitates easy
needle visualization as it approaches and reaches the target fascial plane.
“pop” sensations in the classic approach could be imprecise due to anatomic variability.
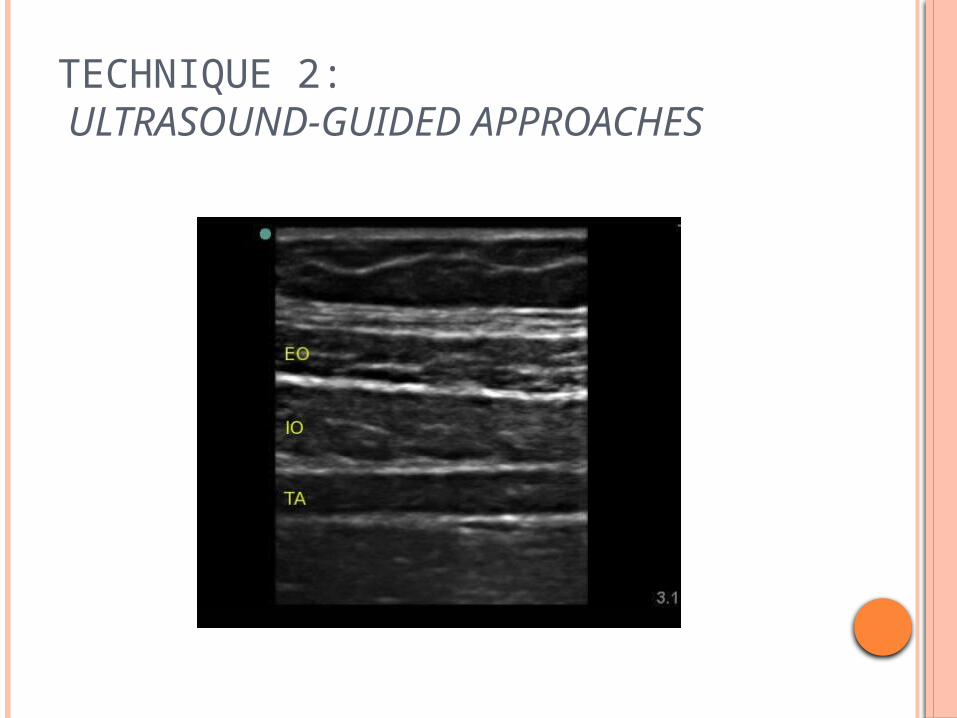
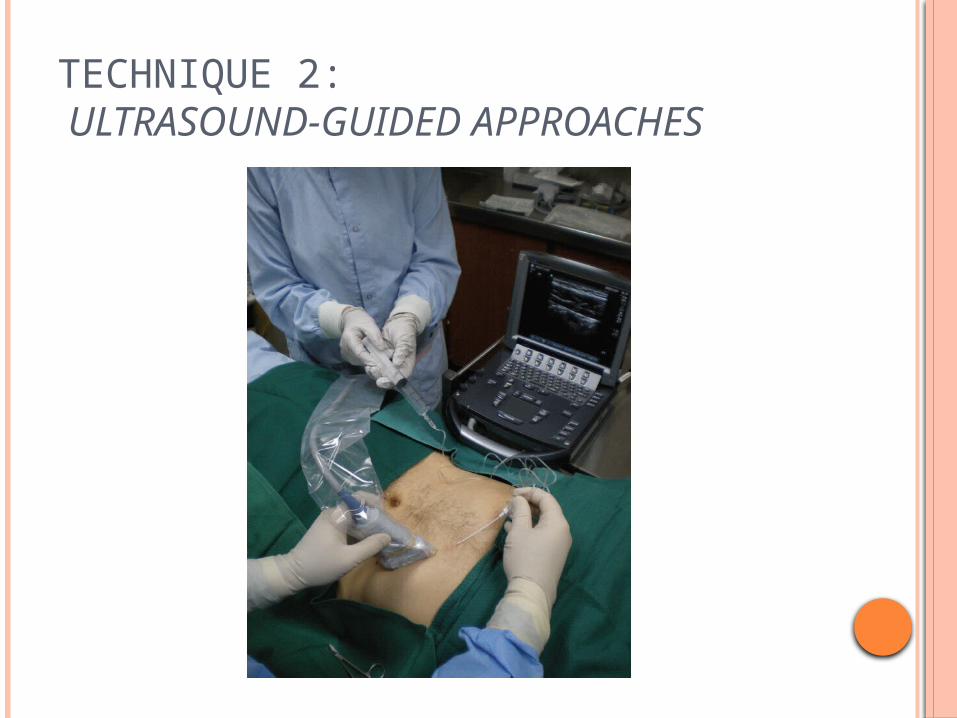
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
Posterior approach Method: Transversely orientated ultrasound probe to the
anterolateral abdominal wall where the three muscle layers are most distinct.
After identification of the TAP between the internal oblique and transversus abdominis muscles, the probe was moved posterolaterally to lie across the midaxillary line just superior to the iliac.
The block needle was then introduced anteriorly and advanced in an in-plane approach.
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
oblique subcostal approach method: needle entered the skin in an area near the
xyphoid. advanced inferolaterally such that local
anaesthetic is delivered to the TAP along the costal margin.
P. Hebbard, “Subcostal transversus abdominis plane block under ultrasound guidance,” Anesthesia and Analgesia, vol. 106, no. 2, pp. 674–675, 2008.
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
TECHNIQUE 2: ULTRASOUND-GUIDED APPROACHES
TECHNIQUE 3:SURGEON-ASSISTED APPROACHES
Anatomical approach assisted with intra-abdominal laparoscopic camera. A peritoneal bulge at the area of injection was seen after local anesthetic was delivered within the TAP.
Surgical TAP block utilizing a transperitoneal approach.
LOCAL ANESTHETIC DOSING
Rafi described the use of 20mL of “a local anaesthetic agent” for each side requiring analgesia.
McDonnell et al. reported the use of 20mL of 0.5% lidocaine for each side in healthy volunteers
TAP catheters was first described in 2009 in a small case series.
G. Niraj, A. Kelkar, and A. J. Fox, “Oblique sub-costal transversus abdominis plane (TAP) catheters: an alternative to epidural analgesia after upper abdominal surgery,” Anaesthesia, vol. 64, no. 10, pp. 1137–1140, 2009.
Two years later, the same group showed similar pain control between epidural and TAP catheter analgesia in a randomized study.
G. Niraj, A. Kelkar, I. Jeyapalan et al., “Comparison of analgesic efficacy of subcostal transversus bdominis plane blocks with epidural analgesia following upper abdominal surgery,” Anaesthesia, vol. 66, no. 6, pp. 465–471, 2011.
LOCAL ANESTHETIC DOSING
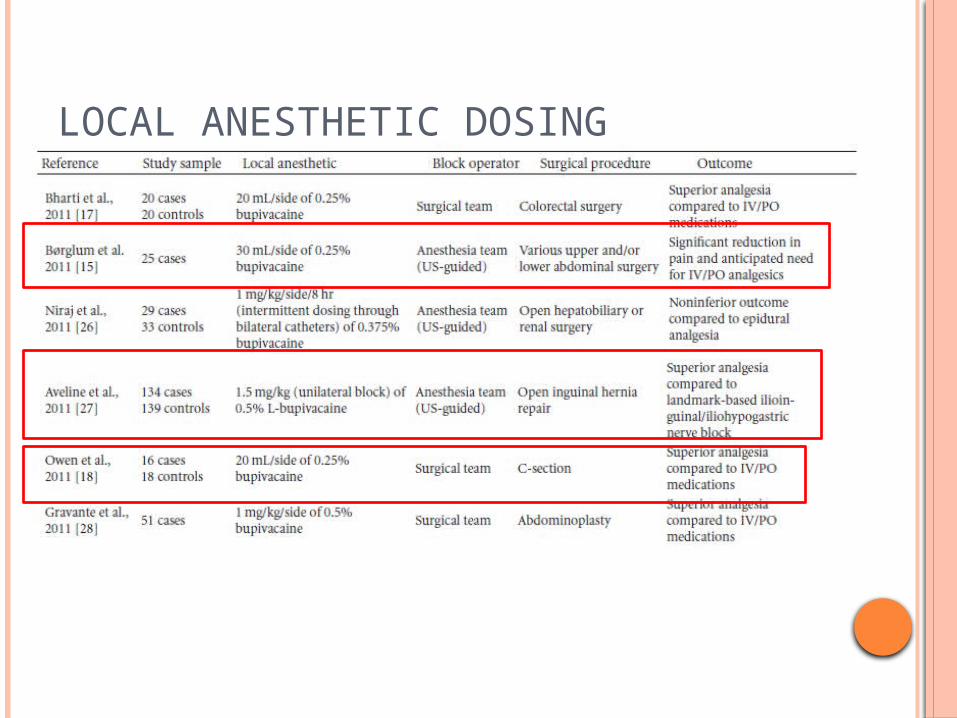
LOCAL ANESTHETIC DOSING
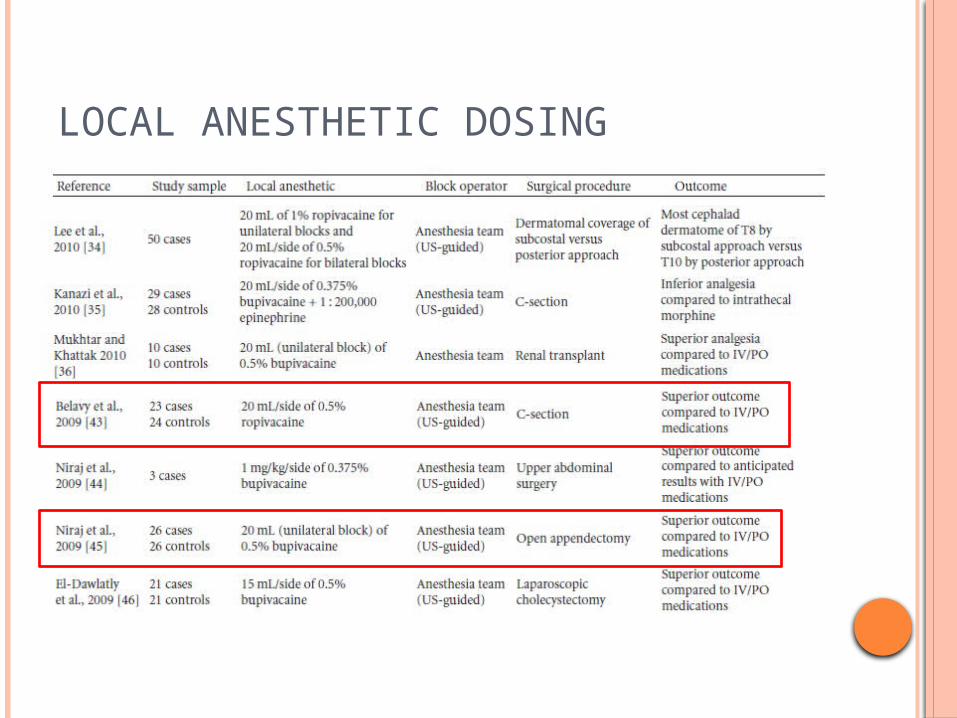
LOCAL ANESTHETIC DOSING
COMPLICATIONS
Systemic toxicity. Liver lacerations caused by right-sided TAP
blocks. Spleen and kidneys laceration. Intraperitoneal injection Bowel hematoma Femoral nerve blocks.

CONCLUSION
TAP block is an effective and safe adjunct to multimodal postoperative analgesia for abdominal surgery.
Good alternative strategy for patients who are highly sensitive to opioids.
Coagulation status is an area of uncertainty with the TAP block and will require further investigation.
Optimal dosing schemes also need to be determined.
CONCLUSION
TAP block is an effective and safe adjunct to multimodal postoperative analgesia for abdominal surgery.
TAP blocks/catheters may provide comparable analgesia as well as patient satisfaction to epidural therapy.
Believes that the posterior approach is ideal for incisions below the umbilicus & subcostal block is best suited for upper abdominal procedures.
Thus combined approach provides the greatest analgesic coverage.
ADDITIONAL REFERRENCE TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK Karim
Mukhtar, The Journal of NYSORA 2009; 12: 28-33
Clinical effectiveness of transversus abdominis plane (TAP) block in abdominal surgery: a systematic review and meta-analysis N. Johns*†, S. O’Neill*†, N. T. Ventham*, F. Barron‡, R. R. Brady* and T. Daniel*
A. N. Rafi, “Abdominal field block: a new approach via the lumbar triangle,” Anaesthesia, vol. 56, no. 10, pp. 1024–1026, 2001.










![li Journal of Anesthesia Clinical Research - Longdom...oblique muscle and the transversus abdominis muscle [7,8]. In recent times, the transversus abdominis plane (TAP) block has been](https://img.pdfslide.net/doc/110x75/5f2868ff73bd59032d6d19c5/li-journal-of-anesthesia-clinical-research-longdom-oblique-muscle-and-the.jpg)


















