Embed Size (px)
Citation preview

POSTGRAD. MED. J. (I962), 38, 695
Clinico-pathological Conference
TRAUMATIC ISCHAEMIAA Saturday Forum held at the Western Infirmary, Glasgow, on Saturday, May i9, I962Chairman: Professor I. A. Donald, M.B.E., B.A., M.D., M.R.C.S., F.R.C.O.G.
Editor: H. I. Tankel, M.D., F.R.C.S., F.R.F.P.S.G.
PROFESSOR DONALD: Ladies and gentlemen, to-day we are going to deal with a research projectwhich opens up an enormous field of therapeuticpossibilities, particularly in traumatic surgery.There are, of course, many uses other than thoseto be discussed today.* We in our own departmenthave benefited from the treatment of the respira-tory distress syndrome, hyaline-membrane atelec-tasis, of the newborn, while the treatment with thepressure chamber of carbon monoxide poisoningis well known.Today Mr. Smith is going to talk about
traumatic ischlemia and it therefore gives me thegreatest pleasure to introduce him.MR. G. SMITH: Traumatic surgery is becoming
more and more important as the incidence ofroad casualties rises. In many instances we feelthat oxygen therapy has something to offer in themanagement of these cases. Let us consider, forexample, the question of diminution of the bloodsupply to a limb. Normally the resting limb tissuesthemselves do not have a very high metabolic rateand they can get on with very much less bloodflowing through them than ordinarily is the case.However, the margin between viability and non-viability of a limb, differing as it does between itsvarious components, may be improved by extraoxygen. The basis of treatment in a pressurechamber is now fairly well known. The extra-cellular fluid is the end reservoir for the availabilityof oxygen to the individual cells. Under normalcircumstances, while breathing air at atmosphericpressure the level of this extracellular fluid oxygenis about 0.25 volume %. By breathing oxygenat two atmospheres pressure we can push this upto about 4.2 volumes % regardless of what thehaemoglobin is carrying. This, you will appreciate,is a very marked increase, which goes far to com-
* See' Treatment of Arterial Occlusion under Oxygenat Two-Atmospheres Pressure ' by Sir Charles Illing-worth, Brit. med. Y. (1962), ii, 1271.
pensate for a diminished arterial input. Further-more, this increase of oxygen in solution shouldbe regarded as occurring in the whole aqueousphase of the body so that we may in point of factput oxygen directly into skin floating on a plasmaexudate and thereby keep it alive.
So far we have treated eight cases of traumaticischamia in a pressure chamber, including twocases from the Southern General Hospital, onefrom Dundee and one from the Vale of LevenHospital, Dumbarton. First, we have two cases ofcompartmental compressions in a limb, one in anupper limb and one in a lower limb. Here thegenesis of the ischamia has been trauma causingmuscle damage and swelling within rigid osteo-fascial compartments with compression of thenerves and blood vessels therein, producing distalischlimia. Secondly, there is a case of nearavulsion of the foot which was sewn back, theposterior tibial artery reconstituted, and much ofthe foot kept alive. Thirdly, we have an exampleof a degloving injury about which Mr. Sillar willspeak. Fourthly, we have a case of cold injuryreferred from Mr. A. B. Kerr's ward with whichDr. Ledingham will deal. Fifthly, apart from theischemic aspect of trauma we have an example ofthe hazard from clostridial infection which occursparticularly in road accidents. Sixthly, there is thetreatment of shock, and we have an example of agirl with multiple injuries in the lower limbs andpelvis and a rupture of the left kidney who neededmassive transfusions. She was transferred fromthe Vale of Leven Hospital with her blood pressurestill down about 8o mm. Hg, and she respondedvery rapidly to treatment in the chamber. And,finally, we have a man who was run over by arailway truck and had a traumatic amputation ofthe foot. Mr. Brown did a Syme's amputation.The heel flap was very dubiously viable and he wastreated in the chamber with the retention of thatflap.
by copyright. on January 1, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.38.446.695 on 1 Decem
ber 1962. Dow
nloaded from

696 POSTGRADUATE MEDICAL JOURNAL December I962
Compartmental CompressionThe first case I wish personally to present is
that of a boy aged 26 who sustained a tibio-fibular diastasis with fracture of the fibula at arugby game in Dundee on November 4, I96I.The fracture was reduced and cross-screwed andat that time there was no suspicion that the bloodflow to the foot was anything other than it shouldbe. But two days later and more especially on thethird day it was quite obvious to both Mr. Smillieand Professor Douglas in Dundee that the bloodsupply to the foot was severely impaired. He wassent here and was seen by Professor Barnes andmyself who concurred with the opinion that theleg was not viable. At that time it was grey, coldand insensitive and there were no peripheralpulses.
Immediately after arrival he was put in thechamber and was kept there for four days, thepressure being allowed down for an hour every I2hours. Compression was in compressed air whilethe patient breathed oxygen through a B.L.B.mask. The foot gradually became pinker over-night and the interesting thing which has beencommon to all these ischaemic cases is that thepain disappeared. With restoration of the circula-tion, bulla appeared over the foot and over theanterior fascial compartment which was tense andexquisitely tender (Fig. i). Tension was alsobuilding up in the posterior compartment. Now,of course, at this stage, one would be tempted toopen the compartments but this almost certainlywould have resulted in muscle pouring out and sowe continued with the hyperbaric oxygen treat-ment. By the end of the next week when he wastaken out of plaster for check X-ray it was quiteobvious that there was still residual tension alongboth the anterior and the posterior osteofascialcompartments. Further, on testing, he had nofunction at all in his anterior or posterior tibialnerve components but did have functioningcutaneous components, both saphenous andmusculo-cutaneous nerves. The small muscles ofthe sole of the foot were probably also partlyinfarcted. Fig. 2 shows the leg at the end of thesecond week and you can see that all the cedema isgone but that there is a small area of full thicknessloss on the dorsum of the ankle. The nervefunction remained fairly stable.On January i8th I put on a little skin graft and
did an arteriogram at the same time which showeda completely normal pattern right down past thearea of injury to the ultimate ramifications. Thisconfirmed the clinical impression that this manhad suffered ischamia from the building up oftension in the osteofascial compartments throughwhich the nerves and vessels were running andthat this had placed the foot in jeopardy. He also
went through a phase where the small bones ofthe foot rarified patchily but they have nowrecalcified satisfactorily, again suggesting anischaemic episode which has been adequately
-. :f:...
FIG. I.-Ischaemic foot one dayafter treatment in the cham-ber with bullee over the dor-sum of the foot and alongthe anterior fascial compart-ment.
.. ... ....:e
FIG. 2.-The same foot as inFig. i at the end of thesecond week showing full-thickness skin loss on thedorsum of the ankle but nocedema.
compensated for. There is still no function in theanterior tibial nerve component so that it mayconceivably have suffered actual physical traumaas well as ischaemic damage at the time of injury.The posterior tibial components are migrating
by copyright. on January 1, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.38.446.695 on 1 Decem
ber 1962. Dow
nloaded from

December I962 Traumatic Ischcemia 697
downwards and have reached the heads of themetatarsals. The saphenous, sural and musculo-cutaneous nerves have stayed intact throughout.He is now walking, and indeed walked down theaisle about four weeks ago.
Near Avulsion of the FootMR. J. STEVENS: The second patient we wish
to present this morning is a i6-year-old youthwho was admitted to the Casualty Department inMarch last year within an hour of being involvedin a motor-cycle accident. He had sustained asevere compound fracture dislocation of the leftankle with anterior displacement of the foot.When we first saw him, the foot was completelywhite and cold with total loss of sensation exceptfor a small area of skin about I.5 cm. in diameterover the lateral aspect of the base of the 5thmetatarsal which was probably subserved by asmall cutaneous branch remaining in a persistentskin bridge which I shall mention in a moment.The soft tissue injury was of an almost circum-ferential bursting type at and just beyond thelevel of the ankle joint. The only intact skinbridge between leg and foot was about 4 cm. wideand situated antero-laterally just beyond the levelof the ankle joint. Immediately proximal to thiswas one of several extensive friction burns andthere was also a 5-cm. laceration over the lowerthird of the anterior compartment of the legthrough which torn muscle had herniated (Figs.3a and 3b). All the tendons in the ankle regionwere intact but the medial collateral ligament ofthe ankle joint itself had been completely tornacross and the lateral collateral ligament was par-tially'divided. Continuity of the posterior tibialnerve remained but extensive haematoma forma-tion within the sheath suggested that it had beenstretched to some degree. The anterior andposterior tibial and peroneal vessels were com-pletely divided with retraction of their torn ends.The initial treatment consisted of the reduction
of the dislocation but this produced no improve-ment in the vascular condition of the foot afterI5 minutes. A formal operation was then em-barked upon. The small leg wound was excisedand the skin loosely sutured so achieving asatisfactory decompression of the anterior com-partment. Inspection of the circumferentialwound showed that only the posterior tibial arterywas suitable for repair and so an end-to-endanastomosis was performed by Mr. Smith. Thisgave a good pulsatile flow of blood into thevessels and resulted in the oozing of blood fromthe distal end of some of the torn veins. After avery limited wound toilet and debridement thewound edges of this circumferential wound wereloosely approximated and the foot was splinted
:..:...:. :. :: .: . :: : E..........
.: ..... :...
..... :.:.: :.:..
.. .. ..-.I.
*,.:::..:..lI...
........,,..........
..
.......
,.'. .. , ...... '.'.'
FIGS. 3a and 3b.-Medial and lateralaspects of foot in a case of nearavulsion showing the extent of skinlaceration and the presence of fric-tion burns.
at right angles on a well-padded piece of Kramerwire. The use of anticoagulants was obviouslyprecluded but the venous outflow from the footwas allowed to drain into the dressings, theestimated blood loss being replaced by transfusion.Four hours after injury the patient was trans-
ferred to the pressure chamber where he breathedoxygen at 2 atmospheres pressure for I2 hours.For the next 8o hours similar treatment was givenfor progressively shorter periods at increasing timeintervals. Skin temperatures were taken andshowed that though the injured foot did notreach the temperature of the normal foot it wasnevertheless considerably higher than the tem-perature of the chamber.
After the patient had been in the chamber for
by copyright. on January 1, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.38.446.695 on 1 Decem
ber 1962. Dow
nloaded from

698 POSTGRADUATE MEDICAL JOURNAL December I962
FIG. 4.-Five days after near-avulsionof the foot with gangrene confinedto the tips of the toes.
about 3 hours the foot became pink and remainedso for about 40 hours afterwards. The change incolour was quite dramatic and there was a slug-gish skin circulation. During periods of decom-pression, however, when normal air was beingbreathed, the condition of the foot deterioratedand it became cyanotic again. Forty-three hoursafter the transfer of the patient to the chamber theooze into the dressings stopped and the toes be-came dusky and congested in spite of furtherintermittent pressurization and high-pressureoxygen. This suggested that the torn veins hadnow thrombosed. A venous obstruction type ofgangrene followed which was confined to the toes.Fig. 4 shows the condition of the foot five daysafter injury with gangrene largely confined to thetips of the toes although the toes as a whole weresomewhat iscbimic. A formal amputation wascarried out through the tarso-metatarsal jointsat which free bleeding was noted at the line ofsection. Healing after this amputation wassatisfactory.
Today, over a year later, the patient is here foryou to see. He has some ankle stiffness which ismore prominent in the mornings and this is notsurprising with this type of fracture dislocation.He also has a little residual hyperwesthesia of theskin of the stump but manages to wear a boot, theforefoot of which is padded with cotton wool. Heis left with end-weight-bearing, earth feeling,normal sensation to the heel and a good heel pad,and this is better than the below-knee amputationthat he would have had without the services ofthe pressure chamber. Furthermore he is at work.At this point the patient was presented.
FIG. 5.-Extensive degloving injury ofleg in a girl of 13. The skin over thesole of the foot was also mobileapart from a tenuous attachmentof the heel pad.
Extensive Degloving InjuryMR. W. SILLAR: This is the story of a 13-year-
old schoolgirl who ran out of school at 12 noonon November 29, I96I, and was knocked downand run over by a lorry. She had a deglovinginjury of one forearm and both legs but only onthe right foot was the circulation impaired. Onthis side the skin was degloved almost completelyfrom midcalf to toes so that a hand could bepassed freely between the skin and deeper struc-tures all the way round the calf and the ankle. Theskin on the heel and the sole of the foot was alsomobile though the heel pad had a tenuous attach-ment and an instrument could be passed betweenthe skin of the sole and the muscles of the footwhich were also grossly damaged (Fig. 5). Thetoes were white and there was no sensation inresponse to pin prick or light touch on either thetoes or the foot. She required resuscitation withI pt. of plasma which were followed by 5 pt.of blood. When the anxsthetic was startedabout 3 p.m. her toes became grey in colourhaving been quite white until then. The skin waslargely defatted, replaced and sutured so thatthere was a nearly linear suture line from the calfto near the big toe. The dead space under theskin was then emptied by gentle compressionwith wool and plaster and the patient returned tothe ward.At 6.30 p.m. the toes were still quite cold and
grey and without any apparent circulation and socontact was made with Mr. Smith and the childadmitted to the pressure chamber in the evening.The toes became patchily pink in the chamber but,in the morning, IO to I5 minutes after decom-
by copyright. on January 1, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.38.446.695 on 1 Decem
ber 1962. Dow
nloaded from

December I962 Traumatic Ischamia 699
-.::
| L.::| l lL| l N ||-| | |Wd l |
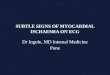
FIG. 6.-Feet of an elderly woman threehours after being admitted as a resultof prolonged exposure to cold. Thecedema and skin discoloration areclearly seen.
FIG. 7.-Residual area of skinnecrosis three weeks after coldinjury, which healed spon-taneously.
pression, became quite blue, quite cold and quitewithout sensation. Periods of pressurization wererepeated and with this it was noticed that theperiods of patchy pinkness became longer.Sensation returned about the second day. Bythe fifth day it was possible to leave the child outof the chamber, the foot remaining a dull duskypink rather than the previous blue colour. Therewas also a little warmth in the toes.She returned to the Southern General Hospital
about this time with extensive skin loss whichrequired skin grafting. She has now left hospitaland returned to school. She walks fairly well,though curiously enough the foot which showsmost swelling at the moment is the left one. At
about io days there was shedding of a completecast of skin of the toes as happens sometimes afterscarlet fever. Underneath was supple; pink, warmskin. At this point the patient was presented.
Cold InjuryDR. I. LEDINGHAM: This is the history of a
44-year-old woman of a vagrant disposition whospent one of the coldest nights last Decembersleeping on a bench in Kelvingrove Park. Herleft fifth toe had been amputated in the RoyalInfirmary following exposure in the winter ofI960. On this occasion she was admitted to Mr.A. B. Kerr's unit and found to have a cold, blue,insensitive left forefoot with bluish-black mottlingof the skin. The right forefoot was also affectedbut to a lesser degree and all the pulses werepalpable. On the left side only the-femoral andpopliteal pulses were palpable but the pedal pulseson this side may have been obscured by cedema.Fig. 6 shows the condition of both feet two tothree hours after admission showing the area ofskin discoloration on the left foot, a similar areaof skin demarcation over the right foot and on thesole.
Six-hourly heparin was instituted immediatelyand the patient transferred to the pressure cham-ber. Within two hours only the tip of the fifthtoe of the right foot remained cyanosed and somesensation had returned to the left forefoot. At theend of the next hour pinkness appeared over thelateral border of the left forefoot and later on thatsame evening only the left third and fourth toesremained doubtfully viable. Later some blisteringappeared over these two toes. Pressure-chambertreatment continued throughout that night andduring the next two days with continuing steadyimprovement until at the end of the third daytreatment had to be terminated prematurely toallow another patient into the chamber. At thisstage there was an area of skin necrosis on thelateral plantar aspect of the left forefoot about thesize of a half-penny and some skin blistering overthe left third and fourth toes. Fig. 7, taken threeweeks later, shows this area of skin necrosis,the rest of the toes and distal part of the foothaving become practically normal. Thereafter, thepatient was returned to the ward and, apart fromtwo short periods of pressurization, was treatedwith anticoagulants and local dressings. Thecedema settled quickly and the left dorsalis pedispulse became palpable shortly thereafter. Thepatient has attended outpatients several times andwhen seen two weeks ago had a tiny healing skinlesion as the only residuum of the original coldinjury. This has given her no trouble at all andno grafting was required.
I would like to draw your attention to two points
by copyright. on January 1, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.38.446.695 on 1 Decem
ber 1962. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
of interest, firstly the rapidity of improvement inthe pressure chamber and, secondly, the fact thatwe have been able to avoid any form of amputationor skin grafting.
DiscussionPROFESSOR DONALD: Dr. Richards, you have
had a lot of experience of this sort of case, wouldyou care to say anything?
DR. R. L. RICHARDS: Yes, thank you. I think thatthis question of cold injury is extremely interest-ing. There is probably less evidence here than inthe other cases, however, that the results have beendue to the pressure chamber. It is natural in coldinjuries for the patients to go through a phase ofextreme hyperamia once they are in the recoveryphase and I would be doubtful whether what Dr.Ledingham has shown us is any different fromwhat would be expected during the hyperxmicphase of a cold injury of this degree.
It is extraordinary how little we really knowabout the pathogenesis of cold injury to peripheraltissues. There have always been two schools ofthought; one, that it is the cold itself that pro-duces the injurious effect, and, the other, that thisis entirely a vascular reaction. The evidence thatthe injuries are due to cold itself is becoming lessand less as time goes on. It is now pretty evidentthat you can chill not only tissues but wholeliving organisms down to extremely low levels andrevive them without any evidence of tissue damagewhatsoever. The general impression now is thatcold injury is a vascular reaction associated withchilling or extreme cold in part of an organismthe rest of which is alive and in which the circula-tion is active. The exact role of anoxia in this isagain in doubt. During World War II, and since,the Americans found that anoxia certainly pre-disposes people to severe cold injury. At onestage in the war they ran into a very bad phase ofcold injuries in their high-altitude pilots, and theyfound thiat this improved considerably when theyprovided additional oxygenation for these peoplewithout any other alteration in the environmentin which the injuries occurred. There is, therefore,no doubt that anoxia is an important factor, andtherefore any attempt- to get additional oxygen tothe tissues is to be commended. I think that theproblem often is that, although the oxygen is thereall right, the tissues cannot use it because they arechilled down to a level below which oxygenutilization fails to occur, so that, even ifyou provideadditional oxygen in the blood and in the extra-cellular fluid, it is sometimes ineffective. Never-theless the provision of oxygen to the extracellularfluid is very important because cold injury isundoubtedly associated with much exudation of
fluid from the damaged small vessels, consistingnot only of ordinary extracellular fluid but also ofserum and even some blood cells. If you can getmore oxygen into this fluid which is actually bath-ing the tissues then at least it has an opportunityto produce a beneficial effect. One would like tohave the opportunity in a patient who has twolimbs affected of putting one foot in an individualpressure chamber and use the other as a control,but this is not a possible experiment as the oxygenwould get into all the tissues and you would beunable to separate one foot from the other.
PROFESSOR DONALD: Thank you very much,Dr. Richards. Another application of the pressurechamber which Mr. Smith mentioned is itsinfluence on anaerobic bacteria. Have you anyviews on this, Dr. Scott?
DR. A. C. SCOTT: Increasing the oxygen poten-tial in the tissues is obviously important in thetreatment of anxrobic infection. Even whenthe anerobes have gained a foothold in the tissuestheir ability to flourish will be cut down, though Ithink it is important to remember that low oxygentension is not the only factor which allowsanerobic infection to occur in tissues. It is veryimportant that these organisms which are veryactive biochemically and produce a large numberof very potent exotoxins should not be given achance to break down devitalized and necroticmuscle and to release their toxins. Low oxygentension, of course, is not the whole answer and theuse of the chamber in anacrobic clostridial infec-tions is only an extension of the other methods ofincreasing oxygen tension which have been advo-cated in treatment, such as local application ofoxidizing agents or even the direct injection ofoxygen into the tissues at the site of the infection.It is probably a very important supportive methodof treatment but cannot and obviously should notbe expected to take the place of excision of muscle,removing dead tissue which provides the idealnidus for the infection, and the use of antitoxinsand antibiotics.
DR. S. FLETCHER: We very often tend to forgetthat there are two sides to infectious disease, firstthe ability of the organism to grow, and secondlythe ability of the defences of the body to deal withthe infection. It may well be that increased oxygentension in the tissue causes the phagocytes to goabout their activities with a little more gusto. Thisidea would be amenable to experimental observa-tion and I wonder if any work has been done onthis-perhaps Mr. Smith could tell us.MR. SMITH: No, I know of none. Most of the
work on clostridial infections has been done withBrummelkamp working in Boerema's laboratory.I think that it has been done mainly by the assess-ment of the survivdl of guinea pigs to a standard
December i962700by copyright.
on January 1, 2022 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.38.446.695 on 1 D
ecember 1962. D
ownloaded from

Traumatic Ischcemia
dose of Clostridium welchii and has not beenrelated to the phagocytic activity.
DR. S. FLETCHER: I think it would be somethingwell worth looking into. It would be relativelysimple to do in vitro.MR. SMITH: I quite agree.PROFESSOR DONALD: Are you suggesting that if
you had a case of overwhelming clostridial infectionthat this treatment alone might help to assistphagocytosis? It seems to me to be an entirelyreasonable suggestion because operative interven-tion at this stage is completely out of the question.
DR. SCOTT: I think this question might possiblybe more easily solved than one might think. It issaid to be characteristic of the effluent from atypical case of gas gangrene that there are very fewpolymorphs in it, because they are rapidly killed bythe toxins produced by the clostridia. If a patientwith typical gas gangrene, clinically and bac-teriologically, was treated with oxygen and foundto have a very purulent exudate this would beevidence that increased oxygenation was helpingphagocytosis and that the phagocytes are able toresist the clostridial toxins a little more readily.
PROFESSOR DONALD: I think that both intraumatic surgery and in septic abortion theremight be a future in this. It should certainly beborne in mind. I remember from my experiencesduring the last war the prophylactic amputationswe used to undertake for infected wounds in theabsence of penicillin or other antibiotics. If thiskind of treatment could be made sufficientlyavailable on the field, it could make quite a lot ofdifference in the conservation of both limb andlife. I would be rather interested to hear what theorthopwedic surgeons have to say about the futureof this in conservative surgery.MR. STEVENS: If I may say a word as a repre-
sentative of the Orthopledic Department. Youhave heard of the application of oxygen underpressure in the treatment of injuries of varioustypes and we have experience of many other cases.I think it has an even wider application than hasalready been said because we have got to bear inmind that we are dealing not only with viability ofskin and muscle and nerve but also with theviability of bone which is a very tenuous thing inmany respects, particularly in the adult. The bonecell itself is in a precarious position buried in apiece of solid bone tissue and if it happens to bemore than one-tenth of a millimetre away from auseful capillary then it is likely to die. So it isquite clear that extensive anoxia of bone couldcause extensive death of bone and in this regard itmay be that in the future we will see a moreextensive application of this technique in, forexample, the investigation of avascular necrosis of
bone such as follows fracture of the neck of afemur.Another important application is in Volkmann's
isckiemic contracture which is not very commonnowadays but is obviously an outstanding candi-date for this sort of treatment. Yet another onewhich is terribly important and does have somerelationship to hyaline membrane disease in thepremature newborn is fat embolism. This com-plication occurring 48 hours after injury can be ofthe pneumonic or of the systemic type. Quiteclearly both of these types of fat embolism arevery strong candidates for treatment by oxygen ata pressure of 2 atmospheres and we are justwaiting for an opportunity to try it.MR. A. D. Roy: What measurements, if any,
have been made of tissue oxygen in these cases?MR. SMITH: As far as available instruments in
this area are concerned it is possible but by nomeans easy to do tissue oxygen. We haven't donethis-I only wish there was a more easily availablecheap apparatus for doing it.
PROFESSOR DONALD: No one has mentioned thequestion of burns yet. I would like to ask Mr.Smith if this kind of treatment might in any wayassist in the treatment of major burns?MR. SMITH: We have not had the opportunity
to treat any of these cases. Possibly in certaincases of marginal viability of skin, some skin diesunnecessarily from the action of hyperanmicexudation fluid. One could imagine that thechamber could have some effect on this but wehave not had any opportunity to test this. It wouldbe a reasonable proposition.MR. G. H. PARKER: Does the prolonged in-
crease in oxygen tension have any adverse effecton brain tissue or on the cerebral circulation suchas producing oxygen convulsions and so on?MR. SMITH: We have almost two years' ex-
perience of this chamber now without anyevidence of oxygen toxicity but then we are using2 atmospheres pressure and this is probably wellwithin the safety limits. Mr. Jacobson, a neuro-surgeon, is here and he might be able to elaborateon this. We have not seen it.MR. I. JACOBSON: If you do cerebral blood
flows with the nitrous oxide method or with anyof the more accurate radio-isotope methods, thenby getting the patient to breathe pure oxygen andusing the simple relationship between blood pres-sure, blood flow and peripheral resistance you willfind a io to I5% increase in cerebro-vascularresistance-this has no effect on the patient. Nowwhen this is done under a pressure of 31 atmo-spheres the cerebro-vascular resistance goes up-byabout 35% but again the significance of this isdoubtful. However, volunteers breathing pureoxygen at 3_ atmospheres did encounter difficulties
December i962 701by copyright.
on January 1, 2022 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.38.446.695 on 1 D
ecember 1962. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
and did have oxygen toxicity. It is interesting thateven at that high pressure level the arterio-venousoxygen difference between samples from thejugular bulb and the internal carotid arteryincreases-the explanation for this is difficult.
DR. A. FAIRLEY: Mr. Chairman, I would liketo ask Mr. Smith if he is of the opinion that it isworth while putting patients on oxygen with aB.L.B. mask as a temporary measure in theabsence of a pressure chamber. Are there anycomparative figures which he could perhapsgive us?MR. SMITH: I think that if you admit the
reasonableness of the pressure chamber then thenext best thing is to go on to pure oxygen at iatmosphere. I think the answer is distinctly ' yes '.MR. PARKER: Would there be any place for
intravenous dyes to show if there is circulation inthe affected extremity before putting the patientin the pressure chamber? If there is no communi-cation at all then it would presumably be a wasteof time putting the patient in the chamber.MR. SMITH: Yes, that is true. We have thought
about that but the answer becomes self-evident ina matter of 24 hours or thereby because the skindoes not become pink at all. Obviously this treat-ment is useless unless there is a trickle of bloodgoing in and, most important, the same amountcoming out. An ischemic leg with a venous blockin addition to the arterial disease just will notimprove.
PROFESSOR DONALD: Another obvious field ofapplication here is already being explored inSt. Thomas's Hospital. All malignant tumours arerelatively hypoxic and become more radio-sensitive if you can increase their oxygen satura-tion. In St. Thomas's Hospital there is a differentsort of pressure caisson in which the patient isput in at 4 atmospheres and exposed to the cobaltbomb. The oxygen saturation of the malignanttumour is increased from about 6o to 97% andthis greatly increases its radio-sensitivity relativeto the surrounding tissues. However, they have alot of trouble from cartilage which is an anoxicstructure.MR. H. I. TANKEL: Mr. Smith, do you have any
views on the treatment of non-traumatic ischxmia?Is the chamber of any value in the ordinaryischwmic foot?MR. SMITH: Well, I think that this is a difficult
thing to judge. As far as one can say the vastmajority of patients with isclhamic neuritis doimprove in the tank. This is one observationwhich I think is significant. We now have severalpatients in whom treatment was continued for overa month and in whom the ischaemic neuropathyhas subsided enough to allow the patient to carryon his everyday existence with the limb still intact,
where I would have thought previously that theseparticular cases would require a major amputation.We have also tried some five or six patients withindolent thromboangietic ulcers of the foot of upto a year's duration and have healed all these byprolonged treatment in the chamber. Again, wethink this is a positive indication and that somegood is being done. We have the impression thatsome cases who would have required majoramputations have got off with minor amputations.We also have some patients with arterial emboliwhere treatment in the tank has saved a majorpart or all of the limb. All this, as you willappreciate, is a very difficult thing to assess.DR. A. PRINGLE: You say, Mr. Smith, the
oxygen is dissolved in the plasma. When you saythat a limb becomes pink does it mean that theoxygen is being transferred to the hlemoglobin?MR. SMITH: I don't know exactly what the
state of the capillary bed and the small arterioleshas been, but obviously to get a pink skin youmust have enough oxidized hlemoglobin in thecapillary layer, apart from the skin plasma. I ammerely saying that the increased oxygen saturationof the plasma provides a better tension gradientfor diffusing out into the cells at jeopardy fromanoxia. I don't know how much flow you needthrough a limb to give a pink limb. When you arecold, the answer is very little indeed, and one mustnot equate pinkness with flow. Pinkness in the ab-sence ofextreme cooling indicates that there is flow.
PROFESSOR DONALD: But you can also get theoxygen into the cells without the medium oflzmoglobin.MR. SMITH: If you get a foot staying pink
whereas before it was dusky black or blue-blackthen there must be transport of oxygen by theplasma element alone to keep the hlemoglobinfrom reducing.
PROFESSOR DONALD: But obviously there iscartilage at stake too which has survived and thiscould not have been done so through the mediumof hbmoglobin, could it?
DR. RICHARDS: I think that part of the point inthe management of these cases of trauma and ofcold injury is that the toes are blue because thereare red cells which have given up their oxygentrapped in the small cutaneous vessels. Inexperimental cold injuries certainly at this stagethere is still a flow of plasma going on. If you getoxygen into this plasma, it flows into the tissueand the red cells become oxygenated in situ as itwere and this is why they become pink. As thetissue oxygenation improves the major circulationmay restart.MR. PARKER: Are there any contra-indications
to pressure therapy, for example, a patient who haschronic carbon dioxide retention?
December i962702by copyright.
on January 1, 2022 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.38.446.695 on 1 D
ecember 1962. D
ownloaded from

Traumatic Ischa-mia
DR. FAIRLEY: I think one should take measuresto ensure that the carbon dioxide retention wascorrected by the use of buffers and so on andperhaps by the use of adequate respiratorymeasures.
PROFESSOR DONALD: I should have thought thatadequate respiratory ventilation under such con-ditions would have blown off the carbon dioxide.Would this factor of supersaturation with oxygenworry you?
DR. FAIRLEY: Well, it would perhaps produceapncra in the presence of carbon dioxide retentionand one would perhaps have to think of forcedventilation.MR. SMITH: I think what you have in mind is
the type of patient who has chronic emphysemaand you interfere with his carbon dioxide drive.If, however, you are faced with such a patientrequiring this sort of treatment in an emergencyI think you might well carry such a patient throughsuccessfully, if you have adequate biochemicalcontrol in the chamber as, of course, we have.PROFESSOR DONALD: Little has been said this
morning about biochemical control in the chamberbut I can say that in the cases of the respiratorydistress syndrome in infants, there is biochemicalcontrol throughout, coupled with the pressurizedoxygen treatment and one could not have the onewithout the other.MR. TANKEL: I think it is worth while pointing
out that if you happen to be dealing with a patientin whom there is a waterseal drain into the chestyou must clip it off as near the chest as possibleotherwise the fluid in the waterseal drain will bepushed into the chest.MR. SMITH: Yes. There is a lag in stabilization
between the intra- and extra-pulmonary pressuresbut not much and now we can quite easily com-pensate for it by putting on suction via a smallpump on the chest drain, providing the airway isnot blocked.
PROFESSOR DONALD: Well, we've had a mostexciting morning and there are many angles ofthis we can think about for days to come. Wouldyou care to say anything in conclusion, Mr. Smith?MR. SMITH: Thank you. You have heard the
gamut of cases we wish to deal with and nowperhaps just to add a final note to this discussionit is obvious that one should think about a servicewith pressurized ambulances if this treatmentshould become more universally adopted. Glasgownow has its first pressurized ambulance with aportable pressure chamber which can be taken outand left in a hospital for continuing treatment whilea spare is loaded into the same ambulance whichcan then go back on the beat again. This shouldbe of value in the treatment of carbon monoxidepoisoning but its use for transport of patientssuffering from various forms of anoxia is likely tofollow.
December I962 703by copyright.
on January 1, 2022 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.38.446.695 on 1 D
ecember 1962. D
ownloaded from











![Myocardial Ischaemia - national audit project [MINAP] 2011 - UCL](https://img.pdfslide.net/doc/110x75/620349a224f6b61e9c664083/myocardial-ischaemia-national-audit-project-minap-2011-ucl.jpg)