Embed Size (px)
Citation preview

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 1 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Traumatic Brain Injury: Pathophysiological Mechanisms and Potential Nutrient Needs
Angus G. Scrimgeour PhDMilitary Nutrition Division
U.S. Army Research Institute of Environmental MedicineNatick, Massachusetts 01760

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 2 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Disclaimer: The opinions or assertions contained herein are the private views of the author and are not to be construed as official or as reflecting the views of the Army or the DoD. Any citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement of approval of the products or services of these organizations.
Disclaimer

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 3 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Objectives
Defining the problem IOM 2011 RecommendationsNutrient Interventions for TBIPharmaceutical vs. NutriceuticalSummary & Conclusions

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 4 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
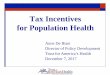
Defining the problem: Incidence in the USA
8%
13%
1%
4%
10%
8%2%
3%
51%
Concussion Rates among US high school athletes
Boys' Soccer
Girls' Soccer
Volleyball
Boys' Basketball
Girls' Basketball
Wrestling
Baseball
Softball
Football
1%1% 10%
82%
6%
DoD Numbers for TBI
Penetrating
Severe
Moderate
Mild
Not Classifiable
TBIs account for approximately 2.5M emergency department visits, hospitalizations & deaths in the U.S./yr. Of these, approximately 87% (2,213,826) are treated in EDs, and released; 11% (283,630) are hospitalized
and discharged, and 2% (52,844) die. DoD data from 2000 - 2017, indicate 379,519 service members were diagnosed with a TBI (dvbic.dcoe.mil).
The numbers do not account for persons who did not receive medical care, or had outpatient visits.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 5 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Source: www.afhsc.mil/msmr [2015 Vol 22 (2)].
Deployment-related conditions of special surveillance interest, US Armed Forces, by month and service, January 2003-January 2015.
Defining the problem: US Warfighter incidence

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 6 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Classification of TBI by Injury Severity
Mild Moderate Severe
GCS 13-15 GCS 9-12 GCS <9
Altered or LOC < 30 min with normal CT and/or MRI
LOC < 6 hours with abnormal CT and/or MRI
LOC > 6 hours with abnormal CT and/or
MRI
PTA < 24 hrs PTA < 7 days PTA ≥ 7 days
DoD:n=312,495 36,269 3,974
Source: dvbic.dcoe.mil

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 7 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM 2011 Recommendations:Reliance on Evidence-Based Reviews
Summary of Recommendations

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 8 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM (2011): Standardize the Provision of Energy and Protein to Patients with Severe TBI
Recommendation 6-1: Evidence-based guidelines should include the provision of early (within 24 h after injury)
nutrition (more than 50% of total energy expenditure and 1-1.5 g/kg protein) for the first 2 weeks after injury.
Intervention will limit the intensity of the inflammation response due to TBI, and improve outcome.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 9 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM (2011): Assessing Nutrition Status
Recommendation 5-1: DoD should conduct dietary intake assessments in different military settings (e.g. when eating in military dining facilities or when subsisting on a predominantly ration-based diet) both pre-deployment and during deployment to determine the nutritional status of Soldiers as a basis for recommending increases in intake of specific nutrients that may provide resilience to TBI.
Recommendation 5-2: Routine dietary intake assessments on TBI patients in medical treatment facilities should be undertaken as soon after hospitalization as possible to estimate pre-injury nutrition status, and to provide optimal nutritional intake throughout the various stages of treatment.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 10 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM (2011): Most Promising Research Recommendations
Recommendation 6-2: DoD should conduct human trials to determine appropriate levels of blood glucose (BG) following TBI to minimize morbidity & mortality. These should be clinical trials of early feeding using intense insulin therapy to maintain BG concentrations at less than 150-160 mg/dl versus current usual care of acute TBI in ICU settings for the first 2 weeks.
Recommendation 6-3: DoD should conduct clinical trials of the benefits of insulin therapy for care of acute TBI in inpatient settings with total parenteral nutrition (TPN) alone (or plus enteral feeding) versus enteral feeding alone. The goals for BG in the TPN group should be lower (e.g. < 120 mg/dl) than in the enteral group (e.g. < 150-160 mg/dl). Variables to measure include clinical outcomes and incidence of hypoglycemia.
Recommendation 8-1: DoD should continue to monitor the literature on the effects of nutrients, dietary supplements, and diets on TBI, particularly those that may emerge as potentially effective in the future.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 11 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Recommendation 9-1:
DoD should monitor the COBRIT trial that is examining the effect of CDP-choline and genomic factors on cognition & functional measures in severe, moderate, and complicated mild TBI.
If successful, DoD should conduct animal studies to define the optimal dose & duration of treatment following TBI, as well as to explore choline’s potential to promote resilience to TBI when used pre-injury.
IOM (2011): Most Promising Research Recommendations

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 12 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Citicoline update
Citicoline, an intermediate in the generation of phosphatidylcholine from choline, is found in eggs, beef liver, milk, yogurt and cruciferous veggies.
The COBRIT Trial (Citicoline Brain Injury Treatment) Trial was a phase III, double-blind study comparing citicoline vs placebo. 1,213 study participants with complicated mild, moderate, or severe TBI were randomized to receive 2,000 mg of citicoline or placebo daily for 90 days. This 4-yr trial (2007-2011) was terminated early due to futility. Among patients with TBI, the use of citicoline compared with placebo did not result in improvement in functional and cognitive status (1).
Sources:1. Zafonte et al 2012 Effect of citicoline on functional and cognitive status among patients with TBI: Citicoline Brain Injury Treatment Trial (COBRIT). JAMA 308: 1993-2000.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 13 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Recommendation 10-1: Based on the evidence supporting the effects of creatine on brain function and behavior after TBI in children & adolescents, DoD should initiate studies in adults to assess the value of creatine for treating TBI patients.
IOM (2011): Most Promising Research Recommendations
Update: there have been no human trials to date and currently there are not any human trials in the process of evaluating the effects of creatine and concussion/mild TBI.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 14 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Recommendation 13-1:
DoD should conduct animal studies that examine the effectiveness of pre-injury and post-injury oral administration of commercial purified n-3 fatty acids on TBI outcomes.
As fish oil decreases inflammation within hours of continuous administration, human clinical trials that investigate fish oil as a treatment for TBI are recommended.
Continuous enteral feeding with a formula containing fish oil should provide equivalent effects for this purpose in the early phase of severe TBI when enteral access becomes available.
IOM (2011): Most Promising Research Recommendations

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 15 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Omega-3 update
Currently, there are 3 double-blind randomized control trials examining DHA supplementations and concussions.
East Carolina University – 62 NCAA division 1 athletes supplemented with 2200 mg of DHA for 30 days after onset of a concussion and measured the number of days to full, unrestricted participation and the number of days for balance and cognition to return to baseline. Study ended July 2017, with no preliminary data to share (1).
University of Texas Southwestern Medical Center – kids ages 14-18 years supplemented with 2 g of DHA daily for 12 weeks and measuring the time to return to competitive play and resolution of balance impairment. Study is expected to end June 2018 (2).
University of Michigan – the OPTIMA-TBI Pilot study will enroll 50 adult subjects with mild TBI to receive 6 g DHA+EPA for one month followed by 1.2 g DHA+EPA for two months. Capsules contain fish oil 1000 mg (contains 500 mg DHA & 100 mg EPA) or placebo. Study is expected to end July 2019 (3).
Sources:1. http://clinicaltrials.gov/show/NCT018145272. http://clinicaltrials.gov/show/NCT019035253. http://clinicaltrials.gov/show/NCT03345550

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 16 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Recommendation 16-1:
• DoD should conduct animal studies to determine the best practices for zinc administration after concussion/mild, moderate, and severe TBI, such as determining the therapeutic window for Zn administration, the length of treatment time for greatest efficacy, and the optimal level of Zn to improve outcomes.
• These trials should also evaluate concerns about Zn toxicity and overload.
• Results should be used to design human clinical trials using Zn as a treatment for TBI.
IOM (2011): Most Promising Research Recommendations

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 17 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Zinc update
Preclinical studies indicate that after an initial period of total parenteral nutrition, dietary Zn supplementation of 22 mg/day using Zn-gluconate significantly increases visceral protein mass in post-TBI patients, is associated with improved GCS’s, as well as mortality decrease from 26% to 12% (1).
With the recommended upper limit of dietary Zn being 40 mg/day, further clinical studies will clearly define the optimal doses/timing to improve post-TBI deficits and prevent neurotoxicity and undesired effects to other organs (2).
Sources:1. Cope et al. 2012 Improving treatments and outcomes: an emerging role for zinc in TBI. Nutr Rev. 70: 410-32. Zhu et al. 2007 Alterations of pulmonary zinc homeostasis and cytokine production following TBI in rats. Ann Clin Lab Sci. 37: 356-61

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 18 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM (2011): Other Research Recommendations
Recommendation 7-1: DoD should consider a clinical trial with TBI patients using an array of antioxidants in combination (e.g. vitamins E and C, selenium, beta-carotene).
Recommendation 11-1: DoD should conduct animal studies to examine the specific effects of ketogenic diets, other diets (e.g. structured lipids, low-glycemic index carbohydrates, fructose), or precursors of ketones bodies that affect energetics and have potential value against TBI. Results from these studies should be used to design human studies with these various diets to determine if they improve outcome against severe TBI.
Recommendation 14-1: Based on positive outcomes in animal models of TBI with curcuminand resveratrol, DoD should consider conducting human trials. In addition, other flavonoids(e.g. isoflavones, flavanols, epicatechin, theanine) should be evaluated in preclinical models.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 19 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Curcumin (Turmeric) update
Animal-based studies have shown that supplementation with curcumin before sustaining a concussion resulted in improved balance as well as transduction and monitoring of cellular energy compared with controls (1).
Supplementation with curcumin after a concussion has been shown to improve membrane function, restoration of homeostasis, neuronal plasticity (2), synaptic plasticity, and neuronal signaling as well as significantly reduced neural inflammation by decreasing the levels of microglia and macrophages that aid in neuronal apoptosis (3).
However, there have been no human trials to date and currently there are not any human trials in the process of evaluating the effects of curcumin and concussion.
Sources:1. Sharma et al. 2009 Dietary curcumin supplementation counteracts reduction in levels of molecules involved in energy homeostasis after brain trauma. Neuroscience. 161:1037-44.2. Sharma et al. 2010 A pyrazole curcumin derivative restores membrane homeostasis disrupted after brain trauma. Exp. Neurol. 226:191-9.3. Zhu et al. 2014 Curcumin attenuates acute inflammatory injury by inhibiting the TLR4/MyD88/NF-κB signaling pathway in experimental TBI. J. Neuroinflammation. 11:59.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 20 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Resveratrol update
The two animal studies evaluating resveratrol in regard to treatment of concussions report that supplementation with resveratrol after a concussion increased cell survival by suppressing autophagy and apoptosis that are mediated by a pathway induced by glutamate toxicity (1) as well as improve motor performance, visual spatial memory, and behavior (2).
University of Texas Southwestern Medical Center - the REPAIR study evaluated the use of 500 mg resveratrol in 30 boxers who have sustained a mild to moderate concussion. The study was a double-blind, placebo-controlled RCT measuring cognitive performance with ImPACT testing and axonal injury via MRI. This study has been completed, but not published (3).
Sources:1. Lin et al. 2014 Resveratrol protects astrocytes against TBI through inhibiting apoptotic and autophagic cell death. Cell Death Dis. 5:e1147.2. Singleton et al. 2010 Resveratrol attenuates behavioral impairments and reduces cortical and hippocampal loss in a rat controlled cortical impact model of TBI. J. Neurotrauma. 27:1091-9.3. http://clinicaltrials.gov/show/NCT01321151

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 21 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM (2011): Other Research Recommendations
Recommendation 15-1:
Conduct more animal studies to determine if vitamin D enhances the beneficial actions of progesterone in the treatment of TBI.
If this synergistic effect is confirmed in animals, then studies in humans should be conducted to evaluate the extent to which vitamin D supplementation might improve the efficacy of progesterone treatment.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 22 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Vitamin D3 update
Vitamin D deficiency
↑ IL-6 ↓ Testosterone
↑ PTSD symptoms↑ mTBI severity
↑ Post-concussive symptoms
Source: Wentz (2014) Vitamin D status may affect resilience and recovery from mild TBI in Military personnel. Austin J Nutri Food Sci. 2:1030.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 23 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Clinical studies using vitamin D
By itself, vitamin D has not shown great promise for TBI, though in combination with progesterone, there are some promising results.
In rodent studies, the combination of progesterone and vitamin D showed significantly reduced neuronal loss & proliferation of reactive astrocytes after a TBI (1).
In the two human-based Phase II studies, the combination of progesterone and vitamin D in patients with sTBI resulted in significantly improved Glasgow Outcome Scale scores, a better recovery rate (2), and a greater efficacy in reducing neuroinflammation (3).
However, the ProTECT (Progesterone for the Treatment of TBI) and SyNAPse (Efficacy and Safety Study of Progesterone in Patients with Severe TBI) trials were large Phase III clinical trials that were SUSPENDED due to lack of efficacy.
Sources:1. Tang et al 2013 Progesterone and vitamin D: Improvement after TBI in middle-aged rats. Horm. Behav. 64:527-38.2. Aminmansour et al. 2012 Comparison of the administration of progesterone versus progesterone and vitamin D in improvement of outcomes in patients with TBI: A randomized clinical trial with placebo group. Adv. Biomed. Res. 1:58.3. Tang et al. 2015 Progesterone and vitamin D combination therapy modulates inflammatory response after TBI. Brain Injury 29: 1165-74.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 24 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
IOM (2011): Future Update of Evidence-Based Guidelines
Recommendation 2-1: Evidence-based nutrition guidelines specific to severe TBI should be updated. Guidelines should address unique nutritional concerns of severe TBI when different from
generic critical illness nutrition guidelines (e.g. meeting energy needs and benefits of specific nutrients, food components, or diets).
Current guidelines to manage mild and moderate TBI should include recommendations for nutritional interventions. The guidelines should be developed in collaboration with the various key stakeholders (e.g. American Dietetic Association, Department of Veterans Affairs, DoD).

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 25 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Common mTBI/Postconcussive Symptoms
• Headache • Poor concentration• Memory difficulty • Irritability• Fatigue • Depression• Anxiety • Dizziness• Light sensitivity • Sound sensitivity
• Immediately post mild TBI, 80-100% describe one or more symptoms
• Most individuals return to baseline functioning within a year
Source: Ferguson et al. 1999, Carroll et al. 2004; Levin et al. 1987
Research Gaps:
• The interventions should be selected to address symptomology;
• Combination nutrients may be more effective than single-nutrient interventions.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 26 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Objectives
Defining the problem IOM 2011 RecommendationsNutrient Interventions for TBIMedicinal Food vs. Nutriceutical

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 27 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Number of clinical trials initiated over the past 30 years, differentiated by studies of neuroprotective agents (n=24) vs. therapeutic strategies (n=13)
Why no pharma?

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 28 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Medicinal Food vs. Nutriceutical
Variability of active ingredients: only 1/3 of vitamin D supplements tested met the US Pharmacopeial Convention standards requiring pills to contain between 90-100% of the active ingredient. Active ingredients ranged from 9% to 146% (1).
Inconsistent recommendations: the benefits of n-3 intake have resulted in intake recommendations ranging from 250 to 500 mg/d from various professional organizations, including the AHA and the International Society for the Study of Fatty Acids & Lipids (2). Current estimates of dietary DHA and EPA intake for Americans are 90–120 mg/d for females and males aged ≥ 20 y, which is less than 50% RDA.
Sources: 1. LeBlanc et al. (2013) Over-the-counter and compounded vitamin D: is potency what we expect? JAMA Intern. Med. 173:585-6.2. USDA, ARS. Nutrient intakes from food: mean amounts consumed per individual, by gender and age. What we eat in America, NHANES 2009–2010. Available from: www.ars.usda.gov/ba/bhnrc/fsrg

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 29 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Summary of Nutrition for TBI, based on site of injury
Parietal LobeNutrition: currently unknown.
Occipital LobesNutrition: currently unknown Anterior Cingulate Gyrus
Nutrition: increase B-6, B-12, vitamin D3, magnesium, DHA, inositol.
Limbic SystemNutrition: B-6, magnesium, folate, zinc, vitamin C, DHA.
Temporal LobesNutrition: increase protein intake, B-6, magnesium, folate, zinc, copper, DHA, vitamin D3, vitamin C, bifidobacterium.
Prefrontal CortexNutrition: avoid gluten, increase protein intake, B-6, magnesium, folate, zinc, copper, DHA, vitamin C, probiotics.
Source: Swanson (2017) The best supplements for concussion recovery. Available from www.thehealthbeat.com

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 30 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
Conclusions
The chronic neurological deficits of TBI are complex and clinical treatments are limited. Several clinical trials have failed because heterogeneous TBI patients
with a wide range of injury severities were grouped together in the same studies. Ongoing failure of clinical trials for TBI treatment has questioned the
direction of therapy. Combination therapies of dietary supplementation and pharmaceutical
agents are likely to yield the best results.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-18Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email addressAngus Scrimgeour PhD (508) 233-5155 2-3 APR 2018Slide 31 of 30UNCLASSIFIED//FOUO
UNCLASSIFIED//FOUO
mTBI is a significant source of morbidity in deployed U.S. service members. No in-field ration component exists to enhance recovery from cognitive, sensory or motor deficits following exposure to mTBI.
Dietary
Supplementation
Dysregulated Neurogenesis in Hippocampus
mTBI
IED
CognitionDeficits
•Hypothesis: Pre-injury and/or post-injury dietary supplementation will improve resiliency to concussion/mild TBI, and post-concussive syndrome.
Extra slide: The Problem – as we see it