Embed Size (px)
Citation preview

Contra Costa Health Services Emergency Medical Services Agency
Trauma System Plan Status Report
September 2011
SUMMARY OF TRAUMA PLAN STATUS REPORT
Contra Costa County’s initial Trauma System Plan was developed in 1985, approved by the
Board of Supervisors on November 19, 1985, and approved by the State Emergency Medical Services Authority (EMSA) on December 20, 1985 based upon the draft trauma regulations available at that time. The format and information contained in the plan were updated in October 1987 and again in December 2001 to comply with State trauma regulations. These plans were re-approved by EMSA on November 28, 1988, March 7, 2003, and January 2010 respectively. In August of 2010 the Trauma System Plan Status Report was submitted to EMS addressing comments and questions included in EMSA correspondence dated January 20, 2010. In September 2010 EMSA accepted the Contra Costa Trauma System Status Report with commendation.
Key elements of the current Trauma System Program include the following:
▸ Designation of a single Level II trauma center to serve all of Contra Costa County. ▸ Trauma center designation made on the basis of an open competitive process including
use of an outside team of experts to evaluate trauma center applications. ▸ Maintenance of the American College of Surgeons Committee on Trauma Level II Trauma
Center Verification.1 ▸ Recognition of the Level I pediatric trauma center designated by Alameda County as the
appropriate facility to serve the needs of pediatric trauma patients. ▸ Full integration of the trauma system into the existing EMS system. ▸ Field triage of all major trauma patients to a designated trauma center when possible. ▸ Use of air ambulance (helicopter) services to reduce trauma transport times when
appropriate. ▸ Maintenance of a trauma registry to track trauma system and trauma center performance
on a case-by-case basis. ▸ A bi-county trauma audit (quality assurance and improvement) process to assure outside
expert review of the trauma center and the trauma system on an ongoing basis. ▸ Full participation in regional and state trauma system activities. ▸ Full participation in CEMSIS Trauma and EMS data sharing. ▸ Development of a county-wide pediatric and neonatal disaster plan to support traumatic
injury as the result of catastrophic earthquake or multicasualty events involving traumatic injury.
▸ Active injury prevention activities supporting preventable injuries in children in collaboration with John Muir Trauma Center and Children’s Hospital and Medical Center Oakland.
▸ Re-evaluation of the current Trauma System Plan to support efficient system oversight. ▸ Re-evaluation of current intra-facility transfer processes to support enhanced trauma
patient destination workflow.
1 See letter of certification at end of report

ORGANIZATIONAL STRUCTURE The Contra Costa County trauma system is an integral part of the EMS system
shown in Figure II-1. The Contra Costa Health Services Department is the Local EMS Agency (LEMSA) as designated by the Board of Supervisors. The LEMSA staff include the EMS Director, EMS Medical Director, the Assistant EMS Director, the Health Services Emergency Preparedness Manager, two nursing positions, three prehospital care coordinators (nurse or paramedic), and two support staff.
Figure II-1. Contra Costa County EMS system
John Muir Medical Center was designated in May 1986, following a request for proposal process as the County’s sole Level II Trauma Center. John Muir’s designation was renewed in May 1992, following a second request for proposal process providing an additional opportunity for hospitals to seek trauma center designation. The term of the existing contract is through May 2, 2021 with conditional automatic renewal to 2031.
While John Muir is the sole County-designated trauma center, the County recognizes Children’s Hospital and Research Center Oakland as an Alameda County designated Level I Trauma Center with specialized capability to care for pediatric trauma and has established mechanisms to assure that most pediatric trauma is transported directly to Children’s Hospital.
The EMS Agency is responsible for overall trauma system monitoring and quality improvement, and for administration of the trauma center designation contract. The
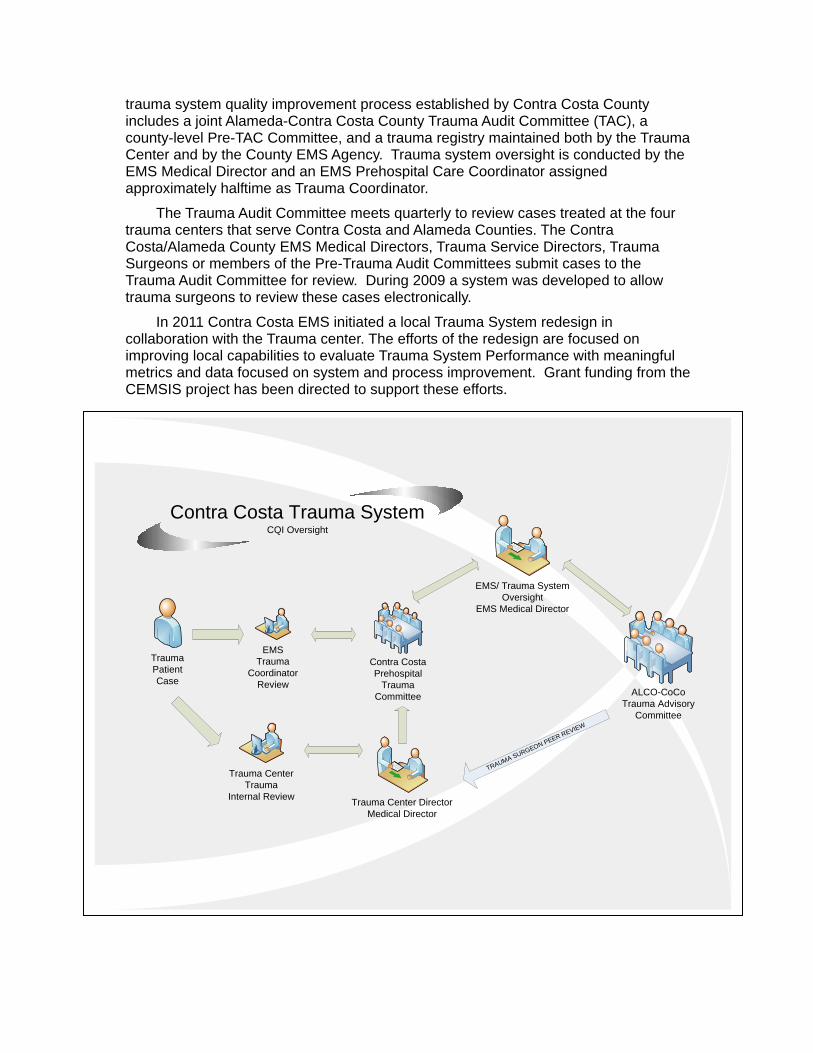
trauma system quality improvement process established by Contra Costa County includes a joint Alameda-Contra Costa County Trauma Audit Committee (TAC), a county-level Pre-TAC Committee, and a trauma registry maintained both by the Trauma Center and by the County EMS Agency. Trauma system oversight is conducted by the EMS Medical Director and an EMS Prehospital Care Coordinator assigned approximately halftime as Trauma Coordinator.
The Trauma Audit Committee meets quarterly to review cases treated at the four trauma centers that serve Contra Costa and Alameda Counties. The Contra Costa/Alameda County EMS Medical Directors, Trauma Service Directors, Trauma Surgeons or members of the Pre-Trauma Audit Committees submit cases to the Trauma Audit Committee for review. During 2009 a system was developed to allow trauma surgeons to review these cases electronically.
In 2011 Contra Costa EMS initiated a local Trauma System redesign in collaboration with the Trauma center. The efforts of the redesign are focused on improving local capabilities to evaluate Trauma System Performance with meaningful metrics and data focused on system and process improvement. Grant funding from the CEMSIS project has been directed to support these efforts.
Trauma PatientCase
Contra Costa Prehospital
TraumaCommittee ALCO-CoCo
Trauma Advisory Committee
EMS Trauma
Coordinator Review
EMS/ Trauma SystemOversight
EMS Medical Director
Trauma CenterTrauma
Internal Review Trauma Center Director
Medical Director
Contra Costa Trauma SystemCQI Oversight
TRAUMA SURGEON PEER REVIEW
Trauma System
In 1986, the Board of Supervisors approved a comprehensive Trauma System Plan for the County and designated John Muir Medical Center (Walnut Creek) as the County's Level II Trauma Center, and in June of that year, ambulance personnel began transporting critical trauma patients directly to John Muir, Walnut Creek. Ambulance and base hospital personnel use triage protocols, which include evaluation of mechanisms of injury and anatomic factors as well as a physiologic trauma scoring system to identify critical trauma patients. In 2001, a revised trauma system plan was developed to meet new State trauma system planning requirements.
In 2010, 2,630 patients were identified as requiring trauma triage, 1,463 of which were transported directly to John Muir Trauma Center. One hundred eight patients were transported to Children’s Hospital Oakland, and 29 to out-of-county adult trauma centers, primarily Eden Hospital, Castro Valley and Highland Hospital, Oakland, U.C. Davis, and Santa Clara Valley Medical Center. Patients in traumatic full arrest or whose airway cannot be managed are triaged to the closest basic emergency department for resuscitation. During the past 24.5 years of operation, more than 66,000 patients have been triaged through the County trauma system.
In 2010, the definition of “Major Trauma Victim” (MTV) was modified in the system to include only patients with an Injury Severity Score (ISS) of greater than 15. Injury Severity Score is a standardized retrospective assessment of the level of severity of injury. Previously, patients with ISS score of 10-14 with length of stay of three days or more were also considered MTVs. This new definition is the one utilized by most trauma systems across the nation.
Critically injured patients who arrive at non-trauma center hospitals may be transferred to trauma centers. One hundred and nine of 294 injured patients transferred to John Muir, Walnut Creek from within Contra Costa were retrospective MTVs per the new definition.
John Muir Trauma Center also received 365 trauma patients from surrounding counties, generally by air transport. One hundred fifteen of the injured out-of-County patients were retrospective MTVs. In particular, John Muir Trauma Center receives a significant number of trauma victims from neighboring Solano County as triaged pursuant to Solano County EMS policy. In 2010, Solano County patients comprised 18.4% of trauma patients transported to John Muir Trauma Center.
Patients with more serious injuries increasingly have been noted to be in older age groups (65 and over). Triage of elderly patients is more difficult and remains a problem throughout the nation because their presentation is frequently much more subtle, with more minor mechanisms of injury (primarily falls). Many have overlying medical issues that cloud the ability to determine if their symptoms and findings are truly related to trauma.
In 2010, a study of head injury triage was undertaken. Results of the study are pending.
If trauma center resources are temporarily overwhelmed, the trauma center may consider "Trauma Center Bypass,” directing any critical trauma patients to out-of-County trauma centers until resources are again available. In 2010 John Muir Trauma Center bypass rate was 0.6%.
Trauma System Evaluation
A major aspect of the trauma system is an extensive trauma system and trauma center monitoring program. Part of this program is a unique, bi-county audit system called the Trauma Audit Committee (TAC) held in conjunction with Alameda County EMS and Alameda County trauma centers. This review process has been in place since the inception of the County trauma system. Trauma surgeons from other California trauma systems also participate in the trauma system evaluation and monitoring process, bringing outside perspectives and the additional expertise from teaching facilities.
Historically, selection of cases to be presented at TAC meetings was done through the Pre-Trauma Audit Committee (PreTAC) meetings. Trauma Surgeon Directors on a rotating basis traveled to another of the four trauma centers to review care (chart review) provided trauma patients. In 2005 a new case review selection process was implemented which provided for Trauma Surgeon Director case review off site. The PreTAC continues to review EMS system issues related to trauma care.
John Muir Trauma Center also has its own internal monitoring and evaluation systems coordinated by an RN Trauma Program Coordinator. The Coordinator meets weekly with nurses, social service, physical therapists, neuropsychology, rehabilitation, nutritional services, pastoral care and patient accounting to analyze patients on the trauma service from a multidisciplinary perspective.
The Trauma System Plan for Contra Costa EMS was approved and updated in March of 2009 and submitted to EMSA in the fall of 2009. The Trauma System Plan was accepted by EMSA with recommendations for improvement. In August 2010 Contra Costa EMS submitted a Trauma System Status Report addressing the recommendations. In September of 2010, EMSA accepted the report as in full compliance with State guidelines.
Trauma Injury Prevention Program
The John Muir Injury Prevention Program has received National Awards of Recognition for its programs and service to the community. The John Muir Medical Center Trauma Service has reached over 20,000 Contra Costa residents directly. During 2010 the Trauma Center developed two new injury prevention/intervention projects through the Trauma Service, Beyond Violence and Alcohol screening and Brief Intervention for High Risk Drinking behavior.
Beyond Violence: Modeled after Highland Hospital’s “Caught in the Crossfire,”
“Beyond Violence” is aimed at reducing retaliation and re-injury to trauma patients, ages 15-25 years that result in street violence. The program is a collaborative project between John Muir Health, Contra Costa County Health Services, Richmond’s Office of Neighborhood Safety, One Day at a Time and the Williams Group.
Alcohol Screening and Intervention for High Risk Drinking Behavior: Research shows that there is a strong correlation between alcohol use and risk for injury and can be influenced by even brief encounters with a health care provider. This program is aimed at trauma inpatients, the goal is to screen and intervene eligible patients before discharge.
Childhood Occupant Protection: Aimed at children 0-15 years, parents and other
caregivers, the primary goal is to educate the target population in the use and proper use of child restraint devices. In August 2010 car seat fitting station program was re-vitalized under the leadership of Carol Powers MA director of the program. These efforts have greatly expanded the number of certified technicians in the community.
Occupant Protection for Teens: Although a variety of strategies are used to address
this very high-risk population, the largest and most active project, the “Every 15 Minutes” program, is an intense two-day crash scene reenactment aimed at increasing awareness among teens and their parents of the medical, legal, social and financial consequences of drinking and driving. Eleven schools in Contra Costa participate in the program. There are over 50 John Muir Medical Center nurse volunteers serving the community in this emotionally engaging program. There are seven programs planned for 2011.
Bicycle Safety: In both 2009 and 2010, the Trauma Center partnered with Contra
Costa Fire’s “Bikes for Tykes” program distributing over 350 bicycle helmets and ensuring each helmet was matched with a child to ensure proper fit. There are plans for a 2011 distribution also.
County and Regional Injury Prevention Programs
Child Injury Prevention Network-Bay Area (CIPN): This organization began in 2007 with the aim of bringing together individuals, agencies and organizations that share a common goal: to keep children safe from injury through education and outreach into our communities. The CIPN-BA is a multidisciplinary group of individuals and agencies crossing county lines committed to building community awareness of injury as a public health priority. Trauma is a major cause of pediatric preventable injury. The group provides networking opportunities, information and data-sharing and offers individual expertise in various areas in injury prevention. Contra Costa and Alameda County EMS partner with Children’s Hospital and Research Center Oakland to support network activities. For more information go to ww.childrenshospitaloakland.org/healthcare/depts./trauma_overview.asp
Contra Costa County Pediatric and Neonatal Disaster and Medical Surge
Network: This is an informal “grassroots” network of pediatric, neonatal, emergency care, and disaster professionals, from all disciplines, working to support Pediatric and Neonatal Surge Preparedness efforts in our communities. There are no costs or fees. The only requirement is a willingness to participate with like-minded colleagues.
The listserve connects participants with ideas, information, resources and strategies for supporting regional pediatric surge and disaster preparedness on the local, regional and state level. It is anticipated that in a major earthquake > 380 pediatric trauma victims will require care in Contra Costa County. For more information go to https://sites.google.com/site/pedineonetwork/

Trauma System Goals and Objectives

Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Overview: A number of goals and objectives have been identified to assure 1) rapid identification of severely injured patients in the field, with 2) prompt transport to a trauma center, where 3) well-qualified physician and nursing staff are equipped and prepared to provide immediate intervention and ongoing care appropriate to the needs of the patient. The following describes the Contra Costa Trauma System goals and objectives: Category Goal Objective Process/Metric Timeframe Trauma system planning
Trauma plan incorporates applicable standards and guidelines from American College of Surgeons Committee (ACSCOT) on Trauma Resources for Optimal Care of the Injured Patient 2006 and as may be revised from time to time.
Compare document standards to current EMS trauma policies and procedures to identify areas for improvement.
TAC case review and Trauma registry data used in the evaluation of trauma system policies, procedures and protocols for consistency with ACSC guidelines.
Policy and procedures reviewed annually and as needed per ACSC guideline updates.
Implement identified areas for improvement using a process designed for input from the Medical Advisory Committee (MAC) and the trauma center.
Pre TAC case review and EMS patient/provider safety reporting (EMS Event Reporting) used to identify gaps in trauma system planning and performance.
Reported annually with monthly, quarterly and as needed review.
Progress to date:
In January 1, 2009 the definition of “Major Trauma Victim” (MTV) was modified in the system to include only patients with an ISS of greater than 15. EMS and the Trauma Center agreed this would be more consistent with ACSCOT guidelines. This new definition is the one utilized by most trauma systems across the nation. Policies and procedures were updated to reflect that change. Historical data was retrospectively evaluated based on the new definition so trending metrics would be meaningful. The most current copies of these updated policies, procedures and protocols are available on our website at www.cccems.org

Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Category Goal Objective Process/Metric Timeframe
EMS Response
Rapid, well prepared response to injured patients in the field.
Monitor and evaluate fire first responder compliance with established response times monthly to assure a paramedic response to all 9-1-1 requests within each emergency response area.
Response times reflecting both fire first responders and ambulance providers for all 9-1-1 requests should be within 10 minutes at least 90% of the time.
Reviewed as part of fire first responder and ambulance contract compliance.
Reported annually with monthly, quarterly and as- needed review.
Monitor and evaluate emergency ambulance compliance with established response times monthly to assure a paramedic response to all 9-1-1 responses areas. Assure through annual contract compliance evaluations that fire first responder and ambulance personnel are well prepared to provide quality care for trauma victims by requiring ongoing training that meets or exceeds that established by the ACS as outlined in ITLS and PHTLS.
Documentation of appropriate training consistent with ITLS and/or PHTLS within the last year reviewed as part of contract compliance for both fire first responders and ambulance providers.
Annually.
Progress to date: In 2010 EMS system standard response time for metro/urban reflecting both fire first responders and EMS transport units averaged 6.84 minutes 90% of the time. Standards are met for all transport and enhanced first responder providers as locally defined using criteria based on local definitions of service areas with the approval of the Board of Supervisors. Additional information on response time metrics can be found in the Contra Costa EMS Annual Report posted on our website at www.cccems.org.
First responder fire and transport agencies track compliance with ITLS and PHTS training on in-house e-learning systems and submit training compliance reports at intervals as part of EMS and provider agency contract compliance. In May 2010, Contra Costa EMS recognized the successful completion of the ATT (Assessment and Treatment of Trauma) Course as being equivalent to ITLS and PHTLS. All three courses are now recognized as meeting prehospital trauma training requirements in Contra Costa County.
Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
1 No uniform methodology for calculating overtriage rates exist at the state or national level although ACS guidelines suggest that an overtriage rare of < 50% is preferred. 2 Excludes out-of-county transports, transfers, patient walk-ins, and patients transported to the trauma center as a receiving facility rather than as part of the trauma system. Considerations from evaluation include discharges from the emergency department and trauma team non-activations on EMS transports based on triage. 3 Undertriage Rate = number of under triages/number of patients triaged to trauma centers. 4 Undertriage Percent = number of under triages/number of patients triaged to receiving facilities.
Category Goal Objective Process/Metric Timeframe
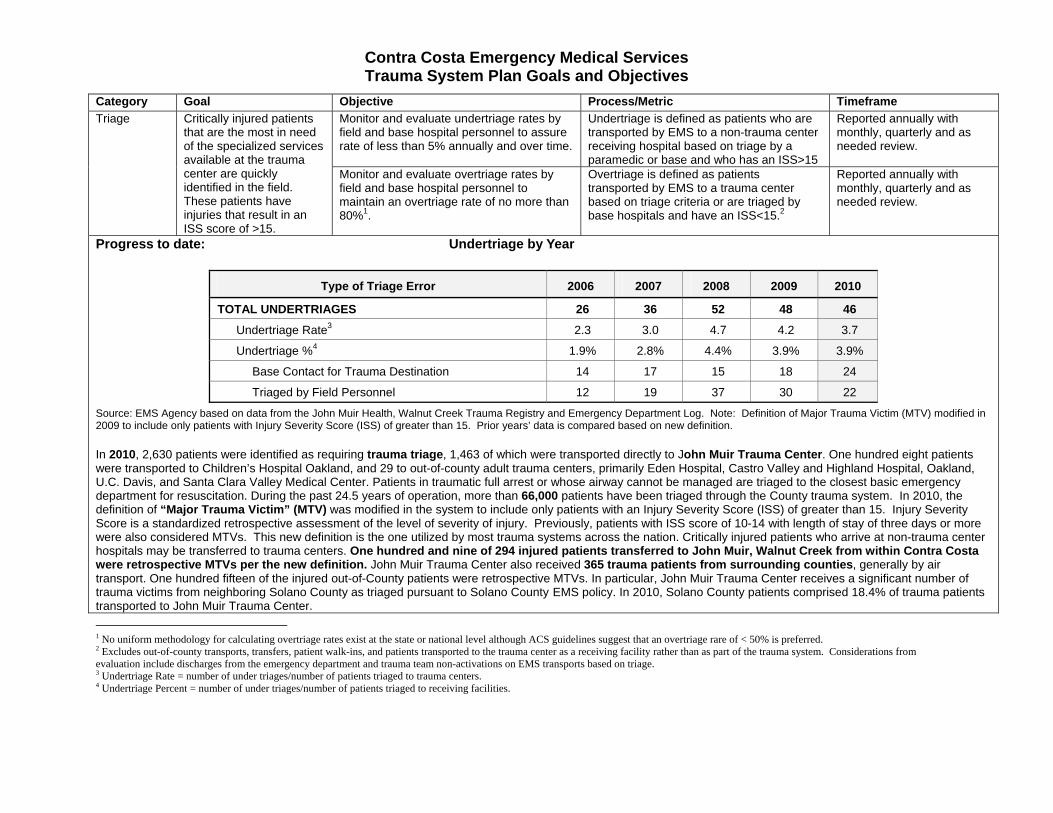
Triage Critically injured patients that are the most in need of the specialized services available at the trauma center are quickly identified in the field. These patients have injuries that result in an ISS score of >15.
Monitor and evaluate undertriage rates by field and base hospital personnel to assure rate of less than 5% annually and over time.
Undertriage is defined as patients who are transported by EMS to a non-trauma center receiving hospital based on triage by a paramedic or base and who has an ISS>15
Reported annually with monthly, quarterly and as needed review.
Monitor and evaluate overtriage rates by field and base hospital personnel to maintain an overtriage rate of no more than 80%1.
Overtriage is defined as patients transported by EMS to a trauma center based on triage criteria or are triaged by base hospitals and have an ISS<15.2
Reported annually with monthly, quarterly and as needed review.
Progress to date: Undertriage by Year
Type of Triage Error 2006 2007 2008 2009 2010
TOTAL UNDERTRIAGES 26 36 52 48 46
Undertriage Rate3 2.3 3.0 4.7 4.2 3.7
Undertriage %4 1.9% 2.8% 4.4% 3.9% 3.9%
Base Contact for Trauma Destination 14 17 15 18 24
Triaged by Field Personnel 12 19 37 30 22
Source: EMS Agency based on data from the John Muir Health, Walnut Creek Trauma Registry and Emergency Department Log. Note: Definition of Major Trauma Victim (MTV) modified in 2009 to include only patients with Injury Severity Score (ISS) of greater than 15. Prior years’ data is compared based on new definition.
In 2010, 2,630 patients were identified as requiring trauma triage, 1,463 of which were transported directly to John Muir Trauma Center. One hundred eight patients were transported to Children’s Hospital Oakland, and 29 to out-of-county adult trauma centers, primarily Eden Hospital, Castro Valley and Highland Hospital, Oakland, U.C. Davis, and Santa Clara Valley Medical Center. Patients in traumatic full arrest or whose airway cannot be managed are triaged to the closest basic emergency department for resuscitation. During the past 24.5 years of operation, more than 66,000 patients have been triaged through the County trauma system. In 2010, the definition of “Major Trauma Victim” (MTV) was modified in the system to include only patients with an Injury Severity Score (ISS) of greater than 15. Injury Severity Score is a standardized retrospective assessment of the level of severity of injury. Previously, patients with ISS score of 10-14 with length of stay of three days or more were also considered MTVs. This new definition is the one utilized by most trauma systems across the nation. Critically injured patients who arrive at non-trauma center hospitals may be transferred to trauma centers. One hundred and nine of 294 injured patients transferred to John Muir, Walnut Creek from within Contra Costa were retrospective MTVs per the new definition. John Muir Trauma Center also received 365 trauma patients from surrounding counties, generally by air transport. One hundred fifteen of the injured out-of-County patients were retrospective MTVs. In particular, John Muir Trauma Center receives a significant number of trauma victims from neighboring Solano County as triaged pursuant to Solano County EMS policy. In 2010, Solano County patients comprised 18.4% of trauma patients transported to John Muir Trauma Center.
Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
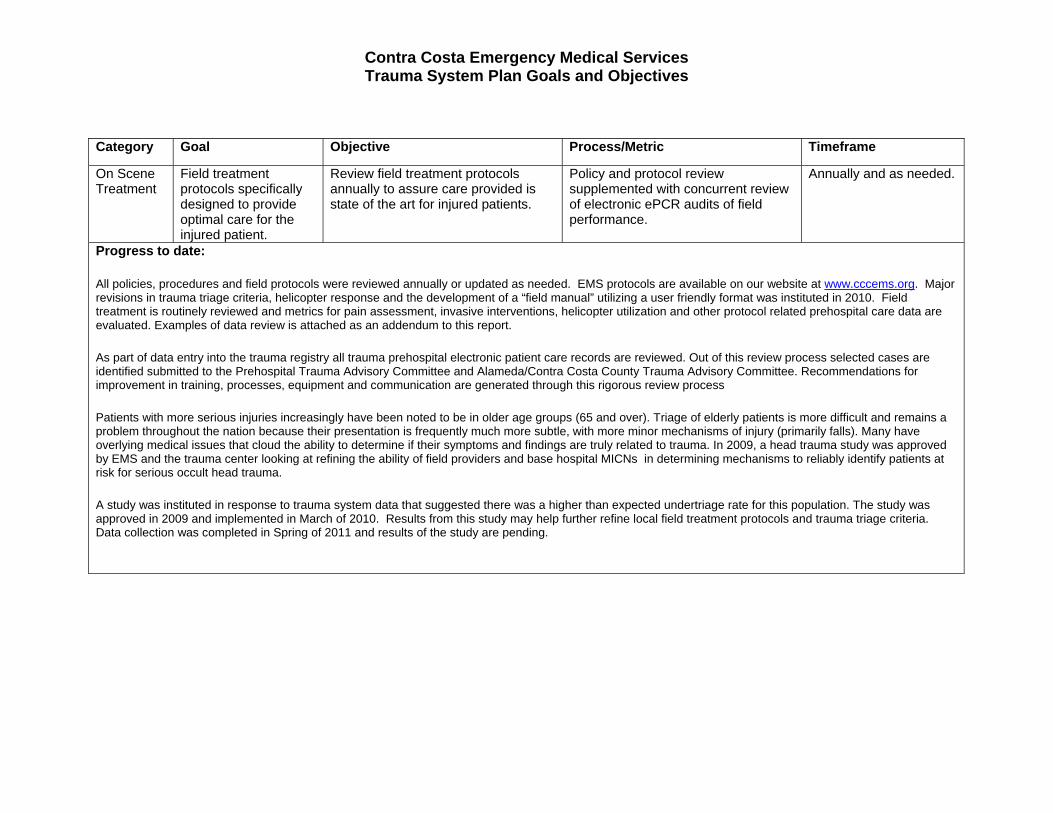
Category Goal Objective Process/Metric Timeframe
On Scene Treatment
Field treatment protocols specifically designed to provide optimal care for the injured patient.
Review field treatment protocols annually to assure care provided is state of the art for injured patients.
Policy and protocol review supplemented with concurrent review of electronic ePCR audits of field performance.
Annually and as needed.
Progress to date:
All policies, procedures and field protocols were reviewed annually or updated as needed. EMS protocols are available on our website at www.cccems.org. Major revisions in trauma triage criteria, helicopter response and the development of a “field manual” utilizing a user friendly format was instituted in 2010. Field treatment is routinely reviewed and metrics for pain assessment, invasive interventions, helicopter utilization and other protocol related prehospital care data are evaluated. Examples of data review is attached as an addendum to this report.
As part of data entry into the trauma registry all trauma prehospital electronic patient care records are reviewed. Out of this review process selected cases are identified submitted to the Prehospital Trauma Advisory Committee and Alameda/Contra Costa County Trauma Advisory Committee. Recommendations for improvement in training, processes, equipment and communication are generated through this rigorous review process
Patients with more serious injuries increasingly have been noted to be in older age groups (65 and over). Triage of elderly patients is more difficult and remains a problem throughout the nation because their presentation is frequently much more subtle, with more minor mechanisms of injury (primarily falls). Many have overlying medical issues that cloud the ability to determine if their symptoms and findings are truly related to trauma. In 2009, a head trauma study was approved by EMS and the trauma center looking at refining the ability of field providers and base hospital MICNs in determining mechanisms to reliably identify patients at risk for serious occult head trauma.
A study was instituted in response to trauma system data that suggested there was a higher than expected undertriage rate for this population. The study was approved in 2009 and implemented in March of 2010. Results from this study may help further refine local field treatment protocols and trauma triage criteria. Data collection was completed in Spring of 2011 and results of the study are pending.
Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Category Goal Objective Process/Metric Timeframe
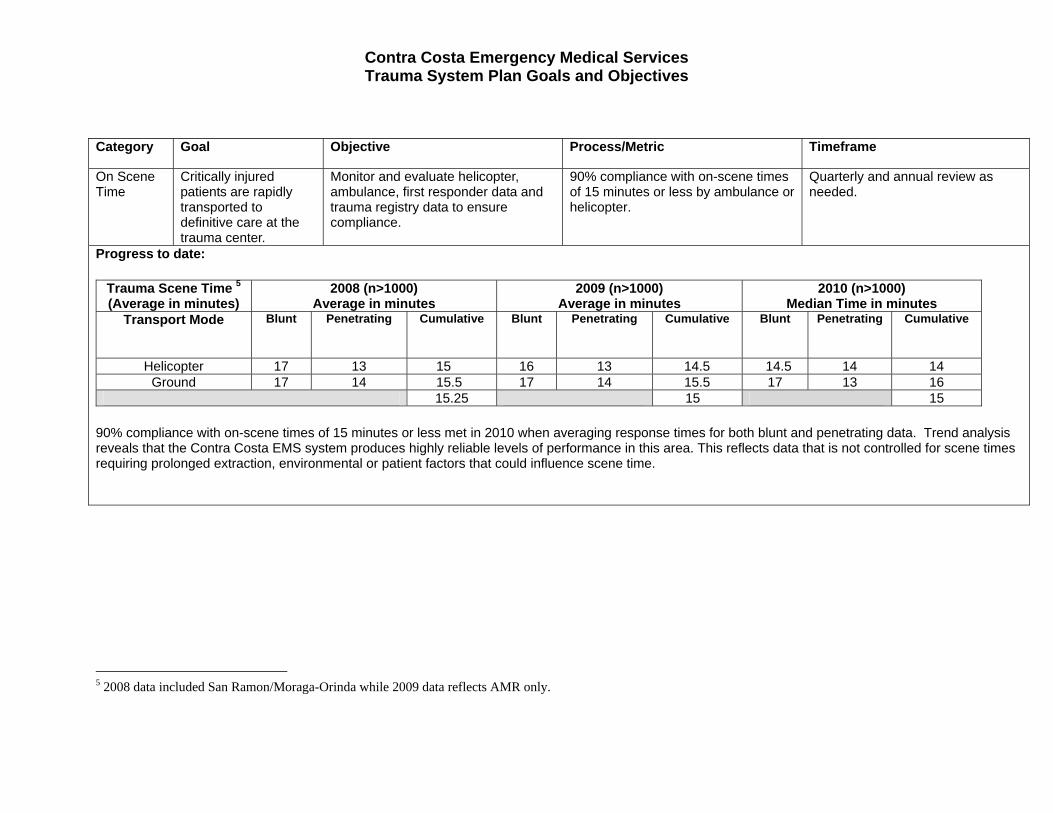
On Scene Time
Critically injured patients are rapidly transported to definitive care at the trauma center.
Monitor and evaluate helicopter, ambulance, first responder data and trauma registry data to ensure compliance.
90% compliance with on-scene times of 15 minutes or less by ambulance or helicopter.
Quarterly and annual review as needed.
Progress to date:
Trauma Scene Time 5 (Average in minutes)
2008 (n>1000) Average in minutes
2009 (n>1000) Average in minutes
2010 (n>1000) Median Time in minutes
Transport Mode Blunt Penetrating
Cumulative Blunt Penetrating Cumulative Blunt Penetrating Cumulative
Helicopter 17 13 15 16 13 14.5 14.5 14 14 Ground 17 14 15.5 17 14 15.5 17 13 16
15.25 15 15
90% compliance with on-scene times of 15 minutes or less met in 2010 when averaging response times for both blunt and penetrating data. Trend analysis reveals that the Contra Costa EMS system produces highly reliable levels of performance in this area. This reflects data that is not controlled for scene times requiring prolonged extraction, environmental or patient factors that could influence scene time.
5 2008 data included San Ramon/Moraga-Orinda while 2009 data reflects AMR only.

Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Category Goal Objective Process/Metric Timeframe Transport Mode Critically injured trauma
patients are transported from the field to a trauma center rapidly and in a safe manner.
Monitor and evaluate ground vs helicopter utilization data to ensure there is identified and measurable time-savings compliance.6
90% helicopter scene time meets or exceeds 25 minute local metric and outliers demonstrate other benefit to the patient.7
Quarterly and annual review as needed.
Progress to date:
Contra Costa EMS has been working with CALSTAR, REACH and the Helicopter Task Force to develop appropriate EMS System Performance Metrics for Air Medical Response. Efforts being made to link electronic patient care data to EMS for review and analysis. Current system relies on many non-electronic processes and needs to be improved to facilitate appropriate data management.
Trauma Scene Time 8 (Average in minutes)
2008 (n>1000) Average in minutes
2009 (n>1000) Average in minutes
2010 (n>1000) Median Time in minutes
Transport Mode Blunt Penetrating
Cumulative Blunt Penetrating Cumulative Blunt Penetrating Cumulative
Helicopter 17 13 15 16 13 14.5 14.5 14 14 Ground 17 14 15.5 17 14 15.5 17 13 16
15.25 15 15
90% compliance with on-scene times of 25 minutes or less met in 2010 when averaging response times for both blunt and penetrating data. Trend analysis reveals that the Contra Costa EMS system produces highly reliable levels of performance in this area. This reflects data that is not controlled for scene times requiring prolonged extraction, environmental or patient factors that could influence scene time.
6 Ground ambulance transport times set the maximum standard and helicopter transport is used only if there is a measurable timesaving or if treatment needed is only available by helicopter staff. Helicopter field care and transport time (which includes on-scene, flight and transport from helipad to ED) is optimally 20-25 minutes in most cases. 7 See footnote #2. 8 2008 data included San Ramon/Moraga-Orinda while 2009 data reflects AMR only.
Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Category Goal Objective Process/Metric Timeframe Trauma Center Designation
A Level II trauma center is designated within Contra Costa County and is committed to providing care to critically injured patients.
Maintain a written agreement with a local Level II trauma center that requires compliance with State and local trauma system plan.
Written contract on file and maintained.
Reviewed annually and renewed per contract terms.
Progress to date:
A new trauma center contract was approved, by the Contra Costa Board of Supervisors (BOS), on May 22, 2010. The contract term is through May 21, 2021 with conditional automatic renewal to 2031. Contracts are on file at Contra Costa EMS offices.
Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
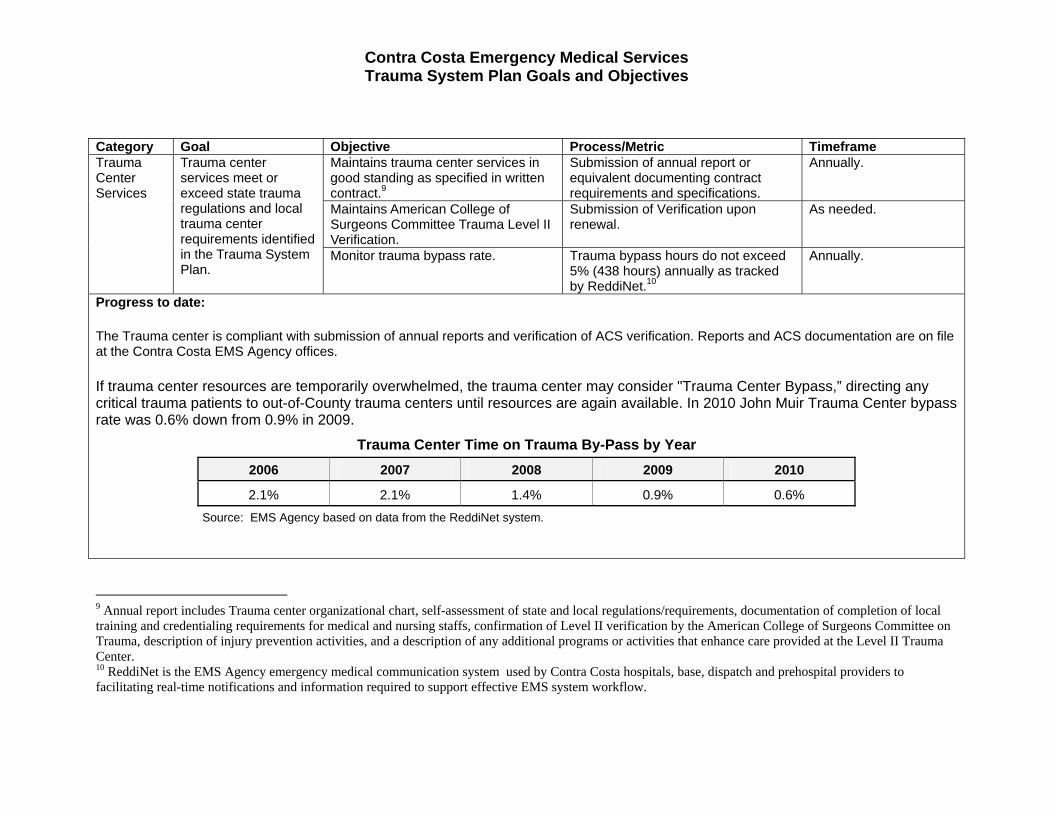
Category Goal Objective Process/Metric Timeframe Trauma Center Services
Trauma center services meet or exceed state trauma regulations and local trauma center requirements identified in the Trauma System Plan.
Maintains trauma center services in good standing as specified in written contract.9
Submission of annual report or equivalent documenting contract requirements and specifications.
Annually.
Maintains American College of Surgeons Committee Trauma Level II Verification.
Submission of Verification upon renewal.
As needed.
Monitor trauma bypass rate. Trauma bypass hours do not exceed 5% (438 hours) annually as tracked by ReddiNet.10
Annually.
Progress to date:
The Trauma center is compliant with submission of annual reports and verification of ACS verification. Reports and ACS documentation are on file at the Contra Costa EMS Agency offices.
If trauma center resources are temporarily overwhelmed, the trauma center may consider "Trauma Center Bypass,” directing any critical trauma patients to out-of-County trauma centers until resources are again available. In 2010 John Muir Trauma Center bypass rate was 0.6% down from 0.9% in 2009.
Trauma Center Time on Trauma By-Pass by Year
2006 2007 2008 2009 2010
2.1% 2.1% 1.4% 0.9% 0.6%
Source: EMS Agency based on data from the ReddiNet system.
9 Annual report includes Trauma center organizational chart, self-assessment of state and local regulations/requirements, documentation of completion of local training and credentialing requirements for medical and nursing staffs, confirmation of Level II verification by the American College of Surgeons Committee on Trauma, description of injury prevention activities, and a description of any additional programs or activities that enhance care provided at the Level II Trauma Center. 10 ReddiNet is the EMS Agency emergency medical communication system used by Contra Costa hospitals, base, dispatch and prehospital providers to facilitating real-time notifications and information required to support effective EMS system workflow.

Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Category Goal Objective Process/Metric Timeframe
Trauma Center and Trauma System Evaluation
The trauma center maintains a comprehensive trauma registry and collects EMS related data that includes a minimum of those patients described in “Patient Inclusion Criteria” for the National Trauma Data Bank.
Assure data is available to evaluate care provided to all injured patients at the trauma center.
All required data readily available and accessible to evaluate both objectives.
As needed and annually.
Assure data is available to evaluate triage, transport and field treatment of all critically injured patients.
Progress to date:
The Trauma Registry is maintained by the Trauma Center and data is accessible through National Trauma Data Bank.
Contra Costa EMS actively participates in the CEMSIS Trauma Grant program and successfully submitted data during the 2009-2011 to State EMSA at designated intervals as part of the CEMSIS demonstration grant project. Support for data linkages to the State are being facilitated by Lancet.
A Contra Costa EMS Trauma Coordinator supports prehospital data entry and access to Trauma System data. Data is analyzed and reviewed routinely by EMS Staff and Dr. Joe Barger, Contra Costa EMS Medical Director. Dr. Barger serves on the State EMS Trauma Commission collaborating with trauma systems throughout the state to improve outcomes for patients. Contra Costa EMS continues to actively contribute to the development of Trauma System data evaluation on the local, regional and state level and is a strong advocate for data driven Trauma and EMS System evaluation.
Contra Costa Emergency Medical Services Trauma System Plan Goals and Objectives
Category Goal Objective Process/Metric Timeframe
Trauma Center and Trauma System Evaluation
Mechanisms are in place to assure that quality trauma care is provided all critically injured patients in Contra Costa County.
Compliance with Trauma Policy 16 and the associated Trauma System Quality Improvement Program.
Full compliance is equivalent to at least four Trauma Audit Committee meetings annually and six to eight prehospital trauma care review meetings.
Annually.
Annual review of trauma system plan. Submission of Trauma System Plan status report of equivalent to the state EMS authority.
Annually.
Progress to date:
Contra Costa was in full compliance with its Trauma System Plan. In 2011 Contra Costa engaged its Trauma Center in a trauma system CQI redesign process to enhance the Trauma CQI program. The new program in development will support a strong systems based approach to CQI defining meaningful metrics focused on improving patient outcomes and patient flow to definitive care.
Contra Costa Trauma System status reports are submitted to State EMSA as required annually.

2010 Helicopter Utilization Report
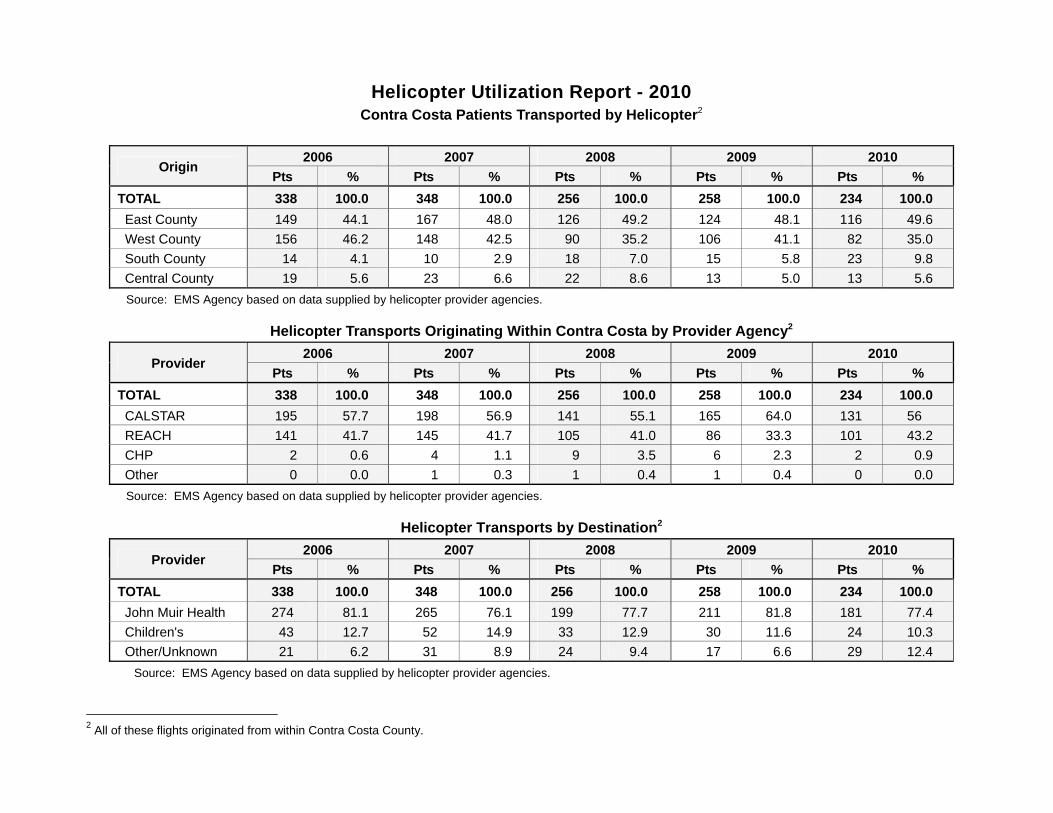
Helicopter Utilization Report - 2010 Contra Costa Patients Transported by Helicopter2
Origin 2006 2007 2008 2009 2010
Pts % Pts % Pts % Pts % Pts %
TOTAL 338 100.0 348 100.0 256 100.0 258 100.0 234 100.0
East County 149 44.1 167 48.0 126 49.2 124 48.1 116 49.6
West County 156 46.2 148 42.5 90 35.2 106 41.1 82 35.0
South County 14 4.1 10 2.9 18 7.0 15 5.8 23 9.8
Central County 19 5.6 23 6.6 22 8.6 13 5.0 13 5.6
Source: EMS Agency based on data supplied by helicopter provider agencies.
Helicopter Transports Originating Within Contra Costa by Provider Agency2
Provider 2006 2007 2008 2009 2010
Pts % Pts % Pts % Pts % Pts %
TOTAL 338 100.0 348 100.0 256 100.0 258 100.0 234 100.0
CALSTAR 195 57.7 198 56.9 141 55.1 165 64.0 131 56
REACH 141 41.7 145 41.7 105 41.0 86 33.3 101 43.2
CHP 2 0.6 4 1.1 9 3.5 6 2.3 2 0.9
Other 0 0.0 1 0.3 1 0.4 1 0.4 0 0.0
Source: EMS Agency based on data supplied by helicopter provider agencies.
Helicopter Transports by Destination2
Provider 2006 2007 2008 2009 2010
Pts % Pts % Pts % Pts % Pts %
TOTAL 338 100.0 348 100.0 256 100.0 258 100.0 234 100.0
John Muir Health 274 81.1 265 76.1 199 77.7 211 81.8 181 77.4
Children's 43 12.7 52 14.9 33 12.9 30 11.6 24 10.3
Other/Unknown 21 6.2 31 8.9 24 9.4 17 6.6 29 12.4
Source: EMS Agency based on data supplied by helicopter provider agencies.
2 All of these flights originated from within Contra Costa County.

Helicopter Transports by Patient Assessment3
Provider 2006 2007 2008 2009 2010
Pts % Pts % Pts % Pts % Pts %
TOTAL 338 100.0 348 100.0 256 100.0 258 100.0 234 100.0
Trauma 305 90.2 322 92.5 233 91.0 241 93.4 213 91
Burn 2 0.6 13 3.7 13 5.1 8 3.1 14 6
Other 5 1.5 13 3.7 10 3.9 9 3.5 7 3
Unknown 26 7.7 0.0 0.0 0 0.0 0 0.0 0 0.0
Source: EMS Agency based on data supplied by helicopter provider agencies.
Helicopter to Trauma Center Transports by Age and Severity (Major Trauma Victim “MTV”)
Origin 2006 2007 2008 20094 2010
Pts % Pts % Pts % Pts % Pts %
TOTAL 315 322 229 238 208
Adult 277 100.0 269 100.0 193 100.0 205 100.0 183 100
MTV (ISS > 15) 96 34.7 106 39.4 80 41.5 86 58.0 73 39.9
Non-MTV (ISS < 15) 181 65.3 163 60.6 113 58.5 119 42.0 110 60.1
Pediatric 38 100.0 53 100.0 36 100.0 36 100.0 25 100
MTV (ISS > 15) 6 15.8 5 9.4 7 19.4 10 27.8 4 16
Non-MTV (ISS < 15) 32 84.2 48 90.6 27 80.6 26 72.2 21 84
Source: EMS Agency based on data from the Trauma Registries at John Muir Walnut Creek, Children’s Hospital, Eden Medical Center and UC Davis Medical Center.
3 All of these flights originated from within Contra Costa County. 4 Definition of Major Trauma Victim (MTV) modified in 2009 to include only patients with Injury Severity Score (ISS) of greater than 15. Prior years’ data is compared
based on new definition. Some outcomes were not available.

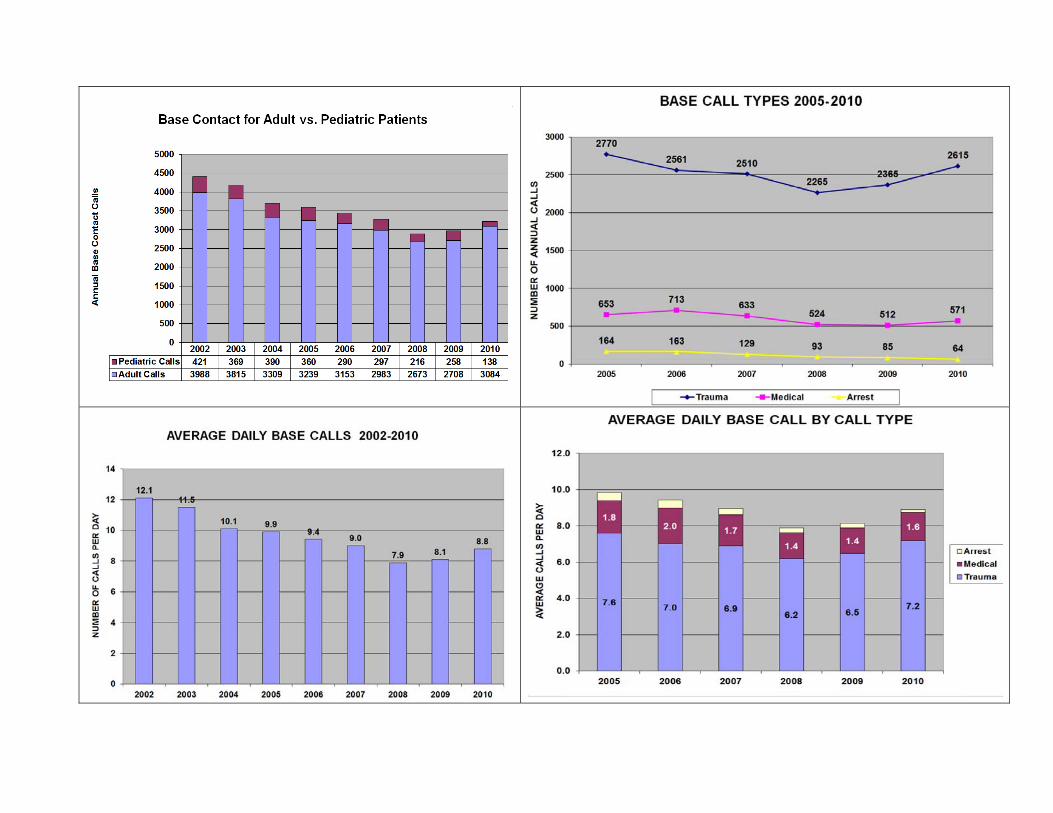
Base Hospital Contact Report
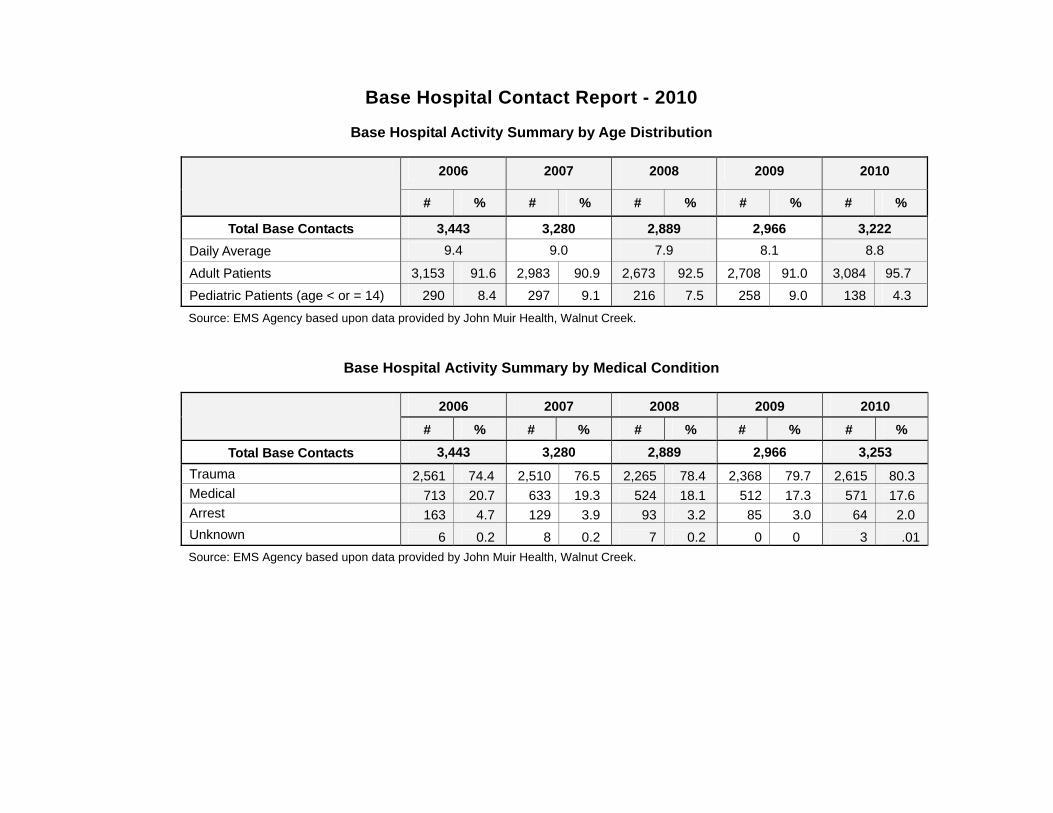
Base Hospital Contact Report - 2010
Base Hospital Activity Summary by Age Distribution
2006 2007 2008 2009 2010
# % # % # % # % # %
Total Base Contacts 3,443 3,280 2,889 2,966 3,222
Daily Average 9.4 9.0 7.9 8.1 8.8
Adult Patients 3,153 91.6 2,983 90.9 2,673 92.5 2,708 91.0 3,084 95.7
Pediatric Patients (age < or = 14) 290 8.4 297 9.1 216 7.5 258 9.0 138 4.3
Source: EMS Agency based upon data provided by John Muir Health, Walnut Creek.
Base Hospital Activity Summary by Medical Condition
2006 2007 2008 2009 2010
# % # % # % # % # %
Total Base Contacts 3,443 3,280 2,889 2,966 3,253
Trauma 2,561 74.4 2,510 76.5 2,265 78.4 2,368 79.7 2,615 80.3 Medical 713 20.7 633 19.3 524 18.1 512 17.3 571 17.6 Arrest 163 4.7 129 3.9 93 3.2 85 3.0 64 2.0
Unknown 6 0.2 8 0.2 7 0.2 0 0 3 .01
Source: EMS Agency based upon data provided by John Muir Health, Walnut Creek.
Trauma System Report

Contra Costa Trauma System Report - 2010
On-Scene Triage of Patients within Contra Costa Meeting Field Trauma Criteria
2006 2007 2008 2009 2010
TOTAL PATIENTS TRIAGED 2,491 2,488 2,269 2,381 2,420
Transported to a trauma center 1,123 1,184 1,097 1,155 1,253
John Muir Health, Walnut Creek 1,006 1,026 953 1,018 1,134
Children's Hospital, Oakland 94 107 93 108 94
Other trauma center 23 51 51 29 25
Transported to non-trauma center hospitals 1,368 1,304 1,172 1,226 1,167
Contra Costa Regional Medical Center 80 79 66 61 89
Doctors San Pablo 201 190 135 136 159
John Muir Health - Concord 209 169 153 138 142
John Muir Health - Walnut Creek5 216 235 220 253 232
Kaiser Antioch 18 83 99 135
Kaiser Richmond 102 75 75 71 82
Kaiser Walnut Creek 116 136 110 115 170
San Ramon Regional 21 26 33 41 36
Sutter Delta 257 238 176 201 196
Out-of-county 38 28 30 25 34
Unknown 128 110 91 86 112
Source: EMS Agency based on data from the John Muir Health, Walnut Creek Trauma Registry and Emergency Department Log.
Undertriage by Year
Type of Triage Error 2006 2007 2008 2009 2010
TOTAL UNDERTRIAGES 26 36 52 48 46
Undertriage Rate6 2.3 3.0 4.7 4.2 3.7
Undertriage %7 1.9% 2.8% 4.4% 3.9% 3.9%
Base Contact for Trauma Destination 14 17 15 18 24
Triaged by Field Personnel 12 19 37 30 22
Source: EMS Agency based on data from the John Muir Health, Walnut Creek Trauma Registry and Emergency Department Log. Note: Definition of Major Trauma Victim (MTV) modified in 2009 to include only patients with Injury Severity Score (ISS) of greater than 15. Prior years’ data is compared based on new definition.
Trauma Center Time on Trauma By-Pass by Year
2006 2007 2008 2009 2010
2.1% 2.1% 1.4% 0.9% 0.6%
Source: EMS Agency based on data from the ReddiNet system.
5 These patients were triaged as not having major trauma but were transported to John Muir, Walnut Creek as the closest facility. 6 Undertriage Rate = number of under triages/number of patients triaged to trauma centers. 7 Undertriage Percent = number of under triages/number of patients triaged to receiving facilities.
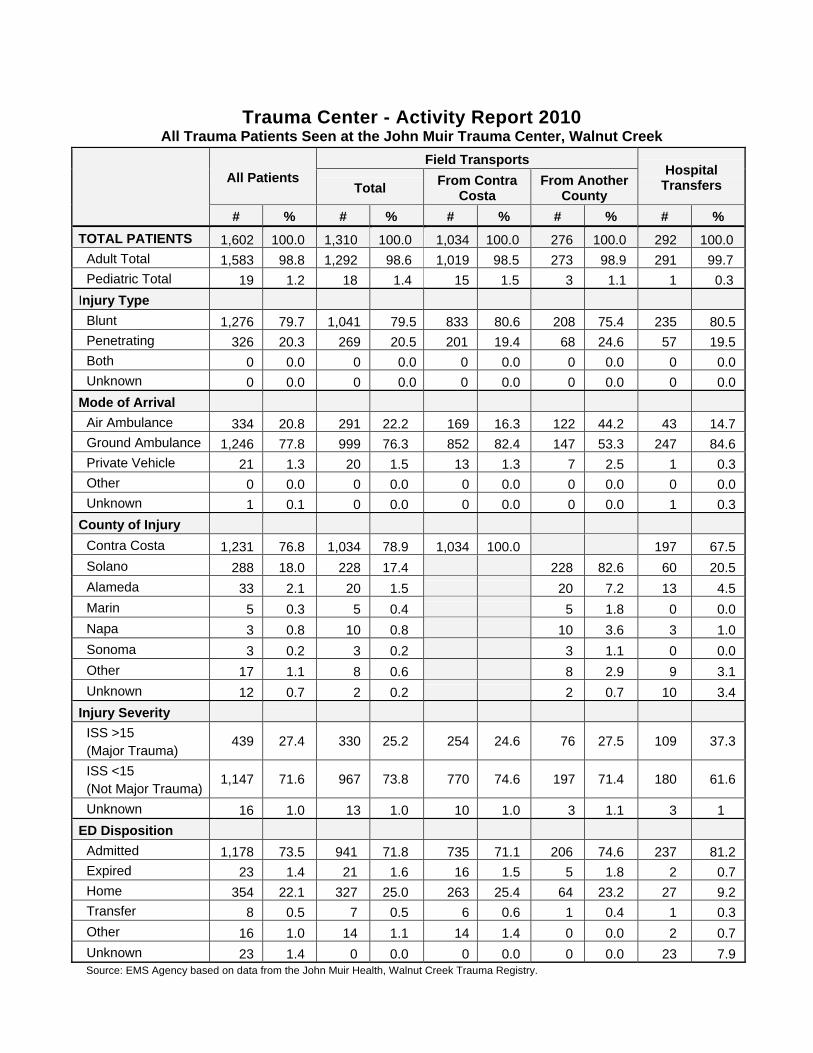
Trauma Center - Activity Report 2010 All Trauma Patients Seen at the John Muir Trauma Center, Walnut Creek
All Patients
Field Transports Hospital
Transfers Total From Contra
Costa From Another
County
# % # % # % # % # %
TOTAL PATIENTS 1,602 100.0 1,310 100.0 1,034 100.0 276 100.0 292 100.0
Adult Total 1,583 98.8 1,292 98.6 1,019 98.5 273 98.9 291 99.7
Pediatric Total 19 1.2 18 1.4 15 1.5 3 1.1 1 0.3
Injury Type
Blunt 1,276 79.7 1,041 79.5 833 80.6 208 75.4 235 80.5
Penetrating 326 20.3 269 20.5 201 19.4 68 24.6 57 19.5
Both 0 0.0 0 0.0 0 0.0 0 0.0 0 0.0
Unknown 0 0.0 0 0.0 0 0.0 0 0.0 0 0.0
Mode of Arrival
Air Ambulance 334 20.8 291 22.2 169 16.3 122 44.2 43 14.7
Ground Ambulance 1,246 77.8 999 76.3 852 82.4 147 53.3 247 84.6
Private Vehicle 21 1.3 20 1.5 13 1.3 7 2.5 1 0.3
Other 0 0.0 0 0.0 0 0.0 0 0.0 0 0.0
Unknown 1 0.1 0 0.0 0 0.0 0 0.0 1 0.3
County of Injury
Contra Costa 1,231 76.8 1,034 78.9 1,034 100.0 197 67.5
Solano 288 18.0 228 17.4 228 82.6 60 20.5
Alameda 33 2.1 20 1.5 20 7.2 13 4.5
Marin 5 0.3 5 0.4 5 1.8 0 0.0
Napa 3 0.8 10 0.8 10 3.6 3 1.0
Sonoma 3 0.2 3 0.2 3 1.1 0 0.0
Other 17 1.1 8 0.6 8 2.9 9 3.1
Unknown 12 0.7 2 0.2 2 0.7 10 3.4
Injury Severity
ISS >15 (Major Trauma)
439 27.4 330 25.2 254 24.6 76 27.5 109 37.3
ISS <15 (Not Major Trauma)
1,147 71.6 967 73.8 770 74.6 197 71.4 180 61.6
Unknown 16 1.0 13 1.0 10 1.0 3 1.1 3 1
ED Disposition
Admitted 1,178 73.5 941 71.8 735 71.1 206 74.6 237 81.2
Expired 23 1.4 21 1.6 16 1.5 5 1.8 2 0.7
Home 354 22.1 327 25.0 263 25.4 64 23.2 27 9.2
Transfer 8 0.5 7 0.5 6 0.6 1 0.4 1 0.3
Other 16 1.0 14 1.1 14 1.4 0 0.0 2 0.7
Unknown 23 1.4 0 0.0 0 0.0 0 0.0 23 7.9 Source: EMS Agency based on data from the John Muir Health, Walnut Creek Trauma Registry.
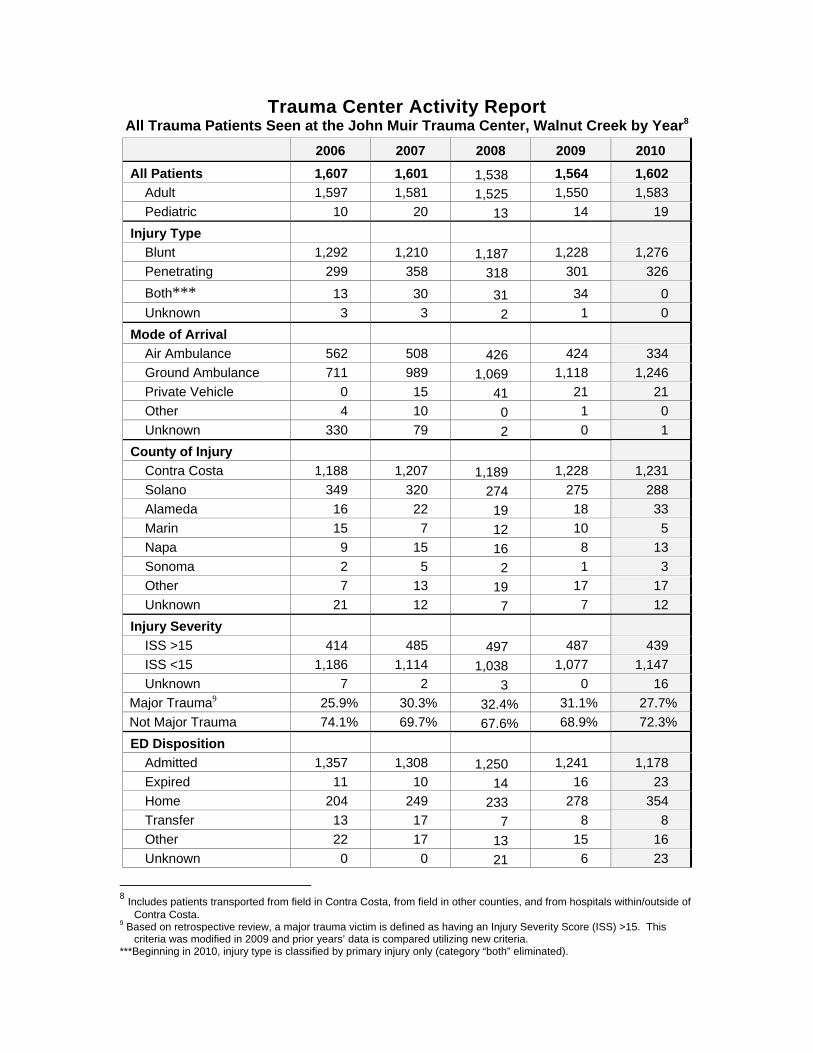
Trauma Center Activity Report All Trauma Patients Seen at the John Muir Trauma Center, Walnut Creek by Year8
2006 2007 2008 2009 2010
All Patients 1,607 1,601 1,538 1,564 1,602
Adult 1,597 1,581 1,525 1,550 1,583
Pediatric 10 20 13 14 19
Injury Type
Blunt 1,292 1,210 1,187 1,228 1,276
Penetrating 299 358 318 301 326
Both*** 13 30 31 34 0
Unknown 3 3 2 1 0
Mode of Arrival
Air Ambulance 562 508 426 424 334
Ground Ambulance 711 989 1,069 1,118 1,246
Private Vehicle 0 15 41 21 21
Other 4 10 0 1 0
Unknown 330 79 2 0 1
County of Injury
Contra Costa 1,188 1,207 1,189 1,228 1,231
Solano 349 320 274 275 288
Alameda 16 22 19 18 33
Marin 15 7 12 10 5
Napa 9 15 16 8 13
Sonoma 2 5 2 1 3
Other 7 13 19 17 17
Unknown 21 12 7 7 12
Injury Severity
ISS >15 414 485 497 487 439
ISS <15 1,186 1,114 1,038 1,077 1,147
Unknown 7 2 3 0 16
Major Trauma9 25.9% 30.3% 32.4% 31.1% 27.7%
Not Major Trauma 74.1% 69.7% 67.6% 68.9% 72.3%
ED Disposition
Admitted 1,357 1,308 1,250 1,241 1,178
Expired 11 10 14 16 23
Home 204 249 233 278 354
Transfer 13 17 7 8 8
Other 22 17 13 15 16
Unknown 0 0 21 6 23
8 Includes patients transported from field in Contra Costa, from field in other counties, and from hospitals within/outside of
Contra Costa. 9 Based on retrospective review, a major trauma victim is defined as having an Injury Severity Score (ISS) >15. This
criteria was modified in 2009 and prior years’ data is compared utilizing new criteria. ***Beginning in 2010, injury type is classified by primary injury only (category “both” eliminated).
May 27, 2011 Kacey A. Hansen, RN MBA Director, Trauma and Transfer Services John Muir Medical Center 1601 Ygnacio Valley Road Walnut Creek, CA 94598 Dear Ms. Hansen: The Verification Review Committee (VRC), a subcommittee of the American College of Surgeons Committee on Trauma, has carefully reviewed the additional documentation submitted by the hospital on May 13, 2011. With the additional documentation, the one Type II criterion deficiencies (11.14) has been successfully addressed. The Level II Trauma Center verification for the John Muir Medical Center has been extended for an additional two years. The Committee on Trauma’s certificate of verification for the additional two years (November 7, 2011 to November 7, 2013) will arrive under separate cover within the next several weeks. Included with the certificate will be a press release documents to assist the hospital with its advertising. Congratulations on your verification as a Level II Trauma Center! Thank you for your interest and participation in the Consultation/Verification Review Program of the Committee on Trauma of the American College of Surgeons. We are always glad to answer any questions you may have and look forward to working with you in the future. Sincerely, Chris Cribari, MD FACS Chair, Verification Review Committee