Embed Size (px)
Citation preview

828
A blood smear taken on March 31 had been reported assuggesting leucopenia, with lymphocytes predominating,and retrospective inquiry showed that no polymorphs wereseen. A firm diagnosis of agranulocytosis was not, however,made until April 5, when her total white cells numbered900 per c.mm.After admission to hospital on April 5 treatment was with
penicillin 62,500 units three-hourly ; intravenous pyridoxine300 mg. within, the first twenty-four hours and folic acid100 mg. followed by 20 mg. daily.Within forty-eight hours her temperature had settled and
granulocytes had returned to the blood-stream.A bone-marrow smear, taken ten to twelve hours after
the start of therapy, showed maturation arrest at the
promyelocyte level; no mature granulocytes were seen. Afurther marrow smear, taken just over twenty-four hours
later, showed
granulocytedevelopmentalong normallines.
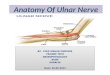
Fig. 2 showsthe time-rela-tion betweentreatment and
improvement.
COMMENTS
These twocases illus-trate thevalue of
penicillin in
maintaininglife duringthe period ofagranulo-cytosis.Pyrexia,however,continuesdespite peni-cillin anddoes notsettle untilpo,lymorphsreappear inthe circula-
ting blood.There is no
a-priori reason to
suspect that
penicillin hasany stimulant action on leucopoiesis, and in both
patients granulocytes had not returned after five days’penicillin therapy. Apart from penicillin, the onlydrug other than folic acid given to both patients waspyridoxine ; in the first patient pyridoxine had beengiven, without response, for three days before folic acidwas added. We realise that spontaneous remission mayoccur at any time in this disease, and that the appearanceof granulocytes within forty-eight hours of giving folicacid to these two patients may have been merely acoincidence. We propose to treat subsequent patientswith folic acid and penicillin alone ; but, since agranulo-cytosis is comparatively rare, others may have an
opportunity of testing the value of folic acid beforeanother case is available to us.
We are indebted to Messrs. Lederle, Inc., New York, forsupply of Folvite.’
Fig. 2-Treatment, temperature, and white-cellcounts in case 2.
REFERENCES
Menten, M. L., Graff, E. (1946) Amer. J. med. Sci. 211, 672.Watson, C. J., Sebrell, W. H., McKelvey, J. L., Daft, F. S. (1945)
Ibid, 210, 463.Wilson, H. E., Doan, C. A., Saslaw, S., Schwab, J. L. (1942) Proc.
Soc. exp. Biol., N.Y. 50, 341.
TRAUMATIC NEURITIS OF THE DEEP
PALMAR BRANCH OF THE ULNAR NERVE
W. RITCHIE RUSSELLM.D. Edin., F.R.C.P.
C. W. M. WHITTYB.M. Oxfd, M.R.C.P.
From the Department of Neurology, Radcliffe Infirmary,Oxford
THE correct diagnosis of the cause of wasting of the-muscles of the hand is clearly a matter of practicalimportance, and in this connexion Russell Brain et al.
(1947) have recently clarified the causes of medianneuritis. We draw attention here to another cause of
wasting of the hand which is in our experience speciallyliable to faulty diagnosis.
Traumatic, occupational, or pressure neuritis of the-ulnar nerve is a relatively common cause of such wasting.In most cases the neural injury occurs either at the-elbow or at the wrist, and injury at these sites can be-distinguished by studying the muscles paralysed and the-extent of the sensory loss.
Injury to the deep palmar branch of the ulnar nerve’may, however, provide a clinical picture quite unlike thatgenerally associated with ulnar paralysis. When, itoccurs without any obvious injury to the hand, thenature of the lesion is apt to be overlooked by the clinician,and indeed there is a danger that motor-neurone disease-may be diagnosed.
Anatomy.—The anatomy of the nerve in the palmis given in Cunningham’s (1937) textbook as follows :
" The ulnar nerve in the hand divides under cover ofthe palmaris brevis muscle into its two terminal branches-superficial and deep. The deep palmar branch is almostpurely motor. It passes deeply between the flexor andabductor minimi digiti ; it supplies these muscles and theopponens digiti minimi, then turning laterally along theline of the deep palmar arch, and under cover of the deep,flexor tendons, it supplies branches to the following muscles : interossei, third and fourth lumbricals, the adductor pollicis,and the deep part of flexor pollicis brevis."
This is its usual anatomy, but it should be borne in mindthat there may be variations. The nerve occasionallysupplies opponens and abductor pollicis brevis ; flexorpollicis rarely has an entirely median supply (Highet.1943) ; and the first two palmar interossei are some-
times innervated by the median (Pollock 1919). Thismay cause some difficulty in interpreting the clinicalsigns of injury.When the deep palmar branch is injured at its origill
without involvement of the superficial branch, themuscles supplied by the ulnar nerve are paralysed withoutsensory loss. Hunt (1914) quotes six cases observedby him in which this occurred. When, however, thedeep palmar nerve is injured after its branches to thehypothenar muscles have been given off, and while
running laterally with the deep palmar arch, the interosseiand adductor pollicis are paralysed but the hypothenarmuscles are unaffected. This isolated muscular paralysiswithout sensory loss constitutes the essential clinicalfeature of the cases here recorded.
’
Case 1.—An R.A.S.C. sergeant, aged 24, reported weaknessof the right hand, with difficulty in writing, which had beenpresent for about 15 days. Some 3 weeks previously he hadridden a motor-cycle with a defective twist-grip throttlefrom Algiers to Sousse, at times over rough and. difficultroads. For 24 hours after completion of this journey he hadnoticed paraesthesia in the little and ring fingers of the righthand. This had cleared spontaneously. During the ensuing3 weeks he had been employed on routine short motor-cyclejourneys. He had noted the weakness when trying to writea letter about a week after his long journey. It appeared to’be increasing.On examination he appeared a healthy rather thick-set man-
The only abnormality in the central nervous system was:weakness and slight wasting in the interossei and adductor

829
pollicis of the right hand ; the hypothenar muscles wereintact, and there was no objective sensory loss.He was put off cycling duties and told to rest the hand as
much as possible. He was seen again some 3 months later.He had only stayed off cycling for about 3 weeks, by whichtime he thought his hand so much better that he resumedfull duty. He now had no disability and no detectable weak-ness, though there was still a slight reduction in the musclemass of the first interosseus space.Case 2.-A Pioneer Corps private, aged 32, reported weak-
ness of the left hand for about 1’ month. He dated the
symptoms from a time when he had been preparing the sitefor a tented camp. For about a week his chief occupationhad been putting tent-pegs into clay soil, pushing them inby hand and then hammering them home. Since then hehad been employed on digging.On examination he had evident wasting of first interosseus
and adductor pollicis, and weakness of all interossei, third andfourth lumbricals, and adductor and flexor pollicis brevis of theleft hand. There was no involvement of the hypothenarmuscles and no sensory loss.He was put on light duty and instructed to rest the hand as
much as possible. He did not report again, but his medicalofficer stated 6 weeks later that he had made no furthercomplaints.Case 3.-A retired civil engineer, aged 61, complained of
weakness of the right hand and difficulty in holding a penfor writing for about 2 months. One evening after a heavyday’s gardening he had noticed painless swelling of the righthand. This had subsided gradually in a few days, and hehad begun to note the weakness which had remained stationarysince then. His gardening activities at the time of onset hadconsisted of breaking up hard clods of earth with a spade,which he held in his right hand and crashed down on the earth.On examination there was weakness, with some wasting, of
all interossei, third and fourth lumbricals, and adductorpollicis of the right hand. The hypothenar muscles werenormal, and there was no sensory loss. No other abnormality.He was advised to rest his hand and to wear a thick glove
to prevent trauma to the palm. A follow-up 4 months latershowed improvement in the weakness and wasting. The
patient, who was an accurate observer, gave a good descriptionof the recovery he noted. At first full power returned tothe little finger (the disability here had been of adductiondue to interosseus weakness) ; next it returned to the middleand index fingers ; and improvement in thumb movementswas slowest. Difficulty in holding a pen for writing haddecreased considerably.Case 4.-A pressed-steel worker, aged 33, complained of
weakness of the left hand for 6 weeks, with wasting for about2 weeks. For the past 2 months his work had involved
straightening dents in various pieces of pressed steel. Forthis he had rested a block of wood on the palm of his left hand,while with his right hand he hammered the dent out againstthe block.On examination there was marked weakness of all interossei,
third and fourth lumbricals, and adductor pollicis, withobvious wasting of first interosseus and adductor pollicis.The hypothenar muscles were unaffected, and there was nosubjective or objective sensory disturbance.He was advised to change his work. When seen again
7 weeks later there was much improvement in weakness andwasting. He no longer noted any subjective disability, andhad changed his job to that of milk roundsman.Case 5.-An insurance agent, aged 48, reported weakness
of the right hand and difficulty in writing, of gradual onset,over the past 3 months. He had a Dupuytren’s contractureof the palm which had been slowly increasing for years but hadnot interfered with his work. During the past 3 months hehad noticed a gradually increasing weakness of the right hand,showing itself particularly in difficulty in holding a pen forwriting. There had also been some wasting of the hand.On examination a Dupuytren’s contracture could be felt and
seen centred mainly over the flexor tendons of the fourthfinger. There was evident wasting of the interossei andadductor pollicis, and weakness of interossei, third and fourthlumbricals, adductor and flexor pollicis brevis. The hypo-thenar muscles were not involved, and there was no subjectiveor objective sensory loss.
In view of a possible constriction of the nerve by fibroustissue, surgical exploration was undertaken by Prof. H. J.Seddon. However, no mechanical obstruction was found to
a seeker passed across the palm in the course of the nerve.Electrical stimulation gave a normal response in branches tothe hypothenar muscles, but none beyond this. Electro-
myograms from the muscles affected showed no evidence offibrillation.
DISCUSSION ’
There are few published reports of this traumatic orpressure palsy of the deep palmar branch. RamsayHunt (1914) does not describe this particular condi-tion, but Harris (1929) gives details of two such cases,one in a bootmaker and one in a cyclist. In the furthercases here described, the connexion between trauma tothe palm of the hand and the onset of the paralysiswas quite definite, but it must be emphasised that carefulinquiry is often needed to elicit the cause of the injury,as the patient is usually unaware that’he has damagedhis hand in any way.The deep palmar branch of the nerve, after turning
laterally in the hand, lies in close relation to the proximalend of the metacarpal bones, and these no doubt
provide a hard surface against which the nerve can becompressedThe obvious treatment, which consists in avoiding the
causes of trauma, is usually successful in allowing recoveryto occur spontaneously.
SUMMARY
Pressure on the deep palmar branch of the ulnar nervemay cause a neuritis. Various occupations can inflicttrauma of this kind.The result is paralysis and wasting of the interossei
and adductor pollicis muscles. There is no sensory loss,and the hypothenar muscles may be unaffected. ,
Recovery usually follows discontinuance of traumato the hand.
REFERENCES
Brain, W. R., Wright, A. D., Wilkinson, M. (1947) Lancet, March 8,p. 277.
Cunningham, D. J. (1937) Textbook of Anatomy, London.Harris, W. (1929) Brit. med. J. i, 98.Highet, W. B. (1943) Lancet, i, 227.Hunt, R. (1914) Rev. Neurol. Psychiat. 12, 137.Pollock, L. (1919) Arch. Neurol. Psychiat. 2, 518.
A CASE OF HICCUPREVIVAL OF AN OLD REMEDY
R. C. NAIRNM.B. Lpool
LATE SURGEON LIEUTENANT R.N.V.R.
Tms case is recorded mainly because of the treatmentadopted, but the aetiology is also worthy of discussion.During operational minesweeping off Malaya a request was
received from another ship for medical attention for a navalstoker who had had hiccup for forty-eight hours. Treatmentwas prescribed, to be carried out in, the rating’s ship till hecould be transferred. He did not respond to the remediessuggested—all old and well-tried methods, such as breath-holding, breathing in and out of a paper bag, traction on thetongue, and eating or drinking such things as sugar andeucalyptus oil (we had no cajuput) or sugar and vinegar.He was transferred for treatment on the same evening,
Sept. 6, when he was found to be truly suffering from hiccup ofan unbelievable forcefulness. He had vomited twice duringthe day, and this was not surprising, from the mechanicaleffect of his spasms alone. He had diarrhoea on this day only.There were no other symptoms, no domestic or other worries,and no relevant past illnesses. He gave a history of a normalpulmogram earlier in the year. His wife had had a pleuraleffusion but was recovering rapidly, and he was not concernedabout her. The patient was 30 years old.On àamination he was well built, reasonably cheerful in
spite of having been hiccupping for the past two and a halfdays, and looked vry fit. There was violent frequent hiccup,with a periodicity of about 30 sec. (This was later noted topersist while he slept.) No pyrexia, pulse normal, tongue cleanand moist. No abnormal abdominal, respiratory, or cardiacsigns ; blood-pressure normal.








![DOI: Journal of Clinical Case Reports...The term “ulnar tunnel syndrome” was coined by DuPont in 1965 to describe the condition of 4 patients with acquired ulnar neuritis [1]](https://img.pdfslide.net/doc/110x75/6085e428a47e3f5d3e52106c/doi-journal-of-clinical-case-reports-the-term-aoeulnar-tunnel-syndromea-was.jpg)